48420349-study
TRANSCRIPT

Now get homework help from our live expert on rea ltime basis
Join us and get homework help
http://homeworkping.com/
Abstract
Anemia of critical illness, a commonly encountered clinical situation, is hematologically similar to that of chronic
anemia, except that the onset is generally sudden. The etiology is usually multifactorial, occurring as a
consequence of direct inhibitory effects of inflammatory cytokines, erythropoietin deficiency, blunted
erythropoietic response, blood loss, nutritional deficiencies, and renal insufficiency. Although anemia is not well
tolerated by critically ill patients, aggressive treatment of anemia can be just as detrimental as no treatment.
Different types of anemia may coexist in a patient in the intensive care unit, making diagnosis and
differentiation among these anemias complex, therefore requiring good diagnostic skills. Although several
therapeutic options are available to treat anemia, critically ill patients often receive a transfusion, and yet, most
recent studies indicate that blood transfusions in critically ill patients are associated with worse outcomes,
including higher morbidity and mortality. These studies have generated interest in the administration of
exogenous erythropoietin and iron therapy. Unfortunately, the accurate determination of iron status can be a
rather difficult task, an undertaking that is made even more difficult by the presence of comorbid conditions that
can affect the commonly used parameters for guiding iron therapy. The use of erythropoiesis-stimulating
agents is rapidly gaining acceptance, although they also present potential problems of their own.
Introduction
Anemia, because of its associated morbidity and mortality, is of clinical importance in critically ill patients.
Among patients who have normal hemoglobin levels on admission to an intensive care unit (ICU), nearly all
become anemic during the course of their ICU stay.[1,2] Anemia occurs as a result of inflammation, decreased
erythropoietin production, blunting of erythropoietin response, blood loss, nutritional deficiencies, or renal
failure.[1,3-5] Its hallmark is the development of disturbances of iron homeostasis, leading to diversion of iron from
circulation into storage sites and limiting the availability of iron for erythropoiesis. Although the definition and
grading of anemia vary among different organizations, most agree that a hemoglobin level below 6.5 g/dl
indicates severe or life-threatening anemia.[6] Whereas no consensus exists on the optimum hemoglobin
concentration or hematocrit value for patients in the ICU, clinicians uniformly agree that anemia must be
managed in critically ill patients to improve morbidity and mortality.[7,8]
Occurrence Rate
Approximately 29% of patients have lower than normal hemoglobin levels when admitted to an ICU, and about
95% develop anemia within 3 days of admission; this persists throughout the duration of their stay, with or
without red blood cell transfusion.[2] In a prospective, observational study, hemoglobin concentration was
evaluated in 91 nonbleeding patients in an ICU.[9] The authors reported that hemoglobin concentrations typically
declined by more than 0.5 g/dl/day during the first few days in the ICU. Beyond the third day, hemoglobin
concentrations remained relatively constant in nonseptic patients but continued to decrease in septic patients
as well as in patients with high sepsis-related organ failure assessments or high Acute Physiology and Chronic
Health Evaluation (APACHE) II scores.
Etiology
Anemia of critical illness has multiple causes, including blood loss from trauma, surgery, phlebotomy,
gastrointestinal hemorrhage, renal failure, blunted endogenous erythropoietin response, low erythropoietin
concentrations, decreased erythropoiesis, nutritional deficiencies, increased red blood cell destruction, and

reduced red blood cell life span. These causes may be grouped into three main categories: blood loss,
decreased red blood cell production, and increased red blood cell destruction.
Blood Loss
Phlebotomy. Blood loss from phlebotomy, once considered insignificant, can no longer be overlooked. It can
contribute to a reduction in hemoglobin concentrations, a condition referred to as iatrogenic or nosocomial
anemia.[10,11] The amount of blood phlebotomized in the hospitalized patient varies according to the population
studied, the length of stay evaluated, and type of catheter used. The Anemia and Blood Transfusion in Critical
Care (ABC) trial was a prospective, observational study conducted in 1136 patients from 145 Western
European ICUs.[12] During a 24-hour period, in almost half of the patients, blood was drawn 5 or more times,
with an average total volume of 41.1 ml of blood. There was a significant positive correlation between organ
dysfunction and the number of times blood was drawn (r = 0.34, p<0.001).
In another study, the phlebotomy records of 100 hospitalized patients were analyzed.[13] The authors found that
50 patients who spent part or all of their hospitalization in the ICU underwent phlebotomy a mean of 3.4
times/day, with a mean blood sample volume of 41.5 ml/day and total mean volume of 762 ml. Patients in the
ICU who had arterial catheters had even more blood drawn (total volume 944 ml) compared with those who did
not have such catheters (300.9 ml). However, in 50 patients who spent all their hospitalization on a general
medicine ward, blood was drawn only 1.1 times, with a mean volume of blood of 12.4 ml/day and a total volume
of 175 ml.
Results of a third study suggested blood loss from phlebotomy alone may exceed 70 ml/day.[14] However, other
studies have not shown such substantial losses, probably due to increased cognizance of the problem and the
implementation of blood-conservation strategies in the ICU.[3] In any case, the volume of blood loss due to
phlebotomy in critically ill patients appears to be positively correlated to the ICU length of stay and quantity of
blood transfusions required.[15]
Active Bleeding. Critically ill patients may become anemic due to surgical blood loss, intraoperative
hemodilution, and septic insults. Available data from retrospective studies suggest that active bleeding occurs
in 30% of critically ill patients, and that 35% of these patients require transfusion secondary to acute blood loss.[1] Blood loss due to surgery is also significant. For example, blood loss from orthopedic surgery is estimated to
range from 3 units during total hip arthroplasty to almost 6 units during bilateral total knee arthroplasty. [16,17] This
may result in a 3-6-g/dl decrease in hemoglobin level since, in an adult weighing 70 kg, 1 unit of blood loss
results in a 1-g/dl decrease in hemoglobin level. Critically ill patients also have a propensity to develop
gastrointestinal bleeding, especially those with head trauma and those receiving mechanical ventilation. These
conditions may cause stress ulceration, leading to a gastrointestinal bleeding event. It has been reported that
bleeding from the gastrointestinal tract accounts for about 30% of all significant bleeds in the ICU.
Proinflammatory cytokines, elevated during critical illness, may also exacerbate intestinal or other bleeding
disorders through vasodilation and increased permeability of the intestinal wall.[18] Coagulopathy, a commonly
encountered problem in the ICU, may exacerbate the blood loss and make control of bleeding even more
challenging.
Renal Failure. The increased prevalence of anemia in patients with renal failure may be attributed, at least in
part, to an insufficient compensatory increase of erythropoietin production in response to blood loss and
increased destruction of erythrocytes. Available data indicate that there is an inverse correlation between red
blood cell survival and serum blood urea nitrogen concentration.[18-21] In uremic patients, the normal response to
hypoxemia is partially blunted. With initiation of dialysis, these patients usually show improvement in anemia
symptoms and decreased transfusion requirements.[22] One group of authors found that a decrease in

hematocrit value parallels declines in renal function, and they reported that anemia is more likely to develop
when creatinine clearance decreases below 40 ml/minute/1.73 m2 and worsens with progression of renal
insufficiency.[23]
Decreased Red Blood Cell Production
Decreased red blood cell production in the critically ill patient is attributed to low concentrations of
erythropoietin, blunted response to erythropoietin, inflammatory cytokines, immune-mediated functional iron
deficiency, and other nutritional deficiencies. Erythropoiesis is the development of mature erythrocytes (red
blood cells). A decrease in oxygenation to the tissues signals the kidneys to increase production and release of
erythropoietin, stimulating stem cells to differentiate into preerythroblasts and erythroblasts, increasing the
release of reticulocytes and their subsequent maturation into erythrocytes.[22] In an otherwise healthy patient, an
acute decrease in hemoglobin level leads to an almost immediate increase in serum erythropoietin levels,[24]
which persists for at least 1-2 days. However, this is not the case in critically ill patients. It has been found that
endogenous levels of erythropoietin were 8 times higher in anemic ambulatory patients than in critically ill
patients who had anemia and sepsis with the same concentration of hemoglobin.[24] In a prospective,
observational study of 23 patients with multiple severe trauma, the authors concluded that erythropoietin
response in trauma patients is blunted despite low hemoglobin levels and adequate iron stores.[25] Although one
would expect an inverse correlation between hemoglobin and erythropoietin levels, the authors did not find
such a relationship.
