4th year gastroenterology lectures abdominal pain jaundice gi bleeding 4 th year gastroenterology...
TRANSCRIPT
44thth year Gastroenterology year Gastroenterology LecturesLectures
Abdominal painAbdominal painJaundiceJaundice
GI bleedingGI bleeding
Yasir M KhayyatMBcHB,FRCPC,FACP
Assistant Professor of Medicine
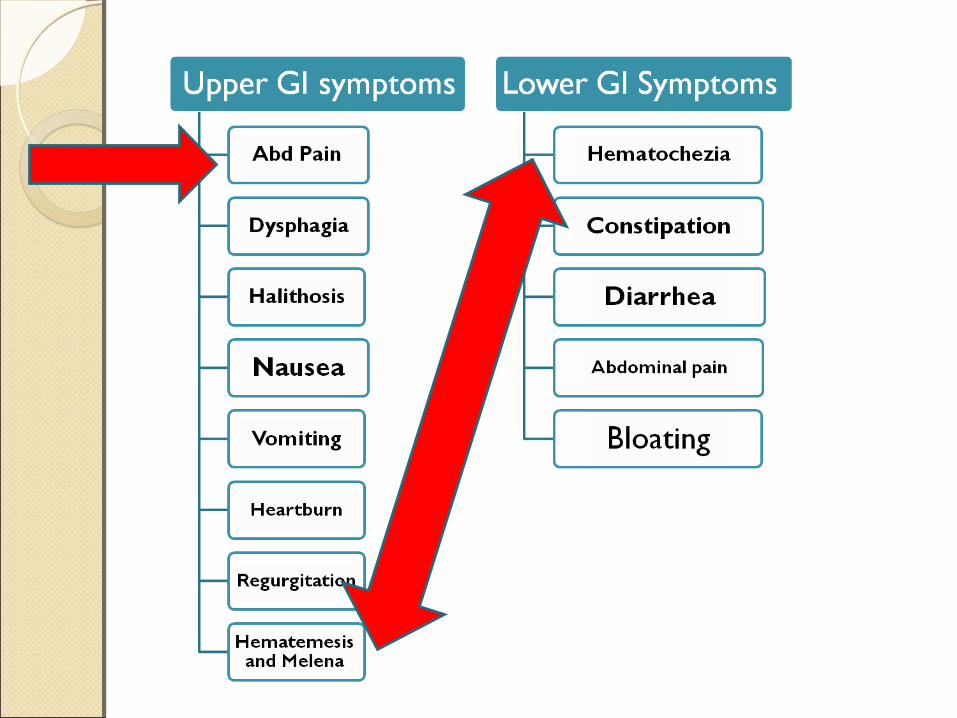
Objectives of approach to Objectives of approach to abdominal painabdominal pain
Recognize the appropriate analysis of abdominal pain and consistently apply it.
Understand the differential diagnosis of abdominal pain by location and patient setting.
Apply the necessary investigations pertinent to the presenting abdominal pain
Approach to abdominal pain
Clinical AssessmentClinical Assessment
