2014 06 manejo de las varices gastricas
TRANSCRIPT

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 111
PERSPECTIVES IN CLINICAL GASTROENTEROLOGYAND HEPATOLOGY
Management of Gastric Varices
Juan Carlos GarciandashPagaacuten Marta BarrufetDagger Andres Cardenassect and Agravengels Escorsellk
Hepatic Hemodynamic Laboratory and kICU Liver Unit Hospital Clinic Institut d rsquo Investigacions Biomegravediques August Pi-Sunyer (IDIBAPS) Ciber de Enfermedades Hepaacuteticas y Digestivas (CIBEREHD) Barcelona DaggerDiagnostic Imaging CenterHospital Clinic Barcelona sectGIEndoscopy Unit Institut de Malalties Digestives i Metaboliques Hospital Cliacutenic University of Barcelona IDIBAPS CIBEREHD Barcelona Spain
This article has an accompanying continuing medical education activity on page e52 Learning ObjectivesmdashAt the end of this activity the successful
learner will understand the prevalence classi1047297cation and therapy of gastric varices in patients with cirrhosis
According to their location gastric varices (GV) are clas-
si1047297ed as gastroesophageal varices and isolated gastric
varices This review will mainly focus on those GV located
in the fundus of the stomach (isolated gastric varices 1 andgastroesophageal varices 2) The 1-year risk of GV bleeding
has been reported to be around 10ndash16 Size of GV
presence of red signs and the degree of liver dysfunction
are independent predictors of bleeding Limited data sug-
gest that tissue adhesives mainly cyanoacrylate (CA) may
be effective and better than propranolol in preventing
bleeding from GV Generalmanagement of acute GV bleeding
must be similar to that of esophageal variceal bleeding
including prophylactic antibiotics a careful replacement of
volemia and early administration of vasoactive drugs Small
samplendashsized randomized controlled trials have shown that
tissue adhesives are the therapy of choice for acute GV
bleeding In treatment failures transjugular intrahepatic
portosystemic shunt (TIPS) is considered the treatment of
choice After initial hemostasis repeated sessions with CA
injections along with nonselective beta-blockers are recom-
mended as secondary prophylaxis whether CA is superior to
TIPS in this scenario is not completely clear Balloon-
occluded retrograde transvenous obliteration (BRTO) has
been introduced as a new method to treat GV BRTO is also
effective and has the potential bene1047297t of increasing portal
hepatic blood 1047298ow and therefore may be an alternative for
patients who may not tolerate TIPS However BRTO oblit-
erates spontaneous portosystemic shunts potentially
aggravating portal hypertension and its related complica-
tions The role of BRTO in the management of acute GV
bleeding is promising but merits further evaluation
Keywords Gastric Varices Variceal Bleeding Portal Hyperten-
sion Cirrhosis Cyanoacrylate Transjugular Intrahepatic Por-
tosystemic Shunt (TIPS) Balloon-occluded Retrograde
Transvenous Obliteration (BRTO)
Prevalence of gastric varices (GV) in patients with
cirrhosis is estimated to be near 17 However
this estimation is based on only one study1 therefore the
actual magnitude of the problem is not well known
According to their location within the stomach GV are
classi1047297ed as gastroesophageal varices (GOV) and isolated
gastric varices (IGV) GOV are divided as GOV1 which are
esophageal varices that extend below the gastroesophageal
junction along the lesser curve of the stomach and GOV2
which are those that extend beyond the gastroesophagealjunction into the fundus of the stomach IGV includes IGV1
which are those located in the fundus of the stomach and
also called fundal varices and IGV2 which refer to ectopic
varices located anywhere in the stomach (Figure 1) This
classi1047297cation initially described by Sarin et al1 has
important clinical implications regarding incidence risk of
bleeding and management According to Sarin et al GOV1
represent almost 75 GOV2 21 IGV1 less than 2 and
IGV2 4 of all GV GOV1 are a continuation of esophageal
varices and share the same vascular anatomy and response
to treatment and thus will not be further discussed This
review will mainly focus on the management of IGV1 andGOV2 the so-called cardiofundal varices Data regarding
prevalence bleeding risk and management of IGV2 are
scarce and therefore no speci1047297c recommendations are
made on this type of GV However in our center the man-
agement of IGV2 is similar to that of IGV1 Although recent
studies speci1047297cally detail the different types of GV most of
the available data comes from series of patients with mixed
types of GV and portal hypertension etiologies (cirrhotic
and noncirrhotic) and the results may not be applicable to
all types of GV As a result the optimal treatment of gastric
fundal varices has not fully been determined
Primary Prophylaxis
In a prospective study including 117 patients with
cirrhosis and cardiofundal varices (69 IGV1 and 31