Inflammation. The role of elevated circulating levels of proinflammatory cytokines, such as tumor necrosis
factor-α, interleukin-6, interleukin-1, Creactive proteins, and interferon-α, -β, and -γ, as a cause of anemia in
critically ill patients has become a major area of debate and discussion recently. Several studies have reported
that the levels of these cytokines are elevated during critical illness, with the subsequent inhibition of the gene
that encodes erythropoietin, suppression of erythropoietin production, and blunting of the erythropoietic
response.[3,18,25-28] Cytokines also appear to stimulate iron-binding proteins that sequester iron and also exert
direct toxic effects on erythropoietin-producing cells.[29,30] Deficient erythropoiesis, as seen in inflammatory
disease states, in which cytokines and other inflammatory mediators are elevated may explain why critically ill
patients develop anemia despite the absence of active bleeding.[3,22,28,31-34] Inflammation due to critical illness may
also lead to a decreased erythrocyte half-life along with anticipated damage to erythrocytes by proinflammatory
cytokines and free radicals.[35,36] Anemia of chronic disease, once believed to occur over weeks to months, is
now believed to occur in less than a week;[34] hence, the preferred term is now anemia of inflammation.
Increased Red Blood Cell Destruction
In critical illness, there is an increase in red blood cell destruction due to decreased deformability (a process
whereby red blood cells change their concave shape, allowing them to go through smaller capillaries),
hemolysis, and decreased red blood cell life cycle. Red blood cells stored for more than 15 days before
transfusion, which is common in ICUs, have a decreased ability to deform. Such poorly deformable cells cause
capillary sludging and obstruction, impeding passage and delivery of oxygen to the tissues and predisposing
the patient to ischemia.[37] Hemolytic anemia occurs when red blood cells are destroyed faster than the bone
marrow can produce them. It may be categorized into two types: intrinsic and extrinsic. Hemolytic anemia is
described as intrinsic when red blood cells are destroyed due to a defect in the red blood cells themselves. This
may be inherited, such as thalassemia, sickle cell anemia, and enzyme deficiencies, or it may be acquired,
such as malaria, hepatitis, and disseminated intravascular coagulation. In extrinsic hemolytic anemia, healthy
red blood cells are produced but are damaged by therapeutic interventions, such as rapid infusions of
hypotonic solutions, and mechanical trauma due to the use of invasive devices such as intraaortic ballon

pumps. Several drugs including penicillin, sulfa drugs, acetaminophen, antimalarial drugs, procainamide, and
methyldopa can cause extrinsic hemolysis.[23,34]
Laboratory Assessment
Once the diagnosis of anemia is established, the next step is determination of its etiology and type. The most
common types of anemia seen in an ICU are iron-deficiency anemia, functional iron deficiency (due to diversion
of iron from circulation into storage sites), and anemia of chronic disease or inflammation, which is
hematologically similar to that of critical illness. Common to the three types of anemia frequently encountered in
an ICU is decreased available iron to erythrocytes, resulting in decreased erythropoiesis. Because
malabsorption, frequent phlebotomy, and inflammation are common in an ICU, the three types of anemia may
coexist.[38] Coexistence of two or more types of anemia, sometimes referred to as mixed-factor anemia, has
recently been reported in 21% of critically ill patients.[39] Although a detailed discussion of the different types of
anemia is beyond the scope of this review, a brief discussion of the laboratory parameters used in diagnosis is
warranted.
Hemoglobin Level
Hemoglobin level provides a quantitative measure of the severity of iron deficiency once anemia has
developed. Although it is reported to have low specificity and sensitivity, it is probably the most useful
hematologic assessment for diagnosing anemia in an ICU.[15] Its normal values range from 12-16 g/dl for
females and 13-18 g/dl for males. If hemoglobin level is unavailable, the hematocrit value gives a rough
estimate since it is approximately 3 times the hemoglobin value.
Serum Iron Concentration
Serum iron concentration is an unreliable marker for total-body iron stores.[34] It is affected by a variety of
conditions, including inflammation, infection, neoplasms, liver disease, and alcoholism. Its sensitivity and
specificity are reported to be as low as 77.5% and 35.6%, respectively;[40] therefore, it is rarely used alone in
determining the etiology of anemia.
Serum Ferritin Concentration
Serum ferritin concentration, an acute-phase reactant, has a positive correlation with acute or chronic
inflammation.[41] It also correlates well with changes in total-body iron stores and is useful in diagnosing iron
deficiency. Although a low serum ferritin level is highly suggestive of iron deficiency, an iron-deficient patient
may have a high serum ferritin level.[42] With a reported sensitivity and specificity of only 71% and 69%,
respectively, serum ferritin concentration may be elevated in a variety of conditions, including infection,
inflammation, and malnutrition. With a normal range of 100-800 ng/ml, absolute iron deficiency in patients with
chronic kidney disease is defined as a serum ferritin level below 100 ng/ml in those not receiving hemodialysis
or peritoneal dialysis, and below 200 ng/ml in those receiving hemodialysis.[41] There has been no such cutoff
value in critically ill patients; whether these values can be accurately used in this patient population remains to
be determined.
Transferrin Saturation
Unlike ferritin, transferrin saturation is a negative acute-phase reactant.[41] It has a reasonable sensitivity of
81%, but a specificity of only 63%. It is calculated by dividing the serum iron concentration by total iron-binding
capacity and multiplying the result by 100. The National Kidney Foundation's recommended value for
transferrin saturation is 20-50%. Serum iron concentration and transferrin saturation give an indication of the
amount of iron that is immediately available for erythropoiesis. A transferrin saturation of less than 20% usually

indicates diminished iron availability and, depending on the clinical setting, the need for iron supplementation.
However, a transferrin saturation greater than 55% may indicate possible iron overload.[43] In critically ill patients
with a high ferritin level and low transferrin saturation, functional iron deficiency may be suspected.
Reticulocyte Count
Reticulocytes are immature erythrocytes; therefore, anemic patients with an intact erythropoietic system should
display an elevated reticulocyte count. In anemia of critical illness, patients characteristically have a low
reticulocyte count, which indicates underproduction of erythropoietin and therefore red blood cells.[44]
Reticulocyte Hemoglobin Content
Reticulocyte hemoglobin content is a direct measure of iron in reticulocytes and, hence, might be a good
parameter for guiding iron therapy.[45] In one study, reticulocyte hemoglobin content was reported to be highly
specific and sensitive for iron deficiency and was therefore a good predictor of those who need and will most
likely respond to iron therapy.[46] In this study, the authors demonstrated that reticulocyte hemoglobin content is
more reliable than serum ferritin concentration or transferrin saturation in assessing iron stores in patients
receiving hemodialysis. Another study, however, found a lower sensitivity for reticulocyte hemoglobin content.[47]
Subsequent studies have produced conflicting results.[48,49] Few facilities measure reticulocyte hemoglobin
content, which limits its clinical utility in the ICU.
Prevention
To a certain extent, the frequency of anemia of critical illness may be reduced by using blood conservation
practices. Recommendations include using smaller test tubes; using point-ofcare microanalyzers for blood gas,
electrolyte, and hemoglobin analyses; and scheduling diagnostic tests simultaneously so the same blood
sample can be used for all of them. Other recommendations include documenting blood loss due to
phlebotomy on ICU flow sheets so that clinicians are aware of the loss,[13,60] reducing standing orders, and
developing policies for minimizing waste. Studies show that using smaller test tubes to draw blood can reduce
total blood losses due to phlebotomy by 33-47% and that discarded blood volumes account for 24-30% of the
total daily blood loss in an ICU.[61-63] This waste can be greatly reduced by using a closed method of blood
sampling whereby the initial sample component is returned to the patient. Using microanalyzers for point-of-
care testing can also reduce blood loss due to phlebotomy. They require 1 ml or less of blood, whereas 9 ml of
blood is required for tests in the laboratory.[64] The use of cell-saving devices (which gather the patients own
blood from surgical drains and then reinfuse it with or without processing), bloodless surgery, and transfusion of
autologous blood are also measures being advocated. Other measures include using perioperative parenteral
iron, erythropoiesis-stimulating agents, and crystalloids or colloids to replace blood loss.
