a novel mutation of the cathepsin c gene in papillon-lefévre syndrome
TRANSCRIPT
J Periodontol • March 2002
307
A Novel Mutation of the Cathepsin C Genein Papillon-Lefèvre SyndromeVanessa F. Cury,* José E. Costa,* Ricardo S. Gomez,* Wolfanga L. Boson,† Cyro G. Loures,‡and Luiz De Marco†
Background: Papillon-Lefèvre syndrome (PLS) is a disor-der that involves destruction of the periodontium and abnor-mal hyperkeratosis of the palms of the hands and soles of thefeet. Mutations of the lysosomal protease cathepsin C gene(CTSC) have been associated with PLS. However, genotypicand phenotypic correlation has not been established. In thepresent study we investigated the CTSC gene in a Braziliancohort affected by PLS.
Methods: Eight consanguineous members of a kindredwith PLS were studied. DNA was extracted and all exons ofthe gene amplified by the polymerase chain reaction (PCR)using specific primers. Mutations were identified by DNAsequencing of the coding region and introns of the CTSCgene.
Results: Sequence analysis of CTSC from subjects affectedby PLS identified a novel mutation (587T → C) in exon 4, pre-dicted to cause a Leu196Pro amino acid substitution. Threeof 3 subjects were homozygous for cathepsin C mutationsinherited from a common ancestor. One patient was het-erozygous and showed plantar hyperkeratosis without peri-odontal disease. Two other family members were also het-erozygous but did not present palmoplantar hyperkeratosisand/or periodontal disease.
Conclusions: This study describes a novel mutation of thecathepsin C gene in a Brazilian kindred with Papillon-Lefèvresyndrome. J Periodontol 2002;73:307-312.
KEY WORDSCathepsin C; keratoderma, palmoplantar; Papillon-Lefèvresyndrome; perodontitis, early-onset/etiology; geneticfactors.
* Department of Oral Surgery and Pathology, School of Dentistry, Universidade Federal deMinas Gerais, Belo Horizonte, Brazil.
† Department of Pharmacology, Instituto de Ciências Biológicas, Universidade Federal deMinas Gerais.
‡ Private clinic, Belo Horizonte, Brazil.
Papillon-Lefèvre syndrome (PLS) is arare autosomal recessive disordercharacterized by severe aggressive
periodontitis associated with palmoplantarhyperkeratosis.1 It has an estimated preva-lence of 1 in 4 million people and consan-guinity demonstrated in one-third of thecases.2 Both genders are equally affectedand no racial predominance appears toexist.3,4 PLS can manifest itself as early as2 months of age with the appearance ofhyperkeratotic lesions of the hands and feet.Both the deciduous and permanent denti-tions are affected, resulting in prematuretooth loss. The patient is usually totallyedentulous by age 15.2
Severe periodontitis involving the teethin order of their appearance usually startsat the beginning of the primary dentition.After the loss of the primary dentition, thegingival inflammation subsides until sec-ondary dentition eruption, when the processresumes. An increased susceptibility toinfection chiefly leading to pyoderma orfurunculosis has been reported in a num-ber of families.3
The PLS locus has been mapped to chro-mosome 11q14-q21.5-7 Correlation ofphysical and genetic maps of this intervalindicate it includes at least 40 ESTs(expressed sequence tags) and 6 knowngenes including the lysosomal proteasecathepsin C gene (CTSC).8
Cathepsin C, or dipeptidyl amino pepti-dase I, is a lysosomal protease capable ofremoving dipeptides from the amino ter-minus of protein substrates. It is expressedat high levels in the lungs, kidney, placenta,polymorphonuclear leukocytes, alveolarmacrophages, and their precursors. The
1118_IPC_AAP_553092 3/1/02 2:21 PM Page 307

A Novel Mutation of the Cathepsin C Gene in Papillon-Lefèvre Syndrome Volume 73 • Number 3
308
CTSC message is expressed at high levels ina variety of immune cells including poly-morphonuclear leukocytes, macrophages,and their precursors.9 The 4.7 kb CTSC geneconsists of 7 exons.8
The genomic structure of the CTSC genehas been defined and mutations in familiesaffected by PLS described.8,10-13 In addition,mutations in this gene were also found in aJewish-Hindu family with Haim-Munk syn-drome14 and prepubertal periodontitis.15 Themajority of mutations so far described arelocalized to exons 5 to 7, indicating that thisregion is important for enzyme activity.11,15
Although phenotypic variations exist amongpatients affected by PLS,16-18 the associa-tion between such variations and the geneticabnormalities of the CTSC gene is notknown.8,10 The aim of the present study wasto investigate the CTSC gene in a Braziliankindred affected by PLS.
