a fully automated device fordeter- bacterial laboratorylaem.asm.org/content/22/6/980.full.pdf ·...
TRANSCRIPT

APPLIED MICROBIOLOGY, Dec. 1971, p. 980-986 Vol. 22, No. 6Copyright © 1971 American Society for Microbiology Printed in U.S.A.
Prototype of a Fully Automated Device for Deter-mination of Bacterial Antibiotic Susceptibility
in the Clinical LaboratorylHENRY D. ISENBERG, ALLEN REICHLER, AND DONALD WISEMANThe Long Island Jewish Medical Center, New Hyde Park, New York 11040, and
Technicon Instrument Corp., Tarrytown, New York 10591
Received for publication 12 July 1971
A completely automated system for the performance of antibiotic susceptibilitytests in the clinical laboratory is described. With a modicum of personnel involve-ment, data on 40 specimens tested against 13 antibiotics are obtained every hourafter an initial 3-hr period. The step by step explanation of the functioning of thisprototype system, based on a thoroughly tested manual model, is presented. Thesystem compares well with the standard diffusion test and has a potential for applica-tion to other endeavors of the clinical microbiology laboratory with a comparablesaving in time and labor.
The overriding responsibility of clinical micro-biology is the presumptive and rapid recognitionof a significant microorganism in a clinical spec-imen and the report of its presence, along with itsantibiotic susceptibility profile, to the clinicianwhile this information is still of consequence tothe diagnosis and treatment of the patient (7, 8,11). Although other divisions of laboratory medi-cine have successfully employed modern advancesin automation, clinical microbiology has beencontent to use the methods of 100 or more yearsago. Now that the clinician has finally acknowl-edged the need for specific guidance of antibiotictherapy, as predicted by Ericsson (3) and Barberand Garrod (1), this need cannot be met with themodem instruments and modalities at the disposalof other laboratory scientists. This consideration,coupled with the suggestion that some standard-ized method be used for the performance of theantibiotic susceptibility test (1, 2, 4, 5, 12), madeit seem natural to use this particular test to ac-quaint clinical microbiologists with the advan-tages of automation.Automated monitoring procedures for manu-
facturing processes involving microorganismshave been used for a number of years. They usu-ally involve onrly a single genetically stable assaymicroorganism and most frequently a single prod-uct, such as an antibiotic agent. In contrast, pro-cedures in the clinical field must provide informa-tion on the reaction of different bacteria to a
I Presented in part at the 71st Annual Meeting of the AmericanSociety for Microbiology, Minneapolis, Minn.
dozen or more drugs. Thus, the convenient indi-cators used in the automation of industrial proc-esses or quality control, such as carbon dioxideproduction and pH or Eh changes, could not beapplied universally to all of the fast-growingbacteria subject to screening for antibiotic suscep-tibility in the clinical laboratory. It was this im-portant requirement, namely, universal applica-bility of the monitoring method, which led toseveral attempts to find a rapid and accurateindicator of microbial proliferation and its inhibi-tion. To this end, natural and radioactive isotopesof phosphorus, glucose utilization, adenosinetriphosphate and other compounds were exam-ined. These approaches were accompanied byvariations in microbial responses, difficulties inreagent standardization, lack of reproducibility,and expense which made their suitability as uni-versal indicators questionable. However, a modi-fied particle-counting system was quite satisfac-tory.To investigate this modality, a manual progen-
itor of the fully automated system was devised.This system, reported earlier (6, 9), outlined stepsrequired for the fully automated system. Briefly,the methods consisted of preparing an inoculumof clinically significant organisms isolated onenrichment or selective media in the clinical labo-ratory. The inoculum consisted of 5 to 10 colonieswhich were suspended in 2 ml of optically cleanEugonbroth. Their turbidity was adjusted with abarium sulfate standard (2). A 1: 1,000 dilution ofthe inoculum was prepared in the same medium,
980
on June 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from

FULLY AUTOMATED ANTIBIOTIC TEST
distributed in 2-ml portions, and incubated at37 C for a 30-min equilibration; this was followedby the addition of antibiotics in the form of discsor appropriate dilutions of antibiotic solution.Two control tubes without antimicrobial agentsaccompanied each particular test run for eachbacterium. Bacteria in one of the tubes were killedwith Formalin at time zero, i.e., after the 30-minpreincubation and at the time of the addition ofantimicrobial agents. At the end of 150 min, For-malin was added to all of the remaining tubes. Thesecond tube without antibiotic thus served as agrowth control. After a 10-min hold, to insurekilling, the contents of the tubes were decantedinto a carrier system which was assayed automat-ically with the particle counter. All antimicrobialsusceptibility examinations were accompanied bythe performance of agar diffusion tests accordingto the instructions of Bauer et al. (2).
