a conceptual model of quality of life in schizophrenia: description and preliminary clinical...
TRANSCRIPT

A conceptual model of quality of life inschizophrenia: Description and preliminary clinical validation
Quality of Life Research . Vol 6 . 1997
A. George Awad,* L. N. P. Voruganti and R. J. Heslegrave
Department of Psychiatry, University of Toronto, Toronto, Ontario, Canada (A. George Awad, R. J. Heslegrave); Department of Psychiatry, University of Western Ontario, London, Ontario, Canada (L. N. P. Voruganti)
The utility of quality of life (QOL) as an evaluativetool in clinical psychiatric research and drug trialscould be enhanced by developing appropriateconceptual models of QOL, specific for psychiatricdisorders. In our proposed model, QOL of individualsmaintained on antipsychotic drug therapy for schizo-phrenia, is viewed as the subject’s perception ofthe outcome of an interaction between severity ofpsychotic symptoms, side-effects including subjec-tive responses to antipsychotic drugs, and the levelof psychosocial performance. In order to test thevalidity of the model in clinical setting, we selecteda sample of 62 schizophrenic patients clinically sta-bilized on antipsychotic drug therapy, and measuredtheir subjective QOL and other potentially relevantclinical and psychosocial factors. Standardizedscales including the positive and negative syndromesscale (PANSS), abnormal involuntary movementsscale (AIMS), Hillside Akathisia scale (HAI), and thesocial performance schedule (SPS) were used forthis purpose. Results of a multiple regression analy-sis using subjective quality of life as the outcomevariable, indicated that severity of schizophrenicsymptoms (partial R 2 = 0.32, p < 0.0001) and subjec-tive distress caused by akathisia (partial R 2 = 0.11,p < 0.01) and neuroleptic dysphoria (partial R 2 = 0.06,p < 0.05), accounted for nearly half of the variance,while the contribution from the psychosocial indi-cators was negligible. These results broadly endorsekey aspects of the proposed model, and suggestfurther studies in this direction. These resultssuggest that improvement in patients’ subjectiveexperiences during antipsychotic therapy canenhance patients’ QOL. This conceptual model hasbeen developed with particular focus on the impactof antipsychotic medications on the QOL of personswith schizophrenia. As such, it is more applicable toclinical trials of new antipsychotic medications butmay not be broad enough to be applicable for othersocial or vocational interventions.
Key words: Conceptual models, qual i ty of l i fe,schizophrenia.
Introduction
Quality of life (QOL) has become a popular conceptin health sciences over the past two decades. It hasbeen used as an outcome variable in clinical trials, arequirement for the approval of new medications byregulatory agencies, a promotional tool in marketingdrugs by pharmaceutical firms and a basis of variouspharmacoeconomic evaluations such as cost-utilityanalysis.1–3 There are, however, several conceptualand practical limitations surrounding the use of QOLin the context of drug therapy and clinical trials.4,5
These include the lack of comprehensive models ofQOL specific to major mental disorders, the unavail-ability of appropriate QOL measures sensitive enoughto pick up small changes, and the lack of adequateinformation about the psychometric characteristicsand performance of the available instruments.6
Developing and evaluating appropriate conceptualmodels of QOL, with reference to schizophrenicpopulation is the objective of the present study.
Review of literature
Literature on QOL models, and the determinants ofQOL in schizophrenia has been varied and inconsis-tent. Lehman, using a hierarchical model of QOL,and the quality of life interview (QLI) schedule,identified safety, unemployment, financial issues andfamily and social relations as primary determinantsof QOL.7–10 A similar study conducted in Mississippialso found social relations and finances as maindeterminants of QOL of the chronically mentally ill.11
However, a Canadian study involving patients in a
© 1997 Rapid Science Publishers
Quality of Life Research, 6, pp. 21–26
* To whom correspondence should be addressed atProfessor of Psychiatry & Director, PsychopharmacologyProgram, University of Toronto, Clarke Institute of Psychiatry,250 College Street, Toronto, Ontario, Canada, M5T 1R8.
