a framework for building capacity to improve health
TRANSCRIPT

A Framework for Building Capacity
to Improve Health
01/646 Capacity Cover.qxd 3/28/01 3:44 PM Page 2

NSW HEALTH DEPARTMENT
This work is copyright. It may be reproduced in whole or in part for study training purposes subject to the inclusionof an acknowledgement of the source and no commercialusage or sale.
© NSW Health Department 2001
SHPN: (HP) 990226 ISBN: 0 7347 3124 8
For further copies please contact:
Better Health Centre – Publications WarehouseLocked Mail Bag 5003 Gladesville, NSW 2111Tel. (02) 9816 0452Fax.: (02) 9816 0492
A full copy of this report and others in this series can be downloaded from the NSW HealthWeb site:www.health.nsw.gov.au
March 2001
01/646 Capacity Cover.qxd 3/28/01 3:44 PM Page 3
NSW Health A Framework for Building Capacity to Improve Health i
CAPACITY BUILDING is…An approach to the development of sustainable skills, organisational
structures, resources and commitment to health improvement in health
and other sectors, to prolong and multiply health gains many times over.
Hawe et al: 1999

A Framework for Building Capacity to Improve Health NSW Healthii
NSW Health has one of the largest and best health systems in the world.The recently releasedHealth - Working as a Team: the way forwardcommits NSW Health to further improvements in service delivery.While primarily focused onclinical care, these improvements also include anemphasis on preventing illness and promotinggood health, health service providers workingtogether, community participation, and a high level of leadership across the system.
One mechanism available to the health system tocontribute to preventing illness and promoting health,is to incorporate effective health promotion programsinto the routine work of services from across thewhole health care continuum (prevention, diagnosis,treatment, rehabilitation and palliative care). Manyparts of the system are already doing this.
This document, A Framework for Building Capacity toPromote Health provides a guide for enhancing thecapability of the system to improve health. It is mainlyfocussed on building capacity within programs but it is paramount that when thinking about buildingcapacity within programs, or within the community,that we are also focussed on building the capacity of the system to support change. Most importantly,the document emphasises five key action areas incapacity building: organisational change, workforcedevelopment, resource allocation, partnerships and leadership.
Using this framework will increase the likelihood thathealth promotion programs will be sustained and thatpeople working on programs will have a greatercapacity to address future health challenges, whateverthose challenges may be.
This is useful information and I encourage healthworkers to adapt the framework to their setting orwork environment with the understanding that indoing so, they will enhance the potential of the NSWHealth system to maximise health investments andmultiply health gains.
Michael ReidDirector GeneralNSW Health Department
orewordF

NSW Health A Framework for Building Capacity to Improve Health iii
Section 1
Introduction ......................................................................................................................................................... 1
Section 2
Understanding capacity building ..........................................................................................................................3
What is capacity building? ................................................................................................................................3
Principles of capacity building practice .............................................................................................................5
Why focus on capacity building?.......................................................................................................................7
Section 3
Strategies for capacity building .............................................................................................................................8
Key action areas
� Organisational Development .........................................................................................................................10
� Workforce Development...............................................................................................................................12
� Resource Allocation......................................................................................................................................14
Key elements of context
� Leadership ....................................................................................................................................................16
� Partnerships ..................................................................................................................................................18
Section 4
Monitoring and evaluating practice.......................................................................................................................20
Section 5
Useful resources ....................................................................................................................................................24
Section 6
Challenges for the future? .....................................................................................................................................26
Section 7
References............................................................................................................................................................27
Appendix 1
Acknowledgments ................................................................................................................................................29
ontentsC
Please note The term ‘health promotion practitioner’ or ‘practitioner’ is used within this document to refer to any personskilled in health promotion and working with others to increase their capacity to improve health.This meanshealth promotion professionals, other health staff, staff from other organisations and community members.


Introduction
NSW Health A Framework for Building Capacity to Improve Health 1
1
i
Building capacity to improve health is animportant element of effective health promotionpractice. It increases the range of people,organisations and communities who are able toaddress health problems, and in particular,problems that arise out of social inequity andsocial exclusion.
“Coupled with a new notion of shared responsibility, andthe building of new coalitions with common goals and acommon purpose, capacity-building is a key ingredient inredressing social exclusion, inequality and vulnerability inour community”
1
Robert Fitzgerald,NSW Community Services Commissioner
Capacity building is an approach to development that builds independence
2. It can be:
� a ‘means to an end’, where the purpose is for others to take on programs
� an ‘end’ in itself, where the intent is to enableothers, from individuals through to governmentdepartments, to have greater capacity to worktogether to solve problems
� a process, where capacity building strategies areroutinely incorporated as an important element of effective practice.
What emerges in discussion and debate about thepurpose and process of capacity building is thatdifferent organisations have quite different ways of conceptualising capacity building
3.
A Framework for Building Capacity to Improve Healthis a revised edition of an earlier document, CapacityBuilding Framework
4. It's purpose is to guide the
development of effective capacity building practicewithin health promotion. It has been developed inconsultation with health promotion practitioners andother key stakeholders and it draws on capacitybuilding work funded, or partly funded, by NSWHealth.This includes:
� The Capacity Building Process and OutcomesIndicator Project which was conducted by SydneyUniversity.The project report Indicators to Help withCapacity Building in Health Promotion
5presents the
research findings and the checklists developed toinform and monitor capacity building practice.
� The NSW Health Promoting Hospital Projectwhich gathered a significant amount ofinformation about health promoting health servicesand identified a range of issues for health servicemanagers
6.
� Work located in the Northern Rivers HealthService Area and conducted by the University of Queensland which resulted in the developmentof an audit tool to monitor capacity building incommunity based projects
7,8.
The model presented below (Figure 1) reflects thispre-existing work, feedback from practitioners and the work of other researchers. It links the:
� key areas for strategy development (organisationaldevelopment, workforce development, resourceallocation, partnerships and leadership); to
� the three dimensions of capacity building identifiedby Hawe, King and Noort (infrastructuredevelopment, program sustainability and enhancedproblem solving).
In addition, the model highlights the importance ofthe 'context' within which capacity building happensand reinforces the message that all capacity building iscontext rich: that strategies and approaches need totake account of context at all times.

A Framework for Building Capacity to Improve Health NSW Health2
The intent of this document is to further explain theabove model and guide the development of capacitybuilding strategies across the key action areas.
The first section of the document provides anoverview of capacity building and the principles thatunderpin its practice, and introduces practitioners tosome of the language of capacity building.The secondsection explains the components of the frameworkand lists suggested strategies for each area.The thirdsection provides some suggestions for assessing andmonitoring progress, and the final sections provide alist of useful resources to inform and support capacitybuilding practice.
The Framework has grown out of information gainedin developing Indicators to Help with Capacity Buildingin Health Promotion.
5Questions are often asked about
the links between the key action areas suggestedwithin this document (organisational development,workforce development, resource allocation, and theelements of partnerships and leadership) and thechecklists presented within the 'Indicators' document.
While these links are still being explored it seems that
� Some checklists may reflect activity across a number of the key action areas.
For example, checklist number seven, ‘Assessing thecapacity of a particular organisation to tackle ahealth issue’ could be used to guide and monitor arange of strategies from across all of the actionareas.
� Others will primarily reflect one aspect of aparticular strategy.
For example, checklist number two, ‘Assessingopportunities to promote incidental learningamong other health workers’, captures some of thestructural and informal links that form part of aneffective 'workforce development' strategy.
Our understanding of these links will be strengthenedas more and more practitioners apply the Frameworkand the Indicators and the breadth and depth ofresearch increases.
Capacity Building Framework
Organisational development
Workforce development
Resource allocation
Partnerships
Leadership
Context
Build Capacity� Infrastructure
� Programsustainability
� Problem solving
Figure 1 Capacity Building Framework

