26 patient safety and quality in ambulatory care · wolters kluwer, inc. unauthorized ... chapter...
TRANSCRIPT

2 9 9
IntroductIonThe majority of patient safety and quality research has focused on the inpatient set-ting, leaving a lack of intervention-based research in patient safety and quality for the ambulatory setting. There were an estimated 1.1 billion ambulatory visits in the US in 2010 with this number expecting to rise due to the shift from inpatient to outpatient care and the aging population.1 Given these numbers, the potential harm in outpa-tient medicine is immense. According to the Colorado and Utah Medical Practices Study, an estimated 75,000 hospitalizations per year are due to preventable adverse events in the ambulatory setting. The most common types of ambulatory adverse events were medication events, surgical events, or diagnostic adverse events.2 Safety and quality principles, such as just culture, infection prevention, event identification and analysis, and communication and medication safety, have been researched for inpatients and can be modified for the outpatient setting. On the other hand, differ-ences between caring for inpatients and outpatients can make other safety methodol-ogy less relevant (Table 26-1).
Outpatient care encompasses a wide variety of patients, acuity of care, and health care settings. Outpatient practices can range from a single provider to a
Patient Safety and Quality in Ambulatory CareEmily Fondahn and Michael Lane
26cl In Ical V IgnetteMs. R is a 45-year-old woman who presented to her primary care physician (PCP) for her yearly physical examination. She pointed out a new mole on her right arm and on her right thigh to her PCP and was referred to a local dermatologist. At the derma-tologist’s office, she had a biopsy performed of both moles. After 2 weeks, she called the dermatology office for her test results and was told that the lesion was benign. The following year, she returned to her PCP for her yearly exam. Her PCP shared the same EMR as the dermatologist and discovered that the lesion on her right arm was melanoma and the lesion on her right thigh was benign. Later, it was discovered that the pathology report for the right arm lesion was accidentally misfiled, so the nurse only reported the results of the benign lesion.
• What are some key differences between patient safety for inpatients and outpatients?• What are the most common types of errors in the outpatient setting?• What methods are used to decrease the risk for failing to communicate results
to patients?
0002608487.INDD 299 2/17/2016 12:24:27 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.

3 0 0 T H E W A S H I N G T O N M A N U A L® O F PAT I E N T S A F E T Y
large, multispecialty group, with or without hospital affiliation. Given the variety of outpatient settings, there is likewise a wide range of quality and safety programs and initiatives.
Types of outpatient settings
1. Physician practices and clinics2. Ambulatory surgery centers3. Urgent care facilities4. Emergency departments5. Dialysis centers6. Imaging centers7. Oncology centers8. Endoscopy centers9. Rehabilitation centers
10. Sleep centers
Multiple barriers exist for initiation and sustainment of quality and safety pro-grams in the outpatient setting. Within a large medical group, there can be a wide range of management policies, resources, and electronic health record use, especially if the medical group is a merger of multiple smaller, relatively independent practices. Hospital-affiliated centers may have safety and quality resources provided by the hos-pital. Smaller practices may have more difficulty obtaining and maintaining quality measurements due to financial and personnel constraints.3 Team members, including the physicians, may not have sufficient training or protected time for safety and quality work. Additionally, with the advent of hospitalists, many primary care providers do not see patients in the inpatient setting resulting in decreased interaction with other pro-viders and increasing isolation. However, given the increasing amount of care provided in the ambulatory setting, these barriers need to be addressed to improve patient care.
taBle 26-1 differences between Inpatient and outpatient care
Inpatient outpatientEpisodic, high-intensity care Longitudinal care
Technologically complex Larger volume of patients
One medical record Multiple medical records frequently with pertinent information
Comprehensive care of patient Diffuse care settings requiring information exchange
Quality and safety officers employed by the hospital
Fewer resources with more staff multitasking
Services and providers readily available
Offsite laboratories and providers
Medical team arranges care coordination
Patients responsible for care coordination
More regulatory agencies More diversity of patients
0002608487.INDD 300 2/17/2016 12:24:27 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.