Basic principles:Introduce yourselfKnow what system or disease type
you are evaluatingWrite downBe brief and focused
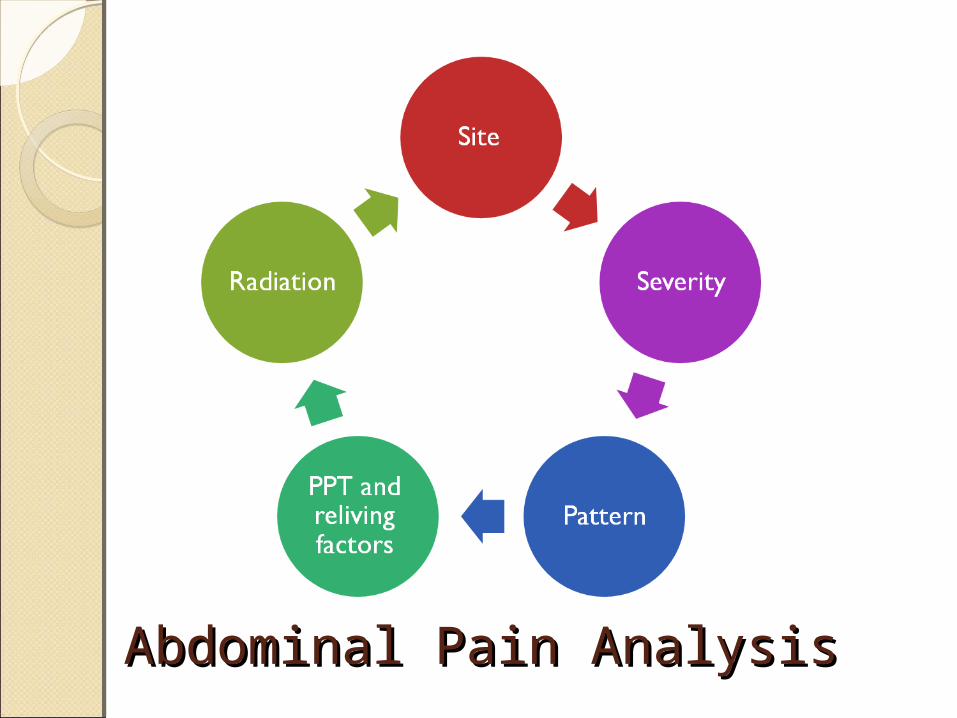
Abdominal Pain AnalysisAbdominal Pain Analysis
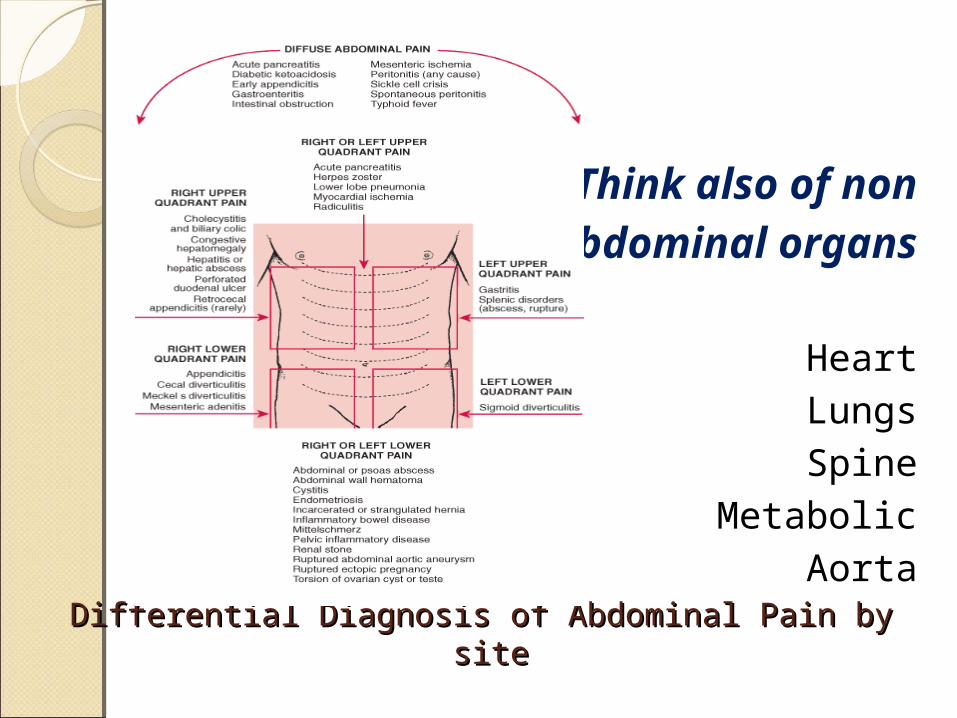
Differential Diagnosis of Abdominal Pain by siteDifferential Diagnosis of Abdominal Pain by site
Think also of non Abdominal organs
Heart LungsSpine
MetabolicAorta
Approach to Jaundice
Objectives of the approach to Objectives of the approach to JaundiceJaundiceRecognize the appropriate
analysis of clinical jaundice and consistently apply it.
Perform the physical examination necessary to elicit the diagnosis.
Prioritize the common causes of jaundice and apply it in investigations.

