2017 enrollment benefits roadmap · benefits eligibility ... financial dependency, ... the...
TRANSCRIPT


This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
2
TABLE OF CONTENTS
Contact Information ................................................................................................. 3
Benefits Eligibility Overview .................................................................................... 4
Dependent Eligibility ................................................................................................ 5
Health Care Benefits Overview ............................................................................... 6
Health Savings Account (HSA) Overview ............................................................... 7
Teledoc Overview .................................................................................................... 8
Hylant Script Navigator Online Tool Overview ........................................................ 9
Choosing the Right Plan for You ........................................................................... 10
Dental Benefits Overview ...................................................................................... 11
Vision Benefits Overview ...................................................................................... 12
Employee Contributions (Payroll Deductions) ...................................................... 13
Life and AD&D Insurance Overview...................................................................... 14
Disability Overview ................................................................................................ 15
Flexible Spending Accounts (FSA) Overview ....................................................... 16
Healthcare FSA Overview ..................................................................................... 17
Dependent Care FSA Overview ............................................................................ 18
Employee Assistance Program ............................................................................. 19

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing
documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern. 3
CONTACT INFORMATION
CONTACT INFORMATION
General Claims and Benefit Information
Health Care CoreSource (800) 521-1555 www.coresource.com www.mycigna.com
Prescription Drug EHIM (800) 311-3446 www.ehimrx.com
Health Savings
Account
BenefitWallet HSA (through Bank of New
York Mellon) (877) 472-4200 www.mybenefitwallet.com
Telemedicine TelaDoc (800) 362-2667 www.teladoc.com
Dental Delta Dental of Michigan (800) 524-0149 www.deltadentalmi.com www.consumertoolkit.com
Vision EyeMed (866) 939-3633 www.eyemedvisioncare.com
Life/AD&D Lincoln Financial Group (800) 423-2764 www.LincolnFinancial.com
Reference ID: EDUDATASYS
Disability Lincoln Financial Group (800) 423-2764 www.LincolnFinancial.com
Reference ID: EDUDATASYS
Flexible Spending
Account Infinisource (866) 370-3040 www.infinisource.com
Employee Assistance
Program
EmployeeConnectSM (through Lincoln
Financial Group)
(888) 628-4824 www.Lincoln4Benefits.com or
www.Guidanceresources.com
Login:
Password: LFGsupport LFGSupport1
Travel Assistance
Program
TravelConnectSM (through Lincoln
Financial Group)
(800) 527-0218 www.Lincoln4Benefits.com
Global ID#: 322541
General information
and Life status
changes
Human Resources
Katie Theisen (313) 271-2660 [email protected]
When contacting any of the companies above, it is important to have the insurance card or ID number(s) of the subscriber for the
coverage you are calling about as well as any appropriate paperwork, such as an explanation of benefits, a denial letter, receipts, etc.

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
4
2017 BENEFITS ELIGIBILITY OVERVIEW
Health and welfare plans
are available to all
employees who work 30
or more hours per week.
Educational Data Systems, Inc. is pleased to offer its
employees an excellent benefits program. These health
and welfare benefits are designed to protect you and
your family while you are an active employee.
Eligibility Health and welfare plans are available to all employees
who work 30 or more hours per week.
Open Enrollment This is the only opportunity you will have to make
changes to your benefit elections. During the Open
Enrollment period you may add, drop or modify
coverage.
Annual Elections It is important that you make your choices carefully,
since changes to those elections can generally only be
made during the annual open enrollment period.
Exceptions will be made for changes in family status
during the year, allowing you to make a midyear benefit
change. A family status change includes one or more of
the following:
Marriage
Divorce
Birth or adoption
Death of a dependent
Change in your spouse’s employment
Loss of coverage by a spouse
If you have a family status change, you must change
your benefit elections within 30 days of the qualifying
event. Otherwise, you will need to wait until the next
annual open enrollment period.
New Hire Coverage As a new hire, your plan eligibility date is the first of the
month following 30 days of employment with Educational
Data Systems, Inc. for Medical, Dental, Vision, Voluntary
Life/AD&D and FSA benefits and 1st of the month
following 60 days of employment for Basic Life/AD&D,
and Disability benefits.
New employees have up to 30 days after their hire date
to enroll. If you do not enroll by that deadline, you will not
be eligible for coverage until the following annual open
enrollment period unless you experience a qualifying
event.
COBRA Continuation Coverage When you or any of your dependents no longer
meet the eligibility requirements for health and
welfare plans, you may be eligible for continued
coverage as required by the Consolidated Omnibus
Budget Reconciliation Act (COBRA)
of 1985.

