a community health nursing plan of...
TRANSCRIPT
A Community Health Nursing Plan of Care
Pam Beringer, Erin Burdi, Debra Francik , and
Ashley Jacobson

Assessment & Analysis
Epidemiological Concepts
Host: Due to the “rural” classification of
Mecosta County, residents of this community
are at an increased risk for a shortage of
Health Care Providers (HCP’s) .

Assessment & Analysis:
Epidemiological Hosts
Rural areas (also referred to as "the country," and/or
"the countryside") are settled places outside
towns and cities (Farlex, 2010, para 1).
According to the US Census Bureau, the classification of “rural” includes all territories, populations, and housing units located outside of an Urbanized Area (UA) or Urban Cluster (UC) (2000).

Assessment & Analysis:
Epidemiological Host
In the year 2000, the Mecosta County total
population census was 40,553
(MSUE,2007).
The rural population of Mecosta County was
28,780 residents or 70.6% of the total population (US Census Bureau, 2000)
*27,642 (96% )of these residents lived in Non-Farm areas & 1,138, (4%) of residents
lived in farm areas (MSUE, 2007, p.5)

Assessment & Analysis
United States 21% 59,061,367 281,421,906
Michigan 25.3% 2, 518,987 9,938,444
Mecosta 70.6% 28,780 40,553
Percentage of
Population Rural Population
Census Total Population
Rural Population Comparison
*According to Census Data, Mecosta County has a greater percentage of
rural resident population than both the State & National census combined! (US Census Bureau, 2000)

Vulnerable Groups
“To be considered vulnerable, a person or group generally has aggravating
factors that place them at greater risks for ongoing poor health status then
other at-risk persons” (Fisher, pg. 533).
An example : “ A middle-aged obese man with a sedentary lifestyle
and hypertension would be considered at risk for cardiac problems. If that
man also had an income below the poverty level, no health insurance, and
stressors related to living conditions, he would be more likely to be
vulnerable to ongoing poor health status then a man with similar risk
factors but with an adequate income and health insurance. The man in
poverty would be more likely to experience difficulties obtaining and
maintaining a relationship with a primary care provider, would have
problems accessing tests and procedures for diagnosis and ongoing
monitoring, and would have difficulty obtaining and paying for the
appropriate medications”(Fisher, pg. 5330.

Specific groups this especially effects
According to Fisher, “A vulnerable population is a group or
groups that are more likely to develop health-related problems,
have more difficulty accessing health care to address those health
problems, and are more likely to experience a poor outcome or a
shorter life span because of those health conditions” (Fisher, pg.
533).
Characteristics, traits , and different circumstances enhance the
potential for poor health (Fisher, pg. 533).
“Department of Health and Human Services, had identified certain
groups as more vulnerable to health risks, including the poor, the
homeless, disabled, the severely mentally ill, the very young, and
the very old” (Fisher, pg. 533).
Not all people at risk for poor health are considered vulnerable
Assessment & Analysis
Community Groups of Interest
“What is it like to live in a small rural town? What do nurses know about rural
populations and their nursing needs? Although each community is unique, the
experience of living in a small town is similar in all 50 states” (Fisher, pg. 820-
821).
The typical rural lifestyle is characterized by
the following: Greater spatial distances between people and services
An economic orientation toward the land and nature
Work and recreational activities that are cyclic and seasonal
Social interaction that facilitate informal, face-to-face negotiations,
because most, if not all, residents are either related or acquainted
(Fisher, pg. 821)

Assessment & Analysis
Community Groups of Interest
“There is increasing evidence that community members who are informed and active in planning their health care system are more likely to use and support that system” (Fisher, pg. 825).
The community decision making model helps to identify a problem and try to come up with a solution. The steps in the model are:
- 1. Identify the problem.
- 2. Assess the community’s perspective
- 3. Analyze the data
- 4. Develop a long-range plan
- 5. Take action
- 6.Evaluate the program

Assessment & Analysis
Existing Health Resources in Mecosta
“There is ongoing debate as to whether anything is unique
about rural nursing practice, because nursing care is similar
regardless of the setting” (Fisher, pg. 822).
There is little information in periodical and in nursing texts on
what actually makes community/public health nursing
different in rural settings (Fisher, pg 824).

Assessment & Analysis
Community Groups of Interest
“In brief, for rural residents, a small town is
the center of trade for a region, and its
churches and schools usually are the centers
for socialization” (Fisher, pg. 821).
This helps for planning and implicating
public health and community nursing
programs for rural clients (Fisher, pg. 821).

