202458482 final-case-presentation-abnormal-uterine-bleeding
TRANSCRIPT

Get Homework/Assignment Done
Homeworkping.comHomework Help https://www.homeworkping.com/
Research Paper helphttps://www.homeworkping.com/
Online Tutoringhttps://www.homeworkping.com/
click here for freelancing tutoring sitesIntroduction
Abnormal uterine bleeding is a condition in which a woman bleeds from
her uterus at an unexpected time or in a way that is unusual for her. For
example, bleeding between periods, a period that is heavier longer-lasting than
normal, bleeding after sexual intercourse, clots or spots in the menstrual blood
and any bleeding after menopause may all be considered abnormal uterine
bleeding.
The most common reason for irregular uterine bleeding is pregnancy.
Spotting or very light bleeding may occur with no real significance, but you
should always check with your doctor if you’re bleeding while pregnant. Another
common reason for abnormal menstrual bleeding is having too much or too little
of certain hormones. This often occurs during adolescence, when hormone levels
fluctuate. Intrauterine device (IUD) can cause abnormal bleeding by irritating the
uterine lining. The bleeding is usually accompanied by cramping. Also called
Stein-Leventhal syndrome, Polycystic Ovarian Syndrome occurs when you don’t
ovulate regularly. If your period comes with pain or foul-smelling greenish
discharge you may have an infection of a pelvic organ, such as your uterus,
cervix or ovaries. Bleeding would commonly follow sex or douching. These
1

infections are often caused by sexually transmitted diseases. Fibroid tumors are
non-cancerous tumors that grow in the uterine muscle. They usually affect
women in their 30s or 40s. most common among black women, they are also
fairly common among white women, but extremely rare in Asian women. Other
possible reasons for abnormal menstrual bleeding include polyps, small growths
that develop in the cervix or uterus. Their causes are unclear, but are related to
an excess of estrogen, which may be result of an infection, hormone treatment or
some types of ovarian tumors.
The most probable etiology of abnormal uterine bleeding relates to the
patient’s reproductive age, as does the likelihood of serious endometrial
pathology. The specific diagnostic approach depends on whether the patient is
premenopausal, perimenopausal or postmenopausal. In premopausal women
with normal findings on physical examination, the most likely diagnosis is
dysfunctional uterine bleeding (DUB) secondary to anovulation, and the
diagnostic investigation is targeted at identifying the etiology of anovulation.
Abnormal uterine bleeding (AUB) in nonpregnant women is a common
problem. In fact, AUB accounted for almost 4 million outpatient visits (mostly to
physicians’ offices) in the United States in 1996. Indeed, this problem may
prompt more than 20% of all visits to OB/GYNs, and may account for more than
one fourth of all hysterectomies. AUB is rare in prepubertal females. Newborn
girls occasionally have a slight bloody vaginal discharge secondary to withdrawal
of placental estrogens. AUB is common in adolescents because of the 1- to 5-
year delay in development of regular ovulatory menstrual cycles after menarche.
AUB also tens to be more common during the fifth decade of life (the
perimenopausal years). In the worst case, AUB may be a sign of atypical
endometrial hyperplasia, which, if undiagnosed and untreated, can progress to
uterine cancer-the most common female genital cancer. In 1998, estimated
36,100 women were diagnosed with uterine cancer, which led to approximately
6,300 deaths.
One popular form of treatment for abnormal uterine bleeding is birth
control pills, which contain hormones that can prevent the uterus lining from
2

thickening. If birth control pills are’nt stopping the bleeding, a doctor may
prescribe an intrauterine (IUD) device. An IUD is a plastic device that is inserted
into a woman’s uterus to prevent pregnancy. In rare cases, surgery may be
needed to stop abnormal bleeding. Two surgical procedures are recommended:
hysterectomy and endometrial ablation.
OBJECTIVES
General Objectives
This study attempts to examine the case of the client with abnormal
uterine bleeding, specifically it attempts:
1. To obtain clients data
2. To perform thorough physical assessment to the client
3. To discuss the anatomy and physiology of the reproductive system
4. To trace the pathophysiology of abnormal uterine bleeding
5. To present laboratory results and its interpretation
6. To formulate appropriate nursing diagnosis who has abnormal uterine
bleeding
3
7. To develop nursing care plan for client based to identifies nursing
problems.
8. To present drug studies as medications given to client as a part of
treatment regimen.
9. To provide health teaching to patient and significant others about
prevention of recurrence of AUB.
PERSONAL DATA
Name: Cristy Joy Lactason
Address: Brgy. Naje, Arakan, Cotabato
Date of Birth: August 7, 1990
Birthplace: Brgy. Naje, Arakan, Cotabato
Age: 19 years old
Sex: Female
Civil Status: Single
Religion: Roman Catholic
Educational Status: Second year high school
Nationality: Filipino
MEDICAL DATA
Hospital: Kidapawan Medical Specialists Center Inc.
Ward: NS 2
Room & Bed No. Room 218-A
4

Chief Complaints: Profuse menstruation/Menometrorrhagia
Date & Time Admitted: July 25, 2010, 4:30 pm
Physicial: Dr. Phillen Drama Ureta
Admitting Diagnosis: T/C abnormal uterine bleeding
Final Diagnosis: Abnormal Uterine Bleeding
FAMILY BACKGROUND
I. History of Present Illness
The condition started about 1 month prior to admission as onset of
prolonged vaginal bleeding lasting for 15 days soaking 4-6 pads per day
associated with dysmenorrhea. No consultation done and no medications taken.
Two days prior to admission patient’s vaginal bleeding spontaneously
regressed.
One day prior to admission patient’s vaginal bleeding recurred and
completely soaked several pads associated with pallor and dizziness prompting
to consult an OB-Gynecologist (Dr. Phillen Drama Ureta) and subsequent
admission.
II. History of Past Illness
Patient was hospitalized last March 2010 at Antipas Hospital due to
profuse vaginal bleeding and was treated with Diane pills taken with poor
compliance. She is non-asthmatic, non-diabetic, non-hypertensive with no known
food and drug allergies.
5

III. Medical History of Family
No heredofamilial diseases such as hypertension, diabetes, asthma and
cancer were reported in the family.
X,
IV. Personal and Social History
Patient is a second year high school student at Arakan National High
School. She is the second child among 3 siblings. Her father is a farmer and her
mother is a plain housewife. She is a non-smoker, an occasional alcohol
beverage drinker and denies any use of prohibited drug. She has a boyfriend but
denies coitus at her age. She spends most of her time watching television.
V. Menstrual History
She started her menarche at the age of 13 years old, with an interval of
28-30 days and duration of 4-6 days. Amount of blood is heavy soaking 3-4 pads
per day accompanied with dysmenorrhea.
6

