a boy with fever, hypertension and impaired renal function · widal’s test vdrl monospot, ebv...
TRANSCRIPT
A boy with fever, hypertension and impaired renal function
DEPARTMENT OF PAEDIATRICS
QUEEN ELIZABETH HOSPITAL
One fine afternoon......
Consulted for…… M/12 years admitted to Adolescent ward
- Hypertension
- Proteinuria
Background information 12 years old boy
Good past health
Immunisation up to date
Strong family history of hypertension on paternal side
Height 160cm
Weight 75kg
BMI 29kg/m2
Background information Admitted to adolescent ward due to
◦ Abdominal pain with pyrexia of unknown origin
◦ P/E showed hepatosplenomegaly
◦ Extensive workup was performed with no cause found
Noted hypertension and proteinuria during hospitalization • SBP 160-180 mmHg
• DBP 110-120 mmHg
• Urine protein ++ and RBC trace/ +
Workup Creatinine 60-75 umol/L (eGFR 78-97ml/min/1.73m2)
Cortisol 513 nmol/ L (N 101 – 536)
TSH 1.05 mIU/ L (N 0.35 – 4.94)
Renin supine 2.75 ng/ml /hour (N 0.50 – 3.30)
Aldosterone supine 78 pmol/ L (N erect <= 583; supine values are on average 50% lower)
Echocardiogram: no coarctation of aorta; normal contractility; No LVH
Renal Doppler USG: no renal artery stenosis; kidneys normal in size
24 hour urine catecholamine: normal
Urine microscopy: nothing abnormal seen; culture negative
Workup Fasting glucose 5.6/5.3
OGTT: normal
HbA1C 5.1 normal
Lipid profile normal
Workup 24-hour urine:
◦ Protein 0.91 gram/ day (22.3mg/m2/hour)
◦ Albumin 477.5 mg/ day
◦ Creatinine 10.3 mmol/ day
Impression Hypertension
Proteinuria
Obesity
Strong family history of hypertension
PUO?
Elevated Creatinine?
Progress Started Norvasc 10mg daily with good BP control
24 hour BP (while on Norvasc 10mg daily) signified good control of hypertension
◦ Daytime average BP 114/77, MAP 89mmHg
◦ Nocturnal average BP 100/61, MAP 74mmHg
A course of antibiotics was started empirically
PUO spontaneously resolved
Patient discharged by parent team with follow-up in clinic
Upon follow-up…… BP partially controlled with Norvasc 10mg daily
Ramipril was added
Creatinine level was static 70-90umol/L