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing
documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern. 5
DEPENDENT ELIGIBILITY
If you wish, your dependents may also be covered under the medical, dental, vision and voluntary life
plans.
Eligible dependents include:
Legal spouse, as defined by federal law. Employees can only cover a spouse if they do not have other
coverage available (i.e. through their employer); and
Children under age 26; and
MEDICAL – Your children up to age 26 regardless of marital status, financial dependency,
residency with the eligible employee, student status, employment status, or eligibility for
other coverage. Coverage will terminate at the end of the year in which the child turns age
26.
DENTAL – Your children up to age 26 regardless of marital status, financial dependency,
residency with the eligible employee, student status, employment status, or eligibility for
other coverage. Coverage will terminate at the end of the year in which the child turns age
26.
VISION – Your children up to age 26 regardless of marital status, financial dependency,
residency with the eligible employee, student status, employment status, or eligibility for
other coverage. Coverage will terminate at the end of the year in which the child turns age
26.
VOLUNTARY LIFE – Your children up to age 26 regardless of marital status, financial
dependency, residency with the eligible employee, student status, employment status, or
eligibility for other coverage. Coverage will terminate at the end of the year in which the
child turns age 26.
YOUR UNMARRIED CHILDREN THROUGH AGE 20, OR THROUGH AGE 24 IF THEY
ARE FULL-TIME REGISTERED STUDENT THE CHILD TURNS AGE 26. It is your responsibility to provide the Human Resources Department with proof of your dependents’
eligibility, if requested. If you do not provide the required documentation your dependents will not be
covered. A list of acceptable documentation is illustrated below:
Relationship Acceptable Documentation
Spouse Copy of most recent Federal Income Tax Return, Copy of Marriage
Certificate
Child (Biological,
Adopted and Stepchild
under 26)
Copy of most recent Federal Income Tax Return, Copy of Birth/Adoption and
Marriage Certificate (if applicable)

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
6
HEALTH CARE BENEFITS OVERVIEW
HEALTH CARE BENEFITS ARE AMONG THE MOST IMPORTANT AND NECESSARY PARTS OF YOUR
BENEFIT PACKAGE. The following is a summary of your medical benefits offered through CoreSource using the Cigna network. For a more
detailed explanation of benefits, please refer to your certificate of coverage. You may access a list of participating
providers through the carrier’s website (see page 3 of this guide for contact information).
Traditional PPO 500 Traditional PPO 1750 HSA PPO 1500
In
Network
Out of
Network
In
Network
Out of
Network
In
Network
Out of
Network
What you pay What you pay What you pay
DEDUCTIBLES Calendar Year Calendar Year Calendar Year
Individual $500 $1,000 $1,750 $3,500 $1,500 $3,000
Family $1,000 $2,000 $3,500 $7,000 $3,000 $6,000
COINSURANCE
Plan Pays 80% 60% 100% 80% 80% 60%
You Pay 20% 40% 0% 20% 20% 40%
Individual Maximum $500 $4,000 $0 $5,000 N/A N/A
Family Maximum $1,000 $8,000 $0 $10,000 N/A N/A
SERVICES
Preventive Care Services Covered 100% Not covered Covered 100% Not covered Covered 100% Not covered
Primary Care Office Visits $20 copay 40% after ded $30 copay 20% after ded 20% after ded 40% after ded
Specialist Office Visits $20 copay 40% after ded $30 copay 20% after ded 20% after ded 40% after ded
Urgent Care $30 copay 40% after ded $50 copay 20% after ded 20% after ded 40% after ded
Emergency Room $150 copay $150 copay 20% after ded
Labs and X-rays 20% after ded 40% after ded 0% after ded 20% after ded 20% after ded 40% after ded
Hospital Care 20% after ded 40% after ded 0% after ded 20% after ded 20% after ded 40% after ded
Mental Health Treatment 20% after ded 40% after ded 0% after ded 20% after ded 20% after ded 40% after ded
Chiropractic Care $20 copay 40% after ded $30 copay 20% after ded 20% after ded 40% after ded
24 visits per calendar year 24 visits per calendar year 24 visits per calendar year
Telemedicine
TelaDoc Visit $0 $0 $45 copay
PRESCRIPTIONS EHIM Prescription Drug Program
Generic $10 $10 $10 after ded
Preferred $50 $50 $50 after ded
Non-preferred $100 $100 $100 after ded
90 Day Retail or Mail Order 2 times applicable copay 2 times applicable copay 2 times applicable copay after ded
ANNUAL MEDICAL OUT OF POCKET MAXIMUMS (Deductibles, Copays & Coinsurance)
Individual
Medical
Rx
TOTAL
$4,100
$2,500
$6,600
N/A
$4,100
$2,500
$6,600
N/A
Combined
$3,000
N/A
Family
Medical
Rx
TOTAL
$8,200
$5,000
$13,200
N/A
$8,200
$5,000
$13,200
N/A
Combined
$6,000
N/A
LIFETIME MAXIMUM Unlimited Unlimited Unlimited

