a conceptual model for detecting interactions among medical recommendations...
TRANSCRIPT

A Conceptual Model for Detecting Interactionsamong Medical Recommendations in
Clinical Guidelines
A case-study on multimorbidity
Veruska Zamborlini12 ?, Rinke Hoekstra13, Marcos da Silveira2, CedricPruski2, Annette ten Teije1, and Frank van Harmelen1
1 Dept. of Computer Science, VU University Amsterdam, The Netherlands{v.carrettazamborlini, rinke.hoekstra, a.c.m.ten.teije,
f.a.h.van.harmelen}@vu.nl2 Public Research Centre Henri Tudor, Luxembourg{marcos.dasilveira, cedric.pruski}@tudor.lu
3 Faculty of Law, University of Amsterdam, The Netherlands
Abstract. Representation of clinical knowledge is still an open researchtopic. In particular, classical languages designed for representing clini-cal guidelines, which were meant for producing diagnostic and treatmentplans, present limitations such as for re-using, combining, and reasoningover existing knowledge. In this paper, we address such limitations byproposing an extension of the TMR conceptual model to represent clini-cal guidelines that allows re-using and combining knowledge from severalguidelines to be applied to patients with multimorbidities. We providemeans to (semi)automatically detect interactions among recommenda-tions that require some attention from experts, such as recommendingmore than once the same drug. We evaluate the model by applying it toa realistic case study involving 3 diseases (Osteoarthritis, Hypertensionand Diabetes) and compare the results with two other existing methods.
Keywords: Clinical knowledge representation, Reasoning, Combiningmedical guidelines, Multimorbidity
1 Introduction
Clinical guidelines (CGs) are documents that support health care professionals inpatient diagnosis and treatment plan design. Computer Interpretable Guidelines(CIGs) are formal representations of CGs, intended to increase flexibility overpaper based CGs, to minimize errors and to generalize the use of guidelines acrossinstitutions. CIGs are expressed in dedicated languages such as GLIF [1], Asbru[5] or PROforma [7]. They are mainly designed to promote the execution of
? Funded by CNPq (Brazilian National Council for Scientific and Technological De-velopment) within the program Science without Borders.

CIGs, i.e. to apply them to patient data for supporting diagnostics or treatmentplans.
Unfortunately, these CIG languages are not flexible enough to support caseswhere (parts of) multiple guidelines need to be combined to handle situationswhere a patient suffers from several diseases, called multimorbidity. For instance,Aspirin is recommended as anti-platelets to patients diagnosed with TransientIschemic Attack. On the other hand, Aspirin is not recommended (admonished)for Duodenal Ulcer patients to avoid increasing the risk of bleeding. ExistingCIG-based approaches CIGs fail to detect such conflicts automatically [3, 4].
In previous work [8], we introduced a conceptual model (TMR - Transition-based Medical Recommendations) that increases the reasoning capabilities ofCIGs. The model relies on a refined definition of the notions of recommendation,transition, care action type and situation type. TMR paves the way towards anautomatic identification of potential conflicts or interactions that can happenwhen merging guidelines, but it requires additional features to fully automatizethe identification process. In this paper we provide an extension of the TMRmodel, called TMR4I, that allows automatic detection of interactions among rec-ommendations that require some attention from experts, such as recommendingmore than once the same drug. We evaluate our model by applying it on a re-alistic case study that involves three guidelines concerning Osteoarthritis (OA),Hypertension (HT) and Diabetes (DB). We further show the added value of ourmodel by comparing to existing approaches [3, 4].
The remainder of this paper is structured as follows: Section 2 discussesrelated work. Section 3 introduces the preliminaries, including the concepts ofthe TMR model that underlie TMR4I. Section 4 presents the TMR4I extension.Section 5 describes our case study for multimorbidity. Section 6 discusses theresults and outlines future work.
2 Related Work
Different CIG description languages were proposed to represent clinical knowl-edge (PROforma [7], GLIF [1], Asbru [5], etc.). Since the main focus of theselanguages was set on guideline execution, they have some limitations mainlyrelated to the interoperability (CIG cannot be mixed), semantics (free text isoften used to describe conditions and actions) and reasoning capabilities (e.g.,the inference of new actions or restrictions is not supported) [2, 6].
The increasing demand for clinical decision support systems (CDSS) that as-sist healthcare professional to define treatments for multimorbid patients high-lights the limitations of classical CIG languages and indicates the necessity fornew formalisms or for adapting existing ones. In [8], we have reviewed exist-ing approaches for merging treatments plans or guidelines and we categorizedthem into: (i) guideline-level verification, (ii) on-prescription verification, (iii)after-prescription verification and (iv) on-treatment-execution verification. Asre-usability is one of our major concerns, we focused on approaches of the firstcategory. In this paper we are particularly interested in approaches addressing

