244 simion.qxd 4/7/09 10:06 am page 244 - ykdent.com.t · 244_simion.qxd 4/7/09 10:06 am page 244...
TRANSCRIPT
The International Journal of Periodontics & Restorative Dentistry
244_Simion.qxd 4/7/09 10:06 AM Page 244
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Effective vertical regeneration ofseverely atrophied edentulous alveo-lar ridges often continues to elude sur-geons’ best efforts, in spite of signifi-cant advances in bone regenerativetherapeutics. Restoration of verticalbone height in these atrophied jawsegments is critical to successful long-term implant survival and function.Numerous procedures, including bonesplitting, distraction osteogenesis,forced tooth eruption, guided boneregeneration, and autogenous onlaybone grafting, provide surgeons withan array of alternative approaches tothe management of severe alveolarbony atrophy.1–6 Although viable, eachof these procedures presents potentialcomplications and has shown limitedsuccess when addressing severe alve-olar bone loss. Autogenous bonegrafts remain perhaps the mainstay ofcurrent approaches to augmentseverely atrophied alveolar bone.
Autogenous bone grafts repre-sent an ideal matrix by providing animmunologically compatible source ofbone complete with viable osteo-progenitor and mature osteoblasticcells, an effective osteoconductivescaffold, and abundant numbers of the
Vertical Ridge Augmentation Using anEquine Block Infused with RecombinantHuman Platelet-Derived Growth Factor-BB: A Histologic Study in aCanine Model
Massimo Simion, MD, DDS1/Myron Nevins, DDS2/Isabella Rocchietta, DDS3/Filippo Fontana, DDS4/Emilio Maschera, MD, DDS5/Peter Schupbach, PhD6/David M. Kim, DDS, DMSc7
This preclinical study evaluated the efficacy of purified recombinant human platelet-derived
growth factor (rhPDGF-BB), combined with a novel equine hydroxyapatite and collagen (eHAC)
bone block, in providing vertical bone regeneration in critical-size defects simulating localized
mandibular alveolar bone atrophy. In addition, the impact of barrier membrane placement in
growth factor–mediated bone regeneration was also studied. Bilateral posterior mandibular
defects simulating severe localized bony atrophy were created in 12 adult foxhounds following
removal of all four mandibular premolars. Three months later, the defects were grafted as fol-
lows: group A: eHAC block alone; group B: eHAC block + collagen membrane; group C: eHAC
block + rhPDGF-BB; group D: eHAC block + rhPDGF-BB + membrane. The animals were sacri-
ficed after 5 months and the grafted areas were examined histologically, radiographically, and
clinically. Groups A and B (controls) exhibited little to no vertical bone regeneration. Group C
demonstrated significant vertical bone regeneration, with dense, well-vascularized bone, high
bone-to-implant contact, and accelerated replacement of graft particles with newly formed
bone. In group D, with the imposition of a barrier membrane, robust bone regeneration was
less evident when compared to group C. As in the first study in this series, the importance of
the periosteum as a source of osteoprogenitor cells in growth factor–mediated regenerative
procedures is examined. (Int J Periodontics Restorative Dent 2009;29:245–255.)
Massimo Simion and Myron Nevins equally contributed to this article.1Professor and Chairman, Department of Periodontology, School of Dentistry, University of Milan, Italy;Institute for Dental Research and Education, Milan, Italy.
2Clinical Associate Professor, Department of Oral Medicine, Infection and Immunity, Division ofPeriodontics, Harvard School of Dental Medicine, Boston, Massachusetts.
3Research Assistant, Department of Periodontology, School of Dentistry, University of Milan, Italy; Institutefor Dental Research and Education, Milan, Italy.
4Research Assistant, Department of Implantology, School of Dentistry, University of Milan, Italy; Institutefor Dental Research and Education, Milan, Italy.
5Private Practice, Milan, Italy; Institute for Dental Research and Education, Milan, Italy.6Adjunct Professor, School of Dental Medicine, University of Pennsylvania, Philadelphia, Pennsylvania. 7Assistant Professor, Department of Oral Medicine, Infection and Immunity, Division of Periodontics,Harvard School of Dental Medicine, Boston, Massachusetts.
Correspondence to: Prof Massimo Simion, Institute for Dental Research and Education, Viale Tunisia 48,20100 Milano, Italy; email: [email protected].