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing
documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern. 7
HEALTH SAVINGS ACCOUNT (HSA) OVERVIEW
HSAs are tax savings tools. Here are some things you should know:
You must be covered by a high-deductible health
plan to be eligible.
HSAs are portable, meaning you can keep your HSA
even if you change jobs, change medical coverage or
make other life changes. As the owner of the HSA,
you are responsible for annually reporting HSA
contributions and distributions to the IRS as an
attachment to their IRS Form 1040.
An HSA is a tax-exempt savings account established
for the purpose of paying for the individual and/or his
or her spouse and tax dependents. HSAs are
designed to provide eligible individuals with triple
federal tax-free benefits: 1) HSA contributions are
tax-free. 2) Interest and other earnings on HSA
contributions accumulate tax-free. 3) Amounts
distributed from an HSA for qualified medical
expenses are tax-free as well.
You can contribute up to $3,400 / $6,750 (single /
family) for 2017 by payroll deduction or by writing a
check. Your contributions are tax deductible.
You can even make a one-time transfer from your IRA.
Contributions can be made until April 15 of the following
year. Those 55 or over can contribute $1,000 more.
You do not need to submit expenses for
reimbursement; it is up to you to use the money
appropriately. We are all subject to an IRS audit; the
penalty for using ineligible HSA money in 2017 is
20 percent.
You can always find the most up-to-date list of
qualifying expenses online, in Publication 502 on the
IRS website (www.irs.gov). Below are a sampling of
qualifying expenses:
Long-term care (medical expenses &
insurance)
Nursing services
Medical doctors
Physical therapy
Christian Science practitioners
Psychoanalysis
Emergency care
Chiropractic care
Use for treatments not covered by insurance:
Dental care including dentures
Medical equipment
Vision care
Alcoholism or drug addiction treatment
Fertility treatment
Over-the-counter medications (with prescription)
Hearing aids
Trips/travel exclusively for a treatment
What Expenses Do NOT Qualify? The following expenses are just a sampling of
expenses you can’t pay for with your HSA.
(Remember, most over-the-counter medications are
no longer eligible without a prescription.)
Cosmetic surgery
Teeth whitening
Household help or babysitting
Health club dues
Food supplements not prescribed by a
doctor
Hair transplants
Over-the-counter vitamins or diet drinks
Dependent Coverage and Your HSA The company plan allows for employees to elect
coverage for their dependents to age 26; however,
the money in the employee’s HSA account may only
be used for eligible expenses incurred by covered
dependents that meet the IRS definition of a tax
dependent. If you list a dependent on your federal
income tax return, then you can use the money in
your HSA account for the eligible expenses. When an
adult dependent child does not qualify as a tax
dependent, then any HSA distributions for the child
would be taxable and subject to IRS penalty.

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
8
TELADOC OVERVIEW
Your access to Teladoc® allows you to talk to a doctor anytime, no matter where you happen to be. Teladoc gives you 24/7/365 access to a doctor who can resolve many medical conditions through phone or video consults.
GET THE CARE YOU NEED Teladoc doctors can treat many medical conditions, including: • Cold & flu symptoms • Allergies • Bronchitis • Urinary tract infection • Respiratory infection • Sinus problems • And more! MEET OUR DOCTORS
Teladoc is simply a new way to access qualified doctors. All Teladoc doctors: • Are practicing PCPs, pediatricians, and family medicine physicians • Average 15 years experience • Are U.S. board-certified and licensed in your state • Are credentialed every three years, meeting NCQA standards WHEN CAN I USE TELADOC?
Teladoc does not replace your primary care physician. It is a convenient and affordable option for quality care. • When you need care now • If you’re considering the ER or urgent care center for a nonemergency issue • On vacation, on a business trip, or away from home • For short-term prescription Refill
With your consent, Teladoc is happy to provide information about your Teladoc consult to your primary care physician.
Talk to a doctor anytime for Free
Teladoc's U.S. board-certified doctors are available 24/7/365 to resolve many of your medical issues through phone or video consults. Set up your account today so when you need care now, a Teladoc doctor is just a call or click away. SET UP YOUR ACCOUNT It's quick and easy online. Visit the Teladoc website at MyDrConsult.com, click "Set up account" and provide the required information. You can also call Teladoc for assistance over the phone.
REQUEST A CONSULT Once your account is set up, request a consult anytime you need care.
PROVIDE MEDICAL HISTORY Your medical history provides Teladoc doctors with the
information they need to make an accurate diagnosis. Online: Log into MyDrConsult.com and click "My Medical History". Mobile app: Log into your account and complete the "My Health Record" section. Visit Teladoc.com/mobile to download the app. Call Teladoc: Teladoc can help you complete your medical history over the phone