Assessment & Analysis
Community Groups of Interest
Community Groups that might be interested
in helping are:
Churches
Nursing Students
Volunteers
Nurses
Community Centers
American Red Cross

Assessment & Analysis: Epidemiological Environment
There are Three Major Factors that
Influence Rural Health
1. Availability of Services
2. Accessibility of Services
3. Acceptability of Services (Maurer & Smith, 2009, p.815)

Assessment & Analysis:
Rural Health Influences
Availability of Services
“refers to the existence of services and sufficient personnel to provide those
services”
(Maurer & Smith, 2009, p.815)

Assessment & Analysis:
Rural Health Influences Acceptability of Services
“refers to the degree to which a particular is offered in a manner
congruent with the values of a target population” (Maurer & Smith, 2009, p.816)

Assessment & Analysis:
Rural Health Influences
Barriers to Acceptability
Urban Orientation of
most HCP’s
(Maurer & Smith, 2009, p.816)

Assessment & Analysis
Rural Health Influences
Accessibility of Services “ refers to the ability of a person to obtain and afford
needed services” (Maurer & Smith, 2009, p.815)
Common Barriers to Accessibility Include: Long Travel Distances
Lack of Public Transportation
Lack of Telephone Services
Shortage of Health Care Providers Inequitable Reimbursement policies
Unpredictable Weather Conditions
Inability to Obtain Entitlements
(Maurer & Smith, 2009, p.815)

Multiple factors also affect specific groups
Lower socioeconomic status
Lifestyle behaviors
The psychological impact of poverty
Genetic inheritance
Race
Ethnicity
Gender
Poor education
Poor health
Sudden change in financial situation
(Fisher, pf. 541)

Health Professional shortage areas
“Concerns about rural health care services, especially in regions with insufficient numbers of all types of health care providers,(designated as health professional shortage areas [HPSA]) have become a national priority since the early 1990’s” (Fisher, pg. 809).
“The U.S. Bureau of the Census estimates that there are 54 million people living in rural areas of the United States. They make about 1/5 (20%) of the total population but are spread out across 4/5 (80%) of the land area” (Fisher, pg. 809).

Assessment & Analysis
Shortage of Health Care Providers
As of 2005, Mecosta County had only
34 Practicing Physicians located in Big Rapids area
to care for a Population of
42,391
That ‘s a 1 : 1247 Physician-Patient
Ratio!!!
As of 2005, in the
State of Michigan
there are 25,146 active
physicians*
with a State
Population of
10,120,860
That’s a 1:420
Physician –Patient
Ratio!
*(excluding physicians with unknown
addresses, inactive statuses, and osteopathy)

Assessment & Analysis: Epidemiological Agents
Major Health Problems for Rural Areas
Accidents & Trauma
Chronic Illness
Suicide & Homicide
Alcohol & Drug Abuse

Assessment & Analysis: Epidemiological Agents
Top Ten Causes of Death in Mecosta County
1. Heart Disease
2. Cancer
3. Chronic Lower Respiratory Disease
4. Stroke
5. Unintentional Injuries
6. Diabetes Mellitus
7. Alzheimer’s Disease
8. Pneumonia/Influenza
9. Kidney Disease
10. Intentional Self Harm
(Michigan Surgeon General’s Health Status Report., 2010)

Assessment & Analysis
Epidemiological Agents The Top Ten Causes of Morbidity/ Mortality for the State of
Michigan where nearly identical to those of Mecosta County
with only a slight difference in numerical order
Mecosta County 1. Heart Disease
2. Cancer
3. Stroke
4. Chronic Lower Respiratory Disease
5. Unintentional Injuries
6. Diabetes Mellitus
7. Alzheimer’s Disease
8. Pneumonia/Influenza
9. Kidney Disease
10. Intentional Self Harm
State of Michigan 1. Heart Disease
2. Cancer
3. Chronic Lower Respiratory Disease
4. Stroke
5. Unintentional Injuries
6. Diabetes Mellitus
7. Alzheimer’s Disease
8. Pneumonia/Influenza
9. Kidney Disease
10. Intentional Self Harm
(Michigan Surgeon General’s Health Status Report., 2010)

Nursing Diagnosis
Risk for Increased Mortality & Morbidity
in Mecosta County
related to
Lack of Health Care Providers.

Plan
Increase the availability of preventative
health resources and measures to citizens
of Mecosta County to decrease the
burden on current Health Care Providers
(HCP).
Rationale: If Residents of Mecosta County have Access to Preventative
Care & become Proactively Involved with Personal Health, the
Over-all Community will Benefit from Improved Health &
Reduction of Health Services Required.