TreatmentTransfusion
Acute anemia is usually managed with red blood cell transfusion, a practice that has long been regarded as
relatively risk free with obvious clinical benefits.[65] Studies show that about 50% of all patients admitted to an
ICU receive transfusions, whereas 85% of those patients who stayed in an ICU for more than 7 days received
transfusions.[1,2,66] In the pediatric literature, it is reported that up to 50% of children in an ICU receive red blood
cell transfusions,[67,68] yet hemodynamically stable children may tolerate the decreased oxygen delivery
associated with a moderate degree of anemia.[69] In the Anemia and Blood Transfusion in the Critically Ill (CRIT)
study, the authors examined the relationship of anemia and red blood cell transfusion with clinical outcomes.[2]
They found that as the number of red blood cell units transfused increased, this was independently associated
with longer ICU and hospital length of stay and with increased mortality. They also observed that patients who
received transfusion experienced more complications and were more likely to experience a complication than
those who did not receive transfusion. In the previously discussed ABC study, the investigators reported a
positive correlation between blood transfusions and 28-day mortality.[12]
Older position statements recommended that patients be transfused when hemoglobin levels decreased below
10 g/dl or hematocrit values decreased below 30% (10/30 rule).[70,71] These recommendations were not based
on randomized controlled trials, but rather on tradition. Thus, this 10/30 rule, first proposed in the early 1940s [72]
and made even more popular in 1982 as a transfusion trigger,[73] is not supported by good clinical evidence in
the critically ill patient. Over the years, data have accumulated suggesting that perioperative and critically ill
patients can tolerate more severe degrees of anemia without adverse outcomes.[53,74,75] For example, in
Jehovah's Witnesses (whose beliefs include refusal of blood transfusions) who had major surgeries, the
mortality rate attributed to anemia was only 1.4%.[76] Thus the traditional hemoglobin concentration threshold at
which transfusion was justified is being questioned.
The authors of the Transfusion Requirements in Critical Care (TRICC) study attempted to clarify this debate in
the general medical and surgical critical care community.[8] This randomized, prospective, controlled trial
compared restrictive (418 patients) and liberal (420 patients) transfusion strategies. The restrictive strategy
allowed transfusion if the hemoglobin level was below 7 g/dl with a target hemoglobin level of 7.9 g/dl, whereas
the liberal strategy allowed transfusions when hemoglobin level was below 10 g/dl with a target hemoglobin
level of 10.12 g/dl. The authors concluded that the 30-day mortality rate was similar in the restrictive and liberal
groups (18.7% and 23.3%, respectively). They also reported no significant difference in 30-day survival in a
subset of 357 patients with cardiovascular disease, although those with severe ischemic disease had a
nonsignificant trend toward decreased survival in the restrictive group compared with the liberal group,
suggesting that this patient population may benefit from higher hemoglobin levels.[77] Subgroup analysis showed
that young patients (< 55 yrs) and less severely ill patients (APACHE score ≤ 20) had a significantly lower 30-
day mortality rate in the restrictive group compared with the liberal group; however, subgroup analyses,
notorious for making type 1 errors (creating a difference when none exists),[78] should be interpreted with
caution. The authors recommended the restrictive strategy for most patients with the possible exception of
critically ill patients with ongoing ischemia. The reader must realize that hemodynamically unstable patients,
those with chronic anemia, and those undergoing cardiac surgery were excluded from the study, and therefore
the findings from the TRICC study should not be applied to these patient populations.
Similar findings have been reported in pediatric[69] and trauma[79] patients. Recently, a noninferiority trial enrolled
637 critically ill children in stable condition and assigned them to either a restrictive group with a hemoglobin
concentration threshold of 7 g/dl (320 patients) or a liberal group with a threshold of 9.5 g/dl (317 patients). [69]
No significant differences were found in adverse outcomes between both groups. The results of these
studies[8,69,79] were unexpected since previous observational studies had shown that as hemoglobin level
decreased below 9.0-9.5 g/dl, critically ill patients had increased adverse outcomes.[74,80]
The available data suggest that, in the absence of acute bleeding, hemoglobin levels of 7.9 g/dl are well
tolerated by most hemodynamically stable critically ill patients. What the optimum hemoglobin level is in the
hemodynamically unstable patient in an ICU remains to be determined. The authors of a recent review article
recommend a hemoglobin transfusion trigger of 7 g/dl in most critically ill patients, including patients with a
history of cardiac disease and those beyond 6 hours of septic shock.[81] They noted, however, that for patients
with early septic shock (≤ 6 hrs) and those with acute coronary syndromes, a higher trigger of 8.10 g/dl may be
needed. Table 1 summarizes their recommendations.
Transfusion Risks. Blood transfusions have been correlated with multiorgan failure and high mortality,[2,12]
increased ICU and hospital length of stay,[2] and numerous adverse reactions including transfusion-related
immunomodulation,[82-84] transfusionrelated acute lung injury,[85-88] transfusionassociated cardiac overload,[89,90]
systemic inflammatory response syndrome,[91] and severe acute hemolytic and nonhemolytic reactions.[92] The
most common of these is hemolytic reactions, caused by mismatching of the patient's blood type and the blood
unit transfused. The mismatching rate is estimated to be 1/14,000 blood units in the United States [93] and
1/18,000 units in the United Kingdom,[94] with a fatality rate of 1/800,000 units.[95]
There is also growing evidence that stored or "old" red blood cells lose their ability to deform and to unload
oxygen.[96-99] On average, critically ill patients receive blood that has been stored for 21 days.[2] In the CRIT
study,[2] the mean age of red blood cells transfused was 21 days, with 25% of transfused red blood cells being
more than 30 days old. It is estimated that 60% of red blood cells of relatively rare blood types such as O
Rhnegative are 28 or more days old when transfused.[100] As stored red blood cells approach the end of their
shelf lives (42 days), biochemical, metabolic, and morphologic changes occur that may negate the anticipated
benefit of the transfusion and may even cause harm.[101]
One such biochemical change is the decline of 2,3-diphosphoglyerate levels, a modifier of hemoglobin affinity
for oxygen. As these levels decline, hemoglobin affinity for oxygen increases, resulting in a decrease in its
ability to unload oxygen to the tissues. In a study of septic patients receiving mechanical ventilation, the authors
not only failed to demonstrate an increase in oxygen uptake after transfusion but also reported that patients
receiving blood older than 15 days developed evidence of splanchnic ischemia, reflected by gastric
intramucosal acidosis.[96] The authors postulated that poorly deformable cells cause occlusions that lead to
tissue ischemia. Transfusion of "old" blood has also been reported to be a risk factor for multiorgan failure, [102,103]
increased length of stay,[97,104] and increased mortality.[105] Note that not all studies reported a difference between
ICU length of stay or the efficacy and safety of old and fresh blood,[106-108] but the data strongly suggest that the
length of storage affects the quality of blood products.
Blood Substitutes. There are two broad categories of blood substitutes, or more specifically, oxygen-carrying
agents: hemoglobin solutions and perfluorocarbons. These agents have high affinity for oxygen and were
developed as a safer alternative to blood transfusion. Both types of agents have much longer shelf lives (up to
3 yrs) compared with that of blood (42 days).[109-111] Unfortunately, clinical trials of these agents have shown
disappointing results in improving tissue oxygenation; hence, they remain investigational. They also present
potential problems of their own, including infection, immunomodulation, oxidative damage, acute immune
reactions, and pulmonary hypertension.
Iron Supplementation
Oral Iron. When erythropoiesis-stimulating agents are administered, large amounts of iron are required.
Therefore, even in patients with adequate iron stores, exogenous iron supplementation may be required to
achieve optimal response to an erythropoiesis-stimulating agent.[112,113] Iron replacement therapy in the non-
critically ill patient is usually begun with oral iron, which comes in several forms. These forms include ferrous
sulfate, gluconate, fumarate, polysaccharide iron complex, and heme iron polypeptide, with each form
containing a different percentage of elemental iron ( Table 2 ).
