a neuroanatomical theory on the aetiology of schizophrenia
TRANSCRIPT
Medical Hypotheses 6: 645-658, 1980.
A NEUROANATOMICAL THEORY ON THE AETIOLOGY OF SCHIZOPHRENIA
P.L.Randall. 14 Anglesea Street, South Hobart, Tasmania 7000, Australia.
ABSTRACT
This theory proposes that schizophrenic symptoms are due to the presence of myelinated interhemispheric nerve fibres which link functional areas in the brains of schizophrenics which are not connected in normal subjects. The role these fibres would have in the production of schizophrenic symptoms is examined in the context of recent neuroanatomical and neurophysiological findings in schizophrenics. The functional emergence of these fibres is examined phylogenetically in conjunction with central nervous system myelination. Genetic, biochemical and therapeu- tic implications are considered.
Key Words: Schizophrenia, Corpus Callosum
INTRODUCTION
A search for anatomical differences in the brains of schizo- phrenics has been unrewarding until the findings of Rosenthal and Bigelow (1972). Their study showed that the brains of schizophrenics have a perpendicularly wider corpus callosum than those of a control group (1). Neurophysiological findings include that reviewed by Ingvar (1976) in which chronic schizo- phrenics were found to have a relatively low cerebral blood flow in the frontal regions of the dominant hemisphere, but a higher blood flow in the post-central structures which are related to somato-sensation, vision and audition (2). EEG differences have been described and include those found by Scott and Schwartz (1975) who found a decrease in the amount and poor organisation of alpha activity as well as atypical spike and wave activity in subjects diagnosed as schizophrenic (3). A disconnection syndrome on a visual matching task in schizophrenics was demon- strated by Beaumont and Dimond (1973) which was interpreted to indicate that in schizophrenia the two cerebral hemispheres are partially disconnected and that this reflects some change in the efficiency of the corpus callosum (4).
645
HYPOTHESIS
Interhemispheric Integration
The findings of Rosenthal and Bigelow do not appear to have been further investigated or interpreted as a possible aetiological factor underlying schizophrenia. Their finding of a wider cor- pus callosum in coronal cross-section could be interpreted to imply:
(a> a greater number of interhemispheric fibres in schizophrenics as compared to normals,
(b) a similar number of fibres to normals but a greater degree of myelination,
Cc> both a greater number of fibres and more myelination,
Cd) no increase in either the number of fibres or in myelinatioqbut a greater amount of connective tissue in the corpus callosum.
In the absence of histological examination of the corpus callosum in chronic schizophrenics the nature of this observa- tion remains unclear. However on neuroanatomical grounds it seems that the first three possibilities are more likely than the fourth,and it is on the basis of the interpretation that there is an increased number of interhemispheric fibres in chronic schizophrenics taken in conjunction with the nature and time course of their myelination, that this theory has been developed.
If there is indeed an increased number of myelinated interhemi- spheric fibres in the corpus callosum of schizophrenics,then it is necessary to examine the function they may serve in the cen- tral nervous system. It is postulated that they would provide extra interhemispheric connection which would functionally link andntegrate areas in each hemisphere which would be concerned with higher brain function.