Quality of Life Research . Vol 6 . 1997 21
day treatment programme identified somewhatdifferent dimensions — number of readmissions inthe previous year, frequency of family contacts, satis-faction with social life, mental health and adulteducation — as the best predictors of QOL.12 Thesestudies were methodologically similar and were basedon a strategy of exploring patients’ living conditionsand identifying objective indicators of QOL. Otherresearchers have focused on subjective–psychologicaldimensions, and used different study approaches andstatistical techniques. One such study conceptualizedQOL as subjective satisfaction derived throughhedonism, achievement and conformity, but notthrough attaining satisfaction with objective needs.13
These studies suggest that the primary dimensionsof QOL differ markedly depending on whetherobjective or subjective criteria is used with relativelyless work being done on the latter.
A new conceptual model of QOL in schizophrenia
To measure QOL, the concept has to be definedoperationally; the principal factors influencing theQOL of the population under study to be established,a conceptual model of QOL specific to the situationand population under study to be developed, and ameasurement strategy based on the model to be usedto choose appropriate rating scales to capture therelevant dimensions of QOL. Such a measure has tobe psychometrically sound and proven to be useful.With these criteria in mind, evaluative studies andoutcome research — adopting a narrowly definedhealth-related quality of life (HRQOL), as opposedto a comprehensive concept of QOL that encompassesbroader issues such as housing, finances or neigh-bourhood facilities — is likely to be more productivein studying the impact of health-related deficits,disabilities, treatments and other interventions.14
Similarly, the varied needs of populations withdifferent disorders also warrant a ‘disease-specific’and a ‘situation-specific’ approach to the QOL assess-ment capable of reflecting their unique circumstances.
Based on these principles, Awad4,6 proposed anintegrative model of QOL, with reference to schizo-phrenic patients receiving antipsychotic drugtherapy. Schizophrenia is a severe and disablingmental disorder that affects approximately 1% of thepopulation; its course is generally chronic with acutepsychotic exacerbations. The illness requires long-term therapy with antipsychotic medications thatfrequently produce a wide range of side-effects thatcan impact negatively on the functional status of theindividual. According to the proposed model, QOL
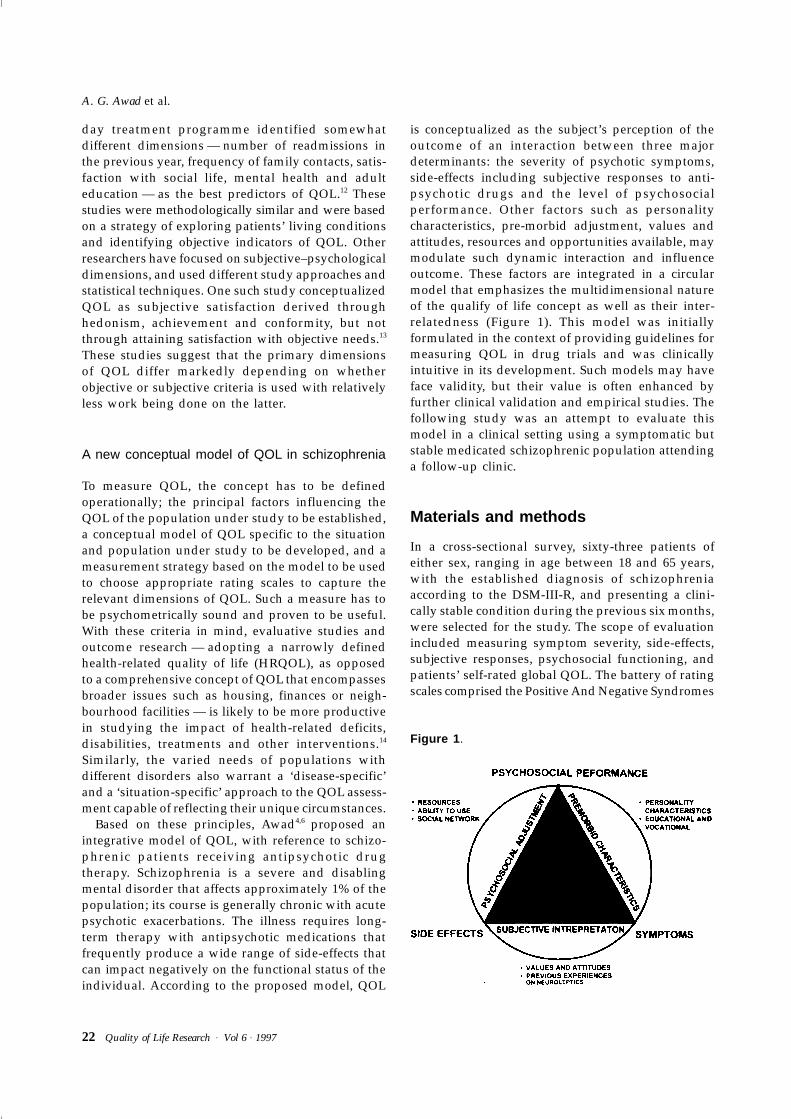
