a functional testing approach to geriatric rehab
TRANSCRIPT

Your Top Choice in Continuing EducationTM
A Functional Testing Approach to Geriatric RehabDesigning Test-Driven Rehab Programs to Safely Improve
Function and Mobility in Older Adults
Seminar Manual 1852IMPORTANT:Customer Service is available weekdays between 6AM-6PM Central time at 800-433-9570 Option 1. For weekend calls, contact Customer Service on the following Monday.
John B. Perry, PT, CSCS, FAFS, CAFS, 3D MAPS, is an APTA Licensed Physical Therapist with over 20 years of experience in clinical, outpatient, and home settings. The author of ‘Hip To Be Fit’, Mr. Perry has developed and presented programs across the country on lower extremity injuries, propriobility, motor development and Applied Functional Science principals for patients and clients of all types and purposes.

Welcome!Welcome to today’s Summit Professional Education workshop! We are committed to the quality of our instructors, and content they present, and look forward to showing you this commitment today. Additionally, our Customer Service team is only a phone call or email away and wants to work hard to provide you with the highest level of service available.
At the end of the day you’ll be asked to complete a program evaluation form. Please be candid as each evaluation is reviewed by our workshop development team. We also appreciate any topic ideas you recommend for future workshops – your suggestions matter!
We thank you for being a customer of Summit Professional Education and hope to see you again soon.
Enjoy the workshop!
-The Summit Team
Phone: (800) 433-9570Fax: (615) 376-8233Email: [email protected]: www.summit-education.com

• Guidelines exist whereby all speakers must disclose any relevant relationships. All relevant relationships are published in the workshop brochure.
• Summit Professional Education does not accept commercial support of any kind.
• Approvals of this activity refer only to continuing education activities and do not imply that there is real or implied endorsement of any product, service, or company referred to in this activity nor of any company subsidizing costs related to the activity.
• You will be notified if a presentation relates to any product used for a purpose other than that for which it was approved by the U.S. Food and Drug Administration.
DISCLOSURES
Summit Professional Education is a national professional development company whose focus is designing and delivering dynamic and relevant educational content to professional audiences. The purpose of this instruction is to help professionals achieve (re certification or obtain continuing education credit for relicensing and to gain the knowledge necessary to compete in and contribute to today’s health care marketplace.
The professional development workshops on orthopedic, therapeutic, pediatric and adolescent, geriatric, behavioral health, and regulatory topics are scheduled in all 50 states and provide continuing competence activities to thousands of participants each year. Known as leaders in their fields of expertise, Summit Professional Education instructors design interactive workshops with evidence-based content that attendees can use immediately with their patients to improve outcomes, performance and results.
About Summit
About Today’s Instructor
Phone: (800) 433-9570Fax: (615) 376-8233Email: [email protected]: www.summit-education.com
John B. Perry, PT, CSCS, FAFS, CAFS, 3D MAPS, is an APTA Licensed Physical Therapist with over 20 years of experience in sports/fitness, out patient, hospital, home and skilled settings. The author of ‘Hip To Be Fit’, Mr. Perry has developed and presented programs nationally and internationally on lower extremity injuries, proprioception, movement awareness and Applied Functional Science principals for patients and clients of all types and purposes. An NSCA Certified Strength and Conditioning Specialist, Fellow of Applied Functional Science and Certified in AFS as well as 3D MAPS functional testing system, Mr. Perry utilizes his background in orthopedic injury rehab, functional lower extremity anatomy, and movement awareness to bring a unique and comprehensive approach to gait analysis.Mr. Perry has worked in many different environments throughout his physical therapy career which gives him insight into gait biomechanics and assessments from a variety of therapeutic settings. Mr. Perry’s well-rounded clinical skills have allowed him to serve a diverse patient population. Co-Owner of Inner Circle Management in Ohio, a faculty member and Director of Live events and Education for the Gray Institute, Mr. Perry received his Bachelors of Science in Physical Therapy from The Ohio State University.