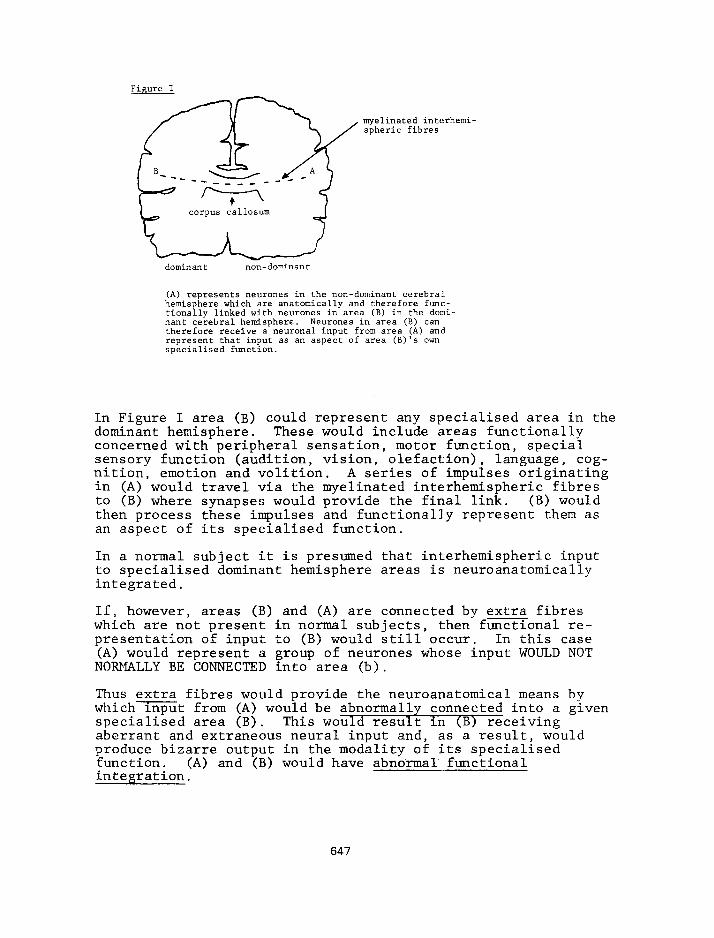
It is possible that such extra fibres would connect functional areas in the brains of schizophrenics that would not be ana- tomically connected in normal subjects. This is illustrated in Figure I.
646
myelinated interhemi- spheric fibres
dominant non-dominant
(A) represents neumnes in the non-dominant cerebral hemisphere which are anatomically and therefore func- tionally linked with neumnes in area (B) in the domi- nant cerebral hemisphere. Neurones in area (B) can therefore receive a neuronal input from area (A) and represent that input as an aspect of area (B)'s own specialised function.
In Figure I area (B) could represent any specialised area in the dominant hemisphere. These would include areas functionally concerned with peripheral sensation, motor function, special sensory function (audition, vision, olefaction), language, cog- nition, emotion and volition. A series of impulses originating in (A) would travel via the myelinated interhemispheric fibres to (B) where synapses would provide the final link. (B) would then process these impulses and functionally represent them as an aspect of its specialised function.
In a normal subject it is presumed that interhemispheric input to specialised dominant hemisphere areas is neuroanatomically integrated.
If, however, areas (B) and (A) are connected by extra fibres which are not present in normal subjects, then functional re- presentation of input to (B) would still occur. In this case (A) would represent a group of neurones whose input WOULD NOT NORMALLY BE CONNECTED into area (b).
Thus extra fibres would provide the neuroanatomical means by whichinput from (A) would be abnormally connected into a given specialised area (B). This would result in (B) receiving aberrant and extraneous neural input and, as a result would produce bizarre output in the modality of its specialised function. (A) and (B) would have abnormal functional inteeration.
647
Although the Rosenthal and Bigelow study has been interpreted here to imply that chronic schizophrenics have additional in- terhemispheric fibres, the central concept of this theory is that of abnormal functional integration between the cerebral hemispheres,and that the postulated extra fibres would pro- vide the neuroanatomical connections.
As abnormal connections from the non-dominant hemisphere could link into any specialised dominant hemisphere area, the results would include bizarre motor, sensory, linguistic, cognitive! emotional and volitional disturbances in any degree or combina- tion in a subject possessing them.
It is this mechanism which is proposed as the neuroanatomical basis of schizophrenic symptomatology.
Myelination
Myelination of fibres within the brain is basic to this theory and must now be examined in order to extend it. Myelination in the central nervous system begins in the fourth intra-uterine month and continues to maturity (5). Paralleling the increase in white matter is an increasing range and complexity of higher brain function which involves both cerebral hemispheres.
In a study of hemispheric function in split-brain subjects, Nebes (1974) described the dominant hemisphere as processing in- put data in a sequential analytic fashion,whereas the non- dominant hemisphere was described as having an ability to organise data in terms of complex wholes and view the total rather than the parts (6). Generally the dominant hemisphere could be described as processing information in a logical, step by step concrete manner compared with the abstract, conceptualiz&g properties of the non-dominant hemisphere which has the ability to produce a gestalt of its input.
These different methods of processing data are similar to the cognitive developmental stages delineated by Piaget who des- cribed the child progressing from concrete operational thought to abstract or prepositional thought between 12-15 years of age. This increase of complexity of information processing within the brain as a whole would reflect a greater degree of inter- hemispheric integration of function due to greater and more efficient interhemispheric transfer as an increasing number of commissural fibres became myelinated.
