a randomized, placebo-controlled, crossover trial of ...gwallace/papers/wisley et al. (2008).pdf ·...
TRANSCRIPT

AC
BH*C†
‡
C§
�
Tnat
R1SfAoADS1©d
The Journal of Pain, Vol 9, No 6 (June), 2008: pp 506-521Available online at www.sciencedirect.com
5
Randomized, Placebo-Controlled, Crossover Trial of Cannabisigarettes in Neuropathic Pain
arth Wilsey,* Thomas Marcotte,† Alexander Tsodikov,‡ Jeanna Millman,§
eather Bentley,� Ben Gouaux,� and Scott Fishman§
VA Northern California Health Care System, Department of Anesthesiology and Pain Medicine, University ofalifornia, Davis Medical Center, Davis, California.Department of Psychiatry, University of California, San Diego, California.UC Davis/VANCHCS General Clinical Research Center and Department of Public Health Sciences, University ofalifornia, Davis Medical Center, Davis, California.Department of Anesthesiology and Pain Medicine, University of California, Davis Medical Center, Davis, California.University of California Center for Medicinal Cannabis Research, University of California, San Diego, California.
Abstract: The Food and Drug Administration (FDA), Substance Abuse and Mental Health ServicesAdministration (SAMHSA), and the National Institute for Drug Abuse (NIDA) report that no soundscientific studies support the medicinal use of cannabis. Despite this lack of scientific validation, manypatients routinely use ”medical marijuana,” and in many cases this use is for pain related to nerveinjury. We conducted a double-blinded, placebo-controlled, crossover study evaluating the analgesicefficacy of smoking cannabis for neuropathic pain. Thirty-eight patients with central and peripheralneuropathic pain underwent a standardized procedure for smoking either high-dose (7%), low-dose(3.5%), or placebo cannabis. In addition to the primary outcome of pain intensity, secondary outcomemeasures included evoked pain using heat-pain threshold, sensitivity to light touch, psychoactive sideeffects, and neuropsychological performance. A mixed linear model demonstrated an analgesicresponse to smoking cannabis. No effect on evoked pain was seen. Psychoactive effects were minimaland well-tolerated, with some acute cognitive effects, particularly with memory, at higher doses.Perspective: This study adds to a growing body of evidence that cannabis may be effective atameliorating neuropathic pain, and may be an alternative for patients who do not respond to, orcannot tolerate, other drugs. However, the use of marijuana as medicine may be limited by its methodof administration (smoking) and modest acute cognitive effects, particularly at higher doses.
© 2008 by the American Pain Society
Key words: Neuropathic pain, analgesia, cannabis, clinical trial, neuropsychological testing.tinmsonmp
vej(r
he case for the clinical utility of cannabis as an an-algesic derives from experimental studies as well asanecdotal reports. Activation of the endocannabi-
oid system suppresses behavioral responses to acutend persistent noxious stimulation through both cen-ral71 and peripheral45 mechanisms. Cannabinoid recep-
eceived June 25, 2007; Revised December 10, 2007; Accepted December8, 2007.upported by grant C01-DA-114 from the University of California Centeror Medicinal Cannabis Research.lexander Tsodikov is currently at the School of Public Health, Universityf Michigan, Ann Arbor, MI.ddress reprint requests to Dr. Barth L. Wilsey, Pain Academic Office, UCavis Medical Center, 3020 Ellison Ambulatory Care Center, 4860 Ytreet, Sacramento, CA 95817. E-mail: [email protected]/$34.002008 by the American Pain Society
doi:10.1016/j.jpain.2007.12.010
06
ors are localized in neuroanatomic regions intimatelynvolved with transmission and modulation of pain sig-als: The periaqueductal gray (PAG), the rostral ventro-edial medulla (RVM),40,66 and the dorsal horn of the
pinal cord.66 Animal experimentation has clearly dem-nstrated that synthetic and endogenous cannabinoidsot only produce analgesia but also interact in someanner to potentiate opioids,18,70 particularly in neuro-athic pain.41
Surveys involving the use of medicinal marijuana re-eal that pain, sleep, and mood improve with only mod-st side effects.72,73 In one human pain experiment, sub-ects had a significant dose-dependent antinociceptionincreased finger withdrawal latency) effect that was noteversed by opioid antagonism.31 In a somewhat contra-
ictory manner, hyperalgesic activity and enhancement
ouc9otHfs
rcntmiCawwttecciauac
tmacdps“bpwaiwatat
M
P
t(HdwS
amt
Vipcipeemsdw(tfitmag
nqtdtswpjc4
ptICetda11wBnspiccplcoe
507ORIGINAL REPORT/Wilsey et al
f the perception of pain on acute exposure in chronicsers of marijuana was reported.20 Experience with can-er pain revealed that 120 mg codeine and 20 mg delta--tetrahydrocannabinol (9-THC) were similar to eachther and significantly superior to placebo for the sum ofhe pain intensity differences and total pain relief.55,56
owever, there was a clear dose-response relationshipor sedation, mental clouding, and other central nervousystem (CNS) related side effects from the 9-THC.When taken alone, 9-THC or dronabinol does not fully
eplicate the effect of the total cannabis preparation, indi-ating that there might be other active cannabinoidseeded for a full range of effects.77 As a result, combina-ions of cannabinoids are being sought for clinical imple-entation. Sativex is one of the first cannabis-based med-
cines to have been approved as a prescription medicine inanada.5 It has been found to be effective in reducing painnd sleep disturbances in patients with multiple sclerosisho have central neuropathic pain, and it appears to beell-tolerated.62 The rationale for a combination is that
he cannabidiol, normally present in insignificant concen-rations in cannabis, purportedly antagonizes undesirableffects of 9-THC such as intoxication, sedation, and tachy-ardia while contributing analgesic, anti-emetic, and anti-arcinogenic properties.64 However, in one direct compar-son between this combination and 9-THC alone,dditional effectiveness was not evident.11 Therefore, eval-ating herbal cannabis remains a worthwhile endeavorwaiting more definitive proof of a specific combination ofannabinoids that can enhance effectiveness.Despite support from the basic and clinical sciences,
he clinical utility of cannabis in the United States re-ains mired in controversy.13,48,57 Akin to the medical
nd social controversy surrounding the use of opioids inhronic pain,23 clinical trials will be a critical factor in theebate concerning medical marijuana. In defense of thisosition, the National Institutes of Health (NIH) Work-hop on the Medical Utility of Marijuana1 concluded,Inhaled marijuana merits testing in controlled, double-lind, randomized trials . . .”. Furthermore, the NIHanel concluded that neuropathic pain is a condition inhich currently available analgesics are, at best, margin-lly effective, suggesting that cannabis might hold prom-se as a treatment. To address this issue, we examinedhether smoking cannabis produces dose-dependentnalgesia on both spontaneous and evoked pain in pa-ients with neuropathic pain. In addition, we studied thedverse effects of cannabis to better understand its po-ential detrimental effects on patients.
aterials and Methods
atientsThis study was approved by the Human Subjects Insti-
utional Review Boards at the UC Davis Medical CenterUCDMC) and the Veterans Affairs of Northern Californiaealth Care System (VANCHCS). At the state level, en-orsement by the Research Advisory Panel of Californiaas obtained to proceed with the investigation of a
chedule I controlled substance. The approval process f
lso included national review by the Food and Drug Ad-inistration, the National Institute on Drug Abuse, and
he Department of Health and Human Services.Participants were recruited from the UCDMC andANCHCS pain clinics through initial contact by providers
ntimately involved in the patient’s care as well as news-aper advertisements and postings in newsletters. Allandidates were initially screened via a brief telephonenterview. Qualified candidates with complex regionalain syndrome (CRPS type I), spinal cord injury, periph-ral neuropathy, or nerve injury were interviewed andxamined by the principal investigator who invited thoseeeting inclusion and exclusion criteria to enroll in the
tudy. The diagnostic criteria for CRPS type I followed aecision rule compiled by a research consortium workingith the International Association for the Study of Pain
IASP),14,27,33 which required at least 2 signs and 4 symp-oms to be positive. The specific historic and physicalndings included burning pain, skin sensitivity to lightouching or cold, skin color changes, swelling, limitedovement of the affected body part, motor neglect or
bnormalities in skin temperature, hair growth, nailrowth, and/or sweating.To reduce the risk of adverse psychoactive effects inaive individuals, previous cannabis exposure was re-uired of all participants. All participants were requiredo refrain from smoking cannabis or taking oral syntheticelta-9-THC medications (ie, Marinol; Solvay Pharmaceu-icals, Inc., Marietta, GA) for 30 days before study ses-ions to reduce residual effects; each participant under-ent urine toxicology screening to confirm thisrovision. To further reduce unsystematic variation, sub-
ects were instructed to take all other concurrent medi-ations as per their normal routine during the 3- to-week study period.To ensure that potential subjects did not have depression
rofound enough to compromise their ability to toleratehe psychoactive effects of cannabis, the Beck Depressionnventory-II (BDI-II) was administered as a screening tool.andidates with a BDI-II score of 17 or higher were thenvaluated with the Composite International Diagnostic In-erview, a structured interview used to assess mental disor-ers and to provide diagnoses according to the definitionsnd criteria of the ICD-10 (World Health Organization992, 1993) and DSM-IV (American Psychiatry Association,994). If the criteria for severe major depressive disorderere met, the candidate was excluded from participation.ecause the effects of cannabis can exacerbate mental ill-ess24,54 and have been linked to an increase in the risk ofuicide,22 candidates with a history or diagnosis of schizo-hrenia or bipolar depression were also excluded. Medical
llnesses were also evaluated, and exclusion criteria in-luded uncontrolled hypertension, cardiovascular disease,hronic pulmonary disease (eg, asthma, chronic obstructiveulmonary disease), and active substance abuse. Routine
aboratory analysis included a hematology screen, bloodhemistry panel, and urinalysis. Urine drug toxicologies forpioids, benzoylecgonine (cocaine metabolite), benzodiaz-pines, cannabinoids, and amphetamines were also per-
ormed through the use of urine quick tests.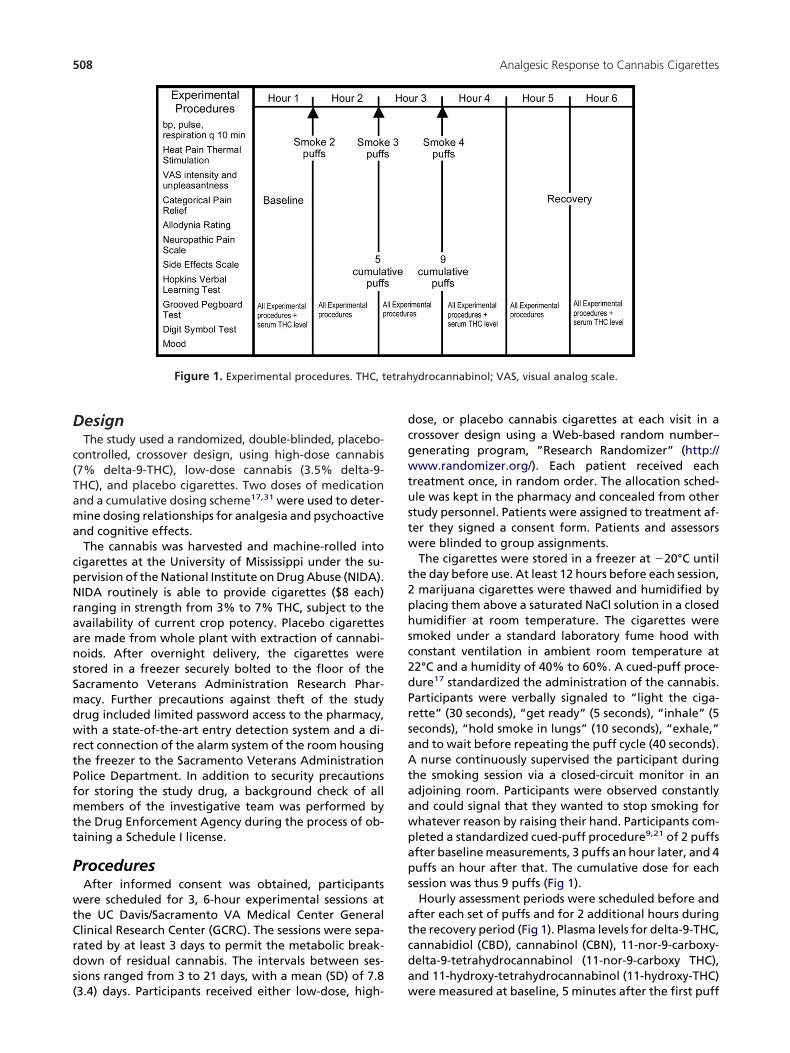
D
c(Tama
cpNraansSmdwrtPfmtt
P
wtCrds(
dcgwtustw
t2phsc2dPrsaAtaawpaps
atcda
etrah
508 Analgesic Response to Cannabis Cigarettes
esignThe study used a randomized, double-blinded, placebo-
ontrolled, crossover design, using high-dose cannabis7% delta-9-THC), low-dose cannabis (3.5% delta-9-HC), and placebo cigarettes. Two doses of medicationnd a cumulative dosing scheme17,31 were used to deter-ine dosing relationships for analgesia and psychoactive
nd cognitive effects.The cannabis was harvested and machine-rolled into
igarettes at the University of Mississippi under the su-ervision of the National Institute on Drug Abuse (NIDA).IDA routinely is able to provide cigarettes ($8 each)
anging in strength from 3% to 7% THC, subject to thevailability of current crop potency. Placebo cigarettesre made from whole plant with extraction of cannabi-oids. After overnight delivery, the cigarettes weretored in a freezer securely bolted to the floor of theacramento Veterans Administration Research Phar-acy. Further precautions against theft of the studyrug included limited password access to the pharmacy,ith a state-of-the-art entry detection system and a di-
ect connection of the alarm system of the room housinghe freezer to the Sacramento Veterans Administrationolice Department. In addition to security precautionsor storing the study drug, a background check of allembers of the investigative team was performed by
he Drug Enforcement Agency during the process of ob-aining a Schedule I license.
