2.4.3.1terminology - epubs.surrey.ac.ukepubs.surrey.ac.uk/808709/1/final correction july...
TRANSCRIPT

An ethnographic study exploring the
over-representation of black and minority
ethnic (BME) employees in the disciplinary
process in a National Health Service
(NHS) Trust
by
HarjinderSehmi
A thesis submitted for Doctorate in Clinical Practice
PART ONE
Faculty of Health and Medical Sciences
Division of Health and Social Care
University of Surrey
May 2014
© HarjinderSehmi 2015

Statement of originality
This thesis and its research content are the results of my efforts. Any ideas, data, images or
text resulting from the work of others (whether published or unpublished) are fully identified
as such within the thesis and attributed to their originator in the references. This thesis has
not been submitted in whole or in part for any other academic degree or professional
qualification.
HarjinderSehmi
2 February 2015
1

Contents
Statement of originality.............................................................................................1
Content ......................................................................................................................2
Abstract......................................................................................................................8
Acknowledgements.................................................................................................10
Acronyms.................................................................................................................11
Chapter 1: Introduction........................................................................................141.1 Introduction..............................................................................................................141.2 The NHS....................................................................................................................14
1.2.1 BME employees...................................................................................................151.2.2 Disciplinaries........................................................................................................17
1.3 Overview of the study..............................................................................................181.3.1 Literature review..................................................................................................181.3.2 Methodology........................................................................................................181.3.3 Findings...............................................................................................................181.3.4 Discussion...........................................................................................................18
1.4 Summary...................................................................................................................19
Chapter 2: Literature review.................................................................................202.1 Introduction..............................................................................................................202.2 Accessing the literature...........................................................................................202.3 Search strategy........................................................................................................20
2.3.1 Database searching.............................................................................................212.4 Results from the literature search..........................................................................21
2.4.1 Disciplinaries outside the NHS............................................................................222.4.2 Poor performance, suspensions and disciplinaries in the NHS...........................252.4.3 Presentation of BME staff....................................................................................31
2.4.3.1 Terminology...............................................................................................................322.4.3.2 ‘Black and black’........................................................................................................352.4.3.3 ‘Saviours’, ‘exploited’ and ‘exploiters’?......................................................................362.4.3.4 Overseas staff...........................................................................................................372.4.3.5 Perceptions of behaviours and attitudes of BME staff...............................................38
2.4.4 Organisation and management culture of the NHS.............................................402.4.5 E&D agenda........................................................................................................48
2.5 Summary of literature review..................................................................................522.6 Gaps..........................................................................................................................532.7 Formulation of the research question....................................................................54
Chapter 3: Methodology.......................................................................................543.1 Introduction..............................................................................................................54
Figure 1: Study process and data collection methods.....................................................553.2 Qualitative approach................................................................................................56
2

3.3 Research site............................................................................................................573.3.1 Negotiating and gaining access to the Trust.......................................................58
3.4 Ethnography as a methodology.............................................................................623.4.1 Rationale for using ethnography..........................................................................633.4.2 Characteristics of ethnography............................................................................643.4.3 Focused ethnography..........................................................................................643.4.4 Critical ethnography.............................................................................................65
3.5 Core concepts from ethnography..........................................................................663.5.1 Culture.................................................................................................................66
3.6 Methodology.............................................................................................................673.6.1 Fieldwork.............................................................................................................683.6.2 Emic and etic perspectives..................................................................................693.6.3 Secondary data....................................................................................................693.6.4 Participant observation........................................................................................733.6.5 Interviewing..........................................................................................................75
3.6.5.1 Semi-structured interviews........................................................................................763.7 Selection, recruitment and undertaking interviews with participants...................77
3.7.1 Selection – inclusion and exclusion.....................................................................773.7.2 Recruitment.........................................................................................................783.7.3 Special measures taken for employees who had been investigated...................783.7.4 Undertaking interviews........................................................................................793.7.5 Outcomes from the interviews.............................................................................79
3.8 Data recording..........................................................................................................803.8.1 Field notes...........................................................................................................803.8.2 Digital audio recording.........................................................................................813.8.3 Fieldwork journal/diary.........................................................................................82
3.9 Data analysis............................................................................................................823.9.1 Thematic analysis................................................................................................833.9.1.1 Presentation of findings from data collected................................................................... 82
3.10 Triangulation...........................................................................................................853.11 Ethics.......................................................................................................................863.12 Reflexivity...............................................................................................................883.13 Summary.................................................................................................................91
Chapter 4: Descriptive statistics..........................................................................934.1 Ethnic profile of the population the Trust serves.................................................934.2 Workforce profile......................................................................................................94
4.2.1 2011 profile..........................................................................................................954.2.2 2012 profile........................................................................................................100
4.3 Disciplinaries..........................................................................................................1044.3.1 Reasons for disciplinary action..........................................................................108
4.4 Conclusion..............................................................................................................108
Chapter 5: Observation of a disciplinary hearing and interviews with three employees involved in the case...........................................................................110
5.1 Introduction............................................................................................................1105.2 Observation of a disciplinary hearing..................................................................110
3
5.2.1 Disciplinary hearing...........................................................................................1105.2.1.1 Employee under investigation.................................................................................1115.2.1.2 Clinical team and environment................................................................................1135.2.1.3 Outcome of the hearing...........................................................................................113
5.3 Interviews................................................................................................................1145.3.1 Interview with Sam, the witness........................................................................114
5.3.1.1 Uncovering poor clinical practice in the team..........................................................1155.3.1.1.1 Poor clinical practice and conduct....................................................................1155.3.1.1.2 Managers ‘turning a blind eye’..........................................................................1155.3.1.1.3 Déjà vu.............................................................................................................1165.3.1.1.4 Collective responsibility....................................................................................116
5.3.1.2 Managing a poor-functioning clinical team..............................................................1175.3.1.2.1 Why had previous managers not stayed?........................................................1175.3.1.2.2 Ethnic composition of the team.........................................................................1175.3.1.2.3 Joyce returning to the team..............................................................................1175.3.1.2.4 Poor uptake of clinical supervision...................................................................1175.3.1.2.5 Sam’s perceptions of how the team viewed him...............................................118
5.3.1.3 Impact of dealing with poor conduct and practice on Sam......................................1185.3.1.3.1 Professional and personal toll...........................................................................1185.3.1.3.2 Support to manage the clinical team................................................................119
5.3.1.4 Patient group treated...............................................................................................1195.3.2 Interview with Paul, the chairperson..................................................................120
5.3.2.1 Uncertain future of the Trust....................................................................................1205.3.2.2 Unveiling poor conduct and practice leading to disciplinary action..........................121
5.3.2.2.1 Ethnicity is not an issue....................................................................................1225.3.2.2.2 Grievance taken out.........................................................................................1225.3.2.2.3 Managing the consequences from disciplinaries..............................................1235.3.2.2.4 Inconspicuous discussions on disciplinaries.....................................................123
5.3.2.3 Quality of staff supervision and support...................................................................1235.3.2.3.1 Lack of meaning of appraisals..........................................................................1245.3.2.3.2 Lack of supervision and support as mitigating circumstances..........................124
5.3.2.4 Undertaking the role of chair...................................................................................1255.3.2.4.1 Consequences of lack of training in making decisions on the outcome............1255.3.2.4.2 Maintaining impartiality and fairness.................................................................1265.3.2.4.3 Maintaining impartiality and transparency........................................................126
5.3.3 Interview with Monica, the BME HR manager...................................................1265.3.3.1 Disaggregation and reconfiguration of services.......................................................127
5.3.3.1.1 Impact on clinical staff......................................................................................1275.3.3.1.2 Changes in team managers..............................................................................1285.3.3.1.3 Why do some areas in the Trust have less disciplinaries than others?............128
5.3.3.2 Training and experience of the chair.......................................................................1285.3.3.2.1 Absence of E&D training..................................................................................1295.3.3.2.2 Perceptions of the chair of the panel................................................................1295.3.3.2.3 Quality of decision-making...............................................................................129
5.3.3.3 Consequences of increased administration.............................................................1305.3.3.3.1 Withdrawal of administrative support................................................................1305.3.3.3.2 Loss of strategic planning to minimise disciplinaries........................................1305.3.3.3.3 Lack of preparatory work with managers..........................................................1315.3.3.3.4 Lack of preparatory work with staff under investigation....................................131
4

5.3.3.3.5 Lack of preparatory work to reintegrate the employee into the team................1315.3.3.4 Maintaining impartiality and adhering to the facts of the case.................................132
5.3.3.4.1 Observations of IOs presenting their case........................................................1325.3.3.5 Key themes emerging from disciplinaries................................................................133
5.3.3.5.1 Disparity between outcomes for white and BME staff.......................................1335.3.3.5.2 Difference in articulation...................................................................................1345.3.3.5.3 Disproportional representation of BME staff in the disciplinary process...........1345.3.3.5.4 Perceptions of the HR department...................................................................135
5.4 Summary.................................................................................................................135
Chapter 6: Findings from participant observations and interviews with employees involved in the disciplinary process in the Trust............................136
6.1 Introduction............................................................................................................1366.2 The context of the Trust........................................................................................137
6.2.1 The pressure to secure Foundation Trust (FT) status.......................................1376.2.2 Reconfiguration of services...............................................................................1376.2.3 Recruitment of BME staff...................................................................................1416.2.4 Perceptions of the Trust E&D initiatives............................................................1426.2.5 Perceptions towards the study..........................................................................1446.2.6 Observations of behaviours...............................................................................147
6.3 Perceptions of BME employees in the Trust.......................................................1476.3.1 Links to the historical, societal, political and personal context..........................1476.3.2 Senior managers perception of BME employees particularly black African nurses
...........................................................................................................................1516.3.3 Senior managers perceptions of relationships and tension within BME employees
1536.3.4 Perceptions of BME staff commitment and lack of trust placed on them..........1546.3.5 Perceptions of BME employees treated unfairly................................................1576.3.6 Playing the ‘race card’.......................................................................................1596.3.7 Perceptions of cultural differences in working practices....................................159
6.4 Perceptions of the disciplinary process..............................................................1626.4.1 Perceptions of managers dealing with BME staff..............................................1626.4.2 Underuse of capability procedures....................................................................1656.4.3 Suspension of staff............................................................................................1666.4.4 Perceptions around the descriptive statistics....................................................1686.4.5 Perceptions of the phenomenon investigated...................................................170
6.5 Perceptions of employees directly involved in the disciplinary process.........1706.5.1 Role of an IO......................................................................................................1716.5.2 Lack of training to undertake the role of chair...................................................1726.5.3 Diminished administrative support.....................................................................1736.5.4 Conducting investigations..................................................................................1736.5.5 Relationships between the investigating team and investigated employees.....1776.5.6 The disciplinary panel........................................................................................1786.5.7 Role of the professional lead.............................................................................1806.5.8 Perceptions of TU representation......................................................................1826.5.9 The employee under investigation.....................................................................1846.5.10 Mitigating circumstances.................................................................................185
5

6.5.11 Reactions to disciplinary outcomes.................................................................1886.6 Conclusion..............................................................................................................191
Table 1: Summary of the key themes............................................................................192
Chapter 7: Discussion...........................................................................................1937.1 Introduction............................................................................................................1937.2 Discussions of the findings..................................................................................1907.3 The Trust.................................................................................................................191
7.3.1 Leadership in the Trust......................................................................................1917.3.2 The impact of disaggregation and reconfiguration on services and staff..........1937.3.3 Management in the Trust..................................................................................1957.3.4 Changes to organisation culture.......................................................................1977.3.5 Patient care........................................................................................................1987.3.6 Breakdown in staff supportive structures...........................................................200
7.4 BME employees in the Trust.................................................................................2017.4.1 Recruitment of BME staff...................................................................................2027.4.2 Socialisation and working practices of BME staff..............................................2037.4.3 BME staff treated with suspicion and distrust....................................................2057.4.4 Impact on BME staff..........................................................................................2077.4.5 The 'Black African'.............................................................................................2087.4.6 Discrimination and racism within and between employees...............................209
7.5 Disciplinaries in the Trust.....................................................................................2107.5.1 Descriptive statistical data on disciplinaries......................................................2117.5.2 The wider context: outside the NHS..................................................................2137.5.3 Capability procedures........................................................................................2137.5.4 Reactions to the phenomenon investigated......................................................2147.5.5 Equality and diversity.........................................................................................2167.5.6 Disciplinary hearings and investigations............................................................2177.5.7 Disciplinary outcomes........................................................................................221
7.6 Summary.................................................................................................................224
Chapter 8: Conclusion..........................................................................................2218.1 Introduction............................................................................................................2258.2 How does this study advance research in the field?..........................................225
8.2.1 Implications of this study for policy and clinical practice....................................2278.3 Study limitations....................................................................................................2308.4 Dissemination of the findings...............................................................................2338.5 Summary.................................................................................................................234
References.............................................................................................................236
Appendices............................................................................................................254Appendix 1: The disciplinary procedures examined in this study.............................256Appendix 2: Recruitment letters....................................................................................259Appendix 3: Participant information sheets.................................................................261Appendix 4: Consent forms...........................................................................................273
Chapter 9: Overview of the integration of knowledge, research and practice.2779.1 Introduction............................................................................................................277
6

9.2 Development of self...............................................................................................2779.3 Advanced research methods................................................................................2789.4 Service evaluation..................................................................................................2799.5 Leadership in healthcare organisation................................................................2809.6 Emotional intelligence...........................................................................................2809.7 Policy, politics and power.....................................................................................2819.8 Dissemination of the findings...............................................................................2829.9 Conclusion..............................................................................................................283
Chapter 10: Research log.....................................................................................28410.1 Introduction..........................................................................................................28410.2 Why I took a taught clinical doctorate programme and not a PhD route?.....28410.3 Selecting the subject to investigate...................................................................28510.4 Framework, tools and skills needed to undertake the study...........................285
10.4.1 Gaining access to a Trust................................................................................28710.5 Research process................................................................................................28810.6 Academic supervisors.........................................................................................29010.7 Peer support.........................................................................................................29010.8 Conclusion............................................................................................................291
7

Abstract
Aim: This study was undertaken to explore the over-representation of black and minority ethnic (BME) staff in the disciplinary process in a National Health Service (NHS) Mental Health Trust.
Background: The Trust where this study was undertaken recognised there was a disproportional representation of BME staff involved in the disciplinary process. No reasons were given by the Trust for why this phenomenon existed. The over-representation of individuals from BME groups in NHS disciplinary hearings was raised as a topic for investigation by Parliament in 2008. Seminal work by Archibong and Darr (2010) has explored reasons for this over-representation. Ethnographic methodologies have not been used previously to develop our understanding of this area.
Methods: Critical and focused ethnography were used to observe a disciplinary hearing and gain the perspectives of employees directly involved in the disciplinary process in a single trust. To examine the culture of the Trust, data were collected through fieldwork, participant observation, semi-structured interviews, journal/diary and secondary data. Thematic analysis devised by Braun and Clarke (2006) was used to analyse the data collected.
Findings: Negative perceptions towards BME staff, particularly ‘black African’ nurses and healthcare assistants were uncovered. Tensions and rivalries within and between BME staff were also found.
Disciplinary investigations were not always based on facts and not all the findings were presented. Investigating officers and the chair of the panel were not always given training to undertake their roles. In some cases, BME personnel were intentionally selected onto the disciplinary panel to avoid accusations of racism, particularly when BME employees were likely to be dismissed. Disparity of the sanctions imposed for similar cases were reported. There was a perception that BME staff were not articulate and treated more harshly than their white counterparts. Equality and diversity initiatives also remain on the periphery.
The disaggregation and reconfiguration of services had some bearing on the performance of staff. Line management and clinical supervision was underutilised. Some managers who confronted BME employees were accused of ‘racism’ and had grievances taken out against them.
Conclusion: Disciplinary processes involving BME staff cannot be discussed in isolation. Key factors, such as the impact of disaggregation and the reconfiguration of the Trust at a time of continuous change in the NHS, the employment of BME staff as well as the disciplinary process itself, need to be considered together. The discussion also needs to shift from the polarised division between ‘black and white’ staff and focus on the differences and tensions within and among BME staff.
8

Acknowledgements
First and foremost, I thank the Trust, which allowed me to undertake this study, and
all the participants who have contributed. I am grateful for the support given to me by
my supervisors, Professor Helen Cowie and Dr Debbie Cooke, and thank them for
their comments and guidance. I am also thankful for the support and understanding
from Dr Iris Gault. A special thank you also goes to: Roger Palmer, Satwant Lahoria,
Karen Stobart, Dr Earl Hopper, Dave and John Sandhu. Finally, with heartfelt love I
thank my partner Tracy Knight for being with me throughout this journey. Tracy, I look
forward to reacquainting myself with you and cannot wait to do all those jobs you
have lined up for me.
I dedicate my doctorate to my parents, Surinder Kaur and Ajit Singh Sehmi, whose
spirit lies within me, and my siblings Nani, Shanti, Pam and Vindy.
9

Acronyms
Acas – Advisory, Conciliation and Arbitration Service
AHP – Allied health professional
BAME – Black, Asian and minority ethnic
BME – Black and minority ethnic
CHI – Commission for Health Improvements
CPA – Care Programme Approach
CQC – Care Quality Commission
DoH – Department of Health
DRE – Delivering Race Equality
E&D – Equality and Diversity
FT – Foundation Trust
FtP – Fitness to Practise
GMC – General Medical Council
GP – General practitioner
HCA – Healthcare assistant
HR – Human resources
10

IO – Investigating officer
NAO – National Audit Office
NCAS – National Clinical Assessment Service
NHS – National Health Service
NMC – Nursing and Midwifery Council
NNRU – National Nursing Research Unit
NRES – National Research Ethics Service
PADR – Performance Appraisal Development Review
RCM – Royal College of Midwives
RCN – Royal College of Nursing
R&D – Research and Development
RES – Race Equality Scheme
SSI – Site Specific Information
SUI – Serious Untoward Incident
TU – Trade Union
TUC – Trades Union Congress
UREC – University Research Ethics Committee
11

Chapter 1: Introduction
1.1 Introduction
This chapter provides a brief background about the National Health Service (NHS),
black and minority ethnic (BME) staff and disciplinaries. It also describes the
structural overview for this study.
1.2 The NHS
Funded by the taxpayer, the NHS came into existence on 5 July 1948 (Gorsky,
2008). Since its creation, numerous management and structural reforms have taken
place. These have been in response to dealing with rising costs (as a result of new
medical procedures and drug treatments), an ageing population and greater public
expectations. To meet these demands, competition has been introduced into the
NHS by incorporating the independent and voluntary sector in providing services
(Gorsky, 2008). With limited funding and resources, recent governments have
concentrated on improving efficiency, cost-effectiveness and productivity in order to
meet the needs of service users (Doherty, 2009). High-quality care and standards
are emphasised through meeting performance indicators and clinical outcomes set
by the Department of Health (DoH) (Buchan and Seccombe, 2013).
To undertake the tasks of the NHS, the government relies on staff to deliver its
programme. There is much public sentiment about preserving the values of the NHS,
as observed by politicians from the main political parties. However, since its
inception, Labour and Conservative governments have had problems recruiting NHS
staff (particularly in nursing) from the United Kingdom. Over time, part of the
reluctance of the indigenous population to work in the NHS has been due to the 12
dwindling status, low pay and poor working conditions (Hart, 2004). In addition to
these factors, the stressful nature of the job has also contributed to the attrition of
qualified nurses (Doherty, 2009). To meet the shortfall of nurses and doctors at
various times of depletion and crisis, governments of either political party have relied
on their former colonies.
1.2.1 BME employees
Today the NHS is the biggest UK employer and the principal employer of BME staff
in England (Healy and Oikelome, 2006; Siva, 2009). Since its inception, BME
employees from the indigenous population or abroad have featured as part of the
NHS. However, their experiences and contributions have not always been positive.
For example, from a historical perspective, BME doctors and nurses were recruited
and appointed in less sought-after roles and particular areas of care such as
psychiatry, working with the chronically sick and elderly. Student nurses from the
Commonwealth, particularly the Caribbean, were discriminated against and forced to
undertake pupil nurse training to become state enrolled nurses. Questions were
raised about the motivation, racial characteristics and intellectual capacity of
Caribbean people who wanted to train as state registered nurses (Trant and Usher,
2010).
The experience of discrimination and ill treatment of first-generation nurses from
colonial countries has put off the second generation from following in their footsteps.
Consequently, governments have had to rely and depend on recruiting from abroad.
A mixed reaction prevails. On one side, for the government of the day, overseas
nurses have provided a constant supply of cheap labour to meet the shortage of
staff. Governments have used them to control public sector wage demands. On the
13

other side, overseas and BME employees perceive themselves as being
undervalued, treated unfairly and marginalised.
Governments have introduced legislation and policy initiatives to tackle the disparity
and discrimination around the experiences of BME people. However, huge doubt
remains about the lack of commitment by NHS Trusts and the effectiveness of these
schemes (Ali et al., 2013).
Simpson et al. (2010) stated how the positive contribution of migrants in the history
and shaping of the NHS has been denied. Migrants and BME staff in the NHS have
focused on their lack of opportunities: BME nurses are over-represented at lower
grades and under-represented in senior and leadership positions (Ashraf, 2013);
there is a lack of recognition of the skills and experiences of BME nurses, particularly
those from overseas (Allen and Larsen, 2003); the experience of racism, harassment
and discrimination is widely reported. Some of this behaviour is from patients and
carers. Sprinks (2008) reported that older people were more likely to be racist. Some
patients do not want to be nursed by staff of a particular ethnicity and this is accepted
by some health services (Jönson, 2007); BME applicants shortlisted for jobs are less
likely to be appointed than white applicants (Kline, 2013); qualified overseas nurses
have been appointed as healthcare assistants (HCAs) (Nichols and Campbell, 2010);
BME employees face disciplinary or grievance proceedings more than their white
counterparts (Archibong and Darr, 2010; Archibong et al., 2013); disproportionate
BME registrants have been referred to the Nursing and Midwifery Council (NMC).
Disciplinaries involving BME employees will be looked at more closely in this study.
14

1.2.2 Disciplinaries
When employees have continually been unable to perform their tasks and persistent
issues have arisen and been breached, disciplinary action is legitimate to manage
the situation. Disciplinaries have been used to reinforce standards of performance,
minimise improper conduct and correct employee behaviour. Disciplining staff should
be used as a final option. The aim of discipline is to improve employee conduct, not
to punish and humiliate the employee. Disciplinary issues in the workplace can
usually be resolved informally. However, if unsuccessful, a formal route is taken. The
use and application of disciplinary procedures in the NHS follow a process that is
stipulated in a disciplinary policy for each NHS Trust. For this study, the stages of
disciplinary procedures and the role of employees involved in the process are
identified and discussed in Appendix 1. The process and procedures are there to
reinforce fairness, transparency and the rights of the employee regardless of their
race, colour, ethnicity, sexual orientation and gender. The policy around disciplinary
procedures complies with the Advisory, Conciliation and Arbitration Service (Acas)
Code of Practice on Discipline and Grievance (Acas, 2009).
The work of Beishon et al. (1995), Carter (2000) and Archibong and Darr (2010)
highlighted that BME healthcare professionals are twice as likely to be disciplined in
comparison to their white counterparts in the NHS. This study will explore the
phenomenon of the disproportional representation of BME employees in an NHS
Trust.
15

1.3 Overview of the study
1.3.1 Literature review
Current literature retrieved on the over-representation of BME employees involved in
the disciplinary process will be reviewed in chapter 2. This will provide a context of
the gaps that currently exist and also a rationale for undertaking this study.
1.3.2 Methodology
Ethnography as a qualitative approach has been used for this study. Justification for
this approach and the characteristics of ethnography adopted to meet the aims will
be outlined in chapter 3.
1.3.3 Findings
Descriptive statistics related to disciplinaries from the Trust under investigation will be
introduced in chapter 4. Findings from an observation of a disciplinary hearing, and
interviews with three employees involved in the case, will be presented in chapter 5.
Chapter 6 will pay attention to the findings from interviews with employees involved in
other disciplinary cases in the Trust. A summary of the findings from chapters 4 to 6
will be given in chapter 7.
1.3.4 Discussion
Discussion of the findings will also be presented in chapter 7. These findings will be
discussed and linked to existing literature on the subject being investigated. The
study limitations will also be discussed. Finally, recommendations to inform the
practice around disciplinaries involving BME staff will be provided.
16

1.4 Summary
A brief background and context to the study have been provided in this opening
chapter. An outline of the structure of this thesis has also been given.
17

Chapter 2: Literature review
2.1 Introduction
In this chapter, an overview of the current literature retrieved on the disproportional
representation of BME staff involved in the disciplinary process in the NHS is
reviewed. Five themes are explored. This background information not only provides a
context of the gaps that currently exist but also supports the reasons for undertaking
this study.
2.2 Accessing the literature
University learning resource centres and a medical school library attached to a
teaching hospital were used to, access the computers, healthcare databases,
download articles, photocopy articles from journals and borrow books. To access the
databases, NHS Athens registration was needed and obtained. Further help during
the literature search was obtained from the staff in these settings.
The literature retrieved was sourced from journal articles, reports, government
circulars, conference proceedings, grey literature and references within relevant
articles.
2.3 Search strategy
To limit the number of searches, the literature needed to be in English, UK based and
available as full texts.
2.3.1 Database searching
OvidSP, a specialist search tool was used. In addition to allowing access to Medline,
OvidSP allowed access to Embase, Health Management Information Consortium, 18
Maternity and Infant Care and PsycINFO. Databases on the EBSCOhost search
platform allowed access to AMED and CINAHL.
Other databases accessed were the British Nursing Index and Cochrane. As there
was limited literature available, the librarian helpfully directed me to the Health
Business Elite and Social Care Online databases.
2.4 Results from the literature search
In 2008, the South East Coast BME Network published its Race Equality Service
Review. Although 15% of staff came from BME groups, 25% of BME employees
were involved in the disciplinary process. This concern was raised in the House of
Commons (Hansard, 2008). Lord Darzi, responding for the government, reported that
the NHS Institute for Innovation and Improvement was commissioning a study to
investigate this serious matter.
As a result, a seminal research study looking at The Involvement of Black and
Minority Ethnic Staff in NHS Disciplinary Proceedings was undertaken by Archibong
and Darr (2010). Aspects of this significant study are incorporated into the themes
below. Its limitations are discussed at the end of this chapter, as the gaps identified
have contributed to the title and nature of this research study.
Relevant papers that have been retrieved from the literature search will be reviewed
under five themes. Owing to the complexity of the subject, there will be some content
that will overlap between themes:
2.4.1 Disciplinaries outside the NHS;
2.4.2 Poor performance, suspensions and disciplinaries in the NHS;
19

2.4.3 Presentation of BME staff;
2.4.4 Organisation and management culture of the NHS;
2.4.5 Equality and Diversity (E&D) agenda.
These five themes have been selected as they have been directly and indirectly
conspicuous around the subject related to the disproportional representation of BME
staff involved in the disciplinary process.
2.4.1 Disciplinaries outside the NHS
This section presents the international picture and touches on disciplinaries in
English-speaking westernised countries. It includes disciplinaries in other public and
private organisations, outside the NHS, in the UK.
Although the literature review concentrated on disciplinaries in the UK, international
studies from the USA and Australia were found in the search. These articles present
a mixed depiction of the inclusion of BME nurses in the studies. For example, a study
by the National Council of State Boards of Nursing (2009) found a slightly higher
percentage of African-American, Native American and Hispanic nurses were
disciplined in comparison to the general nurse population. In a study of the incidence
of disciplinary action towards advanced practice registered nurses, Hudspeth (2007)
did not state the race and ethnicity of the nurses. He also excluded race and ethnicity
when examining the discipline of nurse practitioners by boards of nursing in the USA
(Hudspeth, 2009). Pugh (2009) examined the unprofessional conduct of nurses, but
did not mention the ethnicity of the 21 Australian nurses interviewed. Both Hudspeth
and Pugh did not recognise that the race and ethnicity of nurses may influence the
likelihood of receiving disciplinary action. These findings should be considered with 20

caution as a comprehensive literature review in English-speaking westernised
countries is needed. This would determine the scale of BME nurses disciplined in
comparison with their white counterparts internationally.
Using evidence from monitoring carried out under the Race Relations Amendment
Act, 2000, the Trades Union Congress (TUC) report of the Black Workers
Conference (TUC, 2009) stated that black workers continued to be over-represented
in disciplinary action. However, the report did not indicate which sectors were
monitored. It is unclear if this disproportional representation is in the private and/or
public sector.
Archibong and Darr (2010) undertook a literature review to compare the disciplinaries
of BME staff in the NHS to those in other public sector organisations. In their study,
they examined the disciplinary process involving BME staff in the police service,
Transport for London, local government, central government and higher education.
Their findings for the police service and local government are similar to the
experience of BME employees in the NHS: managers quickly formalise the
disciplinary process; discriminatory attitudes prevail; ambiguity around disciplinary
policies exists; staff lack training. Harrow Council reported BME employees were
disproportionally affected by its disciplinary procedures at investigation/hearing
stages and by the sanctions imposed (Harrow Council Consultative Forum, 2007). In
terms of monitoring disciplinary proceedings, only a quarter of higher education
institutions observe this practice (Archibong et al., 2013). In its literature review into
the experiences of BME staff working in higher education, the Equality Challenge
Unit (2009) reported disproportionate levels of scrutiny of BME staff in comparison
with their white counterparts. Using data from the Home Office (2008), Archibong and
21
Darr (2010) also showed the Home Office was not analysing data on disciplinaries to
the optimal level.
Other studies have also examined the police force. Smith et al. (2012) found: Asian
police officers in the West Midlands police force were twice as likely to be subjected
to misconduct investigation as white officers; black police officers and staff with
Greater Manchester police were more than two times likely to be investigated for
misconduct than their white counterparts. Hagger Johnson et al. (2013) found ethnic
disproportionality in internal misconduct proceedings in the West Midlands police
force, Greater Manchester police force and the British Transport police.
Solicitors have also been investigated. Building on the work of Ousely (2008) and
Kandola (2010), John (2014) reported disproportional regulatory outcomes for BME
solicitors. John’s (2014) study revealed BME solicitors were subjected to severe
sanctions in comparison to white solicitors.
These studies show that disproportional representation of BME employees involved
in the disciplinary process is also found outside the NHS. Archibong and Darr (2010)
identified benchmarks and began to make comparisons between the NHS and
bodies outside the NHS. The rest of this study will now focus on disciplinaries in the
NHS.
2.4.2 Poor performance, suspensions and disciplinaries in the NHS
Analysing data obtained from NHS Trusts on disciplinaries, Archibong and Darr
(2010) found BME employees were almost twice as likely to be disciplined as their
white counterparts. They also found BME staff over-represented in the disciplinary
process were mainly employed in primary care, mental health and learning
22

disabilities. The scale of the problem and the number of staff disciplined nationally
are unclear as the data recorded by NHS Trusts is inconsistent (Archibong and Darr,
2010) and there is no centralised body collecting this information (Traynor et al.,
2013).
King and Wilcox (2003) and Archibong and Darr (2010) acknowledged the reasons
given for disciplinary action being necessary. An undisciplined workforce can impact
on low morale and poor levels of outcomes (King and Wilcox, 2003). Consequently
managers take disciplinary action (usually as a last resort) to change and correct the
behaviour and attitude of the individual not performing to the expected professional
standards. However, some managers do not use disciplinary measures as the last
resort (Archibong and Darr, 2010; Cooke, 2006a). After examining formal disciplinary
records and interviewing management and trade union (TU) officials, King and
Wilcox (2003) highlighted the difficulty managers have with the task of imposing
disciplinary action. This is as a result of: disciplinary guidelines and policies being
unclear; managers lacking skills and fearing the reaction from the person being
disciplined; the manager imposing the disciplinary action not receiving support from
their own manager; some inexperienced managers ignoring the issue and only
reacting when there is no choice after the issue has escalated to a crisis situation.
King and Wilcox’s (2003) study did not look at specific groups of the workforce and
was oriented towards employee-proposed discipline.
Archibong and Darr (2010) showed that line managers found it difficult to manage
disciplinary issues, and disciplinary policies were inconsistently applied. Managers
also lacked confidence in instigating informal strategies of the disciplinary process
with BME staff. It was perceived that BME employees were more likely to be
23

disciplined over insignificant matters, and BME staff felt that they were treated
harshly and unjustly by human resources (HR) managers. Managers were also
erroneously using disciplinary procedures to deal with performance issues. Further
perceptions arose of managers not being provided with the necessary skills to deal
with a diverse workforce and handle conflict situations effectively. Finally, Archibong
and Darr (2010) found that there was a lack of clarity between disciplinary, capability
and performance issues.
A review of how poor performance in nursing and midwifery is managed in the NHS
has been undertaken by the National Nursing Research Unit (NNRU, 2010).
Evaluation of the definition of poor performance by the National Clinical Assessment
Service (NCAS) as: “any aspects of practitioner’s performance or conduct which:
pose a threat or potential threat to patient safety; expose services to financial or other
substantial risk; undermine the repetition or efficiency of services in some significant
way; are outside acceptable practice guidelines and standards” (NCAS, 2010, p.2) is
used and challenged by the NNRU. It reported the robustness and application of this
definition was neither assessed nor tested. On closer examination of this review
study, it is unclear why the NNRU uses a definition from a document relevant to
doctors, pharmacists and dentists, and applies it to nurses. The NNRU does not give
its rationale for doing so.
In addition to 68 studies reviewed from 1998 onwards, the NNRU obtained further
evidence by analysing reports from NMC hearings and observations of an NMC
Fitness to Practise (FtP) hearing. Nationally, it is difficult to find out how many nurses
are ‘poorly performing’ as NHS Trusts are not required to report cases of
suspensions to the DoH. Again, this highlights that there is no centralised body
24

collecting national data on suspensions. The NNRU also found that suspensions
resulting from actual and potential threats to the safety of patients were uncommon.
The biggest reason for referral to the NCAS was not complaints made by patients but
complaints made by clinicians against ‘poor-performing’ colleagues.
In terms of the management of poor performance in nursing and midwifery, the
NNRU found the quality and rigour of initial investigations varied. Local procedures
were open to interpretation and extensive inconsistency. The suspension of nurses,
when patient safety was not compromised, was a common practice. Managers often
used suspension as their first choice. Approaches to addressing poor performance
were perceived as punitive. Nurses did not always know the reasons for their
exclusion. Finally, clinicians who reported poor-performing colleagues did not always
know the outcomes of their referral.
Stone et al. (2011) undertook a literature review, collected data from the NMC and
observed NMC FtP hearings on how poorly managed nurses and midwives were
handled in the NHS. Their overall significant findings were an absence of recorded
data on suspensions of NHS staff and the non-existence of systematic research into
this area.
Reviewing the National Audit Office (NAO, 2003) report, Stone et al. (2011) found
nurses and midwives made up 53% of the total suspensions in the NHS from April
2001 to July 2002. This emphasised that nurses were more likely to be suspended
than doctors. The decision to suspend nurses was not always as a result of patient
safety being compromised but automatic reactions by managers without undertaking
an adequate initial investigation. They found the DoH guidance on suspension of
25
nurses was perceived as confusing; the interpretation and application of the guidance
was open to abuse by managers and the management of suspension was
inconsistent and poorly conducted.
Stone et al. (2011) also reviewed the study by Murray (2005) on the experiences of
nurses suspended in the workplace. They observed that most nurses returned to
work after being suspended; the suspension varied between two weeks and six
months; again there was an inconsistent approach to the use of suspension; some
nurses were suspended without being informed of the nature of allegations from the
preliminary investigation; the probability of suspensions increased for nurses who
were aged over 40 and/or male and/or from BME groups.
Attempts have been made to calculate the costs of suspensions in the NHS. Using
information from the NAO (2003) report and the recorded number of nurses
suspended during 2002, Murray (2005) estimated that it cost the NHS £4.5m. The
findings of Roper (2006) estimated that it cost the NHS up to £100m to suspend 375
nurses, 152 doctors and 35 other clinical staff. The academic rigour of Roper’s
findings needs to be treated with caution as Roper was working for the Daily Mirror
and obtained this information under the Freedom of Information Act 2000. In another
study, Kmietowicz (2005) found that delaying disciplinary cases cost the NHS £40m.
The formal suspension of healthcare staff in law is considered to be ‘a neutral act’
(NAO, 2003). This is not always the case, particularly the impact on the well-being of
the suspended person. The effect of suspensions has been included by Murray
(2005) in his study. Using data from the Royal College of Nursing (RCN) counselling
service, Murray (2005) discussed the acute and chronic emotional responses of
26

shock, anxiety, anger and distress experienced by nurses who have been
suspended. Nurses barred from going into work and contacting colleagues suffered
from a post-traumatic reaction, adjustment to loss and threat to identity. Murray
(2005) used the Clinical Outcome Routine Evaluation system and analysis of
individual interviews to arrive at these findings. Reiterating Fagan’s (2004) findings,
Stone et al. (2011) described the negative impact of suspension in terms of personal
and professional costs. Alleyne (2004) found a large proportion of the participants in
her study reported considerable negative effects to their emotional and physical well-
being.
In their conclusion, Stone et al. (2011) highlighted the lack of empirical data available
and inadequate recording of information on poor performance. The role of support,
mentoring and remediation for nurses performing poorly was inconsistent and varied.
To minimise the high quantity of disciplinary action and increased costs of disciplining
staff, Stone et al. (2011) drew on the work of Cooke (2006a) into the use of quasi-
formal discipline by some managers. Cooke’s (2006a) study is also reviewed
separately.
Using the data collected from in-depth interviews with managers, nurses and TU
representatives, Cooke (2006a) presented a model of discipline used by some
managers. A quasi-formal discipline in some cases was employed instead of
implementing the formal disciplinary procedures set in place to punish nurses. This
method was used with ‘problem nurses’ who could not be disciplined formally.
Nurses who underwent quasi-formal disciplinaries felt that they were being singled
out and bullied. This form of disciplinary action was not reported at Trust Board
meetings and was hidden from its executives.
27

Examining the decisions to discipline nurses formally, Cooke (2006a) found: HR
personnel felt managers decided themselves to initiate disciplinary action without
contacting HR at the early stages of the investigation and only contacted them when
they found themselves in difficulty; TU representatives perceived disciplinary action
was excessively used by insecure and inexperienced managers; managers felt
disciplinary action would improve performance and used it when the nurse being
investigated failed to show remorse; the decision to discipline nurses in some cases
was based on the instincts of the manager rather than collecting the actual evidence
related to the issue.
Scrutinising the conduct of disciplinary cases, Cooke (2006a) also reported that it
varied. Managers again considered that disciplinary action would correct behaviour to
a professional standard; TU representatives countered that the investigations were
carried out in a hostile environment and often mishandled; both nurses and TU
representatives reported that managers lacked professional integrity.
Finally, Cooke (2006a) noted that those nurses who were taken to disciplinary
hearings, and as a consequence resigned or were sacked, often went on to work in
nursing homes. Thus, the issue of public safeguarding, poor performance and
transgression moved into the independent sector.
Professional regulatory bodies involved in the disciplinary process have been
scrutinised by the DoH because of their lack of stringency, conduct and transparency
of process in dealing with incompetent and deviant professionals on their registers
(Cooke, 2006a). Regulatory bodies interviewed in the study by Archibong and Darr
28

(2010) reported that the disciplinary panels were composed of white, middle-class
males and did not represent the diversity of the workforce.
Archibong and Darr (2010) also found: BME staff subject to disciplinary action did not
know where and how to access support; overseas-trained staff felt isolated; TU
representation was not always sensitive to the needs of BME staff; perceptions of
discrimination experienced by BME staff going through disciplinary action were
minimised.
During the literature search, several anecdotal reports in various healthcare-related
journals around disciplinary processes involving BME staff have been found.
However, these findings have not been included because of their lack of academic
rigour and also their journalistic quality.
2.4.3 Presentation of BME staff
To begin this section, the work carried out by the NHS North West (2008) is
introduced. Its work included an exhibition, a booklet and a short film on the history,
experiences and contributions of BME people in the establishment and running of the
NHS since 1948. It also referred to the prejudice and racism experienced by Mary
Seacole, when she offered to look after sick and wounded soldiers on the front line
during the Crimean war and nursing agencies declined her services. The NHS North
West (2008) highlighted that Florence Nightingale refused to interview Mary Seacole.
Black migrants who wanted to become nurses discussed their frustrations of being
offered and forced to undertake the two-year pupil nurse training instead of the three-
year student nurse programme, as they were not perceived good enough. Those who
protested were threatened with being sent back to their homeland. General
29

practitioners discussed their limited opportunities and being restricted to working in
poor inner city areas of the UK. Interviews with senior clinicians and managers
counteracted the anecdotal claims that migrant workers were to blame for the
performance of the NHS.
The strength of the material produced by the NHS North West (2008) provided a
context and an overview of the chronological significant events and landmarks.
Various clinicians from different bandings/grades, ethnic backgrounds, gender and
professions shared their negative and positive experiences around diversity and
equality. Although its material is not an actual study, it has been included as it
provides a brief historical synopsis and starting point.
2.4.3.1 Terminology
Madison (2004) stated the interpretation of how people were presented and
represented as holding power and meaning. The issue of how people and groups are
defined and presented in many of the articles tends to be overlooked or polarised
between simplistic categories of ‘black’ and ‘white’. Rarely are these categories
looked at, challenged and critically analysed. Allen (2006) argued that the politics of
description created differences; difference necessitated classification; categorisation
involved power. Drawing on the work of Hurtado (1996) and Myser (2003), Allen
(2006) emphasised:
“The power ‘we’ have as white persons to represent the other groups is not evenly
distributed. Most of it has been produced by and for white men even though white
women also benefit… Many scholars have argued that most conversations about
cultural ‘differences’ depend upon and reproduce a privilege white norm.” (p. 66)
30

When closely scrutinised and deconstructed, the term ‘white’ is seen as the hallmark
for the norm, power, knowledge, western civilisation and goodness (Allen, 2006). In
all the literature retrieved and reviewed, the term ‘white’ (when used): is not defined;
remains subtly in the background; continues to be the same; is depicted as neutral;
on the surface is depoliticised and perceived as the norm; is not questioned. The
issue of whiteness being at the centre and the mainstream is challenged and linked
to the historical colonial past and how this manifested in ‘institutional racism’, as
illustrated in the MacPherson Inquiry (1999).
Although there are no variations in the term ‘white’, a complex and confused account
is depicted in the language and labels used to describe the ‘non-white’, which is
weighted with various descriptions. For the ‘non-white’ person and groups, numerous
terms, such as ‘black’ (Alleyne, 2004), ‘minority ethnic groups’ (Healthcare
Commission, 2009), ‘overseas trained’ (Larsen et al., 2005), ‘internationally recruited’
(Pike and Ball, 2007), and ‘black and minority ethnic (BME)’ (Johns, 2005), are used
in the literature reviewed.
Without clarification, there is an assumption that the term ‘BME’ (applied to
individuals, staff or groups) has a standardised defined meaning. Consequently BME
employees are presented as one homogenised body. Alleyne (2005) outlined that
blacks were seen as ‘special’ cases and/or ‘victims’. Differences within ethnic groups
are denied as everyone is seen as the same. The key research on the
disproportional representation of BME staff involved in disciplinary procedures by
Archibong and Darr (2010) presented this problem. In their landmark study, who and
what BME employees were are not defined and are overlooked by the authors. Other
writers give a generalised account, as observed in Alleyne (2005) who wrote:
31

