a new treatment method to retract anterior
DESCRIPTION
klTRANSCRIPT

7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 1/19
A New Treatment Method to Retract AnteriorTeeth with the Double J Retractor System inClass III Malocclusions
Bo-Hoon Joo
The double J retractor (DJR) is a novel method to close extraction space
with the aid of mini-implants. DJR is placed lingually on the incisors and hasa lower profile compared with the conventional lingual bracket appliance. Itconsists of a newly designed lingual level arm retractor connected to thelingual of the 6 splinted anterior teeth. The anterior segment is retractedwith a mini-anchor-screw as a temporary skeletal anchorage device withoutbrackets and wires on the posterior teeth. Compared with conventionalorthodontic procedures, such as leveling, space closure, and finishing, theprocedures used with DJR are reduced to 2 steps: space closure and align-ment/finishing. With DJR, the anterior teeth are retraced first without the
leveling stages, and then the leveling and finishing procedures are per-formed together for individual tooth alignment and detailing with conven-tional fixed appliances or invisible clear thermoplastic appliances, such asInvisalign (STAR28 Dental Group, Invisalign Center, Seoul, Korea). With newand simple appliances, the anterior teeth can be retracted with propertorque control and shorten the treatment period. Patient satisfaction couldbe maximized by prompt anterior teeth and lip retraction at the beginning oftreatment. In this article, the biomechanics in the use of DJR are discussedtogether with the application for treatment of Class III malocclusions. (Se-
min Orthod 2011;17:149-167.) © 2011 Elsevier Inc. All rights reserved.
P atients with skeletal Class III malocclusionscan be treated by orthognathic surgery or
camouflaged by orthodontic tooth movement de-pending on the severity of the malocclusion. Anedge-to-edge or anterior cross-bite can be cor-rected by en-masse retraction of the lower arch orextraction of the mandibular premolars. For pa-tients who require surgery to improve the skeletalproblem, extraction of the maxillary first premo-lars and retraction of the maxillary incisors areusually required to decompensate the dentition
before orthognathic surgery. Retraction of either
the maxillary or mandibular 6 anterior teeth re-quires considerable anchorage from the posteriormolars. With the advent of implant anchorage, themanagement of molar anchorage in extractioncases becomes less difficult and complex.1-11 Themini-implant provides temporary but powerful re-inforcement of orthodontic anchorage as well assimplicity and effectiveness of orthodontic appli-ances in treatment. The present article introducesa new method to retract the anterior teeth with acombination of a level arm and 2 bilateral mini-
implants called the Double J Retractor (DJR) sys-tem.
Components of the DJR System
The DJR is a new type of orthodontic appliance toretract incisors without conventional brackets. TheDJR is placed lingually on the anterior teeth withlow profile lingual brackets. To activate the ante-
STAR28 Dental Group, Invisalign Center, Seoul, Korea.Address correspondence to Bo-Hoon Joo, DMD, MS, MSD, PhD,
STAR28 Dental Group, Gangnam Main Center, 9th Floor, Hanil Building, Yeoksam-dong, Gangnam-Gu, Seoul, Korea. E-mail: [email protected]
© 2011 Elsevier Inc. All rights reserved.1073-8746/11/1702-0$30.00/0 doi:10.1053/j.sodo.2011.01.002
149Seminars in Orthodontics, Vol 17, No 2 (June), 2011: pp 149-167
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 2/19
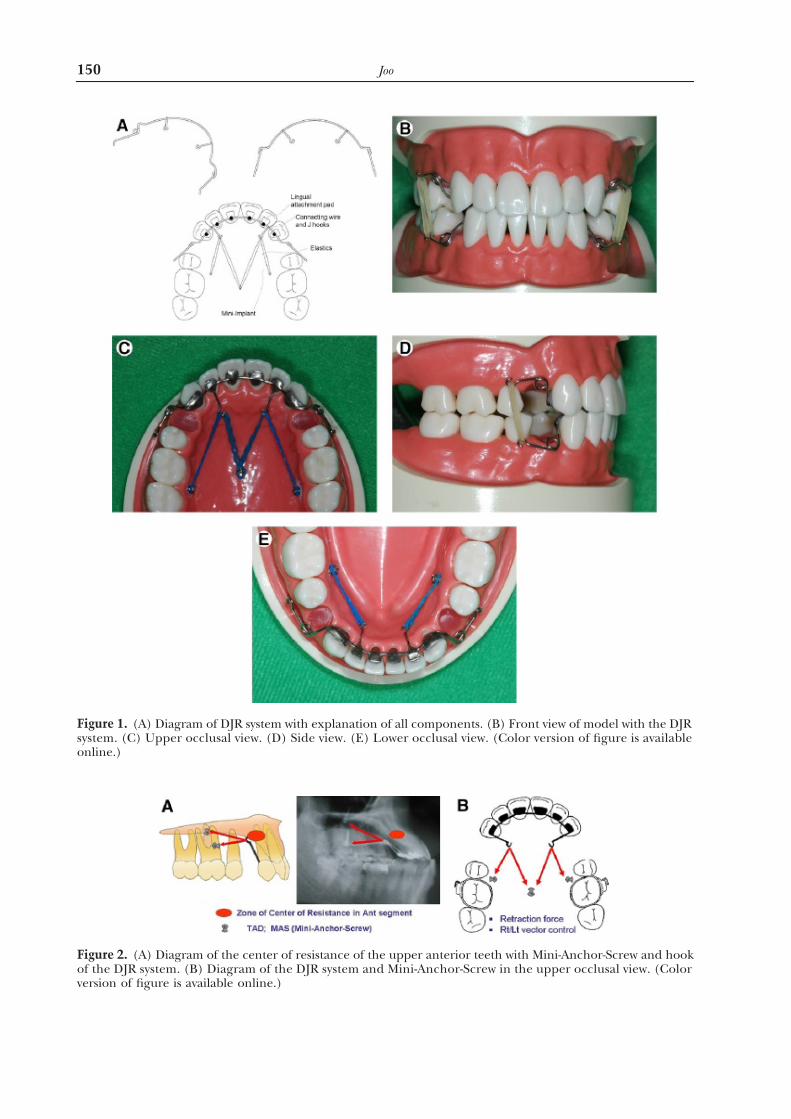
Figure 1. (A) Diagram of DJR system with explanation of all components. (B) Front view of model with the DJR system. (C) Upper occlusal view. (D) Side view. (E) Lower occlusal view. (Color version of figure is availableonline.)
Figure 2. (A) Diagram of the center of resistance of the upper anterior teeth with Mini-Anchor-Screw and hookof the DJR system. (B) Diagram of the DJR system and Mini-Anchor-Screw in the upper occlusal view. (Color
version of figure is available online.)
150 Joo

7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 3/19
rior retraction, the DJR is activated with elasto-meric power-chains or springs with orthodontic
mini-implants that act as the resistance component of the retracting force. The mini-implants for theDJR system are placed on the lingual side of alve-olar bone. The DJR system provides an invisible,comfortable orthodontic appliance with abso-lute anchorage in the retraction of anteriorteeth (Fig 1).
The DJR is consists of 3 major components: (1)the attachment part, (2) the mini-implant part,
and (3) the force-generating part. The attachment part is a combination of bonding pads, a connect-ing wire, a level arm extension wire, and an anti-tipping spring (Fig 1). The attachment pads arebracket pads that are bonded onto the lingualsurfaces of the teeth. They are connected to allanterior teeth with a connecting lingual wire. Lin-
Figure 3. Thediagram of effect (blue arrow in the onlineversion)of theantitipping cantileverspring of the DJR to reduceand control the lingual tipping tendency (red arrow in the online version) from the force of anterior retraction. (Color
version of figure is available online.)
