38th adrian e. flatt residents & fellows conference
TRANSCRIPT

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain.
38th Adrian E. Flatt Residents & Fellows
Conference
Co-Chairs: Daniel A. Osei, MD, MSc and Samir K. Trehan, MD
Program Syllabus
September 30, 2020
75TH ANNUAL MEETING OF THE ASSH
OCTOBER 1 – 3, 2020
822 West Washington Blvd
Chicago, IL 60607
Phone: (312) 880-1900
Web: www.assh.org
Email: [email protected]

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain.
38th Adrian E. Flatt Residents & Fellows
Conference
Sponsored by the American Foundation for Surgery of the Hand, The Adrian E. Flatt Residents
and Fellows Conference in Hand Surgery is specifically geared to hand surgery fellows and
residents in orthopaedic, plastic and general surgery. The conference includes review of common
hand surgical conditions, interactive case discussions with small group faculty, review of
resources/opportunities available through the American Society for Surgery of the Hand, invited
faculty lectures on topics specifically relevant to trainees (such as starting practice, career
planning and burnout), and a scientific program where residents and fellows present original
research. Participants are invited to submit research abstracts relevant to hand and upper
extremity surgery.
CME CREDIT HOURS
The ASSH designates this live activity for a maximum of 5.00 AMA PRA Category 1 Credits TM.
Physicians should claim only the credit commensurate with the extent of their participation in the
activity.
The ASSH is accredited by the Accreditation Council for Continuing Medical Education to
provide continuing medical education for physicians.
DISCLAIMER
The material presented in this continuing medical education program is being made available by
the American Society for Surgery of the Hand for educational purposes only. This material is
not intended to represent the best or only methods or procedures appropriate for the medical
situation discussed; rather the material is intended to present an approach, view, statement or
opinion of the authors or presenters, which may be helpful, or of interest to other practitioners.
The attendees agree to participate in this medical education program, sponsored by ASSH with
full knowledge and awareness that they waive any claim they may have against ASSH for
reliance on any information presented in this educational program. In addition, the attendees
also waive any claim they have against the ASSH for injury or other damage that may result in
any way from their participation in this program.
All of the proceedings of the 75th Annual Meeting, including the presentation of scientific
papers, are intended for limited publication only, and all property rights in the material
presented, including common-law copyright, are expressly reserved to the speaker or the ASSH.
No statement or presentation made is to be regarded as dedicated to the public domain. Any
sound reproduction, transcript or other use of the material presented at this course without the

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain.
permission of the speaker or the ASSH is prohibited to the full extent of common-law copyright
in such material.
The ASSH is not responsible for expenses incurred by an individual who is not confirmed and
for whom space is not available at the meeting. Costs incurred by the registrant such as airline or
hotel fees or penalties are the responsibility of the registrant.
The approval of the U.S. Food and Drug Administration is required for procedures and drugs that
are considered experimental. Instrumentation systems discussed and/or demonstrated in or at
ASSH educational programs may not yet have received FDA approval.
Claim your CME hours through www.ASSH.org
• How to Claim: You can claim your CME for attending the live event in the same
way you've claimed CME at previous ASSH Annual Meetings. Simply login to your
ASSH account, choose the 75th Annual Meeting of the ASSH, and indicate which
sessions you attended.
Physicians should claim only the credit commensurate with the extent of their
participation in the activity.
Questions? Problems? Contact the American Society for Surgery of the
Hand at (312) 880-1900 or by email at [email protected].

Conflict of Interest Disclosures for 2020
Program Committee and Course Faculty
Program Faculty & Disclosures
The American Society for Surgery of the Hand gratefully acknowledges those who have
generously volunteered considerable time and effort to plan, organize and present this CME
course. The ASSH appreciates the faculty’s dedication to teaching, their support of the ASSH
mission, and their significant contribution to the educational success of this program.
The following is a list of disclosures for all participating faculty and program staff.
CONFLICT OF INTEREST POLICY
According to the ASSH conflict of interest policy, individuals involved in continuing medical
education activities are required to complete a disclosure statement. The ASSH acknowledges
this fact solely for the information of the listener. Non-conflicted reviewers have examined,
documented and resolved financial relationship disclosures for this course content.
Financial Disclosure – represented by ●
Instructors, planners, content reviewers and managers who affect the content of a CME/CE
activity are required to disclose financial relationships they have with commercial interests (i.e.
any entity producing, marketing, pre-selling, or distribution health care goods or services
consumed by, or used on, patients) associated with this activity.
FDA Disclosure – represented by ▲
Some drugs or medical devices demonstrated at this course may have not been cleared by the
FDA or have been cleared by the FDA for specific purposes only. The FDA has stated that it is
the responsibility of the physician to determine the FDA clearance status of each drug or medical
device he or she wishes to use in clinical practice.
The ASSH policy provides that “off label” uses of a drug or medical device may be described in
the ASSH CME activities so long as the “off label” use of the drug or medical device is also
specifically disclosed (i.e., it must be disclosed that the FDA has not cleared the drug or device
for the described purpose). Any drug or medical device is being used “off label” if the described
use is not set forth on the product’s approval label.

Planners
2020 Annual Meeting Program Chairs
Dawn M. LaPorte, MD
No relevant conflicts of interest to disclose
Ryan P. Calfee, MD, MSc
No relevant conflicts of interest to disclose
Session Co-Chairs/Moderators
Daniel A. Osei, MD, MSc
No relevant conflicts of interest to disclose
Samir K. Trehan, MD
No relevant conflicts of interest to disclose
Faculty
Martin I. Boyer, MD, FRCS(C)
● Intellectual Property: Exsomed, LLC (patent submitted)
● Consulting Fees: Exsomed. LLC; Hand Surgery Medicolegal Consultation; A Gift of Hope
Adoptions
Joseph A. Buckwalter, MD
No relevant conflicts of interest to disclose
Kevin Chan, MD
No relevant conflicts of interest to disclose
A. B. Chhabra, MD
No relevant conflicts of interest to disclose
Rafael J. Diaz-Garcia, MD
● Consulting Fees: Axogen, TelaBio and Smith + Nephew
Christopher J. Dy, MD, MPH, FACS
No relevant conflicts of interest to disclose
Felicity Fishman, MD
No relevant conflicts of interest to disclose
Paige M. Fox, MD, PhD
No relevant conflicts of interest to disclose

Michael J. Franco, MD
No relevant conflicts of interest to disclose
Louis Christopher Grandizio, DO
No relevant conflicts of interest to disclose
Curtis M. Henn, MD
No relevant conflicts of interest to disclose
Nikolas H. Kazmers, MD, MSE
No relevant conflicts of interest to disclose
Scott D. Lifchez, MD, FACS
● Ownership Interests: Co-founder and equity holder of EduMD, LLC, an educational
assessment company that makes the Operative Entrustability Assessment surgical assessment
tool.
Mary Claire Manske, MD
No relevant conflicts of interest to disclose
Walter B. McClelland, Jr., MD
● Consulting Fees: MicroAire, Acumed
Kenneth R. Means, Jr., MD
● Contracted Research: Axogen
Gregory A. Merrell, MD
No relevant conflicts of interest to disclose
Daniel J. Nagle, MD
No relevant conflicts of interest to disclose
Sameer Kumar Puri, MD
No relevant conflicts of interest to disclose
Peter C. Rhee, DO, MS
● Consulting Fees: TriMed Inc., Integra LifeSciences
Julie B. Samora, MD, PhD
● Consulting Fees: (Spouse) Walter Samora with Globus Medical
Apurva S. Shah, MD, MBA
No relevant conflicts of interest to disclose

Steven S. Shin, MD
● Royalty: Arthrex Hely & Weber
● Consulting Fees: Arthrex
● Speakers Bureau: Arthrex
Brandon S. Smetana, MD
● Consulting Fees: Axogen
● Speakers Bureau: Axogen
Eric R. Wagner, MD
● Consulting Fee: Stryker, Wright Medical
● Contracted Research: Arthrex
Lindley B. Wall, MD
No relevant conflicts of interest to disclose

38th Adrian E. Flatt Residents & Fellows Conference Co-Chairs: Daniel A. Osei, MD, MSc and Samir K. Trehan, MD
Description
Sponsored by the American Foundation for Surgery of the Hand, The Adrian E. Flatt Residents
and Fellows Conference in Hand Surgery is specifically geared to hand surgery fellows and
residents in orthopaedic, plastic and general surgery. The conference includes review of common
hand surgical conditions, interactive case discussions with small group faculty, review of
resources/opportunities available through the American Society for Surgery of the Hand, invited
faculty lectures on topics specifically relevant to trainees (such as starting practice, career
planning and burnout), and a scientific program where residents and fellows present original
research. Participants are invited to submit research abstracts relevant to hand and upper
extremity surgery.
Program
3:00 PM - 8:00 PM
Daniel A. Osei, MD, MSc | Samir K. Trehan, MD
3:00 PM - 3:05 PM
Welcome
Daniel A. Osei, MD, MSc | Samir K. Trehan, MD
3:05 PM - 3:10 PM
Introduction
Martin I. Boyer, MD, FRCS(C)
3:10 PM - 3:15 PM
Adrian Flatt Memorial
Daniel A. Osei, MD, MSc
3:15 PM - 3:30 PM
Research
Nikolas H. Kazmers, MD, MSE
3:30 PM - 3:45 PM
Nerve Repair
Kevin Chan, MD

3:45 PM - 3:55 PM
Nerve Case Presentation
Rafael J. Diaz-Garcia, MD
3:55 PM - 4:05 PM
Distal Radius Fracture
Sameer Kumar Puri, MD
4:05 PM - 4:15 PM
Wrist Case Presentation
Louis Christopher Grandizio, DO
4:15 PM - 4:20 PM
Private Practice Career
Walter B. McClelland, Jr., MD
4:20 PM - 4:25 PM
Privademics Career
Kenneth R. Means, Jr., MD
4:25 PM - 4:30 PM
Academic Career
Julie B. Samora, MD, PhD
4:30 PM - 4:45 PM
Panel: PP, Privademics, Academics
Walter B. McClelland, Jr., MD | Kenneth R. Means, Jr., MD | Julie B. Samora, MD, PhD
4:45 PM - 4:50 PM
Break
All Faculty
4:50 PM - 4:55 PM
Boyes Award
Daniel A. Osei, MD, MSc | Samir K. Trehan, MD
4:55 PM - 5:05 PM
Sports Injuries of Hand
Steven S. Shin, MD
5:05 PM - 5:20 PM
Pediatric Fractures
Lindley B. Wall, MD | Apurva S. Shah, MD, MBA

5:20 PM - 5:30 PM
Pediatric & Trauma Case Presentation
Mary Claire Manske, MD
5:30 PM - 5:50 PM
Panel: Pearls for Starting Practice
Joseph A. Buckwalter, MD | Peter C. Rhee, DO, MS | Gregory A. Merrell, MD
5:50 PM - 5:55 PM
Fellowship Update
A. B. Chhabra, MD
5:55 PM - 5:56 PM
Introduction to Richard Smith Lecture
Martin I. Boyer, MD, FRCS(C)
5:56 PM - 6:26 PM
Richard Smith Lecture
Christopher J. Dy, MD, MPH, FACS | Paige M. Fox, MD, PhD
6:26 PM - 6:46 PM
Physician Value
Daniel J. Nagle, MD
6:46 PM - 6:56 PM
Hand/Finger Flaps
Michael J. Franco, MD
6:56 PM - 7:09 PM
Arthritis Case Presentation
Eric R. Wagner, MD
7:09 PM - 7:11 PM
Mary S. Stern Scholarship Announcement
Daniel A. Osei, MD, MSc | Samir K. Trehan, MD
7:11 PM - 7:31 PM
Nightmare Cases: Lessons I Learned Early in Practice
Curtis M. Henn, MD | Brandon S. Smetana, MD
7:31 PM - 7:41 PM
Ethics: COI
Felicity Fishman, MD

7:41 PM - 7:55 PM
Ethics: Burnout
Scott D. Lifchez, MD, FACS
7:55 PM - 8:00 PM
Closing remarks
Daniel A. Osei, MD, MSc | Samir K. Trehan, MD

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
3:15 PM - 3:30 PM
Research
Nikolas H. Kazmers, MD, MSE No relevant conflicts of interest to disclose

9/18/2020
1
DISCLOSURES
Nikolas H. Kazmers, MD, MSE
Speaker has no relevant financial relationships
with commercial interest to disclose.
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
Incorporating Research
Into your New PracticeNikolas H. Kazmers, MD MSE
Department of Orthopaedics
September 30, 2020
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
DISCLOSURES
• No financial disclosures
• JHS Am Associate Editor
1
2
3

9/18/2020
2
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
OUTLINE
• The need for clinical research
• Common barriers
– Balance
• Clinical practice
• Personal / family life
– Resources
• Monetary
• Non-monetary
• Strategies to address barriers
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
THE NEED FOR CLINICAL RESEARCH
• Often no literature pointing to the “right answer”
• Expand the knowledge base of our subspecialty
– Broad spectrum of pathology
• Complete understanding is lacking for:
– Anatomy
– Diagnosis
– Treatment
– Measurement of outcomes
– Costs and value
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
THE NEED FOR CLINICAL RESEARCH
Why you?
• You are best equipped, and…
– There’s a lot we don’t know!!!!!
– Consistently work with the patient population
– Observe trends and patterns
– Pros and cons of treatment options
– Recognize when literature is lacking
– Were hired to do it!
4
5
6