MATERIALS AND METHODSPatientsEight consanguineous members of a kindred with PLSwere studied (Fig. 1). Patients were examined by adermatologist and a dentist who performed a com-plete periodontal examination, and the diagnosis ofPLS was made following previously established crite-ria.1-3 All family members provided written consentfor this study, which was approved by the University’sEthics Committee. Figures 2 to 6 illustrate clinicalmanifestations of PLS seen in patient IV.5.
DNA ExtractionDNA was extracted from whole blood as previouslydescribed.19 Blood samples were obtained frompatients III.2, IV.2, IV.3, IV.5, IV.6, IV.8, IV.9, and IV.10.Briefly, leukocytes were resuspended in 900 µl lysesbuffer (970 mg/ml guanidine HCl; 0.1 mol/L Tris, pH6.4; 0.2 mol/L EDTA, pH 8.0; 26 mg/ml Triton X-100)plus 40 µl silica suspension and incubated at 56°C for10 minutes. After 2 washings with buffer (970 mg/mlguanidine; 0.1 mol/L Tris, pH 6.4), the precipitate wasdried in 70% ethanol and acetone. DNA was thenextracted from silica by TE buffer (10 mmol/L Tris,pH 8.0; 1 mmol/L EDTA, pH 7.4) at 56°C for 10 min-utes.
Polymerase Chain ReactionThe CTSC gene comprises 7 exons that were ampli-fied by the polymerase chain reaction (PCR) usingspecific primers as previously reported.8 PCR reac-tions were performed in a final volume of 50 µl con-taining 100 ng of template DNA, 200 µmol/l dNTPs,10 pmol/L of each primer, and 1.25 U Taq polymerase.Thirty-five cycles of amplification were done in a PTC-
100-60 thermocycler§ at 94°C for 40 seconds; 59°Cfor 60 seconds; 72°C for 90 seconds; and a final exten-sion for 5 minutes at 72°C.
Sequence AnalysisAfter amplification, the single band generated by thespecific PCR product was excised from the 1.5%agarose gel and the DNA fragment extracted accord-
Figure 1.Pedigree of a kindred with Papillon-Lefèvre syndrome (PLS). Subjects III.1 and III.2 aresecond cousins. Subjects IV.5, IV.8, and IV.9 are PLS affected patients. Subject IV.6showed only plantar hyperkeratosis. (��, affected; ��, carrier ; ��,unaffected;��, heterozygous).
Figure 2.Intra-oral view showing generalized severe inflamed and swollengingiva around the remaining teeth (Subject IV.5).
§ MJ Research, Watertown, MA.
1118_IPC_AAP_553092 3/1/02 2:22 PM Page 308

J Periodontol • March 2002 Cury, Costa, Gomez, Boson, Loures, DeMarco
309
Figure 3.Soles of the feet with well demarcated hyperkeratotic lesions (SubjectIV.5).
Figure 4.Dorsal view of hands, showing diffuse hyperkeratotic lesions (SubjectIV.5).
Figure 5.Periapical radiograph showing severe alveolar bone loss of permanentincisors (Subject IV.5).
Figure 6.Panoramic radiographs following the progression of the periodontaldisease in the propositus (subject IV.5). A. The subject at 10 years ofage with severe periodontal destruction. B. The same individual at age12 and C. at the age of 14, showing severe bone loss, having lostalmost all permanent teeth.