Further investigations ◦ Repeat 24 hour urine for creatinine, protein
◦ Repeat 24 hour blood pressure 6 months later
◦ MRI renal angiogram and captopril MAG3 scan were arranged
Four months later……
Fever again!
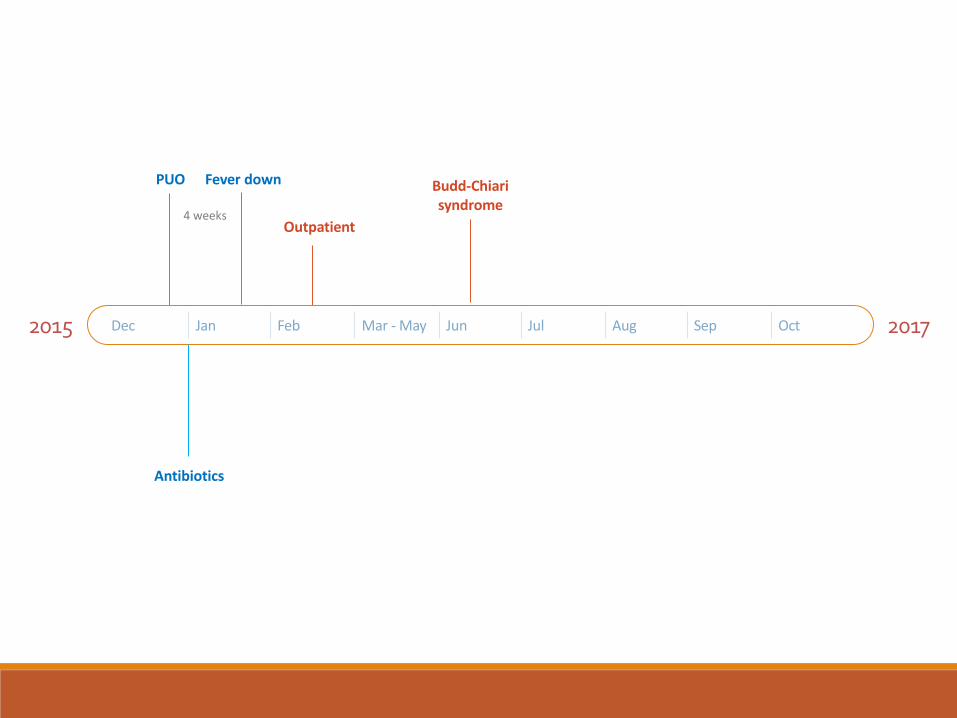
2015 2017 Dec Jan Feb Mar - May Jun Jul Aug Sep Oct
PUO
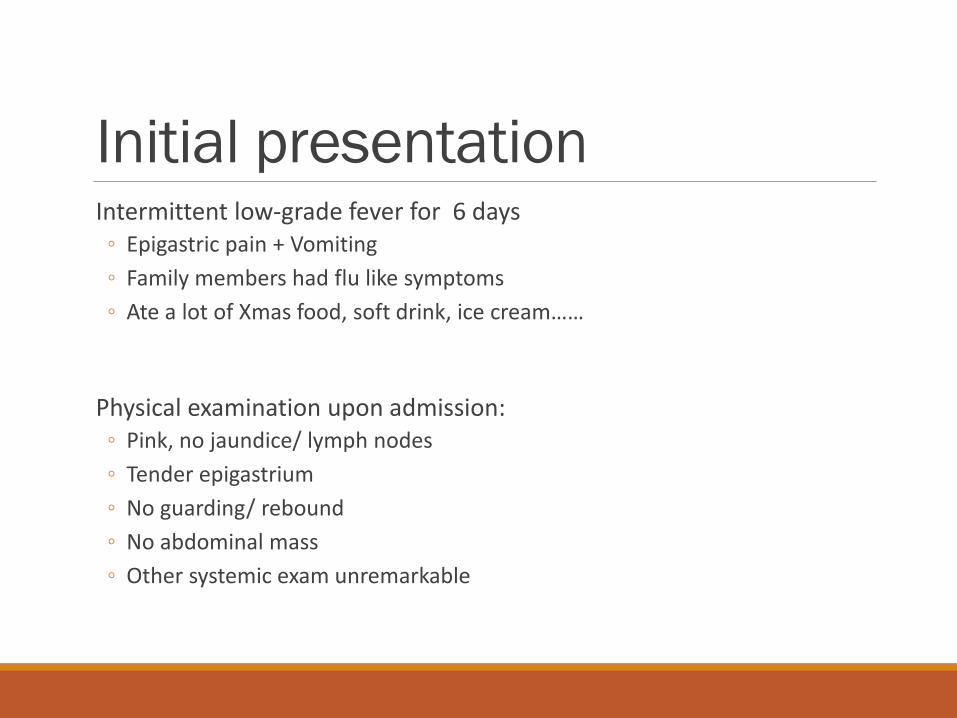
Initial presentation Intermittent low-grade fever for 6 days
◦ Epigastric pain + Vomiting
◦ Family members had flu like symptoms
◦ Ate a lot of Xmas food, soft drink, ice cream……
Physical examination upon admission: ◦ Pink, no jaundice/ lymph nodes
◦ Tender epigastrium
◦ No guarding/ rebound
◦ No abdominal mass
◦ Other systemic exam unremarkable
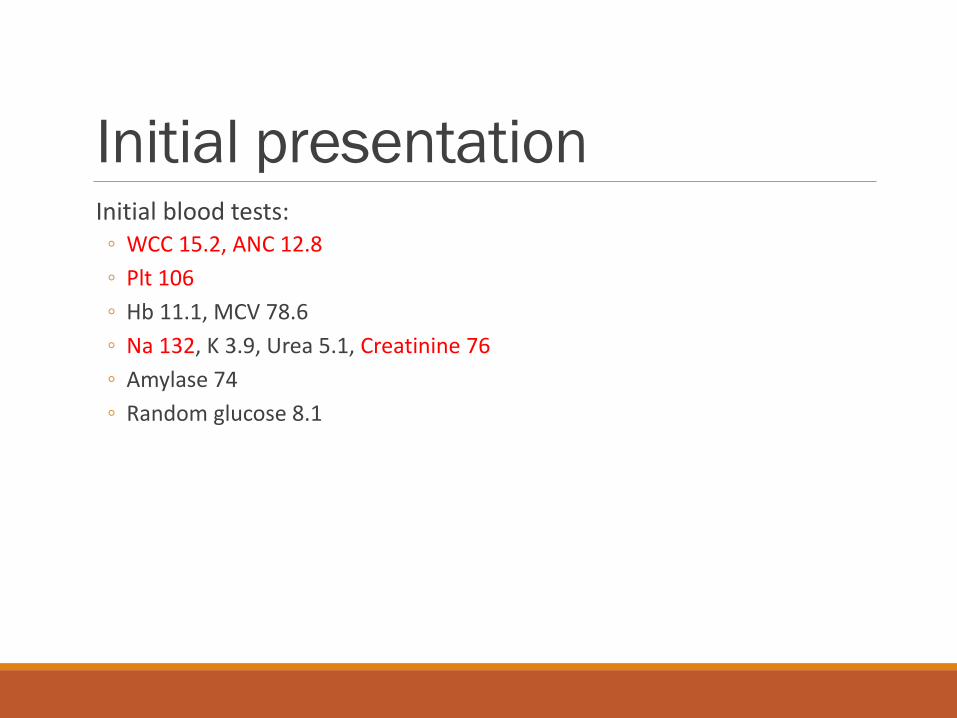
Initial presentation Initial blood tests:
◦ WCC 15.2, ANC 12.8
◦ Plt 106
◦ Hb 11.1, MCV 78.6
◦ Na 132, K 3.9, Urea 5.1, Creatinine 76
◦ Amylase 74
◦ Random glucose 8.1
Initial presentation Increasing epigastric pain on Day 2 admission
Repeated blood tests: ◦ WCC 15.0, ANC 11.3 ◦ Plt 106 84 ◦ Hb 11.1 10.4 ◦ ESR 115 ◦ CRP 131 ◦ PT 18.1, INR 1.51, APTT 62.4 ◦ D-dimer >5000, Fibrinogen >6 ◦ Na 135, K 4.2, Urea 5.0, Creatinine 70 ◦ CK 28, LDH 249 ◦ Total bilirubin 33 ◦ ALP 138, ALT 29, AST 26; GGT 106
Initial presentation Urgent USG abdomen on Day 2 admission:
◦ Splenomegaly, measuring ~14.8cm in length
◦ Normal liver, biliary tree, gallbladder, pancreas and kidneys
Started IV cefuroxime + metronidazole
Later switched to IV meropenem
Initial presentation Persistent symptoms
◦ Intermittent fever without obvious pattern ◦ Epigastric + RUQ pain ◦ Vomiting
Gradually enlarging hepatosplenomegaly ◦ smooth tender hepatomegaly 5-6cm below costal margin ◦ palpable spleen 5-6cm below costal margin
Blood tests showed persistent finding of: ◦ Low platelet and haemoglobin ◦ Elevated PT, APTT, D-dimer, fibrinogen ◦ Elevated inflammatory markers
Workup – infection Blood culture
Nasopharyngeal swab
Urine culture
Stool culture (bacterial, ova/cyst, clonorchis sinensis)
Mantoux, interferone gamma tuberculin stimulation
Widal’s test
VDRL
Monospot, EBV serology
Hepatitis serology