Patients usually require a minimum dose of 200 mg/day of elemental iron for sufficient supplementation. The
questionable absorption of oral iron, coupled with gastrointestinal issues and the binding of iron to other drugs
in the gastrointestinal tract, limits its use in the critical care setting. A new generation of oral iron product, heme
iron polypeptide, is expected to overcome the limitations of traditional forms of oral iron. Heme iron polypeptide
(Proferrin; Colorado Biolabs, Aurora, CO, www.coloradobiolabs.com) uses the heme porphyrin ring to supply
iron to intestinal absorption sites, which are different from those of traditional forms of iron.[45] The bioavailability
of heme iron polypeptide in healthy volunteers has been found to be up to 10 times higher than that of
nonheme iron.[114] The increased bioavailability has been confirmed by other studies.[115-118] One group of authors
reported that the use of oral heme iron polypeptide can successfully replace intravenous iron and maintain
hematocrit values in most patients undergoing hemodialysis.[118] Oral heme iron polypeptide, with its superior
absorption rate, lower frequency of gastrointestinal adverse effects, and improved patient tolerance, may be a
feasible alternative for iron repletion to sustain erythropoietin-driven erythropoiesis.
Parenteral Iron. Because of frequent patient intolerance to oral iron as well as its poor bioavailability,
intravenous iron is frequently used in the ICU for treatment of severe iron deficiency. Numerous studies have
shown that oral iron does not provide iron quickly enough to support the accelerated erythropoiesis that occurs
with erythropoietin therapy.[119-121] Parenteral iron has been shown not only to support erythropoiesis during
erythropoietin therapy by supplying sufficient iron quantities at the required rate,[112] but also to decrease the
erythropoietin dose requirements in patients with anemia.[119] In a prospective, multicenter, openlabel study of
157 patients with chemotherapyrelated anemia, patients were randomly assigned to four treatment groups: no
iron, oral ferrous sulfate 325 mg twice/day, iron dextran 100-mg intravenous bolus at each visit to the
calculated required iron dose, and total dose infusion of iron dextran.[120] All patients received epoetin alfa
(recombinant human EPO [r-HuEPO]) 40,000 units subcutaneously once/week and were followed for 6 weeks,
except for those in the bolus group, who were followed until the end of their treatment course. The authors
reported that iron supplementation by the intravenous route provides the optimal environment for augmenting
erythropoiesis and improving quality of life. Of interest, the efficacy of oral iron was found to be similar to that of
no iron. The improved efficacy of erythropoiesis-stimulating agents with parenteral iron has also been
documented in several other patient populations including patients with Crohn's disease[122] and postpartum
women.[123]
In the United States, three parenteral iron formulations are available: iron dextran, iron sucrose (or saccharate),
and iron gluconate. It appears that all the formulations are efficacious in replenishing body iron stores and
improving response to erythropoietin. Patients undergoing hemodialysis generally require a cumulative dose of
1000 mg of intravenous iron, but no such dose has been established for critically ill patients. Although iron
dextran is slowly released from its complex, iron gluconate and sucrose are immediate-release products.
Therefore, the total dose of iron dextran can be administered at once as a slow intravenous infusion; in
contrast, iron gluconate or sucrose may be given in smaller doses over a longer period of time, although the
safety of higher doses (iron sucrose 500 mg and iron gluconate 250 mg) has been established.
Laboratory Parameters for Determining the Need for Iron Supplementation. Despite their limitations,
transferrin saturation and serum ferritin concentration remain the most commonly used and probably the best
laboratory parameters for determining if iron supplementation is needed in patients with anemia due to chronic
kidney disease.[41] Since anemia due to chronic kidney disease and that due to critical illness are
hematologically similar, it stands to reason that the same parameters could be used in critically ill patients. Iron
supplementation is recommended for patients with chronic kidney disease who have transferrin saturation less
than 20% or a serum ferritin concentration less than 100 ng/ml. Even when the serum ferritin concentration is
100-500 ng/ml, if transferrin saturation is less than 20%, iron supplementation still may be beneficial.
The newest guidelines from the National Kidney Foundation do not recommend iron administration when the
serum ferritin concentration is greater than 500 ng/ml.[41] Previous guidelines recommended an upper limit of
800 ng/ml; however, evidence is insufficient on the responsiveness of iron therapy when the ferritin
concentration exceeds 500 ng/ml since such a situation represents a state of functional iron deficiency
(impaired release and utilization of iron from storage),[45] which may be caused by acute-phase response to

inflammation. Administration of iron may indeed be harmful in this scenario. Hence, when a patient has a
transferrin saturation less than 20% and ferritin concentration greater than 500 ng/ml, which is common in an
ICU, clinicians should assume that an inflammatory process is present and treat accordingly.[44] C-reactive
protein levels, which measure inflammation, should be obtained. If there is no evidence of active inflammation,
a low reticulocyte hemoglobin content may justify a trial of iron therapy.[44]
The new guidelines on ferritin and iron administration from the National Kidney Foundation have been
questioned by the recently published results of the Dialysis Patients' Response to IV Iron with Elevated Ferritin
(DRIVE) study.[124] This study evaluated the efficacy of intravenous ferric gluconate in patients undergoing
dialysis who had high ferritin levels (500-1200 ng/ml) and low transferrin saturation (≤ 25%) and who remained
anemic despite receiving adequate doses of epoetin. The authors concluded that the administration of ferric
gluconate (125 mg for 8 doses) was superior to no iron therapy in the study patients. Furthermore, no
significant difference was noted in the frequency of serious or total adverse events between the treatment and
control groups. This study's results suggest that intravenous iron is effective in overcoming inflammation-
mediated reticuloendothelial blockade. The authors recommend that ferritin concentration alone should not be
used to guide iron therapy decisions except when low (< 300 ng/ml), when it is highly predictive of iron
deficiency. It seems prudent to make treatment decisions by using several laboratory parameters rather than a
single parameter.
Problems With Iron Administration. Infections. The virulence of several common pathogens, including
Pseudomonas species, Escherichia coli, Salmonella species, and Klebsiella species, is markedly increased in
the presence of free iron. These pathogens compete with proteins, such as transferrin (a protein that transports
iron), by producing iron chelators known as siderophores.[125,126] Other pathogens, such as Staphylococcus
aureus and Haemophilus influenzae, however, produce transferrin receptors that allow them to compete for
free iron.[126] Several authors have suggested that during critical illness, humans have evolved a response
system to divert iron from circulation into storage sites to deprive invading microorganisms.[49,127-129] Others have
proposed that iron administration alone does not appear to enhance bacteria growth until transferrin saturation
exceeds a critical threshold whereby exogenous administration of free iron becomes available for bacteria
utilization.[130] Under normal conditions, transferrin is less than 50% saturated in the blood, leaving little to no
free iron for bacteria utilization. However, as transferrin saturation increases, the ability to inhibit bacterial
growth is lost.[131] For example, in vitro studies suggest that as transferrin saturation increases, Pseudomonas
aeruginosa and Klebsiella cultures increase proportionally, with bacterial growth occurring when transferrin
saturation exceeds 60%, in the case of Klebsiella. Inhibition of Staphylococcus epidermidis is reportedly lost
once the transferrin saturation exceeds 80%.[125]
It is worth mentioning that most of the human studies that showed a link between risk of infection and iron
administration were in the setting of iron overload rather than just the administration of iron. [130] Some of the
studies showed an increase in infection risk when the serum ferritin level was above 500 or 1000 ng/dl.[132-135]
Other studies offered conflicting or inconclusive results, but none, to my knowledge, have directly implicated
exogenous iron administration as a cause of infection in humans,[136-138] although animal studies suggest iron
administration may exacerbate infection. Randomized controlled trials in critically ill patients are needed to
determine whether there is a link between exogenous iron administration and infection. Although the available
data are not definitive, clinicians are cautioned to consider risk versus benefit before administering iron to
patients.
Iron deficiency, however, is known to increase the susceptibility to common infections by impairing certain host
defense mechanisms such as a reduction in the absolute number of T cells and a defect in neutrophil function.[139] In one study, 23 (74%) of 31 patients with mucocutaneous candidiasis showed evidence of mild iron
deficiency that was confirmed by bone marrow examination.[140] The evidence that these observations have
clinical relevance is still debatable.