1118_IPC_AAP_553092 3/1/02 2:22 PM Page 309
A Novel Mutation of the Cathepsin C Gene in Papillon-Lefèvre Syndrome Volume 73 • Number 3
ing to a standard protocol. After this step,each PCR product was sequenced in a geneticanalyzer.�
RESULTSEight of 11 members of the fourth genera-tion of this kindred were clinically examinedand 3 (IV.5, IV.8, and IV.9) were diagnosedwith PLS. IV.8 and IV.9 were totally edentu-lous while IV.5 presented only the teeth 1, 16,17, and 32 at age 15 years old when firstexamined by one of the authors. All 3 exhib-ited palmoplantar hyperkeratosis. Anotherfamily member (IV.6) had only plantar hyper-keratosis. No other family members hadaggressive periodontitis or a history of pal-moplantar hyperkeratosis.
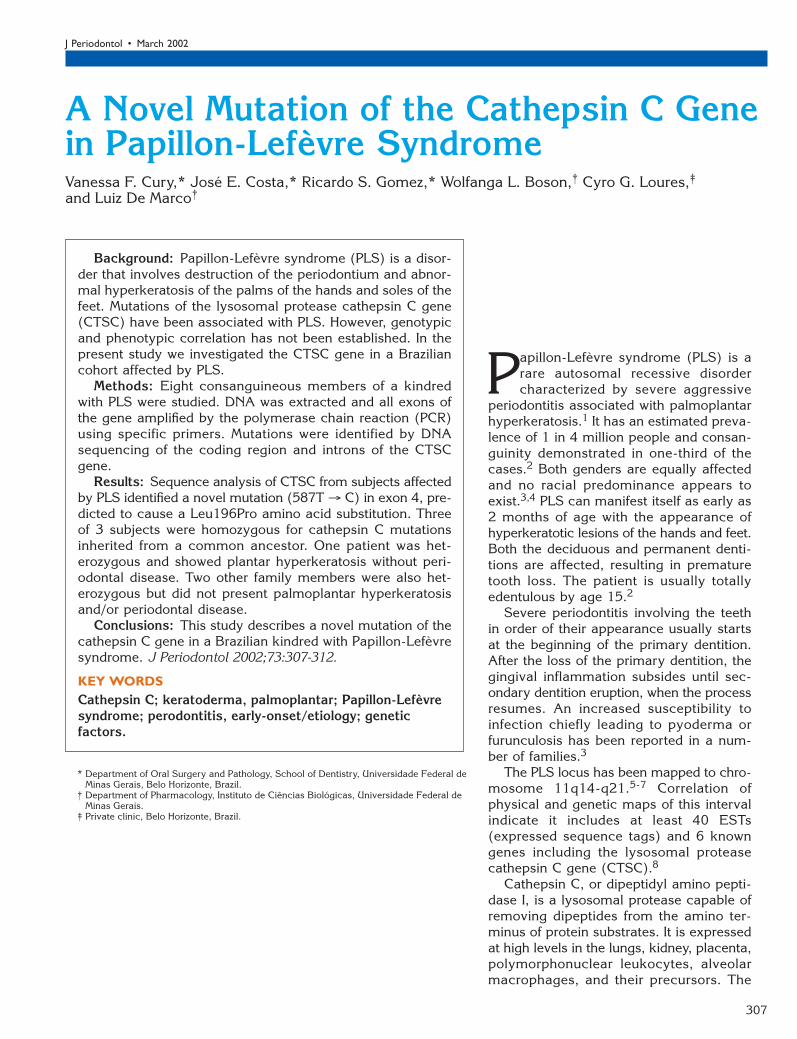
Sequencing AnalysisSequence analysis of exonic, intronic, andthe 5� regulatory regions of the cathepsin Cgene showed that PLS affected subjects werehomozygous for a mutation in codon 196 ofexon 4 (587 T → C), that altered the origi-nal CTT codon to a CCT codon (Fig. 7). Thismutation results in substitution of a con-served leucine residue at position 196 by aproline (Leu196Pro). The mother of theaffected subjects (III.2) was a heterozygouscarrier of the Leu196Pro mutant. The sisterwho presented only with palmoplantar hyper-keratosis (IV-6) was also a heterozygous car-rier. No other family members who were het-erozygous (IV.2 and IV.10) manifestedclinically identifiable characteristics of pal-moplantar hyperkeratosis nor had a historyof severe, early onset periodontitis. Onemember (IV.3) was homozygous for the nor-mal CTSC gene and did not show periodon-tal or dermatological abnormality. Analyses of theCTSC coding region was also performed in DNAsextracted from 20 normal volunteers and thesequences obtained were not different from publishedwild type.9
DISCUSSIONPLS is an autosomal recessive disorder characterizedby palmoplantar hyperkeratosis and severe aggressiveperiodontitis. Several case reports in the literatureshowed phenotypic variations among patients affectedby this syndrome. In some patients, primary teeth werenot affected either by periodontitis or by prematureloss.16,17,20,21 The nature of the periodontal diseaseaffecting the permanent teeth can vary from an acutefulminating type infection on their eruption, resultingin their early loss in spite of treatment22,23 to a disease
310
Figure 7.Sequence analysis of exon 4 of the CTSC gene. A. Wild type sequence, B. DNAsequence from patient IV.5; arrow indicates a T → C (Leu196Pro) mutation.C. DNA sequence from subject IV.6; arrow indicates a heterozygous sequence atnucleotide 587. D. DNA sequence from patient III.2 (mother); arrow indicates aheterozygous sequence.