Michigan Center for Rural Health
“Supporting and engaging rural Michigan communities and their residents in eating healthy, being physically active, and achieving and maintaining a healthy weight should reduce the burden of chronic disease and also contribute to an improved quality of life. Collaborative efforts involving communities, schools, worksites, families, and others are needed to create environments that support sustainable healthy behaviors.”
(Michigan Center for Rural Health, 2008, pg.23)

Primary Prevention
“Primary prevention is aimed at altering the susceptibility or reducing the exposure of persons who are at risk for developing a specific disease” (Fisher, Pg. 170).
“Primary prevention includes general health promotion and specific protective measures in the pathogenesis stage, which are designed to improve the health and well-being of the population” (Fisher, pg 170).

Plan: Primary Prevention
Sources for Volunteers & Community Venues
Volunteers *Professors & Nursing Students
from Ferris State University
located in Big Rapids
*Health Care Personnel from
Local Mecosta County Hospital
& Private Practices
* Church Volunteers
Venues
*Churches
*Community Centers
*County Hospital
*Urgent Care Centers

Plan: Primary Community
Prevention Utilize Local Volunteers & Venues to Educate &
Encourage Preventative Health Measures & Provide Free Health Screenings that Target Top 10 Causes of Morbidity & Mortality in Mecosta
County.
*For the purpose of this power
point we will only show examples
for the top three causes of
morbidity & mortality in Mecosta.

Plan: Primary Prevention Services
Heart Disease Provide Free Blood Pressure Screenings
Free Cholesterol Quick Tests
Free Risk Factor Assessment
Education
Proper Exercise & Nutrition According to American Heart Association
Guidelines
Stress Reduction
Early Signs & Symptoms of Heart Attack

Plan: Primary Prevention Services
Cancer
Assessment of Risk Factors (Genetics, Lifestyle, & Environmental)
Education
Different Types of Cancer
Nutrition
Exercise
Early Detection: Signs & Symptoms
Self Screening Tools
(Self-Breast & Testicular Exams)
Smoking Cessation

Plan: Primary Prevention Services
Stroke
Risk Assessment (Genetics, Lifestyle, Environmental)
Education Nutrition & Exercise
Smoking Cessation
Stress Reduction
Early Detection-Signs & Symptoms!!
Blurred Vision

Plan: Secondary Prevention
“Secondary prevention is aimed at early detection and prompt treatment either to cure a disease as early as possible or to slow its progression, thereby preventing disability or complications” (Fisher, pg. 171).
Examples:
1.Preventing transmission of a communicable disease
2. Preventing or slowing of a disease
3. Preventing complications from a disease
(Fisher, pg. 171)
Plan: Tertiary Prevention
“ Tertiary prevention is aimed at limiting existing disability in persons in the early stages of disease and at providing rehabilitation for person’s who have experienced a loss of function resulting from a disease process or injury” (Fisher, pg. 171).
We need to provide:
Education to people
Nursing Care
Referrals
Resources

Plan
Offer Incentives for Future HCP’s to
Practice in the Mecosta County area.
Rationale: Through offering Incentives for HCP’s to practice in the
Mecosta area, one can increase the number of HCP’s to residents.

Reason Healthcare Providers Avoid
Practicing in Rural Areas
“The reasons given for not wanting to practice
in rural areas had less to do with the amenities
or social activities associated with urban areas
than with the patient base (large numbers of
uninsured or poor people) or the quality of the
facilities” (Health Professions Resource Center,
2006).

Plan: Recruitment & Retention
Recruitment and Retention of HCP’s is a
challenge for rural areas.
Nationally, there is a projected provider shortage
along with a projected increase in demand for
services, as the baby-boomer population reaches
retirement age.
Recruitment and Retention was identified as an
issue in all three components of the rural
community health assessment (Michigan Center for Rural Health, 2008, pg.23)

The Michigan Center for Rural Health has developed a plan to increase the
number of practicing health professionals in rural Michigan
Increase by 20% the number of rural health sites approved as Michigan State Loan
Repayment sites.
Increase by 10% the number of rural providers participating in the State Loan
Repayment Program. (MSLRP).
Increase by 20% the number of rural health sites approved as
National Health Service Corps sites; from 127 to 152.
Increase by 10% the number of National Health Service Corps
provider placements at rural sites.
Develop a retention model to assist rural hospitals, certified rural health clinics and
federally qualified health centers in their retention planning efforts.
Develop a rural component to the “Practice Michigan” campaign to promote the
benefits and positive aspects of rural practice.
(Michigan Center for Rural Health, 2008, pg.29-30)
Plan: Recruitment & Retention
The Michigan Center for Rural Health

Measurable Outcomes
Increased number of HCP’s in Mecosta County
Decrease in HCP to Patient Ratio.
Attendance Rate of > 60% to Local Prevention
Seminars & Screenings.
Less admissions into the hospital.