9/18/2020
3
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
COMMON BARRIERS
• Balancing Clinical Practice:
– 3 A’s:
• Availability, affability, ability
– Growing pains of a new practice:
• Lots of reading for patient care
• How do I do this surgery?
• Clinic and OR workflow
• Getting to know your team
• Meet & greet referring physicians
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
COMMON BARRIERS
• Balancing Personal Life / Family:
– Adjustment to a new location
– New living situation
– New friends and social scene
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
COMMON BARRIERS
• Resources for Research:
– Monetary
– Non-monetary
• Ideas / questions and the
patient population to tackle
them
• Statistics help
• Collaborators
• Chart review
• IRB considerations
8
9
10

9/18/2020
4
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
• Residency and Fellowship Contacts:
– Opportunity to continue projects that may not
be immediately feasible in your new practice
– May have a more developed infrastructure
– Familiarity
– Don’t forget about current trainees
– Caveat: will want to branch out and develop your own program over time
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
• Things to Consider when On-Boarding:
– Salary vs support
• Research stipend
• Research assistant/coordinator
• Infrastructure for patient follow-up / PRO collection
• Access to statisticians / databases
• Master’s programs
11
12
13

9/18/2020
5
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
• Things to Consider when On-Boarding:
– What are your partners working on / interested
in?
• Opportunity to jump-start select projects
– Research assistant/coordinator job search
– Schedule / academic day?
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
• Help with Pending Projects:
– Opportunity to make progress before your own
ideas take off
– Tackle loose ends and drive it home
• Remaining data collection, analysis, editing, etc
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
• Get to Know the Residents (and Fellows):
– Smart, eager, and hard-working
– Need at least 1 research project
– If you are approachable and accessible:
• They will ask you interesting clinical questions
• May ask you for mentorship
14
15
16

9/18/2020
6
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
• Be a Useful Resource to Medical Students:
– Also are smart, eager, and hard-working
– Orthopaedics / plastics training is competitive
• Advice
• Interest groups
• Opportunity to collaborate on projects
– Approachability and accessibility
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
• Identify Motivated Collaborators:
– Answer questions you can’t alone
• MSK Radiology
• Rheumatology
• Emergency Medicine
• Health Economics
• Engineering Department
• Laboratory
– Your microsurgery skills are unique
• Ortho / Plastics (esp. if separate programs)
→ Finding the right team is they key
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
STRATEGIES TO ADDRESS BARRIERS
• Miscellaneous:
– What are your non-hand colleagues are working on?• Read CVs
• Skim non-hand journals
– Write down your research ideas
– “Night school” analogy
– Take advantage of unique pathology / unique resources
– Take advantage if ‘not busy’
17
18
21

9/18/2020
7
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
SUMMARY
• Barriers exist
• Ways to overcome some of them exist
• Mentorship makes it more fun
• Study what is feasible, yet interesting to you,
and important to the hand community
• Find a niche
© U N I V E R S I T Y O F U T A H H E A L T H , 2 0 1 8
THANK YOU
22
23

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
3:30 PM - 3:45 PM
Nerve Repair
Kevin Chan, MD No relevant conflicts of interest to disclose

9/29/2020
1
DISCLOSURES
Kevin Chan, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
Nerve repairs
Kevin Chan MD
Clinical Assistant Professor
Spectrum Health | Michigan State University
Basic science of nerve regeneration
• Within injured axon, rapid influx of ions (calcium) and disruption of transport protein signalling leads to upregulation of RAG in neurons → promotes axonal outgrowth
• Distally, Wallerian degeneration occurs»Schwann cells dedifferentiate to “repair”
phenotype: clear axon and myelin debris, upregulate neurotrophic factors
»Recruits innate immune cells (neutrophils, macrophages): phagocytic function, promote angiogenesis
»SC migrate down this network, forming cellular cords with fibroblasts, which enables axon growth across nerve defect
Pan et al. Advances in the repair of segmental nerve injuries and trends
in reconstruction. Muscle Nerve. 2020;61:726–739.
1
2
3

9/29/2020
2
Where is the lesion?
• PIN MCP extension
Thumb IP extension
– Radial wrist extension– Radial nerve
Wrist extension
BR
Triceps
– Sensory loss
• 1st webspace vs posterior aspect of arm & posterolateral arm
• Posterior cordAxillary nerve, thoracodorsal n
• C7 radiculopathyPronator teres, FCR
– Sensory loss middle finger
Radial Nerve Reinnervation
• Reinnervation order can be variable
• Order of innervation of the radial nerve (proximal to distal):
1. brachioradialis
2. extensor carpi radialis longus,
3. supinator
4. extensor carpi radialis brevis
5. extensor digitorum communis
6. extensor carpi ulnaris
7. extensor digiti quinti
8. abductor pollicis longus
9. extensor policis longus
10. extensor policis brevis
11. extensor indicis proprius.
Abrams RA, Ziets RJ, Lieber RL, Botte MJ. Anatomy of the radial nerve motor
branches in the forearm. J Hand Surg Am. 1997 Mar;22(2):232-7.
4
5
6

9/29/2020
3
Beware of median-ulnar interconnections
• Forearm: Martin-Gruber anastomosis
• Hand: Riché-Cannieu anastomosis
• May account for preservation of muscle function even if median/ulnar
nerves are not intact
– E.g. The MGA between the median and ulnar nerves can account for
intrinsic function despite the presence of a more proximal ulnar lesion
Grades 1, 2, 3 “Favorable, recoverable” vs grades 4, 5 “non-favorable, non-
recoverable”
Non-op vs op
Mackinnon SE. Nerve Surgery. Thieme 2015.
7
8
9

9/29/2020
4
Distinguishing nerve injury severity
• History and physical exam
- Mechanism of injury: blunt vs penetrating trauma
• EDX
- Presence of fibrillations distinguish a neurapraxia from more severe injuries
- MUAPs are absent in fourth/fifth degree injuries
- MUAPs can signify collateral sprouting as early as 12 weeks postinjury in
second/third degree injuries
Will it make it?
• Nerves regenerate at ~ 1 mm/day or 1 inch/month
• Irreversible motor end plate degeneration by 12-18 months post-injury
• Motor recovery dependent on time to muscle reinnervation and number
of regenerated motor axons
10
11
12

9/29/2020
5
The value of Tinel’s test
• The progress of nerve regeneration can be followed using the Tinel’s
test
• Reflects axons that have not obtained myelinization
• An advancing Tinel’s test with distal radiation is a promising sign for
regenerating axons across nerve repair site
Principles of nerve repairs
• Timing
• Trim
• Tension
• Technique
13
14
15

9/29/2020
6
“Timing”
1. Better functional outcomes occur in patients with
spontaneous recovery who do not require a surgical
intervention
2. Surgical intervention is indicated for patients with no hope
for spontaneous recovery or for further recovery
3. Surgical outcome is inversely proportional to the time
interval from injury to surgery (i.e., outcomes are better if
surgery is per- formed earlier)
Timing of nerve repairs
• Sharp, penetrating injuries
• Injuries with high index of suspicion for nerve transection
• Observe blunt injuries, crush, avulsion for signs of spontaneous
recovery:
- EDX around 8-12 weeks postinjury
- EDX may precede clinical evidence of returning muscle function
- MUAPs signify nerve recovery
‘Technique’: Types of Nerve Repair
Mackinnon SE. Nerve Surgery. Thieme 2015.
16
17
18

9/29/2020
7
“Trim”
• Recognize “zone of injury”: scarring of nerve following injury; inhibits
nerve recovery; not fully present until about 3 weeks after injury
Mackinnon SE. Nerve Surgery. Thieme
2015.
“Bread loaf”
“Tension”
• Excess tension leads to ischemia and scar formation
• When faced with a nerve laceration, how much tension and strain is too
much?
• Smetana et al (JHS 2019) recommended using 9-0 nylons
Treatment of nerve gaps
• Autogeneous nerve graft
• Processed acellular allograft
• Nerve conduits
• Nerve transfers
Moore A. Processed acellular nerve grafts. 2018
19
20
21

9/29/2020
8
Autografts
• Sural
• MABC
• LABC
• PIN
PART
V
NERV
E
38
1252
Important attributes of nerve transfers are as follows:
1. Closer to the end-organ (increased likelihood of more
rapid or more reliable recovery, or both)
2. Delivery of a large number of “ pure” axons
3. Repair outside the injured and scarred zone
4. Avoidance of nerve graft and their two repair sites
5. Ease of relearning, especially with synergistic transfers
Common intraplexal and extraplexal nerve transfers are
described in the following sections.
Spinal Accessory Nerve Transfer
SURGICAL ANATOMYThe spinal accessory nerve (cranial nerve XI) innervates the
sternocleidomastoid and trapezius muscles. It originates in
the posterior cranial fossa from spinal and cranial nerve
roots, passes through the jugular foramen, and divides into
an internal branch (containing fibers originating from the
“ cranial part” ) that joins the vagus (X) nerve and an external
branch (consisting of fibers from the “ spinal part” ). The
external branch of the spinal accessory nerve supplies the
sternocleidomastoid and trapezius muscles. After its division,
the spinal accessory nerve supplies the sternocleidomastoid
muscle and then descends obliquely in the posterior triangle
of the neck between the superficial and deep layers of the
deep cervical fascia (Figure 38.17). In this area the nerve is
embedded in loose connective tissue and is in contact with
the cervical lymph node chain. This is the most common
location for iatrogenic injuries to the spinal accessory nerve
during lymph node biopsies. The spinal accessory nerve
provides two or three branches to the upper part of the
trapezius muscle before passing under its anterior edge.
Tissue adhesive can be used to approximate multiple strands
of nerve graft and simplify the coaptation with proximal and
distal nerves (Figure 38.16). We generally reinforce the
nerve coaptation sites with the use of a bivalved nerve tube
and tissue adhesive.
Nerve Conduits
Nerve conduits are increasingly being used in nerve surgery
for small-caliber (more commonly sensory) nerves, for short
nerve gaps, or as an adjunct to nerve repair or transfer;
however, in proximal brachial plexus injuries, this technique
is not recommended at this time as a substitute for nerve
grafts.
Nerve TransferThe terms nerve transfer, neurotization, and nerve crossing
are used interchangeably and describe the transfer of a
normal or nearly normal fascicle or nerve branch to a more
important sensory or motor nerve that has sustained irrepa-
rable proximal damage. The term nerve transfer is used most
frequently in the current literature; nerve transfer and neu-
rotization will be used in this text without distinction. It
should be noted that muscular neurotization is different in
that it describes direct implantation of nerve ends into a
denervated muscle for reinnervation.
Indications
1. Irreparable preganglionic injury
2. Selected postganglionic injury
3. Reinnervation of FFMTs
Figure 38.16 Nerve repair with tissue adhesive. The graft strands
are first glued together (A), the graft ends are freshened with a
sharp blade (B) and then coapted with conventional epineurial
sutures (C). (Copyright Elizabeth Martin.)
A
B
C
Sural n. graft
Edgesfreshened
Fibrin glue
Figure 38.17 The course of the spinal accessory nerve. The nerve
can readily be identified in the lateral portion of a supraclavicular
incision on the anterior surface of the trapezius muscle several
centimeters above the clavicle. (By permission of Mayo Foundation
for Medical Education and Research. All rights reserved.)
Green’s Operative Hand Surgery
• Lack supportive
cells
• 3-D scaffold
PNAProcessed nerve allografts
22
23
24

9/29/2020
9
PNA in the literature
• No cases of tissue rejection
• S3 or M4 achieved in ~86% of procedures
• 89% digital nerves
• 75% median nerves
• 67% ulnar nerves
Moore A. Processed acellular nerve grafts.
2018
Processed nerve allografts
Nerve Transfers
Definition
• Surgical coaptation of a healthy nerve donor to a denervated nerve
• To regain a necessary function by sacrificing another function that is
less essential
Nerve transfers
Indications
• When the proximal nerve end is nonfunctional
• Nerve reconstruction would require an excessively long nerve graft or
exceed the expected viability of motor end plates and muscle
Contraindications
• Excessive time between injury and reinnervation (ie, >18 months)
• Donor nerve motor strength of less than MRC 4
• Superior reconstructive option
25
26
27

9/29/2020
10
Nomenclature
Lee SK, Wolfe SW. Nerve transfers. JAAOS 2012; 20: 506-517.
Reverse end-to-
side
End-to-sideEnd-to-end
Thank you!
28
29

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
3:45 PM - 3:55 PM
Nerve Case Presentation
Rafael J. Diaz-Garcia, MD ● Consulting Fees: Axogen, TelaBio and Smith + Nephew
9/29/2020
1
DISCLOSURES
Rafael J. Diaz-Garcia, MD
Consulting Fees: Axogen, TelaBio and Smith +
Nephew
Rafael J. Diaz-Garcia, MD, FACS
Hand and Upper Extremity SurgeryAllegheny Health Network
Clinical Assoc. Professor of Plastic SurgeryUniversity of Pittsburgh School of Medicine
1
2
3
9/29/2020
2
24yo RHD male with laceration of the right hand after assault. Exam notable for anesthesia of R thumb radial sensory nerve distribution. After exploration and debridement, 8mm nerve gap of RDN.
Treatment Options?
- Primary repair after mobilization- Repair with nerve conduit for gap- Repair with vein conduit for gap- Repair with allograft for gap- Repair with autograft for gap- Nerve transfer
Trade-offs- Primary repair after mobilization
cheap, easy, but possible tension- Repair with nerve conduit for gap
additional cost, but fast & tension free- Repair with vein conduit for gap
cheap, but additional time and donor site- Repair with allograft for gap
expensive, but fast and tension free- Repair with autograft for gap
additional time and donor site- Nerve transfer
additional time and donor site
4
5
6

9/29/2020
3
64yo RHD female with R open olecranon fracture and ulnar nerve laceration. Exam notable for anesthesia of R small and ½ ring finger, intrinsic paralysis. After exploration and debridement, 8cm nerve gap of ulnar nerve at elbow.
Treatment Options?
- Primary repair after mobilization- Repair with nerve conduit for gap- Repair with vein conduit for gap- Repair with allograft for gap- Repair with autograft for gap- Nerve transfer
7
8
9