roceduresAfter informed consent was obtained, participantsere scheduled for 3, 6-hour experimental sessions at
he UC Davis/Sacramento VA Medical Center Generallinical Research Center (GCRC). The sessions were sepa-ated by at least 3 days to permit the metabolic break-own of residual cannabis. The intervals between ses-ions ranged from 3 to 21 days, with a mean (SD) of 7.8
Figure 1. Experimental procedures. THC, t
3.4) days. Participants received either low-dose, high- w
ose, or placebo cannabis cigarettes at each visit in arossover design using a Web-based random number–enerating program, ”Research Randomizer” (http://ww.randomizer.org/). Each patient received each
reatment once, in random order. The allocation sched-le was kept in the pharmacy and concealed from othertudy personnel. Patients were assigned to treatment af-er they signed a consent form. Patients and assessorsere blinded to group assignments.The cigarettes were stored in a freezer at �20°C until
he day before use. At least 12 hours before each session,marijuana cigarettes were thawed and humidified bylacing them above a saturated NaCl solution in a closedumidifier at room temperature. The cigarettes weremoked under a standard laboratory fume hood withonstant ventilation in ambient room temperature at2°C and a humidity of 40% to 60%. A cued-puff proce-ure17 standardized the administration of the cannabis.articipants were verbally signaled to “light the ciga-ette” (30 seconds), “get ready” (5 seconds), “inhale” (5econds), “hold smoke in lungs” (10 seconds), “exhale,”nd to wait before repeating the puff cycle (40 seconds).nurse continuously supervised the participant during
he smoking session via a closed-circuit monitor in andjoining room. Participants were observed constantlynd could signal that they wanted to stop smoking forhatever reason by raising their hand. Participants com-leted a standardized cued-puff procedure9,21 of 2 puffsfter baseline measurements, 3 puffs an hour later, and 4uffs an hour after that. The cumulative dose for eachession was thus 9 puffs (Fig 1).Hourly assessment periods were scheduled before and
fter each set of puffs and for 2 additional hours duringhe recovery period (Fig 1). Plasma levels for delta-9-THC,annabidiol (CBD), cannabinol (CBN), 11-nor-9-carboxy-elta-9-tetrahydrocannabinol (11-nor-9-carboxy THC),nd 11-hydroxy-tetrahydrocannabinol (11-hydroxy-THC)
ydrocannabinol; VAS, visual analog scale.
ere measured at baseline, 5 minutes after the first puff

betsa(h
tctaw$
O
aispdVwc
scpfppmsTiaustc“e“I““tsVrvwft
tfiAt
msqprvlaiuwswtdfitsaonndcc
pwstssLspepebvtp
pfvfemptmpavpslo
509ORIGINAL REPORT/Wilsey et al
out, and again at 3 hours after the last puff cycle. Afterach blood draw, plasma was separated by centrifuga-ion and immediately frozen. Plasma samples were sub-equently evaluated for enzyme-linked immunosorbentssay of delta-9-THC and metabolite content. Vital signsaural temperature, blood pressure, respiratory rate, andeart rate) were recorded at baseline and at every hour.Participants were allowed to engage in normal activi-
ies, such as reading or listening to music, between puffycles and measurement periods. After each session, par-icipants were accompanied home by a responsibledult. After completing all 3 study sessions, participantsere debriefed and paid a modest stipend (prorated at25 per hour) for their participation.
utcome MeasurementsSpontaneous pain relief, the primary outcome vari-
ble, was assessed by asking participants to indicate thentensity of their current pain on a 100-mm visual analogcale (VAS) between 0 (no pain) and 100 (worst possibleain). Pain unpleasantness, a measure of the emotionalimension of pain, was also measured by using a similarAS. In addition, the degree of pain relief was monitoredith a standard 7-point patient global impression of
hange scale.26
The Neuropathic Pain Scale,28 an 11-point box ordinalcale with several pain descriptors, was a secondary out-ome. When present, allodynia (the sensation of un-leasantness, discomfort, or pain when the skin in a pain-ul area of the patient’s body was stroked with a foamaint brush) was measured using a 100-mm VAS. Heat-ain threshold was determined by applying mild-to-oderately painful heat to the most painful area of the
ubjects’ body32 with the commercially available MedocSA 2001 Peltier thermode (Medoc Ltd. Advanced Med-cal Systems, Ramat Yishai, Israel). This device was used topply a constant 1°C per second increasing thermal stim-lus until the patient pressed the response button tohow that a temperature change was considered painful;he heat pain threshold (mean of 3 attempts) was re-orded in degrees Centigrade. Subjective intensities forany drug effect,” “good drug effect,” and “bad drugffect” were measured using a 100-mm VAS anchored byno side effect” at 0 and “strongest side effect” at 100.n addition, psychoactive effects, including “high,”drunk,” “impaired,” “stoned,” “like the drug effect,”sedated,” “confused,” “nauseated,” “desire more ofhe drug,” “anxious,” “down,” and “hungry” were mea-ured similarly. Mood was measured using 6, 100-mmAS ratings for: Feeling sad versus happy; anxious versuselaxed; jittery versus calm; bad versus good; paranoidersus self-assured; and fearful versus unafraid. Subjectsere prompted to provide their current rating for the
oregoing items at each measurement of these subjec-ive states.Neurocognitive assessments focused on 3 domains: At-
ention and concentration, learning and memory, andne motor speed. Subjects completed the Wechslerdult Intelligence Scale (WAIS-III) Digit Symbol Test,75 a
est of concentration, psychomotor speed, and grapho- c
otor abilities. This pen and paper test involves havingubjects substitute a series of symbols with numbers asuickly and accurately as possible during a 120-seconderiod. The results are expressed as the number of cor-ect substitutions. The Hopkins Verbal Learning Test Re-ised (HVLT)7 provided information on the ability toearn and immediately recall verbal information as wellt the ability to retain, reproduce, and recognize thisnformation after a delay. Alternate forms (A–F) weresed to minimize practice effects.6,8 A list of 12 words (4ords from each of 3 semantic categories) were pre-
ented, and the subject was asked to recall as manyords as possible in any order. After a 20-minute delay,
he subject was asked to recall the words once again (ie,elayed recall). The Grooved Pegboard Test,47 a test ofne motor coordination and speed, was also adminis-ered. In this test, subjects were required to place 25mall metal pegs into holes on a 3 � 3-inch metal boards quickly as possible. All pegs are alike and have a ridgen one side, which corresponds to a randomly orientedotch in each hole on the metal board. First the domi-ant hand is tested and then repeated with the non-ominant hand, and the total time for each test is re-orded. A 5-minute limit is used for those unable toomplete the task.Performance on neuropsychological tests often im-roves as a result of practice effects.39 This can be some-hat ameliorated by the use of alternate forms8 and,