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
9
Hylant Script Navigator Online Tool Overview
The Hylant Script Navigator
(www.hylantscriptnavigator.com) is the ultimate
pharmacy search engine that will help you identify
discounted generic drug programs that are available
at pharmacies throughout the USA. Just log on and
enter the following:
1
Name of the drug
2
Dosage
3
Zip code
Pharmacies nationwide sell select generic
drugs at a discounted rate. You can find the
best deals on your medications by identifying
the pharmacies that offer these programs.
Generic drugs are distributed as the equivalent
to the brand name however you should talk to
your doctor if you have specific questions
about your prescription. Below are just a few of
the current discounts available:
Meijer: a variety of oral antibiotics for
FREE
Kroger: get a 30-day supply for ONLY
$4 and a 90-day supply for $10
Wal-Mart: $4 for a 30-day supply and
$10 for a 90-day supply of some
generic medications
Walgreens: Over 300 generics for
$12.99 for a 90-day supply
To find out more, call your local pharmacy or
visit its website.
Many pharmacies
now offer discount
prescriptions—often
even lower than your
copay.

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
10
CHOOSING THE RIGHT PLAN FOR YOU
Choosing between plans can be confusing. Review the basics of each plan and consider your total
cost – including payroll deductions, predicted copays, and other expenses toward deductibles:
Traditional PPO
500
Traditional PPO
1750
HSA PPO
1500
A) Annual payroll deductions
B) Gross contribution to HSA/FSA
C) Tax savings (25% x B)
D) Net contribution to HSA (B-C)
E) # of office visits at $ (or copays)
F) # of prescriptions at $ (or copays)
G) X-ray and lab, hospital, other
H) Dental, vision, other
I) Out-of-pocket expenses (D+E+F+G+H)
J) Total cost (I-B)+A
Things to Consider Before You Pick a Plan:
1. What does the plan cover?
2. How much does the plan cost?
3. Which doctors and hospitals are in-
network?

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing
documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern. 11
DENTAL BENEFITS OVERVIEW
Dental Coverage – Provided through Delta Dental of Michigan The dental coverage is provided by Delta Dental. With Delta Dental you have access to an extensive network of dentist’s.
With the flexibility of a PPO you have the option of visiting any provider, however, by choosing a network provider you’ll
receive the highest level of benefit and save on out of pocket costs. For a more detailed explanation of benefits, please
refer to your certificate of coverage. You may access a list of participating providers through the carrier’s website (see
page 3 of this guide for contact information).
Delta Dental Low Plan High Plan
You Pay You Pay
PPO Dentist Premier®
Dentist*
Non-Network
Dentist* PPO Dentist
Premier®
Dentist*
Non-Network
Dentist*
Diagnostic & Preventive Services: Covered 100% 10% after
deductible
10% after
deductible Covered 100% Covered 100% Covered 100%
Basic Services: 40% after
deductible
50% after
deductible
50% after
deductible
20% after
deductible
20% after
deductible
20% after
deductible
Major Services: 50% after
deductible
75% after
deductible
75% after
deductible
50% after
deductible
50% after
deductible
50% after
deductible
* When services are received from a Premier or Nonparticipating Dentist, the percentages in these columns indicate the portion of Delta Dental's PPO dentist Schedule (or the Nonparticipating Dentist Fee) that will be paid for those services. This amount may be less than what the dentist charges or Delta Dental approves and you are responsible for that difference.
ANNUAL DEDUCTIBLE Calendar Year Deductible Calendar Year Deductible
Individual / Family
$50 / $150*
($100 / $300 when visiting premier
or non-participating dentists)
$50 / $150*
*Diagnostic & Preventive Services Waived
ANNUAL MAXIMUM BENEFIT
Per Covered Person
$1,000
($750 when visiting premier
or non-participating dentists)
$1,000