DEVELOPMENTAL DATA
Age/Stage Description according to Theories Analysis• 19 y/o
Havighurst-Adolescence
Erikson-Adolescence (12-20)
Kohlberg-Adolescence and Adulthood
Havighurst Erikson KohlbergOn Havighurst theory, the patient has met the indicators of an adolescent except achieving assurance of economic independence.
On Erikson’s theory, client indicates positive resolution, she has a sense of self and plans to actualize her abilities.
On Kohlberg’s theory, the client is concerned in maintaining expectations and rules of the family group.
Adolescence1. Achieving new and more mature relations with age-mates of both sexes2. Achieving masculine or feminine social role3. Accepting one’s physique and using the body effectively4. Achieving emotional independence from parents and other adults.5. Achieving assurance of economic independence.6. Selecting and preparing for an occupation7. Preparing for marriage and family life.8. Developing intellectual skills and concept necessary for civic competence9. Desiring and achieving socially responsible behavior10. Acquiring a set of values and ethical system as a guide to behavior.
Central task-Identity vs. Role Confusion
Indicators of Positive Resolution-Coherent sense of self; Plans to actualize one’s abilities
Indicator of Negative Resolution-feelings of confusion. Indecisiveness and possible anti-social behavior
Conventional Level-Person is concerned in maintaining expectations and rules of the family group, nation or society. A sense of guilt has developed and affects behavior. The person values conformity, loyalty and active maintenance of social order and control. Conformity means good behavior or what pleases or helps another and is approved.
Law and Order Orientation-The person wants established rules from authorities, and the reason for decision and behavior is that social and sexual rules and traditions demand the response.
7

PHYSICAL ASSESSMENT
Date of Assessment:
I. General Apperance
Date: July 26, 2010 Time: 9:45AM
Received client conscious and coherent on bed with PNSS 1L @ 20
gtts/min at the level of 200 cc infusing well @ right metacarpal vein. Patient appeared
ungroomed with uncombed hair and wrinkled clothes with black nail polish. When nail
polish was removed, client’s nail bed showed pallor. Client was generally pale.
II. Vital Signs and Clinical Measurements
Weight: 43 kg Height: 5’1”
Vital Signs upon Assessment:
BP: 110/90 mmHg PR: 70 bpm
RR: 18 cpm Temp: 36.2℃III. Hair
Hair is black, straight and well distributed. No presence of lice and
dandruff noted.
IV. Head
Normocephalic. No deformities noted.
V. Eyes
Eyes are symmetrically aligned and equal in movement, eyelashes are
evenly distributed and curled. Pupils are equally reactive to light and accommodation on
8

examination (using a penlight). She has good visual acuity based on snellen’s test.
Conjunctivas are pale and eyeballs are in good position and alignment.
VI. Ears
Hearing is normal upon assessment using Weber’s test, no gross
deformities noted. She is able to locate the direction of the sound of her ringing
celphone.
VII. Nose
No asymmetry, no nasal discharges noted and can identify odors.
VIII. Neck/Throat
No neck vein engorgement, no lymphadenopathy, tonsils are in normal
size, no difficulty on swallowing. The neck can move from left to right and can be flexed,
extended and hyper extended.
IX. Chest and Lungs
Equal chest expansion, no retractions noted, clear breath sounds and with
bilateral chest movements. RR: 18 cpm
X. Heart and Circulation
Distinct heart sounds, regular rhythm, BP: 110/90mmHg
PR: 70 bpm.
XI. Breasts
Breast size and symmetry are relatively equal with slight variation. Shape
is round and firm. Color is flesh and skin surface is smooth. Nipples are pink in color
9

with no discharges noted. She uses brassieres, no lumps or masses noted upon
palpation.
XII. Abdomen
No scars noted, soft, normoactive bowel sounds noted. No tenderness.
XIII. Genito-urinary
Normal external genitalia, abundant pubic hair with moderate bleeding.
No alteration in urinary and bowel habits. She experiences 15 days of menstruation
and soaks 4-6 sanitary napkins a day. She also urinates every 20 minutes during this
period.
XIV. Extremities
A. Upper Extremities
No skin lesion is noted. No growth deformities. She can move her upper
extremities freely and are both symmetrical in size and length. With PNSS 1L @ 20
gtts/min at the level of 200 cc infusing well @ right metacarpal vein.
B. Lower Extremities
No skin lesion is noted. No growth deformities. Her lower extremities are
both symmetrical in size and length with limitation of movement because movement and
straining or any forceful activity can aggravate profuse vaginal bleeding.
XV. Food Preference
Patient verbalizes fondness of eating meat, fish and vegetables.
XVI. Identified Needs
The patient needs to maintain fluid and electrolyte balance, needs to keep
body clean and well groomed and protect the integument and needs
performance of activities of daily living.
10

XVII. Nursing Diagnoses
• Risk for Fluid Volume Deficit R/T Uterine Bleeding
• Risk for Activity Intolerance related to decreased hemoglobin
• Self-care deficit: bathing/ hygiene related to decreased motivation
• Easy fatigability related to decreased hemoglobin
TERMINOLOGIES
Abnormal Uterine Bleeding – excessive and prolonged menstruation.
Endometriosis – ectopic growth and function of endometrial tissue.
Fibroids – a fibroma or myoma particularly of the uterus
Fibroma – a benign neoplasm consisting largely of fibrous or fully developed
connective tissue.
Menometrorrhagia - excessive menstrual and uterine bleeding other than that caused
by the menstruation.
Menorrhagia - abnormally heavy or long menstrual periods. Menorrhagia occurs
occasionally during the reproductive years of most women’s lives.
Metrorrhagia – uterine bleeding other than that caused by menstruation. It may be
caused by uterine lesions and may be a sign of uro-genital malignancy.
Myoma – a common benign fibroid tumor of uterine muscle.
11
Polyps – small, tumor like growth that projects from a mucous membrane surface.
Proliferation – the reproduction or multiplication of similar forms.
Retroverted uterus- titled or tipped backwards.
Snellen’s Chart - an eye chart used by eye care professionals and others to measure
visual acuity. It is printed with eleven lines of block letters. The first line consists of one
very large letter, which may be one of several letters, for example E,H or N. subsequent
rows have increasing numbers of letters that decrease in size.
Snellen’s Test – a test wherein a person covers one eye and reads aloud the letters of
each row beginning at the top. The smallest row that can be read accurately indicates
the visual acuity in that eye.
Withdrawal bleeding – the passage of blood from the uterus, associated with the
shedding of endometrium that has been stimulated and maintained by hormones.
Weber’s Test – a test for differentiating conductive hearing impairment from
sensorineural hearing impairment. A vibrating tuning for is applied to one of several
points in the middling of the forehead; if the sound is heard better in the impaired ear,
the middle-ear apparatus is at fault; if the sound is heard better in the normal ear, the
hearing impairment is caused by diseased sensorineural apparatus.
12

ANATOMY AND PHYSIOLOGY
Vagina:
The vagina is a fibro muscular tubular tract leading from the uterus to the
exterior of the body in female mammals. The vagina is the place where semen from the
male is deposited into the female's body at the climax of sexual intercourse, commonly
known as ejaculation.
13

