8847016541 traumab
TRANSCRIPT


Imaging ofPediatric Bone and Joint Trauma


Fabio Martino . Claudio Defilippi . Roberto Caudana (Eds.)
Imaging of Pediatric Boneand Joint Trauma
Foreword byCarlo Masciocchi
~ Springer

EditorsFabio MartinoRadiology DepartmentPoliclinico - Giovanni XXI1I HospitalBari, Italy
Roberto CaudanaMedica l Imaging ServiceMilan, Italy
Claudio Defili ppiPediatric Radiology ServiceRegina Margherita Children 's HospitalTurin, Italy
The contents of this book are based on:Imaging del trauma osteo-articolare in eta pediatrica. F. Martino, C. Defilippi, R. Caudana (Eds.)© Springer-Verlag Italia 2009
ISBN 978-88-470-1654-5
DOl 10.1007/978-88-470 -1655-2
e-ISB N 978-88-470-1655-2
Springer Milan Dordrecht Heidelberg London New York
Library of Congress Control Number: 20 I0924122
© Springer-Verlag Italia 2011
This work is subject to copyright. All rights are reserved, whether the whole or part of the material isconcerned , specifically the rights of translation, reprinting, reuse of illustrations , recitation, broadcasting, reproduction on microfilm or in any other way, and storage in data banks. Duplication of thispublication or parts thereofis permitted only under the provisions of the Italian Copyright Law in its current version, and permis sion for use must always be obtained from Springer. Violations are liable to prosecution under the Italian Copyright Law.
The use of genera l descriptive names, registered names, trademarks, etc. in this publication does notimply, even in the absence of a specific statement , that such names are exempt from the relevant protective laws and regulations and there fore free for general use.
Product liability: The publishers cannot guarantee the accuracy of any information about dosage andapplication contained in this book. In every individual case the user must check such informat ion byconsulting the relevant literature.
9 8 7 6 5 4 3 2 I
Cover design : Ikona S.r.l., Milan, Italy
Typese tting: Graphostudio, Milan, ItalyPrinting and binding : Arti Grafiche Nidasio, Assago (MI), ItalyPrinted in Italy
Springer-Verlag Italia S.r.l. - Via Decembrio 28 - 1-20 137 Milan
Springer is a part of Springer Science+Business Media (www.springer.com)

Foreword
The role of diagnostic imaging in the evaluation of fractures and soft-tissue injuries inskeletally immature patients continues to evolve as the technique s increasingly enabledetection and characterization of abnormalities and provide results that affect decisionsabout patient care.
Written by the leaders in the fie ld, Imaging of Pediatric Bone and Joint Traumaanswers the questions arising in the diagnosis of these conditions, which are peculiar topatients who are still growing, and offers a valuable and comprehensive tool to all thosecalled to prevent the often disabling deformities that are secondary to these conditions,and may be observed in adults.
The chapters are ideally divided into three parts, and offer an accurate, complete, andupdated analysis of the different locations, mult iple lesions, and dramat ic consequences ofthese injuries on other parts of the body.
For its didactic value, the volume will certainly meet the requirements of the readerand will particularly appeal to radiologists who will turn to it during their daily work.
My warmest congratulations go to the authors and co-authors for a book that will certainly be a great success.
L'Aquila, October 2010 Carlo MasciocchiChief of the Departm ent of Radiology
University of 1.,'AquilaPast-President of the European Society of Musculoskeletal Radiology (ESSR)
v


Preface
Acute and chronic orthopedic injuries in children are unique in term s of the mech anisms of injury, pathophysiology, and healing. In fact , because of the dynamic stateof growth and development, pattern s of skeletal injur y in children are frequently differen t in type and presentat ion from tho se in adults, and so often require differentdiagnostic and treatm ent algorithms. The role of diagnostic imaging in the evaluationof fractures and soft-t issue injuries in skeletally immature patients continues toevolve, as the techniques increasingly enable detect ion and characterization of abnormaliti es and provide result s that affect decision s about patient care.
The aim of this volume is to use a practical approach to provide an up-to-date andcomp rehensive text on the all important aspects of musculo skeletal trauma imagingin children and adol escents. Accidental trauma, chronic and sport-re lated injuries,birth fractures, and batt ered child are described and illustrated, highl ighting corresponding features in imaging, and providing an overview of find ing s in the differentanatom ical sites of the body.
Rome, Octob er 2010 Fabio MartinoClaudio DefilippiRoberto Caudana
vii


Contents
Major Traumatic Bone and Joint Injuries: Overview .F. Martino , L. Falcone , M. lndolfi, M. Matarazzo and G. Martino
1.1 Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . I1.2 Development and Growth of Bones. . . . . . . . . . . . . . . . . . . . . . . . . . . 31.3 Characteristics of the Growing Skeleton. . . . . . . . . . . . . . . . . . . . . . . 61.4 Fractures and the Healing Process: Clinical and
Radiological Evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71.5 Typical Osteo-traumatie Lesions of the Immature Skeleton 91.5.1 Complete Fractures 101.5.2 Plastic Deformation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121.5.3 "Torus"-type Fracture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131.5.4 "Green-stick" Fracture. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.5.5 Metaphyseal-epiphyseal Fractures (of the Physeal Plate) 141.5.6 Apophyseal Detachments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 211.6 Imaging in the Follow-up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241.7 Fracture and/or Dislocation Reduction - Synthesis - Consolidation . 24I. 7.1 Growth Arrest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 271.8 The Role of Diagnostic Imaging 281.8.1 Conventional Radiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281.8.2 Ultrasonography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 291.8.3 Computed Tomography (CT) .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301.8.4 Magnetic Resonance Imaging 31Suggested Readings 32
2 Micro-traumatic Lesions Caused by Overuse: OverviewC. Defil ippi, P. Pautasso and C. Faletti
35
2.1 Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 352.1.1 Stress Fractures 37
ix

Contents
2.1.2 Osteochondro sis and Osteochondrit is Dissecans . . . . . . . . . . . . . . . . . 392.1.3 Osteochondr itis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 412.1.4 Chronic Lesions of the Physis 432.2 The Upper Limb. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 432.2.1 Little League Shoulder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 432.2.2 Osteochondrosis of the Humeral Condyle (panner Disease) . . . . . . . . 442.2.3 Osteochondritis Dissecans of the Humeral Condyle . . . . . . . . . . . . . . 442.2.4 Little League Elbow Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 452.2.5 Osteochondritis of the Olecranon Apophysis . . . . . . . . . . . . . . . . . . . . 452.3 The Lower Limb. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 462.3.1 Osteochondrosis of the Epiphyseal Nucleus of the Femur
(Legg-Calve-Perthes Disease) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 462.3.2 Epiphysiolysis of the Epiphyseal Nucleus of the Femoral Head. . . . . 462.3.3 Osteochondritis Dissecans of the Femoral Condyle
(Konig Syndrome) 462.3.4 Osteochondritis of the Inferior Pole of the Patella
(Sinding-Larsen- Johansson Syndrome) 462.3.5 Osteochondritis of the Anterior Tibial Apophysis
(Osgood- Schlatter Disease) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 472.3.6 Shin Splints 472.3.7 Osteochondritis Dissecans of the Talus . . . . .. . . .. . .. . . . . .. . .. .. 472.3.8 Osteochondritis of the Calcaneal Apophysis (Sever Disease) .. . . .. . 472.3.9 Osteochondritis of the Apophysis of the Base of the Fifth Metatarsal
(Iselin Disease) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 482.3.10 Osteochondrosis of the Head of the Second Metatarsal
(Freiberg or Koehler II Disease) 48Suggested Readings 48
3 Osteoarticular Trauma in the Pediatric Age:Overview - Apophyseal Injuries 49M. Valle, A. Tagliafico, L. Oppezzi, N. Gandolfo, P. Toma and C. Martinoli
3.1 Introduction 493.2 Tendons . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 503.2.1 Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 503.2.2 Imaging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 523.2.3 Chronic Apophyseal Lesions Due to Tendon Traction . . . . . . . . . . . .. 533.2.4 Acute Apophyseal Lesions from Tendon Traction . . . . . . . . . . . . . . .. 563.3 Ligaments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643.3.1 Apophyseal Injuries Due to Ligament Traction . . . . . . . . . . . . . . . . .. 65Suggested Readings 67

xiContents
4 Major and Minor Pediatric Traumatic Musculotendinous InjuriesE. Genovese, A. Leonardi, L. Callegari, M.G. Angeretti,M. Albrizio, E. Spano and C. Fugazzola
69
4.1 Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 694.2 The Role of Imaging in Detection . . . . . . . . . . . . . . . . . . . . . . . . . . . . 694.3 Muscolar Lesions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 714.3.1 Muscular Distract ive Lesions . .. . ... . ... ... . ... . ... .. ... . ... . 714.3.2 Muscolar Contusions 744.3.3 Complications and Follow-up 744.4 Tendon Lesions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 754.4.1 Tendinopathy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 754.4.2 Insertional Tendinopathies (Enthesopathies) 764.4.3 Bursitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 784.4.4 Tendinous Ruptures 784.5 Abnormalities of Ligaments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 784.5.1 Extra-articular Ligaments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 784.5.2 Intra-art icular Ligaments 80Suggested Readings 81
5 Traumatic Lesions of the Peripheral Nerves 83E. Paeeiani, F. Randisi, C. Orazi, M. Valle and C. Martinoli
5.1 Introduction 835.2 Ultrasound Scanning 845.3 Magnet ic Resonance Imaging 89Suggested Readings 95
6 Imaging of Regional Injuries: The Axial Skeleton - the Skull, VertebralColumn, and Thoracic Cage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97C. Fonda, M. Mortilla, C. Cesarini and M. Basile
6.1 The Skull 976.1.1 Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 976.1.2 Orbital and Nasoethmoid Fractures . . . . . . . . . . . . . . . . . . . . . . . . . . . 1036.1.3 Maxillofacial Fractures 1056.1.4 Mandibular Fractures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1076.1.5 Zygomatic and Maxillary Fractures . . . . . . . . . . . . . . . . . . . . . . . . . .. 1086.2 The Vertebral Column 1086.2.1 Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1086.2.2 Radiological Examination 109

xii Contents
6.2.3 Evaluation of Spinal Trauma I 106.2.4 Pathophysiology 1126.2.5 Superior Cervical Spine Injuries 1146.2.6 Occipito-atl anto-axiallnstability 1146.2.7 Odontoid Process Fractures 1156.2.8 Extension Fractures of the Atlas and Axis. . . . . . . . . . . . . . . . . . . . .. I 176.2.9 Flexion Trauma of the Inferior Cervical Spine 1176.2.10 Extension Trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . I 196.2.1 I Fractures of the Thoracolumbar Spine. . . . . . . . . . . . . . . . . . . . . . . .. I 196.3 The Thoracic Cage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 12I6.3.1 Chest Wall Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 121Suggested Readings 123
7 The Upper Limbs 125D. Barbuti , E. Pacciani , M. Cirillo, A. Magistrelli and L. Tanturri De Horatio
7. I The Shoulder and Arm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 1257.2 The Elbow and Forearm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 13 I7.3 The Wrist and Hand 146Suggested Readings ISO
8 The Pelvis and Lower Limbs lSID. Barbuti , E. Pacciani, A. Magistrell i, M. Cirillo, F. Fassari andL. Tanturri De Horatio
8.1 The Pelvis, Hip, and Femur lSI8.1.1 Fractures of the Pelvis 1528.1.2 Sacro-coc cygeal Fractures 1588.1.3 Traumatic Luxation of the Hip in Children . . . . . . . . . . . . . . . . . . . .. 1598.1.4 Fractures of the Femur . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 1608.2 The Knee and Leg 1648.2.1 Fractures of the Distal Epiphysis of the Femur 1648.2.2 Fractures of the Patella . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 1668.2.3 Fractures of the Tibia .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 1668.3 The Ankle and Foot 1698.3.1 Lesions of the Ankle Region 1698.3.2 Fractures of the Foot 1738.3.3 Fractures of the Astragalus 1748.3.4 Fractures of the Calcaneus 1748.3.5 Fracture of the Scaphoid 1758.3.6 Lisfranc Fracture 1758.3.7 Fractures of the Metatarsals and Phalanges 176Suggested Readings 177

Contents xiii
9 Birth Trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179C. Defil ippi, B. Santoro and P. Pautasso
9.1 Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1799.2 Obstetric Pseudo-paralysis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1799.3 "Birth Fractures" 180Suggested Readings 182
10 Toddlers' Fractures 183C. Defil ippi, B. Santoro and P. Pautasso
10.1 Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18310.2 The Concept of Toddlers' Fractures. . . . . . . . . . . . . . . . . . . . . . . . . . . 18310.3 Imaging 184Suggested Readings 186
11 Bony Lesions from Non-accidental Trauma 187C. Defil ippi, B. Santoro and P. Pautasso
11 .1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18711 .2 The "Battered Child": Imaging 18711.3 Fractures in Specific Anatomical Sites 19011.4 Fractures in Non-specific Anatomical Sites, with Particular
X-ray Characteristics for Dating of Fractures 19111 .5 Fractures with Particular Radiographic Characteristics . . . . . . . . . . . . 19311 .6 Differential Diagnosis 19611 .6.1 Defective Osteogenesi s 19711 .6.2 Infantile Cortical Hyperostosis (Illness of Roske-De Tone-
Caffey-Silverman) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19811 .6.3 Dysmetabolic Bone Disease of Premature Infants 19911 .6.4 Menkes Disease 20011 .6.5 Rickets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20011 .6.6 Congenit al Syphilis 20 I11.6.7 Scurvy 202Suggested Readings 202
12 The Battered Child: Guidelines and Medical-legal Implications . . . . . . . . . 203M. Solarino and B. Solarino
12.1 Introduction 20312.2 Current Regulations and Medical-legal Considerations 20612.3 Conclusions 207References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 208Suggested Readings 208


Contributors
Maria Gloria AngerettiDepartment of Radiolog yCircolo Hospital Macchi FoundationVarese, Italy
Domenico BarbutiDepartment of Diagnostic ImagingPediatric Hospital "Bambino Gesu"Rome, Italy
Massimo BasileDepartment of Pediatric RadiologyChildren's Hospital MeyerFlorence, Italy
Leonardo CallegariDepartment of RadiologyCircolo Hospital Macchi FoundationVarese, Italy
Cecilia CesariniDepartment of Pediatric RadiologyChildren's Hospital MeyerFlorence, Italy
Marco CirilloDepartm ent of Diagnostic ImagingPediatric Hospital "Bambino Gcsu"Rome, Italy
Claudio DefilippiPediatric Radiology ServiceRegina Margherita Children's HospitalTurin, Italy
Lorenzo FalconeRadiology DepartmentPoliclinico - Giovanni XXlll HospitalBari, Italy
Carlo FalettiDepartment of RadiologyAOCTOTurin, Italy
Fausto FassariDepartment of Diagnostic ImagingPediatric Hospital "Bambino Gesu"Palidoro (RM) , Italy
Claudio FondaDepartment of Pediatric RadiologyChildren's Hospital MeyerFlorence , Italy
Carlo FugazzolaDepartm ent of Radiolog yCircolo Hospital Macchi FoundationVarese, Italy
xv

xvi
Nicola GandolfoIM2S - Institut Monegasque de Medecine& Chirurgie SportiveMontecarlo , Monaco
Eugenio GenoveseDepar tment of Radiolog yCircolo Hospital Macchi FoundationVarese, Italy
Mariantonietta IndolfiComplex Structure of Radiology"Valle d'Itria " HospitalMart ina Franca (TA), Italy
Anna LeonardiDepar tment of Radiolog yCircolo Hospital Macchi FoundationVarese, Italy
Andrea MagistrelliDepartment of Diagnostic ImagingPediatric Hospital "Bambino Gesu"Rome, Italy
Davide MarianiDepartment of RadiologyCircolo Hospital Macchi FoundationVarese, Italy
Fabio MartinoRadiology DepartmentPoliclinico - Giovanni XXlII HospitalBari, Italy
Gianluigi MartinoSchool of MedicineUniversity of BariBari, Italy
Carlo MartinoliRadiology Department - DISCUniversity of GenoaGenoa , Italy
Contributors
Maurizio MatarazzoOrthopedic Departm entPoliclinico - Giovanni XXlII HospitalBari, Italy
Marzia MortillaDepartm ent of Pediatric RadiologyChildren's Hospital MeyerFlorence, Italy
Leila OppezzlDepartment of RadiologyUniversity of GenoaGenoa, Italy
Cinzia OraziDepartm ent of Diagnostic ImagingPediatric Hospital "Bambino Gesu"Palidoro (RM) , Italy
Enzo PaccianiDepartment of Diagnostic ImagingPediatric Hospital "Bambino Gesu"Palidoro (RM), Italy
Patrick PautassoDepartment of RadiologyAO CTOTurin, Italy
Francesco RandisiDepartment of Diagnostic ImagingPediatric Hospital "Bambino Gesu"Palidoro (RM) , Italy
Bianca SantoroPediatric Radiology ServiceRegina Margher ita Children's HospitalTurin, Italy
Biagio SolarinoSection of Legal MedicineUniversity of BariBari, Italy

Contributors
Michele SolarinoSection of Radiology"Fallacara" HospitalTriggiano - Bari, Italy
Alberto TagliaficoRadiology Department - DISC
University of GenoaGenoa, Italy
Laura TanturriDepartment of Diagno stic ImagingPediatric Hospital "Bambino Gesu"
Rome, Italy
Paolo TomaDepartment of RadiologyPediatric Hospital "Bambino Gcsu"
Rome, Italy
Maura ValleDepartment of RadiologyIstituto Scientifico "Gi annina Gaslini"
Genoa, Italy
xvii


Major Traumatic Bone and Joint Injuries:Overview
F. ~ Iarli no. L. Falco ne. ~1. lndolfl, F. ~ 1. ~ Ia laral.lo and G. Ma r tino
1.1Introduction
1
During childhood and adol escenc e, urgent osteo- art icul ar trauma tic pathology is a
frequ ent occurrenc e, and constitutes on e of the main ca uses of dem and for med ical
care in the emergency dep artment of a pediatric hospital (more than 15-20% of all
vis its ). Injuri es cau sed by skeletal trauma dur ing childhood occur more than in
adulthood, although in most cases the extent of anatomica l damage is mod est. Males
are affected mo re often than females. In a lmos t 50% of cas es traum a is due to a fall
and , in these cases, elbow and wri st fractures are the most common injuries. Carpalfractures, however, are uncommon lesion s in children and, when present , almost
always invol ve the scaphoid.
Traumat ic bon e and joint inj uries in children differ from those in the adults in the
range of ana tomica l features, as well as biomechanical and phy siological aspects that
are related to skeleta l growth and are strongly influenced by endocrine-metabolic
factors (growth hormone, thyro xin , es trogens, testo sterone) act ing particularly on
the growth cartilage . In addition to their effect on how the ana tomic damage occurs,
the se features may affect the healing time and bone remodeling, and can lead to
deformities when inj uries are not promptly diagnosed and properly treated. It is also
important to remember that a fracture during the growing years can result in an over
growth of the bone involved, resulting in hype rmetria, mo st frequently at the expense
of the femur and humerus, due to the increased blood flow in the inj ure d area re lat
ed to the rep air process .
Not only do traum at ic injuries of the immature skeleton vary when compared with
an adult, but there are also differenc es related to the age of the chi ld or adolescent,
F. Martino (C8J)Radiology Department, Policlinico - Giovanni XXIII Hospital, Sari, Italy
Imaging of Pediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag ItaJia 20II

2 F. Martinoet al.
1because of the continuous ana tomical and biomechanical changes during the growing period, and because of the wide variati ons in lifestyle dur ing different stages ofgrowth. For example, fractures of the clavicle and femoral diaph ysis are frequent inearly childhood, while they becom e unu sual in adolescence, when the mo st affecte danatomical site is the distal end of the radius. Fractures of the upp er limb in chi ldre nare three times mor e frequent than tho se of the lower limb, but thei r re lative importance increases after adolescence, especially in males, and injuries are oft en relatedto the pract ice of sports (especiall y football , skiin g, and rugby). The same conside rations apply to dislo cat ions, whic h are generally far less frequent than fract ures inthose of a developm ental age . The reas on is related to the presence of an area ofweakness, represe nte d by the growth car t ilage plate, which is mor e vulne rable thantendons and ligam ent s befo re a capsular- ligament injury may occur. Since closur e ofthe physis occurs at different ages in different bon e segments, it is not uncommon todetect a dislocated elbow after the age of 7 years, while a subluxation of the hum eral physis will be detected abo ve the age of 12 to 14 years, that is, after the corresponding hum eral physis is clo sed.
As in adults, a traum atic injury in a developing chi ld may be linked to a nonaccidenta l cause ; such an occurrence is particularly important in the pediatricpat ient as it can suggest the so-called "m altreatment syndrome" or battered child,with corresponding specific medical-legal responsibilities that may invol ve the radiologist. Trauma tic injuries in children unde r the age of 3 years should always beregarded with suspicion and clo sely examined by the rad iologist , as 5-10% of traumas in th is age group are not accidental, but are caused by malt reatment. Therefore,in cas es whe re the re is suspicion of a non- accidental traum a, diagnostic inve stigation s should be address ed to sea rching for and repor ting inj uries that may be rel ated, with high speci f ici ty, to mistreatment (be at ing s and /or violent shaking).Multiple fractures on different skeleta l segments , often bilateral, with evidence ofinj uri es in di fferent stages of repai r and with an intense and extensive perioste alreaction, are among the lesions that be st characterize a typical radiographic example of battered child. The radiologi st must, howe ver, pay particular attention, to thedifferenti al diagnosis between malt reatment lesions and injuries indu ced by intenseosteopenia, such as tho se occurring in osteogenesis imperfecta, wh ich strongly predispo se to pathological fra ctures, and, if not properly ass ess ed, can be con fused witha battered child case .
Sometimes a pathological bone fracture can be an unexpected finding, shown bythe radiological invest igat ion as an occasional con sequence of a mino r traum a to askeleta l segment that has been made fragile by the presence of a pre-ex isting foca llesion (Fig. 1.1).
Traum atic inj ury of the skeleton in developmental age, therefore, can manifestitself in di fferent ways due to the man y possible causes, and also because of the highvariability of all fac tors that , taken together, influence the mode of onset , anatomicalfeatures, and healing proc ess of a traumati c inj ury, as well as influencing the selection of diagnostic modalities and therapeutic treatm ent.

1 Major Traumatic Bone and Joint Injuries:Overview
Fig.l .l Radiography of the right knee in frontal (a) and lateral (b) view. Pathologic fracture of thetibia on a large aneurysmal bone cyst. The injury resulted in a cortex expansion and thinning,which appears discontinuous on the antero-medial side and shows a pathologic fracture in theprocess of consolidation, associated with a fallen fragment sign
1.2Development and Growth of Bones
In the development and growth of bones, star ting in the womb, two types of ossification have been identified: indirect and membranous.
Indirect ossification, which occurs in mo st bones of the skeleton and is typi cal oflong bones, starts from a primitive cartilage outline developing in the embryo, progressing to a subsequent repl acement of the cartilage matrix with bone ti ssue , bothsuperfi cially (perichondral ossi fi cat ion) and intern all y (endochondral ossifi cat ion).
In membranous ossification , bon es do not follow the patt ern of evolution and arecreat ed directl y from the mesenchymal connect ive tissue, without passing through acartilage stage . An exce ption to th is pattern is the mandibl e, in which direct ossification tak es plac e near a cartilage support that does not j oin to the fin al bon e (mantle ossification).
The long bones, as mentioned before, show an indirect ossification pattern, andare represented in the emb ryo by hyaline cartilage models cove red by per ichondrium,and configured in a diaphysis with two end s, or epiphyses (Fig. 1.2) . During the seventh week of embryonic life , the chondrocytes, in the middle section of the diaphy sis,

4 F. Martino etal.
1are rich in glycog en and calcif ied intercellular substance. Meanwh ile, at the surface ,at the same level as the diaphysis, the perichondrium acquires osteoblast ic activityand depo sits th ick trab ecular bone tissue layers on the surface, thu s form ing a primitive diaphyseal bone pock et (Fig. 1.2a) ; therefo re, the per ichondrium becom esperiosteum . Subsequently, around the tenth week, vascul ar infiltrat ions of the periosteum capillary networ k penetrat e and cross the bone sleeve, thus creating the diaphyseal trophic foramen (Fig. 1.2b). The vesse ls penetrate the central part of the boneand then branch out , helped by the erosive action on cart ilage calci fied by the chondroclasts (also derived, along with vessels, from periosteum) . At this stage, osteoblasts(also of perio steal orig in) place bone trabeculae on the remaining cartilage, thus forming a medull ary cavity in the central bone sleeve, containing blood vessels, someosteocart ilaginou s trabeculae, and hematopoi et ic stem cells. At this very early stag e,the epiphyses are still cartilaginous (Fig. 1.2c). In the later stages , due to the appositive osteoblast activity in the deep layer of the periosteum, the perichondral ossification increases the outer diameter of the primit ive diaphyseal pocket; on the other hand,the medullary cavity osteocl asts erode the deeper layers of the sleeve, thus wideningthe cavity and maintaining the thickn ess of the pocket. The activity of the osteoblastsand osteoclasts is different in different parts of the diaphysis and helps to determin ethe shape and fin al depth of the medull ary cavity in each diaphyseal part. This thenextends toward the epiphysis, along the long itud inal axis of the bone , through the calcific ation and subsequent erosion , created by chondroclasts, which create long pathswhere vessels and cart ilaginou s trabecul ae run long itud inally. The development of themedull ary cavity toward the two extremes come s to an end near the growth plate , theso-called physis, which thus defines the boundaries of the diaphysis (diaphysis literally means "between physis") and identifies the metaphy sis area (lite rally "close tothe physis") . Throughout the growth phase of the bone , the physis, also known as conjugation cartil age , is where active prol iferation of cartil age on the oppo site side of thediaphysis occurs, along with endochondral ossif ication on the side facing the diaphysis, thereby providing furthe r growth in bone length. The two cartil aginous extremesof the bone growth , which lie beyond the physis, correspond to the epiphysis (literally "above the physis") . During development, endochondral ossification nuclei appearin the epiphysis, follow ing the penetration of vascul ar chip s from the epiphyseal perichondrium, with subsequent depos ition of bone lamell ae, formation of spongy bone ,and expansion of the se nuclei toward the surface of the epiphysis (Fig. 1.2d) . At thesame time , a layer of subperichondra l cart ilage remains on the epiphysis surface,which proliferates on one side and is graduall y replaced by bone tissue on the othe rside, contributing to the development of the epiphy seal growth nucleus. Once the boneis fully grown , the two ossifi cation fronts, diaphyseal and epiphyseal , invade the conjugation cartil age and merge , ending the growth in bone length . When ossification iscomplete, only a thin hyaline cartilage cap remains in the epiphysis, corre spond ing tothe articular car tilage. It should be remembered, however, that some epiph yses (forexample, the humeral distal epiphysis ) have more ossification nuclei, which are separated from one another and remain separated for a long time by a thin layer of hyalin ecar tilage, befor e they fuse completely. Ossifi cat ion of short bones occurs in a similarway to that of epiphyses .

1 Major Traumatic Bone and Joint Injuries:Overview 5
Fig. 1.2a-d Explanatory scheme of growth and indirect ossification of long bones
y.1 4·1511·20
Fig. 1.3 Schematic illustration of the location of the epiphyseal and apophyseal growth nuclei ofthe appendicular skeleton. In black, the average age of onset, and in red the closure age of the corresponding physis
In flat bon es, direct ossi fi cation takes place, where, in some area s of the outline,the mesenchyme becom es rich in blood vessels and cell s. Mesenchymal cells becomeost eobl asts that synthesize bon e tissue in which minerals are deposited. At the sam e
tim e, the periosteum shapes the final bon e with an appositional mechanism .It is crucial for the radiologi st to have knowledge of the different epiphyseal and
apophyseal ossi fic ation centers, their age of on set , and the clo sure time of the corresponding growth plate , in order to limit mistake s in diagnosis and to avoid the needfor radiographs of the contralateral side (Fig . 1.3) .

1
6
1.3Characteristics of the Growing Skeleton
F. Martino etal.
Anatomical and physiological characte ristics of the grow ing skeleton (which mainlyinfluence the biom echanics and cl inical-p athological expression of the typical traumatic lesion s in the immature ske leton), concern both the osteop erio steal pock et, andthe cartilag inou s growth plat e, or physis, which are absent in adults (Fig. 1.4).
In childr en, the bone matrix has a lower density, becau se the mesh in the spongyweb is wider and the compact bone has a greate r porosity, with an incre ased pre senceand size of Haver sian channel s, and is richly vascularized, resulting in lower elasticity but greater plasticity. This feature makes the bone yield more eas ily, so it is morelikely to deform than to fracture.
The periosteal sheath is much thic ker (rel ative thickness) than in adults, but lesstenacious, bec ause the surface of bone adhesi on has less-de veloped Sharpey 's fibers.The refo re, when the periosteum is exposed to traum a it easily dissect s itself, butrarely breaks. This feature results in a limit ation in both the propagation of the fracture (comminuted fractures are in fact less frequent) and the degree of its displacement. This is also why some compound fractu res in a ch ild may be unrecogni zed atan early stage, and a reparative bon e callus is onl y found some time later at the site
Fig. 1.4Anatomical scheme of the epiphyseal-metaphyseal portion of the growth bone

1 Major Traumatic Bone and Joint Injuries:Overview 7
of the earlie r trauma. Furthermore, as there is a very rich subp erio steal vascular network, a lesion involving the perio steum is usually accompanied by an extensivehematom a.
The cartilaginous growth plate, or physis, consist s of a car tilaginous matri xlocated between the metaphysis and the secondary ossifica tion epiphyse al nucl ei,and is typ ical of childhood, as it is totall y absent in the mature skeleton . In relationto the biom echanical prop erti es of cartilage, the physis represent s an area of weakness as it is mor e fragi le in the face of traum a, if compared to the bone, tendons andligaments. This feature makes the presence of cart ilag e (both in the physis and in thetendon attachment to the apophysea l cartilag e) act as a shock-absorber for the musculoskelet al struc ture s, preserv ing them from harm , and focus ing the force of thetrauma on itself. In fact , in childr en, and especially in adol escent s, an epiphyse aland/or apoph yseal displacement is more likely to occur rather than a ligamentousinjur y, as ligam ents are much more resistant to tension or torsion forces (2- 5 times)than the cartilag e. In the knee, for instance, epiphyse al displacement or apoph ysealavulsion (that occur in adol escent s) may be cons idered, in some ways, to be the counterpart of injury to the cruciate ligament s that occurs in adults. For the same reason s,even a meniscal lesion is a rare event in pediatr ic knee trauma, and is generally associated with the presence of a predi sposing condition, such as a discoid meni scu s.
1.4Fractures and the Healing Process: Clinical and Radiological Evaluation
The pecul iar characteri stic s of the grow ing bone, and, ther efor e, the anatom ical andphysiological differences between children's bones and adults' bones, mean that theprognostic assessment and choice of treatment for pediatric fractures is often different from that for adults .
Typically, pediatric fractures recover much mor e rapidly than in adults, which onone hand is an advantage, becau se of the lower time of immobiliza tion; but on theother hand it represents a limit ation , because the time available to correct an inadequate fracture reduction is shorter (8-10 days in adults, 3- 5 days in children).However, with skeletal trauma in a child there is a reasonable toleranc e for misalignments, as the activ e and continuous remod el ing of growing bone enables recoveryfrom deformities that would be unacceptable in adults. In fact , the younger thepatient is, the closer to the physis the frac ture is, and the mor e the frac ture angulardeformity lies in the plane of motion of the nearest art iculation , and so the greaterthe recovery of defo rmities will be. The deformit ies that recover best from remod eling are angular ones; even deformities with part ial overlapping of the stumps, andthose with shor tening of the skeletal segment can be repa ired by remod eling andcompensated by the incre ase in length-growth activity of the bone, which usuallytakes place in the physis near the site of fractu re . In contrast, tor sion skeletal deformit ies are less well tole rated in a subject of developmental age than in an adult.
The combination of the se characteris tics , of course, affects both the method used

8 F. Martino etal.
1for the statement of diagnostic imaging, and the qual ity of information that must bederived from it. Clin ical and radiological evaluation of each fracture in the pediatricpatient must take into account the patient's age , fracture location and type, degree ofdisplacement , and angle of the stumps.
The child 50 age is one of the first and most important factors for assessing thetype of treatment; reparative osteogenesis is, in fact , faster than in adults because ofthe thick periosteum layer, which has a strong osteogenic activity. As the periosteumgets thinn er and the subperiosteal vascular network decreases with advancing age ,the speed of repair decreases as welI: in a newborn, fractures consolidate and re-ossify completely in about 3 to 4 weeks, while in an adolescent this takes about 12 weeks .
Regarding the fracture location and its distance from the bone extremity, it mustbe remembered that as one approaches the conjugation cartilage, bone remodeling ismore active , so that in children younger than 8-10 years , in the mid-diaphyseal area,it is important to minimize the misalignment and the angle between the stumps withthe lesion, while in the metaphyseal area a certain degree of axial or angular deviation of the remaining stumps is also acceptable, since at that level bone remodelingis able to restore its own norm al alignment. The best tolerated angular deformities(and most eas ily recoverable from remodeling) are those in the same plane as thedominant motion of the nearest joint.
The fracture type, degree ofdisplacement, and angle ofthe stumps should be evaluated with extreme care because on one hand it is true that the lateral or angular misalignment of the stumps (as we have already mentioned) is partly restored by theremodeling power of new bone growth (angul ar deformities of 15° to 25° in patientsyounger than 7 years , and up to 15° in patients under the age of 10 years are considered acceptable) ; it is also true , on the other hand, that any presence of torsional misalignment (not recoverable by remodeling) may result in significant developmentalabnormalities of the joints where the site of fracture is interposed. The fracture typethat is most vulnerable to a delayed fracture consolidation is a "green-stick" one,where the convex side of the bone is under tension and is thus less affected by thecompaction pressure force of the fragments, which is an important stimulus to consolidation (Fig . 1.5). It should be noted, however, that consolidation delay andpseudoarthrosis are particularly rare events in children, apart from in cases of openedand infected fractures in older children. In the developmental years, re-fractures arealso rare, as are cases of myositis ossificans and post-traumatic articular stiffness.Even in the case of apophyseal avulsions, it is important that imaging allows avulsionquantification, for its magnitude affects the therapeutic choice, which also depends onwhich apophyseal nucleus is involved. Avulsion of the apophyseal growth nucleus ofthe ischial tuberosity may, for example, be treated conservatively up to a displacementof 2 em, beyond which a surgical reduction with synthesis should be expected. In thecase of avulsion of the growth nucleus of the medial epicondyle at the elbow, an indication for aggressive treatment is given by nucleus dislocation that is ~5 mm .
From the above it is clear that the treatment of immature bone fractures (whoseaim is obviously to achieve and maintain a satisfactory reduction avoiding complications and, in particular, growth arrest) is essentialIy conservative, since the youngbone heals quickly and growth reshapes the majority of reduction defects.

1 Major Traumatic Bone and Joint Injuries:Overview 9
Fig. 1.5 Delay of consolidation of a "greenstick" fracture, in the middle third of theradius' diaphysis (arro w)
1.5Typical Osteo-traumatic Lesions of the Immature Skeleton
The anatomical peculi ar itie s of the immature skeleton, which make it different fromthe adult skeleton, are more pronounced in younger patient s, and gradually becomeless pronounced with the prog ression of skeleta l maturat ion .
The increased bone plasticity (and elasticity) , which results in a gre ater absorption of the damaging force s responsible for the traumatic event , make complete rupture of the matrix bone in children a rarer event than in adults; therefore, different ,incomplete fractu res type s are most commonly seen, and are typ ical of the developmental age but not of adults. Also, since ligaments are gene rally stronger than theopened physis, a low-energy trauma such as a distor tion that can cause a ligamen tinjury in an adult, result s more frequently in a physeal fractu re in a skeleta lly immature individual. Fina lly, as long as the physis is open , the presence of a relative lowresistance zone help s to ensure that disloc ations are extremel y rare in children, particularly in pre-adolescence.
Childre n, therefore, present a wide variety of fractures, which no universally recognized classi fi cation includes entire ly. In addition to comp lete fractures, which arealso found in adults, there may be other types of fractures that are exclusive to andtypical of childhood, such as (Fig . 1.6): plastic defor mation , "torus"- type compres-

1
10
NORMAL PLASTICDEFORMATION
GREENSTICKFRACTURE
F. Martino et al.
BUCKLEFRACTURE
Fig.1.6 Several types of incomplete fracture oflong bones, characteristic of the immature skeleton
sion fracture, "green-stic k" fracture, and metaphyseal- ep iphyseal or apophysea l fractures, with or without detachment.
1.5.1Complete Fractures
In children and adolescents, complete fract ures are usually the result of high-energytraumatic event s, such as fall traum a or be ing run over by a car. Just as with adults ,for complete ped iatri c fractu res the site should be described, as well as the possibledisplacement of the stumps, the numb er of fractures, and the progre ssion of the fracture line (which can be transver se, spira l, obl ique , longitud inal, or branched ). Theorient ation and the course of the fracture may suggest the mech anism by which ittook place . Complete fractures in children most frequently affect the diaphysis oflong bon es.
In transver se fractures , the fractu re line is perpendicular to the majo r axis of thebon e. Thi s type of fracture is typic al of adolescence and of stage II-Ill childhood,and may also involve the met aphysis. Transverse frac tures are usually the resul t of adirect impact or shear forces (Fig. 1.7).
In obl ique fractures , the frac ture line is variously angled (usually about 30° to45°) to the longitudinal axis of the bone. The fractu re is usually caused by axial overload ing forces or by shear forces simi lar to those determining a transverse fracture(Fig. 1.8).

1 Major Traumatic Bone and Joint Injuries:Overview 11
Fig.l .7Transverse complete fracture of the distal metaphysis of the radius, in frontal (a) and lateral(b) view; complete transverse fracture of the femoral shaft in frontal (c) and lateral (d) projection
Fig. 1.8 Anteroposterior (a), and lateral (b) radiograph of the radius, showing oblique fracturethrough the distal diaphysis; oblique fracture of the ulnar diaphysis, in anteroposterior (c) and lateral (d) view, with undisplaced fracture of the midshaft of the radius
In spira l fractures, the "spiral" fra cture line oc curs more frequently in the di aph
ys is of th e long bone, and is caused by torsion forces rath er than direct forces. These
fractures , though often du e to maltreatmen t, arc not un common in trauma caused by
acc id ental fall with a blocked limb, as happen s, for exam ple, with spi ral tib ia frac
tures in toddl er s. On the oth er hand, humeral spira l fra ctures ar c highly sus p ici ous for

12 F. Martino etal.
1
Fig.1.9 Spiroid fracture of the femoral diaphyseal upper third, in frontal (a) and lateral (b) projection; tibia and fibula distal meta-diaphyseal spiroid fracture, in frontal (c) and lateral (d) projection
a non- accidental traum a caused by ill-t reatment, secondary to the application of torsiona l forces such as tho se occuring when a limb get s twi sted. It is not always possible on radiograms to distinguish an oblique fracture from a spira l one , and the typeof fracture that is detected may require additional projections (Fig . 1.9).
In longitudinal fractures, the course of the fracture line follows the long axis ofthe bone. Thi s type of fracture, which can also propagate in an oblique or spiraldirection, occurs more frequently in adolescence and stage III childhood, when thebone diaphy sis undergoes a progressive maturation of its bone component.
In comminuted fractures, the fracture line propagates in different directions,branching and causing multiple fragments of var iable size. The se fractures are rarein children, but can occur during adolescence, part icul arly at the tibia.
1.5.2Plastic Deformation
Plastic deformation con sist of a stabl e bowing of the bon e, with no evident fracture,and occurs when the diaphy sis of an imm ature bone recei ves a bending stress from alongitudinal compress ion of such intensity and dur ation that it exceeds the limit s ofelasticity but is not suff icient to produce a frank fracture . This stable curvature isactua lly caused by micro-fractures that are not visible rad iogr aph ically, occurring on

1 Major Traumatic Bone and Joint Injuries:Overview 13
a
Fig. 1.10 Plastic deformation. a Schematicexample; b plasticdeformation of the radius with"torus"-typefracture (arrow)
the concave side of the invol ved bon e. Plast ic deformation is mor e frequent at thefor earm (uln a and radius), where it restr ict s or even prevent s pronosupination movement s; it can also be seen (although to a lesser extent) at the level of the femur (ininfants) or fibul a. It usually displays fracture at the bone adjacent to the affectedlimb , and occasion ally it is associated with subluxation (di slo cation) of the corresponding joint s. Sometimes it affect s both bones of the skeletal segm ent involv ed. Insome cases there is co-existing perio steum dissect ion with subperiostea l hematomaform ation. If this occurs in a child und er the age of 4 years, or if the angle is less than20°, the deformity usuall y adjusts itself with growth . In other cases, particularlywhen combined with a fracture or dislocation of the adjacent bon e, the reduction maybe particularly complicated or even impossible (Fig. 1.10).
1.5.3"Torus"-type Fracture
"Torus"-type frac tures are due to an exce ssive cur vature of the immature bone, produc ing a compression fracture on the side of the concavity . Usua lly they result froma fall on a hyperext ended limb . They are determined more often at the level of themetaphysis, in the transitional region (from the metaphyseal bone tissue to the diaphyseal lamellar bon e), where the compact bon e is th inner and the spongy bon e isbetter represented. Typically, they are manifested as a swelling of one or both sides

14 F. Martino et al.
1
Fig.l .ll "Torus"-type fracture a Schematic example. b, c Distal metaphyseal fractureof the radius,in frontal (b) and lateral (c) projection
of the cortex; hence the architec tural comp arison with the "torus" is derived - that is,a compari son with the bul ge that separates the shaft of a column from its capital.Such lesions most commonly affect the wrist and tibia metaphysis (Fig . 1.11) .
1.5.4"Green-stick" Fracture
"Green-stick" fracture s, whose radiograph ic appearance resembles that of a greenbranch that is not fully broken , are dete rmined when bone flex ion exceeds its ownendurance limits on the side of ten sion, namely the convex side. Typically they resultfrom indirect trauma such as a fall on an outstretched hand (on an extended arm) .These are incomplete fractures, with the fractu re line branching from the side of convexity with in the marrow, without reaching the cortex and the periosteum of the concave side, which , therefo re, remai ns intact although it may suffer a plastic deformation. These fractures occur preferenti ally in the diaphyseal-metaphyseal forearm,although they can also be found at the clavicle level , in the leg and in other longbones. It is not unusual to find a "green-sti ck" fracture in one of the fore arm bonesand a complete fracture (or an incomplete "torus"-type fracture) on the other bone(Fig. 1.12) .
1.5.5Metaphyseal-epiphyseal Fractures (of the Physeal Plate)
Fractures of the metaphyseal-epiphyseal complex (incl uding the epiphysis, thegrowth cartil age plate , surrounded by the Ranvier osteo- f ibrous zone, and the metaphysis) are typical in pedi atri c patients and are the equ ivalent of an adult ligamentinjury and/or (complex) met aphyseal-epiphyseal fractures. In the age of skeletal

1 Major Traumatic Bone and Joint Injuries:Overview 15
growth , es pecially in adoles cence, approximate ly 35% of fractures invol ve the physi s
mo re or less ex tensively. In th ese les ions, involvem ent of the cartilaginous growth
plate can be preci sely ob ser ved, and can be divided, from a hi stological standpoint
into four zones (Fig. 1.13) . Sta rt ing from the epiphysis these are :
I . th e germinal zone of reser ve cart ilage
2. th e zone of cartilage proliferat ion
3. th e zone of hyp er trophic ca rt ilage
4 . th e zone of provisional calc ifi cation.
Fig. 1.12 "Green-stick" fracture. a Schematic example. Radial distal metaphyseal "green-stick"fracture (arrow) and ulna "torus" (arrowhead) in frontal (h) and lateral (c) projection
Fig.l .B a Anteroposterior wri st radi ogr am ,which indicates the radio-transparent bandwidthaspect corresponding to the physis of theradius (inset); b anatomical diagram of thecarti laginous growthplate

16 F. Martino et al.
1Zones I and 2, with the characterist ic columnar arrangement of chondrocytes,
correspond to germ inative activity of the physis, which induces cartilage prolife ration and ensure s the lengthening of the bone . Zone 3, with large swollen chondrocytes, corr esponds to the region where the chondrocytes degene rate and meet the calcifi cation (zone 4) and ossific ation (metaphyseal border). The fi rst two areas, closerto the epiphysis, are rich in car ti lage mat rix and are therefor e more resis tant tomechan ical stress. The third zone, characterized by the presence of hypertrophicchondrocytes, has less resis tance to both shear forces and flexion and traction . Thefourth zone, closest to the metaphysis (and made more durable by calcification) , isthe reg ion with more resistance, between the cartil age on one side and the bone onthe other, but it is weaker than the firs t two zones. Therefo re, the epiphysea l displacements concern zones 3 and 4 of the growth cartilage in particular.
The traumatic mechan ism of this type of fracture also depends on the child's age.In fact , as long as the epiphysis is cart ilaginous, it works as a sort of shock-absorber,transmitt ing the forces directly to the metaphysis, and involving only part of thephysis.
With advancing ossification, the amortization characteristics of the epiphysea lcartilage are gradually impaire d, and therefore the forces are transmitted, in a concentrated manne r, to the physis, which , as already mentioned, is involved in almost35% of immat ure skeletal trauma , with the incidence increasing with age (from 10%durin g childhood to 35% during adolesce nce). Over 75% of metaphyseal-epiphysealfract ures present between the age of 10 and 16 years, with the exception of elbowfracture s, which are more frequent between 3 and 6 years.
The majority of fractures of the physis (over 80% of cases) are caused by cuttingforces (tangenti al) or avulsion force s. Lesions of the physis by compre ssive forcesare less frequent (less than 20%), becau se the porou s bone structure makes the metaphysis less resis tant than the growth plate to thi s kind of stress .
In summary, in childhood, when the physis is thicker, cutting and avulsion forcesmore frequently determine epiphyseal displacements, which in older children andadolescents are more often determined by a comb ination of shear and angular (torsion- distraction) forces . Near the end of growth , when part of the physis is more subtle or partially closed, intra-articular cutt ing forc es with or without angular forcesmost frequently cause metaphyseal-ep iphyseal ar ticular fractures. Instead, when acompressi on force is acting , it fir st results in a fracture of the metaphyseal region,and then prop agate s to the physis, damaging all layers. Although, as noted earl ier, thegrowth carti lage is weaker than the adjacent bone , fractures of the bone structures inchildren and adolescents are always more frequent than fracture s of the physis, dueto the size and type of forces required to damage the physeal plate.
Similarly, since children's tendons and ligaments are more resistant than the physeal plate, it is more likely that a trauma will cause an epiphyseal avulsion fracture(or a fracture of the apophysis) rather than a rupture of the ligament (or tendon). Themost vulnerable physcs, more often involved at the occurrence of a traumati c event,are those of the wrist and ankle. The major complications of th is type of fractur e arearrested development and alterat ion of articular congruity.

