a prospective, randomized trial of transapical transcatheter aortic valve implantation vs. surgical...
TRANSCRIPT

A Prospective, Randomized Trial of Transapical Transcatheter Aortic
Valve Implantation vs. Surgical Aortic Valve Replacement in Operable Elderly Patients
with Aortic Stenosis
The STACCATO Trial
Hans H. M. Nielsen, Kaj E. Klaaborg, Henrik Nissen, Kim Terp, Poul E. Mortensen, Bo J. Kjeldsen, Carl-Johan
Jakobsen, Henning R. Andersen, Lars R. Krusell, Henrik Egeblad, Evald H. Christiansen, Jacob R. Greissen, Erik
Sloth, Leif Thuesen, Vibeke E. Hjortdal

Conflicts of interests for Leif Thuesen, M.D.
Edwards Lifesciences:
Physician proctor
A Prospective, Randomized Trial of Transapical Transcatheter Aortic
Valve Implantation vs. Surgical Aortic Valve Replacement in Operable Elderly Patients with
Aortic Stenosis
The STACCATO Trial
Background
Transcatheter aortic valve implantation (TAVI) has become a treatment option for patients with aortic valve stenosis, who are not amenable or at high risk to surgical valve replacement (SAVR)
The role of TAVI in surgically lower risk patients remains to be defined

Purpose
In a prospective, randomized trial to compare transapical transcatheter aortic valve implantation (a-TAVI) with surgical aortic valve replacement (SAVR) in operable elderly patients

Funding
Academic study funded by the participating centers
We received a study grant from the Danish Heart Foundation
The study was conducted without relationship to the industry

Material and methods
Planned number of patients
n= 200
Randomization
1:1
Participating centers
Departments of Cardiothoracic Surgery and Cardiology, Aarhus University Hospital and Odense University Hospital, Denmark

Criteria of inclusion
• Valvular aortic stenosis (valve area <1cm2)
• Age ≥70 or 75 yrs
• Condition accessible both by SAVR and a-TAVI
• Expected survival >1 year following successful treatment

Criteria of exclusion
• Coronary artery disease to be treated by PCI or CABG
• Previous myocardial infarction or cardiac surgery or PCI within 12 months
• Need for emergency surgery
• Unstable cardiac condition (assist device or inotropes)
• Stroke within 1 month
• Reduced pulmonary function
• Renal failure to be treated by hemodialysis

Primary endpoint
• The composite of 30-day all cause mortality, major stroke, and/or renal failure

Secondary endpoints
• Myocardial infarction
• Operation for bleeding
• Permanent pacemaker treatment
• Duration of hospital stay
• Echocardiographic parameters (aortic valve area, peak aortic valve gradient, aortic valve leakage, left ventricular ejection fraction)
• NYHA class, SF-36 composite physical and mental functional scores

Definitions
For endpoint definitions, we used the Valve Academic Research Consortium recommendations

Sample size
We anticipated a primary endpoint rate of 13.5% in the SAVR group based on Western Denmark Heart Registry SAVR data on patients aged ≥70 yrs from 1998 through 2008.
The estimated event rate of 2.5% in the a-TAVI group was based on our experience from non-operable patients with significantly higher risk than the study population. At study initiation, our a-TAVI event rates were 0%.
Given an alpha of 5% and a beta of 80%, 96 patients should be included in each group to document the difference. Therefore, we planned for inclusion of 200 patients.