Figure 4. Facial photographs of 16-year-old girl who had a concave profile, and lip incompetence, and upperand lower lip protrusion. (Color version of figure is available online.)
151 Double J Retractor System in Class III Malocclusions

7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 4/19
gual J-shaped hooks are soldered to the pads of themaxillary lateral incisors as level arm extension wires to form hooks for the orthodontic elastics
attaching from these hooks to the mini-implant.Both ends of the lingual connecting wire can beextended to the buccal sides to make antitipping
springs to provide the countermoment of the an-terior teeth against the lingual tipping tendency by the retracting force. The orthodontic mini-im-
plants are placed on the lingual side of alveolarbone and connected with the elastic chains to the J hooks.
Figure 5. The intraoral photographs illustrate an anterior cross-bite and spacing in the lower arch. (Color version of figure is available online.)
Figure 6. The initial cephalometric and panoramic radiographs and measurements. The patient had a skeletalClass III malocclusion with proclined upper and lower anterior teeth. (Color version of figure is availableonline.)
152 Joo
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 5/19
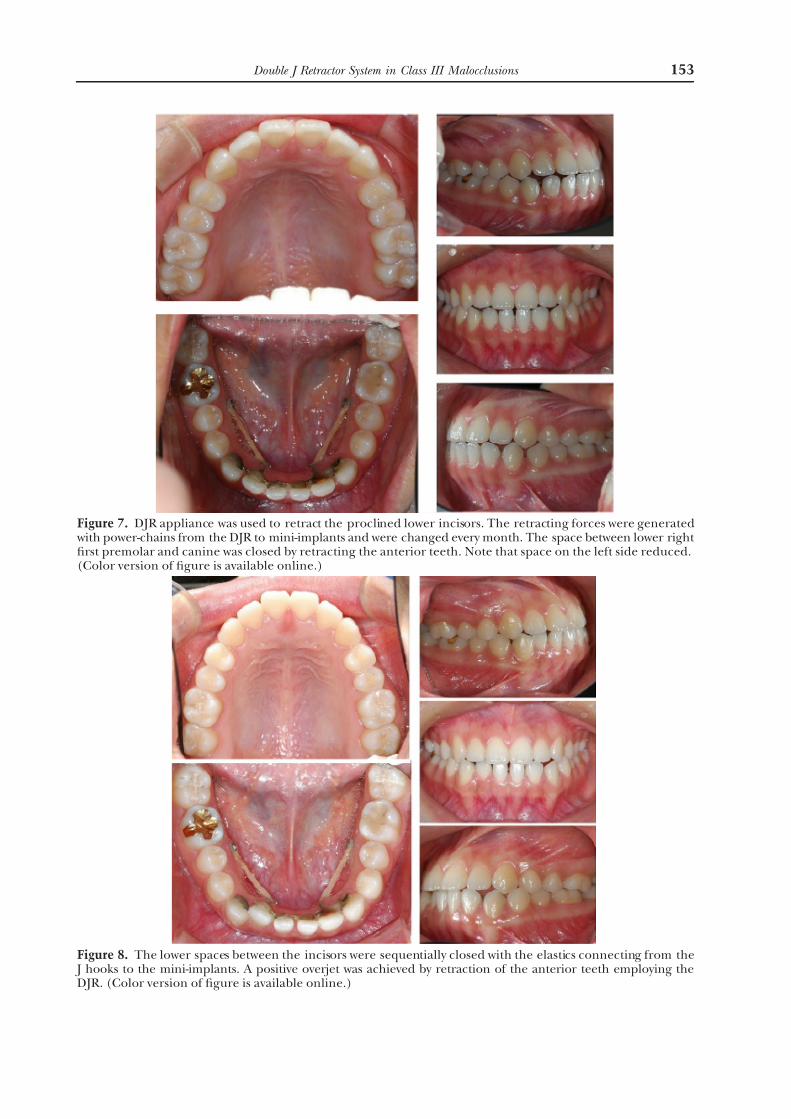
Figure 7. DJR appliance was used to retract the proclined lower incisors. The retracting forces were generated with power-chains from the DJR to mini-implants and were changed every month. The space between lower right first premolar and canine was closed by retracting the anterior teeth. Note that space on the left side reduced.(Color version of figure is available online.)
Figure 8. The lower spaces between the incisors were sequentially closed with the elastics connecting from the J hooks to the mini-implants. A positive overjet was achieved by retraction of the anterior teeth employing theDJR. (Color version of figure is available online.)
153 Double J Retractor System in Class III Malocclusions
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 6/19
Biomechanical Considerations of DJRSystemIn extraction treatment, the mode of anterior re-traction is an important consideration. The main-
tenance and control of incisal torque is one of thedifficult aspects in incisor retraction following ex-tractions. Many studies have been published toinvestigate the center of resistance of the anterior
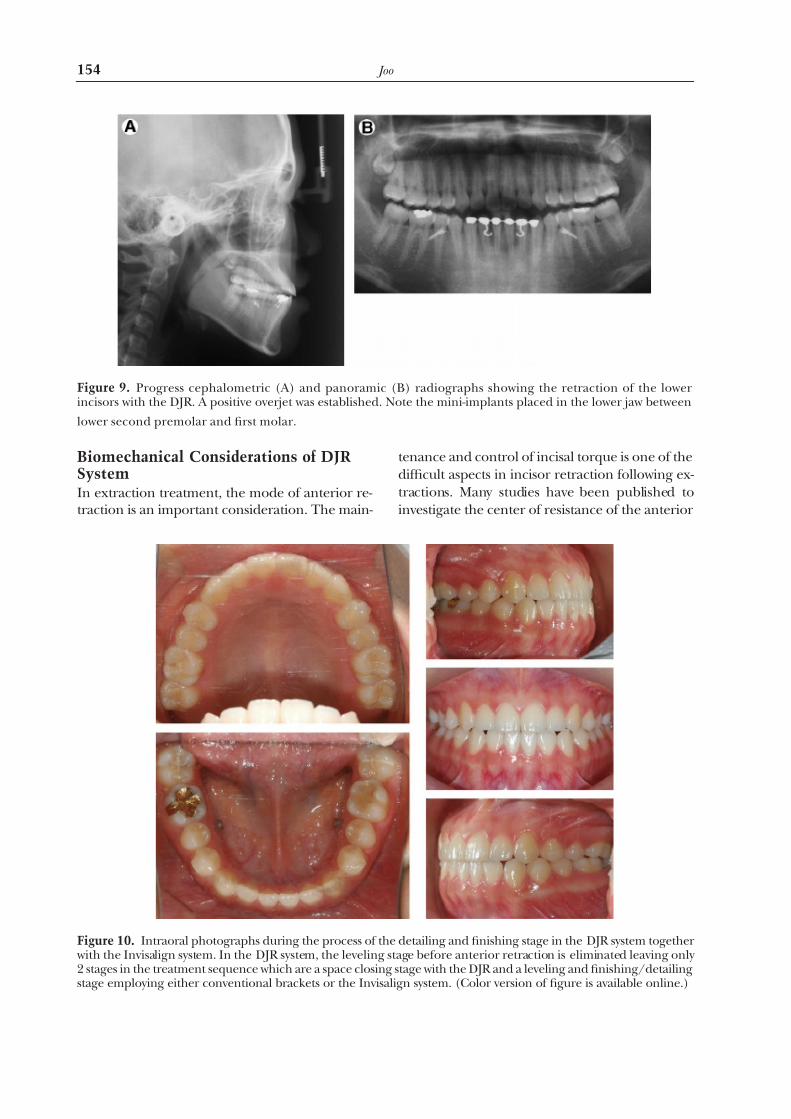
Figure 9. Progress cephalometric (A) and panoramic (B) radiographs showing the retraction of the lowerincisors with the DJR. A positive overjet was established. Note the mini-implants placed in the lower jaw between
lower second premolar and first molar.