is conceptualized as the subject’s perception of theoutcome of an interaction between three majordeterminants: the severity of psychotic symptoms,side-effects including subjective responses to anti-psychotic drugs and the level of psychosocialperformance. Other factors such as personalitycharacteristics, pre-morbid adjustment, values andattitudes, resources and opportunities available, maymodulate such dynamic interaction and influenceoutcome. These factors are integrated in a circularmodel that emphasizes the multidimensional natureof the qualify of life concept as well as their inter-relatedness (Figure 1). This model was initiallyformulated in the context of providing guidelines formeasuring QOL in drug trials and was clinicallyintuitive in its development. Such models may haveface validity, but their value is often enhanced byfurther clinical validation and empirical studies. Thefollowing study was an attempt to evaluate thismodel in a clinical setting using a symptomatic butstable medicated schizophrenic population attendinga follow-up clinic.
Materials and methods
In a cross-sectional survey, sixty-three patients ofeither sex, ranging in age between 18 and 65 years,with the established diagnosis of schizophreniaaccording to the DSM-III-R, and presenting a clini-cally stable condition during the previous six months,were selected for the study. The scope of evaluationincluded measuring symptom severity, side-effects,subjective responses, psychosocial functioning, andpatients’ self-rated global QOL. The battery of ratingscales comprised the Positive And Negative Syndromes
Figure 1 .
A. G. Awad et al.
22 Quality of Life Research . Vol 6 . 1997

Scale (PANSS), Hillside Akathisia Scale (HAS), Ab-normal Involuntary Movements Scale (AIMS), DrugAttitude Inventory (DAI), Social Performance Schedule(SPS), Global scale of Adaptive Functioning (GAF),and Gurin’s global QOL question. A brief descriptionof these scales follows:
Positive and Negative Syndromes Scale (PANSS): ThePANSS is a semi-structured rating scale for measuringclinical symptoms and related aspects such ascognitive, affective and social functioning in schizo-phrenia.15 It has 30 items of which seven itemsrepresent the positive symptoms, another seven itemsare related to the negative symptoms and the remain-ing 16 items cover related aspects of generalpsychopathology and functioning.
Hillside Akathisia Scale: This scale was designed tocharacterize the frequency and magnitude of observedakathisia phenomena, and observe changes in akathisiaover time or in response to pharmacotherapy withina subject.16 The HAS rates two subjective items, andthree objective items, in three different body posi-tions. All the items are rated on an interval scale of0–4 (0 being absence of akathisia, and 4 indicative ofa severe degree of akathisia) yielding a total score.
Abnormal Involuntary Movements Scale (AIMS): TheAIMS is a scale specifically designed to measure thepresence and severity of abnormal movements inseven areas of the body: muscles of facial expression,lips and perioral area, jaw, tongue, upper extremities,lower extremities and trunk. Ratings of tremor arespecifically excluded. A 5-point rating scale is usedto rate the movements in each body area, and overallseverity of abnormal movements, incapacitation dueto abnormal movements and patients awareness anddistress due to abnormal movements, are also rated17
yielding a total score.