Abbreviations used in this paper BRTO balloon-occluded retrogradetransvenous obliteration CA cyanoacrylate EBL endoscopic band liga-tion EIS endoscopic injection sclerotherapy EUS endoscopic ultraso-nography GOV gastroesophageal varices GV gastric varices IGVisolated gastric varices RCT randomized controlled trial TIPS trans-
jugular intrahepatic portosystemic shunt
copy 2014 by the AGA Institute1542-3565$3600
httpdxdoiorg101016jcgh201307015
Clinical Gastroenterology and Hepatology 201412919ndash928
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 211
GOV2) the incidence of bleeding was 16 36 and
44 at 1 3 and 5 years respectively Size of varices
presence of red signs and the degree of liver dysfunction
were directly related with the risk of bleeding (ranging
from an annual incidence of bleeding of 4 in patients
with Child class A with small varices without red signs to
65 in pat ients with Child class C with large varices with
red signs)2 (Figure 2) However these data must be
cautiously interpreted because of the small number of
patients followed for more than 1 year and the unusually
high prevalence (52) of concomitant hepatocelullarcarcinoma The 1-year bleeding risk of the small (n frac14 30)
untreated group of a recent prospective randomized
controlled trial (RCT) comparing cyanoacrylate (CA)
(n frac14 30) vs beta-blockers (n frac14 29) was around 103
Variceal size and liver function evaluated by the Model
for End-Stage Liver Disease score were again factors
associated with a high risk of bleeding In this study GV
were mainly GOV2 with few IGV1 There were signi1047297cant
differences in favor of CA for the prevention of bleeding
and survival when compared with no treatment and only
for prevention of rebleeding when compared with pro-
pranolol However larger studies are needed before a
formal recommendation in regard to the need and typeof primary prophylaxis for GV can be made Until then
our recommendation is not to use primary prophylaxis in
GV or alternatively use nonselective beta-blockers
Management of Acute Gastric VaricealBleeding
Although no studies have been speci1047297cally devoted to
address this issue in patients with cardiofundal varices
general consensus is that the initial management is
similar to that of esophageal variceal bleeding including
the use of prophylactic antibiotics careful replacement of
volemia with a restrictive transfusion policy and the
early administration of vasoactive drugs (terlipressin
somatostatin or a somatostatin analogue)45 IGV1
varices which often appear as a consequence of large
spontaneous splenorenal shunts may bleed with portal
pressure gradients lower than those needed for
esophageal varices It can then be hypothesized that
more powerful vasoconstrictors are needed not only
to decrease portal pressure but also to markedly
reduce portal and collateral blood 1047298ow to control acute
cardiofundal variceal bleeding In our experience
nearly 40 of patients with bleeding IGV1 who wereonly receiving vasoactive drugs require rescue therapy
mainly transjugular intrahepatic portosyst emic shunt
(TIPS) to achieve 5-day control of bleeding6 Therefore
we currently do not recommend using vasoactive drugs
alone but always with concomitant endoscopic therapy
Speci1047297c high-quality data on the use of endoscopic
therapy for acute GV bleeding are limited and in most
published RCTs only half of patients included in the trials
had cardiofundal varices Despite these limitations most
uncontrolled series report a high rate of control of
bleeding with the use of tissue adhesives such as CA
(gt
90) (Table 1) In addition small-size RCTs comparingtissue adhesives vs either endoscopic band ligation (EBL)
or endoscopic injection sclerot herapy (EIS) have shown
that tissue adhesives are equally7 or more89 effective than
EBL in the control of acute bleeding and more effective
than both in preventing rebleeding In addition tissue
adhesives perform better than sclerotherapy in
achieving initial hemostasis910 GOV1 varices are usually
treated as esophageal varices with EBL although some
investigators also recommend the use of tissue
adhesives for GOV1 varices11 Overall experts agree that
endoscopic therapy with tissue adhesives mainly CA is
the therapy of choice for acute bleeding from IGV1 and
GOV241213 If tissue adhesive is not available band
Figure 1 Sarinrsquos classi1047297cation of GV Modi1047297ed with permis-sion from the American Gastroenterological Association(AGA) Institute Gastroslides ndash Cirrhosis and PortalHypertension
Figure 2 A large gastric varix (IGV1) with a recent nipple sign
920 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 311
ligation seems to have some bene1047297t in small GOV2 varices
However no speci1047297c studies have evaluated this issue5
The standard protocol uses CA and lipiodol in 11ratio injecting with no more than 1 mL at the varix each
time14 (Supplementary Video) In most cases CA is
usually extruded into t he stomach lumen within 1ndash3
months after injection15 Multiple complications from CA
injection have been reported among published studies A
recent report of 753 patients indicated that most com-