245
Volume 29, Number 3, 2009
244_Simion.qxd 4/7/09 10:06 AM Page 245
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

growth factor–signaling moleculesrequired for optimal bone regenera-tion.7 However, pain and morbidity atthe donor site, as well as a limited sup-ply of autogenous graft material, oftenpreclude or discourage the use ofautogenous grafts.8
Tissue engineering may offer aviable and attractive alternative to cur-rent treatment modalities for the surgi-cal management of severe jawboneatrophy. Recombinantly producedhuman platelet-derived growth factor-BB (rhPDGF-BB), with its potentchemotactic and mitogenic effects onsuch target cells as periodontal liga-ment and alveolar bone, as well as itscritical role in angiogenesis, may poten-tially play an effective role in the treat-ment of severe alveolar bone atro-phy.9–11 Simion et al achievedsignificant vertical bone regeneration insevere mandibular alveolar ridgedefects using a deproteinized bovineblock infused with rhPDGF-BB in acanine model.12 A human case reportproduced similar results, with place-ment of an rhPDGF-BB–saturateddeproteinized bovine block prior toimplant placement in the posteriormandible.13 Growth factor–mediatedbone regeneration obviated the needfor autogenous grafting in both studies.
Placement of a user-friendlymatrix with appropriate growth factorattachment and release kinetics is crit-ical to successful bone and tissueregenerative procedures. An equinehydroxyapatite and collagen boneblock (eHAC) appeared to be bio-compatible and easily managed whenapplied to atrophied bony surfaces ina canine model.14 The purpose of thecurrent study was to assess the safety
and efficacy of the eHAC block,infused with rhPDGF-BB and appliedwith and without a collagen barriermembrane, to achieve vertical boneaugmentation in severe mandibularcritical-size defects in a standardizedcanine model.
Method and materials
The study protocol was approved andconducted in accordance with theBiomatech Ethical Committee in Lyon,France.
Tooth extraction and defect creation
Twelve foxhounds (each weighing atleast 25 kg) were selected for the study.A critical-size alveolar bone defect withboth the buccal and lingual bonyplates removed was created by bilat-eral extraction of all four mandibularpremolars and surgical reduction ofthe ridge height and width with rotaryand hand instrumentation. The dimen-sions of the standardized defects were20 to 25 mm mesiodistally, 7 to 8 mmapicocoronally, and 10 mm buccolin-gually (Fig 1a). Primary wound closurewas achieved by means of interruptedsutures (CV-5, W. L. Gore & Associates).Periapical radiographs were obtainedprior to and immediately followingsurgery. Sutures were removed after10 to 14 days.
246
The International Journal of Periodontics & Restorative Dentistry
244_Simion.qxd 4/7/09 10:06 AM Page 246
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
Vertical ridge augmentationprocedure
To create a chronic bony defect, a heal-ing period of 3 months preceded theaugmentation procedure. At that time,bilateral mandibular full-thickness buc-cal and lingual mucoperiosteal flapswere elevated, extending from themesial aspect of the canine to the dis-tal aspect of the first molar. All soft tis-sue remnants were removed from thedefect surface, and cortical perfora-tions were made with a round carbide
control group, received the eHACbone block in conjunction with an over-lying resorbable collagen membrane(Bio-Gide, Geistlich Pharma). Group Canimals were treated with an eHACblock infused with rhPDGF-BB(Osteohealth) and group D animalswere treated with an eHAC blockinfused with rhPDGF-BB and coveredwith a resorbable collagen membrane.Ten defect sites were randomly allo-cated to groups A and B, whereas 14sites were randomly allocated togroups C and D, for a total of 24 sites.
bur, exposing the underlying medullaryspaces (Fig 1b). An eHAC bone block(Geistlich Pharma) was closely adaptedto the bony defect site and stabilizedwith two titanium implants (3.3 � 10mm, Speedy Groovy, Nobel Biocare)that penetrated both the block andthe native mandibular cortical bone(Fig 2). Cover screws were then placedover the implants.