Summit Professional Education works to develop new programs based on your comments and suggestions, making your feedback on the program very important to us. We would appreciate you taking a few moments to evaluate this program.
P r o g r a m E v a l u a t i o n F o r m
May we use your comments and suggestions in upcoming marketing materials?
If you have any general comments on this topic or program please explain. You may use the back of this form to elaborate.
Thank you for participating and taking the time to join us today!(Optional)
Please comment on the instructor’s presentation:
Please tell us what other programs or topics might interest you?
Whatwasthemostbeneficialpartoftheprogram?
Theleastbeneficial?
What would you like to see added to the program?
Please rate the following items on a SCALE of 1 = (poor) to 5 = (excellent).
Please rate the following items on a SCALE of 1 = (poor) to 5 = (excellent).
Please rate the following items on a SCALE of 1 = (poor) to 5 = (excellent).
INSTRUCTOR
CONTENT
OBJECTIVES
____ Teaching ability ____ Organization of material ____ Knowledge base ____ Effectiveness
Yes No
1
2
3After attending the program, how well do you feel you are able to:
(fill in the blank)
(fill in the blank)
(fill in the blank)
(fill in the blank)
Name: Professional Title: Setting/Population:
____ Relevance/value of information for your work____ Content matched the stated objectives____ Completeness of coverage of materials
____ Usefulness of hand-outs/visuals____ Meeting facility & accommodations____ Convenience of meeting facility location
Instructor Name: Cindy Lee, M.S.Ed Location Attended: Date:
__ Identify early warning signs of potential autism spectrum disorders in preschool children.__ Select appropriate treatment approaches for preschool children.__ Identify the difference between atypical and typical developmental patterns.__ Select instructional strategies/interventions that are appropriate for the presenting characteristics
(behavioral, cognitive, social, emotional, sensory).__ Plan for structured and organized facilitation of play and socialization.__ Describe ways to support families through the period of diagnosis and throughout early development.
Preschoolers & AutismKeeping Calm When They’re Carrying On
John B. Perry, PT, CSCS, FAFS, CAFS, 3D MAPS
ѩ Describe the anatomical changes in the aging adult in order to provide an optimum treatment plan with respect to strength, flexibility, and balance.
ѩ Perform patient-appropriate, research-based functional tests.
ѩ Recognize the key assessment tools and treatment concepts involved in fall prevention.
ѩ Incorporate the most appropriate rehab program to improve functional progression.
ѩ Implement evidence-based strategies for post-operative rehab in the geriatric patient.
ѩ Design functional home exercise programs to increase continuous progression in the geriatric patient.
A Functional Testing Approach to Geriatric RehabDesigning Test-Driven Rehab Programs to Safely Improve Function and Mobility in Older Adults


JOHN B. PERRY, PT, CSCS, FAFS,
CAFS,
3D MAPS
• Consultants- ICM, Inc.
• Sports Med, Acute, Swing Bed, Inpatient, SNF, LTC, HH settings
• Author, Speaker, Blogger and Creative Thinker :)
JOHN B PERRY, PT, CSCS,
FAFS, CAFS, 3D MAPS
(FELLOW OF APPLIED
FUNCTIONAL SCIENCE)• Right Brain Thinking
• Einstein’s Theory of Insanity
• Gary Gray(www.grayinstitute.com)
• Wayne Dyer
• Tim Ferriss
7

WHO’S HERE?
• Specialties
• Settings
Same Landscape ...different set of eyes..
OVERVIEW
•T------F-----A-------R
8

COMMON DISORDERS
• http://www.rightdiagnosis.com/symptoms/gait_disorders/causes.htm
• Ms
• Stroke
• Parkinson’s
• Injury
The moment we want to believe
something, we suddenly see all
the arguments for it, and become
blind to the arguments against it.George Bernard Shaw
9

MAIN THEME
• We are using gait to problem solve
• The test is the exercise and the exercise is the test
• We are using movement to find solutions for
assessment and treatment
• We are positioning our clients for success
• It’s all about...
•The ability of the body to move and react
in 3 planes, with and against gravity,
while efficiently and effectively loading
and unloading producing the proper
amount of speed.
Movement Awareness
10
Proprioception
The ability to sense the position and location and orientation and movement of
the body and its parts
The ability to use the nervous system and its proprioceptors correctly. Creating movement awareness within a constant changing environment.
PROPRIOBILITY
11

• 3 planes
• Gravity /ground reaction
• Transformational zone-Load and Unload
• Speed/Reaction
Principles
• Place in transformational zones
• Move body in all 3 planes concurrently
• Train for ideal load to unload
• Speed
STRATEGIES
12

• Proximal and distal attachment
• Uniplaner
• NonWeight Bearing
• Segmental
• Attack what Hurts
• Gravity/Ground
Reaction
• 3 Planes
• Load/Unload
• Attack the Culprit
• Chain Reaction
PST
What We Learned
- Change the Way You Look at Things
- Stride, Arm Swing, Transverse Plane Motion
- What is not smooth or fluid (fluidity)
Gait- Big Picture
13

WHERE TO FOCUS
• Where to put the “X”
• Dancing Monkeys
GAIT: WHAT SHOULD IT LOOK
LIKE?
• Load and Unload in 3 Planes Of Motion
14