plications occurred from rebleeding that was due to
extrusion of the glue cast (44) sepsis (13) distant
emboli (pulmonary cerebral splenic 07) gastric ulcer
formation (01) major gastric variceal bleeding (01)
and mesenteric hematoma associated with hemoper-
itoneum and bacterial peritonitis (01) The complica-tion-related mortality was 0516 Other studies have
reported a higher incidence of embolism that may occur
in up to 2ndash3 of cases1317
Combination therapy of endoscopy and pharmaco-
logic therapy is considered the st andard of care in acute
esophageal variceal bleeding45 However because of
the paucity of data it is unknown whether this
recommendation also applies to GOV2 or IGV1 variceal
bleeding Because in most cases drug therapy is
started before diagnostic endoscopy (and therefore
before the identi1047297cation of the gastric variceal origin
of bleeding) it seems the most rational approach is to
combine drug therapy plus endoscopic treatment
(preferably tissue adhesives) in patients with acute GV
bleeding
In massive bleeding with hemodynamic instabilityballoon tamponade can be used as a temporary ldquobridgerdquo
(for a maximum of 24 hours) until de1047297nitive treatment
can be instituted Tamponade may achieve hemostasis
in up to 80 of the patients although more than 50
of the cases rebleed af ter balloon de1047298ation A single
study from Teres et al18 comparing the LintonndashNachlas
vs the SengstakenndashBlakemore tube demonstrated that
LintonndashNachlas tube was more effective in fundal var-
iceal bleeding because of the large volume (600 mL) of
its single gastric balloon allowing an appropriate
compression of the fundal varices Nevertheless if the
Lintonndash
Nachlas balloon is not available compressionwith the gastric balloon of a SengstakenndashBlakemore
tube maximally in1047298ated may be appropriate
TIPS is considered the treatment of choice in patients
bleeding from GOV2 or IGV1 after failure to control initial
bleeding or rebleeding with combination therapy1920
Contrary to what is suggested in esophageal variceal
bleeding a second-attempt endoscopic therapy is
usually not considered Embolization of collaterals
feeding GV has been proposed to increase the ef 1047297cacy of
the TIPS procedure Two retrospective studies analyzed
the ef 1047297cacy of embolization combined with TIPS in acute
variceal bleeding Few patient s with cardiofundal
variceal bleeding (2121 and 3122 respectively) were
Table 1 Results of Published Studies on Endoscopic Treatment of Acute Bleeding From GV
First author year (reference) Design n
Treatmentreceived (n)
Initial control ( )overall (according
to treatment)
Mortality ( )overall (according to
treatment)Follow-up a
( mo )
Ogawa 199969 Retros 33 EIS (21) vs glue (12) 67 (53 vs 100) NR mdash
Kind 200070 Obs 174 Glue 97 64 36Huang 200071 Obs 90 Glue 100 40 36
Akahoshi 200272 Obs 52 Glue 96 30 12Rengstorff 200473 Pilot 25 Glue 100 12 11Mahadeva 200323 Obs 43 TIPS (20) vs
glue (23)93 (90 vs 96) 20 (25 vs 15) 6
Cheng 200730 Obs 146 Glue 95 10 36Mumtaz 200774 Obs 50 Glue 100 12 In-hospitalMarques 200828 Obs 48 Glue 88 44 18Paik 200875 Obs 121 Glue 91 12 1Procaccini 200944 Retros 105 TIPS (61) vs
glue (44)91 (90 vs 93) NR mdash
Monsanto 201276 Obs 97 Glue 96 9 In-hospitalOho 19959 RCT 53 EIS (24) vs
glue (29)81 (50 vs 88) 53 (67 vs 38) mdash
Lo 20018 RCT 26 EBL (11) vs glue (15) 69 (45 vs 87) 42 (48 vs 29) 24Sarin 200210 RCT 17 EIS (8) vs
glue (9)59 (38 vs 78) 18 (25 vs 11) 16
Tan 20067 RCT 97 EBL (48) vsglue (49)
93 (93 vs 93) 64 (63 vs 65) 36
Hou 200977 RCT 91 Glue (05 vs10 mL)
88 NR mdash
NOTE All the studies included IGV1 GOV1 and GOV2Obs observational study Retros retrospective comparative study aMedian
June 2014 Management of Gastric Varices 921
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 411
included No 1047297rm conclusions can be drawn from these
small studies However although evidence on the target
portal pressure gradient to be reached to prevent
rebleeding from fundal GV is not clear and it has been
suggested that fundal varices may rebleed despite a
portal pressure gradient slightly below 12 mm Hg the
small previous studies suggest that there is not a clear
rationale to perform embolization particularly if theportal pressure gradient after TIPS is reduced below 12
mm Hg
There is no RCT evaluating the use of TIPS as the
initial treatment to achieve hemostasis in patients with
IGV1 a cohort study suggested that it is highly effective
in achieving initial hemostasis in GOV1 and GOV2 vari-
ces23 A recent RCT showed that early (72 hours from
bleeding) polytetra1047298uoroethylene-coated TIPS can be
considered as a 1047297rst-line treatment in patients with
esophageal variceal bleeding at high risk of treatment
failure (de1047297ned by Child class C less than 14 points or
Child class B with active bleeding) because it reduces the
risk of treatment failure and improves survival in com-
parison with convent ional treatment with drugs plus
endoscopic therapy24 Although patients with GV were