What is capacity building?Capacity building is sometimes described as the‘invisible work’ of health promotion
10. It is the ‘behind
the scenes’ efforts by practitioners that increases thelikelihood that effective health promotion programswill be sustained.
This can include activities as diverse as canvassing the opportunities for a program, lobbying for support,developing skills, supporting policy development,negotiating with management, guiding theestablishment of partnerships, or contributing toorganisational planning.
Capacity building is defined as an approach to ‘thedevelopment of sustainable skills, structures, resourcesand commitment to health improvement in health and other sectors to prolong and multiply health gains many times over’.
5
The language of ‘capacity building’ and its relatedconcepts are used in many fields. Bush notes that‘social determinants’, ‘prevention’, ‘community’and ‘partnerships’ are the substance of the language of capacity building across a wide range oforganisations
11. In addition, much work has been
done which points to the importance of capacity to work in partnership
12,13, and the value of this in
contributing to more effective health outcomes.
Capacity building occurs both within programs ormore broadly within systems and leads to greatercapacity of people, organisations and communities topromote health (Figure 2).This means that capacitybuilding activity may be developed with individuals,groups, teams, organisations, inter-organisationalcoalitions, or communities.
Understanding capacity building
NSW Health A Framework for Building Capacity to Improve Health 3
2
Health Promotion Practice
Greater capacity of people, organisations andcommunities to promote health
Within programs Within systems
Build Capacity� Infrastructure
� Program sustainability
� Problem solving
Hawe et al
Figure 2 Levels of Capacity Building

A Framework for Building Capacity to Improve Health NSW Health4
At any one time a practitioner may be buildingcapacity at many levels within one health promotionprogram. For example, a practitioner may be workingwith:
� an individual, to develop particular healthpromotion planning skills
� a manager, to negotiate allocation of resources tosupport the program
� the project team, to develop their skills to manageand support the program, and identifyopportunities to integrate the project into routinework practice
� people from other sectors, to cultivate projectchampions in health and other sectors, and identifypotential project partners.
Each of these instances involve identifying andbuilding on existing capacities to enhanceindependence in health promotion.
Hawe, King and Noort5have identified three
distinctive dimensions to capacity buildingpractice(Figure 3).
This work represents a major step forward for health promotion practitioners by clearly articulatingthe intent of capacity building efforts. Eade alsohighlights the importance of being clear aboutcapacity building intent. She argues this assists in thedevelopment of relevant and focussed capacitybuilding objectives and strategies.
2
For example a practitioner may wish to engage an organisation in thinking about their contributionto health more broadly, and as a first step they mayengage their interest by working with them on aprogram of mutual interest. In addition to programstrategies, the practitioner may develop strategies that also contribute to the longer term goal.For example, they may develop planning processeswithin the program to engage senior managers in decision making about health or provide opportunities for incidental learning about health promotion concepts and processes.
The program itself may not be sustained. Not allprograms need to be sustained.What is moreimportant to sustain is the capacity for individuals,organisations and communities to mobilise themselves, when required, to initiate new action for new health challenges.
Dimensions of capacity building
1. Health Infrastructure or service development
Capacity to deliver particular program responses to particular health problems. Usually refers to the
establishment of minimum requirements in structures, organisations, skills and resources in the health sector.
2. Program maintenance and sustainability
Capacity to continue to deliver a particular program through a network of agencies, in addition to, or instead
of, the agency which initiated the program
3. Problem solving capability of organisations and communities
The capacity of a more generic kind to identify health issues and develop appropriate mechanisms to address
them, either building on the experience with a particular program or as an activity in its own right.
Reproduced from Indicators to Help with Capacity Building in Health Promotion. Hawe 2000
Figure 3 Capacity Building Dimensions

The following example illustrates how capacity to improve healthcan develop over time and how early work to build commitmentand enhance skills may be reinforced and supported by laterstrategies and support.
Principles of capacity building practiceWhatever the capacity building strategy or approach, orwhomever a practitioner may be working with (individuals,organisations or communities), a number of key principles always underpin effective capacity building practice:
Respect and value pre-existing capacitiesBefore beginning to build capacity within programs, practitionersneed to identify pre-existing skills, structures, partnerships andresources and work with, and respect these.
Effective capacity building practice links local people with contentand context expertise with health promotion practitioners withtechnical and capacity building expertise. It allows for an exchange ofexpertise between groups.
In addition, programs that are integrated into existing structures,and linked into existing positions and accountability processes,are more likely to be sustained.
14While it may seem simpler
to establish a separate vertical structure for management of aprogram, this often duplicates the workload of the peopleexpected to be involved and may suggest a lack of confidence inexisting structures or mechanisms. In the longer term this mayundermine existing political and workplace relationships andcontribute to a lack of support for a program.
One of the major criticisms of capacity building is that it is a ‘top-down’ approach that is often linked to a government's agendasfor change. Fitzgerald makes the point that this can also be astrength.
15He argues that when initiatives are supported and
reinforced by 'systems' they are probably more likely to be sustainable.
Develop trustThe notion of trust is ‘absolutely imperative to capacitybuilding’
15. Fitzgerald believes that capacity building is
underpinned by trust and respect, and these qualities ‘sit at theheart’ of why so many otherwise good initiatives have failed.He argues that the lack of trust between partners, families,children, and government is at an all time low, and that this isborn out of a failure of mutual respect or long term commitmentto the genuine needs and aspirations of all stakeholders.According to McPeake
16one of the key elements in developing
trust is perseverance.
"We earned their trust not by anything else but probably by the factthat we kept going back and they kept talking to us".
Building capacity for promotinghealth within a Western Sydneyschool community
� Following involvement in several healthpromotion initiatives, a communityworker from a neighbourhood centreattended a health promotion trainingprogram provided by the Area HealthService.
� Working with a community nurse, and in response to concern from parents,the worker suggested a project todevelop a canteen policy at the school,The principal negotiated with them toestablish a breakfast project instead.A project team was established andgained a $4000 health promotion seedinggrant.The process was supported byhealth promotion staff.
� Parents were assisted by the communityworker and the community nurse todevelop job descriptions for volunteersand guidelines for the breakfast program.A second round of funding was linked todevelopment of a nutrition policy for theschool. Health promotion staff continuedto support change.
� Over time, the parent volunteers tookresponsibility for the day-to-daymanagement of the breakfast programand the community worker continued to support them as needed.
� The community worker developedsophisticated planning skills and increasedher understanding of the determinants of health. She assisted the school submitfor and run a computer training programfor parents (with child care provided).The school and the community workercontinue to identify and support otherhealth promoting initiatives.
NSW Health A Framework for Building Capacity to Improve Health 5

Be responsive to contextContext refers to the range of physical, economic, political,organisational and cultural environments within which a programsits. 'Context' is often thought about as the environmentalconstraints on a program that are generally not amenable tochange. Programs never exist in isolation. Context can have anegative or positive impact on a program and is ever changing.Practitioners need to be aware of and be ready to respond tochanges in context.
Bush11
refers to work that was first proposed by Pawson andTilley
17and argues that researchers need to work out better ways
to capture context within program evaluation. He states that thepublic health field is very good at measuring problems andstrategies but an evaluation method that only focuses on themechanisms for change, tells only half the story (Figure 4).
Avoid pre-packaged ideas and strategies Capacity building is an approach to development not a set of pre-determined activities.There is no single way to build capacity.Although experience tells us there is a need to work across thekey action areas, practitioners approach each situation separately to identify pre-existing capacities and develop strategies particularto a program or organisation, in its time and place.
Capacity builders need the ability to observe accurately, to interprettheir observations intelligently and impersonally and then to deliver the appropriate intervention at the appropriate time.
18
It is also important to remember that the relationship between the program management group and the capacity builder willchange as decision making and program management skills evolve.The relationship may move from being a ‘hands on’ developmentrelationship to a ‘hands off ’ consultative or facilitative relationship.Practitioners need to be mindful of, and ready to change theirroles and responsibilities as capacity is increased.
For example, a newly established project team will have differentcapacity building needs to one that has been established for sometime and is competent and ready to contribute to problem solvingon broader health issues.
Capacity building within aNorthern Sydney LocalGovernment Tobacco Sales toMinors Project
� Cultivation of project champions withinlocal government to advocate for andsupport the program.
� Development of Memoranda ofUnderstanding between individualCouncils and the Health Service.
� Provision of training, information,and access to expertise in compliancemonitoring and prosecutions to Council officers.
� Strategies to enhance Councilcommitment to the program such as a submission to the National,Local Government Awards.
� Allocation of Council resources to cover legal costs.
� Development of a regional localgovernment structure for planning.
� Incorporation of responsibilities for theprogram into local government managementplans, staff work plans and policy
� Monitoring and review processesestablished within individual Councils to enhance project effectiveness.
� Enhancement of understanding withinCouncil of its ability to impact on health.
� Increased problem solving by Councils onthe most appropriate tobacco and otherstrategies for their communities
� Establishment of a regional localgovernment partnership to plan for andproblem solve broader health issues
A Framework for Building Capacity to Improve Health NSW Health6
Mechanismsfor change + Context = Outcome
Figure 4 Pawson and Tilley model for evaluating capacity building