Premature termination
After inclusion of 70 patients, the study was terminated prematurely after advice from the Data Safety Monitoring Board
Conduct of the study• June 2008; protocol
─ Scenario; a-TAVI safe, predictable procedure
• September 2008; MEC approval
• November 2008; 1. patient included
• Study on hold after inclusion of 11 patients
─ 3 potentially severe adverse events in the a-TAVI group
─ Contact with DSMB and MEC
─ Inclusion and exclusion criteria modified (age limit increased to 75 yrs, earlier heart operation reason for exclusion)
─ Inclusion resumed
• Study on hold May 2011
─ DSMB advised study termination due to an excess of events in the a-TAVI group

Assessed for eligibility(n= 525)
Randomized (n= 72)Excluded after randomization (n= 2)
Excluded (n = 453)•Medical Tx (n=24)•Surgical Tx (n=285)•TAVI (n= 144)
a-TAVI (n=34)
SAVR (n=36)
Patient flow-diagram

Baseline characteristics
Characteristics a-TAVI SAVR p Value
Age (yrs) 80±3.6 82±4.4 0.15
Male sex 9/34 (26.5) 12/36 (33.3) 0.61
Diabetes 1/34 (2.9) 3/36 (8.3) 0.62
Cerebral vascular disease 1/34 (2.9) 1/36 (2.8) 1.00
Peripheral vascular disease 2/34 (5.9) 3/36 (8.3) 1.00
COPD 1/34 (2.9) 1/36 (2.8) 1.00
Creatinine level >200µmol/L 1/34 (2.9) 0/36 (0.0) 0.49
Logistic EuroSCORE 9.4±3.9 10.3±5.8 0.25
STS score 3.1±1.5 3.4±1.2 0.43
NYHA class III or IV 18/34 (58.1) 16/36 (44.4) 0.63
EF (%) 56.5±9.7 56.3±10 0.92
Aortic valve area (cm2) 0.66±0.17 0.71±0.17 0.21
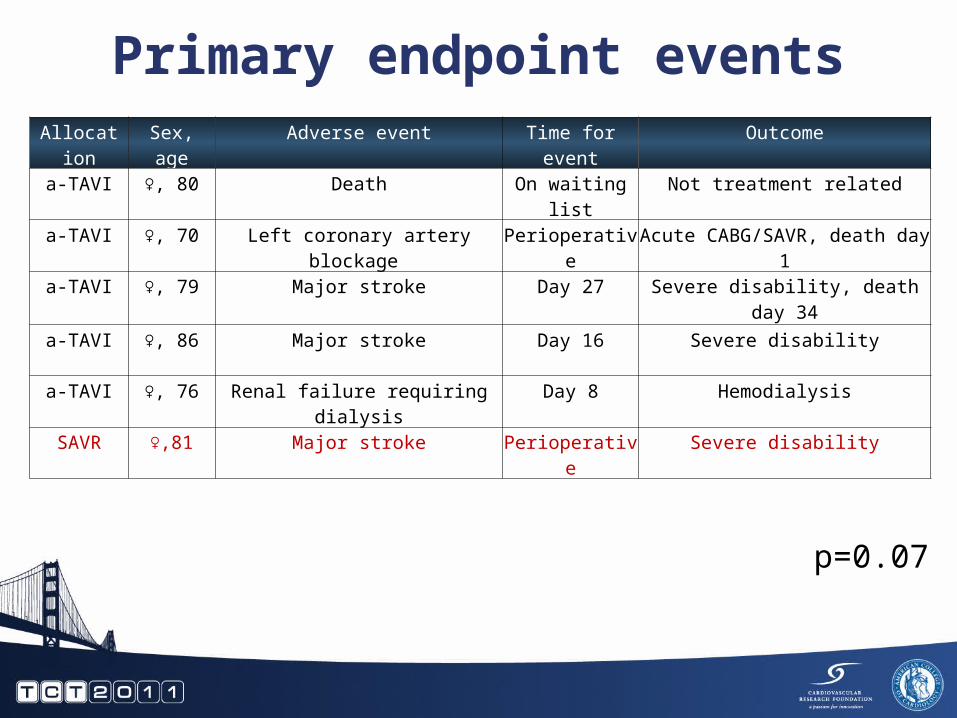
Primary endpoint eventsAllocation Sex, age Adverse event Time for event Outcome
a-TAVI ♀, 80 Death On waiting list Not treatment related
a-TAVI ♀, 70 Left coronary artery blockage Perioperative Acute CABG/SAVR, death day 1
a-TAVI ♀, 79 Major stroke Day 27 Severe disability, death day 34
a-TAVI ♀, 86 Major stroke Day 16 Severe disability
a-TAVI ♀, 76 Renal failure requiring dialysis Day 8 Hemodialysis
SAVR ♀,81 Major stroke Perioperative Severe disability
p=0.07