the multimorbidity problem which consists of combining recommendations re-garding more than two diseases taken from their respective guidelines. In thiscontext, the works done by Jafarpour [3] and Lopez-Vallverdu et.al [4] stand out.
Lopez-Vallverdu’s approach [4] relies on Rules and Actions that regards ad-ministration of drugs, and adopts a standard terminology called ATC (Anatom-ical Therapeutic Chemical Classification System for drugs4). Therefore, usingknowledge available in clinical guidelines, they manually built “knowledge units”for pairwise combination of three diseases: Hypertension, Diabetes Mellitus andHeart Failure. Those knowledge units regards the co-existence of incompatibledrugs (drug-drug interaction), the existence of a drug incompatible to a disease(drug-disease interaction) and the absence of a drug necessary for a combinationof diseases. Based on these units, they manually built a minimal set of combi-nation rules in the format pre-condition : condition → action, where the firstone regards the diseases, the second regards the presence or absence of drugrecommendations for each disease, and the latter regards recommendations foradding, removing or replacing drugs. Although it is not clear from the knowledgeformat whether it is limited to two diseases, the strategy adopted by the authorsfor addressing the three aforementioned diseases is by pairwise combining them.Moreover, the manual identification of the interactions and their solutions is initself a limiting factor for combining multiple diseases. Their approach is imple-mented in a proprietary system for combining treatments.
Jafarpour’s approach [3] defines both (i) a OWL+SWRL based formalism forrepresenting and executing CIGs (CPG-DKO) and (i) an OWL+SWRL basedformalism for combining two CIGs. The latter defines Constraints (rules) asentities that relates pairs of interacting Tasks (actions). Therefore, for each pairof CIGs the potential conflicts or interactions are manually represented, togetherto their solution, by instantiating different types of constraints, for instance avoidrepeating tasks, reusing test results, defining time-constraints or replacing tasks.This approach is then limited to pairwise combination of tasks within two CIGs,although several CIGs can be executed together. They apply their approach ina number of case studies, including one for combining OA+HT+DB. Section 5presents more details about this approach.
Although both approaches introduce features for expressing the interactionsand their solutions, both formalisms are still not expressive enough to supportthe automatic detection of inconsistencies like having “administer insulin” and“avoid administering insulin” since both rely on a textual expression of the careactions and the features linked to it. They assume that all potential inconsisten-cies are manually detected by domain experts and rules are created to deal withthem, often introducing new recommendations to address the conflict. Moreover,the introduction of new recommendations requires further verification to checkfor eventual new conflicts that could arise. If all potential conflicts need to besolved by adding rules, it may lead to a combinatorial explosion of rules. Thisin turn, increases the complexity of detecting conflicting rules; especially if theverification is done manually by experts. Jafarpour defines SWRL rules that al-
4 http://www.whocc.no/atc/

low automatically detecting specific time/priority-related conflicts between pairsof the introduced constraints, but does not address other types of conflicts anddoes not find eventual conflicts with existing tasks. Finally, both approachesgather the knowledge they created for the pairwise combined CIGs in order toaddress the combination of more than two CIGs. For example, the constraintscreated between OA+HT, OA+DB and HT+DB are gathered to address thecombination of the three CIGs OA+HT+DB. However, this strategy is limitedsince it does not cover for instance a constraint from OA+HT whose solutionconflict with recommendations from DB. They cope with comorbidity but areproblematic in case of multimorbidity.
As illustrated in this section, existing works are not tailored to our objectiveof increasing the reasoning capability of CIGs to handle multimorbidity. We aimto define a method that allows evaluating set of recommendations and derivingcertain types of interactions requiring little or no human intervention (e.g. rulesmanually created). The TMR model (proposed in [8], overviewed in Sect 3), sup-ports this goal by enriching the description of actions (with the pre-conditionsand the potential consequences) and separating actions from recommendationstatements (pursue or avoid an action). Section 6 presents a summarized com-parison among the related works and our approach.
3 Overview of the TMR Model
This section briefly summarizes a slightly extended version of the TMR model,originally presented in [8] where we investigated the core concepts required forrepresenting recommendations within CGs. Figure 1 shows a UML diagram ofthe TMR model. The concepts and relations presented as they were in the orig-inal version are depicted in gray shade to differ from the the new concepts andrelations changed or introduced in this work. Those that have a slash sign beforetheir names are further defined by FOL formulas (e.g. /similarTo). We considerthe concepts as being atomic, since its compositionality is out of scope of thiswork.
– A Guideline is an aggregation of Recommendations, whilst the latter ispart of one Guideline. It can be a Single Disease Guideline, or it can bea Composed Guideline, which is derived from the combination of twoor more Guidelines.
– A Recommendation either recommends to pursue or recommendsto avoid (originally recommends and non-recommends) one Transition.
– A Transition is promoted by a single Care Action Type, which in turncan promote one or more Transitions. A Transition can be similar to orinverse to another one (definition is further provided).
– Situation Types can be Pre or Post-Situation Types in the context ofdifferent Transitions.
– Every Transition have:• one Transformable Situation Type through the relation has trans-
formable situation,