This report describes the prototype apparatusfor a fully automated system capable of perform-ing antibiotic susceptibility testing on clinicallysignificant, fast-growing bacteria and applicablein the clinical microbiology laboratory.
MATERILAS AND METHODS
Bacteria. Microorganisms which were isolated asdescribed (8) from pathological specimens, and whichwould normally have been tested for antibiotic suscep-tibility profiles, were included in the study. In addition,Escherichia coli ATCC 25922 and Staphylococcusaureus ATCC 25923 were tested with each battery ofmicroorganisms undergoing examination.
Inoculum broth. The earlier study had shown thatEugonbroth (BBL) contained the least number ofoptically discernible particles after autoclaving. Eu-gonbroth was therefore chosen as the medium for usein the automated antibiotic susceptibility tests. For thepreparation of the inoculum, one-quarter strengthEugonbroth (OCIB), filtered through 0.45-Mm mem-brane filters (Millipore Corp.) before autoclaving, wasused.Medium. For the automated procedure, full strength
Eugonbroth (OCB), Millipore-filtered as describedprior to autoclaving, was contained in a large plasticbag from which it was delivered automatically to thedispensing mechanism for the individual test.
Formalin. A 25% aqueous solution of Formalin wasstored within the machine and delivered to the variousstations as required for killing the microorganisms.
Agar diffusion tests. Each and every bacteriumtested by the automated procedure was also examinedby the standardized Kirby-Bauer method (2). Theprocedure was followed to the letter. Only high-con-tent discs, certified by the Food and Drug Administra-tion, were employed. Mueller-Hinton agar plates filledto the proper depth, supplied through the courtesy ofBioquest, Division of Becton, Dickinson & Co., wereused. After 18 hr of incubation at 35 C, the zones ofinhibition were measured with calipers, recorded in
TABLE 1. Discs usedfor the automated determinationof antibiotic susceptibility
Disc Content Final concn/ml
Penicillin.............. 2 units 1 unitMethicillin .......... 10 ,ug 5 ,gAmpicillin............. 10 ,g 5 ,gCephalothin .......... 10 ,g 5 ,ugTetracycline .......... 20 ,g 10 4gErythromycin.......... 10 jAg 5 ,gOleandomycin ........ 10 ,ug 5 jugChloramphenicol ...... 10 ,g 5 ,ugLincomycin............ 2 ug 1 ,ugKanamycin............ 20 ,Ag 10 ,ugColistin ............... 10 ,ug 5 ugGentamicin............ 50,ug 25 jgCarbenicillin .......... 100 ,ug 50 ,g
millimeters, and interpreted according to the guidepublished by the originators of the method.
Antibiotic discs for the automated system. The anti-biotic discs in strengths listed in Table 1 were deliveredto each proper individual carrier for the determinationof antibiotic susceptibility. As reported earlier (6, 9),the delivery of these antibiotic discs served merely tocarry the antimicrobial agents into the broth. It is nec-essary to reiterate the published findings that the lib-eration of antibiotic agents from the carrier paper oc-curs in all instances in 1 min or less (6, 9).
Additional system specifications. All excess materialaspirated in the process ofcounting goes. into a collec-tion unit. The cups are practically dry at the end of thedetermination. It is important to appreciate that theentire system is maintained at 37 C, and 100% of theair is circulated through a HEPA filter. Thus, 10%fresh air and 90% recirculated air constitutes eachlaminar flow cycle. The 10% of air exhausted carrieswith it the Formalin fumes.