Four cohorts were included in thestudy design. Group A, one of twocontrol groups, received an eHACbone block alone. Group B, the second
247
Volume 29, Number 3, 2009
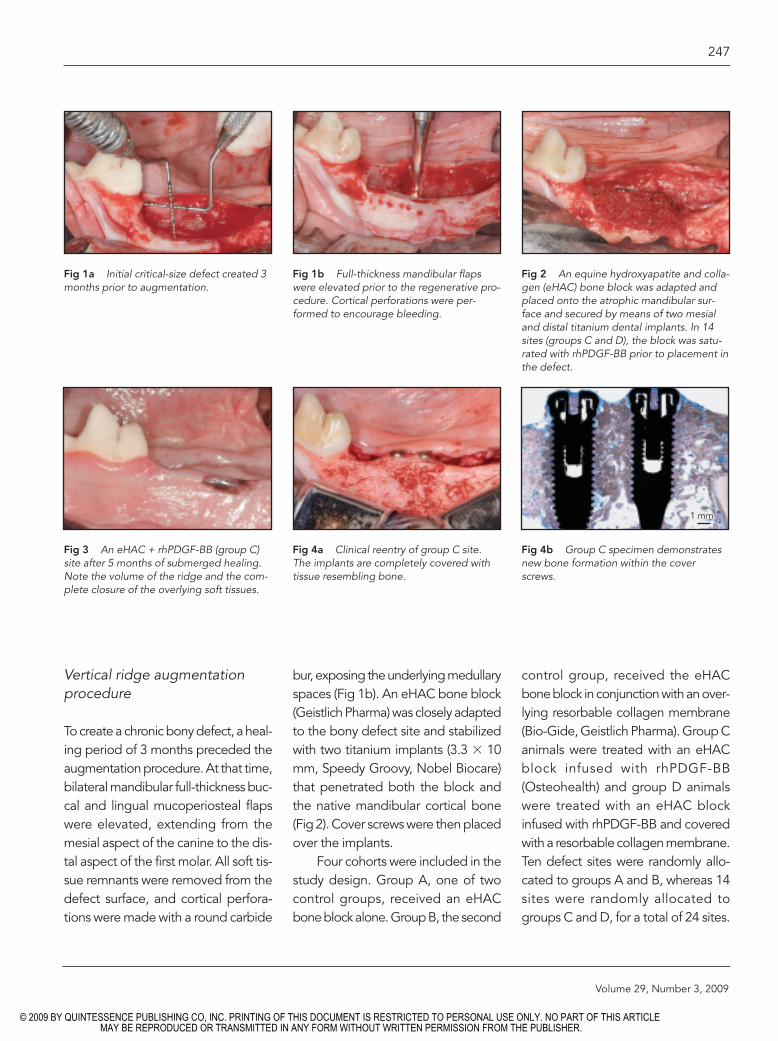
Fig 1a Initial critical-size defect created 3months prior to augmentation.
Fig 1b Full-thickness mandibular flapswere elevated prior to the regenerative pro-cedure. Cortical perforations were per-formed to encourage bleeding.
Fig 2 An equine hydroxyapatite and colla-gen (eHAC) bone block was adapted andplaced onto the atrophic mandibular sur-face and secured by means of two mesialand distal titanium dental implants. In 14sites (groups C and D), the block was satu-rated with rhPDGF-BB prior to placement inthe defect.
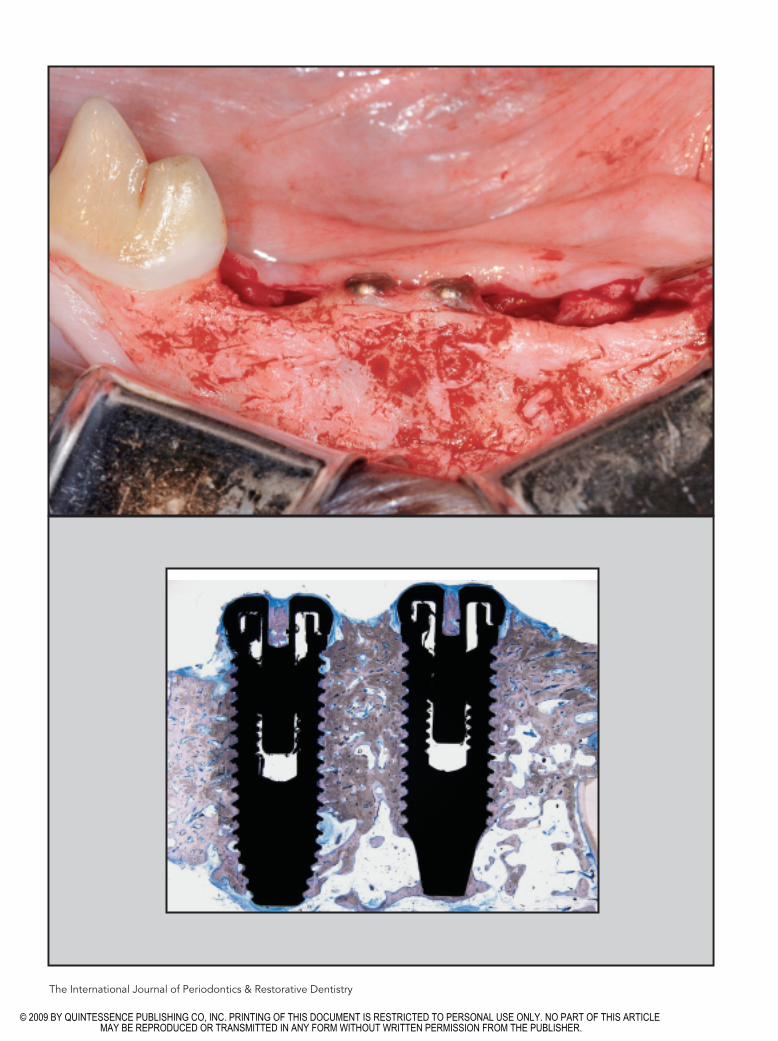
Fig 3 An eHAC + rhPDGF-BB (group C)site after 5 months of submerged healing.Note the volume of the ridge and the com-plete closure of the overlying soft tissues.