NSW Health A Framework for Building Capacity to Improve Health 7
Develop well planned and integrated strategiesTo be most effective, capacity building needs to workat a number of levels (eg. with individuals, groups oracross organisations) and use a combination ofstrategies from the action areas of organisationaldevelopment, workforce development, resourceallocation, partnerships and leadership.The followingexample presents a range of interactive strategiesdeveloped within a Local Government project.
Kaplan18
discusses the importance of integratedstrategies as a key element in the development ofeffective capacity building organisations in Africa.Those organisations that had had most success wereconsistently found to be those who had first clearlyidentify their corporate goals, then developedworkforce strategies to meet these goals, and finallyre-allocated resources against their organisationalpriorities and goals.
Why focus on building capacity?There are a number of important reasons for the health system to focus on capacity building.These include:
� Multiplying health gainsA focus on capacity building will increase thelikelihood that other people and organisationswithin health and other sectors will also be able to promote health.This will multiply health gainsmany times over.
� VisibilityA focus on capacity building increases therecognition given to the diverse efforts ofpractitioners working with others to take on and sustain programs. It gives a ‘name’ to a largeportion of work carried out by practitioners indeveloping effective programs.
� AccountabilityOne of the difficulties of working ‘invisibly’ is thatpractitioners are not readily accountable for thispart of their work. Similarly, managers have lackedclear guidelines for assessing the quality of workpurporting to build capacity for health promotion.
� Responsive systemsCapacity building involves a focus on the processes that support change within and betweenorganisations. It leads to systems which valuecritical problem solving and leadership acrossorganisations. Responsive systems are more likelyto work in partnership to address health challenges.This is in contrast to a ‘silo’ approach whereorganisations may be working on similar problemsin isolation from each other.
� Address inequityThere is increasing evidence that poorer health islinked to the conditions that arise out of inequityand social exclusion. Capacity building is promotedacross government as a mechanism for addressinginequity and building stronger communitiesthrough increasing community and civicparticipation.
� Unifying themeThe language of capacity building is not owned by any one sector and therefore provides a unifying theme under which governmentdepartments and other organisations can worktogether to address inequities.
� Reorientation of health servicesThis is one of the main strategies advanced in the Ottawa Charter for Health Promotion.The message is that along with treating ill health, health services need also to take greaterresponsibility for improving the health of thecommunities they serve.

A Framework for Building Capacity to Improve Health NSW Health8
Health promotion practitioners are typicallyskilled program planners. Developing strategies tobuild capacity is no different to developingstrategies in any well planned program.They aredeveloped to meet particular capacity buildinggoals and objectives and the choice of strategies isinfluenced by:
� the particular context within which the program will apply
� pre-existing capacities to support change
� a practitioner’s role in achieving change
� a practitioner’s sphere of influence to effect change.
Practitioners need to be clear at the outset about their intent in building capacity. Is it to develop aninfrastructure to design and deliver a program? Is it to ensure program sustainability? Is it to enhanceproblem solving capacities? Clarifying the intentmakes it more likely practitioners will developachievable capacity building goals, objectives, andrelevant strategies.
To be successful, it is recommended that the strategiesspan the three key action areas of organisationaldevelopment, workforce development, and resourceallocation. It is also recommended that the strategieswork at a number of different levels, such as withservice providers, their managers and programpartners.
In addition, strategies may need to be developed toenhance the leadership and partnerships available to a program. In particular, a practitioner will need to identify:
� the level of leadership and range of leadershipqualities already in existence within an organisation and among team members
� the quality and range of partnerships that are in existence or can potentially be developed tosupport a program.
The following pages provide a short description of each of the components of the capacity buildingframework and suggests strategies for building capacity within each of them.
Strategies for building capacity3

NSW Health A Framework for Building Capacity to Improve Health 9
Capacity building framework key action areas
� Develop infrastructure
� Enhance program sustainability
� Foster problem solving capablities
Organisational Development
� Policies and procedures
� Strategic directions
� Organisational structures
� Management support
� Recognition and reward systems
� Information systems
� QI systems
� Informal culture
Workforce Development
� Workforce learning
� External courses
� Professional developmentopportunities
� Undergraduate andPost Graduate degrees
� Professional support andsupervision
� Performance management systems
Resource Allocation
� Financial resources
� Human resources
� Access to information
� Specialist advice
� Decision making tools and models
� Administrative support
� Physical resources
Leadership
� Interpersonal skills
� Technical skills
� Personal qualities
� Strategic visioning
� Systems thinking
� Visioning the future
� Organisational management
Partnerships
� Shared goals
� Realtionships
� Planning
� Implementation
� Evaluation
� Sustained outcomes

A Framework for Building Capacity to Improve Health NSW Health10
Organisational developmentThe practitioner who understands principles oforganisational change and who has tools and skills for analysing and facilitating such change will be more successful than his or her counterpart who does not possess such knowledge
22.
Organisational development refers to processes thatensure that the structures, systems, policies, proceduresand practices of an organisation reflect its purpose,role, values and objectives and ensure that change ismanaged effectively.
6An organisation that is more
likely to take up new ways of working in order torespond to changes in strategic directions is one that is often described as a learning organisation.
Senge suggests that learning organisations are places wherepeople continually expand their capacity to create the resultsthey truly desire, where new and expansive patterns ofthinking are nurtured, where collective aspiration is set free,and where people are continually learning how to learntogether.
23
Building the capacity of an organisation to improvehealth is a complex task. No single theory is sufficientfor explaining how and why organisations change.Health promotion draws on theories such as Systemstheory,
24Organisational Change theory,
22and Domain
theory25
to inform understanding about organisationaldevelopment.
Auer and Rippon propose a hierarchy of issues thatneed to be considered in progressing change.
26
They proceed in the following order:
1. Environmental context (what are the externalfactors impacting on the organisations ability tocontribute to the program)
2. Goals (what you want to achieve, with and for whom)
3. Roles (whose job is what to enable you to achieve your goals)
4. Organisational structures, systems andprocedures (the way people are supported to fulfil their roles)
5. Relationships (peoples ability to get along andrespect each other)
Some other factors influencing the choice oforganisational development strategies include:
� Change often progresses in stages: awareness,adoption, implementation and institutionalisationof change.
25
� The level of change can be from incremental,which may only involve fine tuning, through to transformational change which may involve a major restructure.
� Different strategies will require different styles of leading to support integration of the programinto the organisation: collaborative, consultative,directive, and coercive.
25
� Organisations are often divided informally andformally across domains:
24Policy (strategic and
policy directions), Management (achievement ofeconomic and organisational targets) and Service(professional and service groupings). Each domainis dominated by different interests and ethics.Managing processes between domains may requireconflict resolution whilst managing processeswithin domains may require consensus building.