RESULTSThe sequential steps carried out by the fully
automated device are demonstrated in Fig. 1. Ofcourse, fully automated is not meant to implythat no human intervention is required. At station1 an individual will have to load trays into themachine. The supply of sterile Eugonbroth has tobe stored in the machine at various time intervalsdepending on the requirements of the individuallaboratory; routinely, one plastic soft containerholds broth for testing 100 samples. Unknownand control samples are introduced at station 3a;antibiotic disc supplies are maintained at station5. At this station, as well as at station 7, Formalindelivery from a general reservoir is required. Thereservoir provided can serve for several days'examinations.Sample preparation is in keeping with the con-
ventional method. Approximately 10 colonies ofan isolated organism recognized on the basis of
981VOL. 22, 1971
on June 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from

ISENBERG, REICHLER, AND WISEMAN APPL. MICROBIOL.
Dispense Load SamplerStorihs \ Wilh Tubes (S)Broth Inoculum Disp.ns@_ __ (i) ~~~~~~~~~~~~~~~~~Antibiotics(13X)
Trays oi Fomalin(1X)
Into l l Incubate Incubate30 minm 377C 15 min@37C
r.
Kill All Test Ie
@ @ ~~~~~~~~~~~~~~and ControlTi I
Data OpticalResults Roduction Count _
Alam SampleSignals Disposal
FIG. 1. Schematic representation of the automateddevice.
3a (Fig. 1). This introduction does not interferewith the maintenance of the temperature and air-flow environment of the device.
Light metal scaffold trays bearing plastic dis-posable cups or vessels are introduced into thesystem at station 1 (Fig. 1). Each tray consists of10 rows, and each row contains 15 individual dis-posable cups. Each cup has a volume of 4 ml.Each row of 15 vessels represents a single test run.Thus, each tray is suitable for the performance of10 antibiotic susceptibility determinations by theautomated system. Trays are advanced automat-ically. This advance is predetermined, synchro-nized with the entire system, and controlled by aresetting clock mechanism. At station 2 (Fig. 1),prewarmed OCB is dispensed into each of the 15cups sequentially. As can be seen in Fig. 3, a metaldelivery needle attached to the dispensing systemadvances to each cup and delivers 2 ml of brothinto each cup. At the end of the row and after aprogrammed hold, the tray advances one stop andthe delivery needle fills the following row of vesselsin the opposite direction. When a tray reachesstation 3 (Fig. 1), an inoculum-dispensing arm
FIG. 3. Close-up view of broth dispensing. Noteneedlelike tip of dispensing mechanism centered oversingle cup.
FIG. 2. Inoculum tubes with specially designedpipetteclosure, added after nephelometric standardization, incarrier tray used for insertion into the system.
colonial morphology are suspended in a tube con-taining OCIB. It is more convenient to use tubeswith stainless-steel or plastic closures. The inocu-lum is then standardized in a nephelometer, aninstrument supplied but separate from the fullyautomated device. The nephelometer is so cali-brated that a specified reading on the scale cor-responds to approximately 105 bacteria per ml.After nephelometric standardization, the tubesare closed with a special disposable pipette con-taining closures and are inserted into the carrieras demonstrated in Fig. 2. This carrier holding 20tubes of inoculum preparation broth is then intro-duced into the fully automated system at station
FiG. 4. Inoculum pipette pick up. The inoculwnaspirator arm descended, aspirated inoculwn, and, whileretaining the inoculated broth, has descended and is nowready to proceed toward the cups seen in the back-ground.