ince the largest practice effects typically occur betweenhe first and second testing,21 preexposure to the mea-ures (ie, dual baselines) are recommended.6,69 For thistudy, we used 6 separate versions of the Hopkins Verbalearning Test, and incorporated a practice testing ses-ion at the time of the screening interview to lessen earlyractice effects. Despite our attempts to limit practiceffects (using alternate forms, conducting a prebaselineractice session), these effects cannot be completelyliminated when subjects are tested repeatedly over arief period. However, this is likely to result in increasedariance, thus attenuating the treatment effect. In addi-ion, practice effects were also mitigated by the use of alacebo arm.To estimate the level of functioning at baseline and torovide a common metric for interpreting treatment ef-ects on cognition, the raw scores on each test were con-erted to demographically corrected T scores (adjustingor age, gender, highest educational level achieved, andthnicity).37,38 In normal control groups, T scores have aean of 50 with a standard deviation of 10. Based on
revious research to determine the optimal cut-pointhat balances sensitivity and specificity in mild impair-ents,36 a T score below 40 was classified as an impaired
erformance. Neuropsychological test performance waslso summarized using the global deficit score (GDS), aalidated approach for detecting neuropsychological im-airments across multiple measures.16 The GDS empha-izes both the number and the severity of deficits, givingess weight to average and above performances. T scoresn the individual neuropsychological measures were
onverted using the following algorithm: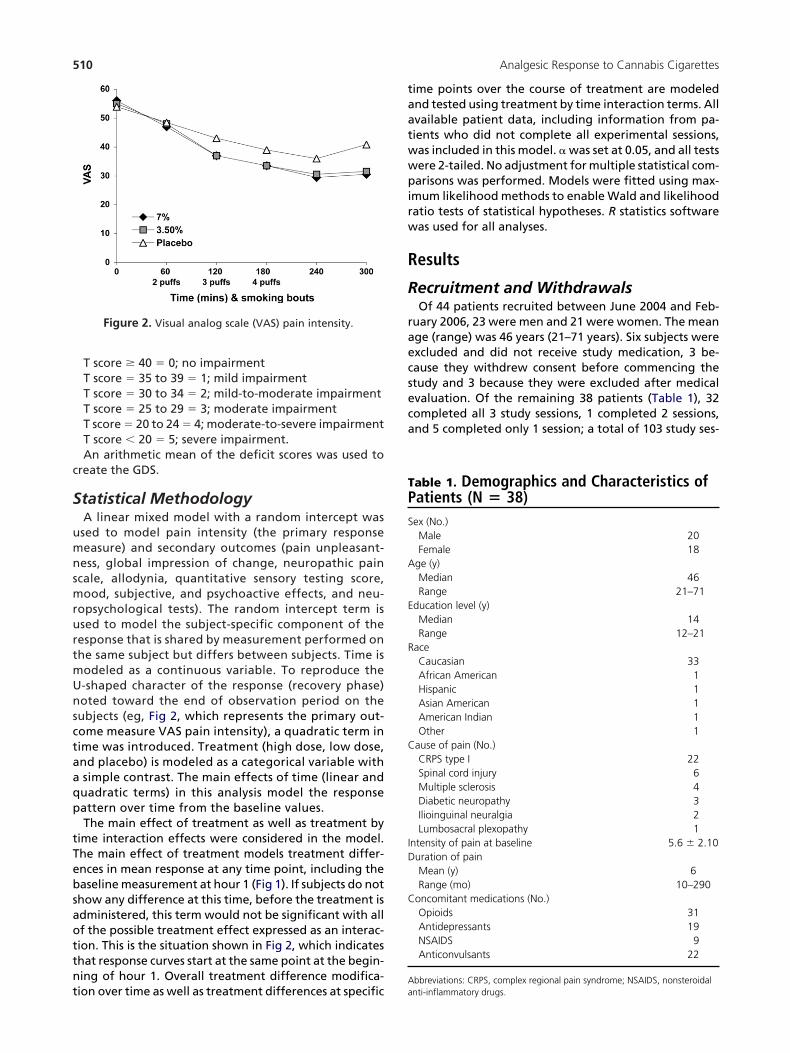
c
S
umnsmrurtmUnsctaaqp
tTebsaottnt
taatwwpirw
R
R
raecseca
TPS
A
E
R
C
ID
C
A
510 Analgesic Response to Cannabis Cigarettes
T score � 40 � 0; no impairmentT score � 35 to 39 � 1; mild impairmentT score � 30 to 34 � 2; mild-to-moderate impairmentT score � 25 to 29 � 3; moderate impairmentT score � 20 to 24 � 4; moderate-to-severe impairmentT score � 20 � 5; severe impairment.An arithmetic mean of the deficit scores was used to
reate the GDS.
tatistical MethodologyA linear mixed model with a random intercept wassed to model pain intensity (the primary responseeasure) and secondary outcomes (pain unpleasant-ess, global impression of change, neuropathic paincale, allodynia, quantitative sensory testing score,ood, subjective, and psychoactive effects, and neu-
opsychological tests). The random intercept term issed to model the subject-specific component of theesponse that is shared by measurement performed onhe same subject but differs between subjects. Time isodeled as a continuous variable. To reproduce the-shaped character of the response (recovery phase)oted toward the end of observation period on theubjects (eg, Fig 2, which represents the primary out-ome measure VAS pain intensity), a quadratic term inime was introduced. Treatment (high dose, low dose,nd placebo) is modeled as a categorical variable withsimple contrast. The main effects of time (linear anduadratic terms) in this analysis model the responseattern over time from the baseline values.The main effect of treatment as well as treatment by
ime interaction effects were considered in the model.he main effect of treatment models treatment differ-nces in mean response at any time point, including theaseline measurement at hour 1 (Fig 1). If subjects do nothow any difference at this time, before the treatment isdministered, this term would not be significant with allf the possible treatment effect expressed as an interac-ion. This is the situation shown in Fig 2, which indicateshat response curves start at the same point at the begin-ing of hour 1. Overall treatment difference modifica-
Figure 2. Visual analog scale (VAS) pain intensity.
ion over time as well as treatment differences at specific a
ime points over the course of treatment are modelednd tested using treatment by time interaction terms. Allvailable patient data, including information from pa-ients who did not complete all experimental sessions,as included in this model. � was set at 0.05, and all testsere 2-tailed. No adjustment for multiple statistical com-arisons was performed. Models were fitted using max-
mum likelihood methods to enable Wald and likelihoodatio tests of statistical hypotheses. R statistics softwareas used for all analyses.
esults
ecruitment and WithdrawalsOf 44 patients recruited between June 2004 and Feb-
uary 2006, 23 were men and 21 were women. The meange (range) was 46 years (21–71 years). Six subjects werexcluded and did not receive study medication, 3 be-ause they withdrew consent before commencing thetudy and 3 because they were excluded after medicalvaluation. Of the remaining 38 patients (Table 1), 32ompleted all 3 study sessions, 1 completed 2 sessions,nd 5 completed only 1 session; a total of 103 study ses-
able 1. Demographics and Characteristics ofatients (N � 38)
ex (No.)Male 20Female 18
ge (y)Median 46Range 21–71
ducation level (y)Median 14Range 12–21
aceCaucasian 33African American 1Hispanic 1Asian American 1American Indian 1Other 1
ause of pain (No.)CRPS type I 22Spinal cord injury 6Multiple sclerosis 4Diabetic neuropathy 3Ilioinguinal neuralgia 2Lumbosacral plexopathy 1
ntensity of pain at baseline 5.6 � 2.10uration of painMean (y) 6Range (mo) 10–290
oncomitant medications (No.)Opioids 31Antidepressants 19NSAIDS 9Anticonvulsants 22
bbreviations: CRPS, complex regional pain syndrome; NSAIDS, nonsteroidal
nti-inflammatory drugs.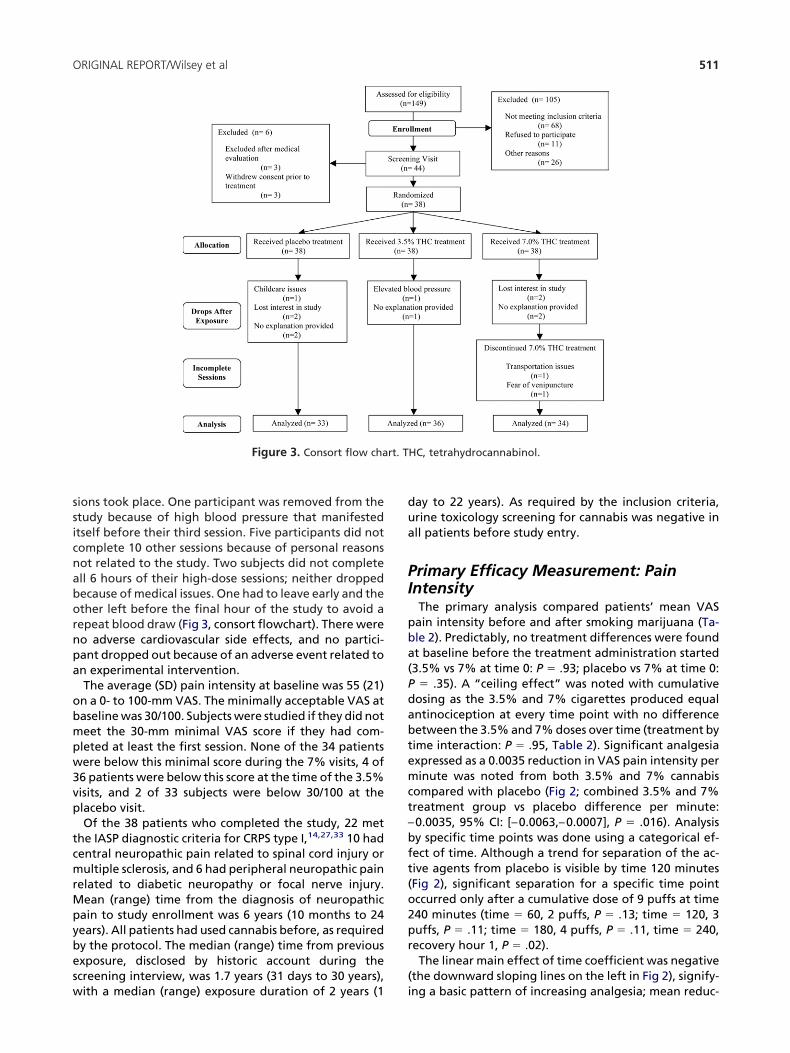
ssicnabornpa
obmpw3vp
tcmrMpybesw
dua
PI
pba(Pdabtemct–bft(o2pr
(
rt. T
511ORIGINAL REPORT/Wilsey et al
ions took place. One participant was removed from thetudy because of high blood pressure that manifestedtself before their third session. Five participants did notomplete 10 other sessions because of personal reasonsot related to the study. Two subjects did not completell 6 hours of their high-dose sessions; neither droppedecause of medical issues. One had to leave early and thether left before the final hour of the study to avoid aepeat blood draw (Fig 3, consort flowchart). There wereo adverse cardiovascular side effects, and no partici-ant dropped out because of an adverse event related ton experimental intervention.The average (SD) pain intensity at baseline was 55 (21)n a 0- to 100-mm VAS. The minimally acceptable VAS ataseline was 30/100. Subjects were studied if they did noteet the 30-mm minimal VAS score if they had com-leted at least the first session. None of the 34 patientsere below this minimal score during the 7% visits, 4 of6 patients were below this score at the time of the 3.5%isits, and 2 of 33 subjects were below 30/100 at thelacebo visit.Of the 38 patients who completed the study, 22 met
he IASP diagnostic criteria for CRPS type I,14,27,33 10 hadentral neuropathic pain related to spinal cord injury orultiple sclerosis, and 6 had peripheral neuropathic pain
elated to diabetic neuropathy or focal nerve injury.ean (range) time from the diagnosis of neuropathic
ain to study enrollment was 6 years (10 months to 24ears). All patients had used cannabis before, as requiredy the protocol. The median (range) time from previousxposure, disclosed by historic account during thecreening interview, was 1.7 years (31 days to 30 years),
Figure 3. Consort flow cha
ith a median (range) exposure duration of 2 years (1 i
ay to 22 years). As required by the inclusion criteria,rine toxicology screening for cannabis was negative inll patients before study entry.