9/29/2020
4
Trade-offs- Primary repair after mobilization
even with ulnar nerve transposition, too large a gap- Repair with nerve conduit for gap
no commercial conduits at length > 4cm, outside FDA indication- Repair with vein conduit for gap
cheap, but unlikely to bridge a gap this long- Repair with allograft for gap
expensive, but fast ; unclear data for long gap mixed nerves- Repair with autograft for gap
additional time and donor site, traditional gold standard- Nerve transfer
additional time and donor site, shorter distance
10
11
12

9/29/2020
5
13
14

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
3:55 PM - 4:05 PM
Distal Radius Fracture
Sameer Kumar Puri, MD No relevant conflicts of interest to disclose

9/21/2020
1
DISCLOSURES
Sameer K. Puri, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
Distal Radius Fractures
Sameer Puri, MDLoyola University Medical Center (until Oct 2020)/Indiana Hand to Shoulder Center (as of Nov 2020)
Outline
• Epidemiology/Incidence
• Pertinent Anatomy
• Imaging
• Fracture Characteristics
• Indications
• Surgical Options
1
2
3

9/21/2020
2
Epidemiology
• Very common– 3% of all upper extremity injuries
• ~640,000 annually in US (2001)
• Bimodal distribution– Early peak (5-24)
• Young, male, sports and high energy
– Late peak• Old, female, low energy and fragility fractures
Pertinent Anatomy
• 3 articular facets– Scaphoid
– Lunate
– Sigmoid notch
• Bony landmarks– Styloid
– Lister’s tubercle
– Volar lip
Pertinent Anatomy• Volar wrist ligaments
– Radioscaphocapitate• Role in position of
scaphoid
• Role in controlling midcarpal position
– Short radiolunate
• Keeps lunate in lunate fossa
4
5
6

9/21/2020
3
Pertinent Anatomy
• Dorsal wrist ligaments
– Dorsal radiotriquetral
• Lister’s to triquetrum
– Dorsal intercarpal
• Triquetrum to STT
From Green’s Operative Hand Surgery, 7th Ed.
Pertinent Anatomy
• TFCC– Forms the ulnar
articular surface– Attaches to
styloid• Deep limb of
radioulnarligaments
• Multiple parts– Articular disc– Meniscus
homologue– Radioulnar
ligaments– Volar ulnocarpal
ligaments– ECU subsheath
Imaging/Alignment
• Good X-rays
– PA
– Fossa lateral
– Oblique
7
8
9

9/21/2020
4
Imaging and Alignment – PA
• Looking down the DRUJ
✓ ✖
Imaging and Alignment - PA
• Wrist neutral– Pronation shortens the radius
Neutral Pronation
Imaging and Alignment - Lateral
• Rotation
– SPC
10
11
12

9/21/2020
5
Imaging and Alignment - Lateral• Fossa lateral
Imaging and Alignment - PA
• Radial height
• Radial Inclination
• Ulnar Variance
• Coronal alignment
Imaging and Alignment - PA
• Volar and dorsal rim
– Distal line usually dorsal rim
– Depends on volar tilt
13
14
15

9/21/2020
6
Imaging and Alignment - Lateral
• Volar tilt
Classification / Common Patterns
• Many flavors
– Young, high energy probably not same as old, fragility fracture
• Eponymous fractures may be just as useful to understand these…
Classification / Common Patterns• Colles Fracture
– Dorsal bending mechanism
– Apex volar angulation
– Dorsal comminution
– Shortening
– With or without
ulnar styloid
16
17
18

9/21/2020
7
Classification / Common Patterns
• Smith
– Palmar angulation
– Type 1 - Extra-articular
– Shortened
– DRUJ incongruity
Classification / Common Patterns
• Smith
– Type 2 Smith / Volar Barton’s
– Partial articular volar shear
– Carpus goes with the volar
piece
Classification / Common Patterns• Dorsal Barton’s
– Rare, ~ 2%
– Partial articular dorsal shear
– Radiocarpaldislocation• Short radiolunate
injury
• Lunate loses association with the radius
19
20
21

9/21/2020
8
Classification / Common Patterns
• Chauffeur Fracture
– Styloid fracture
– Often with associated SL
dissociation
– Probably part of perilunate injury spectrum
Classification / Common Patterns
• Die punch
– Intraarticularimpaction
– CT can be helpful
Who to treat?
• Articular surface– Intraarticular stepoff < 2mm– Maybe can accept more in older
patients
• Length– Ulnar variance– Ulnar-sided pain in some series
>40% non-op Colles– Associated with loss of grip and
pinch strength
22
23
24

9/21/2020
9
Who to treat?
• Carpal Malalignment
– Loss of volar tilt
– “Adaptive DISI”
– “Nondissociative Carpal Instability”
– Is the center of the capitate over the radius?
Who to treat?
• Carpal Malalignment
– McQueen et al JBJS 1996
– Single most predictive for loss of strength and functional outcomes
Who to treat?
• Coronal shift
– Related to radial height
– Distal IOL
– DRUJ
Trehan et al JHS 2015
25
26
27

9/21/2020
10
Who to treat?
• Associated carpal tunnel syndrome– Approximately 5%
• Occasionally with nondisplaced, especially if baseline symptoms
– First attempt reduction
• Associated ligament injuries– Some have ligament injuries by definition
• Radiocarpal dislocation
– Some have high suspicion• Chauffeur’s fracture
– Arthroscopic studies show as high as 30% SL, 15% LT injuries• Geissler JBJS 1996
Nonoperative Management
• Functional goals
• Previously discussed alignment criteria
• Fracture stability
Nonoperative Management
• Elderly patients may accept more deformity
– Metanalysis Chen et al JHS 2016
• 2 RCTs, 6 high quality retrospective studies
– Operative treatment
» Better radiographic outcomes
» Earlier return of grip strength
» Slightly higher complication
» No significant difference in endpoint ROM
» No significant difference in DASH or PRWE
» No significant difference in endpoint VAS
– Cast
» Potential delay in return to function and grip
» Lower complication rate overall, but maybe higher CRPS
28
29
30

9/21/2020
11
Nonoperative Management
• Functional goals are paramount
– Early return to function, even if endpoint the same, is not meaningless
– Neither is a complication
• Final outcome related to fingers
– Watch your splints!!
– Keep them short and thin in the
palm
Nonoperative Management
• Fracture stability
– Some fractures tend to fall back to injury films
– Risk factors for loss of reduction
Nonoperative Management• Fracture stability
– Lafontaine’s criteria
• Dorsal angulation > 20
degrees
• Dorsal comminution
• Intraarticular extension
• Associated ulnar fracture
• Age > 60
31
32
33

9/21/2020
12
Nonoperative Management
• Fracture stability
– Other factors have been shown
• Mackenney, McQueen et al JBJS 2006– Age
– Dorsal comminution
– Ulnar variance increase >3 mm
Nonoperative Management
• Fracture stability
– Other factors have been shown
• Lamartina, Tornetta et al JHS 2015– “volar hook”
•✔✔✔
✔ ✖
Operative Treatment
• Open
• Poor alignment
• Unstable– Shear
– Comminuted
– Impacted
– Fracture-dislocation• Associated ligament injury
– Metadiaphyseal extension
– Concomitant nerve injury
34
35
36

9/21/2020
13
Operative Treatment Options
• Fixed angle volar plate
• Fixed angle volar plate
• Fixed angle volar plate
• Fixed angle volar plate
• Fixed angle volar plate
Operative Treatment Options
• Closed reduction percutaneous pinning
• External fixation
• Augmented external fixation
• Dorsal bridge plating
• Open reduction internal fixation– Dorsal plate
– Nail
– Fragment specific fixation
– Volar locked plating
Fixed Angle Volar Plate
• Internal buttress for articular surface
• Previous plates placed dorsally had high rates of tendon complications
• Designed to tuck under volar rim
37
38
39

9/21/2020
14
Fixed Angle Volar Plate - Prominence
• Plate position is key– Soong grade (JBJS 2011)
• 0 – dorsal to critical line and proximal to volar rim
• 1 – volar to critical line• 2 – at or distal to volar
rim
– Kitay et al JHS 2013• At risk for tendon
ruptures– 2mm volar to critical line– Within 3 mm of volar rim
Fixed Angle Volar Plate – Volar Rim
• Volar rim fragment
– Attachments of volar ligaments
– Can escape over or around the plate
Fixed Angle Volar Plate – Volar Rim
40
41
42

9/21/2020
15
A Nascent Malunion
43
44
45

9/21/2020
16
Fixed Angle Volar Plate - Not Quite Enough
Dorsal Plates
• Improved designs
– Dorsal shear fractures
– Articular impaction
Dorsal Plates
• Improved designs
– Dorsal shear fractures
– Articular impaction
46
47
48

9/21/2020
17
Dorsal Bridge Plating
• Favorable reported outcomes– Elderly patients with highly
comminuted fractures
– High energy injuries with proximal extension
– Control of hand to radius connection (volar rim or short radiolunate ligament)
– Polytrauma with need for load-bearing through wrist
• Requires a second surgery
49
50
51

9/21/2020
18
52
53
54
9/21/2020
19
Summary
• Different fractures with different characteristics
• Identify the deformity
• Identify the stability
• Get the fingers moving
• Customize your fixation
– Not all volar plates!
55

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
4:05 PM - 4:15 PM
Wrist Case Presentation
Louis Christopher Grandizio, DO No relevant conflicts of interest to disclose
9/29/2020
1
DISCLOSURES
Louis Christopher Grandizio, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
WRIST CASEASSH 2020
L. Christopher Grandizio, DO
Hand and Upper-Extremity Surgery
Geisinger Commonwealth School of Medicine
Disclosures
None
| 3
1
2
3

9/29/2020
2
CASE
HPI: 15yo RHD healthy male was tackled during football and fell onto outstretched left hand.
Presented to ED.
EXAM: closed, NVI w/o evidence of acute CTS.
| 4
Diagnosis?
Great arc vs Lesser arc
4
5
6

9/29/2020
3
Initial Management?
Trans-styloid, trans-scaphoid, perilunate fracture dislocation
s/p closed reduction in ED with sedation
Definitive management?
7
8
9

9/29/2020
4
ScaphoidORIF
Radial styloid fixation, L-T stabilization, L-C stabilization
Returned to sports around 4 months
10
11
12

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
4:15 PM - 4:20 PM
Private Practice Career
Walter B. McClelland, Jr., MD ● Consulting Fees: MicroAire, Acumed

9/29/2020
1
DISCLOSURES
Walter B. McClelland, Jr., MD
Consulting Fees: MicroAire, Acumed
Career in Private Practice
Walter B. McClelland, Jr., MD
Peachtree Orthopedics; Atlanta, GA
2018 AAOS Census Data
1
2
3

9/29/2020
2
2018 AAOS Census Data
2018 AAOS Census Data
2018 AAOS Census Data
4
5
6

9/29/2020
3
Workforce Trends 2012-2018
• Relative decline in private practice, increase
in hospital employment
• Academic practice has remained relatively
stable
Comparing Practice Models
How to Evaluate a Private Practice
• Must have a well organized governance structure
• Our Practice: 35 physicians, 29 partners
• Full C-suite (CEO, COO, CFO), Physician President
• Executive Committee (C-suite, Clinical Mgr, President, 5 Elected MDs)
• Committees (Relevant Mgrs, Physicians)
• Quarterly business meetings, twice yearly retreats
7
8
9

9/29/2020
4
How To Decide
• Determine what is your most important variable:
• Location
• Financial Compensation
• Work/Life Balance
• Practice Autonomy
• Practice Scope
• Research Production
• Quality of Partners
No Such Thing As A Perfect Job
• Maximize what’s most important to
you
• Accept that there may be some
things you don’t love, but these will
be less impactful
• Everything is a trade-off, try to think
long-term
“You can’t always get what you want”
Thank You
Walter B. McClelland, Jr., MD
Hand, Shoulder & Elbow Surgery
Peachtree Orthopedics; Atlanta, GA
Cell: 404-550-3025
10
11
12

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
4:20 PM - 4:25 PM
Privademics Career
Kenneth R. Means, Jr., MD ● Contracted Research: Axogen

8/28/2020
1
DISCLOSURES
Kenneth R. Means, Jr., MD
Contracted Research: Axogen
38th Adrian E. Flatt Residents & Fellows Conference
Privademic Hand Surgery Practice
Kenneth R. Means, Jr., MD
The Curtis National Hand Center
MedStar Union Memorial Hospital
P a n
1
2
3

8/28/2020
2
= mt2h
Academic Privademic Private
More Less
Research OptionsGrant OpportunitiesTeaching/Academia
Protected TimePrestige
Breadth of Pathology
Research OptionsGrant OpportunitiesTeaching/Academia
Protected TimePrestige
Breadth of Pathology
Less More
EfficiencyFreedom
CompensationBusiness Opportunities
EfficiencyFreedom
CompensationBusiness Opportunities
Curtis National Hand Center Privademic Practice
•1 vs. 2 practices
4
5
6

8/28/2020
3
List Them!!
7
8
9

8/28/2020
4
10

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
4:25 PM - 4:30 PM
Academic Career
Julie B. Samora, MD, PhD ● Consulting Fees: (Spouse) Walter Samora with Globus Medical

9/29/2020
1
DISCLOSURES
Julie B. Samora, MD, PhD
Consulting Fees: (Spouse) Walter Samora
with Globus Medical
Julie Balch Samora, MD/PhD/MPH
Academic Medicine-
Is it for me?
Disclosures
Acknowledgement: Thank you to
Dawn LaPorte for sharing some of
these slides
Board or Committee member:
RJOS, AAOS, POSNA, ASSH, AOA
Spouse: Consultant for Globus Medical
1
2
3