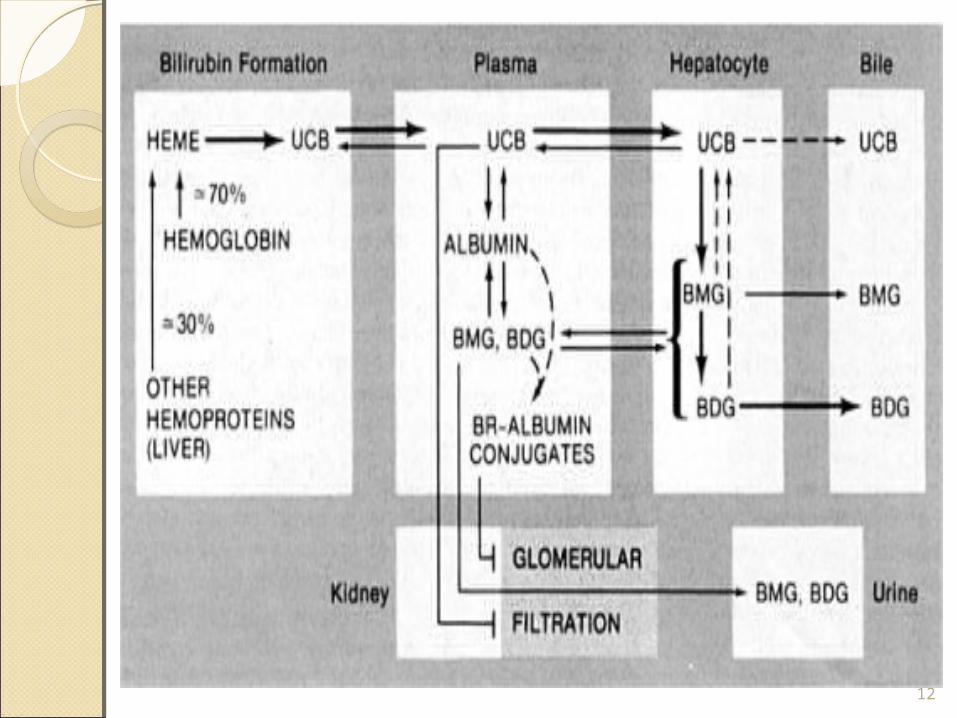
Yellow discoloration of the tissues caused by retention of bilirubin.( skin,sclera,mucosa)
Detected when serum bilirubin exceed 2.5-3 mg/100 ml.
Direct bilirubin undergoes postproduction processing in the liver ,this helps in differentiating between
Pre-hepaticHepaticPost-hepatic
Jaundice : definitionJaundice : definition
11
12
History: Age Onset Duration :short hx of
malaise,anorexia and myalgia= viral Long hx weight loss ,anorexia =
carcinoma Pregnant females Noticed: by the Patient/Relative Progression Associated Symptoms: fever: cholangitis Abdominal pain: gall stones,
pancreatic carcinomaviral prodrome
13

Past medical history: Hem-Liver,contact with febrile patient
Past surgical history: including post operative phase
Travel history Previous Drugs/Illict drugs,Alcohol
Previous GI Imaging or Lab works