Anaphylaxis. Despite the proven effectiveness of parenteral iron, clinicians are reluctant to prescribe it primarily
because of the relatively rare but sometimes fatal occurrence of anaphylaxis. The frequency of severe
anaphylactic reactions is 0.6-0.7% in patients undergoing hemodialysis who are receiving iron dextran,[141] which
carries the highest risk of lifethreatening reaction of all the available iron formulations. The exact mechanism by
which the hypersensitivity reaction occurs is unknown, but the dextran component may be antigenic. A test
dose is strongly recommended before initial administration of iron dextran. However, an anaphylactic reaction
may still occur despite a negative test dose and after many uneventful administrations.[142] The available data
suggest that patients with previous reactions to iron dextran will generally tolerate iron gluconate or sucrose,[44]
both of which lack the dextran component; however, administration of a test dose in these patients is
recommended.
Iron Overload. The concept of iron overload is easy to understand when one realizes that humans have no
physiologic mechanism for iron excretion. Thus, caution must be exercised during iron supplementation,
especially parenteral iron supplementation, which bypasses normal gastrointestinal regulation of iron
absorption. When plasma iron content exceeds the iron-binding capacity of transferrin and ferritin, the excess
iron is deposited in the parenchymal cells of the liver, the heart, and endocrine tissues, causing tissue damage
and fibrosis.[143]
Erythropoiesis-stimulating Agents
Because of the problems with transfusion and to overcome the reduced production and blunted response to
erythropoietin, much attention is now on erythropoiesis-stimulating agents. As discussed earlier, anemia of
critical illness is due, at least in part, to diminished production and response to erythropoietin. Therefore, it
seems reasonable to expect exogenous erythropoietin to be effective in the correction of anemia. Two
erythropoiesis-stimulating agents are available in the United States: r-HuEPO and darbepoetin alfa. Although
structurally similar with the same mechanism of action as that of endogenous erythropoietin, the two agents are
biochemically distinct, with darbepoetin alfa containing two additional carbohydrate chains, which has been
found to increase its serum half-life and biologic activity. Although both agents have clinically significant lag
times (time between initiation and response),[144,145] r-HuEPO, by virtue of its short duration and fast onset of
action, demonstrates a shorter lag time. The clinical significance of the difference in lag time between the two
agents is left to speculation. Because of the lag time, early initiation of these agents is advisable. The limited
available data from head-to-head comparative trials indicate that, at equivalent doses, the two products are
equally effective in increasing hemoglobin concentrations in different patient populations.[137,146,147]
Effectiveness. The effectiveness of erythropoiesis-stimulating agents in the ICU setting has been investigated
in a number of randomized controlled trials.[33,121,148-150] One group of investigators enrolled 160 critically ill patients
in a multicenter, randomized, double-blind, placebo-controlled study.[33] Patients were assigned to receive either
r-HuEPO 300 units/kg (80 patients) or placebo (80 patients) for five doses beginning on ICU day 3 (study day
1). The patients received r-HuEPO or placebo for a minimum of 2 weeks or until discharge from the ICU, with a
maximum duration of therapy of 6 weeks. All patients received oral or parenteral iron. Patients in the r-HuEPO
group received transfusion with a total of 116 red blood cell units, which was significantly lower than the total of
305 red blood cell units transfused in the placebo group. In addition, patients who received r-HuEPO had a final
hematocrit value that was significantly higher than that in the control group (35.1% vs 31.6%, p<0.01) despite
receiving fewer transfusions. The investigators reported that the administration of r-HuEPO was associated
with a 45% reduction in the number of red blood cell units required, and this was achieved without any
significant adverse effects. A similar finding was reported in surgical patients.[150] Another group of investigators,
however, recently found no significant reduction in the rate of red blood cell transfusions by using r-HuEPO
between days 1 and 29.[151] According to those investigators, a likely explanation for this unexpected finding was
the adoption of a more restrictive transfusion strategy as a result of the TRICC study. Furthermore, it is
generally accepted that in the first 2-4 weeks of administration, erythropoiesisstimulating agents do not
increase hemoglobin level and therefore should not influence the need for transfusion because of their reported
lag times.
Cost-effectiveness. The available data indicate erythropoiesisstimulating agents are effective in the critical
care setting, although their cost-effectiveness is still controversial. Depending on the primary end point, the
findings from different clinical studies have varied. One group performed a costeffectiveness analysis in a
hypothetical cohort of critically ill patients; they calculated the absolute risk reduction, the number of patients
needed to treat (NNT), and the incremental cost required to avoid one transfusion-related adverse event by
using erythropoiesis-stimulating agents in critically ill patients.[152] Their main finding was that the NNT to avoid
one transfusion-related adverse event was 5246 at a cost of almost $5,000,000, whereas the NNT to avoid a
serious or likely fatal transfusion-related adverse event was 25,000 at a cost of $25,000,000. These estimates
are well beyond acceptable limits of cost-effectiveness. Thus, from the standpoint of decreasing transfusion-
related adverse events, this study suggests that the use of erythropoiesisstimulating agents in the critical care
setting is not cost-effective. However, an editorial questioned whether such events are the most appropriate
outcomes to measure with regard to the use of erythropoiesis-stimulating agents in the critically ill patient.[153]
The authors suggested that a decrease in the number of red blood cell units transfused, the complete
avoidance of red blood cell transfusions, decreased length of mechanical ventilation, and 30-day all-cause
mortality are more relevant outcome measures. The cost-effectiveness cohort study[152] has also been criticized
for not comparing r-HuEPO with other blood safety and conservation interventions such as leukoreduction,
improved blood screening procedures, and transfusion of autologous blood.
Another group of investigators examined the cost-effectiveness of using erythropoiesisstimulating agents to
reduce red blood cell transfusions in a mixed ICU patient population.[154] They concluded that the agents appear
to be costeffective, assuming red blood cell transfusions increase the risk of nosocomial bacterial infections.
The authors of another study also showed a marked decrease in transfusions from 43% to 12% with an overall
cost savings of 39%, justifying the use of erythropoiesis-stimulating agents in patients undergoing surgery.[155] It
must be stressed that regardless of any study's end point, it is important for clinicians to keep in mind that
blood is a limited and valuable resource and conserving it is worthwhile. The approach to transfusion medicine
must therefore be driven by other outcomes, not just economic ones.
Dosing Guidelines. Treatment guidelines recommend erythropoiesisstimulating agents for patients with
symptomatic anemia who have hemoglobin levels below 10 mg/dl, with a target hemoglobin level of 12 mg/dl.
For patients with hemoglobin levels of 10-12 mg/dl, the decision to begin these agents should be determined by
the patient's clinical circumstance or manifestation of the anemia.[58] According to the package inserts, the initial
dose of an erythropoiesis-stimulating agent should be decreased by 25% if the increase in hemoglobin level is
more than 1 g/dl in any 2-week period.[156-158] In nonresponsive patients, the dosage can be escalated by 25%
once in 4 weeks for epoetin or once in 6 weeks for darbepoetin. Therapy should be discontinued if there is no
response (i.e., < 1-g/dl increase in hemoglobin level) 4-6 weeks after dose escalation.[159] Serum ferritin
concentration and transferrin saturation should be assessed and iron supplemented if indicated to optimize the
response to erythropoiesis-stimulating agents.
Safety Concerns. There have been reports of increased thrombotic events and progression of tumor growth in
different patient populations receiving erythropoiesis-stimulating agents who have hemoglobin levels above 12
g/dl.[160,161] These reports have led to a recent black-box warning from the United States Food and Drug

Administration. The agency's instructions require erythropoiesis-stimulating agents to be withheld from patients
whose hemoglobin levels exceed 12 g/dl and until the level decreases below 11 g/dl.[162] Clinicians are urged to
use the lowest dose that will gradually increase the hemoglobin concentration to the lowest level sufficient to
avoid the need for transfusion. On the contrary, the National Kidney Foundation has set a lower hemoglobin
limit of 11.0 g/dl as "an evidencebased recommendation," whereas the upper limit is set at 13.0 g/dl as a
"clinical practice recommendation."[41] The National Kidney Foundation's concern was that the narrow range of
11-12 g/dl could not be achieved because of hemoglobin cycling.[41,58]
Conclusion
Although patients with anemia of critical illness have an increased risk of mortality, overcorrection of anemia
with erythropoiesisstimulating agents or blood transfusions does not necessarily improve their outcomes.