NORMAL GAIT
• Calcaneal Eversion
• STJ Pronation
• Ankle Dorsiflexion
• Tibial IR
• Adduction of Knee with IR and Flexion
• Hip Adduction with Flexion and IR
NORMAL GAIT
• Opposite Ankle Dorsiflexion
• Knee Extension with ER and Abduction
• Hip Extension, Abduction and IR
15

NORMAL GAIT
• Lumbar and Thoracic opposite rotation to pelvis
• Opposite arm swing to leg that is forward
• Cervical spine rotation same as pelvis
Constant balance between both sides of body
We are reciprocal beings
Multi-planar
Fluid
16

More focus on Fluidity- Less on Rigidity
Systematic....with Functional Eye
VIDEO ANALYSIS
• Videos
• Lab
17

FUNCTIONAL
ANATOMY
• Muscle Function During Locomotion
• Synergistic Approach
18

MUSCLE FUNCTION
DURING LOCOMOTION
• Muscles are Reactors
• Everyone Is Different
• Muscles control loading then synergistically help
produce unloading utilizing gravity, ground reaction and
momentum (speed)
SYNERGISTIC
APPROACH
• How to Network
• Full Body Approach
• Chain Reaction
19

"Loading" improves " Mostability" or Stability
(Networking)
“Unloading” is more of challenge ( taking friends away)
BIOMECHANICAL
EVALUATION• Mindset
• Subjective/Listen
• Posture
• ROM
• MMT
• Palpation
• Movement Awareness/Balance
20

Hip Flexors Gastroc HIP
Ilio Sol ITB Adductors Rotators
Saggital Plane: ACTIONLE
Persuasion Long Stride x x
Short Stride x
UE Persuasion Arm Swing x x x
Elbows Bent x x
Frontal Plane:LE
Persuasion Wide Gait x x
Narrow Gait x x
UE Persuasion OH Same x opp x opp x opp
OH Opposite x same x same x opp
Transverse Plane
LE Persuasion Toes In x x x x
Toes Out x x
UE Persuasion Arms Same Side x opp x opp x both x same
Arms Opposite x same x same x both x
Verbally
Physically Demonstrate
Hands On
Goal is Subconscious Reaction
Change One Thing At A Time
How Do We “Drive” Our Patients?
21

• Start With Success
• Begin with the End in Mind
• 1-2 Tasks per Visit
• 3 exercises
• 1 gait change
Initiating The Plan
Put Them In The "Garage" and Influence Your "X"
( Muscle or Movement)
This Will Confirm Your "Hunch"
22

FUNCTIONAL
EXERCISES
• Strategies andTechniques based on
our Principles we used with our Gait
and biomechanical eval.
XXX
LXX
RXX
23

3 Plane Pelvic Drives
3 Plane Arm Reaches
24

3 Plane Leg Drivers
Narrow
Wide
Stagger/Narrow
25

Toe In and Out
Squats
26
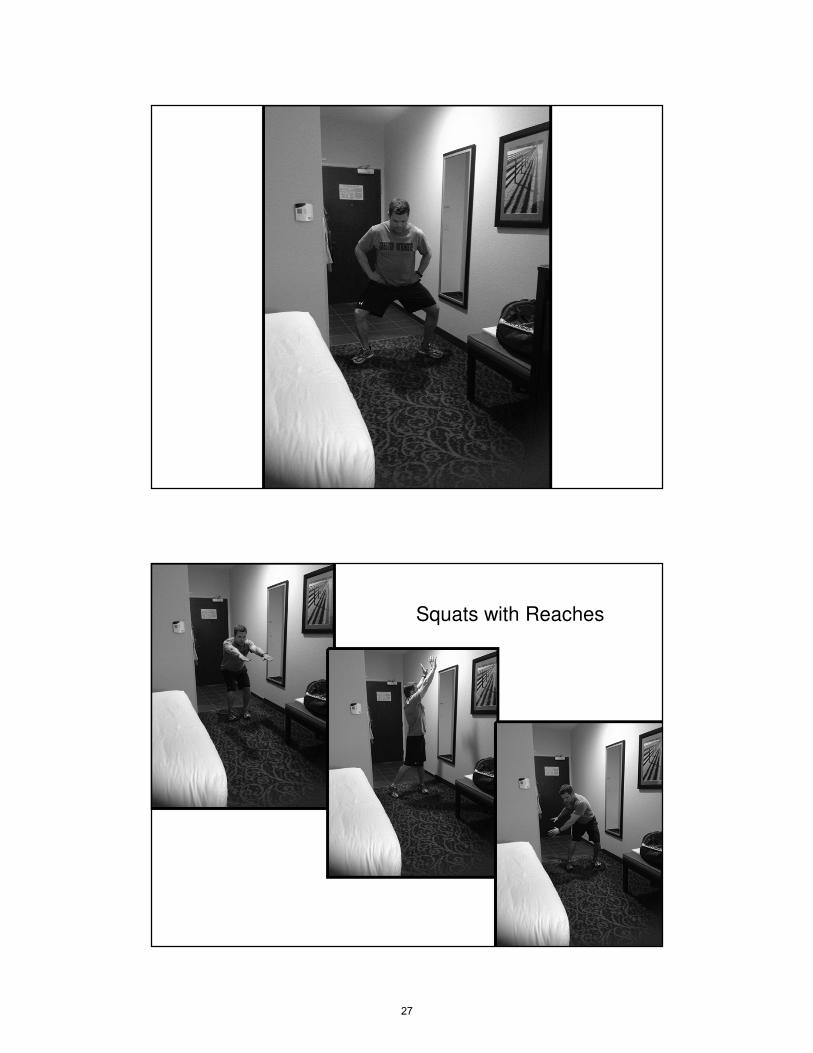
Squats with Reaches
27