Chapter 26 • Patient Safety and Quality in Ambulatory Care 3 0 1
In the inpatient setting, medical care is delivered by a multidisciplinary team including physicians, nurses, respiratory therapists, and physical and occupational therapists, allowing for coordination of all care aspects. In the outpatient setting, the individual patients are often responsible for coordinating the majority of their health care without the same level of support; the burden of care is on the patient and his or her outpatient caregivers (family, friends, etc.). Poor patient outcomes and adverse events can occur due to the patient’s increased accountability for managing his or her own health and making treatment decisions. For example, patients with congestive heart failure will make numerous decisions to guide their health every day, such as taking their medications as prescribed, eating a low-salt diet, regularly weighing them-selves, and calling their health care provider with worsening symptoms. However, if patients do not follow or understand their care instructions, they may be at increased risk for worsening disease and a poor outcome.
PatIent Safety In amBulatory careOutpatient care may also be viewed as safer given the lower acuity of illness in healthier patients. However, patient harm can and still does occur. Errors are frequently not reported in the ambulatory setting. Outpatient visits outnumber hospital discharges by more than 30–1. On average, an individual will have approx-imately 4 visits to an ambulatory care center each year; however, only approxi-mately 10% of Americans will have an inpatient stay in a given year.1 Despite the fact that the vast majority of medical care is delivered in the ambulatory set-ting, only 4.1% of sentinel events reported to the Joint Commission occurred in the ambulatory setting.4 Error reporting is difficult in the ambulatory setting due to short patient interactions, multiple providers in different settings, lack of con-sensus about error definitions, and lack of ambulatory error reporting systems.5 Improved classification of outpatient errors can help create categories for future study.6 In 2011, the American Medical Association (AMA) published a 10-year review entitled “Research in the Ambulatory Patient Safety,” which identified the top six errors made in the ambulatory setting and current gaps in research.7 The top six errors identified include the following:
• Medication errors• Diagnostic errors• Laboratory errors• Clinical knowledge errors• Communication errors• Administrative errors
Understanding these errors helps teach us when to recognize an error when it occurs and prevent future errors. Some of these topics are covered in more detail in other chapters (Medication Safety, Diagnostic Errors).
medIcatIon errorSMedication errors are very common in the outpatient setting. This section highlights some of the unique difficulties with medication safety for the ambulatory setting. In the inpatient setting, physicians can generally assume that the patient is receiving what is listed on the medication list at the correct times and dosages and can monitor closely for adverse events and drug levels. However, given the longer feedback loops
0002608487.INDD 301 2/17/2016 12:24:27 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.

3 0 2 T H E W A S H I N G T O N M A N U A L® O F PAT I E N T S A F E T Y
in outpatient care, providers lose much of this control and become more reliant on patients to accurately report all medications and dosages they are taking. The number of patients experiencing medication errors in the ambulatory setting is staggering; a report from the Institute of Medicine in 2006 estimated 530,000 Medicare beneficia-ries in ambulatory clinics experienced a medication-related error in the year.8,9
medication reconciliationMedication reconciliation should occur at every transition of care and patient appoint-ment. However, patients frequently do not know medication names or doses, and time is not available to go through the entire medication list. It has been estimated that a complete medication reconciliation process takes between 15 and 30 minutes.10 Given the time pressures on clinicians in the ambulatory setting, it is not surprising that medication reconciliation may not routinely be completed. There is significant potential for harm though as on discharge from the hospital, 23% of patients were not taking their discharge medications and 29% had a discrepancy between their discharge medication list and what they were actually taking.11
Patient adherenceHealth care providers may fail to recognize the contribution of nonadherence to a patient’s health and medical condition. In one study examining 195,000 newly prescribed e-prescriptions, only 72% were filled.12 Medications for chronic condi-tions, such as diabetes, hypertension, and hyperlipidemia, were more likely to have noncompliance. Health care providers may overestimate patient’s understanding of medications. In one study of 359 adults waiting for an ambulatory appointment, understanding of prescription label instructions ranged from 53% to 89%.13 Tools to help patients adhere and understand their medications include providing a medica-tion list at every visit, encouraging patients to bring medications to all appointments, providing patients with a pill box, using patient-friendly language on the prescription instructions, and educating patients and caregivers about important side effects and interactions.
medication monitoringMany medications require careful monitoring in the outpatient setting. Outpatient clinicians must create reliable processes to accurately monitor these medications. The most common errors are failure to act on available information, such as signs, symp-toms, or laboratory values of drug toxicity (e.g., failure to respond promptly to systems suggestive of digoxin toxicity) and inadequate laboratory monitoring of drug therapies (e.g., checking International normalized ratio [INRs] for patient on warfarin).9
medication PrescribingPrescribing errors are some of the most common in ambulatory medicine. In one study evaluating 1879 prescriptions, 7.6% had a medication error that was life threatening, serious, or significant.14 E-prescribing has shown promise to decrease this amount of errors by requiring complete, legible prescriptions, checking interac-tions, and checking allergies. A small study of 15 providers showed a decrease in error rates from 42/100 prescriptions to 6/100 prescriptions after implementation of an e-prescribing system with clinical decision support including dosing recom-mendations and checks for drug–drug interactions, patient allergies, and duplicate therapy.15
0002608487.INDD 302 2/17/2016 12:24:27 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.