Despite impressive advances in the safety of the blood supply, a number of investigators have reported an
association between blood transfusion and organ failure, nosocomial infections, increased length of stay, and
increased morbidity and mortality. Therefore, the search continues for safer therapeutic alternatives to a blood
transfusion. Blood substitutes have so far failed to live up to expectation. The use of erythropoiesis-stimulating
agents has shown promise, although these drugs are associated with increased risk of serious cardiovascular
events when administered to a target hemoglobin level above 12 g/dl.

The incidence of pneumonia during cold months in the Philippines (January-February) could increase. Reports on TV already indicated deaths in Baguio City, Benguet, Cagayan and even in Ilocos Norte (where I live). Pneumonia is a respiratory disease which often affects children and the elderly. The cold months in the Philippines will definitely affect these groups because the air is thin due to the high moisture in the atmosphere.
During times like this, our lungs work harder in order to transport the required oxygen throughout our entire system to keep our organs functioning well. This is because during cold months, our bodies get lesser amounts of oxygen. Boxers even train in high altitudes to increase cardiovascular strength and stamina because their lungs are forced to work harder. On the other hand, for non-athletes, the cold weather can be very unfriendly.
According to health experts, the medical term pneumonia actually covers over 50 respiratory illnesses which concern the function of the lung’s air sacs, or alveoli. There are a number of irritants which can cause pneumonia to develop, including bacteria, viruses, mycoplasm, fungi and chemicals. Once one of these irritants manages to bypass the body’s natural defenses, an infection forms in the deepest part of the lungs. As the body releases white blood cells to fight off this infection, fluids fill up the alveoli and bronchi. It is this fluid build-up and subsequent illness that many of us consider pneumonia.
Viral pneumonia is the most common form, although ironically it doesn’t always produce the worst symptoms. Many people contract viral pneumonia shortly after another upper respiratory disease has already formed. Viruses expelled from the lungs through coughing may be re-aspirated into the air sacs and form a new infection. Patients with viral pneumonia may notice a gradual increase in symptoms, starting with a persistent cough and leading to high fever and nausea. Severe cases of viral pneumonia may require hospital treatment, but many doctors suggest allowing the infection to run its course over a few weeks.
In the Philippines, pneumonia sometimes leads to death because cases of pneumonia, especially in the barrios, are left untreated either because of knowledge deficit about the symptoms of pneumonia or lack of money to pursue treatment. These factors usually aggravate pneumonia and reflects the type of healthcare a country has. I will update this post in the near future to discuss the Philippine healthcare system from a researcher’s point of view. I know many Filipinos are not given proper care particularly those from far-flung localities. That is the reason why cold weather in the Philippines can has already taken its toll on the people. Cases of pneumonia and deaths caused by pneumonia might continue to rise until February due to the cold weather reaching an all-time low of 7.5 degrees Celsius in Baguio City since 1961 (which recorded a 6.3 degrees Celsius reading on January 18).
INTRODUCTION
Pneumonia is an inflammation of the lungs caused by an infection. It is also called Pneumonitis or Bronchopneumonia. Pneumonia can be a serious threat to our health. Although pneumonia is a special concern for older adults and those with chronic illnesses, it can also strike young, healthy people as well. It is a common illness that affects thousands of people each year in the Philippines, thus, it remains an important cause of morbidity and mortality in the country.There are many kinds of pneumonia that range in seriousness from mild to life-threatening. In infectious pneumonia, bacteria, viruses, fungi or other organisms attack your lungs, leading to inflammation that makes it hard to breathe. Pneumonia can affect one or both lungs. In the young and healthy, early treatment with antibiotics can cure bacterial pneumonia. The drugs used to fight pneumonia are determined by the germ causing the pneumonia and the judgment of the doctor. It’s best to do everything we can to prevent pneumonia, but if one do get sick, recognizing and treating the disease early offers the best chance for a full recovery.A case with a diagnosis of Pneumonia may catch one’s attention, though the disease is just like an ordinary cough and fever, it can lead to death especially when no intervention or care is done. Since the case is a toddler, an appropriate care has to be done to make the patient’s recovery faster. Treating patients with pneumonia is necessary to prevent its spread to others and make them as another victim of this illness.
ANATOMY AND PHYSIOLOGY
The lungs constitute the largest organ in the respiratory system. They play an important role in respiration, or the process of providing the body with oxygen and releasing carbon dioxide. The lungs expand and contract up to 20 times per minute taking in and disposing of those gases.Air that is breathed in is filled with oxygen and goes to the trachea, which branches off into one of two bronchi. Each bronchus enters a lung. There are two lungs, one on each side of the breastbone and protected by the ribs. Each lung is made up of lobes, or sections. There are three lobes in the right lung and two lobes in the left one. The lungs are cone shaped and made of elastic, spongy tissue. Within the lungs, the bronchi branch out into minute pathways that go through the lung tissue. The pathways are called bronchioles, and they end at microscopic air sacs called alveoli. The alveoli are surrounded by capillaries and provide oxygen for the blood in these vessels. The oxygenated blood is then pumped by the heart throughout the body. The alveoli also take in carbon dioxide, which is then exhaled from the body.Inhaling is due to contractions of the diaphragm and of muscles between the ribs. Exhaling results from relaxation of those muscles. Each lung is surrounded by a two-layered membrane, or the pleura, that under normal circumstances has a very, very small amount of fluid between the layers. The fluid allows the membranes to easily slide over each other during breathing.
PATHOPHYSIOLOGY
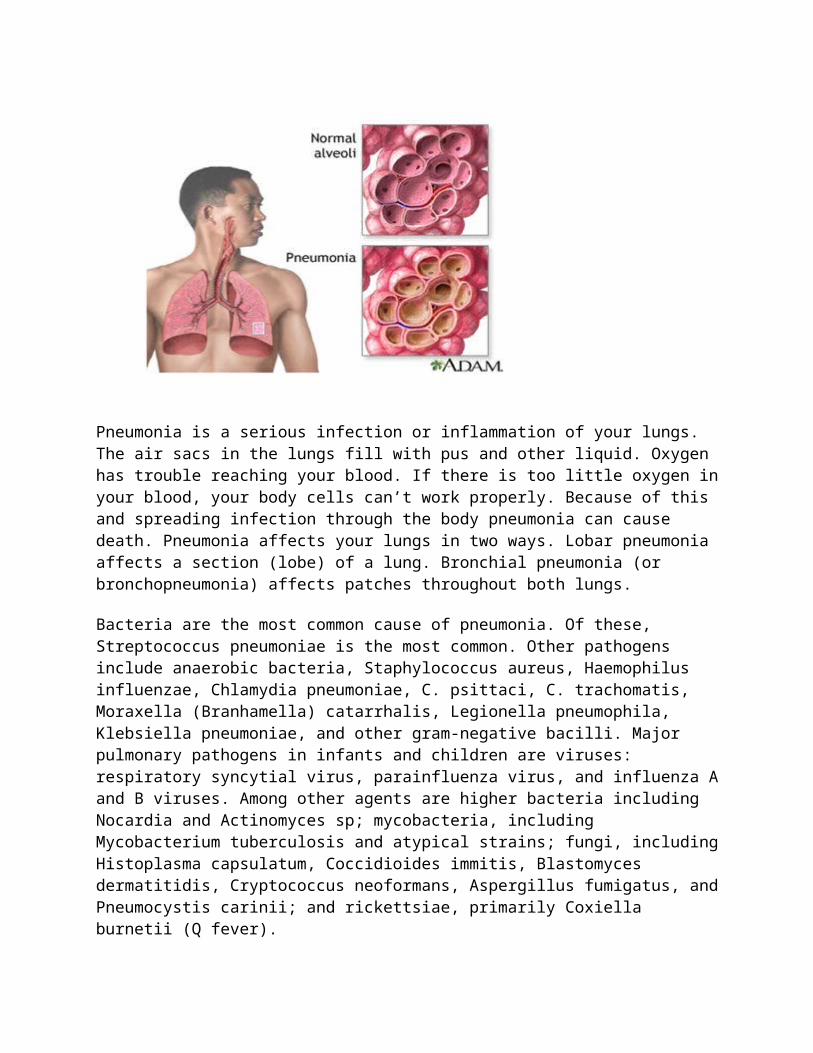
Pneumonia is a serious infection or inflammation of your lungs. The air sacs in the lungs fill with pus and other liquid. Oxygen has trouble reaching your blood. If there is too little oxygen in your blood, your body cells can’t work properly. Because of this and spreading infection through the body pneumonia can cause death. Pneumonia affects your lungs in two ways. Lobar pneumonia affects a section (lobe) of a lung. Bronchial pneumonia (or bronchopneumonia) affects patches throughout both lungs.