Family history ( such as hemolytis disorders,wilson’s disease,Gilbert’s disease,alpha 1 antitrypsin defeciency ) 14
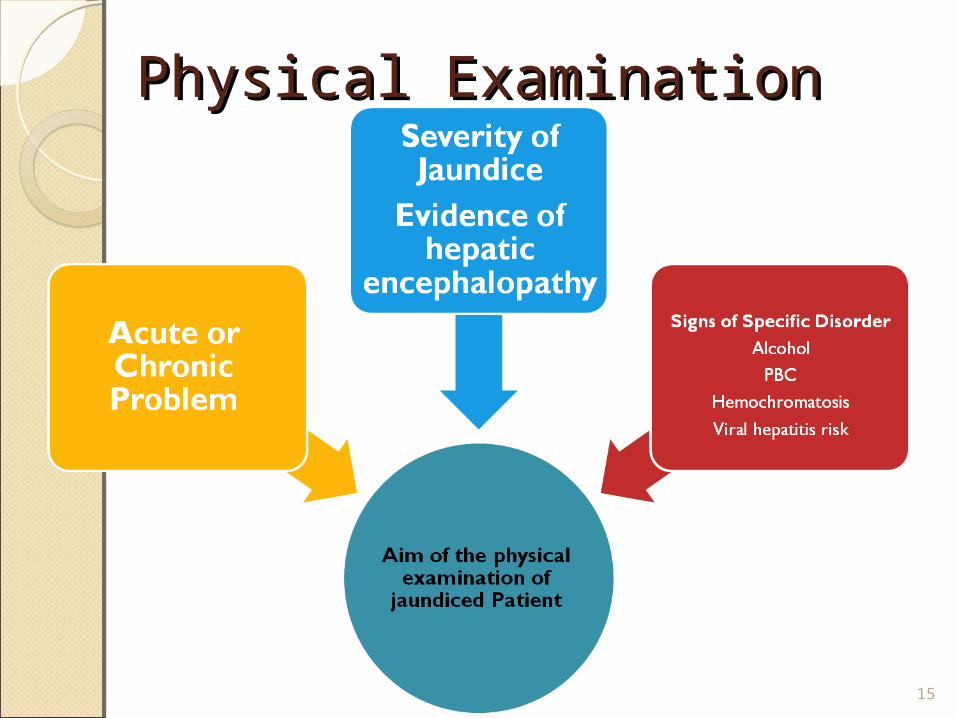
15
Physical ExaminationPhysical Examination
Physical examination:
General appearance : Wasted/Weak
Vital Signs Hands : Yellow, Clubbing, vasculitic
lesions,SBE Face : Malnutrition,Icterus,Fetor
hepaticus Trunk : signs of CLD Abdomen : Ascites,signs of
CLD,Splenomegaly,masses LL : LL edema 16
Isolated Disorders of Bilirubin MetabolismIsolated Disorders of Bilirubin Metabolism Congugated hyperbilirubinemiaCongugated hyperbilirubinemia Uncongugated hyperbilirubinemia Uncongugated hyperbilirubinemiaLiver DiseaseLiver Disease Acute hepatocellular dysfunctionAcute hepatocellular dysfunction Chronic hepatocellular dysfunction Chronic hepatocellular dysfunction Hepatic disorders with prominent Hepatic disorders with