Cervix:
The cervix is the lower, narrow portion of the uterus where it joins with the
top end of the vagina. It is cylindrical or conical in shape and protrudes through the
upper anterior vaginal wall. Approximately half its length is visible, the remainder lies
above the vagina beyond view. The vagina has a thick layer outside and it is the
opening where baby comes out during delivery. The cervix is also called the neck of the
uterus.
Endometrium
Is the inner membrane of the mammalian uterus. The endometrium
functions as a lining for the uterus, preventing adhesions between the opposed walls of
the myometrium, thereby maintaining the patency of the uterine cavity. During the
menstrual cycle or estrous cycle, the endometrium grows to a thick, blood vessel-rich,
glandular tissue layer. This represents an optimal environment for the implantation of a
blastocyst upon its arrival in the uterus. The endometrium is central, echogenic
(detectable using ultrasound scanners), and has an average thickness of 6.7mm.During
pregnancy, the glands and blood vessels in the endometrium further increase in size
and number. Vascular spaces fuse and become interconnected, forming the placenta,
which supplies oxygen and nutrition to the embryo and fetus.
Ovary
Is an ovum-producing reproductive organ, often found in pairs as part of
the vertebrate female reproductive system. Ovaries in females are homologous to
testes in males, in that they are both gonads and endocrine glands. Ovaries are oval
shaped and, in the human, measure approximately 3 cm x 1.5 cm x 1.5 cm (about the
size of a Greek olive). The ovary (for a given side) is located in the lateral wall of the
pelvis in a region called the ovarian fossa. The fossa usually lies beneath the external
iliac artery and in front of the ureter and the internal iliac artery.
14
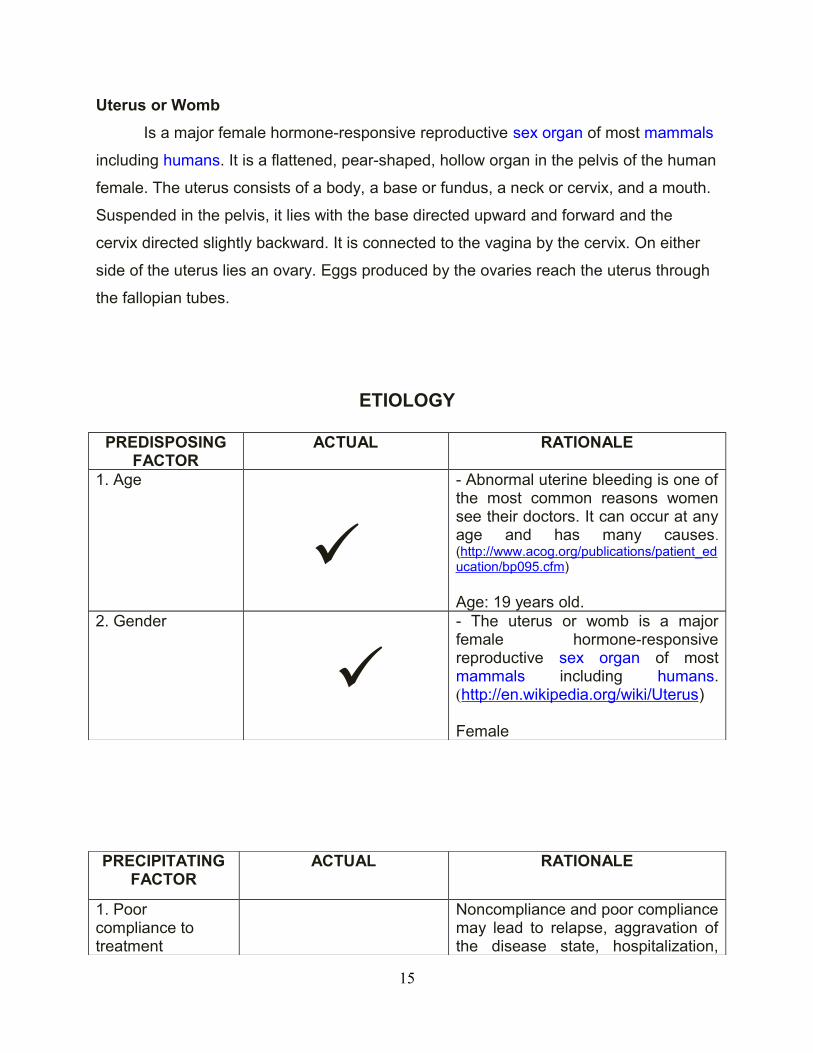
Uterus or Womb
Is a major female hormone-responsive reproductive sex organ of most mammals
including humans. It is a flattened, pear-shaped, hollow organ in the pelvis of the human
female. The uterus consists of a body, a base or fundus, a neck or cervix, and a mouth.
Suspended in the pelvis, it lies with the base directed upward and forward and the
cervix directed slightly backward. It is connected to the vagina by the cervix. On either
side of the uterus lies an ovary. Eggs produced by the ovaries reach the uterus through
the fallopian tubes.
ETIOLOGY
PREDISPOSING FACTOR
ACTUAL RATIONALE
1. Age
- Abnormal uterine bleeding is one of the most common reasons women see their doctors. It can occur at any age and has many causes. (http://www.acog.org/publications/patient_education/bp095.cfm)
Age: 19 years old.2. Gender
- The uterus or womb is a major female hormone-responsive reproductive sex organ of most mammals including humans. (http://en.wikipedia.org/wiki/Uterus)
Female
PRECIPITATING FACTOR
ACTUAL RATIONALE
1. Poor compliance to treatment
Noncompliance and poor compliance may lead to relapse, aggravation of the disease state, hospitalization,
15

escalating health care costs, and even death.(http://www.pharmacytimes.com/issue/pharmacy/2003/2003-07/2003-07-7310)
Complying only for 1 month and stopping thereafter.
SYMPTOMATOLOGY
SYMPTOMS ACTUAL RATIONALE1. More than 4 to 6 days of menstruation.
Causes may be due to disruption of normal hormonal regulation of periods or disorders of the endometrial lining of the uterus.(http://en.wikipedia.org/wiki/Menorrhagia)
She experiences 15 days of menstruation.
2.Blood loss of greater than 80 ml.
Without subsequent progesterone secretion, estrogen secretion continues and causes extreme proliferation in the endometrium. (Maternal and Child health Nursing, Volume 2, 4th edition , Pillitteri)
Easily soaks 4 to 6 sanitary napkins a day. ( 1 sanitary napkin is equal to 25 ml)
3.Anemia
> Dizziness > Pallor
Bleeding causes loss of blood. This causes an abnormally low number of red blood cells which causes anemia. Red blood cells, also called erythrocytes, contain hemoglobin, a red, iron-rich protein that carries oxygen in the blood to the body’s tissues. These symptoms include pale skin, shortness of breath, rapid heartbeat, low
16