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
12
VISION BENEFITS OVERVIEW
Voluntary Vision Coverage – Provided through EyeMed EyeMed’s vision care network consists of private practicing optometrists, ophthalmologists, opticians and optical retailers.
You have the option of visiting any provider. However, by choosing a network provider, you’ll receive the highest level of
benefit and save on out-of-pocket costs. You may access a list of participating providers through the carrier’s website (see
page 3 of this guide for contact information).
EyeMed Insight Network
In Network Out of Network *
Vision Care Services Member’s Cost Reimbursement
Examination
Eye Exams $10 copay Up to $35
Standard Contact Lens Up to $55 N/A
Premium Contact Lens 10% off Retail Price N/A
Standard Plastic Lenses
Single Vision $25 copay Up to $25
Bifocal $25 copay Up to $40
Trifocal $25 copay Up to $60
Standard Progressive Lens $90 copay Up to $40
Lens Options
UV Treatment $15 N/A
Tint (Solid and Gradient) $15 N/A
Standard Plastic Scratch Coating $15 N/A
Standard Polycarbonate $40 N/A
Standard Anti-Reflective Coating $45 N/A
Other add-ins 20% off Retail Price N/A
Frames $0 copay; $120 allowance
20% off balance over $120 Up to $48
Contact
Lenses
Conventional $0 copay; $135 allowance
15% off balance over $135 Up to $95
Disposable $0 copay; $135 allowance
plus balance over $135 Up to $95
Medically Necessary $0 copay Up to $200
Laser Vision Correction 15% off Retail Price, or
5% off promotional price N/A
Additional Pairs Benefits
Members also receive 40% discount off complete
pair of eyeglass purchase and a 20% discount off
non-prescription sunglasses along with 20% off the
remaining balance beyond plan coverage
N/A
Hearing Care 40% off hearing exams and low price guarantee on
discounted hearing aids N/A
Frequency
Examination Once every 12 months
Lenses or Contact Lenses Once every 12 months
Frame Once every 12 months
* Member Reimbursement Out of Network will be the lesser of the listed amount or the member’s actual cost from the out of network provider. In
certain states members may be required to pay the full retail rate and not the negotiated discounted rate with certain participating providers. Please
see EyeMed’s online provider locator to determine which participating providers have agreed to the discounted rate.
This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing
documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern. 13
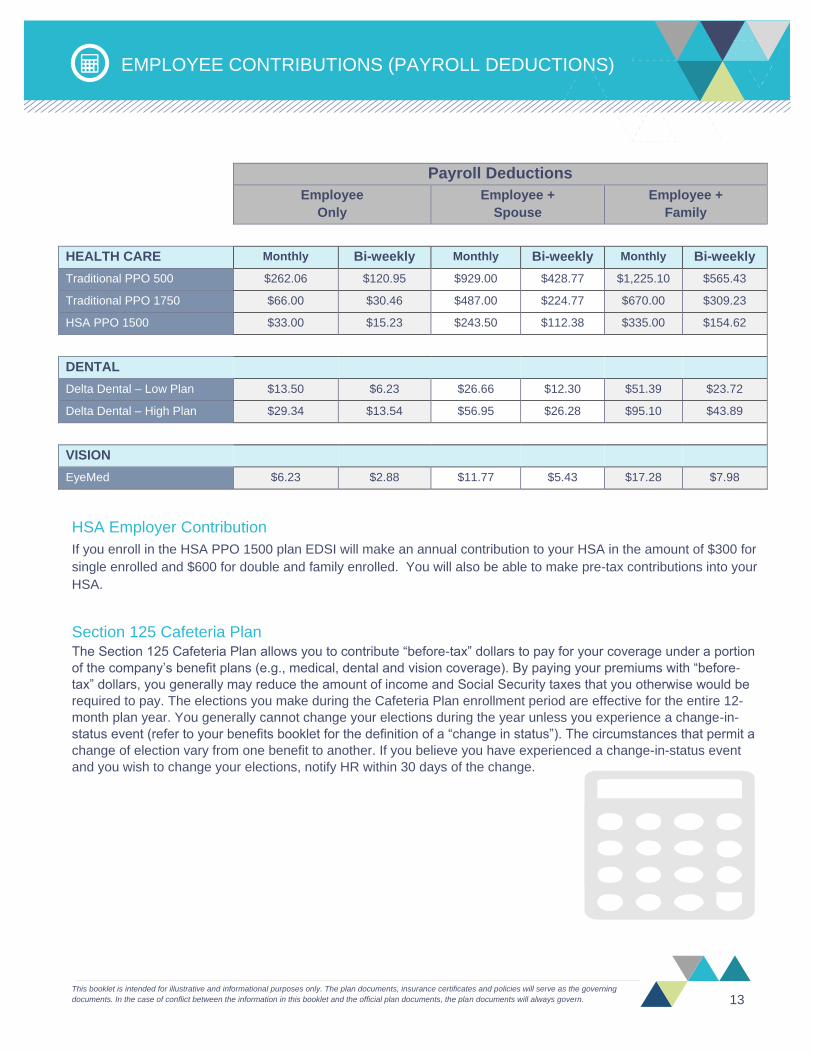
EMPLOYEE CONTRIBUTIONS (PAYROLL DEDUCTIONS)
Payroll Deductions
Employee
Only
Employee +
Spouse
Employee +
Family
HEALTH CARE Monthly Bi-weekly Monthly Bi-weekly Monthly Bi-weekly
Traditional PPO 500 $262.06 $120.95 $929.00 $428.77 $1,225.10 $565.43
Traditional PPO 1750 $66.00 $30.46 $487.00 $224.77 $670.00 $309.23
HSA PPO 1500 $33.00 $15.23 $243.50 $112.38 $335.00 $154.62
DENTAL
Delta Dental – Low Plan $13.50 $6.23 $26.66 $12.30 $51.39 $23.72
Delta Dental – High Plan $29.34 $13.54 $56.95 $26.28 $95.10 $43.89
VISION
EyeMed $6.23 $2.88 $11.77 $5.43 $17.28 $7.98
HSA Employer Contribution
If you enroll in the HSA PPO 1500 plan EDSI will make an annual contribution to your HSA in the amount of $300 for
single enrolled and $600 for double and family enrolled. You will also be able to make pre-tax contributions into your
HSA.
Section 125 Cafeteria Plan The Section 125 Cafeteria Plan allows you to contribute “before-tax” dollars to pay for your coverage under a portion
of the company’s benefit plans (e.g., medical, dental and vision coverage). By paying your premiums with “before-
tax” dollars, you generally may reduce the amount of income and Social Security taxes that you otherwise would be
required to pay. The elections you make during the Cafeteria Plan enrollment period are effective for the entire 12-
month plan year. You generally cannot change your elections during the year unless you experience a change-in-
status event (refer to your benefits booklet for the definition of a “change in status”). The circumstances that permit a
change of election vary from one benefit to another. If you believe you have experienced a change-in-status event
and you wish to change your elections, notify HR within 30 days of the change.

