20160919 scientific rationale for the inclusion and exclusion criteria for intravenous alteplase in...
TRANSCRIPT

IV-tPA ✘
Scientific Rationale for the Inclusion and Exclusion Criteria
R1 Jin-Yi Hsu

Inclusion criteria
< 3hours
Ischemic stroke
Age 18 - 80

Time
H & P
Lab
Image
3 hours
IV-tPA process

IV-tPA check list

✘
IV-tPA check list

Neuro Non- Neuro
SystemicPlatelet/ aPTT/ INR
Blood sugar/ Blood pressure
NIHSS < 4NIHSS > 25

Time
H & P
Lab
Image
3 hours
IV-tPA process
sICHHemorrhage

t-PA treatment rate
Hospital-based
20-30%

t-PA treatment rate
National-based
3-5%
Hospital-based
20-30%

Delay in presentation
t-PA treatment rate

Delay in presentation
t-PA treatment rate
Potential treatable, modifiable or reversible
before t-PA
Delay in presentation
Potential treatable, modifiable or reversible
before t-PA
Controversial criteria
t-PA treatment rate

IV-tPA evaluation
43 recommendation
Class I Class IIa Class IIb Class III

IV-tPA evaluation
43 recommendation
Class I
Class IIa
Class IIb
Class III
Class I
Class IIa
Class IIb
Class III

IV-tPA evaluation
43 recommendation
Class I
Class IIa
Class IIb
Class III
Class I
Class IIa
Class IIb
Class III

Time
3 hours
Age
Age
80 y/o
18 y/o
Equal Outcome

Time
3 hours
Age
Age
80 y/o
18 y/o
Risk elevation

Time
3 hours
Age
Age
80 y/o
18 y/o

Time
3 hours
Onset time
4.5 hours
As fast as possible

Time
3 hours
Onset time
4.5 hours
Not DM & CVANIHSS < 25No OACs
Ischemic zone not reach 1/3 MCA
Age < 80
NINDS