vitality, dizziness, and, if left untreated, stroke or heart failure. (Microsoft ® Encarta ® 2008. © 1993-2007 Microsoft Corporation.)
Client has pale conjunctiva and nail beds. She experiences dizziness
17
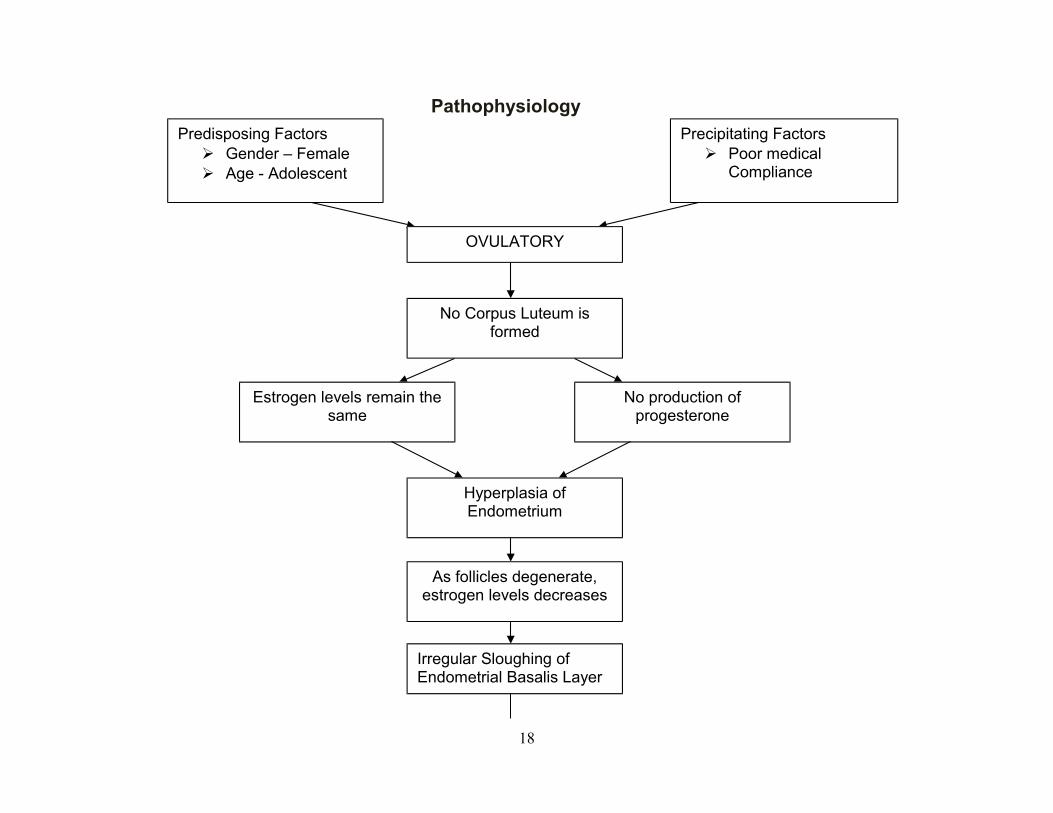
Pathophysiology
18
Predisposing Factors Gender – Female Age - Adolescent
Precipitating Factors Poor medical
Compliance
OVULATORY
Irregular Sloughing of Endometrial Basalis Layer
No Corpus Luteum is formed
Estrogen levels remain the same
No production of progesterone
Hyperplasia of Endometrium
As follicles degenerate, estrogen levels decreases

NURSING CARE PLANS
19
Heavy Prolonged Bleeding (Duration of 15 days Menstruation
and soaking 4-6 Pads per day).AnemiaDecreased Serum
Hemoglobin(Hgb Lab. Result 102)
Abnormal Uterine Bleeding
Decreased O2 Carrying Capacity of Blood
(Dizziness)Dizziness and Pallor
If not treated
Complications
Death
If treated:
Back to normal Homeostasis
Meds. ALTHEA 1 Tab.
O.D X3 months
FeSO4 Tab. 200 mg BID
Prognosis Good

Date: July 26, 2010
Assessment Needs Diagnosis Goal Intervention Rationale Expected/Outcome
Subjective Cues: > “Gagawas pirmi akoang dugo. Gamens ko ug 15 days” as verbalized.
Objective Cues:> Pallor of conjunctiva and nail beds.>Consumes 4-6 sanitary napkin per day> Menstruation lasting for 15 days
PHYSIOLOGICNEEDS
To facilitate in the
maintenance of fluid and
electrolyte imbalance.
According to: Abraham Maslow’s Hierarchy of Needs
>Risk for Fluid Volume Deficit R/T Uterine Bleeding
Scientific Basis: Blood is composed of blood cells suspended in a liquid called blood plasma. Plasma, which constitutes 55% of blood fluid, is mostly water (90% by volume) (http://www.wikipedia. org)
After 8 hours of nursing care, patient will be able to maintain fluid volume within functional level as evidenced:
a. cessation of bleeding
b. V/S within normal range
c. Good skin turgor and moist mucous membrane.
Independent
1. Monitored Vital Signs for changes
2. Counted number of pads consumed to monitor actual fluid loss.
3. Encouraged increase oral fluid intake
4. Promoted high water content fruits.
Dependent
1. IVF PNSS 1L @ 80cc/hr
2. Tranexamic Acid 500mg QID as ordered by physician
>Indirect indicators of fluid status.
>Serves as baseline data
> To provide volume to volume replacement
> To replacefluid lost.
> Fluid replacement.
>It stops bleeding.
>Goal met.
After 8 hours of nursing care, patient was able to: Show good fluid volume status as evidenced by
a) Minimal bleeding
b) Vital Signs within normal range
c) Lips and mucous membranes are moist with good skin turgor.
Date: July 26, 2010
20
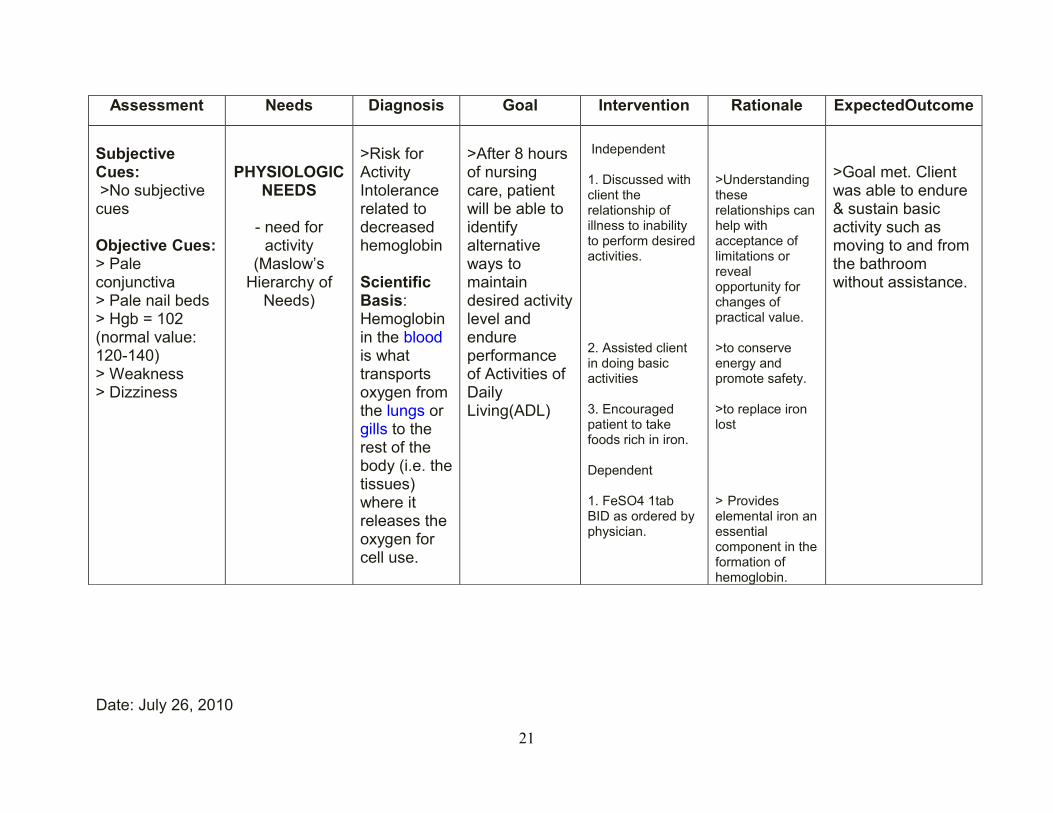
Assessment Needs Diagnosis Goal Intervention Rationale ExpectedOutcome
Subjective Cues: >No subjective cues
Objective Cues:> Pale conjunctiva> Pale nail beds> Hgb = 102(normal value: 120-140)> Weakness> Dizziness
PHYSIOLOGIC NEEDS
- need for activity
(Maslow’s Hierarchy of
Needs)
>Risk for Activity Intolerance related to decreased hemoglobin
Scientific Basis: Hemoglobin in the blood is what transports oxygen from the lungs or gills to the rest of the body (i.e. the tissues) where it releases the oxygen for cell use.
>After 8 hours of nursing care, patient will be able to identify alternative ways to maintain desired activity level and endure performance of Activities of Daily Living(ADL)
Independent
1. Discussed with client the relationship of illness to inability to perform desired activities.
2. Assisted client in doing basic activities
3. Encouraged patient to take foods rich in iron.
Dependent
1. FeSO4 1tab BID as ordered by physician.
>Understanding these relationships can help with acceptance of limitations or reveal opportunity for changes of practical value.
>to conserve energy and promote safety.
>to replace iron lost
> Provides elemental iron an essential component in the formation of hemoglobin.
>Goal met. Client was able to endure & sustain basic activity such as moving to and from the bathroom without assistance.
Date: July 26, 2010
21