NSW Health A Framework for Building Capacity to Improve Health 11
Examples of organisational development strategies
Elements Strategies
Policies and strategic � Identify and enhance opportunities to incorporate health promotion action and
plans population health approaches into core business of the service or organisation.
� Develop policies that ensure an appropriate proportion of funds are allocated to support
health promotion action.
Organisational � Establish health promotion positions within executive structures.
management structures � Incorporate health promotion action into performance agreements and job descriptions
at all levels of the service / organisation.
� Monitor work practices to ensure appropriate time is allocated to health
promotion action.
Management support � Develop systems to support service and organisational commitment to
and commitment health promotion.
� Develop mainstream line management positions and accountabilities for health
promotion within the organisation.
� Involve senior managers in steering committees for health promotion projects.
Recognition and � Acknowledge achievements, develop formal feedback and acknowledgment systems
reward systems for those undertaking health promotion work. Integrate health promotion award systems
into mainstream health service award schemes.
Information systems – � Develop systems that accurately identify the amount and type of health promotion action
monitoring and evaluation undertaken by staff.
� Develop / utilise appropriate evaluation strategies.
� Incorporate health promotion into staff appraisal processes.
Quality Improvement � Use available best practice tools for health promotion work (eg. Program Management
systems Guidelines, Competency Based Standards for health promotion action, Quality
Management Service and EQUIP standards, Indicators to Help with Capacity Building in
Health Promotion).
Informal organisational � Seek to encourage attitudes which support health promotion action.
culture

A Framework for Building Capacity to Improve Health NSW Health12
Workforce developmentWorkforce development refers to a process initiatedwithin organisations and communities, in response tothe identified strategic priorities of the system, to helpensure that the people working within these systemshave the abilities and commitment to contribute toorganisational and community goals.Workforce refersto both the paid and unpaid workforce withinorganisations and communities.
Workforce learning can be achieved in three ways:5
1. incidental learning where the learning appears tobe by ‘accident’ and people are not aware that they are learning. For example, in casualconversations or when a person is engaged inactivities such as attending the launch of a health promotion program or product.
2. informal learning where the learner is aware ofbeing engaged in the learning process.There arethree types of informal learning activities:
� Proactivity, such as encouraging people to take on new responsibilities
� Creativity, such as encouraging people to break out of old patterns of thinking
� Reflectivity, which is learning from reframing a problem or issue and looking at new solutions which may be superior to the ones initially tried by the learner.
3. formal learning strategies where the learner ortheir workplace has identified learning or trainingneeds and develops strategies to meet these. Forexample mentoring schemes, training programs orpost graduate university courses.
Workforce development strategies represent animportant component of building the capacity of an organisation or community. However whendeveloped in isolation from other capacity buildingstrategies, they are unlikely to bring about effectiveand sustainable changes in work practices.
Examples of how strategies might be linked are:
� Engage managers in decision making about healthpromotion priorities and integration of healthpromotion targets into organisational planningdocuments
� Engage managers in monitoring and evaluating thehealth promotion practice of their staff by makingmanagers accountable for seeding grant budgetsand targets
� Ensure any training is competency based27
and linktraining with work place performance review andprojects supervised by the worker’s line manager
� Target two or more levels of a service ororganisation. For example, the professionaldevelopment of primary health nurses could belinked with programs for Nursing Unit Managersand Directors of Community Health to ensure thatthe skills and knowledge acquired by the workers issupported and applied within the workplace
� Take advantage of existing or emergingopportunities. For example, acquiring project fundsfor priority health issues or campaigns providesopportunity for workers to apply health promotionskills and knowledge to contemporary issues.

NSW Health A Framework for Building Capacity to Improve Health 13
Examples of workforce development strategies
Elements Strategies
On the job learning including � Provide a range of opportunities for people across the health system
incidental and informal to learn about health promotion, including:
learning opportunities � Health promotion committees
� Health promotion seeding grants project
� Scholarships, traineeships or mentoring programs
� Secondments and job rotations
� Planning guides to support self directed learning
� Participant implementation and management of projects
� Information sharing initiatives
Course development � Incorporate competency based standards into courses for health professionals.
Professional development � Disseminate information about, and support graduate and post graduate
opportunities / continuing studies relevant to health promotion
Education/undergraduate � Where appropriate support incorporation of health promotion into
and post graduate studies graduate and post graduate degrees.
� Develop skills-based courses including:
� Core skills courses
� Conferences
� Workshops
� Seminars
� ‘In service’ programs on specific health issues
Professional support and � Establish formal supervision or support arrangements for health promotion work.
supervision systems This may be provided individually or in groups and provided internally or externally.
� Establish peer support systems, buddy systems or networks for people working on
similar issues.
� Provide access to specialist advice and support through networks and consultancies.
Performance management � Incorporate health promotion work into regular performance appraisal or performance
systems management systems.
� Develop specific performance management guidelines to be used by team leaders or
coordinators in other parts of the health system for health promotion work conducted
by their workers.
� Utilise Indicators to Help with Capacity Building in Health Promotion as a tool to assist
in performance review

A Framework for Building Capacity to Improve Health NSW Health14
Resource allocationResource allocation is an economic process, not just aplanning one. Economics is primarily concerned withthe efficiency of resource allocation.
28It requires
technical efficiency to minimise the use of availableresources (which could be used elsewhere), andallocative efficiency to ensure the mix of goods andresources yields the greatest benefit to society.
‘Resources’ includes those things needed to support a program.This includes people, physical space,administrative support, planning tools, and financialsupport. It can also include commitment of ‘in kind’allocations from inter-organisational groups orpartners.
Some of the questions that may be considered indeciding whether resources will be made available to support a program are:
� Will the program create an on-going demand forresources beyond the current allocation, and if so,does this fit with the organisation’s goals?
� If the organisation invests in this program,what will it de-invest in to free up resources?
� Will the returns on this investment be short,medium or long term?
� Who will benefit from this investment?
� Is there strong organisational commitment to the program?
� Are the program goals and objectives realistic and achievable?
� Is evaluation clearly defined?
� Is it realistic to expect staff to pick up thisprogram?
� What mechanisms and structures can be put in place to integrate the program into routinework practice?
The availability and sustainability of resources is often a crucial point in whether a program will bedeveloped or maintained. In research by SouthEastern Sydney Area Health Service to evaluate theirSeeding Grant program, researchers were consistentlytold that a major reason for seeking a seeding grantwas to access financial resources. In addition, thedriver for some early Area Health Service capacitybuilding approaches was a scarcity of resources.For example, one of the reasons the Wentworth AreaHealth Promotion Service sought to engage thebroader health system in health promotion, was toincrease the allocation of mainstream health serviceresources towards health promotion.
Deeble27
describes a range of techniques that mayassist in resource allocation decision making.Theseare: cost-benefit analysis; cost-effectiveness analysis;cost-utility analysis; burden of disease and capacity tobenefit; program budgeting marginal analysis (PBMA);purchaser-provider contracting; and health benefitgrouping/ disease based economic modelling.
A workshop auspiced by the National Public HealthPartnership identified there needed to be a nationalapproach to exploring how best to use these tools,how public health could influence broader strategicdecision making on resource allocation and the needfor better understanding across the public health fieldon economic decision-making principles andmethods.

NSW Health A Framework for Building Capacity to Improve Health 15
Examples of strategies to enhance resource allocation
Elements Strategies
Financial resources � Lobbying for an appropriate proportion of service or organisation’s budget to be
allocated to health promotion action.
� Obtaining short and long term funding for special projects.
� Develop a seeding grant program.
� Actively disseminate information about funding opportunities from health and other
sectors (eg RTA – Bikesafe) to other organisations so that they might become engaged
and interested in health promotion.
Human resources � Establishment of ‘core’ health promotion positions to support program
development � Lobbying for a fixed percentage of worker’s time to be devoted to health
promotion action.
� Developing opportunities for others outside the health system to do health promotion.
� Build a base of advocates for health promotion within health and other sectors and in
particular, at senior management levels
Information � Ensuring availability and use of information (eg. health status, risk factors, national goals
and targets, literature reviews, information about effective practice) to support health
promotion action.
� Negotiate for health promotion material and access to data bases be available through
health service and other libraries and share this information with program partners.
Specialist advice � Ensuring access to expertise when required (eg research and evaluation, planning, media
and marketing, workforce development).
� Provide ‘no-cost’ or ‘low-cost’ access to health promotion skills development courses for
potential program partners in the community and other sectors.
Decision making tools � Utilise best practice models, guidelines and/or standards for health promotion action
and models (eg Competency Based Standards, Program Management Guidelines, Quality Management
Service standards, Program Budgeting Marginal Analysis (PBMA) tools).
Administrative and � Ensuring the availability of clerical or administrative support, equipment, office and
physical resources meeting spaces.