1 Major Traumatic Bone and Joint Injuries:Overview 17
Fig.1.14 Schematic representation of Salter-Harris classification
If there is no damage at the germ inal layer of the carti lage cell s or at the locoregion al vascularization , consolidation of a fracture of the growth plate is very fast.A full restoration of the growth plat e occurs in about 3-4 weeks.
The most commonl y used classification to encode metaphyseal-epiphyseal fracturesis that described by Salter and Harris (Fig. 1.14), which divides them into five types, andcorrelates radiological events, place, incidence and morbid ity, with each one.
Type I follows an impact lesion of the physeal plate, and is characterized by a tearof the growth cartil age along the horizont al plane , corresponding to the layer ofhypertrophic or degenerated cell s, while the rest of the cartil age remains supportive to the epiphysis, with a cross- slip of the epiphyseal nucleus. In the se fracture s, the per iosteum usually remai ns attached to the growth cartil age , thu s preventing a serious breakdown of the fractu re. If there is a minimal perio steal lesion ,the only radiographic sign evident is a slight diastasis of the physis (Fig. 1.15) .These fractures are more common in children youn ger than 5 years, when thephysis is relat ively thick, with the exception of prox imal humerus fractures inwhich the peak age of incidence is between 10 and 12 years. The diagno sis ismainly based on clini cal suspicion, eventually validated by the radiographicdemonstration of an epiphysis disloc ation (mo st often due to slipping, with orwithout physis diastasis) . In doubtful cases, the diagno sis can be easily confi rmed by performing a magnetic resonance imaging (MRI) examination.Salter-Harr is type I lesion may also be minimal and take place without a recognizable epiphyseal displacement, thus resulting in a negative radiographic inspect ion. In such cases, a new rad iographic evaluation, performed after an inter val of8-10 days since the traum a, may have a positive result and may show the presence of a thin band of spongioscle rosis close to the physis, with irregular appearance of the bord er of the physis (repairing side), orienting the diagno sis toward

1
18 F. Martino etal.
Fig.1.1S Salter-Harris type I fracture ofthe distal edgeof thetibia. a Schematic example; b contralateral healthytibia; c, d physeal fracture, with mildepiphyseal separation, in frontal (c)and lateral (d) projection
this type of fracture . The prognosis for the se fractures is good, even when they aredisplaced, provided the re is a prompt reduction. Although thi s type of injury isnot usually assoc iated with vascul ar disorders, a complete det achment of the epi phy sis at the femora l proximal extreme may cause ischemic necrosis and growtharrest.Type II is character ized by the coexistence of an incomplete fracture of the phy sisand a fracture of a met aphy seal edge (Fig. 1.16). The injury mechanism generate sa viol ent bending stress in the metaphyseal-epiphyseal segm ent , resulting inperio steum inj ury on the side subjected to traction forc es, with a tear in thegrowth cartil age along the transvers e plan e; the contextual angular displacementof the epiphysis, with rotation on the point of flexion , induces an oblique deviation of the fracture plan e in the direction of the metaphysis , inducing an angulardetachm ent of the metaphyseal edge (Thurston-Holland sign). The periosteum isusuall y damaged on the involved side dur ing traction (site of lac eration andphysis widening) , but it is intact on the compression side, where the metaphysealfragm ent is found (where the growth cartilage is intact). This type of fracture ismor e common at the distal radius and phalanges, in chi ldren older than 10 years(Fig . 1.17). In most cases the reduction is not part icularly complicated and theprognosis is favorable .
• In type III the re is incomplete growth carti lage plate injury combined with a vertic al and/or oblique fracture of the epiphyseal nucleus, with involvement of thecartilaginous lining of the articular surface (Fig . 1.18). On the side of the growth

1 Major Traumatic Bone and Joint Injuries:Overview 19
Fig. 1.16 Salter- Harris type II compo sed fracture. a Schematic example ; b, c radial fracture(arrow) without stumps dislocation, in frontal (b) and lateral (c) projection
Fig. 1.17Salter- Harris type II displaced fracture. Fracture with dislocation of stumps of the base of the4th toe proximal phalanx, in frontal (a) and oblique (b) projection
Fig. 1.18 Salter- Harris type III fracture. a Schematic example; b tibial distal epiphyseal fracture(arrows)

20 F. Martino etal.
1
Fig.l.19 Ten-year-oldpatient withangular varus deformity of the distal third ofthe lowerright limb, withshortening ofthe tibia, secondary to the formation ofa transphysealbone bridge (arrow) andfocal growth arrest, resulting fromSalter-Harris typeVmisdiagnosedfracture
cartilage tear , a metaph yseal- epiphyseal diastasis is observed, as well as a dislocat ion (usu ally small) of the epiphyseal fragment, which is detached and mobilized from the metaphy seal surface, because of the fracture. These quite rarelesion s are caused by int ra-articular shear force s (with or without the combination of angular forces) and they usually occur at the level of the prox imal and distal tibia epiphysis. Arrest of growth and residu al bone deformit ies are rare event s,except in a case of non-reduced fractures.In type IV lesion s, the epiphyseal fracture line extends obliquely in a proximaldirection, with a full-thickness growth cartil age lesion , reaching the met aphy sis,where it produces det achment of a bone 's edge . It is always rel ated to unstablefractures, which require appropriate treatment. They are more common at the distal humerus and distal tibi a level s. These are lesion s with the worst prognosis,bec ause of involvement of the growth cartil age germinal layer, situated close tothe metaphysis, and they may comprom ise the regul ar growth of the long bone.Typ e V lesions are the result of compression forces that affect the growth car tilage surface, more or less orthogonally, caus ing its destruction by crushing and/orcausing serious damage to the loco-regional vascul atu re, but without invol vementof the epiphyseal nucleus. These relatively rare lesion s are often locali zed at thefemur, knee, and ankle level. As with type IV lesion s, physis impact inj uries alsoconstitute a high risk of a longitudinal foc al arrest of bone growth, with secondary deformity. Complete arrest of bone growth can result in a signif icant limblength discrepancy, with functional lim itations. Parti al arrest may cause an angular deformity (Fig . 1.19) or a progressive shortening. In the se cases, as in type Ilesions, radiograph s may not be diagnostic, so if there is cl inical suspicion of atype V lesion , running an MRI survey is highly useful for both diagno sis and subsequent controls.
The Salt er-Harris cla ssification was subsequentl y extended by Ozonoff, Rangand Ogd en, with the assistance of more careful study of lesion s using MRI , and fouradditiona l types were added (Fig. 1.20) :

1 Major Traumatic Bone and Joint Injuries:Overview 21
Fig. 1.20 Schematic representation of Salter- Harris additional fracture types (type VI, VII, VIII,and IX) according to Ozonoff, Rang, and Ogden
Type VI involves the perichondrium and the edge s of the physis, with reactiveperiostiti s loca ted out side the physeal plate . The secondary form ation of a bonebridge limit s and/or stops the physeal plate growth, resulting in a metaphy sealepiphyseal angulation. These fractures are rare and are usually caused by a directblow (direct traum a).Type VII only affects the epiphysis, without involving the physis. It is a relatively frequent and important fracture, which , be ing a transcondral fracture, canaffect the elbow, hip, knee , or ankle.Type VIII is an isolated fracture of the met aphy sis, which reduces the metaphyseal vascul arization and inte rfere s with the endochondral ossifi cation .Type IX affects the periosteum and the emergent membranou s bone.
1.5.6Apophyseal Detachments
The apophyses are bony outg rowth s onto which tendon s or ligament s inser t. In children and adolesce nts these apophyses are originally made up of cartilage, which laterbecome s the site of secondary ossif ication, until it reaches full development andfusion with the adjacent metaphy seal-epiphyseal bone . The apophyseal cart ilage sidefacing the teno chondral junction, consists of growth cartilage, the so-called apophyseal physis (with a typ ical columnar arrangement of chondrocytes), on which tendons

22 F. Martino etal.
1
Fig.l.2l Schematic representationof the apophyseal tendon insertion in the growth skeleton
and ligament s insert via Sharpey 's fibers, which partly continue in the perichondriumand are partly anchored directl y on it (Fig. 1.21).
The apophyseal hyal ine cartil age is a weak point when traumatic insult occur s;therefo re, abrupt avul sion hyper- sol icitation , which usually spares tendons, ligaments , and bon e, can lead to cartilage fractures (a particularly weak area is betweenthe growth nucl eus and the metaph yseal bone) producing a detachm ent. Apophysealdet achments are more common in adoles cents engaging in sporting activiti es (or inoth er leisur e activi t ies with intense physical stress, such as dancing) and mainlyaffect the pelvis and the knee, since these are the most stressed part s in the most popular spor ts (football , tenn is, etc) as well as repre senting the locations with the highest numb er of apophyseal growth nucl ei compared to other skeletal sites (Fig. 1.22).In the apophyseal detachment s, the instrumenta l document ation uses both ultr asoundand the conventional radiological examination in a comprehensive way; in doubtfulcases, MRI plays a definitive diagnostic role .
As already discu ssed, the pelvis and knee are the skele tal sites most commonlyinvolved in apophysea l detachment s that, in order of frequency, affect : the ischi altuberosity, the anterior superior iliac spine (ASIS), the anterior inferior iliac spine(AilS), and the pubic symphysis at the pelvic level, and the ante rior tibial tubero sityand the tibi al spine at the kne e level.
Detachm ent of the ischia l tuberos ity is caused by a forc ed contracture (gymnastics, socce r, fencing, athl etics, etc) or by passi ve distension s (dance) of the ischialtibial mu scles. Detachemnt of the ASIS , on which the sartorius and tensor fasc iaelatae muscles insert, is caused by a forced hip extension, particularly in football players , sprinters, and jumpers. AilS det achment is secondary to a forced direct tendonhyperextension of the femur's stra ight muscle, as happens in the case of an "emptykick" with a posture of maximum hip flexion and knee extension (Fig . 1.23) .

1 Major Traumatic Bone and Joint Injuries:Overview 23
Fig.l.22 Integrated imaging depicting an apophyseal detachment of the growth nucleus distal portion from the left iliac crest (arrows) in a 16-year-old injured football player. a Ultrasound; b conventional radiography; c CT
Fig.l.23 Sagittal ultrasound images (a) and CT (b) of AilS detachment (arrows) in an adolescentathlete
Pubi c symphys is detachments are ca use d by sudden or rep eat ed forced adductionmovements, involving the long and short adductor mu scles, which insert on the angular surface of the pubis. Acute det achments of the anterior tibi al tuberosity (apophysea l fracture-detachments) are avuls ion of the anteri or tibi al apophyses, where thetraum atic event is rep resented by a violent, active knee extension (football , rugby),or by its sudden passive flexion contrasted by a qu adriceps mu scle contraction(basketball , volleyba ll, gym equipment). These det achments corre spond to type I orIII of the Salt er-Harr is classi fic ation, and are subj ect to a spec if ic thr ee-type classific ation system as de scribed by Wat son-Jones and modified by Ogden.
Det achments of the tibi al spine occur mo st frequently in children between theage of 8 and 14 years, and are the res ult of a knee hyperextension and extra rota tiontrauma - an eve nt that can ca use an ant erior cruciate ligament rupture in adults .
Bon e detachmen t alwa ys occurs in the po sition of the anteri or inte rcondy la r emi nenc e. Physical ac t ivities frequently involve d in th is lesion are cycling and skii ng.Meyers and McK eever described thr ee ma in types of intercondy lar fra cture.

24 F. Martinoet al.
1Physeal inj uries of the verte bra l body can also occur at the spine (at the growth cartilage/ring apophysis junction) , due to the insertion of the anu lus periph eral f ibers(Sharpey's fi bers) in the apoph yseal sec ondary ossification point of the ver tebral soma.
1.6Imaging in the Follow-up
The purpose of an imaging investigation at follow-up (immediately post-treatm ent)is to che ck the corre ct fracture reduct ion and/or dislocation, along with the correctpositioning of the therapeutic materials. The goals of subsequent imagings are toconfirm that consolida tion has taken place and to veri fy the abs ence of any ass ociated unfavorabl e evolution, the mo st important being di sturbance of foc al growth, secondary to a circumscribed insult that has dam aged the growth cartilage ; avas cularnecrosis; and septic complications.
1.7Fracture and/or Dislocation Reduction - Synthesis - Consolidation
The reduct ion and synthesis of a fracture or dislocation usually need a radioscopiccontrol , in orde r to gu ide the surgica l procedure during the intervention , and a radiogr aphic ass ess ment soon after the surgery, to veri fy that the therapeutic treatm enthas been successful or that it needs fur ther correction s. After reduct ion , fra cture stabilization is achieve d by con servativ e treatment with cast immobilization, or bymean s of surgica l procedures of f ixation, depending on the stabi lity of the reducedfrac ture (Figs. 1.24 and 1.25) .
Fig.1.24 Femoral Salter- Harris type II distal diaphysis-metaphyseal fracture, in frontal (a) and lateral (b) view. c Radiographic postoperative control after fracture reduction and fixation throughKirschner wires. d Control after the removal of fixation devices, which allows visualization ofth egood fracture reduction in the process of consolidation

1 Major Traumatic Bone and Joint Injuries:Overview 25
Fig. 1.25a Lateral radiograph of the knee, showing a Salter-Harris type II proximal metaphysealdisplaced fracture of the tibia. b Image intensifier view of intra-operative control after fracturereduction by trans-skeletal traction. Radiographic control in A-P (c) and L-L (d) projection, inplaster with included tension wire. Radiographic control in A-P (e) and L-L (f) view, performedafter removal of the plaster cast and traction wire, which allows visualization of the good reduction of the fracture in the process of consolidation
Th e con sol idation and stabilization process of the fracture is ac hie ved with the
formation of bon e ca llus . Initiall y, the subperios teal fi brous callus sur rounds thefracture, joining the fragment s at th e top and thereby pro vid ing th e best guarantee forth eir immobil it y and stabi liza tion. Th e callus extensi on dep end s on the extent of dislocation suffere d by the stumps during traum a, becau se the gr eat er the d islocation,
th e mo re extensive th e perio steum di ssect ion and subsequen t hematoma will be.During the growing age , th e per io steum is thi cker and more robust than in adults, and
rar ely break s. On th e con cave side of angulated displ aced fractures, the periosteummo stly remain s int act (th is is useful for reduction maneuvers) , although the
pe rio ste al str ipping predominantly occu rs on thi s side . The radiological sign of a
sta ble con solidat ion is given by the pre sence of a subperiostea l calcified callus,
which has approxima te ly the same den sity as the adjacent cor tica l bone (Fig . 1.26)

26 F. Martino etal.
1
Fig.l .26Various stages of consolidation of a spiroid fracture in the middle third of the femoral diaphysis in a young patient aged 2 years. a Radiographic examination on the day of trauma; b the testperformed after 18 days demonstrates the calcification ofthe subperiosteal callus; c the radiographic control 40 days after the trauma shows the initiated ossification of the perilesional callus
and is recognized in at least three out of four cortica l bone profiles represented in theA-P and L-L orthogonal projection s. Such a radiographic outline, combined with theabsence of pain during palpation, can determine the success ful sta biliza tion of a fracture. The appearance of the callus below the lesion occurs later, and is manifested bythe obliteration of the fracture line ; a "green-stick" type of fracture take s more timeto rep air. The subsequent rep air is carried out through ossification of the calci fiedcallu s, whi ch requires a few months afte r the function al recovery, and later throughremodeling, wh ich requires a few years. During growth, then, residu al deformitie s(tolerated stumps angle or callus exuberance) are reworked and remodeled to getclo ser to the or iginal morphological structure, helped by a regained physiologicalfunction .
A con solidation del ay is not common and usually occurs whe re there is littlecompression of the fragments, as may happen in insuffic iently reduced "green-stick"fractures, or in stumps angulation fractures with a less favorable orientation (anangular devi ation on the sagitta l plane is more recoverable than one on a coron alplane , and generally a varu s devi ation is mo re favorable than a valgus one). The radiogr aphic control shows per sistence of the fracture line , on which the pre sence of asubperiostea l callus inte rruption is observed (Fig. 1.27) . The se del ays in con sol idation represent weak points, and can induce a fracture recurrence within one year ofthe initial trauma. However, with the exception of tho se occurring at the elbow level,post-traumatic pseudoarthrosis usually has a favorable prognosis in childhood andadolescence .

1 Major Traumatic Bone and Joint Injuries:Overview
1.7.1Growth Arrest
27
Fig. 1.27 Delay of consolidation in a proximalmetaphyseal-diaphyseal fracture of the humeruswith a mild valgus deviation and discontinuityof the subperiosteal callus on the medial side(arrows)
Prem ature clo sure of the physis, with growth arrest and con sequent skeletal de formitie s, represents a feared and unfavorable outcome of a trauma. Fortunately, thi s is avery uncommon event , which in most cases affects the knee and the ankle. In thi s situation, the physis is exception ally involved throu ghout its enti re extension , whereasa lesion usually only part ially affects the cartil age growth plate . The cartil age lesionmay occur as a result of a cru shing destruct ion (Salter-Harr is type V) that is a tearwith a severe and irreparable loc ali zed vascul ar damage (about 35% of cases inwh ich the re is stumps disloc ation) . Trauma -related severely damaged cartilageundergoes ossification, with form ation of a bone bridge between the epiphysis andthe met aphysis. In the place of inj ury, then, the bone has a foc al growth arre st wherecart ilage damage occurred, wh ile smooth growth take s place , as usual , in theunharmed surr ounding bone. The result is an anomalous sha ping of the skeleta l segment, which leads to an angular deformity in cases whe re the lesion is loc ated in aperipheral area . In mo st cases, conventional radiography cannot detect the presenceof the transphyseal bone bridge and, the refore, if there is th is diagno stic suspicion, itis essential to complete the ass ess ment using either a CT, or, preferably, an MRI sca nconducted with appropriate sequences for the cart ilage study. Once the lesion hasbeen diagnosed, treatment may include transphyseal bone br idge resection, and theprogno sis is good if the damage involves less than 50% of the physis, and if there issti ll a gro wth expectation of at least two years . Oth erwise, the angul ar deformity canbe correct ed by real ignment osteotomy (Fig. 1.28) .

1
28
1.8The Ro le of Diagnostic Imaging
F. Martino etal.
Fig.1.28 a Varus angular deformity by growth arrest of thedistal end of the left femur,secondary to fracture, subsequently subjected to metaphyseal osteotomy for correctivetreatment of varus malalignment (b)
In the diagnostic pathway for pedi atric skeletal trauma, imaging plays a major role ,
thanks to the many tool s ava ilable today, although a conventional rad iographic
approa ch is often suff icient and recommended. With re spect to radiation protection
for young patients, it is a good premise th at any radiographic ex amination should be
re served only for situa tions when it is abs o lutely essential for a proper diagnosi s
and/or it can influence the therapeutic stra tegy, or it is needed as a basic reference in
the follow-up during tre atment. Th is obviously requires the radiologist to have a deep
understanding not only of the use of diffe rent im ag ing modalities, but also of the
pathogenic mechani sms and cl in ical as pects of the di fferent pathological patterns of
pediatr ic trauma, and po ssible interrelat ion ships with other coexi sting and predispos
ing pathologies.
1.8.1Conventional Radiology
Conventional rad iology still represents the fir st level of diagnost ic study of bone
trauma, although it gives poor inform at ion about pe ri skeleta l soft ti ssue injury, espe
ci ally if compared with ultrasound and MRI. A correctly performed radiologic study,
however, allows an ove rall evaluat ion of soft ti ssues, and ca n often show indirect
signs of joint effu sion or hemarthrosi s (such as the " sail sign" , an indirect sign of an

1 Major Traumatic Bone and Joint Injuries:Overview 29
elbow occult fracture, determined by lift ing of the hum eral coronoid fossa fat pad,due to ca psular distension cau sed by an intra-art icul ar bleeding) .
Recognition of fractures in childhood, more than in adults, requ ires at least twoproj ections, usuall y in orthogonal planes, allowing accurate determination of possible misal ignment and deformities that are liabl e to affect the therapeut ic treatm ent.It should be noted that standar d proj ect ions are som etimes not able to show sma llfracture lines or fractu res local ized in specific anatomical sites; so, where the doubl eA-P and L-L proj ect ion of the radiologica l examina tion is negative, but there rema inssuspicion of a lesion from the pati ent 's clin ical evaluation, it is important to performadd itional proj ect ions, which will differ dependi ng on the ana tomica l region und erexamination . It is also recommend ed that at least one of the two joints corres pondingto the traumati zed bon e segment (preferabl y the near est one and/or the mo st painful)are repr esent ed on the rad iogram. Where trauma has occur red, therefo re, the use ofconvent ional radiology will be primarily directed to evaluating the major traum at icinjuries (fr actur es, epiphyse al and apophyse al displacement , disloc ations) and theiroutcomes (dise ase of the bon e callus, myositis ca lci f ication, etc ).
1.8.2Ultrasonography
Ultrasound invest igat ion is complementary to convent ional rad iology, and is eas ilyavail able, at low cost , with the benefit of being free from ioniz ing rad iat ion .Ultrasonography provides a good repr esentation of periskeleta l soft t issues, allowingclarification and/or conf irmation of suspec ted radiographically hidd en fractures(Fig. 1.29), apophyseal det achments and th e apophyses (an example isOsgood-Schl att er 's disease) , which are much mor e frequent in a development al agethan tendon or ligament injuries.
Fig. 1.29 a Negative confirmation of the radiographic control performed after blunt trauma to theskeleton rib. h On the basis of symptoms, an ultrasound check is performed focusing on the siteof pain, which documents the rib fracture (arrowhead) , which was missed on radiological examination, and the corresponding parosteal hematoma (arrows)

30 F. Martinoet al.
1Furthermore, especi ally in infants where the epiphyseal nuclei are not yet calci
f ied, ult rason ography allows immedia te and thorou gh study of the carti lagi nousnucle us and eva luation of any post-traumatic dislocat ion (for example, epiphysealnucle us avulsion) that conve ntional rad iographic inves tigation may not be able tohighli ght. Sup erfi cial hematomas and intr a-arti cular depo sit are other pathologicalconditions that are easi ly diagnosed using ult rasonograph y. The use of color mod eand, in par ticular, power-Doppler, may also be advantage ous for bett er def inition ofthe events taki ng pla ce in the repa ir of ske letal mu scle injuries.
1.8.3Computed Tomography (CT)
Due to its large use of rad iat ion , th is is rare ly used in the eva luat ion of trauma inyoung pat ients, except in cases where the firs t-level investi gat ion s have not pro videdsufficient detailed in formation on the extent and seve rity of the injury (with exactdefinition of the number, size, and relat ion s between bon e fragments, and the possible presence of loo se intra-articular bod ies) to enable prop er treatm ent to be und ertaken, such as during spina l injuries, complex pel vis and knee fractu res, or problematic osteo-arti cul ar circum stances (Fig . 1.30) . The advent of multi sl ice CT, with thepossibil ity of multiplanar and three-dimensional reconstruction s, has offered anadditional perspective that is more helpful for the surgeon in the extensi on study and
Fig. 1.30 Salter-H arris type III proximal metaphyseal-epiphyseal fracture of the tibia and proximaldiaphyseal, oblique and broken fracture of the fibula. a-c Radiographic control (a), CT in axialsection (b) and in reconstruction in the coronal plane (c)

Major Traumatic Bone and Joint Injuries:Overview 31
the follow-up for complex traum atic lesion s, as it allows bett er planning of the therapeut ic inter vention, as well as early detect ion of development of possibl e defo rmities, or, in the case of extended growth cartil age fractures, premature clo sure of thephysis, res ulting in growth arr est.
The inevitability of CT in polytraum ati zed young pati ent s must be rememb ered,where the execution of a singl e examination, without add it ional radiograph ic examination s, is less stress ful because the pat ient does not have to change posit ion dur ingimage acqu isition . It also allow s a compl ete assessment of both the cran ial parenchymatous, visce ral thoraco- abdominal , and skele ta l components . ln fact , one of theadvantages, part icul arly with mult islic e CT, is the possib ilit y of retrospective reconstruc tion of coll ected dat a (usuall y with 5-mm-thick layers) acco rd ing to differentalgo rithm s, using thinner layers and a smalle r scan rang e.
1.8.4Magnetic Resonance Imaging
Like CT, this is a second-level examination reserved for tho se cases that are not full yresolved with the primary methods. So far the use of MR[ has been limited by itscost, the fact it is not available in all departments, and its longer than average examination time . lt is inherently a multiplanar and multiparametric examin ation, allowing direct acquis ition of informati on on di fferent space planes, and offering differentti ssue-t ype representations of the same structure , high lighting the evidence of theti ssue component in relation to the diagnostic probl em under investigation .
Tr-weightcd sequences in part icul ar provide great anatomical detail ; they highlight fat well and are particu larly suitable for studies with intravenous injection ofcont rast medium , whereas Tz-weight ed sequences allow an accurate assessme nt ofedema and flu id effusion. In combination with algorithms for suppressi on from thefat signa l, and enhance me nt from the fluid , they are useful in assessing impac t bonelesions, stress fractures, and osteochondrit is dissecan s. Grad ient- echo sequences alsoallow an accurate study of ligament s, tendons, meni scus fibrocartilag e and art icularcartilag e, as they provide precise evidence of hemo rrhage and labral lesion s.
MR[ provides useful information and has valuabl e advant ages for demon stratingsome radiograph icall y hidd en fractures, and in assessing impact bon e lesion s, balancing the extent of dislo cation of ossification nucl ei (in order to addr ess a conse rvative or surgical therapeut ic approac h), in complex epiphyseal and apophyseallesion s, and in subsequent determination of a possible growth ar rest caused by premature closure of the physis (partial or full), in stress fractures (tib ia, calc aneus, andcuboid), and in osteochondriti s dissecan s (knee , elbow hum eral condyle, talu s), aswell as in demon strating meniscal , ligament , cartilage and intra- and extra- articulartendon lesion s (Fig . 1.31).
ln mon itor ing physis traum a, MR[ shows the extent and dire ction (transverse orlongitudinal) of the lesion , and is also capable of recognizing the possible presenceof a post-t raum atic transphy seal vascul arity that pred ispo ses to the form ation ofosteo-fibrous bridge prodromal growth disorde rs (g rowth arrest, angular defo rmit ies,

32 F. Martinoet al.
1
Fig. 1.31 Sagitta l and corona l MR images of the left knee. The investigation documents the ACLlesion (a) , with evidence of artic ular effusion and hypointense focal area in T I (b) and hyperintense in T2 sequences with fat signal suppression (c) at the lateral condyle, attributable to a bonelesion caused by impact (asterisk)
shortenings) if no t promptly treate d (r esect ion fo r bon e brid ges involvi ng less th an
50% of th e physi s or epi physiolysis for more ex te ns ive bone brid ges) . In thi s regard,
the Shapir o pathophysiological cl assif ic ation of fracture s involving the ph ysis, has
become w id el y used, and recognizes th ree types:
• type A, in wh ich th e avascular ph yse al cart il ag e becomes a barrier between the
vascula r ization of th e epi physis and th at o f the metaphysis, prev enting the forma
tion of trans physea l fi brous or bony bridges
type B, in wh ich the frac tured phy sis all ows a tr an sphyse al vascu lar communic a
t ion betwe en the epiphy sis and metaphy sis (th is often occurs in Sal ter-Harris
type IY and Y fr actures)
type C, in which the fracture cause s an interruption of the epi physea l vascu la riza
t ion .
Suggested Readings
Andrish JT (1990) Upper extremity injuries in the skeletally immatu re athlete. In: Nichols JA, Hershmarm E (eds) The upper extremity in sports medicine. CY Mosby, St. Louis, pp 673-688
Ecklund K, Jaramillo D (2002) Patterns of premature physeal arrest. MR imaging of I II patients.AJR Am J Roentgenol 178:967-972
Jaramillo D, Shapiro F (1998) Growth cartilage: normal appearance, variants and abnormalities. MagnReson Imaging Clin N Am 6:455-47 1
Jaramillo D, Shapiro F (1998) Musculoskeletal trauma in children. Magn Reson Imaging Clin NAm 6:52 1-536
Johnson KJ, Bache E (2008) Imaging in pediatric skeletal trauma. Springer Berlin HeidelbergKujala U, Orava S (1993) Ischial apophysis injuries in athletes. Sports Med 16:290-294Landin LA (1997) Epidemiology of children 's fractures . J Ped Orthop B 6:79-83Light TR, Ogden DA, Ogden JA (1984) The anatomy of metaphyseal torus fractures. Clin Orthop
188:103-11

1 Major Traumatic Bone and Joint Injuries:Overview 33
Micheli LJ, Purcell L (2007) The Adole scent Athlete. Springer Science, New YorkOgden JA (2000) Skeletal injury in the child. Springer-Verlag, New YorkOgden JA, Gan ey TM , Ogden DA (1996) The biol ogical aspect s of children 's fractures. In: Rock
wood CA, Wilkin s KE, Beaty JH (eds) Fractures in children , 4th edition. Lippincott-R avenPublisher s, Philadelphia, pp 19-52
Ozonoff MD (1991) Pediatric orthopaedic radiology, 2nd edition. WB Saunders, PhiladelphiaPeterson HA, Madh ok R, Benson JT et al ( 1994) Physeal fractures : part I & 2 1979-1988. J Pedi-
atr Orthop 14:423-438Rang M (1983) Children 's fracture s. lB. Lipp incott Company, Philadel phiaSalter RB, Harri s WR (1963) Injuries involving the epiph yseal plate . J Bone Joint Surg 45 :587-622Siffert RS ( 1997) The effect oftrauma to the epiphysis and gro wth plate. Skeletal Radiology 2:21-
30Stevens MA, EI-Khoury GY, Kathol MH et al (1999) Imag ing features of avulsion injurie s. Radio
Graphics 19:655-672Thornton A, Gyll A (1999) Childre n's fracture s. A radiological guide to safe practice. WB Saun
ders Publishers, London, UKVon Laer Lutz (200 I) Pediatric fracture s and dislocation , 4th editi on . Georg Thieme-Verlag, Ger
manyWilki ns KE (1996) The incidence of fractu res in children. In: Rockwo od CA, Wilkin s KE, Beaty
JH (eds) Fractures in children, 4th edition . Lipp incott-Raven Publishers, Philad elphiaWootton JR, Cross MJ, Holt KW (1990) Avulsion ofthe ischial apophysis: the case for open reduc
tion and internal fixation. J Bone Joint Surg Br 72:625-627Wulff RN, Schmidt TL (1998) Carpa l fracture s in children. J Pediatr Orth op 18(4):462-465


Micro-traumatic Lesions Caused by Overuse: 2Overview
C. Defllippi, P. Pautasso and C. Falett i
2.1Introduction
In recent years the incidence of traum atic mu sculoskeletal lesion s experienced byind ividu als of pediatric age has been con stantly increasing; the majority of suchtraum a is linked to sporting activity.
It is es timated that in the USA more than one-th ird of the total trauma in the5-17 years age group is rela ted to sports, especially competitive sports . Althoughthere is a lack of preci se epidemiological data in Italy, the mo st recent studies sug ge st the inc idence is about the same.
There are severa l reason s for thi s:inc rease d numbers of tho se participating in sports, and a greater avai lability ofnew sporting activitiesa reduction in the age at which ch ildr en firs t part icipate in competitive sportsgreater socia l pressure , espe cially the "mass medi a" portrayal of "winningsportsmen" pushes young athl etes to go beyond their physiological limits in theirdesire to emulate in competitive sports, and parents may also be pushing theirchi ldren to succeed .Regardless of the reas ons for th is increas e in incidence of ped iatric spor ts trau
ma , it is important for the physici an to have a good knowl edg e of the num erous differences that exi st between adults and children; in the mu sculoske letal context it isparticularl y important not to assum e that a ch ild is a small adult.
In the subj ect of ped iatric age, it is important to understand the pathological pic ture in term s of the particular anatomy of the maturing skeleton (Fig. 2.1) especiallythe growth cart ilage (physis), the epiphyseal and apophyseal nuclei of ossification ,
C. Defilippi ( ~)
Pediatric Radiology Service, Regina Margherita Children's Hospital, Turin, Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
35

2
36 C. Defilippi etal.
Fig. 2.1 Magnetic resonance image of thegrowth plate
and the tendons and jo ints. In young athle :es the se sites repre sent the centers of leastresistance in the musculo skeletal apparatus, and are the sites of most frequent injury,wherea s in adult sportsmen when bony m..turation is compl ete the struc tures that are
least resis tant to mechanical injury are th» cap sular ligam ents and tendon s.Thus, similar mechanic al challenges c.m be the cau se of very different lesions, as
for instance in the case of acute traum a 0 f the knee, which in an adult may result in
lesion of the ligament s, while in a child tile same pathogenic mechanism will , in themajority of cases, instead cau ses a separa :ion-av ulsion of the tib ial apophysis.
It should also be rememb ered that lesion s of the oth er structures ment ioned arealso possible in children, although le ss common; the pathogenic mech ani smdescribed above is nearly always present i ll chronic lesion s resulting from functionaloverlo ad or overu se.
There are two separa te groups of traumatic lesion s related to sporting activity:acute lesion s and those resulting from overu se.
Acute lesion s are caused by situations of ten sion , load, or tor sion , and are characterized by immediate awareness of the damage and appearance of symptoms, withacute pain and functional immobility, and the damage is readi ly apparent from rad iographic imag es. Thi s group includ es mai Illy fractures, as well as jo int disloc ation s
and, in late adolescence, injuries to the j oints, tendons, and ligaments. In both thechild and adolescent, " incomplete" fractu res are also found , at the level of the nucleus of ossific ation and the metaphy seal ca ·tilage, as well as apophyseal avulsion andosteochondral fractures.

2 Micro-traumaticLesionsCaused byOveruse:Overview 37
These types of lesion s, which are discussed in greater detail in other chapters, canusually be easi ly related back to the traumatic mechani sm, and, if correctly treated,usually have an exce llent prognosis.
Lesion s of overu se are instead determ ined by microtraumatic processes; the trauma may be endogenous, for example violent movement s that tend to excee d the physiolog ical limits of excursi on of a part icular joint, or forc e it to move in a plane thatis not natural ; or it may be exogenous, cau sed for example by the ground the athleteis running on, or by a particular piece of apparatus or sports equipment.
Microtrauma represent s a mechanical act ion that determ ines damage that is silentfrom the clinical point of view and is qu ickly repaired by the organism under norma lcond itions; however, when the micro trauma is repeated many times in a short spaceof time, as in cont inuous sporting pract ice, there is no time for structural recoveryand the repeated sma ll lesion s summate to resul t in anatomical alteration s that areultimately presented to the clinician.
In the young athlete these types of lesions , which are less common in the adult,represent more than hal f of the total of spor ting trauma; th is is mainly because during the growing phases, relatively sudden changes in body dimension s caus e problems of motor coordination in the athletic maneuver, changing the type of stress andincre asing the likelihood of mic rot rauma.
Thi s group , which forms the basis of discussion in thi s chapter, includes stressfractu res, osteochondrosis, osteochondritis dissecans, variou s forms of osteochondritis and chron ic lesions of the physis, and insertional tendonit is.
It goes without saying, particularly considering the age of the patient, that timely and correct identi ficat ion of such lesions is essent ial for suitable treatment, inorder to redu ce the long-term sequelae and allow rapid and optimal resumption ofphysical activi ty.
In the diagnostic context of this traum a, diagno stic imaging has a role of fund amental importance, which, thanks to the tool s available tod ay, allow s early recognition from specif ic radiological images, which can be correlated to the pathologicalinjuries and allow monitoring of the repair processes over time .
2.1.1Stress Fractures
Stress fractures are defined as bone lesion s cau sed by repeated microtraumas thatdeterm ine the physiological process of remodeling bony tissue, with the phenom enonof osteocl astic bone resorption and a fai lure of cortical and cancellous bone.
The lower limb is most commonly involved in thi s type of lesion , particularly atthe level of the diaphysis of the tibia and fibula, and especia lly in runn ers.
These injuries are less common in the upper limb , where they occur particularlyat the diaphy sis of the ulna and radiu s, primarily in tenn is players, and of the olecr anon apophysis particularly in gymn astics and throwing sports.
They typic ally present with swelling and pain that correlates to the physical activity, but without a preci se and reliable hi story for direct acute trauma.

38 C. Defilippi et al.
2
Fig. 2.2 A-P (a) and L-L (b) radiograph show a stress fracture of the right tibia. Note sclerosis andperiosteal new bone deposition (red arrows) through the upper tibia and the appearance of healing (white arrows) of the stress lesion
From the point of view of imaging, the se traum as are not easily identified by conventional radiography, particularly in the early stages when dense cortical th ickeningis not yet apparent. (Fig. 2.2).
In the initi al phase , the examination of cho ice is magnetic resonance imagi ng(MR/), which is parti cul arly sensi tive in detecting the physiological changes takin gplace in the se fractu res, mainl y characteri zed by edema of the spongiosa, which iseasily identifiable with the supressi on of fat sequences (Fig. 2.3) ; the ability to produc e a multiplanar represe ntation ensures optimal demonstration of the fractu re rim.
However, th is doe s not result in a definit ive diagno sis, and although ult rasonography is sensitive in the earl y phase it doe s not absolutely specify a diagno sis, whil ecomputed tomography (CT) is relatively specif ic but not suff iciently sensitive.
The onset of low back pain in the adolescent athle te is not unu sual and in over40 % of cases it is caused by the presence of a lumb ar spondy los is, with or withoutspondy lolisthesis . Therefore, when faced with such symptoms in a young athlete, th iswill be the f irst hypothesis to be con firmed or ruled out by diagnostic imaging. Thespondy los is may be the result of a stress fractu re of the interpeduncular line of thevertebral arch, and can have signif icant inc idence in particular sport ing specia lties,such as gymnastics, swi mming butt erfly stroke, and diving. The conventi ona l radiological investigation should see k the "sign of the littl e dog" in obl ique projectio ns.CT or MRI can be used in case of doubt.
A separate cons ideration is a stress failure fracture, i .e. a fracture occurring in a

2 Micro-traumaticLesionsCaused byOveruse:Overview 39
Fig. 2.3 Tibial stress fracture. The earlyMRI shows the fracture line (a, blackarrow) and bone marrow edema (b, whitearrows)
bon e that ha s become less resi stant to stress because of a deficit of bon e mineral.Thi s is ob ser ved mo st commonly in females who tak e part in inten se sporting
acti vites (part icul arl y gymnastics and long-distanc e run ning) , who show th e "female
athl ete tr iad " sy ndrome of reduced power, ol igo-am enorrhoea, and osteoporo sis,
often triggered by str ict d iet s coupled with in tense physical act ivity. This is a syn
drome with subtle on set , where a stress fracture could repr esent th e first sy mptom,
but it can be very dangerous for the health of the young athl ete.
2.1.2Osteochondrosis and Osteochondritis Dissecans
Osteochondrosi s and osteochondri tis d issecan s def ine a necrotic-degenerati ve type
of pathology, relatively common in adolescents, which may affect epiphyseal growthof the nuclei and is generally secondary to repe ated compressive mech an ical ins ult.
Th ese conditions are characterized by mi cro vascul ar lesions in the area submitte d to
mechan ical overload, resulting in a locali zed deficien cy of blood supply leading to
necrotic-degen erat ive phenomena, th e so-calle d osteochondrosi s. In the younges t
subjects «11 -13 yea rs), in which th e nucleu s is sti ll in form at ion , the normal endo
chondral ossification is compromised, and th e nucleu s becomes irr egul ar, frag ile,

40 C. Defilippi etal.
2and liable to collapse. On the other hand, in most adult subjects (> 13-14 years), inwhom the physis is settled and the epiphyseal nucl eus is fully develop ed, the avascular chall eng e can produ ce a circum scribed bony necro sis, which may develop fur therto result in separation of a necrot ic fragment, so-called osteochondritis dissecans.
Non-advance d cases of osteochondrosis and osteochondritis dissecans can bemanag ed if the overload is rapidly reduced, avoiding the fragmentation and osteochondra l separation, and move toward s recovery with res titutio in integrum. Everynucleus of ossification can be the center of osteochondrosis, often with an earlyasy mptomatic cl inical cour se; however, there are some sites, linked to the repeatedactions of a part icular athletic movement , where this has part icular clinical importance.
In some cases, cor relation of the osteochondrosis with the overu se is intuit ive andnow universally accepted, with repeated sporting microtraumas in which compression is dynamic; this is the case in Parmer disease, in which a lesion of the humeralcondyle is linked to the athletic throwing movement. In other cases (for instanceLegg- Cal ve-Perth es disease of the proximal epiphysis of the femur, Scheuermann 'sdisease of the spine), the pathogenic mechanism is att ributable to the physiologicalgravi tational load, sometimes with endocr ine-metabolic influ ences, to which compression and overuse overlo ad, linked to the sporting practice are sometimes added.
The process of osteo chondritis dissecans begins with dissection of an osteochondral fragment, typi cally at a convex articular surfa ce, with sub sequent appearance ofsubchondra l necro sis followed by formation of an osteo chondral sequestra tionformed by the nec rotic bone and overly ing cartil age . Conventional radiologicalinvestigation sometimes reveals the det ached fragment in more advanced cas es(Fig. 2.4) , but it is better documented by CT.
Once again, the most accura te method is MRI , which clearly underl ines the lesionas a defect on the cortical surface, which appears as an area of depre ssion ; subsequently, the osteo chod ral fragment can be observed as an area of intermediate intensity on both T,- and Tz-weighted sequences.
Fig.2.4 Osteochondritis dissecans oftheknee. X-ray appearance of the typicalbony defect of the medial femoralcondyle (arrows)

2 Micro-traumaticLesionsCaused byOveruse:Overview 41
Fig.2.5 Osteochondritis dissecansof the knee. The MRI shows asmall condylar bony defect
In the intermediate stages, where the separation is sti ll adjacent to the cortex, anarrow zone of low intensi ty on T2 is see n, which reveals separation of the lesionfrom health y bon e; conversely, when there is tot al separa tion of the necrotic fragment , a bord er of high-d ensity separati on is observed in T2, which shows the presence of joint flu id (Fig. 2.5).
It may be necessary to perform an MRI evaluation of the joint for a mor e prec iseevaluation of the stability of the fragment, but only in cases where the arthrographiceffect, induc ed by the intra-articular fluid .
2.1.3Osteochondritis
The term osteo chondriti s indicates a group of disorders of growth of the apophysea lnuclei of ossific ation that are infl amm ato ry-degenerative in nature and secondar y torepe ated avulsion-type mechanic al insult . They are characterized by insertionalchondral and tendon microlesions, followed by inflamm atory and reparative proce sses.The chondral microlesion s and infl amm atory hyperemia result in acc elerated endochondral ossification of the apophysis , which is disorg anized and multicentric.Therefore, the growth nuclei of the apophys is are larger, irregular, and mult iple .However, the mo st characteristic pathological change is inflammation of the ar ticular cart ilage , which appears thickened and hype rem ic.
The disorder has a slow course, which is benign, in which the infl amm ator ydegenerative process spontaneous ly regresses, with subsequent rep air and definit iveossifi cat ion of the nucle us; however, there are residual hypertroph ic morphologicalalterat ions of the apophyseal nucl ei involved.
The pelvi s and knee are the sites with the great est numb er of apophyse al growthnucl ei, and are therefore also the sites most frequently affe cted by apophyseal

42 C. Defilippi etal.
2detachment in situa tions of viol ent insults and acute avuls ion, or of apophyseal
osteochondriti s where th ere is repe ated chronic traction .
From the point of vie w of imaging, th ese pathologi es have a very typical presentat ion , which is eas ily identified by the different methods. On convent ion al radiogra
phy, sclero sis and defo rmity in the nu cleu s of ossification, whi ch often results in
fragm entat ion and diasta sis from the adjacent bon y stru ctures (Fig 2.6), are ob ser ved .
Th ese finding s are also visibl e on ultrasound exami na tion, which also shows swell ing
of the apophyseal car tilage, signs of tendon dam ag e (th ickened and hypo echoic) , and
the po ssib ility of as sociated bursitis (Fig. 2.7).
Fig 2.6 Osgood-Schlatter disease. X-rayappearance of the sclerosis, diastasis, andfragmentation of the tibial tubercle
Fig.2.7 Ultrasonographic pattern of Osgood-Schlatter disease. a Irregular appearance of the tibialtubercle; b color-Doppler scan shows a chondro-tendinous insertion with hyperemia of the infrapatellar tendon; c deep infrapatellar bursitis

2 Micro-traumaticLesionsCaused byOveruse:Overview 43
Fig.2.8Osgood- Schlatter disease. Magneticresonanceappearance of thetibial irregularity and the tendon involvement
These finding are better vis ualized on MRI (Fig. 2.8), but thi s should be reservedfor rare cases of sonographic-negative fir st-level exam inations in the presence of asuggestive clinica l history, and for osteochondritis.
2.1.4Chronic Lesions of the Physis
Chronic lesion s of the physis represent the result of repea ted mechanical overload,against the cartilage growth plat e, which can be impose d by vectors of strength avulsion - tangent ial or tor sional. Chronic anatomical damage, equivalent to a type ISalt er-Harris lesion (fo r example, little leagu e shoulder), or a mechanical insult maybe expresse d as vectors of forc e in compressi on, causing chronic cru shing injury ofSalt er-Harris type V (e.g. crus hing and prevent ion of growth of the distal physis ofthe radius in gymn asts) .
In the next sections, we will revie w some of the mo st common bon e and joint diseases resulting from overuse, involving the appendicular skele ton, which are oft encorrelated to specific sporting specialties.
2.2The Upper limb
2.2.1Little League Shoulder
Thi s term refers to a type of lesion that mainl y affe cts athl etes who enga ge in throwing sports, particularly tho se involv ing "over the head" actions, or a movement where

44 C. Defilippi etal.
2the limb is plac ed in an anterior elevation of 90° and maximum externa l rotation .Sports parti cipant s falling into this category are prim arily pitch ers in baseball andlight athl etics, and secondarily volley ball and tennis players and swimme rs.
This pathology represent s a good example of how repeated stress at an osteoarticular structure can give rise to different clinical pictu res, according to the degreeof maturation of the musculoskeletal apparatu s. In adults, the chronic microtraumafrom tract ion leads to injury of the capsular ligam ent , while in the adolescent it act sat the level of car ti lage growth of the proximal hum eru s, where it result s in a pathological chang e comparable to a Salter-Harris type I lesion.
The onset is typically between II and 14 years of age, with gradu al emergence ofpa in at the lateral proximal hum eru s during athletic movement , which increases toprevent prop er use.
It is therefo re a chronic avulsion-ty pe lesion of the physis, charac terized by abroadening of plate car tilage growth , which is easi ly recogni zed on radiographs ofthe humeru s, part icularly if performed with a bilat eral comparison, and especia llyevident on the lateral margin .
The avulsion microtrauma respon sible for the carti lage injur y is typicall y accompan ied by an inflamm ato ry component , which makes for a hyperint ense signal thatlocates the physical suffer ing as a result of damage in the early stages, while Tz
weighted MRI sequences also show fat suppressi on.
2.2.2Osteochondrosis of the Humeral Condyle (Panner Disease)
Panner disease is an osteochondrosis of the hum eral cond yle that characteristicallyoccurs in children who play baseball and other throwing discip lines, and less often inyoung gymna sts, and is due to repeated micro traum a from lateral compression of thehum eru s-radius articulation , cau sing alteration s in the cartilag e growth nucleus ofthe hum eral cond yle. It is clinicall y charac terized by latera l elbow pain, with progressive funct ional impotence, that begins befo re the age of 10 years; the early onsetsuggests a differential diagnosis in comp arison to osteochondritis dissecan s, alsoconfi rmed by diagno stic imaging, but which, by definition , only occur s after closureof the physis, after the age of 13-14 years .
2.2.3Osteochondritis Dissecans of the Humeral Condyle
The distal humeru s, and particularly the hum eral cond yle, is one of the places wherethis pathology is frequently seen. The young athletes most affected are those practi cing activities that involve a valgu s stress of the elbow, subjecting it to repeated lateral compression traum a, with particular side-impact on the hume ral condyle. Prompt

2 Micro-traumaticLesionsCaused byOveruse:Overview 45
diagnosis and sub sequ ent removal of the load will enable rec overy; oth erw ise, thedisord er will prog ress to dissection and separat ion of the osteochondral joint. Earlydiagnosis may require ultra sonography or MRI.
2.2.4Little league Elbow Syndrome
Thi s syndrome, which is exclus ively observed in pitch ers (baseball and oth er throwing specialties ), is characte rized by the involvement of different struc tures that formthe ar ticulation of the elbow, and therefo re repr esent s a valid mod el for the study ofoverload lesions in pediatri c age, due to microt raumas from both compressi on andtract ion.
The complex biom echanics of the athletic gesture mu st be tak en into acc ount.These include a tor sional twist with a rapid rotation of the shoulde r and elbow extension; this is followed by a violent stress in valgus extensi on at thi s joint , which produc es injury from compression aga inst the lateral compartment and tract ion at themedial and lateral level.
In adults this picture is usually translated into pathologies of the lig aments andtendons, in disorders such as late ral uln ar ligament lesions, due to valgus stress ;insertional enthesop athy of the olec ranon ; and medial epicondylitis.
In contrast, in young athl etes, the tract ion is ins tea d loaded onto the corresponding ca rtilage growth plate, resulting in apophyse al endochondrosis of the corresponding medial epicondy le of the olecranon. In additi on, the presenc e of osteochondrosis ca use d by compressi on of the hum eral condyle (Pann er di sease in the younges tathl etes and osteochondritis di ssecans in late adoles cence ) is associat ed with a simi lar pro cess at the radi al head.
The onset of symptoms is typ icall y between 9 and 14 years, at fi rst with a reduction in the spee d and precision of throwing , and subse quently with the app ear anc e ofdiffuse pain in the whol e joint , which is mor e inte nse in the medial epicondy le .
2.2.5Osteochondritis of the Olecranon Apophysis
Unlike the forme r case, this lesion is observed part icul arl y in sporting act iviti eswhere there is a re peated and viol ent contraction of the triceps mu scle against aresistan ce; typical examples are power laun ch ing, such as in weight tra ining andgymn astics.
The mic rotrauma acts on the olecranon inser tion of the triceps, provo king thetypical osteochondritis of apophyseal tract ion , characterized clinicall y by pain andfun ctional limitation.

2
46
2.3The Lower Limb
C. Defilippi etal.
2.3.1Osteochondrosis of the Epiphyseal Nucleus of the Femur (legg-Calve-Perthes Disease)
This rare disorder is found as a pathogenic osteochondrit ic cofacto r in mechanicalinsult from overuse. [t particularly affects children aged between 5 and 8 years,although they may not be performing any strenuous overactiv ity. The disorde r is usually bilater al but may be unilater al. There is a possible link with overu se, but pathogene sis is very margin al.
2.3.2Epiphysiolysis of the Epiphyseal Nucleus of the Femoral Head
This type of lesion may be the result of chronic overlo ading with combined shear andcompressi on forces acting on the growth plate cartilage, lead ing to a complete orincomplete Salte r- Har ris type [ lesion. ln the case of a complete lesion of the physis,separation of the epiphysis and its slippage is verifie d. [f it is the result of a rela tiveoverload (or insufficiency), a normal load can becom e excessi ve for a growth platethat has been weakened by previous unfavorable hormonal influences (oft en hypogonadism).
2.3.3Osteochondritis Dissecans of the Femoral Condyle (Konig Syndrome)
The convex articular surface of the femor al condyle (part icularly the medi al part)represents the most frequent center of osteochond rit is dissecans, and is apparentlyrelated to repe ated comp ression microtrauma in sport ing activites such as footb all ,involving energetic stress in the knee jo int .
2.3.4Osteochondritis of the Inferior Pole of the Patella (Sinding-larsen-JohanssonSyndrome)
This corresponds to Osgood-Schlatter dise ase at the inferior growth plate of the poleof the patell a. lt is not frequent as an isolated lesion, but is often found in conj unction with patellar tendinits (jumper's knee).