excluded in the study it is likely that the bene1047297t of the
use of early TIPS may also apply to patients with GV and
the same high-risk criteria however this needs to be
studied further
Secondary Prophylaxis
Rebleeding rates after an acute GV bleeding episode
treated with tissue adhesives (mainly CA) range from7ndash65 with most of the large series reporting rates
below 15 Thus after initial hemostasis with tissue
adhesives repeated sessions are performed on a 2- to
4-week basis until endoscopic obliteration is achieved
Several case series and controlled studies have specif-
ically evaluated the effect of long-term injections
of tissue adhesives (mainly CA) to prevent GV
rebleeding1725ndash30 (Table 2) In most of these studies
eradication is achieved with 2ndash4 injections with a
volume ranging from 1ndash2 mL per session
Similar to what occurs with initial hemostasis CA
has been shown to be superior to both sclerotherapy
and band ligation for secondary prophylaxis On the
contrary comparison with nonselective beta-blockers
offers con1047298icting results In a small randomized study
41 patients who bled from esophageal (n frac14 31) or GV
(GOV 1 and GOV 2) (n frac14 10) treated initially with CA
were randomized to repeated CA injections (n frac14 21) or
propranolol (80ndash160 mg) (n frac14 20)31 No signi1047297cant
differences were observed between the 2 groups in theincidence of variceal rebleeding and death The inci-
dence of complications was higher in the CA group
(47 vs 10) A major limitation of the study was the
small number of patients with GV31 In a more recent
RCT 64 patients who bled from GV (54 GOV 2 and
10 IGV1) were allocated to receive either repeated CA
(n frac14 33) or propranolol (n frac14 34) for secondary pro-
phylaxis32 Rebleeding in the CA group was signi1047297cantly
lower than in the beta-blocker group (15 vs 55
P frac14 004) and after a 26-month follow-up the mortality
rate was lower as well (3 vs 25 P frac14 026) The rate
of complications in the CA group was 3
A recent report indicates that endoscopic ultraso-
nography (EUS)ndashguided therapy for fundal GV (IGV1 and
GOV2) with CA and 1047297bered coils may improve the ef 1047297-
cacy of this technique33 In this study 30 patients un-
derwent successful transesophageal EUS-guided therapy
of IGV1 and GOV2 The mean number of GV treated was
13 per patient and the mean volume of CA injected was
14 mL per varix GV were obliterated after a single
treatment session in the vast majority of patients (96)
who underwent follow-up endoscopy Rebleeding
occurred in 1 patient who was successfully treated with
a second session There were no procedure-related
complications Although this is a small series EUS-guidedtherapy seems to be a promising approach in selected
cases however more data are needed to consider it a
routine tool for the management of GV
Finally in a recent study 95 patients with GV (GOV2
n frac14 77 IGV1 n frac14 18) who bled and were successfully
treated with CA were assigned to receive treatment with
beta-blockers plus repeated CA (every 3ndash4 weeks until
the varices were obliterated) or repeated CA injections
alone34 After a mean follow-up of 19 months the overall
rebleeding (22 vs 26 patients P frac14 336) and survival
rates (22 vs 20 P frac14 936) were not different between the
2 groups One-year rebleeding free survival was also
Table 2 Results of Published Studies on Long-term Injection of Tissue Adhesives in the Prevention of GV Rebleeding
First author year (reference) n Eradicationhemostasis ( ) Rebleeding ( )
Follow-up(median) Survival ( ) Complications ( )
Rajoriya 201125 31 90 10 4 y 65 (1 y) 64Mishra 201032 33 100 10 26 mo 90 (2 y) 3Choudhuri 201026 108 89 10 307 thorn 172 mo NA NA Belletrutti 200827 34 84 12 11 mo 82 (1 y) 3Marqueacutes 200828 48 87 20 18 mo 56 (NA) 6Cheng 200730 613 77 8 25 mo 95 (1 y) 5Joo 200717 85 98 29 24 mo NA 35
922 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 511
similar (77 vs 765) The results of this study suggest
that contrary to what has been demonstrated for
esophageal variceal bleeding adding beta-blocker ther-
apy to repeated sessions of CA provides no important
bene1047297t for prevention of rebleeding and mortality in
patients with GV bleeding Despite these 1047297ndings and
because nonselective beta-blockers are effective in pa-
tients with concomitant esophageal varices until largerstudies with longer follow-up are available we still
recommend the use of nonselective beta-blockers as an
adjunct to endoscopic therapy in the prevention of GV
rebleeding
Other Endoscopic Therapies
Other endoscopic treatments have also been used to
prevent rebleeding Sclerotherapy has been abandoned
because of high rebleeding rates (50ndash90) Variceal
band ligation may be used for those patients with GOV1
and in some cases of small GOV2 and it is generallyperformed every 2 weeks until apparent endoscopic
obliteration However band ligation is limited by the fact
that it cannot be used in large GOV2 or IGV17 Detachable
loop snares to treat large GV (gt2 cm) along with pro-