A Framework for Building Capacity to Improve Health NSW Health16
LeadershipLeadership is a function of training, experience andpersonality.Within a capacity building approachpractitioners are seeking to foster the characteristics of leadership within programs and across organisations,by developing and building leadership qualities inthemselves and others.
Leaders are people who are systems thinkers andfuture orientated.They are ready to critically analysetheir work and are people who
30:
� Search out opportunities to change and grow,and experiment with leadership;
� Enable others to act by giving power away,providing choice, developing competence, assigningcritical tasks, and offering visible support
� Set example by behaving in ways that are consistent with shared values
� Engage, mobilise, inspire and team with other to make thing happen
� 'Encourage the Heart' by recognising individualcontributions to the success of every project andcelebrating team accomplishments regularly.
Leaders recognise the need for ‘adaptive work’ toprecede change and are able to ‘stage-manage tension’and ‘create a holding environment’ until those they areworking with realise what needs to change
31. Senge
22
has described leaders in learning organisations as:
� DesignersLittle credit goes to the designer, and their work is often behind the scenes and invisible. ‘The consequences that appear today are the result of workdone in the past’. Leaders see how the parts fittogether to perform as a whole and recognise theconnections between programs, systems and thebroader environment.
� StewardsLeaders have a sense of the larger purpose of theirprogram and are willing to craft the program inresponse to the needs and views of others so thatthe purpose and vision of the program are ownedmore broadly.
� TeachersLeaders foster learning for everyone and remaincommitted to the truth.They have a capacity tosee current reality and do not persist in seeingeverything as ‘fine’ simply to avoid uneasiness.
One aspect of leadership that is familiar to manyhealth promotion practitioners is the notion of‘managing up’.This involves the development ofstrategies to engage managers in decision makingprocesses about health promotion, and to recognisesources of authority (our own as well as others) and to work with these.
Rather than identifying leadership as a position ofauthority or a person with certain personality traits,Senge
22believes it is more meaningful to identify
leadership as an art. Leadership needs to be apparent at every level of a program, not merely at the top.
Health promotion practitioners use their personalqualities as leaders as resources that are applied invarious settings to build leadership in others.

NSW Health A Framework for Building Capacity to Improve Health 17
Examples of strategies to build leadership30,32
Elements Strategies
Personal growth � Identify and work with mentorsand learning
� Utilise opportunities to develop and test new skills eg. step forward to participate in and chair committees
� Foster a leadership learning team
� Seek and respond to feedback about your leadership skills
Visioning the future � Have your own personal vision
� Understand health promotion needs and issues
� Identify emerging trends
� Balance the tension between a focus on results and current realities
� Continuously test assumptions
Systems and � Develop planning skills in yourself and others strategic thinking
� Be aware of the complexity of relationships within health and between the health systemand other sectors.
� Contribute effectively to the organisations strategic plan
� Reflexivity – see yourself within the bigger picture
� Strategically manage resources
Creative collaboration � Promote an environment of creativity, innovation, performance reflection and lateral solutions.
� Form and use partnerships
� Build visions through consultation and collaboration
� Use opportunities to integrate strategies between health and other sectors
Communication skills � Demonstrate actions that motivate and inspire others
� Communicate information effectively and articulate outcomes in ways that are meaningful to others
� Value diversity
� Provide opportunities for reflection and analysis
Political and social � Be aware of the broader political and social context
change strategies � Become familiar with the policies and processes that will impact on your work
� Use policy development processes to influence change
� Be prepared to articulate health promotion priorities
Team learning � Tap the potential for many minds to be more intelligent than one mind, foster dialogue and discussion
� Be conscious of other team members – develop ‘operational trust’ and operate as colleagues
� Foster ‘learning team’ approaches in other teams
� Make time to practice team learning
� Celebrate team accomplishments regularly

A Framework for Building Capacity to Improve Health NSW Health18
PartnershipsThe development of effective partnerships to addresshealth problems is important because many of thedeterminants of health are outside the realm of health services.
The establishment of the National Public HealthPartnership
33(NPHP) is testament to Commonwealth
and State commitment to the importance ofpartnership approaches.Work for the NPHP hasidentified that there are two main types ofpartnerships:
1. Strategic partnerships in which systems engage with systems
2. Local or community partnerships that focus on people.
The opportunity to work collaboratively with otherorganisations (or sectors) is often missed whenorganisations do not have the capacity to initiate andsustain involvement. Building capacity requires actionfrom within organisations as well as between them.Health workers who know how to motivate theirown organisation have a powerful means for effectingchange.
Enabling behaviours by organisations include:
� A clear written and stated focus on partnerships,that they are important, and that this is the normal means by which outcomes are achieved in public health
� Modelling of the desired behaviours by leaderswithin the organisation so that working inpartnership becomes part of the culture.
The terms applied to partnerships are varied and seemto be interchangeable. Bush
8describes the various
types as:
� Joint venturesThe association of people, natural or corporate,who agree by contract to engage in some commonundertaking for joint profit by combining theirrespective resources
� CollaborationShared planning and/or delivery of work acrossdifferent organisations, involving differentprofessional traditions and skills
� AlliancesCollaboration between two or more parties topursue agreed goals
� Intersectoral collaborationActivities by part or parts of the health sectorwhich involve a direct relationship or partnershipwith another sector and which involve jointplanning or action on a health related issue, andactions taken outside of the health sector, generallywith the health sector, with the explicit intentionof improving individual and community health
� CoalitionsAlliances among different sectors, organisations orconstituencies for a common purpose
� PartnershipsCapitalise on each organisations unique strengths,to work together to achieve shared or related goals that neither could achieve as well by working alone.
NSW Health A Framework for Building Capacity to Improve Health 19
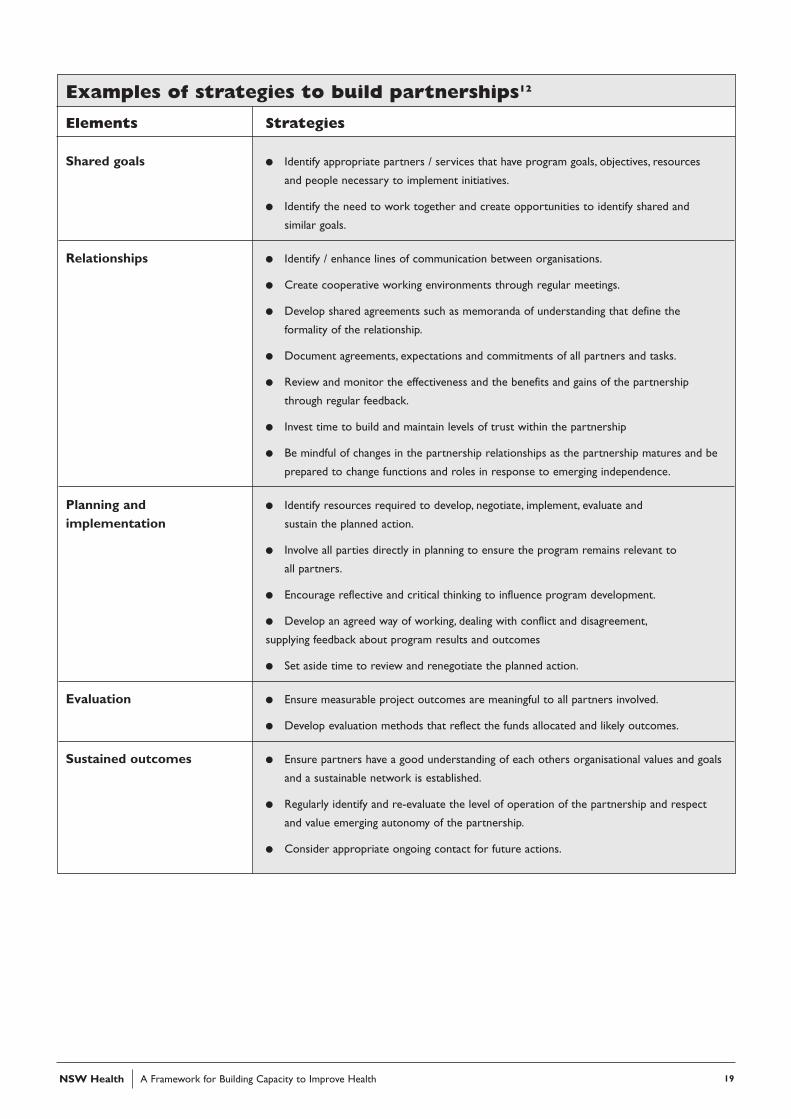
Examples of strategies to build partnerships12
Elements Strategies
Shared goals � Identify appropriate partners / services that have program goals, objectives, resources
and people necessary to implement initiatives.
� Identify the need to work together and create opportunities to identify shared and
similar goals.
Relationships � Identify / enhance lines of communication between organisations.
� Create cooperative working environments through regular meetings.
� Develop shared agreements such as memoranda of understanding that define the
formality of the relationship.
� Document agreements, expectations and commitments of all partners and tasks.
� Review and monitor the effectiveness and the benefits and gains of the partnership
through regular feedback.
� Invest time to build and maintain levels of trust within the partnership
� Be mindful of changes in the partnership relationships as the partnership matures and be
prepared to change functions and roles in response to emerging independence.
Planning and � Identify resources required to develop, negotiate, implement, evaluate and
implementation sustain the planned action.
� Involve all parties directly in planning to ensure the program remains relevant to
all partners.
� Encourage reflective and critical thinking to influence program development.
� Develop an agreed way of working, dealing with conflict and disagreement,
supplying feedback about program results and outcomes
� Set aside time to review and renegotiate the planned action.
Evaluation � Ensure measurable project outcomes are meaningful to all partners involved.
� Develop evaluation methods that reflect the funds allocated and likely outcomes.
Sustained outcomes � Ensure partners have a good understanding of each others organisational values and goals
and a sustainable network is established.
� Regularly identify and re-evaluate the level of operation of the partnership and respect
and value emerging autonomy of the partnership.
� Consider appropriate ongoing contact for future actions.