prominent cholestasischolestasis Jaundice in pregnancy Jaundice in pregnancy Jaundice in the postoperative period Jaundice in the postoperative periodObstruction of the Bile DuctsObstruction of the Bile Ducts CholedocholithiasisCholedocholithiasis Diseases of the bile ducts Diseases of the bile ducts Extrinsic compression of the bile ducts Extrinsic compression of the bile ducts
17
HemolysisViral hepatitisAlcoholic liver diseaseDrugsBile duct stonesPancreatic carcinomaLiver metastasis
Most Common causes of Most Common causes of JaundiceJaundice
18
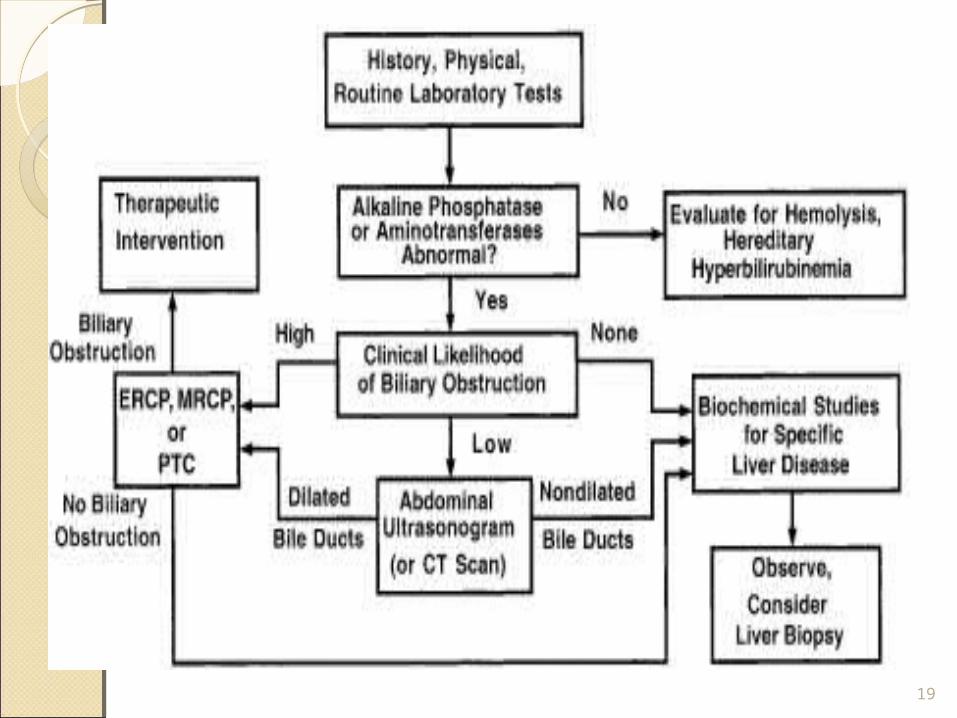
19

CBC : hemolysis ( Hb , Bilirubin ,LDH
LFT : AlK P, GGT
Hepatitis Virus serology : HBV ( HBsAg , HBeAg ) – HCV (HCV Ab ) – HAV ( IgM,IgG )
PBC ( AMA , IgM ) , PSC ( MRCP , ERCP )
Imaging Modalities : Abd US , MRI , MRCP
Jaundice Work upJaundice Work up
20

21