Other events at 3 monthsAllocation Sex, age Adverse event Time for event Outcome
a-TAVI ♀, 81 Transient ischemic attack with later major stroke
Perioperative Partial recovery
a-TAVI ♂, 80 Left main occlusion during balloon valvuloplasty
Perioperative SAVR, recovery
a-TAVI ♀, 79 Aortic rupture Perioperative Emergency implantation of homograft, recovery
a-TAVI ♂, 75 Severe paravalvular leakage Perioperative SAVR, recovery
a-TAVI ♀, 82 Severe paravalvular leakage Perioperative SAVR, death day 38
a-TAV ♂, 78 THV embolization upstream Perioperative Implantation of another THV, recovery
a-TAVI ♀, 80 Abnormally positioned heart Perioperative SAVR, recovery
a-TAVI ♀, 86 Bleeding Postoperative Re-operation, recovery
SAVR ♀,83 Conversion to a-TAVI because of intrathoracic goiter
Perioperative a-TAVI, recovery
SAVR ♂,82 Bleeding Postoperative Re-operation, recovery

Aortic valve areaBaseline and after treatment
p=0.15
p=0.15
‡ ‡
‡ p<0.0001 as compared to pretreatment values
cm2

Peak aortic gradientBaseline and after treatment
p=0.07
‡ p<0.0001 as compared to pretreatment values
‡ ‡
mmHg

Paravalvular leakageafter treatment
n=13(43%)
n=13(43%)
n=4 (13%)
n=33(94%)
n=2(6%)
p<0.001

NYHA classBaseline and at 3 months
p=0.001p=0.01
p=0.16n

Other outcome parametersParameters a-TAVI SAVR p Value
Myocardial infarction *n/N (%)
0/0 (0) 0/0 (0) 1.00
Permanent pacemakern/N (%)
2/34 (5.8) 1/36 (2.7) 0.52
Hospital stay(days)
8.8±6.7 7.6±2.4 0.32
Composite physical functional score before treatment (%)
35±10, n=27 37±12, n=32 0.48
Composite physical functional score 3 months after treatment (%)
42±14, n=27‡ 43±15, n=32‡ 0.91
Composite mental functional score before treatment (%)
47±10, n=27 46±17, n=32 0.66
Composite mental functional score 3 months after treatment (%)
53±14, n=27‡ 50±17, n=32‡ 0.44
* Valve Academic Research Consortium definition‡ ns; as compared to pretreatment values

Limitations
• Premature study termination; only one third of the anticipated number of patients included
• The excess of adverse events in the a-TAVI group might be a play of chance
• Only two centers were actively including. The SAVR results were excellent, but a-TAVI results might have been different with participation of more centers
• Multi-slice computed tomography (MSCT) was not used in the preoperative assessment
Issues for discussion• Stroke
~ Perioperative; 1 major stroke in the SAVR group, 1 TIA in the a-TAVI group
~ Two major strokes after 2-4 weeks in the a-TAVI group during dual antiplatelet treatment
• Paravalvular leakage~ Absent in the SAVR group
~ Moderate to severe leakage in 13% of a-TAVI patients, probably because of valve under sizing. Preoperative MSCT might have optimized valve sizing
• Perioperative coronary artery occlusion~ Might have been avoided by preoperative MSCT assessment
of annulus to left main distance and valve/left main relation

Conclusion
• In its present phase of development, transapical transcatheter aortic valve implantation seems inferior to surgical aortic valve replacement in operable elderly patients

Final remarks
• After study termination, our procedures have been optimized by routine preoperative MSCT assessment and by availability of the 29 mm valve
• Further improvement is likely to take place with improved devices and pre-procedure assessment