Anti-HIV
Urine CMV
Beta-1-D-glucan
Echocardiography
Workup – autoimmune ANA, anti-ENA, ANCA – negative
Direct coomb’s test – negative
C3 1.33 g/ L (N 0.80 – 1.70)
C4 0.14 g/ L (N 0.14 – 0.44)
Ig pattern: ◦ IgA 1.72 g/L (N 0.63 – 4.84)
◦ IgG 18.7 g/L (N 5.4 – 18.22)
◦ IgM 4.41 g/L (N 0.22 – 2.40)
Workup - malignancy Blood smear
◦ no blast cells, only occasional atypical lymphocytes
◦ RBC Rouleaux
◦ Occasional schistocytes
Bone marrow examination: ◦ active marrow with mild plasmacytosis
◦ Chromosome 46 XY, not diagnostic for haemic malignancy
◦ no cytogenetics abnormalities detected
AFP, HCG – normal
24 hour urine catecholamine – normal
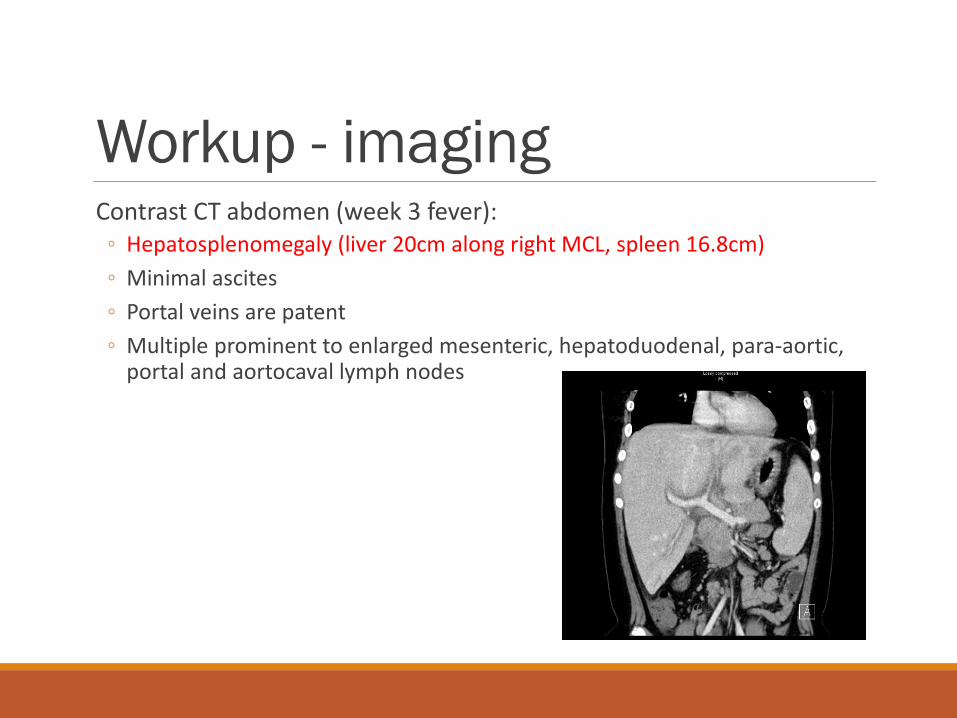
Workup - imaging Contrast CT abdomen (week 3 fever):
◦ Hepatosplenomegaly (liver 20cm along right MCL, spleen 16.8cm)
◦ Minimal ascites
◦ Portal veins are patent
◦ Multiple prominent to enlarged mesenteric, hepatoduodenal, para-aortic, portal and aortocaval lymph nodes
Workup - malignancy Contrast CT neck + thorax:
◦ No significant lymphadenopathy
◦ Prominent right level II lymph node of indeterminate significance
Cervical lymph node biopsy – high risk (lymph node closely abut the right common carotid artery)
Workup - miscellaneous Triglyceride, ferritin, NK cell count – normal
◦ Diagnostic criteria for HLH not met
Initial presentation Antibiotics given for 3 weeks
No steroid/ immunosuppressant were given
Day 24: fever down by lysis
Day 27: afebrile
Day 28: decreasing size of hepatosplenomegaly, CRP normalized
Day 32: platelet 179
Day 39: haemoglobin 11.0
2015 2017 Dec Jan Feb Mar - May Jun Jul Aug Sep Oct
PUO Fever down
Outpatient 4 weeks
Antibiotics
During out-patient follow-ups Late Feb – March,
◦ Intermittent fever for 2 weeks
Late March, ◦ Re-appearance of splenomegaly
◦ Platelet count 80-110
Booked follow-up USG abdomen
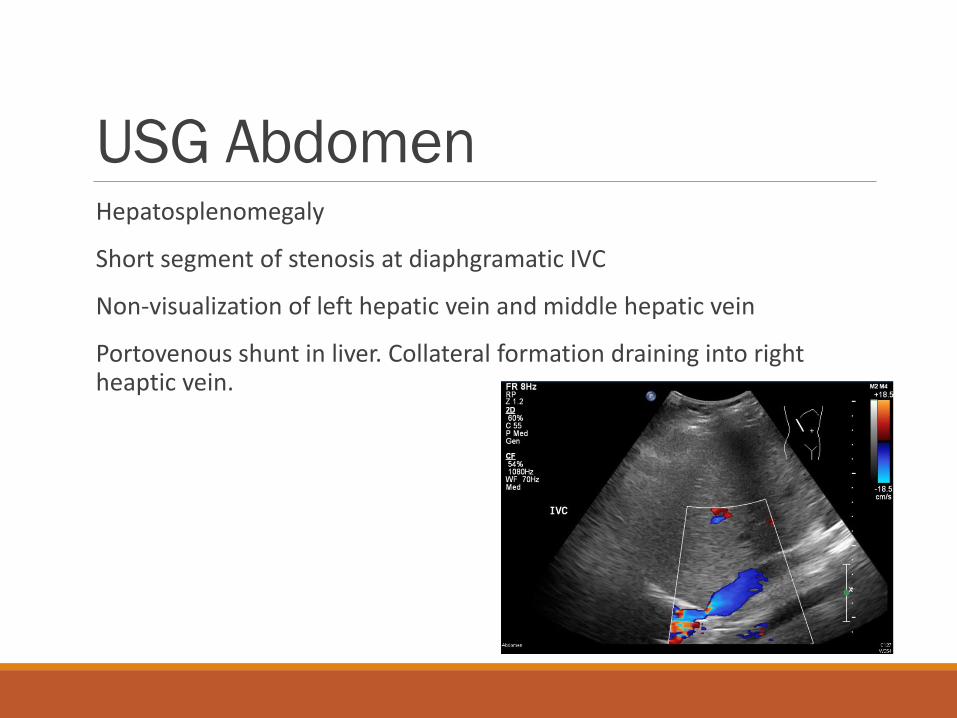
USG Abdomen Hepatosplenomegaly
Short segment of stenosis at diaphgramatic IVC
Non-visualization of left hepatic vein and middle hepatic vein
Portovenous shunt in liver. Collateral formation draining into right heaptic vein.