The Availability of Health
Care in rural areas is
challenging for health care
providers to promote
primary care and
preventative measures.

The community health
nurse can use the statistics
from previous years to
observe the trends and the
growing need for
interventions.
(Beringer, 2010)

Intervention
“An intervention is an
interference so as to
modify a process or
situation.” “An intervention is
designed to improve the
health of a patient or
change the conditions
which have negative
impact on the well-being
of the patient.” (Farlex, 2010)
The State Rural
Health Plan
serves as a
guide to aid in
providing care
to rural areas in
Michigan.
The approved goals by the Advisory Group for
rural residents are:
Access to dental care
Access to mental health
Access to primary care & specialty care
Practicing health professionals
Targeted education & training opportunities
The number of applications and admissions into health professions & training programs
The rate of obesity
The activity level of the population
Healthy eating in the community
The communities can use this plan as a
guide to develop interventions that
increase care to patients in rural areas
(Michigan Center for Rural Health, 2008, pp. 1-2)

Available Services In Mecosta County
34 Physicians
Hospice care
Nursing Care
Social services
Home care aide or homemaker services
Volunteer care
Physical, occupational, and/or speech therapy
Respite care
Grief support
Spiritual care
EMS Services:
(Jacobson, 2010)
Recruitment & Retention in Mecosta County
☼Recognize the shortage of health care providers
☼Evaluating the ratio of health care providers to the number of patients
☼Showcase the environment to draw health care workers to the area
☼Describe the different religious organization
☼Illustrate the different cultural groups in the area
☼Highlight the civic activates and cultural arts available in the area
☼Offer incentives for relocation
☼Illustrate the recreation activities that are offered in the area

Health Care Providers
Mecosta County has one 74 bed hospital
located 45 minutes North of Grand Rapids
Mecosta County Medical Center. (2010)
Mecosta County Medical Center provides services in:
●Maternity
●Cardiopulmonary & Rehabilitation
●Critical Care Unit
●Emergency Care
●Home Health Care
●Inpatient Medical Rehabilitation
●Laboratory Services
●Medical Imaging
●Nutrition and Dietary Services
●Occupational Medicine
●Outpatient Physical Rehabilitation
●Pharmacy
●Specialty Clinics
●Surgical Services
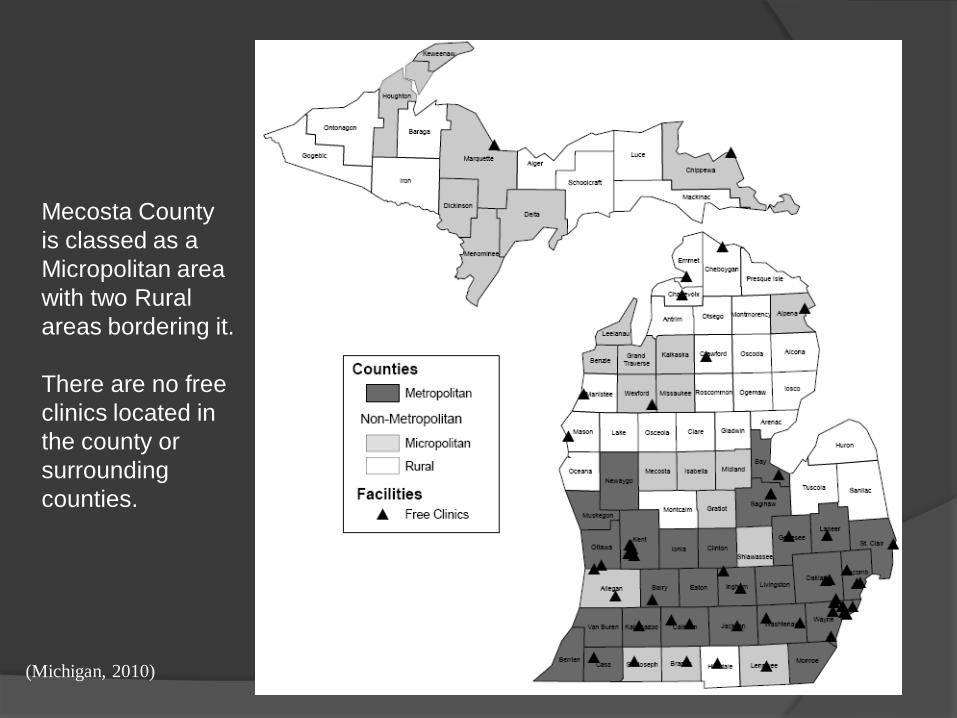
Mecosta County
is classed as a
Micropolitan area
with two Rural
areas bordering it.
There are no free
clinics located in
the county or
surrounding
counties.
(Michigan, 2010)