Chapter 26 • Patient Safety and Quality in Ambulatory Care 3 0 3
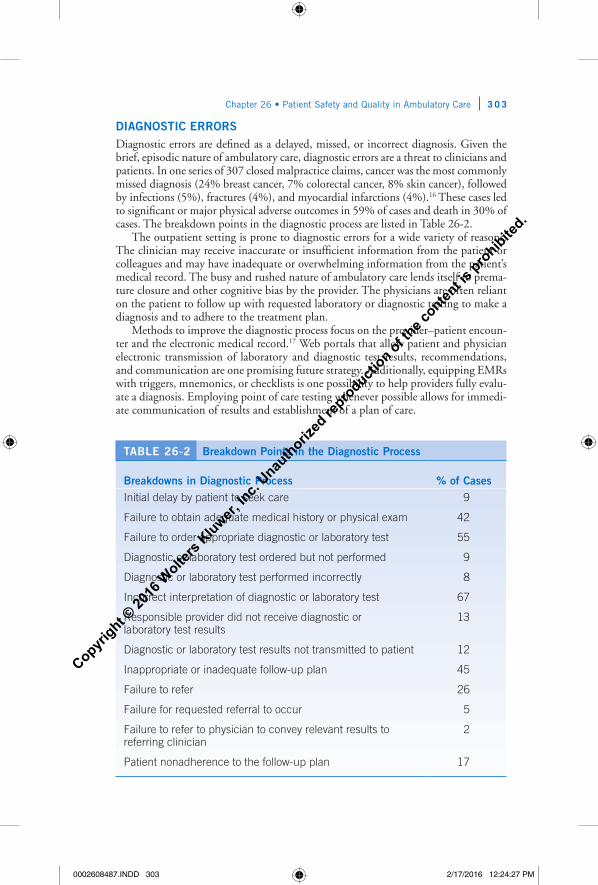
dIagnoStIc errorSDiagnostic errors are defined as a delayed, missed, or incorrect diagnosis. Given the brief, episodic nature of ambulatory care, diagnostic errors are a threat to clinicians and patients. In one series of 307 closed malpractice claims, cancer was the most commonly missed diagnosis (24% breast cancer, 7% colorectal cancer, 8% skin cancer), followed by infections (5%), fractures (4%), and myocardial infarctions (4%).16 These cases led to significant or major physical adverse outcomes in 59% of cases and death in 30% of cases. The breakdown points in the diagnostic process are listed in Table 26-2.
The outpatient setting is prone to diagnostic errors for a wide variety of reasons. The clinician may receive inaccurate or insufficient information from the patient or colleagues and may have inadequate or overwhelming information from the patient’s medical record. The busy and rushed nature of ambulatory care lends itself to prema-ture closure and other cognitive bias by the provider. The physicians are often reliant on the patient to follow up with requested laboratory or diagnostic testing to make a diagnosis and to adhere to the treatment plan.
Methods to improve the diagnostic process focus on the provider–patient encoun-ter and the electronic medical record.17 Web portals that allow patient and physician electronic transmission of laboratory and diagnostic test results, recommendations, and communication are one promising future strategy. Additionally, equipping EMRs with triggers, mnemonics, or checklists is one possibility to help providers fully evalu-ate a diagnosis. Employing point of care testing whenever possible allows for immedi-ate communication of results and establishment of a plan of care.
taBle 26-2 Breakdown Points in the diagnostic Process
Breakdowns in diagnostic Process % of casesInitial delay by patient to seek care 9
Failure to obtain adequate medical history or physical exam 42
Failure to order appropriate diagnostic or laboratory test 55
Diagnostic or laboratory test ordered but not performed 9
Diagnostic or laboratory test performed incorrectly 8
Incorrect interpretation of diagnostic or laboratory test 67
Responsible provider did not receive diagnostic or laboratory test results
13
Diagnostic or laboratory test results not transmitted to patient 12
Inappropriate or inadequate follow-up plan 45
Failure to refer 26
Failure for requested referral to occur 5
Failure to refer to physician to convey relevant results to referring clinician
2
Patient nonadherence to the follow-up plan 17
0002608487.INDD 303 2/17/2016 12:24:27 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.