� ABI Prism 310, Applied Biosystems, Foster City, CA.
recognized only later in life (third decade) that has amore subdued clinical presentation.20,21
The finding that distinguishes PLS from other pal-moplantar keratoderma is severe periodontal destruc-tion. In the classical report, the periodontal diseasecomponent of the syndrome affects the deciduous den-tition causing destruction of the periodontium and earlytooth loss followed by a rapid destruction of the sup-port of the permanent dentition and edentulism by age15. Destruction of the alveolar bone is usually severe,complicating dental therapy. Of the 3 affected patientsin this report, 2 were totally edentulous while the thirdaffected patient presented with only teeth 1, 16, 17,and 32.
It has been suggested that the susceptibility to peri-
1118_IPC_AAP_553092 3/1/02 2:22 PM Page 310

J Periodontol • March 2002 Cury, Costa, Gomez, Boson, Loures, DeMarco
311
odontal disease results from interactions of geneticalterations and polymorphisms with numerous envi-ronmental agents.24 Several diseases are associatedwith aggressive periodontitis, including Papillon-Lefèvresyndrome, Down syndrome, leukocyte adhesion defi-ciency, and others.24 In contrast to adult forms of peri-odontitis, there is evidence that genetic factors areimportant in aggressive periodontitis. It has been sug-gested that juvenile periodontitis is genetically het-erogeneous and, although the gene(s) responsible havenot been identified, a major gene for a localized formwas mapped to chromosome 4q12-21.25,26
In the present study we demonstrated a novel muta-tion of the CTSC gene responsible for Papillon-Lefèvresyndrome in a consanguineous kindred. The 3 patientswith PLS were homozygous for the mutated allele. Thesubstitution of leucine to proline, both neutral andhydrophobic amino acids, may cause a conformationalalteration, as a proline residue can disrupt the usualorganization of the backbone of the polypeptide27 andmay decrease or cease activity. The patients’ mother(III.2) is a heterozygous carrier of one mutated allele.Although edentulous, she did not present with palmo-plantar hyperkeratosis at the time of examination,therefore, it is somewhat difficult to conclude whethertooth loss has any relationship with genetic findings.One patient (IV.6) who showed only plantar hyper-keratosis also was heterozygous for the CTSC genealteration. However, other heterozygous individuals hadneither periodontal nor skin alterations. Therefore, theimpact of the mutated plus wild type allele on peri-odontal or dermatological picture remains to be estab-lished.