Lunge with Reaches
3 D Exercise
28

BUTTERFLY
EFFECT
• In chaos theory, the butterfly effect is the sensitive
dependence on initial conditions, where a small change at
one place in a deterministic nonlinear system can result in
large differences to a later state. The name of the effect, coined by Edward Lorenz, is derived from the theoretical
example of a hurricane's formation being contingent on whether or not a distant butterfly had flapped its wings
several weeks before.
BUTTERFLY
EFFECT• Make One Change... See Chain Reaction
29

Butterfly Effect
3-5 Exercises Day One
30 Seconds ea.
3 Times/Day
Start With Success
PUTTING SYSTEMS
IN PLACE
• Start Globally
• Choose a Direction
• Drive
• Analyze
• Repeat
30

See Systems Sheet, See Pics
PelvisArmsLegs
Movement
Drivers
Lengthen in one plane,
Drive in other two
What Is Our Focus ?
31

RE-EVALUATION
• Your Work is Never Finished
• Marathon not a Sprint
• It’s the Process not the Outcome
Second Visit:
Gait
Review ExercisesModalities
ManualAdd Exercise?
Gait
Notes
*** Did Plan/ Goals Change?***
32
Exercise Progressions
Stance
Squats
Lunges
Step ups
( Reaches with all movements)
Matrices
Documentation
Test Is Exercise And Exercise Is Test (FAFS)
33

PROBLEM SOLVING
• Locate Potential Culprit
• What would not allow the painful or restricted
area to load/unload as it should?
• What is solution for today?
The people who get on in this world
are the people who get up and look
for the circumstances they want and
if they can't find them, make them.
George Bernard Shaw
34

GERIATRIC GAIT
EVALUATION
• Antalgic
• Cautious
• Cerebellar/Ataxia
• Choreic
• Dystonic
• Frontal Gait Disorder (Apraxia)
• Hemiparetic
• Paraparetic
• Parkinsonian
• Psychogenic
• Sensory Ataxia
• Steppage
• Vestibular Ataxia
• Waddling
35

BIG
ROCKS• Story
• What is the list for your setting?
BIG ROCKS
• Posture
• Weakness
• Dormant Butts
• Health related issues
• Environment
• Communication
36

FLUIDITY WITH
PROPRIOBILITY
• Improving propriobility (one’s ability to use proprioceptors to gain functional mobility and fluidity)
• There is no reception without proprioception
TECHNIQUES
• Persuading
• Driving
• Exercise
• Movement Awareness
• Listening
• Communicating
• Learning
• Improving
• Teaching
• Positioning for Success
• Feeling
• Understanding
37

• Use what you have available to work with-
Strengths/Success
• If Based on Applied Functional Science, You
are NOT Wrong...Know your “Why”
• “Influence” the chain reaction and build on
success
• Influencing the body’s proprioceptors-
consciously and subconsciously
THE ART OF PERSUASION
T-F-A-
R• YOU are in Control
• YOU drive the movement based on your
observations.
• BE in the moment
38

• Start With Success
• Begin with the End in Mind
• 1-2 Tasks per Visit
• Don’t overwhelm patient
• Keep it simple
ADJUSTMENTS AND
TIMING
ONGOING ANALYSIS
Gravity
Ground Reaction
3 planes
load/unload
Chain Reaction within the
Transformational Zone
Work with what is available to you
39

HOMEWORK• One task /goal to work on or staff/family to
assist with for that day or week
• To be done when you are not there
• Looking for carryover from work you have
done
40