2 Micro-traumaticLesionsCaused byOveruse:Overview
2.3.5Osteochondritis of the Anterior Tibial Apophysis (Osgood-Schlatter Disease)
47
Osgood-Schlatter disease perhaps represents the best known and studied form of osteochondr itis of the whole skeletal apparatus. It is found in young athletes who undertakerunning and jumping sports, and is caused by repeated traction microtraumas that act atthe anterior tibial apophysis and the site of insert ion of the patellar tendon.
It man ifests bilat erally in 20-30% of the cases in children aged between 10 and15 years, with knee pain exacerbated by activi ty linked to swelling of the apophysis .
From a diagnostic imaging point of view, the most usual examination is ultrasonography, which, in addit ion to radiographic identif ication of ir regular fragmentation of the ossificat ion nucl eus of the apophysis , also gives evidence of the alterations that are typical of th is pathology, such as patellar tendon itis, deep infrapatellarbursitis, and, above all , swelling of the apophyse al cartilag e.
2.3.6Shin Splints
This is defined as damage to the periosteum of the anterior (or, more rarely, poster ior)tibi al cortex, due to cont inuous stress tract ion occurring as a result of running, at theposterior of the extensor digitorum longus (or, if posterior, the flexor digitorumlongus and soleus) in children, where, because the perio steal acti vity is higher, thi scl inical picture is most often found .
The clini cal symptoms are typically pain with redness and swelling at the lesion .The pathological picture is characterized by disconnected periosteum (periostealstri pping), which is recurrent and of low grade, but over time stimulates perio stealosteogenic activi ty and determ ines the appearance of a focal periostitis on the rad iographic or CT image . MRI performed in the acut e phase and sequences using highcontrast can highl ight a characteristic hyperintense band.
2.3.7Osteochondritis Dissecans of the Talus
The talar dome is a relatively frequent center of pathology caused by compr essionmicrotraumas, especia lly in running and jumping sports (landing phase). The evolutionof the patholog y and diagno stic imaging is as usual for dissecting osteochondritis.
2.3.8Osteochondritis of the Calcaneal Apophysis (Sever Disease)
Thi s is similar to the previou sly describ ed apoph yseal chondritis, and has been recognized since the early years of the last century to be a result of tract ion overlo ad on

48 C. Defilippi etal.
2th e calcan eal apophysi s from th e Achill es ' tendon in young runners. Th e clinic al and
imagi ng pictures are simi lar to those described above, although th e ra d iog raphi c p ic
ture can be confus ed by th e ph ysiological den sity of the nucl eus of ossifi cation,
whi ch is often ob served . In cases of doubtful inte rpretati on it is th erefore useful to
use MRI.
2.3 .9Osteochondritis of the Apophysis of the Base of the Fifth Metatarsal (Iselin Disease)
This is caused by traction inj ury of th e base of th e f ifth m etatarsal , by th e tendon of
th e sho rt per in eal muscl e, and is es pec ia lly found in young j um pers .
2.3.10Osteochondrosis of the Head of the Second Metatarsal (Freiberg orKoehler II Disease)
This is osteochondrosi s th at is prefe rent iall y lo cated at the ep iphyse al nucleus of the
head of th e second m et atarsal , but can be found, less fre que ntly, at th e th ird
m et ata rsal. The disea se progression an d imagi ng are th e same as usu al for ost eochon
drosi s. It is enc ounte red most frequently in young runner s .
Suggested Readings
Abraham E (1992) Sports-related injuries in children and young adults. Compr Ther 18(12) :33-7AokiY, Yasuda K, Tohyama H et al (2004) Magnetic Resonance imaging in stress fractures and shin
splints. Clin Orthop Relat Res (421):260-267Bernhardt DT, Landry GL (1995) Sports injuries in young athletes. Adv Pediatr 42:465- 500Cain EL Jr, Dugas JR, Wolf RS, Andrews JR (2003) Elbow injuries in throwing athletes: a current
concepts review. Am J Sports Med 31(4):621-635Cassas KJ, Cassettari-Wayhs A (2006) Childhood and adolescent sports-related overuse injuries. Am
Fam Physician 73(6):1014-22Hatem SF, Recht MP, Profitt B (2006) MRI of Little Leaguer 's shoulder. Skeletal Radiol 35: 103
106Maffulli N, Bruns W (2000) Injuries in young athletes. Eur J Pediatr 159(1-2) :59-63Pommering TL, Kluchurosky L (2007) Overuse injuries in adolescents. Adolesc Med State Art Rev
18( I):95-120Raissaki M, Apostolaki E, Karantanas AH (2007) Imaging of sports injuries in children and ado
lescents. Eur J Radiol 62( I):86-96Wilder RP, Sethi S (2004) Overuse injuries: tendinopathies, stress fractures, compartment syndrome,
and shin splints. Clin Sports Med 23( I):55-8 1

Osteoarticular Trauma in the Pediatric Age: 3Overview - Apophyseal Injuries
M. Valle, A. TaJ,:lial1co. L. Oppezzl, N. Gandolfo, P.Toma and C. i\lartinoli
3,'Introduction
From the anatomical point of view, apophyses are protuberances on bone (fromGreek u1toqn<JlS, composed of apo "to bring forth " and physis "to grow") that makeup specialized struc tures for the atta chment of tendons and ligaments. Among chi ldren and adolescents, lesion s on the apophysis are a common clinical probl em re lated to sporting and recreat ional activities . This is due to the fact that , between the ageof 12 and 16 years, the structure of apophyses makes them vuln erabl e: the development of the ir ossific ation center is not yet complete, and the cartilage , under hormon al infl uence, loses elas ticity and is unabl e to give f irm sta bi lity to the osteo tendinous junction. Hence, rough application of shear or tor sion force s, exer ci sedupon the apophyse s by tendons and ligam ent s, can overcome the thr eshold of cartilage and bone resistance. Thi s may result in fragmentat ion or detachment, whichconsequently impairs fun ction to an extent that can be mo re or less disabling for thepat ien t. The range of apophysea l injuries is extremely bro ad and is influenced by thefollowing factors: degr ee of bon e and cartilage maturat ion (and, therefore, age of thech ild or adolescent at the time of trauma) ; anatomical loc ation of the apophysis; andthe geometry and degree of the forces appli ed to the myotendinous sys tem. Th ispathophysiologic complex ity may expl ain the large number of terms used to definethi s type of injury, often generat ing confus ion in descriptions of the proc ess itself.Term s range from "apophyseal irritat ion ", to "traction apophys itis", "osteochondrosis", "c hron ic apophysitis" , "osteochondritis", and "apophysea l separation" . Duringskeletal maturation , apophyseal injuries are caused by a traction mechan ism thatproduces traum at ic inj ury to the cart ilage and bon e. Then , there is a sequence of
C. Martinoli ([2;1)Radiology Department - DISC, University of Genoa, Genoa, Italy
Imaging of Pediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
49

50 M.Valleet al.
3overlapping damage-repair events . Under these circum stanc es, the diagno sis influence s the decision with respect to the treatment strategy and the resumption of sporting activity. In the diagno stic work-up, imaging plays an important role in confirming the clinical findings. In this chapter, we will first consider apophysea l injur iescaused by tendon tract ion, then look at those deri ved from ligament tract ion .
3.2Tendons
Substantial differences exist between the pathology of tendon s occurring in the pediatric age comp ared to that of the adult. Thi s is because in a child or an adolescent, adegenerative proce ss of the tendon substance is never pre sent , except in exceptionalcases and in relation to systemic disord ers or to severe osteo-articular abnormalities .Tendons in the child are fibrillar structures , whose image in radiolog y differs fromthat of an adult only by their sma ller size and the ir insertion, which at thi s age consists parti ally, if not totally, of cartil age on the apophysis .
3.2.1Pathophysiology
At the site of insertion into apoph yses, tvo main categor ies of tendon lesions mayoccur: chronic and acute. The first, which is more frequent, is caused by microtraumafrom repeated tract ion, often in relation to a funct ional overlo ad (overu se) duringsporting activities. These injur ies lead to abnormalit ies of the tendon-to-bone interface , with fragmentation of the apophysesI cartil age and fibrocartilage and/or of theunderlying immatu re bone . The degree of avulsion of the apophy seal structuresinduced by traction trauma is minim al a id does not signif icantly compromise thebiom echanics of the structure s attaching on it. When detachment involves fragm entsof cartilage of an immature apophysis, the se can later become ossified, forming smallfoci of heterotrophic ossification in the so ft-tissues - in general the se are easily identifi ed by imaging modalities. These foci are separated from the apophysis and localized in cont inuity with the tendon fiber:.. The distance intervening between theseossicles and the apophysis is short, and almost invar iably filled with fibrocartil age orwith a fibrous bridge. If the degree of displac ement of the oss icles is not much andthey are in close contact with the apophyseal cartil age, they can be totally reabsorbedinside the apophysis during the maturati on proce ss of bone, as growth eventuallyencompasse s them . In these cases , a subtle prominence (callu s) or deformity maydevelop with apophysea l enlargement : dit ferent ial diagnostic problems with aggressive lesions are unusual in these cases. 011 the other hand, when the fragment is dislocated far away from the growing apophysis, it can be transformed into a permanentossicle, totally separated from the main bone, and may assume a spherica l or ovalshape with a thin cortical cover. The typi cal location of the ossicle along the course

3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries 51
of a tendon or a ligament and near its insertion allows its identification as differ entfrom sesamoid bones. The faet that these lesion s are the consequence of repeatedinjur ies over time - even if minimal - lead s to an intermittent eour se of symptoms,with alterna ting phases of exacerb ation and rem ission of pain .
In contrast to chronic lesions, acute apophyseal inj uries derive from a uniqueindi rect major trauma. In these inj uries, the tendon applies an excess ive tract ionforc e with respect to the resis tance posed by an apophysis that has not yet reachedfull matur at ion and biomechanic al consol idation . The result is parti al or completedetachment of the apophysis on which the tendon is inserted or, more rarely, avulsionof the tendon from its bony insertion. Acute apoph yseal injuries can be subdividedinto major and minor types based on the degree of dislocation of the apophyseal fragment. Majo r apophysea l lesions cause dislocation of the apophyseal fragment, whichis avulsed to such a gre at extent that it cannot any longer be reabsorbed. Growth maybecome comp romised or cease, and, in the case of complete avulsion, a significantbiomechanical deficit occur s. In general, and especially at the ischia l tuberosity, aninjur y is considered major when the distance between the bone fragment and thenidu s of avulsion is greater than 2 em, or when the avulsed fragment is exceedinglylarge : in these cases, the treatment is surgical and is based on reattachment andanchoring of the apophysis onto the bone by means of a screw. When the appliedforce is not enough to cause complete avulsion of the apophysis , the pattern of fragment ation can differ, involving variable amounts of car tilage and bone . This proce ssis modul ated by the method of applica tion of the force, the conformation of theapoph ysis, its degree of matur ation , and the physical activity. Generall y speaking,these minor injuries can be easily distinguished from the most common chronic ones,based on their location and morphologic appearance, since detachment does notcause loss of relat ion between the avulsed fragment and the nidus of avulsion. In bothmajor injuries and the minor form s, the detachm ent is related to the damage of oneof the histological component s of the apophysis that are arranged "in series" to resisttract ion . The se structures are:
the growth car tilage of the apophysisthe secondary ossification center (if present)a layer of fibrocar tilage or, less commonly, of perio steum on which the tendonfibers directly inser t.In most cases, the lesion occurs at the level of the apophyseal cartil age located
above the secondary ossific ation center.From the clinical point of view, chronic and acute apophysea l lesion s differ from
each other in many respect s. Conce rning chron ic lesions, the f irst occur rence ofsymptoms is only vaguely remembered by the young athlete; symptoms are typicallymilde r and inte rmittent ; sporting or othe r physical activities are not hindered by pain ;and patients can be treated conservatively with rest, support, and symptomatic therapy. On the other hand, in patient s with acute lesion s, the functional disability andpain are typically related to a recent trauma that is easily remembered by the patient(who can describe in detail the mechanism underlying it). There is a sudden onset ofpain, immediately causing the subject experience a disablin g condition with difficulties in standing or walk ing. The sporting activity can eventu ally be resumed, upon the

S2 M.Valleet al.
3recovery of strength in the mu scle group invol ved, and when movements can be executed without rest rict ion and pain. The treatm ent , which depend s upon the size of theavulsed fragment and the degree of dislocation , can, in extreme cases, include surgery. The prec ise timing to correctl y carry out this approach is st ill being debated,but in all cases the prognosis is exce llent.
3.2.2Imaging
In chronic apophyseal lesions, plain film s are generally suff icient to mak e the diagnosis by showing fragm ent ation of the apophysis. Ultr asound can be used in thephases of re-exacerbation of symptoms to check the status of the tendon insertion.Although magn etic resonanc e (MR) imaging can show marrow edema at the level ofapophyses, its use is not justified in typ ical cases. This is because the decision tores ume sport ing activities by the child or the adolescent is esse ntially based on clinica l criteria, and not on imaging findings. Instead, MR imaging can be helpful incases with atypical present ation , when there is any doubt about wheth er oth er pathology may be present. An example of th is could be a patient with anterior knee pain,when patellar inst ability, bone mi salignments, or other os seous pathology(osteomyelitis) is suspected in the differential diagnosis list for an Osgood-Schlatteror a Sind ing-Larsen-Johansson disease.
In acute apophyseal lesions, the patt ern of avuls ion may be variabl e at imagingbased on the structure involved, especially in the phases immediately after the trauma,when the amount of detached bone and/or cartilage can vary greatl y. In general , theradiographic examination can demonstrate the apophysea l detachment, althoughinj uries with minimal dislocation and parti al apophyse al involvement may be hard torecognize. Side compar ison can be useful in case of mild apophyseal dislocation. Inchronic avul sion s that have already been stabilized, pla in film s can occasionallydepict a hypertrophied callus at the level of the apophysis (apophyseal hyperostosis),possibly mim icking an aggress ive lesion . In these cases, know ledg e of the exactanatomic sites of tendon insertion into bone may help to prevent misdi agnoses. In theacute sett ing , if radiography does not provide conclusive information (this especiallyhappens in the event of minor dislocations), ultrasound and MR imag ing can playadec isive role in confirm ing the apop hyseal inj ury. Ultrasound has the advantage ofbeing a clinical examination, directed towa rds the pat ient 's symptoms and, with highreso lution small-parts transducers, it is able to identify even minimal abnorma litie sof cartilage and bone. MR imaging can recogni ze the pre sence of effus ion and edematou s chang es around the apophyseal growth cart ilage. Hemorrhage often extendsalongs ide the tendons involved, in a location far from the bone insertion. In minorapophyse al injuries, ultr asound used as a part of a compl ement of radiographic examinations can be enough to diagnose and characterize the inj ury. However, for cost rel ated reasons, the use of MR imaging should be rese rved for the evaluation ofmajor apophysea l lesions and to make a preo perative evalu ation .

3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries
3.2.3Chronic Apophyseal Lesions Due to Tendon Traction
S3
In the pedi atric age group, the main examples of apophyseal lesion s that deriv e fromchronic microtrauma occur at th e level of the kne e - with the so-calle dOsgood-Schlatt er and Sind ing-Larsen-Johansson diseases ; and at the level of theankl e - with Seve r's dis ease and accessory navicular syndrome.
Osgood-Schlatter di sease re fers to an apophysit is (although the term is usedsome what inappropriately) of the tibial tub erosity, which is oft en obs erv ed in infantsand adoles cents, reac hing its peak between the ages of 10 and 15 years . Th is condition occurs mo st frequentl y in boys who pract ice sporting activities that involvejumping (e.g. basketball , voll eyball) and apply repeated stress forc es on the extensormech anism of the knee. Osgood-Schlatt er disease is typically secondary to repeatedtract ion exe rted by the pat ellar tendon on the secondary nucl eus of ossifi cat ion of thetibial tuberos ity. The lesion occurs when the chondral cell s of the apophysis arehypert roph ied, in the so-ca lled "pre-ossi f ication" phase. Once the trauma hasoccurred, the cartilage and bon e fragm ent s proceed with the proc ess of oss ificationand increase in volume until they become visible on pla in films in the pretibi al area .The space between the se fragments and the avulsion site is filled with fibrous ti ssueor fibroc artilage . In the late phases, ossification of the intervening space can occurif the gap between the fragments and the tibi al tuberosity is of limited extension . Onthe other hand, if the di sloc at ion is greater in extent, the avulsion fragments tend toossify inside the tendon, forming ossicles, which become perm anent after growth hascompleted. Clinica lly, Osgood-Schlatte r disease presents with a lump located superfici ally to the tibi al tube rosity . The lump may be tot ally asy mptomatic or may beass ociated with recurrent pain that is typ ically exacerbated by physic al activity. Plainfilms demonstrate a fragmented tibi al tuberosity ; in early disease, however, the bonesurface may appear normal. It should be taken into account that the ossification center of the tuberosity can be multicentric : thi s may cause problems in the different ialdiagno sis between normal and pathological cases. Fragments are typ ically found infront of or crani al to the ossific ation center, and have a thin sclerotic rim whichallows th is condition to be di stinguished from acute avulsive inj ures (Fig. 3.1a).Ultras onography (US) can identify early abnorma lities in the soft and chondral tissues, onto which the patellar tendon inserts. The mo st typical signs are soft-tissueswelling, tenderness, and fragmentation of the secondary ossific ation center, thi cken ing of the tendon inser tion with ass ociated echotextural abnormalities , and infra patellar edema (Fig . 3.2a, b) . The se signs , however, do not correlate with clinicalsymptoms, disease severity, and patient outcome. In acute pha ses with intense painand functiona l disability, a distended deep or superf icial infrapa tellar bursa andint ra- and per i-tendinous hyperemia at color- and power-Doppler imag ing can befound . Compared with US, MR imaging seems to be more sens itive for demonstrating early signs of disease, allo wing identification of marrow edema at the level of thetibial tub ero sit y (Ti -hypo int ensit y and T2-hyperintensit y) in the ea rly phases oftrauma , when rad iography is sti ll nega tive (Fig. 3.2c). Osgood-Schlatt er disease see msto accel erate physeal ossificat ion but is not assoc iat ed with an incre ase d ris k of

3
54 M.Valleet al.
Fig.3.1 Chronic traction injuries. a Standard lateralradiogram ofthe knee in apati ent wit h OsgoodSchlatter disease revealsbone fragments (arrow) atthe level of the distal patellar tendon . b Bone fragmentation at the proximal(white arrow) and distal(open arrow) insertions ofthe patellar tendon reflecting Osgood- Schlatter andSinding- Larsen- Johansson diseases
Fig.3.2 Osgood-Schlatter disease. a Sagittal US image (17-5 MHz) of the normal tibial tuberosity shows the patellar tendon (1) inserting into the tibial tubero sity (3). A thin layer of hypoechoiccartilage (2) that represents the residual of the growth cartilage ofthe tubero sity is observed. Notethe bone notch (4) that separates the tuberosity from the tibial metaphysis (5) and the patellar tendon (arrowheads) that overlies the tuberosity to insert, with its most caudal fibers, on the latter.b Corresponding US image in a patient with Osgood-Schlatter disease. The tibial tuberosity hasan irregular bony surface with detachment of some bone fragments (arrows). At the same time,the cartilage is not adherent to the underlying bone owing to the traction exerted by the patellartendon. c Sagittal fat-suppressed turbo spin-echo (tSE) T2-weighted MR image of the knee in thesame patient shows bone marrow edema (asterisk) at the level ofthe tuberosity and the most anterior part of the tibial epiphysis. Deep infrapatellar bursitis is also seen (arrowhead)

3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries ss
fracture-avuls ion of the tuberosity. Treatm ent is conservative and requi res rest, nonsteroidal anti- inflammatory drug s (NSAlDs), time and - for complete resolution full bone maturity.
Sinding-Larsen-Johansson disease affects the origin of the patellar tendon fromthe infer ior pole of the patella. This disord er is similar to but far less common thanOsgood-Schlatter disease. [t occurs in children who are slightl y older (10-12 years)than those affected by Osgood-Schlatter disease and is often associated with this latter cond it ion, given that the risk factors and the pathological mechanism are thesame. Radiographic examinat ion shows fragmentation of the distal pole of the patella,a pattern that may mimic a type I bipartite patella (Fig. 3. Ib). At some stages ofmaturation and in predisposed subjects, the traction exerted by the patellar tendon onthe inferior pole of the patella (which is entirely chondral) can lead to an increa sedprominence of bone instead of fragmentation patterns. In these patients , the protuberant bone can create a conflic t with the deep fib ers of the patellar tendon , especially during knee flexion , causing patellar tend inosis (jump ers ' knee), a condition thatcan becom e symptomatic in adoles cents or in adulthood. In jumper 's knee,tendinopathy has a more chronic evolution compared with Osgood- Schlatter orSinding-Larsen-Johansson disorders. US is able to distinguish the apophysealinvolvement from primary tendon abnormalities.
Another typical site for chronic apophyseal injurie s is the posterio r heel apophysis .This cond ition , which is also referred to as Sever s disease, occurs in pre-adole scentathletes who take part in sports activities such as racing and jumping (football, basketball , etc) . Similar to the other disorders described previously, calcaneal apophysitis isrelated to chronic microtraumas and fragmentation of the secondary ossification center of the heel at the insertion of the Achilles tendon. Often bilateral , Sever 's diseasecauses local soft-tiss ue swelling and heel pain that is worsened by activity and movement. In pathogenetic terms, it must be remembered that the age of appeara nce andfusion of the poster ior ossification center of the calcaneus is variable and does notallow a clear identi fic ation of pathology based on the patterns of apophyseal developmen t. lt has been shown that Sever's disease occurs when the ossificat ion nucleushas already appeared but has not yet fused . Although calcaneal apophysitis has beenrelated, in the past, with the sclerotic appeara nce of the ossific at ion cente r, this signdoes not seem to be pathologic in itself, as it may be encountered in normal children.On the other hand, a mult ifragmented nucleus at an extent gre ater than the contralateral side can be regarded as a diagno stic sign that correlate s well with clinic al symptoms. Similar to Osgood-Schlatte r disease, US can show degenerative change s in theret rocalcaneal portion of the Achilles tendon. Intra- and peri-tendinous hyperemiacan also be identif ied.
Around the med ial aspect of the midfoot, apophysea l injuries may occur at theinsert ion of the posterior tibi al tendon into the tubercle of the navicul ar. This lesionoccurs when the secondary ossifi cation cente r of the tube rcle has not yet fused withthe main body of the navicu lar and is joined to this latter through a f ibrocart ilaginou sor fibrous bridge, which is oriented transversely to the tendon axis. The result is formation of an ossicle, which is present in almost 10-15% of the normal population inthe first decade of life. This ossicle is commonly known as type 2 accessory navicular.

56 M.Valleet al.
3Part of the superficial fibers of the posterior tibial tendon insert on the accessory ossicle , instead of the navicular. Espec ially in children who practice sporting activ ities orhave flatfeet, the repeated tractions exerted by the posterior tibial tendon on the synchondrosis and some lack of stability of the ossicle can lead to a painful syndrome,the so-called accessory navicular syndrome. With time and repeated mierotrauma,degenerative osteoarthritic changes can develop at the level of the synchondrosis, withareas of subchondral sclerosis, pseudoeystie changes, and an irregular surface of theossicle . Plain films can display these bone changes. MR imaging is able to recognizesigns of bone marrow edema in the subchondral bone , thus confirming the presenceof a chronic traction injury. US can correlate the painful area with the locat ion of thesynchondrosis and can exclude pathology affecting the distal posterior tibial tendon(which looks normal in accessory navicular syndrome) and the spring ligament. Whensymptoms become relevant, the ossicle can be removed surgically and the posteriortibial tendon can be reinserted directly into the navicular.
3.2.4Acute Apophyseal lesions from Tendon Traction
In the child and adolescent, one of the most common sites of acute apophyseallesions is the pelvic ring , an area where several muscle-tendon structures find theirattachment, thus pred ispos ing the immature bone to a wide range of tract ion injuries.The apophyses of the pelvis, which are most frequently involved, arc :
the secondary ossification center of the iliac crest, on which the muscles of theabdominal wall insertthe anterior inferior iliac spine , from which the sartorius and the tensor fasc iaelatae arisethe anterior inferior iliac spine, which gives off the rectus femoris tendonsthe pubis , to which the adductors are attachedthe isch ial tuberosity, on which the hamstrings insertthe lesser trochanter to which the iliopsoas tendon anchors.Avulsion injuries at the anterior superior iliac spine, at the origin of the sartorius
and the tensor fasciae latae muscles are typically observed in adol escents and areusually secondary to a forced extension of the hip while the knee is flexed . In general , this kind of avulsion creates symptoms that are less severe and debilitating thanthose that occur at other pelvic sites. Anteroposterior radiograph of the pelvis showsa fleck of bone avulsed from the anterior inferior iliac spine: the fragment is usuallysmall in size (normally <2 em) and has a triangular aspect. If the fragment is barelydislocated, the lesions can be difficult to recognize radiographically. With chroniclesions , hyperostosis and deformity of the anterior inferior iliac spine may occur. Ifthe injury is quite old, the bone can assume a teardrop shape (teardrop sign) as aresult of irregular reattachment of the fragment. US and MR imaging can show anavulsed fragment (that on occasion can be palpable), which is most often in continuity with the sartorius tendon rather that with the tensor fasciae latae.
Avulsion injuries at the anterior inferior iliac spine are more common than those

3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries 57
affect ing the ant erior superior iliac spine . These injuries occur at the origin of thedirect tendon of the rectus femoris, a structure which is much more expose d biomech anicall y than the sartorius . The traum a mech an ism is simi lar to that producinginjuries around the anteri or superior iliac spine, being due to a forc ed extensi on ofthe hip . Th is very common condition occurs not only in the adol escent but also in thechild, and is oft en assoc iated with socce r and running activ ities. In general , pla infilms demonstrate an area of cortical avul sion of less than 2 cm in size inferiorly tothe iliac spine, and exte rna l to the marg in of the acetabulum. The lateral displacement of the fragm ent is related to the action of the ind irect tendon of the rectu sfemoris, which becomes prevalent when the direct tendon is disinsert ed (Fig. 3.3).The avul sed bon e can be confuse d with the adjacent iliac bon e on ante roposteriorradiogram s: obl iqu e or axial views can , therefore, be useful if thi s lesion is suspectcd on clinical grounds. For lesions in the pre-adol escent age (und er 10 years), US andMR imag ing can playa role in iden tify ing purely chondral fragm ent s without dislocation, whereas radiography may remai n negat ive (Figs. 3.4 and 3.5) . In doubtfulcases, the same imaging mod alities can allow distinct ion between an apoph yseal dislocation of the ant erior inferior iliac spine which has migrated inferiorly, and a dislocation of the anter ior inferior iliac spine . In mo st cases, the treatment is con servative, as the deg ree of dislocation is only mild, due to the resistance offe red by theintact indirect and reflected tendon components.
Avulsion inj uries ofthe apophysis ofthe iliac crest at the insertion of the mu scle sof the abdomina l wall are typically observed in adolescents pract icing sporting activitie s before the apophysea l nucleus has fused . It should be taken into account that theapophys is of the iliac cre st star ts to ossify at the age of 15 years and is fused at theage of 18 years. Most avulsion tears of the apophysea l nucleus of the ili ac cre st
Fig. 3.3 Avulsion fracture of the anterior inferioriliac spine. The anteroposterior radiogramdemonstrates anomalous bone at the level ofthe anterior inferior iliac spine (arrow) as aresult of previous traction trauma

58 M.Valleet al.
3
Fig.3.4 Avulsion of the anterior inferior iliac spine. a Sagittal US image (17-5MHz) of the normalanterior inferior iliac spine (AIlS) on the contralateral side of the lesion, shows the direct tendon(arrowheads) ofthe rectus femoris muscle that arises from an apophyseal surface that is still cartilaginou s. The apophysis has a flattened ossification center (arrow). b On the symptomatic side,avulsion and rotation of the secondary ossification center is seen in continuity with the tendon ofthe rectus femoris. Between the avulsed nucleus and the base of the apophysis, heterogeneouscartilaginous tissue (curved arrow) due to hemor rhage and local edema is seen. c, d Axial fat-suppressed tSE Tz-weighted (c) and GRE Tz" (d) MR images show diffuse signal hyperintensity atthe level of the anterior inferior iliac spine (arrow) and iliac bone adjacent to it (asterisk) . On theGRE sequence, note signs of bone fragmentation (white arrowheads) on the affected side, whichare not visible on the contralateral side (open arrowhead)
Fig.3.5 Avulsion of the anterior inferior iliac spine. a Sagittal fat-suppressed tSE Tz-weighted MRimage over the anterior inferior iliac spine reveals a large piece of bone (arrow) avulsed from theanterior inferior iliac spine (open arrowheads), in continuity with the rectus femoris muscle(asterisk). b Note the perifascial and intramuscular reactive edema (white arrowheads). c USdemonstrates deformity of the anterior inferior iliac spine (arrows), related to avulsion trauma,and signs of muscle edema in the rectus femoris (1) and the iliopsoas (2)

3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries S9
deri ve from rep eated trauma associated with an acute direct trauma to the iliac cres t,
or , eve n more commonly, a sudden to rsion of the body (tenn is, soccer). Th e disloca
tion typicall y occurs anteriorly, ncar the ante rior infer ior iliac spine, with lat eral slipping of an apophyseal fragm ent of var iabl e size . Th e segme nta tion of the apophyseal
nucl eu s of th e iliac cres t is not a rel evant fi nd ing as it is obser ved in normal subjects .
In some cases, th is condit ion is bil at eral and may create problems in the differ ential
diagnosis between a normal state and a minimall y displaced lesion. MR imagi ng can
show T2-sign al hyp erinten sit y in th e growth cart ilag e of th e iliac crest , and ede matous ch anges in the soft-tissues located above and below the avulse d fragm ent and at
th e level of th e mu scl e insertions (Fig. 3 .6) .
Apophyseal avulsions f rom the symphysis pub is and th e inferior pub ic ramus at
th e origin of the adductors (adductor longus, adductor brevi s, adductor magnus, gra
cil is) and th e rectus abdominis arc secondar y to e ithe r mierotrauma or re peated trac
tion with an exce ssive rot ation of th e body or during resi sted abduc tion of the th igh(e.g . two pla yers kick ing the ball at th e same tim e) . Soccer and tennis arc the sport-
Fig.3.6Avulsion of the nucleus of ossification of the iliac crest. a Plain film shows sliding of themost anterior part (arrowheads) ofthe nucleus of ossification of the iliac crest, which appears lateralized and anteroinferior (arrow) in location relative to the rest of the same nucleus. b Coronalfat-suppressed tSE To-weighted MR imaging shows the nucleus (arrowhead) dislocated laterallyto the iliac bone (asterisk), in continuity with the external oblique (straight arrows) and transverseabdominis (curved arrow) cranially, and the tensor fasciae latae (TFL) caudally.The intense perifascial edema makes it possible to distinguish the profile of these muscles, which are dislocatedexternally by the avulsed nucleus. Note the spared internal oblique and the gluteus medius (Gill)'
c Biomechanics of the avulsive lesions of the nucleus of the iliac crest. Observe the position ofthe aponeurotic insertions of the internal oblique (I), transverse abdominis (2), and externaloblique muscle (3) on the ossification nucleus of the iliac crest. The schematic drawing on theright corresponds to the case shown in b

60 M.Valleet al.
3ing activi t ies most commonly as sociated with these injuries. Dep end ing on the severity of trauma, distinguishing adductor injuries from oth er caus es of pub algia, including ost eit is pub is, sacro-ili itis, hernias, and lesions around the hip and the acetabularlip may be not strai ghtforward. In most cases, a true bon e avuls ion does not occur, asthe detachment selectively involves the tendon. Radiography can , therefore, be neg
ative in the acute phases; on the oth er hand , in a chronic setting, sclerotic changes inthe pub is can be identified at the level of the tendon inse rt ion. US and MR imagingare abl e to identify the retr act ed tendon end and to distinguish an isolated lesion ofthe adductor longus from extended traumas invo lving mor e than one muscl e.
Avulsion injuries of the ischial tuberosity are re latively common. Th ey derivefrom an excessive ecce ntric contract ion applied from the long head of the biceps
femoris, the sem itend ino sus and the semimembranosus, which arise from it. In general, these injuries are associated with inten se sport load as they occur during racingor activities involving forc ed flexion of the thighs on the pelvis (e.g. gymn astics,dance) . The trauma is felt by the patient, with a sen sat ion lik e "a kick rec eived on theback" , which lead s to intense pain in the glut eal region and the poster ior aspect ofthe thigh , making walking difficult (Fig. 3.7). In cases of mild apophyseal d isp lacement , a thin elongated bony fragm ent which recalls the degr ee of curvatur e of the ischi
um (ischium epiphy sio lysis) can be identified. Thi s may be not easily recognized
Fig. 3.7 Ischial apophysitis. a Radiography and b coronal fat-suppressed tSE T2-weighted MRimage show a lesion caused by chronic traction on the hamstring insertion (7) with swelling anddeformity of the secondary ossification center (arrows) of the ischial tuberosity. The finding ofsubcondral sclerosis (arrowheads) demonstrates the chronic nature of the process, but the marrow edema of the tuberosity (asterisk) indicates that a recent trauma has also been superimposed
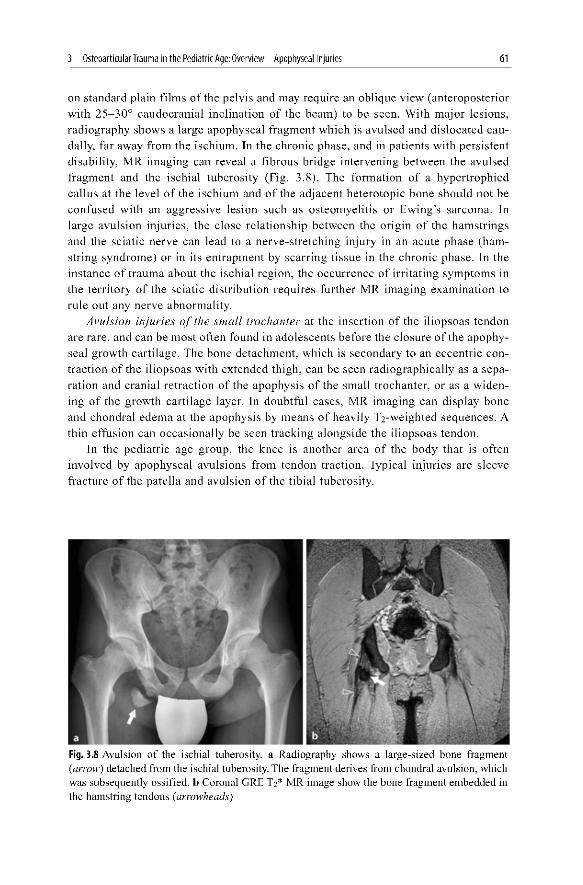
3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries 61
on standard plain film s of the pelvis and may require an oblique view (ant eroposteriorwith 25-30° caudocrani al incl inat ion of the beam) to be seen . With major lesion s,radiography shows a large apophyseal fragm ent which is avulsed and dislocated caudall y, far away from the ischium. In the chronic phase, and in pat ient s with per sistentdisability, MR imaging can reveal a fibrous bridge inter vening between the avulsedfragment and the ischi al tub ero sity (Fig. 3.8) . The form ation of a hypertrophiedcallus at the level of the ischium and of the adjace nt heterotopic bon e should not beconfused with an aggressive lesion such as osteom yelitis or Ewing 's sarcoma. Inlarg e avulsion injuries , the clo se re lat ions hip betw een the origin of the ham str ing sand the sciati c ner ve can lead to a nerve-stretching injury in an acute pha se (hamstring syndrome) or in its entrapment by scarr ing tissue in the chronic phase. In theinstanc e of trauma about the ischial region , the occurrenc e of irr itating symptoms inthe territory of the sciatic distribution requ ires furth er MR imaging examina tion torul e out any nerve abnormality.
Avulsion inj uries of the small trochanter at the inse rtion of the iliop soas tendonare rare, and can be mo st oft en found in adol escents before the closure of the apophyseal growth cart ilage. The bone detachment , which is seconda ry to an ecce ntric contract ion of the iliopsoas with extended thigh , can be see n rad iog raph icall y as a separation and crani al retraction of the apophysis of the sma ll trochanter, or as a widening of the growth cartilage layer. In doubtful cases, MR imaging can display boneand chondral edema at the apophysis by me ans of heavily Tj-weighted sequences . Athin effusion can occ asionally be seen track ing alongsi de the iliopsoas tendon.
In the pedi atric age group, the knee is another area of the body that is ofteninvolved by apophysea l avulsions from tendon traction. Typical injuries are sleevefracture of the patella and avulsi on of the tibi al tuberosity .
Fig. 3.8 Avulsion of the ischial tuberosity. a Radiography shows a large-sized bone fragment(arrow) detached from the ischial tuberosity.The fragment derives from chondral avulsion, whichwas subsequently ossified. b Coronal ORE T2* MR image show the bone fragment embedded inthe hamstring tendons (arrowheads)

62 M.Valleet al.
3Sleeve fractures ofthe patella are avulsions of a thin bony edge (often difficult to
see using x-rays) from the upper or lower pole of the patella attached to a moreextended slab of articular cartilage. Clinically, this lesion presents with full knee disability, is observed with a peak incidence between 8 and 12 years of age, and is secondary to the traction exerted by the quadricipital or the patell ar tendon on the polesof the patella, which are not yet ossified. Such sleeve fractures occur as a result ofspecific biomechanics (both tendons insert on the anterior side of the patella) and onthe basis of the fact that , during the maturation process, the growth cart ilage seems tobe, at this stage , more vulnerable than the underlying bone. If the avulsion extendsposteriorly to involve the art icular cartilage, the fracture is intra-articular in locat ionand associated with hemarthrosis. US can confirm the lesion by showing the avulsedchondral component, which is predominant compared with the bony one, and the tendon inserted into the detached fragment instead of the patella. Similarly, MR imagingcan reveal bone marrow edema in the patella, and is able to demonstrate the avulsedchondral component and to differentiate it from the effusion (owing to a lower Tz signal intensity) and the bony component (gradient recall ed echo [GRE] sequence). Thetreatment for undisplaced fractures «4 mm) is conservative, with the knee blocked inextension with a brace or soft cast. If displaced (>4 mm), the sleeve fracture of thepatella requires surgical reduction, re-alignment of the joint surfaces with or withoutinternal anchoring, and reconstruction of the extensor mechanism.
Avulsion injury of the tibial tuberos ity occurs when the traction applied to theextensor apparatus by the patellar tendon during rapid acceleration or decelerationphases exceeds the resistance offered by the physis and the perichondrium/peri ostium. This injury can be considered the extreme of the spectrum of the class oflesions which include, at the other extreme, Osgood-Schlatter disease . The maturation of the tibial tuberosity can be divided into four successive stages:I . cartilagineous, in which the tibi al tuberosity is fully chondral2. apophyseal, in which an ossification center appears in the tuberosity (in girls at
approximately 8-12 years of age, in boys at 9-14 years)3. epiphyseal, in which the secondary ossification centers of the tuberosity and the
proximal tibial epiphysis join to form a continuous bony bridge4. mature bone, in which there is bony closure between the tuberosity and the meta
physis of the tibia.
Avulsion-fracture of the tibial tuberosity can be divided into three types based onthe distance of the fracture edge from the top of the tuberosity (according toWatson-Jones):
in type 1, the fracture line passes through the distal part of the physis of thetuberosity and involves the nucleus of ossificationin type 2, the fracture line separates the ossification centers of the tuberosity andthe tibial epiphysisin type 3, the fracture extends into the proximal tibial epiphysis and involves theknee joint.

3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries 63
Sinc e the tub ercl e lies in a slightly lateral posit ion relative to the midl ine, plainfilm s should be obt ained in slight internal rotation . Type 2 and type 3 lesion s requiresurgica l reduction and stabilization .
In the arm , the elbow is the mo st common site of apophyseal avulsion by tractionmech anism. The medial epicondye (epitrochlea) , with its apophysea l nucl eus, is particul arl y vuln erabl e to biom echanical stresses as it gives origin to multiple tendons(common flexor tendon origin and pron ator teres tendon) and ligament s (medi al collat eral ligament) . Avul sion of the ossification cent er of the medi al epicondy le is mor ecommon in the USA rather than in Europe, due to the common practice of baseballin school-aged boys (so-called " litt le league elbow"). In th is sport, the trauma occur sdur ing repetit ive overh ead throwing motion s (pitching) . This cau ses a valgus stresson the elbow joint , which causes damage to structures at the medial epicondy le of thehum erus, par ticularly the growth plate. Of course, similar overload can be exerted inoth er sports that involve laun ching obj ect s (e.g. javelin, handball) as well. Theappl ied stress is parti cularly strong using techniqu es to pitch "cur ve" balls: this is thereason why the use of these techniqu es is forbidden in the age range between 9 and 14years, when the nucl eus of ossification has not yet fused. The repeated microtraum acan lead to acceleration of the epic ondy lar growth , tract ion apophysiti s with bonefragmentation, and apophys ea l det achment (Fig . 3.9) . Treatment is con serv at ive forundi splaced «5 mm) lesions; surgery is required for displaced (>5 mm) injuries andinvolves reconstruction of the medial coll ateral ligament and anchoring of the medi alep icondyle.
Fig.3.9 Avulsion of the secondary ossification center of the medial epicondyle. a In the acute phases of trauma, anteroposterior radiography shows diastasis between the humerus and the secondary ossification center of the medial epicondyle (arrow). b Follow-up radiogram reveals anintense periosteal reaction (arrowheads) over the ossification center

3
64
3.3Ligaments
M.Valleet al.
From both an anatomic and a functiona l point of view, th e ligament s of children and
adoles cen ts are int rinsically mo re lax than those of an adu lt, and thi s lead s to somej oint hyp erext en sib ilit y (Fig. 3.10). Upon reaching adulthood, th is ligam ent laxity,
which tend s to be particularl y acc entuated in females during pub erty du e to hormonal influenc es, tend s to redu ce progressively with a corresponding increase of j oint
stabi lity. In it self, the laxity protect s lig aments from po ssib le spra ins, but cannot be
considered really protective for the joint, since it leads to a ce rt ain degree of ins ta
bility. Ap art from these cons idera tions, lig ament inj ur ies in chi ldren mo st often
invol ve the atta chments into the immature bone , rather than the ligament subs tance.
US exam ination of ligaments in ch ildren is only po ssible at ce rtain body areas and,
of course , only when the ligament is exposed to the US beam through adequa te
acous tic windows. US allows a dyn am ic study du ring lig ament ten sion ing or loo sen
ing , thus identi fying injuries with lig ament elongation without rupture . MR ima ging
is mandatory to evalu ate some deep-seated intra-articul ar lig aments, such as the ante
rior cruciate .
Fig.3.10Bursitis of the medial collateral ligament of the knee. a Coronal ORET 2* MR image, andh corresponding US image show prominent fluid distension (asterisk) of the medial collaterall igament bursa, with separation of the superficial component of this ligament from the meniscofemoral and meniscotibial components (arrowheads) that overlie the condylar cartilage and themeniscus (arrows). Such a high-degree separation in the components of the medial collaterall igament is rarely encountered in the adult population and can be regarded as an indirect sign ofligament laxity in children and adolescents

3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries
3.3.1Apophyseal InjuriesDue to Ligament Traction
65
Although all ligament s can theor etically be the target of traumat ic injuries in children, most lesion s involve the ankle ligam ents following inversion traumas, themedial collate ral ligam ent , and the ante rior cruciate ligam ent of the knee in association with a fra cture of the intercondylar eminence .
In the school-aged child and adoles cent, the ligament s of the lateral compartment of the ankle are commonly affected during inver sion sprains. In most cas es ,the pathologic mechan ism involves sudden changes of dir ect ion while runn ing , ashapp ens in socc er, basketb all , or jumping sports . The anterior talofibula r ligamentis by far the most commonly damaged ligam ent. US demonstrates the avuls ion of anosteochondral fragments of sma ll size at the level of the insertion (fibular) of theligament , rather than a defect of continu ity of the ligam ent f ibers (Fig . 3. l la, b).Oft en, these fragm ent s are entirely cartilag inous and cannot be seen on plain f ilms.Thi s is the reason why ligam ent lesion s can be confused with Salt er-Harris type Ifra ctures. The fate of avulsed fragm ent s is twofold. If their size is small and theirposit ion is adj acent to the avuls ion site, newly apposed bon e will fill the distanc ebetween them and the bone, reabsorbing the avuls ion. On the other hand, if theosteochondral fragment is displ aced far away from the nidus of avulsion, thi s canlead to progressive ossification and growth of the fragment within the ligament,to cre ate an ossicle (Fig. 3.11c-e). In general , the lesion of the anter ior talo f ibul arligament is isol ated and US is suff icient for the diagnostic work-up .
Ultrasound is unable to evalu ate fra ctures of the intercondylar eminence of thetibia, at the distal insertion of the anterior cruciate ligament. These fractures are normally encountered between 8 and 14 years of age and are the consequence of a hyperextension mechanism of the knee, with or without ass ociated later al stress force s orrot ational components. The se fractures often occur after the patient has fallen from abicycle or has a knee sprain while ski ing, or they may be the consequence of directtraum a on the distal femu r when the knee is flexed . The classification of fractures ofthe intercondylar eminence (according to Meyer s-McKeever) is based on the degreeof disloc at ion (Fig. 3.12a):
in type 1, the fracture line has a hori zont al course and occurs at the base of theanterior port ion of the osseou s eminence with slight rising of the anterior edge ofthe fragmentin type ll, the inte rcondylar em inence is raised and angled posteriorly relative tothe tibi al plate au, but still in continuity with itin type lIlA, the eminence is completely avulsed by the tibi al surface but is notangled (Fig. 3.12b-d)in type IllB , the intercondy lar em inence has completely separated from the tibia,and is ra ised and rotated posteriorl y.Although these fractures can be iden tif ied on standard ante roposterior or lateral
views, obl ique projections for the intercondylar sulcus demonstrate the avulsed bonemuch better. In doubtful cases, a useful indirect sign for the diagnosis of type 1lesion s is detection of a distend ed supra-pate llar recess with a fluid-l evel appearance

3
66 M.Valleet al.
Fig.3.11 Anterior talofibular ligament sprain. a, b , Recent trauma. US image (a) and corresponding radiograp h (b) show avulsion of a thin cortical layer (arrowheads) from the latera l malleolus, in continui ty with a swollen but continuous ligament (arrows). c-c Old trauma. US (c), radiography (d) and Ti-weighted MR imaging (c) demonstrate a large ossicle (arrow) with regular margins embedded in the ligament (open arrows)
Type I Type II Type III Type IIIB
Fig. 3.12 Fracture of the intercondylar eminence cause d by anter ior cruc iate ligament traction .a Class ification acco rding to Meyers-McKeever (see text). b-d Type ili A lesion. Standard lateral radiog ram (b) and CT scan with sagitta l reconstruction (c) and 3D rendering (d) show avulsionof a large intercondylar fragment (arrow), with para llel orientation to the tibial plateau

3 Osteoarticular Trauma inthe Pediatric Age:Overview- Apophyseal Injuries 67
(lipohemarthrosis) . In children , th e av ulse d fragment can be a lm os t enti re ly made of
ca rt ilage. MR imagi ng should be used not onl y for bone and cruciate ligament
assessm ent but al so for the study of assoc iated les ions, such as meni sc al or medial
collat er al lig am ent tears, whi ch are frequently seen as asso ciated findings in th e ado
lesc en t. Surger y is indicat ed in typ e III les ions. Th e outcome is favoarable . On th e
other hand, avul sion fracture at th e t ib ial in sertion of th e po sterior cruciat e ligament
is exce ptiona l.
Suggested Readings
Bates DG, Hresko MT, Jaramillo 0 ( 1994) Patellar sleeve fracture: demonstration with MR imaging. Radiol 193:825- 827
Gottsegen CJ, Eyer BA, White EA et al (2008) Avulsion fractures ofthe knee: imaging findings andclinical significance. RadioGraphies 28: 1755-1 770
Hirano A, Fukubayashi T, Ishii T et al (2002) Magnetic resonance imaging ofOsgood-Schlatter disease: the course of the disease. Skeletal Radiol 31:334-342
Hogan KA, Gross RH (2003) Overuse injuries in pediatric athletes. Orthop Clin N Am 34:405--415Pisacano RM, Miller TT (2003) Comparing sonography with MR imaging of apophyseal injuries
of the pelvis in four boys. AJR Am J Roentgenol 181:223- 230Rossi F, Dragoni S (200 I) Acute avulsion fractures ofthe pelvis in adolescent competitive athletes:
prevalence, location and sports distribution of 203 cases collected. Skeletal Radiol 30:127-131Sanders TG, Zlatkin MB (2008) Avulsion injuries of the pelvis. Sem Musculoskel Radiol 12:42-53Stevens MA, EI-Koury GY, Kathol MH et al (1999) Imaging features of avulsion injuries. Radio
Graphics 19:655-672Volpon 18, de Carvalho Filho G (2002) Calcanea l apophysitis: a quantitati ve radiographic evalua
tion ofa secondary ossification center. Arch Orthop Trauma Surg 122:338-341