The shortage of Health Care Providers is an
issue with today’s economy. Extending care
and services suffer due to cut back in the
budgets. The existing care institutions
needs to reach out to communities and other
business’s to facilitate the growing need for
health care providers and facilities.
Community involvement can increase
awareness of services in the community.
Showcasing Mecosta County
Mecosta County offers diverse terrain
Rolling hills
Marsh land for wild life
(Ertman, 2010)
Northern woods for stunning color
The Congregations In Mecosta County Allows For Varied
Religious Practice
United Methodist Church - 9
Lutheran Church - 2
United Church of Christ - 1
The Wesleyan Church - 3
Evangelical Lutheran Church in America - 1
Evangelical Free Church of America - 1
Free Methodist Church of North America - 4
Christian Churches and Churches of Christ - 3
Wisconsin Evangelical Lutheran Synod - 2
Church of Jesus Christ of Latter-day Saints - 1
Episcopal Church - 1
Presbyterian Church - 1
Church of God – 3
Old Order Amish - 3
Christian Reformed Church in North -America - 1
General Association of Regular Baptist Churches - 1
Assemblies of God - 2
Church of God (Cleveland, Tennessee) - 1
Conservative Baptist Association of America - 1
Church of the Nazarene - 1
Community Church of Christ - 1
Seventh-Day Adventist Church - 1
Sothern Baptist Convention - 1
Churches of Christy - 1
Baha’i – 15 members (no congregations)
Salvation Army - 1
Buddhists - 1
(Rousseau, 2010)

Population Affiliation Percentage
in Mecosta County
(Rousseau, 2010)

Mecosta County Is The Home To Many Different Cultures
And The Most Common Reported Are:
• German (26%)
• English (11%)
• United States or American (10%)
• Irish (9%)
• Polish (5%)
• Dutch (4%)
• French (except Basque) (4%)
Amish also reside in the area
(Dixon, 2010)

Highlighting The Activities That Are Provided In The Community
Can Enhance The Benefits Of Living In A Small Rural Area
Monthly Rise ‘N’ Shine’s
Monthly Business After Hours
Mecosta County Community and Family EXPO!
Pioneer Group Chamber Open
Annual Morley Free Festival / Bike Show
Annual Labor Day Arts and Crafts Festival
Bulldog Bonanza
Annual Mecosta County Community Holiday Gala
Showing the activities that are monthly & annually gives a feel of community closeness
( Rousseau, 2010)

Offering Incentives For Relocation Can Draw New Health
Care Providers To An Area
▪Institutions sometimes offer incentives
with signed contracts that will insure a
bonus after so many years of service.
▪Repaying student loans
▪Health care workers that work in the more
remote areas receive higher pay
(Shinohara, 2010)

Mecosta County Offers A Wide Range Of Recreation For Everyone
☺City Parks - 14
☺Lakes and Rivers - 5
☺Hiking
☺Camping – x3 local areas
☺Mountain Biking – x4 different areas
☺Ferris State Racquet & Fitness Center
☺Hunting
☺Snowmobiling
☺Cross Country Skiing Francik, 2010

Promotion Of Healthy Lifestyle Decreases
The Work Load Of Health Care Providers
Interventions are needed to promote good health in the community
Primary, secondary, and tertiary preventive care
is ideal, but the services that provide this care
may be hard for rural areas to access.
⌂ Reaching out to the local venues for participation
⌂ Provide health fairs
⌂ Promote community physical activities
⌂ Provide screening services in different areas of the community
⌂ Provide workshops on good nutrition
⌂ Provide stress management classes
⌂ Provide information on social support in the community
(Pender, 2006)
Ways to reach out and help other people

Primary Medical Care Providers
53 free clinics are located in Michigan with only 10 located in the northern
part of Michigan
Air Ambulance is used in many areas to transport critical patients to qualified Medical Centers
(Michigan Center for Rural Health, 2008)
Provide primary care that is reimbursed by health care payers
Eight counties in the northern part of Michigan have no hospitals. Out-patient
clinics is the only available health care facility
Health departments are shared with other larger districts
There are 7 sites of Federally Qualified health Centers located in Micropolitan areas
with 36 sites in rural areas in Michigan
There are three Rural Health Clinics in Mecosta County and 156 in the state
Objectives ◘ Form a committee to target healthy eating and fitness to decease
heart disease
Encourage school participation by:
Replacing vending machine with water & health alternatives
Encourage the use of healthy models when preparing lunches
Have healthy eating seminars for families
Encourage the local farmers and markets to form a partnership with
school for lower rates for food purchases
Develop exercise programs that include the whole family at
affordable rates
Encourage a partnership with Ferris State Racquet and Fitness Center
Decreasing health problems decreases the work load of HCP’s
(Michigan Center for Rural Health, 2008)