3 0 4 T H E W A S H I N G T O N M A N U A L® O F PAT I E N T S A F E T Y
communIcatIon errorSNumerous studies have shown that lapses in communication contribute to poor quality care and patient safety. As discussed previously, the providers rely on the patients to bring forward concerns, symptoms, and accurate medical histories to help them diagnose problems and identify potential adverse medication errors. However, during the clinical encounter, physicians often lack the information needed. In a sur-vey of 253 clinicians in 32 Colorado practices, important information was missing at the time of the visit in 13.6% of cases.18 The lack of information was thought to likely lead to delayed care or duplicated care in 59.5% of the cases. The likelihood of missing information increased as the number of active medical problems increased (Fig. 26-1).
Similarly, the patients expect that their providers will provide them with prompt information from study or laboratory results and clear follow-up and treatment plans. Numerous gaps currently exist in the follow-up of laboratory or radiology results. Reasons for errors in laboratory result notification can be as simple as misfiling a paper or not having a chart available. If patients do not hear from their physician, they may incorrectly assume that the results were within normal limits and “no news is good news.” Physicians report spending well over an hour per day managing test results (74 minutes/day), but 83% reported that they wished they had reviewed at least one test in the last 2 months earlier.19 Among surveyed ambulatory medical practices, 52% reported having a system to record tests ordered while only 32% of practices had systems to detect if patients missed tests.
In the outpatient setting, the referral process is prone to breakdowns and errors. Both specialists and primary care providers express frustration about the referral pro-cess and communication between providers. The referral process can be difficult due to physician time restraints, lack of clarity regarding reason for referral, patient self-referrals, insurance limitations, different medical record systems, and unclear follow-up plans (Table 26-3).20 In a survey of 48 primary care providers, 63% reported being dissatisfied with the referral process. Additionally neither the PCP nor the specialist felt like they were receiving the information needed from the other provider. In the
Patient ProviderSymptomsPast medical historyAllergiesMedications
Laboratory ordiagnostic test resultsFollow-up planTreatment plan
PCP SpecialistReason for referralPrevious laboratory ordiagnostic studies Patient medicalproblemsPatient medications
Timely recommendationsResults of test andprocedures
Plan for future care and rolein medical management
• •
••
•
•
••
•
•
•••
figure 26-1. Ambulatory lapses in communication.
0002608487.INDD 304 2/17/2016 12:24:28 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.

Chapter 26 • Patient Safety and Quality in Ambulatory Care 3 0 5
outpatient setting, much of the referral process occurs via notes and letters, rather than conversations between practitioners. This lack of clear communication hinders the utility of many referrals.
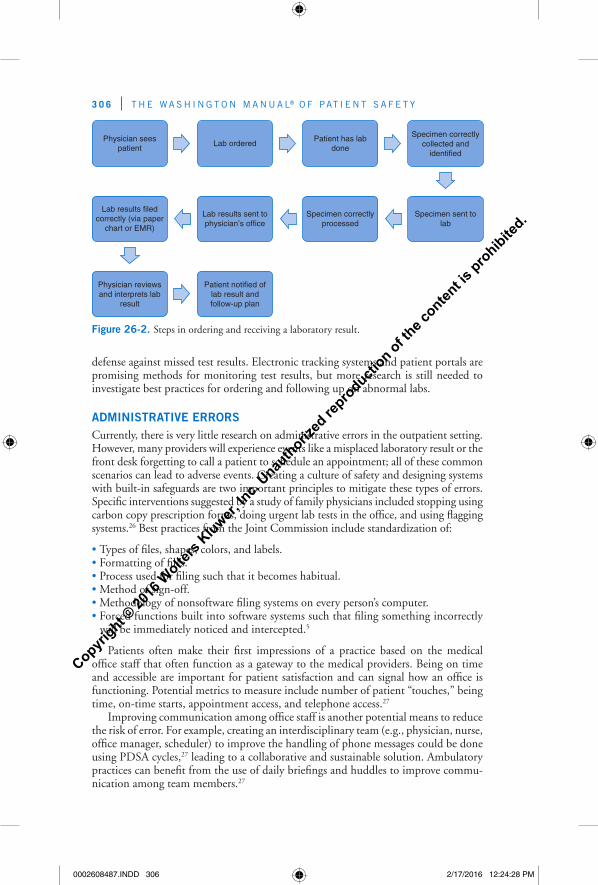
laBoratory errorSPrimary care providers order lab tests on an estimated 29–38% of encounters.21 These laboratory tests can contribute to between 15% and 54% of errors in primary care. Primary care providers review a tremendous amount of test results per week—one report found that a full-time primary care provider will review 930 chemistry/hematology reports and 60 pathology and radiology reports in a week.22 Given that there is usually a delay between seeing the patient, ordering the test, and obtaining the test result, it is easy to forget about test results. Ambulatory offices lag behind hospitals in developing and implementing systems to prevent errors from occurring. There are multiple steps that occur between ordering a test to acting upon the test results; errors may occur at each of these steps (Fig. 26-2). Types of errors include missed/delayed provider of test results, patient follow-up of test results, patient notification about test result, and laboratory errors such as incorrectly labeling or processing a specimen. Unfortunately, few practices have systems in place to accurately track labs ordered, reporting