Figure 10. Intraoral photographs during the process of the detailing and finishing stage in the DJR system together with the Invisalign system. In the DJR system, the leveling stage before anterior retraction is eliminated leaving only 2 stages in the treatment sequence which are a space closing stage with the DJR and a leveling and finishing/detailingstage employing either conventional brackets or the Invisalign system. (Color version of figure is available online.)
154 Joo
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 7/19
teeth for the orthodontic mechano-therapy withextraction therapy.12-17 An understanding of theissue of the center of resistance for anterior teethretraction is essential to control the tooth move-ment. Most biomechanical studies have indicatedthat the location of the center of resistance of theanterior segment in anterior retraction is approx-imately two-thirds of the root length from the gin-gival margin in the vertical dimension and distal tothe lateral incisor in the anteroposterior dimen-sion (Fig 2).
However, the center of resistance in the ante-rior segment is affected by root length, alveolarbone height, bone density, and applied retractingforces, among other factors.12-17 In clinical treat-ment, the theoretic consideration of the orthodon-
tic biomechanics does not follow exactly as de-signed or intended because the center of resistance of the anterior segment continuously changes as treatment and tooth movement pro-gresses. Therefore, the adjustable component of the appliance is very useful to allow clinicians tomonitor and correct for undesirable side effects.The DJR has an adjustable component to reduceor control the lingual tipping tendency of theanterior segment when the orthodontic forces areapplied to retract the anterior teeth, with the ad- justable component being the antitipping cantile- ver spring of the DJR (Fig 3).
When the incisors are retracted into the extrac-tion space, the DJR also provides control betweenthe right and left sides attributable to the differ-
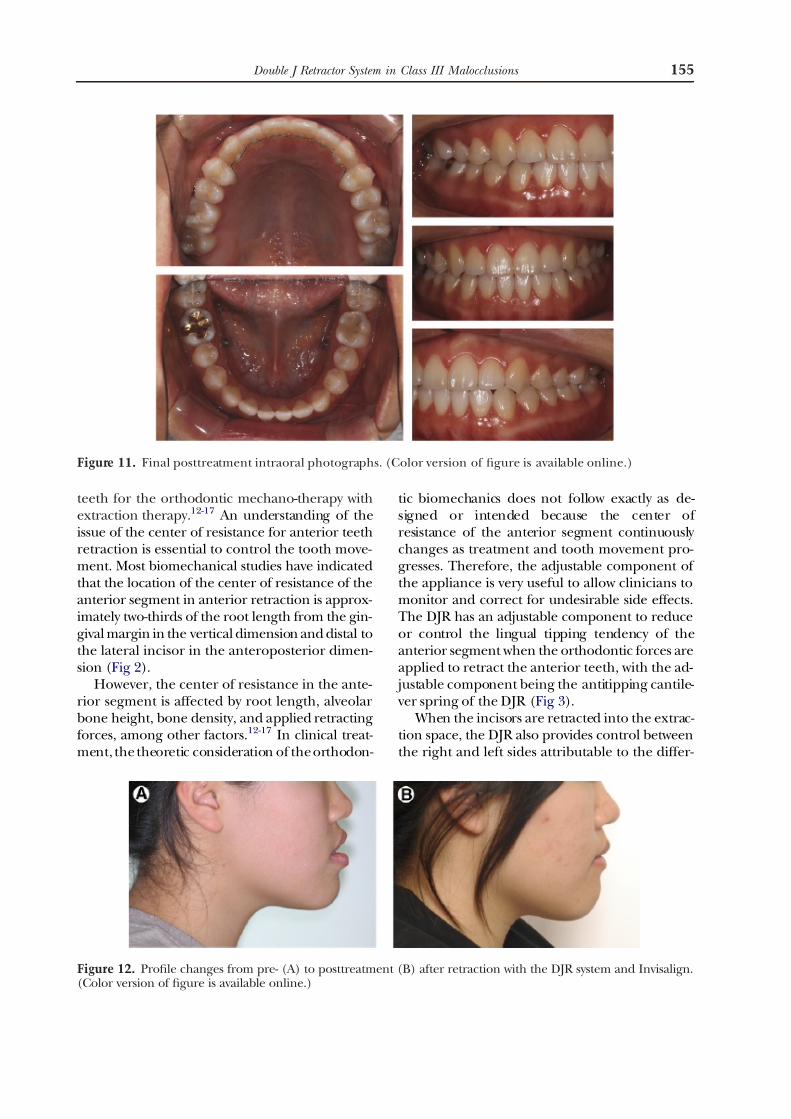
Figure 11. Final posttreatment intraoral photographs. (Color version of figure is available online.)
Figure 12. Profile changes from pre- (A) to posttreatment (B) after retraction with the DJR system and Invisalign.(Color version of figure is available online.)
155 Double J Retractor System in Class III Malocclusions
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 8/19
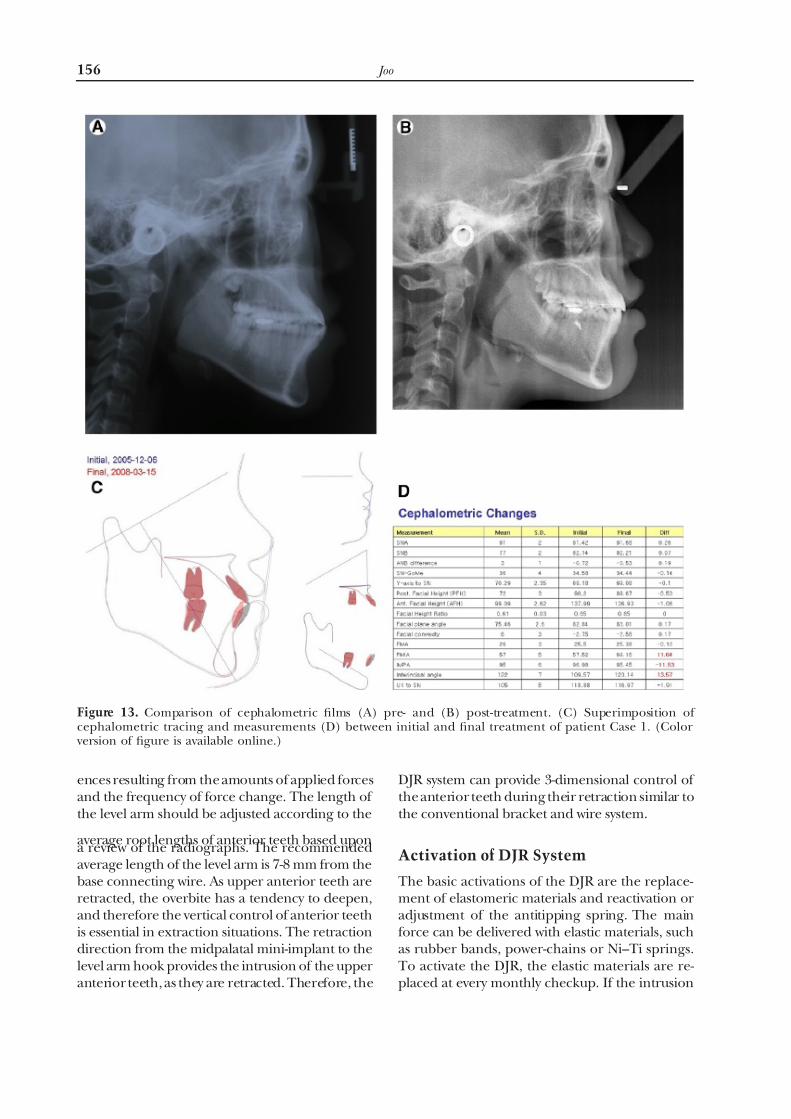
ences resulting from the amounts of applied forcesand the frequency of force change. The length of the level arm should be adjusted according to the
average root lengths of anterior teeth based upona review of the radiographs. The recommendedaverage length of the level arm is 7-8 mm from thebase connecting wire. As upper anterior teeth areretracted, the overbite has a tendency to deepen,and therefore the vertical control of anterior teethis essential in extraction situations. The retractiondirection from the midpalatal mini-implant to thelevel arm hook provides the intrusion of the upperanterior teeth, as they are retracted. Therefore, the
DJR system can provide 3-dimensional control of the anterior teeth during their retraction similar tothe conventional bracket and wire system.