Increase Education
◘ Provide adequate educational material to the community
Increase awareness of eating healthy and eating fruits and vegetables
Provide educational means at different times of the day and week to facilitate
the whole community
Develop web resources with learning material, premade meal planning, quick and
easy to follow recipes, tips on sales and coupons, and interactive games on
healthy living for the family
Advertise with healthy eating commercials on television and the radio
Provide links on the web site to state-wide nutritional sites
(Michigan Center for Rural Health, 2008)
Provide informational hotlines for the community to call

Vulnerable members of the community
◘ Identify vulnerable members of the community
Form a committee to identify the vulnerable members of the community
Identify the members that are elderly, handicapped, poverty stricken, and
people with lack of transportation
Provide information on Meals on Wheels, Women Infant and Children (WIC),
and transportation alternatives schedules
Encourage local venues to assist with transportation, shopping, and
companionship,
(Michigan Center for Rural Health, 2008)
An evaluation is a critical appraisal
or assessment; a judgment of the
value, worth, character or
effectiveness of that which is being
assessed (Farlex, 2010).
Evaluation
Evaluations are needed in
every plan of care to see if
the plan is working
There are five steps in the evaluation process
► Plan the evaluation
► Collect evaluation data
► Analyze the data
► Report the evaluation
► Implement the results

The plan is evaluated periodically
(depending on the time set in the
beginning) during the course of the
process.
Our evaluation would consist of:
∆ Did the number of HCP’s increase during the time frame?
∆ If the number of HCP’s increased did the work load decrease?
∆ Did attendance increase at the screenings, seminars, and other events held?
∆ Did the hospital admissions decrease and was it due to our interventions?

Did the number of HCP’s increase during the time frame? ●If the number of HCP’s did not increase, different means of recruiting,
incentives and advertising may be needed.
If the number of HCP’s increased, did the work load decrease?
●This is based on the increase of the HCP’s. If the number of HCP’s did not
increase the work load would not decrease
●If the number of HCP’s increased, did the work load decrease?
Outcomes
●If the attendance increased and was above 60% as planned, what was more
beneficial the screenings, seminars, and/or the events held?
●If the attendance was below 60%, reevaluation of the area held in, time held,
and type of screening, seminar, or event was held.
●Did hospital admission drop and what type of admission have decreased.
●If hospital admissions did not drop, what type of patients continue to get admitted?
Did attendance increase at the screenings, seminars, and events held?
Did the hospital admissions decrease and was it due to our interventions?

Conclusions and Recommendations
Conclusions from the data would
be formed with all involved parties
&
Recommendations are made and
changes are made if needed

Federal Authority in Health Care
Responsible for protecting the health of its population.
Regulates, interprets the law, and administers services mandated by law.
Responsible for supervision and compliance with health law regulations.
Involved indirect services.
Maurer & Smith, 2009, p. 64
State Authority in Health Care
Finances care of the poor and disabled.
Manages Medicaid programs.
Operates state mental health hospitals.
Oversees licensure and regulation of health providers and facilities.
Attempts to control health care costs.
Regulates insurance companies.
Maurer & Smith, 2009, p. 68

County Authority
Health department
Special Supplemental Nutrition Program for Women, Infants, and Children (WIC)
State Children's Health Insurance Program (SCHIP)
School health programs
Mental health programs
Community health education
Maurer & Smith, 2009, p. 69

Hypothetical State Superagency
Incorporating the Health Department
Maurer & Smith, 2009, p. 69

0 20 40 60 80
100 62
81 80 80 84 66
79 61
81
Race/Ethnicity
Race/Ethnicity
Percentage
83 percent of persons under age 65 years were covered by health insurance in 1997.
Note: Age adjusted to the year 2000 standard population
Increase the Number of People with Health Insurance
(Healthy, 2010)

0
10
20
30
40
50
60
70
80
90
FEMALE MALE
FEMALE
MALE
Increase the Number of People with Health Insurance
Female vs. Male
83 percent of persons under age 65 years were covered by health insurance in 1997.
Note: Age adjusted to the year 2000 standard population
(Healthy, 2010)

0%
20%
40%
60%
80%
100%
66% 69%
91% 83%
80% 83% 83%
FAMILY INCOME LEVEL
FAMILY INCOME LEVEL
Increase the
Number of
People with
Health
Insurance at
the Family
Level
83 percent of persons
under age 65 years were
covered by health
insurance in 1997.
Note: Age adjusted to the
year 2000 standard
population (Healthy, 2010)