Budd-chiari syndrome!
2015 2017 Dec Jan Feb Mar - May Jun Jul Aug Sep Oct
PUO Fever down
Outpatient 4 weeks
Budd-Chiari syndrome
Antibiotics
Positive findings Fever
Hepatosplenomegaly
Hypertension, proteinuria
Thrombocytopenia with DIC-like picture
Rouleaux, schistocyte on blood smear
Borderline elevated creatinine
Mildly deranged LFT and mildly elevated bilirubin
Elevated ESR and CRP
Budd-chiari syndrome

Differential diagnosis?
Further workup Anti-cardiolipin IgM 9.2 MPL (N < 12.5)
Anti-cardiolipin IgG 98.3 GPL U/ ml (N ≤ 13.3)
Lupus anti-coagulant present
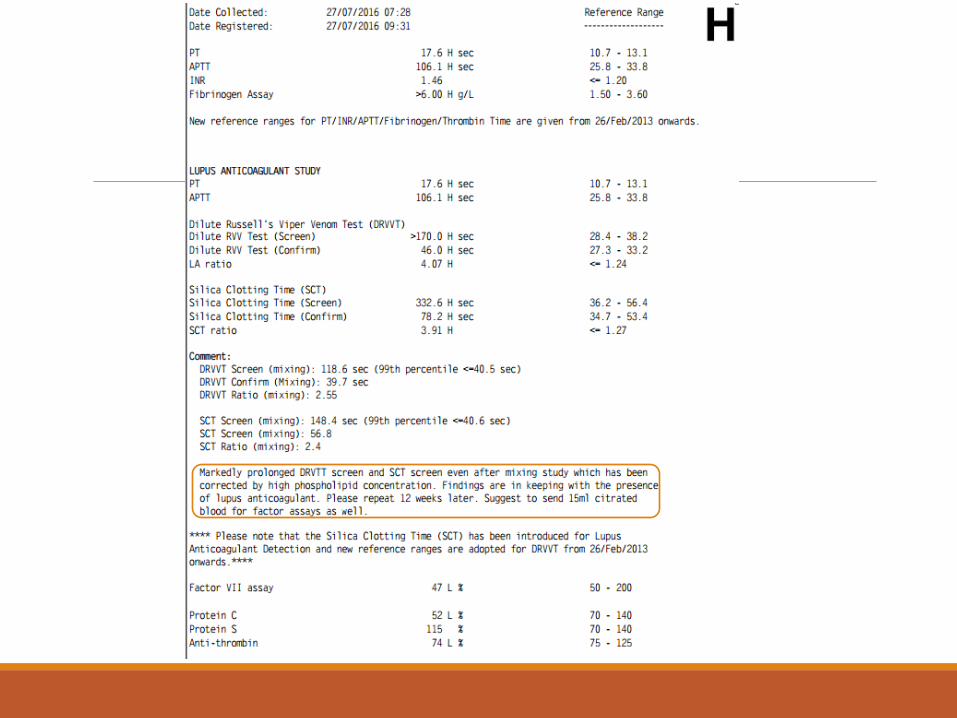
Further workup Protein C 52% (N 70 – 140)
Protein S 115% (N 70 – 140)
Anti-thrombin III 74% (N 75 – 125)
Factor VII 47% (N 50 – 200)

Further workup Proteinuria
Hypertension
Impaired renal function
Suspected underlying autoimmune disease
Decided to proceed to renal biopsy
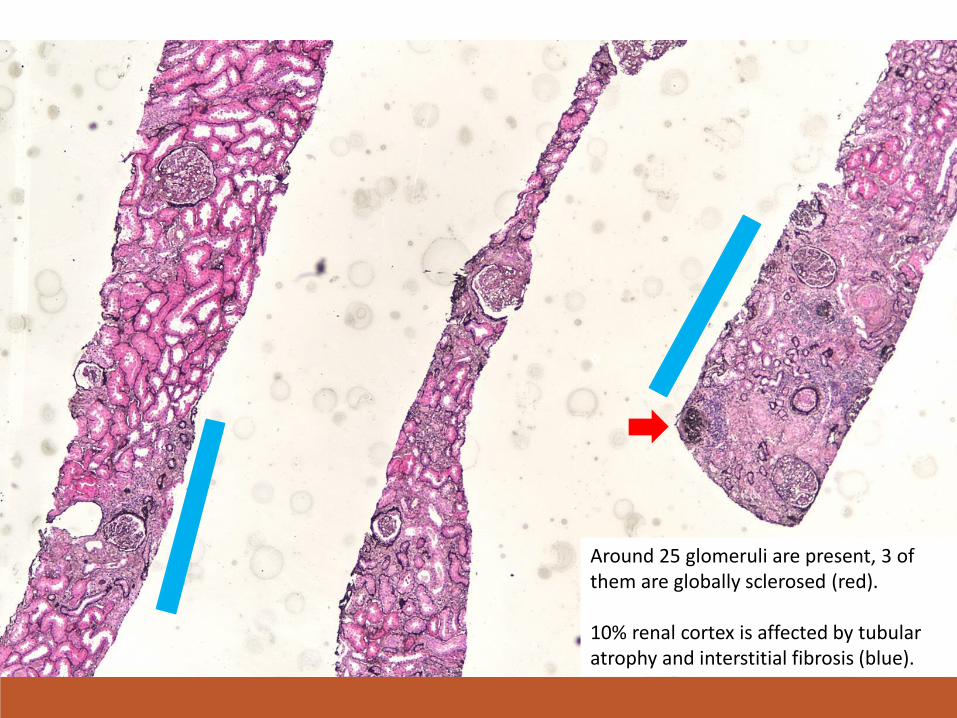
Around 25 glomeruli are present, 3 of them are globally sclerosed (red). 10% renal cortex is affected by tubular atrophy and interstitial fibrosis (blue).