A Framework for Building Capacity to Improve Health NSW Health20
Mechanisms to successfully evaluate and monitor capacitybuilding efforts are still being explored.A key tool tosupport evaluation are the checklists developed by Hawe,King and Noort which are described and presentedwithin the project report, Indicators to Help with CapacityBuilding in Health Promotion
5.Table 1 presents a summary
of the checklists and their application.
A research project to support dissemination intopractice of the checklists and gather stories of practiceis currently being undertaken by NSW Health.Progress information about the use of the indicatorsand common questions from the field will be availableon a NSW Health, Health Promotion ‘CapacityBuilding’ web page www.health.nsw. gov.au.
Monitoring and evaluatingpractice4
Table 1 Capacity Building Indicator Checklists
Scenario Applications
1. Assessing the strength of a coalition Use this to assess how well an inter organisational coalition is functioning or to set
objectives or tasks in relation to coalition planning.
2. Assessing opportunities to promote Use this for situations where the aim is to promote invisible skills transfer (ie not
incidental learning among other pertaining to formal training programs). For gaining health promotion skills
health workers unknowingly or ‘by accident’
3. Assessing opportunities to promote Use this for situations where the aim is to promote invisible skills transfer (ie not
informal learning among other pertaining to formal training programs).To encourage others to be more engaged
health workers in ‘on the job’ health promotion skills development.
4. Assessing if a program is likely Use at the conclusion of a program to assess the presence of program,
to be sustained organisational and community level factors known to be associated with program
uptake and maintenance.
5. Assessing the learning environment Use to assess whether or not the structure and function of a group is optimal for
of a team or project innovation or learning. It is assumed that a dysfunctional unit is unlikely to take on
new roles successfully.
6. Assessing capacity for Same as above but for organisations.
organisational learning
7. Assessing the capacity of a particular Arranges critical factors that may be assessed separately or in combination.
organisation to tackle a health issue Includes an assessment of partnership capacity and program delivery capacity.
8. Assessing the quality of Assesses one component of checklist 7 in more detail.
program planning
9. Assessing community capacity Sorted into predisposing, enabling and reinforcing factors.
to address community issues

NSW Health A Framework for Building Capacity to Improve Health 21
Work by Robert Bush and Allyson Mutch, from theUniversity of Queensland involved the developmentof a Community Capacity Health Development Index(Figure 5).This material is being produced as a manualand the authors propose that the index could be used
in a wide range of research and planning situations.This tool is still in draft form and the authors shouldbe contacted for more information.The audit toolmaps four domains: network partnerships; knowledgetransfer; problem solving; and infrastructure.
Domain 1 Domain 2 Domain 3 Domain 4
Network Partnerships Knowledge Transfer Problem Solving Infrastructure
Levels of Capacity Levels of Capacity Levels of Capacity Levels of Sustainability
1. There is capacity to 1. There is capacity to 1. There is capacity in 1. Policy investments
identify the organisations develop a program that the network to work
and groups to implement meets local needs together to solve
sustain a program problems
2. There is capacity to 2. There is the capacity to 2. There is the capacity to 2. Financial investments
deliver the program transfer knowledge in identify and overcome
through a network of order to implement/ problems/barriers, to
organisations and groups sustain the program implementing/sustaining
within a network within your own
organisation
3. There is a sustainable 3. There is the capacity to 3. There is the capacity to 3. Human investments
network established to integrate a program into sustain flexible problem
maintain and resource the mainstream practices solving over time across
the program through a of the network partners the network
network of partnerships
4. Social investments
Figure 5 Health Development Index by Robert Bush
Structure of the Community Capacity Health Development Index

A Framework for Building Capacity to Improve Health NSW Health22
The Health Promoting Hospitals Project developed acapacity building matrix (Table 2) to assist in mappingresponses from health service managers about healthpromotion and their understanding of healthpromoting organisations.The matrix was also used as a format for the gathering of information in theHealth Promoting Hospitals Awards.
The format appeared to be useful in assisting thejudges in assessing the quality of award submissions.The matrix links the three dimensions of capacitybuilding: infrastructure, program sustainability and problem solving; and the components of thecapacity building framework: organisationaldevelopment (structure), workforce development(skills) and resources.
Some practitioners may find this a useful tool forthinking about and mapping out the breadth of theirwork within a particular program. It can be used tomap strategies or as a way to monitor outcomes. Inreality, it is highly unlikely that any two people wouldfill out the table in quite the same way! In addition,practitioners will find their strategies can fit into anumber of boxes equally well – depending on howyou think about the strategy. None of this isparticularly neat! Its not really important where theindividual strategies fit, its more important to begintrying to capture capacity building information andexploring strategies to continuously enhance capacity,and especially to enhance problem solving capacity.Table 3 provides a worked example of how the matrixmight be used.
FrameworkDimensions
Infrastructure Program sustainability Problem solving
Organisational structures
Skills
Resources
Table 2 Matrix used to map managers responses within the HPH research and as a reporting formatfor the Health Promoting Hospitals Award Scheme submissions.

