a clinical pharmacology perspective
TRANSCRIPT

A Clinical Pharmacology Perspective
diazepam 10mg2 tabs, stat, po

Drug Interactions
Matt DoogueChristchurch, NZ

n When one drug alters the effect of another drugn Interactions between current medsn Starting new medicinesn Tools for DDIs Ln My clinical approach to DDIs
Drug-Drug Interaction (DDI)

Drug-Drug Interaction (DDI)
n When one drug alters the effect of another drugn Increase effectn Decrease effect
n Can be beneficial or harmful.

Assessing Drug Drug Interactions1. Interactions between existing drugs in a given patient
have already occurred -relevant to diagnoses
2. Potential pharmacodynamic DDIs can be recognised by knowledge of the pharmacological effects of drugs and of patient physiology together
3. Drugs with a narrow therapeutic index are more likely to be ‘objects’ of PK-DDIs.
4. A small number of drugs are important ‘perpetrators’ of PK-DDIs.
5. Stopping a drug is a prescribing decision that may cause a DDI.

100%
10
Number of drugs
50%
5
Chance of DDI

Clinical Relevance
n Common, often ‘mild’, often missedn May be
n beneficial or harmful,
n increase or decrease effect
n Interindividual variabilityn eg. frailty, organ function,

Actions1. Change drug
2. Change dose
3. Change monitoring


Drug Drug Interactions
• Common
• Cause harm
• Poorly anticipated
• Current predictive tools are of limited utility

Potential DDIsA
B
C
D
E
F
G
A B C D E F GABCDEFG
21 combinations


Existing Drugs New Drugs
Potential DDIs
A
B
C
D
E
F
G
Premise 1: Interactions between existing drugshave already happened

n Relevant to differential diagnosisIs this patient presenting because of…
n Adverse effect?n Treatment failure?
Interactions between existing drugshave already happened

Existing Drugs
Actual DDIs
Two questionsn Is there harm?n Is there benefit?
A
B
C
D
E

Existing Drugs
Actual DDIs
Is there harm?n Is the presentation due to
(or contributed to by) their medicines?
n Are there any ADRs I should look for?
n If yes, is this because of an interaction?
A
B
C
D
E

Existing Drugs
Actual DDIs
Is there benefit?n Is the presentation due to
(or contributed to by) treatment failure?
n If yes, is this because of an interaction?
A
B
C
D
E

Existing Drugs New Drugs
Potential DDIs
A
B
C
D
E
F
G
21 11 combinations

Potential DDIsA B C D E F G
ABCDEFG

Classifying DDIs

Black Box
Clinical Pharmacology

Prescription
Concentration
PatientHealth
concentration at target
affinity to target
molecular effect/s
physiological effect/s
Dose
Effect/s
Pharmacokinetics
Pharmacodynamics
absorptionfirst pass metabolism
± activation
Bioavailability
metabolismexcretion
Clearance
Administrationadherence route
Distributiondiffusiontransport

Classifying DDIsPharmacokinetic
- bioavailability: absorption, first pass metabolism- clearance: metabolic, renal, other- distribution: trans-membrane transport
Pharmacodynamic- mode: physiological effect- mechanism: molecular target
Other- pharmaceutic - behavioural

Classifying DDIsPharmacokinetic
- bioavailability: absorption, first pass metabolism- clearance: metabolic, renal, other- distribution: trans-membrane transport
Pharmacodynamic- mode: physiological effect- mechanism: molecular target
Other- pharmaceutic - behavioural

Potential Pharmacodyamic Interactions?
• Potential pharmacodynamic DDIs can be recognised based on knowledge of the pharmacological effects of drugs andpatient physiology together
• Consider the drugs’ effects - additive or opposing

Additive EffectsMay be beneficialn ACE inhibitor + thiazide in hypertensionn Metformin + SGLT2 inhibitor in diabetes
n mycophenolate + prednisone + tacrolimus in renal transplant
May be harmfuln CNS depression e.g. alcohol + benzodiazepines
n Serotonin toxicity e.g. SSRIs + tramadol
n QTc prolongation e.g. erythromycin + antipsychotics

Opposing Effects
Molecularn b-blocker + b-agonist
n morphine + naloxone
Physiologicaln NSAIDs + antihypertensivesÞ ¯ antihypertensive effects
n Immunosuppressants + vaccines
Þ failure to seroconvert

Classifying DDIsPharmacokinetic
- bioavailability: absorption, first pass metabolism- clearance: metabolic, renal, other- distribution: trans-membrane transport
Pharmacodynamic- mode: physiological effect- mechanism: molecular target
Other- pharmaceutic - behavioural

Pharmaceutic InteractionsHappen outside the body - drugs/solutions/equipment � inactivation or
precipitation
Only admix when interactions are known to be absentask the pharmacist
Examples:• ciprofloxacin IV + amoxicillin IV = INCOMPATIBLE• insulin adsorbs to plastic IV lines/bags• phenytoin precipitates in solutions pH<7 e.g. D5W

Classifying DDIsPharmacokinetic
- bioavailability: absorption, first pass metabolism- clearance: metabolic, renal, other- distribution: trans-membrane transport
Pharmacodynamic- mode: physiological effect- mechanism: molecular target
Other- pharmaceutic - behavioural