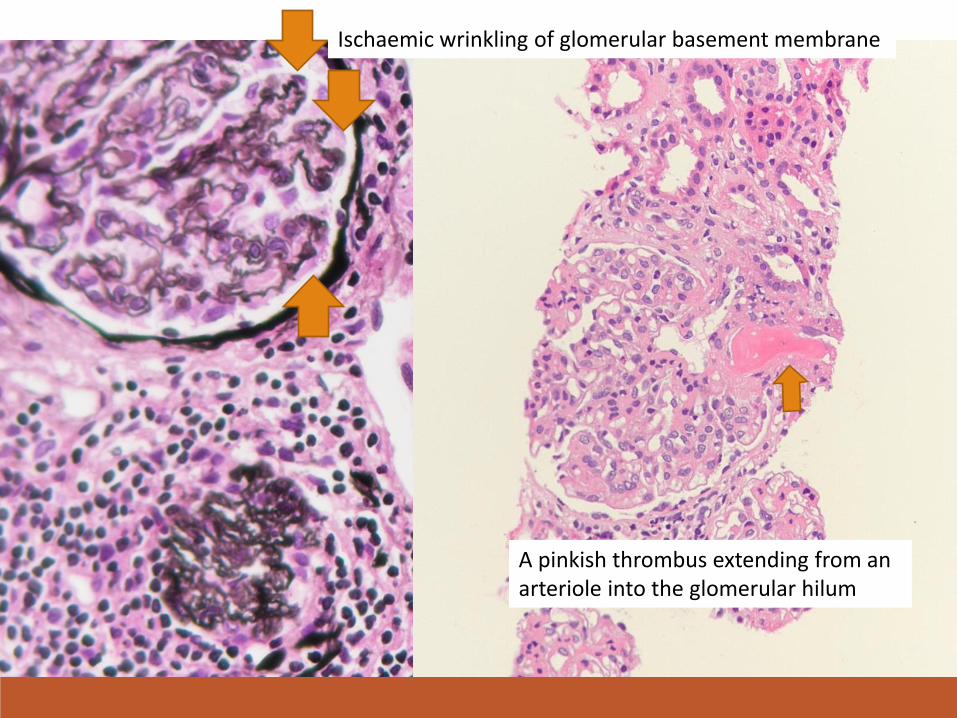
Ischaemic wrinkling of glomerular basement membrane
A pinkish thrombus extending from an arteriole into the glomerular hilum
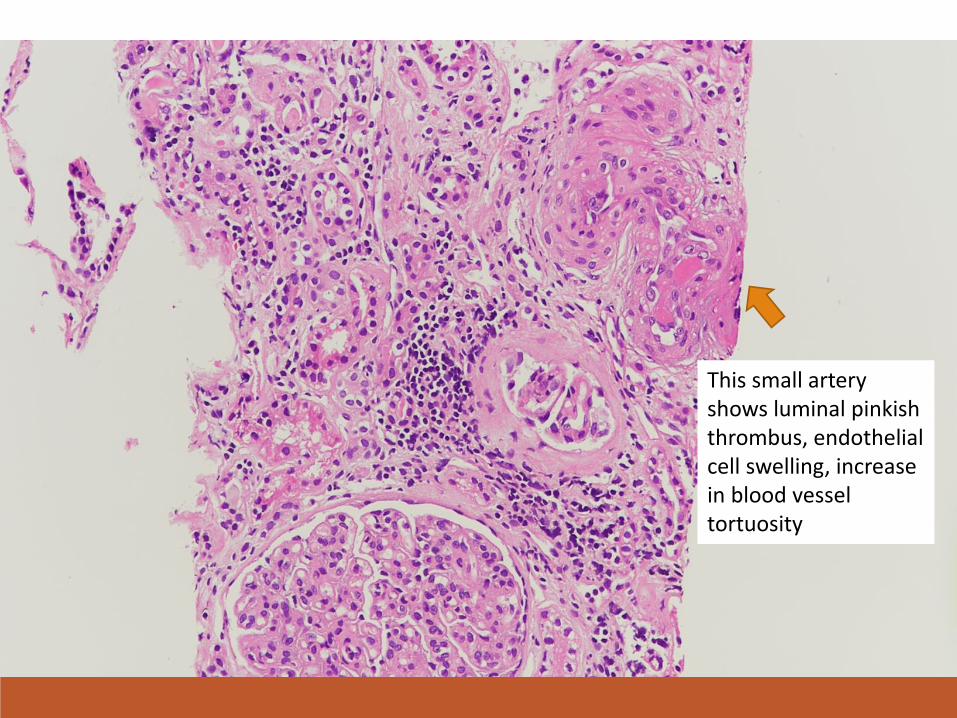
This small artery shows luminal pinkish thrombus, endothelial cell swelling, increase in blood vessel tortuosity

Some renal tubules show luminal pinkish granular casts (blue). Some renal tubules show irregular spacing of nuclei and apical sloughing (red). These are compatible with ischaemic acute tubular injury
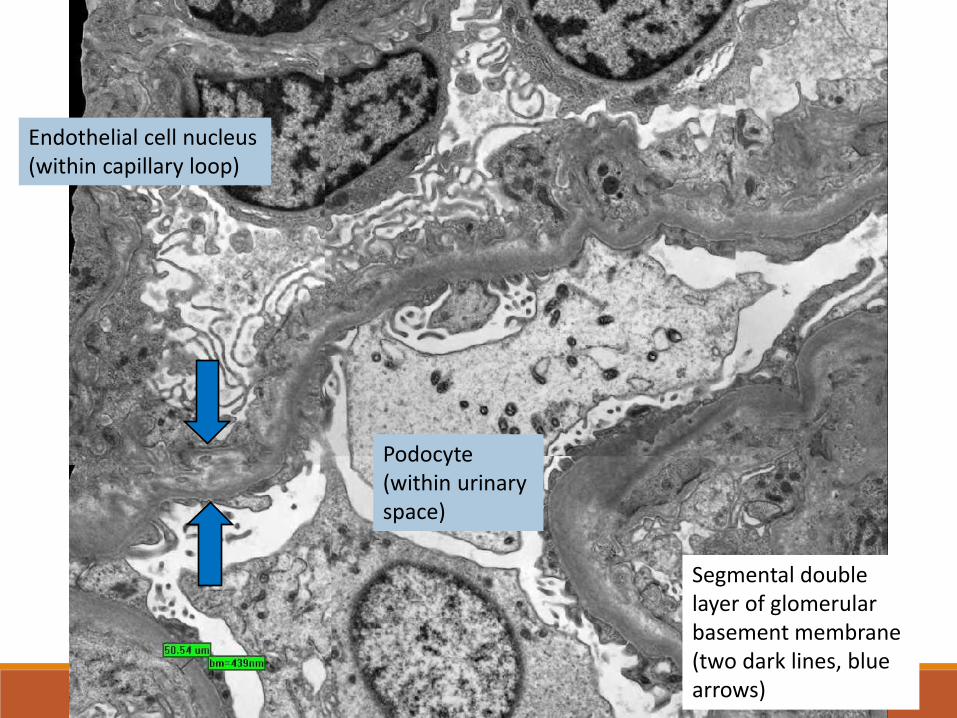
Segmental double layer of glomerular basement membrane (two dark lines, blue arrows)
Podocyte (within urinary space)
Endothelial cell nucleus (within capillary loop)
Comment Crescents/ subepithelial spikes not seen.