982
on June 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from
FULLY AUTOMATED ANTIBIOTIC TEST
the rotary inoculum tray advances one stop, per-mitting the inoculating device to center on the nexttube to serve as inoculum. This event does not oc-cur until the tray within the system has advancedone row. After inoculation, the trays enter the pre-incubation phase. This 30-min preincubation per-
a ll5..mits the bacteria to equilibrate and overcome the6 | |It-initial lag phase. At the conclusion of the 30-mm
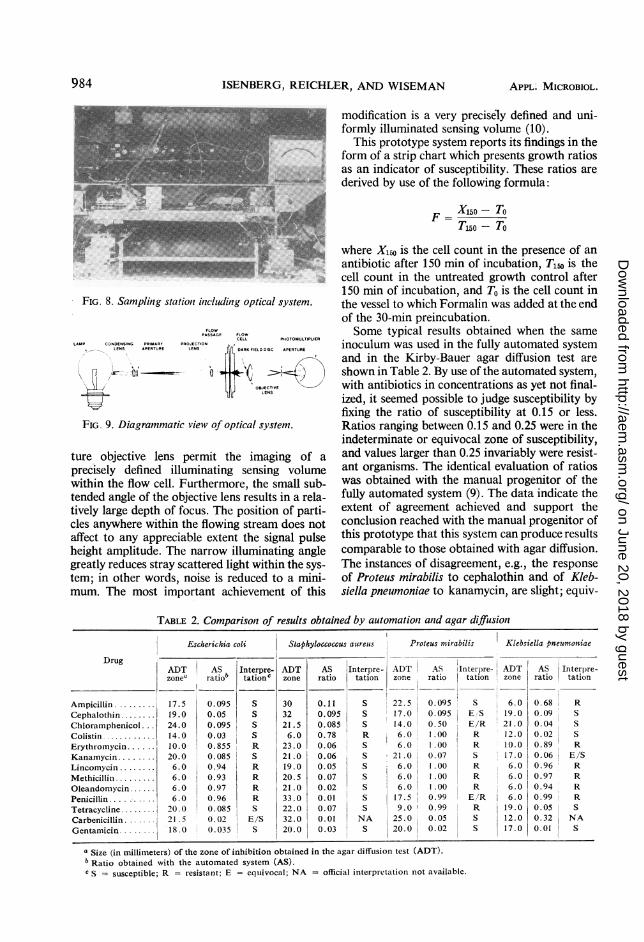
l period, the tray has arrived at the antibiotic-dis-pensing station (station 5, Fig. 1). Here, the firstcup in each row receives 0.5 ml of 25% Formalin.The second cup has no addition, and the remaining13 cups each receive an antibiotic disc as shown inFig. 6. Once the antibiotic has been delivered to
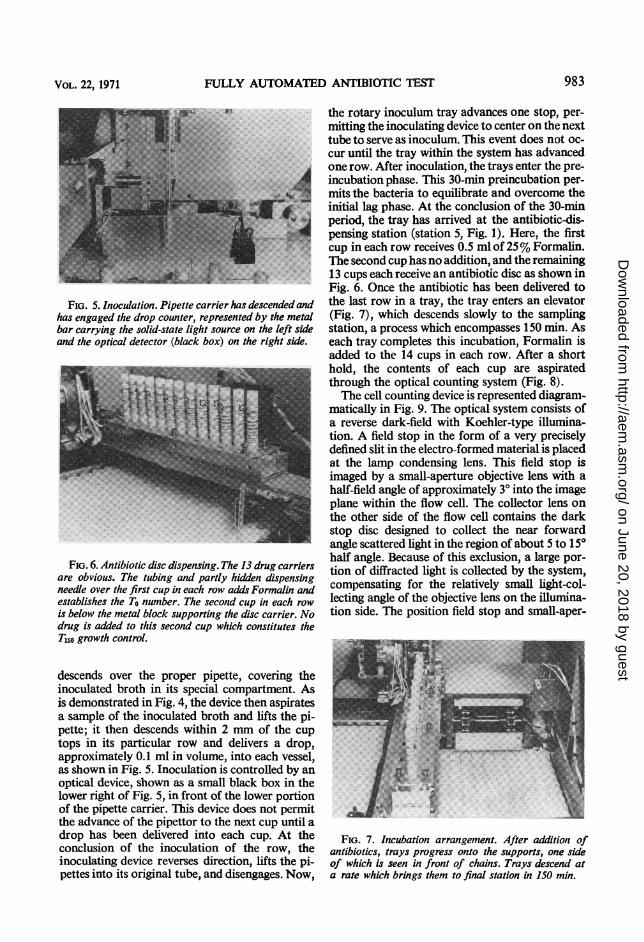
FIG. 5. Inoculation. Pipette carrier has descended and the last row in a tray, the tray enters an elevatorhas engaged the drop counter, represented by the metal (Fig. 7), which descends slowly to the samplingbar carrying the solid-state light source on the left side station, a process which encompasses 150 min. Asand the optical detector (black box) on the right side. each tray completes this incubation, Formalin is
added to the 14 cups in each row. After a shorti62K>ohold, the contents of each cup are aspirated
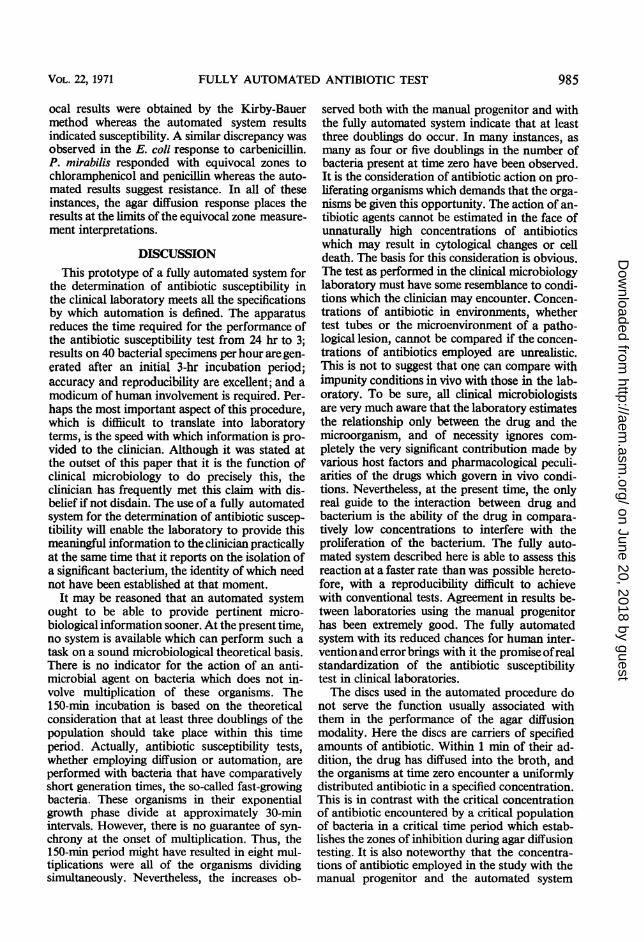
through the optical counting system (Fig. 8).The cell counting device is represented diagram-
matically in Fig. 9. The optical system consists ofa reverse dark-field with Koehler-type illumina-tion. A field stop in the form of a very preciselydefined slit in the electro-formed material is placedat the lamp condensing lens. This field stop is