Fig 4a Clinical reentry of group C site.The implants are completely covered withtissue resembling bone.
Fig 4b Group C specimen demonstratesnew bone formation within the coverscrews.
1 mm
244_Simion.qxd 4/7/09 10:06 AM Page 247
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The eHAC bone block used ingroups C and D was inserted into anempty sterile syringe and infused underpressure with rhPDGF-BB (three units)for 5 minutes. In all surgical sites, ten-sion-free primary soft tissue closure wasachieved by means of periosteal releas-ing incisions, followed by horizontalmattress and interrupted sutures.Periapical radiographs were obtainedprior to and immediately followingsurgery. Antimicrobial prophylaxis con-sisted of spiramycin 750,000 IU and
metronidazole (125 mg, 1 tablet/10 kgper day per os) beginning at least 5days before and continuing for at least14 days after surgery (Stomorgyl,Merial). Oral hygiene was maintainedwith chlorhexidine digluconate wipesthree times a week for 2 weeks. Sutureswere removed after a healing period of15 days. Following a healing period of5 months after grafting, periapical radi-ographs were obtained and the ani-mals were then killed.
Histologic processing
Block sections were dissected free,fixed in 10% neutral buffered forma-lin, dehydrated, and processed forlight microscopy without demineral-ization. The blocks were embedded inKulzer Technovit 7200 VLC resin andsliced with an Exakt cutting unit. Theslices were reduced using an Exaktgrinding unit to an even thickness of30 to 40 µm and stained with toluidineblue/ pyronine G and examined with
248
The International Journal of Periodontics & Restorative Dentistry
Fig 5 Representative periapical radio-graphs of each of the four groups prior tosacrifice. Groups A (top left) and B (topright) exhibit no evidence of increasedradiopacity. (middle) Group C samples showsignificant increased radiopacity and suggestgood integration of newly formed bone withpre-existing bone. (bottom) Except for onespecimen, group D samples showed littlenew radiopacity coronal to the underlyingbasal bone.
244_Simion.qxd 4/7/09 10:06 AM Page 248
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

a Leica DM6000B light microscope.Ground sections were prepared in amesiodistal direction.
Results
Clinical observations
Healing proceeded uneventfully for all24 surgical sites during the 3 monthsfollowing creation of the mandibulardefects. The mandibular alveolarridges appeared flat with no-walldefects, simulating localized atrophicposterior mandibles.
The 5-month postgrafting healingphase was uneventful for 13 of the 24sites, with four sites exhibiting smallsoft tissue fistulae and six sites exhibit-ing soft tissue dehiscences. One site ingroup A (eHAC block alone) lost theimplanted block and the associatedimplants. Four of the six soft tissuedehiscences occurred in sites thatreceived the block with or without themembrane but without the rhPDGF-BB(groups A and B). Hence, an unevent-ful clinical healing rate of 85.7% wasseen in sites treated with rhPDGF-BB,
defect surface. In one group D speci-men, increased radiopacity extendedcoronally to the level of the coverscrews, indicating significant new boneregeneration (Fig 5).
Histologic observations
Group A (eHAC block)Sites grafted with the eHAC blockalone demonstrated little to no boneregeneration coronal to the native basalbone (Fig 6). Abundant amounts ofunresorbed HA particles were embed-ded in healthy connective tissue thatwas devoid of inflammation. An intactepithelium covered the grafted areas.
Group B (eHAC block + membrane)Group B sites demonstrated histologicfindings similar to those seen in groupA. Little to no bone regeneration wasevident coronal to the apical nativebone. Healthy, inflammation-free con-nective tissue surrounded theimplants. As in group A, unresorbedmatrix material was seen throughoutthe specimens (Fig 7).
compared to 50% in sites that did notreceive the growth factor.
Surgical reentry of one of thegroup C sites (eHAC block + rhPDGF-BB) revealed implants that were com-pletely covered with bonelike tissue(Figs 3 and 4).