IF: No significant deposit
Diagnosis: Thrombotic microangiopathy with acute* and subacute changes^
Comment: Can be related to antiphospholipid syndrome. Pathological features overlap with malignant HT and haemolytic uraemic syndrome
* e.g. endothelial cell swelling, thrombus, GBM wrinkling, acute tubular injury, etc. ^e.g. double contour of GBM, parenchymal scarring, etc.
Further workup Urine pneumococcal antigen negative
Stool culture no growth
ANA, ANCA, Anti-ENA negative
ADAMTS13 activity 105% (normal)
MRI brain pending
(Neurological exam normal, no seizure)
Diagnosis ANTI-PHOSPHOLIPID SYNDROME (APS)
APS NEPHROPATHY
Lupus anticoagulant +ve Anti-cardiolipin IgG +ve
Clinical thrombosis (Budd-chiari syndrome) Renal biopsy: Thrombotic microangiopathy
Before going to management… DR. ALVIN HUI
Progress
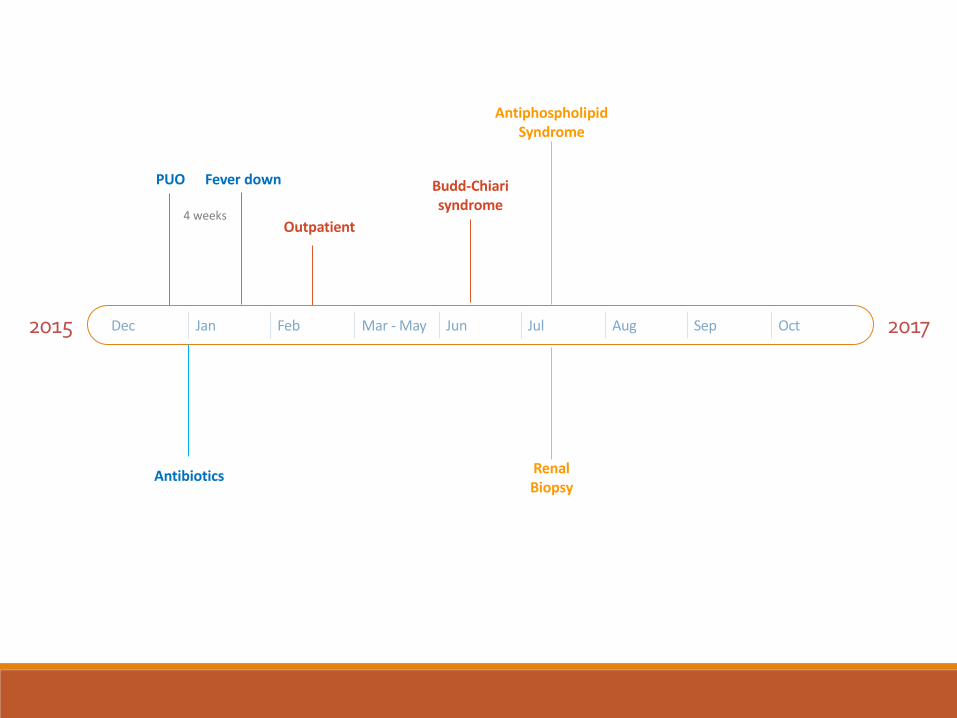
2015 2017 Dec Jan Feb Mar - May Jun Jul Aug Sep Oct
PUO Fever down
Outpatient
Antiphospholipid Syndrome
4 weeks
Budd-Chiari syndrome
Antibiotics Renal Biopsy
28th July 2016 Day 7 fever
P/E:
- pallor, jaundice
- no rash
- no joint swelling/ tenderness
- abdomen distended, large hepatosplenomegaly, both ~6cm below costal margin
- systolic BP 140-150mmHg and diastolic BP 85-105mmHg
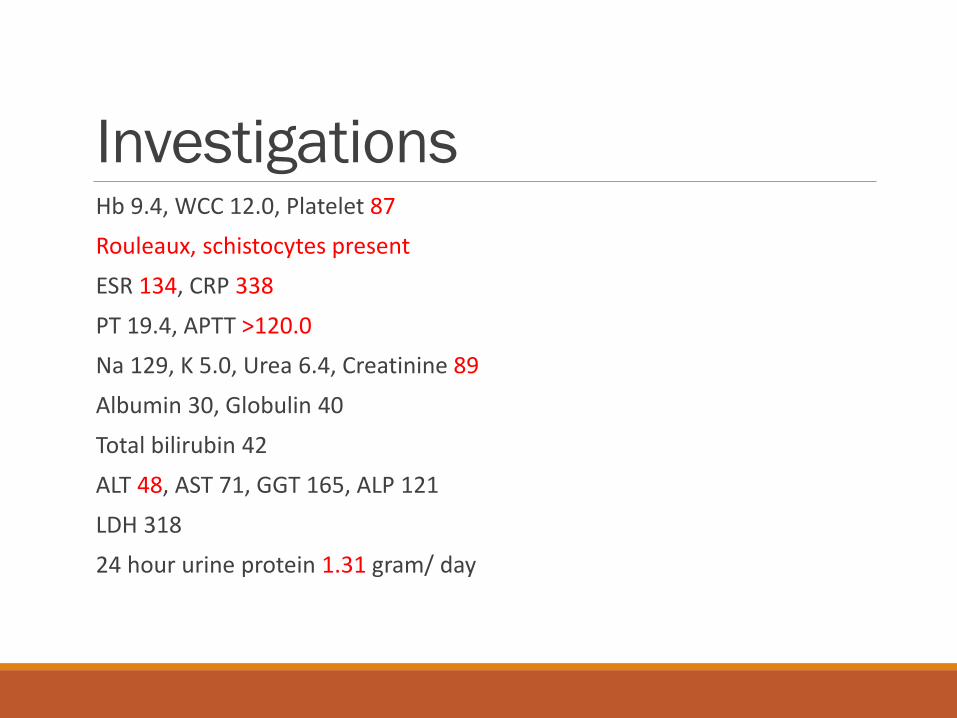
Investigations Hb 9.4, WCC 12.0, Platelet 87
Rouleaux, schistocytes present
ESR 134, CRP 338
PT 19.4, APTT >120.0
Na 129, K 5.0, Urea 6.4, Creatinine 89
Albumin 30, Globulin 40
Total bilirubin 42
ALT 48, AST 71, GGT 165, ALP 121
LDH 318
24 hour urine protein 1.31 gram/ day
Management Anti-thrombosis
◦ LMWH
◦ Warfarin
Hypertension, proteinuria ◦ ACEI
◦ Labetalol
◦ Diuretics
Immunosuppression ◦ Steroid, hydroxychloroquine
◦ Azathioprine