MUSCLE FUNCTION DURING ADL
• Ideal Gait muscle function
• Visible body APP
• Muscles control loading then synergistically
help produce unloading utilizing gravity,
ground reaction and momentum (speed)
ADL’S AND MUSCLE FUNCTION
• Sit to Stand
• Lat Lunge and Reach
• Pick up slipper
• Reach into Cabinet (high and low)
• Opening a door
41

MOVEMENT AWARENESS LAB
• Crawling
• Kneeling
• getting up from floor
• standing
• Lunges
• walking
MOVEMENT AWARENESS LAB
• Jogging
• Hopping
• Skipping
• Starts and Stops
42

GERIATRIC GAIT
EVALUATION
• Supine
• Sitting
• Standing
• Ambulation
43

GARAGE VS.
TRACK
• Bed mobility level?
• Transfer Level?
• Can they ambulate and at what level?
• Garage= supine, sit or wt. bearing
• Track = actual ambulation
TAKING THE NEXT STEP
• Reassessments performed Daily by all staff
• What needs/issues to be progressed/changed/modified today?
• and Why?
44

FUNCTIONAL
MEASURES• Berg Balance Scale
• 5 Rep STS
• Timed Get Up and Go
• Falls Efficacy Scale
• Four Square Step Test
• Dynamic Gait Index
• 3D MAPS
FUNCTIONAL
MEASURES• Scores from Standardized Testing
should improve based upon our ability to enhance proprioception
• Using Applied Functional Science
• Training Movements not Muscles
45

HH/ASSISTED LIVING
• 84 y/o male, Pneumonia, General Debilitation,
HTN, decreased balance, rollator for
ambulation with Min A-CGA
• Lives at Home with 3 hours passport daily
• 3 stairs enter/exit home for medical appts
• step down into living room
ACUTE/INPATIEN
T• 68 y/o B knee replacement with CHF, DM and
HTN
• Lives with Elderly Husband and Daughter to
assist daily
• Day 1 and 2
46

SNF / ECF / LTC
• 91 year female with senile dementia, depression with
mood disorder, DM, HTN, frequent falls, UTI’s
• Min A with bathing and dressing;Feeds self
• ambulates without device
• 2 falls in last week/Prior PT and OT
OUTPATIENT
CLINIC• 74 y/o female, Frozen R shoulder following fall
resulting in Humerus Fx , Immobilized 8
weeks, may begin gentle ROM, B Knee OA,
fairly good health otherwise
• Son assists during day, Pt alone at night and
that is how she prefers it
• Uses cane and furniture walks,
47
LAB
• Assessment-Garage vs Track or both
• 3 possible exercises~ 1 task for homework (
What would you do currently?)
• Focus on functional muscle function
• What is missing? What is available to work
with?
48

What are Your BIG Rocks?
Know Your “Why”
Teach your “Why”
WHAT DID WE
SEE?
SIMILARITIES?
STRATEGIC ADJUSTMENTS
AND TIMING• Begin where Pt is successful
• Begin with Garage work(Pelvis,UE,LE)
• 3 planes of motion
• Emphasizing Load/Unload with full body
synergistic approach
• Progress to transfers and gait, applying same
principles
49

EXERCISE
PROGRESSIONS• Supine >>Rolling>>Side Lying >> Sitting>>
Dynamic Sitting>> Partial Standing >> Standing>> Stepping >> Squats >> Lunges >> Pivots >> Ambulation >> Stairs >> Stooping >> Dynamic Reaches with Gait
• All focusing on 3 plane proprioceptive driven movements
EXERCISE
PROGRESSIONS• Positioning
• Repetitions
• Duration
• Speed
• Loads
• Feedback, manual or verbal
50

DOCUMENTATION• A Necessary Evil
• Makes us “Skilled”
• Gets us “Paid”
• Enhances communication between disciplines
• Makes us “Authors” within our craft
51

DOCUMENTATION:
SKILLED
• Patient ambulated 100’ with wheeled walker with 6
verbal cues to increase heel strike. Tactile cues given
x’s 2 for safe maneuvering of walker.
• Patient performed upper body dressing with SBA.
Moderate verbal cueing needed for finding shirt front
and modified technique to get T-shirt over head.
• Patient presents to PT after recent hospitalization for CHF. Exacerbation of CHF has caused decreased exercise tolerance due to skeletal muscle maladaptations that have affected the patient’s functional strength. Patient presents with balance deficits, inability to ambulate safely and decreased ability to transfer as evidenced by specialized testing. Patient will benefit from skilled progressive resistive exercises, and mobility and balance retraining to return safely to independent living in home environment.
DOCUMENTATION:
Assessment
52

