340b integrity audit: is your hospital ready for a … · 340b overview the 340b drug discount...
TRANSCRIPT

340B Integrity Audit: Is Your Hospital Ready for a HRSA Audit?
February 4, 2013
1

Agenda
340B Program Overview Why HRSA Audits? What will HRSA Audits Cover?
Verification of Eligibility: Covered Entity, GPO Exclusion Prevent Diversion: Outpatient Definition Prevent Duplicate Discount: Medicaid Exclusion Contract Pharmacy Compliance Sample Drug Encounters
How to Prepare for HRSA Audit Questions/Answers
2

340B Overview
The 340B drug discount program is a section of the Veterans Health Care Act of 1992, which requires pharmaceutical manufacturers whose drugs are covered by Medicaid to provide discounts on outpatient covered drugs purchased by 340B covered entities
Covered entities can receive discounts based on the utilization of pharmaceuticals by covered outpatients. Retrospective procurement is used to realize the discounts based on this utilization
The program is administered by the Office of Pharmacy Affairs (OPA). The OPA and drug manufacturers have the right to conduct compliance audits of participating facilities. A clear audit trail must be created to remain in compliance with the regulations of the program
The purpose of the 340B program is to enable covered entities to stretch scarce federal resources, reaching more eligible patients and providing more comprehensive services
Estimated savings are 25%-50% of a drug’s average wholesale price (AWP) Approximately $6 billion in 340B purchases in 2010
3

Hospital Covered Entities
DSH Hospitals - acute care hospitals with a DSH Adjustment Factor greater than 11.75%
Children’s Hospitals - pediatric hospitals with a 3300-series Medicare provider number that can perform a DSH calculation on worksheet S-3 and show a factor greater than 11.75%
Sole Community Hospitals - hospitals with sole community designation with a DSH Adjustment Factor greater than 8.0% on most recently filed Medicare Cost Report
Rural Referral Centers - hospitals with Rural Referral Center designation with a DSH Adjustment Factor greater than 8.0% on the most recently filed Medicare Cost Report
Critical Access Hospitals - all Critical Access Hospitals, regardless of DSH factor
Free Standing Cancer Hospitals - free standing cancer centers with a DSH Adjustment Factor greater than 11.75 on most recently filed Medicare Cost Report or be eligible under separate indigent care calculation
4
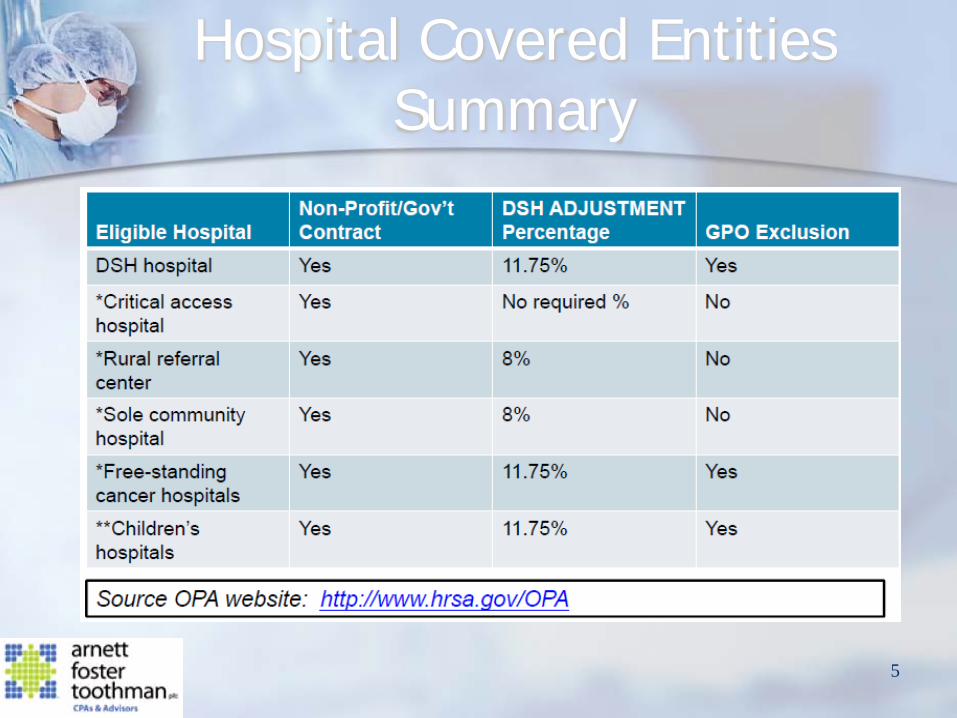
Hospital Covered Entities Summary
5