Fig. 1. UML class diagram for the TMR Model
• one expected Post-Situation Type through the relation has expectedpost situation, and
• zero or more Non-Transformable Situation Types through the re-lation have as filter condition.
For example, Table 1 presents the recommendation “If the patient’s tempera-ture is over 37 degrees and he/she is over 10 years old then reduce the temperatureby administering aspirin” decomposed into the TMR concepts.
We introduce the binary relations /similarTo and /inverseTo betweenTransitions, which are required for detecting Interactions. In this work we con-sider a simple approach of comparing equality among Pre and Post-SituationTypes, though these definitions would benefit from a richer definition of Situ-ation Types and possible matches among them. Therefore, similar transitions(def. 1.1) are those whose Pre-Situation Types are the same, as well as thePost-Situation Types, but that are promoted by different Care Action Types(otherwise they are the same transition). Two transitions are inverse (def. 2.1) ifthe Pre-Situation Type of one is equal to the Post-Situation Type of the other.Both relations similarTo and inverseTo are symmetric (def. 1.2 and 2.2).
(1.1) ∀t1, t2, sa, sb, ca1, ca2 Transition(t1) ∧ Transition(t2) ∧ CareActionType(ca1)∧ CareActionType(ca2) ∧ promotedBy(t1,ca1) ∧ promotedBy(t2,ca2)∧ ca1 6= ca2 ∧ SituationType(sa) ∧ SituationType(sb)∧ hasTransformableSituation(t1,sa) ∧ hasTransformableSituation(t2,sa)∧ hasExpectedSituation(t1,sb) ∧ hasExpectedSituation(t2,sb)
↔ similarTo(t1,t2)(1.2) ∀t1, t2 similarTo(t1,t2) ↔ similarTo(t2,t1)(2.1) ∀t1, t2, sa, sb Transition(t1) ∧ Transition(t2)
∧ SituationType(sa) ∧ SituationType(sb)∧ hasTransformableSituation(t1,sa) ∧ hasTransformableSituation(t2,sb)∧ hasExpectedSituation(t1,sb) ∧ hasExpectedSituation(t2,sa)
↔ inverseTo(t1,t2)

Table 1. TMR Concepts Summary
Situation Type Represents a property and its admis-sible values
TransformableSituation Type
Regards the situation that is ex-pected to be changed
Patient’s temperature isover 37 degrees
Non-TransformableSituation Type
Regards the situation that holds asfilter condition
Patient’s age is over 10years old
Post-SituationType
Regards the situation that is ex-pected to be achieved
Patient’s temperature isbelow 37 degrees
Care ActionType
Represents the action types that canbe performed by health care agentsin order to change a situation.
Administer aspirin
Transition Represents the possibility of chang-ing a situation regarding a patientby performing a care action type.
Administering aspirin inpatient over 10 years oldreduces its temperature be-low 37 degrees
Recommendation Represents a suggestion to eitherpursue or avoid a transition pro-moted by a care action type (in or-der to achieve a goal).
(2.2) ∀t1, t2 inverseTo(t1,t2) ↔ inverseTo(t2,t1)
In [8] we illustrated the applicability of TMR by describing the possibleinteractions among recommendations. These interactions can be contradictory,optimizable or reflect alternative recommendations (redefined in Sect. 4). We ad-vocated that the TMR concepts favor the detection of such interactions, whichmay require some attention from experts when combining CGs due to comorbid-ity. Moreover, we considered not all interactions are unwelcome (e.g. the recom-mendations to inverse transitions may be desirable and the alternative ones areuseful to avoid conflicts) although they could still require attention (e.g. defin-ing which alternative recommendation is preferred). In the following section weextend the TMR model for the specific task of representing and detecting inter-actions among recommendations.
4 The TMR4I Model
The TMR4I (Transition-based Medical Recommendations for [detecting] Inter-actions) model is meant for detecting interactions among recommendations whenaddressing multimobidity cases. In this cases more than one disease, originallyaddressed in different CIGs, need to be taken into account. Therefore, the rec-ommendations combined from the different CIGs may interact, e.g. presentinginconsistencies or being susceptible to optimization. The main concept in TMR4I