◦ IVIG
◦ Plasmapheresis
Management – thrombosis Enoxaparin since 28/7
◦ Anti-Xa level adequate
Switched to warfarin since 31/8
Management – BP Labetalol
Enalapril
Lasix
0
50
100
150
200
250
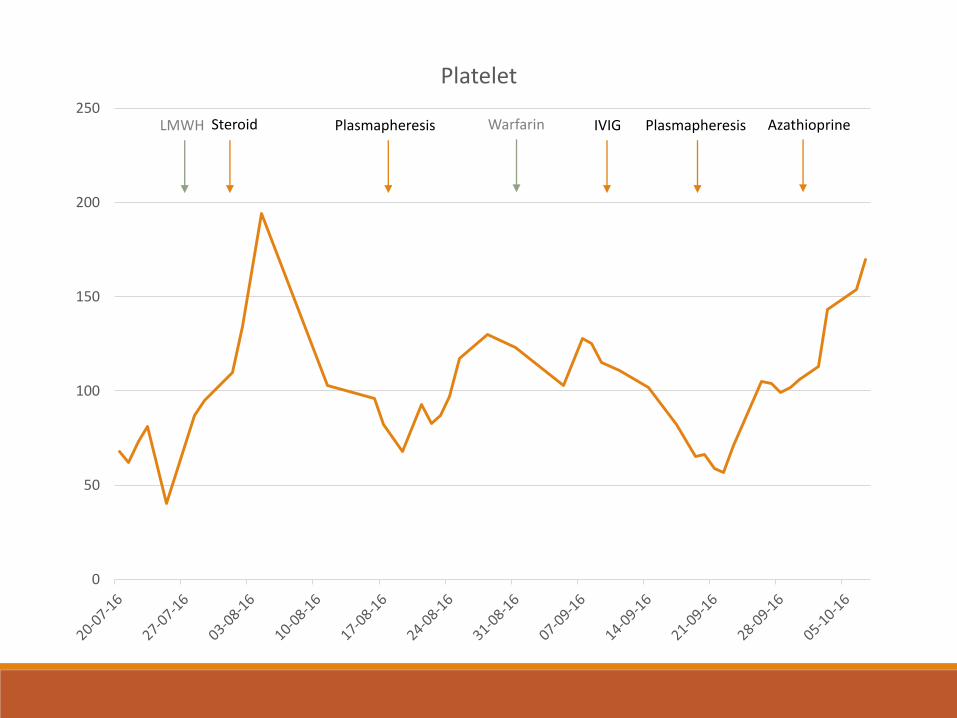
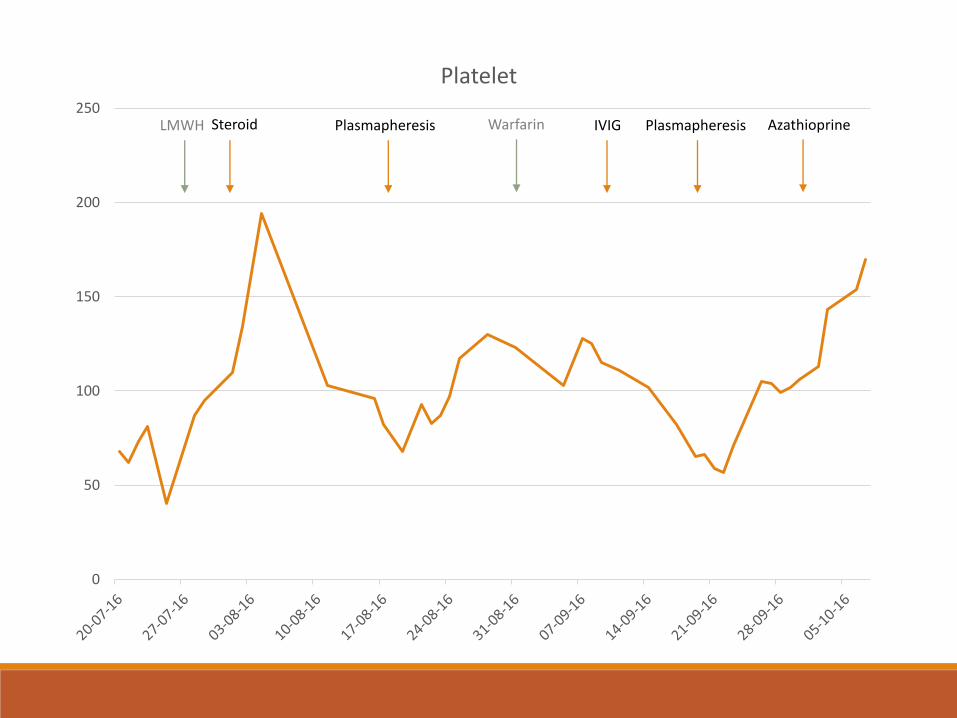
Platelet
LMWH Steroid Plasmapheresis IVIG Plasmapheresis Azathioprine Warfarin
Immunosuppression Methylprednisolone 1 gram daily for 3 days,
then prednisolone 60mg/ day ◦ Since 28/7/2016
◦ Total 6 weeks P60, then gradually wean down
Fever down soon after starting steroid
Decreased in size of hepatosplenomegaly
Platelet transiently rose to ~190
Immunosuppression Since early August (1 week after admission):
◦ Gradually dropping platelet, deranged LFT, re-appearance of splenomegaly
1st course plasmapheresis (5 sessions) was started three weeks after admission
After initial course of plasmapheresis ◦ Platelet transiently normalized
◦ Anti-cardiolipin IgG <13.3 normalized
Immunosuppression 2 weeks later, platelet downtrend again
◦ Started hydroxychloroquine 200mg daily
◦ Given a course of [email protected] gram/ kg/ day
◦ Diluted to 3%, slow infusion
◦ (Concentration >5% is associated with risk of thrombosis)
No significant improvement
Immunosuppression 2nd course of plasmapheresis (5 sessions) was started (One month after 1st course) ◦ Decreased in size of hepatosplenomegaly
◦ Platelet normalized
Started tailing down steroid gradually
Azathioprine was started
Monitoring
Clinical Fever
Liver and spleen size
Blood pressure
Proteinuria
Laboratory Platelet
LDH
Others? ◦ ALT, bilirubin
◦ APTT
◦ ESR, CRP
◦ Lupus anticoagulant
◦ Blood smear – Schistocytes, rouleaux
0
50
100
150
200
250
Platelet
LMWH Steroid Plasmapheresis IVIG Plasmapheresis Azathioprine Warfarin