9/29/2020
2
Background
• 70% change jobs after 5 years
– Beatty, AAOS Now 2014
• Medical Group Management Association (MGMA):
compensation in academic practices continues to trail
that of private practices
• Academic surgeons earn an average of 10% or $1.3
million less in gross income across their lifetime than
surgeons in private practice
https://www.mdedge.com/obgyn/article/96879/practice-
management/private-academic-surgeon-salary-gap-would-you-pick-academia/page/0/1
“CARTSQ”
• Clinical practice
• Administrative obligations
• Research
• Teaching/ education
• Service
• Quality Improvement
Research Options
• Bench/laboratory science research,
translational research, clinical
research, outcomes research,
epidemiological, multi-center studies,
trial involvement
4
5
6

9/29/2020
3
Pros• Surrounded by like-minded colleagues, intellectually
stimulating
• Intelligent trainees with curious minds
– med students, residents, fellows
• Staying up to date with research and surgical trends
– Journal clubs, GR, lectures
• Increased complexity of patients
– Ability to discuss odd/unusual case
• Opportunity to present at conferences regionally, nationally
and internationally
Pros
• Clinical, Research and Administrative support
• Call can potentially be less burdensome than in private
practice
• Surgeons may have a more ‘consistent’ salary that is not
completely dependent on being ‘maximally productive’ at all
times
– This allows you more time to explore other avenues including
education and research
Cons
• Less dedicated time for patient care
– potentially less revenue/ fewer RVUs
• Increased responsibilities (CARTSQ)
• Pressure to publish while still producing
clinically
7
8
9

9/29/2020
4
Cons
• These benefits aren’t consistent across every
academic institution
• Academic surgeons (generally speaking)
are employees, and don’t really have the opportunity
to be “their own boss”
– Academic clinicians may feel constrained by the fact that they often
cannot make all of their own decisions
– Scheduling, medical staff, what types of patients they see
Compensation
• Collections
• wRVU
• Hybrid
• Bonus structure (admin, research, QI,
service)
• Chair’s discretionary ‘bonus’
Academic Rank
• Instructor - <5 publications
• Assistant Professor
– Many start at this level (>5 publications)
• Associate Professor
– National reputation
– >15 publications (not case reports)
• Professor
– International reputation
– >15 publications (not case reports)
– Extramural funding
10
11
12

9/29/2020
5
Tracks
Research Clinical Care Education
CLINICIAN
Physician with clinical distinction for outstanding clinical skills
Clinical Program Builder – developed a broad-reaching clinical program
Physician-Innovator – developed a diagnostic tool, assay, or clinical procedure
Clinician /Educator- patient care and local educational leadership
EDUCATOREducational Scholars
Clinician/Educator
RESEARCHER
Physician-Basic Scientist
Physician-Clinical Investigator/Translational Researcher
Basic Scientist/Educator
Research Innovator – developed novel research assay
Promotional pathways Major Categories
Specific areas of career focus
P&T
• Extramural funding
• Invited talks (national, international)
• Editorial Boards
• National leadership roles/awards
– National committees
• Teaching awards
• National teaching courses
13
14
15

9/29/2020
6
P&T
• Journal peer reviewer
• Local/regional talks/teaching
• Videos/ chapters
• Citizenship/service
• Travelling fellowships
Professor
• H-index > 15 (Mean/Median– 25/23)
• Extramural funding – sustained record
• NIH Study Sections
• National Leadership
• Invited talks (national, international)
• National/international awards/selective fellowships
• Board examiner
• Book – author/editor
Conclusion
• Academic medicine does include administrative
obligations, research, teaching, service, and
quality improvement involvement -above and
beyond clinical duties
• Exposure to trainees/didactics, and complex case
mix
• Multiple pathways for P&T
• There is potentially less earning potential and less
control in academic medicine compared to private
practice
16
17
18

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
4:55 PM - 5:05 PM
Sports Injuries of Hand
Steven S. Shin, MD ● Royalty: Arthrex Hely & Weber
● Consulting Fees: Arthrex
● Speakers Bureau: Arthrex
1
Steven S. Shin, MD, MMScDirector, Orthopaedic Center
Associate Professor & Executive Vice ChairmanDepartment of Orthopaedic Surgery
Cedars-Sinai Health SystemLos Angeles, California
38th ASSH Residents/Fellows Conference: Sports Injuries of the Hand
DISCLOSURES: Steven Shin, MD
Royalties: Arthrex, Hely & WeberConsulting Fees: ArthrexSpeakers Bureau: ArthrexEditorial Boards: JBJS, Orthopedics TodayCommittees: ASSH, AAOS
Things to Think About
• Level of Play (high school, college, professional, weekend warrior)
• Timing • Which sport? Which position? Which hand?
Metacarpal and Phalanx Fractures
When do we operate?Rotational deformity
Articular step-offOpen fracture
Multiple fractures
EARLIER RETURN TO PLAY (?)
Return to Play
• My experience:– NBA: 3-5 weeks (after
ORIF)– NFL: 1-4 weeks (after
ORIF)– MLB: 4-8 weeks (with or
without ORIF)
1 2
3 4
5 6

2
Risk of Re-Injury (IMO)Without Plate and Screws• 3 weeks: 50%• 4 weeks: 25% • 5 weeks: 10%• 6 weeks: ”near” 0%
With Plate and Screws• 3 weeks: “near” 0%
19 yo RHD D-1 wide receiver
• 19 yo RHD D-1 wide receiver
• Injured right hand while throwing a block during game
Injury X-rays Surgery 2 days later (Monday)
• 2 and 3 days after surgery (Wednesday and Thursday)
5 days after surgery
• Padded metacarpal brace• 8 catches, inc 72-yard TD• 138 yards• One of his best games of
the season
7 8
9 10
11 12

3
RHD NHL player: Left MF P1 Fx
RTP 3.5 weeks
Pro Boxer, Left IF: P1 fx
Hook of Hamate FractureHistory• Felt sharp pain in left hand
(bottom hand) after a swing• X-rays: “negative”• CT: hook of hamate fx• Exam
– Tender at hook– Check ulnar nerve, RF/SF
flexor tendons, ulnar artery
Surgery
• 2012-2017• 41 baseball players
• Single surgeon• 12 professional, 17 collegiate, 12 high school• Median RTP: 5 weeks (range: 3-7 weeks)• HITS study: 51.5 days missed (7+ weeks)
Acute Thumb UCL Tears• Common sports injury, “skier’s thumb”• UCL: 90%; RCL: 10%• Usually distal• When to operate
– Complete tear WITH INSTABILITY (compared to opposite thumb)
– Avulsion fracture that is DISPLACED
• Earlier Return to Play/Activity?
13 14
15 16
17 18

4
Repair (suture anchor)• Post-op immob x 4 weeks,
then start ROM• RTP 8-12 weeks +/- splint
Repair + Internal Brace• Immediate ROM• RTP when comfortable,
usually 5-6 weeks
Thumb UCL Tear: Surgical Options CASE: UCL Tear, QB Throwing Hand
POD #2
IntraOp
Conclusion
• Different hand requirements in different sports
• Both NON-OPERATIVE and OPERATIVE treatments should be discussed (pros and cons of both)
• Sometimes OPERATIVE is preferred for RTP
• Player should always make the final decision
THANK YOU
19 20
21 22
23

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
5:05 PM - 5:20 PM
Pediatric Fractures
Lindley B. Wall, MD | Apurva S. Shah, MD, MBA
Lindley B. Wall, MD
No relevant conflicts of interest to disclose
Apurva S. Shah, MD, MBA
No relevant conflicts of interest to disclose

9/21/2020
1
DISCLOSURES
Apurva S. Shah, MD, MBA
Speaker has no relevant financial relationship
to disclose.
Pediatric Wrist & Forearm FracturesOperative vs. Nonoperative Management & Remodeling Potential
Apurva S. Shah, MD MBA
Assistant Professor of Orthopaedic Surgery
Director of Orthopaedic ResearchDirector of the Brachial Plexus Program
2020 ASSH Annual Meeting
Disclosures
I have no relevant financial disclosures
1
2
3

9/21/2020
2
Epidemiology
Distal radius & forearm fractures represent 24% fractures in children (most common long bone fracture)Christoffersen et al Arch Osteoporos 2016
Distal radius fractures incidence 5.7/1,000 children per yearHofer et al Gesundheitswesen 2019
Forearm fractures incidence of 0.7/1,000 children per yearLyman et al JPO B 2016
Clinical Presentation Distal Radius Fx
Fracture PatternsTorus
Bicortical metaphyseal
Physeal
Greenstick (rare)
Associated ulnar fracture rarely places role during initial treatmentStyloid
Physeal
Metaphyseal
Diaphyseal
Basic Principles of Distal Radius Fx Care
Closed reduction and castingShort arm or long arm cast acceptable
Bivalving does not increase risk of loss of reduction or surgeryBae et al JPO 2015
Goal cast index < 0.7Webb et al JBJS 2006
Poor casting often due to excess padding & lack of three-point mold
Management influenced by remodeling potential of the distal radius in growing children
4
5
6

9/21/2020
3
Remodeling Potential – Distal Radius Fxs
Distal radial physis provides 75% of radial growth
~5.25 mm longitudinal growth/year
Injury
Reduction
After 10 Days
After 6 Months
Overriding Distal Radius Fxs
Prospective evaluation of overriding distal radius fractures (Hawaii)Crawford et al JBJS 2012
51 consecutive children, average 5 mm shortening on presentation
No formal reduction, SAC x 6 weeks
Final sagittal angulation 2.2° and final coronal angulation 0.8°
All children achieved radiographic union with full wrist motion
Cost of closed reduction or surgery ~5-6x and ~9x higher, respectively
Overriding Distal Radius Fxs
Injury
After 6 Weeks
After 2 Years
7
8
9

9/21/2020
4
Operative Indications – Distal Radius Fxs
Open fracture
Floating elbow
Displaced intra-articular fractures (Salter-Harris type III or IV)
Irreducible fracture or loss of reductionNeeds careful monitoring over first 2 weeksFriberg Acta Orthop Scand 1979, Houshian et al JPO 2004, Zimmermann Arch Orthop Trauma Surg 2004
Children 5-10 YearsAngulation > 20-25°Translation > 50%
Children > 10 YearsAngulation > 10°
Translation > 25%
Children < 5 YearsAngulation > 30-35°Translation > 50%
Operative Intervention
Only 2.7% of distal radius fractures undergo surgery at tertiary care children’s hospitalsMahan et al POSNA 2016
Considerations in Physeal Injuries
4.4-7.0% risk of physeal arrest following distal radius physeal fracturesCannata et al JOT 2003, Lee et al CORR 1984
43% risk of physeal arrest following SHIII and IV fracturesKallini JPO 2020
Does late or repeat attempt at reduction increase risk of physeal arrest? ProbablyLee et al CORR 1984
6/22 pts with ≥ 2 reduction or late attempts developed physeal arrest
1/78 pts with ≤ 1 reduction attempt developed physeal arrest
10
11
12

9/21/2020
5
Distal Radius Fx – Case 1 12 yo M
Injury
After 10 Days
Distal Radius Fx – Case 2 6 yo F
Injury
Reduction
After 3 Weeks
Distal Radius Fx – Case 2 6 yo F
After 6 Months
After 6 Weeks
After 3 Weeks
13
14
15

9/21/2020
6
Clinical Personation in Forearm Fxs
Fracture PatternsPlastic deformation
Greenstick
Complete
Comminuted
Fracture LocationDistal 1/3
Middle 1/3
*Proximal 1/3
Basic Principles of Forearm Fracture Care
“True” orthogonal radiographs
Closed reduction and castingFactor the mechanism into the primary reduction strategy
Long arm cast
Poor casting often due to excess padding & lack of three-point mold
Management influenced by remodeling potential of radius & ulna
Since 80% of radial growth occurs at the wrist, remodeling in proximal and middle third considerably less than distal third
Operative Indications – Forearm Fxs
Open fracture
Floating elbow
Unstable Monteggia fracture-dislocations
Failure of closed reduction or loss of reduction (careful monitoring over first 2-3 weeks)
F 8-12 & M 8-14 YearsAngulation > 10-15°Translation > 50%
F > 12 & M > 14 YearsMinimal Angulation or
Translation
Children < 8 YearsAngulation > 20°
Bayonet apposition ok
16
17
18

9/21/2020
7
Operative Indications – Forearm Fxs
Rotation > 45°Bicipital tuberosity and radial styloid should be opposite on the AP radiograph
Coronoid process and ulnar styloid should be 180° with limited cut CT
Isolated middle third radius fractures with ulnar displacement that significantly narrows the interosseous space
Proximal third fractures
Impact of Malunion on Forearm Rotation
Degree of AngulationMatthews et al JBJS 1982
10° angulation of a single bone does not compromise forearm rotation
10° angulation of both forearm bones results in a 10-20° loss of supination and pronation
20° angulation of a single or both bones results in a 40° loss of supination and pronation
Fracture LocationTarr et al JBJS 1984
Angular deformity in distal third fractures result in greater pronation losses
Angular deformity in middle third fractures result in greater supination losses
Both Bone Forearm Fx – Case 1
19
20
21

9/21/2020
8
Both Bone Forearm Fx – Case 2
Take Home Points
1. Management influenced by remodeling potential of radius & ulna
2. Overriding fracture of the distal radius generally acceptable
3. Surgery may be indicated in distal radius fractures with > 20-25°angulation in children < 10 years
4. 10° angular deformity in forearm fractures only concerning when both bones angulated
5. Beware of malrotation and collapse of the interosseous space
22
23