Drug Attitude Inventory (DAI): The DAI is self-reportscale developed to measure subjective responses andattitudes of chronic schizophrenic patients towardsmaintenance antipsychotic treatment.18 The originallonger version of the scale contains 30 items coveringseven categories of patients’ attitudes: subjective posi-tive, subjective negative, health and illness, physician,control, prevention and harm. A shorter version ofthe scale containing 10 key items from the subjectivecategories was developed subsequently. The items arepresented as self-report statements with which thepatient agrees or disagrees. The scale is concise; itspsychometric properties are well-established, con-firming its high internal consistency (r = 0.93, p < 0.001),
test–retest reliability (r = 0.82), and fair degree ofdiscriminant, predictive and concurrent (r = 0.76)validities.19
Social Performance Schedule (SPS): The SPS is an inter-viewer administered, semi-structured scale, designedto measure patients’ performance in eight types ofsocially acceptable roles: household management,employment, management of money, child care,intimate relationship with spouse or close friend,other relationships, social presentation of self andcoping with emergencies.20
Global Scale of Adaptive Functioning: The GAF is arevised version of an earlier Global Assessment Scale(GAS), which has been formally incorporated as theAxis V into the American Psychiatric Association’sDSM-III-R and DSM-IV. It is a single rating scale forevaluating the overall functioning of a subject duringa specified time period on a continuum frompsychological or psychiatric sickness to health.21 Thescale values range from 1, which represents thehypothetically sickest individual, to 90 which repre-sents the hypothetically healthiest.
Gurin’s global quality of life question: This is a singlequestion aimed at eliciting a global subjectiveimpression of an individual about his/her QOL, andanswered on a five-point Likert format from ‘verygood’, ‘good’, ‘fair ’, ‘poor ’ and ‘very poor ’, ornumerically scored from 1–5.22
In the analysis, means and standard deviationswere calculated for scores obtained from all the scales,and attempts were made to identify the predictorsof subjective QOL through correlational and regres-sion analysis. Pearson’s correlation coefficients werecomputed to examine the association betweensubjective global QOL (scores obtained on Gurin’squestion), and other clinical and psychosocial vari-ables (PANSS, AIMS, HAS, DAI and SPS scores). Also,a multiple regression analysis was conducted withsubjective global QOL as the outcome variable, andscores from other clinical and psychosocial indicesas predictor variables.