Ym _ imaged by a small-aperture objective lens with ahalf-field angle of approximately 30 into the imageplane within the flow cell. The collector lens onthe other side of the flow cell contains the darkstop disc designed to collect the near forwardangle scattered light in the region of about 5 to 15°
F.G6.Antibioticdisc dispens. The13drugcahalf angle. Because of this exclusion, a large por-FIG. 6. Antibiotic disc dispensing. The 13 drug carriers tion of diffracted light is collected by the system,
are obvious. The tubing and partly hidden dispensingneedle over the first cup in each row adds Formalin and compensating for the relatively small light-col-establishes the To number. The second cup in each row lecting angle of the objective lens on the illumina-is below the metal block supporting the disc carrier. No tion side. The position field stop and small-aper-drug is added to this second cup which constitutes theT150o growth control.
descends over the proper pipette, covering theinoculated broth in its special compartment. As_is demonstrated in Fig. 4, the device then aspirates Sa sample of the inoculated broth and lifts the pi-pette; it then descends within 2 mm of the cuptops in its particular row and delivers a drop,approximately 0.1 ml in volume, into each vessel,as shown in Fig. 5. Inoculation is controlled by anoptical device, shown as a small black box in thelower right of Fig. 5, in front of the lower portionof the pipette carrier. This device does not permitthe advance of the pipettor to the next cup until adrop has been delivered into each cup. At the FIG. 7. Incubation arrangement. After addition ofconclusion of the inoculation of the row, the antibiotics, trays progress onto the supports, one sideinoculating device reverses direction, lifts the pi- of which is seen in front of chains. Trays descend atpettes into its original tube, and disengages. Now, a rate which brings them to final station in 150 min.
983VOL. 22, 1971
on June 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from
ISENBERG, REICHLI
FIG. 8. Sampling station inicluding optical system.