NSW Health A Framework for Building Capacity to Improve Health 23
Table 3 An example of an audit of capacity building strategies and/or outcomes within a school
Infrastructure Sustainability Problem Solving
Organisational � School supports � Planning for a particular � School community members
development development of health health promoting program involved in the program are
promotion initiatives is integrated into school contributing to identifying
� Health service policy planning processes and addressing health issues in
ensures health workers are � The program reinforces the community that impact
working with schools using and supports Key on the school community, in
whole of school approach Learning Areas partnership with other sectors
� Health Promotion reflected � Clearly identified lines of � Parent participants in the
in school policy documents communication and program report on the
� Good links between the reporting for the program program at P&C and other
school and its community, within the school system school decision making forums
and the health sector.
Workforce � Teachers and others � Health workers and � Parents and teachers
Development working within the school teachers are skilled in involved in the program
community have access to working with whole of reflect on and enhance
health promotion expertise school approach and this skills in working in
� HP tools utilised to support is integrated into staff partnership and problem
effective hp practice performance review solving
� Health workers contribute � Students /staff/ parents
to planning for, and actively contribute to health
support teacher workforce program development,
development program evaluation and reporting
based on school health
priorities
� Skills required to
implement and sustain the
program are developed
Resource � School ensures mandatory � Resources allocated to � School allocates resources
Allocation health education provided support integration of the (usually worker time) to
to students health program into regular support the school in
work practices (eg. admin, contributing to problem
practical support) solving with the community
� Resources allocated and other sectors
to health promotion
contribute to achievement
of existing educational goals

A Framework for Building Capacity to Improve Health NSW Health24
� Argyris, C and Schon, D. Organisational Learning IITheory, Method, and Practice Adison Wesley, USA,1996 - organisational development - how to measure organisational learning, page 174 scoring a conversation page 98 a map of perseverance ofcounterproductive actions; leadership - 256-258 how managers can use their artistic sense and 7 points to make a process of strategy encompassrealisation and intent; partnerships- how defensivecovers must be broken down within organisations and between organisations, research on how toincrease the likelihood of partnerships.
� Bush, R. and Mutch, M Capacity Building for HarmReduction at the District Level: Conceptual Developmentand the Dimensions of Practice, paper presented at theFourth Symposium on Community Action andResearch and the Prevention of Alcohol and OtherDrug Problems. Kettil Brunn Society ThematicMeeting, New Zealand, February 1998 - lists fourfundamental shifts necessary for capacity building and four features of a sustainable health system.
� Compendium of Healthcare Policies- endorses bestpractice guidelines and benchmarking, internet sitehttp://www.achse.org.au/nsw/policy/group3.htm,a guide for organisational development/partnerships is Measuring Up:A Primer for Benchmarking in theAustralian Public Service- Department of Finance,1996 internet site www.finance.gov.au/pubs/pig/benchmk/benchm.htm explains the key concepts,lists 10 factors for greater success De Bono, E The Use of Lateral Thinking, Jonathan Cape, England,1967 - lateral thinking is a process used in capacitybuilding, chance processes lead to major discoveriesand advances and generate new ideas - Chapter 7.It follows from this analysis that an increase inmeetings/interactions between different people/organisations is likely to increase their capacity andtheir ability to promote health.
� Capacity Building Website NSW Health has developeda site to bring together key NSW Healthpublications on capacity building, other usefulcapacity building information, stories of practice,
frequently asked questions, and links to useful sites.The site may be accessed through the NSW Healthsite www.health.nsw.gov.au
� Community Capacity Building and Asset MappingModel internet sitewww.cha.ab.ca/commdev/capmodl.htm Has been developed by the CommunityDevelopment Office of the Capital Heath Regionin Edmonton,Alberta.This model has 6 key stepsand the site is useful for resources and organisationaldevelopment.
� De Bono, E Handbook for the Positive Revolution,Penguin, England, 1991 -organisational development is about people and perception, and creating circles of concern, circles of community, quality, projects and concern pages 90-97, page 119 sources ofpower; workforce development -page 112-115 asimple technique for constructive thinking, sixthinking hats
� De Bono, E. Atlas of Management Thinking, Penguin,Great Britain, 1981 - resources/ leadership -information and symbols for innovative creativethinking
� Deeble, John. Resource Allocation in Public Health:An Economic Approach. A background report onplanning and resource allocation methods ofpotential interest to public health has been producedunder the auspices of the National Public HealthPartnership (NPHP).The report is available on theNPHP websitehttp://hna.ffh.vic.gov.au/nphp/resalloc/index.htm
� Eade, Deborah. Capacity Building.An Approach toPeople-Centred Development. Oxfam 1997.Talks aboutcapacity building from the perspective of aninternational aid organisation but much of thediscuss about what is capacity building is extremelyrelevant to work within the health system.Highlights that capacity building is an approach todevelopment, that will have a positive, or negativeimpact depending on the political, economic andsocial context within which activity occurs. Presents
Useful resources5

NSW Health A Framework for Building Capacity to Improve Health 25
7 models within which Oxfam programs fit.Thesedemonstrate that capacity building projects do notexist as separate entities but exist within broadersystems.
� Edwards, M. and Ewen,A. 360 Degree Feedback,The Powerful New Model for Employee Assessment andPerformance Improvement,ANACOM, 1949 -workforce development and organisationaldevelopment, this book has been re-printed in 1996
� Fitzgerald, C and Kirby, L. Developing LeadersResearch and Applications in Psychological Type andLeadership Development, Integrating Reality and Vision,Mind and Heart, Davies-Black, California, 1997 -leadership - how it can be developed using theMyers-Briggs Type Indicator
� Karpin, David S. Industry Taskforce on Leadershipand Management Skills,AGPS, Canberra ACT,(1995) Enterprising Nation: Renewing Australia’sManagers to meet the challenge of the Asia-PacificCentury: Executive Summary, - organisationaldevelopment - identifies gaps to be bridged for small to medium enterprises to meet world bestpractice, partnerships - suggests study tours;leadership/ workforce development - identifies skills lacking in Australian managers, contrasts oldand new management paradigms with an 11 itemchecklist, describes emerging senior managementprofile, recommends Williamson FoundationLeadership Program, recommends development of core generic management competencies
� Kaplan,Alan Community Development ResourceAssociation, South Africa.This organisation, and in particular Alan Kaplan, its director, come highlyrecommended by Deborah Eade. In her view he is the one person who really challenges her thinkingon capacity building.Although their material iswritten for NGO’s and other organisations indeveloping countries – their thoughts and ideas on capacity building have broad applicability.Theyhave a commitment to sharing information and all their articles are available on their websitehttp://www.cdra.org.za. Capacity Building. Mythor Reality is at http://www.cdra.org.za/ar9495.htm
� Pawson, Ray. and Tilley, Nick. Realistic EvaluationSage, London. 1998
� An accessible, practical text on evaluation writtenwith humour and humility.The source text for the'context + mechanism = outcome' model.A usefulreference since capacity building is so contextdependant. Builds from 'a history of evaluation in28.5 pages' which challenges the foundationalassumptions of the main evaluation theories, andcumulates in a rigorous model of how programsinteract with their environment.
� Quality Management Services. National CommunityHealth Accreditation and Standards Project,A Manual ofStandards for Community Health AustralianGovernment Printing Service, Canberra 1985 -organisational development and resources standards -4,5,6,8,9,10,11; partnerships - standard 4; workforcedevelopment - standards 7, 11
� Raphael, D. How to Carry Out a Community Quality of Life Manual information about this approach isavailable at the internet site www.utoronto.ca/qol
� Reid, E. Keynote Address, Symposium: Power andPartnerships for Health Promotion Leadership,VicHealth, Melbourne,August 1996 - partnerships -necessary conditions for them; leadership - tacticalapproaches, five radical changes required fortransformative health promotion; sustainablity - brief outline of Bruce Parnell’s (of Mc FarlandBurnett Centre for Medical Research) methodologyfor measuring capacity building approach�
� Ruslin, R. Human Resource Management in LibrariesTheory and Practice Neal Schuman, New York, 1991 -leadership - Chapter 3, checklists that could begeneralised for leadership skills, 34 key issues forconsideration in subordinate evaluation; workforcedevelopment - prerequisites for performanceevaluation, list of effective evaluation techniques
� Sacher and Associates, Performance Measures Applied,A Practical Manual to Measure Performance in AustralianCompanies, Sacher and Associates,Australia, 1994 -workforce development by performancemanagement
� Senge, Peter. The Fifth Discipline.The art and practice ofthe learning organisation. Lots of thought provokingideas on leadership and the five aspects of learningorganisations (systems thinking, personal mastery,mental models, building shared vision, and teamlearning).