pranolol have resulted in low rebleeding rates however
data are very scarce and the procedure is labor inten-
sive This approach has not been further evaluated and
has not been compared with other modalities and thus
cannot be routinely recommended
Thrombin
Thrombin converts 1047297brinogen to a 1047297brin clot thus
forming a clot inside the GV and occluding blood 1047298ow
The use of bovine thrombin was banned because of the
risk of potential prion transmission This is not the case
when using commercially available human thrombin
Each vial is reconstituted with 5 mL distilled water for a
concentration of 250 UmL35 The average dose of
injected thrombin ranges between 1500 and 2000 U
Available data indicate that thrombin is safe and effective
in the treatment of acute GV bleeding with hemostasis
rates of 70ndash100 however rebleeding rates may
range from 7ndash
5036ndash41
There are scarce data inregard to follow-up and eradication rates After initial
hemostasis repeated thrombin injections are
performed every 2ndash3 weeks until eradication Because
of the paucity of data mostly coming from case series
the routine use of thrombin cannot be routinely
recommended
Transjugular Intrahepatic PortosystemicShunt
The role of TIPS vs CA in preventing GV bleeding has
been evaluated in 3 small studies (2 retrospective
observational studies and 1 prospective) Remarkablyin all
3 studies most patients included had GOV1a fewGOV2 and
only anecdotal IGV1 varices In addition the stents used
were uncoated which hasbeen shownto be associatedwith
lower TIPS patency ef 1047297cacy and survival than coated
stents42 Two of these studies2343 showed a higher
rebleeding rate in the CA group (30 and 59) vs the
TIPS group (15 and 40) (Supplementary Table 1)Frequency of complications was similar in the 2 groups
but TIPS-treated patients showed a higher incidence of
hepatic encephalopathy234344 and long-term morbidity
requiring hospitalization44 than endoscopically treated
patients The studies found no signi1047297cant differences in
survival Mahadeva et al23 analyzed the costs after 6
months of therapy and found that CA injections were
more cost-effective than TIPS in a small group of 43
patients with GV bleeding In summary TIPS is a very
effective therapy to prevent GV rebleeding Nevertheless
because of the previously mentioned drawbacks more
data are needed to clarify the role of TIPS in the
secondary prophylaxis of GV bleeding and determine
whether this therapy must be universally applied or
reserved as a rescue therapy after failure of more
conservative approaches
Surgery
Surgery has currently fallen out of favor for patients
with portal hypertension because of the wide avail-
ability of less invasive techniques such as endoscopy
and interventional radiology In selected cases pa-
tients with GV and segmentalleft-sided portal hyper-
tension that is due to isolated splenic vein thrombosis
may be candidates for splenectomy or splenic emboli-
zation as a means of de1047297nitive therapy however data
are scarce
Balloon-occluded RetrogradeTransvenous Obliteration
Balloon-occluded retrograde transvenous obliteration
(BRTO) has been introduced as a treatment method that
aims to directly oblit erate the GV Since its introduction
by Kanagawa et al
45
BRTO has become widely acceptedin Japan and in some centers in the United States as a
minimally invasive and highly effective treatment for GV
The technical dif 1047297culty of BRTO relies on the anatomy of
the afferent and draining veins of the GV Accurate
assessment which is mainly based on imaging studies of
the variceal hemodynamic pattern is the most important
factor in ensuring successful treatment This anatomy
and how it alters the approach have been t horoughly
reviewed by Hirota et al46 Kiyosue et al4748 and
Al-Osaimi et al49
In most cases there is a gastrorenal or gastrocaval
shunt In this situation under 1047298uoroscopic guidance a
balloon catheter is inserted into the outlet of the
June 2014 Management of Gastric Varices 923
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 611
gastrorenal or gastrocaval shunt through a sheath placed
in the right femoral vein Immediately afterward
venography is performed with an injection of 10ndash15 mL
contrast medium via the in1047298ated balloon catheter and
GV are slowly intermitt ently and completely 1047297lled with
a sclerosant (Figure 3)454650ndash63 Thirty to 50 minutes
after the injection as much of the remaining sclerosant
as possible is aspirated via the catheter Finally the
balloon is de1047298ated and the catheter is withdrawn
Ethanolamine oleate is the predominant and traditional
sclerosant agent used in the BRTO procedure
particularly in Asia454650ndash60 Detergent sclerosants in a
foam or frot h have also been studied in both Japan
(polidocanol)6162 and the United States (3 STS)63
Figure 3 ( A ) Basic porto-systemic venous anatomyof GV with the classic gas-trorenal or splenorenalshunts ( B ) ConventionalBRTO procedure throughtransfemoral approach withballoon in the gastrorenalshunt IVC inferior venacava LGV left gastric veinLRV left renal vein MV