Bacteria are the most common cause of pneumonia. Of these, Streptococcus pneumoniae is the most common. Other pathogens include anaerobic bacteria, Staphylococcus aureus, Haemophilus influenzae, Chlamydia pneumoniae, C. psittaci, C. trachomatis, Moraxella (Branhamella) catarrhalis, Legionella pneumophila, Klebsiella pneumoniae, and other gram-negative bacilli. Major pulmonary pathogens in infants and children are viruses: respiratory syncytial virus, parainfluenza virus, and influenza A and B viruses. Among other agents are higher bacteria including Nocardia and Actinomyces sp; mycobacteria, including Mycobacterium tuberculosis and atypical strains; fungi, including Histoplasma capsulatum, Coccidioides immitis, Blastomyces dermatitidis, Cryptococcus neoformans, Aspergillus fumigatus, and Pneumocystis carinii; and rickettsiae, primarily Coxiella burnetii (Q fever).
The usual mechanisms of spread are inhaling droplets small enough to reach the alveoli and aspirating secretions from the upper airways. Other means include hematogenous or lymphatic dissemination and direct spread from contiguous infections. Predisposing factors include upper respiratory viral infections, alcoholism, institutionalization, cigarette smoking, heart failure, chronic obstructive airway disease, age extremes, debility, immunocompromise (as in diabetes mellitus and chronic renal failure), compromised consciousness, dysphagia, and exposure to transmissible agents.
Typical symptoms include cough, fever, and sputum production, usually developing over days and sometimes accompanied by pleurisy. Physical examination may detect tachypnea and signs

of consolidation, such as crackles with bronchial breath sounds. This syndrome is commonly caused by bacteria, such as S. pneumoniae and H. influenzae.
What is the Pathophysiology of Pneumonia
Pneumonia is a commonly occurring serious disease that affects about 1 out 100 people every year. As mentioned above, many factors are responsible for development of pneumonia. Pneumonia can be divided into various categories like community acquired and hospital acquired infection. The common type of community acquired infection is pneumococcal pneumonia and Mycoplasma pneumonia. Many times in people with lowered immunity or geriatric patients, pneumonia is seen after a bout of influenza. Most of the hospital acquired infections of pneumonia are the serious infections, as they body lacks the mechanism to fight against the condition. Aspirational pneumonia, pneumonia in immunocompromised host and viral pneumonia are some of the pneumonia related specific disorders. Let us go into the details of pathophysiology of pneumonia. You can read more about chronic pneumonia and acute pneumonia.
The causative agent or organism gains entry into the body through the respiratory tract by way of inspiration or aspiration of oral secretions. The organisms that can reach the lungs through blood circulation are staphylococcus and gram negative bacilli. You can read more on bacterial pneumonia.
The body's defense mechanism, that is, pulmonary defense mechanism in case of lungs comes into action. A cough reflex, mucocillary transport and pulmonary macrophages try to protect the body against the infection. However, in some people there defense mechanism is either suppressed or overwhelmed by the invading agent and leads to development of infection. You can read more on mycoplasma
pneumonia symptoms.
The invading organism starts to multiply and release damaging toxins that cause inflammation and edema of the lung parenchyma. This action leads to accumulation of cellular debris and exudes within the lungs. Soon the airless state of the lungs is changed to a consolidated state due to the fluid and exudate filling up.
The ciliated epithelial cells are damaged in case of viral pneumonia. The virus reach the lungs through air borne droplets inhaled through the mouth and nose. The virus after gaining entry into the lungs, begins an invasion of the cell lining of the airways and alveoli. This leads to cell death by direct action of the virus or through a cell controlled self destruction called apoptosis. With the body's response to the invasion, there is further damage to the lungs as the fluid is leaked into the alveoli. Viral infection of the lungs damages the lungs and makes them even more susceptible to bacterial infections. This complicated the matters even more in viral pneumonia. You can read more on viral pneumonia symptoms.
The fungal pneumonia is a rare condition, and is often seen in individuals with compromised immune system like AIDS, etc. The pathophysiology of pneumonia in case of fungal invasion is very much similar to bacterial pneumonia. The most common fungal agents that cause pneumonia are Histoplasma capsulatum, Cryptococcus neoformans, Pneumocystis jiroveci, blastomyces and Coccidioides immitis.
Pathophysiology of pneumonia caused by parasites occurs when they travel to the lungs by gaining entry through skin or begin swallowed. There is cellular destruction and immune response that leads to disruption of oxygen transportation. The common parasite that causes pneumonia are Toxoplasma gondii, Strongyloides stercoralis and Ascariasis
Pathophysiology of anemia and nursing care implications
MedSurg Nursing, April, 2008 by Sharon M. Coyer, Ayhan Aytekin Lash
1 2 3 4 5 6 7 8 9 10 Next
As many as 4 million Americans have anemia; women younger than age 65 have six times more anemia than men. Anemia is increasingly a health problem for older adults, especially men over age 85 (Goddard, McIntyre, & Scott, 2000). Anemia occurs when there is a decrease in red blood cell numbers or a decrease in the amount of hemoglobin (Gaspad, 2005; Hodges, Rainey, Lappin, & Maxwell, 2007; Kumar, Cotran, & Robbins, 2003). It is recognized most often when laboratory screening tests are done because individuals often do not present with the signs and symptoms of advanced anemia. Acute anemia usually is due to blood loss or hemolysis (Adamson & Longo, 2001). Gastrointestinal bleeding or bleeding from colon cancer can cause chronic blood loss that also produces anemia (Goddard et al., 2000). In this article, the pathophysiology of anemia, clinical manifestations, and selected diseases that cause anemia will be reviewed, and the implications for nursing practice discussed.
More Articles of Interest
Documentation of anemia management interventions. Case study of the anemic... Anemia Management: Recognizing Opportunities and Improving Outcomes Through... Patient education and the nursing process: meeting the patient's needs Management of Anemia in Chronic Kidney Disease Patients: Nephrology Nursing... Anemia: Pointing the way to a deeper problem
PATHOPHYSIOLOGY OF ANEMIA
All blood cells are produced by hematopoiesis in the bone marrow. The major raw material essentials for this process are proteins, vitamin [B.sub.12], folic acid, and iron. Table 1 shows the substances needed for hematopoiesis in this well-orchestrated cell function. Pathophysiology of anemia differs according to its etiology. Acute or chronic red blood cell loss, inadequate production of red blood cells in the bone marrow, or an increased hemolysis can produce anemia (Gaspad, 2005; Hodges et al., 2007). When anemia develops because of hemorrhage, the

reduction in red blood cell numbers causes a decrease in blood volume and the cardiovascular (CV) system becomes hypovolemic. Anemia becomes evident when the maximum level of hemodilution occurs, usually within 3 days after the acute blood loss. Hemodilution occurs in response to decreased blood volume when fluid moves from the interstitium into the intravascular space to expand the plasma volume. The decrease in blood viscosity from the lower number of red blood cells, along with increased intravascular fluid, causes the blood to flow faster through the CV system and the flow becomes more turbulent. This process causes pressure on the ventricles, the heart dilates, and heart valve dysfunction develops (Metivier, Marchais, Guerin, Pannier, & London, 2000).