Phylogenetically, on-going myelination would progressively in- tegrate the disparate functions of the two hemispheres so that information processing, initially largely a reflection of dominant hemisphere function, would gradually become extended and modified by sphere function
increased integration with non-dominant hemi-
648
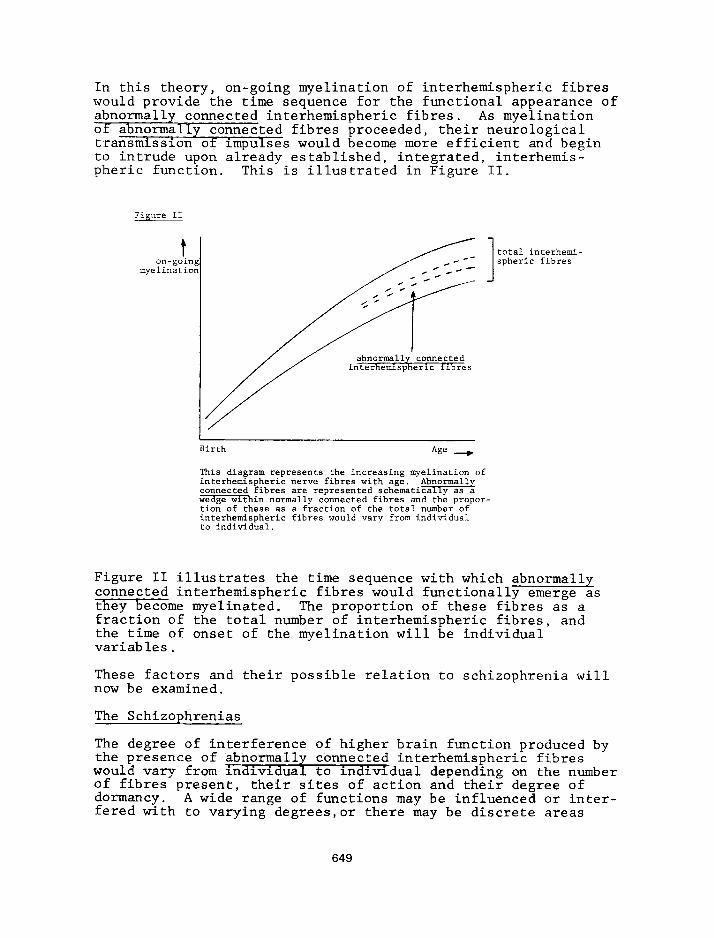
In this theory, on-going myelination of interhemispheric fibres would provide the time sequence for the functional appearance of abnormally connected interhemispheric fibres. As myelination of abnormally connected fibres proceeded, their neurological transmission of impulses would become more efficient and begin to intrude upon already established, integrated, interhemis- pheric function. This is illustrated in Figure II.
Figure II
t on-going
myelination
total interhemi- spheric fibres
I
Birth Age -
This diagram represents the increasing myelination of interhemispheric nerve fibres with age.
.*w connected fibres are represented schematlca y as a wedge within normally connected fibres and the propor- tion of these as a fraction of the total number of interhemispheric fibres would vary from individual to individual.
Figure II illustrates the time sequence with which abnormally connected interhemispheric fibres would functionally emerge as they become myelinated. The proportion of these fibres as a fraction of the total number of interhemispheric fibres, and the time of onset of the myelination will be individual variables.
These factors and their possible relation to schizophrenia will now be examined.
The Schizophrenias
The degree of interference of higher brain function produced by the presence of abnormally connected interhemispheric fibres 1 . . would vary from indrvrdual to individual depending on the number of fibres present, dormancy.
their sites of action and their degree of A wide range of functions may be influenced or inter-
fered with to varying degrees,or there may be discrete areas
649
within otherwise normal overall higher brain function which are clinically affected. Each case of schizophrenia will be unique in itself due to the permutation and combinations of these variables.
The aetiology of schizophrenia will now be described in terms of this theory.