Activation of DJR System
The basic activations of the DJR are the replace-ment of elastomeric materials and reactivation oradjustment of the antitipping spring. The mainforce can be delivered with elastic materials, suchas rubber bands, power-chains or Ni–Ti springs.To activate the DJR, the elastic materials are re-placed at every monthly checkup. If the intrusion
Figure 13. Comparison of cephalometric films (A) pre- and (B) post-treatment. (C) Superimposition of cephalometric tracing and measurements (D) between initial and final treatment of patient Case 1. (Color
version of figure is available online.)
156 Joo
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 9/19
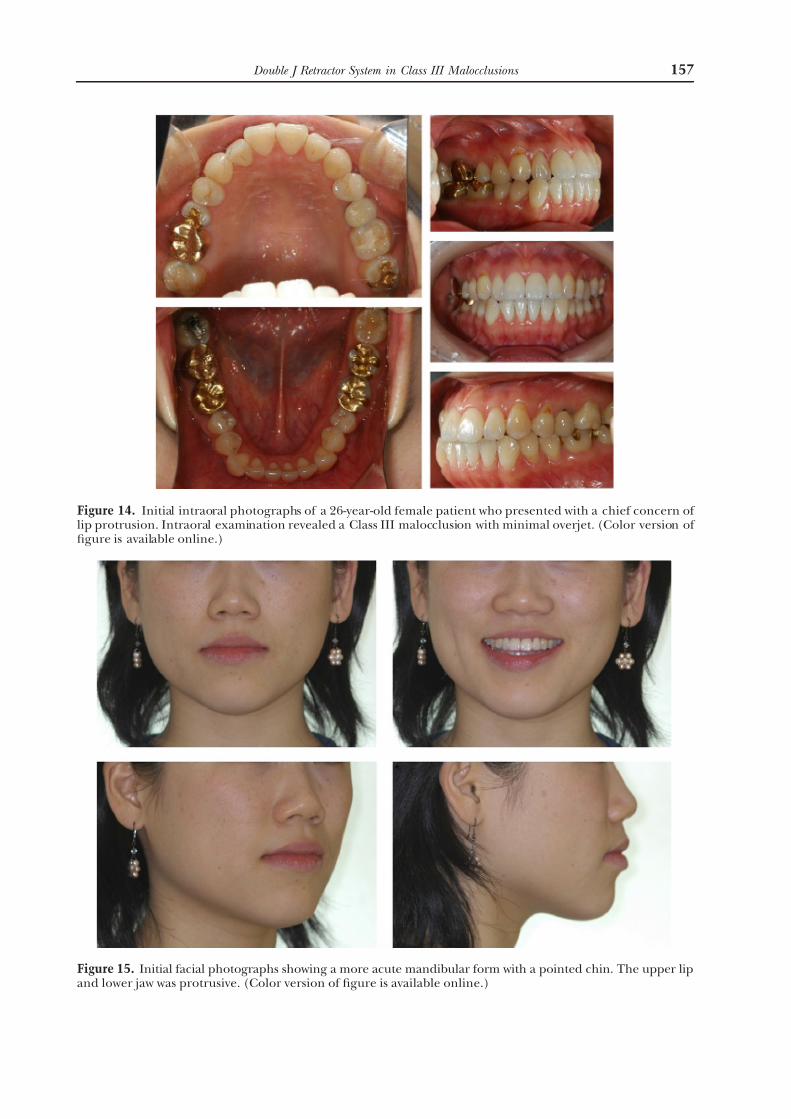
Figure 14. Initial intraoral photographs of a 26-year-old female patient who presented with a chief concern of lip protrusion. Intraoral examination revealed a Class III malocclusion with minimal overjet. (Color version of figure is available online.)
Figure 15. Initial facial photographs showing a more acute mandibular form with a pointed chin. The upper lipand lower jaw was protrusive. (Color version of figure is available online.)
157 Double J Retractor System in Class III Malocclusions
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 10/19
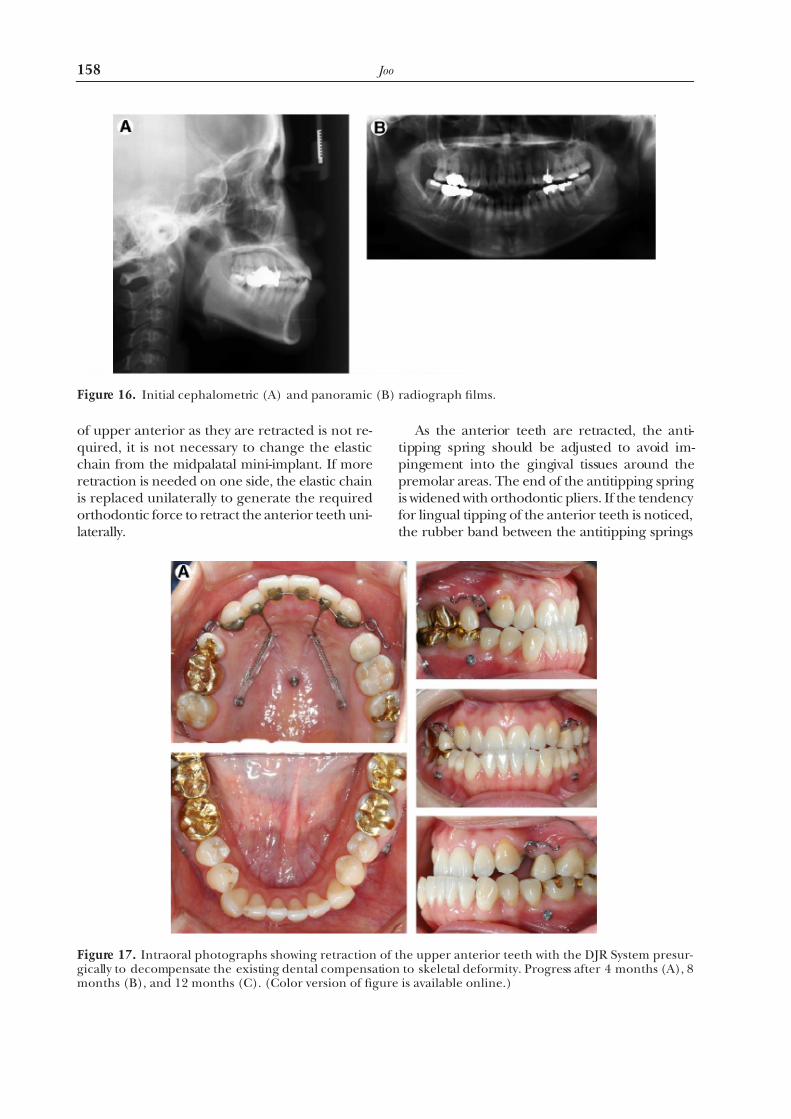
of upper anterior as they are retracted is not re-quired, it is not necessary to change the elasticchain from the midpalatal mini-implant. If moreretraction is needed on one side, the elastic chainis replaced unilaterally to generate the requiredorthodontic force to retract the anterior teeth uni-laterally.