Other Covered Entities
Federally Qualified Health Centers Federally Qualified Health Center Look-Alikes Black Lung Clinics Ryan White HIV/AIDS Program Grantees Native Hawaiian Health Centers Tribal/Urban Indian Health Centers Comprehensive Hemophilia Diagnostic Treatment Centers Title X Family Planning Clinics Sexually Transmitted Disease Clinics Tuberculosis Clinics
6

Polling Question #1
1. How long have you participated in the 340B Program?
a. Less than 1 year b. Between 1-3 years c. Over 3 years d. N/A
7

Covered Drugs
Program covers only covered entity’s outpatient drugs: FDA-approved prescription drug Prescribed OTC drug Biological drugs that can be dispensed only by
prescription FDA-approved insulin Excludes vaccines Orphan drug exclusion and proposed regulations
Permitting orphan drug purchases on 340B for patients treated for a non-orphan disease (i.e. Remicaide for use with rheumatoid arthritis)
Prohibiting orphan drug purchases on 340B for patients treated for the orphan disease (i.e. Remicaide for Chrohn’s disease)
8

WHY HRSA AUDITS?
9

Covered Entity Growth
10

Increased Scrutiny Continued
11
Letter to HRSA on July 18, 2012
Letter to SNHPA on March 5, 2012

Increased Scrutiny Continued
Letter to UAB on May 10, 2012
Letter to UNC Hospital on September 28, 2012
12

HRSA 340B Integrity Audits
Nearly 20 years after creation of 340B, HRSA exercising authority to audit covered entities. On February 10, 2012, 340B participants received notice from HRSA that audits would occur
HRSA had been under pressure from Congress and federal oversight groups to prove that only those parties eligible for the program’s benefits receive them
According to HRSA, they will make its audit results public after the agency ensures its methods are consistent and audited entities have an opportunity to respond to the findings
Focused compliance problems: Diversion – Refers to a covered entity providing drugs bought through the 340B
program to people not eligible for the program’s prices. Duplicate Discounts – These occur when a state obtains Medicaid rebates for a
drug that a covered entity bought through the 340B program. Group Purchasing Organization (GPO) prohibition
13

340B Integrity Audit Purpose
The findings that are derived from these audits will assist HRSA and all 340B stakeholders to provide additional insights into the status of 340B operations and to assess overall compliance with the 340B operations and to assess overall compliance with the 340B program
These audits will help HRSA and participating covered entities identify and mitigate program risk as well as identify best practices regarding 340B program compliance
14
Source: HRSA 340B Program Audits/Clarification of HRSA Audits of 340B Covered Entities

WHAT WILL HRSA AUDIT COVER?
15

340B Audits
According to Safety Net Hospitals for Pharmaceutical Access, HRSA has already completed 51 audits, most involving hospitals
HRSA has planned as many as 400 for 2013 2012 audits included covered entities that included hospitals
and retail pharmacies The audits will include pharmacy contracts between 340B
covered entity and any outside pharmacy 2013 and forward:
Easily retrievable data All covered entities audited in the future Regulations will be tightened, not sure when
16

Audit Process
According to HRSA, the first question asked is, “Do you have policies and procedures in place to define who is and who is not a patient?”
Required standard information in pharmacy data file, such as: Prescriber Patient NDC number Fill date Billing amount Acquisition cost Encounter dates
17

HRSA Audit Example Timeline
2/4/13 - Email from HRSA Director informing Pharmacist in Charge of the audit
2/8/13 - Email from auditor to make arrangements for on-site visit on 2/28-3/1/13 2/9/13 - Email with data requests forwarded to Director of
Pharmacy and Pharmacist in Charge 2/11/13 - Received site visit agenda from auditor 2/15/13 - Conference call with both auditors to review
data requests (request electronic files by 2/18/13) 2/28-3/1/13 - HRSA On site visit 3/15/13 - Exit conference call
18