An individual with a large number of abnormally connected inter- hemisnheric fibres mav show abnormalities of function well be- fore 'the appearance of frank schizophrenic symptoms. Before becoming myelinated, abnormally connected fibres will have an effect on higher brain function but this will be masked by phy- logenetically earlier functions to a variable degree. Although these abnormally connected fibres will be less efficient in neural transmission prior to myelination, their effect will be similar though it will not be so marked. The prepsychotic ef- fect on an individual possessing a large number of abnormally connected fibres would be clinically manifested as a schizoid personality or other abnormality of personality,or there may be a number of subtle disturbances in the functions of the specialised areas into which these fibres are connected. As the abnormally connected fibres progressively become myelinated their effects would gradually influence and intrude upon higher functions so that there would be an insidious development of schizophrenic symptoms.
Individuals with a large number of abnormally connected inter- hemispheric fibres would show a greater oremorbid disturbance. have 'an insidious onset of schizophrenicLsymptoms paralleling' on-going myelination,and display a wider range of symptoms. This would apply to the early onset, poor prognosis schizo- phrenics.
Abnormally connected interhemispheric fibres will produce ex- traneous input into the areas into which they are linked,with the production of schizophrenic symptoms.
In the auditoryarea such input would result in auditory hallu- cinations. For example this may be in response to input from a contralateral cognitive area with "thoughts heard aloud" or from an area concerned with memory storage so that verbal memories are actually heard at a conscious level, Any abnormal input producing auditory hallucinations may be experienced so loudly that they seem to be "broadcast".
In the motor area,abnormal input would produce a variety of idio syncratic motor movements. Simple input signals may produce simple and repetitive motor mannerisms. Simultaneous contra- dictory input would produce ambivalence of action and if there were an overwhelming amount of abnormal input, a state of neutrality of action would result, i.e. catatonia.
650
The somatosensory area would respond to abnormal input by cen- trally representing a variety of bizarre sensations localised to the areas receiving the input. An example would be the sen- sation of "electric shocks" in various limbs or other parts of the body.
In areas functionally concerned with cognition, abnormal input may be experienced as withdrawal".
"insertion of thoughts",or "thought "Thought blocking" may occur due to a sudden ab-
normal input which transiently interferes with the line of thought,or it may change the line of thought with "derailment". With a greater and more frequent amount of interference,thought may become totally fragmented. Conceptualisation would become similarly fragmented resulting in disorders of association. There would be a breakdown of integration of the disparate interhemispheric functions in that elements of a concrete or sequential analytic process would be mixed up and out of order in themselves, at the same time being arranged within or super- imposed on a mixture of conceptual frameworks. Linguistic ab- normalities would reflect this internal disorganisation and may be seen at the level of words, with the production of neologisms and word salads,or as sentences with gross syntactical and seman tic disturbances,
Various emotional responses may be evoked by abnormal input. This would result in the experiencing and expressing of emotion which is not normally associated with a given verbalised topic, and which would be observed as incongruity of affect. Two con- tradictory emotions present simultaneously would result in ambivalence of affect,and if a number of emotions were evoked simultaneously, they would become diffused, resulting in a state of emotional neutrality or blunted affect.
In perceptual areas as a whole,a large and overwhelming amount of abnormal input would result in a subject who was experiencing it being unable to attend to any particular stimulus originating either internally or externally. This would produce a gross deficit in selective attention. At its extreme this would re- sult in autistic withdrawal.
In general,a high level of internal interference due to large amounts of abnormal input would result in states of relative neutrality of function. Those mentioned are catatonia, blunting of affect and autistic withdrawal. As a result of these dis- turbances as a whole,volition would become diffused and result in a lack of goal-directed behaviour.
Areas concerned with aspects of personality may be subject to internal interference due to abnormal input,and other aspects of personality will be neglected due to pre-occupation with the internal phenomena produced by abnormal input. The result would be deterioration of personality.
651
The phenomena described would be seen at their extremes in an individual with a large number of abnormally connected inter- hemispheric fibres - that is, the chronic schizophrenic.
An individual may have a few abnormally connected interhemi- pheric fibres which remain dormant until their function is released by other factors. A given specialised area may re- ceive its interhemispheric input via a number of normally con- nected fibres among which there are a few abnormally connected fibres. The input from the abnormally connected fibres would be masked by the input from the others. It however the pro- portion of normal to abnormal input were to decrease due to destruction of normally connected fibres, then the abnormal input would become more influential and become apparent as a disorder of function of that specialised area. Factors which could destroy normally connected fibres include tumours, pene- trating brain injuries, demyelinatingdiseases and Huntington's Chorea - all of which can precipitate schizophrenic symptoms in some individuals.