(Wolf, 2010)
Percentage of Uninsured Rises In USA

Uninsured Increase Cost to Area
Hospitals in 2000
Hospital
Name
Uninsured
Patient Pay Costs
Uninsured State
Costs
Total Uninsured
Costs
Uninsured Payments
Net
Uninsured Costs
Mecosta County
General Hospital
809,784
0
809,784
15,455
794,329
Memorial Medical
Center of West
Michigan
958,577
0
1,123,980
953,934
170,046
Metropolitan
Hospital, Grand
Rapids Michigan
7,861,364
0
8,604,570
1,028,514
7,576,056
(Citizens, 2000)
Public Policy Implications Form a committee/coalition to work with local
agencies to support the recruitment of primary care providers.
Offer incentives to attract primary health care providers.
Increase the availability of free health clinics.
Offer primary care physicians financial support in caring for those who are uninsured to prevent and manage chronic illness.

Support Groups Healthy People 2010
American Nurses Association (ANA)
Institute of Medicine
State Children’s Health Insurance Program (SCHIP)
American College of Health Care Executives

Founded on data that enable progress and trends to be
tracked, Healthy People 2010 provides a set of 10-year
evidence-based objectives for improving the health of all
Americans.
The first goal of Healthy People 2010 is to help individuals of all
ages increase life expectancy and improve their quality of life.
The second goal of Healthy People 2010 is to eliminate health
disparities among different segments of the population.
(Healthy, 2010)
Healthy People 2010
Supports Access to Quality Health Care

American Nurses Association ANA believes health care is a basic human right that should be provided to all
individuals.
ANA believes that the health care system must ensure access, which means health care services must be affordable, available and acceptable.
ANA believes that all individuals should have access to a standard package of essential health care services.
ANA believes the health care system must be redirected from the overuse of more expensive, technology‐driven, hospital‐based services to a more balanced approach with greater emphasis on community‐based care and preventive services.
ANA supports incorporating into health policy changes the six major aims identified by the Institute of Medicine – safe, effective, patient‐centered, timely, efficient and equitable. (New Hampshire Nurses Association, 2010)
Institute of Medicine
Mission Statement is to serve as adviser to the nation to improve health.
The IOM asks and answers the nation’s most pressing questions about health and health care. Our aim is to help those in government and the private sector make informed health decisions by providing evidence upon which they can rely. Each year, more than 2,000 individuals, members, and nonmembers volunteer their time, knowledge, and expertise to advance the nation’s health through the work of the IOM.
Many of the studies that the IOM undertakes begin as specific mandates from Congress; still others are requested by federal agencies and independent organizations. While our expert, consensus committees are vital to our advisory role, the IOM also convenes a series of forums, roundtables, and standing committees, as well as other activities, to facilitate discussion, discovery, and critical, cross-disciplinary thinking. (National Academy of Sciences, 2010)
(National Academy of Science, 2010)

State Children’s Health Insurance
Program
The State Children's Health Insurance
Program, or SCHIP, was established by
the federal government ten years ago to
provide health insurance to children in
families at or below 200 percent of the
federal poverty line.
(National Center for Public Policy Research, 2010)

American College of Healthcare
Executives
An important role for healthcare executives has
always been to translate social values into workable
healthcare programs. In keeping with this role,
healthcare executives have the opportunity to
participate in public dialogue about new ways to
finance and deliver healthcare so no one is denied
care because of the inability to pay. (American
College of Healthcare Executives, 2008)

Healthcare Executives Developing and communicating access-to-care policies within their organizations
and to the community.
Managing their organizations efficiently to help underwrite healthcare costs
associated with uncompensated and undercompensated care.
Collaborating with other healthcare providers in their community to develop
shared approaches to ensure access to care.
Encouraging and assisting trade and other professional associations to take
proactive roles in access-to-care issues.
Promoting shared leadership and funding responsibilities among government,
healthcare organizations, employers, private insurers and consumers.
Organizing grassroots advocacy efforts to secure needed funding from local, state
and federal government bodies.
Organizing or participating in local, state and regional initiatives to resolve access
problems.
Spearheading discussions with key decision makers (e.g., legislators) and key
stakeholders (e.g., public agencies) to identify community health priorities so
available resources can be allocated equitably and effectively. (American College of Healthcare
Executives, 2008).

