a physician’s guide to bariatric & metabolic surgery
TRANSCRIPT

A physician’s guide to Bariatric & Metabolic Surgery
Nick Carter Consultant Upper GI & Bariatric Surgeon
Portsmouth Hospitals NHS Trust
Royal College Physicians GP Update Southampton April 2017

A physician’s guide to Bariatric & Metabolic Surgery
• What it is
• How we do it
• What is the evidence
• What are the results
• What are the problems


Professor Rachel Batterham BBC 2
April 2017


Obesity and related co-morbidities
[1] Adapted from Ashrafian H et al. Circulation 2008;118:2091–102.
Obesity
T2D
CV
Retinopathy
Neuropathy
Nephropathy
Hypertension
Hypercholesterolaemia
IHD/TIA/CVA
Obstructive Sleep Apnoea
Musculo-skeletal problems
Idiopathic
intracranial
hypertension
GORD
PCOS
ED/Male infertility
Thromboembolic
disease
Nutritional deficiencies Ferritin Folate Vit D
Gallstones, Urinary stress incontinence Dysmenorrhea or amenorrhea Osteoarthritis, Depression Cancer : Colon, Breast, Endometrial, Oesophageal, Gallbladder

How do you refer a patient for surgery?
• NICE criteria
• Local Tier 3 program • Weigh Ahead (Spire NHS service) - Southampton
• Integrated Complex Obesity Service (ICOS) - Portsmouth

Bariatric surgery is a treatment option for anyone with a BMI≥40 Offer an expedited assessment for people with a BMI≥35 with onset of type 2 diabetes in past 10 years Consider an assessment for people with a BMI of 30-34.9 with onset of type 2 diabetes within 10 years Consider an assessment for people of Asian origin with onset of type 2 diabetes at a lower BMI than other populations Bariatric surgery is the option of choice for adults with BMI >50 when other interventions have not been effective People fitting the above criteria are also required to be receiving or to receive assessment in a specialist weight management service before referral to a surgical team


Tier 4
MDT
Physician
Anaesthetist
Dietitian Specialist
Nurse
Psychologist Surgeon

Surgery
• 2 week liver reducing diet
• Laparoscopic surgery
• 3x12mm, 2x5mm ports
• 1 – 1½ hours
• Drinking same day
• Sloppy diet day 1 post op
• Home day 1 or 2
• 8 week post operative diet







Bariatric Surgery Follow Up
• 2/52 LMWH, 3/12 PPI
• LRGYB/LVSG – Multivitamins, Calcium, Iron
• 2 year follow by hospital
• 3/12 visits
– Dietitian, Nurse specialist, Surgeon, Physician
• Monitor vitamin levels

22 randomised controlled trials of bariatric surgery found that it is more effective and cost effective for the treatment of severe obesity than non-surgical measures after two years.

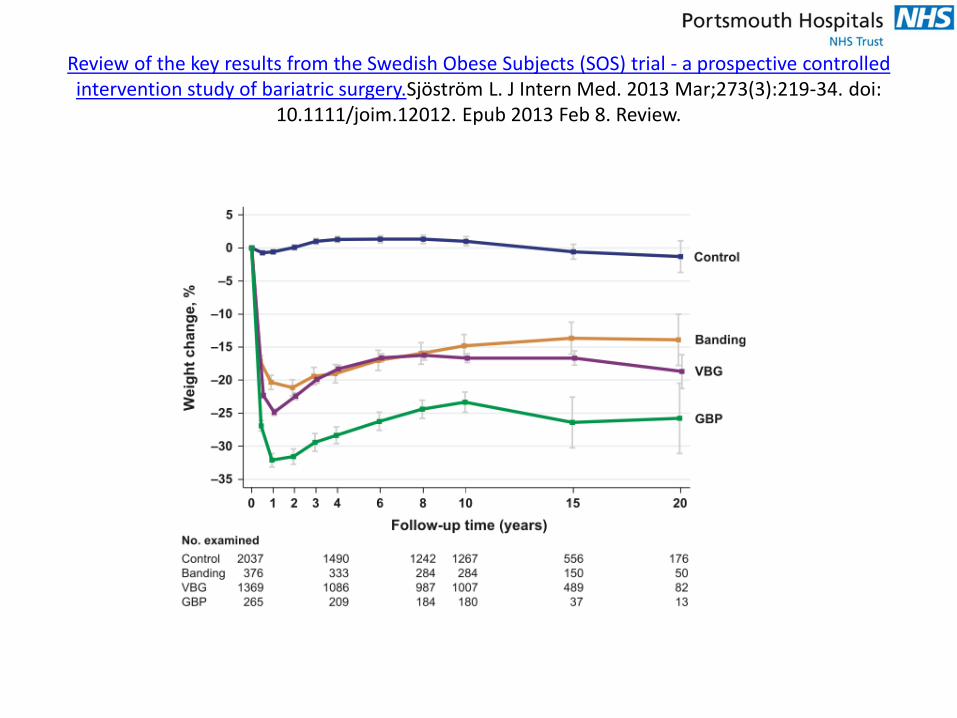
Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery.Sjöström L. J Intern Med. 2013 Mar;273(3):219-34. doi:
10.1111/joim.12012. Epub 2013 Feb 8. Review.

Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery.Sjöström L. J Intern Med. 2013 Mar;273(3):219-34. doi:
10.1111/joim.12012. Epub 2013 Feb 8. Review.

2500 surgical patients, 7400 matched controls
JAMA. 2015;313(1):62-70. doi:10.1001/jama.2014.16968


Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery.Sjöström L. J Intern Med. 2013 Mar;273(3):219-34. doi:
10.1111/joim.12012. Epub 2013 Feb 8. Review.

Body of Evidence High Quality (Level I & II-1,2) Studies on Bariatric / Metabolic Surgery in Diabetic Patients
Investigator Study Type # Diabetic Patients Primary Endpoint Study Duration
Carlsson Non-randomized, prospective,
controlled 3429 pts, 2 arms (1658 surgery)
Rate of incident type 2 diabetes mellitus
15 years
STAMPEDE (Schauer)*
RCT, single center 150 pts, 3 arms HbA1c < 6 with or w/o meds Year 1 of
5-year study
Mingrone RCT, single center 60 pts, 3 arms HbA1c < 6.5 without meds 2 years
Buchwald* Systematic Review &
Meta-Analysis 135,000 pts, 621 studies,
888 arms Effect of bariatric surgery on
Type 2 diabetes N/A
Klein* Matched Cohort, Claims data 1600 pts, 2 arms Economic impact & clinical benefits of bariatric surgery
3 years
AHRQ (Segal)* Matched Cohort, Claims data 8400 pts, 2 arms (2100 surgery)
Impact of surgery to reduce utilization of CV meds
Year 1 of 3-year study
Bolen* Matched Cohort, Claims data 14,000 pts, 2 arms
(6300 surgery) % Obesity-related co-
morbidities between groups 5 years
Cohen Non-randomized, prospective 66 pts, 1 arm Safety and % of patients experiencing diabetes
remission
5 years (median)







342 patients, median 48.6 months follow up

For patients with a body mass index (BMI) ≥40, the incremental cost effectiveness ratios for surgery ranged between £2000 and £4000 per quality adjusted life year (QALY) gained over 20 years

Bariatric surgery is a treatment option for some patients with severe obesity, particularly those with type 2 diabetes. Such patients should be assessed for their suitability for this treatment

In patients with diabetes the cost of surgery will be recouped within three years through reduced prescriptions.
Obesity (2011) 19, 581–587



Rates of bariatric surgery per 100,000
0 20 40 60 80 100 120 140 160
UK
Greece
Italy
Czech Republic
Finland
Portugal
Iceland
Austria
USA
France
Sweden
Belgium
Israel

Post Bariatric Surgery Complications
• Gastric Bands – red flags
– Infection over port site
– Epigastric pain
– Reflux
– Dysphagia/vomitting



Post Bariatric Surgery Complications
• Bypass surgery – red flags
– Recurrent severe LUQ pain
– Bowel obstruction
– Nutritional deficiencies
– Ulcers
– Pregnancy

Post Bariatric Surgery Complications
• Sleeve Gastrectomy– red flags
– Reflux
– Vomiting
– Pregnancy




Diagnosis: Initial morbid obesity, weight 192.6 kilos, BMI 59 Treatment: Laparoscopic gastric bypass February 2012. Current weight 114 kilos, BMI 34.


A physician’s guide to Bariatric & Metabolic Surgery
Nick Carter Consultant Upper GI & Bariatric Surgeon
Portsmouth Hospitals NHS Trust
Royal College Physicians GP Update Southampton April 2017

Bile Salt theory

Microbiome theory

A physician’s guide to Bariatric & Metabolic Surgery
Nick Carter Consultant Upper GI & Bariatric Surgeon
Portsmouth Hospitals NHS Trust
Royal College Physicians GP Update Southampton April 2017