DOCUMENTATION:
MEDICAL
NECESSITY• Patient will continue to benefit from skilled PT to increase
balance and decrease fall risk as patient completed 4 square step test in 17 seconds indicating they are at high risk for falls. Patient remains at risk for falls and falls with injury due to complicating factor of osteoporosis, but has demonstrated good progress over past week by decreasing 4 square step test by 4 seconds.
DOCUMENTATION: GOALS
• STG x 2 weeks: Patient will achieve 120
degrees of shoulder flexion to reach into upper
cabinets independently at home to allow for
safe food preparation.
• LTG x 4 weeks: Patient will independently
ambulate 1.2 m/sec with walker without loss of
balance on outside surfaces to allow patient to
safely cross the road at home to get mail from
mailbox.
53

DOCUMENTATION:
DISCHARGE
• Patient was seen for 12 visits of PT services. Patient has made excellent progress towards heel strike goal. The patient is now able heel strike 100% of time with no verbal cues compared to needing verbal cues every 10 feet on eval. Patient showed great benefit from estim program combined with PRE for ankle dorsiflexors and neuromuscular reeducation. Patient to return home with no adaptive equipment and no further PT needed. Patient is I in home exercise program to maintain goals and continue at a lower risk for fall.
• Pt amb min A of 1 with gait belt using RW. Trunk flexed
posturing, fwd head, kyphotic posture with flexion of knees
B. Step-to gait with LLE, shuffle step pattern with decreased
stride length. mod VC for proper gait pattern and RW use.
Proprioceptive deficits in LE and trunk musculature
including strength and flexibilty issues are contributing to
above pattern. When combined with bed mobility, sitting
posture and MMT , it is felt pt could benefit from skilled P.T.
consisting of 3 plane pelvic UE and LE driven exercises in
supine, sitting,modified standing and standing. Focus on
Strengthening, flexibility, proprioception, gait, transfers,
safety awareness (etc.)........for improved functional
mobility, transfers, safety, improved functional
independence, return to PLOF and or Decrease BOC on
staff....then will list goals.
Example
54

WORDS TO LIVE BY:
• Proprioceptive enhancement with focus on...
• Loading and unloading of trunk, UE and LE
• Functional mobility
• Safety awareness
• Skilled, PLOF
• 3 planes, driven
• Trunk Disassociation from pelvis
• Step-though pattern
• Heel toe pattern
• Adequate arm swing
• proper posturing
• environment awareness
WORDS TO LIVE BY:
55

FALLS RISK ASSESSMENT
Musculoskeletal disorders
Cervical spondylosis
Gout
Lumbar spinal stenosis
Muscle weakness or atrophy
Osteoarthritis
Osteoporosis
Podiatric conditions
Sensory abnormalities
Hearing impairment
Peripheral neuropathy
Visual impairment
Neurologic disorders
Cerebellar dysfunction or
degeneration
Delirium
Dementia
Multiple sclerosis
Myelopathy
Normal-pressure hydrocephalus
Parkinson disease
Stroke
Vertebrobasilar insufficiency
Vestibular disorders
FALLS
PREVENTION• Screening Protocol
• Communication with Disciplines
• History
• Medication Review
• Physical Exam
• Gait and Balance Performance Testing
• Presence of Environmental Hazards
56

FALLS
PREVENTION
• Enhance Propriobility through the Art of
Persuasion using Applied Functional Science
Principles, Strategies and Techniques.
• Communicate!
• Focus on “homework” tasks
• 3 plane dynamic movements in sitting and
standing
SUMMARY
• What did we learn? BIG ROCKS
57

• Summary
• Questions
• Contact Info
WRAP UP AND
EVALUATIONS
www.youtube.comPropriobility
REFERENCES
• www.grayinstitute.com
• www.imovebetter.com
58