“…the use of the term black will refer to people with known African heritage.” (p. 298)
It is unclear to which heritage in the continent of Africa she is referring as there are
many to choose from. Some authors began to give a definition but then did not
expand on it. Obrey and Vydelingum (2004) stated:
“The term ‘black’ is a political category to describe people’s race, colour or ethnic
origins to differentiate them from the white population.” (p. 14)
Closer scrutiny of the terminology arouses discomfort, as shown in the research of
Dhaliwal and McKay (2008). They politicised and explicitly brought in emotive factors
into their definition:
“The term ‘black’ is used in this report to refer to non-white nurses of African,
Caribbean, South Asian, Chinese, South East Asian and South American descent to
connote their shared experience of colonialism, migration and racism.” (p. 3)
Research into specific ethnic and racial groups has been undertaken: Henry (2007
and 2008) looked at the experiences of Ghanaian nurses and midwives in the NHS;
Likupe and Archibong (2013) studied the experiences of black African nurses.
2.4.3.2 ‘Black and black’
The studies are simplified to a ‘black versus white’ issue and ignore the complexities
of the subject of race, ethnicity and culture within the NHS. BME employees are
presented as ‘oppressed’ and ‘victims’ while white staff as the ‘oppressors’ (Alleyne,
2004 and 2005).
The difference in progression and the tensions between different ethnic groups, as
well as the perception of inequalities between them, are not captured by current
32

monitoring processes (Healy and Oikelome, 2006). Rarely did studies and
government reports show the antagonism within ethnic and racial groups. Until
recently, this area has been overlooked, but now the problems that have appeared
within these groups have been exposed. Through semi-structured interviews, Henry
(2008) discussed how Ghanaian nurses and midwives perceived managers as
preferring African Caribbean nurses to black African ones and as a result promoting
them more quickly than black African nurses. In looking at the experiences of black
African nurses, Likupe and Archibong (2013) revealed the perceived racism among
and between overseas nurses. Black African nurses perceived nurses from the
Philippines as passive and compliant. Within the ‘white’ group, there was a
perception that East European nurses needed more reassurance and lacked the
initiative to assert their autonomy.
Finally, the subjects of race and ethnicity have been treated separately and are rarely
linked and associated to class and gender. The only studies retrieved from the
search that combined these issues are by Dhaliwal and McKay (2008) and Healy and
Oikelome (2006).
2.4.3.3 ‘Saviours’, ‘exploited’ and ‘exploiters’?
BME staff are presented as being ‘saviours’ of the NHS, ‘exploited’ by the NHS or
‘exploiters’ of the NHS. BME staff, particularly nurses, are portrayed as saviours for
governments especially when there has been a shortage of staff and problems
around recruitment (Obrey et al., 2007; Snow and Jones, 2011). Healy and Oikelome
(2006) argued that the NHS could not exist in its current form if overseas qualified
professionals and BME staff left it.
33

In contrast, Larsen et al. (2005) and Henry (2008) examined the perception that
overseas-trained nurses were exploited or only working for their own economic and
financial gains. Henry (2008) pointed out the complexities and context of the
motivations of Ghanaian nurses and midwives migrating to Britain, and what
happened to them when they got locked into a stagnated and despondent position.
Despite participants in the study ‘acting up’ into senior positions, they failed to secure
permanent positions after not passing their interviews. These participants felt
managers did not provide the necessary support to facilitate their career progression
and attributed discrimination to their stagnation. With little choice and poor promotion
prospects, some of these nurses focused their attention on monetary gains to extend
their property and financial investments when retiring and returning to their homeland
in Ghana.
Lewis (2011) reported how black nurses and HCAs were targeted by NHS anti-fraud
investigators; 66 out of the 98 prosecuted were African Caribbean; 59% of the cases
constituted around fraud or criminal offences related to false documents. Questions
are raised about the academic rigour and methods used to test the validity of Lewis’s
(2011) findings.
2.4.3.4 Overseas staff
The recent arrivals and experiences of overseas health professionals, particularly
nurses and doctors, have been explored in several studies (Allan et al., 2009; Healy
and Oikelome, 2006; Henry, 2007 and 2008; Hunt, 2007; Larsen et al., 2005; Larsen,
2007; Likupe, 2006; Obrey and Vydelingum, 2004; Oikelome, 2007; Pike and Ball,
2007).
34

Archibong and Darr (2010) found overseas-qualified clinicians, who had been trained
differently and were acquainted with different ways of working, were given insufficient
support to make the transition to adapt to the values and culture of the NHS. Hunt
(2007) stated that overseas BME nurses became alienated, devalued and
demoralised. He emphasised how their qualifications were denigrated as second
class and inferior as British nursing theory and clinical practice were idealised. In the
clinical area BME nurses were expected to integrate into the culture of the NHS. Hunt
(2007) discussed a sense of unfairness prevailing among overseas nurses who felt
that adjustments solely relied on them adapting. He argued that managers did not
consider how the culture of the NHS impacted on overseas-trained staff.
A phenomenological study by Obrey and Vydelingum (2004) found overseas nurses
were humiliated and embarrassed when their English was corrected in front of
patients and colleagues. This led to these nurses being alienated and left them
feeling isolated and disillusioned. Behaviour that was deemed as bullying could not
be challenged as they feared reprisal.
Allan et al. (2009) established discrimination in the form of racist bullying experienced
by overseas nurses. These findings arose out of three interviews and re-analysis of a
national study, undertaken by Smith et al. (2006), that recognised how racial
discrimination was experienced by overseas nurses at an interpersonal and
organisation level while working in UK healthcare settings. They found overt and
indirect discrimination.
Archibong and Darr (2010) identified overseas-qualified nursing employees working
in higher bandings as being disciplined after patient complaints. Saundry et al. (2008)
35

found BME employees were less aware of their employment rights than their white
counterparts. This restricted BME workers from challenging any disciplinary action
initiated against them.
2.4.3.5 Perceptions of behaviours and attitudes of BME staff
The perceptions of ward managers on the functioning, competence and
professionalism of BME nurses has been investigated. Carter’s (2000) study in a
Trust with a disproportional representation of BME nurses involved in the disciplinary
process revealed how some ward managers perceived BME staff as ‘troublemakers’
and so were reluctant to employ this group in their clinical areas. These managers
reinforced their Eurocentric attitude by deducing from the high number of ethnic
minority staff going through the disciplinary process that this was indisputable
evidence that they were difficult to manage.
Alleyne (2004) found that conflict experienced by black people arose from subtle
comments and behaviours aimed at their race and cultural identity. This took the form
of some white staff: failing to notice the presence of black employees; refusing to
make eye contact when appropriate; excluding black colleagues; using words like
aggressive, scary, angry, frightening, threatening, difficult and problematic when
describing black people.
BME nurses who cannot present themselves in the ‘white way’ or the mainstream
established ways are perceived negatively by white managers and colleagues. Johns
(2005) suggested that ‘fitting in’ was seen as more important than the ability of the
BME nurse and as a result the different skills, qualities and experiences of BME
workers were unrecognised. To have a rapport with managers, black nurses had to
36

‘speak the same language’ and socialise with them. However, their home and family
circumstances prevented this.
Two studies conducted by the RCN (Dhaliwal and McKay, 2008; Pike and Ball, 2007)
found many BME female nurses were single parents with dependent children. The
working hours and shift patterns in nursing made it incompatible with the home lives
of these mothers. Consequently, their work had to be based in community settings as
the working hours in other clinical areas were not compatible with their childcare
arrangements. Reduced income, having additional jobs to supplement the main
income and lack of career opportunities were reported by the participants in the study
(Dhaliwal and McKay, 2008) who were all black and female. Additional findings from
these two studies noted that BME nurses perceived they were closely monitored,
they had to work harder and their managers did not consider them to be capable of
achieving managerial and supervisory roles.
Archibong and Darr (2010) found that BME employees at lower positions were
perceived as not being committed and/or performing to the accepted standards of the
NHS. A literature review undertaken on the experiences of black African nurses by
Likupe (2006) found that they were employed in low-skill and low-paid work. Their
skills and training were undervalued and unrecognised. Questions were raised about
the authenticity of their qualifications.
Archibong and Darr (2010) noted how different styles of communication were
negatively interpreted by colleagues, managers and patients. In an earlier and
separate study, Nairn et al. (2004) examined the problem of cross-cultural
37

communication and misinterpretations around eye contact, time, attitudes towards
authority figures and group/individual dispositions.
2.4.4 Organisation and management culture of the NHS
As well as healthcare employees not performing to the standards required by their
professional regulatory bodies and Trusts, studies by Carter (2000), Cooke (2006a
and 2007) and Stone et al. (2011) suggested management styles and organisational
factors contributed to discrimination and poor standards.
Politicians from all sides have accused the NHS of being monolithic, inefficient and
unresponsive to patients’ needs. This has led to major structural reform. To reduce
costs, do more for less and increase efficiency, market styles of management have
been introduced and used in the NHS. Trusts employ a style of management
characterised by explicit standards and measurement of performance, competition
and private sector mode of management. Carter (2000) argued this ‘new public
management’ has reduced ethnic equality in the NHS, as managers have become
preoccupied with stringent control on finances and resources. Despite the duties
imposed by the Race Relations (Amendment) Act 2000, the E&D agenda has
become marginalised because managers have become preoccupied with economic
factors.
Carter’s (2000) research also revealed that some white ward managers became
resentful and hostile towards equal opportunities policies. From the questionnaires
and in-depth interviews, these managers disclosed feelings of equal opportunities
policies being ‘politically correct’, humiliating white people and treating Asians with
‘kid gloves’. As a consequence of these attitudes, clinical areas could become
38

segregated and racialised. There was an assumption that an ethnic diverse team
would threaten the efficient running of the ward as BME staff were perceived as
problematic. Carter (2000) argued:
“The increasing pressure as a result of new public management to exert more and
more control over the workforce has implications for any social group who are
regarded ‘difficult’ to manage.” (p. 79)
The style of management adopted has led to BME staff being indirectly discriminated
against and many managers being averse to employing BME nurses because of their
perceived difficulty in integrating with white staff. Rather than recruiting staff that are
perceived as being difficult to control and manage, anecdotal evidence suggests that
Filipino nurses are being employed as they are perceived as being passive,
submissive and easy to manage (Likupe and Archibong, 2013).
Overall, Carter’s (2000) study still holds value today, as other studies have
incorporated the significance of his work into their research and found similar findings
(Archibong and Darr, 2010). The research design of Carter’s study incorporated a
directorate of medicine and directorate of psychiatry. The response rate to the 1400
questionnaires sent out is very respectable. Data was collected from 1993 to 1997. It
is unclear how many participants were interviewed. The interviews included different
ethnic groups from different levels within the directorate.
Duffin (2003) reported that the lack of competency among BME staff might not be the
fault of the nurse and might well arise from: poor training and supervision; managers
offering minimal support to nurses struggling with certain practices; workplace
39

context having a profound effect on the nurse’s performance, particularly where there
was low morale, high turnover of staff and heavy workload.
Healy and Oikelome (2006) found discriminatory practices continued to be replicated
and rationalised in the workplace. They found that overseas-qualified doctors were
contracted to work longer hours, closely supervised, had their work regularly
scrutinised and had low morale in comparison to UK-qualified doctors. In the
workplace, they found discrimination and racism were not confronted by the
institutional structures and policies linked to E&D. These findings are from research
investigating the working experiences and career opportunities of skilled and low-
paid BME workers in the health sector.
Using findings from a literature review, interviews with DoH policy advisors, NHS
employers, TUs and health service managers, semi-structured biographical
interviews and statistical data, Healy and Oikelome (2006) emphasised that BME
workers had to work harder than their white counterparts to succeed. Over 50% of
the participants in the interviews revealed that they had experienced workplace
racism. Also, a person with an English-sounding name was more likely to be
shortlisted for a job than a person with a foreign-sounding name. Noticeably, Healy
and Oikelome (2006) are among the few researchers who link issues around class
and race together.
From their detailed research, Healy and Oikelome (2006) argued that initiatives
around E&D were focused more on changing individuals rather than changing and
challenging the culture of the NHS. They asserted more resources needed to be
invested to challenge and transform the organisational culture that prevented the
40

implementation of these schemes, and greater honesty and transparency was
needed from managers. In terms of producing effective change, there is a perception
that TUs are powerless to effect any positive change in the work setting and white
people are blinded to understand the nature of workplace racism.
The modernisation programme of the NHS has led to contradictions in the style and
management. Reflecting on the work of Pollitt and Bouckaert (2000), Cooke (2006b,
p. 224) catalogued the contradictions that were played out every day in the NHS as:
“• Increase political control but free managers to manage;
• Save money and raise standards;
• Motivate and empower staff but intensify work and downsize;
• Reduce bureaucracy but increase audit, measurement and juridification;
• Decentralize responsibility but centralize control.”
Cooke (2006b) argued that the search for cost savings and getting more with fewer
resources meant clinical staff carried heavy workloads, worked over and above their
contracted hours and experienced intense pressure that led to nurses complaining of
stress, exhaustion and low morale. Working in these circumstances made it difficult
for nurses to provide holistic and high standards of patient care and, hence, a
production line approach was adopted. Patient dissatisfaction led to nurses not only
bearing the brunt of complaints over poor standards of care with patient safety
compromised, but also being scapegoated and on the receiving end of disciplinary
action.
41

Cooke’s (2006b) findings demonstrated the contradictions identified above led to
tensions between nurses and managers over inconsistent and opposing
management style. Participants from her study referred to this as ‘seagull’
management which denoted:
“We have seagull managers here, they fly in from a great height, make a lot of noise,
drop a lot of crap, then they fly off again.”(p. 223)
Cooke (2006b) described seagull management as consisting of four characteristics:
1. Managers who rarely visited the clinical area or visited if there was a
complaint/serious incident;
2. Distrust between managers and clinical staff. Clinical staff mentioned feeling
unsupported;
3. Destructive criticism in the form of clinical staff being humiliated and shamed;
4. Defensive culture adopted to counteract complaints, litigation and bad publicity.
In another study, Cooke (2007) investigated scapegoating that was hidden and in the
subconscious and unconscious of organisations. She defined the scapegoat as: “one
who is blamed or punished for the sins of others” (Cooke, 2007, p. 178). Her theories
of scapegoat are drawn from psychoanalysis and also the work of Girard (1986) and
Bonazzi (1986). Her findings came from data drawn from interviews with ward
managers/charge nurses, staff nurses, managers, TU representatives and directors
of nursing. Data was also collected from observations and documents. The findings
discussed the unpopular nurse, the incompetent ward manager and the
insubordinate nurse.
42

Drawing on her findings, Cooke (2007) profiled the characteristics of the unpopular
nurse as: an outsider who did not fit in the team; a problem nurse no one wanted to
protect; someone not pulling their weight; somebody set up by the team to fail; a
person taking the blame for the rest of the team; somebody vulnerable. The
environment where errors and standards of care fell below acceptable levels was
often chaotic, highly charged with inadequate staffing and low morale. Rather than
recognising shared responsibility for the delivery of poor standards of care, one
individual was blamed. From her data, Cooke (2007) showed that the unpopular
nurse was singled out and held to account for the misdemeanour.
Cooke (2007) also identified incompetent ward managers as scapegoats. Usually
they were accused and disciplined for managerial incompetence around the failure to
cope with reorganisation of services. There was a failure by senior figures to think
about the wider systems and processes leading to the failings. Using the theories of
Bonazzi (1986) on ‘instrumental scapegoating’, Cooke (2007) argued that holding the
ward manager responsible excused Trust executives and higher managers, who
introduced the poorly planned changes, from blame and accountability. Attention
from those in power and instigators of change was averted.
Another group identified as scapegoats were nurses labelled as insubordinate and
described as ‘having a bad attitude’, ‘bad apples’ and ‘troublemakers’. Nurses with a
bad attitude were those who challenged the status quo and were frequently
subjected to disciplinary action. Outcomes of dealing with insubordinate nurses were:
to move them to other clinical settings; make an example of them to warn others
what would happen if they questioned the authority of higher management.
43

From a literature review, and using the work of Murray (2005), Stone et al. (2011)
linked suspension with: low morale and bullying often by managers; increased
workloads; harassment and conflicts with colleagues or managers that led to
complaints and insubordinates facing disciplinary action. Reflecting the assertions of
Henry (2000) and Oulton (2003), Stone et al. (2011) emphasised that errors did not
occur because nurses were reckless or poorly trained. They happened as systems in
organisations were not designed to prevent errors from occurring.
Following a Freedom of Information Request sent to 24 Trusts in London, the Royal
College of Midwives (RCM) found 60% of midwives had been subjected to
disciplinary action (RCM, 2012). To understand this issue, the RCM suggested,
organisation culture, poor management practice, poor leadership, lack of awareness
of E&D and the attitudes of all staff needed to be investigated. However, as the
findings of the RCM (2012) were limited to London, it was unclear if this problem
existed across the country, and so more research is needed.
Researching BME staff involvement in the disciplinary process, Archibong and Darr
(2010) revealed several findings in the areas of management practices and
competencies as well as organisation culture.
Their results about management practices highlighted: inconsistent application of
disciplinary policies with line managers finding it difficult to deal with disciplinary
issues involving BME staff; some managers lacked confidence in applying informal
strategies, particularly when dealing with minor issues involving BME staff; BME staff
were more likely to be disciplined over insignificant matters; HR managers felt BME
staff were not treated fairly; line managers were using disciplinary procedures
44

inappropriately to deal with performance issues; some managers could not deal with
a diverse workforce and manage conflict effectively.
In terms of organisation culture, Archibong and Darr (2010) found that issues of
equality were not always considered in formulating and putting policies into
operation. They also found that Trusts adopted a subtle culture that rebuked
employees who did not follow the conventional organisational customs and the issue
of race could influence the decision to discipline staff.
A recent scoping study commissioned by the NCAS and undertaken by Traynor et al.
(2013) concentrated on the conflict between managers and healthcare professionals
in the management of poor performance among UK nurses and midwives. From the
evidence gathered, Traynor et al. (2013) found NHS Trusts managed poor
performance in a costly and unsatisfactory manner. The lack and low quality of data
on poor performance publicly available served these organisations as they could
conceal their practices and shun scrutiny.
Drawing on the work of Berg (2006), Traynor et al. (2013) reported the authority of
managers was challenged by clinicians, particularly doctors. The relationship
between managers and clinicians was marked by different concerns and challenges.
For some managers, the main priority was control over healthcare professionals,
their spending and increasing their outputs. Traynor et al. (2013) also acknowledged:
the vulnerability of NHS managers, particularly around the pressures they faced to
meet targets set by central government; increased monitoring by external and
internal bodies; the outbreak of serious incidents around patient safety and dignity as
reported in the local and national media. Finally, Traynor et al. (2013) noted:
45
“As members of a relatively weak professional group, nurses who are disciplined
carry the individualised blame for organisation failings such as poor resources, poor
training and target driven cultures.” (p. 6)
The solution prescribed by NHS Trusts for better training, clinical supervision and
appraisals has not addressed the complex systemic and political aspects of the
issue.
2.4.5 E&D agenda
The racist murder of Stephen Lawrence in 1993 led to the MacPherson Inquiry in
1999. Following the inquiry, the Labour government introduced the Race Relation
(Amendment) Act 2000 that has placed a statutory general duty on public bodies to
promote race equality. Since the introduction of this legislation, greater attention and
a higher profile has been given to E&D policies and practices. In spite of the DoH
claiming that the NHS was making improvements in E&D, Healy and Oikelome(2006)
reported scepticism expressed by BME staff who felt wary of the stream of schemes
and that these initiatives made no impact.
Carter (2000) reinforced the findings of Beishon et al. (1995) that equal opportunities
policies: were poorly communicated; lacked information; were paper commitments
that held little significance; were poorly embraced and put into practice and lacked
direction. He added two other significant findings from his study: equal opportunities
policies were marginalised when economic pressures were placed on hospitals to
control their budgets; managers were resistant to incorporate equal opportunities
policies when appointing staff.
46

Covering the changes of the past 25 years around the E&D agenda, the Wainwright
Trust (2012) reported the key achievements and challenges that remained. It
highlighted: a greater awareness of prejudice-based inequalities; discrimination was
institutionalised and indirect; E&D was on the political agenda. It identified ongoing
challenges as: inserting E&D in practice and the mind-set; discrimination driven
underground; political correctness; the limited understanding of racism and
institutionalised racism; the Conservative–Liberal Democratic coalition government’s
lack of commitment to E&D as economic challenges took priority; the coalition
government possibly reversing employment protection law.
To collect the data, the Wainwright Trust (2012) sent out four questions to everybody
on its database. Recruitment and respondent details were not disclosed in its report.
In the report, the Trust acknowledged that the findings were not representative and a
comprehensive study was needed. It is unclear how many of the views expressed in
the responses are personal or the views of the organisation.
Alleyne (2005) studied the impact of race equality training and analysed the
perceived motivating factors of NHS managers seeking equality training for their
staff. She asserted:
“The immediate pay-offs for the organisation are creating an acceptable face to the
external world and a sense of security within. Guilt, shame and blame are temporarily
absolved from the organisation’s conscience, and everyone can sit back with an ease
of mind that they have done the right thing.” (p. 3)
A sense of cynicism prevails that NHS Trusts could be ‘seen to be doing’ and tick the
box of complying with E&D policies in their organisations. Alleyne (2005) emphasised
47

the training received had minimum bearing and impact on staff attitudes and
relationships.
With a background in psychotherapy and research involving diversity and stress in
the workplace, Alleyne (2005) analysed her experiences as an independent trainer
facilitating training groups for public sector staff undertaking diversity training. Using
a psychodynamic approach, she examined the working relationships in how
employees address issues of difference, prejudice and oppression in their teams and
workplace.
Alleyne (2005) found that the agenda of managers commissioning the training was
vast, muddled and homogenised. There was an unrealistic expectation from
managers that this agenda could be covered in half a day. Alleyne (2005) interpreted
this as: the organisation and staff perceiving ‘blacks are all the same’ and ‘black
people being seen only as special and victims’; the request to allocate the bare
minimum of time was an avoidance to look at the primitive fears in the unconscious;
denial was used to evade the complexity of emotions surrounding race and culture.
Rather than engage with the unpleasant strong emotions, processes and reactions,
employees looked for prescriptive and cognitive recipes in how to behave and what
language to use. Using ‘politically correct’ language exempted staff and organisations
from being labelled “racists”.
Alleyne’s (2005) other findings were: sessions were highly charged with hostility and
ambivalence; resistance was encountered when individuals and groups were
challenged about their defensive behaviour; white participants in the session
experienced shame and took up a guilt-ridden position due to Britain’s colonial and
48

imperial past when black participants discussed oppression. Absolution of these
feelings led, in some situations, to white people asking for forgiveness from black
participants.
In Alleyne’s (2005) study, her psychodynamic approach focused on the psychological
unconscious forces operating within the psyche of individuals, teams and the
workplace. She has tried to understand in depth and go beyond the adverse
challenges of how people related to each other in the complex area of race and
culture. However, there are drawbacks to her study particularly around the questions
asked about the lack of rigour and the scientific evidence base of psychodynamic
approaches used.
Despite this rhetoric stance from the then Labour government to its commitment to
the E&D agenda, the Audit Commission published The Journey to Race Equality in
2004. It directly addressed what prevented progress to race equality in the public
sector. In the main, the auditors reported organisations needed to address
institutional behaviours that hindered positive outcomes for BME groups. These
behaviours were found in institutional racism reported in The Stephen Lawrence
Inquiry, Report of an Inquiry by Sir William MacPherson of Cluny (1999). The Audit
Commission (2004) identified the main barriers as: low priority given to race equality;
lack of understanding about incorporating race equality in day-to-day work;
insufficient resources allocated; difficulty relating to BME groups; too many or too few
objectives.
49

2.5 Summary of literature review
The disproportional representation of BME staff in the disciplinary process in the
NHS came to the attention of Parliament in 2008. On behalf of the NHS Institute for
Innovation and Improvement, Archibong and Darr (2010) undertook a study to
investigate this phenomenon. They found BME staff over-represented in the
disciplinary process. It was difficult to ascertain the extent and depth of this issue as
there is no centralised body collecting quantitative and qualitative details on
disciplinaries in the NHS. The literature reviewed predominantly involved nurses.
The literature review on disciplinary hearings and BME staff has been divided into
five sections: disciplinaries outside the NHS (including international studies and other
sectors); poor performance, suspensions and disciplinaries in the NHS; presentation
of BME staff; organisation and management culture of the NHS; E&D agenda. Some
of the themes overlap. Anecdotal evidence has not been included in the review.
From the literature review, various qualitative methods (including web audits, focus
groups, interviews, scoping studies, case studies and questionnaires) have been
identified as methods of investigation. There is a dearth of studies that specifically
focus on BME staff and the disciplinary process in the NHS. Carter (2000) and
Archibong and Darr (2010) are the exceptions. Studies on disciplinaries have been
included in the review even though they might not directly refer to BME staff.
2.6 Gaps
The seminal study by Archibong and Darr (2010) specifically considered the
neglected area of the disproportional representation of BME staff involved in the
50

disciplinary process. However, the authors did not acknowledge their study
limitations which, on closer inspection, are:
1. Professions, ‘overseas qualifiers’ and BME staff are homogenised. The different
BME groups working in the NHS are not identified.
2. Rationale behind disciplinary actions is needed and the type of disciplinaries
used by managers was outlined in the study. No definition of ‘disciplinary’ or
‘disciplinary proceedings’ is given.
3. The researcher, being an instrument to the study, is absent. As researchers,
Archibong and Darr relied on participants’ perceptions and experiences and
incorporated these into their final findings. The realities of what participants have
witnessed and shared with the researchers are valid. As there are ‘multiple
truths’, Archibong and Darr’s own ‘realities’ could not be ascertained or offer
another dimension to the findings.
4. There is no literature review of the disciplinary process relating to BME staff in
the NHS.
5. The study findings fail to recognise critical studies that have investigated some
areas of disciplinary action and proceedings in the NHS. For example, the
important work of Hannah Cooke (2006a and b; 2007) on scapegoating and
examining the disciplinary process in the NHS is ignored.
6. There is a lack of attention to the wider context of the continuous changes and
reconfiguration of the NHS. The pressure to make savings, which led to a
shortage of nurses and services being redesigned when public expectations and
51

demands continued to grow, is not addressed. The consequences of how this
impacts on the roles and responsibilities of staff and the tension and dynamics
created in teams, working relationships and ultimately on the quality of patient
care, were not wholeheartedly considered. The bigger picture of the politics of
daily life in the NHS is sidestepped in the study.
7. It is hard to ascertain from the study if Archibong and Darr had direct contact with
BME staff undergoing the disciplinary processes. The study findings are based
on the perceptions of participants who only seem to be senior staff who are
presenting the views of the majority. Contradictory views are shunned.
8. Apart from two semi-structured interviews carried out with representatives from
the General Medical Council and NMC, all the data is collected within group
settings. Participants in group settings could be silenced from expressing what
they actually think and feel if their views were against popular opinion and were
controversial.
2.7 Formulation of the research question
In light of the dearth of research, no studies using ethnography have been found in
the literature search to investigate the over-representation of BME staff involved in
the disciplinary process in the NHS. There is also an absence of research examining
the disciplinary process in terms of investigations, hearings and staff directly involved
in this process. Although the Trust (where this study will be undertaken) has
recognised there is a disproportional representation of BME employees involved in
the disciplinary process (this phenomenon) over the past five years, the reasons are
unclear as no research has been undertaken to investigate this phenomenon.
52

The research question is ‘what are the key factors that influence the over-
representation of BME staff in the disciplinary process in this Trust?’ This is an
exploratory study to determine and begin to understand why this phenomenon exists.
Ethnography is used as the methodology. This study will build on the work of Carter
(2000), Cooke (2006a and b) and Archibong and Darr (2010) by adding another
perspective to an under-researched area.
53

Chapter 3: Methodology
3.1 Introduction
This chapter begins with an outline of a qualitative approach that embraces
ethnography. Justification for using ethnography as a methodology to meet the study
aim is outlined. Focus is then on how the Trust was secured and accessed to carry
out this research. The ethnographic aspects used in this study to collect data through
fieldwork, secondary data, participant observations, semi-structured interviews and
journal/diary are discussed and presented in Figure 1. Recruitment and selection of
participants are then considered. The recording of data precedes the thematic
analysis that is used to analyse the data collected. Ethical matters relating to this
research are addressed. Finally, reference is made to reflexivity.
54
Figure 1: Study process and data collection methods
55

3.2 Qualitative approach
Qualitative and quantitative research have been presented as opponents with
randomised and controlled trials being distinguished as the best. This debate is
questioned by Mays and Pope (1995) and considered superfluous as:
“The crucial question, therefore, is not what is the best research method? But what is
the best research method for answering this question most effectively and efficiently.”
(Al-Busaidi, 2008, p. 1)
Qualitative research is compatible with discovering the meaning that people place on
events, processes and structures of their life experiences, behaviours and beliefs (Al-
Busaidi, 2008). Attention is given to the social context where people live and work
and researchers want to gain an understanding from the perspective of participants
in how they construct their social world. With qualitative research, there is no single
truth but multiple realities that are there to be described and discovered. To access
the subjective realities, researchers need to enter the participants’ social world,
experience their culture first-hand and engage with them in their day-to-day lives.
Qualitative research emphasises that a phenomenon needs to be studied in a holistic
manner and not isolated and reduced into multiple parts (Ryan et al., 2007).
Qualitative research relies on the researcher to act as the research instrument (Pope,
2005) and conduit for language, beliefs and experiences to be shared by the
members of the group being studied. As the researcher is immersed in the field, the
similarities and differences in the human experiences of the cultural group and
setting are brought to the surface and analysed. The subjectivity of using a qualitative
method where the researcher and research are directly connected has its challenges
56
(Topping, 2010). Critical self-reflection of the researcher’s own predisposition and
biases need to be examined (Polit and Beck, 2012). This process is also known as
‘reflexivity’ and discussed further at the end of this chapter.
Qualitative methods aim to explore the social problems that a culture or group of
individuals experience (Goodson and Vassar, 2011). Ethnography in particular is
different from other qualitative research methods as it concentrates on culture and is
used to highlight sensitive areas and give voice to marginalised and unspoken issues
in health care (Dixon-Woods, 2012). For this study, ethnography is used to meet the
study aim, which is to determine the key factors that influence the over-
representation of BME staff in the disciplinary process in an NHS Trust.
3.3 Research site
This section has been included as the Trust had some effect on the methodology,
particularly around the size of the sample selected. Before, and in addition to, putting
a research proposal together for ethical clearance, it was pivotal to secure a research
site. It would have been futile to undertake the proposed research study without
having an NHS Trust willing to participate.
Trying to initiate a study to investigate the disproportional representation of BME staff
in the disciplinary process presented numerous issues and obstacles. The first was
selecting a Trust where the phenomenon of the over-representation of BME
employees involved in the disciplinary process existed. The next stage was to
negotiate and establish relationships of trust with key senior influential figures so that
access to the site could be obtained for the study to be undertaken. As well as finding
and accessing a research site, a research proposal needed to be composed so that
57
ethical approval could be granted for a study to be carried out. The rationale for
selecting the Trust as a potential research site was:
1. The initial online search identified the Trust as having a disproportionate number
of BME staff involved in the disciplinary process;
2. I had a connection with the Trust;
3. In terms of practicalities, distance and travel, the potential research site was
accessible and manageable to collect data.
The nature of the research subject is regarded as a sensitive area. McGarry (2010)
described sensitive research as “intimate, discreditable or incriminating” (p. 8). For a
Trust to allow a researcher into its setting to conduct a study on a sensitive ‘taboo’
subject, such as the disciplinary process involving its BME staff, could raise much
anxiety, particularly as it is unclear what the findings would reveal, including potential
repercussions for the Trust.
3.3.1 Negotiating and gaining access to the Trust
Currently I work at a university that is connected to the Trust. As a researcher who
has some position of an ‘insider’ in the Trust, there are certain advantages. Bonner
and Tolhurst (2002) described these advantages as: rapport and relationships are
already established; there is some understanding of the culture being studied;
disruptions are minimised. The potential drawbacks are: the research perspective
being lost if too much rapport with participants is established; the balance between
objectivity and subjectivity being impeded; familiarity with the environment leading to
assumptions being made and subtle data being ignored (Bonner and Tolhurst, 2002;
McGarry, 2006). Consideration of having a connection with the Trust before the start 58

of the study and the impact of this relationship is discussed further under section 3.12
Reflexivity.
Before making any ethical application to the University Research Ethics Committee
(UREC) and the local NHS Research and Development (R&D) ethics committee, key
employees in the Trust were contacted. Pope (2005) stated:
“The point of entry and alliances with powerful gatekeepers in the organisation
influence how group members perceive the research.” (p. 1180)
The identified gatekeepers had a significant role, particularly around sanctioning the
study, providing access to the Trust site, sources of data and meetings needed for
participant observations. Six meetings were held over a four-month period. During
the intervals between our meetings, the gatekeepers consulted and discussed the
proposed study with colleagues involved in E&D issues related to the workforce and
disciplinary process. Simmons (2007) stressed that the relationship between
gatekeepers and bodies they liaise with is important. She said:
“The more trust the group places in the gatekeeper, the more trust is extended to the
ethnographer.” (p. 13)
Emphasis in the dialogue with senior managers and gatekeepers focused on the
balance between the benefits, risks and potential outcome of the study. It was made
clear that the proposed research would not involve service users, carers or any form
of clinical trials. Potential participants would be Trust employees involved in
disciplinary-related matters and their participation would be voluntary.
59
To gain authorisation, as needed for the NHS Site Specific Information form, some
amendments stated by a Trust Board executive needed to be made to the original
research proposal. The word ‘apparent’ needed to be inserted into the title as it was
not definite in the mind of one Trust Board executive that there was an over-
representation of BME staff in disciplinary hearings. The initial number of 12 semi-
structured interviews needed to be increased to a minimum of 20 so that there was
more representation and depth in the study. (The sample size of 12 was also queried
by the UREC who stipulated that this needed to increase.)
The changes were discussed with the academic supervisors. Consideration was
given to this study being the intellectual property of the researcher and autonomy
being maintained over the methodology used to investigate the phenomenon. This
was balanced with the need to secure a research site. It was agreed to make the
changes. Once ethical clearance had been approved, a working space, honorary
contract, title of honorary researcher, identity badge and parking permit were issued
by the Trust.
3.4 Ethnography as a methodology
The word ethnography is derived from the Greek ethnos meaning people/folk and
grapho meaning to write (Cull, 2011). From this translation, ethnography is writing
and describing particular people. It is not simple to define ethnography as there is
extensive uncertainty about what ethnography is (Savage, 2006) and there have
been many variations and interpretations of ethnography (Lambert et al., 2011).
According to Hammersley (2006), there are issues in describing ethnography as
there is no standard definition due to its complex history. As a methodology,
ethnography has originated from anthropology and sociology. Today the discipline of
60

ethnography has become so wide and complex to describe that it has been marked
by diversity rather than consensus (Atkinson and Hammersley, 1994). Focused and
critical ethnography (as explained in 3.4.3 and 3.4.4) are used in this study.
3.4.1 Rationale for using ethnography
To reiterate, the study aim is to determine the key factors for the disproportional
representation of BME employees involved in the disciplinary process in an NHS
Trust. To understand this phenomenon, it was important to get on the inside of the
Trust and examine the context, culture, structures, procedures and the personnel
involved in the disciplinary process. Ethnography encompasses a method to
investigate this.
Rather than relying on a single approach, additional methods commonly used in
ethnography were adopted to support the fieldwork in the Trust, triangulate the
findings and maintain rigour. These other methods included collecting secondary
data, undertaking participant observations and conducting interviews in the natural
setting.
As established in the literature review, no ethnographic studies were found on the
over-representation of BME staff in the disciplinary process in the NHS. Methods
identified in the review were web audits, workshops, focus groups, case studies,
interviews, semi-structured interviews and questionnaires. By undertaking an
ethnographic approach, this study will add another layer to the existing knowledge in
order to understand this complex, challenging and under-researched area.
61

3.4.2 Characteristics of ethnography
Despite there being no consensual definition of ethnography, Skeggs’ (2001)
definition of ethnography has been applied as this encapsulates the ideas used in
this study. She described ethnography as:
“A theory of the research process – an idea how we should do research. It usually
combines certain features in specific ways: fieldwork that is conducted over a
prolonged period of time; utilizing different research techniques; conducted within the
settings of participants, with an understanding of how the context informs the action;
involving the researcher in participation and observations; involving an account of the
development of relationships between the researcher and researched and focussing
on how experiences and practice are part of a wider process.” (p. 426)
Ethnography does not come under one epistemological belief. The assortment of
ethnographic approaches are differentiated by epistemological and ontological
perspectives such as naturalism, realism, relativism, modernism and postmodernism
(Savage, 2006). There are several ethnographic approaches: classical, critical,
feminist, narrative and focused. Focused and critical ethnography are used in this
study.
3.4.3 Focused ethnography
Focused ethnography is a useful method in capturing data on a specific topic or
shared experiences (Higginbottom et al., 2013). The main attributes identified by
Muecke (1994) – and reasons for using focused ethnography in this study – are:
1. Problem-focused and context-specific – the issue is the apparent over-
representation of BME staff in the disciplinary process;
62
2. Focus on a discrete organisation phenomenon – the unexplored phenomenon
exists in an NHS Trust;
3. Conceptual orientation of a single researcher – one researcher undertaking this
as part of a taught clinical doctorate programme;
4. Involvement of a limited number of participants – this involves staff engaged in
the disciplinary process;
5. Episodic participant observation – as I was undertaking the taught clinical
doctorate programme on a part-time basis and needed to complete the study
within a specific time frame, only periodic participant observations could be
undertaken in the field;
6. Participants hold specific knowledge – the staff involved in the disciplinary
process hold experiences and knowledge about the phenomenon;
7. Used in academia as well as for development in healthcare services.
3.4.4 Critical ethnography
Critical ethnography is influenced by critical theory that perceives reality produced by
social, political, cultural, economic, ethnic and gender values (Denzin and Lincoln,
1994). Critical theory centres on understanding power relationships, social structures,
oppression and social justice (Vandenberg and Hall, 2011).
Critical ethnography focuses on social oppression and injustice by highlighting issues
related to power and control (Madison, 2004). Institutions and social practices that
restrict choice, denigrate identities and communities are scrutinised. Using critical
ethnography for this study is fitting as BME employees highlighted in the literature
63

review are more likely to be disciplined than their white counterparts in the NHS
(Archibong and Darr, 2010; Royal College of Midwives, 2012; South East Coast BME
Network, 2008).
3.5 Core concepts from ethnography
Any ethnographic approach has two principle concepts, which are at the core of this
methodology: culture and fieldwork (Lambert et al., 2011).
3.5.1 Culture
According to Roper and Shapira (2000), questions that should guide the study are:
“What is it like being a member of the particular culture? What are the rules guiding
social behaviour?” (p. 3)
The knowledge that is gained from these questions by the researcher needs to be
contextualised in the wider setting. Does what goes on in the system reflect and
mirror what goes on in other systems, the wider organisation and society? Is the
culture specific to the setting? Can new insight be found from the study and add to
existing knowledge?
One of the main objectives of ethnography is to interpret culture (Fetterman, 2010).
Ethnography can reveal the culture of people’s natural workplace setting. This is
done by examining and understanding the patterns of employees’ social interactions
and their interpersonal relationships with colleagues who occupy the same space.
Holloway and Todres (2010) defined culture as:
“A way of life of a group, the learnt patterns of behaviour that are socially constructed
and transmitted. This includes shared communication system in language, gestures
64

and expressions – the message that most cultural members understand and
recognise.” (p. 166)
Individuals in groups share behaviours, differences and diversity. This needs to be
considered as culture is not homogenous and something that operates on its own.
Institutions, such as hospitals, are complex cultures within themselves (Goodson and
Vassar, 2011) and various cultures intertwine and operate at the same time. In a
complex and challenging organisation, such as the NHS, the context is constantly
changing and this has a bearing on the culture. Historical, social, political and
economic forces on the conscious, subconscious and unconscious level also exist
(Obholzer and Roberts, 2003). These forces impact on the cognitions, behaviours
and emotions of staff. How much of these dynamics influence and reflect how
employees perceive themselves, their relationships with others and how they function
in groups and the organisation setting needs to be elicited and interpreted by the
researcher. Fetterman (2010) described this as ‘cultural interpretation’. Being
culturally immersed (Streubert and Carpenter, 2011) in the field allows the researcher
to see the power of dominant values, beliefs and ideas operating in the organisation.
This falls in line with critical ethnography.
The other core concept of fieldwork is discussed in the next section.
3.6 Methodology
The methods used from ethnography to collect data were fieldwork, secondary data,
participant observations, semi-structured interviews and journal/diary.
65

3.6.1 Fieldwork
Primary data collection in ethnography is undertaken through fieldwork. Fieldwork is
one of the core traits of ethnography. Wolcott’s (1995) described fieldwork as:
“A form of inquiry that requires a researcher to be immersed personally in the
ongoing social activities of some individual or group carrying out the research.” (p. 3)
According to Roper and Shapira (2000), ethnography is a process of learning about
people by learning from them. An insider’s view is obtained to understand the
phenomenon investigated in its natural context. For this study, 63 days (472.5 hours)
spread over three months were spent in the Trust collecting data related to
disciplinaries, as outlined earlier in Figure1 in section 3.1.
Being in the field allows the researcher to observe, ask questions and compare what
people say they do with what they actually do in their work settings. Watching what
happens in the moment and noting the subtleties, congruence and incongruence of
verbal and non-verbal communication first-hand lie at the heart and strength of
ethnography (Lambert et al., 2011). Being in the field allows the researcher to
experience the culture and witness how people relate to, perceive and construct their
social world (Reeves et al., 2008). Tacit and latent information is revealed. Research
methods such as surveys, questionnaires and interviews do not capture this valuable
data.
Ethnographic research is produced by the quality of the relationship between the
researcher and participants through emic and etic viewpoints.
66

3.6.2 Emic and etic perspectives
The important theoretical concepts of emic and etic were derived from the works of
Kenneth Pike, a linguist, and Marvin Harris, an anthropologist. Using emic and etic
approaches in ethnography reveal different perspectives when the same
phenomenon is being investigated and analysed by the researcher from the inside
and the outside (Brown, 2003).
Emic research is undertaken inside the group to investigate the culture of systems,
whereas the etic approach is conducted outside the group through observing the
actions and behaviours of people in their natural settings. The emic method
considers the views of members of the group; in this study it was the various
employees involved in the disciplinary process as they held specific knowledge,
values, beliefs and experiences. In addition, the emic approach allows the researcher
to access and uncover spoken and unspoken rules and rituals of the culture
(Holloway and Todres, 2010).
The emic approach in ethnography allows the researcher to observe and investigate
the subjective reality of the insider. Where there are people from diverse ethnic and
racial backgrounds linked to a specific situation, such as disciplinaries, multiple truths
and realities exist. These subjective realities might not conform to the reality, norms
and conventional values and beliefs of the majority culture (Fetterman, 2010). Issues
around the differences in roles, relationships and dynamics between employees not
apparent to the outsider become evident to the researcher on the inside. The
dynamics that occur in and from these complex and configured relationships on
many levels in people’s working lives can highlight issues of power, authority,
inequality, control and conflict, and how they affect the culture of teams, groups and
67

the organisation involved in a specific situation (Smith, 2001). The role of critical
ethnography is also taken into account here.
For the purpose of reflexivity (which is described in section 3.12), the position of
having a connection with the Trust before commencing the study was considered.
The impact of this as an insider and outsider during the collation of data was
reflected on in my research journal/diary. These aspects, together with field notes
made during participant observations, were discussed with academic supervision.
The work of Bonner and Tolhurst (2002) was considered. The benefits and the
drawbacks of insider and outsider were closely monitored. As an insider, the
following benefits were noted: I had some awareness beforehand of how the Trust
performed; relationships with some employees (in my role as a university lecturer)
were already ascertained; with rapport and trust already established in some parts of
the Trust, disruption could be minimised, particularly during participant observation.
The potential disadvantages considered were: the focus of the research could be lost
by having too much affinity and closeness with research participants; ‘over-familiarity’
of the Trust might lead to making assumptions and subtle data being overlooked;
conflict in my roles and responsibilities as a lecturer and researcher.
Although I was known in some parts of the Trust, I was unfamiliar with the areas and
personnel involved in the disciplinary process. From an etic perspective, this had
benefits: knowing little about a specific culture, situation or event allowed some
research participants to share personal information with myself as I was perceived as
being impartial and not as a threat; subtle differences were observed and routines
that were taken for granted by research participants were sensitively discussed to
seek further clarification. However, the disadvantage of being an outsider and based
68

within the HR department aroused some speculation about impartiality and trust. As
participants were observed in the field, they could feel they were being inspected,
judged and might not conduct themselves naturally in the presence of the researcher
(Dixon-Woods, 2012). From the onset, the study was presented as the initiative and
sole property of the researcher. Potential recruits were informed the research had
undergone scrutiny by the Trust and university ethics committees to ensure the
identity of participants would be protected.
In undertaking ethnography, the researcher needs to strike a balance of being an
‘insider’ and ‘outsider’ (Bonner and Tolhurst, 2002). As part of reflexivity, the position
of the researcher needs to be monitored in academic supervision as this can affect
the quality of data collection and analysis.
3.6.3 Secondary data
In traditional ethnography, the use of written material and documents is overlooked.
Hammersley and Atkinson (2007, p. 128) stated:
“It is easy (but wrong) to assume that the spoken account is more ‘authentic’ or more
‘spontaneous’ than the written.”
They later asserted (p. 129):
“There is still, apparently, a tacit assumption that ethnographic research can
appropriately represent contemporary social worlds as essentially oral cultures.”
Secondary data refers to existing data (Dixon-Woods, 2012). On face value, existing
data is valuable as this provides initial insight into the depth and extent of the
phenomenon being investigated and how the organisation represents this issue and
69

themselves in the public domain (Atkinson et al., 2001). For the researcher, written
material in formal and informal texts allows access to the social world and provides
another piece of the jigsaw regarding the context, structure and purpose of the
organisation in relation to meeting its tasks to manage employees who have
transgressed. Existing information available online to the general public provided a
surface picture of the culture of the organisation and the size of phenomenon. Insight
into the opinions of employees, particularly diverse and marginalised groups, was
obtained from Care Quality Commission (CQC) reports, NHS staff surveys and
statistics around disciplinaries.
This gathering of available secondary data online helped to identify gaps, generate
the research question and decide on the methodology to investigate the
phenomenon. Once permission and ethical clearance were given to collect data in
the Trust, existing written information not available to the general public and wider
staff on disciplinaries was attained. Documents related to the over-representation of
BME in disciplinary hearings were also obtained, some more easily than others.
These included: the Race Equality Scheme (RES); minutes of the RES; Equality and
Diversity Framework; Trust Interim Equality Objectives; Service and Workforce
Equality Report particularly on the descriptive statistics around disciplinaries; Trust
Board meetings where E&D issues were discussed; NHS Staff Survey for the Trust;
previous audits into disciplinaries; draft action plans; quarterly Trust magazine; and
information from the Trust intranet.
The validity, use and value of this written data needs to be considered and then
triangulated with other methods used to obtain findings (Roper and Shapira, 2000).
70