Tests to determine specific Tests to determine specific etiologyetiology

Approach to
Gastrointestinal
Bleeding
Objectives of approach to GI Objectives of approach to GI bleeding bleeding Ask the appropriate history and
perform the physical examination necessary to safely stabilize the patient .
Emphasize the importance of hemodynamic stabilization prior to proceeding with the endoscopy.
Refer the patient with GI bleeding to Gastroenterologist at the right time and on stable condition.
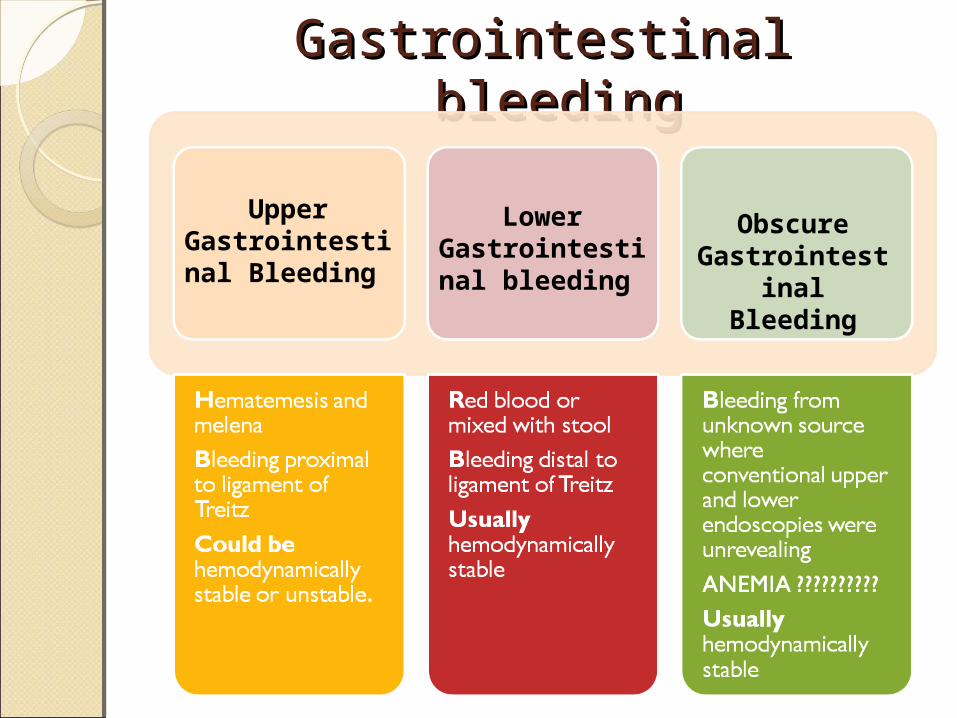
Gastrointestinal bleedingGastrointestinal bleeding
Upper Gastrointestinal Bleeding
Lower Gastrointestinal bleeding
Obscure Gastrointestinal Bleeding

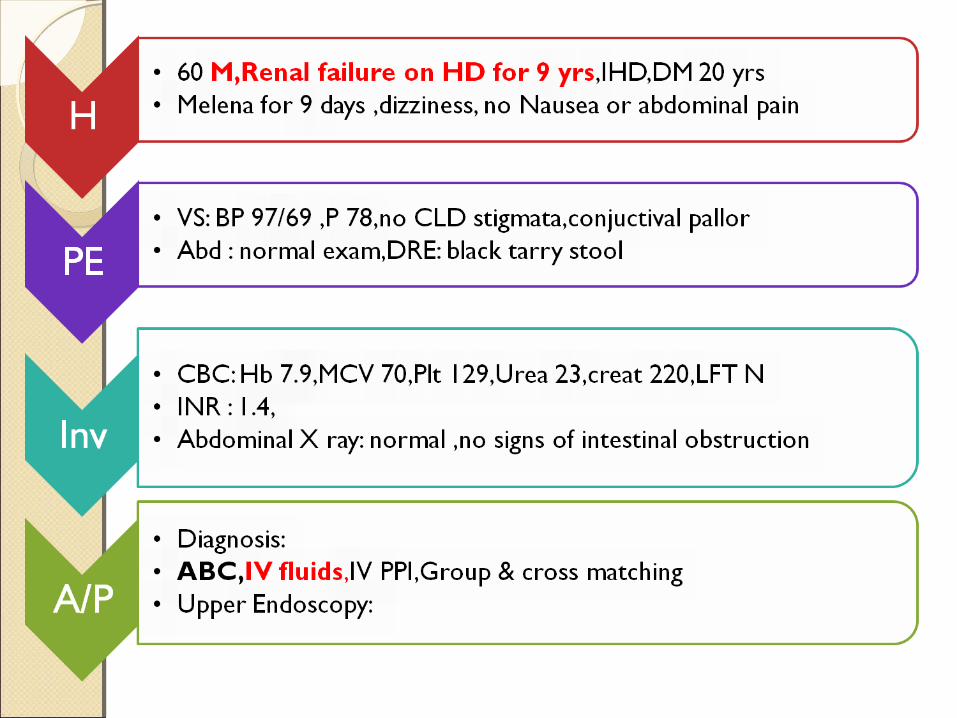
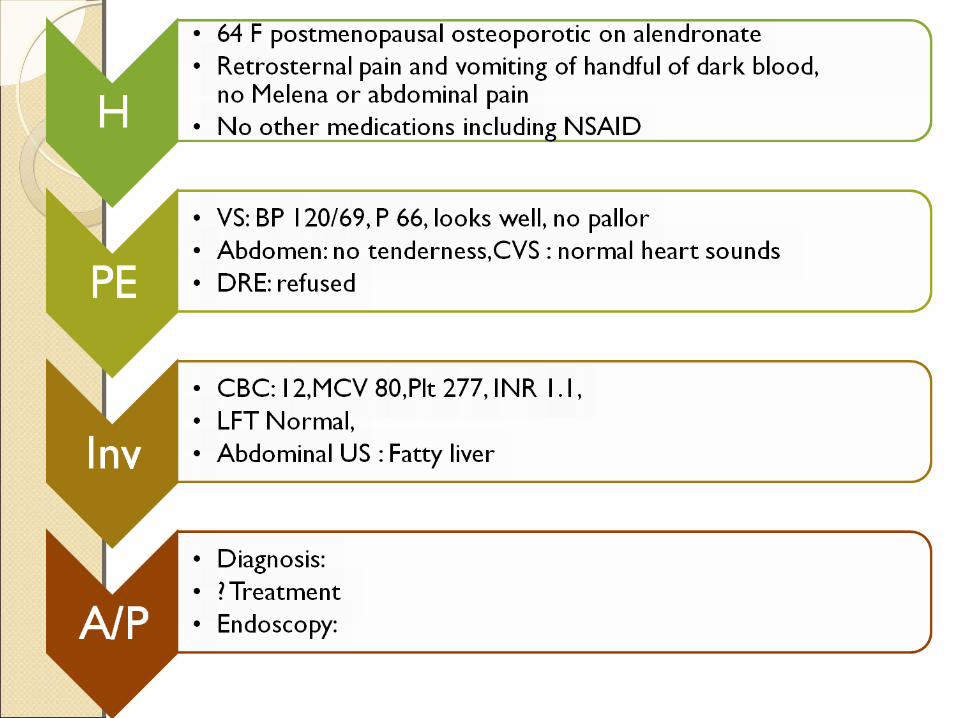
Melena: passage of blackTarry offensive stool due to Bleeding form the upper GIT proximal to ligmant ofTretiz ( > 100 ml).