Pharmacokinetic DDIs (PKDDIs)
A “perpetrator” drug causes a change in concentration of a “object” drug with clinical consequences.
Premise 2: If clinical consequences are unlikely PKDDIs are not important
2 - fold concentration change

Concentration mg/L = Dose mg/24hr Clearance x F L/hr
time
conc
entra
tion

narrow therapeutic index
time
conc
entra
tion

NarrowPerpetrator
WideNon perpetrator
Object drugtherapeutic Index?
Perpetrator druginducer or inhibitor?
Probable
Unlikely
Drug Interaction?
Possible

Are there important
perpetrators or objects of
PKDDIs?
IdentifyNEW DRUG PAIRS
that include perpetratorOR object drugs(s)
EstimatePK change
to the object drugof each pair
Considerlikely clinical consequences
of the PK changesfor that patient
PK-interactionunlikely
yes
no

www.pkis.org

Narrow Therapeutic Index Drug Classes
Drug class ExampleAnticoagulants warfarinImmunosuppressants tacrolimusAntiepileptics phenytoinAntiarrhythmics amiodaroneAntineoplastics docetaxel, imatinib
Therapeutic index: • easier to recognise than define,• would doubling or halving the dose of this drug
have a major effect on this patient?• the vulnerability of the patient
- affects the dose–response relationship.
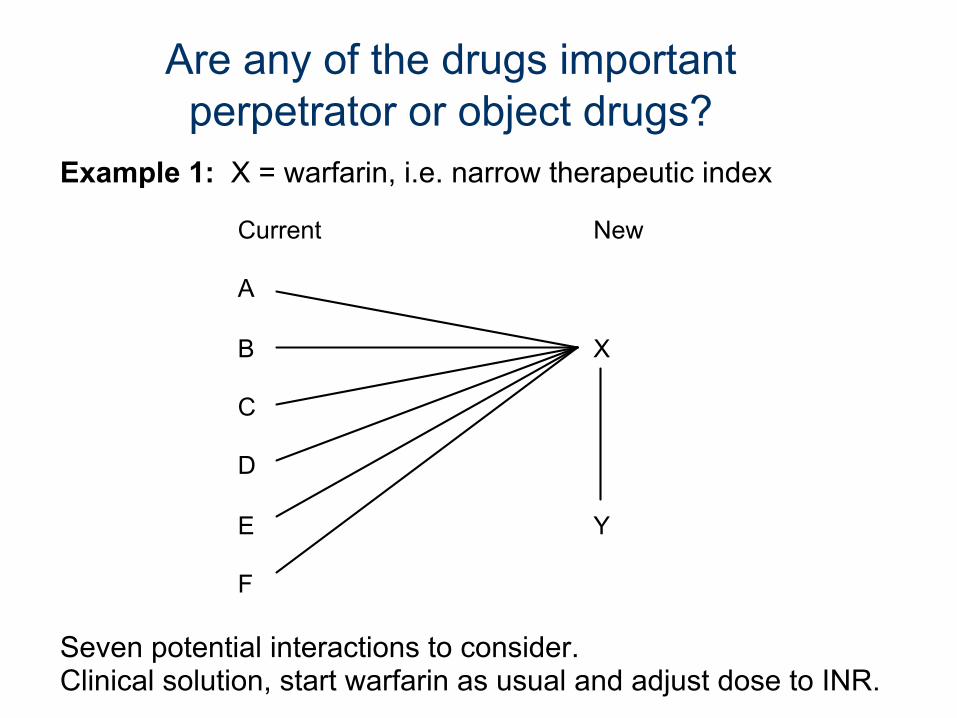
Example 1: X = warfarin, i.e. narrow therapeutic index Current New
A
B X
C
D
E Y
F
Seven potential interactions to consider. Clinical solution, start warfarin as usual and adjust dose to INR.
Are any of the drugs important perpetrator or object drugs?

Example 2: B = warfarin, i.e. narrow therapeutic index Current New
A
B X
C
D
E Y
F
Two potential interactions to consider. Clinical solution, start new drugs, adjust warfarin dose to INR.
Are any of the drugs important perpetrator or object drugs?

Are any of the drugs important perpetrator or object drugs?
Example 3: X = rifampacin an important enzyme inducer. Current New
A
B X
C
D
E Y
F
Need to consider 7 potential DDIs1. High risk - ?alternative drug2. Consider each pair and select doses and monitoring

Are any of the drugs important perpetrator or object drugs?
Example 4: B = rifampacin an important enzyme inducer. Current New
A
B X
C
D
E Y
F
Two potential interactions to consider. Clinical solution, consider potential effect of rifampacin on X & Y
(e.g. if renal clearance no problem). Select initial doses,
review and adjust doses based on appropriate biomarkers.

What I do
• How is the patient?– Any adverse effects or treatment failure?
• Group medicines by effects– What are the PD interactions?
• Are there any major inducers or inhibitors?• For medicines I start, which of the patients
medicines might they interact with?• Monitor, monitor, monitor

Assessing Drug Drug Interactions1. Interactions between existing drugs in a given patient
have already occurred -relevant to diagnoses
2. Potential pharmacodynamic DDIs can be recognised by knowledge of the pharmacological effects of drugs and of patient physiology together
3. Drugs with a narrow therapeutic index are more likely to be ‘objects’ of PK-DDIs.
4. A small number of drugs are important ‘perpetrators’ of PK-DDIs.
5. Stopping a drug is a prescribing decision that may cause a DDI.

We are all individuals