3.6.4 Participant observation
As with ethnography, there is no single agreed definition of participant observation
(Savage, 2000). Polit and Beck (2012) exemplified participant observation as:
“Periods of intense social interaction, between the researcher and participant, in the
participant’s socio-political and cultural milieu.”(p. 544)
Participant observation in ethnography has its origin in anthropology (Watson et al.,
2010) and is increasingly used as an instrument to produce more in-depth knowledge
of a culture in healthcare research (Holloway and Todres, 2010). Observation and
participation are another hallmark and core activity of ethnography allowing the
researcher an opportunity to immerse in the lives of others and describe how
participants perceive their world (Emerson et al., 2001) by looking, listening and
asking questions (Roper and Shapira, 2000). Participant observation is used to
investigate the social life of people in their natural setting. The researcher is looking
through the cultural lenses (Streubert and Carpenter, 2011) of the participant and
putting aside their own perceptions and assumptions. An insider’s experience is
looked for. What is ascertained from participant observation in ethnography is
summarised by Mack et al. (2005, p. 14):
“Participant observation is also useful for gaining an understanding of the physical,
social, cultural and economic contexts in which study participants live; the
relationships among and between people, contexts, ideas, norms and events; and
from people’s behaviours and activities – what they do, how frequently and with
whom.”
71

Gold (1969) stressed that there are four levels of observation detected in
ethnography:
1. Complete participant – the researcher fully participates in the activities and
observations might be done with or without the group’s or individual’s knowledge.
Examples for this study were engaging with employees during informal and
unstructured times such as lunchtimes, before and after meetings;
2. Participant as observer – most of the time by the researcher is spent participating
in activities of those being observed with less time spent on formal observations.
Examples for this study were attending meetings covering workforce issues;
3. Observer as participant – participation by the researcher is brief with most of the
time spent observing activities and people. Examples for this study were
predominantly in meetings when employment matters relating to disciplinaries
were discussed;
4. Complete observer – the researcher just observes people, behaviours,
interactions or events and had no interactions with the observed. Examples for
this study were attending Trust Board meetings and a formal disciplinary hearing.
Researchers move between these levels and generally occupy the ground of
participant as observer and observer as participant. The levels of participant
observation undertaken are not always linear and depend on the role, position and
situation of the researcher. Balancing and combining the roles of observation and
participation in ethnography and how passive or active the researcher should be can
be confounding. The level of trust, rapport and connectedness depends on the length
72

of time the researcher is immersed in the field and the relationships that are formed
with participants.
Spradley (1980) identified three types of observation: descriptive observation is
undertaken at the start of the study when the ethnographer enters the social situation
to gain an overview and find out what is going on; focused observation concentrates
on selected events and interactions related to the aims of the research; selective
observation looks at specific features of activities, processes, culture and people.
For this study, participant observations were undertaken in the following areas within
the Trust:
Disciplinary hearing x 1;
Trust Board meeting x 1;
BME Staff Group x 3;
E&D Group (quarterly meeting) x 1;
Race Equality Steering Group (quarterly meeting) x 1;
Workforce Equality Group (quarterly meeting) x 1;
Senior Nurses Forum x 1;
Trust executive leaving event.
3.6.5 Interviewing
Informal conversations and formal in-depth interviews allow the researcher
opportunities to gain further clarification, understanding and meaning of behaviours
73

and language that might not be comprehensible during participant observation
(Holloway and Todres, 2010). Interviews have the ability to describe, explain and
explore subjects from the participant’s stance (Tod, 2010).
Within the definition of ethnographic interviewing, Heyl (2001, p. 369) stated:
“Researchers have established respectful, on-going relationships with the
interviewees, including enough rapport for there to be genuine exchange of views
and enough time and openness in the interviews to explore purposefully with the
researcher the meaning they place on events in their world.”
This definition differentiates ethnographic interviewing from other types of interviews
by empowering participants to focus in their own language on cultural meaning of
actions and events. Participants are in a position to share personal experiences of
their interpersonal relationships and the cultural value they encounter in their daily
lives. To achieve this task, the interviewer needs to spend a considerable amount of
time building a rapport and relationship with participants. The concept of rapport
generates mutual respect, empathy and understanding so a safe space can be
created for the participants to share their viewpoints (McGarry, 2006). This, in most
cases, was achieved as some participants were able to share their perceptions and
feelings around disciplinaries openly and frankly. However, owing to the limited time
spent in the field, it was difficult to do follow-up interviews, as is discussed further in
section 8.3.
3.6.5.1 Semi-structured interviews
After observations, interviews in ethnography are an important source of information
to gather understanding and subjective meaning (Fetterman, 2010). For this study,
74

27 semi-structured interviews were undertaken with employees directly involved in
the disciplinary process. Semi-structured interviews are commonly used in
ethnography (Fetterman, 2010). Pre-determined questions and themes within an
interview guide were used. This flexible framework allowed the researcher to vary the
wording and order of the questions to suit each interview (Dearnley, 2005). Open-
ended questions allow the researcher to explore further issues with the participant
that arise on their own accord and that have not been anticipated (Doody and
Noonan, 2013).
3.7 Selection, recruitment and undertaking interviews with
participants
This section looks at how employees were chosen for the semi-structured interviews.
3.7.1 Selection – inclusion and exclusion
Having identified the issue to investigate and gained access to the site, consideration
was given to selecting and recruiting employees from the Trust to participate in the
study. Fetterman (2010) identified two methods: choose who and what not to study;
select who and what to study. To manage, carry out and investigate the phenomenon
realistically under the time constraint, ‘purposive sampling’ (Polit and Beck, 2012)
was used to select employees, events, settings and documents associated with the
disciplinary process.
The eligibility criteria (Polit and Beck, 2012) were that participants should be Trust
employees and able to give informed consent. These included all types of employees
in different roles and positions; both male and female; from white and BME
background; and involved in the disciplinary process.
75
The exclusion criteria (Polit and Beck, 2012) included employees unable to give
informed consent and where, through participation, there might be adverse effects to
their well-being.
3.7.2 Recruitment
After selecting the type of participants to be interviewed, attention was paid to
recruiting volunteers. Once ethical approval had been granted, time was spent
disseminating the study in the Trust. A synopsis of the study was put on the Trust
website with contact details. Employees were contacted by email and telephone.
Attached to the initial email were the invitation letter (Appendix 2), participation
information sheet (Appendix 3) and consent form (Appendix 4). Follow-up face-to-
face meetings were arranged to discuss the research with staff expressing interest in
the study. Presentations were also made to the Senior Nurses Forum, E&D Group,
BME Staff Group and the Race Equality Steering Group to discuss the nature and
purpose of the study. After the presentation, time was set aside to answer questions.
Written details of the study were also provided for interested staff to look at the
details of the research at their leisure. Reactions to the study and resulting
behaviours noted during participant observations are highlighted in sections 6.3.5
and 6.3.6.
3.7.3 Special measures taken for employees who had been investigated
Recruiting potential participants who had disciplinary action brought against them
was given further consideration. The UREC asked for special measures to be taken
when approaching and recruiting these employees. In this instance, to minimise
further distress and harm, the researcher did not directly contact the employee.
76

Instead he liaised with a third party (the TU representative) who was directly involved
in the disciplinary process and could pass on the details of the study.
This sampling method, known as ‘snowballing’ where one person (i.e. the
researcher) finds another (i.e. the TU representative), is useful with those who are
difficult to recruit (Streubert and Carpenter, 2011).
Relying on TU representatives to pass on details to employees who had a
disciplinary action initiated against them had drawbacks. Officials admitted that
details were not always passed on as they would ‘forget’. Employees under
investigation and without TU representatives could not be contacted to participate in
the study.
3.7.4 Undertaking interviews
To reiterate, employees who were interested in participating in interviews were given
the invitation letter, participant information sheet and consent form. The interviews
with willing participants were conducted at a time that suited their convenience and a
place where they felt safe. Some interviews took place in participants’ offices. Before
the interview was conducted, the information given was again discussed, queries
answered and, if the employee was satisfied to continue, the consent form was
signed. The interviews on average lasted up to one hour. Approaches to promote
diversity and antidiscrimination practices during interviews are discussed under 3.12.
3.7.5 Outcomes from the interviews
There were 27 participants who volunteered to be interviewed for this study. They
included: employees under investigation; members of the disciplinary and appeals
panel; investigating officials and support; TU representatives; witnesses; and
77

members of various groups where workforce issues related to disciplinaries were
discussed. For reasons of ethics (see section 3.11), the specific roles and positions
of participants involved in the research are not identified in this study.
3.8 Data recording
For this study, field notes, fieldwork journal/diary and transcriptions of interviews
recorded on digital audio equipment were used. The digital audio recorder was only
used for the interviews with prior consent.
3.8.1 Field notes
Field notes are a conventional technique used in ethnography to document data.
Handwritten field notes were used for participant observations and interviews where
audio recording was deemed unsuitable and could hinder meaningful dialogue and
interaction with participants. Undertaking field notes is a selective process as it is not
possible to encapsulate everything. Hammersley and Atkinson (2007) suggested
when to write field notes and what to write down are significant when data is being
collected.
1. When to write down – the timing of writing down notes can impact on the
situation. Participants can become self-conscious when notes are recorded. This
distraction can disrupt and affect the natural flow of interactions and generate
mistrust. In some meetings, I could not write anything down as participants were
sitting next to me and observing what information I was writing on my notepad. In
these situations, detailed field notes were made as soon as possible after the
meeting had ended;
78
2. What to write down – attention needs to be paid to the form and content of what
is documented. Owing to the mass of data accumulated for this study, selection
had to be made between breadth and depth of notes, capturing significant
events, experiences and interactions in the field (Emerson et al., 2001). In this
study, I recorded significant events related to disciplinary matters in my field
notes. Some field notes from participant observations related to the physical
environment, the mood and atmosphere of the setting, seating arrangements, the
level and depth of interactions and non-verbal behaviours. This information could
not be captured by audio digital recordings (Gibbs, 2007). Depending on the
situation, written information ranged from detailed actual words to jotting down
key phrases and words. Chapter 6 will discuss data collected from field notes.
3.8.2 Digital audio recording
Undertaking the traditional method of pen and paper during long interviews has its
pitfalls as the finer details and focus can be lost. A digital audio recorder was used
when participants consented to its use during semi-structured interviews. As well as
assuring the accuracy of capturing the interview verbatim (Gibbs, 2007), this could
allow active engagement and listening by the researcher so additional questions
could be formulated and asked (Roper and Shapira, 2000). However, being recorded
can hinder participants from speaking in a frank and open way.
After the interviews, the recordings were transferred into a password-protected
computer and erased on the audio digital recorder. Each interview was fully
transcribed and on completion was double-checked by reading the transcript in
conjunction with listening to the interview for accuracy.
79

3.8.3 Fieldwork journal/diary
In addition to field notes, a separate fieldwork journal/diary was kept during the
research. For reflexive purposes, it was important to examine aspects of my own
subjective lived experience and the potential impact this had on the study so biases
and prejudices could be identified and addressed (Emerson et al., 2001). This
journal/diary captured emerging ideas, gut reactions and reflections of my own
thoughts and feelings. This material was considered in the context of the study. For
example, when I felt despondent about senior managers showing a lack of interest in
the study, I associated this to various initiatives from the E&D agenda such as the
RES and the Equality Delivering System being on the periphery of the Trust. The
E&D agenda, as discussed in section 6.3.4, was not embraced by the Trust Board
and had little impact to the working lives of BME staff. Adopting this approach
allowed me space to be objective, avoid becoming stuck and not to take issues
personally.
3.9 Data analysis
Having collected data from the field, participant observations, transcribed interviews
and documentary sources, the next stage involved analysing this data. There is no
single agreed method or a ‘once size fits all’ approach for analysing data in
ethnography (Angrosino, 2007). The collection and analysis of data in ethnography
simultaneously starts in the field at the outset. This continues in order for additional
investigations to be carried out to address questions that have not been anticipated
so that further data can be collected as the research progresses (Rebar et al., 2011).
Ethnography aims to explain the culture. Identifying cultural themes involves careful
scrutiny of the data collected. Analysis involves looking for patterns in behaviour,
80

thoughts and the rules of the group studied. The analysis proceeds to an overview of
what people believe and how they behave in their social setting (Roper and Shapira,
2000). Latent patterns become clearer in understanding the culture in relation to the
phenomenon investigated (Polit and Beck, 2012).
3.9.1 Thematic analysis
For this study, thematic analysis devised by Braun and Clarke (2006) is used to
examine the data. They defined thematic analysis: “as a method for identifying,
analysing and reporting patterns (themes) within data” (p. 6). Their framework has six
phases, which are:
Phase 1: Gaining familiarisation by reading and rereading the data so that depth and
content are attained. Through this process ideas and patterns begin to emerge;
Phase 2: Generating initial codes to arrange the data into meaningful categories;
Phase 3: From all the data that has been coded and collected, overarching themes
are revealed;
Phase 4: Reviewing themes that support the data;
Phase 5: Defining and naming each theme;
Phase 6: Producing the scholarly report.
This qualitative research tool provides a flexible approach to evaluate areas that are
under-researched. Thematic analysis is not dependent on specialised theory. How
thematic analysis is applied to findings uncovered will be discussed in the next
section.
81

3.9.1.1 Presentation of findings from the data collected
Having spent time in the field, vast amounts of data was accumulated. The next task
was to structure and analyse the data and then present the identified themes. The
data analysis was considered in the context of focused and critical ethnography. It
involved interpreting and examining: the impact of political, social, economic and
historical forces permeating into the Trust; the various cultures operating in the Trust
where disciplinaries were taking place; the diverse staff group employed and their
experiences of being in the Trust; the phenomenon under investigation; the multiple
realities of the vast range of employees involved in the disciplinary process; the
relationships, structures, systems and processes involved in disciplinaries. The
purpose of adopting this approach was to begin to identify and understand the key
factors for the disproportional representation of BME employees involved in the
disciplinary process in the Trust.
To aid this process, thematic analysis devised by Braun and Clarke (2006) was used.
After the data was collected, time was spent to familiarise myself with the data
corpus from the interviews, participant observation, field notes and secondary data.
For the semi-structured interviews (that made up most of the information collated),
careful attention was given to active listening of the recorded interviews in
conjunction with active reading of the transcripts, so depth and breadth could be
obtained from the data. This lengthy, complex, challenging and absorbing process
was repeated many times to draw out and define the themes.
Not all the information from the data corpus was used in this study. For this study, the
data set refers to all the data presented for the phenomenon investigated. The data
82

item is each interview, participant observation, journal/diary or secondary data
utilised to make up the data set. Once the data set had been extracted from the data
corpus manually, overarching themes were identified, reviewed, refined and coded.
To ensure validity, rigour and reliability of the analysis, methodological and data
triangulation was used. All the data collection methods were used in the analysis.
The data collected from the interviews, participant observations, field notes,
journal/diary and documents were then compared and contrasted to determine the
themes and multiple realities related to the phenomenon. As most of the data was
collected from interviews with participants occupying different roles and positions,
multiple realities and perspectives were captured and reported.
Overarching themes are identified and presented in this chapter and summarised in
Table 1 in section 6.7: the context of the Trust; perceptions of BME employees in the
Trust; perceptions of the disciplinary process; perceptions of employees directly
involved in the disciplinary process. Each of the four themes has sub-themes.
Issues did arise from applying thematic analysis to determine and present the
findings. With the vast quantity of data collected, it was overwhelming, particularly
around how best to proceed. Observance of maintaining objectivity of the data
collected and not making premature interpretations before all the data was analysed
was closely monitored. Academic supervision over this period was invaluable.
3.10 Triangulation
To test the quality of the data gathered, triangulation is commonly used as a tool in
ethnography. Triangulation is a principle used in surveying land (Gibbs, 2007). This
metaphor is used in ethnography where a phenomenon is analysed from different
83

perspectives (Rebar et al., 2011). Two or more methods are used to substantiate the
findings from one source with the other (Simons and Lathlean, 2010). The application
of multiple strategies provides a more holistic and improved understanding of the
phenomenon and improves the validity and reliability of the data (Streubert and
Carpenter, 2011).
Relying on a single method can limit the scope and depth of the study (Hammersley
and Atkinson, 2007). For this study, methodological and data triangulation were
used. Methodological triangulation is when the methods used to collect the data are
compared and contrasted to offer a thorough insight into the phenomenon
investigated (Reeves et al., 2008). In this study, field notes, participant observations,
interviews, journal/diary and secondary data are weighed against each other during
data analysis. Data triangulation involves using a range of data sources from different
settings (Simons and Lathlean, 2010). Data collected from various employees
occupying different roles and positions in the disciplinary process are examined.
Their experiences were compared and contrasted so that multiple realities related to
the phenomenon in the Trust could be obtained.
3.11 Ethics
The research governance in the UK seeks, promotes and maintains high standards
of research (Griffiths, 2008). The design, methodology and how the research is
undertaken must be rigorous, transparent and trustworthy (Johnson and Long, 2010).
All research conducted in the NHS requires ethical approval to safeguard participants
from risk and harm. The purpose of an ethics committee is to ensure and maintain
the legal rights of research participants and the following principles are strictly
84

observed: autonomy; informed consent; dignity; non-coercion; privacy; confidentiality;
and non-maleficence (Griffiths, 2006 and 2008).
The research proposal did not need to be approved by the National Research Ethics
Service (NRES) as the study did not involve patients and carers. However, the
proposal needed to be approved by the UREC and the Trust’s own R&D ethics
committee. The submission of the first application to the UREC was rejected as it
wanted: the number of samples to be increased; clarification about anonymity of staff
who had been through the disciplinary process and were willing to participate in the
study; amendments to the structure of language on the patient information sheet;
clarification of how employees who had been investigated under the disciplinary
process would be approached. These issues were addressed and the proposal was
then accepted by the UREC. With the amendments incorporated, the Trust’s R&D
ethics committee also accepted the proposal.
Measures were put in place to safeguard participants. It was anticipated that
particular issues around a discomforting and sensitive subject could arise for the
Trust and employees participating in the study. During one interview a participant
became emotional. A break was taken until the participant was ready to continue. On
their return, the participant stated they were aware they could withdraw from the
study but wanted to continue with the interview.
For ethical reasons related to protecting the anonymity of the Trust, its employees
and groups, the identities, roles and backgrounds have not always been disclosed in
this study as some of the employees could be easily identified. Deductive disclosure
takes place when groups and individuals could be identified in research reports
85

(Kaiser, 2009). The breach of confidentiality and anonymity by deductive disclosure
is a concern of the researcher as ethnographic studies contain a wealth of personal
experiences and opinions about research participants and groups. The concerns are
that research participants could potentially face negative consequences if their
identities are exposed. Each participant in this study was given an identification
number so their anonymity was protected and details of their participation were
stored in locked filing cabinets and password-protected computers. This was to
minimise potential harm and uphold the principle of non-maleficence.
3.12 Reflexivity
Reflexivity is a significant feature of ethnography in assessing the quality and rigour
of the research process. Cruz and Higginbottom (2013) stated:
“Reflexivity is focussed on making explicit and transparent the effect of the
researcher, methodology and tools of data collection on the process of the research
and the research findings.”(p. 42)
Researchers come into the field with their past experiences, prejudices, culture,
attitudes and belief systems intact. If these factors are not monitored and critically
scrutinised, they can inevitably impact on the investigation and ultimately the findings
of the study. To minimise biases, reflexivity as a critical self-reflection process is
undertaken (Vandenberg and Hall, 2011). In the course of this self-examination, the
researcher is constantly enquiring about the effect on the process and outcome of
the study and the research on the researcher (Pellat, 2003). In particular, attention is
given to the potential effects of the interpersonal dynamics in social situations. The
researcher’s own position of power and privilege needs to be considered and brought
86

to the fore. These dynamics can influence how the data is collected and analysed
(Walker et al., 2013).
In the field notes, connections with the Trust and the impact of this relationship
before the start of research have already been acknowledged in section 3.6.2.
Reflecting on the relationship was important in that the role adopted for the research
was different to my previous roles and responsibilities occupied in the Trust. To
support my position as a researcher, a sabbatical was obtained to concentrate solely
on the study. In introductions at formal and informal meetings, I stated my role of
‘honorary researcher’, which was further reinforced and displayed on the identity
badge worn and visible at all times.
Consideration was also given to being a male, coming from a BME background and a
migrant from a country that was once ruled by Britain during the course of this study.
The motives for carrying out a politically charged study were reflected on in my
journal/diary. My knowledge, experience and clinical skills as a mental health nurse
and a qualified psychotherapist were utilised in the study. Aspects of self-awareness
were brought to the fore. My behaviours, thoughts, emotions and fantasies were
frequently checked before, during and after interactions with participants and the time
spent in the Trust collecting data. This was to monitor distractions as I did not want
these to influence how I was observing, participating, listening and reporting during
the collection and analysis of data. For example, what was analysed from participant
interviews needed to be separated from my own perceptions, subjectivity and
partiality.
87

For this study, attention was also paid to: not homogenise BME and white
employees; look beyond ‘black versus white’ dynamic; allow for differences to
emerge within and between the different BME participants and groups. To help,
Papadopoulos and Lees’ (2002) model of cultural competence in research was
incorporated in the study. Through cultural awareness, my own personal values,
beliefs, attitudes and prejudices and how these might impact on the research process
were closely examined and reflected on. Coming from a Sikh background, the
historical aspect of Sikhs having been at war with Muslims and the British in the past,
was taken into account. It was important that historical conflicts on my part were not
subtly played out when engaging with Muslim and British participants. I was also
aware of how Sikhs in East Africa (where I was born) had subjugated black people in
their own homelands. Cultural knowledge was also reflected on. I realised my
limitations, that I was not always aware of every cultural nuance, particularly with
staff from the vast continent of Africa. I avoided making stereotypical assumptions
and was aware there was no such person as a ‘black African’. This allowed me to
reflect on the difference, similarities and inequalities between and across ethnic
groups. Through cultural sensitivity, power relationships and potential oppressive
practices, my interactions with participants were closely monitored. For example: I
always asked participants where they wanted to be interviewed so they had the
choice to be in a safe and comfortable environment; I took into account the age,
disability, gender, sexual orientation (as openly revealed by one participant), race,
culture and religion of Trust employees. In my interactions, I was careful not to agree,
disagree, collude and offer interpretations to what participants were reporting. Where
possible I tried not to interrupt and allowed for silence to prevail. Attention was given
to the non-verbal cues and verbal communication in order to maintain a non-
88

judgemental stance. During the interviews, consideration was given to the physical
environment such as the decor, lighting, seating arrangement and gender
positioning. When participants were happy to come to a venue of my choice, identical
chairs were selected. On entry to the room, I gave the participant a choice of which
chair to sit in. A small table with a box of tissues was placed in the room just in case
someone became upset. When I was invited by participants to be interviewed in their
offices I was always aware where I was asked to sit. There were several occasions
where the participants being interviewed sat behind big desks. All these participants
were white managers. On a couple of occasions, participants answered their
telephones or responded to people who were knocking on their doors during the
interviews. On one level, as recorded in my journal/diary, I found this behaviour
irritating and had to be aware not to react. On another level, I considered this
behaviour in the context of the study and related this to the lack of authentic
engagement and commitment from managers regarding E&D issues and how they
perceived BME staff in the Trust.
Regular academic supervision was also undertaken with two supervisors who were
outside of the Trust and in a position to challenge the positionality of the researcher.
3.13 Summary
In this chapter, the methods adopted from ethnography to achieve the study aims
have been presented and discussed. Rationale to explain why focused and critical
ethnography were used has been provided. Obtaining ethics and gaining access to a
Trust and the ethnographic methods of fieldwork, participant observations, interviews
and secondary data used to investigate the over-representation of BME staff involved
in the disciplinary process have been highlighted. The process of analysing the data
89

through thematic analysis has been outlined. To improve the quality and validity of
the data and minimise bias, triangulation and reflexivity have been discussed.
90

Chapter 4: Descriptive statistics
4.1 Ethnic profile of the population the Trust serves
The most recent (2009) figures of the ethnic profile of the local population served by
the Trust are presented in Figure 1. Most of the served population is white
comprising white British, white Irish and other white background. When the 2009
ethnic profile of the local population is compared to that of staff working for the Trust
in 2011 (Figures 2 and 3), there are some notable features: 80.1% of the local
population is white compared to 54% (1305) of white staff working for the Trust;
18.5% of the local population are from BME backgrounds compared to 38% (918) of
BME staff. If the Trust staff figures are further broken down to specific ethnic groups
and comparison is made between the local population and those staff groups,
notable aspects are observed: 5.6% of the local population are black compared to
27% of black staff; the percentage of the local population of Asians compared to
Asians working in the Trust is similar – 9%.
91

Figure 1: Population served by the Trust – 2009 (data source: Census, Office for
National Statistics, 2009)
However, making comparisons between the percentage of the ethnicity of the 2009
local population and that of the staff employed in 2011 by the Trust, needs to be
treated with caution as there is no information currently available of how many Trust
staff also live among the local population served by the Trust.
4.2 Workforce profile
There is only descriptive statistical data available for 2011 and 2012 and none for
2008 to 2010. During 2011 the total workforce of the Trust was 2416. Note that
figures in parentheses indicate number of Trust staff.
92

4.2.1 2011 profile
Figure 2: Ethnicity profile of staff
As shown in Figure 2, 54% (1305) of staff employed by the Trust come from a white
background and38% (918) from BME groups. In Figure 3, the percentage of each
group has been further broken down.
Figure 3: The ethnicity and percentage of each group
White British are the largest group of staff within the Trust (991 and 42%) and black
African staff are the largest group (459 and 19%) within the BME workforce.
93

Figure 4: Ethnicity of occupational staff groups
Within the Trust, BME staff comprise the largest group within ancillary, nursing,
HCAs/support staff and other medical roles. White staff prevail in the positions of
consultants, senior management, allied health professionals (AHP), AHP assistants,
psychology and psychotherapy.
94
Figure 5: Registered nurses (693)
Within the role of nursing, BME staff represent over 60% (423) of this professional
group.
Figure 6: Registered nurses – ethnicity and banding
In 2010, Agenda for Change paybands and gradings were introduced in the NHS.
Newly qualified registered nurses start at band 5 and progress to band 8, which is
divided into four bands – a, b, c and d. As the graph clearly shows, the number of
BME nurses declines as they progress through to the higher bands. With the white
95

nurses, the proportion of numbers increases as nurses move up the banding
hierarchy.
Figure 7: Ethnicity of HCAs/support staff (349)
There is a higher proportion of BME staff within the HCA and support staff role
relative to the numbers of BME people in both the Trust 2011 workforce and the 2009
local population served by the Trust. This is reflected in the higher numbers of BME
HCAs and support staff from bands 2 to 5 (see Figure 8).
96

Figure 8: Ethnicity and banding of HCAs/support staff (349)
In comparison to 2011, the workforce numbers decline slightly from 2416 to 2330 in
2012. The Trust has also changed its presentation of data in its 2012 Service and
Workforce Equality Report. This will be reflected on in chapter 7.
97

4.2.2 2012 profile
Figure 9: Ethnicity profile of staff
In comparison to the previous year, there is no change in the number of staff from a
white background. There is a 2% increase in the numbers of BME staff employed by
the Trust. As described earlier, 80% of the 2009 local population served by the Trust
is white (Figure 1); however, this group makes up 54% (1258) of the Trust 2012
workforce. The opposite picture is found when the black population is examined.
Although 5.6% of the local population is black, this group has risen to 26% (606) of
the Trust 2012 workforce. Asians make up 9% (210) whereas others represent 6%
(140).
In Figure 10, the ethnicity of non-medical and non-nursing staff is shown. Overall the
percentage of white staff increases as they progress up the bands. The opposite is
observed for black staff whose numbers decrease. For other BME groups, the
proportions are too small to make significant comments.
98

Figure 10: Ethnicity of non-medical staff and non-nursing staff (bands 1–5)
In Figure 11, there is a higher percentage of white staff in each band in comparison
to BME staff.
Figure 11: Ethnicity of non-medical staff and non-nursing staff (bands 6–9)
99

In comparison to the 2011 figures, the Trust has grouped together HCAs and
registered nurses in its 2012 Workforce Equality Report. This will be reflected on in
chapter 7.
Figure 12: Ethnicity of nursing staff (bands 2–4)
Within Figure 12 significant differences are noted. The numbers of BME nursing staff
decreases from bands 2 to 4. There is a reverse trend for white staff.
A similar pattern emerges in Figure 13 with the proportion of white staff increasing in
numbers and a reverse trend occurring for BME staff moving up the banding
hierarchy.
100

Figure 13: Ethnicity of nursing staff (bands 5–8c)
In Figure 14, higher proportions of white staff occupy each medical staff group apart
from specialist registrars and staff grade.
Figure 14: Ethnicity of medical staff
101

4.3 Disciplinaries
The total workforce number in the Trust was 2330 for 2011 to 2012. There were 56
disciplinaries during that period, that is, 2.4% of the total workforce (Figure 15).
Figure 15: Disciplinary figures from 2008 to 2012
When comparison is made about the number of disciplinaries from 2008 to 2011,
there has been a slight decline. From 2011 to 2012, there was an increase in the
number of disciplinaries at a time when there was a small decline in the total
workforce in the Trust.
Figure 16: Ethnicity of disciplinaries from 2008 to 2009
102

In Figure 16, the outcome of each category for 2008 to 2009 is broken down by
ethnic group. During this period there were 37 disciplinaries. Of these, 12 (32%) were
people who reported their ethnic background as white (British or other) and 25 (68%)
were from BME backgrounds. Data for the type of BME group was not available from
the Trust. In terms of the outcome of each disciplinary, no formal action was taken for
18 of these, action was taken outside of the disciplinary process for five individuals,
four people received a first written warning, five staff received a final written warning
and five were summarily dismissed. For four of these outcome types (no formal
action, action outside the process, final written warning and summary dismissal), the
number of BME individuals is higher in each group.
Figure 17: Ethnicity of disciplinaries from 2009 to 2010
From Figure 17, BME employees involved in the disciplinary process receive higher
levels of sanctions in comparison to their white counterparts in the following areas:
final written warning, dismissal, summary dismissal and resignation.
103

Figure 18: Ethnicity of disciplinaries from 2010 to 2011
From Figure 18, there is a noticeable difference in the number of BME staff receiving
final written warnings and summary dismissals in comparison to their white
counterparts facing disciplinary action. In other areas of no formal action, first written
warning, dismissal and resignation, there is no difference between the two groups.
104

Figure 19: Ethnicity of disciplinaries from 2011 to 2012
In comparison to the previous four years (2008–2011), there has been an increase in
the number of staff involved in the disciplinary process; 80% of BME staff went
through the disciplinary process. For the first time, data for suspension of staff is
reported in the Workforce Equality Report. BME employees are suspended almost
three times more than white staff (21:8). Sanctions of first written warning, final
written warning and summary dismissal are higher for BME staff in comparison to
white employees.
105

Figure 20: Disciplinaries in terms of banding from 2011 to 2012
Before the publication of the Trust’s Workforce Equality Report, the Director of
Workforce and Deputy Director of HR stated that disciplinaries undertaken in the
Trust were at a lower banding. These figures reveal three times as many staff from
bands 5 to 8 are involved in the disciplinary process than employees from bands 1 to
4. However, the ethnic profile of these staff is not available from the data.
4.3.1 Reasons for disciplinary action
The types of issues, which have emerged over the past four years, that have resulted
in disciplinary action could be categorised as: unprofessional behaviours towards
colleagues; unprofessional behaviours towards patients; misconduct; other.
4.4 Conclusion
The population served by the Trust is predominantly white. Some areas have a
higher proportion of BME groups than white groups. In the Trust, the gap between
106

white and BME groups has narrowed in the workforce. Black Africans are the largest
group within the BME group. Within nursing, HCAs/support staff and ancillary
occupations, BME staff comprise the largest groups. There are more white staff in
the position of consultants, senior management, AHPs, psychology, psychotherapy
and AHP assistants.
The numbers of BME nurses declines as they progress to the higher banding. There
is an opposite trend for white staff in nursing. A similar picture between BME and
white staff appears in medical, non-medical and non-nursing groups. For HCAs and
support staff, there is a higher proportion of BME employees.
There is a slight decline in disciplinaries from 2008 to 2011. From 2011 to 2012 there
is an increase in disciplinaries. During this period, there is a slight decline in the
numbers of staff employed. In each of the categories white staff never exceed their
BME counterparts.
Suspensions and bandings appear for the first time in 2011/2012. There is a higher
proportion of BME staff suspended in comparison to their white counterparts. Also,
more staff are disciplined in bands 5 to 8 than 1 to 4. More BME staff are put through
the disciplinary process than white staff. BME employees receive more first and final
warnings and summary dismissals than white staff.
107

Chapter 5: Observation of a disciplinary
hearing and interviews with three employees
involved in the case
5.1 Introduction
This chapter focuses on the findings taken from field notes of an observed
disciplinary hearing and interviews with three of its participants. The researcher did
not have access to written and other details of the case before or after the hearing.
Interpretation of the findings will be discussed in chapter 7.
5.2 Observation of a disciplinary hearing
From the disciplinary hearing, the following observations were recorded in the field
notes:
The hearing centred on a suspended BME employee, Joyce, who worked in the
community. Joyce was accompanied by a white TU representative. The management
case against Joyce was presented by a white investigating officer (IO) supported by
a white HR manager. The case was heard by a panel consisting of a white
chairperson (Paul), a white professional lead and a BME HR manager (Monica). A
BME witness (Sam) gave evidence to the panel. A note taker, who was white, was
also present. The hearing took place within the Trust site.
5.2.1 Disciplinary hearing
On meeting and formally shaking hands, I noticed that the palm of Joyce’s hand was
damp. Although she and her TU representative consented for me to observe and be
108

present at the hearing, both of them separately declined to be interviewed. In another
room, I was introduced to Sam who was the only witness to the case. He was asked
to wait in the room until he was called by the chair. Sam was keen for me to observe
the hearing and interview him.
Before everybody convened into the room where the panel members were privately
meeting, there were pairings at opposite ends of the corridor. Joyce and her TU
representative had their backs to everyone. The IO and HR manager presenting the
case at the other end were whispering to one another. In between these pairings, I
stood alone. The atmosphere was tense and heavy.
In the meeting room, the tables were positioned in a rectangular shape. At one side,
Paul was sitting between Monica and the professional lead. Across from the panel,
Joyce and the TU representative were at one end and the IO and HR manager at the
other. There was a large empty space between these two pairs (a similar pattern to
the positions as noted when they stood in the corridor). I sat at the side near the note
taker.
Before the formal introductions, I was introduced to the hearing. Everyone present
was already familiar with my research. The chair asked if there were any objections
to my presence. There were none.
5.2.1.1 Employee under investigation
For most of the hearing, Joyce avoided eye contact and gazed at the surface of the
tables. She only gave fleeting eye contact to the panel when they were conversing
with her. Joyce barely looked at Sam when he gave evidence. She had prepared a
written statement. She read this out when asked by the chair if she wanted to add
109

anything to her defence. As she started to read, Joyce became distressed, tearful
and inaudible. She pushed her statement to the TU official and asked her to continue
to read from where she had stopped. Joyce did not refute any of the allegations
made about her clinical practice and conduct.
Joyce had been suspended from her duties as there were concerns around
safeguarding issues. From the evidence presented, various colleagues had
expressed their concern over Joyce’s clinical practice, lack of engagement with her
clients and poor level of functioning for her grade. Another particular concern was
Joyce holding onto a credit card given to her by a client and not returning it. It was
unclear from the hearing what Joyce had done with the credit card.
An example of one of Joyce’s cases was given by the IO. In the space of nine
months, she saw one client four times. A support worker was also involved in this
case. Despite the support worker expressing his serious concerns to Joyce about the
well-being of this client on many occasions, Joyce failed to respond to the requests
and liaise with the worker. The clinical notes written by Joyce gave a different
account to the actual experience and reflection of the case. The quality of her clinical
notes also failed to mention mental health issues and action plans to maintain the
safety and well-being of the client. Concerns around Joyce’s clinical practice became
so great that the team manager (Sam) refused to give her new cases.
It was also reported that Joyce failed to engage with clinical supervision despite
being prompted verbally and via email by Sam to book supervision. This was ignored
by Joyce who, in her defence, perceived Sam did not like her and was going around
collecting evidence to build a disciplinary case against her. She also mentioned other
110

poor-performing staff in the team who were not as closely scrutinised as she was by
Sam. Up until Sam had arrived, none of the previous managers had commented and
raised concerns about Joyce’s practice.
5.2.1.2 Clinical team and environment
The team was described as ‘difficult’ by the IO and later on by Sam when he was
giving evidence. There was recognition of the lack of continuity in managers as there
had been several within a short space of time. Each manager had their own system
of supervision that was different to previous ones and this led to some confusion in
the team around booking supervision. The team manager had the responsibility of
supervising 17 clinicians. Many of the clinicians in the team were from a different
discipline to the team manager. Some clinicians expressed their concern about
interdisciplinary supervision between social and health care. Sickness in the team
was high and this led to colleagues carrying extra workload to cover the sickness.
Morale in the team was low.
Since Sam had arrived to manage the team, Joyce and her TU official reported ten
members of staff had left: four had been suspended; two were moved to another
area; one had resigned; one had taken early retirement; two had been sacked.
5.2.1.3 Outcome of the hearing
A decision on the outcome of the hearing was not made on the day of the hearing.
Paul, the chair, stated he needed more time to reflect on the evidence presented with
panel members before he could arrive at a decision. He also informed Joyce that she
would receive the outcome within seven working days by letter.
111
Joyce did return to the team and it is unclear if she received a first or final warning.
After this hearing, some members of the team, including Joyce, put in a collective
grievance against Sam. The contents are not known but both Sam and Paul mention
this grievance in their interviews.
5.3 Interviews
The observations recorded in the field notes presented what had happened in this
disciplinary case. The semi-structured interviews allowed an opportunity to probe,
seek further information and ask for clarity. Three employees from this hearing
consented to take part in separate semi-structured interviews: one interview took
place with the BME witness after the hearing; another with the white chairperson of
the panel was before the disciplinary hearing; the final one with the BME HR
manager sitting on the panel took place after the case had been heard.
5.3.1 Interview with Sam, the witness
The interview was conducted in Sam’s office. Sam has worked in the Trust for many
years. He comes from a BME background and has been a team manager for six
months. Before him, there has been a succession of six managers in two years.
Since joining the team, Sam has noticed poor clinical practice in the team and four
BME members of the team have been taken to disciplinary.
The themes elicited from the interview with Sam are:
5.3.1.1 Uncovering poor clinical practice in the team;
5.3.1.2 Managing a poor-functioning clinical team;
5.3.1.3 Impact of dealing with poor conduct and practice on Sam;
112

5.3.1.4 Patient group treated.
Each of the themes is explored in depth.
5.3.1.1 Uncovering poor clinical practice in the team
Managing the performance and conduct of staff to deliver the highest standards of
care is an ongoing responsibility of the Trust.
5.3.1.1.1 Poor clinical practice and conduct
In terms of his appointment, Sam says: “I was quite shocked at some of the clinical
practices that were happening…. And within a very short period of time all these cases were
just hitting me in the face… and I thought ‘How the hell has this been allowed to go on for so
long?’”
One of the main issues Sam found was around poor practice related to medication.
He reports: “At one point the Trust has introduced something called the MMA, the
Medication Management Assessment… and at one point out of eight nurses I had six who
failed.”
5.3.1.1.2 Managers ‘turning a blind eye’
Sam also describes other poor practice that he has witnessed: “There were some
managers there… who let them get away with blue murder… I used to sit in team meetings
and everyone… they were all supplied with a laptop and everyone would be typing away and
doing this, doing that, I thought great. But then when I get up and walk around they would be
answering emails, they were catching up with progress notes on the system, they were
surfing the internet, whilst we’re talking about patients’ lives. And I always put myself in the
perspective of a patient and thought well, if I was being treated by this team, how would I
feel? And I thought no, this has got to stop, so I stopped them from doing it.”
113

5.3.1.1.3 Déjà vu
The problems of the clinical team Sam manages are not new and senior managers
have been aware of these problems for a while. Preliminary measures have not
resolved the issues as they continue to persist. Sam conveys the team has been put
on an ‘At Risk’ register for the second time: “So it’s a team that has been seen as being
difficult. The team has been on the At Risk register before and is now on the At Risk register
again … So At Risk, in terms of how the borough directorate sees it, is this a team where
there have been numerous concerns and it could be about practice, low staffing levels, a
series of SUIs [Serious Untoward Incidents] etc.”
5.3.1.1.4 Collective responsibility
According to Sam, there has been some relief, particularly from the consultant, that
the long-standing issues around poor clinical practice and conduct are being picked
up. Sam states: “They were… pleased that I had seen it and noticed it and was doing
something about it.”
When Sam is asked how the consultant and other disciplines in the team are
collectively admitting there are problems in the team, he replies: “Well… they sort of
say… ‘It’s up to the managers to deal with’ and he was actually one of the consultants that
said to me that this has been going on for a long time, it’s always being tried to be tackled,
but down the succession of team managers it has always got lost…”
The many issues in this team have been left to one person to manage and deal with.
It is not surprising there has been a high turnover of managers in a short time.
5.3.1.2 Managing a poor-functioning clinical team
Several themes arose from this interview with Sam about his experience in managing
this service.114

5.3.1.2.1 Why had previous managers not stayed?
When Sam is asked if he has established why there has been a quick succession of
six managers, he replies: “I have reflected on it non-stop. It’s a difficult team, it’s a very
large team, it’s the largest team actually in the borough in terms of bodies and patients, and
it’s a bloody hard job in that team, it’s very, very hard. There’s too much for one person, way
too much…”
5.3.1.2.2 Ethnic composition of the team
Sam describes the ethnic composition of the team as: “It’s predominantly black British,
sort of black Caribbean, black British. At one point … when I first actually went into the team,
it was all black British, … in terms of what I call front-line staff…. Two white consultants, two
white secretaries and a black secretary…”
5.3.1.2.3 Joyce returning to the team
Sam mentions the team were given short notice of Joyce returning to the team: “We
notified the team on the Thursday that this person would be coming back on the Monday… it
was quite clear looking at her that I think she was struggling with being in a team where no
doubt people knew… about what had happened… But just looking at that person’s face…
they looked actually very unhappy about being back in the team, and very anxious…”
5.3.1.2.4 Poor uptake of clinical supervision
Although Sam is from another discipline, he found nurses in particular were avoiding
supervision with him: “The nurses weren’t booking in for supervision, I made it clear to the
Nursing Directorate I have got nurses who are not booking in for supervision because they
saw me coming from a non-nursing background…”
115