rimary Efficacy Measurement: PainntensityThe primary analysis compared patients’ mean VASain intensity before and after smoking marijuana (Ta-le 2). Predictably, no treatment differences were foundt baseline before the treatment administration started3.5% vs 7% at time 0: P � .93; placebo vs 7% at time 0:
� .35). A “ceiling effect” was noted with cumulativeosing as the 3.5% and 7% cigarettes produced equalntinociception at every time point with no differenceetween the 3.5% and 7% doses over time (treatment byime interaction: P � .95, Table 2). Significant analgesiaxpressed as a 0.0035 reduction in VAS pain intensity perinute was noted from both 3.5% and 7% cannabis
ompared with placebo (Fig 2; combined 3.5% and 7%reatment group vs placebo difference per minute:0.0035, 95% CI: [–0.0063,–0.0007], P � .016). Analysisy specific time points was done using a categorical ef-ect of time. Although a trend for separation of the ac-ive agents from placebo is visible by time 120 minutesFig 2), significant separation for a specific time pointccurred only after a cumulative dose of 9 puffs at time40 minutes (time � 60, 2 puffs, P � .13; time � 120, 3uffs, P � .11; time � 180, 4 puffs, P � .11, time � 240,ecovery hour 1, P � .02).The linear main effect of time coefficient was negative
the downward sloping lines on the left in Fig 2), signify-
HC, tetrahydrocannabinol.
ng a basic pattern of increasing analgesia; mean reduc-

t[tssbChptd
eco
tsab
iiscd
S
e
T
D
D
B
A
NDz in the
T
U
G
A
H
N
512 Analgesic Response to Cannabis Cigarettes
ion VAS pain intensity per minute in the placebo group�0.0050, 95% CI: (�0.0073, �0.0026)]. The quadraticime coefficient for recovery was positive (ie, repre-ented by the U-shaped pattern seen on the right-handide of Fig 2), signifying a change in direction towardaseline; with the quadratic term being 3.3 � 10�5, 95%I: (0.00002, 0.00005). Both of these time effects wereighly significant (P � .0001), suggesting that cannabisroduced an analgesic response with cumulative dosinghat began to reverse within 1 to 2 hours after the lastose.Using the model, we considered whether there is any
vidence that the results might differ by the type of painondition. No significant differences were found; a testf no effect of pain type showed a P value of .39. Pairwise
able 2. Visual Analog Scale (VAS) Pain Intensi
EFFECT D
ifferences atbaseline
7% vs 3.5% �7% vs placebo �3.5% vs placebo �
ose effect on top ofbasic pattern,treatment by timeinteraction
7% vs 3.5% �7% vs placebo �
3.5% vs placebo �
7%�3.5% vs placebo �
asic analgesiapattern, placebo,combined3.5%�7% fit
Pain intensity reduction perminute, time linear term
�
Pain intensity reduction over time,quadratic term
bsolute effects bytime, Pain intensityreduction perminute
Placebo �
3.5% dose �
7% dose �
OTE. Significant results (P � .05) are bolded. Point estimates of differences aose effect point estimate represents a difference in VAS pain intensity changeero difference at baseline would produce identical mean VAS curves over time
able 3. Secondary Pain Measures Analysis
PAIN MEASURE EFFECT
npleasantness Basic analgesia pattern, placebo Time, linear tTime, quadra
Treatment effect, interaction bytime
3.5% vs plac7% vs Placeb
lobal impressionof change
Basic analgesia pattern, placebo Time, linear tTime, quadra
Treatment effect, interaction bytime
3.5% vs plac7% vs Placeb
llodynia Basic pattern Time, linear tTime, quadra
Treatment effect, interaction bytime
3.5% vs plac7% vs placeb
eat stimuli Basic pattern Time, linear tTime, quadra
Treatment effect, interaction bytime
3.5% vs plac7% vs placeb
OTE. Significant results (P � .05) are bolded.
ests did not show any significant differences, either. Ithould be noted, however, that the sample size in thebove analysis was small, and a type II error may haveeen present.Order of treatment administration (placebo, 3.5% or 7%)
n this crossover study was not a significant factor (P � .37)n analyzing the primary outcome variable. However, thetudy may not have enough power to detect order orarryover effects. Generous spacing of patient visits wasesigned to alleviate this concern.
econdary OutcomesA sample of the results of model fit to secondary pain
nd points is shown in Table 3.
rimary Efficacy AnalysisN
ENCE
STANDARD
ERROR CONFIDENCE INTERVAL P VALUE
0.23 �0.47 0.43 .930.23 �0.66 0.24 .350.23 �0.64 0.26 .40
01 0.0017 �0.0034 0.0032 .9535 0.0017 �0.0068 �0.0002 .0436 0.0017 �0.0069 0.0003 .0335 0.0014 �0.0063 �0.0007 .0250 0.0012 �0.0073 �0.0026 < .01
003 0.0001 0.00002 0.00005 < .01
40 0.0010 �0.0060 �0.0021 < .01
85 0.0010 �0.010 �0.0066 < .01
85 0.0010 �0.010 �0.0065 < .01
line represent mean difference in pain intensity at time before treatment.inute (slope) between 2 dose levels. A zero dose effect point estimate and2 groups.
MEAN
DIFFERENCE
STANDARD
ERROR CONFIDENCE INTERVAL P VALUE
23.67 8.42 7.16 40.18 < .010.14 0.050 0.044 0.23 < .01
�0.21 0.06 �0.33 �0.09 < .01�0.21 0.06 �0.33 �0.09 < .01
�22.62 4.04 �30.53 �14.70 < .01�0.13 0.023 �0.18 �0.08435 < .01
0.12 0.029 0.064 0.18 < .010.12 0.029 0.065 0.18 < .013.66 3.66 �3.50203 10.83 .320.022 0.021 �0.01938 0.063 .300.00007 0.034 �0.066 0.066 .99
�0.009 0.034 �0.076 0.058 .79�2.64 6.52 �15.42 10.14 .69�0.015 0.038 �0.089 0.059 .69
0.11 0.06 �0.0046 0.23 .060.085 0.060 �0.034 0.20392 .16
ty PMEA
IFFER
0.020.210.190.000.000.000.000.00
0.00
0.00
0.00
0.00
t baseper m
ermticebooermticebooermticebooermticeboo

P
s1td3mcd
G
p7wg9hd
N
iewbschmppb
A
th1fatw
Q
tn(d
S
fe(t
S
tdTecsr(
“m5n(t.nep
P
dfiic
ectiv
513ORIGINAL REPORT/Wilsey et al
ain UnpleasantnessPain unpleasantness, a measure of the emotional re-
ponse to pain, was also measured by using a similar00-mm VAS bordered by “not at all” at 0 and “ex-remely unpleasant” at 100. A trend for the treatmentifference increase over time is found to be the same in.5% and 7% dose groups (mean difference change perinute � �0.21, 95% CI: (�0.33, �0.09), P � .01), indi-
ating that pain was more tolerable at higher cumulativeoses of cannabis that it was with placebo.
lobal Impression of ChangeIn addition to VAS ratings for pain intensity and un-leasantness, the degree of relief was monitored by a-point scale of patient global impression of change. Asith the VAS ratings, cannabis provided a greater de-ree of relief than placebo (3.5% or 7% placebo � 0.12,5% CI: (0.064, 0.18), P � .01). Once again, the low- andigh-dose groups showed virtually identical results andid not differ significantly (P � .76).
europathic Pain ScaleMeasurements from the Neuropathic Pain Scale (NPS)
ndicate that smoking cannabis positively affected sev-ral of the multidimensional pain descriptors associatedith neuropathic pain. Modeling of sharp (P � .001),urning (P � .001), aching (P � .001), sensitive (P � .03),uperficial (P � .01) and deep pain (P � .001) showed thatannabis improved pain scores more than placebo. Theigher dose provided no additional benefit on these di-ensions, except that the high dose lowered superficialain more than the low dose (P � .04). Cannabis im-roved neither cold nor itching over placebo (P � .05 foroth dimensions).
llodyniaThe mean values of allodynia were relatively low
hroughout all sessions, with the average VAS for the 6ourly measurements ranging between 20 and 35 on a00 millimeter scale. These low scores are related to theact that 15 of the 38 participants (39%) did not havellodynia. No effect of treatment with different concen-rations of cannabis (P � .40) or cumulative dose (P � .29)
Figure 4. Subj
as observed. s
uantitative Sensory TestingMild to moderately painful heat stimuli delivered to
he most painful area of the participant’s body producedo significant change in response to treatment over timeP � .2) as well as no indication of any trend in treatmentifferences (P � .1).
ubjective and Psychoactive EffectsThe linear mixed effects modeling explored side ef-
ects data using several variables. A continuous linearffect of time, a categorical main effect of treatmentlow dose vs high dose vs placebo), and an interaction ofime with treatment was used.
ubjective EffectsThe “any drug effect” approached a VAS of 60/100 in
he high-dose group after the maximum cumulativeose, but the effect receded rapidly thereafter (Fig 4A).he analysis of this end point showed significant mainffect of treatment (Fig 4A), with the low-dose and pla-ebo values being lower than the corresponding re-ponses for the high-dose values (P � .002, P � .001,espectively). Time did not modify this treatment effectP � .17).The low-dose and high-dose groups had more of a
good drug effect” (Fig 4B) than placebo (P � .001). Theaximum “good drug effect” was between 30/100 and
0/100 for the 2 doses (Fig 4B) and was greater in mag-itude than the 25/100 recorded for a “bad drug effect”Fig 4C). A “bad drug effect” (Fig 4C) was not evident forhe low-dose group when compared with placebo (P �2), and initially the high dose-group did not differ sig-ificantly from placebo either. Eventually, however, thisffect built up with time for the high dose (effect changeer unit time � 0.275, P � .03).