Time
3 hours
Onset time
4.5 hours
Not DM & CVANIHSS < 25No OACs
Age < 80
ECASS III
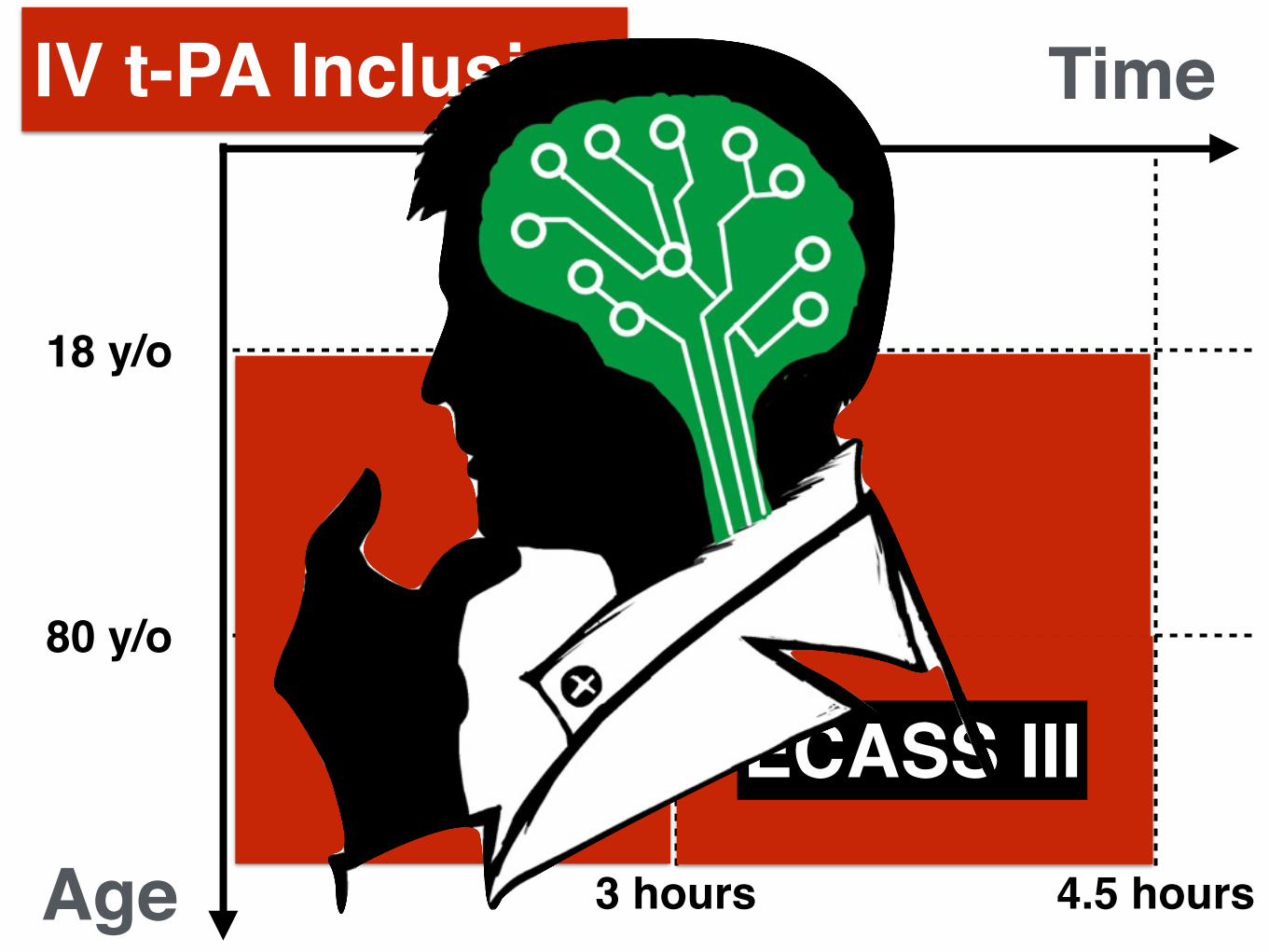
Time
3 hours 4.5 hours
IV t-PA Inclusion
Age
80 y/o
18 y/o
ECASS III

Time
3 hours 4.5 hours
IV t-PA Inclusion
Age
80 y/o
18 y/o
Not delaying IV-tPA due to obtain penumbral imaging

Stroke severity
4 25NIHSS

Stroke severity
4 25NIHSS
< 3 hours

Stroke severity
4 25NIHSS
< 3 hoursDisability

Stroke severity
4 25NIHSS
< 3 hoursNo Disability

Rapid improving
Remain moderately impaired
Potential disabled

Rapid improving
Remain moderately impaired
Potential disabled
Don’t wait to observe severity

Ischemic stroke within 3 months

History of ICH
Previous ICH

History of ICH
Cerebral microbleeds

Suspicion of SAH clinically

Un-ruptured intracranial aneurysm
< 1cm

Un-ruptured intracranial aneurysm
>1cm

Intravascular malformation

Intra-cranial neoplasm
Intra-axialParenchymal lesion

Intra-cranial neoplasm
Extra-axialNon-parenchymal lesion

ICH on CT

Severe
EICs on CT

Mild/Moderate
EICs on CT

Intracranial/ Spinal surgery within 3 months

Major surgery within 14 days
Individualized

Severe head injury within 3 months

Post-traumatic infarction

Major trauma within 14 Days
Carefully considered

Seizure at stroke onset
Real Weakness?
Post-Ictal?