is the interaction, which can be internal, among the recommendations them-selves, or with some external knowledge base holding e.g. patient data (allergyinformation) or clinical knowledge (e.g. overdose). In this paper we focus onthe internal interactions, as described in Table 2. Moreover, since the tempo-ral/sequence aspects are still not addressed in this work, the interactions heredefined are considered either time-independent or simultaneous.
Figure 2 illustrates in a graphical notation the interactions discussed in Table2. We depict the three main types of Interactions, Repetition, Contradictionand Alternative Interactions as the initial letters followed by an exclamationmark connected to the interacting recommendations. An arrow that connectsa Recommendation to a Transition means that the latter is recommended tobe pursued, while an arrow ending with a cross means that the Transition isrecommended to be avoided. Another dotted arrow connecting a Care ActionType to a Transition means that the latter is promoted by the former. Finally aTransition is connected to Pre and Post-Situation Types respectively at its leftand right hand sides. For example, the third interaction (from top to bottom) is
Table 2. Interactions Summary
ContradictionInteractions
two recommendations that would lead to a conflict if rec-ommended together (i.e. they cannot be both followed atthe same time)
Opposed recommenda-tions to the same careaction
- Do not administer aspirin to avoid increasing the riskof gastrointestinal bleeding- Administer aspirin to handle inflammation
Opposed recommenda-tions to similar transi-tions
- Do not adm. beta-blockers to avoid lowering blood pres-sure- Administer ACE inhibitor to lower blood pressure
Recommendations to in-verse transitions
- Administer ACE inhibitor to lower blood pressure- Administer midodrine to increase blood pressure
RepetitionInteractions
set of recommendations that are susceptible to optimization
Repeated recommenda-tions to the same careaction
- Administer aspirin to reduce the risk of thrombus- Administer aspirin to relief pain- Administer aspirin to handle inflammation
AlternativeInteractions
set of recommendations that hold as alternatives.
Repeated recommen-dations to the similartransitions promoted bydifferent care action
- Administer aspirin to handle inflammation- Administer ibuprofen to handle inflammation- Administer naproxen to handle inflammation
Non-recommended tran-sition whose inverse tran-sition is recommended
- Do not administer aspirin to avoid increasing the riskof gastrointestinal bleeding- Adm PPI to decrease risk of gastrointestinal bleeding

Fig. 2. Instance-schema for illustrating interactions among recommendations
a Repetition Interaction among three recommendations for different Transitionspromoted by Administer Aspirin.
Figure 3 presents an UML class diagram for the TMR4I model. Elementspresented in a gray-shade mean they were previously introduced. The conceptRecommendation is specialized into /Internally Interacting Recommenda-tion (def. 3) to denote the ones that interacts with other recommendations.
(3) ∀r, ∃i Recommendation(r) ∧ InternalRecommendationInteraction(i)∧ relates(i,r) ↔ InternallyInteractingRecommendation(r)
The interaction relation is reified as /Internal Recommendation Interac-tion and /relates two or more Recommendations in the context of a Guideline.The latter concept is specialized according to the classifications discussed in Ta-ble 2. They are further described and defined according FOL rules (def. 4 to9).
Repetition due to Same Action: when Transitions promoted by a sameCare Action Type are recommended to be pursued (def. 4.1). This interaction iscumulative within a CIG, i.e. if a recommendation is related to two interactionsof this type, they are the same interaction (def. 4.2)