mesenteric vein PGVposterior gastric vein(s)PV main portal vein SGVshort gastric vein(s) SVsplenic vein Afferent vein( thin arrows ) Drainage vein( thick arrow )
924 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 711
The advantage of foam is that it reduces the sclerosant-
to-volume ratio requiring less sclerosant per procedure
In cases that involve complex types of afferent or
draining veins the use of additional techniques is required
for successful treatment These techniques include step-wise injection of the sclerosing agent selective injection of
the agent via a microcatheter coil embolization of the
afferent gastric veins double-balloon catheterization and
BRTO performed with percutaneous transhepatic portal
venous access or transileocolic venous access48
Epigastric and back pain (76)56 fever (26)5660
and transient hematuria (53) are the most common
complications of BRTO Bacterial peritonitis was found in
8 of patients in one study but t hese patients recovered
after only conservative therapy45 and this complication is
otherwise rarely mentioned in the literature Portal
(43) and renal vein thrombosis (5) can be found in asmall number of patients and bot h are usually clinically
silent465059 Pulmonary embolism59 pulmonary edema61
coil migration46 and anaphylaxis to ethanolamine oleate46
have also been reported
Technical success de1047297ned by complete obliteration of
the GV with sclerosant occurs in 77ndash100 of pa-
tients64 In some studies repeat BRTO was necessary to
achieve such high percentages465260 GV bleeding af t er a
successful BRTO ranges from 0ndash15465052555659ndash6165
or from 0ndash31666 when factoring in an intent-to-treat
basis (including technical failures) Some authors suggest
that BRTO might be better than TIPS67 or glue65 in the
prevention of GV bleeding However the fact that in
most patients treatment was administered as primary
prophylaxis for high-risk GV the studies had a small
sample size and the ef 1047297cacy of the comparative groups
(either TIPS or glue therapy) was poorer than expected
precludes de1047297nitive conclusions There is only a smallstudy54 that randomized 15 patients with acute GV
bleeding to receive TIPS (n frac14 7) or BRTO (n frac14 8)
without observing signi1047297cant differences in rebleeding
hepatic encephalopathy or survival
BRTO has the potential advantage of increasing portal
blood 1047298ow and potentially improving liver function525457
Therefore it may represent an alternative in patients who
may otherwise not tolerate TIPS59 In that regard in 4
studies including patients with hepatic encephalopathy
there was resolution or signi1047297cant reduction in
encephalopathy in all patients after BRTO46505158 By
contrast BRTO obliterates a spontaneous portosystemicshunt and therefore aggravates portal hypertension and
its related complications An increase in the size of
esophageal varices and the risk of esophageal variceal
bleeding after BRTO has been reported (between 73
and 27 after 1 year)525556 Other complications related
to the increase of portal hypertension after BRTO are the
development of portal hypertensive gastropathy (in 5ndash
13 of cases) ascites (0ndash44)65 and hydrothorax
pleural effusion (0ndash72) As a consequence of the
worsening of portal hypertension in some cases TIPS has
been performed after BRTO68
In conclusion although BRTO seems to be a feasible
technique that is able to successfully control and prevent
Figure 4 Suggested algo-rithm for management of GV EBL in small GV if tissue adhesives notavailable HE hepaticencephalopathy
June 2014 Management of Gastric Varices 925
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 811
GV bleeding there is a lack of good quality data to
routinely recommend BRTO in the management of GV In
our opinion BRTO could be considered in patients with
GV bleeding and large gastrorenal shunts in whom TIPS
may be contraindicated (such as those with refractory
hepatic encephalopathy or elderly patients)
Summary
The best management strategy for GV has not been
completely established because of a paucity of data of
RCTs in this area Speci1047297c treatments such as CA injec-
tion and BRTO are not widely available in all centers
Another limitation is the fact that tissue adhesives such
as CA are not approved by the Food and Drug Adminis-
tration in the United States and thus recommendations
arising from published studies guidelines and expert
opinion cannot be extrapolated to routine practice We
recommend a stepped care approach to the management
of GV as described in Figure 4 There are scarce data onthe role of CA or beta-blockers for primary prophylaxis
of GV bleeding and thus speci1047297c recommendations
cannot be made however patients should receive beta-
blockers if they have concomitant esophageal varices
After initial resuscitation and implementation of vaso-
constrictors and antibiotics endoscopic therapy with CA
should be the 1047297rst line of therapy if available After the