Assessment Needs Diagnosis Goal Intervention Rationale Expected Outcome
Subjective Cues:> “Wala pa koy ligo” client verbalized
Objective Cues:> dirty nail noted> unfixed hair noted.
PHYSIOLOGIC NEEDS
- need to keep body clean and well groomed
and protect the integument (Maslow’s
Hierarchy of Needs)
>Self-care deficit: bathing/ hygiene related to decreased motivation.
Scientific Basis: Motivation is the psychological feature that arouses an organism to action toward a desired goal.(http://www.thefreedictionary.com/motivation)
.After 8 hours of nursing care, patient will be able to:Perform proper hygiene
Independent
1. Monitored vital signs.
2. Performed cleansing bed bath to patient.
3.Encouraged patient to take a bath explain the possible risks for infection.
4. Encouraged patient to do oral care.
5. Trimmed patients nails.
> Serves as baseline data.
> To promote comfort and reduce risk for infection.> To denote importance of proper hygiene.
> To promote taste and decrease bacteria.
> To prevent microorganism from staying under nails.
>Goal met.
After 8 hours of nursing care, patient was able to perform proper hygiene and good grooming.
Date: July 27, 2010
22
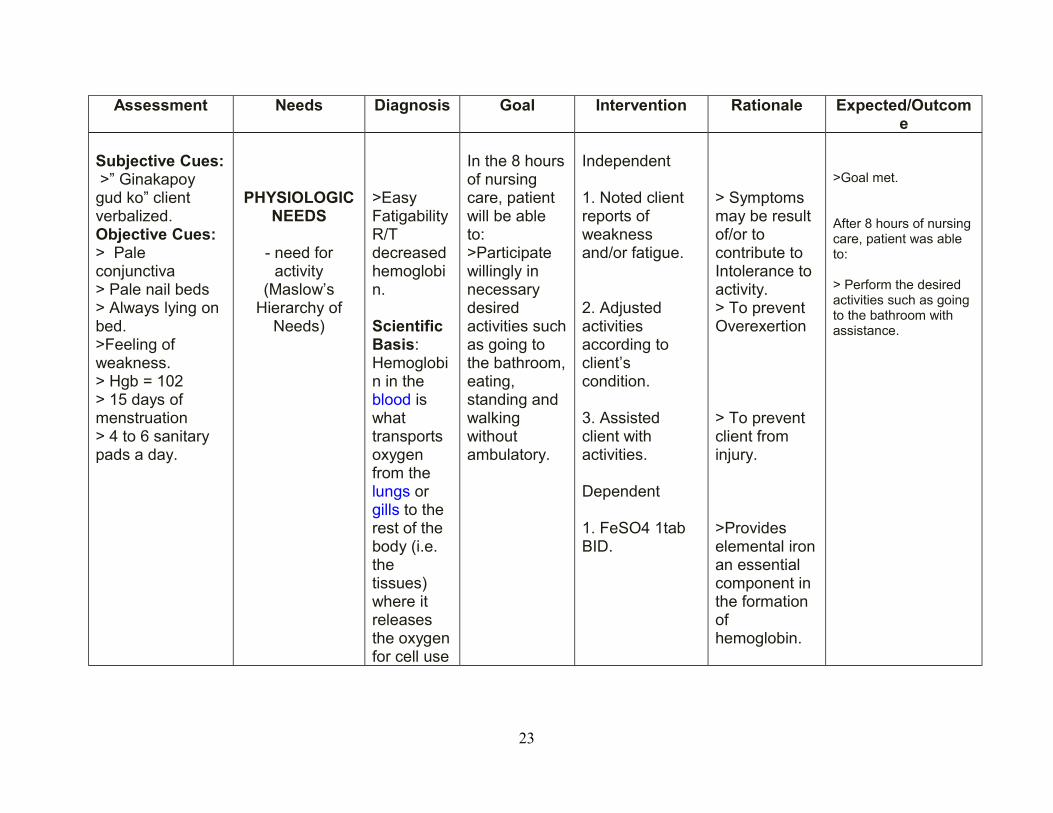
Assessment Needs Diagnosis Goal Intervention Rationale Expected/Outcome
Subjective Cues: >” Ginakapoy gud ko” client verbalized.Objective Cues:> Pale conjunctiva> Pale nail beds> Always lying on bed.>Feeling of weakness.> Hgb = 102> 15 days of menstruation> 4 to 6 sanitary pads a day.
PHYSIOLOGIC NEEDS
- need for activity
(Maslow’s Hierarchy of
Needs)
>Easy Fatigability R/T decreased hemoglobin.
Scientific Basis: Hemoglobin in the blood is what transports oxygen from the lungs or gills to the rest of the body (i.e. the tissues) where it releases the oxygen for cell use
In the 8 hours of nursing care, patient will be able to:>Participate willingly in necessary desired activities such as going to the bathroom, eating, standing and walking without ambulatory.
Independent
1. Noted client reports of weakness and/or fatigue.
2. Adjusted activities according to client’s condition.
3. Assisted client with activities.
Dependent
1. FeSO4 1tab BID.
> Symptoms may be result of/or to contribute to Intolerance to activity.> To prevent Overexertion
> To prevent client from injury.
>Provides elemental iron an essential component in the formation of hemoglobin.
>Goal met.
After 8 hours of nursing care, patient was able to:
> Perform the desired activities such as going to the bathroom with assistance.
23