Results
The sociodemographic profile and clinical charac-teristics are presented in Tables 1 and 2. The sampleconsisted of a predominantly male, Caucasian, young-adult, unemployed, unmarried patient population whotended to live alone. Their illness onset was in theirearly 20s, duration was about nine years, all were
Conceptual model of quality of life
Quality of Life Research . Vol 6 . 1997 23
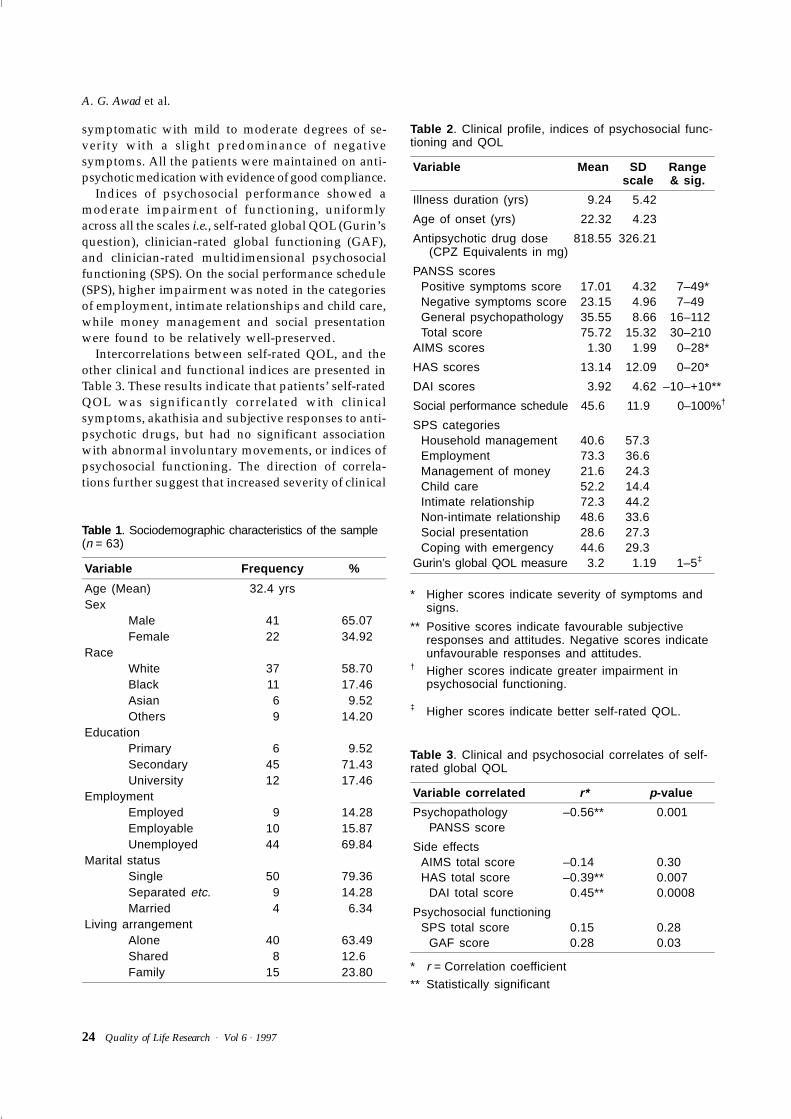
symptomatic with mild to moderate degrees of se-verity with a slight predominance of negativesymptoms. All the patients were maintained on anti-psychotic medication with evidence of good compliance.
Indices of psychosocial performance showed amoderate impairment of functioning, uniformlyacross all the scales i.e., self-rated global QOL (Gurin’squestion), clinician-rated global functioning (GAF),and clinician-rated multidimensional psychosocialfunctioning (SPS). On the social performance schedule(SPS), higher impairment was noted in the categoriesof employment, intimate relationships and child care,while money management and social presentationwere found to be relatively well-preserved.
Intercorrelations between self-rated QOL, and theother clinical and functional indices are presented inTable 3. These results indicate that patients’ self-ratedQOL was significantly correlated with clinicalsymptoms, akathisia and subjective responses to anti-psychotic drugs, but had no significant associationwith abnormal involuntary movements, or indices ofpsychosocial functioning. The direction of correla-tions further suggest that increased severity of clinical
Table 1 . Sociodemographic characteristics of the sample(n = 63)
Variable Frequency %
Age (Mean) 32.4 yrsSex
Male 41 65.07Female 22 34.92
RaceWhite 37 58.70Black 11 17.46Asian 6 9.52Others 9 14.20
EducationPrimary 6 9.52Secondary 45 71.43University 12 17.46
EmploymentEmployed 9 14.28Employable 10 15.87Unemployed 44 69.84
Marital statusSingle 50 79.36Separated etc. 9 14.28Married 4 6.34
Living arrangementAlone 40 63.49Shared 8 12.6Family 15 23.80
Table 2 . Clinical profile, indices of psychosocial func-tioning and QOL
Variable Mean SDscale
Range& sig.