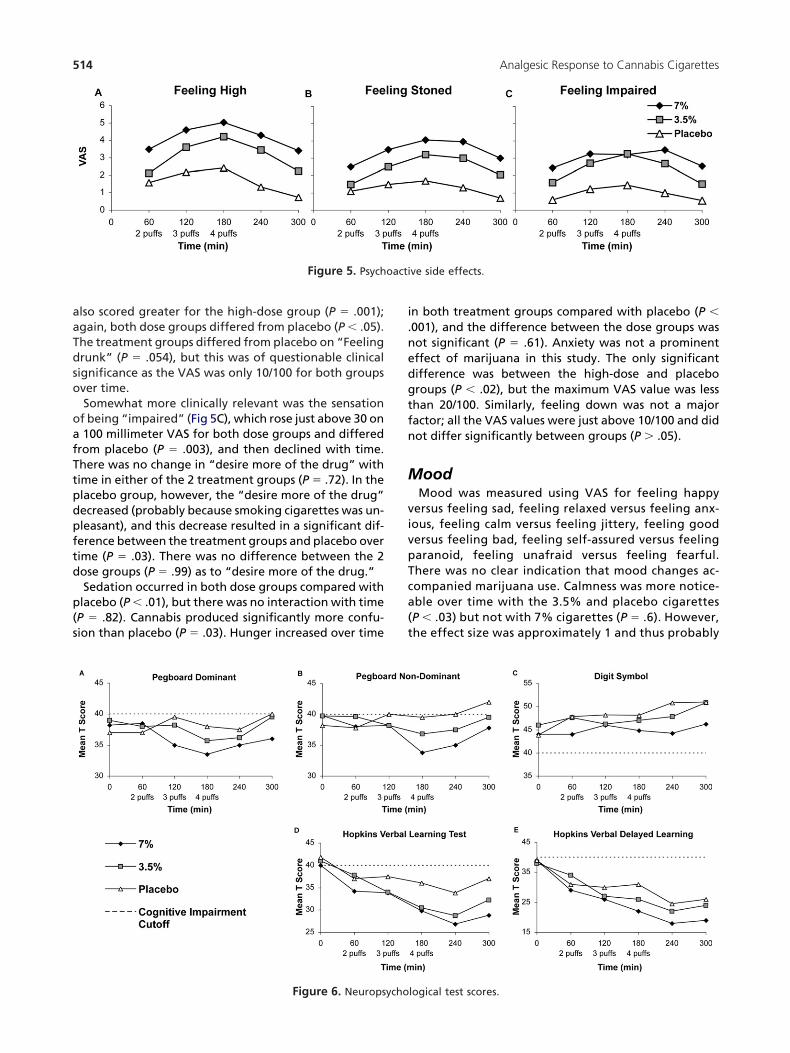
sychoactive Effects“Feeling high” (Fig 5A) scored greatest for the high-ose group (P � .001), and both dose groups differedrom placebo (P � .05). Recovery was gradual after smok-ng cessation; no interaction with time occurred (P � .2),mplying that the differences between active and pla-ebo cigarettes remained similar at all time points de-
e side effects.
pite cumulative dosing. “Feeling stoned” (Fig 5B) was
aaTdso
oafTtpdpftd
p(s
i.nedgtfn
M
vivpTca(t
oacti
514 Analgesic Response to Cannabis Cigarettes
lso scored greater for the high-dose group (P � .001);gain, both dose groups differed from placebo (P � .05).he treatment groups differed from placebo on “Feelingrunk” (P � .054), but this was of questionable clinicalignificance as the VAS was only 10/100 for both groupsver time.Somewhat more clinically relevant was the sensationf being “impaired” (Fig 5C), which rose just above 30 on100 millimeter VAS for both dose groups and differed
rom placebo (P � .003), and then declined with time.here was no change in “desire more of the drug” withime in either of the 2 treatment groups (P � .72). In thelacebo group, however, the “desire more of the drug”ecreased (probably because smoking cigarettes was un-leasant), and this decrease resulted in a significant dif-erence between the treatment groups and placebo overime (P � .03). There was no difference between the 2ose groups (P � .99) as to “desire more of the drug.”Sedation occurred in both dose groups compared withlacebo (P � .01), but there was no interaction with timeP � .82). Cannabis produced significantly more confu-ion than placebo (P � .03). Hunger increased over time
Figure 5. Psych
Figure 6. Neuropsycho
n both treatment groups compared with placebo (P �001), and the difference between the dose groups wasot significant (P � .61). Anxiety was not a prominentffect of marijuana in this study. The only significantifference was between the high-dose and placeboroups (P � .02), but the maximum VAS value was lesshan 20/100. Similarly, feeling down was not a majoractor; all the VAS values were just above 10/100 and didot differ significantly between groups (P � .05).
oodMood was measured using VAS for feeling happy
ersus feeling sad, feeling relaxed versus feeling anx-ous, feeling calm versus feeling jittery, feeling goodersus feeling bad, feeling self-assured versus feelingaranoid, feeling unafraid versus feeling fearful.here was no clear indication that mood changes ac-ompanied marijuana use. Calmness was more notice-ble over time with the 3.5% and placebo cigarettesP � .03) but not with 7% cigarettes (P � .6). However,he effect size was approximately 1 and thus probably
ve side effects.
logical test scores.

nm
N
cmbgeomArst
mTbputdd
tdDsd(gtngterows
imrmpit
T
P
P
D
H
H
S vised.
515ORIGINAL REPORT/Wilsey et al
ot an important consideration. The other measure-ents were similarly of little clinical significance.
europsychological TestingThe linear mixed effects modeling for this data in-
ludes the main effect of time (continuous), a categoricalain effect of treatment (7% vs 3.5% vs placebo canna-is), an interaction of time with treatment, and a cate-orical effect associated with the last time point (recov-ry effect). The recovery effect involving measurementf the last time point was performed as this point esti-ate showed departure from the linear pattern (Fig 6,–E) of earlier measurements in other models. For this
eason, we used this special model term to address rever-al of the neuropsychological decline. Detailed results forhe normalized data are presented in Table 4.The main effect of time models the cognitive impair-ent associated with the cumulative dose of cannabis.
he pretreatment scores (intercept terms) were equalecause participants did not have residual effects fromrevious treatments and had been instructed not tose marijuana for 30 days before study entry or duringhe intervals between study sessions. Cannabis pro-uced a general cognitive decline, as indicated by the
able 4. Neuropsychological T Scores
SCORE EFFECT
egboard dominanthand
Initial impairment 7% vs 3.5%7% vs placebo
Change per minute inmean difference
7% vs 3.5%7% vs placebo3.5% vs place
Recovery effect Last point vs liegboard nondominanthand
Initial impairment 7% vs 3.5%7% vs placebo
Change per minute inmean difference
7% vs 3.5%7% vs placebo3.5% vs place
Recovery effect Last point vs liigit symbol test Initial impairment 7% vs 3.5%
7% vs placeboChange per minute in
mean difference7% vs 3.5%7% vs placebo3.5% vs place
Recovery effect Last point vs liVLT–Learning Initial impairment 7% vs 3.5%
7% vs placeboChange per minute in
mean difference7% vs 3.5%7% vs placebo3.5% vs place
Recovery effect Last point vs liVLT–Recall Initial impairment 7% vs 3.5%
7% vs placeboChange per minute in
mean difference7% vs 3.5%7% vs placebo3.5% vs place
Recovery effort Last point vs li
ignificant results (P � .05) are bolded. HVLT, Hopkins Verbal Learning Test Re
ifference in the slopes of scores over time between d
reatment groups. The high-dose and placebo groupsiffered significantly on all dimensions, except theigit Symbol Test, where the difference bordered on
ignificant, at P � .051. The low- and high-dose groupsid not differ significantly; however, point estimates
Table 4) indicate that the high-dose group hadreater cognitive impairment. More notably, many ofhe neurocognitive results in the low-dose group didot differ significantly from those in the placeboroup. The deviation of the last point from the generalime pattern is modeled by the categorical recoveryffect constructed using an indicator dummy variableepresenting the last time point. Recovery at the lastbserved time point after discontinuation of cannabisas significant for all scores, with the average score
howing a P value of � .01.The analysis comparing the effect of smoking cannabis
n the low- and high-dose and placebo sessions usingean values could minimize group differences on neu-
opsychological testing since above average performersay offset poor performance by others. To obviate this
otential bias, deficit scores were used to reduce thenfluence of the high-functioning individuals.16 Usinghis approach, both low- and high-dose cannabis in-
MEAN
DIFFERENCE
STANDARD
ERROR
CONFIDENCE
INTERVAL P VALUE
0.07 1.6 �3.07 3.21 .97�1.77 1.63 �4.96 1.42 .28
0.46 0.41 �0.34 1.26 .271.14 0.42 0.32 1.96 .0070.68 0.41 �0.12 1.48 .1
trend 3.22 1.03 1.20 5.24 .0020.29 1.51 �2.67 3.25 .85
�2.52 1.53 �5.52 0.48 .10.33 0.39 �0.43 1.09 .391.34 0.39 0.58 2.10 < .0011.01 0.39 0.25 1.77 < .01
trend 3.19 0.96 1.31 5.07 < .012.09 1.82 �1.48 5.66 .250.18 1.85 �3.45 3.81 .920.43 0.47 �0.49 1.35 .360.93 0.48 �0.01 1.87 .0510.50 0.47 �0.42 1.42 .28
trend 1.30 1.16 �0.97 3.57 .0011.59 2.22 �2.76 5.94 .470.15 2.26 �4.28 4.58 .950.28 0.57 �0.84 1.40 .621.31 0.58 0.17 2.45 .021.03 0.57 �0.09 2.15 .07
trend 6.19 1.42 3.41 8.97 < .0011.5 2.25 �2.91 5.91 .5
�0.45 2.30 �4.96 4.06 .840.48 0.58 �0.66 1.62 .411.30 0.59 0.14 2.46 .030.82 0.58 �0.32 1.96 .16
trend 6.16 1.44 3.34 8.98 < .000
bonear
bonear
bonear
bonear
bonear
uced moderate to severe impairment for verbal learn-

idtltfpiumtwfTgPtw
omcocwpcD(Tss
C
mmaossla(aesrmCnwe
D
Caam3tl
T
P
PN
D
H
H
AG
A
N
C
T irmen3 nt), T
516 Analgesic Response to Cannabis Cigarettes
ng and recall (Table 5). Of note, subjects on placebo alsoeclined in learning and recall, most likely due to proac-ive interference resulting from exposure to multipleearning lists in a short time frame. Nonetheless, despitehis pattern, performance on these measures still dif-ered by cannabis levels, and one would expect that anyotential confounding might likely lessen any discern-
ble treatment effects. Since cannabis may affect individ-als differently and the impact on cognitive perfor-ance may be obscured if one just analyzes individual
ests, the global deficit score was used to determinehether treatment with low-and high-dose cannabis af-
ected overall cognitive performance. As can be seen inable 5, there were significant group differences onlobal cognitive functioning at each treatment level.articipants using low-dose cannabis had poorer cogni-ive function than placebo and performed least wellhen on the high dose.In summary, the 7% cannabis demonstrated evidencef neurocognitive impairment in attention, learning andemory, and psychomotor speed, whereas, the 3.5%
annabis resulted in a decline in learning and memorynly. When looking across all measures, subjects on 7%annabis had greater impairment than those on 3.5%,ho in turn had greater impairment than subjects onlacebo. Of note, a significant proportion of subjects hadognitive impairment at baseline: Grooved Pegboardominant (71%) and non-Dominant (68%), Digit Symbol
61%), and HVLT Learning (76%) and Recall (76%).wenty-nine of the 38 subjects (76%) had a global deficitcore in the impaired range (�.50) at baseline before
able 5. Global Deficit Scores (GDS)
TREATMENT 0 MIN
60 MIN
2 PUFFS
egs Dom 7% 1.3 1.53.5% 1.3 1.5Placebo 1.8 1.4
egsondom
7% 1.2 1.43.5% 1.1 1.3Placebo 1.4 1.4
igit Symbol 7% 0.9 0.93.5% 0.6 0.8Placebo 0.8 0.6
VLT–Learn 7% 1.2 2.23.5% 1.1 1.9Placebo 1.2 1.6
VLT–Delay 7% 1.5 2.83.5% 1.6 2.3Placebo 1.5 2.5
verageDS
7% 1.2 1.83.5% 1.1 1.5Placebo 1.3 1.5
bbreviation: HVLT, Hopkins Verbal Learning Test Revised.