Radiographic observations
All ten sites in groups A (eHAC blockalone) and B (eHAC block + mem-brane), which did not receive rhPDGF,demonstrated no evidence of addi-tional radiopacity superior to thegrafted defect surface, indicating nonew bone formation (Fig 5). Group Csites (eHAC block + rhPDGF-BB)exhibited radiographic evidence ofnew bone regeneration, with a numberof implants completely embedded inbone. Radiographically, the newlyregenerated bone appeared well inte-grated with both the underlying basalbone and the grafted eHAC block. Inall but one specimen, group D (eHACblock + rhPDGF-BB + membrane) sitesdemonstrated little to no increasedradiopacity coronal to the grafted
249
Volume 29, Number 3, 2009
Fig 6 (left) Group A specimen (eHACblock alone) in a coronal ground sectiondemonstrates abundant amounts of con-nective tissue with no evidence of boneregeneration. Intact matrix material remainsevident (magnification �8).
Fig 7 (right) Group B specimen (eHACblock + membrane) demonstrates theimplant embedded in connective tissuewith no evidence of vertical bone regenera-tion. Unresorbed matrix material is seenthroughout the section (magnification �8).
1 mm1 mm
244_Simion.qxd 4/7/09 10:06 AM Page 249
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Group C (eHAC block + rhPDGF-BB)Five of seven group C sites demon-strated histologic evidence of newbone formation. Complete boneregeneration up to the implant coverscrews was evident in three of the fivesites that exhibited new bone forma-tion (Fig 4). Dense, well-vascularizedbone was seen surrounding the entirebody of the implant in a typical exam-ple within this cohort (Fig 8). Of par-ticular importance was the amount ofbone-to-implant contact seen histo-logically. Indeed, the density of theregenerated bone exceeded that seenin the apical native bone. Additionally,
few if any residual matrix particles werefound within the grafted area, whichwas almost completely replaced bynewly formed bone. Interestingly, inone of the specimens, new bone hadformed within the cover screws them-selves (Fig 9).
High-power magnification pro-vided further insight into the intensepro-osteogenic and angiogenic effectsmediated by rhPDGF-BB. In Fig 10,intense osteogenic activity can be seenat the advancing margin of new boneformation, mediated by chemotacti-cally recruited osteoblasts. Activeremodeling and resorption of eHACmatrix particles by multinucleated
giant cells was noted throughout therhPDGF-BB–grafted sites but waslargely missing in sites where thegrowth factor was excluded (Fig 11).Importantly, intimate, seamless inte-gration occurred between well-formednewly regenerated bone and theunderlying native bone (Fig 12).Osseointegration occurred betweennewly formed bone and the implantthreads, allowing for high bone-to-implant contact (Fig 13). Finally, theoccasional residual eHAC matrix par-ticle seen under high magnificationlikewise showed intimate, seamlessintegration with the surrounding newlyregenerated bone (Fig 14).
250
The International Journal of Periodontics & Restorative Dentistry
Fig 8 Group C test specimen (eHAC block + rhPDGF-BB)exhibits new bone formation up to the implant cover screw.Dense, well-vascularized bone surrounds the entire implant. Few,if any, residual matrix particles remain at 5 months postgrafting(magnification �8).
Fig 9 Group C specimen demonstrates new bone formation with-in the cover screws.
1mm 1mm
244_Simion.qxd 4/7/09 10:06 AM Page 250
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

251
Volume 29, Number 3, 2009
Fig 11 Light microscopic view (group Cspecimen) of ongoing resorption phenome-na in eHAC particle areas. Note the pres-ence of multinucleated giant cells formingresorption seams, as well as osteoclasticactivity resulting in osteoclastic lacunae(ground section, toluidine blue).
Fig 12 (above) Light microscopic view (group C specimen) of theborder (arrows) between native bone and newly formed bone in aneHAC specimen with rhPDGF-BB without membrane. Note thehigh remodeling activity in newly formed bone (ground section,toluidine blue).
Fig 13 (above right) Light microscopic view (group C specimen)of the osseointegration of the implant by newly formed wovenbone (NB) formation in an eHAC specimen with rhPDGF-BB with-out membrane. Note the high remodeling activity in woven bone(ground section, toluidine blue).
eHACCT
Osteoid
Osteoblasts
NB
eHAC
eHAC
Resorption
Resorption
Resorption
Osteoclastlacunae
Multinucleatedcells
200 µm
Native bone
New bone
Fig 14 Light microscopic view (group Cspecimen) of residues of the eHAC blockembedded in newly formed bone. Note thehigh remodeling activity in newly formedbone (ground section, toluidine blue).
eHAC
eHAC
Fig 10 Light microscopic view (group Cspecimen) of ongoing bone formation inareas previously occupied by eHAC matrixparticles. Note new bone formation and theseam of osteoid lined with osteoblasts(ground section, toluidine blue). NB = newbone; CT = connective tissue.