As the anterior teeth are retracted, the anti-tipping spring should be adjusted to avoid im-pingement into the gingival tissues around thepremolar areas. The end of the antitipping springis widened with orthodontic pliers. If the tendency for lingual tipping of the anterior teeth is noticed,the rubber band between the antitipping springs
Figure 16. Initial cephalometric (A) and panoramic (B) radiograph films.
Figure 17. Intraoral photographs showing retraction of the upper anterior teeth with the DJR System presur-gically to decompensate the existing dental compensation to skeletal deformity. Progress after 4 months (A), 8months (B), and 12 months (C). (Color version of figure is available online.)
158 Joo
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 11/19
should be changed to a larger diameter to increasethe force. If the DJR is only applied on the onearch, the activation of antitipping spring can bedone with placement of an additional mini-im-plant in the opposite arch for connection of the
elastics.
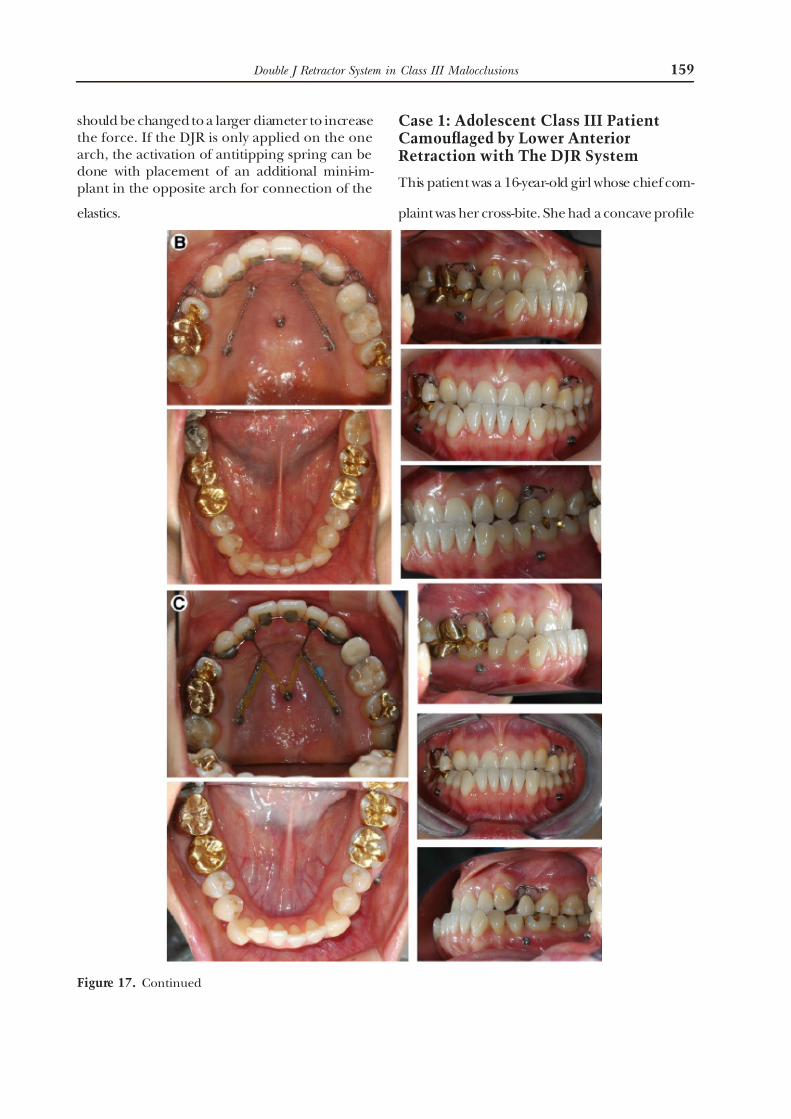
Case 1: Adolescent Class III PatientCamouflaged by Lower AnteriorRetraction with The DJR System
This patient was a 16-year-old girl whose chief com-
plaint was her cross-bite. She had a concave profile
Figure 17. Continued
159 Double J Retractor System in Class III Malocclusions

7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 12/19
with protrusion of both her upper and lower lips. At rest position, her lips were incompetent andmore than half of her upper front teeth wereshowing (Fig 4).
She had a negative 3.0-mm overjet with spac-
ing in her lower dentition. There was minorcrowding in the upper arch, which was wide.The canine and molar relationships were Class I with a good posterior occlusion (Fig 5).
The cephalometric analysis showed a skeletalClass III malocclusion with 0.72° of ANB and2.75° of facial convexity angle caused by aprognathic mandible. The lower two-thirds of her facial height were increased and both upperand lower incisors were proclined (Fig 6).
A DJR was placed on the lingual surface of her lower front teeth to retract them closing her
existing spaces. A power-chain was connectedfrom the DJR to mini-implants between lowersecond premolar and first molar (Fig 7).
When the lower right canine was moved backand contacted the first premolar, the connecting wire of DJR was cut off distal to the lateral incisors.Sequentially, the spaces between the incisors wereclosed with the elastics connecting from the Jhooks to the mini-implants (Fig 8).
By retraction of the lower incisors, the ante-rior cross-bite was improved and eventually apositive overjet was achieved. The progress ceph-alometric radiograph shows the retracted and
uprighted lower incisors and the DJR and mini-implant (Fig 9).
The anterior retraction was completed and theDJR was removed. To continue and complete thetreatment in this patient a thermoplastic appliance(Invisalign; Align Technology, Santa Clara, CA) was designed and used. After anterior retraction,completion of treatment can be accomplished with either a fixed appliance system or the Invis-align system. In the DJR system, the treatment procedures can be reduced to 2 stages, that is,spacing closure and a detailing stage. Some fixed
appliance treatment involves 3 stages of treat-ment, that is, leveling, spacing closure, and fin-ishing and detailing. Photographs of the finish-ing and detailing stages in the DJR System areshown in Figure 10.
For aligning and detailing individual teeth,the Invisalign system was used for this patient. With the clear thermoplastic appliance, the up-per and lower anterior teeth were retractedmore with additional interproximal reduction to
reduce her lip protrusion. The final post treat-ment occlusion is shown on the (Fig 11).
After retraction of the lower and upper inci-sors and alignment of teeth, the lip protrusion was reduced and the facial profile was improved
compared with pretreatment photographs (Fig12). Figure 13 shows the pre- and post treatment lateral cephalograms depicting the amount of incisors retraction using the DJR system.
Case 2: Adult Class III Patient TreatedBy Orthognathic Surgery with UpperAnterior Retraction by DJR System
This patient was a 26-year-old female whose chief complaint was lip protrusion. Intraoral examina-tion revealed a Class III molar and canine relation-
ship with minimal overjet. Both the maxillary andmandibular arch forms were parabolic with mini-mum arch length discrepancy. There was a local-ized cross-bite between the upper lateral incisorand the lower canine on the right side (Fig 14).Her facial examination revealed square frontal view with strongly pointed chin (Fig 15). On the3/4 view and profile, the upper lip protruded, thelower jaw protruded strongly, and the gonial anglearea was more acute and strong.