THANKS FOR PLAYING!
59

Gait Biomechanics and Analysis-Article Bibliography
Biomechanical and Neuromuscular Characteristics of Male Athletes: Implications for the Development of
Anterior Cruciate Ligament Injury Prevention Programs. Sugimoto D, Alentorn-Geli E, Mendiguchía J,
Samuelsson K, Karlsson J, Myer GD. Sports Med. 2015 Feb 7.
Pivoting neuromuscular control and proprioception in females and males. Lee SJ, Ren Y, Kang SH, Geiger
F, Zhang LQ. Eur J Appl Physiol. 2014 Nov 28.
Improvement in upper leg muscle strength underlies beneficial effects of exercise therapy in knee
osteoarthritis: secondary analysis from a randomised controlled trial. Knoop J, Steultjens MP, Roorda LD,
Lems WF, van der Esch M, Thorstensson CA, Twisk JW, Bierma-Zeinstra SM, van der Leeden M, Dekker
Physiotherapy. 2014 Aug 13.
Principles of postoperative anterior cruciate ligament rehabilitation. Saka T. World J Orthop. 2014 Sep
18;
Discriminant analysis of neuromuscular variables in chronic low back pain. Rossi DM, Morcelli MH,
Cardozo AC, Denadai BS, Gonçalves M, Navega MT. J Back Musculoskelet Rehabil. 2014 Aug 28. [Epub
ahead of print]
Progress in sensorimotor rehabilitative physical therapy programs for stroke patients.
Chen JC, Shaw FZ. World J Clin Cases. 2014 Aug 16;2(8):316-26. doi: 10.12998/wjcc.v2.i8.316. Review.
Complex muscle vibration patterns to induce gait-like lower-limb movements: proof of concept.
Duclos C, Kemlin C, Lazert D, Gagnon D, Dyer JO, Forget R. J Rehabil Res Dev. 2014;51(2):245-51. doi:
10.1682/JRRD.2013.04.0079.
Exercise for reducing fear of falling in older people living in the community. Kendrick D, Kumar A,
Carpenter H, Zijlstra GA, Skelton DA, Cook JR, Stevens Z, Belcher CM, Haworth D, Gawler SJ, Gage H,
Masud T, Bowling A, Pearl M, Morris RW, Iliffe S, Delbaere K. Cochrane Database Syst Rev. 2014 Nov
28;11:CD009848. doi: 10.1002/14651858.CD009848.pub2. Review.
Effect of light and vigorous physical activity on balance and gait of older adults. Pau M, Leban B, Collu G,
Migliaccio GM. Arch Gerontol Geriatr. 2014 Nov-Dec;59(3):568-73. doi: 10.1016/j.archger.2014.07.008.
Epub 2014 Aug 2.
Functional benefits of tai chi training in senior housing facilities. Manor B, Lough M, Gagnon MM,
Cupples A, Wayne PM, Lipsitz LA. J Am Geriatr Soc. 2014 Aug;62(8):1484-9. doi: 10.1111/jgs.12946.
Erratum in: J Am Geriatr Soc. 2014 Nov;62(11):2233.
Improvements in gait characteristics after intensive resistance and functional training in people with
dementia: a randomised controlled trial. Schwenk M, Zieschang T, Englert S, Grewal G, Najafi B, Hauer K.
BMC Geriatr. 2014 Jun 12;14:73. doi: 10.1186/1471-2318-14-73.
60

Upper limb contributions to frontal plane balance control in rollator-assisted walking. Tung JY, Gage WH,
Poupart P, McIlroy WE. Assist Technol. 2014 Spring;26(1):15-21; quiz 22-3.
Creaby MW, Bennell KL, Hunt MA. Gait Differs Between Unilateral and Bilateral Knee Osteoarthritis.
Arch Phys Med Rehabil. 2012 Feb 29. [Epub ahead of print] PubMed PMID: 22385873.
Simonsen EB, Tegner H, Alkjær T, Larsen PK, Kristensen JH, Jensen BR, Remvig L, Juul-Kristensen B. Gait
analysis of adults with generalised joint hypermobility. Clin Biomech (Bristol, Avon). 2012 Feb 22. [Epub
ahead of print] PubMed PMID: 22364778.
Cimolin V, Galli M, Albertini G, Crivellini M, Romkes J, Brunner R. Quantitative analysis of upper limbs
during gait: a marker set protocol. J Appl Biomater Biomech. 2012 Feb 15:0. doi:
10.5301/JABB.2012.9040. [Epub ahead of print] PubMed PMID: 22367686.
Hamacher D, Bertram D, Fölsch C, Schega L. Evaluation of a visual feedback system in gait retraining: A
pilot study. Gait Posture. 2012 Mar 15. [Epub ahead of print] PubMed PMID: 22425191.
Bradley M, Sabatier JM. Acoustically-observable properties of adult gait. J Acoust Soc Am. 2012
Mar;131(3):EL210-5. PubMed PMID: 22423810.
Barthuly AM, Bohannon RW, Gorack W. Gait speed is a responsive measure of physical performance for
patients undergoing short-term rehabilitation. Gait Posture. 2012 Mar 7. [Epub ahead of print] PubMed
PMID: 22406292.
61