of results, and patient notification.23 A survey of primary care providers similarly showed that 37% of providers had seen a patient in the last 2 weeks with a missed test result.24 The most commonly missed diagnostic studies included imaging (29%), common clinical pathology (22%), anatomic pathology (9%) and other stud-ies (40%). The most common diagnosis that had a delay in care was cancer (34%). In addition to the process steps, errors can occur if the provider orders the wrong test or when the appropriate test is not ordered.25 Standardization of the test result process is one important tool to decrease errors. Practices should have a standard way to order tests, track results, respond and document test results, and notify patients.21 Engaging patients to be active participants in their care is one potential strategy for mitigating risk. Although many patients may assume that “no news is good news,” encouraging patients to actively seek out their test results may add another layer of
taBle 26-3 Breakdowns and errors in the outpatient referral Process
Primary care Providers SpecialistsTimeliness of information from specialists
Timeliness of information from PCP
Redundant aspects of current process
Time required for insurance approvals for studies and procedures
Time required to create adequate referral note
Time required for medication manage-ment approvals
Difficulty in finding a specialist Lack of clarity of note content from PCP
Lack of knowledge of role of medical management
Time required to create an adequate note for PCP
Time required for medication management approvals
Redundant aspects of current process
0002608487.INDD 305 2/17/2016 12:24:28 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.
3 0 6 T H E W A S H I N G T O N M A N U A L® O F PAT I E N T S A F E T Y
defense against missed test results. Electronic tracking systems and patient portals are promising methods for monitoring test results, but more research is still needed to investigate best practices for ordering and following up on abnormal labs.
admInIStratIVe errorSCurrently, there is very little research on administrative errors in the outpatient setting. However, many providers will experience events like a misplaced laboratory result or the front desk forgetting to call a patient to schedule an appointment; all of these common scenarios can lead to adverse events. Creating a culture of safety and designing systems with built-in safeguards are two important principles to mitigate these types of errors. Specific interventions suggested by a study of family physicians included stopping using carbon copy prescription forms, doing urgent lab tests in the office, and using flagging systems.26 Best practices from the Joint Commission include standardization of:
• Types of files, shapes, colors, and labels.• Formatting of files.• Process used for filing such that it becomes habitual.• Method of sign-off.• Methodology of nonsoftware filing systems on every person’s computer.• Forced functions built into software systems such that filing something incorrectly
will be immediately noticed and intercepted.5
Patients often make their first impressions of a practice based on the medical office staff that often function as a gateway to the medical providers. Being on time and accessible are important for patient satisfaction and can signal how an office is functioning. Potential metrics to measure include number of patient “touches,” being time, on-time starts, appointment access, and telephone access.27
Improving communication among office staff is another potential means to reduce the risk of error. For example, creating an interdisciplinary team (e.g., physician, nurse, office manager, scheduler) to improve the handling of phone messages could be done using PDSA cycles,27 leading to a collaborative and sustainable solution. Ambulatory practices can benefit from the use of daily briefings and huddles to improve commu-nication among team members.27
Physician seespatient
Lab orderedPatient has lab
done
Specimen correctlycollected and
identified
Specimen sent tolab
Specimen correctlyprocessed
Lab results sent tophysician’s office
Lab results filedcorrectly (via paper
chart or EMR)
Physician reviewsand interprets lab
result
Patient notified oflab result andfollow-up plan
figure 26-2. Steps in ordering and receiving a laboratory result.