acute episode patients should receive beta-blockers
along with repeated sessions of CA injection if available
TIPS is very effective in controlling active GV bleeding
and for secondary prophylaxis However it carries a risk
of hepatic encephalopathy TIPS is the best treatment
strategy for patients who fail endoscopic therapy
Supplementary Material
Note To access the supplementary materials accom-
panying this article visit the online version of Clinical
Gastroenterology and Hepatology at wwwcghjournalorg
and at httpdxdoiorg101016jcgh201307015
References1 Sarin SK Lahoti D Saxena SP et al Prevalence classi1047297cation
and natural history of gastric varices a long-term follow-upstudy in 568 portal hypertension patients Hepatology 1992161343ndash1349
2 Kim T Shijo H Kokawa H et al Risk factors for hemorrhagefrom gastric fundal varices Hepatology 199725307ndash312
3 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric variceal bleeding comparing cyanoacrylate injection andbeta-blockers a randomized controlled trial J Hepatol 2011541161ndash1167
4 de Franchis R Revising consensus in portal hypertensionreport of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension J Hepatol 201053762ndash768
5 Garcia-Tsao G Sanyal AJ Grace ND et al Prevention andmanagement of gastroesophageal varices and variceal hemor-
rhage in cirrhosis Hepatology 200746922ndash938
6 Escorsell A Abraldes JG Pipa-Muntildeiz M et al Prognosis of acute bleeding from isolated fundal varices in patients withcirrhosis a European cohort Hepatology 201256(Suppl)748A
7 Tan PC Hou MC Lin HC et al A randomized trial of endoscopictreatment of acute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus band ligation Hepatology 200643690ndash697
8 Lo GH Lai KH Cheng JS et al A prospective randomized trial
of butyl cyanoacrylate injection versus band ligation in themanagement of bleeding gastric varices Hepatology 2001331060ndash1064
9 Oho K Iwao T Sumino M et al Ethanolamine oleate versusbutyl cyanoacrylate for bleeding gastric varices a non-randomized study Endoscopy 199527349ndash354
10 Sarin SK Jain AK Jain M et al A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolatedfundic varices Am J Gastroenterol 2002971010ndash1015
11 Lo GH Lai KH Should GOV1 be treated as for esophagealvarices Gastroenterology 20041271014ndash1015
12 Greenwald BD Caldwell SH Hespenheide EE et al N-2-butyl-cyanoacrylate for bleeding gastric varices a United States pilot
studyand cost analysis Am J Gastroenterol 2003981982ndash1988
13 Caldwell SH Hespenheide EE Greenwald BD et al Enbucrilatefor gastric varices extended experience in 92 patients AlimentPharmacol Ther 20072649ndash59
14 Seewald S Ang TL Imazu H et al A standardized injectiontechnique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundalvarices (with videos) Gastrointest Endosc 200868447ndash454
15 Wang YM Cheng LF Li N et al Study of glue extrusion after endoscopic N-butyl-2-cyanoacrylate injection on gastric vari-ceal bleeding World J Gastroenterol 2009154945ndash4951
16 Cheng LF Wang ZQ Li CZ et al Low incidence of complica-tions from endoscopic gastric variceal obturation with butyl
cyanoacrylate Clin Gastroenterol Hepatol 20108760ndash766
17 Joo HS Jang JY Eun SH et al [Long-term results of endo-scopic histoacryl (N-butyl-2-cyanoacrylate) injection for treat-ment of gastric varices a 10-year experience] Korean JGastroenterol 200749320ndash326
18 Teres J Cecilia A Bordas JM et al Esophageal tamponadefor bleeding varices controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube Gastroenterology197875566ndash569
19 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepatic portosystemic shunts gastric fundal compared withesophageal variceal bleeding Gastroenterology 1998114981ndash987
20 Azoulay D Castaing D Majno P et al Salvage transjugular intrahepatic portosystemic shunt for uncontrolled varicealbleeding in patients with decompensated cirrhosis J Hepatol200135590ndash597
21 Gaba RC Bui JT Cotler SJ et al Rebleeding rates followingTIPS forvariceal hemorrhage in the Viatorr era TIPS alone versusTIPS with variceal embolization Hepatol Int 20104749ndash756
22 Xiao T Chen L Chen W et al Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone versus TIPScombined with embolotherapy in advanced cirrhosis a retro-spective study J Clin Gastroenterol 201145643ndash650
23 Mahadeva S Bellamy MC Kessel D et al Cost-effectivenessof N-butyl-2-cyanoacrylate (histoacryl) glue injections versus trans-
jugular intrahepatic portosystemic shunt in the management of
926 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
Edso nGuzman FirmadodigitalmenteporEdso nGuzmanNombredereconocimiento(D N)cn=EdsonGuzmanoou=HNERMemail=e dson_guzmanhotmailcomc=PEFecha20140526200159-050 0
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 211
GOV2) the incidence of bleeding was 16 36 and
44 at 1 3 and 5 years respectively Size of varices
presence of red signs and the degree of liver dysfunction
were directly related with the risk of bleeding (ranging