Hypoxia contributes to the changes in the CV and respiratory systems in anemia by causing the blood vessels to dilate and the heart to contract more forcefully, which further increases the demand for oxygen. Tissue hypoxia causes the rate and depth of breathing to increase. Hemoglobin, the oxygen-carrying protein in the red blood cells (RBCs), releases that oxygen to the tissues more rapidly. When anemia becomes severe, the body directs blood to the vital organs, such as the heart and the brain, and renal blood flow decreases. Decreased renal blood flow in turn causes an activation of the renin-angiotensin system response, leading to salt and water retention. This process increases blood volume to improve kidney function without changing tissue hypoxia in other organs (Gaspad, 2005; Metivier et al., 2000).
Hemolytic Anemia
The pathophysiology of hemolytic anemia involves the destruction of erthythrocytes and the subsequent acceleration of erythropoesis. Hemolytic anemia may be inherited or acquired. The inherited form occurs from cellular abnormalities in the membrane or the enzymes that influence the production of hemoglobin. Acquired hemolytic anemia occurs as a result of infection, chemical agents, and abnormal immune response. Hemolytic anemia produces hemolyis within the blood vessels or lymphoid tissue that filters blood. Immunohemolytic anemias are caused by extravascular hemolysis and associated with autoimmune mechanisms or drug reactions (Hodges et al., 2007; Mansen & McCance, 2006).
CLASSIFICATION OF ANEMIA Classification by Morphology
Anemia can be classified by cell morphology or by etiology. Morphology, the most common classification, includes cell size (cystic), color (chromic), and shape of the RBCs. Measurements of hemoglobin, hematocrit, and red cell indices provide information about the appearance of the RBC, which aids in the classification. Red cell indices include the mean corpuscular volume, mean hemoglobin, mean corpuscular hemoglobin concentration (MCHC), and red blood cell distribution width (Hoekelman, Adam, Nelson, Weitzman, & Wilson, 2001). In addition, serum ferritin concentration is used to measure iron storage. Measuring ferritin concentration is important in obtaining the diagnosis of iron deficiency anemia. Another test, transferrin saturation, measures dietary iron absorption and transport. Transferrin is the protein to which iron is bound for transport from within the body (Lemone & Burke, 2004; Rote & McCance, 2008; Uphold & Graham, 2003).
Classification by Etiology

Anemia can be caused by impaired cell production, blood loss, and increased rate of destruction of the red cell. Blood loss occurs during acute conditions such as trauma, or chronic diseases and gastrointestinal bleeding. Increased rate of destruction of red cells occurs in hemolytic anemia resulting from conditions inside and outside the cell. Abnormalities within the red cell can result from hereditary or acquired disease. Sperocytosis and elliptocytosis are hereditary conditions causing anemia due to a disorder in the red cell membrane. Disorders in enzymes within the red cell, such as glucose-6-phosphate dehydrogenase and pyruvate synthesis diseases, also can cause anemia. Sickle cell anemia and thalessemia are genetically determined diseases in which RBCs have structural abnormalities (Kumar et. al., 2003).
.
When the body breathes in, the air is drawn into the respiratory system, where it takes a journey throughout the body and then leaves once again in the form of altered gases as waste in the same manner it entered. Dividing the respiratory system into two basic components, upper and lower, it is organized and well understood. The respiratory system is responsible for the exchange of gases, the production of sound, and the assistance of abdominal compression. The most, obvious, the exchange of gases, is its primary function which sustains life.
Respiration as a gaseous exchange refers to the functions, separate yet interdependent. Ventilation is the action of the body’s natural response to breathe in and exhale. The exchange of gases occurs initially between the air and the lungs, then the lungs and the blood cells within the lungs, and finally between the blood cells and the body’s tissue. Oxygen utilization occurs when the body’s tissues creates energy from the oxygenated cells and then return to the cells carbon dioxide which is considered a waste for those cells. This process is known as the process of respiration.
External respiration occurs when the gases are exchanged, oxygen for carbon dioxide with a few other lesser vital gases mixed in there, and then released from the body with the action of exhaling. Internal respiration occurs when the gases are exchanged between the blood cells and the body’s tissues.
On average, an adult body at rest breathes approximately fifteen times per minute and exchanges six liters of air in this time frame, resulting in eight thousand liters exchanged in a twenty four hours duration. An adult body under physical duress increases the need for gaseous exchange by either fifteen or twenty times the resting rate. This results in approximately one hundred liters of air passing through the lungs every minute.
The average adult body will lose consciousness after four, perhaps five, minutes. Brain damage is likely after seven minutes of oxygen deprivation and death usually occurs within eleven minutes.
The respiratory system is a complex and vital part of the human body. With even a laps in the appropriate functions, life and death become eminent. The respiratory system must be fully operation to sustain life or life with quality. To be considered functional, the respiratory system must possess six basic required functions.
The first required function includes the location of the gaseous exchange, as it must occur deep within the lungs so that the air has had a chance to be warmed, moistened, and cleansed on its journey to be exchanged for waste gases. Air born particles must be removed during the oxygen’s journey deep into the lungs.

Secondly, the membrane lining of the lungs must be moist, as carbon dioxide and oxygen can undergo the process of gaseous exchange only in water-like material. This process is called diffusion and can not happen in a dry lung.
The respiratory system must have an extensive network of capillaries to allow the exchange of oxygen within the body’s tissues. An incompetent network of capillaries will result in some of the body’s tissue being denied life sustaining oxygen.
The respiratory system relies on a competent and efficient ventilation mechanism in order for there to be ample replenishment of the necessary oxygen. The body’s tissue can not survive off of a minimal amount of oxygenation.
The respiratory system must be able to function automatically and not require constant conscious monitoring. Monitoring and feedback must all happen automatically throughout the body in order for the respiratory system to respond appropriately. The system also requires a conscious over ride in order to intentionally create a variance in airflow if desired or needed.
By meeting these basic necessities, the respiratory system is designed with very intricate but purposeful properties, which allow it to take on a variety of responsibilities. The metabolic process and the sustaining of life relies entirely on the functions of these basic principles.
The respiratory system is responsible for providing the blood stream with life sustaining oxygen while removing toxic waste gases, enables the production of sound by passing over the vocal cords which in turn cause vibration, and is partially responsible for the compression of the abdominal muscles which assist in urination, defecation, and child birth

as well as assists in laughter and other basic bodily functions surrounding the abdomen. The abdominal muscles rely on the respiratory system for functions which require significant exertion, as these muscles become more effective with a rush of extra oxygen, hence the natural desire to take a deep breath when pushing the abdominal muscles or even lifting a heavy object. In numerous ways, the back muscles benefit similarly from a rush of fresh oxygen.
Without the respiratory functions as they are designed, protective reflexes that require a lapse in breath such as coughing, sneezing, or hiccupping could not effectively occur. These reflexes enable the body to reject foreign substances and keep them from entering the body via the respiratory system.
The structure, design, and passages involving the respiratory system are quite extensive and include the nasal cavity, the larynx, the trachea, the pharynx, the bronchi, the bronchioles, and the pulmonary alveoli within the lungs. The upper respiratory system is segregated by the nasal passages, the pharynx, and the associated and necessary related structures while the lower respiratory system is segregated by the larynx, the trachea, the bronchiole system, the pulmonary alveoli, and the lungs. To keep the segregation and division of the respiratory system simple, it is typically divided by the generalization of conduction and respiration. A percentage of the respiratory system is divided up by its ability to relate to breathing in while the other half is associated with the body’s need for transportation of elements. These divisions are known as the respiratory division and the conduction division, respectively.
The conduction division is created by any and all relative structures or cavities that “conduct” the gases in either form to and from the pulmonary alveoli while the respiratory division is defined by the pulmonary alveoli as well as any and all cavities or relative structures that assist with the exchange of gases in either form between the air and the blood.
The respiratory system, as complex and intricate as it is, is also quite viable and strong. The system is designed to compliment and function cooperatively with other systems to create and sustain life, energy, and endurance in nearly any reasonable situation.
Respiratory System videos
Respiratory System
Organs included in Respiratory System

Alveoli Bronchial tree
Larynx Lungs Nose
Paranasal sinuses Pharynx Pleurae
Trachea
Now get homework help from our live expert on rea ltime basis
Join us and get homework help
http://homeworkping.com/