Major and Minor Pediatric TraumaticMusculotendinous Injuries
E. Cenovese.A. Leonardi, L. Callegari, I\I.G. Angcrclli. 1\1.Alhrizio, E. Spano and C. Fugazzola
4.1Introduction
Tendinous insertions on apophyses, artieul ar surfaces and epiphyses are " weakpo int s" in the mu sculoskeletal sys tem of childre n du e to the presence of growthplates, and these areas are particularly vulnerable to traumatic lesion s.
Although traum at ic lesion s of musculotend inou s and ligam entous soft tissue arenot common dur ing the growing years, their inci dence has risen, probably as a resultof an increase in sporting act ivit ies in th is age group.
Some authors beli eve that, dur ing growth, mu scular development is slower than
that of long bon es and that th is pred ispo ses to mu scul ar lesion s such as sprains and,though less likely, musculotend inou s strain lesions.
Furthermore, during pedi at ric age, tendons are usually more resistant to damagethan the car tilag e and bon e on which they are inser ted. Therefo re tendon tear s arenot as fre que nt as in young athl etes where it is common to diagnose abnorma litiesdue to overload (ins ertional tend inopath ies , bur sit is, tendonit is).
Finall y, acute ligam entous lesions are rare in children because of the elas tici ty ofart icular structures , whereas they are common in athletes .
4.2The Role of Imaging in Detection
The majority of the se lesions are diagnosed with anamnesis and phy sical examination. Imag ing techniques are useful to confirm a working diagnosis, and to loc al ize
E. Genovese (C8J)Department of Radiology, Circolo Hospital Macchi Foundation, Varese, Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
69
70 E. Genovese et al.
4the damage, define its extension, detect comorbidities and, above all, for prognosticreasons.
Ultrasound (US) is the gold stan dard in the study of musculotendinous disease.Ultras ound evaluation, usually using high-frequency (7- 15 MHz) linear probes,allows a high-r esolu tion analysis of the anatomical clements in their path. The idea levaluation is comparative and in dynamic phase. Color/power-Doppler integrationallows visualization of concomitant vascular lesions and the presence of hyperemia,if any.
Skeletal muscle present s a regular "toothbrush" struc ture due to the regular alternation of type III fibers (hypoechogenic) and of the perimysium (hypere chogen ic).
Every muscle is delimited by a thin hyperechogenic layer which is the epimysium;superf icial fasc ia, between the subcutaneous layer and muscle, has the appearance ofa thin hyperechogenic interface , whereas the bone is represented by a stronglyechogenic line followed by high attenuation of the ultrason ic beam.
The tendon has a hyperechogenic f ibri llar echostructure due to various interfacesbetween collagen fibers and endotendinous septa. It is delimited by an echogenic thinline, the external sheath, which assumes the identity of peritenonium for anchor tendons (i.e. Achilles ' tendo n, patella r tendo n, etc) and a synovial peritend inous sheathfor slip tendons.
It is important to emph asize that US scan, with the aid of stress maneuvers of thearea under examin ation, is the fir st-l ine investigation for the extr a-art icular ligament s, which are commonly seen as a thin hyperechogenic, homogeneous structureadjacent to the bone profile .
Magnetic resonance (MR) is usually the second-line investigat ion. Because MRexamination s are mult iplanar and mult iparametric, MR is an important diagnostictool where there is suspicion of lesion s involving contiguous skeletal structures (hidden fractures, apophyseal avulsions, osteochondral lesions, apophysitis , stress fractures), joints, blood vessels or nerves, and in those cases where preope rative planningbecomes nece ssary.
Thanks to its wide range of view and high sensitivity, MR is indicated in allmusculotendinous and ligamentous lesions that are too deep to be seen with US.
In detail , the ideal MR protocol for traumatic muscular lesion s star ts with a coronal comparative high-re solution acquisition that is able to identify the abnormality inits exten sion [proton density (PO) , fat saturation (FAT SAT) or short tau invers ionrecovery (STIR)] through the visualizati on of edem a and hemorrhage.
Then high-contrast axial acquisi tion (fas t spin echo (FSE) proton density (PD)/T2) is carri ed out to identify the damaged muscle , the lesion exten sion , and its relation to the perimu scular and intermuscular fascia e.
Axial T I acquisition enables the cl inician to distinguish between fibrosis and calcifi cations. In addition, in a subacute phase, hemoglobin degradat ion products canmake the hemorrhage hyperintense so that it can be distinguished from edem a whichis hypointense.
In elinical practice, x-ray is only indicated for the diagnosis of distortion traumaswhen an associated bony injury is suspected, or as a diagnostic aid where pathogenetic

4 Majorand Minor Ped iatric TraumaticMusculotendinousInjuries 71
osteo-articular factors (bon e misalignments, dimorphisms , anatom ical variant s) aresuspected.
4.3Muscular Lesions
Traumatic muscul ar lesion s can be div ided, according to the type of trauma, into distract ive lesion s (ind irect traumas) due to longitudinal force s that overcome the elastic resistance of the muscular f ibers, and contusion lesions (direct traumas) due toexternal causes.
The immediate effect of a traumatic lesion is damage to muscle fibers, coll agen ,and elastin , together with damage to capillary vessels, arterioles, and venules; theacute infl amm ation tr iggered by thi s proce ss lasts approximately 24-48 hou rs. Theprocess of repair could lead to "restitutio ad integrum", or replacement of tissue withconnective tissue , and fibrosis .
4.3.1Muscular Distractive Lesions
These involve the musculotendinous unit and can occur in the muscle belly or, mor eoften, at the musculo tend inous j unction.
These lesions are parti cularly common in sports where muscles are maximall ystrai ned; they occur mor e often at the beginning of the sport sess ion and more frequentl y involve those muscles of the lower limb s that participate in the movement oftwo joints; in some cases, less frequ ently in pediatr ic age, these lesion s occur at thelevel of the adductors : these muscles have ecce ntr ic-type contractions even thoughthey are not involved in two joints.
Three degrees of cl inical classif ication exist : a mild (elongation) lesion meansrupture of few muscle fibers with stiffness and light swelling of the ent ire muscle ;a moderate lesion (parti al rupture) con sists of tissue damage in up to two-thirds ofthe muscle belly, and its symptoms and signs are acute pain that is sudden and welllocali zed, with loss of function; a seve re lesion (complete rupture), typ ical at junction al level , involves the enti re muscle thickness and the symptoms are severe painwith complete loss of function. In this case, when the muscle is superfi cia l, palpation can reveal a gap area due to retraction of muscle tissue in the rup ture zone; thi sis generally accompanied by bleeding that may spread up to the surfac e and presentas ecch ymo sis.
Ideally, US scan should be performed between 2 and 48 hours after the lesion . Infact, during the fi rst 2 hour s the hematoma is sti ll build ing up, whereas after the 48thhour the hemorrhage may have spread beyond the muscle.
The Peetrons class if ication divides muscular lesion into four grades from anechographic point of view:

72 E. Genovese et al.
grade 0: absenee of so nographically detectabl e lesions
4 grade I (corresponds to the elongati on) : hypoechogen ic im age, du e to pr esen ce of
small ar ea s of se rohematic in fi lt ra ti on wi thin th e muscl e, m easuring mo re than
5% of th e mu scle volume (F ig . 4.1 a)
grade II: inter ru pti on of muscl e fi bers w ith a hypo-anechogenic gap which cor
responds to dam ag e of 5-50% of th e muscular volume on the ax ia l plane; in th is
ca se th e com pressi on effe ct of th e probe could show flu ctu ant fiber fragments in
a seroche matic flu id (Fi g . 4 .1b)
grade Ill: complete muscular lesion s w ith d istal end retract ions or lesions involv
ing more than 50% of th e muscl e , associate d with flu id pool an d po ssibl e in ter
mu scular ex tensi on of th e hematoma wh en th e lesion invol ves th e apone urosis
(F ig . 4.1 c) .
Possible M R appearances of mu scular lesions are grade d as follows:
Fig.4.1 Echographic appearance of various gradesof muscular lesions. a Elongation or grade Idistractive lesion. The longitudinal US scan ofthe pre-insertional region of the medial gemellus muscle shows abnormal echogenicity of thesuperficial muscle fascicles. At lesion level, anarea of diffuse hypoechogenicity is due to thepresence of edema and blood (arrow). The edema also involves the epimysial fascia, whichappears hazy. b Partial muscular tear or gradeII distractive lesion. Longitudinal US scan alongfemoral biceps muscle shows inhomogeneousabnormal echogenicity, mainly hypoechogenic,which corresponds to an area of fiber tear andhemorrhagic infiltration (arrowhead). c Com-
plete muscle tear or grade III distractive lesion. Longitudinal scan on the rectus femoral muscle showstear of the whole belly with retraction of the tear end (arrow) and a massive anechogenic fluid pool(curved arrow)

4 Majorand Minor Ped iatric TraumaticMusculotendinousInjuries 73
grade / (corresponds to elongation and stage I according to the ec hographic clas
si f ica tion): in long-RT (rep etition tim e) sequences it appears as a hyp erintens e
foc al signa l with hazy margin s due to ede ma and hemorrhage (Fig 4.2 a-c)
grade II: partial mu scl e rupture, with hemorrhage and edema. Interrupted mu scl e
fibers can be see n in the form of a clear hyper int en se area in T2 sequenc es (Fig .4.3a-c)
grade 11/: complete rupture of mu scl e fib ers with ret raction; it can be seen as a
hyper int ens ity in T2 due to hemorrhage, oft en organi zed as hem atoma. It is associated with edem a within and around the muscl e, sometim es with perimuscular
and int erfasci al flu id. The MR appearan ce of the hematom a changes as time passes:in th e hyperacut e phase (within 48 hours) , it app ears isointense with respect to
th e mu scl e in T) and hyp eri nt en se in T2 with or without fat suppress ion. In the
subac ute phase, the hematoma presents hyperinten sit y in T) and T2 and it is
delimited by a hyp erint en se border; th ese signal changes are due to the presenc e
of hemoglobin degradation products. In th e chronic phase, the hem atoma
becom es hypointen se in both T) and T2.
Fig.4.2 MR picture of a grade I distractivelesion of the left semitendinosus muscle.FAT SAT r, (a) and FAT SAT PD (b) sequences show a small hyperintense areawith hazy edges within the belly of themuscle; this is due to edema and hemorrhage (arrowheads). This finding is notrecognizable in the spin echo (SE) T) acquisition of the axial plane (e)

74 E. Genoveseet al.
4
Fig.4.3 MR appearance of a grade II distractive lesion of a left semimembranous muscle (partial musclc tear). FAT SAT PD (Proton Density) on coronal plane (a) and FAT SATT2 (b) on axial planeacquisitions reveal an irregular hyperdense area which corresponds to a small blood pool due tothe rupture of a small amount of tertiary fibers (arrow), with association of interstitial edema(arrowhead) . SET, sequence of the axial plane (c) shows a small area of hypointensity at the samelevel (curved arrow)
In a few cases (for example in pediat ric ag e when femoral perio steal stripping is
pre sent), par am agnetic contrast medium can be use ful for differential diagnosi s of
traumatic and neoplasti c lesions.
In exception al circ umstanc es, the contrast medium ca n be used in young ath letes
in cases of di ff iculty in gradi ng , in particular in low- gr ade lesion s. In fact in T I
acquis iti ons, contrast enhancement can show th e true extent of the mu scl e dam age ,
di fferenti ating it from the peril esion al ed em a.
4.3.2Muscular Contusions
Th ese lesions, the mo st common in pedi atric age, es pecially in con tact sports, usually involve muscl es of the lower limb s (partic ularly the quadri ce ps and an terior tib ial
m us cles) . Th ey present as swe ll ing , con tracture, j oi nt sti ffness, an d pai n, both spon
taneous an d palpat ion/mo vem ent induce d.Imaging of these lesion s is the same as tha t describ ed for di stractive lesions,
althoug h th ey are deep er, du e to thei r mech anism (u p to the bo ne level) .
4.3.3Complications and Follow-up
In the acute phase, compartment syndrome is an important potenti al complication . It
is cau sed by a ris e in inters ti tia l pressure within a mu scular compartment bounded by
an un st retchable common fas cia .

4 Majorand Minor Ped iatric TraumaticMusculotendinousInjuries 75
Other poss ible compl icat ions could be lesion relapse, intermuscular effusion,muscula r pseudocyst, post-tr aumatic fibro sis, and ossification.
In particul ar, the complex picture of myositis ossificans is the result of an extensive ossificat ion process within the scar tissu e present in a non-compl etely absorbedhematom a.
Imaging in thi s case can vary and can different iate different lesions, includingneopl asias.
MR can show an aspec ific mass extended to different muscle group s; calcific ation s are not well visualized, therefor e, in these cases, X-ray can clar ify the pictur e,whereas computed tomog raphy (CT) is for selected cases, particularly in relation topatient age.
US is reliable for monitoring the heal ing process and early detection of compl ications. MR is a second-line investigation in compl ex cases; in young athl etes thisinvestigation is indicat ed to predict the time cour se of rehabilitation and return toactivity; MR is able to ident ify resi dual fluid within fasciae as this is not a good prognostic factor. Furthermore, in these case s MR can differentiate fibrosis from granulation tissue.
4.4Tendon Lesions
In some young athletes, mechanical overload lesions are a possible finding. Thepathogenesis of these lesion s is rep resented by longstanding microtraumas in ananatomical area, due to inten se training with overload on norm al structures subjected to abnormal loads, sometimes as a result of congenital or postural causes (devi ation of the exten sor appara tus alignment, abnormal torsion, varus or valgus knee , pesplanus or cavus, etc).
Even though the weak point at this age is the growth plate, these lesions can occurat tendon level. All the different tendon components (tendon body and its externalsheath, musculotendinous junction, enthesis, and bursae) are subject to differentabnormalities of different inten sity.
4.4 .1Tendinopathy
These abnormalities present with the same set of symptoms: pain, local peritendinous swelling, antalgic limitation of function.
Class if ication is difficult due to the different forms of tend inopathy. However,four abnormalities can be iden tified :
I. paratendinitis, which involves peritend inous tissues (peritendonit is and tenosynovitis); in these cases US can show a hypoechogenic thickening of the peritenon iurn at the enthesis and a hypo-anechog enic fluid distension of the externa l sheath

76 E. Genovese etal.
4at slip-tendon level ; this is well recognized on MR with Tz-wcightcd sequences,as a hyperintense line around the hypo intense tendon
2. parat endinitis with tendinosis, including inflammatory and degenerative alterations of peri tendinous tissu es and of the tendon body
3. tendinosis, which is typ ical of adult age , and characterized by degenerative phenom ena and intr atendinous involution processes. In these cases, US shows a general increase of tendon volume, which presents hypoechogenicity, abnormalechostructure, and metaplasic calcific areas
4. tendonitis: various degrees of inflammatory changes within the tendinous matrix .
4.4.2Insertional Tendinopathies (Enthesopathies)
Thi s group includes clin ical pictures related to flogistic-degenerative involvement ofthe tendon insertion zone on the bone.
Enthesopathies are the clinical manifestation of conditions such as impingementsyndromes, traction tendinopathies that are typical of young athletes, so that someabnorma lities are identified with the most common sporting activity in which theyoccur (jumper's knee , tennis elbow, etc).
Whatever the involved tendon, the US picture is typical : the enthesis is thickened,hypoechogenic, and has irregular echostructure; it may be associated with bursal flogistic distension, and, in an advanced pha se, hyperechogenic calcification can befound within the tendon at insertional and pre-insertional level.
In these cases , MR is useful for evaluating peri tendinous structures (bursae, fatpads, fibrous tunnels) and can reveal if the abnormality is limited to musculotendinousstructures or extended to the bone tissue - i.e. reactive osteitis visible as hyperintensity with hazy marg ins at spongious level in T2 acquisitions with fat tissuesaturation (Fig. 4.4).
During teenage years , enthesopathies associated with apophysitis are rare. This isbecause the tendon insertion does not occur directly on the bone but is on the growthplate, which is not as resistant as the tendon to mechanical forces due to overload ortrauma.
The most frequent apophysitis occurring during teenage years is OsgoodSchlatter disease. This involves the growth cartilage of the anterior tibial apophysiswhere the patellar tendon is inserted.
Imaging is not absolutely necessary to confirm the clinical suspicion but it isimportant to recogni ze pred isposing conditions (low or high patella, external deviation of the patellar tendon, valgus knee, torsional abnormalities of the foot) .
At present, US is able to completely replac e X-ray in diagnosis. In fact it can showthe irregular and fragmented cortical profile of the ossification nucleus, thickening ofthe growth plate, patellar tendon enthesopathy, and deep infrapatellar bursitis.
Possible complications of this syndrome (tibial tubercle avulsion, patellar tendonrupture, early ossification of tibial growth plate) should be considered severe, as theycould influence the regul ar skeletal development.

4 Majorand Minor Ped iatric TraumaticMusculotendinousInjuries 77
Fig.4.4 Insertional tendinopathy of the posterior tibial tendon caused by a osteotendinous impingement syndrome. a With MR, SE Tj sequence on a sagittal plane shows a small sesamoid bone atthe tendon insertion site (arrow) and a hazy hyperintensity ofthe tendon structure at the same Icvel (arrowhead). b T2gradient echo sequence ofthe coronal plane confirm s loss of the typical tendon hypointe nsity (arrowhead) and shows a clear signal hyperintensity ofthe peritendi nous structures due to edema (curved arrow)
Fig.4.5 Sinding-Larsen- Johansen syndrome. At MR FAT SAT T2sagittal acquisition allows highlighting of the fragmentation of the inferior patellar pole(arrow) together with a hazy and inhomogeneous signal hyperintensity at theinsertional portion ofthe patellar tendon(arrowhead) and a light edema of theHoffa 's fat pad (curved arrow)
Sinding-Larsen-Johansen disease is an osteochondrosi s associa ted with in ser
tional tendinopathy of the patellar tendon at the inferior pole of the patell a where the
growth nucl eus lies . Th e X-ray picture is a fra gmentati on of th e patell ar inferior pol e,
and US shows th e typical appearan ce of an insertional tend inopathy.
MR can be useful for differ ential di agnosis (patellar fracture, stress frac ture ,
bipart it e patella typ e I, jumper 's tendonitis) (Fig. 4 .5).

4
78
4.4.3Bursitis
E. Genovese etal.
During pediatric age, involvement of bursae is usualIy secondary to an acute or chronicabnormality involving the tendon. Bursitis assoc iated with apophysitis is typic al butbur siti s with hemorrhagic effusion due to direct traum as may also be seen.
UsualIy, after a first acute phase with edematous thickening and inflammatory effusion, fibrosis can occur and this is responsible for the local friction that causes chronicity.
Both US and MR are able to identify these abnormalities and differentiate them fromcystic lesions of the synovial waII which are in communication with articular space.
4.4.4Tendinous Ruptures
These are rare in ped iatric age and are generalIy associa ted with bone avulsion s.However, in some cases, pers istent mechanical overlo ad could caus e partial or complete rupture at the ost eot end inou s inser tion level or within the tendon body.
US can show interruption of the continuity of tendon fibers, where the hem aticcomponent lies with various degrees of diastasis in the case of complete ruptures.
Complete ruptures are easily seen at MR, whic h shows fluid and hemorrh agewithin the lesion. The se are strongly hyperintense in T2. MR can also show the degreeof retract ion of both tendon ends in ord er to plan the best treatm ent.
4.5Abnormalities of Ligaments
Ligaments can be classified into intra- and ext ra-articular. Thi s dist inct ion is usefulfor a correct diagno stic approach.
4.5.1Extra-articular Ligaments
Symptoms of distractive traum as involving these structures are characterized bypain , local swelling, funct ion limit ation , and various degrees of instability.
US can distinguish acute lesions in three degrees of distortion :
grade 1: moderate ligament thickening at lesion level with diffu se hypo echogenici ty due to edemagrade 11: ligament thickening with internal inhomogeneous appearance andhypoechogenic area s representing the laceration point associa ted with a smallhematic poo l

4 Majorand Minor Ped iatric TraumaticMusculotendinousInjuries 79
Fig.4.6 Muscle vastus intermedius fibers injured from blunt trauma in the acute phase. Longitudinal ultrasound scan shows a retraction of fiber ends and the presence of a large hematoma interposed (hypo-anechogenic collection) (arrows)
grade ll/: complete lig ament rupture, generally in the medi al tract ; in th is case,US is an excellent tool for showing retraction of both end s and the presence of alarge hem atoma whi ch can f ill the capsule (Fig . 4 .6) . If the rupture is at insertional level with oste al-periosteal det achment, US should be integrated with otherimaging techniques (mainly standar d X-ray) .
Ankle spra ins are tho se mo st commonly related to sporting activities . Inver sionand ever sion traum as commonly involve ligaments from the lateral compartment (inparticular the anter ior talofibular ligament). In th is case, completing the inve stig ation with MR could allow evalu at ion of the subta lar joint, wh ich is not easily visiblewith US, to high light po ssible osteal avulsions with per i-in sertional spongious edemaand talar-dome-associ ated bony lesion s.
Collatera l ligaments of the kne e are also commonly involved in traum atic di sto rsive lesion s, particularly in the medi al compartment. In the se cases, MR shows theinvolvement of the bone at insertional level, and osteal imp act lesions, and couldexclude the typic al physeal fractures .
In add ition, in cases of joint effusi on with blood, MR can confirm or exc lude thepresence of ant erio r cruciate ligament- or meni scal-associat ed lesion s.

4
80
4.5.2Intra-articular Ligaments
E. Genoveseet al.
Fig.4.7Acute distractive lesionof anteriorcruciate ligament (ACL). WithMR, FAT SATT2sagittal acquisitionshows diffuse and inhomogeneoussignal hyperintensity at the ACL site,due to interstitial hemorrhage butwithout fiber strain of the ligament(arrow). This picture is associatedwithjoint effusion (arrowhead)
In ped iatric age, knee distortion traumas are usually rel ated to complex hyperextension mechani sms, sudden torsions during direct traum a. They commonly involve theanterior cruciate ligament, who se lesion al pattern varies in relation to skeleta l matu rity. In fact in adulthood, Sharpey 's f ibers att ach ligaments directly on the bone,whereas in childhood collagen fibers of the anterior cruciate ligament are fused withthe perichondrium of the epiphysial cartil age ; th is difference expl ain s why tibial eminence avulsions , typical of the immature bone, do not involve the ligament.
In physiologic conditions, the anterior cruci ate ligament appears as a hypointensestructure at MR . When traum a occurs, it can determine a part ial or complete (di ffuseor locali zed) laceration or a shape deform ation of the ligament without fiber strain;the level of the lesion can be prox imal (w ith det achment of the condylar insertion,with intr asynovial le sion or, rarely, with avul sion of a bone fragment) , medial (withfocal lesion along the ligament) , or distal (with or without bone avul sion) .
During the acute phase, edematous and hemorrhagic phenomena produce localized or di ffuse swell ing of the lig ament, which appears tortuous, and its marg ins aredifficult to di stinguish from the surrounding fluid and synovial infl amm ation . In thi sphase, the ligament appears hyperintense in T2-weighted sequences . Th is picture canbe ass ociated with the classical direct or indi rect magnetic resonance (MR) signs oflesion as intraspongiou s contusion of the posterior portion of the tibial late ral plateand of the corresponding femoral condyle, poster ior dislocation of the lateral meniscus, hypercurvature of the posterior cruciate ligament, anter ior tibia l shift, involve ment of the ant ero lateral capsular ligament, and Segond fracture (a typical avulsionof a cortical bon e fragm ent from the proximal tibial epiphys is) (Fig. 4.7) .

4 Major and MinorPediatricTraumaticMusculotendinous Injuries 81
For this reason , MR not only can identify correctly the site and extent of the lig
amentous damage but can also offer an accurate assesment of the degree of les ion
thanks to evaluati o n of the status of the surroun ding structures .
Suggested Readings
Azouz M, Oudjhane K ( 1998) Disorders of the upper extremity in childre n. Magn Reson ImagingClin N Am 6:677-695
Best T (1995) Muscle-tendon injurie s in young athletes. Clin Sport s Med 14:669-686Busch M (2000) Sport s Medicine in children and ado lescents . In: Lovell and Winter's Pediatric Or
thopaedic s, 5th edition . Lippincott Williams and Wilkins, Philadelphia, pp 1273-1313Clancy W (1990) Tendon trauma and overuse injuries. In: Leadbetter WB, Buckwalter JA, Gordon
JS (eds) Sport s induced inflammation: clinica l and basic science conce pt. Park Ridge, AAOS,pp 609-618
De Marchi A, Robba T, Ferrar ese E et al (2005) Lo studio radiologico delle lesioni musco lari: stato dell'arte. Radiol Med 11 0:11 5-131
Ecklund K (2002) Magnetic Resonance imaging ofpediatric musculoskeletal trauma.Top Magn ResImaging 13:203-218
Emery K (2006) Imaging ofsports injuries ofthe upper extremity in children. Clin Sports Med 25:543568
Gill TJ, Lyle JM ( 1996) The immature ath lete. Clin Sports Med 15:401-423Long G, Cooper JR, Gibbo WW (1999) Magnetic Resona nce imaging of injuries in the child ath
lete. Clin Radiol 54:78 1-79 1Palmer WE, Kuong SJ, Elmadbo u HM (1999) MR imaging of myotendinous strain. AJR Am J
Roentgenol 173:703-709Peetrons P (2002) Ultrasound of muscles. Eur Radio l 12:35-43Prince JS, Laor T, Bean JA (2005) MRI of anter ior cruciate ligament injurie and associated find
ings in the pediatric knee: changes with skeletal maturation. AJR Am J Roentgenol 185:756762


Traumatic Lesions of the Peripheral Nerves 5E. Pacciani, F. Ran disi, C. Orazi, 1\1. Valle and C. Marti no ll
5.1Introduction
Traumatic peripheral nerve lesions are relatively rare in the pediatric age group and
are generally distinguished by a more rapid healing process and an improved prognosis compared to les ions obs erved in adults. The type of nerve injury varies according
to age. Nerve lesions from sprains and accidental insult during treatment of peripheral nerves, as happens in particular with the sciatic nerve, generally occur during the
neonatal period; lacerations from cuts or compression of a nerve can occur in chil
dren over 3 years of age. In pre-adolescence, the most frequent causes of nerve lesion
are intra-articular dislocation, and fractures of the elbow (especially supracondylar
fractures) and knee, which are sometimes a secondary consequence of sports injuries.
Supracondylar fractures of the elbow with severe dislocation of the bone fragments
can lead to a nerve lesion of the median nerve and the ulna, whil e the common lesion
of the peroneal nerve is most frequently caused by spraining the knee during sports
such as football and skiing. Nerve deficits resulting from elbow fractures generallyhave a positive evolution with a relatively rapid spontaneous recovery. In adolescents,
peripheral nerve lesions are similar to those encountered in adults and are mainly
caused by road accidents or by wounds from firearms or knives.
A simplified classification of nerve lesions proposed by Seddon includes the fol -lowing:
traumatic nerve root avulsion of the spinal marrow
neurotmesis, in which there is complete disruption of the nerve and the nerve
sheathaxonotmesis where the nerve sheath is intact but the axons are disrupted
E. Pacciani (C8I)Department of Diagnostic Imaging, Pediatric Hospital "Bambino Gesu", Palidoro (RM), Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
83

5
84 E. Pacciani etal.
neurapraxia , where the damage involves the perineural sheathing while axonalcontinuity is preserved.
Neurotmesic lesions represent the severest degree of nerve lesion, while neurapraxi al lesions correspond to a temporary nerve dysfunction without permanentdamage.
The clinical diagnosis of a peripheral nerve lesion in the pediatric age group isoften difficult, especially in small children , and normally involves the examinationof nerve conduction (neurography) and the spontaneous and voluntary activity ofmuscular regions, which is not always easy to do due to the lack of cooperation fromsmall children. Diagnostic examinations to cre ate images, carried out on completionof electrophysiological studies, are being used increasingly frequently to identify thesite of the lesion and to establish the cause and extent of the dam age. Imaging studies , generally used to identify the presence of hematomas in the seat of the lesion, ormuscular alterations that are secondary to the nerve damage, can also allow identification of nerve structures and possible lesions of them . Ultrasound and magnetic resonance imaging (MRI) are the main imaging methods capable of meeting theserequirements.
5.2Ultrasound Scanning
The identification of nerves using ultrasound scanning is based on precise knowledge of their locali zation and the course of the medical problem and on careful analysis of anatomical relationships with surrounding organs. Modern ultrasound scanningequipment with broadband transducers, which have high spatial resolution for thestudy of superficial structures , is capable of identifying the main nerves that runthrough the limbs and most of the secondary and terminal ramifications, even whenthe ir size is less than a millimeter. When evaluated along the long axis with a highfrequency transducer, the internal structure of the peripheral nerves displays anunusual arrangement , made up of a series of elongated hypoechoic areas with a fascicular appearance, which are parallel to each other and separated by hyperechoicbands. Hypoechoic areas are arranged in series and have a well-defined appearance;they are oriented along the longitudinal axis of the nerve. Using transverse scanning,the fascicles take on a rounded appearance and are embedded in a hyperechoic matrix(Fig . 5.1) .
Comparison between ultrasound scans obtained in vitro and the correspondinghistological sections has demonstrated that the hyperechoic areas correspond to thefascicles , while the hyperechoic matrix is related to the interfascicular epineurium.
With entrapment syndromes, traumatic lesions of nerves constitute one of themost important applications of ultrasound in diagnosis of the peripheral nervous system, thanks to the quality of the diagnostic information provided, which has animportant effect on the clinical handling of the patient.

5 TraumaticLesionsofthePeripheral Nerves
b
85
Fig 5.1 Echostructure of the peripheral nerves. a "Short axis" scanning of the ulnar nerve (arrows)obtained using a 17-5 MHz transducer. b Schematic diagram of the internal structure of a peripheral nerve. In the scanning plane, the structure of the nerve is characterized by a "honeycomblike" appearance, due to the presence of rounded hypoechoic areas (arrowhead) which representthe fascicles
The amputation of a periph eral ner ve usuall y evolves into a post-traumati c neuroma. This can be vis ua lize d usin g ult rasound, as an elongated hypoechoic mass tha tgro ws rel at ively rapidly after the traum a on the edges of the amputated nerve.Ultr asound diagno sis is based on visualization of the connect ion of the neu rom a withthe distal edge of the ner ve. Most of the neuromas cau sed by amputati on have regular edges , although in some cases they can have an irregular appearance when thereare fi brous adhes ions and bands with the sur rounding t issues.
In lesion s caused by deep traumas of the periph eral ner ves of limb s, ultrasoundhas several significant adva ntages over MRI , mai nly in eva luation of the ne rve damage in an acute phase, where the inte nse edema and hemorrhage of the soft ti ssuesalong the stab incisi on of the wound cause a wides pread inc rease of the signal in Tzweight ed sequences , so that it becom es impossi ble to mak e a preci se identi f icationof the cho rdae and the lesions ca use d by them. Oth er sig nifi cant advantages of ultrasound cons ist of the possibil ity of examining, in a sing le scan, long segments ofnerves in limbs in a few seconds and, in the presence of a continuous lesion , the ability to orient the transducer along the longitudinal axis of the ner ve concerned, whichfrequently runs obl iquely compared to the orthogonal plane s used in MRI. Thi s canprove part icul arly important in preoperat ive ass ess ment in the case of complete ne rvelesion s, when it is necessary to obt ain a precise measurement of the di stance betweenthe stumps and the caliber of the ner ve at the level of the lesion, in order to plan atranspo sit ion operation (grafts of sensi tive nerves) or syntheti c tubul izat ion. In thesecases, high-r esolution ult rasound provid es ex tre me ly acc urate resul ts for preoperat ive plann ing. In th is regard , it is useful to rem ember tha t mea su rem ent of the

86 E. Pacciani etal.
5distance betw een the stumps mu st include not onl y the end-to-e nd distanc e of the
nerv e stumps but also, in the presenc e of terminal neuromas , the end-to-end distanc e
of th e neuromas, which must obviously be resected during surge ry (Fig. 5.2). In th is
spe cif ic f ield, ultrasound has undoubted advantages, mak ing it po ssibl e for th e sur geon to follow the course of the nerve branch in real tim e and to fix the reference
points on th e skin re lated to localizat ion of th e lesion s. After reconstruct ive surgery,
ultrasound allows reliable assessme nt of th e continu ity of the ner ve at the level of
anastomos is and exclus ion of a per ineural flu id coll ection. A foc al increase of thevolume of th e ner ve can be registered, corresponding to the suture lines at th e level
of both anastomoses. Thi s inc rease mu st be con sidered within th e standard limits
when it is relat ively small and fu siform.
On the oth er hand, the presenc e of hyp ertrophic fibrous tissue at the ana stomosiscan suggest inadequate fusion of the nerve heads, oft en resulting from excess ive ten
sion or supra-i nfect ion . In th e autogenous gr aft s, the interven ing tract generall y corresponds to one or more segm ent s of a sur al nerve donor inserted in parallel to join
the proximal and distal fascicular structures of th e damaged nerv e. In deep wounds
that cau se partial discontinuity of the fasc icl es without causing a complete interrup
tion of the chorda, ult rasound can mak e it po ssibl e to qu ant ify th e perc entage
involvement of the fascicles, comparing the number of fascicles embedded in the
hypoechoic neuroma with respect to those that maintain a regular mo rphology and
are external to it. In other case s, the neuroma may affect the entire thickness of the
nerve, even though the les ion is not complete, causing a fusiform increase in volume
which take s on a globally hypoechoic echostructure with loss of the fas cicular
appearance (Fig. 5.3) . However, the state of the sing le fascicles (interrupted or con-
Fig.5.2 Complete continuous lesion of the ulnar nerve at the third median of the arm of a 15-yearold girl following a deep wound caused by a glass splinter. The ultrasound image, performed witha 17-5MHz transducer and suitably aligned according to the longitudinal axis of the nerve, demonstrates the proximal stump (open arrows) and distal stump (white arrows) of the nerve, which tcrminate in hypoechoic ovoid areas that correspond to amputation neuromas (N). One can observethe larger size ofthe neuroma in continuity with the proximal stump. Forcorrect pre-surgery mapping, the distance between the stumps must be calculated between the apices ofthe neuromas (dl)and between the junctions between neuromas and the nerve with a normal appearance (d2)

5 TraumaticLesionsofthePeripheral Nerves 87
t inuous) in the context of a ne uroma that has developed in the presen ce of a partial
nerve lesion cannot be defined using ultrasound, given the hypo echoic appearance of
th e ner ve tissue and th e scar t issue that surrounds it.
Sp rain/traction lesio ns may be of a iat rog en ic nature, res ulting from surge ry (for
example, elongation surgery of limbs, po sitioning of osteosyn thetic devices to stabi lize fractures), or they may be secondary lesion s ca used by distortion traumas (part
ly du e to the greate r cap sulo-l igam entous laxi ty of artic ulati ons in pedi atric age ) or
art icular d islocation. If th ese frac tures involve dislo cat ed bon e stum ps , they can
cause sprains of the chordae, lead ing to a functiona l deficit tha t is proportion al to theexten t of th e sprai n. Th e nerves that are principally subject to sprain lesio ns in chi l
dren are the rad ial ner ve (in fractures of the hum eral diaphysis) , uln ar nerve (in
suprac ondy lar fractures of the hum erus) (F ig. 5.4), and common f ibular nerv e (in
distortion traum as of the knee).
In fractures of the hum eral diaphysis, where there is an on set of function al deficit
of the radial ner ve as an event that is both sync hronous with the traum a and subse
qu ent to th e reduc tion surgery, ult ra sound can compens ate for th e limitat ions of MRIrelated to the inadequate contrast betw een loco-reg ion al soft tissues (du e to an
inten se edema and the presence of granulation tissue that alt ers the signal, mak ing it
difficult to identi fy the nerve and qu anti fy the dam age) and the artifa cts ca used by
osteosynthesis equipment. In thi s cl in ical scena rio, in wh ich ele ctrophysiological
examinat ion s often make it impossible to decide on the be st the rapeutic stra tegy,
ult rasound can exclude a lesion-in-continu ity of the radial nerve, identify a confli ct
Fig.5ol Partial traumatic lesion of the median nerve in a 12-year-old boy with a cut wound on thevolar side of the left wrist. a Longitudinal scan of the median nerve (arrows) obtained using a12-5 MHz transducer at the level of the carpal tunnel. The median nerve appears to be widelythickened and hypoechoic (arrowheads), corresponding to the plane of lesion (curved arrow) inthe absence of definite gaps. The flexor tendons of the fingers t tfl , see below) have a normalappearance. In the deepest part ofth e image, it possible to see the bones, still partly cartilaginous,which form the floor of the carpal tunnel; the radius with the secondary nucleus of ossificationof the epiphysis (e), the semilunar valve (SL), and the capitate (Ca). h Corresponding clinical picture, highlighting the cutaneous scar (arrows) of the previous cut wound

88 E. Pacciani etal.
5
Fig 5.4 Neuropathy of the ulnar nerve at the elbow following a supracondylar fracture of thehumerus with significant dislocation of the bone stumps. a X-ray examination of the elbow performed in anteroposterior projection. b "Short axis" echotomographic scan of the ulnar nerve(arrowheads) , examined on the pathological side on a slightly cranial plane with respect to thecubital tunnel, highlights its marked increase in volume with respect to the contralateral nerve (c)as the outcome of the traction induced by a supracondylar fracture
betwe en the ner ve and fracture fragm ents, and different iat e an entrapme nt by scar tissue fro m a simple sprain lesion of th e nerv e, giving indica tions as to whether or not
to revise the surgical strategy.One of th e lesion s cau sed by nerve sprain which is commonly found in pediatric
age involve s the common fibular nerve in th e hamstring (F ig 5.5) . Th is nerve, whichis "anchored" in its seat, between the bifurcation of th e sciatic ne rve and peroneal
tunnel , is particularly susce ptible to sprain traumas in the region of the kn ee due todi stortion s or po sit ion s that involve prolonged stre tching. Th e result is a functional
deficit of var ying magnitude in the inn er vat ion terr itory, and demonstrat ion of an
ex te nsi ve fusiform neuroma of the nerve in th e ham string, extended by bifurcation
until it reaches distally a plane passing betw een th e lateral gemellus and th e tendon
of the biceps femori s tendon jerk reflex . More seri ous traumas, such as dislocation
of the femoral -tibial junction with avulsion of the bic ipita l groove, can lead to
lace ration of the fi bula r ne rve . Fortunately, these traumas are exceptional in pedi
atric age.

5 TraumaticLesionsofthePeripheral Nerves
5.3Magnetic Resonance Imaging
89
Fig.5.5Neuropathy of the common fibular nerve in a patient with previous serious distractive trauma of theknee . a Echotomographic examination of the hamstring, performed with a 12-5 MHz transducer of knee,highlights the widespread fusiform increase in volumeof the commo n fibular nerve (arrows), which is fullyhypoechoic with loss of the fascicula r structure, withrespect to the normal nerve of the contralateral limb (b).c MRI image, obtained with Ti-weighted spin echo sequences, confirms the widespread increase in volumeof the fibul ar nerve of the hamstring, in its course between the lateral gemellus (gl) and the bicep s femoristendon jerk reflex tbf) . d Surgery confirms the conspicuous increase in volume of the fibul ar nerve (arrow),which is probably compatible with a sprain trauma ofthe fibers
In th e case of a peripheral nerve lesion caus ed by trauma, M RI is often used to iden
ti fy the presence of po ssible hematomas (F ig. 5 .6) or hemarthro sis res pons ib le fo r
nerve compression: in this ev en t, the neuropathy ge nera lly presents a complete
regression, with res o luti on of the cause of com pressio n.
M RI is abl e to demonstrate signal modif ications caused by a ner ve les ion an d
prov id es inform ati o n about the durat ion of the les ion. In no rmal co nditi ons th e mus
cl es present an inte rme di ate signal in T i-wc ightcd sequences a nd a low intensi ty o f

5
90 E. Pacciani etal.
Fig.S.6 Neuropathy of the femoral nervecausedby a hematoma in a 12-year-old patient withavulsion of the anterior superior iliac spine.Ti-weighted turbo spin echo axial MRI. performedwith suppression of the adipose signalafter administration of contrast agents, revealsthe presence of a hematic cyst (arrows) lyingbetween the iliac wing and the iliopsoas muscle. The cyst indirectlycauses compression ofthe femoral nerve whichstarts in the muscularplasterapplied between the ileumand the psoas
signa l in Tj-weighted sequences . Chronic mu scul ar denervation is characterized, inT j-we ighted sequences, by atrophy and adipose infi ltration of the mu scle (Fig. 5.7a).In the cas e of subacute lesion s, the denervated mu scle s do not display significantmodificat ion s of the signa l in T j-we ighted image s, while they display an attenuatedsigna l in Tj-weighted sequences with saturation of the fat in rela tion to the edema(Fig. 5.7b) . Identification of the mu scle s involved in the denervation process can provide useful indications for identifying the per ipheral nerve that is affected and thattherefore requires examination.
In norm al condition s, the peripheral nerves di splay a low intens ity of signal, inboth T 1- and T2-weighted sequences, and are frequently surr ounded by adipose tissuealong the ir course ; thi s anatomica l characteristic make s identification easier, in theT j-we ighted sequences as hypointense form ations, with a typical fascicular structure,bounded by a high level of hyperintensity of the per ineural fat (Fig . 5.8).
In the case of an acute ne rve lesion , the peripheral le sion s typically present anincrease in both caliber and intensity of signal in T 1- and T2-weighted sequences ,with an extension that varies prox imally with the pre sence of an intraneura l edemaand with Wallerian degenerat ion (Fig . 5.9) . In chronic lesions, however, usually onlyan increas e in th ickness of the nerve can be recognized (Fig. 5.10).
Locali zed thickening of the nerve can also be correla ted with the presence of anamputation neu roma or per ineural scar tissue . The se circumstances are di ff icult todi stinguish even after administration of param agnetic contras t agents . The amputation neuroma is supported by a non-neop lastic reactive proliferation in the seat of thenerve lesion (Fig. 5.11). The use of paramagnetic contrast agents also makes it possible to recognize the presenc e of scar tissue in the perin eural sea t respon sibl e for theneuropathy (Fig. 5.12).

5 TraumaticLesionsofthePeripheral Nerves 91
Fig 5.7Chronic muscle denervation of the leg caused by lesion of the common fibular nerve (a)and the subacu te nerve of the deltoid musc le caused by lesion of the axillary nerve (b) in two different patients, who are 15 and 16 years old respectively. a The T r-weighted turbo spin echo axia lMR I image displays extensive atrophy and adipose infiltration of the muscles of the anterior andanterior lateral cavities of the leg. b The T2-weighted spin echo coronal MRI image with suppres sion of the adipose signal shows a widespread intensity of the deltoid muscle
Fig.5.STi-weighted spin echo coronal MRI image of the right brachial plexus in a IO-year-old patient shows the cho rdae (black arrows) with a typical fascicular appeara nce, which are parallel tothe course of the subclavian vesse ls (white arrows). The T i-weightcd sequence also highlights theperineural adipose tissue and the relationships between the nerve structures and the subclavian muscles (sm) and the small pectoral muscle (spm)

92 E. Pacciani etal.
5
Fig.S.9 Neuropathy of the radial muscle following a supracondylar fracture of the elbow in a 6-yearold patient. Tr-weighted turbo spin echo axial MRI images (a) and Ts-weighted turbo spin echoaxial MRI images with suppression of the adipose signal (b) display an increase in volume and intensity of the signal of the radial nerve (arrow)
Fig.S.10 Neuropathy of the right sciatic nerve in a 4-year-old patient suffering from recurrent dislocation of the right hip. Tz-weighted spin echo axial MRI shows a moderate increase in volumeof the right sciatic nerve (arrowhead): there is also an alteration of the signal of the musculusquadratus of the right femur
More recently, evolution of MRI techniques has made it po ssib le to use a new
method for studying the peripheral nerve sys tem, indicated using the term MRI neuro
grap hy . This technique makes it po ssible to sh ow peripheral nerves in a simi lar way
to ang iograph ic im ages, with improved di fferenti ation of the nerve stru ctures of the
muscles . The use of MRI neurography in pediatric pat ients is particularly interesting
given th eir intolerance to needle e lectromy ography. MRI neurography invol ves th e
use of m agnet s with a high magnetic f ield (from 1.5 Tesla) and th e us e of sur face
coils. Th e mo st widel y used technique is based on th e use of Tz-w eighted sequences
with suppre ssion of th e ad ipose s ignal. Thin contiguous scanne rs are gen erally used

5 TraumaticLesions ofthe Peripheral Nerves 93
Fig.S.11 Amputation neuromaof the median nerve causedby a cut lesion in a 13-year-oldpatient. a In the saggital spineeho Ti-weighted image, onecan observe marked thickening of the median nerve (arrow), which displays a normalcaliber proximal to the neuroma (arrowhead). b The Tl weighted spin echo axial MRIimage with suppression oftheadipose signal using administration of paramagnetic contrast agents shows intense potentiation of the amputationneuroma (arrows)
Fig.S.12Neuropathy of the ulnar nerve in a 5-year-old patient with a previous supracondylar fracture of the elbow.Ti -weight ed turbo spin echo axial MRI images taken before (a) and after (b) administration ofparamagnetic contrast agents.The ulnar nerve (arrow) has increased in volume andis bounded by a thin hyperintense annulet after the administration of contrast agents (arrowhead) ,which can be ascribed to perineural scar tissue (surgically confirmed)
and ar e or iented along the main course of the nerve structures requiring ex aminat ion.
Exam ination performed using thi s technique all ow s only partial representation of the
ne rves in sing le sca ns; subsequently, reformatting of the im ages using Multipl an ar
Reconstruction (MPR) or Maximum Intensity Projection (MIP), using coronal or
ob lique planes, allows complete identificat ion of the nerve structures und er exami
nation . In peripheral nerve lesions, MRI neurography, performed after completion of
conventional MRI , is capabl e of provid ing a more pr ec is e asse ssment of neural

94 E. Pacciani etal.
5damage, making it possible to identify any possible breaks in the nerve structures.
MR[ neurography is extremely us eful for studying traumatic lesions of the brachial
plexus (Figs. 5.[3 and 5.[4).
Brachial plexus injures du e to accidental trauma in children are relatively rare
compared to obstetric lesions. Recently, Smith and colleagues have described the use
of MR[ neurography in childbirth lesions of the brachial plexus.
Fig.S.H Lesion caused by wrenching of the right brachial plexus in a 16-year-old patient. MRIneurography using oblique-coronal planes reveals the presence of a nerve avulsion (arrowhead)and trauma-induced meningocele of the C7 root (arrow)
Fig. S.14Neuropathy of the radial muscle in a simple supracondylar fracture of the elbow. a TheX-ray shows a marked dislocation of the bone fragments. b MRI neurography using sagittalplanes highlights an entrapment of the radial nerve (arrows) between fracture stumps. c In axialMRI in protonic density it is possible to identify an increase in the volume of the radial nervebetween the fracture stumps (arrow)

5 Traumatic Lesions ofthe Peripheral Nerves 95
In the event of nerve lesions in pediatric age, the diagnostic approach using imag
ing is certain to involve the preliminary use of an ultrasound examination capable of
defining, on the basis of the clinical and electrophysiological measurements, the site
and extent of the lesion. MRI, performed in pediatric age generally involves sedation
of the young patient, and will be used as a diagnostic technique exclusively in select
ed cases where ultrasound is not decisive. In nerve lesions of the limbs, the use of
immobilization devices, such as thoraco-brachial plaster or air cushions, can allow
MRI examination without resorting to sedation, wh ich will have to be used if th e
aforementioned technique fails.
Suggested Readings
Bacigalupo L, Bianchi S, Valle M, Martinoli C (2003) Ultrasonography of peripheral nerves.Radiologe 43:841-849
Carmel P (1982) Peripheralnerve lesions in pediatrics age group. Pediatr Neurosurg, New York, Grune& Stratton , pp 345-360
Filler AG, Maravilla KR, Tsuruda JS (2004) MR neurography and muscle MR imaging for imagediagnosis of disorders affecting the peripheral nerves and musculature. Neurol Clin 22:643682
Fleckenstein JL, Watumull D, Conner R et al (1993) Denervated human skeletal muscle: MR imaging evaluation . Radiology 187:213-218
Howe FA, FillerAG, Bell BA et al (1992) Magnetic resonance neurography. Magn Reson Med 28:32838
Kline D, Hudson A (1995) Nerve Injuries. WB Saunders, PhiladelphiaKoltzenburg M, Bendszus M (2004) Imaging of periphereal nerve lesions . Curr Opin Neurol
17:621-626Seddon H (1975) Surgical disorders of periphereal nerves, 2nd edition . Churchill Livingstone,
Edinburgh-LondonSilvestri E, Martinoli C, Derchi LE et al (1995) Echotexture ofperipheral nerves : correlation of US
with histologic findings and criteria for differentiation with tendons . Radiology 197:291-296Smith AB, Gupta N, Strober J, Chin C (2008) Magnetic resonance neurography in children with birth
related brachial plexus injury. Pediatr Radiol 38(2): 159-163Weig SG, Waite RJ, McAvoy K (2000) MRI in unexplained mononeuropathy. Pediatr Neurol 22:
314-317


Imaging of Regional Injuries: The AxialSkeleton - the Skull, Vertebral Column,and Thoracic CageC. Fonda. 1\ 1. l\lortilla. C. Ces arini and 1\1. Basi le
6.1The Skull
In contrast to head inj ur ies in adults, there are three distinct causes of skull and braintrauma in childr en: birth trauma, acci denta l trauma, and non-accident al trauma.Acci dental trauma includes impact injuries in children and adol escents. Static forcesslowly appli ed to the head can produce skull frac tures, contusions, and lacerations.Falls from low height s can cause linear fractures (2- 3%) and are rarely acc ompanie dby intracranial lesion s. More serious consequences are the res ult of high-energyimpa ct injur ies, which often involve multiple trauma whereby severe skull and braininjuries form a part of the clinical present ation (19 %), oft en proving fatal or cau singsevere disabilit y.
6.1.1Epidemiology
Skull fractures are found in around 27% of children with he ad inju ries - in around75% of major traum a pat ient s and 10% of minor traum a patients. The incidencereported in the literature is highly var iable: some studies report only 2% of fracturesin minor head inj uries.
Most fractures are linear and involve the parietal bones, with the presence ofhem atoma overlying the fracture (Fig . 6.1) . These fractures spontaneously he al. Thepresence of a fracture cannot be ruled out by a negative rad iolog ical exam ination,and the simple visua liza tion of a fracture line says little in relation to the possible
C. Fonda ( 12=<:1)Department of Pediatric Radiology, Children's Hospital Meyer, Florence, Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
97

98 C. Fonda etal.
6
Fig. 6.1 Three-year-old child. Accidental trauma. a Lateral view radiography. Right parietal thinhorizontal fracture line (arrow). b CT with multiplanar coronal reconstruction and bone window.Swelling of the epicranial soft tissue and the underlying thin parietal fracture line can be identified (arrow)
Fig.6.2Three-year-old child. Accidental trauma from a fall. a CT 3D rendering of the skull showsleft parietal fracture line (arrows). b Axial scan with parenchymal window shows the small layerof epidural hematoma below the fracture line and swelling of the epicranial soft tissue (arrow).c Axial scan with bone window: left parietal fracture line can be identified, easily distinguishablefrom the hypoattenuation of the coronal and longitudinal sutures (arrow)
alte rat ion of th e intracrani al structures , and in itse lf do es not modify tr eatment.
Onl y 40% of ch ildren with epidur al hem atoma, and onl y 15% of those with sub
dural hematoma, have a fracture (Fig. 6.2). In ch ildre n, a pathologi cal clinical pres
enta ti on with no sign of fracture but which nonetheless requi res tr eatm ent, including
ex tra-ax ial hem atoma, is not a rare event.
With computeri zed tomography (CT) volume tri c acquis it ions, it ha s become
harder to miss even th in fracture lines, as occurred in ax ia l sections when the frac
ture line was par allel to the scan plane . Demonst ration of the traumatic le sion in
itself becomes important in non-accidental injuries, even in the abs ence of brain
injuries.