FLOWPASSAGE FLOW
CELL PHOTOIIIULTIPLIERLAMtP CONDENSING PRIMARY PROJECTION
LENS APERTURE LENS AR FIEL DISC APERTU
FIG. 9. Diagrammatic view of optical system.
ture objective lens permit the imaging of a
precisely defined illuminating sensing volumewithin the flow cell. Furthermore, the small sub-tended angle of the objective lens results in a rela-tively large depth of focus. The position of parti-cles anywhere within the flowing stream does notaffect to any appreciable extent the signal pulseheight amplitude. The narrow illuminating anglegreatly reduces stray scattered light within the sys-
tem; in other words, noise is reduced to a mini-mum. The most important achievement of this
ER, AND WISEMAN APPL. MICROBIOL.
modification is a very precisely defined and uni-formly illuminated sensing volume (10).
This prototype system reports its findings in theform of a strip chart which presents growth ratiosas an indicator of susceptibility. These ratios are
derived by use of the following formula:
F X150- To1150 - To
where X150 is the cell count in the presence of an
antibiotic after 150 min of incubation, T1w is thecell count in the untreated growth control after150 min of incubation, and To is the cell count inthe vessel to which Formalin was added at the endof the 30-min preincubation.Some typical results obtained when the same
inoculum was used in the fully automated systemand in the Kirby-Bauer agar diffusion test are
shown in Table 2. By use of the automated system,with antibiotics in concentrations as yet not final-ized, it seemed possible to judge susceptibility byfixing the ratio of susceptibility at 0.15 or less.Ratios ranging between 0.15 and 0.25 were in theindeterminate or equivocal zone of susceptibility,and values larger than 0.25 invariably were resist-ant organisms. The identical evaluation of ratioswas obtained with the manual progenitor of thefully automated system (9). The data indicate theextent of agreement achieved and support theconclusion reached with the manual progenitor ofthis prototype that this system can produce resultscomparable to those obtained with agar diffusion.The instances of disagreement, e.g., the responseof Proteus mirabilis to cephalothin and of Kleb-siella pneumoniae to kanamycin, are slight; equiv-
TABLE 2. Comparisont of results obtained by automationt and agar diffusionI
Escherichia coli Staphyloccoccus aureus Proteus mirabilis Klebsiella pneurnoniae
DrugADT AS Interpre- ADT AS Interpre- ADT AS iInterpre- ADT AS Interpre-zone ratiob tationc zone ratio tation zone ratio tation zone ratio tation
Ampicillin. 17.5 0.095 S 30 0.11 S 22.5 0.095 S 6.0 0.68 RCephalothin ........ 19.0 0.05 S 32 0.095 S 17.0 0.095 E S 19.0 0.09 SChloramphenicol 24.0 0.095 S 21.5 0.085 S 14.0 0.50 E/R 21.0 0.04 SColistin............ 14.0 0.03 S 6.0 0.78 R 6.0 1.00 R 12.0 0.02 S
Erythromycin.. 10.0 0.855 R 23.0 0.06 S 6.0 1.00 R 10.0 0.89 RKanamycin.. 20.0 0.085 S 21.0 0.06 S . 21.0 0.07 S 17.0 0.06 E/SLincomycin ........ 6.0 0.94 R 19.0 0.05 S 6.0 1.00 R 6.0 0.96 R
Methicillin.6.0 0.93 R 20.5 0.07 S 6.0 1.00 R 6.0 0.97 ROleandomycin... 6.0 0.97 R 21.0 0.02 S 6.0 1.00 R 6.0 0.94 RPenicillin.6.0 0.96 R 33.0 0.01 S 17.5 0.99 E/R 1 6.0 0.99 R
Tetracycline ....... 2.-0.0 0.085 S 22.0 0.07 S 9.0 I 0.99 R 19.0 0.05 SCarbenicillin.. 1.5 0.02 E/S 32.0 0.01 NA 25.0 0.05 S 12.0 0.32 NAGentamicin.18.0 0.035 S 20.0 0.03 S 20.0 0.02 S 17.0 0.01 S
a Size (in millimeters) of the zone of inhibition obtained in the agar diffusion test (ADT).b Ratio obtained with the automated system (AS).c S = susceptible; R = resistant; E = equivocal; NA = official interpretation not available.
984
on June 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from
FULLY AUTOMATED ANTIBIOTIC TEST
ocal results were obtained by the Kirby-Bauermethod whereas the automated system resultsindicated susceptibility. A similar discrepancy wasobserved in the E. coli response to carbenicillin.P. mirabilis responded with equivocal zones tochloramphenicol and penicillin whereas the auto-mated results suggest resistance. In all of theseinstances, the agar diffusion response places theresults at the limits of the equivocal zone measure-ment interpretations.