The association between CTSC gene alterations andPLS patients’ susceptibility to periodontal disease couldbe explained by two mechanisms. First, CTSC proteinis implicated in the activation of proteases related tophagocytosis, antigen presentation, local activation,and deactivation of cytokines and other inflammatorymediators.8 Therefore, CTSC is involved in a wide vari-ety of immune and inflammatory responses thatinclude the activation of phagocytic cells and T-lym-phocytes, leading to the final elimination of thepathogen. Second, CTSC might influence periodontaldisease progression through its role in epithelial dif-ferentiation or desquamation. As the sulcular and junc-tional epithelium represent the first line of defense,their aberrant differentiation may alter the mechani-cal barrier to periodontal pathogens.8
It has been suggested that genetic factors affectinflammatory periodontal disease progression. This isdemonstrated by the strong familial aggregation seenin aggressive periodontitis.26 However, efforts to dis-sect the specific genetic factors involved in the chronicinflammatory periodontal disease pathogenesis havenot succeeded. The complex interactions between the
environmental and host factors may result in differentclinical forms of the disease. It is difficult to ascertainthe specific role of CTSC on aggressive periodontitis.A recent report demonstrated molecular alterations onthis gene on prepubertal periodontitis.15 The possibil-ity of polymorphism, heterozygosity of the CTSC geneleading to partial activity needs to be established. Inconclusion, we here describe a novel mutation respon-sible for Papillon-Lefèvre syndrome in a Brazilian kin-dred.
ACKNOWLEDGMENTSThe authors are grateful to Dr. Diele C. Barreto forcomments and Ms. Adriana Moreira for technical assis-tance. This study was supported in part by grants fromPRONEX and CNPq (Brasilia, Brazil) and FAPEMIG(Belo Horizonte, Brazil).
REFERENCES1. Papillon MN, Lefèvre B. Two cases of familial symmet-
ric palmo plantar keratosis (Maleda’s disease) in abrother and his sister. Alterations in both cases (inFrench). Bull Soc Francaise Dermatologie Syphiligraphie1924;31:81-84.
2. Gorlin RJ, Sedano H, Anderson VF. The syndrome ofpalmo-plantar hyperkeratosis and premature periodon-tal destruction of the teeth. A clinical and genetic analy-sis of the Papillon-Lefèvre syndrome. J Pediatr 1964;65:895-908.
3. Haneke E. The Papillon-Lefèvre syndrome: keratosis pal-moplantaris with periodontopathy: Report of a case andreview of the cases in the literature. Hum Genet 1979;51:1-35.
4. Hattab FN, Rawashdeh MA, Yassin OM, al-Momani AS,al-Ubosi MM. Papillon-Lefevre syndrome: A review ofthe literature and report of 4 cases. J Periodontol1995;66: 413-420.
5. Fischer J, Blanchet-Bardon C, Prud’homme JF, et al.Mapping of Papillon-Lefèvre syndrome to the chromo-some 11q14 region. Eur J Hum Genet 1997;5:156-160.
6. Laass MW, Hennies HC, Preis S, et al. Localization of agene for Papillon-Lefèvre syndrome to chromosome11q14-q21 by homozigosity mapping. Hum Genet 1997;101:376-382.
7. Hart TC, Bowden DW, Ghaffar KA, et al. Sublocaliza-tion of the Papillon-Lefèvre syndrome locus on 11q14-q21. Am J Med Genet 1998;79:134-139.
8. Toomes C, James J, Wood AJ, et al. Loss-of-functionmutations in the cathepsin C gene result in periodontaldisease and palmoplantar keratosis. Nat Genet 1999;23:421-424.
9. Rao NV, Rao GV, Hoidal JR. Human dipeptidyl-pepti-dase I. Gene characterization, localization, and expres-sion. J Biol Chem 1997;272:10260-10265.
10. Hart TC, Hart PS, Bowden DW, et al. Mutations of thecathepsin C gene are responsible for Papillon-Lefèvresyndrome. J Med Genet 1999;36:881-887.