0002608487.INDD 306 2/17/2016 12:24:28 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.

Chapter 26 • Patient Safety and Quality in Ambulatory Care 3 0 7
Safety and QualIty In PrImary carePrimary care providers have a crucial role in following and managing patients. Given the increasing complexity of health care, many people now are receiving care by a variety of clinicians in many different settings and facilities. The PCP is supposed to be the link between all these different providers. However, PCPs are under increased pressure to see more patients, maximize billing, manage transitions of care, and track quality. The agenda in an outpatient visit is jam-packed: address-ing patient concerns and medical problems, creating and updating a problem list, reconciling medications, reviewing allergies, documenting a review of systems, completing a physical exam, ordering tests, prescribing new medications, making referrals, coordinating testing logistics, allowing time for questions, and doing this all in a patient-centered manner! The average primary care encounter lasts around 17–20 minutes and covers six topics.28,29 Unfortunately, there is little time to do all that needs to be done.
A gap exists between recommended care and actual care received by patients. For example, in 2011, between only 58.4% and 65.4% of patients diagnosed with hypertension had adequate control. The breast cancer screening rate var-ies between 50.4% and 70.5%.30 Another analysis showed that only 54.9% of the population received recommended preventative care.31 Common outpatient quality improvement projects often involve preventive and chronic care. The Ambulatory Care Quality Alliance (AQA) was started in 2004 as collaboration between the American Academy of Family Physicians (AAFP), the American College of Physicians (ACP), America’s Health Insurance Plans (AHIP), and the Agency for Healthcare Research and Quality (AHRQ) to improve collection and reporting of ambulatory quality measures.
A “starter set” of 26 measures was developed for ambulatory care covering cancer screening, vaccination, tobacco use and cessation, coronary artery disease, heart fail-ure, diabetes, depression, asthma, prenatal care, and antibiotic use.32 This starter set is one possible framework for practices that wish to begin collecting, analyzing, and improving on ambulatory quality metrics.
The creation of Primary Care Medical Homes (PCMH) is another possible mechanism to improve the quality and safety provided to patients. The AHRQ defines a PCMH as a “mechanism for organizing primary care to provide high-quality care across the full range of an individual’s health care needs. It focuses on teams of health care professionals proving coordinated and accessible care to an identifiable group of patients.”33 PCMH aim to create care that is patient cen-tered, comprehensive, coordinated, accessible, and committed to quality and safety. Each patient has an ongoing relationship with a personal physician. The practice works as a team to address the patient’s needs, ongoing care, and access to services.34 A systematic review showed that PCMH has a small positive effect on patient expe-rience and small to moderate positive effect on preventative care.33 This concept is also expanding to Patient Centered Medical Home Neighbors for specialty and sub-specialty practices to improve communication and comanagement between PCPs and consultants.
creatIng an outPatIent Safety and QualIty ProgramTo date, much of the safety and quality focus has been on the inpatient setting. However, with increasing emphasis on value-based purchasing and public report-ing, outpatient medical practices will face increasing pressure to create and maintain
0002608487.INDD 307 2/17/2016 12:24:28 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.

3 0 8 T H E W A S H I N G T O N M A N U A L® O F PAT I E N T S A F E T Y
quality and safety programs. The EHR incentive program includes clinical quality measures that practices will have to report on. A recommended core set of measures for adults and pediatrics that focuses on high-priority health conditions and best practices has been complied, which includes controlling high blood pressure, tobacco use screening and cessation, and childhood immunization status.35 Many physicians are being required to perform a self-assessment and quality improvement project for their practice as part of their maintenance of certification through their medical board.
Many practices may feel overwhelmed by quality improvement projects and data reporting. Historically, safety and quality improvement have been a relatively small component in medical education, making it difficult for existing practices to create a safety and quality program that engages the multitude of roles involved in safe medi-cal care. At a minimum, components of an outpatient safety and quality improvement program should include the following:
• Providing training for staff• Identifying key areas for improvement• Identifying and removing barriers of improvement• Creating a tracking system for quality and safety issues• Developing specific safety and quality goals that are reviewed regularly• Developing metrics that measure the safety and quality of care• Assigning of responsibility and accountability to monitor metrics• Supporting a Just culture and reporting of errors• Engaging patients36
Multiple preexisting frameworks exist for quality improvement programs, and some of these programs will assist with the analysis of data. Many different specialty societies have quality programs with suggested metrics. National organizations have preestablished metrics that can be followed based upon disease, specialty, and patient population. These resources can be beneficial for practices learning about quality improvement.