Illness duration (yrs) 9.24 5.42
Age of onset (yrs) 22.32 4.23
Antipsychotic drug dose(CPZ Equivalents in mg)
818.55 326.21
PANSS scoresPositive symptoms score 17.01 4.32 7–49*Negative symptoms score 23.15 4.96 7–49General psychopathology 35.55 8.66 16–112Total score 75.72 15.32 30–210
AIMS scores 1.30 1.99 0–28*
HAS scores 13.14 12.09 0–20*
DAI scores 3.92 4.62 –10–+10**
Social performance schedule 45.6 11.9 0–100%†
SPS categoriesHousehold management 40.6 57.3Employment 73.3 36.6Management of money 21.6 24.3Child care 52.2 14.4Intimate relationship 72.3 44.2Non-intimate relationship 48.6 33.6Social presentation 28.6 27.3Coping with emergency 44.6 29.3
Gurin’s global QOL measure 3.2 1.19 1–5‡
* Higher scores indicate severity of symptoms and signs.
** Positive scores indicate favourable subjective responses and attitudes. Negative scores indicate unfavourable responses and attitudes.
† Higher scores indicate greater impairment in psychosocial functioning.
‡ Higher scores indicate better self-rated QOL.
Table 3 . Clinical and psychosocial correlates of self-rated global QOL
Variable correlated r* p -value
Psychopathology –0.56** 0.001PANSS score
Side effectsAIMS total score –0.14 0.30HAS total score –0.39** 0.007
DAI total score 0.45** 0.0008
Psychosocial functioningSPS total score 0.15 0.28
GAF score 0.28 0.03
* r = Correlation coefficient
** Statistically significant
A. G. Awad et al.
24 Quality of Life Research . Vol 6 . 1997

symptoms, increased severity of akathisia and nega-tive subjective responses towards antipsychotic drugscontribute significantly to lowered QOL.
Results of a multiple regression analysis indicatingthe contribution of various clinical and functionalindices towards the variance (partial R2) in the self-rated QOL scores is presented in Table 4. The scoresobtained from the Positive and Negative SyndromesScale (PANSS), the Drug Attitude Inventory (DAI)and Hillside Akathisia Scale (HAS) accounted for asignificant proportion of the variance on this test,while the contribution from the Social PerformanceSchedule (SPS) and the Global scale of Adaptive Func-tioning (GAF) was negligible. These results indicatethat the severity of psychopathology, side-effects andpatients subjective tolerableness to medicationscontributed significantly to the patients’ subjectiveglobal QOL, while various aspects of psychosocialperformance did not emerge as significant factorsamong this particular clinical population.
Discussion
In this preliminary attempt to validate the proposedmodel of QOL of individuals with schizophrenia,severity of illness and subjective responses to anti-psychotic drugs emerged as the key determinants ofQOL. The subjects included in this study are symp-tomatic but stable psychotic patients, maintained onregular antipsychotic therapy. Such a profile closelyresembles the type of patients seen in outpatientclinics and those who are often included in drugtrials, but may not be representative of a broaderspectrum of schizophrenic population.
Attempts to understand the factors contributing tothe QOL of chronic mental patients has traditionallyemphasized circumstances and standard of living askey issues.23 In recent years, the deficits associatedwith schizophrenia and the limitations of anti-psychotic therapy became the focus of attention.Clinicians and researchers have been attempting toevaluate the patients’ perspective in clinical care anddrug treatment. The distressing nature of the subjec-
tive experiences associated with psychotic symptomshas been elucidated24 and the occurrence of subtleunpleasant side-effects of antipsychotic therapy iswell-recognized.25–27 The unpleasant subjective expe-riences associated with the antipsychotic drug usehave been often implicated in patients’ dissatisfactionwith treatment, poor compliance, drop-outs andfrequent relapses.28–31 In summary, the needs ,expectations and value systems of the severelymentally ill may have been slowly changing, and theissues shaping their QOL needs to be better appre-ciated. The emergence of psychopathology andside-effects in this study as significant determinantsof QOL is also congruent with a growing number ofmore recent observations, that have highlighted thevalue of subjective and intrapsychic factors, asopposed to the contribution of objective or extrinsic,psychosocial issues.32,13 In a recent analysis, Romneyargued that the patient’s QOL is much more influ-enced by symptoms than by social functioning, andchallenges the traditional view that QOL could beimproved regardless of the symptoms.33 Althoughour data surprisingly failed to demonstrate a signifi-cant impact of psychosocial functioning on patients’self-rated QOL, this cannot be interpreted as achallenge to the value of psychosocial interventions.This would be against clinical experiences as well asextensive recent research findings. On the other hand,at least in the population enrolled in this study,severity of symptoms and treatment effects may haveimpacted more on patients’ self-perception of theirQOL and may have overshadowed other aspects oftheir life experiences. This finding underscores whatclinicians already know: adequate control ofsymptoms and side-effects can facilitate psychosocialrehabilitation interventions.