Basic Mechanisms:1. Hyperacidity2. H pylori3. Vascular anomalies4. Autoimmune5. Malignancy Ligament
of Treitz

Management OutlineManagement Outline Airway Breathing Circulation Decide on Admission
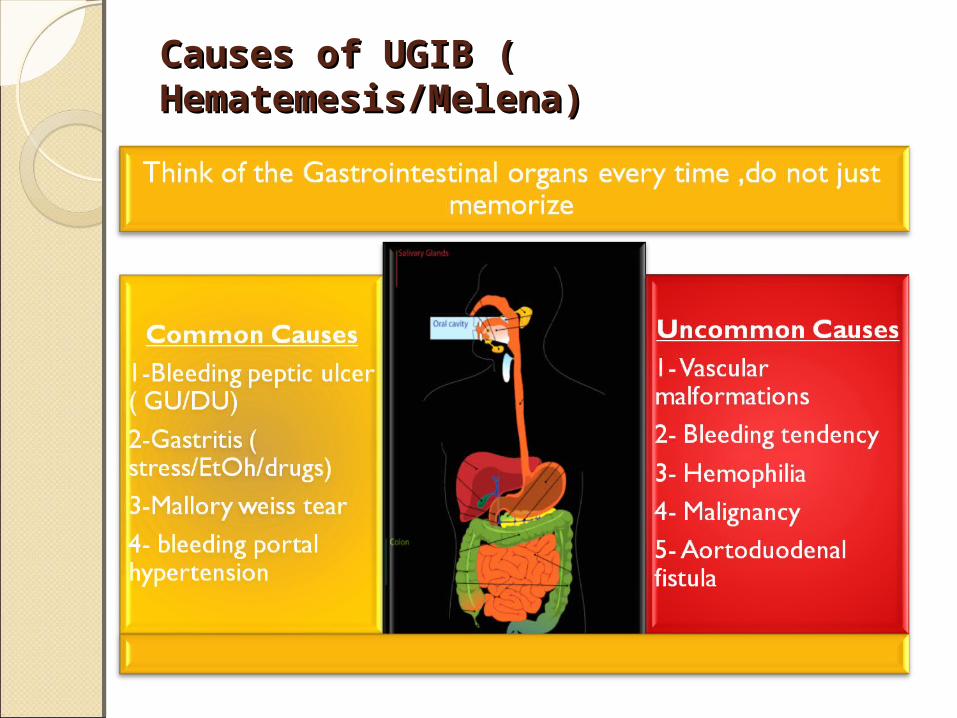
Causes of UGIB ( Causes of UGIB ( Hematemesis/Melena)Hematemesis/Melena)


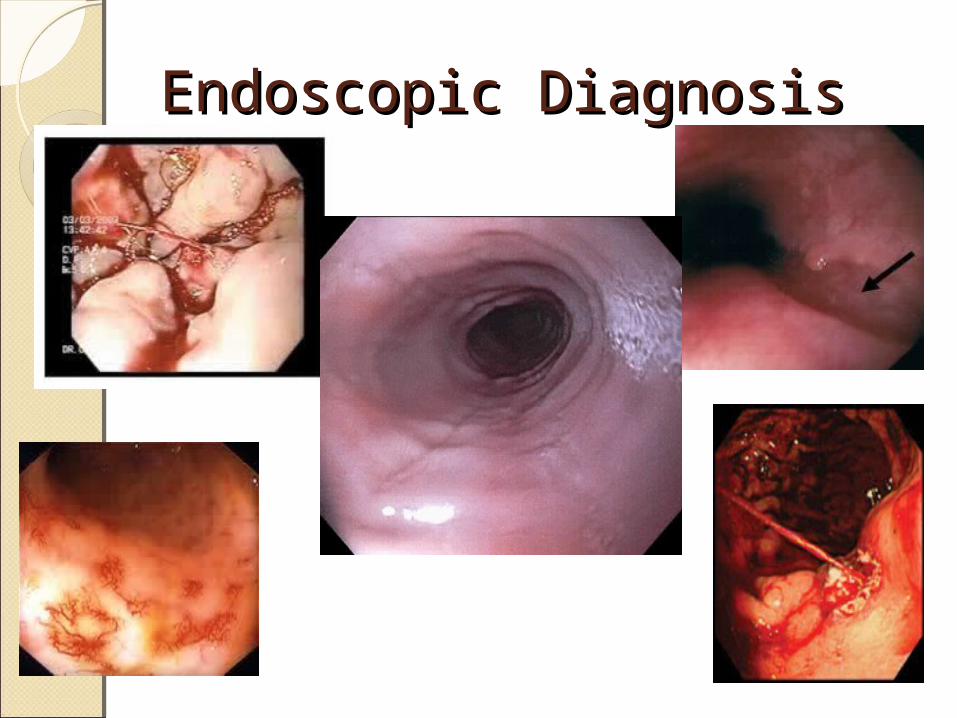
Endoscopic DiagnosisEndoscopic Diagnosis

Take home messageTake home messageAlways think of hemodynamic
stability ABCThen think to do H & PCommon things are commonCareful not to kill the patient and
know when to call for somebody helpCommon diseases are peptic ulcers,
liver disease, drug induced and malignancy.
Decide if you admit ( ward/ICU) or discharge.
Causes of Lower GI Causes of Lower GI BleedingBleeding
1- Anorectal Diseases :Hemorrhoids,Anal fissures
2- Infectious Gastroentritis mixed with blood
3- Colonic Diverticulosis4- Colonic neoplasms5- Vascular malformations:associated with
renal failure/aortic stenosis6-Inflammatory bowel disease.

Lower Gastrointestinal Lower Gastrointestinal BleedingBleedingHistory:Age,Onset,Progression,preceptating
factorsAssociated symptoms: poor appetite,
weight loss, abdominal pain, vomiting, constipation,diarrhea,Tenesmus,Straining.