9/21/2020
1
DISCLOSURES
Lindley B. Wall, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
Pediatric Hand Fractures:
Management and Remodeling
Lindley B. Wall, MD MSc
Washington University
Background
• Hand Injuries in Children
• 56% Nondisplaced
• 64% Nonphyseal
• Approx 75% are quite benign
• Key is to recognize problem injuries
• Phalangeal Neck
• Condylar Fractures
• Displaced Fractures
* Know what you can accept
1
2
3

9/21/2020
2
General Treatment
• Large soft tissue envelope
• Thick periosteum
• Healing is reliable in all cases*
• Physeal fractures rarely lead to growth arrest
• Angulation and displacement within the plane of
motion can remodel over time before skeletal
maturity
• Malrotation cannot
Examination
• Malrotation
• Flexion/Extension
• Deviation
• *If initial exam difficult, see back in
one week to reassess
Scaphoid Fracture
• Fall, higher energy
• Peak at 15 years old
• Very rare under 10 years old
• Physical Exam:
Snuffbox tenderness
Distal pole tenderness
Radial wrist pain with radial deviation
• (confirm with MRI)
4
5
6

9/21/2020
3
Scaphoid Fracture
• Usually nondisplaced
• Cast for 8-12 weeks
Scaphoid Fracture
• Displaced or proximal pole
• Open reduction, screw fixation
• Low threshold for CT to allow return to
activities
Metacarpal Fractures
• Thumb metacarpal base
• “Pediatric Bennett”
• Across growth plate and joint
• Needs anatomic reduction
• CRPP/ORPP/ORIF
7
8
9

9/21/2020
4
Metacarpal Fractures
• Thumb metacarpal base
• Extraarticular
• Excellent remodeling
• Multiple planes of motion
• Can be treated non-op…30o
• Significant displacement –
CRPP/ORPP
Metacarpal Shaft Fractures
• Check rotation
• Extensor lag due to shortening
• ORIF if unstable
• CRPP if transverse
• *Multiple metacarpals, do NOT
always need fixation
Metacarpal Neck Fractures
• Debate regarding acceptable
angulation
• Usually extraphyseal
• Check rotation*
• Assess digit extension
• Frequent recurrence
10
11
12

9/21/2020
5
Phalanx Fractures
• Phalangeal base
• SF “extra octave”
• Adduct to RF?
• Central digits
Cross-over, overlap
• Minimal/no angulation
• See back one week**
Phalanx Fractures
• Phalangeal base
• Cast/brace treatment
• Reduce under local anesthesia
If significantly angulated or malrotated
Buddy tape + cast
• CRPP
Unstable or unable to hold
Not amenable to local reduction
Phalanx Fractures
Thumb
• Skier’s thumb
• Collateral ligament avulsion
• Osteochondral injury
• Palmar and larger*
13
14
15

9/21/2020
6
Phalanx Fractures
• Reduction and
fixation
• CRPP/ORPP
• ORIF
• Need 2 points of
fixation
Phalanx Fractures
• Phalangeal shaft
• Check rotation!
• CRPP/ORIF if rotated, shortened
Phalangeal Neck Fractures
• Usually displaced
• Frequently malrotated
• Adjacent to joint
• Minimal Intrinsic Stability
16
17
18

9/21/2020
7
Phalangeal Neck Fractures
• Phalangeal neck
Remodeling?
Only occurs in the
plane of motion
Cannot be relied
upon
Phalangeal Neck Fractures
• Rotation and coronal plane angulation do
not remodel
Phalangeal Neck Fractures
• Pinning needed
• Closed reduction with osteoclasis
if necessary
• Must be done early (1-2 weeks)
• Avascular necrosis if reduction
done late or open
19
20
21

9/21/2020
8
Phalanx Condyle Fractures
• Intra-articular
• Unstable Injuries
• Fragment larger
• Not uniplanar
• Typically oblique fx line
Phalanx Condyle Fractures
• Need anatomic reduction
• Open dorsal approach
• Visualize in joint
• Clamp/pin
• Screw or K-wire fixation
• Need 2 to control rotation
Phalanx Condyle Fractures
• Malunion problematic
• Osteotomy for correction
• *Preserve vascularity
• Will NOT remodel
22
23
24

9/21/2020
9
Phalanx Fractures
• Beware of the Seymour fracture!
• Physeal fracture
• Open (Nail avulsed)
• Torn nailbed or periosteum
interposed
Phalanx Fractures
• Seymour fracture
• Needs operative treatment to
avoid osteomyelitis*, deformity,
growth arrest
Key Points
• Angulation and malrotation does NOT remodel
• Remodeling occurs in the plane of motion
• ? Age….do not rely in phalangeal necks
• Assess extension with metacarpal shortening
• Articular alignment matters in kids too
25
26
27

9/21/2020
10
Thank you
28

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
5:20 PM - 5:30 PM
Pediatric & Trauma Case Presentation
Mary Claire Manske, MD No relevant conflicts of interest to disclose

9/29/2020
1
DISCLOSURES
Mary Claire Manske, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
M. Claire Manske, MD
Shriners Hospital for Children Northern CaliforniaUniversity of California Davis, Orthopedic Surgery
Sacramento CA
• 23 month old female with a left thumb difference
• L thumb smaller than right
• Doesn’t use L thumb
1
2
3
9/29/2020
2
Left Right
4
5
6

9/29/2020
3
• Diagnosis?
• Clinical Exam?
• Work up?
• Treatment plan?
• Spectrum of deficiency of the radial side of the upper extremity
• 5-15% of congenital hand anomalies
• 50% bilaterally affected, usually asymmetric
• 5 key features
• small, short, narrow thumb
• underdeveloped thenar muscles
• narrow first web space
• joint instability (MCP, CMC)
• extrinsic muscle deficiency
James MA, JHS, 1999 24A; 6: 1145-1155
7
8
9

9/29/2020
4
• 5 key features
• small, short, narrow thumb
• underdeveloped thenar muscles
• narrow first web space
• joint instability (MCP, CMC)
• extrinsic muscle deficiency
Modified Blauth Classification
•Modified Blauth Classification
Type 2
•Modified Blauth Classification
Type 3A Type 3B
10
11
12

9/29/2020
5
•Modified Blauth ClassificationType 4
•Modified Blauth ClassificationType 5
Reconstruction
• Type 2 and 3A thumbs (stable CMC)
• Webspace deepening (Z-plasty)
• Opponensplasty
• MCP stabilization
Ablation and Pollicization
• Type 3B, 4, 5 thumbs (unstable CMC)
13
14
15

9/29/2020
6
• Assess thumb size, webspace, thenar eminence, finger creases (extrinsics), MCP stability
• Does child use thumb or bypass thumb for index finger (CMC status)
• Position of wrist, forearm
• Look at contralateral upper extremity (>60% bilateral, asymmetric)
• Full physical exam
• 67% with associated anomaly
• Severity of RLD predictive of associated anomaly
• Associated conditions
•Cardiac (20%)
•VACTERL (13%)
•Holt-Oram syndrome (4%)
•Fanconi anemia (1%)
•Scoliosis (23%)
•May take priority over upper extremity treatment Goldfarb CA, JHS 2006, 31A; 7: 1176-1182.
Wall LB, PRS 2013, 132; 1: 122-128.
•Complete physical exam
•CBC
•Echocardiogram
•Renal ultrasound
• Spine xrays
•Chromosomal challenge test
•Referral to genetics
• Associated conditions
•Cardiac (20%)
•VACTERL (13%)
•Holt-Oram syndrome (4%)
•Fanconi anemia (1%)
•Scoliosis (23%)
16
17
18
9/29/2020
7
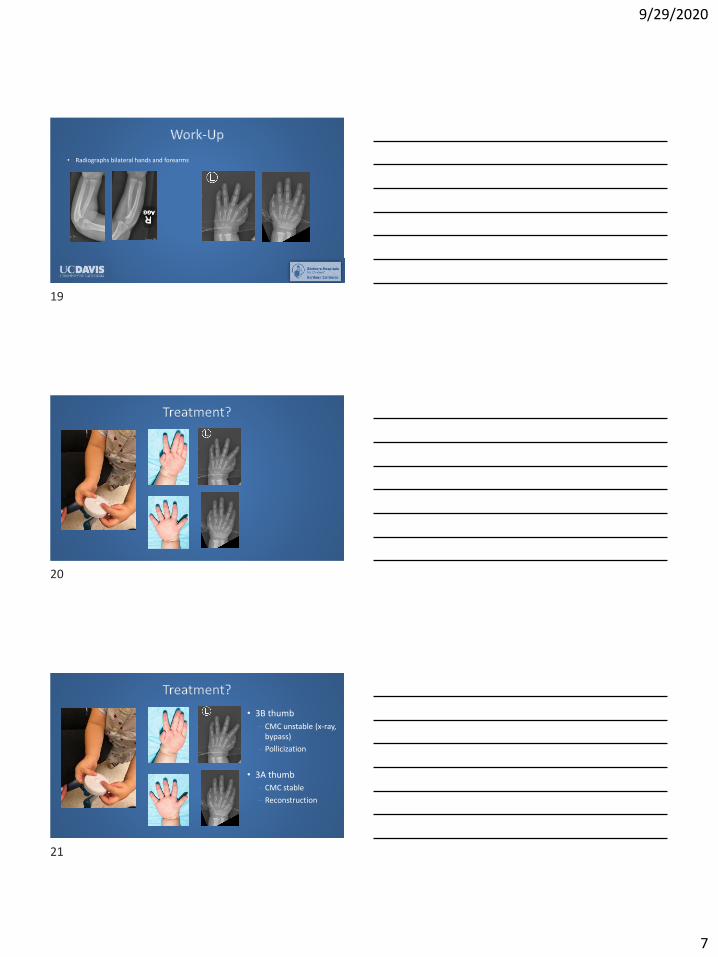
• Radiographs bilateral hands and forearms
• 3B thumb
– CMC unstable (x-ray, bypass)
– Pollicization
• 3A thumb
– CMC stable
– Reconstruction
19
20
21

9/29/2020
8
• Skin incisions
• Ablate hypoplastic thumb, allow rotation of index finger into thumb position
• Elevate 1st dorsal interosseous→ ABP
• Exposed index metacarpal shaft
• Excise metacarpal shaft to shorten index finger
22
23
24

9/29/2020
9
• Elevate 1st VIO→Adductor pollicis
• Release intermetacarpal ligament and RDA to long finger
• Secure metacarpal head in hyperextension
• Position index finger in thumb position
– 90-120° rotation & 40° palmar & radial abduction
• Attach intrinsic muscles
– 1stDIO→APB, 1st VIO→adductor pollicis
• Secure intrinsic muscles
• Close skin
25
26
27

9/29/2020
10
• Thumb hypoplasia is on the spectrum of RLD
– Bone, soft tissue, neurovascular structures
• Work-up for internal organ systems anomalies
• Modified Blauth classification/CMC stability is key to treatment
– 2, 3A thumbs: reconstruction
– 3B, 4, 5 thumbs: pollicization
28
29

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
6:26 PM - 6:46 PM
Physician Value
Daniel J. Nagle, MD No relevant conflicts of interest to disclose

9/2/2020
1
DISCLOSURES
Daniel J. Nagle, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
Physician Value
RVUs
1
2
3

9/2/2020
2
Pre World War II
No one cared Health Care CheapHealth Insurance
4
5
6

9/2/2020
3
InsurersHealth Insurance
Only sick people want insurance!!
7
8
9

9/2/2020
4
Adverse Selection!!
WWII
President Roosevelt
Inflation
10
11
12

9/2/2020
5
October 4, 1942
Stabilization Act
Health Insurance
13
14
15

9/2/2020
6
Young Healthy
Adverse Selection
16
17
18

9/2/2020
7
McCarran-Ferguson Act (1945)
Sen. Homer Ferguson (R-Mich)Sen. Pat McCarran (D-Nev)
Sherman Anti Trust Act
1940
10% 70%
1955
19
20
21

9/2/2020
8
Major Medical
• Hospitalization
Office visit $5
Cheap Drugs
22
23
24

9/2/2020
9
Low Tech
Pay the doctor
Insurance reimbursed the patient
25
26
27

9/2/2020
10
Usual and Customary
July 30, 1965
President Lyndon Baines Johnson
28
29
30

9/2/2020
11
Life expectancy 6615 % > 65 Yrs. uninsured <$500M
“…look like the worst kind of damn fool.”
LBJ 1965
31
32
33

9/2/2020
12
1970
$13,000,000,000
Costs
Advanced Technology
• CABG
• Transplantation
• CT (1972)
• MRI (1977)
34
35
36

9/2/2020
13
1986
•Life expectancy 75
•Medicare budget $106B
Too many peopleLiving too longUsing too much expensive technologyWith no skin the game
37
38
39

9/2/2020
14
Adverse Selection
40
41
42

9/2/2020
15
William Hsiao PhDWilliam Hsiao PhD
• Actuary Connecticut General Insurance
• Head Actuary of Medicare
• Professor of Economics Harvard
• Consultant to Carter, Nixon, Ted Kennedy on
National Health Insurance
RBRVS
ResourceBasedRelative ValueScale
43
44
45

9/2/2020
16
RELATIVE
VALUE
UNITRVU
Objective method to value
physician services
46
47
48

9/2/2020
17
Quantify the real cost
of physician services
quantify the relative cost
of physician services
Magnitude Estimation
49
50
51
9/2/2020
18
52
53
54

9/2/2020
19
Relative Value
•Physician Work
•Practice Expense
•Professional Liability Insurance
55
56
57

9/2/2020
20
PHYSICIAN WORK
Technical skill and physical effort
Mental effort and
judgmentTime
Stress due to
the potential
risk
Work
Practice Expense
Liability Insurance
Opportunity cost& debt
Education debt$200,000
58
59
60