LABORATORY RESULTS
Diagnostic Test
Purpose Result Interpretation Nursing Implication
Complete Blood CountDate: July 25, 2010
Complete Blood Count: General survey of bone marrow functions and evaluates all three cell lines (WBCs, RBCs, platelets)White Blood Cells (WBC): total WBC countHemoglobin: (Hgb): delivers O2 through circulation to body tissues and returns CO2 from tissues to lungsHematocrit (Hct): indicates relative proportions of plasma and RBCs ( volume of RBCs/L whole blood)Platelet: total number of platelets in circulationLymphocytes: integral component of immune systemSegmenters:Monocytes:
Test Result Normal ValuesThe Hemoglobin levels are below the normal range.
The Hematocrit levels are below than the normal levels.
Below than normal levels of Hemoglobin are found in iron-deficiency anemia (Fischbach, 1988).Below than the normal of hematocrit are found in Acute, massive blood loss. (Fischbach, 1988).
WBCHgbHctPlt.ctLymphoSegsMono
9.4 (10 e g/L)1020.353020.300.660.04
5 – 10120-1400.37-0.43
150-350 x10 g/L0.25-0.350.55-0.650.03-0.06
24
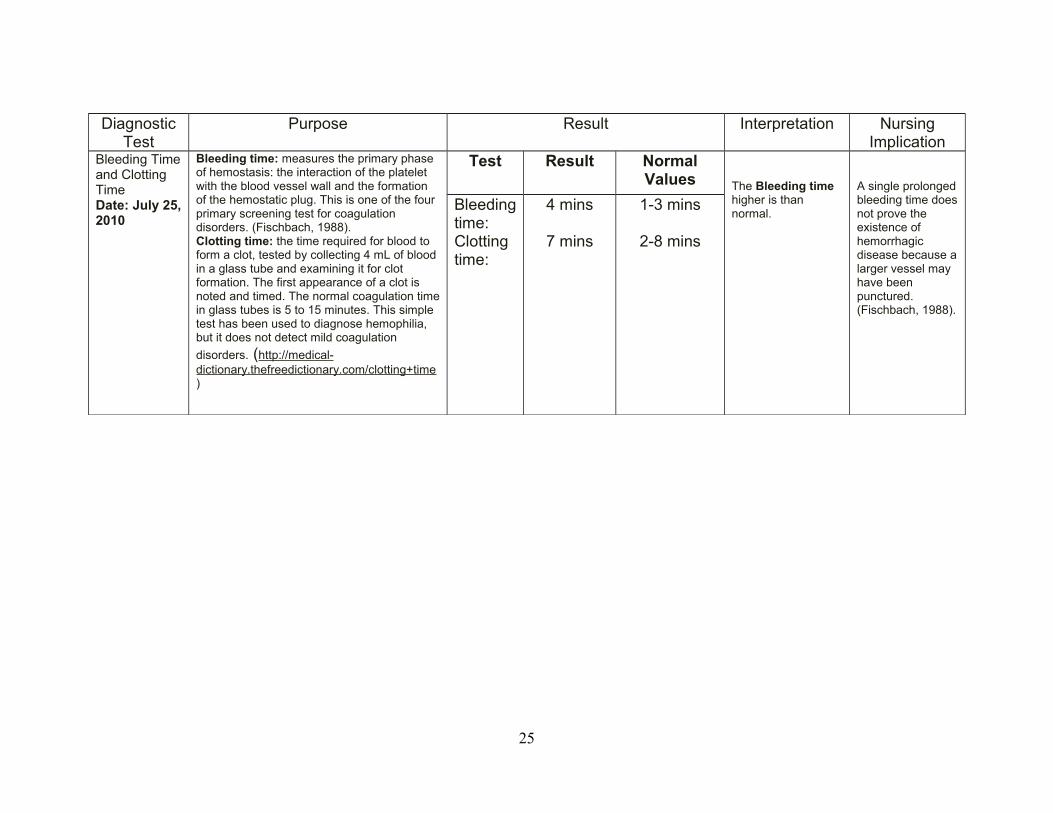
Diagnostic Test
Purpose Result Interpretation Nursing Implication
Bleeding Time and Clotting TimeDate: July 25, 2010
Bleeding time: measures the primary phase of hemostasis: the interaction of the platelet with the blood vessel wall and the formation of the hemostatic plug. This is one of the four primary screening test for coagulation disorders. (Fischbach, 1988).Clotting time: the time required for blood to form a clot, tested by collecting 4 mL of blood in a glass tube and examining it for clot formation. The first appearance of a clot is noted and timed. The normal coagulation time in glass tubes is 5 to 15 minutes. This simple test has been used to diagnose hemophilia, but it does not detect mild coagulation
disorders. (http://medical-dictionary.thefreedictionary.com/clotting+time)
Test Result Normal Values The Bleeding time
higher is than normal.
A single prolonged bleeding time does not prove the existence of hemorrhagic disease because a larger vessel may have been punctured. (Fischbach, 1988).
Bleeding time: Clotting time:
4 mins
7 mins
1-3 mins
2-8 mins
25

Diagnostic Test
Purpose Result Interpretation Nursing Implication
UrinalysisDate: July 25, 2010
Urinalysis: The urinalysis is used as a screening and/or diagnostic tool because it can help detect substances or cellular material in the urine associated with different metabolic and kidney disorders. It is used to detect urinary tract infections (UTI) and other disorders of the urinary tract. (http://www.labtestsonline.org/understanding/analytes/urinalysis/test.html)
Physical ExaminationColor: Yellow
Transparency: Cloudy
Yellow is the normal color of urine. Glucose is normally not present in urine.Normal Urine can be clear or cloudy.
The protein test pad measures the amount of albumin in the urine. Normally, there will not be detectable quantities.The ph reaction of the urine is alkaline.Specific gravity is normal.Pus cells are within normal range.
HCG is not found in urine.
"Normal" urine can be clear or cloudy. Albumin is smaller than most other proteins and is typically the first protein that is seen in the urine when kidney dysfunction begins to develop. A vegetarian diet, a low-carbohydrate diet, or the ingestion of citrus fruits will tend to make the urine more alkaline. (http://www.labtestsonline.org/understanding/analytes/urinalysis/ui_exams.html)Normal urine ranges from 1.010 to 1.025.(Kozier & Erb’s, 2007)Normal value for pus cells in urine is 0-5/hpf(http://www.medhelp.org/posts/Urology/Urinalysis-interpretation/show/731397)The girl is not pregnant. The human chorionic gonadotropin (hCG) test is done to check for the hormone hCG in blood or urine. Some hCG tests measure the exact amount and some just check to see if the hormone is present. HCG is made by the placenta during pregnancy. The hCG test can be used to see if a woman is pregnant or as part of a
Chemical ExaminationAlbumin: Trace pH reaction: 5.0Sugar: Negative Specific Gravity: 1.020
Microscopic findingsPus cells: 1-3/hpf Red Blood Cells: Packed
SerologyUrine HCG - Negative
26