Pre-Audit
Covered entities selected for audit receive an engagement letter explaining what to expect and how to appropriately prepare
HRSA regional auditors conduct an introductory teleconference with the entity to request and obtain specified documents, including policies, procedures, and internal controls
HRSA regional auditors work with the entity to schedule an entrance conference with key entity management to discuss expectations for the onsite audit
19 Source: HRSA 340B Program Audits/Clarification of HRSA Audits of 340B Covered Entities

Onsite Audit
HRSA regional auditors obtain and review select program data and internal controls. Audit procedures include, at a minimum: review of relevant
policies and procedures and how they operationalize; Verification of eligibility, including GPO and outpatient clinic
eligibility; Verification of internal controls to prevent diversion and
duplicate discounts, including appropriateness of inpatient/outpatient designations and Medicaid exclusion file designations;
Review of contract pharmacy compliance; and Test 340B drug transaction records on a sample basis.
HRSA regional auditors conduct an exit interview, sharing areas of concern and preliminary findings
20 Source: HRSA 340B Program Audits/Clarification of HRSA Audits of 340B Covered Entities

Post Audit
HRSA regional auditors forward preliminary findings to OPA for review
OPA reviews the preliminary findings and works directly with the covered entity to obtain any necessary additional information, address any concerns and discuss the appropriate remedy and required corrective action(s), including potential removal from the 340B Program and/or repayment to manufacturers
Once an audit report is finalized by OPA, the findings and the entity’s response will be summarized on the OPA public website at www.hrsa.gov/opa
OPA will pursue further follow up with the entity as needed
21 Source: HRSA 340B Program Audits/Clarification of HRSA Audits of 340B Covered Entities

Polling Question #2
1. Do you review your 340B policies at least annually?
a. Yes b. No c. Not sure d. N/A
22

Findings/Penalties
As of right now, no penalties, take-backs or findings have been posted by HRSA
According to March 5, 2012 program release, findings may be referred to the Office of Inspector General or the U.S. Department of Justice
It is still unknown as to when findings will be released
23

VERIFICATION OF ELIGIBILITY: COVERED ENTITY
24

HRSA Clarification of Hospital Covered Entity
Based on 1994 guidance, any outpatient facility which is an integral component of a DSH will be included on the Medicare Cost Report and therefore eligible for 340B pricing
Included means: HRSA = As-filed cost report Federal Register language = included on the
Medicare cost report Statutory language = hospital and patient of
entity
25

VERIFICATION OF ELIGIBILITY: EMPLOYED OR CONTRACTED LICENSED PROFESSIONAL
26

Employed or Contracted Professional
An individual is a patient of a 340B covered entity only if: the covered entity has established a relationship with the
individual, such that the covered entity maintains records of the individual's health care; and
the individual receives health care services from a health care professional who is either employed by the covered entity or provides health care under contractual or other arrangements (e.g. referral for consultation) such that responsibility for the care provided remains with the covered entity
27

VERIFICATION OF ELIGIBILITY: GPO EXCLUSION
28

GPO Exclusion
Can a 340B hospital that is subject to the group purchasing organization (GPO) prohibition (Disproportionate Share Hospital, Children's Hospitals, Free Standing Cancer Hospitals) continue to purchase items from a GPO that are at a lower cost than 340B pricing? Answer
Hospitals that participate in the 340B Program for covered outpatient drugs and are subject to the GPO prohibition cannot purchase any covered outpatient drugs through a group purchasing organization or other group purchasing arrangement
This “GPO prohibition” is found in the 340B statute, at section 340B(a)(4)(L) and applies even if items are available at a lower price through the GPO
Hospitals can continue to purchase all products for inpatient operations through a GPO, even if the outpatient departments participate in the 340B Program
29

Hospital Covered Entities Summary
30

GPO Exclusion
31

PREVENT DIVERSION: OUTPATIENT DEFINITION
32

Patient Definition Overview
1996 – Final guidance of a patient 2007 – Proposed revisions to definition July 18, 2012 – Members of Congress ask HRSA for
further clarification on definition of eligible patient Program isn’t limited to Medicare, Medicaid or low
income patients Any patient of covered entity may received covered
OP drugs purchased under the 340B program Patient must be treated at a facility that is provider-
based to the covered entity. All new sites must be enrolled with OPA
33