5.3.1.2.5 Sam’s perceptions of how the team viewed him
Sam mentions how the team perceive him: “I think… some of them (not all of them)…
were extremely cautious about me… And I’d probably say they still are now because I’ve
come in, noticed these four cases and I am probably not very well liked because … ‘All these
staff are being disciplined since Sam’s been here,’ so I am probably seen as a bit of a devil
really.”
He declares trying to change the culture of the team has presented him with
numerous issues: “I am definitely seen as the enemy… and I think what has happened
because when I was in the team, and I thought God, I need more staff… and I got staff and…
I won’t say it’s made matters worse but the dynamics are more obvious, that the locum staff
that I have got in, … I have got five extra staff in, three white people and two black people
and within the team at the moment, because we have only been over here for about four
months, the new staff… are all sitting together, there’s not really that mix within the team, so
it’s like the original team members are all up one end…”
5.3.1.3 Impact of dealing with poor conduct and practice on Sam
Sam could discuss and share the impact this has had on him and the support that he
has received over this period.
5.3.1.3.1 Professional and personal toll
Sam states confronting the issues around poor clinical practice in the team has been
challenging: “It’s … not been very pleasant. … It has been tough, it has been difficult for me
at times… I was made aware that it was a difficult team, and I do like a challenge, but I didn’t
realise that it would be as bad as it actually was…”
116

Sam declares the situation around Joyce continues: “…it’s been very, very stressful.
The person that has come back to the team two weeks ago, she has taken out a grievance
against me so I have got to go through that process…”
5.3.1.3.2 Support to manage the clinical team
Sam comments on the support he has received to manage the issues presented to
him: “The support that I had from my immediate manager was excellent. In terms of only one
particular person, there was just no support as well at all, and they were a very senior person
within the Nursing Directorate, I asked them to help me deal with these issues and I got no
help…”
Sam’s managers have provided additional support to help him manage the team:
“What’s happened now is it’s improved because the senior management listen to me and I
now have a deputy manager because it’s such a big team.… So that has improved things…”
Sam emphasises the support he has received from the HR department: “…the
support… and overall my opinion so far is that they have been very supportive…”
5.3.1.4 Patient group treated
Sam describes the type of clients the clinical team manage and treat: “Our client group
is 18–75 and we aim to work with people with a severe and enduring mental illness…there
are some sort of very risky patients.”
Sam perceives many of the clinical staff do not want to work with this type of client
group: “No, they don’t…. They … especially the nurses… prefer the more stable client group
with not a colourful risk history…”
117

5.3.2 Interview with Paul, the chairperson
The interview took place in Paul’s office. Paul describes himself as: “I am not
traditionally a white English person, I am sort of from European stock…” As a general
manager, Paul has specific responsibilities related to disciplinaries. He: decides
whether an investigation should go to a hearing; has the authority to suspend staff;
chairs disciplinary hearings; makes decisions on outcomes and presents the cases at
appeal hearings.
The themes elicited from the interview with Paul are:
5.3.2.1 Uncertain future of the Trust;
5.3.2.2 Unveiling poor conduct and practice leading to disciplinary action;
5.3.2.3 Quality of staff supervision and support;
5.3.2.4 Undertaking the role of chair.
Each of the themes is discussed.
5.3.2.1 Uncertain future of the Trust
Paul discusses the uncertainty of the Trust’s future. He states: “It hasn’t helped by
having four chief [executives]… I think it does send out a very strange message to the staff
that what’s going on at the top is people can’t cope because… Certainly the last two
substantive chief execs, the impression we were given is that they didn’t leave to move on to
greater things, they left because they weren’t doing the job and I think there is a message
there that we’re telling some staff your performance isn’t up to scratch, you need to do better,
you need to work harder, and then people at the very top don’t seem to be doing their job,
don’t seem to be performing…”
118

Economic pressures have forced the Trust to disaggregate and reconfigure its
services with posts being cut and clinicians carrying the extra burden of
responsibilities, as Paul conveys: “And I think there is also an issue with staff feeling
under pressure in terms of the savings that need to be made… and seeing that we are
having to cut posts on a continuous basis.”
To make savings, reduce inpatient beds and treat more patients in the community,
the Trust Board has been forced to scrutinise the performance of employees and
teams in delivering high-quality care. Paul reports: “I think things had been ignored for
some time so it was ‘Actually well we can’t, … we have got less and less resources, we are
looking at having to supply/do more with less’ and so there was ‘what we have got in terms of
staff resources we need to make sure we have got staff who are up to the job and whose
practice is safe’.”
5.3.2.2 Unveiling poor conduct and practice leading to disciplinary action
With services under close scrutiny, serious concerns have arisen about the conduct
and clinical performance of staff. Paul refers to Sam’s team: “Over the last year we
have had quite a number of disciplinary processes, which started when we were aware that
there was some significant concerns about performance… the concerns were so serious…
So… we have probably had around six or seven [disciplinaries] in the last year. I think in
terms of those staff from BME, probably five or six…”
The number of disciplinaries among BME employees in the staff team, as Paul
states, has heightened anxiety: “I can think of one particular team where the staff were
very concerned about well, who is next, and wanting some assurances that we weren’t just
out to get people and it’s very difficult to respond to that because you can’t give any detail
about why someone was suspended or why they were then dismissed, … it’s no one else’s
119

business in a way but we’re very keen to try and get the message out that well actually, if
you’re doing your job, then you have got nothing to worry about.”
5.3.2.2.1 Ethnicity is not an issue
Paul is clear that ethnicity does not come into disciplining staff: “Someone’s ethnicity
isn’t considered as part of the facts, certainly they are not for me, but… it’s just actually ‘Is
their practice safe?’… ‘We are looking unfortunately to have to suspend someone this week,’
and actually saying ‘I am aware that this is going to be the fourth black member of staff who
has gone through the disciplinary process in the last couple of months,’ … because if you
need to suspend someone, you need to suspend someone…”
In light of Paul saying ethnicity is not an issue, he could not explain why there are a
number of BME employees involved in the disciplinary process: “No …I don’t think I
have.”
5.3.2.2.2 Grievance taken out
The heightened anxiety caused by the disciplinary cases in one team (to which Joyce
belongs) has resulted in a grievance lodged against Sam: “There were some concerns
raised about the number of BME staff who have been suspended… and a grievance was
submitted which included some allusions to that… this team manager was sort of trying to
get rid of BME staff on his team, regardless of the fact that he is from a BME background
himself…”
Paul explains the outcome of the grievance: “Well we looked at it in terms of getting it,
getting the grievance investigated as independently as possible… ‘We will get someone in
who has no history to look at this,’ …I think it found no evidence that that particular member
of staff was racist in any way… But the thing that did come up was around supervision and
the quality of supervision…”
120

5.3.2.2.3 Managing the consequences from disciplinaries
Paul depicts a complex picture with many dilemmas presented to management when
a member of staff is disciplined: “We have had some very difficult conversations with
some of the team managers, they’re saying ‘Well what do I tell them? What do I say about
so-and-so…?’ and I say ‘Well you just have to say that they’re currently on leave’ … whilst
the disciplinary policy says if you are suspended you are not to make contact with members
of staff… I am pretty certain that people do because it’s human nature, especially if you have
friends who you work with, I am sure that they will then speak to each other… I am aware
that there have been some occasions where a member of staff has given a slightly different
version or perception of the circumstances than ours…”
5.3.2.2.4 Inconspicuous discussions on disciplinaries
Surprisingly in light of the emotions aroused, the wider discussion on disciplinaries is
low key in meetings as Paul expresses: “I don’t think it comes up very often to be
perfectly honest… For example we have an HR report which gets discussed… at our…
meetings which looks at the number of disciplinaries and the number of suspensions,
sickness procedures and that… but then it’s just numbers in terms of number of staff…”
5.3.2.3 Quality of staff supervision and support
With the Trust’s priority shifting from treating patients in the community, Paul
expresses his frustration: “There’s very little in terms of senior nursing leadership for the
community side which is where the bulk of our service users are…. And we need to address
that balance because at the moment we don’t have anyone, for example, to say ‘Right, OK, I
am going to implement and monitor a supervision structure for nurses.’”
121
5.3.2.3.1 Lack of meaning of appraisals
All employees are expected to have an annual Performance Appraisal Development
Review (PADR) with their line manager to discuss their performance. The purpose of
this review is to reflect on the past year and agree objectives for the year ahead. Paul
questions the robustness of the PADR and links this to disciplinaries: “No, I don’t think
it’s a particularly meaningful process, especially sometimes given the timescales. It’s very
much people … saying ‘Let’s just get you in and get you out.’ …I think it’s very much focused
on the objectives – ‘This is what you should be doing’ which is helpful in terms of disciplinary
processes because then you can say ‘Well actually you knew that you shouldn’t do this, this
and this because it’s there and it was discussed and you agreed to it.’”
5.3.2.3.2 Lack of supervision and support as mitigating circumstances
In the disciplinary hearing, mitigating circumstances are allowed and presented to the
hearing by the employee under investigation and their TU representative. Paul
states: “The mitigating factors, I mean that’s why I am always keen to ask those questions,
… ‘Have you been having supervision and how often was it? If it didn’t happen, was it
because it wasn’t offered or that you didn’t take it?’ … and ‘What was in your development
review?’”
Paul discusses mitigating factors that were partly considered when professional
accountability around clinical practice was challenged in the hearing: “So with that
particular case, we ensured that that person had weekly supervision with a professional lead
because that was part of his defence ‘Actually I had no supervision, no one has raised these
issues with me,’ therefore we would take that on board. But actually… that’s not an entire
defence for your poor practice because you are a registered nurse and you should actually
know that just writing for example ‘depo given, seems stable’ every time you have seen that
person for the last two years isn’t really an adequate assessment of their mental state.”
122

On other occasions, extenuating circumstances are deemed to be misleading as
Paul explains: “…sometimes they’re not [mitigating factors], and so you just think… ‘Hang
on, I appreciate you had some problems with your laptop, but your laptop working wasn’t the
reason that you didn’t identify safeguarding issues, … you don’t need a computer to know
that there’s a safeguarding concern for example.’”
5.3.2.4 Undertaking the role of chair
To undertake the role of chair, Paul explains he has had some training around
investigating cases: “When I was in… my previous role was when I was at a level where I
was more likely to investigate than present management cases, so it’s around the
investigation process and just… looking at all the steps. I mean it’s very similar… training in
how to investigate complaints as well, … there’s a process that you need to follow…”
5.3.2.4.1 Consequences of lack of training in making decisions on the outcome
Paul recognises there is a substantial shift from investigating cases to undertaking
the role of the chair to oversee the disciplinary hearing and process. He states there
is no training available in the Trust to assist in this transition: “Within this Trust very
little. I have had training in previous Trusts, but it was some time ago… So I have had some
training but there’s not a great deal of training available in the Trust…”
Paul comments on the potential consequences of the lack of training on making
important decisions: “And I mean I don’t know whether that then leads us to err on the side
of caution with not having had training and then being absolutely fully competent, but if you
are going to say ‘Right I am afraid…’ For example ‘We are going to dismiss you,’ maybe we
err on the side of caution and don’t dismiss if potentially we think it’s a good case…”
123

5.3.2.4.2 Maintaining impartiality and fairness
Paul usually hears cases of employees from his own borough. Normally these are
heard on the evidence that is provided at the hearing and related specifically to the
allegation. However, Paul cites he would have information about the employee under
investigation that the other panel members would not have. In relation to Joyce, he
was versed in the long-standing problems and issues with individuals and the team.
Although not directly referring to Joyce, Paul acknowledges this added information
might have some bearing: “I would chair the hearings related to the teams that I manage,
and so inevitably if there have been concerns about a member of staff over the last six
months… I would be aware of that. If it then reaches a point where it’s a disciplinary issue,
you can’t just… park that information that you have been aware of…”
Paul emphasises disciplinary hearings chaired for another area are less problematic:
“It’s less of an issue if you’re chairing a disciplinary for another borough, … you have none of
the history… I know that I’m basing it solely on evidence that’s presented today because I
have never met you before…”
5.3.2.4.3 Maintaining impartiality and transparency
To maintain impartiality and transparency, Paul says: “It would be more helpful if we
just… made the process a little bit more independent by, for example, having managers from
a different borough or a different service hearing disciplinary cases, because I think then they
do come to it fresh and… it would add a layer of transparency to that…”
5.3.3 Interview with Monica, the BME HR manager
The interview with Monica was held a week after the observed disciplinary hearing in
her office. In the interview, Monica refers to Joyce’s hearing as well as to other
factors related to disciplinaries.
124

Monica has many years’ experience as an IO and a panel member. In terms of
training to undertake the role in disciplinary hearings, Monica states she has been
given: “No specific training by the Trust, but it comes with the experience.” As a panel
member, Monica perceives her role as: “Ultimately as the HR practitioner you are
there to advise, not make the decision. So if you advise one thing and the general
manager is the decision-maker and wants to do something else, you have to stand
by the decision of…the panel chair.”
The themes elicited from the interview with Monica are:
5.3.3.1 Disaggregation and reconfiguration of services;
5.3.3.2 Training and experience of the chair;
5.3.3.3 Consequences of increased administration;
5.3.3.4 Maintaining impartiality and adhering to the facts of the case;
5.3.3.5 Key themes from disciplinary hearings.
Each of the themes is discussed further.
5.3.3.1 Disaggregation and reconfiguration of services
Within the services Monica oversees, there have been many changes. She
discusses some staff having to move frequently, the impact this has on staff and the
quality of their engagement with patients.
5.3.3.1.1 Impact on clinical staff
The impact of the continuous change leads to Monica citing a recent example: “…
people in the organisation have had five, six, seven moves in the space of three or four
125

years. So in terms of continuity of service and service for the patients, it’s very difficult for
staff then to engage in that team because they’re moved around all the time, so really, as the
service closes here, they are put into another [area], then that service is at risk and then they
move somewhere else and that’s unstabilising for the staff.”
5.3.3.1.2 Changes in team managers
Monica refers to Joyce’s hearing, particularly around the lack of stability in the team
caused by continuous changes of managers and Sam’s attitude towards supervision:
“I mean a case in point was the last hearing that we have – eight or nine managers in the
space of two years. Now in terms of the team morale, what does that do? And it was a
classic case where the individual had no performance issues up to the point where these
issues were raised and then shebang, she gets the performance issues…”
5.3.3.1.3 Why do some areas in the Trust have less disciplinaries than others?
Unlike Paul, who has had to undertake many disciplinaries in his area, Monica
perceives there are less disciplinaries undertaken in her area and contributes this to
several factors: “I personally don’t have that many disciplinaries as potentially other
people/services have. I don’t know if it’s because my managers are experienced – …all my
managers are very proactive in tackling issues at the first level so if it’s sickness, if it’s
attendance etc., …they don’t let it escalate into a case where then it becomes a problem… in
my services at the managerial level there hasn’t been a great deal of turnover, …we have
remained a consistent management team and I think that’s really important.”
5.3.3.2 Training and experience of the chair
In this section, it is unclear how much of what Monica says directly refers to Paul in
his capacity as chair of the disciplinary hearing, although strong hints are made.
126

5.3.3.2.1 Absence of E&D training
Paul, in his interview, reported he did not consider the ethnicity of the employee
under investigation as an issue and also due to his lack of training as a chair he was
cautious. For Monica, the training and experience of panel members listening to
cases involving BME staff under investigation is an issue: “Our disciplinary panels don’t
necessarily consist of managers who have had any E&D training, so that’s number one. …
people aren’t trained… However we get newly qualified managers who are general
managers, who come into the service and are expected to sit and chair these disciplinary
panels and make decisions when they potentially have never sat on a disciplinary panel
before and never had any training…”
5.3.3.2.2 Perceptions of the chair of the panel
In his interview, Paul reported he started chairing disciplinary hearings after joining
the Trust. Monica talks about the experiences of the chair and reveals: “The way the
disciplinary hearing runs is totally dependent on the chair. You get some chairs who are very
experienced… in conducting a hearing, whereas you get others who are very, very
inexperienced, and then again that shows in the hearing. …when they’re in the appeal…,
where I have sat with general managers who when were asked ‘Why did you dismiss the
person?’ started looking in the management case and saying ‘Why were they dismissed?’ So
the chair of the appeal said ‘But you should know, this isn’t written down, what was your
decision-making to dismiss?’ and they couldn’t answer it.”
5.3.3.2.3 Quality of decision-making
In terms of the chair making the decision about the outcome, Monica conveys: “And
it’s so important in terms of the chair of a disciplinary because they then are ultimately the
decision-maker and they will be on a standing in the employment tribunal, so if you don’t
have conviction and you don’t know the case and your rationale for the decision-making,
127

then it shows… And I think a lot of it is dependent on the experience of the chair and the
panel.”
5.3.3.3 Consequences of increased administration
On a wider note, the withdrawal of administrative support has led to issues around
delays in disciplinary hearings and HR managers being unable to take preventative
measures with managers and employees.
5.3.3.3.1 Withdrawal of administrative support
Monica states the withdrawal of administrative support has had implications on
hearings being delayed and suspension of staff prolonged: “Now all the administrative
burden falls onto the HR managers and the advisers which then makes the disciplinary
process a lot longer, both for the member of staff and… management to resolve the issue,
and… well it’s not good for the organisation basically. So we may have a situation where a
member of staff is suspended for months and months…”
It was uncertain if there were any delays in hearing Joyce’s case as the IO
presenting the case was not interviewed.
5.3.3.3.2 Loss of strategic planning to minimise disciplinaries
Not working to her optimal level as an HR manager by having to undertake additional
administrative tasks, Monica conveys strategic opportunities potentially to anticipate
and curtail disciplinaries are squandered: “We then take on the administrative burden
and in terms of the impact on my role, obviously then that doesn’t free up my time to do other
things, so in terms of the strategic and in terms of looking at how potentially these
disciplinaries can be avoided by training managers in giving supervision, good induction,
good recruitment, is all lost… we don’t do enough of the preparatory work to avoid the case
of staff getting into a disciplinary in the first place.”
128

5.3.3.3.3 Lack of preparatory work with managers
Tied down to administrative tasks, Monica points out preliminary work with managers
goes astray: “And it’s… HR working with managers to… do some of that preparatory work
so people are aware of their obligations. I mean we get so many… things like unauthorised
absence, sickness reporting, why are we getting those? If we did the preparatory work,
worked with staff, then maybe that could negate the need for some of these hearings.”
5.3.3.3.4 Lack of preparatory work with staff under investigation
The lack of preparation given to employees referred to a disciplinary and the
emotional impact on them are acknowledged by Monica: “As I said, I feel bad for the
staff because we just take too long and … I think our policy also … you have ‘x’ working
days’ notice doesn’t help, because at the time of the suspension, then we don’t see them for
seven working days, so you imagine sitting at home suspended for seven working days and
then you are called to this meeting and it’s really difficult. And then these disciplinaries drag
on for months and months and months and… We don’t do enough preparatory work on
preparing people of what you’re going to expect in a disciplinary…”
5.3.3.3.5 Lack of preparatory work to reintegrate the employee into the team
Monica provides some reasons why no attention is given to the reintegration process
and preventative measures: “I think it’s a resource issue. I think if we had the mind and the
mind space to think about things, then things might be a bit better, but we can’t continue with
the way, with the volume of cases that we have and the complexity of the cases we have,
working in the way we are. I mean we are paid as aides to sit here and type…”
Monica discloses the tensions when Joyce returned to work: “And never underestimate
the amount of anxiety staff go through to be put through these processes, …you sat on the
hearing last week where Sam is being questioned by the member of staff, and then you think
well, what is that working relationship and that dynamic going to be when Joyce then returns, 129

because there is all that anger, there is all that frustration against Sam…. And do we ever get
that working relationship back?”
Reintegrating Joyce and preparing the team to receive her back was overlooked as
Monica declares: “We don’t do any work on that. We take people through a disciplinary
process and they might get a first written warning and ‘Right, I am back at work.’ There is no
follow-up from that, there is no support after that, there is no reintegration into the team, the
staff are just expected to say OK, and get on with it.”
5.3.3.4 Maintaining impartiality and adhering to the facts of the case
Monica is adamant that investigations and decisions need to be based on facts: “Well
I come from the school of thought that… in an investigation you present what the facts are
and you don’t put in your opinion – it’s not up to me to say ‘They did it wrong because of
this…’”
5.3.3.4.1 Observations of IOs presenting their case
In terms of hearing cases, Monica reports some of the reactions of IOs to having their
cases dismissed. She provides an example: “Some people tend to be a bit ‘Oh, but my
case got thrown out,’ and I have always said that we’re not in the business of getting people
into trouble… it’s not a victory if you give… get a warning for a member of staff, I don’t work
like that…”
Monica continues that the employees presenting the case are looking for a
disciplinary sanction: “The investigating officer and the HR person took real umbrage to
this fact and there was a discussion. ‘Oh but we’ve done this investigation and it took so
long…’ and in supervision I said to my person, it’s not about getting a victory out of a
disciplinary, what it’s about is as an investigation, do it thoroughly, do it fairly, but the ultimate
decision rests with the panel.”
130
5.3.3.5 Key themes emerging from disciplinaries
From the disciplinaries Monica has been involved in, she has noticed significant
recurring themes: “A lot of it centres around for example poor clinical practice because
people don’t have supervision, because they have high caseloads, because they’re not
trained properly, because they’re not inducted properly, because they have a series of
managers coming in and out of the department who have different methods of working, so
it’s a combination of a lot of things.”
Later on in the interview, supervision received by staff comes up again: “ It’s not just
ticking a box that you have supervision, it’s the quality of the supervision…”
In terms of specific themes relating to BME staff, Monica speaks of cultural issues:
“Sometimes there’s an issue about the cultural thing about the shouting and screaming and
aggressiveness and that might be a perception that that’s sort of cultural…”
5.3.3.5.1 Disparity between outcomes for white and BME staff
When discussing the disciplinary outcomes between white and BME staff, Monica’s
tone of voice changes as she reflected on another hearing in which she recently has
been involved: “I had a case where it’s a BME member of staff, safeguarding issue, takes a
bank card from a service user, uses it, deals the money, gambles, dismissed, a criminal
case, the whole shebang. We then have a white member of staff who takes the service
user’s bank card, withdraws money from the cashpoint, acting beyond boundaries in terms of
professional boundaries, trying to sell stuff on eBay for patients, really not acting on the
boundaries, gets summarily dismissed, gets overturned on appeal to a first written warning.”
Tones of anger at the disparity in the outcome are noted: “ I personally was shocked. I
would understand potentially that it was overturned, but not on a first written warning
because she herself admitted that she acted beyond her professional boundaries, she acted
131
beyond her code of conduct, she wasn’t professional, and for it to be overturned to a first
written warning is astounding.”
5.3.3.5.2 Difference in articulation
Monica attributes the difference in the above outcomes to the articulation skills of
each employee under investigation rather than their TU representation: “ I think it’s
about good representation, but more than anything I think it’s the articulation of the individual.
I think it’s if you come across as an individual who is articulate, who can justify your actions
etc., you will get off more lightly than somebody who might not be so articulate and that’s
what I have… That’s what this particular case highlights to me, because the member of staff
who gets the first written warning is extremely articulate, she is very intelligent – no doubt
that other people are as well – but she comes across as a credible person in a disciplinary in
terms of her responses. Whereas my other individual, I think her background is
Thai/Philippine, wasn’t so articulate, was very nervous, was crying and therefore didn’t come
across as a credible person to that panel.”
5.3.3.5.3 Disproportional representation of BME staff in the disciplinary process
Monica finds it hard to measure if there is a disproportional representation of BME
staff involved in the disciplinary process: “Well I think it’s difficult to quantify. Say for
example in the forensic service where you have a make-up of a lot of BME staff, so 80–85%,
so if you have even got four disciplinaries in forensics it’s going to be BME staff because
that’s your population of staff there.”
5.3.3.5.4 Perceptions of the HR department
Monica feels there is a pessimistic view of HR within the Trust: “ I think that we are
perceived as being for the management, I think that’s the first thing, that we’re seen as kind
of the people that would only be visible when there’s something bad happening and I mean I
have had staff say to me ‘Oh God, HR are here.’”132

5.4 Summary
An observation of a disciplinary hearing, particularly focusing on an employee under
investigation, and three interviews with employees involved in the hearing have been
presented. The findings from this chapter will be discussed in chapter 7. In the next
chapter, other interviews with staff directly involved in the disciplinary process will be
highlighted.
133

Chapter 6: Findings from participant
observations and interviews with
employees involved in the
disciplinary process in the Trust
6.1 Introduction
The previous chapter looked at a specific disciplinary hearing around a case. This
chapter will pay attention to the findings from participant observations and interviews
with 27 employees involved in other disciplinary cases in the Trust. For ethical
reasons related to protecting anonymity of employees, the roles and positions of
participants have been generalised as some employees could be easily identified
(See section 3.11).
The findings are presented as:
6.2 The context of the Trust;
6.3 Perceptions of BME employees in the Trust;
6.4 Perceptions of the disciplinary process;
6.5 Perceptions of employees directly involved in the disciplinary process.
134
6.2 The context of the Trust
This section focuses on the context of the Trust where disciplinaries are undertaken.
Most of the findings come from participant observations presented in field notes and
interviews.
These findings come from field notes. Sixty-three days (472.5 hours) spread over
three months were spent in the Trust. All of this time was spent on the main site.
Despite making numerous attempts to contact employees and arrange participant
observation at other sites, this did not materialise. There was a lack of response from
employees on other sites to my communication. For example, emails sent and
messages left on answer phones were ignored. Some employees who responded
subtly refused to participate often citing the pressure of work or stating the
phenomenon not being an issue in their area. These localities were situated where
there was predominantly a white population and white staff group.
6.2.1 The pressure to secure Foundation Trust (FT) status
These findings are obtained from participant observations and recorded in the field
notes. The Trust has not been granted FT status on two separate occasions and is
making a third bid. At a time when the coalition government has implemented cost-
saving measures, numerous employees anxiously spoke of the Trust’s uncertain
future, particularly if its third bid fails. In recent years, there has been a high turnover
of chief executives and this has been linked to their failure to secure FT status. A gulf
and a sense of alienation between the Trust Board and the rest of the organisation
has been reported in the staff surveys and raised in some of the meetings observed
and informal times spent with staff. A common complaint that came up frequently
was the Trust Board’s pre-occupation with the financial state of the Trust at the
135

expense of: the needs and poor-quality care provided to service users and their
carers; the well-being of staff delivering services on the front line at a time of rapid
changes, lack of direction and disarray. A sense of despondency, particularly from
nurses, prevailed towards senior managers who were perceived to be alienated from
the day-to-day realities experienced by front-line staff. Nurses on lower bandings and
HCAs did not convey the same anxiety and were divorced from the Trust failing to
secure FT status and the unknown potential consequences arising from this.
There is a noticeable difference to where Trust executives are based in comparison
to the rest of the staff on the main site. The Trust headquarters is situated on the top
floor of one of the highest buildings. The physical environment has been recently
refurbished with expensive carpets and new furnishings. Employees in this setting
are formally dressed and adopt a business-like approach. There are very few patient
areas situated around the Trust headquarters. Reference to this being the ‘ivory
tower’” was often heard.
The lack of stability in the Trust and heightened anxiety leading to employees not
feeling contained were attributed to poor and inconsistent leadership at the top of the
organisation. During the time spent in the field, two Trust Board executives quickly
departed without any notice. There was a lot of speculation about why these figures
had left after a new chief executive’s appointment. Among some BME employees,
there was relief about these changes with the hope that the E&D agenda would be
re-engaged with so that the needs of BME employees could be recognised and taken
more seriously. Since his arrival, the chief executive (with the chairman) has
attended several BME Staff Group meetings.
136

6.2.2 Reconfiguration of services
To meet the requirements of FT status and the imposed cost-saving measures, the
Trust has been forced to look at its services and staff. Over time the number of
inpatient beds in the Trust has been reduced. Some services have been
disaggregated and reconfigured to curb costs and treat the users of the services in
the community. Patients will only be admitted to hospital if they cannot be managed
in the community. There is a constant demand on beds and a pressure on staff to
stabilise patients so that they can be quickly returned to the community and followed
up by community services.
The turnover of chief executives and the continuous disaggregation and
reconfiguration of the Trust came up in interviews. George, a white nurse, reports the
impact on front-line staff, particularly BME staff delivering treatment to patients: “I
think we have moved from feeling like we are directionless, to actually feel like we are
chaotic; I think there’s a sense of chaos, and that breeds anxiety and when people are
anxious, of course they become much more cautious, they become more divorced… unable
to contain the pressures that come from the patients, …[this] generates incidents, and you
get more complaints and of course who is at the back end of all that is predominantly BME
staff.”
Matt, a white nurse, highlights the consequence of clinicians redeployed to unfamiliar
settings after reconfiguration of services. He refers to a BME nurse: “They said the
BME manager was often not on site… What turned out was, the manager was put in an area
where he lacks expertise… he had no prior experience… and he was put there as manager.
So he was redeployed… he hadn’t chosen to work there, that was the only position in the
Trust. He was given training, he was not the brightest, he failed… He was really stressed, he
was being bullied by the consultant, he brought it up and no one did anything. And then he
137

was dismissed and suspended because of all the issues in his practice and the lack of clear
leadership.”
From participant observations, clinicians often discussed the shortage of nurses in
some clinical areas and the burden placed on staff performance. Complaints of
managers being oblivious to the stresses and strains on clinicians and clinical care
being severely compromised are noted. Nurses often missed their lunch breaks and
worked beyond their contracted hours of employment. Owing to staffing issues,
managers were reluctant to release nurses for training. Poor attendance at
mandatory training required by the Trust is a common problem reported. During the
time spent in the field, the Francis Report (2013) was published. Marcia, a BME
nurse, draws a parallel to the Francis Report and in her interview raises concerns
about the staff shortage arising from the restructuring: “After the Francis Report I think
one of the key issues… was a lack of response to the internal intelligence, so people were
telling them this is happening, …services are short of staff, and all those early warning signs
should have been picked up. I could easily cut and paste from Francis, easily, in terms of
contributing factors… And this is where we come… I think we need to also think about why
people abuse? Stressed and burnt out people who won’t deliver quality services, underpaid
people. And if they work and work they won’t be developed, they won’t keep abreast with
change, they won’t be renewed, refreshed, motivated.”
To meet the pressure of securing FT at a third attempt, the Trust has had to
disaggregate and reconfigure its service. The lack of direction and chaos in the Trust
has been attributed to the turnover of chief executives. In addition, cost-saving
measures have been imposed. Alienation between senior managers and front-line
staff has been reported. Some staff have been redeployed to clinical areas where
138

they do not have the skills. The shortage of staff has had an impact on the
performance of clinicians. Comparison to the findings from the Francis Report (2013)
has been made.
6.2.3 Recruitment of BME staff
This section focuses on the recruitment of BME staff, particularly nurses and HCAs in
the Trust. The findings have predominantly come from interviews. Denise, a white
nurse, compares recent African recruits to others. She states: “I think the Trust has
been ill-prepared for the waves of more recent people who joined in nursing… every few
years you will get a wave of Irish, a wave of Caribbean, but people have come with a very
Northern European cultural perspective, usually because that’s how they have been trained
at school… And now we have got people [African] whose perspective is completely different
and do not have the same reference [British education] points.”
George, a white nurse, reflects on the consequences of employing newly qualified
nurses in the Trust without being interviewed: “This goes back to a recruitment policy
years ago when people were given jobs without interviews. The people who did get through
to work for the Trust who really weren’t suited to the job, they just weren’t, but not that many,
but some of those had proved to be very problematic but I do always think that… by the time
you get to the point where you’re just going to discipline somebody, something fundamental
has gone wrong at whatever level.”
Matt, a white nurse, also mentions the newly qualified nurses who have been
recruited in the past without interviews: “We went through a period when… we wanted to
increase our quota of nurses…, we weren’t robust enough and we took people who weren’t
up for the job and didn’t really want to be nurses and I think that we have paid and still are
139

paying the price for that because those nurses are now staff nurses or senior staff nurses,
ward managers, and they’re not up for the job.”
Pam, a white nurse, refers to the recruitment of African nurses: “The Trust absorbed an
awful lot of people and particularly Africans in a very short space of time… the fact that the
Trust at the time wasn’t interviewing people for the best of reasons… that was the policy that
won a national award, but I think it backfired on us in some ways.”
The perceptions and attitudes towards BME staff by nursing candidates who have
been interviewed for recent posts are conveyed by George, a white nurse, who
frequently sits on interview panels: “We’d ask them questions… ‘you’re going to be
managing staff from different ethnic backgrounds and different races, what issues come up
from that?’ And they would always answer it as a negative, as a problem to be solved. They
would never say ‘Well actually we have got these people who have triumphed over all sorts
of adversity to get here…’”
There is a perception that the Trust is ill-prepared to deal with and manage nurses
who have been appointed from different racial and ethnic backgrounds. In addition,
newly qualified nurses have been recruited without being interviewed at a time of
nursing shortfalls identified by the NHS Plan (DoH, 2000). The consequences of this
initiative to recruit poorly functioning nurses are highlighted. In recent recruitment
interviews, some candidates have revealed their negative attitude towards BME staff.
6.2.4 Perceptions of the Trust E&D initiatives
From field notes taken from participant observations, there are several groups that
look at initiatives related to E&D in the Trust. Notable groups are the Race Equality
Steering Group, Workforce Equality Group, E&D Group and the BME Staff Group.
140

Apart from the BME Staff Group, it is difficult to separate and distinguish the purpose
and task of each of the other groups. Similar agendas are repeated in each group.
How these groups link together is not always clear. At first this lack of clarity is
attributed to the limited time that the researcher spent in the field. However, when
non-clinicians and clinicians (who have been in the Trust for many years) were asked
about the role, function and how these groups interrelated, they too were unclear.
An absence of clinicians was noticed in these groups. Meetings were predominantly
attended by members from one particular team and from the main site. Most
meetings were held over the lunch period. Asian snacks were provided by one group.
Those who attended forfeited their lunch break. These groups were attended by BME
staff. The presence of white staff was rare. Those who did attend were managers
and they often arrived late and sat on the periphery and near the door. They gave the
impression that they did not want to be there; this was confirmed in interviews. Subtle
behaviour towards these managers was noted, particularly around snacks served.
Food was often withheld or managers did not partake in eating it. The underlying
fraught dynamics and the emotions were never discussed and yet they had some
bearing on the meetings. In my journal/diary, I often reflected on my frustration of
attending these meetings, particularly the avoidance of the group looking at how
employees related to each other. However, some participants who were quiet in
these meetings became animated in the interviews.
Through interviews, this section focuses on the perceptions of the E&D agenda in the
Trust. Denzel, a BME official, asserts: “I think that the culture of our organisation has
perhaps got something to do with it as well, and not helped by the fact that we have had
141

perpetual change and I think the culture which has to include the fact that equality is perhaps
still seen as on the periphery, and not in the core.”
With the E&D agenda, Leona, a BME clinician, emphasises: “And I think it requires
courage, leadership, not just goodwill, you need to see it within the values and principles of
the Trust, given the priority, the leadership from the top leading on it, taking responsibility and
driving it through and… you can see it trickling down through the management structure…,
but we don’t see that. It’s at the bottom of the pile.”
Despite the E&D initiatives, Gerard, a white nurse, touches on the inequalities in the
workforce: “I feel slightly uncomfortable because over the years the Trust has always
portrayed it to be an Equal Opportunities Trust with lots of policies… But sadly in practice the
workforce still feels… they are not treated fairly.”
The E&D agenda in the Trust is perceived as not improving and making any
difference to the working lives of its BME staff. Part of this is attributed to the lack of
support from Trust executive figures in embracing and applying the programme into
the core business of the Trust.
6.2.5 Perceptions towards the study
From entering to leaving the Trust, numerous behaviours, thoughts and emotions
towards the study were observed. The findings are taken from participant
observations, interviews and notes from my fieldwork journal/diary.
The reactions of these employees range from hostility to some form of acceptance
that the phenomenon needs investigation. These next comments are made by
informal participants. In terms of considering the feasibility of carrying out this
research, David, a BME nurse, states: “You’ll be lucky if anyone will touch what you are
142

proposing!” The senior white clinician, Leo, expresses: “The subject is provocative and
you’re ‘shit stirring’!” Rosie, a white manager, angrily states: “What has stealing or hitting
patients got to do with race and ethnicity?” At a time when the Trust has failed to secure
FT status, Norman asks: “What are you and the university going to do with this
information? Will it be another stick to beat the Trust with?” Negative consequences of the
outcomes from the study are a concern for Michelle, a white nurse: “The findings may
be misinterpreted of the Trust being racist and discriminatory, and negative publicity may
come out of this?” Tara, a BME nurse, welcomes the study: “It would be good for the
organisation to begin to understand what is going on and why this issue keeps coming up on
a yearly basis?” Nellie, a white manager, reflects: “The Trust in their workforce report says
this needs further investigation. They now have the opportunity to do this and show their
black staff that they are taking this issue seriously and doing something about it.”
From these remarks by informal participants, several emotions and behaviours can
be elicited. All these comments were privately expressed and at times whispered
even though no one else was around.
During the course of the study, my own behaviours, thoughts and emotions were
observed. For reasons around reflexivity, a journal/diary was used to record and
reflect on bias. Personal unconscious motives for undertaking this study are
questioned in this extract: “As a migrant, is this study linked to injustices from the Raj and
Britain’s imperial past over India? Am I trying to redress this imbalance of power rooted from
the historical past?”After presenting this study to a group of white staff, to recruit
participants, I noted down my reactions after leaving the meeting: “There was a lack of
engagement. The ‘uncomfortable’ silence after the presentation makes me feel anxious and
scared. I feel deflated and despondent. I am not sure anyone will come forward… What was
143

the silence about? Have I bitten off more than I can chew?”No staff from this meeting
came forward to participate in the study.
Preserving autonomy, not allowing the study to be hijacked and questioning my being
as a researcher is reported in my journal/diary: “Despite the aims of the study made
clear and ethical approval granted, I cannot understand why my methodology is questioned?
Why have I been asked to go down a quantitative route and provide ‘hard facts’ when the
statistical details provided by the Trust around disciplinaries are scant? What does this say
about the ‘politics of evidence’? On a personal level, are indirect criticisms levied towards me
about not being good enough to carry this work out? Without playing the ‘race card’ is there
unconscious factors raised about my credibility and impartiality as a BME person carrying out
a study involving BME staff? Would my perceptions be different or my motives questioned if I
was a ‘white’ researcher? Am I being defensive?”
At a couple of separate presentations about the study, I felt personally attacked and
this reaction reinforced how emotive the phenomenon was. In one meeting, it was
not clear if this was linked to the nature of the subject, something about me, what I
represented or all these factors. This was precipitated by a white clinician in a senior
position stating: “Why do ‘you’ automatically assume all white people are racists? When are
you going to look at the racism amongst black people?” The tone of voice was hostile and
angry. In another formal meeting over a Christian festive period with senior
managers, a silent uncomfortable response was observed after the study was
presented. This silence was broken by a white employee emphasising: “Too much
attention is being given to Muslim issues and Christians are being ignored.” A sense of
unease among other staff present was noted when this statement was made and the
agenda was quickly moved on to the next item.
144