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
14
LIFE AND AD&D INSURANCE OVERVIEW
Life and Accidental Death & Dismemberment (AD&D) Insurance Provided through Lincoln Financial Group at no cost to the employee. Life insurance provides a monetary benefit to your
beneficiary in the event of your death while you are employed at Educational Data Systems, Inc. AD&D insurance is equal
to your life insurance benefit amount and is payable to your beneficiary in the event of your death as a result of an
accident and may also pay benefits in certain injury instances. It is important to keep your beneficiary information up to
date.
Life and AD&D Coverage
Life Insurance $10,000
Accidental Death and Dismemberment $10,000
Benefit Reduction Schedule (of the original amount) 35% at age 70 and an additional 20% at age 75
Voluntary Life Insurance Employees have the opportunity to elect Voluntary Life/AD&D Insurance. This will provide an additional life insurance
benefit for you, your spouse and/or your dependent child(ren). Contributions for these premiums are 100% employee
paid. If you waive voluntary life coverage when you are initially eligible you will be required to provide Evidence of
Insurability (EOI) when enrolling at a later date. EOI is the documentation of good health in order to be approved for
coverage. The carrier will review and determine approval based on EOI documentation. Benefits may be limited and/or
denied based on EOI results. Claims incurred prior to the approval of your coverage will not be covered. It is important to
keep your beneficiary information up to date.
Voluntary Life/AD&D Coverage
Employee Life/AD&D Insurance Increments of $10,000, up to 5 times your annual salary (rounded to the next higher
$10,000) to a maximum of $150,000
Guarantee Issue Amounts Newly Eligible Employees: $150,000
Spouse Life/AD&D Insurance*
Increments of $5,000, up to 2 1/2 times the employee’s annual salary (rounded to the
next higher $10,000) to a maximum of $75,000, not to exceed 50% of the employee
benefit amount
Guarantee Issue Amounts Newly Eligible Spouses: $50,000
Dependent Child(ren) Life Insurance*
Birth to age 14 days old: No benefit
14 days old to 6 months: $250
6 months to 26 years old: $1,000, $5,000 or $10,000
Guarantee Issue Amounts All amounts guaranteed
Benefit Reduction Schedule (of the original amount) 35% at age 70 and an additional 20% at age 75
* The employee must elect coverage in order for dependents (Spouse and/or Child(ren) to be covered. Spouse rates are based on employee’s age. Dependent Child(ren) rates cover all eligible
children
Please Note: For 2017 there will be a “True Open Enrollment” – if you have previously waived voluntary life insurance you have a one-time opportunity to enroll in the plan up to the guarantee issue
maximum with no evidence of insurability (EOI). After that, you will be eligible to elect or increase your coverage equal to 2 benefit levels on a Guaranteed Issue amount during the Open Enrollment
period without EOI. Any amount over the GI will need a completed EOI approved by the carrier.