SummaryImproving patient safety and quality for the ambulatory setting is a much needed next step for the quality movement. As more care is transitioned to outpatients, the potential amount of harm will be increasing. Creating a taxonomy to define errors is a first step, followed by creating a safe culture and error reporting systems, to finally creating system-based solutions to decrease errors. Major areas of inter-est include communication, medication safety, diagnostic error, laboratory error, and administrative error. While principles learned from the inpatient setting may be useful to improve care, these tools will need to be adapted to the outpatient setting. Despite many of the difficulties, some safety and quality initiatives in the outpatient setting may be more feasible since patients are not as acutely ill, allow-ing them to be more engaged. Additionally, most outpatient clinics will have a smaller staff, which may make it easier to implement and communicate changes. Therefore, smaller, easier tools or system changes can have large impacts with-out as much time and money invested when compared to the inpatient setting.4 Practices need to look at their relationship with consultants, laboratories, hospitals, and home health organizations to ensure that they have methods to track patients and communicate results.
0002608487.INDD 308 2/17/2016 12:24:28 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.
Chapter 26 • Patient Safety and Quality in Ambulatory Care 3 0 9
onlIne reSourceS1. Patient Safety Tools for Physician Practices: http://www.mgma.com/pppsahome/2. The Ambulatory Care Quality Alliance Recommended Starter Set: The
Ambulatory Care Quality Alliance. May 2005. Agency for Healthcare Research and Quality, Rockville, MD: http://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/ambulatory-care/starter-set.html
3. Patient Centered Primary Care Collaborative: http://www.pcpcc.org/
referenceS
1. National Ambulatory Medical Care Survey: 2010 Summary Tables. 2010 [cited 2013 8/18/13]. Available from: http://www.cdc.gov/nchs/data/ahcd/namcs_summary/2010_namcs_web_tables.pdf
2. Woods DM, Thomas EJ, Holl JL, et al. Ambulatory care adverse events and preventable adverse events leading to a hospital admission. Qual Saf Health Care. 2007;16(2):127–31.
3. Landon BE, Normand. National Voluntary Consensus Standards for Ambulatory Care: Measurement Challenges in Small Group Settings. Washington, DC: National Quality Foundation; 2006.
4. Summary Data of Sentinel Events Reviewed by the Joint Commission. 2012. Available from: http://www.jointcommission.org/assets/1/18/2004_4Q_2012_SE_Stats_Summary.pdf
5. The Joint Commission, Fry HM, eds. A Patient Safety Handbook for Ambulatory Care Providers. 1st ed. Oakbrook Terrace, IL: Joint Commission Resources; 2009.
6. Pace WD, Fernald DH, Harris DM, et al. Developing a taxonomy for coding ambulatory medical errors: a report from the ASIPS collaborative. In: Henriksen K, Battles JB, Marks ES, et al., eds. Advances in Patient Safety: From Research to Implementation. Rockville, MD: Agency for Healthcare Research and Quality; 2005.
7. Lorincz CY, Drazen E, Sokol PE, et al. Research in Ambulatory Patient Safety 2000–2010: A 10-Year Review. Chicago, IL: American Medical Association; 2011.
8. Aspden P, Wolcott J, Bootman JL, et al. Preventing Medication Errors: Committee of Identifying and Preventing Medication Errors. Washington, DC: Institute of Medicine; 2006.
9. Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289(9):1107–16.
10. Gleason KM, Brake H, Agramonte V, et al. Medications at Transitions and Clinical Handoffs (MATCH) Toolkit for Medication Reconciliation. Prepared by the Island Peer Review Organization, Inc., under Contract No. HHSA2902009000 13C. Rockville, MD: Agency for Healthcare Research and Quality; 2011.
11. Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166(5):565–71.
12. Fischer MA, Stedman MR, Lii J, et al. Primary medication non-adherence: analysis of 195,930 electronic prescriptions. J Gen Intern Med. 2010;25(4):284–90.
Key Po IntS• Outpatient safety and quality differs from inpatient care due to the large volume of
patients, longitudinal care, and the diffuse care environment.• The wide variety of outpatient settings and providers can make safety and quality
work challenging.• Outpatient practices need to identify ways to standardize systems, identify errors,
and maintain a just culture.• Causes of errors include medication errors, diagnostic errors, laboratory errors, clini-
cal knowledge errors, communication errors, and administrative errors.