The late onset schizophrenias would appear by a similar mecha- nism due to release of relatively dormant abnormally connected interhemispheric fibres by neuronal and axonal attrition or fallout,with age. Patients in the older age group often have a hearing defect,and this would increase the likelihood of ab- normal input to the auditory area becoming apparent because loss of normal external auditory input would change the ratio of nor- mal to abnormal auditory input at a central level.
Individuals who develop schizophrenic symptoms in response to stress would also possess abnormally connected interhemispheric fibres. In these individuals such fibres would be few in number and their sites of action would be in dormant or relatively dor- mant areas. Under stress however,these dormant areas mav be called into function. This would-result in abnormally connected fibres becominz influential and their abnormal inout would then result in the gppearance of schizophrenic symptoms. When the stress has passed and the dormancy of these areas is re- established there may be spontaneous remission of schizophrenic symptoms. Dormant but abnormally connected areas may also be- come functionally apparent as an aspect of: higher function due to other means of arousal, for example with stimulant drugs such as amphetamines. In some manic patients also, schizophrenic symptoms may be observed.
Abnormally connected interhemispheric fibres may be few in number, yet if strategically connected into a given specialised area, they may subtly alter the function of that area. In a cognitive area such fibres may produce a subtle yet consistent change in attitude or belief. This may begin as a primary de- lusion which will become elaborated due to alteration in the on-going processing of even normal input to that area via other and normally connected interhemispheric fibres. Thus a
652
slight interference in such a specialised area may, with time, produce an elaborate, complex, delusional system. This may re- main a relatively discrete disturbance of function, or it may be part of a wide spectrum of symptoms.
Because any of these phenomena could occur in a discrete func- tion, or aspect of function, it is possible to have individuals who possess a well-encapsulated abnormality but who otherwise lead relatively normal lives. Their personalities and higher brain function as a whole remain free of internal interference apart from the isolated abnormality produced by a few abnormally connected interhemispheric fibres. -
Neuroanatomical and Neurophysiological Correlates -
The finding of Rosenthal and Bigelow of a perpendicularly wider corpus callosum in schizophrenics has been interpreted here to imply that chronic schizophrenics possess extra interhemispheric fibres. In this theory, where the central concept of the aetiology of schizophrenia has been postulated to be due to abnormally connected interhemispheric fibres, the possibility of there being extra fibres would provide an additional popula- tion of fibres wm could be abnormally connected.
As described abnormally connected interhemispheric fibres would connect into the specialised areas with which they interfere, where their synapses would provide the final link. As with the fibres their site of action is crucial and it is this which is postulated as abnormal. There is no reason to believe that the synapses themselves would be abnormal, but THEIR PRESENCE as the final link in an abnormal connection would be.
The activity produced in the recipient areas of abnormally con- nected fibres would be reflected both in localised cerebral bloodflow and in EEG patterns. auditory area,
Thus an area, for example the may receive a large number of abnormal connec-
t,ions which would remain synaptically active due to the autono- mous neural activity of those fibres. A constant high blood flow would reflect the activity of these fibres in the recipient dominant hemisphere area. This would be consistent with the findings of Ingvar. Similarly EEG readings would reflect such action,and the findings by Scott and Schwartz of poor organi- sation of alpha activity and atypical spike and wave patterns could be expected on these grounds. Increased and autonomous activity of these fibres would also cause an increase in the turnover of the particular neurotransmitter utilised by their synapses in that functional area.
The disconnection syndrome in acute schizophrenics described by Beaumont and Dimond occurred on a visual interhemispheric matching task. In their experiment a decrement in ability to cross-match visual stimuli across the hemispheres was observed. Matching within a hemisphere was normal except for a deficit
653
in matching letters in the left hemisphere (4). In order to match across the hemispheres,an input to one hemisphere would need to be transmitted via the commissures to the contralateral hemispheric area with which it was integrated in the matching task. If the neural substate receiving the visual input were abnormally connected with a contralateral area concerned with a diiierent specialised function, then the resulting output from the recipient area would appear to bear no relation to the original sensory input. Thus abnormal connection of function would appear as apparent disconnection.
A similar mechanism would occur in the phenomenon of reflex hallucinations which is present in some schizophrenics. Here an input to one sensory modality produces an hallucination in another.