6.2.6 Observations of behaviours
During interactions with individuals and groups about the study, a number of
unspoken and non-verbal behaviours were observed and recorded in the field notes:
uncomfortable and heavy silences with people avoiding eye contact; rolling of eyes;
sighing; raising of eyebrows; staff turning, looking at each other and giving wry
smiles; white skin complexions turning red; individuals physically turning away from
the researcher and not engaging with the subject; quickly changing the subject when
disciplinaries were discussed; shuffling of chairs. These behaviours could not be
captured on digital recorders.
This section has been included as the responses captured around the perceptions
towards the study characterise similar attitudes expressed towards E&D issues in the
Trust.
6.3 Perceptions of BME employees in the Trust
The findings in this section come mainly from interviews. As a starting point,
comparisons are made to colonial history and the current plight of BME people in
society and how this mirrors the current position of BME staff in the Trust.
Perceptions, particularly of how BME staff are viewed and treated, tensions between
and within BME groups and the cultural working practices are highlighted.
6.3.1 Links to the historical, societal, political and personal context
Ann, a BME clinician, relates the predicaments of BME staff in the NHS to the British
colonial regime: “In the colonial regime… it served to keep the people where they wanted
the people… You could wear the master’s clothes and think ‘Yes I have a rich master, look
how well he treats me,’ but you have a master and you’re not free. And I think that for me is
145

the feeling that ‘Yes you can come and work for the NHS, but don’t think that we accept
you.’”
Later, Ann claims that the position of BME people is already defined no matter how
hard they work: “It’s about positioning… I think that’s what I mean by positioning, is this
idea of ‘know your place. We can do it but you can’t do it,’ … you can’t take for granted that
you’re going to have the same experience...”
The current plight of BME staff occupying lower bandings in the Trust is highlighted
by Monica and Martina. Monica, a BME manager, briefly mentions: “ It doesn’t appear
to me that there are many people from BME backgrounds that are at a senior level in the
organisation and I think that’s probably quite significant.”
Martina, a BME administrator, observes: “There is a glass ceiling, so senior managers
are white and the lower bands are black.”
From participant observations, the lack of black role models at the senior level in the
organisation is noticeable during the time spent in the Trust. All the executive
members on the Trust Board are white. Some BME employees complained that they
do not have leading BME figures in the Trust to whom they could aspire. The data
related to the workforce highlights BME nurses and HCAs are the majority in lower
bandings.
According to Leona, a BME clinician, the experiences of some BME people in wider
society have been internalised and brought into the workplace: “Some of the stresses
that BME groups face get played out in a work environment, so… if you have grown up in a
society where you’re always the oppressed, stop and search, low expectation at school, …
you have got that self-fulfilling prophecy, sometimes it gets to the point where you can’t take
146

any more and that may… come out in a work environment where you may shout or you
might say something that doesn’t necessarily go down very well…”
Later, Leona continues: “I don’t even think it’s a Trust issue, I think it’s a societal issue…
and there’s a construct that says people with black and brown skins are lesser in the sense
that they’re not as intelligent as we are, they’re not as articulate as we are…, I think because
the systems and structures are there and systems and structures don’t exist without the
people, so the systems and structures just reinforce… and drive it through”.
Denise, a white nurse, expresses that BME nurses have internalised this lack of
value and worth: “What we found was that their morale was incredibly low and they had
almost absorbed this idea that black nurses couldn’t be good nurses.”
Nellie, a BME nurse, considers the personal histories of BME employees facing
disciplinary action: “There was a consultant and we were talking about disciplinaries and in
the break she came up to me and said, in my experience the individuals that I have dealt with
were coming with baggage… layers upon layers upon layers upon layers… and if we’re not
conscious of its impact on us as an individual, as a clinician, as a carer, where does it bleed
through if we’re not mindful of it?”
Lisa, a white manager, elaborates further on the ‘baggage’ that employees carry into
the work setting: “There was sadly a lady years ago who came from North Africa and had
had a very abusive experience but was very senior – I think princess level – but is working as
a healthcare assistant – and who turned out had… infectious diseases and was incredibly
ill… she hadn’t shared any of that with us…, she died because she was so ill… Now we
found out afterwards that what she was trying to do was fund her children’s education… And
also it was around insurance, she did not want anybody to know that she was so ill because
147

she wouldn’t have had the insurance which would then fund her children’s education later on
after she died.”
Gerard, a white nurse, discusses the issue of discovering information about the
outside status of BME staff and how this impacts on the team: “ I have a healthcare
assistant on one of my units that everybody looks up to, but it’s got nothing to do with work…
but outside of work he’s a very senior pastor. Now I didn’t know this, but I wanted to know
why he was getting preferential treatment for days off, time owing, etc. Now I didn’t
understand this until somebody was willing to explain it to me… So one of the most junior
staff on paper culturally is the most senior staff in the department...”
The issue of social class and how this comes up in clinical work is at the forefront for
Pam, a white nurse, who states: “Yes, for me… something about class and status…
Oddly enough it is as important as BME, but I think class exists much more really as the
heart of the issue, even between people’s own cultural groups and status…”
She continues: “If you start to talk about class you start to think about your own prejudices
towards people, what you have and what you don’t have, and whether you were advantaged
enough in life or not. And for our BME group, if they’re not British born, I guess, are not
educated here, … look upon others who may have had better privileges and easier access
and have been scornful…, it is about status and I think… it’s envy, jealousy, it’s hatred, it…
brings up the worst in people and… in some of our services where you have a predominance
of white middle-class patients, you will have that acted out more towards your black staff
group... And so there will be more disdain shown towards people… and I think often our
[BME] workforce would probably say we don’t protect them enough either.”
From these interviews, the colonial past and the social construct of BME people are
recounted to the present day. There is a perception that the position and lack of
148

worth of BME nurses in the NHS have been pre-determined and reinforced by
systems and structures. According to Leona, there is a limit to what some BME
people can endure before reacting to these held and perceived injustices that can be
acted out in the workplace. Another complex picture begins to emerge involving
many strands, particularly around cultural background, life experiences and
‘baggage’ that staff brought from their outside lives into the workplace. The unknown
status of some BME employees, such as princess, chiefs and pastors outside the
workplace is made known. The complexity and context of social class are tied to the
emotions, tensions and behaviours.
6.3.2 Senior managers perception of BME employees particularly black African
nurses
This section looks at how black Africans: are perceived and treated by senior
managers; react when under scrutiny; have differences in adapting in the Trust and
have similar issues to those identified by the NMC. These findings are taken from
interviews.
George, a white nurse, refers to how black African nurses are regarded by senior
managers: “The perception of how to work with Africans and what to expect from African
nurses was I thought pretty skewed… There was an acknowledgement at the most senior
level that a lot of staff… simply don’t know how to relate to African staff… There wasn’t any
understanding of the African culture as it translates to how people work here and how they
relate to their employer, how they relate to one another, and there was a view that you
categorise all of the staff as African, when in fact of course they’re all from different countries,
they have got very different cultures, very different interrelationships with one another.”
149
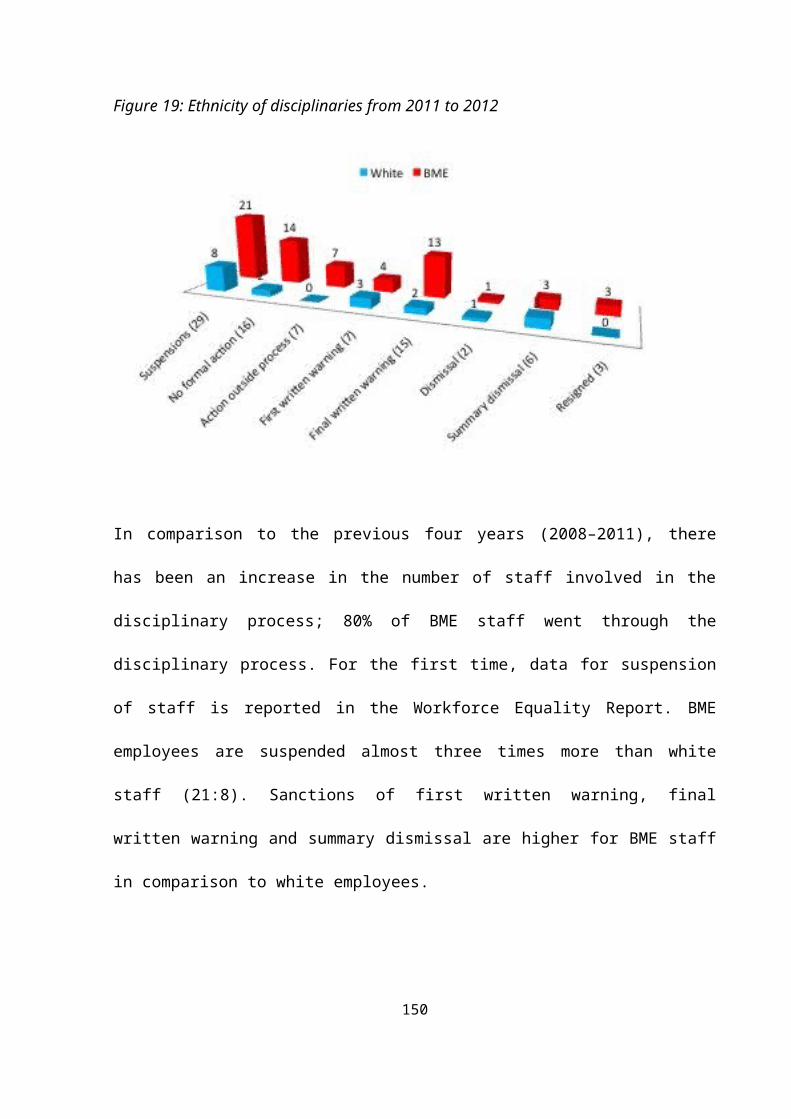
He continues: “When I say the Trust I mean up to Board level… and I think they just don’t
get it, they don’t get how to work with a predominantly African workforce. I think instinctively
they don’t trust them and I think they see… carrot and stick, the stick’s better.”
Gerard, a white nurse, acknowledges there is much that he needs to learn about
black African culture: “I work with an awful lot of African staff and I need to understand the
issues that exist and any tensions that may exist between some of the African staff… There
are issues that do affect their performance in work.”
How black African staff have reacted when under attack from management is closely
observed again by George, a white nurse: “The one thing that was absolutely clear…
was as a group they [black African staff] did band together when there was adversity, and
particularly when they felt they were being attacked from outside and… ‘management’. It is a
particularly African thing, they’re not going to turn round and say to you… ‘This isn’t fair, this
isn’t right, I am better than this, you should treat us with more respect.’ What they’re going to
do is they are going to withdraw. And when they withdraw, they withdraw their cooperation
and when they withdraw their cooperation you can’t get anything done…”
Denise, a white nurse, observes the difference in adaptability of black African nurses:
“I was noticing a difference between the adaptability of some of our African nurses as
opposed to others, so a lot of our more senior black nurses are from Zimbabwe; the more
junior ones, the ones we tend to have more problems with in terms of numbers of
disciplinaries, are from Nigeria, male, and that’s exactly the same as I understand from the
NMC, that most people in mental health… you are more likely to be crossed off the register,
if you’re from West Africa, black and… 40 plus, and you probably also have a gambling and
a bit of a drink problem…”
150

Pam, a white nurse, also draws attention to black African nurses referred to the
NMC: “Well if you look at the NMC de-register notice, you will find predominantly those
mental health nurses that are de-registered are black Africans.”
The perceptions from these interviews highlight the unfair treatment of black staff. In
some areas of the Trust, black African staff are homogenised as one body. It is
observed that senior managers in particular do not know how to relate to staff coming
from the different regions of the African continent. Senior nurses make reference to
the disciplinary outcomes of black African nurses to the NMC.
6.3.3 Senior managers’ perceptions of relationships and tension within BME
employees
Attempts to move away from homogenising BME staff and looking at the differences
and rivalry between various BME groups are found. Gerard, a white nurse, describes
some of the changes that he has noticed in the Trust: “When I first got here, this place
was managed by the Irish… And then we slowly changed and we had more Mauritian
managers but we still had a very white top-level management. So it went from the Irish to the
Mauritian…”
The relationships between BME staff groups arose in several interviews. Pam, a
white nurse, highlights the rivalry between various groups in her service: “We have
Nigerian rivalry within tribes, we have West African/East African rivalries and we have White
European rivalries…”
Ali, a BME manager, describes the various tensions between different ethnic groups
from an investigation he has carried out. BME patients are also included in the
dynamics: “Some people had concerns about racism and it wasn’t about necessarily
151
black/white, but a lot of tension between different staff groups, so there was a Mauritian
corner, a Ghanaian corner and a Nigerian corner, and tension with the patients at that time
were very largely from the Caribbean…”
From these interviews, there is a shift from the polarised position between black and
white groups. The interrelationships between various ethnic and racial groups reveal
tension and rivalry. Racism between these groups is also reported.
6.3.4 Perceptions of BME staff commitment and lack of trust placed on them
The first interviewee is from a BME background and shares her experience of BME
employees that she has investigated. The second interview looks at exclusion of
BME staff in a clinical area. Marcia, a BME nurse, who is involved in the disciplinary
process, reports: “I think culturally or socially people… the BME group here are probably
perceived as people who are not entirely committed to their job role. I mean there’s [there
are] some people, especially when I arrived, who used to work all God sent hours. I have had
a lot of cases where people have been asleep on duty, and a lot of fraud cases.”
Later, Marcia lists the attitudes she has encountered from BME staff: “Well… late
coming on duty, trying to defraud the Trust, working very long hours, conflict within the
workplace, not between whites and blacks but between blacks themselves… and
unprofessional behaviours, eating, unwelcoming behaviours, rigidity… there’s [there are]
some things I see.”
Shauna, a white nurse, tries to make sense of the resistance of some BME HCAs in
her workplace: “They never come into the Care Programme Approach because they don’t
care. It’s… ‘Well actually, have we invited them in? Do they feel that they were welcome to
come in? Have we told them they’ve got something to contribute actually?’ So it’s that
152

different thinking really and making people feel that actually they are part of it. And I am not
sure we are there with that yet.”
A senior BME investigator criticises the unprofessional behaviour and commitment of
black employees. Shauna tries to understand the reasons why black HCAs are
perceived to be apathetic. She learns that they are excluded by the rest of the team.
Various interviews report the lack of trust placed on BME staff, particularly around
sickness, contracted hours of employment, their motives for working with vulnerable
people and their qualifications.
Gerard, a white nurse, highlights how BME employees are perceived: “Sickness and
absence, and finance time and time again. I think the BME side is scrutinised to find if…. is
there any way that they’re fiddling their hours, expenses … if they’re off sick they must be
working somewhere else. I don’t think the same attitude would carry to other members of
staff. So I think they are viewed suspiciously…”
Later, he continues by posing several emotive questions and challenging the
behaviour of some managers: “Why does somebody hold a belief that an African works
here for the money? Why isn’t that a racist comment? Why isn’t it institutional racist if it’s not
directly racist? Why aren’t managers using capability and performance for staff, but will allow
staff to get further and further into trouble and then progress a disciplinary – why do you do
that? That to me is a slightly sadistic thing. You have heard the phrase ‘Let them dig their
own grave’…, why would you let an individual do that, if you actually didn’t feel some degree
of animosity towards them?”
153

Denzel, a BME official, indicates a similar theme: “I think there is [are] some middle and
senior managers who view its black workforce as just being obsessed with money and
earning money… But I do not think the same is applied to white staff.”
Hazel, a white manager, discloses a new computer system in the Trust which has
revealed certain information. She avoids bringing race and ethnicity into the
discussion: “…there are certain individuals, and we went through a spate of people working
whilst off sick and people just going AWOL and that was dealt with… We then had a whole
range of hearings and disciplinaries to deal with excess working, so working at the same
time, working on NHS professionals, doing back-to-back shifts, double claiming, so claiming
NHSP shifts or agency shifts, and of course that’s minimised now hopefully with NHS
professionals and e-rostering, so that will hopefully address that issue.”
Denise, a white nurse, indicates the financial motivation for nurses and HCAs from
overseas: “Obviously some clinical areas attract a lead payment… And people coming from
abroad, who may well want to send money home or be supporting people elsewhere, will
want to, as immigrants throughout history have always wanted to do, perhaps hold down a
few jobs and send money back, so why not go to the area which gives you a premium in
terms of pay, is very well staffed, so perhaps allows you to work somewhere else because
you’re not too tired at the end of that time…”
Nelson, a BME administrator, states delays in BME staff returning from visiting their
families overseas arousing suspicion from managers: “We have many cases around
people going back home and maybe not coming back when they should… and you often
hear comments, sort of raising of eyebrows and body language and so on when it’s someone
of Asian or Afro-Caribbean… that they’re pulling a fast one… My point is, if somebody was
coming back from Ireland and that happened, would that manager have the same point of
154

view immediately without seeing the facts, and I don’t think they would… again it’s a
stereotype and a prejudice that they have.”
The authenticity of Ann’s (a BME clinician) qualifications is questioned as she recalls
her supervisor’s comments: “At that time I had two masters, and she was… ‘Yeah, but
where did you do it? Was it one of these made-up colleges?’ Now who goes to the made-up
colleges? Isn’t that where they send the immigrants to get their papers…, which is so
unnecessary, and discriminatory… So it’s already been decided… I have no place. It doesn’t
matter how many masters you have…”
These interviews reveal the lack of trust and suspicion from senior personnel around
the integrity and conduct of BME staff. There is a perception that BME employees
transgress their contracts of employment and qualifications are not genuine. Their
motivations are questioned. Gerard, a white nurse, wonders why some managers do
not intervene at an early stage to prevent disciplinaries.
6.3.5 Perceptions of BME employees treated unfairly
In these interviews, disparity between how BME employees are treated in
comparison to other members of staff is highlighted. Shauna, a white nurse,
differentiates how white employees are treated more informally than their BME
counterparts: “White staff perhaps are more likely to get dealt with informally; what is it
about black staff that we do not administer and deal with people in that way?”
Lee, a white administrator, speculates about discrimination: “It can only be how we
recruit as an organisation and how we develop people, in fact how we invest in people, and if
it’s neither of those two things then you’re looking at something far more sinister… but could
it be discrimination that’s happening?”
155

Drawing on his interaction with BME staff involved in disciplinary issues, Tariq, a
BME clinician, recalls: “Black staff had a bitter experience… and they were treated really
badly…”
Nellie, a BME nurse, refers to the disparity between black and white staff: “ I am aware
of cases whereby individuals have raised an issue about not getting the supervision that is
required for their post in terms of client contact, so it’s affecting their training, it’s affecting
their progression where other members of staff who happen to be white are getting that…
And it’s in the getting fed up bit that there has been the danger of that behaviour and its
interpretation as aggressive.”
Peter, a BME manager, raises issues related to racism: “I think we will probably have a
mixture of people…, those who will not feel that the organisation is committed to equalities,
and as evidenced through the Staff Attitude Survey that we have, there will be people also
who have experienced harassment on the basis of their race, from service users, from staff,
from managers. There will be those people who continue up to this present day to
experience problems in the workplace, where they are being called ‘Nigger, get out!’ or
having managers slam their hands down on the table to say ‘Move, move, quicker, quicker!’
…in a very bullying fashion – these are black staff I am talking about. There will be those
who talk about issues from white managers, white staff to them, as black individuals. There
will be those who talk about issues arising from Asian staff against black staff members,
which is new…”
Disparity in treatment between BME and white staff is raised. Participants report
discrimination and harassment, but again, as Peter discloses, this behaviour
manifests within different BME groups in the Trust.
156

6.3.6 Playing the ‘race card’
Examples are cited about a BME and white staff using the ‘race card.’ Marcia, a BME
nurse, describes a situation with a BME nurse who has tried to avoid accountability
after a visitor has complained about his conduct: “This gentleman [nurse] who seemed
to be coming up all the time as a problem and he said ‘Well they’re all racist and I have heard
them call me names…,’ so I explored it further with him… He kept a visitor … [waiting] for 15
minutes because this person was a bit early for visiting hours. Now is that a race thing? …
That’s not a race thing.”
Ann, a BME clinician, mentions her white manager’s comment about her applying for
a course that was oversubscribed: “I mean this manager also said to me ‘Well if they are
down on black people applying for the course, you might get in…’”
The issue of playing the ‘race card’ to avoid responsibility and obtain priority is
highlighted in these two interviews. Both interviewees are from a BME background.
6.3.7 Perceptions of cultural differences in working practices
From these interviews, the observed cultural working practices of BME staff are
discussed. Denise, a white nurse, shares an experience from visiting a clinical area
after being promoted to a senior role: “I wasn’t expecting when the first time I went on
[Ward X] as a… to have [BME] people bowing and … I was able to understand that within
what I already knew about race and culture, but there will be many white managers who
wouldn’t and would think ‘Oh my God!’”
She discusses her reaction when a BME staff member approached her for a pay
increase: “And when somebody has asked for a grade increase because they have got a big
family, which would be a very acceptable reason for asking for a raise somewhere else,
157

completely unacceptable here…, a manager can respond to that. They can say ‘Oh my God,
how dare you?’…”
She also describes a situation with a BME charge nurse who was awarding herself
the best shifts: “There was one band 6 black nurse who was giving herself all of the
lucrative shifts. And when I asked her about it, her answer was… ‘But I am senior to band 5s,
so why wouldn’t I give myself those shifts? I need the money’, and so we unpicked it and
yes, that was her expectation that as a more senior person that’s what you would do, reward
yourself, which is completely the opposite from the perspective culturally here…”
Shauna, a white nurse, explores the working ethos informed by culture of a BME
HCA: “I do wonder if that goes back to the cultural and not understanding the culture… I
worked with someone on [Ward F] and staff were getting really frustrated with her… and
when we… took her aside and had a chat with her, …she said in her culture what happens is
you get your list of things to do in the morning and as soon as you have done them, you are
done for the day.”
These interviews look at how cultures are interpreted and the disparity in the level of
tolerance towards different cultures found in the Trust. Peter, a BME manager,
reports difference in culture: “Lack of sensitivity to difference… people from different
cultures, different backgrounds will act/behave in different ways, and that different people will
regard one thing as perfectly normal… The organisation is lacking sensitivity… there is not
the intelligence to recognise and deal with it.”
Gerard, a white nurse, raises perceptions around cultural differences between
manager and subordinate: “Thinking about who the staff are managed by? Are they
managed by other people from BME backgrounds or are they managed by European white
staff? But I wouldn’t say that the practice of BME staff is for me noticeably any different,…
158

but I wonder if there is some level of… where difference comes in that people don’t
recognise, and sometimes I wonder whether that is less about practice and more about
different cultures and that people respond from different ethnicities to different cultures and
behaviours and ways of being, and that maybe comes out/gets misunderstood.”
In terms of the disproportional representation, Denzel, a BME official, separates
cultural difference over ethnicity: “There is a BME over-representation, but somehow
sadly some of those BME being disciplined is because they are not understood and it’s more
of a cultural awareness rather than the colour issue. They say certain things and it’s taken in
a different way and they are being disciplined, without them realising they shouldn’t say
that…”
Lisa, a white manager, emphasises the conflict between personal and the Trust’s
concepts around care:“I came across this reference somewhere that it was alluding to the
different cultural backgrounds of staff, their different takes/perspectives on caring and… how
that sort of influences their interactions with people…, there may be people who might need
support, who are coming from traditions, cultures who may view ill-health as one thing, who
have paternalistic views on matters … ‘You listen to me, I am telling you what to do… I know
best, listen.’ And the person means well but they’re coming from a different paradigm
completely and it’s… not fitting with our model…”
Pam, a white nurse, draws on communication issues, particularly around language: “I
think a big issue… is something about communication because I think often if English is not
your first language, people’s ability to express themselves, and the cultural aspect of that is
quite hard to understand, and some people’s language skills are not so good.”
The next three participants consider the interpretation of aggression from a cultural
stance. Nelson, a BME administrator, states: “Sometimes there’s an issue about, the
159
cultural thing about the shouting and screaming and aggressiveness and that might be a
perception that that’s sort of cultural…”
Janice, a BME manager, gives her perspective: “I am of African descent and in Africa we
are quite animated, and… there’s [there are] some people who … are quite loud… but
people don’t understand that so they see it as aggressive…, I think it’s a lack of cultural
awareness…”
Hyacinth, a BME administrator, raises the issue of losing identity in order to be
accepted: “Our passion is seen as aggression and we have to know that we have to change
the way we are perceived, we have to be like the people who we are going to… And my
negative side took it as… we have got to change and be more white then…”
Both Denise and Shauna, who are white and involved in the disciplinary process, link
the differences of BME staff working practices to culture. Tolerance and interpretation
around the cultural differences towards behaviours and language are highlighted in
these interviews. Behaviours that might be perceived as aggressive are also
mentioned.
6.4 Perceptions of the disciplinary process
This section concentrates on the disciplinary process and is based on findings from
interviews. Attention is paid to managers dealing with BME staff, the use of
capabilities procedures, suspension of staff, the perceptions around the descriptive
statistics (from chapter 4) and the phenomenon investigated.
6.4.1 Perceptions of managers dealing with BME staff
In these interviews, there are perceptions that managers lack competency and are
apprehensive about dealing with issues involving BME staff. Lee, a white
160

administrator, states: “Management practice and competency, managers finding it perhaps
difficult to deal with diversity in teams, inconsistencies in how we apply the policies, …their
confidence levels, maybe depending on who is in front of them and how they might be
presenting themselves.”
Celia, a BME nurse, suggests elements of fear and why some managers quickly
resort to formal procedures: “It could be inefficient, they don’t know how to deal with
because they really are afraid of this race factor. Some of the things could be dealt with
informally but it was left to… reach crisis point.”
Peter, a BME manager, looks at the aptitude of managers: “There’s [There are]
probably questions and issues around how competent managers feel in dealing with and
managing diverse teams. And I know that because of issues that have cropped up within
services that I have been a part of helping to resolve … where you have got issues of race,
culture, African groups, white and black staff…”
Nellie, a BME nurse, raises the capability of managers: “If white staff perhaps more
likely to get dealt with informally, what is it about black staff that we tend to fail in dealing with
people in that way?”
As white managers involved in disciplinaries, these two interviewees discuss issues
related to prejudice. Hazel, a white manager, acknowledges: “I am not naive enough to
think that people aren’t prejudiced, I suppose we are all prejudiced in certain ways…”
Lisa, a white manager, explains prejudice informed from her childhood: “I worry that
my own… because no matter how you try and escape from your background and your
childhood, you will grow up with certain values and certain things that it’s quite hard to
challenge… I worry sometimes that I have always tried to escape from that, but you worry
whether you do completely escape from it or not… when I said you can’t escape cultural 161

background sometimes yourself, no matter how hard you try, so that you don’t mean to have
a prejudice but maybe that still comes up because you can’t escape totally from who you
were and who shaped you in your early life.”
Since the Trust Board has had to review staffing resulting from cost-saving measures
imposed by the coalition government, Gerard (a white nurse) has noticed a change of
approach: “We also need to look at the reasons people are getting disciplined for… ‘Is our
threshold too low, are we jumping more into formal routes?’ Historically we would have dealt
with them outside of the process and sat down and looked at it.”
The following interviewees focus on how managers deal with disciplinary issues.
Hazel, a white manager, in her experience shares how some managers have
exhausted all avenues and have had no alternatives but to take action: “Sometimes it
is a last resort in a legitimate way in terms of saying ‘Well I have met with them, I have
explained the standards, we have supervision, we have this… and do you know what?
Nothing has changed, and we are where we are, and therefore I have no alternative but… to
go down this route.’”
She later on also highlights some managers were waiting for a chance to initiate
disciplinary action: “‘This person has been a complete pain and they have done something
that is a bit out of line and I am going to take this opportunity and go for it’…”
Peter, a BME manager, discusses managers taking the opportunity to ‘go for it’ as
described by Hazel: “I can only go on what BME people have told me because I don’t know
the detail of their cases because a lot of staff come and talk to me about it, …it appears that
the manager… has had a vendetta against them and wanted to get them out for a long time
and was waiting for the opportunity, and when an opportunity came they pushed it all the
162

way.”Peter acknowledges that he only had partial representations of the facts, and
bias might have occurred as only one side of the situation has been shared with him.
Previous experience from practice in the private sector, and how this is transferred
into the NHS, might influence the haste towards disciplinary action, as Martina, a
BME administrator, points out: “If you have a manager that’s come from the private sector
and is new to the public sector, their expectation of how things are managed are quite
different, so sometimes they think well, we can quickly move to quite punitive action…”
Attention is drawn to the disparity between how managers treat BME staff and white
staff. Several perceptions of management attitudes emanate: a more formalised
approach is adopted to deal with the conduct and performance of staff; the approach
adopted ranges from having no alternative but to discipline to taking the first
opportunity to mete out disciplinary action.
6.4.2 Underuse of capability procedures
From secondary data collected, the Trust has a capability policy and procedures in
place to support staff who are underperforming. Gerard, a white nurse, expresses his
frustration that many of the cases he represents could have been avoided if
managers had used the capability and performance measures: “People shouldn’t
always be taken forward to disciplinary. There is not enough use of the capability and
performance policy made. We must have a more effective use of capability and performance
so it doesn’t progress to disciplinaries…”
Denise, a white nurse, comments on the revival of capability procedures by a recent
interim chief executive who has consequently reduced her attendance and
participation at formal disciplinary hearings: “But one good thing the previous… interim
163

chief executive did is make robust the whole capability process which was underutilised…
Well I have two requests… but not as many as there used to be…”
Capability procedures to support staff and prevent them from going straight to
disciplinaries are underused until the backing from a recent interim chief executive.
Since then, Denise reports she attends fewer hearings.
6.4.3 Suspension of staff
As the disciplinary policy states, the suspension of staff is a neutral act, used as a
last resort and not a disciplinary measure. Alternatives to suspending staff where
possible need to be considered. The use of suspensions and monitoring of this by
the Trust Board are discussed. Hazel, a white manager, conveys: “We try not to
suspend unless there are serious concerns about the potential for gross misconduct.” Later
she continues: “We were monitoring that because at one stage we had an awful lot of
people who were on suspension and we were… well we still are actually monitoring that on a
monthly basis… I know they have gone down…, it was… re-emphasising it with managers…
that… suspension should be a last resort.”
Leona, a BME clinician, has experienced accusations of not complying with
employment regulations and the threat of suspension used as a first sanction: “ I
haven’t breached anything, if I had the UK Border Agency would be at my door because they
have got everything about me on their system. So if the UK Border Agency aren’t coming
and knocking down my door, then why are you [HR] trying to suspend me… it infuriated
me…”
164
Although the threat of suspension was eventually dropped, Leona feels she has been
taken through a “cruel and stressful” process with no apology issued and: “everybody
has just acted as if nothing has happened, and ‘Well let’s sweep it under the carpet.’”
Gerard, a white nurse, discloses further the lack of sensitivity demonstrated by
managers around suspending staff: “Suspensions are ones in particular. I don’t think any
managers here have ever really understood what it’s like for people to be suspended – their
family life, their social life, their work life has gone…”
At a time of financial squeeze in the Trust, the economic cost of disciplinaries,
including suspensions, has not been calculated as Hazel, a white manager, states:
“No… It would be awful… because … you have a hearing, everybody gathers and
sometimes they don’t show up, sometimes you have to postpone, sometimes it goes on
longer than you think so you have to rearrange and reconvene, you have an appeal…”
Shauna, a white nurse, reports the lack of preparation and repercussions of a BME
employee returning to work after suspension and the impact this has on a team: “But
the person suspended was brought back to the ward without warning, so one day the people
turned up to work and she walks back on, having said all these things, in a safe environment,
a psychologically safe environment, and… she was there and she continued to harass them,
and now she knew that they had reported her… so they all went off sick.”
From the interviews, suspensions are not used as a last resort. Since the Trust Board
has taken an active interest in the subject, the numbers of suspensions have
declined. However, there is a perception that senior managers lack awareness of the
emotional impact of suspensions on those involved. Despite the fiscal pressure on
the Trust, the economic cost of disciplinaries to the organisation is unknown. In the
165

previous chapter, Monica also refers to the issues surrounding suspended
employees reintegrating into the clinical team without any preparation and support
from management.
6.4.4 Perceptions around the descriptive statistics
Within the Trust, opinions vary among staff about the over-representation of BME
employees in the disciplinary process. These interviews highlight the difference. The
perceptions held by some senior managers that BME staff of lower bandings were
more likely to be disciplined was dispelled by the recent workforce data, as Hazel, a
white manager, highlights: “You assume it’s the lower banded people that get disciplined
more because they’re more junior and they may not be aware or they may not care or
whatever, …but actually this year’s or last year’s figures look like we have disciplined more
senior people which is interesting, and that kind of flies in the face of what people…
thought…”
Tariq, a BME clinician, observes management’s presentation of the disproportional
representation: “Senior management and all the people who were leading it were telling us
this is more of a perception rather than reality.” He continues by citing the Astar* report
that identifies the disproportional representation of BME staff: “it is not a perception, it’s
actually a reality, a day-to-day experience of BME staff … I think the reality is people who
are… maybe not of BME background… I don’t think they get it… you have to be black and
after receiving it, in order to know it…”
*Management consultants commissioned by the Trust to write a report. Several employees referred
to this report. This report was not obtained despite numerous requests made.
166

Leona, a BME clinician, draws on the Delivering Race Equality (DRE) report (DoH,
2005): “All the data and the statistics collected, especially during the DRE, …clearly showed
the over-representation of BME people…”
Nelson, a BME administrator, holds an opposite view to Tariq and Leona: “ I am not as
convinced about the over-representation of BME staff in disciplinaries. There are issues, I do
believe that, in terms of race or racial and cultural awareness… but I am not sure that there
is a hidden agenda which I think many people feel, so I am not sure if I agree with that.”
Denise, a white nurse, stipulates the proportions of the number of BME nurses at
particular bandings need to be compared to the number of BME staff disciplined:
“You could say, quite rightly, nurses are over-represented in disciplinary hearings… so
looking at proportion of staff that we have that is from BME groups at the lower bands is
huge. Is it that there is an over-representation taking into account that 80% of our people at
that level are from a BME group?”
The context of the numbers of BME staff working in clinical and other areas needs to
be considered according to Monica, a BME manager: “When we talk about the over-
representation I think we should also look at the workforce itself. …I think in this team for
argument’s sake, if we say we were about 12 people there and the four people suspended,
they are all black (and they were), were the other eight white? No. I think the other eight–
maybe about four or five of them were black so it’s only minority were white, but none of the
minority white was disciplined.”
Nellie, a BME nurse, goes beyond the polarised debate and acknowledges action
needs to be taken around disciplinaries involving BME staff: “I think it started by saying
it was a perception when the survey was done and people were saying still yes, we have a
167

higher proportion number of people in disciplinaries, and there is acknowledgement that what
are we particularly doing about it?”
These participants have different opinions about the apparent over-representation of
BME staff involved in disciplinaries. The debate is not polarised as a black versus
white issue particularly as Monica and Nelson, who are BME, dismiss the
phenomenon.
6.4.5 Perceptions of the phenomenon investigated
Apart from race and ethnicity, Hazel, a white manager, highlights the complexity of
the phenomenon and looks at other factors that may be associated with
disciplinaries: “If time was no object I would love to do it across the board. I would love to
say ‘Are more men disciplined than women?’ … we do not have great figures on
disabilities…, people’s sexual orientation… Are people victimised because of their sexual
orientation?”
Despite significant factors raised, the Trust does not collate figures on the sexual
orientation and disabilities of employees under investigation.
6.5 Perceptions of employees directly involved in the disciplinary
process
The aim of the Trust’s Disciplinary Policy is to: “Facilitate satisfactory standards of
conduct and performance, to encourage improvements where appropriate and to
ensure that cases of alleged misconduct, unacceptable performance or other acts or
omissions are investigated properly and where disciplinary action is necessary all
cases are dealt with consistently and fairly.”
168

The disciplinary policy identifies the stages and the role of key people involved in the
process. A summary of the disciplinary stages and the employees involved in the
disciplinary is provided in Appendix 1.
Findings from the interviews with employees directly involved in the disciplinary
process are highlighted in this section.
6.5.1 Role of an IO
All investigations around disciplinaries are undertaken by an IO. Issues around
training to undertake the role of an IO are discussed in the following interviews. Paul,
a white manager, declares: “I have been trained on investigating complaints and
allegations against staff so I have been trained in that, and I have been trained in root cause
analysis which I think… that helps when you are investigating something because you look
for different things and maybe that’s where the human element comes in.”
Matt, a white nurse, similarly states: “I have had root cause analysis training with an
external facilitator of the Trust, and also the Being Open training. …which I think has been
relevant; I did some Expert Witness training.”
Gerard, a white nurse, on the other hand, has not received any formal training and
relies on informal support: “None, none. You may be able to ask a senior colleague who is
an experienced colleague who has done it before, ‘How do I do this?’ but there is no training
available…”
Drawing on hindsight, Gerard continues: “Thinking back, I think what would have been
most helpful to be able to shadow somebody undertaking that process so that you really had
a sense of what the roles and responsibilities were with that.”
169

Celia, a BME nurse, who has received no formal training, explains why training
should be provided to undertake the role of an IO: “Yes. There should be training for
everyone who does it…, so it’s a consistent approach… Because the way I investigate will be
slightly different to the way someone else does it or looks at it, and perceives the situation,
so it’s a lot of disparity depending on… what kind of person you are as well. And personality
comes into it, of what you’re looking for. If you are looking to kind of push someone out, you
might look a lot harder and try and dig a lot more to find ways to do it, whereas others won’t,
they’ll just look honestly, more honestly at the situation.”
It is reported that not all IOs have received formal training to undertake investigations
related to disciplinary hearings. Celia advocates training to minimise disparity and
ensure fairness in the investigation. Some IOs look beyond the ‘facts’ for further
evidence to remove the employee under investigation.
6.5.2 Lack of training to undertake the role of chair
All disciplinary hearings have a chairperson to oversee the proceedings. Again,
issues around training to undertake this role are highlighted. The lack of training to
undertake the role of chair is a concern for Pam (a white nurse): “I think there is a huge
gap really in terms of provision for staff training because your decision can be quite life-
changing for people. And if you don’t get it right, the amount of stress, the amount of damage
that you could cause to someone’s career is quite huge. So I think that we should have
training…”
Pam continues to raise concerns, particularly around managing legal issues: “As I
have progressed in my nursing life, as I get older, older and more mature, cases are really
complex… They have lots of legal aspects to them, and one thing I have tempted to have a
conversation with, although people are in disagreement, is actually don’t most people need a
170
lawyer, never mind a union rep… I sometimes think it’s more sophisticated than our
experience and training allows us to be and operate in those roles…”
Marcia, a BME nurse, also mentions the need for training: “I don’t think I was prepared
to find myself in that role defending our decision as a panel which extends beyond nursing
practice, so for that gap I think we need training to help us understand what, as a panel, you
are considering.”
The burden of responsibility, particularly around consequences, is raised by Pam,
who felt her training and experience did not adequately prepare her to undertake this
role. Marcia shares concerns of being out of her depth when asked to justify the
decision made by the chair who was unable to attend an employment tribunal.
6.5.3 Diminished administrative support
In recent years, administrative support offered to IOs has been withdrawn. Shauna, a
white nurse, discusses the repercussions of this: “Even admin support, because if you
are doing an investigation as I did on… where what I heard was so unbelievable I decided to
interview every single person… The Medical Director who has been to see me personally
twice to say ‘Where is the report…? I want the report.’ No admin support so I am typing… I
mean I went to nursing school…”
In the previous chapter, Monica also complains about the diminished administrative
support (as experienced by Marcia) and the delays in cases proceeding within the
timeframe of the Trust policy.
6.5.4 Conducting investigations
These interviews highlight how investigations are undertaken. Celia, a BME nurse,
explains distinguishing facts from emotions: “Well actually the fairest way of treating
171

someone is to look at the bare facts. What I feel is neither here nor there sometimes because
what I feel can fluctuate and can change, but actually if the facts remain the same, then that
should be the way that we make judgements about whether something is right or wrong.”
Pam, a white nurse, emphasises the skills needed to facilitate the investigation and
scrutinise the information: “And actually investigatory skills are one of the key things you
do need, both in terms of being on the panel or whether you are the manager presenting the
case, partly because you need to really question and be able to look at evidence and data
and to make sure it matches and… The other skill you need is to assist the individual to talk
and not to make a judgement in an accusatory way…”
Denise, a white nurse, highlights the quality of investigation is not always factual: “My
last hearing was… for the first time it was a dismissal that I overturned because the quality of
the investigation was really quite poor and I felt that there had been a tendency to want to
dredge for statements…”
Gerard, a white nurse, reveals the process around disciplinaries is not always
adhered to: “So I think managers aren’t mentored, trained and supervised enough when
they’re going in to making a presentation…, I am interested that the process was followed
and that it was fair, that the person presenting the management side knows what they’re
doing, has got all the facts, has interviewed everybody, has got a chronology of timeline, has
done everything they need to do before we go in there, and if they haven’t, forget it, because
the Trust will always lose.”
Investigations are not always based on ‘facts’ from the findings. Sometimes
judgements and unrelated opinions are included. Hearings where the process around
disciplinaries is not followed and poor-quality evidence is presented have led to some
cases being dismissed.
172

Attention is drawn to the relationship between the IO and HR personnel in preparing
the report from the disciplinary investigation. Marcia, a BME nurse, points out the
dilemma of what to include in the report: “Surely, at this stage of collecting information we
can’t start dismissing certain information as not relevant when it’s been highlighted to us. It
just needs to go into the report and let the panel make a decision.”
From this extract, Celia (a BME nurse) questions the influence and neutrality of HR
personnel: “Sometimes I get a sense from HR, …who are supporting me… to actually err on
the side of management. I get that sometimes… you’re asking me to do these things which
are sort of taking me away from being the neutral person… you are now asking me to
present information in such a way that I am saying that this person is guilty when actually
that’s not for me to say…”
Celia continues to discuss the tensions of an experience around a white member of
staff under investigation: “The other case it was a white person… the HR person, …they
were making me feel… they were being dismissive of certain information which I thought was
pertinent. So the HR person was saying ‘Well, that’s not important’ and I was saying ‘Well I
can’t say that’s not important, it’s information that we have received, it needs to go into the
report. We can’t start making judgements about whether it’s important or not for this case,’ …
this HR support person… was actually trying to create a situation where the report would sort
of not highlight the real issues that were going on for this person, … the case was a white
case.”
From Martina’s (a BME administrator) point of view, the competency and experience
of the IO determines how much input the HR representative has on the investigation:
“Again it depends on the competence of the manager who is leading on it… I may end up
stepping in and answering the questions for the manager… So a lot of the time then I can be
173
seen as the person making the decision and so therefore I will be viewed very negatively. …
the manager… may say ‘HR has made me do this, we don’t really want to manage you, HR
are making you do this.’”
The neutrality of HR support in presenting the findings from an investigation is
highlighted. There is a perception that HR personnel influence what to include or
exclude in the investigation report. On the other hand, Martina highlights the HR
advisor might be forced to step in, particularly if responsibility was abdicated by the
IO.
The support from the HR department is highlighted in these next two interviews.
Pam, a white nurse, reports: “When you are investigating you have got support from HR…
I have never been in a situation where I have been left on my own to do an investigation and
to report on it without HR support, so that’s been fantastic.”
Gerard, a white nurse, states: “I think we have a terrific HR department here. I think we
do, however, lack an HR manager from a BME background for specific cases…”
Leona, a BME clinician, who was threatened with disciplinary action, discloses her
negative experience of HR personnel: “And I felt that HR are a part of the organisation
that is meant to work with the human beings, ‘human’ being the key word… There is nobody
I would go to in HR to talk to about anything to do with my personal life, or to deal with any
problems that I am having at work, nobody.”
Peter, a BME manager, echoes the view held by many BME staff: “HR don’t do the
human side of it. Amongst a lot of BME staff, the perception of HR is very… it’s a collusive
place, they are not trusted, the managers or the staff. It’s quite a sweeping statement but a
lot of BME staff are… saying ‘…I don’t trust people in HR…’”
174

George, a white nurse, conveys a similar experience to Celia, above: “The staff
perception of HR is that they are basically part of the management… and I always say to
them that you are supposed to be neutral, and you’re supposed to be looking after the
interests of the staff…”
Employees undertaking investigations report support and a positive experience from
HR. However, on the other side, some employees do not trust HR as they perceive
them not to be impartial and on the side of management.
6.5.5 Relationships between the investigating team and investigated employees
The relationship between the investigating team and the employee under
investigation is further explored. Shauna, a white nurse, states: “I think if you’re the
investigating officer, they can… ‘Well if I can put my case to you and you can get it, then
that’s OK.’ But then there is the other thing you’re almost the enemy straight away.”
Nelson, a BME IO, raises his experience of investigating BME staff: “If a black person
for example comes into a meeting and they see another black face it’s phew! ‘OK, maybe I
have got a chance’… I just have the sense that they’re feeling relieved that I am there – but it
just could be me… it’s about the way that people might look at me.”
Celia, a BME nurse, describes the reactions and behaviours of a black member of
staff: “…a black person is trying by all means to get me to be on their side, to really try to get
me to understand and to present the case in such a way that it’s in their favour… And
somehow, because I am also black…, I have just had to say to them, ‘Look, my role in this
case is to get the facts, and to present the facts to the panel… to make a judgement.’”
Continuing with this case, Celia discusses her reactions of how she might be viewed.
She contrasts this experience with that of white staff being investigated: “I can see a
175

sense of disappointment there. I could almost imagine them going out saying ‘Ah, this black
sister of mine! …If your own people are going to treat you like this, then hey what chance do
you have?’ …I haven’t got the sense from when I am investigating white people’s cases for
example…”
Martina, a BME administrator, comments as an HR advisor having a similar cultural
background to an employee under investigation: “I have seen a lot of West African staff
that have been subject to disciplinaries. I see… the way that they line manage, and maybe I
am more lenient towards that or more understanding… I can see the personality traits or
cultural traits that I can identify with, … I think there had been a couple of disciplinaries…
with West African staff, my response was actually … well due to the nature of the
misconduct… that’s not a cultural thing, that’s a personality issue…”
Further reactions from Celia (a BME nurse) around neutrality, emotions and
judgement from the IO towards the employee being investigated are described: “A lot
of times I think I sympathise… I understand some of the pressures that they might be going
through. I can see sometimes where things have been difficult for them – I am a nurse, I
know what it’s like to work under the front end, so I do see the challenges that they face…”
The relationships between the BME IO/HR advisor and BME employee under
investigation are highlighted. Martina recognises and is also asked to verify cultural
behaviour of staff from a similar background. Keeping ‘neutrality’ and reserving
judgements is not always easy.
6.5.6 The disciplinary panel
The disciplinary panel consists of the chair, professional lead and an HR manager.
Gerard, a white manager, comments on the ethnic diversity of the panel: “Panel
176
composition has improved because it’s moved from predominantly white panels to being
more diverse…”
Denzel, a BME official, separately echoes Gerard’s perception: “There used to be…
only the white panel making the decision, judging, but now you can see, sometimes you can
have all black and BME occasionally…”
Gerard and Denzel report that disciplinary panels are more ethnically diverse with
significant improvements. These next two interviews uncover some of the motives
behind choosing BME employees from the Trust to sit on the panel hearing cases
involving BME staff. Marcia, a BME nurse, reveals: “I have been asked explicitly to sit on
a panel because I am black. I don’t know whether you have met X, she has been asked
explicitly saying ‘We want you on the panel because you’re black…’ But I was there to
assess whether this lady from Namibia… I was asked to help with the competency.
Interestingly when we went to do the competency assessment, she didn’t even relate to me,
she didn’t even want to talk to me… I do not know what the Namibian culture is. We share
the same shade of skin, that’s almost about all… it was bandied there in the hearing, ‘You
are here to provide a cultural perspective.’ I mean for a nurse not to be able to understand
the medication procedures is not a cultural issue, it’s a competence issue…”
Nelson, a BME administrator, discloses: “We were the decision-makers so it was down to
us… Once the case had been presented by the investigating officers, it was down to us to
decide whether the allegations were proven… It ended up that we did dismiss this black lady.
And the two people who were charged with, if you like, dismissing her, were black… And that
case, probably more than any other, made me actually reflect, has this been done on
purpose or deliberately to sort of allay any future accusations of race, racial bias or racial
discrimination? Somebody black has been dismissed by two black people… it can’t be
racist.”
177
In the first interview, sharing the same skin colour is equated to the assumption that
these two people share the same culture when this is not the case. The other
interview reveals two BME panel members are specifically selected for a disciplinary
panel involving a BME employee being dismissed. Nelson speculates on some of the
underlying reasons.
Perceptions of a fellow panel member’s attitude are revealed in this interview. Celia,
a BME nurse, observes: “The one that really comes to mind is ridiculous – I don’t
understand what this guy is saying…, this is my panel member saying… and you can see
them switching off. So this person is trying to explain in whatever way that they can, with the
language barriers that they might have, and you can see it in the discussion where they’re
being cut off in mid-sentence, so they haven’t quite finished explaining what they’re saying…
And I am thinking well, this is about someone’s life is at stake here, can we not allow
someone to express themselves so we can try and understand where they are coming
from?”
Celia exposes the lack of tolerance and perseverance from a panel member to allow
a BME employee under investigation to give a representation of their case.
6.5.7 Role of the professional lead
Each disciplinary panel has a professional lead that comes from the same discipline
as the employee under investigation. Denise, a white nurse, describes her role as a
professional lead: “The person who is sitting before me is a nurse who I am judging her on
the quality of the investigation and what the impact is on practice and whether they can
practise again safely as a nurse. My prime consideration always has to be safety of the
public.”
178