The implications of the study for clinical practiceand research are obvious. Clinicians should becomemore aware of the subjectively distressing nature ofschizophrenia as well as the side-effects of drugtherapy. Efforts should be directed towards effectivecontrol of psychotic symptoms and minimizing theside-effects of antipsychotic drugs, in order toimprove the QOL of schizophrenic patients. Use of
Table 4 . Predictors of self-rated global QOL in schizophrenia (based on multiple regression analysis)
Predictor variable Variance (partial R 2) F test p
Psychopathology (PANSS) 0.24 12.38* 0.001Patient’s subjective responses and attitudes (DAI) 0.11 6.40* 0.01Side-effects (HAS) 0.06 4.03* 0.05Psychosocial functioning, multidimensional (SPS) 0.01 0.81 0.37Psychosocial functioning, global (GAF) 0.01 0.87 0.35
* Statistically significant
Conceptual model of quality of life
Quality of Life Research . Vol 6 . 1997 25

minimal doses of drugs during maintenance phasecan enhance benefits from psychosocial treatmentmethods. It has to be seen whether the developmentof the new atypical antipsychotic medications withtheir improved side-effect profile may contribute toimproved QOL.
For researchers, the immediate challenge is to iden-tify the determinants of QOL and their relativecontribution, and to develop appropriate tools formeasurement. The scope of such evaluation shouldbe broadened especially to include measures ofsubjective responses and self-rated distress. Based onthese principles, the present study illustrates thedevelopment of a rational strategy for evaluatingQOL in clinical trials involving these new anti-psychotic drugs.
References
1. Meltzer HY, Burnett S, Bastani B, et al. Effects of six monthsof clozapine treatment on the quality of life of chronicschizophrenic patients. Hosp Comm Psychiatry 1990; 41:892–897.
2. Awad AG, Voruganti LNP, Heslegrave RJ. Measurementof quality of life in schizophrenia. PharmacoEconomics (inpress)
3. Lancet. Quality of life and clinical trials. Lancet 1995; 346:1–2.
4. Awad AG. Quality of life of schizophrenic patients onmedications and implications for new drug trials. HospComm Psychiatry 1992; 43: 262–265.
5. Awad AG. Methodological and design issues in clinicaltrials of new neuroleptics: an overview. Br J Psychiatry1993; 163(Suppl. 22): 51–57.
6. Awad A. Quality of life issues in medicated schizophrenics:therapeutic and research implications. In: ContemporaryIssues in the Treatment of Schizophrenia. Shariqui CL,Nasrallah H, eds. Washington DC:American PsychiatricPress, 1995.
7. Lehman A, Ward N, Linn L. Chronic mental patients: thequality of life issue. Am J Psychiatry 1982; 139: 1271–1276.
8. Lehman A. The well-being of chronic mental patients:assessing their quality of life. Arch Gen Psychitatry 1983;40: 369–373.
9. Lehman A. The effects of psychiatric symptoms on qualityof life assessments among the chronic mentally ill. EvalProg Plan 1983; 6: 143–151.
10. Lehman A, Possidente S, Hawker F. The quality of life ofchronic patients in a state hospital and in communityresidences. Hosp Comm Psychiatry 1986; 37: 901–907.
11. Sullivan G, Wells K, Leake B. Quality of life of seriouslymentally ill persons in Mississippi. Hosp Comm Psychiatry1991; 42: 752–754.