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 99
Fig.6.3 Radiograph of a right parietal "ping-pong fracture". The depression of the skull is clearlyevident, similar in appearance to a squashed ping pong ball
Fig. 6.4 CT of a right parietal depression fracture radiating superiorly (arrows). a 3D reconstruction. b Axial scan with bone window
Th e mo st common fractures are linear parietal fractures, which can be hori zontalor vertical. Short vertical fractures can be diff icult to di stinguish from accessory
sutures. Th e f ind ing of a fracture may be faci lita ted by evidence of swell ing of theoverl ying epicran ial soft t issu e (Fig. 6. 1b) .
Occipital or frontal fractures are more commonly cause d by a direct blow. Theswell ing of epicranial soft tissue in the area of the blow can be associ ated with leak
age of ce rebros pinal flu id through the fracture (th is occurs at the point of maximumdeform ation of the skull as a result of the ene rgy of the blow) .
The plast icity of the infant skull is such that de form at ion s can occur, g iving riseto depress ion s known as "ping pong fractures" (Figs. 6.3 and 6.4) . Growing skullfracture s, also known as craniocerebral erosion s (Fig . 6.5) , are rare sequelae of skull

100 C. Fonda etal.
6
Fig.6.S CT of seven-year-old child with "growing skull fracture". Lytic area in right posterior parietal location. a Coronal multiplanar reconstruction (MPR) with parenchyma window. h 3D volume rendering. In correspondence with the lytic lesion, involvement of the cerebral parenchymacan be seen through the foramen created by the fracture and in the presence of a dural tear. Theparenchymal pressure causes progressive widening of the lytic area, hence the name "growingskull fracture"
fractures, where a skull defect progressively enl arge s following a tear in the duramate r, as can occur for example in firearm inj uries in war zones . These injuries arecharacterized by a soft, palp able swelling that may be cystic , in the context of anosseous defect of the skull. In the absence of a dur al tear there will be no po st-t raumat ic deficit of the skull, although cases have been described with the dur a intact. Afracture ass oc iated with hemorrhag ic contusi on of the unde rlying br ain, if accompanied by a dural tear, can give rise to a growing skull fracture. Afte r having reachedthe ir max imum extent, the se fractu res stop growing and rem ain sta ble until adolescence. A fracture with diastasis greate r than 4 mm can be con sidered at risk of developing into a growing skull fracture . The mo st common site for the se frac tures is theparietal reg ion . In the pre sence of an extensive and comminuted fracture, the re maybe parti al reabs orption of the bone fragments, leaving a large gap in the skull withirregul ar margins and scattered fragments in the dur a.
Sku ll fractu res can be ass oc iated with various int ra- and ext ra-axial intr acr ani allesion s. These include foci of intra pare nchyma l laceration s/contusion s, extra dura lhematomas (Fig. 6.5), acut e subdura l hematomas (Fig . 6.6) , mixed subdura lhematomas, paratentorial hematomas, subarachnoid hemorrhages, and diffu se axonal injury. The clinical presentation can be complicate d by the presenc e of intracran ialinvolvemen t syndromes , or vasc ular lesions or frac tures to the skull base, with possible cerebrospinal flu id leak age. Ce rebral contusion s occur at the site of impac t andon the opp osite side of the skull as a result of the contrecoup effec t cause d by deceleration of the brain parenchyma within the skull. They are characterized by hyperatte nuating foci at CT, indic ating the presence of punctate hemorrhages. In the hyperacute phases of the se foca l a ltera tions , they may be visualiz ed at magnetic resonance(MR) as areas of marked parenchymal hype rintensit y in images obt ained with T2*weighted gradient-echo (G E) acquis itions . Diffu se parenchymal edema is ass ocia ted,often alongsi de the fracture site.

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 101
Fig.6.6 CT in five-year-old child. Road accident trauma. a, b Axial scans with parenchyma window. Extensive and prevalently hyperattenuating layer with biconvex shape indicative of hyperacute epidural hematoma with left parietal-temporal location. The fracture line is visible in correspondence with the middle meningeal artery, the rupture of which is responsible for the abundant hematoma (arrows)
Epidural hematoma is charac terized by its biconvex shape, is extra-ax ial, andapp ear s prevalentl y hyperatt enu ating at CT in proximity to the impac t site (Fig. 6.6).It does not extend beyond the sutures, unl ess a fracture is present. In 90% of cases itarises from arterial rupture (most commonly the bran ches of the middl e men ingealart ery) in proximity to the fracture; more rarely, the origin is venous (10 %) due tofractures in proxim ity to the venous sinuses . It can reach signifi cant dimensions andcon stitutes a rea l emerge ncy in pediat ric pat ient s. Wh en its extens ion and depth arelim ited, a con servat ive approach can be adopted .
Acute subdura l hematoma appears as a crescent-s haped extra-ax ial collec tion inthe subdura l space (Fig . 6.6), extending over the cerebral convexity. It can cro ss thesutures in re lation to its extens ion between the arachnoid and the interna l layer s ofthe dur a mat er, and extend along the falx cerebri (Fig. 6.7) and the tentorium , in correspondenc e with the middl e, ante rior, and poster ior cranial fossae. The hyperacut eform (wi thin 6 hours from the trauma) can be visualized at CT as a mixed and inhomog enous hyperatt enu at ion , or app ear hypoattenuating ; afte r 6 hours, some 60% ofsubdural hematomas app ear hyperatt enu at ing (Fig. 6.8). ln the con text of clottingdisord ers or mark ed ane mia, hypo att enu at ion may persist. At MR the hyperacut ehematoma tend s to appear hyperint ense in T i-wcig htcd images to then becom e progressively mildl y hypo int ense. In T2-weighted images in the hyperacut e phase, ittend s to appear hyper intense and progress toward s hypo int ensity.
A head injury can be accompanie d by the presence of post-traumatic subarachnoid hemorrhage , due to the pre sence of blood in the cortica l sulci and cisterns. [f itaccompanies other brain injuries, the prognosis is unfavor able . lt can become compli cated with vasospasm, [ate infarction, and hydrocephalu s. At CT it appears as ahype rattenuating area within the cistern s prevalentl y in proximity to the brain contusion

6
102 C. Fonda etal.
Fig. 6.7 CT in an eight-year-old child. Serious road accident. a 3D volume rendering, and b axialscan with parenchyma window. Left parietal-occipital comminuted compound fracture extendinginferiorly in the retromastoid area. Extensive hyperattenuating laceration-contu sion in left parietallocation associated with abundant hypoattenuating perilesional edema and extensive interhemispheric subdural hematoma (arrows)
Fig. 6.8 Trauma from a non-accidental fall in a 26-day old infant. a Axial scan with parenchymawindow; right fronto-parietal depression fracture (ar row) appearing more marked at the apex withassociated hyperattenuating subdural hematoma and subgaleal hematoma. b 3D volume-rendering reconstruction. The broad fracture rim originating from the anterior fontanelle can be identified
or subdura l hematoma ; at MR it appears with signa l hyperintensity in FLAIRsequences, which ar e the mo st sens it ive in MR but le ss speci f ic th an CT.
Head inj ur ies can al so ca use m echanical injury to th e brain paren ch ym a known
as diffuse axonal inj ury (O AI) . Th e focal damage is th e result of a viole nt sw irl ing
motion of the cerebra l cortex wi th resp ect to th e deep br ain structures. This causes a
stre tching of th e axons and th e vessels accompanyi ng th em . Pun ctate hemorrhages

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 103
are thus form ed at the level of the corticom edullar y j unction (67%), the corpus callosum (20%), the deep gray matt er, and the mesencephalic structures . MR is thediagnostic ima ging modality of choice as it enables, in T2*-weighted GE images thatare sensi tive to magnetic susceptibi lity, amplif ication of the hypo intens ity of themicrohemorrhages so they thus become easi ly identifi able thanks to the presenc e ofhemo siderin depo sit s. DAI should be suspec ted in those cases of traum a when thereis a discrepanc y betw een the neurological presentation and the neuroradiologicalimagmg.
6.1.2Orbital and Nasoethmoid Fractures
The orbital cavities and the nasoethmoid components con stitut e important funct ionaland aesth etic units of the face . The severity of the fractures can vary from minor fractur es to complex fractures involving the orb ital-zygomatico-malar complexes . CT isthe preferr ed examination for the evaluati on of these fractur es. Zy gomatico-ma xi llary fractures are uncommon in children, due to the lack of pneum atizat ion in theparanasal sinuses, the elasticity of the bone, and the protective effect of the highercranial to facial skeleton size. Fractures of the orb ito- zygomati co-malar complexes inyoung children are frequently associated with head injuries (Fig . 6.9); comminutedfractures are uncommon.
Fig. 6.9 Fracture of the maxilla, the orbital floor, and the left zygomatic arch. a Axial CT, andh coronal MPR. The presence of blood-filled sinus and radio-opaque shadow over the nasal passages and the inferior orbital extraconal space can be identified (arrows)

104 C. Fonda et al.
6Orbital rim fractures are rare . When struc k abou t the supraorbita l rim , the pres
sure is transferred to the orbital roof, which can fracture. In chi ldren age d less than7 years, fracture of the orb ital roof is much more common. This is usually the resul tof a direct impact to the eye and is known as blow-out. Much mo re uncommon aremul tiple blow-in orbital fractures .
With growth, the frontal sinus becom es pneum atized and extends to the supraorb ital rim, thu s prevent ing direct transmission of the force of a blow to the orbitalroof (with a reduction in the frequency of its frac ture) . As a res ult, fractures of thefronta l sinus prevail.
Fractures of the orbital roof are cons idere d skull fractures . In general, they do notrequire treatm ent , unless there is an extensive breach in the bon e.
Fractures of the orbital floor are mor e uncommon than tho se of the orb ital roof:the incidence of these fractures parall els faci al development. Onl y children abo ve theage of 8 years have suff iciently develop ed paranasal sinuses to allow fracture of theorb ital floor and the parana sal sinuses . These fractures are the result of a direct blowto the inferior orbital rim: a depression of the orbit al soft tissue is generated toward sthe maxillar y sinus, and the rectal and inferi or oblique muscle may remai n entra ppedin the fracture line, causing ocul ar hypomotil ity (Fig. 6.10) . Fracture of the med ialwall of the orbit is the result of a direct blow to the orbi t. In younger children, it is afracture result ing from the earl ier development of the ethmoid sinuses . Subcut aneousemphysema and intraorbita l air are often pre sent (Fig . 6.11) . The need for surgicalrepair of orbital roo f fracture s is rare, whe reas the need for rep air in orbital floo rfractures is much more common. The vari ety of orbital fractures is best unde rstoodwith an ana lysis of the site, direction, and force of the blow.
Fig.6.10 l3-year-old girl. Direct coronalCT. Fracture of the left orbital floor.Entrapment of the inferior rectus musclein the fracture rim, accompanied by fattissue dehiscence corresponding with theunderlying maxillary sinus (arrow)

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 105
Fig.6.11 Fronto-facial trauma in a child. a Coronal MIP and b axial section with bone window.Fronto-nasal and right ethmoid fracture with extension to the medial orbital walls. The fractureline extends to the right zygoma (arrowheads). Air and blood in the orbit and bloodin the ethmoidmaxillary sinus are associated.
6.1.3Maxillofacial Fractures
Maxillofacial fractures are less common in children than they are in adults .Treatme nt need s to take ske letal growth into account, to avoid deformit ies with compromised fun ct ion and app earanc e. In 42-55% of cases, there are ass ociated skullfra ctures, and in 15-24%, there are fractures of the extre m ities (Tabl e 6.1). Thesefractures are most commonly pro cured from fall s (30-43%), dur ing play and sport(22-23%), and from car acc ident s.
Facial fractures in pedi atric pati ents acc ount for 5% of all craniofacial traumas,with mu ch lower frequ enc ies for children below the age of 5 years . The factors
responsibl e for the differenc e with res pec t to the adult population include the mu chhigh er craniofac ial rati o, the greater elas ticity of infant bon es, the great er thicknessof the soft tissue which produces a shie lding effec t, and the reduced or abse ntpneumatizat ion of the und erd evelop ed paranasal sinuses. Th e most common fracturesare nasal fra ctures (60%) , mandibul ar fractures (21 %), and maxill ar y fractures (6%),with ass ocia ted alveol ar fractures. The most common frac tures requiring hospital ization are tho se involvi ng the mandibl e, pa rt icul arl y the mandibular condy les(Fig. 6.12) . Fractures of the med ial maxillofac ial structures are rare, since these frac
tures require a high-energy impac t. Possible cau ses include majo r road accidents or
child abuse. The presenc e of tooth bud s in the mandibl e mak es the bon e mo re res istant to frac ture . A blow with the same force causes less-sign ificant lesions in a chi ld
than it does in an adul t.

6
106
Table 6.1 Pediatric fac ial trauma
I. Incid cn ceLess frcqucnt in children than in adults5-10% of facial fractures in children
asal and mandibular fractures arc thc most commonFalls. road acciden ts, sport. anima l attac ks. child abuse
hili of thc fractures from superior to inferior with increasi ng agc
2. Differences with respect I n adult shortcr timc availab le in thc manageme nt of an emergency
Facial hypodcvclopmcntlixed stage of dentition
Rapid healingommon association with intracranial and spinal injuriesurgical treatment a potentia l cause of deformity
C. Fonda etal.
3. A na to myraniofacial disproportion in favour of the former, olTering a protective clTect
Broad interpu pillary distance and nat na .al dorsumGreater amount of fibroadiposc tissueDevelopment of paranasal sinuses not yet present
tability facili tated by high tooth-to-bone ratioPediatric facial bone with thin cortex
Fig. 6.12 a 3D volume rendering of a fracture with disarticulation of the left mandible (arrow).b Coronal MPR of a bilateral fracture of the mandibular condyles with dislocation of the fractured fragments and on the right fracture of the articular cavity (arrows)
Around 80% of the growth of the max illofaci al stru ctures occurs in the first
2 yea rs of life , and the proce ss is almos t com plete at around 7 years of age, a lthough
it continues into the twent ies, with a craniofac ial rat io at birth of 8: I tha t at complete
maturation becomes 0.5: I , The skull act s as a kind of shi eld for the faci al bones.

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 107
Chi ldren tend to be more pron e to upp er-facial frac tures than lower-facial frac tures ,which are more typical in adults . In add it ion, orbital and skull fractures tend to bemore common. As the parana sal sinuses develop , lower maxillofacial fracturesbecom e more frequent.
The usc of CT has becom e commonplace in both adults and chi ldren. In the pastit was commonplace to perfo rm axial sca ns, and, where possibl e, coronal scans. Withthe advent of mul tislice CT and volumetri c acquisit ion s with isotropic resolution,togeth er with multi planar reconstruction s and the possibil ity of volumetric reconstruc tions, a detail ed ana lysis of the bony structures , the craniofacial soft ti ssue, andthe cerebral parenchyma is now possible, all the while abiding by the ALARA ("aslow as reasona bly achie vable" ) principle of minimum radia tion exposure . For fractur es of the nasal bon es, plain film radiography in the app ropriat e lateral and axialviews is suff icient, as it is for the evaluation of dent al and mandibular fractures .Recentl y, the sys tema tic use of ult rasound in the evaluation of nasal fractures wasproposed. Orthopantomography offers an adequate evaluation of the alveolar anddent al struc ture s and is oft en enough for the evaluation of mand ibul ar integrity. Forevaluation of the mandibular cond yles, the orb its, and the petrous part of the temporal bon e, multisliee CT appears to be the first-cho ice imag ing modality.
Nasa l fractures in pedi atric patients di ffer from tho se in adults due to the prevalent cartilaginou s component and the reduced prominence of the facial profile . Theseelements expl ain the reduced presence of nasal fractures in children , in whom theprevalent lesion tend s to be diffuse facial edem a. If a fracture does occur, it gene rallyinvolves the nasal septum, which can be fractured longitudinally in its anteri or portion , or dislocated - a common finding in neonatal fractures.
6.1.4Mandibular Fractures
Isolated dental or alveolar fractures arc common in child ren: the can ines or inc isor sare frequently avul sed due to their ant erior location. These fractures are considere d adental emergency. Deciduou s teeth do not need to be reimp lant ed, whereas permanent teeth must be rei mplanted, at best within an hou r.
Mandibular frac tures in chi ldren arc often solita ry, unli ke in adu lts where they arcoft en multiple. The condyles arc commonly the site of mand ibul ar fractures in children, given the ample medull ary core sur rounded by a thin cort ical rim. Condylarfractures account for around 3 I% of mandibular frac tures, and midline frac tures ofthe face around 17%, usuall y in older chi ldre n.
After the clini cal examination, radiological diagnosis is always requ ired and,based on standard radiography, pano ram ic radiography and CT.
There arc three types of condylar fractu res:int racapsul ar with fracture of the condylar he adhigh condylar fractures, located at the mandibular neck above the sigmoid notchinferior subcondyla r fractures, ass ocia ted with greenstic k fractures.

108 C. Fonda etal.
6Fractures of the first type are those that mor e readily produce growth deformities.
Mand ibul ar symphysea l and parasymph yseal fractures are not uncommon, with therisk of lesion s to the tooth buds. These frac tures are most frequently encountered inorthop edic or head injur ies. Fractures of the body and angl e of mandible tend to beincomplete in children.
6.1 .5Zygomatic and Maxillary Fractures
Zygomatic fractures are generally caused by a direct blow to the chee kbone .Pneumatizat ion of the maxillary sinus is required to allow dislocation of the bone,which explains why these fractures are uncommon in children. Zygomatic fracturesare associated with conj unctival hemorrhage, swelling of the soft t issues, depressionof the pro file of the cheek, and osseou s asy mmetry at palpation of the orbital rim.The fracture is best visualize d with a submenta l vertex rad iograph or with CT.
Le Fort fractures are characterized by mobility of the maxilla with respect to theskull base, and they present different symptoms and different degrees of severi ty.They all have a high-energy impact in common.
There are three types:Le Fort I fra ctures: these are the result of a blow to the inferior segment of themaxill a. The fracture line extends horizont ally across the maxillary sinuses.Orbital or nasal fractu res are not pre sent. The pterygoid plate and the vomer arefractured in the ir lower port ion .Le Fort II fra ctures : more extensive frac tures result ing from a violent impact tothe maxilla and nasal bones in a downw ard direct ion . The fracture run s inferiorly and later ally along the medi al wall and the floo r of the orbit, and continuesalong the later al wall s of the maxill ary sinuses. The pterygoid plate is fracturedat its middle third.Le Fort III fractures: the se correspond to a complete disassociation as a consequence of a high-energy blow to the nasal bone s. The fracture run s across thenasal bones, the late ral wall s of the orbit , and the zygomatic arch. The nasal septum and the pterygoid plate are fractured superiorly. The fracture may extend tothe skull base.
6.2The Vertebral Column
6.2 .1Epidemiology
Spinal trauma in pediatr ic pati ents can have catas trophic con sequ ences. Childrenhave different injury profil es to adults because of their different anatom y and physiolog y and exposure to different risk factors. Vertebral and spinal cord injuri es are

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 109
relatively uncommon in pediatri c patients. This is due to the greater mobility andelasticity of the spine during growth, and the lower body mass of children, incomplete ossification , and greater compressibility of the bone with respect to adults. InIn England, the frequency of spinal trauma, whether or not it is accompanied by vertebral dislocation , without spinal cord injur y, is reported as 2.7-3% of all cases ofped iatri c trauma. Trauma associated with spinal cord injury instead accounts for16-20% of all cases of spinal trauma, with a frequency of 0.6% of all pedi atric trauma cases. Spinal cord injur y without radiologica l abnormalit y (SCIWOR A) occurs in0.1-0.2% of all pedi atric traum a patients and in 4.5-6% of all pediatric spinal trauma patients, with a greater incidence in children below the age of 8 years. Multipletrauma and thoracic trauma increase the risk of both vertebral lesions and spinal cordinjur y. Road trauma accounts for 50% of spinal trauma in childr en, followed by fallsfrom a height. Skull fractures are the most commonly associated lesion s. Road accidents constitute the most frequent cause of spinal trauma , part icularly in infant s.Falls arc more frequent between 2 and 9 years of age, whereas sports-related traumais more frequently associated with the I0-14-year age group .
Head injur ies are associated in 37% of cases. The most frequently involved tractis the cervical spine (36-40%), followed by the thoracic spine (34%), and lumbarspine (29%). Mult iple contiguous lesions occur in 34% of cases, and non-con tiguou slesion s in 7% of cases . Younger children more frequently present a lesion of the superior cervical spine. The apex of the cer vical curve in flexion is located at a differentlevel in children (C2-C3) than in adult s (C4- C6). Isolat ed disc lesions, radicularlesions of the cauda equina, or frac tures of the transverse or spinous processes without further associations occur in 28.7% of cases. Thoracic lesion s are present in11.4% of patients with spinal trauma.
6.2.2Radiological Examination
Radiography of the spine maint ains its usefulness as a fir st-choice modalit y in theevaluation of spinal trauma, especi ally in the cervical spine. The guidelines of theAmerican Association of Neurologica l Surgeons, however, state that radiologicalexamin ation may not be necessary in children who are awake, able to speak, with noneurologi cal deficit or muscul ar stiffness in the neck , and no pain resulting from thetrauma , and who show no signs of intoxication . The application of the NEXUS studycriteria (Nation al Emergency X-ray Util ization Study) has reduced the need forimaging of the spine in 20% of the pediatric popul ation .
The lateral view is essential in evaluating spinal trauma and alone has a sensit ivity of 79%. In trauma of the cerv ical spine, the th icken ing of the paravertebral softtissue has a low predictive value in ped iatric patient s. The role of flexion and extension maneuvers is currently still controversial , and their application seems to be moreuseful in evaluation of the presence of ligamentous lesion s.
For reasons of radioprotection , CT should be limited solely to the tract suspectedof injury and should not be extended to the entire spine, as in adults. A useful technique

110 C. Fonda et al.
6in the study of the eervical spine is the use of bismuth shie lds to protect the thyroid,which allow s a 30% reduct ion in dose. The isotropic acqu isit ions of volumetric multis lice CT enable mul tiplanar rec onst ructions , bon e maximum -int ensity proj ection s(MIPs), and thr ee-d imension al volume tr ic reconstru ct ion s. With the exception ofsevere mult iple trauma, where CT is indicated as the fi rst-cho ice imaging mod ality,the use of the tec hnique in oth er cases should only follow clinic al-radiologic al evaluat ion .
MR is ind icated in all cas es of spina l cord inj ury. The relative frequ ency of SC IWORA in the pediatric population j ustifies its use in the abse nce of radiologicalabnor malities of the spine. MR has the task of identify ing edema tous and ligamentous lesion s, spinal cord contus ions /lacerations, intra- and extra-ax ial hemo rrh age,subluxa tions/dis locations of the vertebral bod ies, occult fractures , or concomitantdi sc lesion s. These alt erat ions are found in 3 I% of pat ient s with normal radiography.
6.2.3Evaluation of Spinal Trauma
One of the mo st important requirements in the evalu ation of pedi atric traum a, parti cularly when the cervical spine is involved, is to establ ish whether the lesion is stableor unstable . Stab ility depends not only on the integrity of the radiologic ally visibleosseou s struc tures , but also on the integrity of the posterior mu scular, ligamentous,and cap sular struc tures . The rad iological study of a cervical spine inj ury is no simple matt er - it requ ires a good deal of exper ience . Clinical evaluation is alwaysrequired, and may be able to rul e out the need for a radiological study.
Of all the radiological views of the spine , the lateral view is the most impo rtantfor eva luating its stability, particularly at the cervical spine. The radiological studydi ffers on the basis of the degr ee of pat ient compl ianc e, if con sciou s, drowsy, orunconscious. When possibl e, radiograph s in anter oposte rior and lateral and odontoidopen-mouth views should be performed, without moving the pati ent from the table.If the open-mouth view cannot be ach ieved (pat ient intubated) , then a CT studyshould be performed . In add it ion , in early infancy and in children up to 5 years ofage, achievi ng the open-mouth view for the study of the odontoid pro cess can provedi ff icu lt. Radiog raph s in flexi on can be useful for ruling out or demonstr at ing posteri or ligam entous and occult lesion s. CT is useful for the visua lizat ion of intraspinalbon e fragmen ts and for evaluat ing the stability of the osseou s structures . In the studyof the atl anto-occipital j oint, CT is useful in identi fying occult fractures of the occipital condy les . Many of the fractures of the odontoid process in ch ildren und er 2 yearsof age occur at the subdenta l synchondros is of the axis and can be visuali zed in thelateral view.
One element for evaluating trauma at the level of the dens of axis is measurementof the predental width . The variations in pedi atric pat ient s are mu ch more importantthan in adults . In ch ildren, a distance of 3-4 mm can be con side red normal. Thi s canchange significantly in posit ion s of flex ion and extension, with vari ations usually of2 mm. Th is fi nding should be evalu ated with care.

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 111
Spec ific lesion s of the ax ial ske leton during growth include lesion s of the cartilaginous margins of the vertebr al bod ies, and fractures at the level of the synchondrosis of the dens of the axis, atlanto-occipita l dislo cat ion typical among infants, andatl anto-axis rotational and tran slat ion al di slocat ion s. Fractures of the odonto idpro cess are ca use d by shear forces, which can occur in head-on car crashes at spee dsof at least 40 km/h, ass ociated with sudden decelerat ion.
In children , the verte bral bod ies have an oval appearance, and with growth theybecom e cubo id and then rectangular, and rare ly tak e on a flattene d appearance . Theneur al arches and spinous proc esses show mark ed variability. Aberrant bon e formations in the skull base and cervical spine are frequ ent , which, unl ike frac ture fragment s, oft en present rounded marg ins.
The vertebral column in children, pa rticularly the ce rv ical spine, present s a number of physiological characteri stic s that should be well known and should not be erroneou sly interpreted as signs of traum a with dislocation and /o r fracture (Table 6.2).The muscl es of the neck are less developed, and compliance in the bones is great er,which incre ases the frequency of traumatic lesion s of the soft tissue without assoc iated fractures . The anatom ical differenc es betw een the cerv ical spine of ch ildr en andadults are marked up to the age of 8 years, and they persist to a lesser extent unt ilaround 12 years of age. The development of the superior cer vic al spine is differentfrom that of the inferior cerv ica l spine. The atlas (C I) develops from three ossification centers (body and two neural arches). Abnormalities are pre sent when one ofthe se centers fail s to develop or there is fai led fusion . The poste rior arch fuses normally at the age of 3 years . The axis (C2) develops from fou r ossification centers(body, odontoid process, and two neural arches). These are present at birth and theyalso fuse at the age of 3 years. The body and the odontoid proce ss are joined by the dentocent ral synchondrosis, and the body and the neural arche s are joined by two neurocentral synchondroses . The inferior cervical spine develops from three ossificat ion
Table 6.2 Cervical spine: physiological findings in pediatric patients
Anterior arch of I elevated in hyperextension
Increased interspinous distance between I and 2 in flexion
Increased distance between I and the den ' of axis
Posterior vertebral body dislocation
2- 3 angle
Anterior dislocation of 2 on 3 (Hangman)
Physiological wedging of 3 and 4
Epiphyseal ring
Pseudo-widening of the spinal canal
Pscudofractures due to erroneous placement of the superior cervica l spine
Increase in the distance between lateral masses of I and the dens of the axis ininfants <2 years

112 C. Fonda et al.
6centers, one central vertebra l, and two neural arches, also joined by two neurocentr alsynchondroses which fuse between the third and sixth year. The cervical and thoracicvertebrae also have f ive secondary ossification cente rs (one for the spinous process,two for the transve rse processes, and two ring apophyses).
6.2.4Pathophysiology
The und erlying mechan isms of spinal trauma are flexion , lateral flexion , extensi on,rotati on, axial compressi on (Fig. 6.13) , and tear ing. Flexi on induces spinal lesionsmore frequently than extensi on (Fig. 6. 14). The anatomical characterist ics of the various segments influence the onset of various types of lesion s: the hori zontal orient ation of the facet joints of the ce rvica l spine favor the dislocation and rupture of theinte rve rtebral disc without fracture. In cont rast, in the lumbar spine, the prevalentl yvertical direct ion of the facets induces fra ctur es of the facet joint s themselves andlinear fractures of the vertebral bodies. In the presence of seve re trauma, a dissolution of the vertebral body may ensue (Fig. 6. 15). In cases of child abuse, compression fractu res ass ocia ted with hype rflex ion may be silent. If the verteb ral compres-
a
c
Fig. 6.13 Forces involved in the trauma mechanisms of the vertebral column. a Flexion (+%);b extension; c anterior (+%) and posterior rotation; d axial compression

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 113
, tear drop
, ring-shapeepiphysis
' compression
a
, avulsion
, distraction
b
Fig. 6.14Trauma mechanism. a Lesion resulting from flexion and anterior compression trauma ;b lesion resulting from trauma mechani sm in extension
Fig.6.1S Non-spinal cord injury in a 12-year-old girl obtained during karate training. Onset ofpain.CT study performed 2 months after the trauma. a Sagittal MPR; h Ti -weighted sagittal MR; c T2
weighted sagittal MR. Dissolution of T8 vertebral body and alteration of the posterior wall(arrow) . The trauma has caused collapse of the vertebra affected by Langerhans histiocytosis.Note the presence of pathological epidural tissue at the level of the posterior wall of the collapsedvertebra
sion is very marked, the differential diagno sis may includ e those alterations result ingfrom mueopol ysaecharido sis, Langerhans cell histioc ytosis, or other condition s thatfavor vertebral fractures. Lateral dislocation of the vertebral bod ies is usually associat ed with severe fractures . Radiological findings includ e alteration s of the interver tebral space width , an abno rmal configuration of the facet jo ints, a widening ofLuschk a's joints, a widening of the interspinous distance, a lateral shift of the spinous processes, and a widening of the interpedicular space .
Establishing the presence of instability of the cervic al spine is based on the identification of specific radiological signs (Table 6.3) , some of which are easily recognizable , while for others, conventional radiology may not be enough and CT can playan important role .

114 C. Fondaetal.
6Table 6.3 Signs of cervical instability
Anterior. posterior or lateral dislocation of the vertebral body
Widening or narrowing of the intervertebral space
Widened narrowed or dislocated facet joints
Localized widening of the Luschka joints
Bilateral or unilateral facet joint block
cparation of the . pinous processes. sometimes associated with avulsion fracture
Avulsion fracture in flexion or extension
ompression fracture of the anterior border with posterior dislocation of the vertebralbody involved
Widening of the prcdcntal space: external dislocation of the lateral masses of(Jefferson fracture)
nterior dislocation of one of the lateral masses of I (rotatory di.location)
Fracture of the den . with or without di location
Blow-out fracture of the vertebral body
6.2.5SuperiorCervica l Spine Injuries
The spine of neonates and childr en is part icularly vuln erable to distraet ion injuriesseeondary to ligamentous lesions of the sup erior eervical spin e. In child ren below9 years of age, 78% of cerv ical spine inj uries are located in the superior tract , and 68%are cha ract erized by subluxation without fracture or SCIWORA. Atlanto-occ ipitaldisloc ation is mo st common between 5 and 9 years of age . Spinal distract ions/d isjunction s are rare in children and often fatal due to concomitant brain stem inj uries .Survi vors of such lesion s present severe tetrapl eg ia. There are certain pathologicalconditions that favor these lesions , including Klippel-Feil syndrome, Gri sel syndrome, and Down syndrome.
Radiogr aphy of atlanto-occipital disjunctions/disassociations , done in the lateralview, should evaluate the BC:OA ratio by measur ing the basion and the posterior archof C I (BC) divided by the distanc e between the opisth ion and the anterior arch of C I(OA). A ratio greater than 1.0 is considered diagno stic (normal value 0.77). CT is considered the imaging modal ity of choice. MR provides an evaluation of the soft tissue andligaments, and in particular can evaluate the presence of a tectorial membrane lesion .
6.2.6Occipito-atlanto-axial Instability
The atlanto -occipital joints enable the maneuvers of extension and flexion and thecon sequ ent translation of C I and C2. Movement s greater than 5 mm and 3 mm in

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 115
Fig.6.16Sport injury in 14-year-oldchild. Axial CT scan. Jeffersonfracture. Fracture of the left anterior arch of CI (long arrow), anterior to the transverse process,and disjunction of the bone fragments. Concomitant median fracture of the posterior arch of CI(short arrow). Lateraldislocationof the dens of axis due to therotation of C I (round arrow) .Highly unstable lesion
ch ildren below and above 8 years of age, respectively, indicate the pre sence ofat lanto-axial instability and lig amentous laxity, and/or a tear of the tran sve rse ligament. Radiograph s in flex ion can be useful if done with care .
Eva luating the pre sence of a rotatory subluxa tion can be done with dynam ic CTto veri fy the movement of the anteri or arch of atlas with respect to the dens of axis,with scans performed in any posit ion and subse quent rotat ion from both sides of thehead on the neck.
Jefferson fractures of C I, the res ult of an excessive load from above or a contrecoup of the head secondary to a dive, are rare in pediat ric age. Unlike in adults ,where the fracture tends to be ant erior and poster ior, in children it is more commonlya single fracture with pivot on the synchondrosis (Fig. 6. 16).
6.2.7Odontoid Process Fractures
Frac tures of the dens in ac ute trauma are less common in children than in adults. Theanterior angle of the odontoid pro cess is highl y suggestive of a fracture in an ac utetrauma. MR is mor e sensi tive in iden tifyi ng bone marrow edema acc ompany ing thefrac ture line, particul arl y at the level of the dentocentral synchondrosis . (Fig. 6.17).CT provid es a detail ed evaluat ion of the type of fracture and offers an evaluation ofhow chronic the condit ion is. Ande rson and D' Alonzo have classified odon toid fractur es into three types:
type I: avulsion fracture secondary to a tear of the alar ligament. The presenc e ofan os odontoideum can make the diagnosis diff iculttype II: transver se frac ture extending to the odontoid base, oft en with a disjunct ion (Fig. 6.18). Sag ittal and corona l reconstruct ion can be useful , given that the
fracture may be missed in the axial plan etype Ill: the fracture exten ds to the bod y of C2 and is relati vely frequent in children below the age of 7 years . Oft en the fracture crosses the dentocent ral synchondrosis. The synchondrosis stays open unt il lat e infancy.

116 C. Fonda et al.
6
Fig. 6.17 Median (a) and paramedian (b) sagittal MPR. At the level ofC2 the normal appearanceof the synchondrosis between the dens and the body of the axis can be identified, which shouldnot be confused with a fracture line. Pseudo-anterolisthesis of C2 on C3, finding within normallimits. Normal atlanto-occipital relations
Fig.6.18 Non-spinal cord injury resulting from a road accident with hyperflexion of the head on theneck in a 5-year-old child. a Radiograph in lateral view. b Median sagittal MPR. c Axial scan atthe level of the dens of the axis. An increase in the distance between the posterior profile of theanterior arch of Cl (arrow in a and double-headed arrow in c) and the anterior cortical profile ofthe dens ofaxis are visible, with integrity ofthe anterior columns ofC2, due to rupture ofthe transverse ligament of the odontoid process. Increase in the distance between the posterior arch ofC Iand the spinous process of C2 (double-headed arrow in a) due to interruption ofthe posterior aponeurotic and ligamentous complex subsequent to hyperflexion. Reduction in the transverse dimensions of the spinal canal with sufficient dimensions to not exert compression on the spinal cord.Synchondrosis between the dens and the body of the axis is not yet completely fused (arrows in aand b); not signs offractures at this level. Highly unstable lesion which requires fixation

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 117
CT is diagno stic in diff icult cases. Most of these lesions are the result of a posterior dislocation of the dens and can be highl y unstabl e and cause spinal cord compression . Widening of the synchondrosis and its anteri or angle are indicat ive of alesion .
6.2.8Extension Fractures of the Atlas and Axis
The most common is fracture of the posterior arch of C I , follow ed by frac tures of thedens of the axi s and the classical Hangm an 's fractu re of C2.
Fractures of the poster ior arch of C I may be unilateral or bilateral , and can beisolated or associated with other fractures. They can produce stenosis -inducedlesion s as a result of the angle of the dens. CT is extreme ly useful in their evaluation.
Hangm an 's fractures are characterized by bilateral frac tures cro ssing the neuralarches and the ver tebra l peduncles, together with anterior ligam entou s disruption.Unilateral fracture of the arch can be mor e difficult to diagno se since there is usuallyno associated instability of the posterior cervical spine . A Hangm an 's fracture insma ller children may be silent.
6.2.9Flexion Trauma of the Inferior Cervical Spine
Thi s trauma cau ses lesion s of the vert ebral bod ies and their respectiv e ligaments, thefacet joints and their respective ligaments, and the spinous proc esses and theirrespectiv e ligam ents. These lesion s are more common in older child ren. The compression forces are located anteriorl y and the distraction forces posteriorl y. In manycases, a triangular avulsion lesion is present , most commonly at the level of the anterio r-posterior edge of the avulsed vertebral body. Poster ior distrac tion forces, associated with hyperfl exion-induced lesion s, produce ligamentous lesion s across the facetjoint s and between the neural arches and the spinous processes. The dislocation ofthe vertebral body can be minim al, and dislocation of around 3 mm can be considered abnormal. On the other hand, an anteri or angle greater than 12-15° should alsobe considered abnormal. At the level of the neural arch and the spinous processes, theligamentous lesi on produces a separation of the spinous proc esses involved and awidening of the inters pinous distanc e (Fig. 6. 19), and, more rarely, avulsion fracturesof the posterior elements. If there is an altera tion of the anteropo sterior long itud inalligament s, the ligam ents of the facet joints, the neural arch , and the spinous proc esses, then the result will be instabil ity (Figs. 6.20 and 6.21). MR is part icularl y usefulin identifying osteo-Iigamentous alterations .

118 C. Fonda etal.
6
Fig.6.19Trauma mechanism in flexion of the cervical spine
Fig. 6.20 Complete disjunction between C5 and C6 (double arrows) in a 6-year-old child, withresulting acute tetraplegia, subsequent to a road accident. a Pre-fixation anteroposterior view, andb post-f ixation lateral view radiographs. Reduced-height of C6 (arrow)

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 119
Fig.6.21 Sagittal MR of the same patient as Fig. 6.20. The vertebral disjunction between C5 andC6 can be identified (arrows). Extensive posterior fascial and ligamentous lesion (doublearrows). Extensive spinal cord injury with focus of hemorrhagic laceration-contusion, andmarked bone marrow edema extending for around seven segments (red arrows)
6.2.10Extension Trauma
In extension fractures, the tear involves the anterosuperior edge. If, instead, the re isevidence of a teardrop fracture, it is correct to suspect an unstable lesion induced byhyperflexion. In ch ildren , the equivalent of the fracture con sists of slipping of the normal vertebral epiphyseal ring. Extension lesion s are characterized by the presence ofposterior compression forces and anterior distraction force s, with fractu res prevalentlyinvolving the facet joints, the columns, and the posterior elements . Widening of theinterverteb ral space occurs as a result of rupture of the anterior longitudinal ligamentinduced by extension, with involvement of the super ior edge of the vertebral body.The prevertebral tissue swells only in the presence of rupture of the anterior longitudinal ligamen t. If the frac tures of the posterior arch are unilate ral , the fracture is notparticularly unstable ; in cont rast, it will be if the fractures are bilater al.
6.2.11Fractures of the Thoracolumbar Spine
Frac ture -dis locations of the thoracolumbar spine are usually cause d by high- energytrauma. They are uncommon (2.5 % of al1 spina l injuries) and invol ve multipl e verte brae in 50- 70% of cases . In trauma pati ent s aged over 8 years, the rad iological presentation is simi lar to that in adults, whereas below 8 yea rs of age, the finding of

120 C. Fonda etal.
6SC[WORA is not uncommon even in this tract. They are frequently caused by a fallfrom a height, for example from a trampoline (Fig. 6.22). An angle of less than [0 °of the spinal axis simply requires bed rest , whereas a greater angle requires immobilization in extension for 2 months. A vertebral compression greater than 50%requires surgical stabilization. The fractures can involve each of the three columnsdescribed by Denis. Instability also needs to be evaluated at these levels (Fig. 6.23).The finding of a fracture is more common than a dislocation of the vertebral bodiesor the presence of a compromised disc, since the ligamentous structures offer greaterresistance than bone. In seat-belt injuries (most commonly at L I-L3), an anteriorcompression of the vertebra can be observed, tog ether with associated lesions ofinternal organs. Radiological study, done with CT, should identify the presence offree bone fragments dispersed in the spinal canal, and the presence of fractures if theneural arch and the facet join block.
Vertebral compression is the most common finding. The presenc e of a lesion atthe level of the thoracolumbar joint in patients aged less than 2 years suggests thepresence of a non-accidental injury. In cases of minor compression, a lesion can beidentified at the edges of the vertebral body, which appear squashed, and the vertebral end plates have a concave appearance . [n cases of intermediate compression, theanterior wedge shape of the vertebral body or loss of the concavity of the posteriorwall can be identified. In cases of severe compression, collapse of the vertebral bodyis evident, appearing flattened with an alteration of the posterior wall and possiblespinal-cord compression.
Growth plate fractures (Salter-Harris I or 11), with or without associated protrusion of the intervertebral disc , are encountered in adolescent patients. Avulsions withfragments of lumbar processes and fractures of the transverse processes may be
Fig. 6.22 CT of the thoracolumbarspinein multiple trauma with no spinal cordinvolvement in l2-year-old child.a Bone MIP. b CoronalMPR. Fractureof L2 due to hyperflexion and verticalcompression Depression of the vertebral plate with anterior wedge andblow-out fragments in lateroanteriorlocation (arrows). There are no signsof alteration of the posterior arch.Stable fracture

6 Imaging ofRegional Injuries:The Axial Skeleton- the Skull,Vertebral Column,and ThoracicCage 121
Fig. 6.23 Fracture in hyperflexion with fulcrum on L2. a-c Sagittal MPR. Posterior instability.Small antcrosuperior displacement of the vertebral border (arrowhead in b), transverse fracturewith diastasis of the neural arch and vertebral peduncles with posterior opening due to avulsionwith laceration of the corresponding soft tissue (small arrow in h and arrowhead in c). Wideningof the Ll-L2 posterior intervetebral space (double arrow in a). Transverse fracture of the uppervertebral plate and the posterior apophyseal complex (double arrow in b)
found . Even in minor traum at ic lesions, there may be severe lesions of the internalorgan s (60 % involving the kidneys, 35% the liver) .
A specia l type of lesion is the Cha nce fra cture, which is cha racterized by a bil ateral di slocat ion of the fac et joint s, fracture of the ver tebra l peduncles or the laminaeof the neural arc h, and extension of the fracture line a long the vertebral body(Fig . 6.23) . These lesion s, which may be di ff icult to diagnose both with conventional radiography and CT, are not uncommon in sea t-belt injuries. Cases of traum aticspondylos is are rare .
6.3The Thoracic Cage
6.3.1Chest Wall Injury
Ches t wall inj uries are particularly important since they usuall y occur as a result oftrauma that ca uses severe associat ed lesions. Given that the ribcage in children ismo re elas tic than in adul ts, less ene rgy from a blow is absorbed by the ches t wall , andproportionally mo re energy is tran sferred to the intrathoracic organ s (which ca ncause, for example, pulmonary contusion s). Int ernal lesion s are oft en present in the
ab sence of vis ible damage to the chest wall itse lf. A rib fracture sec on dary to close dthoracic trauma is an important ind icator of the seri ousness of the trauma itsel f. Thegreater the number of fractured ribs, the mo re seri ous the complicat ions are.
The mo st common causes of chest wall injuries are road accidents, although the selesions are frequently pre sent in victims of child abuse. Mortality is usually the resultof ass ociated traum a, particularly he ad injuries. In the vari ous studies published in

122 C. Fonda etal.
6the literature, the mortal ity resulting from chest wall inj uries alone varies between4% and 14%, whereas in cases with associated head inj ur ies the percent age rises to28-37%. Chest wall inj uries in children differ from tho se in adults, given the great erflexibility of the structures of the ribcage .
Flail chest, which is the result of multiple fractures of a rib producing a free segment , is rare in children. An early diagnosis is requ ired to avoid consequent pulmonary compl ications. The proportion of patients treated con servatively is around97% in rib fractures.
Rib fractures are associated, in decreasing order, with injuries to the extremities,skull , spleen, and liver, sternal and scapular fractures, rupture of the thoracic aorta,and, rarel y card iac lesion s.
Stern al fractures are rare in children and can be the result of direct or indirecttrauma. They generally arise as the result of clos ed trauma of not excessive kineticenergy. Special attention needs to be paid, in cases of high-impact sternal fractures,to concomitant spina l inj uries . Anterior cortical fractures are common, whereas fractures of the manubriosternal joint are rare (Fig . 6.24) . Sternal fractures are notuncommonly associated with spinal inj ur ies in hyperflexion of the thoracic spine ,with forc e lines being transferred to the sternum by the clavicl es as a result of muscle action in hyperextension of the chest.
In healthy children, fractured ribs are highly speci fic for child abuse. Acute ribfractures can be difficult to identify at chest radiography. Bone scintigraphy or CTmay be needed to evaluate acute-phase fractures . However, the se techniques are notindicated unless it is necessary to identify associated lesions of the pulmonaryparenchyma or vertebral column. Most fractures can be identified two weeks afterthe trauma thanks to the form ation of fibroc artil age callus. In the first 3 years of life ,rib fractures constitute a positive predictive value for child abuse. Fractures resulting
Fig. 6.24 Multiple traumafollowing a roadaccidentina 14-year-oldchild. a Lateral view radiograph,and h sagittal CT MPR. Fracture-luxation of the sternal manubrium is visible. No pulmonarylesions belowthe fracture can be identified. No clavicularlesions

6 Imaging ofRegional Injuries:The Axial Skeleton - the Skull, Vertebral Column, and Thoracic Cage 123
from abuse are most commonly located at the level of the posterior arches, in prox
imity to the transverse processes. In infants in their first year of life, around 80% of
cases are the result of child abuse, while the remaining 20% are due to direct trauma
or metabolic disease . These fractures are very rare in neonates. They may also be the
result of resuscitation maneuvers (0 .6%). Radiographically, they are recognizable as
lucent lines at the level of the costal arch; oblique views are useful for their identifi
cation .
Suggested Readings
Anderson LD, D'Alonzo RT (1974) Fractures of the odontoid process ofthe axis. J Bone Joint Surg56A:1663-1674
Chapman VM, Fenton LZ, Gao D, Strain JD (2009) Facial fractures in children : unique patterns ofinjury observed by Computed Tomography. J Comput Assist Tomogr 33(1):70-72
de P Djientcheu V,Njamnshi AK, Ongolo-Zogo Pet al (2006) Growing skull fractures. Childs NervSyst 22(7) :721
Ersoy G, Karciog?lu 0 , Enginbas , Y et al (1995) Are cervical spine X-rays mandatory in all blunttrauma patients? Eur J Emerg Med 2(4):191-195
Grotboom MJ, Governer S (1993) Acute injuries of upper dorsal spine. Injury 24(6):389-392Leone A, Martino F (eds) (2008) Imaging del rachide. Springer-Verlag Italia, MilanoLosee JE, Afifi A, Jiang S et al (2008) Pediatric orbital fractures : classification, management, and
early follow-up. Plast Recostr Surg 122(3):886-897Martin BW, E Dykes, Lecky FE (2004) Patterns and risks in spinal trauma, archives of disease. Child
hood 89:860-865Mehta S (2007) Neuroimaging for paediatric minor closed head injuries. Paediatr Child Health
12(6):482-484Moore MA, Wallace EC, Westra SJ (2009) The imaging of paediatric thoracic trauma . Pediatr Ra
dioI39(5):485-496Quayle KS, Jaffe DM, Kuppermann N et al (1997) Diagnostic testing for acute head injury in chil
dren : when are head Computed Tomography and skull radiographs indicated? Pediatrics99(5) :EII
Shane SA, Fuchs SM (1997) Skull fractures in infants and predictors ofassociated intracranial injury. Pediatr Emerg Care 13(3):198-203
Struffert T, Grunwald I, Reith W (2003) Craniocerebral trauma in childhood . Radiologe 43( II ):967976
Thornton A, Gyll C (eds) (1999) Spine in children 's fractures . WB Saunders, Harcourt PublishersLimited UK pp 90-105
Tung GA, Kumar M, Richardson RC et al (2006) Comparison ofaccidental and non accidental traumatic head injury in children on noncontrast Computed Tomography. Pediatrics 118(2):626233
Tiiredi S, Hasanbasoglu A, Gunduz A, Yandi M (2008) Clinical decision instruments for CT scanin minor head trauma . J Emerg Med 34(3) :253-259


7.1The Shoulder and Arm
In children, the clavicle (coll arbone) is one of the bone s that is most susceptible tofracture . In most cases, immobilization is the preferr ed choice of treatment; only inexceptional cases does surgery prove necessar y, and thi s is con fined to cases wherethere is a simple frac ture with exposure of the bone. Fractures in neonates may becaused by natural delivery, especi ally in macro somi c children weighing more than4 kg, or by comp ression traum a of the shoulders in the course of dystocic delivery.In old er childr en, the traum a most commonly responsible for fracture is a fall on theshoulder with direct trauma, or with an out stretch ed arm.
Most fractures involve the middl e third of the clavicular diaphysis, making A-PX-ray proj ection suff icient for diagnosis. However, in neonates and very sma ll children, incompl ete lesion s with a thin frac ture rima and normal bone alignment arecommon, and are sometimes mistak en dur ing X-ray diagno sis due to their small sizeor to their position , which is not tang ent ial to the radiograph ic beam. In these cases,where the symptoms (tum efact ion , immobility, pa in on mob il izat ion) do not corre spond to the negative findings from X-ray, ult rasound may identi fy sma ll breakswithout the need to resort to additiona l X-ray projection s (Fig. 7.1a, b). In thesecases, the fracture can then be visualized by X-ray through furth er check-ups thatcan identify the presence of a reparative callu s (Fig . 7.1c, d).
In neonates, discovery of a fracture of the acromial extremity of the clavicle raises suspici ons of non-accidental lesions caused by abuse. In older children and adolescents, fractures are more frequentl y simple fractures, with lowering of the shoulder on the affected side, loco-regional tumefactio n, and pain; treatm ent is based onimmobilization through "fi gure-of-e ight" bandage.
D. Barbuti (C8J)Department of Diagnostic Imaging, Pediatric Hospital "Bambino Gesu", Rome, Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20 I I
125

126 D. Barbuti etal.
7
Fig.7.1 Fracture of the clavicle. 3-year-old girl with a suspected fracture of the clavicle which didnot emerge in X-ray (a), while ultrasound (b) reveals a slight interruption of the bone cortex atthe level of middle-outerthird. X-ray of the clavicle of an II-month-old baby boy in which thereis clear angulation of the clavicle without clear visibilityofthe fracture rima (c), whileat a checkup performed after 20 days (d), the fracture rima and the osseous callus for osteoreparative phenomena can be clearly identified
Dislocation of the clavicle is rare in pediatric age. Fractures of the lateral portionof the clavicle are more frequently observed in connection with the acromioclaviculararticulation, while fractures at the level of the sternoclavicular articulation areextremely rare and involve the physis (type I or 1\ Salter-Harris fractures). Avulsion
of the middle physis with posterior dislocation of the fragment may cause compression of the trachea, the subclavian vessels, or the brachial plexus. Assessment of thistype of lesion can be made by computed tomography (CT) blurring, which makes it
possible to record the position of the dislocated fragment from behind and to identify further complications that provide useful indications for surgery.
Scapular fractures arc rare and generally caused by high-energy traumas; they arcoften associated with traumatic lesions of adjoining skeletal structures (clavicle, ribs,dorsal vertebrae, humerus) or with pulmonary lesions (lacerations/contusions, aeropleura). Traumatic lesions most frequently involve the coracoid (Fig. 7.2) , the
acromion, and the glenoid, and may be associated with lesions of the acromioclaviculararticulation and glenohumeral articulation. The numerous nuclei of ossification ofthe scapula may resemble fracture lesions. Fractures of the neck and body of thescapula are rarer in pediatric age compared to adults and arc generally caused by adirect trauma of significant extent (Fig. 7.3) . A-P and L-L X-ray projections of the
scapula are generally diagnostic; CT can provides further information, especially forfractures of the neck of the scapula, highlighting the extension of the rim fracture tothe glenoid.
Traumatic lesions of the proximal extremity of the humerus are more frequentlyrepresented by epiphyseal separation and by fractures of the proximal metaphysis of

7 The Upper Limbs 127
Fig.7.2a, b Avulsion of the coracoid. The comparative X-ray examination of the shoulders in axialprojection shows a detachment of the left coracoid (arrow in h)
~ ,~
-,, . o4 I "- A,
~
/ -,Fig. 7.3 Fracture of scapula. CT axial scan which shows a slight fracture rima of the body of thescapula (arrow) in a 16-year-old polytraumatized patient
the humerus; the latter are more frequent in stage I and II childhood (Fig. 7.4) . X-ray
assessment of this type of lesion must be performed in the transthoracic frontal and
lateral projection, in order to check the alignment of the bones in orthogonal planes.The presence of dislocation of the humeral head provides indications for surgery; in
these cases, it is advisable to perform a CT examination, complete with 3D recon
structions, in order to assess the position of the bones more precisely (Fig. 7.5) .