Acute myocardial infarction
PCI first
Then IV-tPA

Recent MI within 3 months
NSTEMI
STMEI, RCA

Recent MI within 3 months
STEMI, LM

Endovascular complication

Aortic arch dissectionAortic arch dissection

Extra-cranial artery dissection

Intra-cranial artery dissection

Endocarditis

Pericarditis
Severe stroke
t-PA is reasonable

Pericarditis
Mild stroke
Not well established

L’t heart thrombus
Severe stroke
t-PA is reasonable

L’t heart thrombus
Mild stroke
Not well established

Intracardiac mass
Severe stroke
Maybe reasonable

0 24Drug administration
SBP < 185 mmHg DBP < 110mmHg
Blood pressure

Blood pressure
0 24Drug administration
SBP < 180 mmHg DBP < 105mmHg

50 400Bloodsugar
Blood sugar

50 400Bloodsugar
Blood sugar

50 400Bloodsugar
Blood sugar

50 400Bloodsugar
Stroke mimics
Blood sugar

Platelet & Coagulation
Platelet < 100000
INR > 1.7
aPTT > 40 seconds
PT > 15 seconds

Platelet & Coagulation
Extremely low risk
No reason to wait lab data

Warfarin
LMWH
Rivaroxaban
Dabigatran
Anti-coagulant

Warfarin
LMWH
Rivaroxaban
Dabigatran
INR > 1.7
Anti-coagulant

Warfarin
LMWH
Rivaroxaban
Dabigatran
Within 24 hrs
Anti-coagulant

Warfarin
LMWH
Rivaroxaban
Dabigatran Within 48 hrsaPTT/ INR/ Plt/ ECT TT/ Direct factor Xa
Anti-coagulant

Concurrent anti-platelet
0 24t-PA
AspirinClopedigrol

Concurrent anti-platelet
0 24t-PA
Anti-plateletDual anti-platelet
Low sICH risk

GI bleeding in recent 21 days
Harmful

Hx of bleeding diathesis/ coagulopathy
Individualized

Diabetic hemorrhagic retinopathy
Visual loss risk ⬆

Menstruation & Menorrhagia
Menstruation

Menstruation & Menorrhagia
Menorrhagia

Menstruation & Menorrhagia
Menstruation
Menorrhagia

Non-compressible vessel pucnture within 7 days
Uncertain

Dural puncture within 7 days
Maybe considered

ESRD with normal aPTT
Comorbidity

Dementia
Malignancy
Comorbidity

Give IV t-PA, even no consent
✘
Consent

Psychogenic stroke mimics
Extremely low risk
No reason to wait

Drug use ( Cocaine)

Pregnancy
Moderate-Severe

Post-partum ( < 14 days)
Not well established

Part 1
Part 2
Part 3
IV-tPA check list

• ( Microbleeds
• Actilyse
• 3
• 3
• 3 NSTEMI& STEMI-RCA, STEMI-LM
• 21
• 14
• 10
Part 1IV-tPA check list

• 3
• ( NIHSS < 4
• ( NIHSS > 25
• (
• SBP > 185 mmHg or DBP > 110mmHg
• (Intra-axial VS. Extra-axial) ( <1cm VS. >1cm)
•
•
Part 2IV-tPA check list

•
•
•
• (
•
Part 2IV-tPA check list

Part 3IV-tPA check list• 48 heparin aPTT
• INR > 1.7
• < 100000/mm3
• < 50mg/dL > 400mg/dL
• ( EIC > 1/3 MCA territory)
• 10
•

Neuro Non- Neuro
SystemicPlatelet/ aPTT/ INR
Blood sugar/ Blood pressure
NIHSS < 4NIHSS > 25

Neuro Non- Neuro
SystemicPlatelet/ aPTT/ INR
Blood sugar/ Blood pressure
NIHSS < 4NIHSS > 25
Thanks for your attention
R1 Jin-Yi Hsu
✔✔✔
✔

Conclusion
Clear benefit• Alteplase treatment in elderly stroke patients
• Severe stroke
• Diabetes mellitus and hyperglycemia
• Minor early ischemic changes (EIC)

IV-tPA check list• ( Microbleeds
• Actilyse
• 3
• 3
• 21
• 4.5
•
•
Revised

IV-tPA check list•
• 48 heparin aPTT > 40 secs
• INR > 1.7
• 48
• < 100000/mm3
• SBP > 185 mmHg or DBP > 110mmHg
• < 50mg/dL > 400mg/dL
• ( EIC > 1/3 MCA territory)
Revised

Thanks for your attention
R1 Jin-Yi Hsu
✔✔✔
✔