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing
documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern. 15
DISABILITY OVERVIEW
Short Term Disability Insurance Provided through Lincoln Financial Group at no cost to the employee. Short Term Disability Insurance provides income
protection in the event you become disabled and are unable to work due to sickness or non-occupational injury, including
pregnancy, for a short period of time.
Short Term Disability Coverage
Benefit Amount 60% of weekly earnings
Benefit Maximum $350 per week
Elimination Period 8th calendar days for accident / illness
Maximum Benefit Period Up to 13 weeks
Long Term Disability Insurance Provided through Lincoln Financial Group at no cost to the employee. Long Term Disability Insurance provides income
protection in the event you become disabled and are unable to work for an extended period of time.
Long Term Disability Coverage
Benefit Amount 60% of monthly earnings
Benefit Maximum $6,000 per month
Elimination Period 90 days
Maximum Benefit Period Social Security Normal Retirement Age

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
16
FLEXIBLE SPENDING ACCOUNTS (FSA) OVERVIEW
All eligible employees may participate in a Flexible Spending
Account (FSA) program administered through Infinisource.
What Is a Flexible Spending Account? A Flexible Spending Account, also known as a Section 125
Cafeteria Plan, allows you to set aside money from your
paycheck before income taxes to be used to pay for various
out-of-pocket medical expenses and dependent care
expenses.
What Are the Types of FSAs? 1. Healthcare FSA. You can use this account to pay for
healthcare expenses that you or your dependents
incur even if they are not enrolled in the company
sponsored medical plan.
Healthcare FSA – for those enrolled in the Traditional
PPO plans
Limited Purpose – for those enrolled in the HSA PPO
plan (for post medical deductible, dental and vision
ONLY)
2. Dependent Care FSA. This account is for DAYCARE
expenses ONLY and cannot be used for medical
expenses.
3. Transit and Parking FSA. You can use this account
to set aside money to pay for the expense of getting to
and from work such as parking costs and public
transportation.
How does an FSA Work? First, estimate the amount of out-of-pocket expenses you
expect to incur in the upcoming year (known as your election
amount). This is divided by the frequency of pay periods.
This amount is then deducted from your paycheck each pay
period on a pretax basis. When you incur expenses during
the plan year, you can swipe your FSA debit card at point of
sale or you can submit a receipt for reimbursement.
How Much Can I Contribute to the
FSA Plan? Healthcare Flexible Spending
Annual maximum contribution: $2,600
Dependent Care Flexible Spending
Annual maximum contribution:
$5,000 married couple filing jointly
($2,500 per person if filing separate returns)
Transit and Parking Flexible Spending
Annual maximum contribution: $3,060 each
The Use It or Lose It Rule Section 125 plans are governed by the “use it or
lose it” rule, whereby any amounts remaining at the
end of the year are forfeited due to the IRS
regulations. All claims must be submitted no later
than 90 days after the end of the plan year.
Things to Consider Before You Contribute
to an FSA
Be sure to fund the account wisely as the
funds are use it or lose it
You cannot take income tax deductions for
expenses you pay with your Healthcare
Dependent Care FSA
You cannot stop or change contributions to
your FSA during the year unless you have
a change in status consistent with your
change in contributions
You may have a Health Savings Account
and a Limited Purpose Healthcare FSA

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing
documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern. 17
HEALTHCARE FSA OVERVIEW
Healthcare FSA Claims Reimbursement Through Infinisource, you have a variety of
reimbursement options: debit card, online
submission, fax or email.
Debit Card You will receive a debit card, which is the most
convenient way to receive reimbursement. Simply
swipe your debit card at your provider’s office,
pharmacy, hospital, etc., at time of service and your
claim will be paid instantly. It is important when you
are utilizing the debit card to still ask for and keep an
itemized receipt on file. You may still receive a letter
from www.infinisource.com requesting this receipt
for IRS documentation purposes. Even if you use
the debit card, YOU are ultimately responsible to the
IRS for documentation (i.e., a receipt). YOU are
required to keep it and submit it so the plan is
compliant with government regulations.
Please be advised that if you do not respond to
Infinisource’s request for an itemized receipt,
your card and your account will be suspended.
Online You can submit your claims online at
www.infinisource.com. To log in to your account, go
to www.infinisource.com. Once you are registered
and logged in, you can view your account balance(s)
and see the status of any claims you have
submitted.
Fax or Email You are also able to submit your claim via fax at (800)
379-5670 or by email at [email protected].
Sample Medical Eligible Expenses The following is a partial list of expenses that are
reimbursable tax-free with a Medical Expense FSA. For
a complete list, visit the IRS’s website at www.irs.gov
and search for Section 213 expenses.
Ambulance service
Chiropractic care
Contact lenses (corrective)*
Diagnostic tests
Doctor’s fees*
Drugs (prescription only**)
Eyeglasses
Injections and vaccinations
X-rays
*To be eligible for reimbursement, some treatments, prescription drugs or
services deemed cosmetic in nature require written proof of medical necessity
from your health care provider
**Not all drugs requiring a prescription are approved by the IRS as eligible for
reimbursement.
There are at least
two significant
ways to benefit
from an FSA.
1
2
Take advantage of the tax savings. By reducing your gross income,
you pay less in taxes, take home more pay, and have the freedom to
choose how your money is used.
The second benefit is the “cash flow” increase built into the
healthcare FSA (not the dependent day care FSA). This means that
no matter how much money you have actually contributed to the plan
at any given point, you can still be reimbursed up to your entire
annual election. So a major medical expense at the beginning of the
claim period can be reimbursed even though few, if any, deposits
have been made into the account at that time.