References
1. Nevitt MC, Cummings SR, Kidd S, Black D. Risk factors for recurrent nonsyncopal falls. A prospective
study. JAMA. 1989;261(18):2663–2668.
2. Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin Geriatr
Med. 2002;18(2):141–158.
3. Rubenstein LZ, Josephson KR. Falls and their prevention in elderly people: what does the evidence
show? Med Clin North Am. 2006;90(5):807–824.
4. Rubenstein LZ, Powers CM, MacLean CH. Quality indicators for the management and prevention of
falls and mobility problems in vulnerable elders. Ann Intern Med. 2001;135(8 pt 2):686–693.
5. Thurman DJ, Stevens JA, Rao JK. Practice parameter: assessing patients in a neurology practice for
risk of falls (an evidence-based review): report of the Quality Standards Subcommittee of the American
Academy of Neurology. Neurology. 2008;70(6):473–479.
6. Sudarsky L. Gait disorders: prevalence, morbidity, and etiology. Adv Neurol. 2001;87111–117.
7. Chu LW, Chi I, Chiu AY. Incidence and predictors of falls in the Chinese elderly [published correction
appears in Ann Acad Med Singapore. 2005;34(7):469]. Ann Acad Med Singapore. 2005;34(1):60–72.
8. Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the
community. N Engl J Med. 1988;319(26):1701–1707.
9. Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348(1):42–49.
10. Alexander NB. Gait disorders in older adults. J Am Geriatr Soc. 1996;44(4):434–451.
11. Alexander NB. Differential diagnosis of gait disorders in older adults. Clin Geriatr
Med. 1996;12(4):689–703.
12. Verghese J, LeValley A, Hall CB, Katz MJ, Ambrose AF, Lipton RB. Epidemiology of gait disorders in
community-residing older adults. J Am Geriatr Soc. 2006;54(2):255–261.
13. Bloem BR, Haan J, Lagaay AM, van Beek W, Wintzen AR, Roos RA. Investigation of gait in elderly
subjects over 88 years of age. J Geriatr Psychiatry Neurol. 1992;5(2):78–84.
14. Hough JC, McHenry MP, Kammer LM. Gait disorders in the elderly. Am Fam
Physician. 1987;35(6):191–196.
15. Sudarsky L. Clinical approach to gait disorders of aging: an overview. In: Masdeu JC, Sudarsky L,
Wolfson L, eds. Gait Disorders of Aging: Falls and Therapeutic Strategies. Philadelphia, Pa.: Lippincott-
Raven; 1997:147–157.
62
16. Centers for Disease Control and Prevention. Prevalence and most common causes of disability
among adults—United States, 2005. MMWR Morb Mortal Wkly Rep. 2009;58(16):421–426.
17. Bloem BR, Gussekloo J, Lagaay AM, Remarque EJ, Haan J, Westendorp RG. Idiopathic senile gait
disorders are signs of subclinical disease. J Am Geriatr Soc. 2000;48(9):1098–1101.
18. Winter DA, Patla AE, Frank JS, Walt SE. Biomechanical walking pattern changes in the fit and
healthy elderly. Phys Ther. 1990;70(6):340–347.
19. Elble RJ, Thomas SS, Higgins C, Colliver J. Stride-dependent changes in gait of older people. J
Neurol. 1991;238(1):1–5.
20. Snijders AH, van de Warrenburg BP, Giladi N, Bloem BR. Neurological gait disorders in elderly
people: clinical approach and classification. Lancet Neurol. 2007;6(1):63–74.
21. Verghese J, Lipton RB, Hall CB, Kuslansky G, Katz MJ, Buschke H. Abnormality of gait as a
predictor of non-Alzheimer's dementia. N Engl J Med. 2002;347(22):1761–1768.
22. Moylan KC, Binder EF. Falls in older adults: risk assessment, management and prevention. Am J
Med. 2007;120(6):493.e1–493.e6.
23. Alexander NB, Goldberg A. Gait disorders: search for multiple causes. Cleve Clin J
Med. 2005;72(7):586, 589–590592–594passim.
24. Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and
meta-analysis: II. Cardiac and analgesic drugs. J Am Geriatr Soc. 1999;47(1):40–50.
25. Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and
meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc. 1999;47(1):30–39.
63

Your Top Choice in Continuing EducationTM
Any opinions, findings, recommendations or conclusions expressed by the author(s) or speaker(s) do not necessarily reflect the views of Summit Professional Education. This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold with the understanding that the publisher is not engaged in rendering legal, accounting or other professional service. If legal advice or other expert assistance is required, the services of a competent professional person should be sought.
© Copyright 2014 John B. Perry, PT, CSCS, FAFS, CAFS, 3D MAPS & Summit Professional Education. No part of this workbook may be reproduced in any manner without the expressed written consent of John B. Perry, PT, CSCS, FAFS, CAFS, 3D MAPS and Summit Professional Education.
From a Declaration of Principles jointly adopted by a committee of the American Bar Association and a committee of Publishers.