0002608487.INDD 309 2/17/2016 12:24:28 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.

3 1 0 T H E W A S H I N G T O N M A N U A L® O F PAT I E N T S A F E T Y
13. Davis TC, Federman AD, Bass PF III, et al. Improving patient understanding of prescription drug label instructions. J Gen Intern Med. 2009;24(1):57–62.
14. Gandhi TK, Weingart SN, Seger AC, et al. Outpatient prescribing errors and the impact of computerized prescribing. J Gen Intern Med. 2005;20(9):837–41.
15. Kaushal R, Kern LM, Barrón Y, et al. Electronic prescribing improves medication safety in community-based office practices. J Gen Intern Med. 2010;25(6):530–6.
16. Gandhi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med. 2006;145(7):488–96.
17. Singh H, Weingart SN. Diagnostic errors in ambulatory care: dimensions and preventive strategies. Adv Health Sci Educ Theory Pract. 2009;14(Suppl 1):57–61.
18. Smith PC, Araya-Guerra R, Bublitz C, et al. Missing clinical information during primary care visits. JAMA. 2005;293(5):565–71.
19. Poon EG, Gandhi TK, Sequist TD, et al. “I wish I had seen this test result earlier!”: Dissatisfaction with test result management systems in primary care. Arch Intern Med. 2004;164(20):2223–8.
20. Gandhi TK, Sittig DF, Franklin M, et al. Communication breakdown in the outpatient referral process. J Gen Intern Med. 2000;15(9):626–31.
21. Hickner JM, Fernald DH, Harris DM, et al. Issues and initiatives in the testing process in primary care physician offices. Jt Comm J Qual Patient Saf. 2005;31(2):81–9.
22. Poon EG, Wang SJ, Gandhi TK, et al. Design and implementation of a comprehensive outpatient Results Manager. J Biomed Inform. 2003;36(1–2):80–91.
23. Smith ML, Raab SS, Fernald DH, et al. Evaluating the connections between primary care practice and clinical laboratory testing: a review of the literature and call for laboratory involvement in the solutions. Arch Pathol Lab Med. 2013;137(1):120–5.
24. Wahls TL, Cram PM. The frequency of missed test results and associated treatment delays in a highly computerized health system. BMC Fam Pract. 2007;8:32.
25. Dovey SM, Meyers DS, Phillips RL, et al. A preliminary taxonomy of medical errors in fam-ily practice. Qual Saf Health Care. 2002;11(3):233–8.
26. Dovey SM, Phillips RI, Green LA, et al. Family physicians’ solutions to common medical errors. Am Fam Physician. 2003;67(6):1168.
27. Webster JS, King HB, Toomey LM, et al. Understanding quality and safety problems in the ambulatory environment: seeking improvement with promising teamwork tools and strategies. In: Henriksen K, Battles JB, Keyes MA, et al., eds. Advances in Patient Safety: New Directions and Alternative Approaches. Vol. 3: Performance and Tools. Rockville, MD: Agency for Healthcare Research and Quality (US); 2008:1–15.
28. Tai-Seale M, McGuire TG, Zhang W. Time allocation in primary care office visits. Health Serv Res. 2007;42(5):1871–94.
29. Chen LM, Farwell WR, Jha AK. Primary care visit duration and quality: does good care take longer? Arch Intern Med. 2009;169(20):1866–72.
30. Focus on Obesity and on Medicare Plan Improvement; The State of Health Care Quality 2012. National Committee for Quality Assurance; 2012:1–230.
31. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635–45.
32. Ambulatory Care Quality Alliance. Ambulatory Care Quality Alliance Recommended Starter Set. Available from: http://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/ tools/ambulatory-care/starter-set.html
33. Jackson GL, Powers BJ, Chatterjee R, et al. The patient-centered medical home a systematic review. Ann Intern Med. 2013;158(3):169–78.
34. Patient-Centered Primary Care Collaborative. Available from: http://www.pcpcc.org/35. 2014 Clinical Quality Measures. Available from: https://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/2014_ClinicalQualityMeasures.html. Accessed 12/14/15.
36. Guinane C, Davis N. Improving Quality in Outpatient Services. Boca Raton, FL: CRC Press; 2011.
0002608487.INDD 310 2/17/2016 12:24:28 PM
Copyright ©
2016
Wolte
rs Kluwer,
Inc.
Unauthoriz
ed re
producti
on of the c
ontent is
prohibite
d.