As a professional lead, Pam (a white nurse) considers conscious and unconscious
motivating factors: “Yes, so whether it’s motivated by racism or motivated by … a difficult
relationship because you don’t like somebody of a particular cultural group… when I am on
the advisory panel, certainly in the management case, I do look at those types of
relationships in a … conscious and unconscious way because I think they’re very important
influencing factors.”
Celia, a BME nurse, considers her reactions when listening to the conditions and
pressures placed on nurses: “It’s very emotive when you sit there and you hear what
nurses are doing, how they are working over and above what’s expected of them… I sit there
and we are making such harsh decisions – that always … really doesn’t sit comfortably with
me. If someone has crossed the line, …I always find it… very difficult because it’s… what I
am presented with, this case, doesn’t tell me about the individual nurse in total, about their
whole nursing career in what they have given…”
An insight is given into the role and position of the professional lead in disciplinary
hearings. There is some acknowledgement by a nursing professional lead of the
conditions and pressures faced by nurses on a daily basis. Deciding on the future of
the nurse under investigation without knowing all their experience and commitment
presents a challenge for some professional leads.
As another panel member, Gerard, a white nurse, gives his perception of the
attitudes of professional leads: “My experience of professional leads, it’s almost as though
they want to come up with the harshest sanctions for their own members than anybody
else… It’s almost as though you must beat your staff up… more than anybody else to prove
your independence…”
179

From Gerard’s experience, the sanctions recommended by professional leads from
the same discipline appear to be disproportionate.
Denzel, a BME official, gives his perceptions of the disciplinary panel: “I don’t think all
managers are trained into handling disciplinary… I can see it straight away when I look at the
panel… and I think ‘Oh, I think I may have an easy ride,’ or ‘Oh, I will have a tough ride.’”
He explains: “An easy ride is if they understand and I can manage to persuade them to see
our point of view as to why we made a mistake or where we went wrong, and please try to
see it in the context of the whole case. A tough ride would be… if they say ‘Theft is theft, I
don’t want to know anything else,’ or ‘You were sleeping, full stop.’ It doesn’t matter what the
staffing level was, how tired you were, what your caseload is, …that is a rough ride…”
Denzel could pre-judge the proceedings and outcome depending on the personality
and flexibility of panel members who are present at the hearing.
6.5.8 Perceptions of TU representation
All employees who are under disciplinary investigation have the right to be
accompanied by a TU representative at all stages of the formal procedures. This is
on the proviso that they have joined a TU before the investigation. Gerard, a white
nurse, reveals his frustration about the quality of TU representation that he has
witnessed: “The thing that irritates me is when people are clearly not being represented
well, you know they have only just met them or the union rep is sitting there from whichever
department and doesn’t know anything about the case…”
Celia, a BME nurse, appreciates the depth of knowledge provided by TU officials
about the wider context and failures of systems that might be particularly unknown to
the panel: “The union rep… usually understands the Trust’s workings, so… they can make
180

sound arguments about mitigating factors. …they might say ‘Well actually I know that within
this team, …they have had special measures’, which is something which perhaps me sitting
on the panel wouldn’t necessarily know. But they’ll be using that information to try and sort of
build a case for this person, that actually perhaps they have been left in a situation where the
Trust hasn’t fulfilled some of its responsibilities because actually if a team is totally failing,
how can you then pull out one individual member of that team and say you’re not
performing?”
Hazel, a white manager, highlights the position of TUs against management: “I think if
you talk to unions, they will probably say that HR are part of management and therefore we
are not that objective… In a public forum, the rep will take a certain role which we accept
that’s what they do… but sometimes the rep doesn’t always behave appropriately.”
George, a white nurse, questions the attributes and standing of some TU officials in
their presentation and representation of employees under investigation: “Within our
Trust some reps go all guns blazing but… I don’t think they always give the right advice… I
know that the Trust don’t [doesn’t] take some reps seriously… at a senior level. So when
somebody is in deep trouble…, they’re not on their own but they’re not particularly well
protected.”
Lyn, a BME employee, who had a disciplinary action initiated against her, expresses
her anger about inadequate TU representation from the BME official: “‘I [the TU
official] just wanted to say I could never have produced anything like this’ which didn’t help
me because I actually felt very angry. I just thought you’re a union representative and you’re
telling me that you couldn’t produce this, so I was really quite annoyed.”
Denzel, a BME official, speculates how his role might be perceived: “I have two
camps… There are those who will be really, really grateful to you and say ‘Thank you very
181

much. If it wasn’t for you I wouldn’t have been able to do this or that and I appreciate all your
help.’ Sadly there is still a section of staff who see me and may think… ‘you are part of the
management, we don’t know whether to trust you, whether you’ll listen as part of
management, we are all in together’…”
A conflict of interest around roles could emerge, as described by Gerard. TU officials
are able to provide further details unknown to panel members about the context and
the setting. Opinions towards TU officials are centred on how they present the case
for the employee under investigation and the outcome of the hearing.
6.5.9 The employee under investigation
Over a period of time, Shauna, a white nurse, has noted the variance of the
behaviours exhibited by BME staff under investigation: “A whole range of behaviours
really from people who are so upset and genuinely anxious and worried and allegations were
made against them – they just can’t believe it. And you can tell that it’s really had an effect on
them, right through to someone who is just sort of really quite blasé about it. And with one
case I really felt… even though the person had been suspended, they didn’t get the enormity
of what was happening to them … and maybe that was just how they were coping with it…”
Lisa, a white nurse, observes the capacity of staff under investigation to reflect,
demonstrate insight and accept responsibility has some bearing on the outcome: “I
think it makes a difference when staff take responsibility… for what has happened, so for the
people who show remorse, show insight…”
Celia, a BME nurse, gives some understanding of defensive behaviour and considers
some of the underlying factors that might motivate this behaviour in the disciplinary
hearing: “Different people respond in different ways, and somebody could be seen as being
defensive because they’re anxious. I think when somebody is put on the spot… you want to
182

articulate and defend your position or explain what it is you do, and if you feel then that
you’re not being heard, then you might get a bit more anxious, your voice might become a bit
more abrupt – not because you’re being abrupt but the situation and the circumstances
influence that. …I certainly have seen a situation where someone interrupted one of the
panel members as they were asking a question and somebody then interrupted them before
they finished, and that created some tension. And one of those instances was somebody
from a black and BME background who interrupted. I think it was because they wanted to get
their point across, so they could see how the question was developing so they sort of tried to
answer quickly.”
Lisa, a white manager, tries to empathise with BME staff attending the disciplinary
hearing: “I don’t know what it’s like for the person where the allegation has been made, what
it’s like if they feel they’re from a different cultural group and they’re sitting in front of an all-
white panel say.”
Several behaviours are noted about the employee under investigation. The capacity
of the employee to demonstrate awareness of the concerns raised is deemed
significant by panel members. The chair acknowledges the impact of the stress of the
hearing on the behaviour of the employee having to account for the issues raised.
6.5.10 Mitigating circumstances
Extenuating circumstances for the conduct and clinical practice that are under
investigation is considered in these interviews. The circumstances are related to the
working context, professional support, supervision and personal situation.
Marcia, a BME nurse, describes the context of the work environment and specific
factors that might have influenced the conduct and practice of staff under
183

investigation: “An increased workload… environment, resources, staffing levels, all of those
things are relevant…”
Celia, a BME nurse, reveals mitigating circumstances for a nurse who has been
suspended from her duties: “And so the sickness level was up, people were demotivated,
probably stressed and burnt out. There have been issues about poor practice on the ward.
Now I am investigating and people were suspended in relation to that poor practice, and
when I investigated I found that they’re often short of nurses, obviously people don’t want/like
working on the ward, and people did their very, very best and sometimes the standards were
short of what we would expect because of the circumstances. Somebody was observed to be
restraining inappropriately, but she was the only nurse… there was [were] only two nurses
and a patient that kicked off, so she did the best she could. Somebody who walked in the
ward observed that and the nurse was suspended.”
Paul, as a white chair, provides a space and an opportunity within the hearing for
employees to highlight anything extenuating contributing to their poor conduct and
practice: “I try and make space for it in the hearing, to understand the mitigating
circumstances, so if you have got a single parent who has been putting masses of extra
hours in because of their income issues or… so at least try and weigh what the mitigating
factors are.”
Lisa, a white manager, reports some shocking mitigating circumstances for
employees breaking the law on employment hours: “There was a BME woman that I
think she had worked something like 70 days on a roll without a break… She brought some
mitigating circumstances. Her partner had left her in the lurch with lots and lots of debt that
he had… and she was trying to work it off… So she did bring some mitigating circumstances
to that one which helped her cause.”
184

Lisa also takes into account the mitigating evidence in the context of the employee’s
attitude, which has some bearing on the outcome: “I met an ex member of staff some
while back, and I think she has probably gone on doing what she did, if she can get away
with it in other hospitals and she was quite defiant about it, she didn’t see that… ‘Well I am a
good nurse and… the fact I am working 20-hour shifts effectively is not a problem.’ So she
was someone that actually dismissing her was the right thing to do because she is not taking
it on board.”
Matt, a white nurse, reports a common subject arising at the disciplinary: “ I mean the
theme that emerges is the lack of supervision, …appraisal, objectives are not articulated. …I
mean there’s no role modelling…”
Marcia, a BME nurse, refers to managers and supervisors ‘turning a blind eye’: “With
better supervision, candid conversations… – if those happened earlier we would see less
people come to the disciplinary because what I think happens, the behaviours perpetuate,
mainly because they haven’t been addressed. …I see somebody who has really done
something that’s really disciplinable, but when you look back and I say ‘OK, tell me about it,
how did you come to this, how have you arrived here?’ And I often find, they say ‘Oh well,
since 2002 this has been happening.’”
The professional support given to people under investigation at a hearing needs to
be formalised according to Hazel, a white manager: “Routinely we should be asking
managers who are preparing a management case at a disciplinary to give us supervision,
appraisals records, one-to-one records; it should be part and parcel of the written case… I
am a firm believer that more and better supervision would prevent some of them (not all of
them)…”
185

Gerard, a white nurse, discloses supervision and appraisal are raised by the defence
team: “The truth will always be out and the number of cases that come before disciplinaries
where I will say ‘Was this identified in your last appraisal?’ ‘I don’t remember my last
appraisal.’… As a union rep, I would attempt to dismiss any disciplinaries where no
supervision has taken place…”
Denzel, a BME official found in his investigations: “In my opinion at least 50% because
people were not supervised…, issues were not identified through supervision… If I were
subject to one of these disciplinaries because my manager hadn’t heard me…, I would be
making a grievance against them for not identifying my shortcomings or weaknesses at a
very early stage…”
6.5.11 Reactions to disciplinary outcomes
Regarding making judgements, Denise, a white nurse and appeals panel member,
stresses the decision needs to be based on facts incorporating E&D practices: “The
chair need[s] to be seen to make decisions on the basis of fact, transparent facts, not
supposition and I think that’s particularly important when some white people, not all, some
white people are cautious about making decisions that involve BME groups. …they need
to… have confidence that they are doing the right thing that is based in good equality and
diversity practice, and is transparent and defensible to the Trust staff and beyond.”
Having been in both roles (as an IO and panel member), Celia(a BME nurse) talks
about an experience as an IO when she disagreed with the panel’s decision: “ I mean
there’s a case that I did which was about nursing practice and I seriously felt that this BME
person was working way, way beyond par, it was something that I wouldn’t even have
expected a student nurse not to get right, and I had huge concerns about that person’s ability
to deliver safe care. And when I presented the case to the panel, the outcome was that well,
186

actually this person should be downgraded and put on the ward, and I was thinking well
actually putting them on the ward, they are still unsafe…”
Celia, a BME nurse, who has also been a professional lead, expresses her frustration
around the inconsistency of sanctions applied around similar cases: “ I suppose my
main frustrations with sitting on the other side is my panel members in a way, because there
are times when I have sat on the panel and I have thought my colleagues are not very
appreciative of … Well they have got varying standards of sanction, and I have often
wondered why are we giving certain sanctions in this case, and yet two weeks ago when I
was in a similar case, the sanction was not as severe, what is that about?”
Shauna, a white nurse, discusses the sanctions given for poor administrative tasks
being more harsh than for a failure to provide basic nursing care to patients: “I am
talking about where I was frustrated sitting on the other side and presenting this case and
clearly someone can’t do basic nursing care, I think a month or two months later I was sitting
on a panel, the case was being presented, the nurse has not documented…, the nurse has
used language which perhaps can be misinterpreted – not because they intentionally intend
to do that but there’s a language barrier…”
Part of making a properly considered decision involves incorporating, where
necessary, E&D practices. It is reported that white chairpersons of hearings are too
cautious making decisions involving BME staff. Outcomes for similar cases are
inconsistent. Cases involving legal and bureaucratic issues are treated more severely
than cases involving poor basic care.
Denise, a white nurse, expresses the differences in outcomes: “It’s been one of my
beef for quite a long time… you would expect to look to see that the same penalty is being
187
applied across all cases… I think the Trust hasn’t done as much as it could to look at…
What’s the penalty being applied here? Are we being fair across professions?”
Celia, a BME nurse, makes another brief comparison: “I mean I sit on panels where…
the two cases that I gave as examples actually were one… the person that I felt should have
been fired was a white person, and the person that I felt was being harshly treated was a
black person… it appears to me as if there’s always… much, much harsher outcomes for
BME staff than there is for white counterparts.”
There is disparity in outcomes for similar cases and BME employees are perceived
as being treated more harshly than their white counterparts.
Denzel, a BME official, notes the reasons for the disparity of outcomes results from
articulation, the capacity to reflect on the incident and showing remorse: “That’s where
the cultural thing and the communication comes in. Some of my BME staff gets a harsher
punishment than a non-BME, because the other person may be able to articulate, and then
most of the times the panel want an acknowledgement from the member to say ‘Look I did
something wrong and I won’t do it again’. A white person is better to articulate that better –
this is my experience…”
Shauna, a white nurse, mentions racial bias fleetingly in addition to articulation skills
and demonstrating remorse: “It’s just maybe… just a racial bias thing… perhaps cases are
not given a fair hearing as people are frustrated with language barriers… and therefore…
don’t get to the bottom of things, or they just get frustrated with not understanding someone’s
dialect of whatever. … Usually white counterparts, they are more articulate, they can present
their cases quite clearly and succinctly and to the point. The manner in which they come
across, you could say they are quick to apologise for things that they have done wrong.”
188
The outcome from the hearing in some cases depends on the skills of the employee
under investigation to articulate, demonstrate insight and accept responsibility when
transgression has occurred. There is a perception that white staff could demonstrate
these skills better than their BME counterparts.
6.6 Conclusion
Table 1 provides a summary of the key themes from the findings. The findings from
the descriptive statistics, observations and interviews from a disciplinary hearing and
this chapter will be summarised and discussed in the next chapter.
189
Table 1: Summary of the key themes
The Trust Perceptions of BME employees in the Trust
Perceptions of the disciplinary process
Perceptions of employees directly involved in the disciplinary process
The pressure to secure FT status Links to the historical, societal, political and personal context
Perceptions of managers dealing with BME staff
Role of an IO
Reconfiguration of services Perceptions of BME employees particularly black African nurses
Underuse of capabilities procedures
Lack of training to undertake the role of chair
Recruitment of BME staff Perceptions of relationships and tensions between BME employees
Suspension of staff Diminished administrative support
Perceptions around the Trust’s E&D initiatives
Perceptions of BME staff commitment and lack of trust placed on them
Perceptions around the descriptive statistics
Conducting investigations
Perceptions towards the study Perceptions of BME employees treated unfairly
Perceptions of the phenomenon investigated
Relationships between the investigating team and investigated employees
Observations of behaviours Playing the ‘race card’ The disciplinary panel
Perceptions of cultural differences in working practices
Role of the professional lead
Perceptions of TU representation
The employee under investigation
Mitigating circumstances
Reactions to disciplinary outcomes
190

Chapter 7: Discussion
7.1 Introduction
This chapter discusses the results from the previous three chapters. A summary of
the findings is presented in Table 1 (p191).
7.2 Discussion of the findings
Focused and critical ethnography was undertaken to explore why there was
disproportional representation of BME employees in the disciplinary process in an
NHS Trust. To understand this phenomenon, admittance was needed to a Trust
willing to allow an ‘outsider’ to investigate the culture and obtain access to the
‘multiple realities’ on a sensitive and ‘taboo’ subject in the natural setting (McGarry,
2010).
My literature review revealed a dearth of studies that had used ethnographic
approaches to explore these issues. Participant observations were carried out within
an NHS Trust and employees directly involved in the disciplinary process were
interviewed. In addition, a disciplinary hearing was observed.
The discussion is divided into three sections: the Trust; BME employees;
disciplinaries. This reflects the presentation of the findings in the results chapters.
7.3 The Trust
In this study, to understand the disproportional representation of BME employees
involved in the disciplinary process, the context and the culture of the Trust was
considered. Unstable leadership, at a senior level, within the Trust and continual
disaggregation and reconfiguration of services were issues that appeared to 191
contribute to the disproportionate representation of BME employees involved in the
disciplinary process. To a certain extent, these issues were reflected in the literature
reviewed. The RCM (2012) found that midwives were over-represented in disciplinary
proceedings. Their report recommended investigation of organisational culture,
management practice and leadership in the NHS. Carter (2000), Cooke (2006a and
b), Archibong and Darr (2010) and Stone et al. (2011) highlighted that organisational
factors, management practices and styles contributed to poor standards and
discrimination.
7.3.1. Leadership in the Trust
My findings highlighted the fact that the Trust has failed to secure FT status. Two
bids had already been turned down and a third application was in the process of
development. If that were to fail, the future of the Trust in its present form is
uncertain. To achieve FT status, the Trust needs to demonstrate that it is financially
viable and legally constituted (DoH, 2008). Added to the Trust’s burden, the coalition-
led government in 2010 imposed a £20 billion saving cost on the NHS (King’s Fund,
2011). Interview data with participants and data from my observations indicated that
strong, stable, consistent and effective leadership from the chief executive with the
support of the Trust Board was needed to steer the Trust to FT status. Analysis from
this study implied that this has been weak from the top of the organisation.
During the past eight years, there has been a high turnover of chief executives. The
continual change of chief executives has led to uncertainty and instability in the Trust.
With the preoccupation to secure FT status, chief executives and the Trust Board
have been unable to take a Janus-like position and have lost touch with the day to
day experiences of employees at the grassroots. This study found a gulf between
192
those at the top of the organisation and clinicians delivering clinical care. From
participant observations, staff surveys and interviews a sense of cynicism, a lack of
trust and confidence towards the Trust Board and senior managers was found
particularly amongst nurses.
The uncertainty of the Trust’s future and the lack of its clear leadership came up in
the interviews. This has had a destabilising impact on the workforce, which has
affected staff morale and their motivation. Initially, Trust employees have tried to
adapt to the prerequisite of each new chief executives who have been in post for
brief periods. However, some employees reported that they have disengaged to
adapt to the frequent changes of chief executives. Participants also recounted feeling
despondent, angry and tired caused by the lack of direction and inconsistent
leadership.
7.3.2 The impact of disaggregation and reconfiguration on services and staff
To make itself financially viable and meet the changes in care and treatment, the
Trust has had to review its services and resources particularly staff. As a
consequence of government policies (Modernising Mental Health Services: Safe,
Sound and Supportive, DoH 1998; The National Service Framework for Mental
Health: Modern Standards and Service Model, DoH 1999; The NHS Plan, DoH 2000;
The National Service Framework for Mental Health: Five years on, DoH, 2004),
treatment has moved from inpatient to community settings and some services have
been disaggregated and reconfigured to accommodate the changes. With the
number of inpatient beds being reduced, more emphasis has been placed on treating
patients in the community. Patients are only admitted to inpatient settings if they
193

cannot be safely treated and managed in the community. Once stabilised, they are
quickly discharged and picked up by services operating in the community.
This study found that the changes have led to much uncontained anxiety felt across
the various tiers in the Trust. This has impacted on how employees undertake their
roles and responsibilities particularly in caring for the users of Trust services. Reports
from the CQC and Commission for Health Improvements (CHI), which no longer
exists, have highlighted poor-quality care in some clinical areas in the Trust. The
level of dissatisfaction experienced by some employees has been reflected in the
Trust’s NHS Staff Survey and BME Staff Survey. In addition to these reports and
surveys employees expressed in their interviews that they have been ignored, not
been valued and supported during these tumultuous changes.
The economic pressure has forced the Trust to review its workforce. Posts and
teams have been disbanded or changed. Some clinicians have been downgraded,
redeployed, made redundant or undertaken the mutually agreed resignation scheme.
Redeploying staff into unfamiliar areas was raised as an issue in this study.
Preparing teams for the arrival of an employee from a service that has been closed
came up in the interviews. Negative consequences when staff were moved without
proper consideration was reported. Matt highlighted this issue when he reported a
BME ward manager was redeployed to an unfamiliar clinical area where the team did
not want him. The consultant questioned the clinical skills, competency and
performance of the BME manager who in turn felt bullied by the consultant and the
team. Relationships became fraught and strained. The BME manager was involved
in a serious incident. He was suspended and, after his disciplinary hearing,
dismissed. Duffin (2003) highlighted the lack of competency among BME staff might
194

not be the fault of the nurse and may result from poor supervision and minimum
support. This case also focuses on the need to pay attention to teams that are
resistant to accepting redeployed employees into their services. Cooke (2007)
described how incompetent ward managers were scapegoated particularly when
senior managers ignored the wider systems and processes leading to the failings.
Stone et al. (2011) reported mistakes did not happen in isolation and systems in the
NHS were not designed to prevent errors from happening. From this study it is
difficult to know how much thought has been given by senior managers around
protective measures to prevent mistakes from happening when services have been
reconfigured to curb costs in the Trust. Murray (2005) emphasised context where
employees’ work needed to be analysed and organisational and management factors
should be considered along with individual ones.
Staffing levels, particularly in nursing, have been affected during the reconfiguration.
In the interviews, managers reported that nurses have bigger caseloads and are
doing more with fewer resources and working over and beyond what is expected
from them. Both Marcia and Celia reported this when looking at the mitigating
circumstances surrounding disciplinary investigations. Comparable findings were
also found in Cooke’s (2006b) study.
7.3.3 Management in the Trust
A mixed picture of how white managers and BME staff relate to each other is
depicted in this study. Senior managers were perceived to have a “skewed” picture of
black African nurses and HCAs. BME staff, particularly those in lower positions and
on the front line, speculated that white senior managers lived in white affluent
195

suburbs and did not come into contact with BME people outside the workplace. As a
consequence they did not know how to relate to this group. These managers, as
highlighted by Matt were perceived to distrust particularly black staff from Africa and
took a “stick rather than a carrot” approach when managing this group. BME staff
were perceived to be treated more harshly and unfairly.
This study found the pressure and demands placed on managers in the current
climate are immense. Sam shared his experience of being redeployed as a team
manager to a clinical setting. There had been a quick succession of six managers.
He found staff paid more attention to non-work related issues than providing good-
quality patient care. Four BME staff have been disciplined for poor conduct and
performance since his arrival. Sam could not understand “how the hell has this been
allowed to go on for so long? Some managers let them get away with blue murder.
They [staff] were allowed to get away with it.” Part of the ‘getting away with it’ was
owing to managers and members of the team not challenging poor conduct and
performance. King and Wilcox (2003) and Archibong and Darr (2010) conveyed how
managers found it difficult to deal with disciplinary issues because of not having the
skills and confidence to deal with conduct and performance issues.
When managers confronted inappropriate and unprofessional staff behaviour, this
could be daunting. There was trepidation particularly when managers were
threatened with grievances and accused of bullying and racism. Marcia, a BME
employee, reported the ‘race card’ being played in some instances where she has
challenged the conduct of BME staff and investigated disciplinary cases involving
them. Sam, also a BME employee, has had a grievance taken out against him by
some members of the team when he highlighted and addressed the issues of poor
196

performance and conduct in his team. He was accused of been a racist. Despite
being cleared, the stress and strain of the allegation impacted on his health.
Line management, supervision and appraisals did not always collaborate to deal with
performance and conduct issues. Where there was an absence of collective
responsibility, managers could end up dealing with the stressful situation without any
support. The case mentioned earlier of a poor-functioning team with issues around
staff misconduct in a clinical area that has been put on the ‘At Risk Register’ for the
second time raised many concerns. It is unclear what measures the Trust took first
time round to deal with at risk issues and why these strategies failed. Further
questions from this study can be raised: why did the wider team not challenge the
staff conduct and performance in the context of the clinical work? If staff were
frightened, why did they not report bad practices to managers outside the unit? Or
have poor practices become normalised and a part of the culture in the clinical area
until a robust outsider came and exposed the malpractices? Why did professionals
ignore the code of conduct laid down by their regulatory bodies? Clinicians trained to
treat vulnerable and sick patients did not always behave professionally. Managers
and colleagues observing this behaviour, as Heffernan (2011, p. 1) stated, became
‘wilfully blind’ by “denying the truths that are too painful and frightening to confront.”
This concern was expressed in the Francis Report (2013). Marcia, investigating a
nurse accused of misconduct and poor clinical practice, stated she could quite easily
“cut and paste” from the Francis Report.
7.3.4 Changes to organisational culture
The emic approach provided insight to the culture of work settings (Fetterman, 2010).
This study found the influx of continuous change had some bearing on the context
197

and the culture of the Trust (Goodson and Vassar, 2011). To accommodate the
reorganisation of the Trust, Monica, a BME manager reported some employees had
been moved many times, that made it difficult to engage and integrate with the team
and develop meaningful therapeutic relationships with patients. Team cohesion and
morale was affected. This had a destabilising effect on the employee, the team and
the continuity of care delivered to patients.
As this study found, changing the culture of a clinical area where poor practices have
been exposed could be challenging and slow. Getting employees to change their ‘old
way’ needs careful planning and monitoring as Leona feared there is the potential to
replace one collusive system with another. Bringing new staff into a clinical area
where staff have been sacked and removed can create splits and segregation in the
team. Sam revealed the new staff who joined his team sat at one end of the room
whereas the existing staff sat at the other. The lack of trust and acceptance created
tensions that made it difficult for integration and team cohesion to happen. If tensions
around the splits are not worked through, patients can get caught up in the dynamics
or might exploit the divisions. For patients diagnosed with borderline personality
disorders, this can be a prime setting to play staff off against each other (Bateman
and Fonagy, 2005).
7.3.5 Patient care
Patients can become the recipient of staff frustration. Not all patients are appreciative
of the treatment of care received and can criticise staff. Sam described the patients
who used the services he managed as having severe and enduring mental health
issues with complex and traumatic histories. According to Sam, not all nurses wanted
to work with these patients as they presented huge risks. Presentation of their
198

behaviours can be challenging and result in poor therapeutic engagement and risk
management. The lack of good-quality clinical supervision, as discussed in the next
section, can add to the problems (Duffin, 2003).
Patients who do not respond positively to the treatment can make clinicians feel
inadequate and frustrated. Working with this type of patient can be unrewarding.
Family, carers, relatives and friends can also become critical, blaming and angry
towards staff when their loved ones are not cured of their ailments. Consequently
complaints can be lodged (Cooke, 2006b). Hostile and angry feelings from staff can
be projected and displaced onto patients, colleagues and managers who are or
maybe perceived unsupportive. Similar behaviour in patients towards staff is mirrored
as highlighted by Matt. Overt or subtle retaliatory behaviour can emerge if the
situation is not properly managed. At the extreme end, patients attacking
nurses/HCAs and nurses/HCAs hitting patients occurred in the Trust. These issues
came up in the interviews. Pam found white middle class patients showed more
disdain towards BME staff who in turn felt unprotected by the Trust. Alistair
mentioned nurses physically hitting and neglecting patients.
Speculation about BME staff not born here and discriminated against, having to work
harder, denied opportunities to progress and struggle economically, in comparison to
patients and employees with better privileges are considered by Pam. In addition to
these factors, Pam also reflected upon the constant pressure to deliver services at
times of continuous change, uncertainty, staff shortages and unsupportive
environments taking its toll on BME nurses and HCAs who are on the frontline in
providing care. The repercussion in the form of resentment, jealously, envy and
hatred of not been appreciated and not having the same advantages is considered
199
by Pam during disciplinary investigations. Alleyne (2005) highlighted there is a need
to engage with unpleasant strong emotions in addition to looking at cognitive and
prescriptive approaches. This emotional aversion is also taken into account by
Obholzer and Roberts (2003). Healy and Oikelome (2006), linked social class to
BME employees and Dhaliwal and McKay (2008) looked at class and related this to
working experience of BME female nurses in the NHS.
In addition to Sam’s perceptions of staff “turning a blind eye” and Pam’s claim
mentioned above, Marcia from her disciplinary investigations considers other factors
why some employees abuse patients. She highlighted stress, being burnt out,
underpaid and poorly developed nurses as contributing factors. To minimise this
acting out behaviour, staff need to have a space to reflect on their relationships with
patients who are challenging.
7.3.6 Breakdown in staff supportive structures
Pertinent protective measures that can be utilised by the Trust to support staff from
making mistakes are clinical supervision, training and appraisals (Duffin, 2003). The
subject of clinical supervision and staff support came up in the findings. The lack of
good-quality and regular supervision was a continuous theme. This study found
clinicians do not always take up supervision and supervisors do not always pursue
this non-attendance. The supervisor coming from another discipline also presented
an issue. From the interviews, participants also reported supervision was used for
being reprimanded and the supervisor checking up if targets were being met.
Discussion around clinical work was avoided. Not all supervisees reacted
constructively when challenged about their clinical practice. Some supervisors, as
highlighted by Marcia and Pam, can be reluctant to challenge supervisees as they
200

are not competent, confident and skilled to deal with the reactions from the
supervisee and afraid of a grievance being raised against them (Archibong and Darr,
2010). In disciplinary hearings, the lack of supervision is regularly raised as mitigating
circumstances.
With the low levels of staffing in the clinical area and the constant demand of meeting
patients’, carers’ and managers’ demands and expectations, clinicians in this study
found it difficult to attend clinical supervision and mandatory training. At the same
time, Trusts are being annually measured on the number of staff who have
completed the mandatory training. To address this issue, Trusts have developed
online training where staff can sit in front of a computer screen and undertake this
without having to leave their clinical area. Questions have been raised by participants
in the interviews about the effectiveness of this approach for some training. Training
in equality and diversity has been reduced from a one day to a one-hour online
activity. In this study BME participants in particular expressed anger and cannot
comprehend the value of this method to deliver training around such a complex and
challenging area as race, diversity and culture.
7.4 BME employees in the Trust
Examining the secondary data (Dixon-Woods, 2012), such as the Trust quarterly
magazine and various reports (as the RES) and the Service and Workforce Equality
Report), provided an opportunity to consider the representation of BME staff in the
Trust. On the surface, BME employees are included and represented in magazines
and brochures. Pictures of contentment and inclusion are conveyed in this literature.
Conducting this study within the Trust and using critical ethnography the findings
conveyed other realities.
201

7.4.1 Recruitment of BME staff
To provide services to the population it serves, the Trust is reliant and dependent on
BME staff. This study found BME employees make up 38% of the workforce in the
Trust. Black African employees are the largest group (19%) within the BME labour
force. Within ancillary, nursing and HCAs/support staff BME employees comprise the
largest group. BME staff represents over 60% of registered nurses. Sixty-nine
percent of HCAs and support staff come from BME backgrounds. BME nurses and
HCAs/support staff are an integral resource and the Trust could not exist and provide
the care to the population it serves without this group. Healy and Oikelome (2006)
argued the NHS could not survive without overseas qualified professionals and BME
staff.
At times of staff shortages and government initiatives as the NHS Plan (DoH, 2000)
to increase the number of nurses in the Trust, BME nurses and HCAs have been
recruited. To meet the shortfall of nurses, the Trust in the recent past has appointed
newly qualified nurses without going through the conventional selection and
recruitment process. Repercussions from this initiative came up in the interviews.
Some managers believed incompetent nurses were employed and these nurses
have presented problems. No additional evidence was found in this study to
substantiate this claim. Recruitment details of BME nurses who went through the
disciplinary process were not provided.
The negative perception towards BME staff at the recruitment and selection stage
when candidates were interviewed for posts in the Trust came up in this study. When
asked about managing staff from different and diverse backgrounds, George
reported most candidates responded to this as a problem that needed to be
202

managed. The constructive participation made by BME employees in the NHS were
not acknowledged by candidates seeking employment in the Trust. Simpson et al.
(2010) also reported a denial of the positive participation of BME healthcare staff in
shaping the NHS.
7.4.2 Socialisation and the working practices of BME staff
From this study there is no evidence of nurses appointed to the Trust with an
overseas nursing qualification. The pre-registration nurse training undertaken by
BME nurses was from UK higher educational institutions. There was recognition from
Denise that the Trust has been ill-prepared for black African nurses and HCAs born
outside the UK. Although these nurses have trained here, there is a perception that
the formative education has come from their country of origin. In this study Black
African nurses and HCAs not having a foundation in British education and not
socialised into the British way of life were cited as reasons why this group found it
difficult to integrate with other staff in the Trust. Within the main site of the Trust,
noticeable pockets of segregation were observed around racial lines. Some clinical
areas have predominantly white staff whereas other settings are staffed
predominantly by BME staff.
This study found the difference in the working practices and behaviours of BME,
particularly black African nurses and HCAs was attributed to their divergent
socialisation, education and cultural experiences. From the interviews Black African
nurses and HCAs were perceived as having a more paternalistic attitude in patient
care in comparison to their white counterparts. This approach contradicted the
‘recovery model’ promoted by the Trust.
203
In terms of relating to authority figures this study found, black African staff were
observed bowing to Trust executives when they arrived in the clinical area. Initially
this behaviour was ridiculed but on further investigation bowing was understood to
convey respect. Johns (2005) reported BME nurses who cannot present themselves
in the ‘white way’ or mainstream way are negatively perceived by white colleagues.
For Hyacinth adapting to anglicised behaviour meant BME staff losing their identity.
In another interview Denise reports a BME HCA’s direct approach to a senior
manager for a pay increase was perceived as “shocking”. In their study, Archibong
and Darr (2010) found the different styles of communication and behaviour were
negatively interpreted by colleagues and senior managers.
Shauna found some nurses expressed their frustration to a manager about the
attitudes and performance of an overseas BME HCA who had recently come to the
UK and found employment in the Trust. In accordance with her working experiences
back home the HCA carried out her list of allocated tasks. Once she had completed
them, she felt her work was done. She was unaware of NHS working practices and
had not been advised or supported by her colleagues, who instead reported her to
the manager. Archibong and Darr (2010) stated that managers lacked confidence to
deal with issues informally. For this BME HCA, her colleagues treated this behaviour
formally instead of informally. In this study managers were not the only ones to opt
for the formal route.
Issues around the use of own position to reward oneself came up in this study. A
senior white manager reported a black African nurse felt it was her prerogative to
award herself the financially lucrative shifts as she considered this was the benefit of
working hard to gain a higher banding. Fearfull and Kamenou (2007) found cross-
204

cultural communication and behaviour around working attitudes and authority was
misinterpreted. Alleyne (2004) highlighted that subtle and attacking comments were
made to undermine the culture and behaviour of BME staff.
This study found some white managers, who have been in the Trust for many years
and have worked closely with black African staff in particular, took time to find out
issues presented by BME staff. For example, these managers could not understand
why some BME employees in low positions exerted influence and control over senior
colleagues in the workplace. When these managers took the time to find out, issues
around status were unearthed among BME cultural groups. Details of BME
employees working in low positions in the Trust and occupying positions of chiefs,
nobility or pastors in their homeland came to light.
7.4.3 BME staff treated with suspicion and distrust
In this study there was a perception by some senior managers that BME, particularly
black African employees were only motivated by money and worked in certain
settings that paid extra allowances. As the areas were well staffed and resourced,
there was a held belief that black African nurses and HCAs worked in these settings
to preserve their energy so that they could work elsewhere after their shift. Larsen et
al. (2005) and Henry (2008) found nurses from overseas were perceived as only
working for their own economic gains.
With a new computer program installed in the Trust, managers reported that BME
nurses and HCAs were found to be working back-to-back shifts and working over and
beyond working time regulations in the NHS. Senior BME nurses, who have been
involved in the disciplinary investigation, reported that some BME nurses and HCAs
205

who were found asleep on duty or making mistakes administering medication had
been working excessive hours.
Without evidence provided and figures published by the Trust, it is difficult to
determine the scale of the number of BME employees who are breaking the working
time directives. Although the new computer program was installed to facilitate
efficient use of resources, there was inference about this system also being used to
monitor the working hours of BME nurses and HCAs. Lewis (2011) found BME
nurses and HCAs were targeted by NHS anti-fraud investigators for fraud or criminal
offences related to false documents. In the RCN studies by Pike and Ball (2007) and
Dhaliwal and Mackay (2008), BME employees were closely monitored for their
conduct and performance. This could correspond to the ‘stop and search’ actions of
the UK police towards BME young males.
This study found BME staff who reported in sick were treated with suspicion. There
was a thought that they were working elsewhere. Black African staff visiting their
homelands and not returning at the end of their planned leave due to sickness were
perceived as pulling a “fast one” and lying. Despite producing medical documentation
the validity of the certificate was suspected. In another case around the authenticity
of official documentation the genuineness of qualifications, as Ann reported in her
case, was also questioned. Likupe (2006) found the authenticity of qualifications of
BME employees was doubted. Archibong and Darr (2010) reported BME employees
were perceived not to be committed to their jobs.
When some BME employees had been investigated by senior managers about
breaking working time regulations, extreme personal circumstances were disclosed.
206

Motivation for working extra hours was not intentionally to break the law but due to
personal situations. When senior managers such as Lisa heard these accounts from
their BME employees under investigation, they used a softer tone and had an
empathic attitude. Negative judgements were withheld. In comparison to when
employees were perceived to be intentionally committing fraud, a harsher and
exasperating tone was observed in the interviews.
7.4.4 Impact on BME staff
Some participants in this study observed and reported the impact of these negative
perceptions on BME staff. Denise found morale among BME nurses to be low. These
staff absorbed and internalised the idea that they could not be good nurses. Others
saw themselves as second-rate nurses and placed no value on themselves of being
promoted in the Trust. Henry (2008) reported that BME staff become disillusioned
about their career prospects in the NHS. BME employees perceived as not being
good enough was found by NHS Northwest (2008). Dhaliwal and McKay (2008)
reported there was a perception by white managers that BME nurses were not
capable of achieving managerial and senior positions.
Parallels to oppression are drawn between the plight and experience of BME people
in society to the experience of BME staff in the Trust. Britain’s historical colonial past
and how this permeates to the present day was raised by Ann who felt the position of
BME staff in the NHS was already determined before they arrived. She was
pessimistic that no matter how hard BME people worked, they would never be given
the same status and recognition as their white counterparts. She called this the
“black tax”. To support this perception, several participants in this study gave
examples of the over-representation of BME employees at the lower bandings
207

(Likupe, 2006; Archibong and Darr, 2010) and the under-representation at senior
positions. The descriptive statistics on the Trust workforce show the number of BME
nurses decline as they progress through to higher positions and BME HCAs occupy
higher numbers in lower bandings.
What went on beyond the walls of the Trust was conveyed within the Trust. Leona
talked about how BME people were socially constructed. She described BME people
particularly of black descent as oppressed, treated with suspicion, disproportionally
stopped and searched by the police and perceived as unintelligent.
7.4.5 The ‘Black African’
In reality, there is no such thing as a ‘black African’. The continent of Africa is vast
and made up of many countries. Each country within the vast continent is diverse
and different in their culture and traditions. In this study the black African has been
constructed, perceived, simplified and homogenised as one body. The issue around
black Africans not being able to integrate into the Trust (as discussed above) was
presented as the problem. This study found BME employees were always compared
to their white counterparts. White employees were never compared to their BME
counterparts. Allen (2006) stated ‘white’ was depoliticised and perceived as the norm
of power, knowledge, civilisation and goodness. Madison (2004) emphasised how
people were presented held power and meaning.
In the present study BME nurses and HCAs were distinguished from each other. For
example, Black Africans nurses and HCAs were distinguished and categorised as
‘good or bad’. Zimbabwean nurses were perceived to be responsible and able to fit
into mainstream working practices. Male Nigerian nurses and HCAs were perceived
208
as having problems to adapt to the mainstream culture in the Trust in this study.
Reference to West African nurses having a “gambling and a bit of a drink problem”
was reported by senior managers interviewed in this study. Black African nurses
dismissed from the Trust in this study were compared to black African nurses struck
off the NMC register. Carter’s (2000) study perceived BME staff as troublemakers. In
this study, nurses and HCAs from West Africa (particularly Nigeria) were considered
troublesome by senior nurses. Cooke’s (2006b) concept of ‘bad apples’ could also be
applied to this group. Unlike Henry (2008) where managers preferred African
Caribbeans to black Africans, this study found African Caribbeans absent in the
discussion. An attempt to break away from the homogeneity of BME employees
started to appear in my findings, particularly among black African employees.
Johns (2005) implied BME employees who did not present themselves in the white
European ways were negatively perceived. Fitting in with the main established ways,
namely white European was favoured over BME employees’ skills and experience.
7.4.6 Discrimination and racism within and between employees
The study revealed perceptions of racism and discrimination across the Trust. Some
managers showed their animosity towards BME employees by letting them make
mistakes and then intervening by initiating disciplinary actions for these mistakes.
Some interviewees expressed disbelief around the perception that some managers
held about BME employees’ main motivation being a financial one. These
interviewees such as Gerard could not understand why this held perception was not
being challenged and treated as racism by the Trust. Racism and discrimination, as
observed by Ali were not only polarised between ‘white and black’ staff but also
highlighted between BME individuals and groups.
209

A shift to move away from ‘blacks versus whites’ and the rivalries within and between
the different and diverse BME groups in the Trust is highlighted in this study. Racism
between Mauritian, Ghanaian and Nigerian staff was reported in my findings. As
found by Likupe and Archibong (2013), racism between BME employees surfaced in
clinical areas employing diverse racial and ethnic groups.
Relationships between BME managers and BME staff were unearthed. From this
study some BME managers could distinguish between cultural working practices and
the poor performance and conduct of BME staff. Despite being threatened with
grievances and accusations of racism and bullying, these managers were not afraid
to challenge the improper working practices and would also present evidence against
BME staff at disciplinary hearings.
In the current study, playing the ‘race card’ was not only undertaken by BME staff but
also advocated by some white managers in the Trust. These managers advised BME
employees to use this approach particularly to get on courses and training that were
popular and oversubscribed. Some poor performing BME staff when challenged
about their practices used the ‘race card’ as a defence.
7.5 Disciplinaries in the Trust
Disciplinary action is legitimate to manage employees who breach their contract of
employment and continually fail to meet the required standard of behaviour, conduct
and performance set out by the Trust and professional regulatory bodies. Disciplining
staff should be used as the last option.
210