The production of a wide range of abnormal specialised function by abnormal input at an internal level is similar to that pro- duced by Penrield (1959) by applying an electrode to areas of the cortex (7). He described the evoking of past experiences, emotions, changes in perception of surroundings and hallucina- tions on electrical stimulation. In schizophrenia the ex- periences are postulated to be due to internal electrical stimulation mediated by abnormally connected interhemispheric fibres.
Genetic Considerations
This theory suggests that the presence of abnormally connected fibres (whether extra or not) would be genetically determined. Genetic factors wx also seem to apply to the number present, their sites of action and their degree of dormancy although these factors may be partially determined by phenotypic factors from the moment of conception onward. For example there may be some randomisation in the crossing of interhemispheric fibres during foetal development. For these reasons identical twins may show less than one hundred per cent concordance for schizo- phrenia.
As mentioned, an individual possessing a small number of abnor- mally connected interhemispheric fibres may never display any evidence of schizophrenic symptoms during a lifetime. Such an individual would never be regarded as schizophrenic, yet presumably he would have the genetic potential to propagate the factor or factors underlying the condition. Allusive thinking as described by McConaghy (1974) in both schizo- phrenics and their families may reflect a subclinical ex- pression of this potential (8). Whether or not schizophrenic symptoms were phenotypically expressed in a given individual with this potential would be a matter of decree of the variables already mentioned or the tors at some point in his lifetime
effects of releasing fac-
654
The interpretation that schizophrenics possess extra inter- hemispheric fibres would not necessarily be biologically dis- advantageous provided they were not abnormally connected. Extra fibres would, if normally connected provide a greater range and complexity of higher brain funciion. Studies of adopted children from schizophrenic mothers (Heston 1966, Karlsson 1970) found that about half of these children either had schizophrenia or abnormal personalities whereas the other half had a greater than expected degree of eminence (9). It is possible that both groups had extra fibres with the dif- ference between them being that thenormal group had a pro- portion of abnormally connected interhemispheric fibres while those who achieved eminence did not.
It is tempting to suggest that schizophrenics are the generally less successful products of central nervous system evolution.
Biochemical Considerations
Although a major focus of research into the biochemistry of schizophrenia has been on the dopamine blocking effect of major tranquilisers, there is a different time course between evidence of dopamine blockade as demonstrated by prolactin re- lease (hours) compared to clinical response of target symptoms (at least two weeks) (Crow 1978) (10).
This theory suggests that the antipsychotic effect of major tranquilisers would be due to an action on the abnormally con- nected fibres themselves,and that this may in turn be a property of nature of the myelination of these fibres. The time course between clinical response of target symptoms and the pre- dictable relapse of symptoms in some schizophrenics some months after the withdrawal of major tranquilisers may reflect the solubility of these drugs in myelin. One of the many properties of chlorpromazine is that it is a potent local anaesthetic (11). It is possible that it has a similar central effect on abnor- mally connected interhemispheric fibres.
As the autonomous and abnormal activity of abnormally connected interhemispheric fibres would be reflected in cerebral blood flow and EEG changes in the area into which they are connected, an increase in turnover of the neurotransmitter utilised by their synapses in that area would be expected. Increased dopamine concentrations were found in the brains of deceased schizophrenics by Crow and by Seeman (12). It is possible that the subjects these investigators examined had a predominance of abnormally connected fibres terminating in areas where synap- tic transmission is predominantly dopaminergic. In other schizophrenics the abnormally connected interhemispheric fibres may terminate predominantly in areas where synaptic transmission involves other neurotransmitter substances or, if a range of areas is involved, a variety of neurotransmitters may have a high turnover as a reflection of abnormal activity.
655
Therapeutic Considerations
Implicit in this theory is that abnormally connected inter- hemispheric fibres interfere with specialised areas of the dominant hemisphere and that suppression of the activity of these fibres would release their underlying normal function.
Evidence for normal associative function underlying the schizo- phrenic abnormalities of association has been provided by O'Brian and Weingartner (1970). They concluded that the idio- syncratic verbal behaviour of chronic schizophrenics occurs despite the fact that they have a capacity for discriminating normal free idiosyncratic responses which parallels that of normals (13).
There is some evidence to suggest that interruption of inter- hemispheric fibres produces relief of symptoms in schizo- phrenics.