Previous: similar episodes/Investigations/treatment performed.
Physical ExaminationPhysical ExaminationVital signs: HR,BPSigns of anemiaAbdomen:
contour,tenderness,guarding ( presence or absence)
DRE : bright red or dark blood.CVS,Resp systems
Lower GI bleedingLower GI bleedingABCIV lines,CBC,Blood group and cross
matching/Hold.IV colloids if hypotension/Blood if
anemia.Imaging : CT scan- Abdomen USRefer the pt to GastroenterologyColonoscopy: diagnostic and
therapeuticAngiography of the mesenteric vessels.

Obscure GI bleedingObscure GI bleedingEvidence of Bleeding/anemia
where investigations of the upper and lower GI tracts are unrevealing.
Need to exclude findings related to the GI tract by performing upper endoscopy and colonoscopy.
Causes of Obscure GI Causes of Obscure GI bleedingbleedingMalignancy: Small bowel
neoplasmInflammatory:Crohn’s enteritisVascular: Vascular malformationsMeckel’s diverticulumRadiation related enteritisSmall bowel ulcers ( NSAID
related )

Investigations of Obscure GI Investigations of Obscure GI bleedingbleedingRadiology:CT scan/MRI abdomen & PelvisRBC tagged scan Mickel’s scanEndoscopy:Double ballon EnteroscopyCapsule Endoscopy