100 µm 50 µm
200 µm
100 µm
244_Simion.qxd 4/7/09 10:06 AM Page 251
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
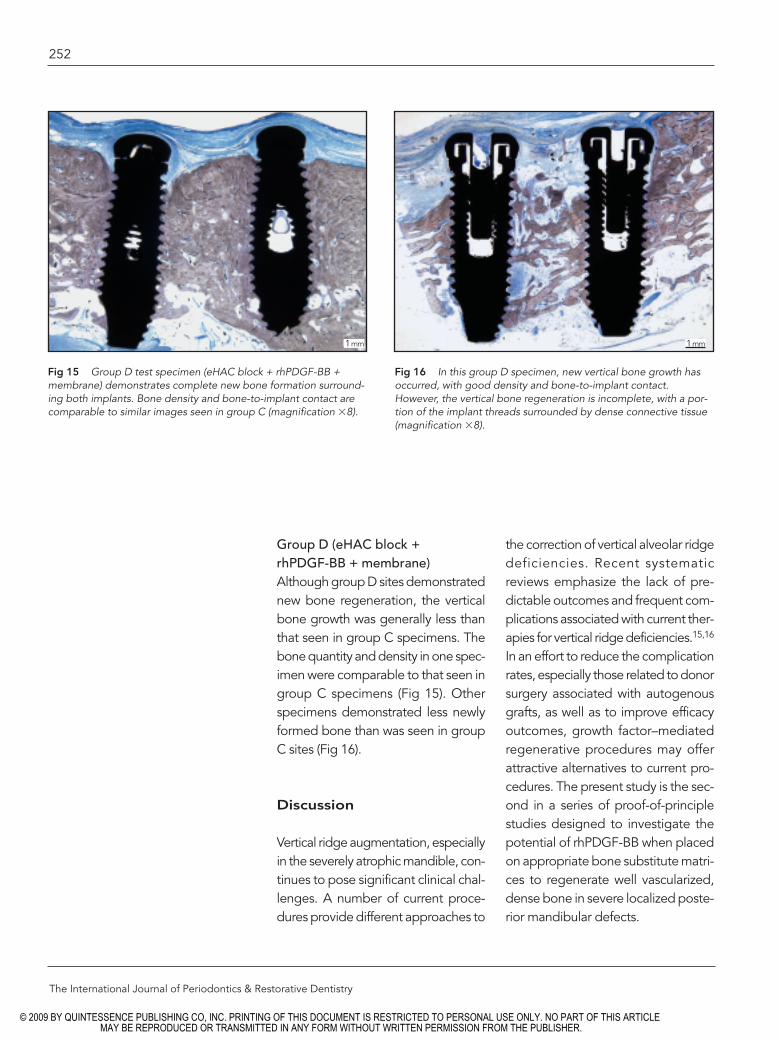
Group D (eHAC block + rhPDGF-BB + membrane)Although group D sites demonstratednew bone regeneration, the verticalbone growth was generally less thanthat seen in group C specimens. Thebone quantity and density in one spec-imen were comparable to that seen ingroup C specimens (Fig 15). Otherspecimens demonstrated less newlyformed bone than was seen in groupC sites (Fig 16).
Discussion
Vertical ridge augmentation, especiallyin the severely atrophic mandible, con-tinues to pose significant clinical chal-lenges. A number of current proce-dures provide different approaches to
the correction of vertical alveolar ridgedeficiencies. Recent systematicreviews emphasize the lack of pre-dictable outcomes and frequent com-plications associated with current ther-apies for vertical ridge deficiencies.15,16
In an effort to reduce the complicationrates, especially those related to donorsurgery associated with autogenousgrafts, as well as to improve efficacyoutcomes, growth factor–mediatedregenerative procedures may offerattractive alternatives to current pro-cedures. The present study is the sec-ond in a series of proof-of-principlestudies designed to investigate thepotential of rhPDGF-BB when placedon appropriate bone substitute matri-ces to regenerate well vascularized,dense bone in severe localized poste-rior mandibular defects.
252
The International Journal of Periodontics & Restorative Dentistry
Fig 15 Group D test specimen (eHAC block + rhPDGF-BB +membrane) demonstrates complete new bone formation surround-ing both implants. Bone density and bone-to-implant contact arecomparable to similar images seen in group C (magnification �8).