Fig. 3. UML class diagram for the TMR4I Model
(4.1) ∀g, r1, r2, t1, t2, ca Guideline(g) ∧ Recommendation(r1) ∧ Recommendation(r2)∧ partOf(r1,g) ∧ partOf(r2,g) ∧ Transition(t1) ∧ Transition(t2) ∧ r1 6= r2∧ recommendsToPursue(r1,t1) ∧ recommendsToPursue(r2,t2)∧ CareActionType(ca) ∧ promotedBy(t1,ca) ∧ promotedBy(t2,ca)
→ ∃i RepetitionDueToSameAction(i) ∧ relates(i,r1) ∧ relates(i,r2)
(4.2) ∀i1, i2, r1, r2, r3 RepetitionDueToSameAction(i1)∧ RepetitionDueToSameAction(i2) ∧ Recommendation(r1)∧ Recommendation(r2) ∧ Recommendation(r3) ∧ r1 6= r3∧ relates(i1,r1) ∧ relates(i1,r2) ∧ relates(i2,r2) ∧ relates(i2,r3)
→ i1 = i2
Contradiction due to Inverse Transitions: when two inverse Transitionsare (simultaneously) recommended to be pursued (def. 5);
(5) ∀g, r1, r2, t1, t2 Guideline(g) ∧ Recommendation(r1) ∧ Recommendation(r2)∧ partOf(r1,g) ∧ partOf(r2,g) ∧ Transition(t1) ∧ Transition(t2)∧ recommendstoPursue(r1,t1) ∧ recommendstoPursue(r2,t2)∧ inverseTo(t1, t2)
→ ∃i ContradictionDueToInverseTransition(i) ∧ relates(i,r1) ∧ relates(i,r2)
Contradictory Interaction due to Same Action: when two Transitionspromoted by the same Care Actions Type are are recommended to be pursuedand the other recommended to be avoided (def. 6);
(6) ∀g, r1, r2, t1, t2, ca Guideline(g) ∧ Recommendation(r1) ∧ Recommendation(r2)∧ partOf(r1,g) ∧ partOf(r2,g) ∧ Transition(t1) ∧ Transition(t2) ∧ r1 6= r2∧ recommendsToPursue(r1,t1) ∧ recommendsToAvoid(r2,t2)∧ CareActionType(ca) ∧ promotedBy(t1,ca) ∧ promotedBy(t2,ca)
→ ∃i ContradictionDueToSameAction(i) ∧ relates(i,r1) ∧ relates(i,r2)
Contradictory Interaction due to similar Transitions: when two similarTransitions are one recommended to be pursued and the other recommended tobe avoided (def. 7);

(7) ∀g, r1, r2, t1, t2 Guideline(g) ∧ Recommendation(r1) ∧ Recommendation(r2)∧ partOf(r1,g) ∧ partOf(r2,g) ∧ Transition(t1) ∧ Transition(t2)∧ recommendsToPursue(r1,t1) ∧ recommendsToAvoid(r2,t2)∧ similarTo(t1, t2)
→ ∃i ContradictionDueToSimilarTransition(i) ∧ relates(i,r1) ∧ relates(i,r2)
Alternative Interaction due to similar Transitions: when similar Transi-tions are recommended to be pursued (def. 8.1). This interaction is cumulativewithin a CIG, i.e. if a recommendation is related to two interactions of this type,they are the same interaction (def. 8.2)
(8.1) ∀g, r1, r2, t1, t2 Guideline(g) ∧ Recommendation(r1) ∧ Recommendation(r2)∧ partOf(r1,g) ∧ partOf(r2,g) ∧ Transition(t1) ∧ Transition(t2)∧ recommendsToPursue(r1,t1) ∧ recommendsToPursue(r2,t2)∧ similarTo(t1, t2)
→ ∃i AlternativeDueToSimilarTransition(i) ∧ relates(i,r1) ∧ relates(i,r2)(8.2) ∀i1, i2, r1, r2, r3 AlternativeDueToSimilarTransition(i1)
∧ AlternativeDueToSimilarTransition(i2) ∧ Recommendation(r1)∧ Recommendation(r2) ∧ Recommendation(r3) ∧ r1 6= r3∧ relates(i1,r1) ∧ relates(i1,r2) ∧ relates(i2,r2) ∧ relates(i2,r3)
→ i1 = i2
Alternative Interaction due to Inverse Transition: when two inverse Tran-sitions are one recommended to be pursued and the other recommended to beavoided (def. 9);
(9) ∀g, r1, r2, t1, t2 Guideline(g) ∧ Recommendation(r1) ∧ Recommendation(r2)∧ partOf(r1,g) ∧ partOf(r2,g) ∧ Transition(t1) ∧ Transition(t2)∧ recommendsToPursue(r1,t1) ∧ recommendsToAvoid(r2,t2)∧ inverseTo(t1, t2)
→ ∃i AlternativeDueToInverseTransition(i) ∧ relates(i,r1) ∧ relates(i,r2)
Given the definitions of which and how internal interactions can be identifiedaccording to the TMR4I model, we present in the next section an approach ofhow to apply this model in a multimorbidity case study.
5 Evaluation on Multimorbidity Case Study
We evaluate the TMR4I model by applying it to a realistic (conceptual) exper-iment on combining 3 CIGs for Osteoarthritis5 (OA), Hypertension6 (HT) andDiabetes7 (DB) taken from Jafarpour’s thesis[3]. We make some simplificationof the original case study both (i) representing only the recommendations thatare relevant for studying the interactions and illustrating the approach and (ii)simplifying the features that are not yet addressed by the TMR model (e.g.quantities). We first introduce the experiment of [3] and then we discuss andcompare with our approach.
5 www.nhstaysideadtc.scot.nhs.uk/TAPG%20html/Section%2010/osteoarthritis.htm6 pathways.nice.org.uk/pathways/hypertension7 pathways.nice.org.uk/pathways/diabetes