9/2/2020
21
$800,000 $300,000
33 years old
Opportunity cost v a v plumber = $500,000
$700,000
61
62
63
9/2/2020
22
“Practice Expense” / Overhead
PRACTICE EXPENSE
19 Step Calculation
Imbedded Budget Neutrality Adjustment
Discount Direct Expense
40%!
DiscountIndirect Expense
61%!
64
65
66

9/2/2020
23
Should
Attorney RBRVS
67
68
69
9/2/2020
24
?
Relative Value?
Ludwig von Mises
70
71
72
9/2/2020
25
Economic Calculations in the Socialist Commonwealth 1920
There is no way to calculate the Relative Value of services and products outside of a free market.
There is no “intrinsic universal” valueof a service or product.
There is only the perceived valueas defined by the individual consumer.
The market is the most efficient at determining the “natural
price.”
1776
73
74
75

9/2/2020
26
“Results, Potential Effects and
Implementation Issues of the
Resource-Based Relative Value Scale”Wm Hsiao, Ph.D., Peter Braun, M.D.
JAMA, Oct. 28, 1988, Vol. 260, No. 16
• “Standardize Payments, Rationalize Incentives and Influence Physician Decisions.”
• “Provide a Neutral Incentive Structure”
• “Enhance Cost Effectiveness and Ameliorate Manpower Shortage in Primary Care.”
Translation
Physician Fees
76
77
78

9/2/2020
27
Proceduralists Primary Care
RBRVS
Calculate Intrinsic Value
79
80
81

9/2/2020
28
Intrinsic Value
Ignores the value perceived by the patient.
« Interchange » 1955 Willem de Kooning
$300,000,000
82
83
84

9/2/2020
29
Market based physician fees
R.I.P.
OBRA 1989
2019 CV $36.05/RVUPE
$193.08/HR
Code DescTotal time Total Fac $ Fac $/hr vs PPIS PE
Total Non Fac $ Non Fac $/hr vs PPIS PE
P&L / Hr P&L / Hr
25600Closed Rx
DR 108 $319.68 $177.60 -$15.48 $339.12 $188.40 -$4.68
25607 Orif Fx DR 275 $760.31 $165.89 -$27.19
25608 Orif Fx DR 305 $853.55 $167.91 -$25.17
25609 Orif Fx DR 358 $1,085.03 $181.85 -$11.23
64721 OCTR 171 $441.72 $154.99 -$38.09 $444.24 $155.87 -$37.21
25000 DeQ 135 $348.12 $154.72 -$38.36
26055 Trigger 154 $320.40 $124.83 -$68.25 $574.91 $223.99 $30.91
25447 CMC 278 $857.87 $185.15 -$7.93
26123 Dup 308 $863.63 $168.24 -$24.84
99203 OV New 29 $109.80 $227.17 $34.09
99213 OV Est 23 $74.16 $193.46 $0.38
And Then
85
86
87

9/2/2020
30
Value Based Payment
Fee for service is Evil
88
89
90

9/2/2020
31
Advanced AlternativePayment Models
ACA
MACRA
Reauthorization
Medicare
Access
CHIP (Children’s Health Insurance Program)
Act
April 16, 2015
91
92
93

9/2/2020
32
SGRQUALITY
PAYMENT PROGRAMQPP
PQRS EHR
VBM
MIPSMerit-Based Incentive Payment System
By implementing MACRA to promote participation in certain APMs, …., we support the nation’s progress toward achieving a patient-centered health care system …we are while finalizing a program that emphasizes high-quality care and patient outcomes minimizing burden on eligible clinicians and that is flexible, highly transparent, and improves over time with input from clinical practices.
94
95
96

9/2/2020
33
16 17 18 19 20 21 22 23 24 2526 & on
Fee
Schedul
e
97
+0.5% each year
No change
+0.25%or
0.75%
MIPS
AAPM
4 5 7 9 9 9Max Adjustment
(+/-)
+5% bonus(excluded from MIPS)
MIPSZero sum game
97
98
99

9/2/2020
34
16 17 18 19 20 21 22 23 24 2526 & on
Fee
Schedul
e
100
+0.5% each year
No change
+0.25%or
0.75%
MIPS
AAPM
4 5 7 9 9 9Max Adjustment
(+/-)
+5% bonus(excluded from MIPS)
OFFICE OF THE ACTUARY
DATE: April 9, 2015
FROM: Paul Spitalnic Chief Actuary CMS
SUBJECT: Estimated Financial
Effects of the Medicare Access and
CHIP Reauthorization Act of 2015
(H.R. 2)
Paul Spitalnic
MACRA Impact
“…. physician payment updates are not expected to keep
pace with the average rate of physician cost increases…we
expect access to Medicare-participating physicians to
become a significant issue in the long term…”
100
101
102

9/2/2020
35
Reauthorization
Medicare
Access
CHIP (Children’s Health Insurance Program)
Act
“MIPS cannot be saved.”
Medicare Payment Advisory Commission
MedPAC
• Burdensome and Complex
• Information is not meaningful
• Will not Improve value
• Will not reward value based care
103
104
105

9/2/2020
36
Almost closing thoughts
The Resource Based Relative Value Scale
Practice Expense
106
107
108

9/2/2020
37
Reauthorization
Medicare
Access
CHIP (Children’s Health Insurance Program)
Act
DOUBLETHINK
109
110
111

9/2/2020
38
Physician ValueLess
0.04 RVU / Minute$86.40 / Hour
Job hourly rate annual rate Barista $ 10.35 $ 21,528.00
Plumber $ 26.35 $ 54,808.00 Electrician $ 26.87 $ 55,889.60
Elementary school teacher (181 d/yr) $ 34.53 $ 50,000.00
Fireman $ 37.02 $ 77,000.00 Police officer $ 38.46 $ 80,000.00
Chef $ 58.70 $ 85,000.00 Pharmacist $ 65.00 $ 135,200.00
Lawyer (50hr / wk) $ 72.12 $ 150,000.00
Medicare MD payment $ 86.40 Golf (median) $ 302.88 $ 630,000.00 NFL (median) $ 413.46 $ 860,000.00
MLB (median) $ 721.15 $ 1,500,000.00
NHL (Ave) $ 1,153.85 $ 2,400,000.00
NBA $ 1,201.92 $ 2,500,000.00
CEO hospital largest $ 3,125.00 $ 6,500,000.00
CEO fortune 500 $ 4,807.69 $ 10,000,000.00 CEO Aetna Mark
Bertolini $28,221.15 $ 58,700,000.00
112
113
114

9/2/2020
39
Sen. Homer Ferguson (R-Mich)Sen. Pat McCarran (D-Nev)
Repeal
McCarran-Ferguson Act (1945)
115
116
117

9/2/2020
40
Executive Order 10-17 (Business Association Insurance - Rules Released 1-18)
• Small business groups to form
Intra and Inter-state health
insurance plans
Allow physician owned hospitalsEliminate Certificate of Need
Just a few more thoughts
118
119
120

9/2/2020
41
We are NOT the problem
Physician and Clinical Services 20%
(8% MC Budget)
Uncontrollable cost driversSenescence (63% healthcare expenditure last years of life)Obesity (10% of healthcare costs)
Life style
121
122
123

9/2/2020
42
We are the good guys
Honesty and Ethics
In Professions
2018
124
125
126
9/2/2020
43
#1#2
Thank you
127
128
129

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
6:46 PM - 6:56 PM
Hand/Finger Flaps
Michael J. Franco, MD No relevant conflicts of interest to disclose

9/21/2020
1
DISCLOSURES
Michael J. Franco, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
Finger and Hand Flaps
Michael J Franco MD
Cooper University Hospital, Camden NJ
Finger and Hand Flaps
• Overview
- V-Y flap
- Cross finger flap
- Thenar flap
- Homo-digital Island flap (anterograde and retrograde)
- First Dorsal Metacarpal Artery Flap (FDMA flap)
1
2
3

9/21/2020
2
Finger and Hand Flaps
• Indications
- Injuries of the finger or thumb not amenable to healing by primary
closure, secondary intention, skin graft or skin graft substitute
- exposure of critical structures (bone, tendon denuded of
paratenon, blood vessels, nerves
- a flap may be needed to expedite healing or allow for earlier range
of motion therapy
V-Y flap
• V-Y Flap is indicated for finger-tip amputations with exposed bone
• Amputation origin needs to be transverse of slight dorsal oblique
• The proximal part of the “V” is at the DIPJ flexion crease
• Dissection goes down to periosteum and flexor sheath. The blood supply is maintained through septi
• The flap is advanced several millimeters and can be anchored to the nail plate if intact
• The proximal part is closed in a line
Finger and Hand Flaps
• 21 yo M s/p avulsion crush injury to R ring finger with open distal phalanx fracture
• Exposed bone and flexor tendon• Wound size 2x2 cm
4
5
6

9/21/2020
3
Cross Finger Flap - markings
• This is a random pattern fasciocutaneous flap
• The blood supply is left intact on the side adjacent to the injured finger
• The flap is raised subfascial in a loose areolar plane, leaving the paratenon intact
Cross Finger Flap – flap inset
• The inset is done along 3 sides being careful to protect the ”hinge”
• The donor site gets a full thickness skin graft harvested from the forearm or groin area
• A bolster is applied to the skin graft and the flap is dressed withnon-stick gauze and a splint is applied
• I do not typically pin or suture the fingers together
• Plan for division at 2-3 weeks
Cross Finger Flap – 2 weeks post inset
7
8
9

9/21/2020
4
Cross Finger Flap – 1 week post division
Cross Finger Flap – 3 months post op
Cross Finger Flap – 3 months post op
10
11
12

9/21/2020
5
Cross Finger Flap – 3 months post op
Cross Finger Flap – 6 month post op
Finger and Hand Flaps
• 20 yo F, RHD, cashier• 2x2 cm defect L LF with
exposed distal phalanx
13
14
15

9/21/2020
6
Thenar Flap
• The flap can be designed proximally or distally based
• I chose the ”H” type design for maximum freedom
Thenar Flap
• The flap is elevated about the neurovascular bundles
• In this case, a portion of the flap was re-inset though both limbs were used
• A non-stick dressing is applied and bulky gauze with a dorsal blocking splint (though this is not critical.
• Again, I do not ”protect” the flap by placing any other sutures
• Plan to divide the flap at 2-3 weeks
Thenar Flap
16
17
18

9/21/2020
7
Thenar Flap – post division
Thenar Flap – 6 weeks post op
Thenar Flap – 6 weeks post op
19
20
21

9/21/2020
8
Thenar Flap – 6 weeks post op
- 25 yo M, manual laborer
- Crush avulsion injury R LF
- Exposed distal phalanx and tendon
- Nail matrix partially intact
Finger and Hand Flaps
Finger and Hand Flaps
22
23
24
9/21/2020
9
Homodigital Flap - midlateral design
• This is a neurovascular island flap• This should be a sensate flap to the
finger tip (as opposed to the thenar and cross finger flap)
• Approximately 2x2 cm flap is designed centered on the pedicle
• This could have a more volar skin paddle or be designed as a “reverse” flap based on retrograde flow. Though the nerve is not included in the reverse flap typically.
Homodigital Flap – midlateral design
Homodigital Flap - midlateral design
• A midlateral incision is made with a zig-zag component into the palm to allow for pedicle dissection and distal excursion of the flap
• Bipolar cautery and or micro clips are used for hemostasis as many small vessel branches or sacrificed
• This flap can be raised a more of an extended V-Y with less direct pedicle dissection
25
26
27

9/21/2020
10
Homodigital Flap - midlateral design
Homodigital Flap - midlateral design
Homodigital Flap - midlateral design
28
29
30

9/21/2020
11
Homodigital Flap
Homodigital Flap
Homodigital Flap – 3 months post op
31
32
33

9/21/2020
12
Finger and Hand Flaps
Photo from Aravind Pothula, MD
• 30 yo M, mechanic• Thumb avulsion/degloving• Treated with bilayer dermal
matrix and skin graft• Erosion of bone at distal
aspect
Finger and Hand Flaps
Photo from Aravind Pothula, MD
• The First dorsal metacarpal artery can often be dopplered out pre op (note: the radial artery is near by in the snuff box, so this signal can be confused)
• Approximately 3x2 flap is designed over the dorsal proximal phalanx with the PIPJ as the distal point.
• The ulnar proximal aspect of the skin paddle is curved to keep it out of the 2nd
web space• A curvilinear incision is designed over
the pedicle
FDMA Flap
• The flap is raised above the paratenon distally and can include the fascia above the dorsal interosseus muscle
• This skin flaps are raised maintaining the fat and soft tissue about a wide vascular leash
• The pedicle is not skeletonized• Dissection stops proximally
before the artery is encountered or until the reach is obtained
34
35
36

9/21/2020
13
FDMA Flap
FDMA Flap
• The flap can be placed through a wide tunnel
• The donor defect is skin grafted• A non stick guaze is applied and
a bulky dressing and splint
FDMA Flap
`
37
38
39

9/21/2020
14
FDMA Flap - complication
`
FDMA Flap
`
FDMA Flap
`
40
41
42

9/21/2020
15
FDMA Flap
`
FDMA Flap
`
Alternative Finger Flap
43
44
45

9/21/2020
16
Alternative Finger Flap
Alternative Finger Flap
Thank You
46
47

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
6:56 PM - 7:09 PM
Arthritis Case Presentation
Eric R. Wagner, MD ● Consulting Fee: Stryker, Wright Medical
● Contracted Research: Arthrex

9/21/2020
1
Wrist Arthritis Case Presentation
Eric R. Wagner, MD MSDivision of Upper Extremity Surgery
Department of Orthopaedic Surgery
Director of Upper Extremity Research
Emory University, Atlanta GA
773-203-5400
Product of My Mentors
1
2
3