7.5.1 Descriptive statistical data on disciplinaries
Under the Equality Act 2010, there is a legal requirement on NHS Trusts to publish
details of their workforce that includes disciplinaries to the public. Although this legal
compliance was met by the Trust in my study, information available on disciplinaries
was minimal. The data on disciplinaries from the Trust was limited as age, gender,
area of work, occupational and professional groups were not recorded. The lack of
these data made it difficult to determine if certain employees in the Trust were more
susceptible than others to disciplinary action and if: a high turnover of staff; issues
around recruitment, retention and high levels of sickness; a disaggregation and
reconfiguration of services were contributory factors to disciplinaries.
From the descriptive statistics in chapter 4, the total number of the workforce for
2011 to 2012 was 2330; 54% (1305) were white and 38% (918) were from BME
background. The total number of staff involved in disciplinaries was 2.4% (56). Eighty
percent (45) of staff came from BME backgrounds. Looking at the data on
disciplinaries, from 2008 to 2012, there were always more BME employees put
through the disciplinary process in comparison to white staff. From 2008 to 2009, out
of 37 employees disciplined 25 were BME staff. Between 2009 and 2010 there was
27 BME staff in comparison to 11 white staff disciplined. From 2010 to 2011, 18 BME
employees were disciplined in comparison to 11 white staff.
These data clearly demonstrated that BME employees in the Trust were over-
represented in the disciplinary process. The findings from this study supported the
work of Beishon, et al. (1995), Carter (2000) and Archibong and Darr (2010). Thus,
this adds to a growing body of research showing a clear over-representation of BME
employees in the disciplinary process in the NHS. Archibong and Darr (2010) also
211

concluded that BME employees were disproportionately disciplined in the mental
health field.
Looking at the data on disciplinaries, from 2008 to 2012, it was noticeable that the
number of white employees did not exceed BME employees in any of the categories
listed. BME employees always received more first, final written warnings and
summary dismissals than white staff.
When suspensions were recorded for the first time in 2011 to 2012, BME employees
were suspended almost three times more often than their white counterparts (21:8). It
was not clear why there was a significant increase in the numbers going through the
disciplinary process from 26 to 56 (2010–2011 to 2011–2012).
Despite taking measures to reduce economic costs, senior managers, in the current
study, reported that the Trust Board had not considered the cost of disciplinaries,
particularly suspensions, on the Trust. The NAO (2003), Murray (2005) and Stone et
al. (2011) have conducted research to calculate the economic and emotional costs of
suspension.
Murray (2005) and Stone et al. (2011) looked at the emotional impact of suspensions
on the employee under investigation but they did not look at the effect suspension
had on the clinical team. My study was able to look at the impact on the clinical team.
After the hearing, the suspended employee usually returned to work quickly (as
described in chapter 5). The team was only informed of this at very short notice and a
lack of consideration was given to preparing all parties for this return. Tensions and
anxiety prevailed particularly if colleagues from the team had to give evidence
against the person under investigation. Team dynamics were affected, relationships
212

became strained and employees started distrusting each other. These issues were
not worked through. Cases of grievances being taken out have been reported
anecdotally in my study.
7.5.2 The wider context: outside the NHS
Outside the NHS a similar picture seems to emerge about the experience of BME
staff and disciplinaries. A disproportional representation of BME employees involved
in the disciplinary process is found in other public institutions and the private sector.
Archibong and Darr (2010) found BME employees in the police service and local
government reported similar experiences to BME employees in the NHS. The
Equality Challenge Unit (2009) found a disproportionate level of scrutiny on BME
staff in higher education. John (2014) revealed BME solicitors were subjected to
severe sanctions in comparison to their white counterparts.
International studies in nursing looking at the phenomenon in English speaking
westernised countries are sparse and needs further investigation. However, from the
USA, the National Council of State Boards of Nursing (2009) found a higher
percentage of African-American, Native American and Hispanic nurses were
disciplined in comparison to the general nurse population. Other international studies
on disciplinaries involving nurses (Hudspeth, 2009 and Pugh, 2009) did not consider
race and ethnicity.
7.5.3 Capability procedures
Archibong and Darr (2010) found managers were erroneously using disciplinary
policies to deal with capability issues. Similar issues were found in the Trust in my
study. Capability policies in this Trust recently revived by an interim chief executive
213

were under-utilised and not seen as user-friendly. In addition Hazel, Ali and Gerard
separately reported managers were not following the suspension policy and not using
suspensions as a last resort. From the interviews with senior managers it was
reported that disciplinaries have reduced since the capability policy was reintroduced
and suspensions have also declined since they have been monitored by the Trust
Board. No further evidence has been provided to corroborate this claim. However,
measures supported by the Trust Board, in this study, were more likely to succeed if
they had financial implications. This was in contrast to the lack of support given by
senior Trust executives to the E&D agenda (Carter, 2000; Healy and Oikelome,
2006).
7.5.4 Reactions to the phenomenon investigated
The subject of the disproportional representation of BME employees in the
disciplinary process is sensitive (McGarry, 2010) and political. From the data
presented in this study, the Trust Board executive’s perceptions (see section 3.3.1)
about the ‘apparent’ over-representation of BME employees disciplined could be
dispelled. However, despite the data presented by some BME and white participants,
particularly managers, it is strongly felt that there was no disproportional
representation of BME employees in the disciplinary process. The other assumption
of BME employees on lower bands 1 to 4 were more likely to be disciplined was
unfounded. More employees from bands 5 to 8 were disciplined.
Participant observation used in ethnography was a useful instrument to investigate
how employees reacted to this over-representation of BME employees in
disciplinaries (Holloway and Todres, 2010). In this study discomfort, hostility and
resistance were observed in the non-verbal behaviours amongst some employees,
214

particularly senior managers. Contemplating the phenomenon was difficult
particularly for senior managers. The size of the issue (2.4%) was derided and
quickly dismissed. Arguments put forward by the participants to stop the discussions
about disciplinaries was that the Trust had to deal with more ‘important’ issues
around its future and focus on poor-quality care. Issues of poor conduct and
performance found in disciplinaries were divorced from the struggle the Trust was
having in some clinical areas in providing good-quality care. The issue of
disciplinaries in this study tended to be compartmentalised and not considered in the
wider context.
In this study, defensive behaviour of separating and denying the phenomenon
seemed to be a strategy to deal with this fear, discomfort and anxiety. To avoid
looking at anxieties that surround contentious subjects, Alleyne (2005) using
psychodynamic concepts stated defence mechanisms were used. One common
mechanism that is used by individuals to evade complex threatening emotions and
reality is denial. Like individuals, Obholzer and Roberts (2002) stated institutions also
develop defences against painful emotions. Another mechanism adopted by
individuals, in this study, is rationalisation. Here, rational reasons are given to make
light of difficult issues (Gabriel, 2004).
Over the past few years, the Trust in this study has reported the high numbers of
BME employees in the disciplinary process. This has been forced by the legal
requirement on the Trust to publish details of their workforce. Up until this study, little
visible attempt has been made to understand why this issue exists in the Trust. This
has frustrated BME staff in particular who felt aggrieved that the Trust was not
actively interested in the welfare of its BME staff. Participants in the interviews
215

reported angry outbursts at BME conferences when disciplinaries have been
mentioned. White senior managers and the Trust Board were also reported to be
absent from the conference. There is a perception from BME participants in the
interviews that these managers did not attend because they were afraid of the
backlash from BME employees. Senior white managers from the Trust have
expressed their discomfort in attending the BME Staff Group and conferences as
they were not made to feel welcomed and were attacked and accused of racism
when issues around inequalities experienced by BME employees surfaced. Owing to
the highly expressed emotions, this study found that an open and authentic dialogue
around disciplinaries involving BME staff is difficult to sustain in the Trust.
7.5.5 Equality and diversity
Apart from meeting the statutory requirements, it was unclear how the data on
disciplinaries was used by the Trust in this study to inform their policies and
practices. Despite there being the Race Equality Steering Group, Workforce Equality
Group, Equality and Diversity Group and the BME Staff Group, it was unclear how
data on disciplinaries informed a coherent strategy and the various initiatives. The
inconsistent use and poor-quality data on disciplinaries provided by NHS Trusts were
highlighted by Archibong and Darr (2010) and Stone et al. (2011).
Many participants in this study claimed Trust executives were not taking the E&D
agenda seriously. Healy and Oikelome (2006) conveyed E&D initiatives make little
difference. Carter (2000) found the E&D agenda was a paper commitment that was
poorly embraced by Trusts and relegated at a time of economic crisis. Senior
managers in this study cited the Trust’s preoccupation with financial issues relating to
216

its uncertain future as a reason for the E&D agenda not being a priority. BME staff
felt their experiences are neglected and marginalised.
There are several groups set up in the Trust that incorporate the E&D agenda.
Notable groups are the Race Equality Steering Group, Workforce Equality Group,
Equality and Diversity Group and the BME Staff Group. The purpose and the task of
each group and how these groups interrelate were unclear. Similar agendas
appeared in each group. From the meetings observed the attendance of white staff
and clinicians were scarce. Questions were raised about the application and
integration of the E&D agenda into the Trust’s daily practices and the impact on the
working experience of BME staff. Healy and Oikelome (2006) found E&D initiatives
focused on changing individuals rather than changing and challenging NHS culture.
In this Trust’s policies related to disciplinaries and capability procedures, an initial
statement on equality was published, affirming that all staff should be treated equally
and fairly. Monica who is closely involved in the disciplinary process highlighted: “our
disciplinary panels don’t necessarily consist of managers who have had any E&D
training.” Paul revealed that he did not consider the ethnicity of an employee under
investigation as an issue. He admitted his lack of training as chair of the disciplinary
panel. He was more cautious in making the ultimate decision of whether or not to
discipline. If some managers do not have any E&D training and do not consider the
ethnicity of a BME employee how can BME employees be treated fairly and equally?
7.5.6 Disciplinary investigations and hearings
In this study, the quality and rigour around the investigation depended on several
factors. Carter (2000) found the disciplinary process was weighted against BME
217

employees. Cooke (2006a) found managers were initiating disciplinary action on ‘gut
feeling’ rather than collecting the facts to make an informed decision. Unlike my
study, Cooke did not consider the role of other employees directly involved in
investigations.
To maintain impartiality, facts rather than the IOs’ opinions need to be presented at
the disciplinary hearing. In this study, it is reported by some panel members that
some IOs presented opinions and unrelated material rather than facts from their
investigation at the hearing. Not all IOs were given training to undertake their role. In
the Trust there was no standardised training to deal specifically with investigating
disciplinary cases. From the interviews, this study found some IOs were determined
to secure a ‘conviction’ at all costs and reacted strongly when the chair has decided
not to discipline an employee. The neutrality and objectivity of the investigation is not
always adhered to.
In the Trust, all IOs have an HR advisor throughout the duration of the case to advise
and ensure that the disciplinary process is followed. In some instances, this study
found from interviews the HR advisor/manager has tried to influence what information
should be included or excluded in the investigation findings. IOs have perceived HR
advisors as erring on the side of management. Some HR advisors reported they
have to intervene when the IOs abdicated responsibility and/or were not confident in
the process. IOs have not always agreed with the outcome made by the chair and
found inconsistencies in outcomes for similar cases. Monica, in her interview
highlighted the disparity in outcomes between white and BME staff.
218
With no administrative support, the writing up of the findings from interviews fell on
the IOs. There have been instances when all the clinical staff related to the employee
under investigation needed to be interviewed. The burden of writing up investigations
has delayed cases from being heard while suspended employees continued to stay
at home. IOs in the interviews also complained that the burden of administrative
tasks associated to disciplinaries prevented them from undertaking preparatory work
to prevent disciplinaries.
Attention has been drawn to the chair of the disciplinary hearing in this study. As
reported by Monica not all managers undertaking this role have had training in
disciplinaries. Also some chairpersons have not undertaken training in E&D.
Archibong and Darr (2010) also found managers were not provided with necessary
training and skills to deal with issues around diversity and difference linked to race
and ethnicity. Managers, such as Pam, who chaired disciplinary hearings have
emphasised that their professional training and experiences did not prepare them for
the complexity of some cases.
This study found the Trust disciplinary panel composition consisted of men and
women from diverse ethnic backgrounds. Some panel members have reported in
their interviews that they have been specifically selected because they were from a
BME background. This has raised suspicion because the cases recalled have
involved ‘problematic’ BME employees who have been dismissed. BME panel
members felt they have been selected to anticipate any accusation of racial
discrimination if the case was referred to an Employment Tribunal.
219

The findings from this study reveal BME panel members were also selected as there
was an assumption that they would understand all BME cultures and they could
distinguish between cultural and competency issues. BME panel members reported
this was an unrealistic expectation and expressed some concern that BME
employees were homogenised.
There was a perception from staff representatives and panel members that the
professional leads sitting on the panel recommended harsher sanctions for members
of their own profession. Gerard reports the sanctions advocated were
disproportionate to the offence. As discussed in section 7.5.1 BME employees
received more summary dismissals, final and written warnings than their white
counterparts.
Cooke (2006a) looked at the role of TU officials in her study. She did not consider the
relationship between the TU official and employee under investigation. This current
study has considered this area. Employees, such as Lyn, under investigations
perceived a conflict of interest between employees who worked full time in the Trust
and undertook the additional role of TU officials. There was a perception that these
TU officials worked closely to managers in their day-to-day work and managers could
influence them so that could impact on the representation. Also there was a lack of
trust around TU officials breaking confidentiality and sharing information with
managers outside the disciplinary process. Archibong and Darr (2010) found TU
representatives were not always aware of and sensitive to the cultural needs of the
BME staff they were representing. This is not found in this study.
220

In this study BME staff perceived HR managers as being discriminatory and not
looking after the well-being of employees. There was a strong perception that the HR
department was part of management and treated BME employees more harshly and
insensitively. Archibong and Darr (2010) also found BME employees were treated
harshly by HR managers. There was a perception from HR managers interviewed
that the HR department was an easy target and a scapegoat for the organisation,
particularly at a time of chaotic change and uncertainty around the Trust’s future.
Cooke (2007) argued Trust executives, who introduced poorly planned changes,
were not held to account as attention was diverted to employees on the front line who
were punished for the mistakes of others.
7.5.7 Disciplinary outcomes
From the qualitative findings in this study, there was a perception that BME
employees were treated more harshly and insensitively than their white colleagues.
Some managers had a low threshold and wanted to take a formalised approach.
Others had a ‘personal vendetta’ and used the discipline process. In other cases,
there was a perception that employees were used to make an example to warn other
employees. Managers in some cases did not always consult HR when considering
the disciplinary route. HR managers themselves did not always follow the disciplinary
policies. Cooke (2006b) found similar findings and stated managers used quasi-
formal disciplinary action against employees who could not be disciplined formally.
Her findings did not report if this included BME employees.
In this study, employees under investigation were treated more fairly if they could:
comprehend the seriousness of the allegation; accept responsibility for their conduct
and performance; reflect and demonstrate insight to the concerns and articulate on
221
the allegation. How BME employees, under investigation, presented themselves in
their hearing in the Trust was reported. They were perceived as inarticulate in
presenting themselves, not showing remorse or accepting responsibility and lacking
insight.
This study found some white chairpersons were more cautious about making
decisions about BME employees under investigation. Also sanctions around similar
cases were inconsistent and BME employees were perceived to be treated much
harsher than their white counterparts. Some IOs and professional leads perceived
individuals from BME groups who were under investigation were scapegoated
(Cooke, 2007). In this study, there was a strong reaction towards managers and
supervisors who had not provided regular support and turned a ‘blind eye’. They
were perceived to be “let off the hook” and not held to account.
7.6 Summary
The findings from the data collected have been discussed in relation to existing
literature in this area. Exploring the over-representation of BME staff involved in the
disciplinary process in an NHS Trust could not be reduced to single factors and
considered in isolation. This study shows the experiences and perceptions of BME
staff, and the personnel involved in the disciplinary process need to be considered in
the constantly changing context of the Trust.
Through focus and critical ethnography this study is able to offer additional
perspectives on the disciplinary process involving BME staff and build on the work of
Beishon et al. (1995), Carter (2000), Cooke (2006a, 2006b and 2007) and Archibong
222

and Darr (2010).The unique findings from this study and how they advance research
in this field will be discussed in the final chapter.
223

Chapter 8: Conclusion
8.1 Introduction
This concluding chapter summarises the contributions this study has made to
understanding the over-representation of BME employees involved in the disciplinary
process in one NHS Trust and how this relates to the wider context.
Recommendations to minimise disciplinaries will be proposed to the Trust. The
strengths and limitations of the study are discussed. Finally, dissemination of this
study’s findings are considered
8.2 How does this study advance research in the field?
From the literature search and review, no studies can be found where ethnography
has been used as a methodology to explore representation of people from BME
groups in mental health disciplinaries, an area that is ‘taboo’ and under-researched.
Confidential research into the disciplinary process was investigated directly from the
inside of an NHS Trust. The use of ethnography is able to uncover new ground and
identify key factors as to why over-representation of BME groups, in comparison to
white ethnic groups, existed in this Trust. Through fieldwork, participant observation,
journal/diary, secondary data and semi-structured interviews, I was able to examine
the culture of a single Trust and investigate the disproportional representation of
BME staff involved in the disciplinary process in the workplace. As part of the study, I
was able to obtain permission to observe a disciplinary hearing and interview staff
with various roles and responsibilities in this and other disciplinary proceedings.
Multiple realities to understand why there is a disproportional representation of BME
staff in the disciplinary process were obtained from employees directly involved in the
224

disciplinary process. These employees came from diverse backgrounds and
occupied different positions, bandings, roles and responsibilities in the Trust.
This research is unique and various perceptions are obtained about the disciplinary
process from the staff directly involved. The study highlights that the disciplinary
investigations are not always impartial and based on ‘facts’. Judgements are
presented in the investigation report compiled by the IO with the support of the HR
representative. IOs carrying out this role are not always trained to undertake the
investigation. The relationship between the IO and the HR representative is
examined. Rather than presenting all the facts, some IOs reported that some HR
representatives tried to influence what to include or exclude in the report. This means
that the findings are presented in a way that favours management. Some HR
representatives emphasised that they are forced to step in to take an active role,
particularly when IOs abdicate responsibility and are not confident in carrying out the
task. Some panel members highlighted the report presented by the IO to the
disciplinary panel has included findings that are not directly related to the employee
conduct and/or performance under investigation. Some HR representatives reported
some IOs are determined to secure a ‘victory’ at all cost and take umbrage when
their case is dismissed by the panel.
There was a perception that some professional leads sitting on the disciplinary panel
recommend the severest sanctions to staff coming from their own discipline. A lack of
tolerance was observed among some panel members, particularly the chair, when
BME staff under investigation were presenting and defending their own cases. In
some cases, the chair of the panel would have more information about the employee
225

under investigation than the other panel members. It was unclear if this had any
bearing on the outcome.
BME staff were selected, on the panel, to offer a race and cultural perspective when
BME staff were investigated. There is an assumption and unrealistic expectation that
these BME panel members were familiar with all BME cultures. Some BME
employees are specifically selected to sit on the panel, particularly when a BME
employee is investigated and likely to be dismissed. This is to anticipate accusations
of racism should the case be referred to an Employment Tribunal.
It was reported that some white chairpersons of the disciplinary panel were too
cautious in making decisions involving BME staff. Varying standards of sanctions are
imposed for similar cases. Some employees have been dismissed when others have
been issued a first warning for offences that are perceived as similar. BME
employees under investigation are perceived to be inarticulate in comparison to their
white counterparts. White staff were perceived to demonstrate insight, accept
responsibility and show remorse for their wrongdoings in comparison to their BME
counterparts.
Using an ethnographic methodological approach, this study provided another
perspective to understand the personnel, structures, systems, processes and
relationships involved in a complex, challenging and sensitive phenomenon in its
natural setting.
8.2.1 Implications of this study for policy and clinical practice
Despite disciplinaries being experienced by 56 employees or 2.4% of the Trust
workforce in 2011 to 2012, 45 (80%) were from BME groups. This matter should not
226

be trivialised. The issues explaining the over-representation of BME staff in
disciplinaries needs to be considered in the wider context and cannot be reduced to
single factors. With limited finances, greater pressures are placed on the NHS to
meet the growing public demands and expectations. People today are living longer
and, as a result, health-related issues are arising from this. As a consequence, the
Trust, as part of the NHS, is going through massive change to deliver more services
with fewer resources. This transformation programme is having a huge impact on
employees who provide these services. Today BME employees make up 38% of the
workforce in the Trust. If all these staff left, the Trust would cease to function in its
present state. It is vital the Trust takes into account the under-representation of BME
figures occupying senior positions; an over-representation of BME applicants who
are not recruited; an over-representation of BME staff in the disciplinary process and
the effect that this can have on BME staff morale.
The issues around disproportional representation of BME employees involved in the
disciplinary process are not only a Trust, but also a wider societal issue. Archibong
and Darr (2010) reported the disproportional representation of BME police officers in
the disciplinary process. Further investigation about this phenomenon also needs to
be undertaken in English-speaking westernised countries as limited international
studies (Pugh, 2009; Hudspeth, 2007 and 2009) were found in the literature search.
These studies did not recognise that ethnicity had any bearing on disciplinary action.
There are various legislations (Equality Act, 2010) and E&D initiatives in place. At a
time of austerity, the E&D agenda has been marginalised by the coalition-led
government. As a consequence of the coalition government making pledges to cut
down on red tape and bureaucracy, ethnic monitoring and reporting needs to
227

continue to determine whether issues facing BME staff are changing for better or
worse. This task must not be perceived as a tick-box exercise with only minimal
information obtained. Meaning needs to be gained from the analysis of the data
collected and this information should be shared. The E&D agenda needs to be
owned from the top and threaded across the NHS to instil confidence in BME
employees that E&D issues are taken seriously and not negatively portrayed in the
NHS and BME Staff Survey.
The economic pressures faced by the Trust in this study and the impact of releasing
staff to undertake training when staffing levels are greatly affected cannot be ignored.
This creates various dilemmas such as the training provided by the Trust. To solve
this issue, the Trust has introduced online training. This raises questions of whether
complex areas such as race, culture and diversity can be reduced to an online
computer activity. Particular attention needs to be given to the training of IOs and
panel members when investigating and hearing cases that involve race, diversity and
culture. In addition, the training of employees undertaking the role of IO and chair of
the panel also should be reviewed. This is to demonstrate that cases are decided on
facts and not supposition.
At a time of continuous disaggregation and reconfiguration of the Trust, consideration
needs to be given to how staff are recruited, inducted and supported to engage with
challenging and complex service users. Focus on redesigning services should not
solely be on curbing costs. The ethnic and skills mix of teams needs to be monitored
to ensure services do not get segregated around racial and ethnic lines. When
employees are redeployed to other services in the Trust, consideration should be
given to how the employee and team are prepared to receive each other.
228

This study reinforces that regular good-quality clinical supervision undertaken in a
safe environment is needed for clinicians to reflect on blind spots, particularly with
service users who present challenges. The working environment and structures need
to support supervisors and supervisees to undertake supervision. Supervisors and
line managers need to be trained and supported by their managers to engage with
teams and employees who present persistent challenges. This study did find
secondary data of nurses and HCAs committing gross misconduct towards patients.
Whatever reasons may lie for poor conduct and performance, nurses need to be
challenged, held accountable and take responsibility for their actions. The clinical
area should not be a forum for nurses to work through their own unresolved issues
and misfortunes, particularly when vulnerable patients are present and need to be
treated. If supervisors and managers are afraid to highlight the conduct and
performance of teams and employees and the employees behave in a defensive
manner, this cannot be ignored or left to one individual to manage. Ultimately the
safety and well-being of patients and their carers need to take precedence over
everything that is undertaken by the Trust. Where appropriate, capability procedures
need to be reinforced with underperforming staff. Disciplinary measures should only
be applied when all other avenues have been exhausted.
Open and authentic dialogue about race, culture and diversity across the
organisation needs to be undertaken. This can only happen if employees feel the
environment is safe to share sensitive and emotionally charged information. The
issue needs to move away from the polarised split between ‘black and white’. This is
a complex issue and attention, as this study highlights, needs to be drawn to the
tensions between and within BME groups. Staff support groups, reflecting on team
229

dynamics and relationships in the context of the clinical work, need to be
incorporated. This is important when relationships in the team are strained, morale is
low and employees are ‘acting out’. Without breaking confidentiality, further thought
needs to be given when employees who have been suspended are reintegrated into
the team. This is to prevent grievances from being raised.
Post-reviews of disciplinaries need to be undertaken to consider lessons that can be
learnt. Reviews need to include processes, systems, structures and outcomes.
Without breaking confidentiality, findings from these reviews could be put into themes
so a meaningful discussion can take place. The dialogue must not centre solely on
the quantitative data but also consider the experiences of all the staff involved. The
focus needs to be on changing the culture of the Trust as well as the employee so
that patient care is never compromised.
The Trust has demonstrated that it is prepared to allow research into a sensitive area
on its site. Further research in this area needs to be considered.
8.3 Study limitations
This study came from one NHS Trust and it is difficult to determine if the findings can
be generalised to other NHS Trusts. The literature search found a dearth of studies
on the disproportional representation of BME employees involved in the disciplinary
process in the NHS. A wider search and review of literature in other public bodies
needs to be considered.
All the data collected for this study came from the main site. It is difficult to know if
the findings from the main site could be applied to other sites within the Trust.
Gaining access to the gatekeepers was challenging as negotiations took a period of
230

time where trust had to be gained. The research under the taught doctorate had to be
completed within a specified time. The pressure of time has had an impact on the
study. Gaining access to undertake a sensitive subject cannot be hurried. How to
access these areas needs to be considered at the planning stage.
Despite permission being granted to undertake the study, accessing forums where
discussions around disciplinaries took place was restricted. For example, each
disciplinary hearing has a pre- and post-panel meeting. Here, panel members meet
outside the disciplinary hearing. Access to meetings where HR managers discuss
workforce issues including disciplinaries at the senior level were denied. Some
meetings could only be attended once as there were long intervals between them.
The time of the next meetings fell outside the period given to collect the data.
Attending a meeting once had its limitations as it made it difficult to capture the
culture. This study presents a fragmented and incomplete representation of the
phenomenon.
For an ethnographic study, the findings came predominantly from interviews.
Interviews could be triangulated. Making comparison of what employees said to what
they actually did could not be observed. There were not many forums to attend and
observe discussions around disciplinaries. Discussions around disciplinaries
happened behind closed doors. Holding focus groups to gain an insight to how
employees react to the disproportional representation of BME staff needs to be
considered. The findings from these groups could be used to triangulate the findings
from interviews and participant observations from other settings.
231

BME employees who had been disciplined did not participate in this study. Initially
four employees who had been disciplined did tentatively express interest in
participating through email. When arrangements were made to hold informal face-to-
face meetings with each employee at a time and a place of their choice and
convenience to discuss preliminary issues such as consent, they withdrew. TU
representatives, who were acting as the intermediaries, let it be known these
employees had declined as they would not want to relive their recent experience of
being disciplined and wanted to put this ‘raw’ ordeal behind them and move on with
their lives.
Having TU officials act as intermediaries presented another issue as this did not
consider staff who had been disciplined and not had TU representation. This group of
employees were inaccessible as not all employees belong to TUs and some might
represent themselves or have non-TU representatives accompanying them.
Another factor why disciplined employees did not come forward was considered. The
researcher being allocated a base within the HR department during the time spent in
the field could have been perceived with scepticism, particularly among BME staff.
The HR department plays a pivotal role in managing and conducting the disciplinary
process. Findings from the BME Staff Survey and interviews overwhelmingly
highlighted a lack of trust and suspicion towards the HR department. HR personnel
from this study were negatively perceived. The researcher being situated in the HR
department could arouse many fantasies about his neutrality and raise suspicion.
This episode raises issues of ‘positionality’ (Borbasi et al., 2005) of the researcher
that was overlooked when designing the methodology for this study.
232

Owing to constraints and the time spent in the field, it was difficult to observe the
criteria required for ethnographic interviewing (Heyl, 2001). Although participants
voluntarily came forward to be interviewed, considerable time could not be spent
building up rapport and undertaking further interviews with the same person.
Participants were only interviewed once. There were no follow-up meetings for the
participants to go through their transcription and for the researcher to seek further
clarification and ask additional questions.
In the end, the findings from this study were constrained to disciplinaries taken
against nurses and HCAs. Access to disciplinary proceedings involving doctors and
other professional groups (outside nursing) could not be obtained. No doctors and
AHPs, such as psychologists, occupational therapists and psychotherapists, came
forward to participate. The perceptions of these groups of staff to the phenomenon
investigated is absent from this study.
Despite the study being restricted to disciplinaries involving nurses and HCAs, an
array of employees from diverse ethnic backgrounds, various bandings and different
roles and responsibilities in the Trust participated in this study. From participant
observations, 27 employees occupying different roles and responsibilities in the
disciplinary process provided their perceptions in interviews.
8.4 Dissemination of the findings
Themes of the findings of this study will be presented to the senior HR manager. This
will be followed by group presentations of the study to employees involved in the
disciplinary process in the Trust. Summaries and abstracts of the study will be sent to
233

academic journals and conferences. Findings will also be adapted and incorporated
into teaching sessions involving healthcare professionals.
8.5 Summary
The findings of this study and how ethnography has contributed to explanations of
the disproportional representation of BME staff involved in the disciplinary process
are summarised. The study will be presented to the Trust together with
recommendations to consider how practices could be improved. The strengths and
limitations of the study are also considered.
References
234
Al-Busaidi, Z.Q. (2008) Qualitative research and its uses in health care. Sultan
Qaboos University Medical Journal, 8 (1), 11–9.
Ali, S., Burns, C. and Grant, L. (2013) Equality and Diversity in the Health Service An
Evidence-Led Culture Change. Journal of Psychological Issues in Organisational
Care, 3 (1), 190–208.
Allan, H.T., Cowie, H. and Smith, P. (2009) Overseas nurses’ experiences of
discrimination: a case of racist bullying? Journal of Nursing Management, 17 (7),
898–906.
Allen, D.G. (2006) Whiteness and difference in nursing. Nursing Philosophy, 7 (2),
65–78.
Allen, H.T. and Larsen, J.A. (2003) We Need Respect: experiences of internationally
recruited nurses in the UK. Report to the Royal College of Nursing. Available from:
http://www.rcn.org.uk/data/assets/pdf_file/0008/78587/002061.pdf [Accessed 23
October 2013].
Alleyne, A. (2005) Invisible injuries and silent witnesses: the shadow of racial
oppression in workplace contexts. Psychodynamic Practice, 11 (3), 283–99.
Alleyne, A. (2004) Black identity and workplace oppression. Counselling and
Psychotherapy Research, 4 (1), 4–8.
Angrosino, M. (2007) Doing Ethnographic and Observational Research, London:
SAGE Publications.
235
Advisory, Conciliation and Arbitration Service (Acas) (2009) Code of Practice 1 –
Disciplinary and Grievance Procedures, London: Acas.
Archibong, U. and Darr, A. (2010) The Involvement of Black and Minority Ethnic Staff
in NHS Disciplinary Proceedings, Centre for Inclusion and Diversity, University of
Bradford.
Archibong, U., Baxter, C.E., Darr, A., Walton, S. and Jogi, M. (2013) Disciplinary and
fitness-to-practice data, policies, and practices in the NHS Trusts and health
professional bodies in the UK. Journal of Psychological Issues in Organisational
Culture, 4 (3), 6–25.
Ashraf, F. (2013) Black and minority ethnic leaders in the health sector. Journal of
Psychological Issues in Organisational Culture, 3 (51), 104–14.
Atkinson, P. and Hammersley, M. (1994) Ethnography and participant observation.
In: Denzin, N.K. and Lincoln, Y.S. (eds) Handbook of Qualitative Research,
Thousand Oaks: SAGE Publications.
Atkinson, P., Coffey, A., Delamont, S., Lofland, J. and Lofland, L. (eds) (2001)
Handbook of Ethnography, London: SAGE Publications.
Audit Commission (2004) The Journey to Race Equality, London: Audit Commission.
Bateman, A. and Fonagy, P. (eds) (2005) Psychotherapy for Borderline Personality
Disorder, Oxford: Oxford University Press.
Beishon, S., Virdee, S. and Hagell, A. (1995) Nursing in a Multi-ethnic NHS, London:
Policy Studies Institute.
236

Benner, P. (1984) From Novice to Expert: Excellence and Power in Clinical Nursing
Practice. London: Addison-Wesley.
Berg, A.M. (2006) Transforming public services – transforming the public servant?
International Journal of Public Sector Management, 19 (6), 556–68.
Bonazzi, G. (1986) Scapegoating in complex organisations: the results of a study of
symbolic blame-giving in Italian and French public administration. Organisational
Studies, 4 (1), 1–18.
Bonner, A. and Tolhurst, G. (2002) Insider-outsider perspectives of participant
observation. Nurse Researcher, 9 (4), 7–19.
Borbasi, S., Jackson, D. and Wilkes, L. (2005) Fieldwork in nursing research:
positionality, practicalities and predicaments. Journal of Advanced Nursing, 51 (5),
493–501.
Braun, V. and Clarke, V. (2006) Using thematic analysis in psychology. Qualitative
Research in Psychology, 3 (2), 77–101.
Brown, T.N. (2003) Critical race theory speaks to the sociology of mental health:
mental health problems produced by racial stratification. Journal of Health and Social
Behavior, 44 (3), 292–301.
Buchan, J. and Seccombe, I. (2013) The end of growth? Analysing NHS nurse
staffing. Journal of Advanced Nursing, 69 (9), 2123–30.
Carter, J. (2000) New public management and equal opportunities in the NHS.
Critical Social Policy, 20 (1), 61–83.
237

Cooke, H.F. (2007) Scapegoating and the unpopular nurse. Nurse Education Today,
27 (3), 177–84.
Cooke, H. (2006a) Examining the disciplinary process in nursing: a case study
approach. Work, Employment and Society, 20 (4), 687–707.
Cooke, H. (2006b) Seagull management and the control of nursing work. Work,
Employment and Society, 20 (2), 223–43.
Cruz, E.V. and Higginbottom, G. (2013) The use of focused ethnography in nursing
research. Nurse Researcher, 20 (4), 36–43.
Cull, D. (2011) “O, Ethnographic Conservation, be some other name!” e-conservation
magazine, 19, 6–8 [online]. Available from: http://www.e-conservationline.com/
content/view/990 [Accessed 25 March 2013].Dearnley, C. (2005) A reflection on the
use of semi-structured interviews. Nurse Researcher, 13 (1), 19–28.
Department of Health (DoH) (2008) Applying for NHS Foundation Trust Status Guide
for Applicants, London: Monitor.
Department of Health (DoH) (2005) Delivering Race Equality in Mental Health Care:
an Action Plan for Reform Inside and Outside Services and the Government’s
Response to the Independent Inquiry into the Death of David Bennett, London:
HMSO.
Department of Health (DoH) (2004) The National Service Framework for Mental
Health – Five Years On, London: HMSO.
238

Department of Health (DoH) (2000) The NHS Plan: a Plan for Investment, a Plan for
Reform, London: HMSO.
Department of Health (DoH) (1999) National Service Framework for Mental Health:
Modern Standards and Service Models, London: HMSO
Department of Health (DoH) (1998) Modernising Mental Health Services: Safe,
Sound and Supportive, London: HMSO
Denzin, N.K. and Lincoln, Y.S. (eds) (1994) Handbook of Qualitative Research,
Thousand Oaks: SAGE Publications.
Dhaliwal, S. and McKay, S. (2008) The Work-life Experiences of Black Nurses in the
UK. A Report for the Royal College of Nursing, London: Royal College of Nursing.
Dixon-Woods, M. (2012) What can ethnography do for quality and safety in health
care? Quality Safety Health Care, 12 (5), 326–7.
Doherty, C. (2009) A qualitative study of health service reform on nurses’ working
lives: Learning from the UK National Health Service (NHS). International Journal of
Nursing Studies, 46 (2009), 1134–42.
Doody, O. and Noonan, M. (2013) Preparing and conducting interviews to collect
data. Nurse Researcher, 20 (5), 28–32.
Duffin, C. (2003) Fair game? Nursing Standard, 17 (11), 12–3.
Emerson, R.M., Fretz, R.L. and Shaw, L.L. (2001) Participant observations and
fieldnotes. In: Atkinson, P., Coffey, A., Delamont, S., Lofland, J. and Lofland, L. (eds)
(2001) Handbook of Ethnography, London: SAGE Publications.
239

Equality Act (2010) Available from: http://www.legislation.gov.uk/ukpga/2010/15/
contents [Accessed 11 November 2013].
Equality Challenge Unit (2009) The Experiences of Black and Minority Ethnic Staff in
Higher Education, London: Equality Challenge Unit.
Fagan, J. (2004) Suspension failure in the NHS: Report for Brian Jenkins MP,
member of the Public Accounts Committee [online], August. Available from:
http://www.ten-percent.co.uk/Reportonfailure.pdf [Accessed 27 March 2013].
Fearfull, A. and Kamenou, N. (2007) Exploring the policy and research implications
for the British National Health Service and its customers. Equal Opportunities
International, 26 (4), 305–18.
Fetterman, D.M. (2010) Ethnography: Step by Step, 3rd edn, London: SAGE
Publications.
Francis Report (2013) The mid Staffordshire NHS Foundation Trust public inquiry.
Available from: http://www.midstaffspublicinquiry.com/report [Accessed 17 January
2014].
Freedom of Information Act (2000) Available from: http://www.legislation.gov.uk/
ukpga/2000/36/contents [Accessed 1 October 2013].
Gabriel, Y. (2004) Organizations in Depth, London: SAGE Publications.
Gibbs, G. (2007) Analyzing Qualitative Data, London: SAGE Publications.
Girard, R. (1986) The Scapegoat, Baltimore: John Hopkins University Press.
240

Gold, R. (1969) Roles in sociological field observations. In: McCall, G. and Simmon,
J. (eds) Issues in Participant Observations: a Text and Reader, London: Addison
Wesley.
Goodson, L. and Vassar, M. (2011) An overview of ethnography in healthcare and
medical education research. Journal of Education Evaluation for Health Professionals
[online], 8 (4), 25 April. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/
PMC3100516 [Accessed 25 March 2013].
Gorsky, M. (2008) The British National Health Service 1948–2008: a review of the
Historiography. Social History of Medicine, 21 (3), 437–60.
Griffiths, P. (2006) Being a research participant: the nurse’s ethical and legal rights.
British Journal of Nursing, 15 (7), 386–90.
Griffiths, P. (2008) Ethical conduct and the nurse ethnographer: consideration of an
ethic of care. Journal of Research of Nursing, 13 (4), 350–61.
Hagger Johnson, H., Smith, G. and Roberts, C. (2013) Disproportionality in internal
misconduct and counter-corruption proceedings in three English police services.
Policing, 7 (4), 359–69.
Hammersley, M. (2006) Ethnography: problems and prospects. Ethnography and
Education, 1 (1), 3–14.
Hammersley, M. and Atkinson, P. (eds) (2007) Ethnography: Principles in Practice,
3rd edn, London: Routledge.
241

Hansard (2008) Available from: http://www.publications.parliament.uk/pa/ld200708/
ldhansrd/text/81124w0004.htm [Accessed 3 February 2013].
Harrow Council (2007) Employees’ consultative forum – issued by Democratic
Service Section, Legal and Governance Department, Harrow Council, London.
Hart, C. (2004) Nurses and Politics: the Impact of Power and Practice, Basingstoke:
Palgrave Macmillan.
Healthcare Commission (2009) Tackling the Challenge: Promoting Race Equality in
the NHS in England, London: Healthcare Commission.
Healy, G. and Oikelome, F. (2006) Ethnicity, Career, Work in the Health Services.
London: Centre for Research in Equality and Diversity, Queen Mary, University of
London.
Heffernan, M. (2011) Wilful Blindness: Why we Ignore the Obvious at our Peril,
London: Simon and Schuster.
Henry, B. (2000) Quality of care, health system errors, and nurses. Journal of
Advanced Nursing, 32 (4), 773–5.
Henry, L. (2008) Disengagement and demoralisation: the roots of Ghanaian nurses’
responses to discrimination in the (UK) NHS. In: Tschudin, V. (ed.) The Globalisation
of Nursing: Ethical, Legal and Political Issues, Oxford: Radcliffe Medical.
Henry, L. (2007) Institutionalized disadvantage: older Ghanaian nurses’ and
midwives’ reflections on career progression and stagnation in the NHS. Journal of
Clinical Nursing, 16 (12), 2196–203.
242

Heyl, B.S. (2001) Ethnographic interviewing. In: Atkinson, P., Coffey, A., Delamont,
S., Lofland, J. and Lofland, L. (eds) (2001) Handbook of Ethnography, London:
SAGE Publications.
Higginbottom, G.M.A., Pillay, J.J. and Boadu, N.Y. (2103) Guidance on performing
focused ethnographies with an emphasis on healthcare research. The Qualitative
Report, 18 (Article 17), 1–16.
Holloway, I. and Todres, L. (2010) Ethnography. In: Gerrish, K. and Lacey, A. (eds)
The Research Process in Nursing, 6th edn, Chichester: Wiley-Blackwell.
Hudspeth, R. (2009) Understanding discipline of nurse practitioners by Boards of
Nursing.JNP: The Journal for Nurse Practitioners, 5 (5), 365–71.
Hudspeth, R. (2007) Survey of advanced practice registered nurses disciplinary
action. OJIN: The Online Journal of Issues in Nursing, 12 (2).
Hunt, B. (2007) Managing equality and cultural diversity in the health workforce.
Journal of Clinical Nursing, 16 (12), 2252–9.
Hurtado, A. (1996) The Color of Privilege: Three Blasphemies on Race and
Feminism, Ann Arbor: University of Michigan.
John, G. (2014) Independent Comparative Case Review: The Solicitors Regulation
Authority. Available from: http://www.sra.org.uk/documents/SRA/equality-diversity/
independent-comparative-case-review-iccr-gus-john.pdf. [Accessed 5 November
2014].
243
Johns, N. (2005) Positive action and the problem of merit: employment policies in the
National Health Service. Critical Social Policy, 25 (2), 139–63.
Johnson, M. and Long, T. (2010) Research ethics. In: Gerrish, K. and Lacey, A. (eds)
The Research Process in Nursing, 6th edn, Chichester: Wiley-Blackwell.
Jönson, H. (2007) Is it racism? Scepticism and resistance towards ethnic minority
care workers among older care recipients. Journal of Gerontological Social Work, 49
(4), 79–96.
Kaiser, K. (2009) Protecting respondent confidentiality in qualitative
research.Qualitative Health Research, 19 (11), 1632–41.
Kandola, P. (2010) Commissioned research into issues of disproportionality.
Available from:
http://www.sra.org.uk/documents/SRA/equality-diversity/disproportionality-final-
report.pdf [Accessed 5 November 2014].
King, K. and Wilcox, D. (2003) Employee – proposed discipline: how well is it
working? Public Personnel Management, 32 (2), 197–209.
King’s Fund (2011) Briefing: The Health and Social Care Bill Report and Third
Reading. London: King’s Fund.
Kline, R. (2013) Discrimination by appointment: how black and minority ethnic
applicants are disadvantaged in NHS staff recruitment. Public World, 1–20.
Kmietowicz, Z. (2005) New suspension procedures aim to cut NHS disciplinary bill.
British Medical Journal, 330 (7489), 437.
244

Lambert, V., Glacken, M. and McCarron, M. (2011) Employing an ethnographic
approach: key characteristics. Nurse Researcher, 19 (1), 17–23.
Larsen, J.A. (2007) Embodiment of discrimination and overseas nurses’ career
progression, Journal of Clinical Nursing, 16 (12), 2187–95.
Larsen, J.A., Allan, H.T., Bryan, K. and Smith, P. (2005) Overseas nurses’ motivation
for working in the UK: globalization and life politics. Work, Employment and Society,
19 (2), 349–68.
Lewis, S. (2011) Minorities ‘targeted’ by NHS fraud squad. Nursing Times.net
[online], 5 July. Available from: http://www.nursingtimes.net/nursing-practice/clinical-
zones/management/minorities-targeted-by-nhs-fraud-squad/5032009.article
[Accessed 21 March 2013].
Likupe, G. (2006) Experiences of African nurses in the UK National Health Service: a
literature review. Journal of Clinical Nursing, 15 (10), 1213–20.
Likupe, G. and Archibong, U. (2013) Black African nurses’ experiences of equality,
racism, and discrimination in the National Health Service. Journal of Psychological
Issues in Organizational Culture, 3 (S1), 227–46.
Mack, N., Woodsong, C. MacQueen, K., Guest, G. and Namey, E. (2005) Qualitative
Research Methods: a Data Collector’s Field Guide, North Carolina, USA: Family
Health International.
MacPherson Inquiry (1999) The Stephen Lawrence Inquiry, Report of an Inquiry by
Sir William MacPherson of Cluny [online], August. Available from: https://www.gov.
245

uk/government/uploads/system/uploads/attachment_data/file/277111/4262.pdf
[Accessed 27 March 2013].
Madison, D.S. (2004) Critical Ethnography: Method, Ethics, and Performance,
London: SAGE Publications.
Mays, N. and Pope, C. (1995) Qualitative research: rigour and qualitative research.
British Medical Journal, 311, 109–22.
McGarry, J. (2010) Exploring the effect of conducting sensitive research. Nurse
Researcher, 18 (1), 8–14.
McGarry, J. (2006) Nursing relationships in ethnographic research: what of rapport?
Nurse Researcher, 14 (3), 7–14.
Muecke, M.A. (1994) On the evaluation of ethnographies. In: Morse, J.M. (ed.)
Critical Issues in Qualitative Research Methods, Thousand Oaks: SAGE
Publications.
Murray, H. (2005) Researching the Lived Experience of Nurses Suspended from the
Workplace: Implications for Practice. PhD diss., Faculty of Humanities, Department of
Education, University of Manchester.
Myser, C. (2003) Differences from somewhere: the normativity of whiteness in
bioethics in the United States. American Journal of Bioethics, 3 (2), 1–11.
Nairn, S., Hardy, C., Parumal, L. and William, G.A. (2004) Multicultural or anti-racist
teaching in nurse education: a critical appraisal. Nurse Education Today, 24 (3), 188–
95.
246