In a group of psychiatric patients which included some diagnosed as schizophrenic, Laitinen (1972) produced stereotactic lesions in the genu of the corpus callosum. Some also had lesions to the cingulum but this was omitted in later cases. Laitinen concluded that the immediate results of stereotactic lesions to the genu were definitely better than those previously obtained by section of the rostra1 cingulum. One patient who was repor- ted as having vivid hallucinations became free of them after the procedure (14). Although the target symptoms for surgery were anxiety and tension in a heterogeneous group of patients, the relief of hallucinations (though the sensory modality was unspecified),is an interesting finding.
If intractable symptoms in chronic patients were relieved during the time course of a temporary blockade of callosal fibres, it may be possible then to localise the fibres responsible for in- terference of function. This would provide a rationale for selective stereotactic interruption of those fibres. This in turn may lead to a topographical localisation of abnormally con- nected fibres within the corpus callosum on the basis oi the presence of a given symptom in a given patient. The presence of specific symptoms may then provide a neurological foundation for physical blockade in those patients whose symptoms do not respond to current therapies.
CONCLUSIONS
This theory postulates that the aetiology of schizophrenic symptoms is due to the presence of abnormally connected inter- hemispheric fibres in the brains of schizophrenics, that these fibres produce symptoms as they become myelinated and that their myelination characteristics may differ from those of other in- terhemispheric fibres.
It provides a number of testable hypotheses. A replication of the Rosenthal and Bigelow study with the inclusion of micro- anatomical investigation of the callosal fibres would reveal whether a wider corpus callosum is a consistent feature of chronic schizophrenics,and whether the number of fibres and their myelination differ from normals. Further blood flow and EEG studies as well as positron emission studies of the schizophrenic brain may support or refute the concept of abnormal dominant hemispheric input proposed here. Blockade of the corpus callosum with relief of schizophrenic symptoms which re-appeared on cessation of blockade would tend to sup- port this theory and provide a rationale for selective inter- ruption of the interhemispheric fibres implicated in the pro- duction of symptoms. Investigation of the effect of major tranquilisers on axonal transmission in the central nervous system, as well as their solubility in myelin and whether their concentration in the white matter in the brains of schizophrenics paralleled their antipsychotic effects with time, would support or refute the action proposed for them here.
References
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
Rosenthal Randall and Bigelow Llewellyn B. Quantitative Brain Measurement in Chronic Schizophrenia. British Journal of Psychiatry: 121, 259-264, 1972.
Ingvar David H. Functional Landscapes of the Dominant Hemisphere. Brain Research: 107, 181-197, 1976.
Scott D.F. and Schwartz Martin S. EEG Features of Depressive and Schizophrenic States. British Journal of Psychiatry: 126, 408-413, 1975.
Beaumont J.G. and Dimond S.J. Brain Disconnection and Schizophrenia. 123, 661-662, 1973,
British Journal of Psychiatry:
Ham Arthur W. Histology. p 524. 5th ed. J.B.Lippincott Company, Philadelphia and Montreal.
Nebes Robert D. Hemispheric Specialization in Com- missurotomized Man. Psychological Bulletin: Vol. 81 No. 1, January 1974.
Penfield Wilder. The Interpretive Cortex. Science: 1719-1725, Vol. 129, 26 June 1959.
McConaghy N. Essays on Schizophrenia VI. Clinical Features of Allusive Thinking. Ethnor Pty. Ltd., Sydney, 1974.
Fish's Schizophrenia. 2nd ed. (Max Hamilton, ed) John Wright & Sons Ltd., Bristol, 1976.
(10) Crow T.J. The Biochemistry of Schizophrenia. British Journal of Hospital Medicine, November 1978.
657
(11) The Pharmacological Basis of Therapeutics. p 161. 4th ed. (Louis S. Goodman, Alfred Gilman, eds) The Macmillan Company, 1971.
(12) Iverson Leslie L. The Chemistry of the Brain. Scientific American, September 1979.
(13) O'Brian John P. and Weingartner H. Associative Structure in Chronic Schizophrenics. Archives of General Psychiatry. Vol. 22, February 1970.
(14) Laitinen Lauri V. Stereotactic Lesions in the Knee of the Corpus Callosum in the Treatment of Emotional Disorders. The Lancet: 26 February 1972.
658