DISCUSSIONThis prototype of a fully automated system for
the determination of antibiotic susceptibility inthe clinical laboratory meets all the specificationsby which automation is defined. The apparatusreduces the time required for the performance ofthe antibiotic susceptibility test from 24 hr to 3;results on 40 bacterial specimens per hour are gen-erated after an initial 3-hr incubation period;accuracy and reproducibility are excellent; and amodicum of human involvement is required. Per-haps the most important aspect of this procedure,which is diffiicult to translate into laboratoryterms, is the speed with which information is pro-vided to the clinician. Although it was stated atthe outset of this paper that it is the function ofclinical microbiology to do precisely this, theclinician has frequently met this claim with dis-belief if not disdain. The use of a fully automatedsystem for the determination of antibiotic suscep-tibility will enable the laboratory to provide thismeaningful information to the clinician practicallyat the same time that it reports on the isolation ofa significant bacterium, the identity of which neednot have been established at that moment.
It may be reasoned that an automated systemought to be able to provide pertinent micro-biological information sooner. At the present time,no system is available which can perform such atask on a sound microbiological theoretical basis.There is no indicator for the action of an anti-microbial agent on bacteria which does not in-volve multiplication of these organisms. The150-min incubation is based on the theoreticalconsideration that at least three doublings of thepopulation should take place within this timeperiod. Actually, antibiotic susceptibility tests,whether employing diffusion or automation, areperformed with bacteria that have comparativelyshort generation times, the so-called fast-growingbacteria. These organisms in their exponentialgrowth phase divide at approximately 30-minintervals. However, there is no guarantee of syn-chrony at the onset of multiplication. Thus, the150-min period might have resulted in eight mul-tiplications were all of the organisms dividingsimultaneously. Nevertheless, the increases ob-
served both with the manual progenitor and withthe fully automated system indicate that at leastthree doublings do occur. In many instances, asmany as four or five doublings in the number ofbacteria present at time zero have been observed.It is the consideration of antibiotic action on pro-liferating organisms which demands that the orga-nisms be given this opportunity. The action of an-tibiotic agents cannot be estimated in the face ofunnaturally high concentrations of antibioticswhich may result in cytological changes or celldeath. The basis for this consideration is obvious.The test as performed in the clinical microbiologylaboratory must have some resemblance to condi-tions which the clinician may encounter. Concen-trations of antibiotic in environments, whethertest tubes or the microenvironment of a patho-logical lesion, cannot be compared if the concen-trations of antibiotics employed are unrealistic.This is not to suggest that one can compare withimpunity conditions in vivo with those in the lab-oratory. To be sure, all clinical microbiologistsare very much aware that the laboratory estimatesthe relationship only between the drug and themicroorganism, and of necessity ignores com-pletely the very significant contribution made byvarious host factors and pharmacological peculi-arities of the drugs which govern in vivo condi-tions. Nevertheless, at the present time, the onlyreal guide to the interaction between drug andbacterium is the ability of the drug in compara-tively low concentrations to interfere with theproliferation of the bacterium. The fully auto-mated system described here is able to assess thisreaction at a faster rate than was possible hereto-fore, with a reproducibility difficult to achievewith conventional tests. Agreement in results be-tween laboratories using the manual progenitorhas been extremely good. The fully automatedsystem with its reduced chances for human inter-ventionand error brings with it the promise ofrealstandardization of the antibiotic susceptibilitytest in clinical laboratories.The discs used in the automated procedure do
not serve the function usually associated withthem in the performance of the agar diffusionmodality. Here the discs are carriers of specifiedamounts of antibiotic. Within 1 min of their ad-dition, the drug has diffused into the broth, andthe organisms at time zero encounter a uniformlydistributed antibiotic in a specified concentration.This is in contrast with the critical concentrationof antibiotic encountered by a critical populationof bacteria in a critical time period which estab-lishes the zones of inhibition during agar diffusiontesting. It is also noteworthy that the concentra-tions of antibiotic employed in the study with themanual progenitor and the automated system
VOL. 22, 1971 985
on June 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from

986 ISENBERG, REICHI
have not been agreed upon finally. Although sev-eral thousand clinical specimens have been ex-posed to analysis, especially by the manual sys-tem, decision has been delayed to allow anexhaustive search for all possible variations. Asstated earlier, these tests are being carried out inconjunction with concomitant screening by thestandardized Kirby-Bauer method. Just as zonesizes for each antibiotic may differ from bacterialspecies to bacterial species, so will it be necessaryto adjust the interpretation of the ratios obtainedwith the fully automated system. These adjustmentsmay involve changing the concentration of anti-biotic in certain discs slightly or adjusting the clas-sification of ratios obtained according to thebacterial species and the drug used. It must alsobe remembered that the usual inoculum prepara-tion for the automated system incorporates 5 to10 colonies, usually 10. Therefore, an overt ex-pression of heterogeneity in a particular bacterialpopulation from a clinical specimen is enhanced.There exists, in addition, the possibility that theestablished differences between dilution and diffu-sion assays of antibiotic susceptibility may be-come manifest occasionally and lead to negligibledifferences of interpretation in results obtained byboth the standard diffusion and the automatedmethods. Complete appreciation of these differ-ences must await the previously mentioned ex-haustive study.