Fig. 4. The instantiation of the CPG-KPO and the parts of the osteoarthritis andhypertension pathways that participate in the merge [3]
Jafarpour (introduced in Section 2) creates constraints to resolve conflictsbetween tasks (recommendations) in two CIGs, as illustrated in Fig. 4. The threetasks regarding the administration of Ibuprofen or Naproxen are considered tobe in conflict with the hypertension pathway, since these drugs may increase theblood pressure, according to experts. Then the constraints named conflict 1, 2and 3 are manually introduced suggesting the replacement of these drugs byTramadol or similar. The role of those constraints is to interfere in the executionof the CIGs, i.e. when a task that is to be executed has one of these constraintsassociated, then instead of executing the task, the constraint instruction will befollowed. In this example, the instructions are for substituting the task.
The goal in Jafarpour’s approach is to produce a reusable pairwise combina-tion of CIGs, such that several pairwised combined guidelines can be executedtogether to handle multi-morbidity. Besides the combination of OA+HT, theapproach is applied to combine OA+DB and HT+DB such that the three ofthem can be executed together. As we discussed in Section 2, the interactionsare not completely addressed by this approach. For instance, Tramadol is recom-mended many times in order to address the aforementioned conflicts and also toaddress another conflict between OA and DB recommendations, where Tramadolis recommended to replace Aspirin as anti-thrombotic. Since recommending thesame drug more than once may lead to overdose, it requires attention from the

experts. However, Jafarpour’s approach does not detect the interaction we justmentioned.
In Fig. 5 we represent a (partial) merged CIG for OA+HT+DB and the iden-tified interactions according to the TMR4I model. First, the effects that mustbe avoided for each disease, which are the reason for the conflicts, are explicitlyrepresented as recommendations within each CIG (if this information is not yetavailable). E.g. for detecting the aforementioned conflict the recommendation“Avoid High Blood Pressure promoted by Administering Aspirin” is explicitlyintroduced in the HT CIG. Although this resembles the manual identification ofthe contradiction, it is actually not the case. Once this information is availableas part of the CIG, it can be used to derive many interactions. The recommenda-tions from the original CIG’s are reused in order to create a merged CIG. Then,some interactions manually identified by Jafarpour can be derived (denoted asC! in the figure): (i) Administer ibuprofen to relief pain from OA contradictsDo not adminster ibuprofen to avoid increase the blood pressure from HT; (ii)Administer thiazide to lower the blood pressure from HT contradicts Do not ad-minster thiazide to avoid increase the level of blood sugar from DB; and (iii)Administer aspirin to lower the risk of thrombus from DB contradicts Do notadminster aspirin to avoid increase the risk of gastro-intestinal bleeding fromOA.
Then, we manually introduce solutions proposed by Jarfapour, depicted inFigure 6 as the last two recommendations (one of the solutions regarding re-ducing the quantity is not addressed, since it is out of scope of this work). Theresultant CIG is further verified by applying the same method and other inter-actions can be derived (denoted as A! and R! in the figure): (i) an alternativeinteraction is derived between recommendations for Painkiller, (ii) another al-
Fig. 5. Instance-schema illustrating the merged CIG for OA, HT and DB and the threecontradictory interactions derived.