Fig 16 In this group D specimen, new vertical bone growth hasoccurred, with good density and bone-to-implant contact.However, the vertical bone regeneration is incomplete, with a por-tion of the implant threads surrounded by dense connective tissue(magnification �8).
1mm 1mm
244_Simion.qxd 4/7/09 10:06 AM Page 252
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

As in the first study in the currentseries,12 critical-size defects were cre-ated to simulate the highly resorbedposterior alveolar ridges that are fre-quently seen in human mandibles. Toreplicate a chronic bone defect, a 3-month waiting period was chosenbetween the time of defect creationand the bone augmentation proce-dure. Unlike the earlier study, an addi-tional control cohort, ie, bone substi-tute block graft alone, was added tothis investigation to provide a parallelcomparison to test group C (block +rhPDGF-BB).
In addition to the extra controlgroup, a different bone substitutematrix was used in the current study.14
In the earlier study, a brittle cancellousdeproteinized bovine block (Bio-Osscancellous block, Osteohealth),designed for indications other thanmandibular vertical ridge augmenta-tion, was prone to fracture duringimplant insertion. In addition, theblock’s friability made proper shapingdifficult.12 In the current investigation,a new equine HA and collagen boneblock (eHAC) appeared to be moremalleable, less prone to fracture, andeasier to trim, and it had diminishedsharp angles and was more readilyadapted to the shape of the nativemandibular basal bone defect. Fewerdehiscences occurred in this secondinvestigation, perhaps as a result ofthe fact that this more malleable blockmaterial exerted less pressure on thecoronally repositioned soft tissues, withfewer sharp angles and corners.
The clinical and histologic resultsof the current investigation parallelthose seen in the prior study in thisseries. In both studies, control groups,
with or without barrier membranes andwithout the addition of rhPDGF-BB,failed to produce new vertical bonegrowth. In all instances, inflammation-free connective tissue surrounded theimplant bodies, with little evidence ofsurrounding new bone regeneration.In addition, although the matriceswere different in each investigation,matrix particles persisted in all controlgroups, showing little tendencytoward remodeling during the timeframes of each study.
Similar, although not identical,results were seen in the test groups ofthe current investigation when com-pared to the earlier study. Vertical boneregeneration was clearly more pre-dictable and consistent when rhPDGF-BB was added to each block matrixwithout the imposition of a barriermembrane. In the current study, five ofseven sites in group C (eHAC +rhPDGF-BB) exhibited vertical bonegrowth, with three sites showing com-plete bone regeneration up to theimplant cover screws. In one case, boneregenerated within the cover screws. Inaddition, the regenerated bone wasdense and well-vascularized, withexcellent bone-to-implant contact. Inthose sites where bone regenerationoccurred, the newly formed boneappeared denser than the native apicalbone. As in the prior study, efficientreplacement resorption of the matrixparticles with newly formed boneoccurred when the matrix was satu-rated with rhPDGF-BB. Acceleratedbone graft substitute resorption, withsubsequent replacement with densenew bone, occurred in both groups Cand D in those specimens exhibitingnew bone regeneration.
253
Volume 29, Number 3, 2009
244_Simion.qxd 4/7/09 10:06 AM Page 253
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Finally, both studies continue tohighlight the importance of the perios-teum as a source of progenitor cellsduring bone regenerative proce-dures.17–19 Growth factor–mediatedbone regeneration benefited whenaccess to the periosteum was not pro-hibited by a barrier membrane. Thesuperior regenerative results seen ingroup C without barrier membranesemphasize the importance of allow-ing chemotaxis to osteogenicperiosteal cells.
Conclusion
Vertical ridge augmentation, especiallyin the severely atrophic mandible, con-tinues to pose significant surgical chal-lenges for the clinician. This proof-of-principle study, which combinedrecombinant human platelet-derivedgrowth factor-BB with a novel equinehydroxyapatite and collagen boneblock without the use of a barrier mem-brane, resulted in significant verticalbone regeneration, with dense, well-vascularized bone; high bone-to-implant contact; and acceleratedreplacement of graft particles withnewly formed bone. Five of sevensites in the group that received boneblocks infused with growth factorexhibited substantial bone regenera-tion, with three of the sites showingcomplete vertical restoration of theatrophied mandible. The current studyprovides further evidence of the poten-tial for tissue-engineered solutions inthe management of difficult-to-treatjawbone defects.
Acknowledgment
Special thanks to Dr Stuart Kay, science writerand consultant, Huntington, New York, for hishelp with the organization and production ofthe manuscript.
References
1. Simion M, Trisi P, Piattelli A. Vertical ridgeaugmentation using a membrane tech-nique associated with osseointegratedimplants. Int J Periodontics RestorativeDent 1994;14:496–511.