Recommendations Based on the provider responses, some possible ways to increase the supply of
health care professionals in rural areas include:
• Increasing the interest of high school students in medical professions,
especially in the rural areas, because providers who were raised in a rural area
appear more likely to practice in a rural area.
• Retaining students as they progress along the education pipeline from high
school through residency.
• Providing more incentives such as loan repayment.
• Providing incentives specifically targeted to those who will practice in rural
areas.
• Increasing awareness of the need in rural areas among healthcare providers
from other places.
• Promoting and advertising the positive aspects of living and working in rural
areas, including greater purchasing power.2
• Providing funds to upgrade the facilities and equipment in rural areas.
• Providing more opportunities for resident training.
(Health Professionals Resource Center, 2006)
Unsupportive Groups Adding health care providers can change the cost of providing
services to a community causes conflict due to over stretched budgets and lack of increased government assistance.
The following may object to changes that will bring health care providers to the community:
Consumers who have private insurance and do not want there taxes increased to support those who lack health care.
Providers who may have to care for the uninsured without proper compensation.
Maurer & Smith, 2009, p. 74

References
●American Nurses Association. (2010, July). Nursing Agenda Fro Health Care Reform. Retrieved November
20, 2010, from http://www.nhnurse.org
●Barnes, J., Barnett, L., Wightman, T., Emge, A., Johnson, S. (2008). Michigan strategic opportunities for rural health improvement. Michigan Center for Rural Health, April. Retrieved from www.mcrh.msu.edu.
●Beringer, P,.(2010). Mecosta county assessment people: demographics: population and trends per race, ages, and genders, including levels of education.. Ferris State University. www.ferris.edu
●Boughton, B. (2009). Improving Healthcare Access, Quality, and Efficiency: An Expert Interview with Public
Policy Analyst Robert Doherty. Retrieved November 19, 2010, from Medscape Medical News:
htt://www.medscape.com ● Citizens Research Council of Michigan. (2000). Components of Uninsured Costs of Individual Hospital for 2000 Listed by Health System. Retrieved November 21, 2010, from CRC Online Almanac: http://www.crcmich.org
●Dixon, B., (2010). Mecosta county assessment people: culture. Ferris State University. www.ferris.edu ●Ertman, H., (2010). Environment: environmental quality. Ferris State University. www.ferris.edu ●Farlex. (2010). The free dictionary. Retrieved November 24, 2010, from http://medical dictionary.thefreedictionary.com/evaluation
●Francik, D., (2010). Mecosta county recreation. Ferris State University. www.ferris.edu
●Health People 2010. (2010). Healthy People. Retrieved November 20, 2010, from http://www.healthypeople.gov
●Health Professions Resource Center. (2006, September). Recruitment and Retention of Health Care Providers in Texas. Retrieved November 19, 2010, from http://www.dshs.state.tx.us
●Jacobson, A., (2010) Social systems: types of health care providers. Ferris State University. www.ferris.edu ,
●Maurer, F. A. (2009). Community/Public Health nursing practice: Health for families and populations (4th ed.). St. Louis, MO: Elsevier Saunders.
●Mecosta County Medical Center. (2010). Advance care with a personal touch. Retrieved November 23, 2010, from http://www.mcmcbr.com/nb_links.asp#

●National Academy of Sciences. (2010, October 10). Institute of Medicene. Retrieved November 20, 2010, from
http://www.iom.edu
●National Center for Public Policy Research. (2007). SCHIP Information Center. Retrieved November 20, 2010,
from http://www.schip-info.org
●New Hampshire Nursing Association. (2010, July). Nursing Agenda For Health Care Reform. Retrieved
November 20, 2010, from http://www.nhnurse.org
●Wolf, R. (2010, September 17). Number of uninsured Americans rises to 50.7 million. Retrieved November 19,
2010, from USA Today: from http://usatoday.com
●Michigan Surgeon General’s Health Status Report. (2010). Healthy Michigan 2010. Retrieved from:
http://www.michigan.gov/documents/Healthy_Michigan_2010_1_88117_7.pdf
●Michigan State University Extension Team . (2007, January 27). Mecosta County Profile. Retrieved from
http://web1.msue.msu.edu/countyprofiles/mecosta/Mecosta.pdf
●Pender, N. J., Murdaugh, C. L., & Parsons, M. A. (2006). Health Promotion in Nursing Practice. Upper Saddler
River: Pearson Education, Inc.
●Rousseau, S., (2010). Mecosta county religious system. Ferris State University. www.ferris.edu
●US Census Bureau . (2002, April 30). Census 2000 Urban and Rural Classification. Retrieved from
http://www.census.gov/geo/www/ua/ua_2k.html
●US Census Bureau. (2007, April). United States Summary: 2000. Population and Housing Unit Counts. Retrieved
from www.census.gov/census2000/pubs/phc-3.html
●Shinohara, R. (2010, February 15). Group advocates incentive to lure health care workers. Anchorage Daily
News. Retrieved from http://www.adn.com