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern.
18
DEPENDENT CARE FSA OVERVIEW
Below is a list of expenses that qualify for reimbursement from the
Dependent Care Account. Generally, eligible expenses include the
cost of childcare for dependents under age 13 or care for a disabled
spouse or dependent that allows you – or you and your spouse – to
work. You’ll also find examples of expenses that do not qualify for
reimbursement because they are not considered legitimate
deductions for federal income tax purposes. To see a full list of IRS-
qualified dependent care expenses, go to www.irs.gov and search for
“publication 503.”
Eligible Expenses Fees paid to a child care center or day care camp that complies
with all applicable state and local regulations if providing care for
more than six children
Full amount paid to a nursery school, even though the cost may
include lunch and education services
Fees paid to a babysitter in or outside your home
Fees paid to a relative who provides dependent care services, other than
your spouse, your child under age 19, or a dependent you claim for federal
income tax purposes
Fees paid to a housekeeper or cook who also is responsible for providing care for an eligible
dependent
Fees paid to a nurse or home health care agency for care for your spouse or legal dependent who is
physically or mentally incapable of self-care
Legally mandated amounts paid on behalf of the provider – Social Security (FICA), federal (FUTA) and
state (SUTA) unemployment taxes
Ineligible Expenses Food, clothing and education
Transportation to and from the place where dependent care services are provided
Fees paid for a child care center that provides care for more than six children but does not comply with all
applicable laws
Expenses for which a federal child care tax credit is taken or which are claimed under the
health care account
Search fees for a dependent care provider

This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and policies will serve as the governing
documents. In the case of conflict between the information in this booklet and the official plan documents, the plan documents will always govern. 19
EMPLOYEE ASSISTANCE PROGRAM
The
Some problems just can’t be solved alone. We all need help sometimes. Relationships are tested,
children act out, parents become ill, plans fail, and emotions
take on a life of their own. Recognizing that we may need
help in these situations is the first and most important step
to solving our problems. All too often, we don’t know where
to turn for assistance.
Educational Data Systems, Inc. recognizes that any
problem affecting your wellbeing and happiness also affects
your job performance and satisfaction and has made available
to you and EAP through EmployeeConnectSM to help.
EmployeeConnectSM provides confidential assistance to you and your eligible family members when personal
problems are affecting quality of life and/or job performance.
Our goal is to help you and your family lead fuller and more productive lives.
Your counselor will help you:
Identify problems and better understand the issues that caused you to seek assistance.
Develop options and explore ways of addressing the problem(s)
Decide on a course of action
The services you receive are completely confidential. No information, written or verbal, will be given to your employer or anyone else without your written consent.
Benefits You Receive: Unlimited telephonic counseling and up to 4 face to face visits per issue.
You and your family can get help with a wide variety of issues, including:
Personal and Work Stress
Depression
Family Relationships
Alcohol/Drug Problems
Elder Care and Aging Concerns
Grief and Loss Issues
Financial Counseling Referrals
Legal Referrals
Stress and Anxiety
Anger Management
Domestic Violence
Employee Assistance
Program is a free benefit
for you, your spouse,
and any eligible
dependents, and it is
totally confidential,
beginning with your first
phone call.

2017 ENROLLMENT
BENEFITS ROADMAP
This booklet is intended for illustrative and informational purposes only. The plan documents, insurance certificates and
policies will serve as the governing documents. In the case of conflict between the information in this booklet and the
official plan documents, the plan documents will always govern. Educational Data Systems, Inc. reserves the right to
change or terminate at any time, in whole or in part, the employee benefit package, with respect to all or any class of
employees, former employees and retireees, if appicable.