The cephalometric radiograph indicated astrong mandible and proclined upper and lowerincisors and the panoramic radiograph showed
the third molars (Fig 16). She was diagnosed ashaving a skeletal Class III malocclusion with bimax-illary protrusion. Two treatment plans were gener-ated and offered. The first treatment option wasthe reduction of her anterior protrusion with ex-tractions of all 4 first premolar teeth. With thisoption, the limitation would be that there was noimprovement of her strong lower jaw. The patient wanted to have an extensive and overall improve-ment of her facial appearance. For her facial im-provement, the second treatment option was thecombination of orthognathic surgery and orth-
odontic treatment. The surgical plan was a bilat-eral sagittal split ramus osteotomy mandibular set-back and angle reduction. The presurgicalorthodontic treatment plan included the decom-pensation of the protruded upper incisors withextraction of the upper first premolar teeth toincrease the amount of surgical setback of themandible.
The upper first premolars were removedand the DJR was placed on the lingual side of
160 Joo
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 13/19
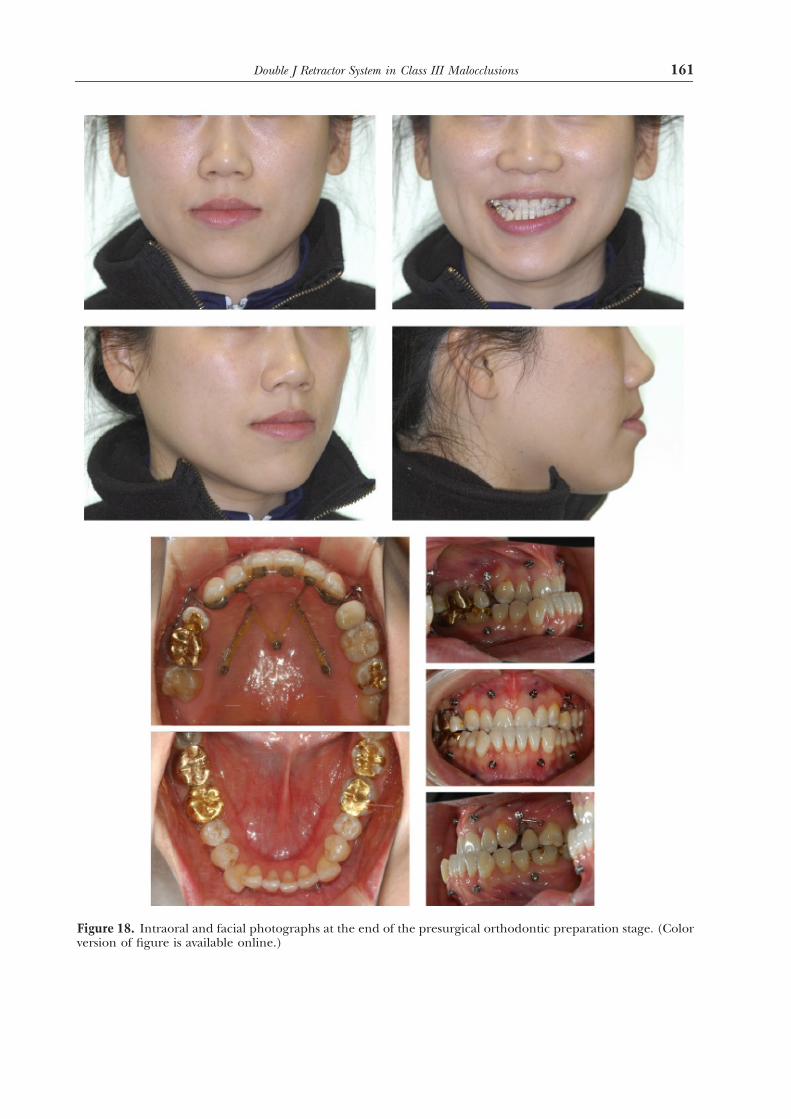
Figure 18. Intraoral and facial photographs at the end of the presurgical orthodontic preparation stage. (Color version of figure is available online.)
161 Double J Retractor System in Class III Malocclusions

7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 14/19
Figure 19. Intraoral and facial photographs after orthognathic surgery. (Color version of figure is availableonline.)
162 Joo
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 15/19
the upper anterior teeth (Fig 17). At eachappointment, the power-chains were changedto generate the retraction force and the ante-
rior relationship was changed into a cross-biteas the upper incisors were progressively re-tracted.
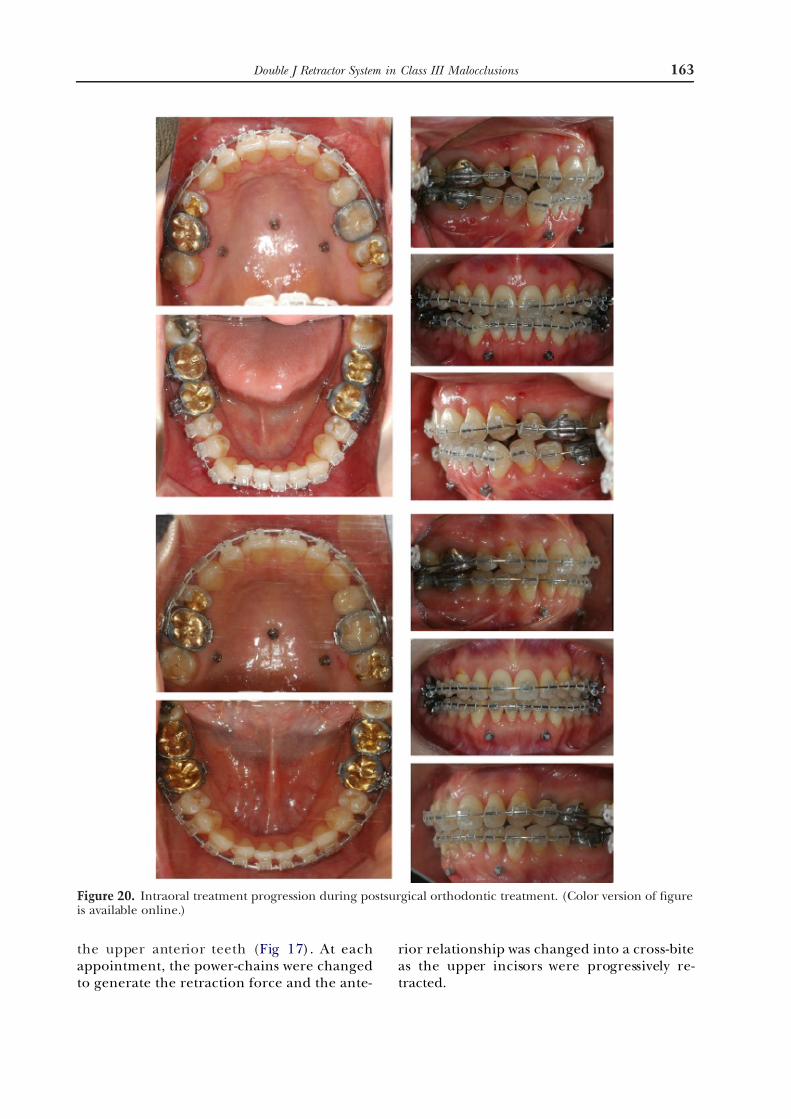
Figure 20. Intraoral treatment progression during postsurgical orthodontic treatment. (Color version of figureis available online.)