Pelvic UltrasoundDate: July 26, 2010
Ultrasonography is an ultrasound-based diagnostic imaging technique used to visualize subcutaneous body structures including tendons, muscles, joints, vessels and internal organs for possible pathology or lesions. Obstetric sonography is commonly used during pregnancy and is widely recognized by the public. (http://en.wikipedia.org/wiki/Medical_ultrasonography)
The uterus is retroverted. It measures
4.2x3.6x3.9 cm and is normal in size for
nullipara. No myoma or adenomyosis is
noted. Endometrial stripe hyperechoic
measuring 0.6 cm. adnexae are free.
Minimal pelvic fluid is seen.
Impression: Normal studies save for
minimal pelvic fluid.
Retroversion of the uterus is not normal
screening test for birth defects. (http://www.nlm.nih.gov/medlineplus/ency/article/003619.htm)
A retroverted uterus is usually diagnosed during a routine pelvic examination.
Lower back pains
It usually does not pose any medical problems, though it can be associated with dyspareunia (pain during sexual intercourse) and dysmenorrhea (pain during menstruation). (http://en.wikipedia.org/wiki/Retroverted_uterus)
27

DRUG STUDIES
Name Dosage and Indication
Mechanism of Action
Adverse Effects Contraindication Nursing Responsibilities
Generic Name: Ferrous Sulfate
Brand Name:Magniferron
Classification:Hematologic Drugs: Hematinics
Iron Deficiency 200 mg
P.O BID
Provides elemental iron an essential
component in the formation of
hemoglobin.
GI: Nausea, epigastric pain, vomiting, constipation, black stools, diarrhea, anorexia.Other: temporarily stained teeth in liquid forms
Contraindicated in patients with Hemosiderosis, primary hemochromatosis, hemolytic anemia (unless patient also has iron deficiency anemia), Peptic ulceration, ulcerative colitis or regional enteritis and in those receiving repeated blood transfusions.Use cautiously on long term basis.
1. Identify the client correctly using the appropriate means of identification, such as checking the identification bracelet or asking the clients name.2. If the client is unfamiliar with the medication, the nurse should explain the intended action as well as any side effects or adverse effects that may occur.3. Administer drug in the prescribed dosage by the route intended and the correct time.4. Record the medication given, dosage, time, any complaints or assessments and your signature.5. Explain to the client that she may have black stool as effect of the drug.6. Administer the drug with juice for faster absorption.
28

Name Dosage and Indication
Mechanism of Action
Adverse Effects Contraindication Nursing Responsibilities
Generic Name:Tranexamic AcidBrand Name:Hemostan Classification:Hematologic Drugs: Hematinics amino acid antifibrinolytics.
Indicated for short term use for hemorrhage or risk of hemorrhage in those with increased fibrinolysis or fibrinogenolysis. Local fibrinolysis as occurs in menorrhagia.
1tab 500mg QID
Tranexamic acid competitively inhibits activation of plasminogen (via binding to the kringle domain), thereby reducing conversion of plasminogen to plasmin (fibrinolysin), an enzyme that degrades fibrin clots, fibrinogen, and other plasma proteins, including the procoagulant factors V and VIII.
GI: nausea, vomiting, diarrhea may occur but disappear when the dosage is reduced.
In patients with acquired defective color vision, since this prohibits measuring one endpoint that should be followed as a measure of toxicity.In patients with active intravascular clotting.
1. Identify the client correctly using the appropriate means of identification, such as checking the identification bracelet or asking the clients name.2. If the client is unfamiliar with the medication, the nurse should explain the intended action as well as any side effects or adverse effects that may occur.3. Administer drug in the prescribed dosage by the route intended and the correct time.4. Record the medication given, dosage, time, any complaints or assessments and your signature.5. Check for presence of spontaneous bleeding.
29
Tranexamic acid also directly inhibits plasmin activity, but higher doses are required than are needed to reduce plasmin formation.
30

Name Dosage and Indication
Mechanism of Action Adverse Effects
Contraindication Nursing Responsibilities
Generic Name:Cyproterone acetateBrand Name:Althea Classification:Natural and semisynthetic estrogens.
OC, control of acne & hsirsutism, regulation of menstrual cycle, reduction of premenstrual tension, relief from pain & excess bleeding during menstruation.
Take 1 tab starting on the 1st day of menses & throughout the cycle.
Oral contraceptive.
Althea is a combined low-dose oral contraceptive pill with antiandrogenic properties. Each tablet contains cyproterone acetate, a progesterone with antiandrogenic and progestogenic properties and ethinyl estradiol, an estrogen.
Oral Contraceptive: Althea stops ovulation, thins the lining of the uterus and thickens the cervical mucus. In combination, these actions prevent pregnancy.
Antiandrogen: Althea contains cyproterone acetate that works as an antiandrogen. It competes at the receptor sites with androgens and reduces their effects. Cyproterone acetate
GI: Nausea, vomiting, chloasma (melasma) & other skin or hair changes, headache, water retention, slight wt change, breast tenderness, changes in libido. Menstrual irregularities eg spotting, breakthrough bleeding & amenorrhea.
Impaired liver function or cholestasis, Dubin-Johnson or Rotor syndromes, hepatic adenoma, estrogen-dependent neoplasms eg breast or endometrial cancer, CV disease, disorders of lipid metabolism, undiagnosed vag bleeding, pregnancy, history of pruritus or cholestatic jaundice during pregnancy, chorea, herpes gestationis, pemphigoid gestationis, deteriorating otosclerosis, severe or focal migraine, lactation.
1. Identify the client correctly using the appropriate means of identification, such as checking the identification bracelet or asking the clients name.2. if the client is unfamiliar with the medication, the nurse should explain the intended action as well as any side effects or adverse effects that may occur.3. Administer drug in the prescribed dosage by the route intended and the correct time.4. Record the medication given, dosage, time, any complaints or assessments and your signature.5. Report any signs of headache.
31
inhibits the influence of the androgens produced in women. Althea reduces the development of acne and seborrhea. It heals existing acne efflorescence after 3-4 months therapy. It also reduces the greasiness of the hair and skin.
32

Name Dosage and Indication
Mechanism of Action Adverse Effects
Contraindication Nursing Responsibilities
Generic name:Ketorolac tromethamine
Brand name:Toradol
Classification:Central nerovous system drugs; Nonsteroidal anti-inflammatoy drugs
Short-term management of moderately severe, acute pain
-30mg IV TT
Unknown. May inhibit prostaglandin synthesis, to produce anti-inflammatory, analgesic, and antipyretic effects.
GI: Nausea, dyspepsia, GI pain, diarrhea, peptic ulceration, vomiting, constipation, flatulence, stomatitis.
Contraindicated in patients hypersensitivity to drug and in those with active peptic ulcer disease, recent GI bleeding or perforation, advanced renal impairement, cerebrovascular bleeding, hemorrhagic diathesis, or incomplete hemostasis and those at risk for renal impairment from volume depletion or at risk of bleeding.
1.identify the client correctly using the appropriate means of identification, such as checking the identification bracelet or asking the client’s name
2.If the client is unfamiliar with the medication, the nurse should explain the intended action as well as any side effect or adverse effects that may occur.
3.Check IV patency and observe for complication of Iv therapy such as infiltration and extravasation phlebitis, thrombophlebitis, hematoma, and clotting of the needle.
4.Administer drug in the prescribed dosage by the route intended and the correct time.
33