11. Allende LM, García-Pérez MA, Moreno A, et al. Cathep-sin C gene: first compound heterozygous patient withPapillon-Lefèvre syndrome and a novel symptomlessmutation. Hum Mutat 2001;17:152-153.
12. Nakano A, Nomura K, Nakano H, et al. Papillon-Lefèvresyndrome: Mutations and polymorphisms in the cathep-sin C gene. J Invest Dermatol 2001;116:339-343.
1118_IPC_AAP_553092 3/1/02 2:22 PM Page 311

A Novel Mutation of the Cathepsin C Gene in Papillon-Lefèvre Syndrome Volume 73 • Number 3
312
13. Zhang Y, Lundgren T, Renvert S, et al. Evidence of afounder effect for four cathepsin C gene mutations inPapillon-Lefevre syndrome patients. J Med Genet 2001;38:96-101.
14. Hart TC, Hart PS, Michalec MD, et al. Haim-Munk syn-drome and Papillon-Lefèvre syndrome are allelic muta-tions in cathepsin C. J Med Genet 2000;37:88-94.
15. Hart TC, Hart PS, Michalec MD, et al. Localisation of agene for prepubertal periodontitis to chromosome 11q14and identification of a cathepsin C gene mutation. J MedGenet 2000;37:95-101.
16. Bullon P, Pascual A, Fernandez-Novoa MC, Borobio MV,Muniain MA, Camacho F. Late onset Papillon-Lefèvresyndrome? A chromosomic, neutrophil function andmicrobiological study. J Clin Periodontol 1993;20:662-667.
17. Soskolne WA, Stabholz A, Van Dyke TE, Hart TC, MeyleJ. Partial expression of the Papillon-Lefèvre syndromein 2 unrelated families. J Clin Periodontol 1996;23:764-769.
18. Fardal O, Drangsholt E, Olsen I. Palmar plantar ker-atosis and unusual periodontal findings. Observationsfrom a family of 4 members. J Clin Periodontol 1998;25:181-184.
19. Boom R, Sol CJ, Salimans MM, Jansen CL, Wertheim-van Dillen PM, van der Noordaa J. Rapid and simplemethod for purification of nucleic acids. J Clin Micro-biol 1990;28:495-503.
20. Willett LM, Gabriel SA, Kozma C, Bottomley WK. Papil-lon-Lefèvre syndrome: Report of a case. J Oral Med1985;40:43-45.
21. Brown RS, Hays GL, Flaitz CM, O’Neill PA, AbramovichK, White RR. A possible late onset variation of Papillon-Lefèvre syndrome: Report of 3 cases. J Periodontol 1993;64:379-386.
22. Shams El Din A, Benton FR, Bottomley WK, et al. Hyper-keratosis, periodontosis, and chronic pyogenic infec-tions in a 15-year-old boy. Part One. Ann Allergy 1984;53:11-14.
23. Haneke E, Hornstein OP, Lex C. Increased susceptibil-ity to infections in the Papillon-Lefèvre syndrome. Der-matologica 1975;150:283-286.
24. Nuckolls GH, Slavkin HC. Paths of glorious proteases.Nature Genet 1999;23:378-380.
25. Hart TC, Marazita ML, McCanna KM, Schenkein HA,Diehl SR. Reevaluation of the chromosome 4q candi-date region for early onset periodontitis. Hum Genet1993;91:416-422.
26. Hart TC, Kornman KS. Genetic factors in the patho-genesis of periodontitis. Periodontol 2000 1997;14:202-215.
27. Lewin B. Genes VI. Oxford: Oxford University Press;1997:3-25.
Send reprint requests to: Dr. Luiz De Marco, Department ofPharmacology, Instituto de Ciências Biológicas, UniversidadeFederal de Minas Gerais, Av. Antonio Carlos 6627, Belo Hor-izonte 31270-901, Brazil. Fax: 55 31 3499-2695; e-mail:[email protected].
Accepted for publication October 1, 2001.
1118_IPC_AAP_553092 3/1/02 2:22 PM Page 312