Imaging USG Abd 9th September 2016
◦ Focal stenosis site at diaphragmatic region of IVC, above the level of hepatic vein confluence, is still seen.
CT Abd 20th September 2016 ◦ Interval decrease in extent of hepatosplenomegaly and intra-abdominal
lymph nodes
◦ Liver: 20cm-->15.3cm along right MCL, Spleen 16.8cm-->14.5cm
MRI abdomen + pelvis booked on December 2016
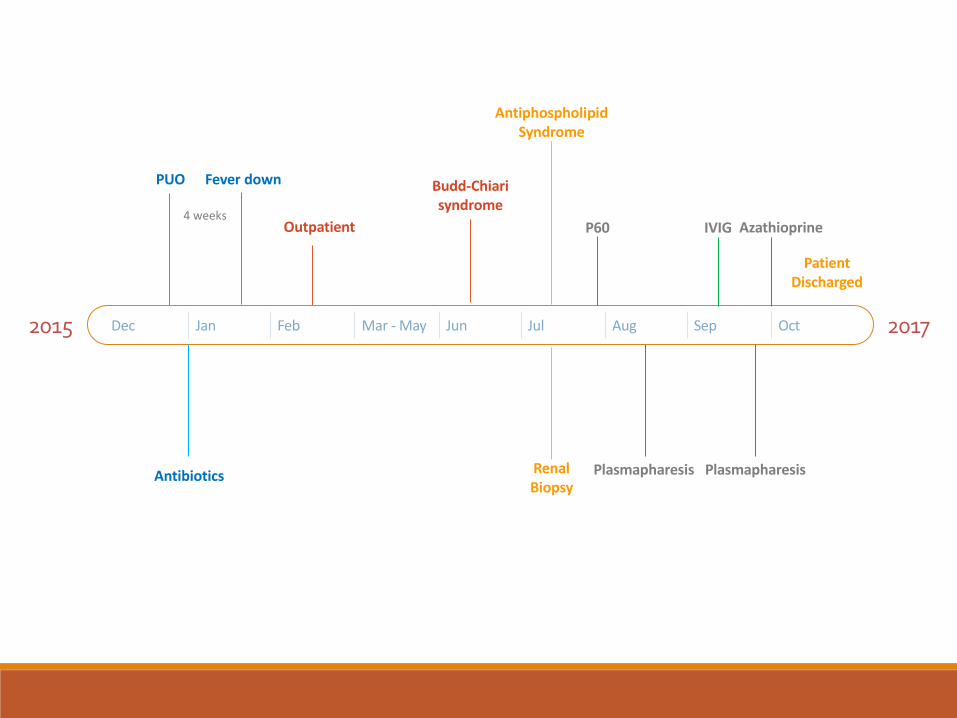
2015 2017 Dec Jan Feb Mar - May Jun Jul Aug Sep Oct
PUO Fever down
Outpatient
Antiphospholipid Syndrome
4 weeks
Budd-Chiari syndrome
Plasmapharesis Plasmapharesis Antibiotics Renal Biopsy
Patient Discharged
P60 Azathioprine IVIG
Follow-up 11th October 2016 No fever after discharge
BP measured at home: SBP 125-135; DBP 88-90
Good compliance to medications
Liver 2cm and spleen 1cm
Blood tests ◦ Hb 11.2; WCC 5.5; Plt 193; smear no schistocytes/ rouleaux ◦ RFT 143 / 3.8 / 9.3 / 83 (eGFR 73ml/min/1.73m2) ◦ HCO3 20; Cl 108 ◦ LFT: ALT 48; GGT 185; Others normal ◦ Albumin 39 ◦ INR 2.26
Current medications Prednisolone 30mg daily
Azathioprine 75mg daily
Hydroxychloroquine 400mg daily
Enalapril 2.5mg daily
Labetalol 300mg Q6H
Warfarin 4.5mg daily
Calcichew 1 tablet daily
Plan Gradually tail down steroid
Maintenance with Azathioprine
Close monitoring in outpatient
Keep warfarin with INR target 2.5-3.0
Repeat imaging for IVC stenosis later
May need further course plasmapheresis/ rituximab if disease not under control
Discussion How to monitor disease activity?
Immunosuppression ◦ Duration of steroid
◦ Choice of maintenance therapy
◦ Role of Rituximab / further courses of plasmapheresis
Anti-thrombosis ◦ Choice of agent (warfarin vs newer agents)
◦ Duration of treatment