9/21/2020
2
Case: 40 y/o M c Advanced Wrist OA
▪ HPI: Progressively worsening pain
▪ No prior wrist surgeries, 2 prior injections, 6 months PT/OT
▪ WSV 20%, VAS 8/10
• SH: home remodeler, enjoys golfing and lifting weights
• 20 pack year smoker, “quit 3 months ago”
• Exam: TTP at radioscaphoid articulation
• Pain with any motion
• +Watson Shift Test
Case: 40 y/o M c Advanced Wrist OA
Work-up
Treatment Options
Considerations
Wrist Arthritis
Etiologies
4
5
6

9/21/2020
3
Wrist Arthritis
Etiologies
Work-up
Treatment Options
Considerations
Wrist Arthritis: Etiologies
SLAC SNAC Inflammatory
Kienbocks Preissers
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
1972
What direction does lunate rotate after SLIL injury?
7
8
9

9/21/2020
4
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
1972
SL → DISI LT → VISI
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
What are the stages of SLAC Arthritis??
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
10
11
12

9/21/2020
5
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
ArthritisGiuffre et al. Hand Clin 31 (2015) 267–275
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
What are the stages of SNAC Arthritis??
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
ArthritisWhite et al. J Am Acad Orthop Surg 2015;23:691-703
13
14
15

9/21/2020
6
What is the likely Diagnosis???
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
1910
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritishttps://www.orthobullets.com/hand/6050/kienbocks-disease?expandLeftMenu=true
What are the risk factors for Kienbocks?
16
17
18

9/21/2020
7
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
➢Risk Factors
➢Ulnar negative, decreased radial inclination
➢Variable vascularity to lunate (Y, X, I)
➢Disruption of venous outflow → AVN???
https://www.orthobullets.com/hand/6050/kienbocks-disease?expandLeftMenu=true
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
What are the stages of Kienbocks?
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritishttps://www.orthobullets.com/hand/6050/kienbocks-disease?expandLeftMenu=true
Stage 1 Stage 2
Stage 3 Stage 4
19
20
21

9/21/2020
8
What is the Diagnosis???
SLAC
Etiologies
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritishttps://www.orthobullets.com/hand/6050/kienbocks-disease?expandLeftMenu=true
What about these???
22
23
24

9/21/2020
9
Etiologies
SLAC
SNAC
Kienbocks
Preissers
Rheumatoid
Arthritis
Ankylotic
Secondary OA
Erosive
Courtesy of Marco Rizzo
Zig Zag
➢Carpus: Supination, volar displacement + ulnar translocation, radial deviation
➢MCP: Ulnar deviation
What is classic deformity in Rheumatoid Wrist???
Etiologies
25
26
27

9/21/2020
10
Work-up
Treatment Options
Considerations
Wrist Arthritis
Etiologies
Work-up
Wrist Arthritis
Etiologies Treatment Options
Considerations
Wrist Arthritis: Evaluation
28
29
30

9/21/2020
11
Wrist Arthritis: Evaluation
Scapholunate Injury
White et al. J Am Acad Orthop Surg 2015;23:691-703
SL Angle >70oLunate Extension >10o
Wrist Arthritis: Evaluation
What advanced imaging is indicated for patients with wrist arthritis?
What examination findings???
Wrist Arthritis: Examination
Watson Shift Test
Gelberman et al. J Bone Joint Surg Am. 2000;82:578.
31
32
33

9/21/2020
12
Wrist Arthritis: Examination
Wrist Arthritis: First Step???
➢Activity Modification +/- Splints
➢NSAIDS
➢Injections: corticosteroids, “biologics”
Nonoperative
Work-up
Treatment Options
Considerations
Wrist Arthritis
Etiologies
34
35
36

9/21/2020
13
Work-up
Wrist Arthritis
Etiologies Treatment Options
Considerations
What are the Surgical Options???
Strauch J Hand Surg 2011;36A:729–735Total Wrist Fusion
PRC
PIN/AIN
4CF CL
TWA
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF
1998
37
38
39

9/21/2020
14
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWFPartial denervation of the wrist: a new approach, Berger, Tech Hand UE Surg, 1998
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWFPartial denervation of the wrist: a new approach, Berger, Tech Hand UE Surg, 1998
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF
1944
40
41
42

9/21/2020
15
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF
1985
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWFAmotz and Sammer, Hand Clin 31 (2015) 495–504
43
44
45

9/21/2020
16
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF
1966
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWFAmotz and Sammer, Hand Clin 31 (2015) 495–504
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF 1973
1977
46
47
48

9/21/2020
17
Wrist Arthritis: Treatments
1st Generation
Swanson
2nd Generation
Meuli Volz
Wrist Arthritis: Treatments
3rd Generation
Biaxial Universal
4th Generation
Remotion Maestro
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF
1942
49
50
51

9/21/2020
18
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF
PIN/AIN
Wrist Arthritis: Treatments
PRC
4CA
CL
TWA
TWF
Weiss et al. (J Hand Surg 2007;32A:725–746
Work-up
Treatment Options
Considerations
Wrist Arthritis
Etiologies
52
53
54
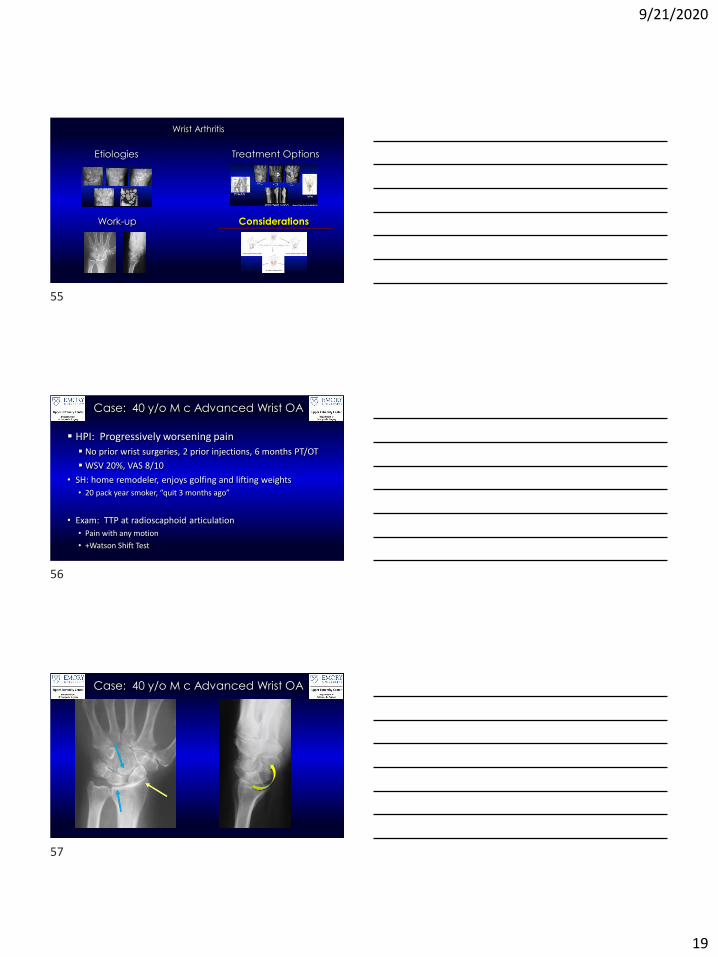
9/21/2020
19
Treatment Options
Work-up
Wrist Arthritis
Etiologies
Considerations
Case: 40 y/o M c Advanced Wrist OA
▪ HPI: Progressively worsening pain
▪ No prior wrist surgeries, 2 prior injections, 6 months PT/OT
▪ WSV 20%, VAS 8/10
• SH: home remodeler, enjoys golfing and lifting weights
• 20 pack year smoker, “quit 3 months ago”
• Exam: TTP at radioscaphoid articulation
• Pain with any motion
• +Watson Shift Test
Case: 40 y/o M c Advanced Wrist OA
55
56
57

9/21/2020
20
Case: 40 y/o M Laborer c Wrist OA
▪ Plan?➢Selective Neurectomy (AIN/PIN)
➢Proximal Row Carpectomy (PRC)
➢ Three or Four Corner Arthrodesis (3CF or
4CF) + Scaphoidectomy
➢Capitolunate Arthrodesis (CLA) +
Scaphoidectomy
➢ Total Wrist Arthroplasty (TWA)
➢ Total Wrist Fusion (TWF)
Case: 40 y/o M c Advanced Wrist OA
6 months postopWSV 75%VAS 2/10
Wrist Arthritis: Considerations
58
59
60

9/21/2020
21
Wrist Arthritis: Considerations
Wrist Arthritis: Considerations
Wrist Arthritis: Considerations
61
62
63

9/21/2020
22
Considerations
➢<45 years old
➢4CA (n=51): 11 years follow-up
➢PRC (n=38): 16 years follow-up
Considerations
Thank you for your time!
64
65
66

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
7:11 PM - 7:31 PM
Nightmare Cases: Lessons I Learned Early
in Practice
Curtis M. Henn, MD | Brandon S. Smetana, MD
Curtis M. Henn, MD
No relevant conflicts of interest to disclose
Brandon S. Smetana, MD
● Consulting Fees: Axogen
● Speakers Bureau: Axogen

Lessons I Learned Early in Practice Curtis M. Henn, MD
Brandon S. Smetana, MD
1. Lesson #1: You Don’t Know What You Don’t Know a. Pay attention to Details b. Debrief c. Take Notes
2. Lesson #2: Be Wary of the “Home Run” cases
a. Look for the snakes in the grass b. Make your life easier always, but especially earlier on c. Extra help (partners), imaging, larger exposures d. Diminish variables e. Keep it simple
3. Lesson #3: Do not be afraid to ask for help
a. Use your lifelines i. Mentors
ii. Residents iii. Co-fellows iv. Partners v. Communities (ASSH)
4. Lesson #4: The best made plan does not always pan out
a. Have bail outs available b. Mental or physical walk through preop

9/21/2020
1
DISCLOSURES
Curtis M. Henn, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
Nightmare Cases: Lessons Learned in
the First Years of PracticeCurtis M. Henn, MD
MedStar Georgetown University Hospital
Case 1: 2nd opinion
• 41M 3.5 months s/p distal humerus ORIF through olecranon osteotomy
• Referred by the therapist for a second opinion after she saw his X rays
1
2
3

9/21/2020
2
H&P
• Doing specialized pull up and fractured humerus
• 3 days later underwent ORIF
• Immobilized 2 weeks then initiated therapy
• Revision surgery discussed at most recent follow up
• Some mild pain, no improvement in ROM in about a month
• Wound healed, tender over olecranon
• 45-90 elbow ROM, NVI
What do you tell the patient?
Key Points
• You were not there
• Avoid throwing others under the bus
• Lay out options going forward
• Get more information
• Consider contacting the previous surgeon
(with patient’s permission)
4
5
6

9/21/2020
3
More Information:
More Information (cont)
Plan?
• More therapy?
• Revise the olecranon?
• Revise both?
• Revise with contracture release, excision HO?
7
8
9

9/21/2020
4
1 week s/p revision of humerus and olecranon, excision HO
6 weeks postop
• No pain
• NVI
• Wound healed
• 40-120 degrees of elbow motion
6 weeks postop
10
11
12

9/21/2020
5
Now what?
• BE HONEST
• Take your time
• Do not be afraid of second opinions
(within your group or community)
• Recruit your mentors, partners, colleagues
• Keep the patient close
(phone or frequent visits)
Plan:
• Discussed with partner and fellowship mentor
• Agreed with plan for revision with small plates, ICBG, no contracture
release
• Obtained labs – metabolic bone disease
• Send cultures
6 days s/p revision #2- ORIF with ICBG
13
14
15

9/21/2020
6
6 weeks s/p revision #2
• 45-80 ROM
• No pain
• Some clicking with ROM
• Start passive ROM?
Good News / Bad News
Now what?
• BE HONEST
• Keep the patient close
• Joint decision-making
• Enlist assistance – mentors/colleagues
16
17
18

9/21/2020
7
Intraop
• Removed the screw but the plate was still impinging
• Diamond-tip burr to remove proximal part of plate
• Unable to achieve last 30 degrees of extension despite removing
olecranon fossa HO
• Called partner who came to the OR and ultimately scrubbed in to help
achieve full ROM
Take Photos
19
20
21

9/21/2020
8
• Full normal elbow use
• Deadlifts 390 pounds
• ROM 30-125
Final Follow up
Take Homes
• Be humble when seeing second opinions – you were not there… and you
could always make the patient worse
• Be honest with yourself and with your patients
• Enlist the help of others – mentors (formal and informal), partners,
classmates, community colleagues
• Keep your complications close
Thank You
Curtis M. Henn, MD
22
23
24

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
7:31 PM - 7:41 PM
Ethics: COI
Felicity Fishman, MD No relevant conflicts of interest to disclose

9/21/2020
1
DISCLOSURES
Felicity Fishman, MD
Speaker has no relevant financial relationships
with commercial interest to disclose.
Conflicts of Interest
Residents & Fellows ConferenceASSH 2020
Felicity Fishman, MD
Associate Professor, Loyola University Medical Center
Shriners Hospital for Children- Chicago
COI Overview
• I have nothing to disclose
• No consulting arrangements with industry
• Academic practice → no shares in MRI,
OT, DME, surgery center
• No research funding with industry
1
2
3

9/21/2020
2
What is a Conflict of Interest?
• A set of conditions in which professional judgement
concerning a patient’s welfare or validity of research
can be influenced by financial gain:
• Examples: paid speaking engagements, gifts, travel, owning
of company shares (Dennis Thompson NEJM 1993)
• A conflict of interest may promote bias that distracts
from primary goal → patient care
What is a Conflict of Interest?
• COI have the potential to skew decision making that
might possibly impact patient care adversely
• COI can arise in professional setting when secondary
interest can distract from primary interest (financial
gain distracts from patient centered care)
Bias Stemming from COI
• Deliberate → surgeon intentionally chooses particular
device/implant due to a financial relationship with
manufacturer
• Unconscious influence → choose device due to a
favorable relationship with manufacturer
4
5
6