A Framework for Building Capacity to Improve Health NSW Health26
There are a number of challenges in progressing acapacity building approach.This includes:
� Language The language of capacity building is seen by some asjargonistic, paternalistic and ‘top-down’. It is also alanguage that is readily understood by leaders acrossthe health system. It may provide a mechanism forengaging in debates about community capacity andthe importance of prevention and addressing inequitiesin health.The challenges are to continue questioningthe language and principles that underpin effectivepractice, and increase understanding of each othersdefinitions and approaches to capacity building.
� Silo effectA major unifying theme in government interest incapacity building is the need to get better at workingtogether to enhance capacity within communities. It isunderstood that the ‘silo effect’, where departmentswork in isolation from each other, leads to duplicationof effort and reduced ability to impact oncommunities. Capacity building has the potential tooffer a solution to this problem.
� Policy into practiceThe gathering of stories of practice, identifying futureindicator development and identifying the linksbetween the Framework and the Indicatorsdocuments are all challenges for the capacity buildingfield. NSW Health has developed a fundedDissemination Grants project to support disseminationof the indicators research and gather stories ofpractice.The grants project is actively supportingpractitioners in their research and will identify if thereare areas of capacity building practice that are notbeing captured with the checklists. NSW Health isalso establishing a data base of practitioners using theIndicators and the Framework to increaseunderstanding about how the tools are being used inpractice.
� Evidence of pathways from capacitybuilding to health outcomes.
Evidence of how capacity building contributes tohealth outcome needs further exploration. In addition,application of the Capacity Building Framework andthe Indicators to designated public health priorityissues (eg. tobacco, physical activity, nutrition andinjury prevention) needs to be progressed.The NSWSafe Communities project has recently tendered for anevaluation of the project and this will include the useof the Indicator checklists as one of their sets ofevaluation tools. NSW Health will continue toexplore the potential for using the Indicators morebroadly across the public health field.
Challenges for the future6

1 Fitzgerald R. (1999) Community services: for sale. AccessIssue 3 December 1999
2 Eade D. (1997) Capacity-Building An Approach to People-Centred Development Oxfam Great Britain
3 NSW Health (2000) Capacity Building:Art of the Invisible.A colloquium at Sydney University on 6 March 2000.www.health.nsw.gov.au/public-health/health-promotion(site in development)
4 NSW Health (1997) Capacity Building Framework.NSW Health Department, Sydney
5 Hawe P, King L, Noort M, Jordens C, Lloyd B (2000)Indicators to Help with Capacity Building in HealthPromotion. NSW Health Department, Sydney
6 NSW Health Promoting Hospitals Project (1998)Research with Managers of NSW Health Services re, HealthImprovement in NSW Health Services: a qualitative study.College of Health Service Executives, PO Box 341,North Ryde NSW 1670
7 Bush R, Mutch A. (1997). District Health Development :Capacity Audit (draft document) Centre for PrimaryHealth Care, University of Queensland
8 Bush R, Mutch A (1999) Draft. Capacity Building forharm reduction at the District Level: Conceptual developmentand the Dimensions of Practice. Centre of Primary HealthCare, University of Queensland
9 Hawe P, Noort M, King L, Jordens C. (1997) MultiplyingHealth Gains: the critical role of capacity-building withinhealth promotion programs. Health Policy ;39:29-42
10 Hawe P, King L, Noort M, Gifford S, Lloyd B. (1998)Working invisibly: health workers talk about capacity-buildingin health promotion Health Promotion International13(4):285-195
11 Bush R. (1999) Achievements, experiences and opportunitiesfor the future – capacity building and public health.Presentation at a NSW Health Capacity BuildingForum, Sydney University.
12 Harris E,Wise M, Hawe P, Finlay P, Nutbeam D (1995)Working together: intersectoral action for health AustralianGovernment Publishing Service, Canberra
13 NSW Health (1999) Future Directions in Public HealthNSW. NSW Health Department, Sydney
14 Bossert TJ. Can they get along without us? Sustainability ofdonor-supported health projects in Central America and Africa.Social Science and Medicine 1990Vol 30 No 9 pp1015-1023
15 Robert Fitzgerald (2000) The new agenda for communityservices. Presentation at Capacity Building: Mastering theArt of the Invisible. Sydney University, 6th March 2000www.health.nsw.gov.au/public-health/health-promotion
16 McPeake K. (2000) Capacity building: why its critical toHealth Services. Presentation at Capacity Building:Mastering the Art of the Invisible. Sydney University,6th March 2000 www.health.nsw.gov.au/public-health/health-promotion
17 Pawson R,Tilley N. (1997) Realistic Evaluation. SagePublications, London
18 Kaplan,A (1994/1995) CDRA Annual Report: CapacityBuilding: Myth or Reality? Community DevelopmentResource Association.http://www.cdra.org.za/ar9495.htm 12/11/1999
19 Harris E, Sainsbury P, Nutbeam D. (1999) Perspectives on Health Inequity.Australian Centre forHealth Promotion, Sydney
20 International Union for Health Promotion andEducation (1999) The Evidence of Health PromotionEffectiveness: Shaping Public Health in a New Europe.ECSC-EC-EAEC, Brussels – Luxembourg
21 World Health Organisation. (1986) Ottawa Charter forHealth Promotion. World Health Organisation, Geneva
22 Goodman RM, Steckler A. (1997) Mobilisingorganizations for health Enhancement in Glanz k, Lewis F,Rimer B. Health Behaviour and Health EducationTheory, Research, and Practice Jossey Bass, San Francisco
23 Senge P (1990) The Fifth Discipline:The Art and Practice ofthe Learning Organisation. Random House, Milson's Point
24 Palmer G., and Short S. (1994) Health Care & PublicPolicy: an Australian analysis. MacMillan: South Yarra
25 Ross HS, Mico PR. (1980) Theory and Practice in HealthEducation Mayfield Palo Alto
26 Auer, J (1993) Just Change:The Cost-conscious ManagersToolkit. South Australian Health Commission, SouthAustralian Community Health Association,Commonwealth Dept of Health, Housing, LocalGovernment and Community Services.
27 NSW Health Department (1994) Competency BasedStandards for Health Promotion in NSW SHPN 94-097
28 Deeble J (1999) Resource Allocation in Public Health:AnEconomic Approach. National Public Health Partnership.Melbourne
29 National Public Health Partnership. (1999) ResourceAllocation in Public Health – moving forward. NationalPublic Health Partnership, Melbourne.
30 Kouzes J, Posner B. (1995) The Leadership ChallengeJossey-Bass, San Francisco
31 Heifetz R (1994) Leadership without easy answers BelknapPress at Harvard University Press, Cambridge, Mass
32 Health Strategies Deakin, Centre for Health inDevelopment (1998) Public Health Leadership Developmentin Victoria. Deakin University, Burwood.
References
NSW Health A Framework for Building Capacity to Improve Health 27
7

A Framework for Building Capacity to Improve Health NSW Health28
The National Public Health Partnership. (1999)Progress through Partnerships.http://hna.ffh.vic.gov.au/nphp/ar99/ch1-1.htm25/3/2000
Representatives from these organisations havesupported the revision of the framework.
� CEIDA
� Central Sydney Drug and Alcohol Services
� Northern Sydney Health
� NSW Health: Health Promotion Strategies Unit
� South Western Sydney Area Health Service
� South Eastern Sydney Area Health Service
� Southern Area Health Service
� Sydney University
� Western Sydney Area Health Service
� Wentworth Area Health Service
cknowledgementsA

SHPN: (HP) 990226
01/646 Capacity Cover.qxd 3/28/01 3:44 PM Page 1