Definition of a Patient
An individual is a patient of the 340B covered entity if: The covered entity has established a relationship with the individual, such that
the covered entity maintains records of the individual's health care; and The individual receives health care services from a health care professional
who is either employed by the covered entity or provides health care under contractual or other arrangements (e.g. referral for consultation) such that responsibility for the care provided remains with the covered entity; and
The individual receives a health care service or range of services from the covered entity which is consistent with the service or range of services for which grant funding or Federally-qualified health center look-alike status has been provided to the entity. Disproportionate share hospitals are exempt from this requirement.
If all 3 requirements are not met, the person is not eligible for 340B drugs
An individual will not be considered a patient of the covered entity if the only health care services received by the individual is the dispensing of a drug or drugs for subsequent self-administration or administration in the home setting
34

Polling Question #3
1. Do you routinely “self audit” to ensure compliance with patient definition?
a. Yes b. No c. Not sure d. N/A
35

340B Inventory Virtual Inventory Process
36

PREVENT DUPLICATE DISCOUNT: MEDICAID EXCLUSION
37

Medicaid Billing: Carve in/Carve out
HRSA guidelines allow covered entities to comply with the statute in different ways: Bill Medicaid at acquisition cost plus the state allowable
dispensing fee and the state does not request a rebate (“Carve In”)
“Carve out” Medicaid drugs from 340B program and allow state to collect rebates
Follow state guidelines for applicable billing limits Covered entities are responsible for working with their state
Medicaid agency to ensure that the agency can identify drugs purchased through the 340B program and avoid obtaining rebates on those drugs
38

CONTRACT PHARMACY COMPLIANCE
39

Contract Pharmacies
No distance or proximity limitation No longer a limit on number of contract pharmacy
arrangements Covered entity responsibility to comply, this is important to
remember for contract pharmacy arrangements Challenges:
Diversion tracking Audits & records Discount Management and tracking Data exchange Inventory management Business terms (payment risk, dispensing fees Advertising/marketing approval
40

Contract Pharmacy Audit Requirements
All covered entities are required to maintain auditable
records Expected to conduct annual audits of contract pharmacies To be performed by an independent outside auditor as a
way to fulfill their ongoing obligation of compliance To the extent that any compliance activity or audit
performed by a covered entity indicates that there has been a violation of 340B Program requirements, such finding should be disclosed to HRSA along with the covered entity's plan to address the violation
41

AUDIT SAMPLE OF DRUG ENCOUNTERS
42

Audit Sample
Small number of encounters sampled Selected from recent 6 months 28 – 50 encounters
Prescription Number NDC Product Name Quantity dispensed Date prescription written Date prescription filled Provider name NPI Patient name Medical record number/Patient ID number Payer The wholesale price paid (acquisition price) The amount billed for the drug The amount actually paid by the payer and patient
43
HOW TO PREPARE FOR HRSA AUDIT
44

Audit Tips
Conduct mock audits Develop effective policies and procedures
Patient eligibility Duplicate discounts Appropriate Medicaid billing
Create 340B task force for program oversight Multidisciplinary: Representation from pharmacy, administration, legal and
finance Group should meet periodically to review organizations operations against the
340B program standards and opinion letters
Keep current on developments/updates Be prepared for 340B integrity audit Risk Assessment HRSA Website
http://www.hrsa.gov/opa/ http://www.hrsa.gov/opa/faqs/index.html
45

How can Arnett Foster Toothman help?
46
Arnett Foster Toothman has assisted multiple clients with 340B mock audits, pharmacy policy and procedure compliance assistance and 340B benefit calculations
Conduct a mock HRSA 340B Integrity audit Review of policies and procedures regarding the procurement, inventory,
distribution, dispensing, and billing for covered outpatient drugs Documentation of internal controls applicable to the policies and procedures
identified above Review of policies and procedures to prevent the resale or transfer of drugs to a
person or persons who are not patients of the covered entity Review records of drug procurement and distribution and test whether hospital
has obtained a discount only for those programs authorized to receive discounts by section 340B of the PHS Act
Arnett Foster Toothman follows HRSA data request and audit protocol in order to mock actual HRSA Integrity Audit
This will provide the organization with a corrective plan of action, if necessary, and readiness when the actual HRSA audit occurs

Q&A
47
Questions ?

Thank You!
Brenda Christman, Member Arnett Foster Toothman PLLC 155 E Broad Street, Suite 2100 Columbus, OH 43215 614-223-9209 [email protected]
Brian Bell, Manager Arnett Foster Toothman PLLC 155 E Broad Street, Suite 2100 Columbus, OH 43215 614-223-9209 [email protected]
48