5.Administer the medication slowly
6.Record the medication given, dosage, time, any complaints or assessment and your signature.
34

COURSE IN THE WARD
Progress notes Doctor’s order
July 25, 2010 - admit under the service of Dr. Ureta- DAT
- V/S Q4 h- Labs: CBC, PLT Count, HCT, Urinalysis, Pregnancy Test
Soaking 1 – 4 napkin/ day for CT, BTFor pelvic ultrasound in AM- IVF: PNSS at 100 cc/hr
- IVF TF: PNSS in at 80 cc/hr
- Meds: Tranexamic acid 500 mg IM – now
Tranexamic acid 500 mg 1 cap, QID, to start in AM FeSO4 1 cap BID
- AP aware
- Refer accordingly
July 25, 2010 Continue Meds8:30 Vaginal bleed Pelvic Ultrasound @ AM tomorrow (07/26/10)
July 25, 201010:10PM IVF TF: PNSS 1L @ 80 cc/hr
July 26, 20106:00AM IVF TF: PNSS 1L @ 80 cc/hr
35
12:30PM(+) for hypogastric pain May give Ketorolac 30mg IV TT now7:20PM Althea 1 tab once and P.O 8 AM10:00PM PNSS 1L @80 cc/hr
July 27, 2010 7:00 AM IVF: PNSS 1L @ 80 cc/hr12:00 PM IVF: PNSS 1L @ 80 cc/hr4:00 PM MGH
Meds:• Tranexamic acid 50 g
3x a day (1 week) (8am– 11am – 7pm)
• Althea 1 tab once a day at 8 AM
Follow up. Aug. 4, 2010 at 2 PM, clinic
• Magniferron 1 cap, OD at 7 PM
Advised:
Bed Rest
No work load
36
PROGNOSIS
FACTORS PROGNOSIS JUSTIFICATION
Medication Regimen Good The client is able to follow the treatment regimen that was
given by the attending physician.
Activity Good The client is able to comply with the advise of bed rest &
no work load.
GENERAL PROGNOSIS:
Patient general prognosis is good since the disease of the patient could be managed through different varied
treatments with the help of her family. She has knowledge of what is medication is she taking & what it is for. She follows
religiously the attending physician’s prescribed treatments and takes willingly the doctor’s prescription medication. The
case of her abnormal uterine bleeding is easier to treat than any other cases of abnormal uterine bleeding.
37

HEALTH TEACHINGS
1) Advised to take medicines religiously as prescribed by the doctor
2) Instructed to avoid strenuous activities such as heavy lifting for it may aggravate
vaginal bleeding
3) Advised to increase foods rich in iron
4) Instruct client to comply with the physicians advice for follow-up check-up
NURSING IMPLICATIONS
A. NURSING EDUCATION
It helps the nursing profession gain more information regarding different
symptoms, different causes, different etiologies and different treatments and nursing
actions related to this case and to impart this information to the younger batches of
nursing students of Notre Dame of Kidapawan College.
It also helps the nursing profession to be aware of the different terminologies
used so that it would be imparted to the future incoming nursing students. It also helps
the nursing students of Notre Dame of Kidapawan College to be more knowledgeable in
dealing with patients who have abnormal uterine bleeding.
B. NURSING PRACTICE
It helps the nursing profession to be more aware in dealing with this kind of cases
in different fields and hospitals.
It also helps the nursing students of Notre Dame of Kidapawan College to be
more skillful in doing the different nursing actions to the patients in different hospitals, to
have safe and quality nursing care that the patient needs.
It also helps the nursing profession to prevent any clinical errors that can harm
the patient and may result to mal-practice or globally known as negligence.
38

C. NURSING RESEARCH
It helps the nursing profession to gain more knowledge regarding this case and
to impart this data to the incoming researchers who may need the said information.
It also helps the researchers to gather more reference to strengthen the validity
of the different information of the said case. It also helps to make the gathered
information to be more truthful in terms and learning that may found in the papers.
39

BIBLIOGRAPHY
A. Books
Andreasen, Charlotte and Aris Jr. Andrews. Et al. © 2006. Mosbys’s Pocket dictionary
of Medicine, Nursing and Health Professions 5th Edition. Elsevier Pte. Ltd.
Singapore.
Berman, Audrey and Shirlee Synder. © 2008. Kozier and Erb’s Fundamentals of
Nursing 8th Edition. Pearson Education Inc. Jurong, Singapore.
Bullock, Barbara and Henze, Reet. © 2000. Focus on Pathophysiology. Lippincot
Williams and Wilkins. Philadelphia.
Doenges, Marilyn E. and Mary Frances Moorhouse, et al. © 2008. Nurse’s Pocket
Guide Diagnosis, Prioritized interventions and Rationales. L.A. Davis Company,
Philadelphia. Thomson Learning Asia. Singapore.
Fischbach, Frances. © 1988. A manual of Laboratory diagnostic Tests 3 rd Edition. J. B.
Lippincot Company. Philadelphia.
McCann, Judith A. and H. Nancy Holmes. et al. © 2008. The Nursing 2008 Drug
Handbook. Lippincot Williams and Wilkins. Philadelphia.
McCann, Judith Schilling. © 2007. Assessment. Lippincot Williams and Wilkins.
Philadelphia.
Pilliteri, Adele. © 2003. Maternal and Child Health Nursing. 4 th Edition. Lippincot
Williams and Wilkins. Philadelphia.
B. Internet
http://findarticles.com/p/articles/mi_m0689/is_3_58/ai_n31438489/
http://emedicine.medscape.com/article/795587-overview
http://www.acog.org/publications/patient_education/bp095.cfm
http://www.uptodate.com/patients/content/topic.do?topicKey=~.p55Sh88wWX6eG
http://familydoctor.org/online/famdocen/home/women/reproductive/menstrual/470.html
http://www.gynalternatives.com/abnormal_uterine_bleeding.htm
40

http://www.medicines.org.uk/emc/medicine/21712/SPC/tranexamic%20acid%20500mg
%20tablets%20(sandoz%20limited)/
http://www.nativeremedies.com/ailment/symptoms-of-hormone-imbalance.html
http://www.medicine.uic.edu/UserFiles/Servers/Server_442934/File/OBGYN%20Med
%20Ed/STUDENTS/Lectures/ELAM%20-%20AUB%20talk.pdf
http://www.medicine.uic.edu/UserFiles/Servers/Server_442934/File/OBGYN%20Med
%20Ed/STUDENTS/Lectures/ELAM%20-%20AUB%20talk.pdf
http://members.aapa.org/aapaconf2006/syllabus/6253TaylorDUB.pdfc
41