128 D. Barbuti etal.
7
Fig. 7.4 Fracture of the proximal metaphysis of the humerus. a A-P X-ray of a seven-year-oldpatient with a proximal metaphysis of the humerus with interlocked fragments and minimal varusangulation. b, c A-P and axial projection of an eight-year-old patient with a compound fracture ofthe surgical neck of the humerus
Fig.7.5Fracture-dislocation of the humeral head. a A-P projection (scout-view) shows the presenceof the fracture-dislocation of the humeral head (IO-year-old child). b CT, complete with 3Dreconstructions, shows with more precision the position of the bone heads and the type of dislocation for surgical purposes. c In the X-ray check-up, in plastered immobilization after surgicalsynthesis with two metal wires, good alignment of the bone heads and a reductionof the dislocationcan be observed
Factures of the proximal epiphyseal nuel eus of the humerus are more rarely
ob ser ved . Traumatic detachment/separation of the proximal epiphysis of the
humerus, almost exclusively of types I and 1\ according to the Salter-Harri s cl assi fi
cation, can sometimes be mo re difficult to detect using X-ray, especially in case s
where the epiphysis is still completely cartilaginous; when the di agnosis is uncertain
(p articularly in case s of Salter-Harris type I sepa ration, without bre aks, caused either
by acute lesions or chronic trauma as in the case of " litt le league shoulder" , the lat
ter be ing particularly common between the age of 12 and 15 years), ult rasound, and
particularly magnetic resonance imaging (MRI), can be helpful in making the diag
no si s (Fig. 7.6) . Pro xim al epiphyse al sep ar ations of the humerus are more frequent
in adolesce nts, generall y du e to falls on the abducted limb or as a re sult of directtrauma. Compl ications are rar e, and it is more common to ob serve sho rtening of th e

7 The UpperLimbs 129
Fig. 7.6 Proximal epiphyseal separation ofthe humeru s ("littleleague shoulder"). A-Pprojections and gradient-echo coronal MRIscans, performed forcomparative purposeson a 12-year-old boy.a, b Definite lesions ofthe physis cannot berecognized with X-ray.c, d MRI shows awidening of the leftproximal physis on theinternal side (arrow ) inrelation to a type ISalter-Harris fracture
humerus as a result of damage to the growth cartil age . Dysmet rias can be a signifi cant and incapac itat ing con sequence of lesions of the physis, and the ir extent is proportional to the growth potential of the carti lage concerned. In the upper limb , theproximal physis of the humerus cont ributes about 80% to the growth of thi s longbone while the distal physis contr ibutes only about 20% by its distal physis, wh ich iswhy lesion s of the prox imal physis are more frequently ass ociated with dysmet rias,including tho se of a serious natu re . In the forearm , mo st of the bone growth involvesblurring of the distal physis (about 75% for the radius and 80% for the uln a).
In the case of fractures of the proximal humerus with a case hi stor y of a slighttraum a, it is also nece ssary to exclude the pre sence of pathological fractures since thehumerus is the mo st frequent site of benign bone lesions, part icul arly solitary bon ecysts.
Traumatic dislocat ions of the glenohumeral articulation are generally caused byindirect traum as; in more than 90% of cases, thi s invol ves anterior disloc ations,while poste rio r and inferio r dislocations are less frequent. In the case of anterior dislocation, the pat ient keep s the limb abducted and rotated inwards . Although the diagnosis of dislocation is cl inical, an X-ray examination is important for identifying thepre sence of possible fractures ass ocia ted with the glenoid or hume ral head(Hill-Sachs lesion) (Fig. 7.7), and to check for correct articular relationship s following the reduc tion man euver (Fig . 7.8) . As in adults, MRI is bett er for record ing bonelesions and lesion s of the circumfe rentia l cartilage . One of the possible complications of shoulder dislocation is lesion of the ascellar nerve, osteonecrosis of thehum eral head, and previou s shoulder dislocations.

130 D. Barbuti etal.
7
Fig. 7.7 Hill-Sachs fracture . Gradient-echo coronal MRI scan (a) and axial Tr-weighted scan (b),which show the presence of an impact lesion (arrows) of the humeral epiphysis in relation to aHill-Sachs fracture in a previous dislocation of the shoulder
Fig.7.8 Scapular-hume ral dislocation in a 15-year-old patient. A-P projection (a) and transthoracicprojection (b) which show the presence of an inferior dislocation of the humeral head. eX-raycheck -up after reduction shows restoration of the joint relations and also shows the presence of aHill-Sachs impact lesion
Fractures of the humeral di aphysi s are more commonly ob served in neonates fol
lowing trauma during delivery and req u ir e clinical assessm ent to exclude a le sion of
the brachial plexus . In older children, an attendant tr aumatic le sion of the radial
n erve is quit e fr equent in th e long course of th e humeral groove.

7 The UpperLimbs
7.2The Elbow and Forearm
131
The elbow of a chi ld is a highly complex ana tomica l reg ion linked to the presence ofnum erous growth nuclei which appear at different ages, with an interval of about2 years between eac h one, although there is wid espr ead variabili ty. Girls also displayearlier appearance of ossif ication nuc lei by about I or 2 years comp ared to boys.The acronym CR[TOE and identifi cat ion of this with the "rule of odd numb ers"([ ,3,5, 7, 9, I l ) represent useful methods for memorizing the chronological orderof appearance of the different secondary nuclei of ossif ication and, for each one , theaverage age of appea rance : capitellum (humeral cond yle - [2 months), radiu s (radialhead - 3 years), internal (internal epicondyle - 5 years), trochlea (7 years), olec ranon(9 years), extern al (external ep icondyle - [I years) (Fig. 7.9).
a b
Fig.7.9 Diagram (a, b) andX-rays (c, d) which illustrate the nuclei of ossification of the elbow of a 10year-old girl

132 D.Barbuti etal.
7Due to the difficult ies linked to the radiological assessme nt of traumatic lesions of
the elbow, oth er lin es of referen ce, or indirect radiographic lines, have been prop osed,
which can help the radiologist to interpre t X-ray images. Th e anterior humer al line is
a straight line that is tangential to the anter ior cortical surface of the humerus in thelat eral proj ection and which, in normal conditions , inte rsects th e rad ial ca pite llum at
the level of the middle th ird ; in th e case of suprac ondy lar frac ture with po ster io r dis
locat ion, th is line cro sses the anterior thi rd of the capitellum or is position ed ant eriorlyto it (Fi g . 7.10) . In orthogonal proj ect ions, the rad io- condylar line is a line tha t pa ss
es throug h the axis of the distal diaphysis, wh ich should intersect the humeralcondy le; if th is is not the case , th is is a sign of d islocation of the radia l epiphys is (F ig .
7.1Ob). A "teardrop" is represent ed, in the lat eral proj ect ion of the elbow, by the cor
tical profile insi de the coronoid fossa (ventrall y) or the olecran ic fo ssa (dorsall y) and
by the humeral condyle which represents the inferi or por tion ; if there is a suprac ondy
lar frac ture of the humerus, thi s leads to deformation of the ima ge of the "teardr op" .
Obviou sly, the reliability of indirec t radiological signs depend s entirely on the techn ical
precisio n with wh ich the elbow X- rays are performed .
a b
Fig. 7.10 Frontal schematic representation (a) and lateral schematic representation (b) of the elbowduring growth. c, Radiographicprojection (lateral) of the elbow:clear articular effusion without recognizable fracture; d presence ofsupracondylar fracture with articular effusion. The anterior humeralline (red and black dotted line inthe X-rays), normally intersects theintermediate portion of the humeral condyle. In the case of a supracondylar fracture with angulateddistal fr agm ent , the hum eralcondyle is posterior to this line (d).The radiocondylar line (continuous red line in h) centrally intersects the humeral condyle nucleus. The "teardrop" can be seen inpink in b

7 The UpperLimbs 133
Suprac ondy lar fractures represent the most frequent type of elbow fract ure inpediatric age (about 50%) and constit ute rou ghly one-th ird of limb fractures in th isage band . In general , they occur in ch ildr en aged 3- 10 years, with a peak ratebetween 5 and 7 years of age. In 96-98% of cases, suprac ondy lar fractures are cau sedby a fall on an outstretched hand with an extended elbow (hyperext ension fractures )(Fig. 7.11a, b); this traumatic mechan ism ens ures that the uln a and tric ipital muscleexer t an opposite force on the distal hum erus, with posterio r dislo cat ion of the distalfra gment of the fracture . Mor e rarely, in 2-4% of cases, supracondylar fracturesoccur following direct traum a to the dor sal part of the flexed elbow, with ant eriorlat eral dislocation of the distal fragment (fl exion fractures ) (Fig. 7. I Ic, d) . In thecase of supracondy lar fracture , the examinati on mu st be aimed at assessing the tum efacti on and the vasc ular and ner ve struc tures . Anter ior dislo cat ion of the pro ximalbon e fragment can lacerate the brachial vessels or cau se damage to the med ian ner ve.Conspic uous tum efact ion mu st rai se the suspici on of a possibl e compar tment syndrom e. In the case of a defect or weakn ess in the ar terial pul se, it is necessar y to perform a Doppl er examina tion of the vessels distal to the frac ture site . Supracondylarfractures in hyperextension of the elbow can be cla ssifi ed into thr ee types accordingto Gartl and (Fig. 7.12) :
Fig.7.11 Supracondylar fractures of the elbow. They can be divided into extension fractures (a, h;frequency 96-98%), and flexion fractures (c, d; 2--4%)
Fig.7.12Classification of supracondylar fractures according to Gartland. a Type I; b type II; c typeIII

7
134 D.Barbuti etal.
type I: undi splacedtype II: displaced, with angulated fragments and intact poster ior cortextype III: compl etel y displaced with posterior dislocation of the distal bone fragment and no cort ical contact.
The main aim of this cla ssification is to dist inguish stable fractures (type I andII), for which con servative treatment may be sufficie nt, from unstabl e fractures (typeIII) where surgery is necessary.
In simple fractures, it is not always possibl e to obtain clear visualization of thefract ure using X-rays, so care ful attent ion should be paid to assessment of indirectsigns that are useful for diagno sing concealed fractures . The fat pad sign is a specificreport of hemarth rosis, or mor e generally of art icular effusion, and is represented bya rad io-transparent image with triangular wedges, which can be visualize d in the latera l proj ection of the elbow, both in front of the anteri or profile of the distal portionof the hum eru s, above the coronoid fossa, and behind the posterior cortic al pro fil e ofthe hum eru s above the olecran ic fossa. A mod est dislo cat ion of the anterior fat padmay be normal ; on the other hand , a con spicuous dislocation with the appearance ofthe sail sign indicates distensio n of the joint capsule and, therefore , in the absence ofcle ar evidence of a fracture in a traum at ized elbow, can be taken as an indir ect signof a concealed fracture. Visualiza tion of the posterior fat pad is never a normal reportand even in the case of no direct visua liza tion of the fracture, immobiliza tion of theelbow and a cl inical and radiographic follow-up is required, as if it were a simplesupracondy lar fracture (Fig. 7.13) .
Fracture of the humeral condyle (Fig. 7.14a) is generally the consequence of afall on an outstretched hand and repre sent s the most commonly observed traum aticlesion in the pediatric elbow, after supracondylar fractures, representing about 20%;fracture of the trochlea is a rare event and should not be con fused with a det achmentof its growth nucleus. The X-ray image of a fracture of the lateral condyle is generally
Fig. 7.13 Concealed supracondylar fracture. a Diagram illustrating the tumefaction of the soft tissues with displacement of the fat pad signs. b L-L projection which does not show signs of fracture, but dislocation of the fat pad signs of the elbow (ar rows). c L-L projection carried out 15days later, which shows the appearance of reparative periosteal apposition (arrow)

7 The UpperLimbs 135
represe nted by the presence of a metaph yseal bon e fragment with poster ior dislo cation (Thurston-Holland fragmen t) . In the case of a fracture with minimal dislo cat ionof the bon e fragment (Fig. 7.14 b), the diagno sis may prove probl emat ic and it is useful to perform obl ique proj ection s of the elbow; in the event of a slight dislocation,the bon e fragment may be confused with a centr e of ossification . MRI and ultra soundcan be used to assess the extensi on of the fracture of the lateral cond yle to the distalepiphyseal car ti lage of the hum eru s. Fractures of the lateral hum eral condyle have anoblique course (from the out side inwards) and generall y affect the hum eral distalmetaphysis; they run through the physis and the epiphysis, and distall y reac h the jointsurface of the elbow. Although rarer, it is also possible that there are fractures that donot involve the distal hum eral metaphysis. According to the Milch classification ,these fra ctur es can be distinguished on the basis of the point at which they reac h thejoint surface:
type I: these reach the joint at the condylar groove lateral to the trochlea . In th istype of fracture the fragments are generally angled but the fractures are stabletype ll: these reach the joint surface more medially, involving the apex and theexterna l third of the trochlea. In th is second type of fracture, the head of therad ius and the olecranon can be dislo cat ed laterall y and the elbow joint provesunstable (subluxed or late rally dislocated) .
Both type s of fractures require "open sky" reduction and internal f ixation incases where the re is diastasis of the distal fragment that is ~2 mm , due to the risk ofunsuccessful con solidation of the fracture or subsequent disloc ation of the bone 'sheads.
Fig. 7.14 Fracture ofthe humeralcondylewith(a) and without(b) dislocation of thebone fragment (different patient in b)

136 D.Barbuti etal.
7Distal humeral epiphyseal fracture-se parat ions are normall y Salt er-Harris type I
av ulsi ons, more fre quen tly ob served in childre n age d und er 2 years, and gen erall y
cause d by rot ato ry or she aring for ces. In old er childre n, they may be the consequ ence of a fall with an outstretch ed hand. In radiological term s, d istal humeral epi
physeal fracture-separa tions with completely car ti lagi nous nucl eus may be diff icul t
to dist ingui sh from dislo cation of th e elbow. In th ese cases, ult rasound is useful for
a correct diagno sis (Fig. 7 .15).
Avulsi on of th e epit roc hlea represents more than 12% of traumatic lesio ns of the
elbow in ped iatri c age , and is very freq uently associat ed (in 50% of cases) with d is
locat ion of th e elbow. Th e lesion is mo st common in chi ldre n aged between 7 and IS
years, and is fre que ntly ob ser ved in sports activi ties in re lat ion to valgus stress . Th e
epitrochlea is the seat of insertion of the med ial colla ter al ligam ent and th e flexormu scl es of the for earm. In chi ldren aged over 6-7 years , avulsi on of the epit rochlea
can easi ly be iden tified on X-ray since it is ossified (Fig. 7 .16) . In the case of vio
lent av ulsive lesion s, the se parate d nucl eus can be d istally dislo cat ed in the hum ero
ulna r ar ticulati on, where it can rem ain incarcerated between th e join t head s, with
conse quent d iasta sis of the j oint head s. In smalle r chi ldre n, where the epitrochlea issti ll not ossifi ed, in the case of clinical suspici on, a comparative radiographic study
of the elbows is required, since demonstr at ion of the indirect sig n of enl argement of
the medial articular spa ce may be the onl y sign of an avuls ion of the cart ilaginous
Fig.7.15 Distal epiphysealseparati on of th ehumerus. a The A-P projection shows a medialdislocation of the bone ofthe forearm with respectto the humerus. b Ultrasound of the affected sideshows a misalignment ofthe cartilaginous distalepiphyseal nucleus of thehumerus with respect tothe metaphysis in relationto the epiphyseal separation. cThe ultrasound examination of the healthyside highlights a normalalignment of the distalcartilaginous nucleus ofthe humerus with respectto the metaphysis

7 The UpperLimbs 137
Fig. 7.16Avulsion of the nucleus of the epitrochlea in two patients of different ages: ossified (a) andcartilaginous (c, d). a Avulsion of the nucleus of ossification with separation of a small block ofbone of the trochlea (arrow) in a IO-year-old boy. b In a seven-year-old boy, the X-ray examination showsa small osseous formation (arrow) including the cartilaginous epitrochlear nucleus (asterisk) detached from the humeral margin with diastasis ofthe humerus. d Normal position of thecartilaginous epitrochlear nucleus (asterisk)
ep itrochlear nucleus and its incarcera tion between the joint head s. In the se cases,con f irm at ion with ultrasound is cle arly very useful. Assessment of the extent of disloc ation of the detach ed nucleus is fundamenta l for the cho ice of tre atment. Indeed,avuls ion of the ep itrochlear nucleus require s surgical reduction if the extent of thedislocation is 2':5 mm . MRI is useful for demonstr ating the presen ce of a part ial lesionof the medial collateral ligament, generally cau sed by functional overload in youngathletes, in the abse nce of radiograph ic signs of avulsi on of the epitrochlear nucl eu s(Fig. 7.17). In the case of fra ctures with con spicuous dislocation of the fra gment,there may be ass ociated lesions of the uln ar ner ve whi ch star ts in the epitrochlearolecran ic groove . Other fai rly frequent complicat ion s that are also worth noting arejoint rigidity and unsuccessful con solidation of the fragment.
A frequently ob ser ved traum at ic event, wh ich doe s not require a radiographic examination, is pain ful pron ation; thi s consists of distraction of the annular ligament andis generally found in sma ll chi ldren up to the age of 4 years : unt il th is age, the diameter of the radia l capitellum and that of the radia l neck are the same . This anatomiccondition pred ispo ses the patient to distraction of the lig ament following traction ofthe elbow with the arm pron ated and out stretched .
Dislocat ion of the elbow, which is rare in pedi at ric age, is mo re common amongadolescents and is mo st commonly ass oc iated with bon e fractures. Poster ior dislocations, which are mo re frequent, are generally caused by fall s with the arm outstretched or parti ally flexed and supine, whereas anter ior dislocations occur as are sult of direct traum a such as a fall on the olecranon. Medi al or late ral dislocat ion s
are the conseque nce of a direct or rotatory trauma. Th e cl in ical pictu re is dom inatedby intense pain at any attempt to mo ve the joint ; a careful periph eral and vasc ular
neurological cl in ical examination is important to highl ight possibl e ass ociatedlesions of the adjoining vasc ular- nerve struc tures (brachial art ery, med ian ner ve, and

7
138 D. Barbuti etal.
Fig. 7.17 Partial lesion of the ulnar collateralligamentof theelbow.T2-weighted gradientechocoronalMRIimagewhichhighlights analteration in the signal of the proximal portion (arrow) of the ligament due to distractive results without diastasis of the nucleusof the epitrochlea
ulnar nerve) . Besides identifying the type of dislocation, the radiographic study
should be aim ed at identifying the associated bone fracture lesions; if performedafter reduction, CT will be able to ensure better identification and definition of thesite of detachments (Fig. 7.18) . Elbow dislocations are often associated with avulsionof the epitrochlear nucleus which, during reduction, can remain trapped between the
humero-ulnar joint heads.Fractures of the olecranon are infrequent (5-7 % of elbow fractures in pediatric
age), because the olecranon of small children is cartilaginous and in older children it
is protected by an extremely thick peri ostium; in general, these are incomplete fractures without significant displacement. In nearly half of cases, they are associatedwith fractures of other bones of the elbow (Fig. 7.19) .
Traumatic lesions of the prox imal extremity of the radius consist more commonlyof fractures of the radial neck, since the epiphysis is cartilaginous until the age of3-6 years, and is therefore more resistant to traumatic lesions. Prox imal fractures of
the radius are caused by a fall on an outstretched hand with the elbow extended anddeviated in the valgus position , and are associated, in 50% of cases, with other fracture lesions of the elbow that involve the same traumatic mechanism. Fractures of the
radial neck vary widely in radiographic terms, and are sometimes scarcely perceptible and lack any displacement (Fig. 7.20) , or are characterized by a different angulation of the proximal metaphysis of the radius .

7 The Upper Limbs 139
Fig.7.18 Dislocation of the elbow. a L-L anterior projection of the elbow with osseous detachm entof the trochlea and the nucleus of the epitrochlea (arrow). b-d Posterior dislocation of the elbow.Lateral projection (b) identifie s the type of dislocation and the presence of a small detachmentof bone. The CT performed in plaster shows, in the saggital reconstruction s (c), restoration of thearticul ar relationships following a reduction procedure, and highlight s the posterior lamellar osseous detachment of the condyle (arrow in d)
Fig.7.19Fracture of the olecranon in a five-year-old girl. X-rays of the elbow in A-P projection (a)and L-L projection (h) show the fracture of the olecranon (arrows), which is associated with thefracture ofthe radial neck. cAT2-weighted saggital MRI image with suppression ofthe signal ofthe adipose tissue shows the complete extent of the fracture rima (arrow) and the presence ofhemarthrosis

140 D. Barbuti etal.
7
Fig. 7.20 Fracture of the neck of the radius in a five-year-old boy. a The X-ray of the elbow in A-Pprojection highlights a small irregularity in the cortical profile of the neck of the radius (ar row) .h Ultrasound confirms the presence of an irregularity of the osseous cortex (arrow)
Fig.7.21 Fracture of the neckof the radius in two differentpatient s with different degrees of angulation. a Fracture withangulation <300 associated with a fracture ofthe proximal ulna; b fracturewith angulation >300
According to Judet and Judet 's classification, these fractures are distinguished on
the basi s of the degree of angula tion (Fig. 7 .21) :
level I: no dislocation
level II: angulation <30 0
level Ill: angulation 30-600
level IV: angul ation >600•

7 The UpperLimbs 141
Diaph yseal fraet ures of the radius and the ulna represent 10-45% of ped iatr iefrae tures, and can involve one or both bon es of the forearm; in the case of completefracture, the bone fragm ent s may have varyi ng degrees of shift, ang ulation, or superimpo sition (Fig. 7.22) . Follow ing a trauma, generally due to a fa ll with an outstre tched hand , there may be other plastic defo rmities of the bon e of the forea rm(bowing fract ures ) involv ing both the rad ius and the ulna , and possible associationwith a complete or "greenstick" fracture (Fig. 7.23). In the case of a fract ure of onlythe bone of the forearm, the radiographic examination should include a study of theelbow and the wrist in order to exclude the possibility of an atte ndant Mont egg ia orGaleazzi fracture . The Monteggia fra cture- dis loca tion (Fig . 7.24) consists of an ant erior dislocation of the proximal radius associated with a fracture of the proximal th irdof the ulna. In pedi atric age, the plastici ty of the bon e structures may, however, leadto dislocation of the proximal extre mity of the rad ius in the abse nce of a fracture ofthe ulna. In Monte ggia frac ture -dis location, the annular ligament of the proximalradius is lacerated or dislo cated with res pect to the radia l capitellum, and may belodg ed in radiohumeral art iculation, thu s prevent ing, especially in the case ofdelayed diagnosis, compl ete reduction of the radia l head; in these cases, MRI is useful (Fig. 7.25). In cases of lateral dislocation of the rad ial head, a nerve lesion is re latively frequent, part icul arly a lesion of the posterior inte rosseou s nerve, a branch ofthe radia l nerve .
Fig. 7.22a, b Compound fracture of thediaphysis of the radius and the ulna

7
142 D. Barbuti etal.
Fig.7.23 Fracture ofthe ulna (arrow) with angulationofthe bone fragment s associated with plastic incurvation of the radius and ulna
Fig.7.24a,b Monteggia fracturedislocation in three -year-oldboy. Lateral and anterior subluxion of the radiu s (dott edlines) associated with a fracture of the proximal ulna (arrows)

7 The UpperLimbs 143
Fig.7.25Dislocation of the radius in a IO-year-old girl. a X-ray image. b Tr-weighted axial MRI image showsstructural irregularity of the annular ligament (arrow). To-weigh ted gradient-echo MRIimages confirm the dislocation of the radius in the saggital plane (c) and the intra-articular dislocation of the annular ligament in the axial plane (arrow in d)
Fractures of the distal extremity of the forearm are the mo st frequently observedlesion s in ped iatric age . In relation to the extent of the traum a, gen erally caused by afall with outstretched arm and hand, there may be "torus" -type fractures (Fig. 7.26a, b),"greenstick" fractures (Fig . 7.26c, d) , or complete fractures . "Torus"-type fracturesof the distal met aphysis of the radius may be so minute that they are not recognizedand are ass ociated to varying degrees with fractures of the di stal por tion of the uln a.Fractures of the di stal met aphysis of the forear m, espe cially of the radius, may alsoinvolve the physis with res ulting epiphysea l separation; in the se cases, the di stal fragment may be disloc ated or dorsally angulated. Indeed, epiphyseal separations of thedistal extremi ty of the radius are common (Figs. 7.27 and 7.28). Fractures of thedistal ext rem ity of the radius and uln a also include Colles ' fractures, generallycaused by a fall with out stretched hand and with the forear m prone in dorsiflexion ;the y are characterized by a po sterior disloc ation of the stump of the distal fracture,which is sometimes also dislo cated laterall y on the front plan e, according to themechanism of the trauma (F ig. 7.29). In contrast, the Smi th fracture (also known asthe Goyrand fracture or inverted Colles' fractur e) is char acterize d by a volar angulat ion of the distal frag ment and is cause d by direct traum as or fa lls on the hand with

144 D.Barbuti etal.
7
Fig.7.26 Incomplete distal forearm fractures. a, h "Torus"-type subperiosteal fracture of the distalmetaphysis of the radius (arrows). c, d "Greenstick" fracture of the diaphysis of the radius and theulna
Fig.7.27a,bEpiphyseal-metaphyseal avulsion ofthe radius with small metaphyseal bone detachmenton the palmar side (Salter-Harris type II)
palmar flexion. While in adults the th reshold of ac ce ptabi li ty of angulation of the
fragments is about 10° and is conditioned by ar ti cular involvement, the se fracture s
do not involve joints in pediat ric ca se s, and the greater capacity for osseous remod
el ing in children m akes a greate r angula tion tolerable be fore having to res or t to sur
gery. The Gale azzi fra cture, rare in pediatric age, cons is ts of a fracture of the distal

7 The UpperLimbs 145
Fig.7.28 Distal epiphyseal-metaphysea l avulsion of the radiu s in twodifferent patients with type I (a) andtype II (b) Salter-Harris dorsal dislocation of the epiphysis
Fig. 7.29a,b Colles' fracture with dorsal dislocation of the distal bone fragments of the radius and the ulna

146 D.Barbuti etal.
7diaphysis of the radius with distal dislocat ion of the ulna . This fracture may sometimes not be recognized, espec ially in the case of subluxation of the distal radio-ulnarart iculation; in these cases , CT, performed with scans in a neutral position and inmaximum prono sup ination , can be used for correct diagno sis of the lesion .
7.3The Wrist and Hand
The wri st is a complex region, made up of the distal epiphyses of the radius and ulna,eight carp al bones, metacarp al bases, and radioulnar, radioulnocarpal, mediocarpal ,and carpo-metacarpal articulations . In cont rast to what happen s in the elbow, theradial volum e is bigger than the ulnar one at the level of the wrist. The carp al bonesare completely car tilaginous at birth and have an abundant car ti laginous componentuntil adolescence; for this reason, a trauma that in an adult would cause fracture of acarpal bone, instead causes a fracture of the distal radius and/or ulna in pediatric age .The fi rst nucleus of carpal ossification is that of the capitate, already present at 2-3months, followed , after about a month , by that of the uncinate. Ossifi cat ion of thepyramidal bone begins at the age of about 2 years, of the smilunar bone at 3 years,of the scaphoid bone at 5 years, of the trapezi um and trapezoid bones at 6 years, andthe last nucleus of ossification to appear is that of the pisiform bone at the age of9-10 years ; also at the level of the car pus (wrist joint), ossif ication always occurs ata younger age in girls.
Carpal fractures, which are rare in pediatric age, are normall y associated withother fractures; as for adults, the most frequent is fracture of the scaphoid (Fig. 7.30),which is extrem ely rare prior to 7 years of age and generally observed in adolescentsdue to a fall or trauma to a hyperabducted limb. These fractures may be associatedwith ligament lesion s. In addition to the use of standard orthogonal projections, diagnosis of a suspected fracture of the scaphoid makes use of the projection with the handin ulnar deviation , which allows more complete visualization of the scaphoid.Part icula r attention should be paid to the structure and profil es of the bone but also tothe radio -tra nsparent fat plane adjacent to the scaphoid, in order to highlight possibledislocation , ideally to be compared with the oppo site side. Demonstration of its dislocation may be represented by the indirect sign of a post-t raumatic hematoma. In a casewhere the patient compl ains of pain on palpation and function al restriction, and apara-ostal tumefac tion is evident in the X-ray, with dislocation of the adjacent fatplane, even in the absence of X-ray signs of fracture, it is advisa ble to perform followup examination s, ideally MRI, in order to identi fy a concealed fracture. If there is limited availability of equipment, it is necessary to repeat the X-ray examination after10-15 days, following immobili zation of the limb in a plaster cast; indeed, X-raycheck-ups carried out some time after the traumatic event frequentl y identify a fracture rima that was previously ignored. Simple fractures are treated with immobilization for 4-8 weeks. In the case of compound fractures of the scaphoid, especially inadolescent athletes, surgical reduction should be carried out to prevent carpal instabil-

7 The UpperLimbs 147
Fig. 7.30 Single transverse fracture of thescaphoid in 14-year-old patient
ity and to enable a more rapid recover y. Given the unu sual arterial supply of terminaltype of the bone, a fract ure of the proximal pole of the scaphoid should, as for adults,lead to sus picion for the presence of a possible compl ication of avascular osteonecrosis; for thi s reas on, the patient should be mon ito red with X-rays and, in the case ofdubious repo rts, should also undergo an MRI exami nation .
In chi ldre n, fractures of other car pal bon es arc eve n rarer ; these fractures mainlyconcern the uncinate, the pyramidal (Fig. 7.3 I), and the capitate bon es. The diagnosis is frequently only mad e after X-rays carri ed out to check for other ass ociated fractures (such as distal radio-ulnar fract ures ) where the presence of thickening of car palbon es is highli ghted in relation to the appearance of osteoreparative phenom ena. Asin adults, in the case of a suspected fracture of a car pal bone which is not eviden t inthe X-ray, it may prove useful to compl ete the diagno sis using CT. Dislocations of thewrist arc pract ically non-existent in chi ldren .
Fractures of the bon es in the hand are more frequent than tho se of the carpus inpediatric age, and occur more frequently as a res ult of falls or being hit by a ball during various sporti ng activi t ies , or as a res ult of compressi on traum a; this latt er mechanis m may cause transverse longitud inal or commi nuted fractures, espe cially in theungual phalan x (Fig. 7.32). For the fi rst metaca rpal bone, the X-ray should be performed with the thumb supported dor sall y (A-P projection) and in lateral project ion ;for the other metacarpal bones, X-ray examination should be performed with P-Aproject ion in palmar support and with oblique projection, ideally with a fluoroscopic guide to ensure optimum vis ualization of the metaca rpu s; lateral project ion is notuseful for the study of metacarpal bones due to their superimposi tion. X-ray examination of the fingers requir es perfect A-P and lateral projections, the latter being particularly import ant for visualization of possible dislocation of bone fragments. Fractures ofthe hand generally require immobilization for about a month , in either plaster or aluminium splints according to the site of the fracture. Surgical synthesis with thinKirschne r wires may be nece ssary if correct reduction of the fracture is not obt ained.

148 D. Barbuti etal.
7
Fig.7.31a,b SmalIosseous detachmentof the rightpyramidal bone in l3-year-old patient (arrow in b)
Fig.7.32a,b Longitudinalcompression fracture of the intermediaryphalanx of the fourth finger withdiastasis of the fragments
Some lesions of the hand are specially rel ated to specif ic sports . Violent imp actfrom a ball may lead to met ac arpal -phalangeal dislocation of the thumb (Fig . 7.33) ,ch aracterized by dor sal dislocation of the proximal phalanx and by a marked angulation with respect to the diaphyseal axis of the met acarpus; in these lesions, the col lateral ligaments of the met acarp al-ph alangeal articulation may be comprehensivelydamaged. Detachment of a fragment of the ba se of the prox imal phalanx of the fir stfinger may frequ ent ly occur, as in the case of "game kee per's thumb", or "goalkeeper 'sthumb"; this may extend to the growth cartilage, leading to a type III lesion or, morerarely, to a typ e II Salt er-Harris les ion , cau sed by traction by part of the collateral
ligam ent of the met acarpal -phalangeal articulation of the thumb.

7 The UpperLimbs 149
Fig. 7.33 Complete dislocation of the metacarpalphalangeal articulation of the first finger
Fig . 7.34a, b Type IISalter-Ha rris fracture ofthe base of th e f ifthmetacarpuswith angulation of the distal fragment
Fractures of the met acarpal bones are rarer in pedi at ric age than in adults .Fracture of the base of the fir st metac ar pal bon e is often cause d by a traum a in hyperextension from a blow with a ball ; known as a Bennett's fracture, th is is frequently acompound fracture and may require surgica l synthes is with Kirschner wi re. Fractureof the distal port ion of the fi fth met acarp al bone is characteristic of a traum a to a fis t("boxer's fracture").
At the level of the phalan ges, epiphyse al separation is mor e frequent, espec iallyamong volley ball players when form ing a "wall" to defend against smas hes at the net(Fig. 7.34). The mall et fi nger lesion occur s due to a mechanism of forced flexion ofthe distal portion of the fi nger (generally the th ird phalanx) with a stretched extensor

150 D. Barbuti etal.
7tendon , wh ich is characteristic of the catch in baseball. In children , this type of lesion
causes a type I or " Salter-Harris lesion at th e base of the distal phalanx, or even a
type III lesion in adolesce n ts .
Suggested Readings
Bishop JY (2005) Pediat ric shoulder trauma. Clin Orthop 432:41 -8Carson S, Woolridge Dp, Colletti J, Kilgore K (2006) Pediatric upper extremity injuries. Pediatr Clin
N Am 53:41-67Cekanauskas E, Degliute R, Kalesinskas RJ (2003) Treatment of supraco ndylar humerus fractures
in childr en, accordi ng to Gartland Classification. Medicina (Kaunas) 39(4) :379-83Chung KC, Spilson SV (2001) The frequency and epidemiology ofhand and forearm fracture s in
the United States. J Hand Surg Am 26(5) :908-15Gartland JJ (1959) Manageme nt of supracondylar fractures of the humerus in child ren. Surg Gy-
necol Obstet 109:145-54Johari AN (1999) Remode lling of forearm fracture s. J Pediatr Orthop 8:84-7Judet H, Judet J (1974) Fracture s et orthopedie de I'enfant. Maloine, Paris, pp 31-39Kay RM, Skaggs DL (1998) The pediatric Monteggia fracture . Am J Orthop 27(9):606-9Kubiak R, Slongo T (2002) Operative treatment ofclavicle fractures in children: a review of2 1 years.
J Pediatr Orthop 22:736-9Heal J, Bould M, Livingstone J et al (2007) Reproducibil ity of the Gartland classification for
supracondylar humeral fractures in children . J Ortho p Surg 15( I):12-4Heras J, Duran 0 , de la Cerda J et al (2005) Supracondylar fracture s of the humeru s in children .
Clin Orthop 432:57 -64Hovelius L, Augustini G, Fredin 0 et al (1996) Primary anterior dislocation ofthe shoulder in young
patient s. J Bone Joint SurgAm 78A :1677-86Lee SS, Mahar AT, Miesen 0 , Newton PO (2002) Displaced pediatric supracondylar humeru s frac
tures: Biomechanical analysis ofpercutaneou s pinning techniques. J Pediatr Orthop 22(4):440443
Magra M, Caine 0 , Maffulli N (2007) A review ofepidemiology ofpaediatric elbow injuries in sports.Sport s Med 37(8) :717-35
Murray OW, Wilson-MacDonald J, Morscher E et al ( 1996) Bone growth and remodeli ng after fracture. J Bone Joint Surg Br 78B:42 -50
Shim JS, Lee YS (2002) Treatment ofcompletely displaced supracondylar fracture of the humerusin childre n by cross-fixation with three Kirschner wires. J Pediatr Orthop 22( I): 12-6
Vioreanu M, Sheehan E, Glynn A et al (2007) A new type of pediatr ic injury. Pediatrics 119:12941298
Vorlat P, De Boeck H (2003) Bowing fracture s of the forearm in children : a long-term followup.Clin Orthop 4 13:233-7
Wilkes JA, Hoffer MM (1987) Clavicle fractures in head-inj ured children. J Orthop Trauma 1:55-8Wu J, Perron AD, Miller MD et al (2002) Orthopedic pitfalls in the ED: pediatric supracondylar
humeru s fracture s. Am J Emerg Med 20:544-9Wuff RN, Schmidt TL (1988) Carpal fracture s in children . J Pediatr Orthop 18:462-465

8.1The Pelvis, Hip, and Femur
The pelvi s is ring shaped and is made up of the iliac bone s, with the ir apophyses, theischium with its apophyses, the pubic bones with the synchondrosis inser ted, thesacrum, and the sacroiliac art iculation s, of which two-th irds are an amph iarthrosissince an articular f ibrocartilaginous disc is inserted between the two joint surfaces,and one-third a synovia l articulation. The stability of the pelvic ring is maintainedby the iliolumbar, sacroiliac, sacrotuberous, and sacropinous ligaments. The pelvis ishighly vascular ized: the hematic contribution is mainly provided by the hypogastricvessels, or inte rna l iliac vessels, which star t clo se to the pelvic arch; other importantvessel s include the upper glut eal arteri es, often damaged in posterior fractures, andthe interna l obturator and pudendal vess els, often damaged in fractures of the pubicbranches. Innervation is provided by the nerves from the lumbar and sacral plexus,
which pass through the posterior part of the pelvic ring. The site of the fracture isgenerally pred ictive of the type of vascular, neurological, and visceral lesion s thatmay be ass ociated.
The fundam ental differenc es between the pediatr ic and adult pelvis include thefollowing : the greater malleability of the bones, the capac ity of the cartilage toabsorb more energy, and the gre ater elasticity of the joints; tr iradiate cartil age ispresent and the periostium is thi cker : an apparent dislo cation may have a shell ofperiostium and heal like a fracture .
The acetabular bone has three centers of ossificat ion : the ilium, the ischium, andthe pubi s; each has its own physis which determines circumferential growth ; at thelevel of the ace tabular bon e the three centers fuse in the trirad iat e cart ilage whic h,
D. Barbuti (C8J)Department of Diagnostic Imaging, Pediatric Hospital "Bambino Gesu", Rome, Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
151

152 D.Barbuti etal.
8on average, ossifi es between the ages of 13 and 16 years. In the course of pubert y,various centers of secondary ossification appear; it is important to know abou t theseto avoid con fusing them with fract ures :
os acetabuli: th is forms the ante rior ace tabular wall ; it appears at 12 years of ageand fuses at 18 yearsacetabular epiphysis (epiphysis of the ilium): this forms the main part of theupper acetabular wallsecondary center of ossification of the ischiumiliac cres t: thi s appears at the age of 13-15 years, in the antero-l ateral portion ; itadvances in a postero-medial direction and fuses at the age of 16-1 8 years, beginning inverse ly from the postero-medial part. The Risser test, the index of skeletalmaturity, is based on its app earance and ossifi cationischiatic apophysis: th is appears at the age of 15-1 7 years and joins at the age of19-25 yearsanterior-superior iliac spine (ASIS) : this appears at the age of 15 years and fusesat the age of 20-25 yearsanterior-inferior iliac spine (AIlS): this appears at the age of 13-15 years andjo ins at the age of 16-1 8 yearspubic spineangle of the pub esischiatic spinelateral wing of the sacrum.
8.1.1Fractures of the Pelvis
Frac tures of the pelvis are not very frequent, representing 2.4- 7.5% of pediatric fractures ; indeed, their incid ence is 10 times lower than in adults. They are due to roadaccidents (especially pedestrians who have been run over) in 98% of cases, a muchhigher percentage than in adults for whom acci dents are the cau se in 50% of cases;seri ous falls and abu se are rarer causes. In most cases they are not serious lesion s butthere may be ser ious associated lesion s. Apophyse al avulsion fractures of the pelvisoccur in older children and adolesce nts, and generally provide few probl ems. Weshall only make brief mention of them because they are dealt with elsewhere(Chapter 3). Avulsion of the isch ial tuberosity (inse rtion of the ham string muscles) iscaused mainly by sports such as hurdling , football, gymnasti cs, fencing , and tenni s.Detachm ent of the ASIS (insertion of the sartoria l muscle) occurs mainly in football,gymnastics, and fencing. Detachm ent of the AIlS (insertion of the rectu s femorismusc le) occurs mainly in football, athletic s, tenn is, and sprinting. Detachment of theiliac crest (inse rtion of the abdom inal muscles) occurs mainly in football , gymnastics,and tenni s.
The most serious lesion s derive from fractures caused by road accidents. Thetraumatic mech ani sms are the same as in adults. Generally, in order to cause a frac-

8 The Pelvis and Lower Limbs 153
ture of the pelvic ring or the acetabular bone, high- energy impacts are requ ired,which often cause associa ted lesion s of a traumatic osteo-articular natur e, such asfractures of the long bones or the spine, lesions of a vascular nature (less frequ ent inadult s), urologi cal lesions, such as injur y of the bladder or the urethra (the lattermainl y in men), or neurological lesion s. In these types of trauma, a general physicalexamination and a local object ive examination are important in order to highl ightareas of bruising , abrasion, lacerations, ecchymosis, or hematomas of the pelviperineal region. It is important to pay particular attention to assessing the "critica lareas", like the iliac crest, the sacro-iliac articulations, the pubic symphysis, theASIS, and the AilS . It is necessary to examine the articular movement of the hips andit is important to perform a vascular and neurological examination as well. In thecase of comp ression trauma s, even in the absence of clear fractur es, there may bedamage to the trir ad iate cartil age (type V Salte r- Har ris lesions), which may result inarr ested growth , acetabular dyspla sia, subluxation of the femor al head, and dysmetria of the lower limbs. Fractures of the femoral neck are extremely rare, but whenthey occur they are associated with a high percentage of complications. Fractures ofthe acetabular bone through triradiate cart ilag e only require minor- energy traumacompared to acetabular fractures in adult s.
X-ray assessment is performed with A-P projection of the pelvi s and withinlet/outlet projections, ideally with oblique projections, although computed tomography (CT) is often nece ssary (associated with 3D recon structions). In the case ofsuspected lesions of the urinary tract , it may be important to per form a cystogr aphyusing a catheter, or a urogr aphy (the latter is only nece ssary when the CT examin ation is not per formed and uses contrast agents injected intravenously). In the case ofsignificant traumas, careful assessment of the whole body must be made to search forsigns of cranial and/or spinal trauma. For unstable compound fractures of the pelvis,with lowering of the hem atocrit, it may be advisable, after assessment with mult islice CT, to perfo rm an angiography and, if there are hem atom as, embol ization of thebleeding vessel. Magnetic reson ance imaging (MRI) can be used as a follow-upexamin ation and may be useful for highl ight ing damage of the triradiate cart ilage or,earl ier than the X-ray, may show signs of avascular necrosis of the femoral head.
There are various type s of classif icat ion of pelvic fractures.The Watts classification, modified by Torode and Zieg , distinguishes pelvic frac-
ture s into the following type s:type I: avulsion fracture stype ll: fracture of the iliac wingstype llI: stable fractures of the pelvic ringtype IV : unstable fracture s of the pelvic ring with free bone fragmen t.
The Tile classification distinguishes between the follow ing types:type A: stable (Fig. 8.1)type B: vertically stable, but with rotatory instability (Fig. 8.2)type C: both vertical and rotator y instabilit y (Fig. 8.3).