OTE. Significant results (P � .05) are bolded.
ategorization of each raw deficit score was performed using clinically relevant
� 40 (deficit score (DS � 0; no impairment), 35 � T � 39 (DS � 1; mild impa; moderate impairment), 20 � T � 24 (DS � 4; moderate-to-severe impairme
moking cannabis. d
annabinoid LevelsThe mean (range) consumption of cigarettes was 550g (200–830 mg) during the low-dose sessions and 490g (270–870 mg) for the high-dose sessions. These
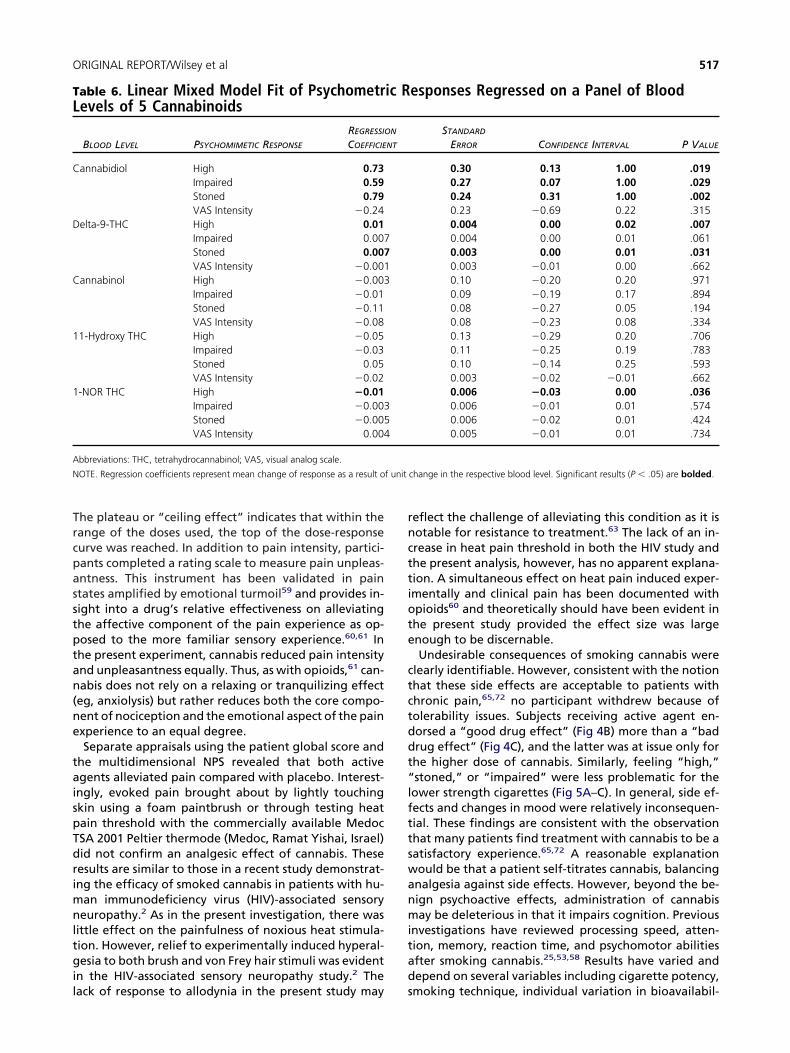
mounts represent smoking slightly more than aboutne-half of a cigarette. The amount of delta-9-THC con-umed was estimated to be 19 mg during the low-doseessions and 34 mg during the high-dose sessions. Serumevels of the primary active cannabinoid D9-THC, second-ry active cannabinoids, cannabidiol (CBD), cannabinolCBN), the primary active metabolite, 11-hydroxy THC,nd the primary inactive metabolite 1-NOR THC werevaluated using linear mixed modeling, with results pre-ented in Table 6. There was no correlation of these se-um levels with analgesia. As expected, several psycho-imetic effects correlated with levels of delta-9-THC,
BD, and the active metabolite 1-NOR THC. However,europsychological testing did not show a relationshipith serum values with the exception of delta-9-THC lev-ls and performance on the Digit Symbol test (P � .034).
iscussionIn the present study, standardized doses of smokedannabis sativa were administered using a uniform puffnd breath-hold procedure.46 The analgesic, subjective,nd neuropsychological effects of cannabis were theneasured. A linear analgesic dose response for both
.5% delta-9-THC and 7% delta-9-THC cannabis substan-iated previous empirical reports of pain relief. Identicalevels of analgesia were produced at each cumulative
120 MIN
3 PUFFS
180 MIN
4 PUFFS 240 MIN 300 MIN
2.0 2.0 2.0 1.71.4 1.8 1.7 1.31.2 1.4 1.6 1.31.5 2.0 1.9 1.71.4 1.5 1.5 1.31.2 1.4 1.3 1.10.9 1.1 1.3 0.80.9 0.7 0.7 0.50.5 0.5 0.5 0.52.4 2.8 3.3 2.92.2 2.7 2.9 2.71.3 1.6 2.1 1.73.3 3.7 4.2 3.83.1 3.4 3.9 3.52.6 2.5 3.5 3.32.0 2.3 2.5 2.21.8 2.0 2.2 1.81.4 1.5 1.8 1.6
f points.
t), 30 � T � 34 (DS � 2; mild-to-moderate impairment), 25 � T � 29 (DS �� 20 (DS � 5; severe impairment).
cutof
ose level by both concentrations of active agent (Fig 2).
Trcpasstptan(ne
taispTdrimnltgil
rncttiote
ctctddt“lfttswanmitad
TL
C
D
C
1
1
A
N f unit
517ORIGINAL REPORT/Wilsey et al
he plateau or “ceiling effect” indicates that within theange of the doses used, the top of the dose-responseurve was reached. In addition to pain intensity, partici-ants completed a rating scale to measure pain unpleas-ntness. This instrument has been validated in paintates amplified by emotional turmoil59 and provides in-ight into a drug’s relative effectiveness on alleviatinghe affective component of the pain experience as op-osed to the more familiar sensory experience.60,61 Inhe present experiment, cannabis reduced pain intensitynd unpleasantness equally. Thus, as with opioids,61 can-abis does not rely on a relaxing or tranquilizing effecteg, anxiolysis) but rather reduces both the core compo-ent of nociception and the emotional aspect of the painxperience to an equal degree.Separate appraisals using the patient global score and
he multidimensional NPS revealed that both activegents alleviated pain compared with placebo. Interest-ngly, evoked pain brought about by lightly touchingkin using a foam paintbrush or through testing heatain threshold with the commercially available MedocSA 2001 Peltier thermode (Medoc, Ramat Yishai, Israel)id not confirm an analgesic effect of cannabis. Theseesults are similar to those in a recent study demonstrat-ng the efficacy of smoked cannabis in patients with hu-
an immunodeficiency virus (HIV)-associated sensoryeuropathy.2 As in the present investigation, there was
ittle effect on the painfulness of noxious heat stimula-ion. However, relief to experimentally induced hyperal-esia to both brush and von Frey hair stimuli was evident
n the HIV-associated sensory neuropathy study.2 The
able 6. Linear Mixed Model Fit of Psychometrevels of 5 Cannabinoids
BLOOD LEVEL PSYCHOMIMETIC RESPONSE
REGRESSIO
COEFFICIE
annabidiol High 0.73Impaired 0.59Stoned 0.79VAS Intensity �0.24
elta-9-THC High 0.01Impaired 0.007Stoned 0.007VAS Intensity �0.001
annabinol High �0.003Impaired �0.01Stoned �0.11VAS Intensity �0.08
1-Hydroxy THC High �0.05Impaired �0.03Stoned 0.05VAS Intensity �0.02
-NOR THC High �0.01Impaired �0.003Stoned �0.005VAS Intensity 0.004
bbreviations: THC, tetrahydrocannabinol; VAS, visual analog scale.
OTE. Regression coefficients represent mean change of response as a result o
ack of response to allodynia in the present study may s
eflect the challenge of alleviating this condition as it isotable for resistance to treatment.63 The lack of an in-rease in heat pain threshold in both the HIV study andhe present analysis, however, has no apparent explana-ion. A simultaneous effect on heat pain induced exper-mentally and clinical pain has been documented withpioids60 and theoretically should have been evident inhe present study provided the effect size was largenough to be discernable.Undesirable consequences of smoking cannabis were
learly identifiable. However, consistent with the notionhat these side effects are acceptable to patients withhronic pain,65,72 no participant withdrew because ofolerability issues. Subjects receiving active agent en-orsed a “good drug effect” (Fig 4B) more than a “badrug effect” (Fig 4C), and the latter was at issue only forhe higher dose of cannabis. Similarly, feeling “high,”stoned,” or “impaired” were less problematic for theower strength cigarettes (Fig 5A–C). In general, side ef-ects and changes in mood were relatively inconsequen-ial. These findings are consistent with the observationhat many patients find treatment with cannabis to be aatisfactory experience.65,72 A reasonable explanationould be that a patient self-titrates cannabis, balancingnalgesia against side effects. However, beyond the be-ign psychoactive effects, administration of cannabisay be deleterious in that it impairs cognition. Previous
nvestigations have reviewed processing speed, atten-ion, memory, reaction time, and psychomotor abilitiesfter smoking cannabis.25,53,58 Results have varied andepend on several variables including cigarette potency,
esponses Regressed on a Panel of Blood
STANDARD
ERROR CONFIDENCE INTERVAL P VALUE
0.30 0.13 1.00 .0190.27 0.07 1.00 .0290.24 0.31 1.00 .0020.23 �0.69 0.22 .3150.004 0.00 0.02 .0070.004 0.00 0.01 .0610.003 0.00 0.01 .0310.003 �0.01 0.00 .6620.10 �0.20 0.20 .9710.09 �0.19 0.17 .8940.08 �0.27 0.05 .1940.08 �0.23 0.08 .3340.13 �0.29 0.20 .7060.11 �0.25 0.19 .7830.10 �0.14 0.25 .5930.003 �0.02 �0.01 .6620.006 �0.03 0.00 .0360.006 �0.01 0.01 .5740.006 �0.02 0.01 .4240.005 �0.01 0.01 .734
change in the respective blood level. Significant results (P � .05) are bolded.