163 Double J Retractor System in Class III Malocclusions
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 16/19
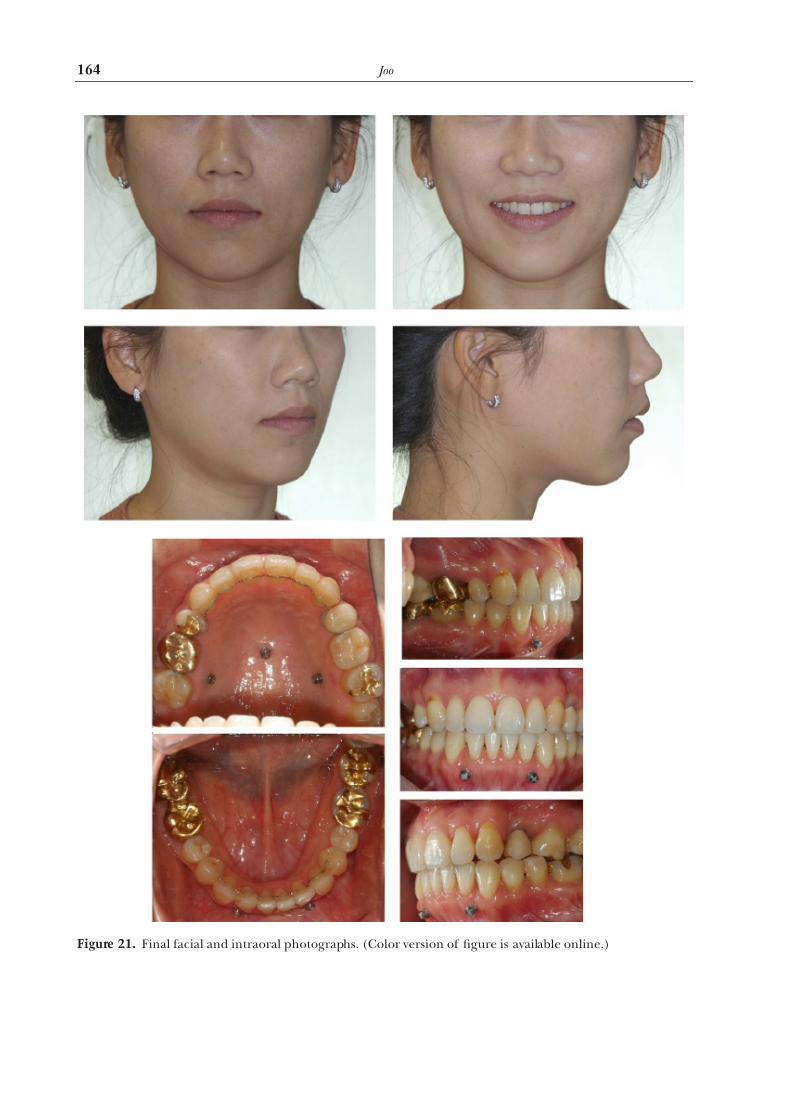
Figure 21. Final facial and intraoral photographs. (Color version of figure is available online.)
164 Joo
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 17/19
The upper incisors were retracted to ensure,
as much as was possible, an appropriate relation-ship of the upper incisor with the craniofacialcomplex. She was ready to have the mandibularsetback orthognathic surgery (Fig 18). The up-
per lip was pleasantly positioned relative to the
nose and other facial structures.The intraoral and facial photographs after the
surgery are shown in Figure 19. The patient had aconvex facial profile and oval frontal facial appear-ance and a positive overjet. There was lack of in-terdigitations in the canine and premolar areasafter the surgery.
To solve the residual problems of tooth align-ment, conventional orthodontic brackets werebonded to all the teeth in both arches (Fig 20).Sequential arch wires were employed to obtain theprogressive improvement of the open bite of the
premolar areas and the individual tooth alignment.The final occlusion and facial changes areshown in Figure 21. Because the patient was study-ing outside of country, her treatment was finished
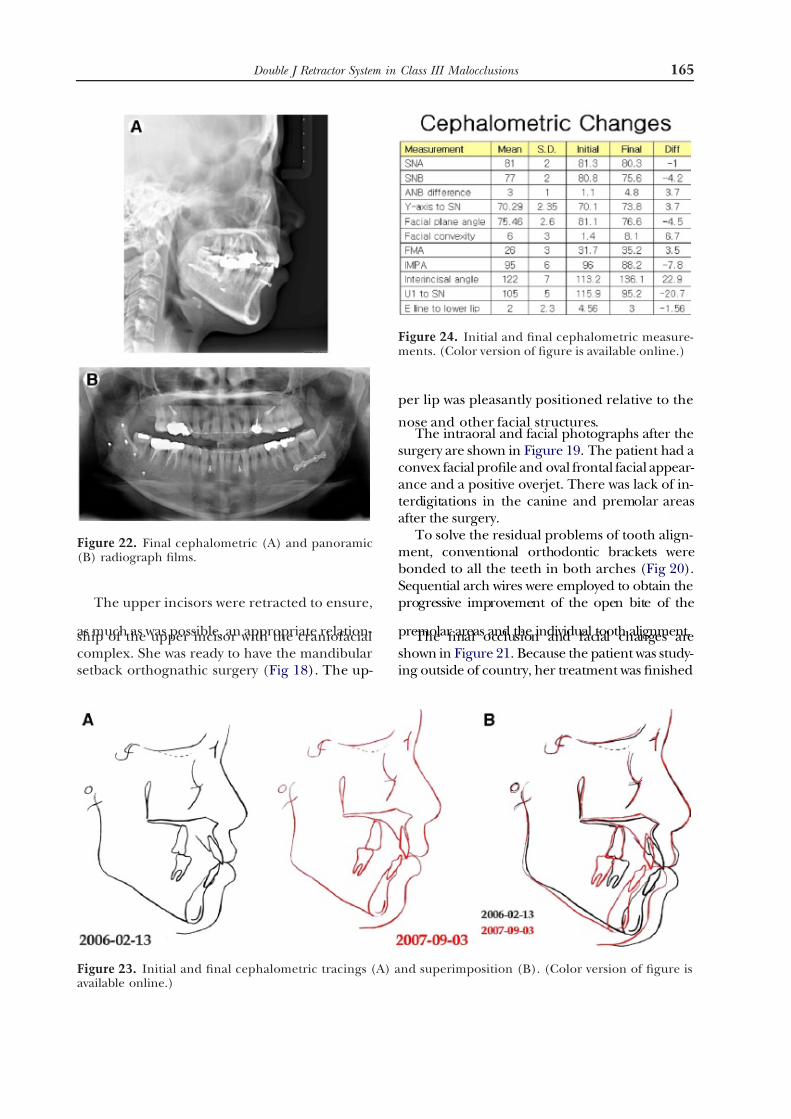
Figure 22. Final cephalometric (A) and panoramic(B) radiograph films.
Figure 23. Initial and final cephalometric tracings (A) and superimposition (B). (Color version of figure isavailable online.)
Figure 24. Initial and final cephalometric measure-ments. (Color version of figure is available online.)
165 Double J Retractor System in Class III Malocclusions
7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 18/19
earlier than planned. Bilateral Class II molar rela-tionships resulted from the extraction of the upperfirst premolars. Cusp and fossa relationships wereobtained with ideal overjet and overbite. However,the dental midline was not completely corrected
because of the tooth size discrepancy and postsur-gical relapse. After consultation, the patient’s ap-pliances were removed because of her going tostudy abroad.