8
154 D. Barbuti etal.
Fig. 8.1 Stable Tile fractures type A. a X-ray image of the fracture of the iliopubic branch, easilyrecognizable using CT (b) , where it is also possible to observe fracture ofthe iliac wing (c), whichis not visible with X-ray. d In another patient , fracture of the iliopubic branch with slight diastasis of the pubis and the left sacroiliac (arrows). e Good situation at the check-up after 2 months
Fig. 8.2 Unstable Tile fractures. a Diastasis of the pubis, an unstable Tile lesion type B. bPostoperative check-up . c Unstable Tile lesion type B, with distasis of the pubis (arrow) and theright sacroiliac joint (black arrow). d Unstable Tile fracture type C with distasis of the pubis(black arrow) and the right sacroiliac joint (red arrow) with vertical and rotatory instability

8 The Pelvis and Lower Limbs 155
Fig.S.3 Five-year-old boy. Unstable Tile fracture type C with associated lesion of the urethra. a TheX-ray shows a fracture of the left ilial and ischiopubic branch (arrows), associated with a fractureof the sacrum with diastasis of the right sacroiliac joint, more clearly visible with CT (b). c Lesionof the urethra at CT cystography. d Clinical appearance (d) and intra-operative view (c). f Checkup after synthesis (images kindly provided by Prof M. Oranski)
The Kane classification dist inguishes fiv e typ es:
type I (58 %): avuls ion or fracture of a segm ent , without break of the ring; there
are gen erally no ass ociationstype II (20%): break ofa singl e ring clo se to th e pubic symphys is or to th e sac ro
iliac articulation; there may be associat ion with abdominal and gen ito-urinary
lesionstype III (7%): un stabl e fracture with doubl e bre ak of the pelvic ring . Th is includesstraddle -type fracture, bilateral ischio-pubic fracture, Malgaigne fracture (doublevertical or double unilateral branch plu s the ileum); bleeding and abdom inal
and /or gen ito-urinary lesions are frequ enttype IV (10%): ace tabular fractures; there are freque nt association with intra
abdominal or genito-urinar y lesions du e to th e high energy of th e trauma
type V (5%): multipl e fractures type" + IV or type III + IV.
The Young and Burgess cla ssific at ion identifies fractures accord ing to th e trau
matic mech anism and the di rection of th e force , distinguishing betw een th e follow
mg:
form s cau sed by lateral compression (50 %)
form s cau sed by "open book" anteroposterior compression (25 %)
form s cau sed by vertical shears, as happens in the case of a serious fall (5%)
mixed form s (20 %) .

156 D.Barbuti etal.
8The mo st widely used classification, especially in pediatr ic contexts, is the Tile
classifi cat ion . Stabl e fractures include isolated fractures of unilateral or bilateralisc hiati c branches (Duverny frac ture ) and isolated sacr al fractures. Unstable fracturesinc lude the Malgaigne f racture (vertical fract ure which involves both arches) ; the soca lled "straddle " fracture, a bilateral fracture of the ilium and ischio-pubic branches,usuall y with raise d fragment and assoc iated in 20% of cases with vesic o-urethrallesion s; pelvic dislocation with distraction of the sacro-i liac art iculation (normalwidth 1-4 mm) and the pubis (ma ximum distance between the pub ic bones 5 mm) ,oft en associat ed with genito-urinar y lesions; and the rare "bucket handl e" fracture inwhich the anterior arc h is damaged on one side and the posterio r arch is damaged onthe opposite side.
Acetabular fractures (Fig. 8.4) occur in about 10% of traum as and are frequentlyass ociated with abdominal or genito-urinary lesions, since high ene rgy is required tocause them. They are class if ied into the following types:
type A: detachment of the poster ior wall with posterior luxation of the hiptype B: compound linea r fract ures ass ociated with fractures of the pelvic rin g
generall y stabletype C: linear fractures with ins tability of the hiptyp e D: med ial frac ture-dis locati ons.
Particularly in type 8 fractures, the re is a possib ility of a lesion of the triradi atecartilage. These lesion s may occur due to two mechanisms: direct impac t (type VSalte r-Harri s lesion) or shearing force s (type I-II Salte r-Harri s lesion) . They may beass ociated with bone fractures with or without min imal dislocat ion of the fragments.Possible sequelae include: progressive acetabular dysplasia, due to thicken ing of the
Fig. 8.4Acetabular ischio-pubic fracture in a sixteen-year-old patient. a, b X-ray; c axial CT; dcoronal CT and e 3D CT provide a better view of the displacement of the fractures. f Check-upafter ORIF synthesis (images kindly provided by Prof M. Oranski)

8 The Pelvis and Lower Limbs 1S7
med ial ac etabular wall and consequent subluxa tion of th e femoral head ; or a
hypoplasia of th e hem ipelvis due to vascular dam ag e of th e tri radiate cart ilag e which
causes precocious fu sion. Obviously, th e younger th e ag e of th e child, th e more ser i
ous th is eve nt will be. In th e case of tr aumas wh er e th er e is sus pe cte d damage of th e
tr iradiate cartilag e, it is advisable to perform a prolonged follow-up exam inat ion
with MRI (in th e absence of sy nthe ti c metal materi als) or CT, in ord er to identi fy
s igns of pr ecocious ossif ication of th e cartilage its el f (Figs. 8.5-8.7).
Fig.8.S Fracture of the sacrum and of the iliac wing and diastasis of the pubis in an eleven-yearold girl. a On x-ray, only left iliac wing fracture (black arrow) and diastasis of the pubis (redarrow) are visible. b At the CT examination, besides the fracture of the left iliac wing (whitearrow) fractures of the sacrum are also visible (black arrows). c Postoperative check-up (imagekindly provided by Prof M. Oranski). After one year, T2-weighted coronal MRI shows the normalappearance of the right triradiate cartilage (d), while on the left, in coronal section (e) and sagittal section (I) , an ossification bridge has appeared (arrow)
Fig.8.6Fracture of the anterior acetabular column associated with femoral diaphyseal fracture in aseven-year-old boy. a, h X-ray. c Postoperative check-up (image kindly provided by Prof M.Oranski). d CT with coronal reconstructions shows initial closure of the left triradiate cartilage
(cont.7)

158 D. Barbuti etal.
8
Fig.8.6 (cont.) e, f The MRI shows thin hypointense areas caused by ossification of the left triradiate cartilage (I). g The X-ray performed 5 years afterwards demonstrates complete closure ofthe cartilage to the left (ar row)
Fig.8.7 Ten-year-old boy, a year beforepelvic trauma with negative X-ray. a,b Coronal CT shows advanced ossification of the left triradiate cartilage.cAt T2-weighted coronal MRI, islandsof ossification are visible in the context of the triradiate cartilage (type VSalter-Harris lesion)
8.1.2Sacro-coccygeal Fractures
These are rare and are generally caused by direct tr auma; they are usu ally treated
with rest and painkillers .
Stable fractures are treated with immobi lization in a cast for 4-6 weeks. Unstable
fractures can be treated with traction and subseque nt immobil ization, with an external fixative or surgical synthesis (open reduction inte rn al f ixat ion (ORIF)) . In gen
eral , th e fracture heal s aft er about 8 week s, wh ile in adults a longer period is neces-

8 The Pelvis and Lower Limbs 159
sary. The child should be kept under surv eillance for a long time after the fracture toexclude blocks to growth caused by prematur e ossification of the triradiate cart ilagewith disturbance of the axis or dysmetri as of the limbs.
Indicat ions that suggest the need for surgery include a shift in the sacro-il iacart iculations greater than I em, a diastasis of the pubis greater than 4 em, acetabularfractur es with a shift of the load-bearing area of more than 5 mm, instability of thecoxo-femor al artic ulation, and fractur es of the posterior acetabular column of morethan 50%.
Trauma mechani sms, pathological pictures, and compl icat ions vary according toskeletal matur ation. Dislocation of the sacro-iliac art iculations is more frequent inpatient s with immature skeletons. Failure to treat unstabl e fractures can lead to pelvicasymmetri es with consequences in the futur e. Surg ical treatment of pelvi-acetabularfractur es has few compli cat ions when it achieves the greatest possible anatomicalreduction.
Complications frequently arise from associated lesion s such as concussion , andthoracic and visceral injur ies. On the basis of an analysis of 120 fractur es, Reichardand coll eagues recorded retrop eritoneal hematom a in 46% of cases, but in only 3%of cases was surgery required to tampon the vesse l or for embolization using angiography; transfusion s were nece ssary in 11-32 .6% of cases, more frequently in multiple rather than single frac tures (15 as oppo sed to 9) . Vesico-urethral lesion s are lessfrequent than in adults, about 6- 8%, and consist of extraperitoneal bladde r rupture in80% of cases, with hematuri a, suprapubic pain, and hypoten sion . Diagno sis uses CTor CT cystography. Urethra l lesion s, which are more frequent in males, generallyoccur in fractures of the pubic branches. They are typic ally associated with the clinical triad of the presence of blood in the urethral meatus, vesical disten sion , and theimpo ssibil ity of urinating . Diagno sis involves CT cystogr aphy (Fig. 8.3c). This maylead to sexual dysfunctions in male s. Abdominal lesion s are found in 11-20.4% ofcases of pelv ic fractures in pediatric age, with the following percentages: hep aticlesion s 8.4%, splenic lesion s 3.2%, urogen ital lesion s 3.2%, colon 2.1%, small bowel1.1% (Ismail and coli) . Neurological lesion s, the cause of a cert ain degree of morbidity, are much rarer in pediatric age than in adults (21%). They consist of lesionsof the lumbar root s in the case of lesion of the sacro-i liac articulation, with deficit ofthe anterior tibialis and dorsal hypoe sthes ia of the foot in the case of lesion of L5; inthe case of sacra l fracture and lesions of the S I-S2 roots there is weakne ss of theextens ion of the hip and plantar flexion , posterior hypoesthesia of the leg, the sole ofthe foot , and the genitals; and in the case of lesion of S2-S5, or cauda equina syndrom e, there may be hypoesthesia of the perineum, and intestinal and bladder dysfunctions.
8.1.3Traumatic Luxation of the Hip in Children
Much less frequent than in adults, thi s may occur in children under 6 years old, dueto fairly minor traumas such as a fall backwards while the child is bending. In these

160 D.Barbuti etal.
8cases, the redu ction takes pla ce without probl ems and without sequelae . Onl y in15-20% of cases are these fractures assoc iated with acetabular fract ures or fract uresof the femora l head, in contrast to adul ts where the ass ociation occurs in more than50% of cases . In adults this tak es plac e due to more ser ious traum as, such as sportsinj uries, falls, or road acci dents . Diagnosis is performed with X-ra ys. CT may proveuseful due to its greater sensi tiv ity in detecting small bone detachm ent s that mayobstruct redu ction. The prognosis is linked to the extent of the initi al trauma, espec ially if associated with an ace tabular fracture of the femoral head. In children, theinci dence of avasc ular necrosis or arthrosis follow ing traumatic luxat ion is much lessthan in adul ts, but rap id and accurate cor rect ion (whic h may require surgery) is necessary, especially in the case of an assoc iated fracture. A delay of over 24 hours inthe reduction increases the possibil ity of avascular necro sis. Immobilization and proscri pti on from putting weigh t on the limb are also important; putting weigh t on thelimb earlie r than two months aft er the fracture increases the percentage of these complication s.
8.1.4Fractures of the Femur
Fractures of the femora l neck are rare ; only 1.1 % occur in pedi at ric age, but with ahigh percentag e of complications , so they therefore always con stitute an emer gency." Hip fractures in child ren are of interest because of the frequ ency of complicat ion srather than the frequency of frac tures " (Cana le and Bourland).
While in adults a tor sion mech anism is mo re common, in children the cause isdirect traum a, such as a coll ision with a vehicle or a serious fall with direct traum aof the hip . Tran s-cervical and basal fractures are more frequ ent. There are also possibi lities of pathological frac tures of the femoral neck on cystic lesions (frequ ent inthis locat ion ) or histio cytosis, tumors, mal ignant hemol ymph nod es, or in the case ofsyndromes with osteoporosis (imper fec t osteog enesis, ar throgryposis , etc) .
The mo st common complications of these lesion s are avasc ular necro sis (13% inthe ser ies of 108 cases analyze d by Azour and coli but with aver ages in the literatur eof up to 50%) , preco ciou s clo sur e of the cart ilaginous plate (12%), var ism (8.3 %),and unsuccessfu l con sol idation (3.7%).
In ord er to explain the frequent complications of avascular necro sis in the seque lae of these fractures, mention should be mad e of the vasc ularization of the femoralhead and femoral neck. It should be remembered that the art eri al cir cle of the femoralhead is delicate. At birth the cartilage of the physis is extrasynovial. At the age of3 years, the neck lengthens, growing more rapidly medi all y than laterall y, and thephysis becomes mainly intracapsular. The med ial cir cumflex femo ral artery suppliesblood to the femoral head, while the lateral cir cumflex ar te ry supplies blood to thelarge trochante r. This transition from the neon ate-nursling system with small multiplevessel s, to the subsequent stage with two large systems (po stero-superior and posteroinfe rior) predi spo ses the patient for all his/her life to vascu lar insult of the femoralneck due to fractures with di splacement.

8 The Pelvis and Lower Limbs 161
For diagnosis , X-ra y with A-P and lateral proj ection (frog-leg or Dunlap) is neeess ary. CT can be useful in compound fractures for a mor e preci se measur ement ofthe dislocation for surgica l purpo ses.
Fractures of the femoral neck in children follow Delbet and Chung s classifica-tion (five types) :
type I: trans-epiphyseal fracture (12%) (Fig. 8.8b) . Thi s may be cau sed by delivery trauma which man ifests itself with a pseudo-paralysis of the lower limb.Diagnosis is also difficult due to the lack of ossification of the nucl eus. In old erchildren, it should bc dist inguished from acute epiphys iolys is which generall yaffect s chi ldren over 9 years old, who often have endocri ne disorders that caus epain in the growth cartilage and in whom the traum a that provokes the probl emmay be trivi al. Treatm ent involv es immobil ization, in the absence of disloc ation,and cautious reduct ion and surgica l synth esis in the case of a compound fracture .Avascular necrosis is a frequent complicat iontype Il: trans-cervical or mcdio-ccr vical fractu re (Fig. 8.8d, c). This is the mo stfrequent type (27-50%) and is often complicat ed by avascular necro sis (up to50%) (Fig. 8.8g)type Ill: basal or cervi co-trochant er ic fracture (Fig. 8.9) . This is the sec ond mo stcommon type of fracture of the femoral neck (22-35%) and also the second interms of frequency of avas cular nec rosis. It is di sloc ated in two-thirds of cas estype IV: inte rtrochanteric fracture, which is not very frequent (10-19.5%) .Complications are rarer; avas cular necrosis, in particular, is possible thoughinfrequent (Fig. 8.1Oa, b)type V: subtrochanteric fracture (19 .5%) , which many authors do not classifyamong the femoral neck fractures and that generally is not as complicated as theother form s.
,~ . 1
C
Fig.8.8 Pediatric femoral neck fractures. a Schematic classification according to Debelt- Chung.b Type I trans-epiphyseal fracture; c postoperative check-up. d Type II trans-cervical fracture atX-ray (arrow); e CT clearly shows the displacement; f postoperative X-ray; g after I year, thescrews were removed; there are signs of avascular osteonecrosis of the femoral head

162 D.Barbuti etal.
8
Fig. 8.9Type III fracture of the femoral neck. a X-ray; b postoperative check-up; c after I year, thescrews were removed; irregularity of the head and neck and coxa vara is visible
Fig.8.10Type IV and V fractures of the femoral neck. a Type IV; b postoperative check-up. c Type Vtrochanteric fracture; d, e successful outcome with conservative treatment
Surgery is normall y n ecessa ry an d is performed using fixat ion of one or two thi n
tr ans -cer vica l na ils or screws . One-third of ca se s ar e ass ocia ted with pel vi c fracture s
or concussion, wh ich is wh y diagnosi s is del ayed.
Detachment of the small trochanter (i ns er ti on of the iliopso as muscle) is mo re
rare and oc curs due to har sh contract ions aga inst resista nce of this mu scle, l inked to

8 The Pelvis and Lower Limbs 163
sports activities. In general , the fracture is only a few mill imeters because the insertion of the iliopsoas is prolonged in the diaph ysis; ult rasound, and occa sionally MRI ,may be useful for det ect ing associated musculotendinous lesion s. Treatment is generally con serv ative. These fractures sometimes lead to coar se ossification.
Detachment of the large trochanter (in sert ion of the medi al and small glut ealmuscl es, pirifo rm muscl es, and internal obturato r muscles) occurs especially in chi ldren who take part in athl etics, as in the case of forc ed hyperabduction ("th e splits" ).
Fracture of the femo ral diaphysis may occur in young children due to obstetrictrauma or abuse; in older childr en it may be due to a fall, sports lesions with tors ionmechanism, or serious direct traumas. The viol enc e that is required for th is type offracture is less than that requ ired for an adult, which also explains why there is lessbleeding . X-ra y examination with doubl e proj ect ion is suffi cient for diagnosis. Thesimples t treatm ent , in very small children, is traction in order to achi eve good alignment and, subsequently, immobilization in a cast. It may be adv isable, especially inmultipl e traumas, to appl y an exte rna l splint due to the difficulty of immobil izat ionusing a cast. In older childr en, generall y over 8 yea rs of age, and especially if theyare well-built or overweight, synthesis is oft en necess ary, which may invol veintramedull ary synthesis with a Kunt scher nail or elastic nail s, or with a nail-plate(Fig . 8.11) . In preparing the cast, it is important to avoid hyperextension of the knee ,which may lead to damage of the popliteal vessel s. Under the age of 10 years, it isacceptable to use shortening by superimposi tion of 1-2 cm (obviously greater theyounger the child) , which will compensate future bone hypergrowth due to regionalhyperemia linked to healing of the fracture . Over the age of 10 year s, shortening of2 cm is not acceptable bec ause it would not be regained by growth. Other rare complic ations include dysmet rias, most frequently hypergrowth (Fig . 8.12); and disturbance s of the axis in valgus, in varu s, procurved or recurved. The re are other complic ations that are almost non-existent in pedi atric age, such as pseudoarthrosis, consolidation defects, and fat emb ol ism; the latte r, though rare, should be avoided at allcosts and prevented in older children , especi ally if they have to unde rgo surgery.
Fig.8.ll Treatment of diaphyseal fractures of the femur. a Trans-skeletal traction and immobilization; b Kuntcher-type intramedullary nail; c plate with screws; d intramedullary elastic nails;e external fixative

8
164
8.2The Knee and Leg
8.2.1Fractures of the Distal Epiphysis of the Femur
D.Barbuti etal.
Fig.8.12Spiroid diaphyseal fracture ofthe femur. a X-ray in a plaster cast.b Hypermetria at the follow-up afterI year
These may derive from delivery trauma, in the case of dystocic delivery, and in thiscase diagno sis is easier becau se the nucleus is alre ady ossif ied at birth , in contrastto what happ ens in the case of deta chm ent of the cephalic nucl eus whic h is not ossif ied unt il 3- 5 month s. They arc generally type I Salt er-Harris traumas and usuallyinvolve posterior fract ures . The progno sis is usually good . They are more frequent inchildren age d over 7 years, as a res ult of violent traumas; these frac tures are agg ravated by a high percentage of shorten ing or angular deformity (about 40%). It shouldbe remembere d that distal carti lage is respon sible for 70% of the growth of thefemur and 40 % of growth of the entire lower limb. In traumas in hyperextensio n, itis possible to determ ine damage to the popl iteal vasc ular nerve sheath and, if thesymptoms do not improve afte r reduction, surgica l exploration is necessary. In children , sports traum as with mechanism in valgus, which can cause ligament lesion s inadults, can lead to epiphyseal det achment. Sometime s only stress radiography candist ingui sh epiphyseal det achment from a ligament lesion .

8 The Pelvis and Lower Limbs 165
Type I Salter-Harris fractures in old er ch ildren gen erall y cau se anter ior disloca
tion . Ca reful as sessment of th e distal c ircl e is nec es sary. In gen eral , bloodless re duc
tion is required, pr eceded by arthro centes is in th e ca se of abundant hem arthrosis.
Type" and III Salter-Har ris lesions occur with a valgus trauma and may not be rec
ogni zed , inste ad being m istak en for ligam entous lesion. If th er e is no fracture, no
reduction is requir ed . ( Fig . 8. I3a, b). Typ e IV Sa lter- Harr is lesion s (Fi g. 8. I3c) must
Fig.8.B Fractures of the distal epiphysis of the femur through the growth plate (arrows). a Type IISalter-Harris fracture with metaphyseal triangular fragment; b type III Salter-Harris lesion withepiphyseal but not metaphyseal fracture; c type IV Salter- Harris lesion with fracture of both themetaphysis and the epiphysis
Fig.8.14Early physeal fusion. a Shortening and partial fusion of the distal physis of the femur following a type V Salter-Harris fracture. b Multiple fracture of the femoral diaphysis with involvement of the physis, treated with synthesis in the distal part and with immobilization in a cast (c).d After a year, the comparative X-ray shows hypometria and deviation in valgus from the previous setting of the lateral part of the distal physis of the right femur

166 D.Barbuti etal.
8be redu ced with anatom ical synthes is, whic h is oft en only possibl e with surgery, inorder to avoid frequent complicat ion s (Fig . 8.14) . The se are unstable fractures: surve illance of the young pat ient s is necessary with X-r ay check-ups on at least an annual basis until complete matura tion has occurred . Forty per cent of shortenings andangulat ions require surgica l corre ction .
Parcel detachm ent s in the lateral area of the distal growth car ti lage may repr esenta type VI Salte r-Harri s fracture according to Ogden, and may damage the Ranvie rsulcus, causing partial growth arrest of the area concern ed, with possible angulardeformity, which is mor e seri ous the younge r the child.
8.2.2Fractures of the Patella
The se are less frequent than in adults , representing about 1.1% of fractures. Themechanism may be direct trauma or an avulsion, especi ally in the case of luxat ion or
lateral subluxation . The treatment is the same as for adults and is therefore designedto re-establ ish the artic ular sur face and exte nsor mechanism of the knee. The socalled pat ellar "s leeve" fractu re re presents the typical case of fracture of the patell ain chi ldre n, in whic h a small blo ck of bon e is detached, tak ing with it a wide car ti lag inous shell. The mo st vulnerable age is between 8 and 12 years; displacement ofthe cartil age of the inferior polus is po ssible and the det ached bone fragment may bevery small. Treatment should be con servative with displa cement of less than 2 mm
and the extensor apparatus intact.X-ray examinat ion in double projection, supplemented with axia l projection of
the patella, is generally suff icient for the diagno sis. In some cases it may be necessary to carr y out further examination s with CT or MR I. Differential diagno sis mayinvolve the var iants represented by the num erou s accessory nuclei of the patella orSinding-Larsen- Johansson disease.
8.2.3Fractures of the Tibia
Fractures of the tibia mainly affect children aged between 8 and 13 years, with trauma
in extensi on and sudden intra rot ation, especi ally cau sed by cycling . They are cause dby traumas of less power tha n tho se that affect adults . The traum at ic mechanism,whi ch in adults causes lesion of the anterior cru ciate ligament, causes thi s type of
lesion . Meyer s and McKeever classify the se fractures into three typ es:type I: with minimal displacement of the detached fragment from the res t of thetibial spine. Clinically, pain is reported without significant restriction of the flexionextension artic ulation. Treatment involves arthrocentesis and a cast in hyperextension
type ll: with displacement , in ge neral raised with angul ation, of one-thi rd or theanterior half of the fragment of the spine with a "beak-like" appearance in the

8 The Pelvis and Lower Limbs 167
X-ray examination. Clinically, the patient feels pain and has functional restrictiontype 1I1: complete detachment of the spine .
In type 1\ and III reduction, surgical synthes is is necessary but the prognosis isgenerally good. The diagnosis is performed with X-ray in double projection, whichmay be supplemented by proj ect ion of the inter condylar tunn el. CT may sometimesbe useful for precis e identi fi cat ion of the posit ion of the dislocated fragm ent , oraltern atively MRI may be used to assess the state of the ant erior cruciate ligament ,which is generally intact in these types of fracture.
Proximal epiphyseal detachments of the tibia are rarer due to the absence of ligament apparatus for inse rtion in this region. The traum a generally occurs with amechanism of hyperextension . They may rese mble ligament lesion s, and stress rad iography may be necessar y for the diagnosis. Type III and IV Salt er-Harris lesionsmay require reduct ion with bloodless synthes is.
Fractu res of the anterior tibial tuberosity are cau sed by a violent contraction ofth e quadriceps muscle with a flexed knee. Watson and Jon es classify thr ee types(Fig . 8.15):
type I: raising of the tub ercl etype 1I: fractured base with displacementtype Ill : avulsion and raising , equ ivalent to a type III Salter-Harris fracture.
Fig.S.1S Fractures of the anterior tibial tuberosity. Schematic classification (a), X-ray (b), sagittalCT (c), and 3D CT (d) of a case of type III fracture. e Postoperative check-up

168 D.Barbuti etal.
8 The type I fracture may be treated with immobilizat ion in a cast , but th is oft enleads to symptomatic Osgo od-Schl att er di sease. For types II-III , surgical reductionis generall y require d.
Fractures of the proximal metaphysis of the tibia are not frequent; they are genera lly tre ated conservat ively and have a good prognosis. The proximal fracture of thetibia can lead to valgis m of the knee in 15% of cases (Fig. 8.16) . The mechanismsres pons ible for thi s complicat ion have not yet been complete ly cla rified . It has beensuggested that there is par tial damage of the cartila ge of the physis (type VSalter- Harris mechan ism) with precocious asy mmetric knitt ing of the lateral part , ormainly lateral traction forces, or medi al inter posi tion of the soft tissues.
Diaphyseal frac tures of the tibia are frequent however. A frequent type of fracture is the so-called "toddler 's" frac ture, which affect s small child ren tak ing theirfi rst falt ering steps . Their falls easi ly lead to diaph yseal spir oid frac ture of the tibiawith a tors ion mechan ism (Fig. 8.17) . It is generall y a simple fractu re and eas ilytreated, oft en with a delayed diagnosis, when it is already in the healing pha se.
Fig .8 .16 Proximal metaphyseal tibial fracture withoutdisplacement. a X-ray;b appearance of valgism ofthe right knee after one year
Fig . 8.17 a, b "Toddler fractures" of the tibia (arrows).This is a simple spiroid fracture rima, with torsion mechanism, at times the subjectof delayed diagnosis

8 The Pelvis and Lower Limbs
8.3The Ankle and Foot
8.3.1Lesions of the Ankle Region
169
The ankle is one of the most frequent sites of trauma and, although injuries are oftenligament lesion s, the radiologist often has an important role to play in diagnosis . Thedistal tibia has a wide artieular surface, a large medial mall eolu s, and a sma ller posterior mall eolu s; the astragalar dom e is a wedg e that is wider anter iorly. The dist alperon eal extremity, or peroneal mall eolus, is linked to the tibi a by means of the anterior and postero- inferior tibiofibular ligam ents, by an inferior tran sverse ligament ,and by a syndes mosis . The peron eal malleolus is linked to the astragalus by the anterior and posterior talofibular ligaments and to the calcaneus by the calcaneofibularligament. The tibial mall eolu s is linked to the astragalus, to the calcaneus, and to thescaphoid, by mean s of the superf icial and deep parts of the delto id ligam ent.
In the case of lesions, there is tumefaction and pain and it is impossible to put weighton the limb. Clinical reports are similar both in the presence of a ligament lesion and inthe presence of a fracture. It is there fore essential to carry out an X-ray, which must beperformed in A-P, L-L projection and with intrarotated oblique projection of about 20°( "mortar" projection) . In rare cases, other examination s such as CT are useful for making a better spatial assessment of the position of a fragment of dislocated fracture , oralternatively ultrasound with a dynamic technique during maneuve r of the anterior "cassette" if there is a suspected lesion of the lateral ligament s (Fig. 8.18). In the case ofcomplex ligament lesions or osteochondral lesions, MRI may be useful.
Ankle lesion s may occur with four mech ani sms (Weber s classification) :supination-abduction (Weber A) init ially causes a lesion of the later al ligaments,the calcaneo fibul ar ligament at fir st, with transverse fractu re of the perone almalleolus; secondly, because of the impact , the abducted astragalus causes anobl ique fracture of the tibi al malleolussupination-extrarotation (Weber B) is the most frequent mechanism, which causesfour sequential lesions: lesion of the anterior-inferior tibiofibular ligaments; secondly, oblique fracture of the fibula and fracture of the posterior malleolus; and lastly,transverse fracture of the tibial malleolu s and lesion of the deltoid ligament. Thesemay be associated (in 38% of cases) with lateral lesion of the astragalar domepronation-abduction (Weber C I) causes three sequelae of lesion s: ten sion of theprofound portion of the deltoid ligament and transver se fracture of the tibialmalleolus; lesion of the tibiofibular ligament; and lastly, obl ique fracture of thefibul ar malleolus; a distance gre ater than 5 mm between the tibi a and fibu la, inthe A-P projection or the mortar suggests a lesion of the syndesmosispronation-extrarotation (Weber C2) cau ses four lesion s in sequence : the fi rst twoare the same as the previou s fracture of the tibi al mall eolu s and the lesion of thesyndes mosis; next is oblique or spiroid fracture of the f ibula , on average 6-8 emabove the syndesmosis; and lastly, fracture of the posterior malleolus

8
170
k~l -'
ATREST
eTALUS~
ANTERIORDRAWER SIGN
D.Barbuti etal.
Fig.8.18 Lesion of the lateral ligaments of the ankle. a Stress X-ray shows abnormal opening ofthe lateral joint rima (arrow). b During maneuver of the "anterior cassette", the X-ray showsabnormal anterior translation of the astragalus with respect to the tibia. c, d Ultrasound shows theloose appearance of the ligament, which is invaginated towards the capsule in the anterior cassette(arrow). e Diagram of the procedure for dynamic ultrasound
the Maisonneuve frac ture (Weber C3 ) is a spiroid fract ure of the proximal thirdof the f ibul a, ass oc iate d wit h a lesion of the t ib iof ibul ar syndes mosis and a lesion
of the inter osseous memb rane. It is ass ociated with a frac ture of the tib ial mall eolu s or a lesion of the deep portion of the delto id ligam ent. The mechanism is notexactly clear ; probably the start of the sequence is fracture of the internal mall eolu s. Diff icul t to diagno se, it has the same sig nificance that Galeazzi andMonteggia fractures have in the upp er limb .
Fracture of the tibial p illion is often comminuted and involves the tibi al , medial ,and posterior mall eoli but without involvement of the articular surface.
Among the various type s of tibi al epiphyseal det achment, distal ep iphysealdet achment is the mo st common in the lower limb. It is generally caused by entra pment of the foot in the spokes of a bicycle wheel or occurs as a result of a ska tingaccident. The mechan ism invol ves ext ernal rot at ion with a supine foot, whi ch leadsto type I and II Salter-Harri s lesion s, but all type s of Salter-Harr is lesion s may beencountered (Figs. 8. 19 and 8.20). Medi al fractures are the ones with high est risk ofdeform ity; the y are often diagnosed as type I or II Sa lter-Harr is lesion s but are act ually type IV lesion s with the risk of arrest of medial growth an d subsequent angul ardefo rmity (Fig. 8.2 1). For th is reason, a fractur e of the inte rnal tibial mall eolusshould be accuratel y studie d (Fig. 8.22) and, in the case of involveme nt of the growt h
carti lage, undergo surgical tre atme nt.

8 The Pelvis and Lower Limbs 171
Fig.S.19Type I Salter-Harris distal fracture ofthe tibia in an I I-year-old girl. a, b Widening of thedistal growth cartilage of the tibia without dislocation of the nucleus (arrow). c, d Healthy sidefor compari son
Fig.S.20Salter-Harris fractures of the ankle. a Type I Salter-Harris fracture of the distal epiphysisof the tibia with nucleus positioned ju st behind ; b comparison with the healthy side. c Type IISalter-Harris fracture, detached distal epiphyseal nucleus (white arrow) and oblique vertical fracture of the metaphysis (black arrow). d Type IV Salter- Harris fracture which involves the distalmetaphysis, the growth cartilage, and the epiphyseal nucleu s (arrow)
Fig.S.21 Early physeal fusion following Salter-Harris ankle fractures. a Healthy side; b results ofthe fracture with lesion ofthe growth cartilage: asymmetric fusion ofthe physis several years aftera trauma, resulting in serious varism of the talocru ral joint. c Partial fusion of the growth cartilage in another patient after a trauma with negative X-ray report. d Healthy side for comparison;e after 4 years and osteotomy performed to correct the axis, a clear hypometria is visible.Lengthening for growth purposes is planned

172 D.Barbuti etal.
8Tillaux frac ture is a typ e III Sa lter- Harris lesion wh ich affects th e lateral half of
the ti bi al epi physeal nu cl eu s in pre-adolescen ce, the phase in wh ich ce ntral c los ure
of th e carti lage begin s (Fig . 8 .23 a, b) .
Fig.8.22 Pediatric internal "malleolar" fractures. a Fracture rima of the tibial malleolus extendedto the physis; axial CT scan (h) and coronal CT reconstruction (c) show how, in reality, it is a typeIII Salter- Harris fracture. d Apparent detachment of the tibial malleolus; coronal CT reconstruction (e) and 3D reconstruction (t) show the extension of the fracture rima to the phsyis and thedistal metaphysis of the tibia: in reality, it is therefore a type IV Salter- Harris fracture
Fig. 8.23 Tillaux and triplane fractures. a X-ray of Tillaux fracture; b CT shows the level of diastasis of the detached fragment; corona l (c), sagittal (d), and 3D (e) reconstruction of the triplanefracture

8 The Pelvis and Lower Limbs 173
The tr iplane fracture is a type IV Salter-Harris lesion and also appea rs in preadol esc enc e with a mechanism of exte rna l rota tion, postero-lateral displacem ent of
the lateral portion of the epiphyseal plate, or forc ed plantar flexion and ax ial compression of the metaph yseal region (Fig . 8.23c- e) .
8.3.2Fracturesof the Foot
At birth, the calcane us and the astragalus are the onl y tar sal bon es to be ossified. Thecuboid ossi fi es after a few months and, at the end of the fi rst yea r, so does the later
al cunei form. Th e scaphoid is the last tarsal bon e to ossify and the tarsal nucl ei areall present between 3 and 4 yea rs, but the conformation similar to that of an adult
onl y begins at the start of the sec ond decade. At the start of development , the bon esare more oval and less multifaceted ; the calcaneu s sti ll lacks Bohl er 's angle and the
sinus tar si has not developed . The greater elas tici ty and abundance of carti lage mak esfractures of the tarsal bon es rarer ; they are gen erally onl y caused by viol ent traumas
on the road , fa lls of shar p obj ects, or obj ects from a great height, onto the foot. Th efoot represents the ana tomica l site with the large st number of access ory bones; it isessential to have knowledge of all the se to avoid mi staken diagnosis of a parcel bonedet achment (Fig. 8.24) and also bec ause the same access ory bone may be sympto
matic and the site of a pathology.
22
0-- - -1-- 15
Fig. 8.24 Supernumary bones that are more frequent in the foot: 1 tibiale externum; 2 scaphocuneiform; 3 intercuneiform; 4 second cuneo-metatarsal; 5 first cuneo-metatarsal; 6 intermetatarsal;7 tarso-metatarsal; 8 os vesalium; 9 cuboideum secundarium; 10subfibula; II talotibial; 12supratalar; 13 supra-scaphoid; 14 sub-scaphoid; 15 trochlea of the calcaneus; 16 os trigonum; 17 subtibial bone; 18 talus accessorius; 19 sustentaculum tali; 20 talus secundarius; 21 intercalary fibula;22 os retinaculi

8
174
8.3.3Fractures of the Astragalus
D.Barbuti etal.
The se are rare and are due to falls in forced dorsiflexion. Diagno sis should be carried out with X-ray, but sometimes CT may prove necessary, for complex fractures orfor a better assessment of the displacement of fragments .
Four type s can be distinguished according to the Hawkins classification:type 1: without or with minimal disloc ation . These are treated with reduction, ifnece ssary, and immobilizationtype 2: posterior disloc ation of the body and area of medi al fragmentation .Reduc tion is generally obtained using surgery; it is important to re-es tablish thecongruency of the subas tragalar articulationtype 3: posterior dislocation of the body, often with internal rotation of 90° andentrapment of the posterior tibial tendontype 4: with dislocation of the neck and the astraga lar-scaphoid articulation.
In the absence of fracture, or if displacement is minim al, treatment should beconservative. In the case of greater displacement or unstable reduct ion, it may benecessary to create interna l fixation with a thin screw. A possible complicati on isischemic nec rosis, especially in children over 10 years old ; this generally occur s 6months after the trauma .
The "Shepherd's" fracture affects the lateral tubercle of the posterior process andmay simulate an os tr igonum. Osteocondrial detachment of the astragalar dome maybe medial, gene rally larger in size, but less symptomatic , or lateral. Diagnosisrequires an X-ray with A-P, L-L projections and oblique int rarotated projec tion (mortar projection). MRI is useful in these forms of fracture, for assessing cartilage damage and the pain of the adjoining osseous spongi osa. Treatment should generally beconse rvative but surge ry may be necessary if there is no response within 6 months.
8.3.4Fractures of the Calcaneus
These are more frequent, linked to serious falls (e.g. from a tree) and, because of theviolence of the impact, may be associated with fract ures of the rach is and/or the otherfoot. The main types of frac ture of the calcane us are the following: fractures of thetuberos ity, of the sustentac ulum tal i, and of the body, without involvement of the subastraga lar region, and fract ures caused by compressi on of the body, involving thesubastragalar region. There may be "toddler's" frac tures in small children under3 years old, due to modest trauma, and these are difficult to diagnose. In older children,stress fractur es are possible, thou gh rare. Patholo gical fract ures are possi ble on preexisting focal osseou s lesions of a lytic type or in the case of osteopen ia-rel ated diseases, such as imperfect osteogene sis or in cerebropathic children.
Wiley's classification is the most commonl y applied in pediatrics. It distinguishestwo types:

8 The Pelvis and Lower Limbs 175
Fig.8.25 Calcanear fracture with thalamic depression in a seven-year-old boy. a X-ray; h, c CTshows more clearly the displacement; d follow-up after synthesis with screws and cast
type I : without invol vement of the subastragalar articulation ; it includ es A, abeak; B, vert ical; C, hor izontal ; D, avuls ion of the medial rim ; E, fracture of theant erior processtype 2: with involvement of the subastragalar articulation ; it includes A, simpl e;B, "tongue" fracture with opening up to the calc aneal apophysis; C, centrolateralwith displ acement; D, of the sustentaculum tali (Fig . 8.25); E, comminuted.
In non-compound fractures, treatment involves immobilization with the footraised, which is suff icient; heal ing take s place in 6 week s, but with proh ibition ofweight-bearing on the limb for a further 4-6 weeks. In compound fractures, especi allyin adolescents and if accompanied by depression of Bohler 's angle, surgicalosteo synthesis is necessary.
8.3.5Fracture of the Scaphoid
This is a rare and generally not a compound fracture. "Toddler's" fracture of thecubo id may occur in children und er 3 year s old due to relatively mod est traum a, andis difficult to diagnose.
8.3.6Lisfranc Fracture
This is a fracture with luxation of the midfoot, first described by Dr Lisfranc , a doctor who served in Napoleon Bonaparte 's army, in a horseman who fell from his hor sewith his foot trapped in the stirrups. It may occur due to tors ion of the foot in a holeor in sports injuries , and may appear in young people as a navicular-astr agal ar luxation without fracture (Fig. 8.26) . X-ray exami nation in the dorso-plantar, lateral , andoblique proj ect ions shows lateral luxat ion of metatars als II -V, which dev iat e frommetatarsal I with possible fractures of the cunei forms or the metatar sal bases .

176 D.Barbutiet al.
8
Fig.8.26Scapho-talar dislocationina l3-year-old boy due to a fall during a basketball match. a, b FirstX-ray. c Follow-up after reduction
Treatme nt of th is fracture, if the dislo cat ion is less th an 2 mm , involves immobi liza
tion and rest for 6 weeks. In the case of greater displ acement, int ern al surg ica l fi xa
tion is necessary.
8.3.7Fractures of the Metatarsals and Phalanges
These are linked to a di rec t tra uma (Fig . 8.27) or a we igh t fall ing onto the foo t.
Marching f racture of the second metatarsal is one of the mo st freq uent stress frac
tures ; in th e foot , th is may also occur in th e cuboid and the ca lcaneus . Fracture of the
base of the fi fth metatarsal (Jones f racture) occurs due to a trauma in inversion of the
forefoot, often ca us ed by avuls ion of the short fi bula, and may be ass ociated with a
le sion of the lateral ligaments of the ank le . In these event s, it is necessary to make a
di fferenti al diagnosis with the access ory nucleus of the base of the fift h metatarsal ,
a frequent variant (Fig . 8.28). Beside s cl in ical treatment and loc al tumefaction, it is
necessary to take account of the fact th at the avulsion fracture is of a transverse type ,
while the nucleu s is placed longitudinall y.
Fig.8.27Type 1\Salter- Harris fracture of the base ofthe distal phalanx of thebig toe during karate training in a nine-year-old boy.One can observe the fracture of the distal epiphysisof the proximal phalanges2nd and 3rd ray

8 The PelvisandLower Limbs
Suggested Readings
177
Fig.8 .28 Fracture of the Vmetatarsal base in comparison with secondary nucleus ofgrowth . a Fracture ofthe base of the fift hmetatarsal. The fracture hasa transverse course (red ar
row) and is associat ed withtumefaction of the soft tissues (white arrow); b thesecondary nuc leus ofgrowth of the base of thefifth metatarsal has a longitudin al course (arrow)
Azour EM, Karamitsos C, Reed MH et al (1993) Types and comp lications of femoral neck fractures in children. Pediatr Radiol 23:415-420
Canale ST, Bourland WL (1977) Fracture of the neck and intertrocanteric region of the femur inchildren. J Bone Joint Surg 59:43 1-443
Chia JP, Holland AJ, Little D, Cass DT (2004) Pelvic fractures and associated injuries in childre n.J Trauma 56(1):83-88
Connolly JK (1988) Fratture e lussazioni. Verduci editore, RomaHeeg M, Visser JD, Oostvoge l HJM (1988) Inju ries ofthe acetabular triradiate carti lage and sacro
iliac joint. J Bone Joint Surg Br 1:34-37Holden CP, Holman J, Herman MJ (2007) Pediatric pelvic fractures. J Am Acad Orthop Surg
15(3):172-177Ismail N, Bellemare JF, Mollitt DL et al (1996) Death from pelvic fracture : children are different.
J Pediatr Surg 31( I):82-85Letourne l E, Judet R, Elson R (1981) Fractures of the acetabulum. Springer-Verlag, New YorkOgden JA (1990) Skeletal injury in the child. WB Saunders Company, PhiladelphiaReichard SA, Helikson MA, Shorter N ( 1980) Pelvic fractures in childre n - review of 120 patients
with a new look at general manageme nt. J Pediatr Surg 15(6):727-34Salter RB (1974) Injuries of the ankle in children. Orthop Clin North Am 5(1):147-52Schlickewei W, KeckT (2005) Pelvic and acetabular fractures in childhood. Injury 36 [Suppl 1]:57-63Spiguel L, Glynn L, Liu D, Statter M (2006) Pediatr ic pelvic fractures: a marker for injury severi-
ty. Am Surg 72(6) :481 -4Swischuk LE (1994) Emergency imaging of the acute ly ill or inj ured child, 3th edition . Williams
& Wilkins, BaltimoreTile M (1995) Fractures ofthe pelvis and acetab ulum, 2nd editio n. Williams & Wilkins, Baltimore,
pp 41-52


9.1Introduction
It is rar e to detect a traum atic bon y lesion in a very small child. In the f irs t two or
three years of life, children are constantly chec ked by a responsible adult, and the
incidence of skeleta l traum a is low. Instances of traum a include:
obstetri c pseudo-paralysis"bir th fractures "
acci dents that often occur in the nursin g infant , such as fall s from the changingtable, which are often the cau se of cranial fract ure
events that also involve the person caring for the child, such as accidenta l fall s
or, in particular, road accidents
non- accidental lesion s, which include the condit ion of "ba ttered child syndrome"
"toddler's fractures" , or fractures that occur when the child is walking with an
unc ertain gait.
9.2Obstetric Pseudo-paralysis
Obstetr ic pseudo-paralysis includes traumati c lesion s of the cartilage of conj ugation ofthe long bones of the limbs, with chondro-epiphyseal separation, that is Salter- Harr is
type I fractures, which are caused by the maneuvers of del ivery and birth.
C. Defilippi ( ~)
Pediatric Radiology Service, Regina Margherita Children's Hospital, Turin, Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
179

180 C. Defilippi et al.
9
Fig.9.1 Anterior longitudinal ultrasound scan of the hip. a Normal position of a non-ossifiedfemoral epiphysis (arrows); b epiphyseal displacement (Salter- Harris type I fracture)
The diagno stic value of ultr asonography in incomplete separations (Fig. 9.1) isparticularly impor tant in the uppe r limb, where the absence of signs of ossificat ionof the growth nucl ei of the humerus mean that x-r ay examination is of limited value,and may only give positive signs of fractu re after a week, when signs of calci f icationof the reparative callu s appear.
Proximal chondro-epiphyseal separation of the humerus is the most frequentform of obstetric pseudo-paralysis, and is likel y to occur in any birth where it is necessary to subje ct the limb to an axial tract ion of 60 kg or more.
Distal chondro-epiphyseal separation of the humerus, on the other hand, is veryrare, and can easil y be confused clin ically with a paralysis of the brachial plexu s and,at x-r ay examin ation , with a disloc ation of the elbow. The lesion is the result of a violent movement of hyper extension of the elbow.
Manual breech extraction can be linked with the appearance of a proximal chondroepiphyseal separation of the (incomplete or complete) f emur, with or withoutperiostal laceration.
The knee is rarely involved during obstet ric maneuvers, with dista l chondroepiphyseal separation ofthe fe mur; all the described cases refer to shoulder or breechpresent ations.
9.3"Birth Fractures"
" Birth fractu res" frequently occur in cases of breech presentation, shoulder dystoci a,macro somi a, or rapid delivery because of fetal distre ss. They can also occur duringcesa rian section.