Fig. 6. Instance-schema illustrating new recommendations introduced into the mergedCIG for OA, HT and DB and interactions identified.
ternative interaction is derived between Anti-thrombotic recommendations and(iii) an repetition interaction is derived among the introduced recommendationsfor Administering Tramadol.
By performing this conceptual experiment we demonstrate that the TMR4Iapproach allows a more systematic detection of internal interactions both aftercombining CIGs and after introducing new recommendations in order to addressthe interactions. This approach favor the automatization of this task, in contrastwith Jafarpour approach that requires ad-hoc interaction rules.
6 Discussion and Future Work
Our evaluation illustrates the improvements that can be achieved in addressingthe multimorbidity task by applying TMR4I model, with respect to the studiedapproaches. By reusing and combining information, it improves the reasoning ca-pabilities for deriving interactions among recommendations within several CIGs.Although there is still space for improvements in the current model (further men-tioned in this section), we believe the benefits from a more detailed semanticsfor the CIG elements can already be observed.
While the related approaches [3, 4] provide a pairwise identification of con-flicts by manually introducing rule-constraints, we are able to provide the fol-lowing improvements: (i) (semi)automatable identification of interactions amongrecommendations; (ii) detecting interactions among several recommendations
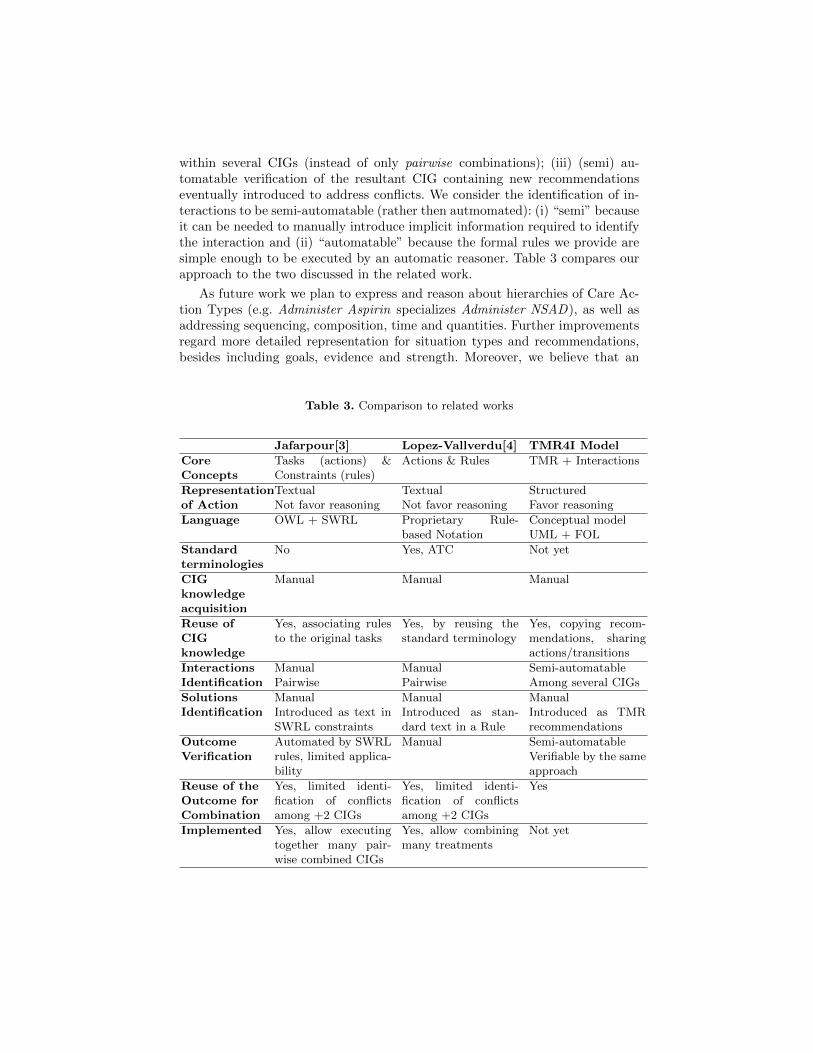
within several CIGs (instead of only pairwise combinations); (iii) (semi) au-tomatable verification of the resultant CIG containing new recommendationseventually introduced to address conflicts. We consider the identification of in-teractions to be semi-automatable (rather then autmomated): (i) “semi” becauseit can be needed to manually introduce implicit information required to identifythe interaction and (ii) “automatable” because the formal rules we provide aresimple enough to be executed by an automatic reasoner. Table 3 compares ourapproach to the two discussed in the related work.
As future work we plan to express and reason about hierarchies of Care Ac-tion Types (e.g. Administer Aspirin specializes Administer NSAD), as well asaddressing sequencing, composition, time and quantities. Further improvementsregard more detailed representation for situation types and recommendations,besides including goals, evidence and strength. Moreover, we believe that an
Table 3. Comparison to related works
Jafarpour[3] Lopez-Vallverdu[4] TMR4I Model
CoreConcepts
Tasks (actions) &Constraints (rules)
Actions & Rules TMR + Interactions
Representationof Action
TextualNot favor reasoning
TextualNot favor reasoning
StructuredFavor reasoning
Language OWL + SWRL Proprietary Rule-based Notation
Conceptual modelUML + FOL
Standardterminologies
No Yes, ATC Not yet
CIGknowledgeacquisition
Manual Manual Manual
Reuse ofCIGknowledge
Yes, associating rulesto the original tasks
Yes, by reusing thestandard terminology
Yes, copying recom-mendations, sharingactions/transitions
InteractionsIdentification
ManualPairwise
ManualPairwise
Semi-automatableAmong several CIGs
SolutionsIdentification
ManualIntroduced as text inSWRL constraints
ManualIntroduced as stan-dard text in a Rule
ManualIntroduced as TMRrecommendations
OutcomeVerification
Automated by SWRLrules, limited applica-bility
Manual Semi-automatableVerifiable by the sameapproach
Reuse of theOutcome forCombination
Yes, limited identi-fication of conflictsamong +2 CIGs
Yes, limited identi-fication of conflictsamong +2 CIGs
Yes
Implemented Yes, allow executingtogether many pair-wise combined CIGs
Yes, allow combiningmany treatments
Not yet