The final cephalometric and panoramic ra-diographs are shown in Figure 22. The initialand final superimposition cephalometric trac-ings illustrate the significant retraction of the
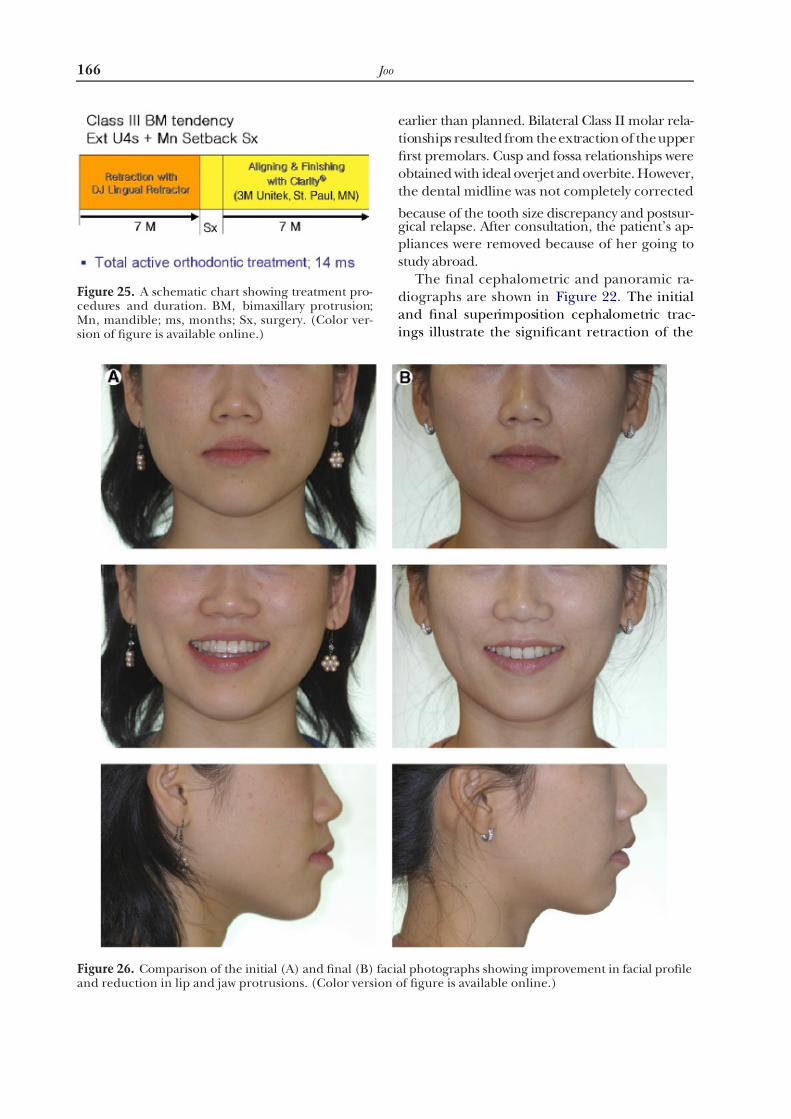
Figure 25. A schematic chart showing treatment pro-cedures and duration. BM, bimaxillary protrusion;Mn, mandible; ms, months; Sx, surgery. (Color ver-sion of figure is available online.)
Figure 26. Comparison of the initial (A) and final (B) facial photographs showing improvement in facial profileand reduction in lip and jaw protrusions. (Color version of figure is available online.)
166 Joo

7/17/2019 A New Treatment Method to Retract Anterior
http://slidepdf.com/reader/full/a-new-treatment-method-to-retract-anterior 19/19
upper anteriors with proper inclination and up-per lip change. The mandible was shortenedand retropositioned by the orthognathic surgery (Fig 23). Figure 24 shows the cephalometricchanges after treatment.
An overall evaluation of her treatment indicatessignificant facial improvement by the upper lipretraction and lower jaw setback through the com-bination of the orthognathic surgery and orth-odontic treatment. By using the DJR, the upperanterior teeth were retracted after 7 months. Aftersurgery, conventional brackets were bonded to im-prove individual tooth position during the align-ment and finishing stages (Fig 25).
Figure 26 shows the comparison between theinitial and final facial photographs. Significant improvement of facial appearance included
changes of front facial type from squarish to oval with more feminine appearance and more pleas-ant smile with a more relaxed lip position. Com-parison of the lateral profile also showed reduc-tion in chin prominence.
Conclusions
The DJR is a new appliance to move the anteriorteeth of the upper and lower arches with mini-implants. The DJR is placed on the lingual surfaceof the front teeth and have a lower profile com-pared with conventional lingual brackets, and
thereby provide easier adaptation by the patient tothe appliance. The most distinguishable advantageof the DJR is the rapid lip and anterior dentalretraction at the beginning of treatment com-pared with conventional orthodontic treatment,the latter which require 6-10 months for teeth tobe aligned during a leveling stage before the ante-rior retraction. The mini-implant together with theDJR enable the clinician to provide better controlof orthodontic anchorage in these circumstances.
The DJR was developed to aid in the correctionof bimaxillary protrusion with four first premolar
extractions and then reduction of the procum-bency by anterior incisor retraction. This tech-nique can also be applied to decompensation by retraction of incisors before mandibular advance-ment procedure for surgical treatment of Class IIpatients with mandibular deficiency.
References
1. Gainsforth BL, Higley LB: A study of orthodontic an-
chorage possibilities in basal bone. Am J Orthod Oral
Surg 31:406-417, 1945
2. Linkow LI: The endosseous blade implant and its use in
orthodontics. Int J Orthod 18:149-154, 19693. Linkow LI: Implanto-orthodontics. J Clin Orthod 4:685-
705, 1970
4. Gray JB, Steen ME, King GJ, et al: Studies on the efficacy
of implants as orthodontic anchorage. Am J Orthod
83:311-317, 1983
5. Sherman AJ: Bone reaction to orthodontic forces on
vitreous carbon dental implants. Am J Orthod 74:79-
87, 1978
6. Smith JR: Bone dynamics associated with the controlled
loading of bioglass-coated aluminum oxide endosteal
implants. Am J Orthod 76:618-636, 1979
7. Robert WE, Nelson CL, Goodacre CJ: Rigid implant
anchorage to close a mandibular first molar extraction
site. J Clin Orthod 28:693-704, 1994
8. Chen J, Chen K, Roberts WE: The effects of orthodonticforces on the stresses in the periodontal ligament of
human mandibular molars. Bioeng Conference ASME
24:269-272, 1993
9. Chen J, Lu X, Paydar N, et al: Mechanical simulation of
the human mandible with and without an endosseous
implant. Med Eng Phys 16:53-61, 1994
10. Chen J, Chen K, Roberts WE: The effects of occlusion
and orthodontic force on the stresses around an endos-
seous implant. Adv J Bioeng 26:431-434, 1993
11. Block MS, Hoffman DR: A new device for absolute an-
chorage for orthodontics. Am J Orthod Dentofac Or-
thop 107:251-258, 1995
12. Melsen B, Fontis C, Burston CJ: Vertical force consider-
ations in differential space closure. J Clin Orthod 24:678-683, 1990
13. Fiorrelli G, Melsen B: Biomechanics in Orthodontics
CD-ROM, version 2.0. Arezzo, Italy, Libra Orthodonzia,
2001
14. Vanden Bulcke MM, Dermaut LR, Sachdeva RCL, et al:
The center of resistance of anterior teeth during intru-
sion using the laser reflection technique and holo-
graphic interferometry. Am J Orthod Dentofac Orthop
90:211-220, 1986
15. Vanden Bulcke MM, Burstone CJ, Dermaut LR, et al:
Location of centers of resistance for anterior teeth dur-
ing retraction. Am J Orthod Dentofac Orthop 91:375-
384, 1987
16. Pedersen, Isidor F, Gjessing P, et al: Location of cen-tres of resistance for maxillary anterior teeth mea-
sured on human autopsy material. Eur J Orthod 13:
452-458, 1991
17. Matsui S, Caputo AA, Chaconas SJ, et al: Center of
resistance of anterior arch segment. Am J Orthod Dento-
fac Orthop 118:171-178, 2000
167 Double J Retractor System in Class III Malocclusions