9 Birth Trauma 181
The clavi cle is the bon e mo st affected, usual1y the middle th ird (Fig 9.2).Fractur es of the distal clavicle are occasional described but are more frequent in
cases of non-accidental trauma.Birth fracture of the clavicl e may be complete or incomplete, and is oft en an
occas ion al find ing dur ing a chest rad iograph y perfo rm ed for oth er reasons (Fig. 9.3) .Ultrasonography can replace radiogra phy, avoiding ionizing radiation (Fig. 9.4).
Th e differential diagnosis includes conge ni tal peudoarthritis and non-acc identalfrac ture but birth fracture is always chara cterized by an exube rant cal1us.
In al1 birth frac tures the cal1us form s early and is voluminous.
Fig. 9.2 Newborn (11 daysof age) birth fracture. Radiograph of the clavicleshows an exuberant callus
Fig. 9.3 Newborn. Chestradiography. Occasionalfinding of birth fractureby the right clavicle

182 C. Defilippi etal.
". b-a
_..~~~. _.~~'W!~..J.' -:.'--~ _.• .-;iT'~ ... - -~ - . ._ , ......~ C .--..- -'......~~_,.~~...... ,;.~:.?"_:.: .~~/;::;;i-~.'O'-c::........ - . , --- -'- ,~""'" .. .,.' , .._, r:> ". .._.....:i'\. .- .:" , " ', '-.-- .. _ -#'-~........... '.~
';~ ~
~....
9
Fig.9.4 Newborn . Ultras onography of the clavicle. a Birth frac ture (arrows) ; b exuberant callus (ar rows)
Th e rep air processes are cl earl y vis ible radiographicall y 7- 12 da ys after birth.
A fracture without si gns of bone re pair in a chi ld o ld er than II days of age is sus
pi cious of non-accid ental injury.
Salter -H ar ri s typ e I and II fr actures arc characteris ti c of femur an d humerus birth
fractures .
Sometimes there ar e multiple r ib fractures th at can re sult in severe re spiratory
sym ptoms.
Suggested Readings
Behrman RE, Kliegman RM, Jenson HB, eds. (2000) Nelson textbook of paediatrics 16th ed,Philadelphia, Pa: Saunders; 455-456
Glass RBJ, Fernbach SK, Norton KI et al (2004) The Infant Skull: A Vault of Information. Radiographi es March 24:507-522; doi: I0.1 I48/rg.242035 I05
Radkowski MA, Merten OF, Leonida JC (1983) The abused child: Criteria for the radiologic diagnosis. Radiographies June 3:262-297

10.1Introduction
The incl usive age between 10 month s and 3 years is denominated "toddler age",because of the typical hopp ing and uncertain mann er in which the child walks,moving autonomously without the direct control of an adult.
In th is period, speci fic fractures of the inferior extrem ities arc common, as aresult of fall s that submit the bon es of the limb to torsion al , hyperexten sion , orimpact traum a.
10.2The Concept of Toddlers' Fractures
The original de scription of "toddler's fracture" (Dunbar et aI., 1964) concerned apart icul ar type of spiroid fra cture of the tibi a, which is difficult to detect on thebasis of a medical hi story comparing a clinical and physic al evalu ation with theevent s leading to the pre sentation .
An objective picture that is almost exclusively rep resented by a moderate limpor refusal to walk often occurs in the pre sence of other bone lesion s of the infe rio rlimb , which can be included in a wider con cept of "toddlers' fractures" and includepart ial fra ctures from imp act (cuboid and calc aneus) and hype rextension fra ctures("buckle" fractures of the base of the fir st met atarsal prox imal tibi a, or distal segment of the fibula and tibi a).
C. Defilippi ( ~)
Pediatric Radiology Service, Regina Margherita Children's Hospital, Turin, Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
183

184
10 10.3Imaging
C. Defilippi etal.
Radiographic chara cterization of these fr ictur es is not often easy, especially in theacute phase immediately after the trauma, although later on (aft er about a week) , theappearance of phenom ena indicating hea ing, often exuberant, facilit ate definitionof the frac ture . However, thi s may present problems with different ial diagno sis, particularly in the case of non-a ccid ental inj uries, and lead to delays in diagnosis andtreatm ent because of the non -spec ific ity I ,f the medical histor y. The presentation isdominat ed by symptoms of pain , spon taneous or provoked, that is invariablyreferred to the ank le region. This is fund unental ly signif icant and is at the root ofthe problem of clin ical identification of 1he possible locat ion of the fractur e. Nonspecific radiography of the ankle joint wi II not necessarily give a corr ect diagno sisunless the projections are specifi cally ada otcd to the type and location of the lesion.
It is advisable to put in plac e a protocol of clinical evaluation to adequatelydir ect the radiographi c investigation, taking account of a series of fundam ental evaluations:
submitting the limb to an accurate inspect ion, looking for pain ful swellings ofthe soft tissues, which are gene rally pre sent in fractures of the base of the firstmet atarsalgrasping the knee and ank le, imparting a tor sion al force on the leg to indic atethe presence of a spiroid fracture of the tib iasubmitting the knee to hyperextension to assess any suspicion of a "buckle" fracture of the proximal tibi acompressing the ankle, tarsus at the cuboid, under the first metatarsal and theheel , in an attempt to evoke a specific pain ful reaction that is characteristic of"toddlers' frac tures" .The clinical evaluation is fundamenta l, not only to ident ify the area of radio
graphic interest but also to address the choice of technique for the investig ation .Certain specific radiogr aph s are essent ial to underline part icul ar lesions, such astangent ial projections for impact fractures of the heel.
Spiroid fra cture of the tibia is generally represented by a thin hyperlucent line(Fig. 10.1), which may extend to include the whole skeletal segment but is alwaysvisible at the level of the distal thi rd of the bone .
Late radiogr aphs of "toddler's fracture" can determine the onset of a violentperiosteal reaction (Fig. 10.2) that can cause problems of differenti al diagno sis withboth non- accidental injuries and infl ammatory pathologies such as osteitis andosteomyeliti s, as well as Ewing's sarcoma and leukemia.
"Buckle fractures" are characterized in the acute phase by a light imprint of theskeletal pro file from depression of the cort ical border on the vent ral side of the bonesufferi ng con sequent hyperextension trauma (Fig. 10.3) . A radial line of fracturebecomes evident later, on the oppo site side, because of the low density of the fracture and its margins, with the appearance of porous canc ellou s bone adjacent to thewidespread perio steal reaction.

10 Toddlers' Fractures
Fig. 10.1 The radiograph shows a spiroidfracture of the tibia (ar row)
Fig.10.3 Buckle fracture of the distal tibia(arrow) . The oblique radiograp h shows alight imprint of the skeletal profi le fromdepression of the cortical border
185
Fig. 10.2 Toddler's fracture of the tibia. Theradiograp h, performed 19 days after injury,showed a diffu se diaphyseal perio stea lreaction
Fig. 10.4 Toddler's fracture of the cuboid. The areaof the trauma looks slightly flattened and sclerotic(arrows)

186 C. Defilippi etal.
10In contrast , "toddler's f racture cuboid" , is ins te ad re pre se nted by a subchondral
fracture of th e dorsal slope of th e cuboid, wh ich is difficult to identify and appe ars
as a light depress ion of th e profile; at a lat er stage, a condition of marginal scle ro
sis in th e imm ed iat e area of th e trauma is al so appa rent. Th is is a subc ort ical fra c
ture resulting from calcaneal-c ubo ida l impact , which will heal spontane ous ly and so
do es not requ ire specific diagnost ic investigation s. Th e use of spec ific ima gingtechniques such as sc intig raph y or magnetic resonance ima ging is reserved for
ex ce ptiona l cases (Fig. IDA) .
It is int eresting to note that osteochondrosis affects not th e cuboid, and th e areaof osteitic processes and osteo arthrit is is locat ed at the ventral surface at th e joint
with th e meta tar sal base .
Suggested Readings
Dunbar JS, Owen HF, Nogrady MB et al (1964) Obscure tibial fracture of infants - the toddler'sfracture. J Can Assoc Radiol 15:136-144
John SO, Moorthy CS, Swischuk LE (1997) Expanding the concept of the toddler's fracture. Radio-Graphics 17:367-376
Swischuk LE, John SO, Tschoepe EJ (1999) Upper tibial hyperextension fractures in infants: another occult toddler's fracture. Pediatr Radiol 29:6-9

11.1Introduction
First of all a fir st fundamental distinction must be made between lesions resulting
from a single act of phy sical violence and tho se occurring as a result of physical
maltreatment. We are better able to clarify the distinction using the definitions pro
posed by the Itali an Penal Code:
physical violence (art.572 c.p): "harmful action that immediately produces an
acute physical effect and requires an urgent interv ention"
physical maltreatment: "r epeated behav ior lead ing to suffering in the vict im, and
resulting in a relation ship with the person responsible that is characterized by
pain".
The definition of phy sical violence also includes the condition termed "shaken
baby" syndrome, characteri zed by serious lesions of the central nervous system
induced by a maneuver of violent sha king and abrupt decelerat ion caused by impact
of the bod y of the baby on a soft surface such as a mattr ess or pillow.
11.2The "Battered Child": Imaging
In 1860, Ambroise Tard ieu described a series of traum atic lesion s in very small ch il
dren from an anatomical-pathologica l and physic ian-legal point of view; the se
lesion s had common characteri stic s, resulting from phy sical maltreatment, and were
C. Defilippi ( ~)
Pediatric Radiology Service, Regina Margherita Children's Hospital, Turin, Italy
Imaging of Pediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
187

188 C. Defilippi et al.
11often accompanied by signs of lack of material care .
Fifty-five per cent of the cases described involved subjects younger than 5 yearsand 30% of these were in children aged under one year. In over 70% of cases, thelesions were intentionally caused by the parents (by both parents in about 35%), andrapid improvement was observed after removal of the child from the household .
In 1946, Caffey not iced in children of a very young age the frequent associati onof chronic subdural hematomas with traumatic lesion s of the long bones of the limb sthat had been ignored or were not adequate ly explained by their parents or the person responsible for their care.
Kempe, in 1962, propo sed definitions for these cases , which are widely usedtoday: "batte red child syndrome" otherwise known as "syndrome of AmbroiseTardieu", or "syndrome of Caffey-Silverman" .
A definition that perhaps more closely reflects the real ity of the situation is thatgiven by the acronym PITS ("parent- infant trauma syndrome"), while the anatomical-pathologica l product of th is specific form of physical malt reatment is more correctly defined by the term "non-accidental traum atic lesions".
The cl inical presentation is dominated by mult iple and compl ex manifestat ions ofsigns that are observed in addition to the skeletal lesions:
brui sing, scratches, burn s, scorching from cigarette s, and other cutaneou s lesions;contu sive defo rmit ies such as the so-called "boxer nose"a general state of lack of physical carelesions of the nervou s systemlesions of the thoracic and abdominal organs.Skelet al damage cannot always be confirmed, but when it can , extreme care must
be exercised in reaching a diagno sis. In only 50% of cases does the subject presentfor clin ical observation in relation to the presence of a fracture, but the suspicion ofphysical maltre atment is nevertheless indic ated by potenti ally non- accident al skeletal injury.
For child-protection reasons, in cases where reliable clini cal-phy sical information is not avai lable, the use of bone scintigraphy can be ju stif ied, balancing thepanoramic view it offers against the dose of ionizing radiation. Although very sensitive, scintigraphy is neverthele ss non-specific and provides little detail of morphology,which, if damage is confirmed, can be obtained by conventional radiology directedat the area(s) of clinical inte rest.
Recogn ition of metaphyseal frac tures is compl icated by the intense uptake ofradioactive indicator by the actively grow ing metaphysis; however, these representthe most typi cal type of injur y.
It is reasonable to assume that if there is suspicion of physical maltre atment insubj ects aged under two years, a radiograph ic examin ation of the whole skeleton isalways necessary.
Between two and five years of age, the choice to assess the whole skeleton by x-raydepends on the indiv idual case, while in children aged over f ive years, whole-bodyx-ray is only used in exce ptional circumstances
There are several reasons for this:

11 Bony Lesionsfrom Non-accidentalTrauma 189
one-th ird of subjects are aged less than one yearmetaph yseal lesions, which are often difficult to diagno se, usually involve theyoungest childrenin infant s and toddl ers, lesions are often not readily apparent and can be underestimated or undetected by parents and relativeschildren aged five years can effectively defend themselves and can give deta ileddescriptions of lesions, as well as being able to accurately point to the center ofpain.Limiting the dose of ionization is a major consideration , and can be achieved by
util izat ion of investigat ive proc edures that maximize the rad iograph ic field of view.It is recomm ended to use large-fo rmat or wide-projection radiog raphs (labeled
"babygrarn s") , becau se those of lower quality are of littl e use for diagno stic purposes; furthermore, in most cases, because of the inadequacy of the find ings, they resultin an unjustified increase in rad iation dose. A high-quality image is esse ntia l in thesecases, to avoid false-negative results, which are extre mely dangerous as they mayprevent removal of the child from the fam ily, thus promoting the recurre nce of crimewith potentially tragic consequences.
The f irst-level imaging is therefor e represented by conventional radiog raphy,supplemented later by additional methods such as ultr asonography to assess the softtissues and mon itor developmental processes in the form ation of bony callu s or tostudy cert ain type s of fracture s such as those of the epiphy ses.
Magnet ic resonan ce imaging (MRl) investigations constitute second-level imaging for the evaluation of articulations and soft tissues, and to search for poss ible hidden frac tures (not identif iable with convent ional radiology alone, although they maybe suspected on the basis of the scintigra phy), or, in particular, for monitor ing andevaluating possible disabling sequelae.
Complex fracture s in particular location s (such as the face and skull base) insteadrequ ire the use of computerized tomog raphy.
Finally, the importance of post-mo rtem imaging must not be overlooked, particularly conventional radiogra phy of the whole skeleton.
The fir st fundamental task, represented by the detection of lesions, requires theradiologist to address a series of issues that are basic to correct organization of thecase:
identi fic at ion of fractures at sites that are considered to be character isticsearch for particul ar anatomical-radiological characteri stic s in fractures that areothe rwise non- specificassessing the date of occurrence of each individual lesion that is verifieddescription of the possible rel ationship between characteri stic s of the lesion andthe type of prec ipitat ing traumatic eventpred ictive assessment of possible disabling consequencesdifferential diagnoses.This is, of course , a complex task, and one that the rad iologist can only achi eve
by full collaborat ion with all oth er pro fessional s involved: the cl ini calpatho logist/anatomist, the psychiatr ist, the coron er, and the judge .

11
190
11.3Fractures in Specific Anatomical Sites
C. Defilippi etal.
In ver y small ch ildre n, some typ es of fracture are highly unlikely to be accidental ,
th is includes fract ures of th e:
shoulde r blade and acromiondistal th ird of the clavicl e
branches of the ilium, ischi um, and pubis (Fig. 11.1 a)
femoral ne ck (Fig . Il.l b)
tubular bones of the super ior and inferior extremities
vertebra l bodies (Fig . 11.2) .
Fig.11.1 a Fracture of the branches of the ischium and pubis (arrow). b Femoral neck fracture
Fig. 11.2 Newborn. Fracture of a lumbar vertebralbody (arrows)

11 Bony Lesionsfrom Non-accidentalTrauma 191
Corre ct visualization and inte rpre tat ion of these lesion s it is esse ntial to addressthe suspici ons raised when the type of improbable justification proposed by the relatives is highl y indicat ive of a cond ition of physical maltreatm ent.
11.4Fractures in Non-specific Anatomical Sites,with Particular X-rayCharacteristics for Dating of Fractures
A diaphyseal fracture , generally of the humerus or femur, is often present, but has no specific characteristics as it is relatively common in children of this age (for example injuryfrom the bars of a cot). This type offracture is, however, also frequent in cases of maltreatment, while evidence of repair processes is also indicative of a lack of care (Fig. 11 .3).
It should be noted that diaphy seal fractu re, along with crani al traum a is one of themo st frequent reas ons for hospit al ization of young children , and is often accompanied by other more specif ic lesion s, often from a different time , and not alwaysdeclared or adequately justi f ied by the family. Mult iple lesion s of different date ,inco rrectly interp reted on the basis and source of explanat ions of acc idental injury,form the basis of most cases of suspected abuse .
The dating of the lesion therefore ass umes a fundamental importance and isesse nt ially based on the findings of a relatively typical pattern of evolut ion:
bevel ing of the bord ers afte r a weekincrease in density beginning from two weeksappea ranc e of new periosteal reaction spec ifically with in four weeksiniti al signs of ossification after around one mon thremod eli ng of the traumatic area beginn ing from about ten weeks.
Fig.11.3 Untreated and not recent fracture ofthe humeral diaphysis (arrows). Exuberantand irregularcallus.Angledand overlappingfragments

192 C. Defilippi etal.
11Salt er-Harr is fractures (lesion s of the grow th plat e with epiphysea l separation) of
appendic ular bon es are oft en found , especi ally in infants; these are generallySalte r- Har ris type I (without direct involv ement of the metaphyseal or epiphysealcomponent) . This type of lesion , which has a preference for the hum erus and theproximal femur is, nevertheless, also non- specific and is commonly present in accidental fo rm, as "birth fracture" or as a result of man euvers of incorre ct nur sing.
The separation, which in the initi al stages is a short distance from the traum a, isclinically suspected, but is diff icult to prove without radiographic evidence of ossif ication at the epiphyse al growth nucleus. Under these cond ition s, ultrasonographicexami nation has a crucial rol e, facil itati ng a safe and timely diagnosis (Fig. 11.4) .
In thi s particular type of fracture, periosteal and reparative calcium depo sitiononly lead to a signif icant radiograph fi nding 10-14 days after the time of inju ry. Ina suspici ous contex t, a finding of an exaggerated osteocalc ification react ion can beindicative of neglect.
Frac tures of the skull are also very frequent in these cases, but are of littl e use inconfi rma tion of suspected "batte red child" as they lack specificity. Cranial fracturesare very common in all chi ldren aged und er two yea rs, but , in the absence of neurolog ical con sequences, are frequentl y underestimated.
Comparison of chroni c subdura l hem atomas, in ass ocia tion with recent int racranial bleeding and bony lesion s (even if from a different date) gives significantinfo rmation in the suspicion of "Caffey- Silverman" syndrome.
Fig.11.4a Ultrasonographyof the distal femoral metaphysis in infants with chondro-epiphyseal separation (Salter-Harris type 1\ fracture). b Corresponding diagram

11 Bony Lesionsfrom Non-accidentalTrauma 193
The cond ition of "s haken baby", the result of a single violent action, is notinclud ed in this type of investigation, although it can fit into a broader contex t ofphysical abuse .
Corre ct dat ing of a linear fracture of the skull is undert aken meticulously; thehyperlucent line identified by convent ional radiography may still be identifiable 6 or12 months after the traumatic event, although the other radiog raphic signs are nonspecific:
pseudo-diastasis of the fracture, by reabsorption of the edgesexaggera tion of the bord ers in relation to the phenom enon of ossificat ion of thecallu sprog ressive gradient of hyperluc ency.The use of more sophistica ted methods such as MRI add s littl e to the possibility
of dat ing this type of frac ture .
11.5Fractures with Particular Radiographic Characteristics
Some form s of traumatic lesion of the child skeleton assume a fundamental importanc e in the radiograph ic diagnosis of physical maltr eatm ent , and they are alwayssought and carefull y evaluated since they are very useful for defining a presumedlink between the type of lesion and a definite cause .
Metaphyse al fragmenta tion, cort ical hypero stosis, and "cup'l-type deformation ofthe metaph ysis are highl y specif ic result s, particularly in childr en who are youngerthan 3 years of age.
Thi s generally concern s lesion s that do not have broad clin ical-ph ysical manifestat ion s, and as such they are often not recognize d by the parents or care rs, who, whencon front ed with their presence, either propo se improbable explanations or confesswhat happ ened.
The cause is generall y a concussion or compression trauma, which is exacerbatedby the insti nctive reaction of the child facilitated by the particular anatomical conform ation of the child's periosteum . In children, and particularly in infants, theperiostium covers the metaph ysis and is intimately connected to the physis where itmerges with the perichondrium.
Thi s favors verif ication of specific metaphyseal fractures, such as the so-called"corne r lesion s" (Fig. 11 .5) and "bucket-handle" fractures (Fig . 11.6).
These traumatic metaphyseal fragmentations can be dated with some precision ,because, as they are already evident immediately after the trauma, they follow a specific patt ern of repa ir charact erized by progr essive cortical periosteal reaction which ,in less than 20 days, lead s to fusion of the fragme nts with subsequent coalescence(Fig. 11.7).
The extent and repetitiveness of the traum a, as well as the absence of suitablecare , facil itate the persistence of gro ss reparative features and the appearance of amet aphyseal cupping (Fig. 11.8).

11
194
Fig.11.SRadiograph ofthe knee. Newborn withmetaphyseal lesions by non-accidental trauma.Metaphyseal "corner lesions" (arrow). Femora land tibial metaphyseal fragmentation
Fig. 11 .7 Battered chi ld . Radiograph of thetibia performed 13 days after the trauma showsmetap hyseal fragmentation sequelae with progre ssive coa lescing (arrows)
C. Defilippi et al.
Fig.11.6 Radiograph of the knee. Newborn withmetaphyseal lesions by non-accidental trauma.Femoral and tibial metaphyseal "bucket-handle" fracture s (arrows)
Fig.11 .8 Radiograph ofthe tibia shows cuppingdeformation of the tibial distal metaphysi s(arrows)

11 Bony Lesionsfrom Non-accidentalTrauma 195
Deformation of the metaphysis develops slowly over weeks and months, andfavors the persistence of perman ent and disabl ing side effec ts such as bend ing andasymm etry of the limb s.
The periosteum of a child is characterized by stong osteogenic activi ty in the cortex and an exuberant germ ination layer, whos e function is to ass ure rapid axialgrowth of the skeleta l segment.
It is not infrequent , especially in premature subje cts, and particul arly dur ing thesecond and third month of life, to see radiograph ic evidence of so-ca lled "periosteallines" at the level of the diaph ysis of the femur, hum eru s, and tibia , which are thephysiological express ion of poor adherence and exuberance of periosteal proliferation; these tend to progressively coalesce with the underlying cortical sur fac e andmust not be con fused with pathological man ifestation s of periosteum.
A periosteum with these anatomical-functional characte ristics is par ticularlyfragil e and easily detaches. Dissect ion of the hypervascul arized osteogen ic layer ofcortical bon e from the surface of the cortical bon e results in frequent subperiostealhemorrhages. This detachm ent and subperiosteal hemo rrh age follow ed by agg ressiveosteogenesis can , with repeated episodes of traum a, lead to establishment of form sof external cortical hyperosto sis, which are sometimes so marked they form largecalci fied diaphyseal "sleeves" (Fig. 11.9) . The form ation of coarse and voluminou s"sleeves" takes severa l week s.
Rib fractures (Fig. 11.10) , which are very frequent , should be ana lyzed with spe-cial attention to sea rching for highly specif ic aspects :
multipl icitybilate ralitylocationdifferent dating .
Fig. 11 .9 "Battered childsyndrome". Widespreadperiosteal newbone depos it ion around thefemoral diaphysis (blackarrows) and metaphysealirregularit y and fragmentation of the distalmetaphysis (white arrows)

196 C. Defilippi etal.
11
Fig.11.10 Chest x-rays of the battered childs. a Scattered and multiple rib fractures date differently. b Another case. The oblique projection shows a recent fractures located near the posterior ribarticulations (arrows)
The child frequently presents in a situation of cris is , with inconsolable cryingass ociated with respiratory di fficulty. The presenc e of multipl e fractures, of differentdat e, in different regions of the thoracic ribs determines the onset of pain with everybreath , assoc iated with a redu ction in the elas ticity of the tho racic wall.
The frequency and depth of the respiratory actions progressively reduces , resulting in stagnation of sec retions and the appearance of dysventilatory events, infectiou s phenomena, and ult imately dyspnea and serious respiratory insuff iciency.
Specific fractures are located at the posterior costal arch, since the energy ofshaking trauma is discharged near the costal- ver tebral junction, i.e. at the point ofgreatest rigidity. However, characte ristic frac tures are also located along a line atmid- axillary level of the front and rib cart ilage, ma inly in associ ation with crushingtraum as.
Non-rece nt fractures are invariably characteri zed by coarse and volum inou s bonycalluses that extend to formation of mult inodular "beads" .
11.6Differential Diagnosis
The contribution of the radiologi st is essenti al to avoid hasty judgments or incorrectdiagnosis, which can have serious con sequences in such a del icate context as that ofchild physical maltreatment.
The non-radiographic diagnosis of accidental bony lesion s is largely a diagnosisof exclusion, and as such asks for a suitable collabora tion among the variou sinvolved exper ts, in light of a careful evaluation of the attitude and the statements oftheir parent s, of family memb ers, and of tho se accompanying the child.

11 Bony Lesionsfrom Non-accidentalTrauma 197
The principal differenti al diagnoses are represented by the following pathologies:defect ive osteogenesisinfantile cortic al hypero stos isdysmetabol ic bone disease of premature infantsMenkes diseaserickets associated with vitamin D deficiencyrickets not associated with vitamin D defi ciencycong enit al syphilisscurvycong enit al insensitivity to pain.
11.6.1Defective Osteogenesis
Defect ive osteogenesis is manifested by qualitative and quantitativ e alteration of collagen with involvement of different gene loci , and is characterized on the basis ofpattern s of expressi on, of varying gravity. These may be subdivided acco rding to avariety of classif ications, one of which is the four-stage classification proposed bySillence.
Lethal (type II to lib), severe (type III and some expression s of type II), andregressive (type la, Ib, IV) form s are described .
The problems of differential diagno sis hardly concern the lethal forms, which areoften diagno sed in utero on the basis of ultrasonog raph ic evidence of spontaneous fractures before birth , or shortening or deformation of the limbs, and related to possibleisolat ion by amniocentesis of the responsible gene or related biochemical alteration.
In subjects who are affected, the generali zed struc tura l rarefaction is very evident , as skeletal deformation s and mult iple fractures, charac ter ized by exuberant calluses, which determ ine a "bamboo-reed" feature of the long bones of the limb s. Somevar iable cha racteristics of the illness may, however, lead to incorrect inter pretations:
cerebral hemorrhages, hematomas, hemarthrosis, and ecchymosis of the softparts, cap illa ry fragi lity, and platelet abnorma litiesareas of circum scribed cutan eous aplasia, with app earanc e that is simi lar to sma llulcerations or foci of scar tissuejoint dislocations as a result of capsulo-ligamentous laxitydiffuse hypotonia.The following can create great diffi culti es for interpretation of skeletal lesions in
some non-l ethal form s:mult iple costal fractures of different datingdiaphyseal fractures from different dates with exuberant callu s and signs of inadequate carefractures of the vertebra l bodie s.The disorder also includes lesions that are occasionally found, which are under
estim ated, for which the dyn amics and trauma are uncle ar, and for which an unconvinc ing explanation is given.

11
198 C. Defilippi etal.
Fig.11.11 Newborn. Defective osteogenesis. Babygram front (a) and lateral(b) projection. Scatteredand multiple rib fracturesdate differently, fracturesof the vertebral bodies,"bell aspect" of the thorax, thinribs and horizontal cotyloid roofs
Som e clinical signs , which are oth erwi se typical , are not always present :blue scleracharacteri stic facieshearing problem s.The same genetic diagno sis present s problems of interpretat ion and is obt ained
with difficulty.Bone loss, with reduction in cortical thickness, hypo-ossification of the skull and
the presence of wormian bones are frequent radiographic obser vat ions.In a signif icant number of cases, the radiograph ic examination of the skeleton
gives eviden ce of a narrow che st , thin rib s, stumpy ili ac wings, and hori zontal cotyloids (Fig. 11.11). In absolute term s, the defective osteogenesis represent s the mo stcommon differenti al diagnosti c question in cases of suspicion for "battered child" .
11.6.2Infantile Cortical Hyperostosis (Illness of Roske-De Tone-Caffey-Silverman)
Infanti le cortical hyperosto sis is a form of del ayed chondro-perio stal hyperosteoge nesis that is alread y present in utero, for which an early diagno sis is possiblearound the fi fth month of pregnancy, by ant enatal ultrasonograph y.
The syndrome, is however, usuall y diagnosed later, within the f irst two years oflife.

11 Bony Lesionsfrom Non-accidentalTrauma 199
Fig. 11.12 Newborn. Infantile cortical hyperostosis. Hyperostosis of the tibial diaphysis
Clinically the illness causes swelling and deformation of the limb s, edema, andpain of the soft parts, vari able degrees of impai red general health , fever, andincr eased erythrocy te sedime ntation rate and alkaline pho sphatase.
The illness has a slow but ben ign evolution, with regression of bone lesion s without sign ificant sequelae .
Identific ation of events of hyperostosis of the long bones of the limbs (Fig. 11.12),but also of some flat bon es such as the shoulder blad es and the jaw, is esse ntial fordiagnosis.
11.6.3Dysmetabolic Bone Disease of Premature Infants
Dysmet aboli c bone disease of prem ature infant s leads to many radiographic manifestations that can lead to problems of diffe rent ial diagnosis:
angular fractu res of the met aphy seal cortexsubperiosteal hem atom ascalci fied "s leeves"diaph yseal fracturesepiphyseal detachmentrib fracturesdefo rmations of the "cup " of the chondro-costal junction .

200 C. Defilippi etal.
11The illness is classified into four stages (0 to 3, based on increasing levels of
severi ty) and fractures only appear in the more seve re forms , cor respond ing to stage3, while in all oth er stages the condi tion is clinically silent. All subjec ts are, however, preterm infants and have low weight for ges tationa l age . Radiog raphic evidenceshows diffuse loss of bone, which has a spongy trabecular appearance, and there ischaracteristic involvement of the bones of the skull.
There is also involvement at metaphyseal level, with heightened irregularity ofthe area of provisional calcific ation and the fi nding of typical "si ckle-shaped spurs" .
Ultrasonogra phic assessment of the level of bone mineral ization may be usefulfor a defin itive diagno sis.
The disease is determin ed by an insuffici ent supply of minerals, parti cularlyphosphorus, result ing in a calcium defici ency of bone. However, high levels in theblood calcium and alkaline phosphatase, and insufficient levels of phosphorus in theblood are not constant.
11.6.4Menkes Disease
In Menke s disease, loss of structural bone density, associated with metaphy seal andcortical hyperosteal alterations and associated genetic characte ristic s (sex-linkedrecessive transmission) , are man ifested as:
a defi cit of copp er absorptionalterat ions of the ar teriesmicrocephal ywormian bonesabnormaliti es of the hai rhypotonia, convulsionsstatural and mental retardation.
11.6.5Rickets
In the variou s form s of rickets, which are characterized by blood chemistry and fromparticular genetic evaluations , the main observation is of fragmentation of the metaphyseal car ti lage of the long bones of the limb s in comparison to lesion s that involvethe metaphyseal cortex.
In rickets the diaphyses are bent and curved and undergo angular fractures, often"gree nstick", which never completely break. The reparative callus is usually extuberant,but littl e calcifie d, and it ossifi es slowly.
Periostoti c "sl eeves" and "shells" develop late and are mildly calcif ied.

11 Bony Lesionsfrom Non-accidentalTrauma
11.6.6Congenital Syphilis
201
Congeni tal syphi lis is also a pathology that is con stantl y increasing in industri alize dcountries (0 .5/10 cases in eve ry 100,000 live births) , and is determ ined by the transmission of Treponema pallidum from the infected moth er to the fetu s through the placenta dur ing the period of incubation (from 10 to 90 days), or dur ing the pr imary andsecondary stage of infec tion.
The illness is rarel y already app arent at birth; the symptoms mor e often appearaft er some months and are determ ined by involvement of a large proportion oforgans, part icul arl y the liver, splee n, kidneys, pancreas, and skele ta l apparatus.
Osteolytic areas with blurred margins appear in the flat bon es and skull. The epiphyses of the appendicular bon es are typ icall y spare d, while at diaphyseal level thereis ev ide nce of periostosis, cor responding to variou s struc tural modificat ion s of themetaphyses, which can be observed in conjunction with alterations of trop ism withtransverse rad iotr ansparent band s, and erosi on and fra gmentation of thick enedpro cesses.
The destructive lesion s are painful and acc ompanie d by hypomobilit y of all theaffected limb s (particul arly the uppe r limbs) , within a picture known as pseudoparalysis of Parrot.
Also characteri stic is the appearance of destructive changes located at the symmetrical level of both tib ias, on the metaphyseal med ial side, known as the sign ofWimberger (Fig. 11.13) .
Fig. 11.13 Infant with congenital syphilis. Radiographof the lower limbs showstypicalerosivechangesat themetaphyseal proximal tibia (Wimbcrger sign)(arrows)

202 C. Defilippi etal.
11Ce rta in di agnosis is a lmost ex cl usi vely obtained from serologi cal inv estigations,
th at allow mea surem ent of spe cif ic anti bod ies, such as Treponema pallidum hem ag
glutin ation (TPHA), fluorescent treponem al antibody-absorb ed ( FTA-ASS), and par
ticularly th e immunoglobulin (Ig) FTA-ASS IgM , wh ich det ect s anti bodies produced
exclusively by th e fetus.
Th e exami na tions that are more widely avai lable such as Ven ereal Disease Research
Laboratory (VORL) and rapid plasm a reagin (RPR) do not exclude fal se-posit ive
results (although values ra ised fourfold in comparison to maternal value s are very
indica tive), sin ce positive results can re fle ct transplacental pass age of maternal IgG.
11.6.7Scurvy
Scurvy is a ve ry rare d isease caused by a defici ency of vitami n C, which can occa
sion ally pr esent in th e neonat e or very young ch ild . It induces alte rations in ske le ta l
features, suc h as met aphyseal den se lin es of Frankel and ra di o luce nt ar ea s (sites of
pathological fracture) , or angular spur s (spurs of Pelkan) in th e re cove ry ph ase. Th ere
is associa ted diffuse subperios tea l hemorrhage, and appear ance of periosteal sleeves .
Suggested Readings
Augarten A, Laufer J, Szeinberg Act al (1993) Child abuse, osteogenesis imperfecta and the greyzone between them. J Med 24:171-175
Caffey J (1946) Multiple fractures in the long bones of infants suffering from chronic subduralhaematoma. AJR Am J Roentgenol 56:163-173
Carty H, Pierce A (2002) Non-accidental injury: a retrospective analysis of a large cohort. Eur Radiol 12:2919-2925
Kempe CH, Silverman FN, Steele BF et al (1962) The Battered Child Syndrome. J Am Med Assoc181:17-24
Mendelson KL (2005) Critical review of temporary brittle bone disease. Pediatr Radiol 35: I0361040
Miller ME, Hangartner TN (1999) Temporary brittle bone disease: association with decresed fetalmovement and osteopenia. CalcifT issue Int 54:137-143
Paterson CR, Burns J, McAllion SJ (1993) Osteogenesis imperfecta: the distinction from child abuseand recognition ofa variant form. Am J Med Genet 45: 187-192
Ruess L, O' Connor SC, Quinn WJ et al (2003) An animal model for the classic metaphyseal lesionof child abuse. Pediatr Radiol 33:s I 12
Tardieu A ( 1860) Etude medico-legale sur les sevices et mauvais traitement exerces sur des enfants.Annales d'hygiene publique et de medecine legale, Paris, 13:361-398
Williams RL, Connolly PT (2004) In children undergoing chest radiography what is the specificity of rib fractures for non-accidental injury? Arch Dis Child 89:490-492
Zimmerman S, Makaroff K, Care M et al (2005) Utility of follow-up skeletal surveys in suspectedchild physical abuse evaluations. Child Abuse Negl 29: I075-1083

12.1Introduction
Child abuse is a top ical issue in modern society and has socia l and medic al implic ations
that directly conce rn the doctor, both as a private citizen and as a health professional.The varie ty and the pecul iarit y of abuse injuries, as the World Health
Organization decl ares [I] , requires a mult idisciplinary and multispe cialty approac h,which must beg in with an accura te med ical examination whe re diagno stic imaging
becom es esse ntia l. The radio log ist, by identifyi ng the chi ld abuse , has great responsibility in conn ect ion with three basics:
identificat ion of traum at ic injuriesdifferential diagnosis between accidenta l inj ury and abuseuse of the opt imum investigationa l imaging method to prove the exis ten ce of
inj ury.
Aside from cases of sexual violence and abandonment/negligence of a child,whe re the radiologi st can make complementary inquiries for diagno sis, batte red
child syndrome represent s one of the most typical forms of ill-treatme nt of child ren,characteri zed by micro - and macro-traumas inflic ted using natural means (such as
the hand s, feet, elbows, and so on) or other objects (sticks, belts, chains, etc) . The setraum as result in different kinds of injuries (ecchymoses, lace rated and contusedwounds, luxations, fractures) to the mu sculoskel etal sys tem, which clearly show thepresence of abuse . As long ago as 1946, the Radio logist Caffey was the first who
found and described new types of fracture and osseou s lesion s obser ved in batte redchildren, especi ally among younger children [2] . Later , in 1962 , Kempe and cowork-
M. Solarino ( ~)
Section of Radiology, "Fallacara" Hospital, Triggiano - Sari, Italy
Imaging ofPediatric Bone and Joint Trauma. Fabio Martino et al. (Eds.)© Springer-Verlag Italia 20II
203

204 M. Solarino andB. Solari no
12ers coined the expressi on "battere d child syndrome" by revea ling in advance thefuture guidelines [3-5]. With th is definit ion they grouped together the cl inical andradiologica l signs that characterize the phenom enon of beaten children. Since then,many other reports in international scientific journal s have shown different aspectsand model s of this kind of abuse, to draw the attention of the medical community tothe problem, which, althou gh steadily escalating, had been totall y disregarded [6-10].
Today there are some internati onal examples of guidelines and standards of procedure relating to the radiologis t's role in the presence of a suspected "battered childsyndrome" . The American College of Radiology drew up some guidel ines to categorize radiological inquires according to the age of the child « 2 years, >5 years) andto the presence or absence of physical or neurological symptopatology (Box 12.1)[II]. Magnetic resonance (MR) is a useful method for investig ating a child under theage of 2 years, becau se at that age it is easy to detect the presence of a direct traumatic brain injury (by blows or by a fall). On the other hand, the use of the computed tomog raphy (CT) of the skull in a "battered child" older than 5 years is a valuablemethod for revealing subdural interhemispheric hemorrhages as a consequence ofshaking inj ury.
A prel iminary objective examination of the child must ant icipate a radiodiagnostic survey. The rating used to evaluate the relev ance of the radiological investig ationperformed in relat ion to the clinical pictu re and to the age of the child, shows that thesurvey of diagno stic investigat ion must be carried out on a case-by-c ase basis, ifchild physical abuse is suspected.
If there are suspicious non- accident al injuries to children, the Brit ish Society ofPediatric Radiologists recommends adopting standard procedures [12] : there are several investigations, all of which need an initial clini cal evaluation of the child. It isimportant to focus attention on the qualit y of the radiod iagno stic instrument used(such as digital radiology, with extreme caut ion regarding techn ical paramete rs relating to the radiobiological danger), and the importance of involving competent healthpersonne l. The main characte ristics of these procedures are:
attention to the importance of a panoramic radiologica l investigation, if there issuspicion of abuse, by focu sing attention on specifi c anatomical areasa "real" collaborat ion between radiology technicians and the radiologis t duringthis kind of investigation, for radiological proceduresthe possibil ity of using control investigat ion some weeks later, if there are suspicious abuse injuries (such as costal fracture s).
The protocols propo sed by the Section of Radiology of the Americ an Academy ofPediatrics [13] are very interesting for two reasons. On one hand they show the utility of panoramic radiology of the skeleton, in cases of suspicious violence to childrenunde r the age of 2 years; on the other hand, they decl are the importance of a goodevaluation of possible thoracic-abdominal injur y: this kind of localization could belinked to an abuse injury. In addition to the useful different ial diagnosis betweenaccidental injury and abuse, the protocol s provide for the performanc e, in the firstins tance , of a CT examination (tho rax and abdomen) and a subsequent controlthrough ultrasonography of the abdom en.

12 The Battered Child:Guidelines and Medical-legal Implications
Box 12.1 ollege of Radiology:physical child-abuse [II]
R appropiatcncss criteria. uspcctcd
205
Fir 'I scenario: child 2 years ofage. or younger: with clinical suspicion ofabuse, billwithout any evident focal signs or symptoms
The most basic imaging examination is the skeletal survey. characterized by frontaland lateral views of the skull and a single frontal view of the long bones of the lateral vertebral column. and thoracic and abdominal frontal view. Oblique radiographsof the ribs. by detecting fractures as a consequence of abuse. are part of the initialskeletal survey. A 1R of the skull could be a valid instrument for a legal documen
tation of the abuse.
Second scenario: child 2 year ofage, or YOl/I/ga, with cranial trauma, bill withoutanyevident 'igll ofneurotogicul abnormalltyA skeletal survey is recommended in the event of a clinical suspicion of abuse. Ifitappear ' negative. but there is a high suspicion of abu sc. a IR of the encephaloncould be appropriate for the legal documentation of abuse. MR is more sensitive than
T in detecting and dating brain parenchyma trauma ' without radiation exposure.
Third scenario: child 1/1' 10 5 y ears old with neurological signs and symptoms, and asuspicion ofabuse with or without any other injuriesA careful clinical assessment is essential. A non-contrast T scan of the brain shouldbe performed if the child presents neurological traumas . If the scan does not showsignificant lesions needing a neurological intervention. the child should be stabilizedand. if necessary. an urgent MR study of the brain with sequences in T I and T2. inaddition to an inver 'ion recovery should be required by the neurologist. If thc child'sclinical condition i. constant but there are neurological symptoms (transient loss ofconsciousnc 's which conditions the alteration of mental statu '. retinal hemorrhage),
IR represents the first diagnostic investigation for evaluation .
Fourth scenario: child ofany age with iuspicious visceral injuries tha) are inconsistent with the clinical hi .tory and/or a clinical examination ora laboratory .1'1111(1' andwithout lilly satisfactory explanationThi: requires an abdominal and pelvic T with contrast medium (or an echography)and a TI IR of the encephalon. ome vi .ccral injuries would include: pancreaticpscudocysts. hemorrhage of the suprarenal capsules. bowel perforation (after blunttrauma). contusions or laceration of viscera. or traumatic bladder perforation. In this
selling. all of these injuries should be considcred signs of abuse. ome radiologistsprefer not to usc oral contrast for the T study: however, there is no clear documcntation of the superiority of either technique: therefore. the issue of oral contrastshould be left to the discretion of the radiologist.
What was stated earlier is only one example of the main directions the radiologistfollow s during diagno sis of child abuse. It stands to reason that, in "battered childsyndrome" , a traum atic action of much gre ater gravi ty could include every anatomi-

206 M. Solarino and B. Solarino
12cal region. As well as the age of the child, the site of trauma and clinical confirmation of possible pre-existent or concomitant pathologies would condition the cho iceof appropriate radiodiagnostic tests, with the exception of panoramic radiography ofthe skeleton (known as "best inquiry") . As result, the use or not of contrast mediumfor the execution of a CT will depend not only on diagnostic suspicion, but also onits real purpose. In any event, the person who exercises parental authority orguardianship, in the event of a suspicious intrafamilial abuse, should give informedconsent.
It follows that such tests could lead to therapeutic treatment procedures and alsohave legal implications, in the event of tests for abuse.
12.2Current Regulations and Medical-legal Considerations
In 1990, the United Nations approved the Convention on the Rights of the Child. Aparagraph of the text titled "Protection from abuse and neglect" established that "TheState shall protect the child from all forms of maltreatment by parents or othersresponsible for the care of the child and establish appropriate social programs for theprevention of abuse and the treatment of victims" . In 2002 , the " Optional Protocolto the Convention on the Rights of the Child on the sale of children, child prostitution and child pornography" was approved which demanded (article 8) that all Stat eParties adopt appropriate measures against child abuse. In 2008 the main rights of thechild resolution was approved: in the third paragraph of the text titled "Eliminationof violence against children" it was specified that the United Nations "Condemns allforms of violence against children, including physical, mental , psychological andsexual violence, torture and other cruel , inhuman or degrading treatment, child abuseand exploitation, hostage-taking, dom estic violence, trafficking in or sale of childrenand their organs, paedophilia, child prostitution, child pornography, child sextourism, gang-related violence, bullying and harmful traditional practices" and urgesStates to strengthen efforts to prevent and protect children from all such violencethrough a comprehensive approach and to develop a multifaceted and systematicframework and strengthen legislation to prohibit and eliminate all forms of violenceagainst children . In Italy, as well as in many other west ern countries , legislationagainst child abuse and every kind of violence are already incorporated in the penalcode. The role preventing against this crime as demand by the United Nations is oft enattributed to physicians who are sometimes involved in such cases.
The entire medical profession, including radiologists, is bound by Italian law tocooperate with police authorities to prevent and combat crime. The protection ofhealth and the full respect of personal liberty are fundamental values guaranteed bythe Italian Constitution (art. 13,32). The medical profession must safeguard all citizens and, in particular, minors, against "intrafamilial childhood maltreatments" or"corrective measures abuse", as also stated in article 571 and 572 of the Penal Code(PC) as well as in articles 581 ("beating") and 582-583 ("personal injury") . In the

12 The Battered Child:Guidelines and Medical-legal Implications 207
event of maltr eatm ent , violence and abuse, the physicians have a fundam ental role inidenti fying such crim es and, as a consequence, avoid children still being the victimof their perpetrators. Art icle 32 of the Medical Deontology Code (2006) states thatthe doctor must protect child ren in cases of physical or psychological maltreatm entor sexual abu se, and in the event of oppo sition from the legal guardians, the doctormust report to the appropriate legal authorities.
Also, article 365 of the PC obliges all medical workers to notify the judicialautho rities whenever they have provided "assistance" or "care" in cases present ingthe characteri stics of an officially pros ecu table crim e. Thi s appl ies, for example, to aradiologist who identi fies signs of child abus e in his or her private or publ ic practice.Thi s obligation is even mor e comp ell ing if the specialis t works within the NationalHealth Service, where he or she acts as a public officer (ar t. 357 and 358 PC) and hasa duty to report any instance of crime that has been brought to his or her attention(art. 361-362, PC) .
Violation or neglect of this obligation is an offence against the administra tion ofju stice. Failure to compl y with this duty is malfeasanc e in office when it is ascertained that the health professional wilfull y and knowingl y fail ed to repor t or delayedreporting the crime.
12.3Conclusions
The phenom enon of child abuse represents one of the most top ical and, at the sametime, controversial subjects in modern soci ety. Too often we hear of presumed physical , psychological , or sexual child abuse based on psychological evaluations withoutany reference to the medical follow-up or specialist investigation s that couldunequ ivocally con firm or exclude this suspicion. The compl exity of child abuserequires a multidi scip linary, mult ispecialty appro ach in which the pediatr ic radiologist plays a key role. Pediatr icians or orthopedic surgeons are unabl e to interpr et theinjur ies identifie d on imaging studies. Only pediatr ic radiologists possess the competence to distinguish between accidental and abu sive injur ies. In fact, they have theknowl edg e to determine the time of mineralization of skeletal segments, recon structthe mechanism of injuri es in relation to the osteoarticular system, and interp ret imaging findings.
Reporting child abuse is invariably a very delicate question, especially becau se italways involves the families. Although a mere suspicion of abuse is sufficient for current regulat ions, the professional must be aware of the consequences of a misdiagno sisfor the famil y and the victim. Therefore, the radiologi st is required to addit ionally makean educated social judgement in evaluating the case in terms of collecting a compl eteclinical history and carefully interpreting the imaging findings. Implementation ofguidelines and protocols, together with cooperation between several specialists, willhelp produce a methodologically flawless evaluation of the true extent of this seriousproblem, which has been neglected and under- reported for too long .

12
208
References
M.Solarinoand B. Solari no
I. World Health Organization (2002) World report on violence and health. World Health Organization, Geneva.
2. Caffey J (1946) Multiple fractures in the long bones of infants suffering from chronic subdural hematoma. AJR Am J RoentgenoI 56:163-1 73.
3. Kempe CH, Silverman FN, Steele BF et al ( 1962) The battered-child syndrome. JAMA181:17-24.
4. Caffey J (1972) The parent-infant traumatic stress syndrome (battered baby syndrome). AJRAm J Roentgenol 114:217-225.
5. Silverman F ( 1972) Unrecognized trauma in infants, the battered child syndrome. Radiology104:337-339.
6. Loder RT, Bookout C (199 1) Fracture pattern s in battered children. J Orthop Trauma; 5:428433 .
7. Kleinman PK, Marks SC ( 1995) Relationship of the subperiostea l bone collar to metaphyseallesions in abused infants. J Bone Joint Surg Am 77:1471-1476.
8. Strouse PJ, Owings CL (1995) Fractures ofthe first rib in child abuse. Radiology 197:763- 7659. Mandelstam SA, Cook D, Fitzgerald M, Ditchfi eld MR (2003) Complementary use ofradi
ological skeletal survey and bone scintigra phy in detection ofbony injuries in suspected childabuse. Arch Dis Child 88:387-390.
10. Tung GA, Kumar M, Richardson RC, Jenny C, Brown WD (2006) Comparison ofaccidentaland nonaccidental traumatic head injury in children on noncontrast computed tomography.Pediatrics 118:626-633.
II. Slovis TL, Smith WL, Strain JD et al (2005) Expert panel on pediatr ic imaging. Suspectedphysical child-abuse. American College of Radiology (ACR), Reston (VA).
12. Bristish Society of Paediatric Radiology. Standard for skeletal surveys in suspected non-accidental injury (NAI) in children. http://www.bspr.org.uk/nai.htm (accessed 19January 20 I0).
13. American Academy of Paediat rics (2000) Section on radiology: diagnostic imaging of childabuse. Pediatrics 105:1345- 1348.
Suggested Readings
Akduman EI, Launis GD, Luisiri A (2005) Skeletal and viscera l radiological imaging. In: Giardino Ap,Alexander R (eds) Maltreatment: a clinical guide and reference, 3 edn. GW Medical Publishing, St Louis, pp 13-36.
Case ME, Graham MA, Handy TC et al (200 I) National Association of Medica l Examiners ad hocCommittee on Shaken Baby Syndrome: position paper on fatal abusive head injuries in infantsand young child ren. Am J Forensic Med Pathol 22:I 12-122.
Drvaric DM, Morrell SM, Wyly 18 et al (1992) Fracture patterns in the battered child syndrome. JSouth Orthop Assoc 1:20-25.
Introna F (2005) Gli obblighi giuridici del pediatra di fronte al bambino maltrattato, al minore abusato,all'i ncesto e altro. Zacchia 78:1-20.
Kleinman PK, Marks SC, Blackbourn e B (1986) The metaphyseal lesion in abused infants: a radiologic-histopathologic study. AJR Am J Roentgenol 146:895- 905.
Kleinman PK, Marks SC Jr, Nimkin K et al (1996) Rib fracture s in 31 abused infants: postmortemradiologic-histopathologic study. Radiology 200:807-810.

12 The Battered Child:Guidelines and Medical-legal Implications 209
Macchiarelli L, Albarello P, Di Luca NM, Feola T (2005) Medicina legale . Miner va Medica, Torino, pp 1215-1219.
Tenenbein M, Reed MH, Black OB (1990) The toddler's fracture revisited. Am J Emerg Med8:208- 214.