ic R
N
NT
moking technique, individual variation in bioavailabil-

isamTmiccspbrmccbbcras
clco(agjetbssccmrw
crcaarpuamoattdvuc
wiammhaoPgpomocs
pmcpntmvttcmspvapte
A
fspsFaawbtNMioaRooh
518 Analgesic Response to Cannabis Cigarettes
ty, and previous exposure to the drug. As in the presenttudy, although analgesia appears to be consistentcross the low and high dosages, cognitive changes wereore problematic with a high dose of delta-9-THC.4,35
his suggests that a therapeutic window may exist thatight be exploited for clinical purposes. However, there
s an additional problem with using cannabis in thehronic pain population. Severe pain coupled with psy-hological distress is associated with below averagecores on cognitive performance tests.43,44,76 As in theserevious reports, the patients in our study were eitherelow or nearly below the cutoff for impairment beforeeceiving study medication. Our study indicates thatodest declines in cognitive performance occur with
annabis, particularly in learning and recall, and espe-ially at higher doses. In combination with the deficits inaseline neurocognitive performance, however, canna-is compounds this problem. This finding necessitatesaution in the prescribing of medical marijuana for neu-opathic pain, especially in instances in which learningnd memory are integral to a patient’s work and life-tyle.Further vigilance is warranted in young patients be-
ause cannabis use in adolescence increases the risk ofater schizophrenia-like psychoses, especially in geneti-ally susceptible individuals.24 There is an increased riskf a psychosis in those who have ever used cannabispooled adjusted odds ratio � 1.41; 95% CI, 1.20–1.65)nd a dose-response effect, with greater risk in sub-roups consuming cannabis very frequently (pooled ad-
usted odds ratio � 2.09; 95% CI, 1.54–2.84).54 Theseffects of cannabis may be consequent on its impact onhe dopamine system.54 There is less evidence of canna-is playing a role in other mental disorders (ie, depres-ion and anxiety). Further research is needed to under-tand the biological mechanisms underlying the effects ofannabis on psychiatric conditions, but the health risks ofannabis in patients with any propensity for psychosisandate caution in this population. Consistent with this
isk, a history of schizophrenia and bipolar depressionere exclusionary criteria in the present study.It is tempting to speculate that a lower strength of
annabis might avoid or at least reduce the adverse neu-ocognitive profile noted above. As the 7% and 3.5%annabis were equianalgesic, it would be certainly beppropriate to test a lower concentration to see if thenalgesic profile is maintained while cognitive decline iseduced or even obviated. Even if the pain-relievingroperties are less than robust, a case could be made forsing the lowest possible strength despite attenuation innalgesic potency. Moreover, as polypharmacy is com-on in the management of chronic pain,12 the addition
f the lowest effective dose of cannabis to another an-lgesic drug (ie, anticonvulsant, opioid, etc) might leado an effective treatment of a neuropathic pain condi-ion otherwise treatment resistant.18,19 Additionally, theiversion potential could be reduced as cannabis with aery low THC content is less desirable for recreationalse.34 In addition to evaluating the efficacy of a lower
oncentration, the potential of use a cognitive enhancer sith cannabis to reverse or at least mitigate cognitivempairment might be considered in the future. Such angent (eg, modafinil) has been used with psychotropicedications to reduce sedation and cognitive impair-ent.9,10,49,67,68,74 New cognitive enhancers are on the
orizon as researchers test cholinergic agents, biogenicmines, and neuropeptides to treat learning and mem-ry deficits associated with neurodegenerative states.sychostimulants, excitatory amino acids, and a hetero-eneous group of compounds of diverse chemical com-osition that allegedly facilitate learning and memory orvercome natural or induced cognitive impairments50
ight someday be useful in combination with cannabisr cannabinoids currently thought to be undesirable be-ause of the depressant effects on the central nervousystem that limit their use.15
In addition to the issues discussed above, the noxiousyrolytic byproducts released through combustion re-ain a public health deterrent to the use of smoked
annabis.42,51 However, a method has been devised torovide a safer and more efficient delivery system. Can-abis vaporization is a technique that avoids the produc-ion of irritating respiratory toxins by heating the herbaledicine to a temperature at which active cannabinoid
apors form but below the point of combustion whereoxins are released.29,52 Gas chromatograph/mass spec-rometer analysis reveals that the gas phase of the vaporonsists overwhelmingly of cannabinoids. In contrast,ore than 111 compounds are identifiable in samples of
moked cannabis, including several potentially harmfulolynuclear aromatic hydrocarbons.30 In a pilot study in-olving healthy volunteers,3 vaporization delivered ther-peutic doses of cannabinoids with a drastic reduction inyrolytic smoke compounds. It is reasonable to assumehat future clinical trials will utilize this alternative deliv-ry method.
cknowledgmentsWe acknowledge the University of California Center
or Medicinal Cannabis Research which provided criticalupport and guidance. They derived direct financial sup-ort from the California legislature as well as logistic andcientific support from several national stakeholders (ie,ood and Drug Administration, Department of Healthnd Human Services, National Institute on Drug Abuse,nd the Drug Enforcement Agency), whose assistanceas invaluable. This publication was also made possibley Grant Number UL1 RR024146 from the National Cen-er for Research Resources (NCRR), a component of theational Institutes of Health (NIH), and NIH Roadmap foredical Research. Its contents are solely the responsibil-
ty of the authors and do not necessarily represent thefficial view of NCRR or NIH. Information on NCRR isvailable at http://www.ncrr.nih.gov/. Information one-engineering the Clinical Research Enterprise can bebtained from http://nihroadmap.nih.gov/clinicalresearch/verview-translational.asp. We also thank Tom Lang foris editorial assistance in the preparation of the manu-
cript.
R
1IM
2KHc
3iA
4ii2
5tp
6Kel
7Vo1
8pa
9a7
1sC
1bpc
1uS
1t
1oERc8
1Rts
1Tsi
519ORIGINAL REPORT/Wilsey et al
1pP
1n
1ta
2ms3
2ocv
2J
2p
2ut
2ch
2Cm9
2fco
2iN
2MB
3ip2
3aD
3qpY
3oCc2
3oc
eferences
. Ad Hoc Group of Experts, Report to the Director, Nationalnstitutes of Health: Workshop on the Medical Utility of
arijuana, February 19-20, 1997
. Abrams DI, Jay CA, Shade SB, Vizoso H, Reda H, Press S,elly ME, Rowbotham MC, Petersen KL: Cannabis in painfulIV-associated sensory neuropathy: A randomized placebo-ontrolled trial. Neurology 68:515-521, 2007
. Abrams DI, Vizoso HP, Shade SB, Jay C, Kelly ME, Benow-tz NL: Vaporization as a smokeless cannabis delivery system:
pilot study. Clin Pharmacol Ther 82:572–578, 2007
. Azorlosa JL, Heishman SJ, Stitzer ML, Mahaffey JM: Mar-juana smoking: Effect of varying delta 9-tetrahydrocannab-nol content and number of puffs. J Pharmacol Exp Ther61:114-122, 1992
. Barnes MP: Sativex: Clinical efficacy and tolerability in thereatment of symptoms of multiple sclerosis and neuro-athic pain. Exp Opin Pharmacother 7:607-615, 2006
. Beglinger LJ, Gaydos B, Tangphao-Daniels O, Duff K,areken DA, Crawford J, Fastenau PS, Siemers ER: Practiceffects and the use of alternate forms in serial neuropsycho-ogical testing. Arch Clin Neuropsychol 20:517-529, 2005
. Benedict RH, Schretlen D, Groninger L, Brandt J: Hopkinserbal Learning Test-Revised: Normative data and analysisf inter-form and test-retest reliability. Clin Neuropsychol2:43-55, 1998
. Benedict RH, Zgaljardic DJ: Practice effects during re-eated administrations of memory tests with and withoutlternate forms. J Clin Exp Neuropsychol 20:339-352, 1998
. Berigan TR: Modafinil treatment of excessive sedationssociated with divalproex sodium. Can J Psychiatry 49:72-3, 2004
0. Berigan TR: Modafinil treatment of excessive daytimeedation and fatigue associated with topiramate. Prim Careompanion J Clin Psychiatry 4:249-250, 2002
1. Berman JS, Symonds C, Birch R: Efficacy of two cannabisased medicinal extracts for relief of central neuropathicain from brachial plexus avulsion: Results of a randomisedontrolled trial. Pain 112:299-306, 2004
2. Black DR, Sang CN: Advances and limitations in the eval-ation of analgesic combination therapy. Neurology 65:S3-6, 2005
3. Bostrom BA: Gonzales v Raich. In the Supreme Court ofhe United States. Issues Law Med 21:47-56, 2005
4. Bruehl S, Harden RN, Galer BS, Saltz S, Bertram M, Back-nja M, Gayles R, Rudin N, Bhugra MK, Stanton-Hicks M:xternal validation of IASP diagnostic criteria for Complexegional Pain Syndrome and proposed research diagnosticriteria: International Association for the Study of Pain. Pain1:147-154, 1999
5. Campbell FA, Tramer MR, Carroll D, Reynolds DJ, MooreA, McQuay HJ: Are cannabinoids an effective and safereatment option in the management of pain? A qualitativeystematic review. BMJ 323:13-16, 2001
6. Carey CL, Woods SP, Gonzalez R, Conover E, MarcotteD, Grant I, Heaton RK: Predictive validity of global deficitcores in detecting neuropsychological impairment in HIV
nfection. J Clin Exp Neuropsychol 26:307-319, 2004 m7. Chait LD, Corwin RL, Johanson CE: A cumulative dosingrocedure for administering marijuana smoke to humans.harmacol Biochem Behav 29:553-557, 1988
8. Cichewicz DL: Synergistic interactions between cannabi-oid and opioid analgesics. Life Sci 74:1317-1324, 2004