It is very important to recall that this is a proto-type system for the performance of antibioticsusceptibility tests in a clinical laboratory. As withall prototypes, many modifications will be incor-porated in future models. Thus, instead of a stripchart displaying the ratios representing antibioticsusceptibility, digital printout of the ratios will bemade available. Easier access to parts of the auto-mated machinery will be incorporated. It will bepossible also to control the length of incubation.Although we do not intend to shorten the incuba-tion or the preincubation periods, it may be desir-
LE-R, AND WISEMAN APPL. MICROBIOL.
able to test microorganisms with longer genera-tion times by doubling or tripling the 150-minincubation. It may also be possible to limit thenumber of cups per row to be inoculated. Thischange or choice will provide the user with theopportunity to expand the versatility of the ma-chine. The application of automation to clinicalmicrobiology is limited only by the ingenuity ofits users; for example, the automated systemmight be used to screen urine specimens quanti-tatively for the presence of viable bacteria per unitvolume, to use simple identification schemes offast-growing bacteria, and to determine minimalinhibitory concentrations.
LITERATURE CITED
1. Barber, M., and L. P. Garrod. 1963. Antibiotic and chemo-therapy. The Williams & Wilkins Co., Baltimore.
2. Bauer, A. W., W. M. M. Kirby, J. C. Sherris, and M. Turck.1966. Antibiotic susceptibility testing by a standardizedsingle disc method. Amer. J. Clin. Pathol. 45:493-497.
3. Ericsson, H. 1960. Rational use of antibiotics in hospitals.Scand. J. Clin. Lab. Invest. 12(Suppl. 50).
4. Ericsson, H. 1964. Standardization of methods for conductingmicrobic sensitivity tests. Preliminary Report of a WorkingGroup of the International Collaborative Study Sponsoredby WHO. Karolinska siukhuset, Stockholm.
5. Ericsson, H., and J. C. Sherris. 1971. Antibiotic sensitivitytesting. Report of an international collaborative study. ActaPathol. Microbiol. Scand. Sec. B 79(Suppl. 217).
6. Isenberg, H. D. 1971. Development of an automated methodto determine antibiotic susceptibility of rapidly growingorganisms. Advan. Automated Anal. 1:371-376.
7. Isenberg, H. D., and J. I. Berkman. 1962. Microbial diagnosisin a general hospital. Ann. N.Y. Acad. Sci 98:647-669.
8. Isenberg, H. D., and J. I. Berkman. 1966. Recent practices indiagnostic bacteriology. Prog. Clin. Pathol. 1:237-317.
9. lsenberg, H. D., and J. Seo. 1971. Experimental foundation forthe automated antibiotic susceptibility test. Advan. Auto-mated Anal. 1:377-380.
10. Mansberg, H. P. 1970. Optical techniques of particle counting.Transactions of the Technicon International Congress-1969,p. 213-219.
11. Steel, K. J. 1962. The practice of bacterial identification.Symp. Soc. Gen. Microbiol. 12:405-432.
12. World Health Organization. 1961. Standardization of methodsfor conducting microbic sensitivity tests. World HealthOrgan. Tech. Rep. Ser. No. 210.
on June 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from