external knowledge base providing extra information about the effects of careactions resulting from clinical trials can support both the identification of exter-nal conflicts (e.g. overdose or drug-drug interaction) as well as identification ofsolutions for conflicts (e.g. other drugs with same effect). Therefore we intend toreapply improved version of the model to new case studies. Finally, we are inves-tigating the use of Semantic Web technologies to implement the TMR4I model.This will allow us to benefit from reusing medical knowledge and terminologiesalready available, as well as by providing reusable clinical knowledge.
7 Conclusion
With the ever aging of the population, multimorbidity is becoming a huge prob-lem and require appropriate tools supporting the physicians to design adaptedtreatment plans. To this end, we have introduced in this paper the TMR4I asa conceptual model for detecting interactions among recommendations withinseveral CIGs. We conceptually demonstrate that some improvements can beachieved in addressing multimorbidity, with respect to other studied approaches,by relying on a more detailed semantics for representing the recommendationsand actions. Our approach favor combining several CIGs since it provide meansfor (semi) automatically identifying interactions among many recommendationswithin many CIGs, and effectively verifying the resultant combined CIG by reap-plying the approach. In the future, we will work on the implementation of theproposed model and we will further extend the TMR4I model in order to addressits limitations like the notion of temporality, besides evaluate the model on otheruse cases like guideline adaptation or re-use.
References
1. Boxwala, A.A., , M., Tu, S.W., Ogunyemi, O., Zeng, Q.T., Wang, D., Patel,V.L., Greenes, R.A., Shortliffe, E.H.: GLIF3: a representation format for sharablecomputer-interpretable clinical practice guidelines. Journal of Biomedical Informat-ics 37(3), 147–161 (2004)
2. Isern, D., Moreno, A.: Computer-based execution of clinical guidelines: a review.International journal of medical informatics 77(12), 787–808 (Dec 2008)
3. Jafarpour, B.: Ontology Merging using Semantically-defined Merge Criteria andOWL Reasoning Services: Towards Execution-time Merging of Multiple ClinicalWorkflows to Handle Comorbidity. Ph.D. thesis, Dalhousie University (2013)
4. Lopez-Vallverdu, J.A., Riano, D., Collado, A.: Rule-based combination of comor-bid treatments for chronic diseases applied to hypertension, diabetes mellitus andheart failure. In: Lecture Notes in Computer Science (including subseries Lec-ture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). vol.7738 LNAI, pp. 30–41 (2013), http://www.scopus.com/inward/record.url?eid=2-s2.0-84893941704&partnerID=tZOtx3y1
5. Miksch, S., Shahar, Y., Johnson, P.: Asbru: a task-specific, intention-based, andtime-oriented language for representing skeletal plans. In: 7th Workshop on Knowl-edge Engineering: Methods & Languages. pp. 1–25 (1997)

6. Peleg, M.: Computer-interpretable clinical guidelines: a methodological review.Journal of biomedical informatics 46(4), 744–63 (Aug 2013)
7. Sutton, D.R., Fox, J.: The Syntax and Semantics of the PROforma Guideline Model-ing Language. Journal of the American Medical Informatics Association 10, 433–443(2003)
8. Zamborlini, V., da Silveira, M., Pruski, C., ten Teije, A., van Harmelen, F.: To-wards a Conceptual Model for Enhancing Reasoning about Clinical Guidelines: Acase-study on Comorbidity. In: Knowledge Representation for Health-Care. LectureNotes in Computer Science, vol. 8903 LNCS. Springer Berlin Heidelberg, Vienna,Austria (2014)