2. Nyman S. Bone regeneration using theprinciple of guided tissue regeneration.J Clin Periodontol 1991;18:494–498.
3. Scipioni A, Bruschi GB, Calesini G. Theedentulous ridge expansion technique:A five-year study. Int J PeriodonticsRestorative Dent 1994;14:451–459.
4. Froum SJ, Rosenberg ES, Elian N, TarnowD, Cho SC. Distraction osteogenesis forridge augmentation: Prevention and treat-ment of complications. Thirty case reports.Int J Periodontics Restorative Dent 2008;28:337–345.
5. McAllister BS, Haghighat K. Bone aug-mentation techniques. J Periodontol2007;78:377–396.
6. Levin L, Nitzan D, Schwartz-Arad D.Success of dental implants placed in intra-oral block bone grafts. J Periodontol2007;78:18–21.
7. Nyström E, Ahlqvist J, Kahnberg KE,Rosenquist JB. Autogenous onlay bonegrafts fixed with screw implants for thetreatment of severely resorbed maxillae.Radiographic evaluation of preoperativebone dimensions, postoperative boneloss, and changes in soft-tissue profile. IntJ Oral Maxillofac Surg 1996:25:351–359.
8. Jensen OT, Laster Z. Preventing compli-cations arising in alveolar distraction osteo-genesis. J Oral Maxillofac Surg 2002;60:1217–1218.
254
The International Journal of Periodontics & Restorative Dentistry
244_Simion.qxd 4/7/09 10:06 AM Page 254
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
9. Nevins M, Lynch SE, Cappetta EG.Treatment of advanced periodontaldefects using bioactive therapies in tissueengineering. In: Lynch SE, Marx RE, NevinsM, Wisner-Lynch LA (eds). TissueEngineering, ed 2. Chicago: Quintessence,2008:67–86.
10. Hollinger JO, Hart J, Gruber R, Doll B.Protein therapeutics and bone healing intissue engineering. In: Lynch SE, Marx RE,Nevins M, Wisner-Lynch LA (eds). TissueEngineering, ed 2. Chicago: Quintessence,2008:3–25.
11. Nevins ML, Mellonig JT. Site developmentfor implant placement: Regenerative andesthetic techniques in oral plastic surgery.In: Lynch SE, Marx RE, Nevins M, Wisner-Lynch LA (eds). Tissue Engineering, ed 2.Chicago: Quintessence, 2008:119–131.
12. Simion M, Rocchietta I, Kim D, Nevins M,Fiorellini J. Vertical ridge augmentation bymeans of a deproteinized bovine boneblock and recombinant human platelet-derived growth factor-BB: A histologicstudy in a dog model. Int J PeriodonticsRestorative Dent 2006;26:415–423.
13. Simion M, Rocchietta I, Dellavia C. Three-dimensional ridge augmentation withxenograft and recombinant humanplatelet-derived growth factor-BB inhumans: Report of two cases. Int JPeriodontics Restorative Dent 2007;27:109–115.
14. Fontana F, Rocchietta I, Dellavia C, NevinsM, Simion M. Biocompatibility and man-ageability of a new fixable bone graft forthe treatment of localized bone defects.Preliminary study in a dog model. Int JPeriodontics Restorative Dent 2008;28:601–607.
15. Rocchietta I, Fontana F, Simion M. Clinicaloutcomes of vertical bone augmentationto enable dental implant placement: A sys-tematic review. J Clin Periodontol 2008;35(8 suppl):203–215.
16. Tonetti MS, Hämmerle CH, EuropeanWorkshop on Periodontology Group C.Advances in bone augmentation to enabledental implant placement: ConsensusReport of the Sixth European Workshop onPeriodontology. J Clin Periodontol2008;35(8 suppl):168–172.
17. Shimizu T, Sasano Y, Nakajo S, KagayamaM, Shimauchi H. Osteoblastic differentia-tion of periosteum-derived cells is pro-moted by the physical contact with thebone matrix in vivo. Anat Rec 2001;264:72–81.
18. Park BW, Hah YS, Kim DR, Kim JR, ByunJH. Osteogenic phenotypes and mineral-ization of cultured human periosteal-derived cells. Arch Oral Biol 2007;52:983–989.
19. Hayashi O, Katsube Y, Hirose M, OhgushiH, Ito H. Comparison of osteogenic abili-ty of rat mesenchymal stem cells frombone marrow, periosteum, and adiposetissue. Calcif Tissue Int 2008;82:238–247.
255
Volume 29, Number 3, 2009
244_Simion.qxd 4/7/09 10:06 AM Page 255
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.