National Audit Office (NAO) (2003) The Management of Suspensions of Clinical Staff
in NHS Hospital and Ambulance Trusts in England: Report by the Comptroller and
Auditor General HC 1143, London: The Stationery Office.
National Clinical Assessment Service (2010) Handling Performance Concerns in
Primary Care: An NCAS Good Practice Guide, London: NPS Agency Editor.
National Council of State Boards of Nursing (2009) An analysis of Nursys®
disciplinary data from 1996–2006. NCSBN Research Brief, 39.
National Health Service (NHS) North West (2008) Celebrating our Diversity and
Multi-Ethnic Contribution. Available from:
http://www.help.northwest.nhs.uk/nhs60timeline/ [Accessed 30 January 2013].
National Nursing Research Unit (NNRU) (2010) Managing poor performance in
nursing and midwifery: does the evidence make the grade? Policy+, 28. Available
from: http://www.kcl.ac.uk/nursing/research/nnru/publications/Policy-plus-Review.pdf
[Accessed 21 March 2013].
Nichols, J. and Campbell, J. (2010) The experiences of internationally recruited
nurses in the UK (1995–2007): an integrative review. Journal of Clinical Nursing, 19
(19–20), 2814–23.
Obholzer, A. and Roberts, V.Z. (2003) The Unconscious at Work, London: Taylor and
Francis.
Obrey, A. Vydelingum, V. and Robbins, I. (2007) Engaging with a new reality
experiences of overseas minority ethnic nurses in the NHS. Journal of Clinical
Nursing, 16 (12), 2221–8.
247
Obrey, A. and Vydelingum, V. (2004) The lived experience of overseas black and
minority ethnic nurses in the NHS in the south of England. Diversity in Health and
Social Care, 1 (1), 13–20.
Office for National Statistics (2009) Population estimates by ethnic group 2002–2009.
Available from: www.statistics.gov.uk [Accessed 13 March 2013].
Oikelome, F. (2007) The recruitment and retention of black and minority ethnic staff
in the National Health Service. A Race Equality Foundation Briefing Paper, March.
Available from: www.darkredweb.net/sites/default/files/publications/downloads/
health-brief4.pdf [Accessed 18 September 2013].
Oulton, J.A. (2003) Patient safety concerns us all. International Nursing Review, 50,
201.
Ouseley, H. (2008) Independent review into disproportionate regulatory outcomes for
black and minority ethnic solicitors. Available from:
http://www.sra.org.uk/documents/SRA/equality-diversity/ouseley-report.pdf
[Accessed 5 November 2014].
Pellat, G. (2003) Ethnography and reflexivity: emotions and feeling in fieldwork.
Nurse Researcher, 10 (3), 28–37.
Pike, G. and Ball, J. (2007) Black and Minority Ethnic and Internationally Recruited
Nurses. Results from RCN Employment/Working Well Surveys 2005 and 2002,
London: Royal College of Nursing.
248

Polit, D.F. and Beck, C.T. (eds) (2012) Essentials of Nursing Research: Appraising
Evidence for Nursing Practice, 7th edn, Philadelphia: Lippincott, Williams and
Wilkins.
Pollitt, C. and Bouckaert, G. (2000) Public Management Reform: a Comparative
Analysis, Oxford: Oxford University Press.
Pope, C. (2005) Conducting ethnography in medical settings. Medical Education, 39
(12), 1180–7.
Pugh, D. (2009) The phoenix process: a substantive theory about allegations of
unprofessional conduct. Journal of Advanced Nursing, 65 (10), 2027–37.
Race Relations (Amendment) Act (2000) Available from: http://www.legislation.
gov.uk/ukpga/2000/34/contents [Accessed 29 June 2013].
Ramsden, P. (2003) Learning to Teach in Higher Education, Abingdon: Routledge
Falmer.
Rebar, C.R., Gersch, C.J., Macnee, C.L. and McCabe, S. (eds) (2011)
Understanding Nursing Research: Using Research in Evidence-Based Practice, 3rd
edn, Philadelphia: Lippincott, Williams and Wilkins.
Reeves, S., Kuper, A. and Hodges, B.D. (2008) Qualitative research methodologies:
ethnography. British Medical Journal, 337 (7668), 512–4.
Roper, M. (2006) 500 docs and nurses off on full pay. The Daily Mirror. Available
from: http://www.mirror.co.uk/news-old/top-stories/2006/07/10/exclusive-500-doc-
nurses-off-on-full-pay-115875-17353312/ [Accessed 13 March 2013].
249

Roper, J.M. and Shapira, J. (2000) Ethnography in Nursing Research, London:
SAGE Publications.
Royal College of Midwives (RCM) (2012) Freedom of Information Request: Midwives
and Disciplinary Proceedings, March, London: RCM.
Ryan, F., Coughlan, M. and Cronin, P. (2007) Step-by-step guide to critiquing
research. Part 2: qualitative research. British Journal of Nursing, 16 (12), 738–44.
Saundry, R., Antcliff, V. and Jones, C. (2008) Accompaniment and representation in
workplace discipline and grievance. Available from: http://www.acas.org.uk/media/
pdf/d/n/0608_Accmpnmnt___rep_in_wplace_D_G-accessible-version-July-2011.pdf
[Accessed 7 March 2013].
Savage, J. (2006) Ethnographic evidence: the value of applied ethnography in
healthcare. Journal of Research in Nursing, 11 (5), 383–93.
Savage, J. (2000) Participative observation: standing in the shoes of others?
Qualitative Health Research, 10 (3), 324–39.
Simmons, M. (2007) Insider ethnography: tinker, tailor, researcher or spy? Nurse
Researcher, 14 (4), 7–17.
Simons, L. and Lathlean, J. (2010) Mixed methods. In: Gerrish, K. and Lacey, A.
(eds) The Research Process in Nursing, 6th edn, Chichester: Wiley-Blackwell.
Simpson, J.M., Esmail, A., Kalra, V.S. and Snow, S.J. (2010) Writing migrants back
into NHS history: addressing a ‘collective amnesia’ and its policy implications.
Journal of the Royal Society of Medicine, 103 (10), 392–6.
250

Siva, N. (2009) Race relations in the UK’s National Health Service. The Lancet, 373
(9679), 1935–6.
Skeggs, B. (2001) Feminist ethnography. In: Atkinson, P., Coffey, A., Delamont, S.,
Lofland, J. and Lofland, L. (eds) (2001) Handbook of Ethnography, London: SAGE
Publications.
Smith, G., Hagger Johnson, H. and Roberts, C. (2014) Ethnic minority police officers
and disproportionality in misconduct proceedings, Policing and Society, Taylor and
Francis.
Smith, G. Hagger Johnson, H. and Roberts, C. (2012) Disproportionality in Police
Professional Standards: An investigation of internally raised misconduct proceedings
in Greater Manchester Police with additional statistical analyses of West Midlands
Police and British Transport Police data; and statistical analyses of counter-
corruption intelligence data in the three services, Manchester: Greater Manchester
Police Force Publications. Available from: http://www.gmp.police.uk/content/Website
Pages78BAC278B27218D780257ADB004A9154? OpenDocument. [Accessed 12
December 2014].
Smith, V. (2001) Ethnographic research in educational settings. In: Atkinson, P.,
Coffey, A., Delamont, S., Lofland, J. and Lofland, L. (eds) (2001) Handbook of
Ethnography, London: SAGE Publications.
Snow, S. and Jones, E. (2011) Immigration and the National Health Service: putting
history to the forefront. History and Policy. Available from: http://
www.historyandpolicy.org/policy-papers/papers/immigration-and-the-national-health-
service-putting-history-to-the-forefron [Accessed 3 May 2011].251

South East Coast BME Network (2008) Race Equality Service Review, Hove: SEC
BME Network.
Spradley, J.P. (1980) Participant Observation, Belmont, CA: Wadsworth.
Sprinks, J. (2008) Diversity Champions needed to tackle racism against NHS staff.
Nursing Standard, 23 (4), 12–3.
Stone, K., Traynor, M., Gould, D. and Maben, J. (2011) The management of poor
performance in nursing and midwifery: a case for concern. Journal of Nursing
Management, 19 (6), 803–9.
Streubert, H.J. and Carpenter, D.R. (eds) (2011) Qualitative Research in Nursing:
Advancing the Humanistic Imperative, 5th edn, Philadelphia: Lippincott, Williams and
Wilkins.
Tod, A. (2010) Interviewing. In: Gerrish, K. and Lacey, A. (eds) The Research
Process in Nursing, 6th edn, Chichester: Wiley-Blackwell.
Topping, A. (2010) The quantitative-qualitative continuum. In: Gerrish, K. and Lacey,
A. (eds) The Research Process in Nursing, 6th edn, Chichester: Wiley-Blackwell.
Trades Union Congress (TUC) (2009) Report of the 2009 TUC Black Workers
Conference. Available from:
http://www.tuc.org.uk/equality-issues/black-workers/black-workers-conference
[Accessed 11 March 2014].
Trant, K. and Usher, S. (2010) Nurse Past, Present and Future. The Making of
Modern Nursing. London: Black Dog Publishing.
252
Traynor, M., Stone, K., Cooke, H., Gould, D. and Maben, J. (2013) Disciplinary
processes and the management of poor performance among UK nurses: bad apple
or systemic failure? A scoping study. Nursing Inquiry, 21 (1), 51–8.
Vandenberg, H.E. and Hall, W.A. (2011) Critical ethnography: extending attention to
bias and reinforcement of dominant power relations. Nurse Researcher, 18 (3), 25–
30.
Wainwright Trust (2012) A Quarter Century of Equality and Diversity: What’s
Changed and What Hasn’t, Wainwright Trust.
Walker, S., Read, S. and Priest, H. (2013) Use of reflexivity in a mixed methods
study. Nurse Researcher, 20 (3), 38–43.
Watson, H., Booth, J. and Whyte, R. (2010) Observation. In: Gerrish, K. and Lacey,
A. (eds) The Research Process in Nursing, 6th edn, Chichester: Wiley-Blackwell.
Whitehead, T.L. (2005) Basic Classical Ethnographic Research Methods. Secondary
Data Analysis, Fieldwork, Observation/Participant Observation and Informal and
Semi-structured Interviewing, Ethnographically Informed Community and Cultural
Assessment Research Systems (EICCARS) Working Paper Series, University of
Maryland, The Cultural Systems Analysis Group.
Wolcott, H.F. (1995) The Art of Fieldwork, Walnut Creek, CA: Altamira Press.
Appendices
253

Appendix 1: The disciplinary procedures examined in this study
This section provides a summary of the relevant stages, the process and personnel
involved in the disciplinary procedures examined in this study.
Informal disciplinary processes
All cases need to be investigated before disciplinary action is taken. The employee is
given an account of the concerns from the onset. Unless the allegations are serious,
informal attempts are made by the line manager to resolve concerns around the
standard of conduct, performance and behaviours of the employee. The line
manager will consult HR representatives. Depending on the employee’s needs,
clinical supervision, extra support as regular meetings and further training may be
introduced with action plans and review dates. This is to ensure all efforts have been
taken by the Trust and the employee to resolve the concerns. Confidentiality must be
maintained by all parties involved.
Formal disciplinary process
Formal disciplinary action is undertaken if there are no improvements in conduct or
there is a serious gross misconduct.
Investigation
An IO with delegated authority is allocated to investigate the employee who has
contravened Trust policy around code of conduct. The IO is supported by an HR
representative who may be a manager. In addition to the employee under
investigation, various staff related to the allegation may be interviewed by the IO and
HR advisor. After the investigation has been completed, the IO will produce the
management statement of the case with evidence to support. The designated officer
254

will decide if the matter will proceed to a formal hearing. If there is no case to answer,
the employee will be informed in writing.
Outcome of investigation
If a formal hearing needs to take place, the employee under investigation will be
given written details of the alleged misconduct and asked to attend the hearing.
Written details of the purpose of the hearing under the Trust’s disciplinary policy will
also be provided to the employee.
Employee representation
Throughout the disciplinary process, the employee under investigation has the right
to be represented by a work colleague or TU representative.
Suspension of staff
For serious allegations, the employee under investigation may be suspended.
Suspension is not a disciplinary action.
The disciplinary hearing and panel
The hearing has a chairperson who is supported by an HR manager and professional
lead. The chair of the panel is a designated manager who has the authority to
dismiss and suspend. The professional lead, where possible, is a senior professional
who comes from the same discipline as the employee under investigation. This lead
will offer advice on professional issues and standards. The HR representative will
assist and advise the chair of the panel. These three employees make up the
disciplinary panel that will hear the case, ask questions, seek clarification and decide
on the outcome of the case. The panel may adjourn the case if more information is
needed and then reconvene at a later date.
255

The employee under investigation is invited to attend the hearing with an employee
representative. The IO will present the case (for the Trust) with evidence against the
employee under investigation. The employee and representative are allowed to
respond to the case presented by the IO and provide explanations and mitigating
factors. Both management and the employee under investigation have the
opportunity to call and question witnesses. After the case has been heard, the panel
will take a break to decide on the outcome.
Outcome of hearing
The outcome can be no formal action or formal action to be taken. The chair of the
panel will convey the decision of the panel to the employee. If disciplinary action is to
be taken, the chair will state and give reasons for the sanction imposed. The
employee has an opportunity to lodge an appeal against the outcome. An appeals
panel will hear the case.
Appendix 2: Recruitment letters
256

RECRUITMENT LETTER – Observations
Version 2 – 31/10/2012
Date
Dear
The Apparent Over-representation of Black and Minority Ethnic (BME) Employees in
Disciplinary Hearings in an NHS Trust
There is recognition in the Trust of the over-representation of BME staff in disciplinary
hearings. The reason(s) for this are not clear. The purpose of this study is to begin to
understand and explain some of the reasons. I am asking you to help me with a project that
involves an observation study investigating the over-representation of BME in disciplinary
hearings. Observations will be undertaken by the researcher of Trust employees involved in
the disciplinary hearings and/or attend meetings where the over-representation of BME staff
in disciplinaries is discussed.
Attached to this letter are a consent form and a participant information sheet that gives more
details of the study.
If you are interested in participating in the study please return the consent form in the prepaid
addressed envelope, enclosed with this letter, to Harjinder Sehmi by DATE. Once this has
been received I will contact you to discuss the next stage.
If you would like more details please contact HarjinderSehmi on 07768 145528 or
Yours sincerely
HarjinderSehmi
RECRUITMENT LETTER – Interview
257
Version 2 – 31/10/2012
Date
Dear
The Apparent Over-representation of Black and Minority Ethnic Employees (BME) in
Disciplinary Hearings in an NHS Trust
There is recognition in the Trust of the over-representation of BME staff in disciplinary
hearings. The reason(s) for this are not clear. The purpose of this study is to begin to
understand and explain some of the reasons. I am asking you as a Trust employee involved
in disciplinary hearings and/or attending meetings where the over-representation of BME
staff in disciplinaries to help me with a study. This will involve an interview about sharing your
experiences and thoughts about the over-representation of BME in disciplinary hearings.
Attached to this letter are a consent form and a participant information sheet that gives more
details of the study.
If you are interested in participating in the study please return the consent form in the prepaid
addressed envelope, enclosed with this letter, to HarjinderSehmi by DATE. Once this has
been received I will contact you to discuss the next stage.
If you would like more details please contact Harjinder Sehmi on 07768 145528 or
Yours sincerely
HarjinderSehmi
Appendix 3: Participant information sheets
258

PARTICIPANT INFORMATION SHEET: OBSERVATIONS
Version 2 – 31/10/2012
The Apparent Over-representation of Black and Minority Ethnic Groups (BME)
Employees in Disciplinary Hearings in an NHS Trust
We would like to invite you to take part in a research study. Before you decide we would like
you to understand why the research is being done and what it will involve for you. I will go
through the information sheet with you and answer any questions you have. Please take your
time to read the following information carefully.
Part 1 tells you the purpose of this study and what will happen to you if you take part.
Part 2 gives you more detailed information about the conduct of the study.
Please contact HarjinderSehmi if anything is not clear and you would like to receive more
information. Take your time to decide whether or not you wish to take part in this study.
The research will investigate the apparent over-representation of BME employees in
disciplinary hearings within the Trust.
Employees involved in the disciplinary hearings and/or attend meetings where the over-
representation of BME employees in disciplinary hearings is discussed are invited to
participate in the research through an observation study.
PART 1
What is the purpose of the study?
The Trust through the superseded Race Equality Scheme, the current Equality and Diversity
Framework and Service and Equality Workforce Report 2012 has recognised that its BME
workforce are over-represented in disciplinaries. The reasons for this are not clear. The
purpose of this study is to begin to understand and explain some of the reasons. 259
Why have I been invited?
You have been invited to take part in this study as you are involved in disciplinary hearings
and/or attend meetings where the over-representation of BME employees in disciplinary
hearings is discussed.
Do I have to take part?
No, you do not have to participate. There will be no adverse consequences in terms of your
employment status if you decide not to participate. If you agree to take part you will be asked
to complete and sign a consent form. You are free to withdraw from the study at anytime,
without giving any reasons.
What will happen to me if I take part?
Once you have consented the researcher will inform you about the date he will be observing
a meeting you are attending where BME employees in disciplinaries is discussed.
Study methods
Observations are a method used to observe, and later analyse, behaviours as they occur in
meetings. For this study the researcher will employ two types of observations: non-
participant observations and participative observations. For non-participant observations the
researcher will be present but will not take part in the meeting. For the participative
observation the researcher will be present in the meeting and will occasionally ask questions
to the group related to the subject investigated. Notes from the observations will be taken by
the researcher and will be used as a part of the data analysis.
What will I have to do?
For the meetings observed by the researcher you will not need to do anything apart from
naturally carrying on as you do in the meeting.
260

What are the possible disadvantages and risks of taking part?
The individual and the group being observed may be distracted with the researcher present
and this may impact on how the individual and the group usually functions. Discomfort may
occur when the subject of BME employees in disciplinary hearings is discussed.
What are the possible benefits of taking part?
We cannot promise the study will help you but the information we get from this piece of work
will help the Trust to understand and explain the over-representation of BME employees in
disciplinary hearings. It may inform future policy, practices and further research.
What if there is a problem?
Any complaint about the way you have been dealt with during the study will be addressed.
The detailed information on this is given in Part 2.
Will my taking part in the study be kept confidential?
Yes. All of the information you give will be anonymised so that those reading and hearing
reports about the study will not know who has contributed to it. The details are included in
Part 2.
This completes Part 1
If the information in Part 1 has interested you and you are considering participation please
read the additional information in Part 2 before making a decision.
PART 2 of the information sheet
What will happen if I do not want to carry on with the study?
If you choose to withdraw from the study at any time no further data will be collected from
you. Any data that has already been collected will remain in the study.
261
Complaints
If you have a concern about any aspect of this study, you should contact the academic
supervisors Professor Helen Cowie and Professor Helen Allan who will do their best to
answer your questions. Contact details are:
Professor Helen Cowie – 01483689726 and [email protected]
Professor Helen Allan – 01483689745 and [email protected]
Address where both academic supervisors can be reached is: University of Surrey, Faculty of
Health and Medical Sciences, Guildford, Surrey. GU2 7XH.
If you remain unhappy and wish to complain formally you can go through the University of
Surrey. Details can be obtained from the Research Office on 01483 689110.
Harm
In the unlikely event that something does go wrong and you are harmed by taking part in this
study, there are no special compensation arrangements. If you are harmed due to
someone’s negligence then you may have grounds for legal action, but you may have to pay
for it.
Will taking part in this study be kept confidential?
All the information that is collected from you during the course of the study will be maintained
in a strictly confidential manner. All names of people and places will be removed and coded.
Pseudo names will be used in the transcription of audio recordings. Your personal details will
be stored in password-protected computers in password-protected files. The offices where
the computers are stored will be locked when the room is not occupied. Signed consent
forms will be stored in locked cabinets in locked rooms. Only the researcher will have access
to your personal details. The personal data will be stored until the end of the study so a
262

summary of the study can be sent to you. After this, all personal information will be disposed
of securely.
The data that has been collected for this study will be stored in a locked facility for 10 years.
Data will be stored securely in accordance with the Data Protection Act, 1998. The custodian
for the data will be HarjinderSehmi.
In the reporting of the project, no information will be released which will enable the reader to
identify participants.
What will happen to the results of the research study?
The results of the study will be written up as a doctoral thesis. A summary of the findings will
be sent to the participants. The results may also be published in academic journals. None of
these publications will reveal the identities of individuals and places who have participated in
this study.
Who is organising and funding the research?
This study is organised by the University of Surrey and no funding has been involved.
Who has reviewed the study?
All research in the NHS is looked at by an independent group of people, called a Research
Ethics Committee, to protect your interests. This study has been reviewed and given
favourable opinion by the Research and Development Department for St George’s University
of London and the University of Surrey Ethics Committee.
Further information and contact details:
If you would like any further information about research, specific information about this
research project, advice as to whether you should participate or are unhappy with the study
you can contact the researcher in the first instance:
263

HarjinderSehmi
Kingston University
Faculty of Health and Social Care
St George’s University of London
Grosvenor Wing
Cranmer Terrace
SW17 0RE
Email: [email protected]
Tel: 07768 145528
PARTICIPANT INFORMATION SHEET: INTERVIEW
264
Version 2 – 31/10/2012
The Apparent Over-representation of Black and Minority Ethnic Groups (BME)
Employees in Disciplinary Hearings in an NHS Trust
We would like to invite you to take part in a research study. Before you decide we would like
you to understand why the research is being done and what it will involve for you. I will go
through the information sheet with you and answer any questions you have. Please take your
time to read the following information carefully.
Part 1 tells you the purpose of this study and what will happen to you if you take part.
Part 2 gives you more detailed information about the conduct of the study.
Please contact HarjinderSehmi if anything is not clear and you would like to receive more
information. Take your time to decide whether or not you wish to take part in this study.
The research will investigate the apparent over-representation of BME employees in
disciplinary hearings within the Trust.
Employees involved in the disciplinary hearings and/or attend meetings where the over-
representation of BME employees in disciplinary hearings is discussed are invited to
participate in the research through an interview.
PART 1
What is the purpose of the study?
The Trust through the superseded Race Equality Scheme, the current Equality and Diversity
Framework and Service and Equality Workforce Report 2012 has recognised that its BME
workforce are over-represented in disciplinaries. The reasons for this are not clear. The
purpose of this study is to begin to understand and explain some of the reasons.
Why have I been invited?265

You have been invited to take part in this study as you are involved in disciplinary hearings
and/or attend meetings where the over-representation of BME employees in disciplinary
hearings is discussed.
Do I have to take part?
No, you do not have to participate. There will be no adverse consequences in terms of your
employment status as a staff member if you decide not to participate. You are free to
withdraw from the study at anytime, without giving any reasons.
What will happen to me if I take part?
Once you have consented a meeting will be arranged with you to explain the interview
process. A date and time at your convenience for the semi-structured interview will be
arranged. This will be followed by the schedule meeting for you to be interviewed by the
researcher.
Study methods
Semi-structured interviews are a method of study where the researcher has pre-determined
themes to be explored with the interviewee during the interview. Open-ended new questions
will be used to follow up what the interviewee says. The interview will be audio recorded so
the interviewer can engage with the interviewee with minimal distractions. The recordings will
later on be transcribed and analysed.
What will I have to do?
Semi-structured Interview: The interview will be carried out face to face in a room with the
researcher. You will be asked about your experiences and thoughts about the over-
representation of BME employees in disciplinary hearings.
The interviews will take no longer than 45 minutes.
266

What are the possible disadvantages and risks of taking part?
Taking part in the interview will involve your time. Interviewees may become emotional,
particularly if they have been the person disciplined.
What are the possible benefits of taking part?
The information we get from this study will help the Trust to understand and explain the over-
representation of BME employees in disciplinary hearings. It may inform future policy,
practices and further research.
What if there is a problem?
Any complaint about the way you been dealt with during the study will be addressed. The
detailed information on this is given in Part 2.
Will my taking part in the study be kept confidential?
Yes. All of the information you give will be anonymised so that those reading and hearing
reports about the study will not know who has contributed to it. The details are included in
Part 2.
This completes Part 1
If the information in Part 1 has interested you and you are considering participation please
read the additional information in Part 2 before making any decision.
PART 2 of the information sheet
What will happen if I do not want to carry on with the study?
If you choose to withdraw from the study at any time no further data will be collected from
you. Any data that has already been collected will remain in the study.
267
Complaints
If you have a concern about any aspect of this study, you should contact the academic
supervisors Professor Helen Cowie and Professor Helen Allan who will do their best to
answer your questions. Telephone and email contact details are:
Professor Helen Cowie – 01483689726 and [email protected]
Professor Helen Allan – 01483689745 and [email protected]
Address where both academic supervisors can be reached is: University of Surrey, Faculty of
Health and Medical Sciences, Guildford, Surrey. GU2 7XH.
If you remain unhappy and wish to complain formally you can go through the University of
Surrey. Details can be obtained from the Research Office on 01483 689110.
Harm
In the unlikely event that something does go wrong and you are harmed by taking part in this
study, there are no special compensation arrangements. If you are harmed due to
someone’s negligence then you may have grounds for legal action, but you may have to pay
for it.
Will taking part in this study be kept confidential?
Yes. All that is collected from you during the course of the study will be maintained in a
strictly confidential manner. All names of people and places will be removed and coded.
Pseudo names will be used in the transcription of audio recordings. Your personal details will
be stored in password-protected computers in password-protected files. The offices where
the computers are stored will be locked when the room is not occupied. Signed consent
forms will be stored in locked cabinets in locked rooms. Only the researcher will have access
to your personal details. The personal data will be stored until the end of the study so a
268

summary of the study can be sent to you. After this, all personal information will be disposed
of securely.
The data that has been collected for this study will be stored securely in a locked university
facility for 10 years. Data will be stored in accordance with the Data Protection Act, 1998.
The custodian for the data will be HarjinderSehmi.
In the reporting of the project, no information will be released which will enable the reader to
identify participants.
What will happen to the results of the research study?
The results of the study will be written up as a doctoral thesis. A summary of the findings will
be sent to the participants. The results may also be published in academic journals. None of
these publications will reveal the identities of individuals and places who have participated in
this study.
Who is organising and funding the research?
This study is organised through the University of Surrey and no funding has been involved.
Who has reviewed the study?
All research in the NHS is looked at by an independent group of people, called a Research
Ethics Committee, to protect your interests. This study has been reviewed and given
favourable opinion by the Research and Development Department for St George’s University
of London and the University of Surrey Ethics Committee.
Further information and contact details:
If you would like any further information about research, specific information about this
research project, advice as to whether you should participate or are unhappy with the study
you can contact the researcher in the first instance:
269

HarjinderSehmi
Kingston University
Faculty of Health and Social Care
St George’s University of London
Grosvenor Wing
Cranmer Terrace
SW17 0RE
Email: [email protected]
Tel: 07768 145528
Appendix 4: Consent forms
270

CONSENT FORM – Version 2 (31/10/2012)
The Apparent Over-representation of Black and Minority Ethnic Employees in
Disciplinary Hearings in an NHS Trust
Consent for observations
1. I confirm that I have read and understand the information sheet dated
_____________________ for the above study. I have had the opportunity
to consider the information, ask questions and have had these answered
satisfactorily.
2. I understand that my participation is voluntary and that I am free to
withdraw at any time without giving any reason and without my legal rights
being affected.
3. I agree to take part in the above study.
__________________________ _____________ _________________
Name of participant Date Signature
__________________________ _____________ _________________
Name of person taking consent Date Signature
271

AFTER THE OBSERVATION
I am happy that the data from the observations can be used for this specific
research project.
__________________________ _____________ _________________
Name of participant Date Signature
__________________________ _____________ _________________
Name of person taking consent Date Signature
CONSENT FORM – Version 2 (31/10/2012)
272

The Apparent Over-representation of Black and Minority Ethnic Employees in
Disciplinary Hearings in an NHS Trust
Consent for interview
1. I confirm that I have read and understand the information sheet dated
_____________________ for the above study. I have had the opportunity
to consider the information, ask questions and have had these answered
satisfactorily.
2. I understand that my participation is voluntary and that I am free to
withdraw at any time without giving any reason and without my legal rights
being affected.
3. I agree to take part in the above study.
__________________________ _____________ _________________
Name of participant Date Signature
__________________________ _____________ _________________
Name of person taking consent Date Signature
273

AFTER THE INTERVIEW
I am happy that the data from the interview can be used for this specific
research project.
__________________________ _____________ _________________
Name of participant Date Signature
__________________________ _____________ _________________
Name of person taking consent Date Signature
Chapter 9: Overview of the integration of
knowledge, research and practice
274

9.1 Introduction
This chapter looks at how modules from the taught clinical doctorate facilitated the
final research project. An overview of the key themes that contributed to this study
and how they were integrated are discussed.
9.2 Development of self
The taught doctorate has empowered me to investigate a sensitive and politically
charged area that is under-researched.
Learning is a complex and individual process that incorporates emotions, cognitions
and behaviours. Moving from novice to expert (Benner, 1984) requires a transition
from surface to deep understanding (Ramsden, 2003) and challenging underlying
assumptions that justify behaviours. Reflections become critical when it uncovers the
dynamics in power relationships and when social and cultural hegemonic practices
are critically analysed. The knowledge gained from this tacit region has supported me
to confront, understand and work through an area of inequalities. Critically reflecting
and learning from experience can empower and liberate marginalised groups and
formulate new understanding so inequality and inequity can be curtailed.
The taught part of the doctorate has allowed me to identify with the child in The
Emperor’s New Clothes by Hans Christian Andersen: the lone child in the audience
of a procession pointing out the emperor is not wearing any clothes.
9.3 Advanced research methods
Before attending the course, my knowledge around the different qualitative and
quantitative methodologies was limited. Looking back on my experience around the
master’s programme that I undertook, I often consider the grounding in methodology 275
at the time was narrow and ‘unscientific’. The epistemology of the theory of
knowledge and science provided a foundation to consider the best method I could
draw on to find out about culture and multiple realities that exist side by side.
I was aware of anthropologists going too far away exotic locations and spending
years with their notepads, binoculars and magnifying glass to gather information to
explain the cultures of these societies. Naively, I did not consider that some of the
methods used by these social explorers could be applied nearer to home.
During this module I was quickly drawn to the sessions on ethnography. On further
reading and discussions with staff delivering this module, I came to the conclusion
that ethnography was the best method to explore the over-representation of BME
employees in the disciplinary process in an NHS Trust. I wanted to explore this
phenomenon from the perspective of employees who were directly involved in the
disciplinary process and hear about their subjective realities.
The fantasy I had was quickly challenged and dispelled when designing the approach
I could undertake. The reality of finding and negotiating with a Trust to gain access to
undertake a study was a challenge. Without securing a site, the study could not
happen.
The module gave me a framework to consider what I would be presenting to senior
managers pressurised by time and heavy workloads and how I could use the time
allocated to engage and commence a trusting relationship. The rationale for the
methods I would use to collect data was questioned. In particular, queries were made
about the use of participant observations. Months of negotiations were rewarded with
consent given to undertake the study at the Trust site.
276

Although the taught doctorate equipped me with the tools to carry out the study,
engaging with gatekeepers to discuss how these tools were going to be applied in
their settings was equally important. Having discussions in the class made me
critically reflect on why certain approaches in ethnography were being used and not
others.
The role of preserving ethics and how this is sensitively conveyed without arousing
further anxiety was crucial. As a novice who had never had to go through an ethics
committee, this was a daunting and yet an important learning experience, particularly
around the blind spots that were unexpectedly uncovered. My proposal had been
rejected by the UREC at the first submission. More clarity was needed on how BME
employees who had been disciplined would be protected. The support, experience
and advice from academic supervisors to solve this problem were invaluable.
9.4 Service evaluation
The NHS Trust where I undertook my study has been going through disaggregation
and reconfiguration in order to improve the efficiency and cost-effectiveness of its
services. This module raised awareness of the realities of health economics in the
NHS which has raised discomfort in me and challenged my political stance. The
impact of cost-effective measures to increase productivity with fewer resources and
their consequences on clinicians delivering services has been visible while I have
been collecting data in the field.
9.5 Leadership in healthcare organisations
The summative assignment for this module highlighted how a leader of a public
organisation inconspicuously rationalised white dominance. Leadership in the context
277

of an organisation made me consider what lies under the surface. The unconscious
psychic life and defences of organisations and individuals that are used to avoid
difficult and painful emotions were discussed in this piece of work. During the
collection of data for the final research, I reflected on how people from diverse and
different backgrounds were presented. The category of BME arouses reactions
where the category white is presented as neutral and the norm. My final study
wanted critically to reflect and analyse the norms that preserve the self-interests,
power and privilege of dominant groups. Also, I wanted to move away from the
polarised debate between ‘white versus black’ and consider the differences within
and between BME groups.
9.6 Emotional intelligence
The taught doctorate programme not only developed knowledge but also considered
how emotions are understood and worked with. My subject area involved dealing
with anxiety. The use of self-awareness to understand my feelings during the time
spent in the Trust, meeting employees and collecting data, was constantly checked. I
also considered how I managed myself, particularly when I felt vulnerable. If I felt too
anxious, this would be picked up and have an impact on the dynamics in the
relationships and potentially the quality of data shared and collected. It was important
to consider what others were saying, feeling and why. The use of reassurance was
constantly monitored. There were concerns from senior managers that the findings
could be negative and the Trust perceived as discriminatory, particularly at a time of
making another bid to gain FT status. Undertaking a position of neutrality is not
always easy. Academic supervision has been a space to work through the issues
that have come up.
278

9.7 Policy, politics and power
The phenomenon of the disproportional representation of BME employees involved
in the disciplinary process is politically charged. Undertaking a module on policy,
politics and power enabled me to think about the context, process and content of the
policy-making process which I incorporated into my research.
To understand the data I was collecting, I needed to reflect on the context of the
Trust. Attention in particular was paid to the historical, political, social and cultural
context. BME staff, particularly nurses and doctors, have been rooted in the NHS
since 1948. The cultural behaviours and working practices and how they fitted in with
the norms of the majority made me critically reflect on the imbalance of power.
Critically reflecting on power relationships was important to consider when I was
collecting data. The complexity of what might be going on between the interviewer
and interviewee was analysed. Consideration was given to the gender, race, age,
status of role and class of the participants. Attention was also given to where the
interviews were being conducted. I would ask the participants where they wanted to
meet. Without discussing this openly, this was to reinforce that the participant had
some control and was in a place where they would be comfortable to talk. What was
striking was that senior managers liked to meet in their offices. Rarely did participants
come to the HR department where I was based.
Disciplined BME employees did not participate in this study despite initially showing
interest. Part of the reason was that they did not want to relive the painful experience,
which was understandable. However, trying to reflect how this could be addressed
279

for future studies continues to pose an issue. This issue is raised as the experiences
of these employees have not been integrated into this study. A gap remains.
9.8 Dissemination of the findings
The findings from this study will be summarised and shared with the Trust.
Presentations and discussions will be held. Attention will be paid to how this will be
facilitated to encourage an open and authentic dialogue.
How this study can be developed and consolidated into further research with the
Trust, which has allowed a sensitive subject to be explored, remains to be seen. It is
important that the ethos of this study is embraced and its findings incorporated into
practice.
Concepts and findings will be integrated into teaching sessions with pre- and post-
registered nurses. Undertaking this study informed by the taught doctorate has made
me critically reflect about the quality of training that healthcare professionals,
particularly nurses, receive. It is unclear if issues around poor conduct and
performance are rooted in how nurses are trained and socialised into the profession.
This aspect has been overlooked as the study did not consider the role of higher
education institutions. In collecting data on disciplinaries, the place of training needs
to be considered. As a lecturer involved in the training of pre- and post-registered
nurses, I have become more aware of my responsibilities in supporting and
challenging student behaviour around conduct and performance.
9.9 Conclusion
Key areas of the taught programme that had significance have been highlighted. I
began this course with a lack of depth and inexperience in the research process. 280
Having the opportunity to engage with a process that allowed me to undertake an
under-researched study has been an achievement.
Chapter 10: Research log
281

10.1 Introduction
This research log is the journey for undertaking a thesis to investigate the
disproportional representation of BME employees involved in the disciplinary process
in an NHS Trust. The journey starts with the application made to the university to
undertake a taught doctoral programme and continues to the submission of the
thesis.
10.2 Why I took a taught clinical doctorate programme and not a
PhD route?
Although I lecture at a university, I have continued to undertake clinical work in the
NHS. Mental health nursing and psychotherapy have informed my teaching of
nursing students and qualified nurses. The context of the setting where clinical work
is undertaken has been consistently at the forefront in my thinking, particularly at a
time of continuous political and economic change. Even though patients are at the
centre of the NHS, the quality of care provided depends on how clinicians on the
front line are supported during chaotic times.
By its nature, the taught clinical doctoral programme has allowed me to continue to
focus and keep the clinical work in mind. It has precluded me from engaging with
something abstract and not directly related to the day-to-day realities of working in
the NHS. Modules from the taught element provided a framework, tools and skills to
undertake a study on a sensitive area that few have embarked on.
A valuable part of my learning has been studying with peers. Undertaking a taught
programme allowed me the opportunity to be with other doctoral students. At the start
of the course, there were four of us.
282
10.3 Selecting the subject to investigate
Originally I wanted to develop my Master of Science (MSc) study to a doctoral level.
The area that I examined for the masters programme was why BME patients,
particularly from South Asia living in Britain, did not engage in psychological
therapies such as group psychotherapy. During the literature search, I was distracted
by the disproportional representation of BME employees involved in the disciplinary
process in the NHS. On further investigation, I found that there was a dearth of
studies in this area to explain the reasons for this phenomenon. Studies that
investigated this phenomenon did not consider the experiences and perspectives of
employees directly involved in the disciplinary process in an NHS Trust.
10.4 Framework, tools and skills needed to undertake the study
There was a ten-year gap between finishing my MSc to starting the application to
undertake the doctoral studies. Although I had successfully completed the master’s
programme, I felt out of touch with the rigour of the research process and lacked
some confidence and skills to undertake a major step towards the doctoral level.
The taught element of the course provided a grounding to build the proposal into a
thesis. This started off with epistemology arising from the philosophy of science and
knowledge. The module on policy, politics and power highlighted the politics of
research. The questions of ‘whose truth’ and which groups in society are
marginalised were considered in the study. Issues around multiple realities existing
alongside each other were also taken into account. Policy analysis took into account
whose health and social care needs are met. Confidence was obtained to analyse
the responses from government that were not always as they appeared. Measures
could be rhetorical. This study wanted to look beyond this. The leadership and 283

management component of the taught programme gave an opportunity to analyse
and reflect critically how leaders followed by managers marginalise under-
represented groups without authority been questioned. To advance knowledge,
thought was given to areas that were emotionally charged and how I could be in this
space to reflect critically on what was happening in an emotionally intelligent and
sensitive way to open discourse. Undertaking the assignment for leadership in
healthcare organisations was invaluable. This provided a framework that supported
me to gain access to an NHS Trust and investigate a sensitive and politically charged
phenomenon that was under-researched.
To undertake this task, advanced research methods provided a structure to think
about the approach I was going to use. Qualitative and quantitative paradigms about
the best methodology to investigate the culture and lived experiences of employees
in a Trust drew me to ethnography. This was an approach that I was unfamiliar with
and at the same time excited about. Tools and skills to understand and use the
concepts from ethnography were provided to enter the world of social anthropology.
The service evaluation brought in the economic realities of governments with limited
resources having to make decisions on what health and social care to provide to the
population. The complexity of the world of health economics that I had ignored was
brought to the fore. This area again has been helpful, particularly being in the field
where services have been disaggregated and reconfigured because of the economic
realities.
284

10.4.1 Gaining access to a Trust
The proposed research depended on finding a Trust with a disproportional
representation of BME employees involved in the disciplinary process. Negotiating
permission to gain consent and access to an NHS Trust to undertake a study
involving a sensitive and politically charged subject took longer than the actual time
that was spent in the field to collect data. The gatekeepers were Trust Board
executives and a senior manager. A number of meetings were held to build up a
trusting relationship. Attention to the use of sensitive language was given. Words
such as ‘racism’ and ‘discrimination’ were avoided. Where possible, neutrality was
maintained and assumptions were avoided. Research jargon was avoided and if it
had to be used it was simplified without becoming patronising.
During negotiations, a Trust Board executive wanted me to make amendments to the
research proposal. The title of the study and the size of sample needed to change
before any authorisation would be given. This was carefully considered with
academic supervisors. I was afraid of losing autonomy and authority over my study.
At the same time, with the pressure to complete the taught programme within a
specified time, I was worried I would lose this site after many months of painstaking
negotiations. The changes were adapted to the research proposal and submitted to
the Trust’s R&D ethics committee and the UREC.
Having gained permission to enter the field and collect data, the senior manager,
who had advocated and supported my study, left the Trust without serving notice.
This was a precarious time as I felt vulnerable. I feared the Trust would withdraw its
consent. I managed to collect the data within the time allocated. However, areas and
meetings to undertake participant observations were restricted.
285
10.5 Research process
As a BME doctoral student, I have been aware of undertaking a study that has
involved BME employees who have been treated unfairly and unequally. I have been
particularly mindful of this when BME employees have spoken openly about
colonialism in the interviews. Coming from a country that was under British colonial
rule, I have tried to reflect on the impact of this dynamic on my motivation to
undertake a study of this nature and the impact this could have on the research
process.
There was a dearth of studies on the over-representation of BME employees
involved in the disciplinary process in the NHS. During the literature search, I
struggled to find academic articles. I felt as if I was not doing the search correctly and
had overlooked something in the process. The support of staff from the learning
resource centre from the university and the medical school to help with finding
academic articles was drawn on. They too struggled in finding articles. Trying to link
the findings from the study to the literature review in the discussion, at times, has not
been consistent and thorough.
Initially I was asked to put in an application to the NRES. This was daunting as I have
never had to undertake this process before. Engaging with making an application
was a challenging and confusing experience. After I submitted my application to
NRES, I was informed that I did not need approval from this body as my study did not
cover patients and carers. However, I did need to go through the Trust’s own R&D
ethics committee.
286

Ethical concerns were raised by the UREC about collecting data from BME
employees who had been disciplined. The committee wanted to know how the
confidence and confidentiality of this group of participants would be protected. The
measures that would be taken were clarified.
This study has not been able to engage BME employees who have been disciplined.
Initially employees did express interest but when times and locations of their choice
were arranged to meet, they withdrew. TU officials acting as intermediaries reported
these employees did not want to relive the experience of the event and its associated
emotions of shame and humiliation.
Gaining permission and access to observe a disciplinary hearing was an
achievement, particularly as these hearings are confidential and happen behind
closed doors. The findings from this study have predominantly come from the 27
semi-structured interviews with employees who have been directly involved in the
disciplinary process. Most interviews were audio recorded and lasted approximately
one hour. The interviews were transcribed and then the transcripts were read while
listening to the audio recordings to check for accuracy. Owing to constraints, the
transcribed interview could not be checked with participants for clarification and
follow-up questions. Finding and analysing themes from the masses of data collected
was overwhelming. The structure of the discussion has centred on the findings.
Writing to the critical level of analysis required for a doctoral level has presented
challenges.
287

10.6 Academic supervisors
Having the support and guidance from academic supervisors has been integral in this
process. A lot can be gained from their experience and knowledge. This is not always
used to the optimal level at the time. Taking on board the constructive challenges
presented by supervisors has not always been easy, particularly when agreed action
plans have not been met at timescales set. The realities of not meeting the tasks
have been appropriately discussed in the annual reviews and supervision sessions.
Supervision has been regular and the supervisors have been available between
sessions.
During the journey, unexpected personal events have happened outside the course
that have led to taking time out from the studies. Supervisors have been there to
provide pastoral support. Re-engaging with studies after time away has not always
been straightforward.
10.7 Peer support
I have always gained from the support and experiences from fellow peers particularly
clinicians from previous courses that I have undertaken. At the beginning of the
programme, four doctoral students enrolled on the course. Over time, the other three
students have left the course without completing. Undertaking doctoral studies has
been an isolated and lonely journey at times. Many things have been put on hold.
Relationships with my partner, family and friends have had to be adapted. This has
had an impact on my learning experiences and how I have engaged with the doctoral
process. People who have been on this quest or are going through this process know
what it is like and can identify with the rollercoaster of emotions and demands.
288

Others who have not undertaken this journey do not understand. I have missed the
peer support of being in a group, particularly at these times.
10.8 Conclusion
This research log gives an overview of the journey that I undertook. Reasons why I
took the taught doctorate and not the PhD route are touched on. Arriving at the
phenomenon that I investigated came from a literature search around another area I
had set out to undertake. Key areas have been identified, particularly around
securing an NHS Trust to allow me to undertake a study about a sensitive subject.
Without having a site, this study would not have taken place.
289