9/21/2020
3
Categories of Conflict of Interest• Industry Relationships:
• Medical devices/Implants, consulting
arrangements
• Research Funding
• Educational courses → teaching, resident
education
• Provider Self-Referral
• MRI, OT, DME, Surgical Centers, Specialty
Hospitals
Why do we have to disclose COI?
• Disclosing COI is an attempt at transparency
• Allows “learner” or patient to be informed as to
possible conflicts/biases and make their own
determinations
Official COI Statements
• Majority of professional medical societies
have adopted a formal statement
regarding COI
• Many healthcare corporations and
academic institutions have also created
formal statements
7
8
9

9/21/2020
4
ASSH
• The Hand Care Professional shall regard responsibility to the patient as
paramount.
• The practice of medicine inherently presents potential conflicts of interest.
Hand Care Professionals must be aware of the potential negative
implications of professional-industry relationships, and other areas of
potential conflict, and not allow conflicts to compromise patient care.
• Whenever an actual or potential conflict of interest arises, it must be
disclosed and resolved in the best interest of the patient
AAOS: Physician-Industry Relations
• Generally acceptable for industry to provide financial
and other support to physicians if support has
substantial educational value and contributes to
improving patient care
• Anything received that could be perceived as
influencing the physician’s obligation to act in the best
interest of the patient is considered a conflict of
interest
AAOS: Physician-Industry Relations
• It is unacceptable for physicians to receive subsidies
from industry to defray the cost of attending a meeting
or for third party CME courses
• Industry can support CME meetings by offering grants,
hosting hospitality receptions and providing support for
residents in training
10
11
12
9/21/2020
5
AAOS SOP Regarding COI
• If anything of significant value is received from industry → a potential
conflict exists which should be disclosed
• Must disclose financial interest in procedure/device/implant if the surgeon
is connected with or has received anything of value from inventor
• Must disclose if surgeon is reporting on research involving device/procedure/implant
• Reimbursement of administrative costs in conducting or participating in
scientifically sound research clinical trial is acceptable
ASPS
• Each leadership year, all Officers, Directors, Trustees, Judicial
Council members, ASPS / PSF / PSPS Committee,
Subcommittee, Work Group and Task Force leaders and
members, and the Editorial Boards of PRS and PRS-Global
Open (“Volunteer Leaders”) must submit an online COI form
• Cannot use affiliation with ASPS to promote anything that may
fall within a COI
• COI statement also provides a framework to resolve conflicts
The Physician –Industry Relationship is Complex…
13
14
15

9/21/2020
6
OIG of the Dept of Health & Human Services
• Reimbursement for valid research expenses is appropriate
• Appropriate to have salary support for research staff and
equipment needs
• Must disclose support from industry and financial relationships
• Must avoid bias favorable to company funding research
Physician Self-Referral
• 5 major fraud and abuse laws
that apply to physicians
• False Claims Act
• Anti Kickback Statue
• Physician Self Referral Law
(Stark law)
• Exclusion Authorities
• Civil Monetary Penalties Law
Physician Self-Referral
• Many realms in which the physician can “self-refer”
• As the practice of medicine became less lucrative,
physicians sought alternative ways in which to improve
income
• MRI, OT, DME, Surgical centers, specialty hospitals
16
17
18

9/21/2020
7
Physician Self-Referral
• # of ASCs ↑ 35% between 2000-2004 with 83% of
existing centers partly or wholly owned by physicians
• Ownership of a facility in which you refer a patient is a
COI
• Secondary interest (income from increased service) has
potential to bias physician's primary interests in patients
welfare
Physician Self-Referral• Stark Laws – federal law prohibits physicians from referring
Medicare or Medicaid beneficiaries for “designated health
services” if the physician or their immediate family have
ownership or investment interests in the entities or comp
arrangements
• Need to disclose ownership in specialty hospitals
• “In-office” or “within practice” exceptions
How do you disclose COI?
• Industry Relationships:
• Most organizations, health care corporations and academic
medical centers have a policy on COI
• Many require annual updating of COI statement/agreement online
• Journals require COI with each submission of a manuscript
• COI slide typically required for all presentations at meetings
19
20
21

9/21/2020
8
How do you disclose COI?
• Financial Interests/Self Referral-
• Infrequently disclosed directly between surgeon and patient
• Typically a handout either within surgical packet or
initial paperwork when first entering the practice
Sunshine Act (2010)• “Open Payments Program”
• Intention was to ↑ transparency in the financial relationships
between the pharmaceutical and medical device industry and
certain types of health care providers
• Manufacturers of devices, medical supplies, biologics and
group purchasing organizations have to annually submit info
about payments and transfers of value made to “covered
recipients” in the preceding calendar year
“Open Payments Program”
• Originally, only physicians and teaching hospitals were
included
• “Covered recipients” expanded in 2019
• includes PAs, NPs, Clinical Nurse specialists, CRNAs, Certified
nurse midwives
• After 2013, all Payments to physicians and institutions
of > $10 must be reported and info must be retrievable
on searchable databases
22
23
24

9/21/2020
9
CMS Open Payments Data (2014)
• https://openpaymentsdata.cms.gov/
Is Simple Disclosure Enough?
• Are COI declarations at CME events largely perfunctory?
• By simply making a declaration, has the speaker provided adequate proof of
COI?
• 71% of surgeons, 39% of learners, 35 % of internist felt COI slide was adequate
• 68% felt that amount of money should be declared
• Halo effect →declaration of possible conflict makes presenter more
believable (roughly 50% of all groups)
25
26
27

9/21/2020
10
How do Patients view Conflicts of
Interest?
• Patients given a form with financial disclosures when
they arrive for informed consent appointment (preop)
• Patients were concerned if physician was paid by a
company that made a product for the surgery
• 50% of patients said they would still have surgery with
a surgeon who developed the prosthesis
• Only 47% were aware of FCOI and only 55% wanted to
learn of the FCOI
• Patients have a poor understanding of FCOI
28
29
30

9/21/2020
11
Summary• Consider your own relationships with industry carefully
• Evaluate your own potential for bias due to interactions with industry
• Always disclose any financial or other relationships with
industry in appropriate fashion (hospital, journal, meetings)
• Disclose physician involvement in ancillary services when
recommending to patient
• Honesty and transparency is the best policy
Thank you!
• Any questions?
31
32

75TH ANNUAL MEETING OF THE ASSH OCTOBER 1 - 3, 2020
38th Adrian E. Flatt Residents & Fellows Conference
7:41 PM - 7:55 PM
Ethics: Burnout
Scott D. Lifchez, MD, FACS ● Ownership Interests: Co-founder and equity holder of EduMD, LLC, an educational
assessment company that makes the Operative Entrustability Assessment surgical assessment
tool.

9/21/2020
1
DISCLOSURES
Scott D. Lifchez, MD, FACS
Ownership Interests: Co-founder and equity
holder of EduMD, LLC, an educational
assessment company that makes the
Operative Entrustability Assessment surgical
assessment tool.
Burnout: Maintaining the Joy
of Hand Surgery PracticeScott D Lifchez, MD, FACS
38th Annual Adrian Flatt Resident & Fellows’ Conference
September 30, 2020
Disclosures
• Scientific advisory board of EduMD, LLC
– MileMarker, OEA surgical assessment tools
3
1
2
3

9/21/2020
2
Burnout Is
• Emotional exhaustion,
depersonalization
• Decreased sense of personal
accomplishment due to work-
related stress
• Consequences:
– Fatigue
– Inefficiency
– Errors
– Suicide
Burnout Among Physicians
• 2014 Shanafelt (6880
physicians):
– 54.4% met criteria for burnout
(10% from 2011)
– Much higher than general
population
• 2009 ACS (7905 surgeons)
– >40% met criteria
• 2000 Physician Work Life Study
– Burnout symptoms 60% more
frequent among women physicians http://www.newdiaspora.com/dr-burnout/
Burnout Among Hand Surgeons
• No data specific to hand surgeons
• Plastic Surgeons
– ASPS members (Faculty): about 30%
– Residents up to 33%
• Orthopedics (Sargent 2011- 384 residents, 264 faculty):
– Faculty: 15% depersonalization, 28% emotional exhaustion
– Residents: 55% depersonalization, 32% emotional exhaustion
• Worse for residents in larger programs
4
5
6

9/21/2020
3
Maslach Burnout Inventory
• Burnout (section A)
– <17: Low-level
burnout
– 18-29: Moderate
burnout
– >30: High-level
burnout
Maslach Burnout Inventory
• Depersonalization
– <5: Low-level burnout
– 6-11: Moderate
burnout
– >12: High-level
burnout
Maslach Burnout Inventory
• Personal Achievement
– <33: High-level burnout
– 34-39: Moderate burnout
– >40: Low-level burnout
7
8
9

9/21/2020
4
Reminders of How Hard We
are Working are Everywhere
June 8, 2019
What Can We Do
About It?
The Rest of the Story
• What I won’t cover (but is still important)
– Systems issues
– Practice/Health system
• Contracts
• Billing/Reimbursement
• EMR
– Pressures outside of work
– Double binds/Moral Injury
10
11
12
9/21/2020
5
Self-Care is Part of Our Job
• Resources available in health system/hospital
– Readily available
• Including after hours if needed
– Often free
• Avoid stigmatizing
• Modeling self-care promotes other team
members doing this as well• Johns Hopkins: mySupport
Aspects of Wellness
• Nutrition
– Healthful food options, scheduled time to eat
• Fitness
• Emotional health
• Mindset and behavior adaptability
• Preventive care
– Dental care, provisions to see a primary care physician
• Financial health
– Debt management, retirement planning emergency fund support
Mindfulness-Based Stress
Reduction• Focus on being present in current
moment
• Practice at home and in work environment– Mental exercises
• Meditation
• Gratitude journal
– Physical exercises• Yoga
• Sports
https://www.magzter.com/articles/6166/151600/56c4e157dae11
13
14
15
9/21/2020
6
Mindfulness-Based Stress
Reduction• Focus on being present in current moment
• Practice at home and in work
environment
– Mental exercises
• Meditation
• Gratitude journal
– Physical exercises
• Yoga
• Sports
– Prospective studies show this actually workshttps://www.mindful.org/10-
ways-to-define-mindfulness/
Promoting Resilience
• Resilience:
– Ability to “bounce back” from negative event
– Grow from situation
• Need to recognize self when stressed
– Fatigue, irritability, feeling outside “comfort zone”
• Use resources
– Peer support
– Mindfulness
16
17
18

9/21/2020
7
Takeaways
• Control the things you can control
– Mental state, mindfulness
– Nutrition & overall wellness
– Approach to how you interact with colleagues/others around
you
• Be aware of system issues
– Participate to improve these if you have opportunity
Acknowledgements
• ASSH Burnout Task Force (2019)
– Sanj Kakar (MBBS) chair
• Erin Gillard, LCSW
– Hopkins mySupport
Resources Available
• American College of Surgeons
– https://www.facs.org/member-services/surgeon-wellbeing/ps328
• American Medical Association
– https://edhub.ama-assn.org/steps-forward/pages/professional-well-being
• American Orthopedic Association
– https://journals.lww.com/jaaos/Fulltext/2016/04000/Orthopaedic_Surgeon_B
urnout___Diagnosis,.1.aspx
• American Society of Plastic Surgeons
– https://journals.lww.com/plasreconsurg/Fulltext/2019/08000/A_Growing_Epi
demic__Plastic_Surgeons_and_Burnout_A.46.aspx
19
20
21

9/21/2020
8
Additional Reading:
• Ames SE, Cowan JB, Kenter K, Emery S, Halsey D. Burnout in Orthopaedic Surgeons: A Challenge for Leaders, Learners,
and Colleagues: AOA Critical Issues. J Bone Joint Surg Am. 2017 Jul 19;99(14):e78.
• Campbell DA Jr, Sonnad SS, Eckhauser FE, et al. Burnout among American surgeons. Surgery 2001;130:696e-702.
• Chaput B, Bertheuil N, Jacques J, et al. Professional burnout among plastic surgery residents: Can it be prevented?
Outcomes of a national survey. Ann Plast Surg. 2015;75:2–8.
• de Vibe M, Solhaug I, Tyssen R, Friborg O, Rosenvinge JH, Sørlie T, Bjørndal A. Mindfulness training for stress
management: a randomised controlled study of medical and psychology students. BMC Med Educ. 2013; 13: 107.
• Dimou FM, Eckelbarger D, Riall TS. Surgeon Burnout: A Systematic Review. J Am Coll Surg. 2016 Jun;222(6):1230-1239.
• Epstein RM, Krasner MS. Physician resilience: what it means, why it matters, and how to promote it. Acad Med. 2013
Mar;88(3):301-3.
• Khansa I, Janis JE. A Growing Epidemic: Plastic Surgeons and Burnout-A Literature Review. Plast Reconstr Surg. 2019
Aug;144(2):298e-305e.
• Maslach C, Jackson SE, Leiter MP (Eds.), Maslach Burnout Inventory manual (3rd ed.), Consulting Psychologists Press
(1996).– http://www.uapd.com/wp-content/uploads/Maslach-Burnout-Inventory-MBI.pdf
• Sargent MC, Sotile W, Sotile MO, et al. Managing stress in the orthopaedic family: avoiding burnout, achieving resilience.
J Bone Joint Surg Am 2011;93:e40.
• Streu R, Hansen J, Abrahamse P, Alderman AK. Professional burnout among US plastic surgeons: Results of a national
survey. Ann Plast Surg. 2014;72:346–350.
THANK YOU
22
23