9. Cichewicz DL, McCarthy EA: Antinociceptive synergy be-ween delta(9)-tetrahydrocannabinol and opioids after oraldministration. J Pharmacol Exp Ther 304:1010-1015, 2003
0. Clark WC, Janal MN, Zeidenberg P, Nahas GG: Effects ofoderate and high doses of marihuana on thermal pain: A
ensory decision theory analysis. J Clin Pharmacol 21:299S-10S, 1981
1. Collie A, Maruff P, Darby DG, McStephen M: The effectsf practice on the cognitive test performance of neurologi-ally normal individuals assessed at brief test-retest inter-als. J Int Neuropsychol Soc 9:419-428, 2003
2. Day R, Wodak A, Chesher G: Cannabis and suicide. MedAust 160:731, 1994
3. Dellemijn P: Are opioids effective in relieving neuro-athic pain? Pain 80:453-462, 1999
4. Di Forti M, Morrison PD, Butt A, Murray RM: Cannabisse and psychiatric and cognitive disorders: The chicken orhe egg? Curr Opin Psychiatry 20:228-234, 2007
5. Dornbush RL, Kokkevi A: Acute effects of cannabis onognitive, perceptual, and motor performance in chronicashish users. Ann N Y Acad Sci 282:313-322, 1976
6. Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM:linical importance of changes in chronic pain intensityeasured on an 11-point numerical pain rating scale. Pain
4:149-158, 2001
7. Galer BS, Bruehl S, Harden RN: IASP diagnostic criteriaor complex regional pain syndrome: A preliminary empiri-al validation study: International Association for the Studyf Pain. Clin J Pain 14:48-54, 1998
8. Galer BS, Jensen MP: Development and preliminary val-dation of a pain measure specific to neuropathic pain: Theeuropathic Pain Scale. Neurology 48:332-338, 1997
9. Gieringer D: Marijuana research: Waterpipe study.APS (Multidisciplinary Association for Psychedelic Studies)
ull 6:59-66, 1996
0. Gieringer D, St. Laurent J, Goodrich S: Cannabis vapor-zer combines efficient delivery of THC with effective sup-ression of pyrolytic compounds. J Cannabis Ther Vol. 4,004
1. Greenwald MK, Stitzer ML: Antinociceptive, subjectivend behavioral effects of smoked marijuana in humans.rug Alcohol Depend 59:261-275, 2000
2. Hansson P, Lindblom U: Hyperalgesia assessed withuantitative sensory testing in patients with neurogenicain, in Willis WDJ (ed): Hyperalgesia and Allodynia. Nework, Raven Press, 1992, pp 335-343
3. Harden RN, Bruehl S, Galer BS, Saltz S, Bertram M, Back-nja M, Gayles R, Rudin N, Bhugra MK, Stanton-Hicks M:omplex regional pain syndrome: Are the IASP diagnosticriteria valid and sufficiently comprehensive? Pain 83:211-19, 1999
4. Harder S, Rietbrock S: Concentration-effect relationshipf delta-9-tetrahydrocannabiol and prediction of psy-hotropic effects after smoking marijuana. Int J Clin Phar-
acol Ther 35:155-159, 1997
3Mt2
3frF
3hmcP
3aI
3TRd
4Cnr
4enr
4Rfd1
4Nc
4Ap
4nd
4mb
4M1
4si
4oc
5wC
5Wts
5b4
5jr1
5Jcr
5pC
5e1
5N
5r5
5tp
6ca
6p2
6cm
6t6
6ac
6spt
6Jr8
6Mat
6ban
6se
7
520 Analgesic Response to Cannabis Cigarettes
5. Hart CL, van Gorp W, Haney M, Foltin RW, FischmanW: Effects of acute smoked marijuana on complex cogni-
ive performance. Neuropsychopharmacology 25:757-765,001
6. Heaton R, Grant I, Matthews C: Comprehensive normsor an expanded Halstead-Reitan Battery: Demographic cor-ections, research findings, and clinical applications. Odessa,L, Psychological Assessment Resources, Inc., 1991
7. Heaton R, Miller S, Taylor M, Grant I: Revised Compre-ensive norms for an expanded Halstead-Reitan Battery: De-ographically adjusted neuropsychological norms for Afri-
an American and Caucasian adults, in Lutz F (ed):sychological Assessment Resources, Inc., 2004
8. Heaton R, Taylor M, Manly J (eds): Demographic effectsnd use of demographically corrected norms with the WAIS-II and WMS-III. San Diego, CA, Academic Press, 2004
9. Heaton RK, Marcotte TD: Clinical Neuropsychologicalests and Assessment Techniques, in Boller F, Grafman J,izzolatti G (eds): Handbook of Neuropsychology. Amster-am, Elsevier Science BV, 2000
0. Herkenham M, Lynn AB, Johnson MR, Melvin LS, deosta BR, Rice KC: Characterization and localization of can-abinoid receptors in rat brain: A quantitative in vitro auto-adiographic study. J Neurosci 11:563-583, 1991
1. Herzberg U, Eliav E, Bennett GJ, Kopin IJ: The analgesicffects of R(�)-WIN 55,212-2 mesylate, a high affinity can-abinoid agonist, in a rat model of neuropathic pain. Neu-osci Lett 221:157-160, 1997
2. Hiller FC, Wilson FJ Jr, Mazumder MK, Wilson JD, BoneC: Concentration and particle size distribution in smokerom marijuana cigarettes with different delta 9-tetrahy-rocannabinol content. Fundam Appl Toxicol 4:451-454,984
3. Iezzi T, Archibald Y, Barnett P, Klinck A, Duckworth M:eurocognitive performance and emotional status inhronic pain patients. J Behav Med 22:205-216, 1999
4. Iezzi T, Duckworth MP, Vuong LN, Archibald YM, Klinck: Predictors of neurocognitive performance in chronic painatients. Int J Behav Med 11:56-61, 2004
5. Johanek LM, Simone DA: Activation of peripheral can-abinoid receptors attenuates cutaneous hyperalgesia pro-uced by a heat injury. Pain 109:432-442, 2004
6. Kelly TH, Foltin RW, Fischman MW: Effects of smokedarijuana on heart rate, drug ratings and task performance
y humans. Behav Pharmacol 4:167-178, 1993
7. Klove H: Clinical neuropsychology, in Forster FE (ed): Theedical Clinics of North America. New York, NY, Saunders,
963
8. Lorber L: Gonzales v Raich: the US Supreme Court’s con-ideration captured the public policy debate about the med-cal use of marijuana. Gend Med 2:124-130, 2005
9. Makela EH, Miller K, Cutlip WD 2nd: Three case reportsf modafinil use in treating sedation induced by antipsy-hotic medications. J Clin Psychiatry 64:485-486, 2003
0. Malik R, Sangwan A, Saihgal R, Jindal DP, Piplani P: To-ards better brain management: Nootropics. Curr Medhem 14:123-131, 2007
1. Matthias P, Tashkin DP, Marques-Magallanes JA,ilkins JN, Simmons MS: Effects of varying marijuana po-
ency on deposition of tar and delta9-THC in the lung during
moking. Pharmacol Biochem Behav 58:1145-1150, 1997 b2. McPartland JM, Pruitt PL: Medical marijuana and its usey the immunocompromised. Altern Ther Health Med 3:39-5, 1997
3. Miller LL, McFarland D, Cornett TL, Brightwell D: Mari-uana and memory impairment: Effect on free recall andecognition memory. Pharmacol Biochem Behav 7:99-103,977
4. Moore TH, Zammit S, Lingford-Hughes A, Barnes TR,ones PB, Burke M, Lewis G: Cannabis use and risk of psy-hotic or affective mental health outcomes: A systematiceview. Lancet 370:319-328, 2007
5. Noyes R Jr, Brunk SF, Avery DA, Canter AC: The analgesicroperties of delta-9-tetrahydrocannabinol and codeine.lin Pharmacol Ther 18:84-89, 1975
6. Noyes R Jr, Brunk SF, Baram DA, Canter A: Analgesicffect of delta-9-tetrahydrocannabinol. J Clin Pharmacol 15:39-143, 1975
7. Okie S: Medical marijuana and the Supreme Court.Engl J Med 353:648, 2005
8. Pope HG Jr, Gruber AJ, Yurgelun-Todd D: Residual neu-opsychologic effects of cannabis. Curr Psychiatry Rep 3:507-12, 2001
9. Price DD, Harkins SW, Baker C: Sensory-affective rela-ionships among different types of clinical and experimentalain. Pain 28:297-307, 1987
0. Price DD, Harkins SW, Rafii A, Price C: A simultaneousomparison of fentanyl’s analgesic effects on experimentalnd clinical pain. Pain 24:197-203, 1986
1. Price DD, Von der Gruen A, Miller J, Rafii A, Price C: Asychophysical analysis of morphine analgesia. Pain 22:261-69, 1985
2. Rog DJ, Nurmikko TJ, Friede T, Young CA: Randomized,ontrolled trial of cannabis-based medicine in central pain inultiple sclerosis. Neurology 65:812-819, 2005
3. Rowbotham MC: Mechanisms of neuropathic pain andheir implications for the design of clinical trials. Neurology5:S66-S73, 2005
4. Russo E, Guy GW: A tale of two cannabinoids: The ther-peutic rationale for combining tetrahydrocannabinol andannabidiol. Med Hypotheses 66:234-246, 2006
5. Schnelle M, Grotenhermen F, Reif M, Gorter RW: [Re-ults of a standardized survey on the medical use of cannabisroducts in the German-speaking area]. Forsch Komplemen-armed 6(Suppl)3:28-36, 1999
6. Tsou K, Brown S, Sanudo-Pena MC, Mackie K, WalkerM: Immunohistochemical distribution of cannabinoid CB1eceptors in the rat central nervous system. Neuroscience3:393-411, 1998
7. Turner DC, Clark L, Dowson J, Robbins TW, Sahakian BJ:odafinil improves cognition and response inhibition in
dult attention-deficit/hyperactivity disorder. Biol Psychia-ry 55:1031-1040, 2004
8. Turner DC, Clark L, Pomarol-Clotet E, McKenna P, Rob-ins TW, Sahakian BJ: Modafinil improves cognition andttentional set shifting in patients with chronic schizophre-ia. Neuropsychopharmacology 29:1363-1373, 2004
9. Van Gorp WG, Lamb DG, Schmitt FA: Methodologic is-ues in neuropsychological research with HIV-spectrum dis-ase. Arch Clin Neuropsychol 8:17-33, 1993
0. Vaughan CW, Christie MJ: An analgesic role for canna-
inoids. Med J Aust 173:270-272, 2000
7p
7nt
7fP
7m
7tT
7Tfo2
7
521ORIGINAL REPORT/Wilsey et al
1. Walker JM, Hohmann AG: Cannabinoid mechanisms ofain suppression. Handb Exp Pharmacol 509-554, 2005
2. Ware MA, Doyle CR, Woods R, Lynch ME, Clark AJ: Can-abis use for chronic non-cancer pain: Results of a prospec-ive survey. Pain 102:211-216, 2003
3. Ware MA, Gamsa A, Persson J, Fitzcharles MA: Cannabisor chronic pain: Case series and implications for clinicians.ain Res Manag 7:95-99, 2002
4. Webster L, Andrews M, Stoddard G: Modafinil treat-
ent of opioid-induced sedation. Pain Med 4:135-140, 2003 t5. Wechsler D: Wechsler Adult Intelligence Scale, Third Edi-ion, Administration and Scoring Manual. San Antonio, TX,he Psychological Corporation, Harcourt Brace & Co, 1997
6. Weiner DK, Rudy TE, Morrow L, Slaboda J, Lieber S:he relationship between pain, neuropsychological per-ormance, and physical function in community-dwellinglder adults with chronic low back pain. Pain Med 7:60-70,006
7. Williamson EM, Evans FJ: Cannabinoids in clinical prac-
ice. Drugs 60:1303-1314, 2000