12. Levitt AJ, Hogan TP, Bucosky CM. Quality of life in chroni-cally mentally ill patients in day treatment. PsychologicalMed 1990; 20: 703–710.
13. Corten P, Mercier C, Pelc I. ‘Subjective quality of life’:clinical model for assessment of rehabilitation treatmentin psychiatry. Soc Psychiatry Psychiatr Epidemiol 1994; 29:178–183.
14. Gill T, Feinstein A. A critical appraisal of the quality oflife measurements. JAMA 1994; 272: 619–626.
15. Kay S, Fiszbein A, Opler L. The Positive and NegativeSyndrome Scale (PANSS) for Schizophrenia. Schiz Bull1987; 13: 261.
16. Fleishhacker WW, Bergmann KJ, Perovich R, et al. TheHillside Akathisia Scale: A new rating instrument for neuro-leptic induced akathisia. Psychopharm Bull 1989; 25: 222–226.
17. Guy W. ECDEU Assessment Manual for Psychopharmacology,Revised 1976. Washington DC: US Department of Health,Education and Welfare, 1976.
18. Hogan TP, Awad AG, Eastwood R. A self-report scalepredictive of drug compliance in schizophrenics: reliabilityand discriminative validity. Psychological Med 1983; 13:177–183.
19. Hogan T, Awad A. Subjective response to neurolepticsand outcome in schizophrenia: A re-examination compar-ing two measures. Psychological Med 1992; 22: 347–352.
20. Wykes T, Stuart E. The measurement of social behaviourin psychiatric patients: an assessment of the reliability andvalidity of the SBS schedule. Br J Psychiatry 1986; 148: 1–11.
21. Endicott J, Spitzer RL, Fleiss JL, et al. The Global AssessmentScale: A procedure for measuring overall severity of psy-chiatric disturbance. Arch Gen Psychiatry 1976; 33: 766–771.
22. Gurin G, Verhoff J, Feld S. Americans View Their MentalHealth. New York, NY: Russel Sage Foundation, 1960.
23. Bachrach L. Deinstitutionalization: An Analytic Review andSociological Perspective. Rockville, MD: National Instituteof Mental Health, 1976.
24. Strauss JS. Subjective experiences of schizophrenia: to-wards a new dynamic psychiatry. Schiz Bull 1987 15: 178–179.
25. Singh MM, Kay SR. Dysphoric response to neuroleptictreatment in schizophrenia: its relationship to autonomicarousal and prognosis. Biolog Psychiatry 1979; 14: 277–294.
26. Van Putten T, May PRA, Marder SR. Subjective responseto thiothixene and chlorpromazine. Psychopharma Bull1980: 16–18.
27. Awad AG, Hogan TP. Early treatment events and predic-tion of response to neuroleptics in schizophrenia. ProgNeuropsychopharma Biolog Psychiatry 1985; 9: 585–588.
28. VanPutten T, May PRA, Marder SR, et al. Subjectiveresponse to antipsychotic drugs. Arch Gen Psychiatry 1981;38: 187–190.
29. Diamond R. Drugs and quality of life: The patient’s pointof view. J Clin Psychiatry 46(5): 29–35.
30. Awad AG. Subjective response to neuroleptics in schizo-phrenia. Schiz Bull 1993; 19: 609–617.
31. Awad AG, Hogan TP, Voruganti LNP, Heslegrave RJ.Patients’ experiences on antipsychotic medications:implications for outcome and quality of life. Int ClinPsyhcopharm 1995; 10(Suppl 3): 123–132
32. Brekke JS, Levin S, Wolkon GH et al. Psychosocial func-tioning and subjective experience in schizophrenia. SchizBull 1993; 19: 599–608.
33. Romney DM. Psychosocial functioning and subjectiveexperience in schizophrenia: A reanalysis. Schiz Bull 1995;21: 405–410.
(Received 2 April 1996;accepted 11 July 1996)
A. G. Awad et al.
26 Quality of Life Research . Vol 6 . 1997