from an annual incidence of bleeding of 4 in patients
with Child class A with small varices without red signs to
65 in pat ients with Child class C with large varices with
red signs)2 (Figure 2) However these data must be
cautiously interpreted because of the small number of
patients followed for more than 1 year and the unusually
high prevalence (52) of concomitant hepatocelullarcarcinoma The 1-year bleeding risk of the small (n frac14 30)
untreated group of a recent prospective randomized
controlled trial (RCT) comparing cyanoacrylate (CA)
(n frac14 30) vs beta-blockers (n frac14 29) was around 103
Variceal size and liver function evaluated by the Model
for End-Stage Liver Disease score were again factors
associated with a high risk of bleeding In this study GV
were mainly GOV2 with few IGV1 There were signi1047297cant
differences in favor of CA for the prevention of bleeding
and survival when compared with no treatment and only
for prevention of rebleeding when compared with pro-
pranolol However larger studies are needed before a
formal recommendation in regard to the need and typeof primary prophylaxis for GV can be made Until then
our recommendation is not to use primary prophylaxis in
GV or alternatively use nonselective beta-blockers
Management of Acute Gastric VaricealBleeding
Although no studies have been speci1047297cally devoted to
address this issue in patients with cardiofundal varices
general consensus is that the initial management is
similar to that of esophageal variceal bleeding including
the use of prophylactic antibiotics careful replacement of
volemia with a restrictive transfusion policy and the
early administration of vasoactive drugs (terlipressin
somatostatin or a somatostatin analogue)45 IGV1
varices which often appear as a consequence of large
spontaneous splenorenal shunts may bleed with portal
pressure gradients lower than those needed for
esophageal varices It can then be hypothesized that
more powerful vasoconstrictors are needed not only
to decrease portal pressure but also to markedly
reduce portal and collateral blood 1047298ow to control acute
cardiofundal variceal bleeding In our experience
nearly 40 of patients with bleeding IGV1 who wereonly receiving vasoactive drugs require rescue therapy
mainly transjugular intrahepatic portosyst emic shunt
(TIPS) to achieve 5-day control of bleeding6 Therefore
we currently do not recommend using vasoactive drugs
alone but always with concomitant endoscopic therapy
Speci1047297c high-quality data on the use of endoscopic
therapy for acute GV bleeding are limited and in most
published RCTs only half of patients included in the trials
had cardiofundal varices Despite these limitations most
uncontrolled series report a high rate of control of
bleeding with the use of tissue adhesives such as CA
(gt
90) (Table 1) In addition small-size RCTs comparingtissue adhesives vs either endoscopic band ligation (EBL)
or endoscopic injection sclerot herapy (EIS) have shown
that tissue adhesives are equally7 or more89 effective than
EBL in the control of acute bleeding and more effective
than both in preventing rebleeding In addition tissue
adhesives perform better than sclerotherapy in
achieving initial hemostasis910 GOV1 varices are usually
treated as esophageal varices with EBL although some
investigators also recommend the use of tissue
adhesives for GOV1 varices11 Overall experts agree that
endoscopic therapy with tissue adhesives mainly CA is
the therapy of choice for acute bleeding from IGV1 and
GOV241213 If tissue adhesive is not available band
Figure 1 Sarinrsquos classi1047297cation of GV Modi1047297ed with permis-sion from the American Gastroenterological Association(AGA) Institute Gastroslides ndash Cirrhosis and PortalHypertension
Figure 2 A large gastric varix (IGV1) with a recent nipple sign
920 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 311
ligation seems to have some bene1047297t in small GOV2 varices
However no speci1047297c studies have evaluated this issue5
The standard protocol uses CA and lipiodol in 11ratio injecting with no more than 1 mL at the varix each
time14 (Supplementary Video) In most cases CA is
usually extruded into t he stomach lumen within 1ndash3
months after injection15 Multiple complications from CA
injection have been reported among published studies A
recent report of 753 patients indicated that most com-
plications occurred from rebleeding that was due to
extrusion of the glue cast (44) sepsis (13) distant
emboli (pulmonary cerebral splenic 07) gastric ulcer
formation (01) major gastric variceal bleeding (01)
and mesenteric hematoma associated with hemoper-
itoneum and bacterial peritonitis (01) The complica-tion-related mortality was 0516 Other studies have
reported a higher incidence of embolism that may occur
in up to 2ndash3 of cases1317
Combination therapy of endoscopy and pharmaco-
logic therapy is considered the st andard of care in acute
esophageal variceal bleeding45 However because of
the paucity of data it is unknown whether this
recommendation also applies to GOV2 or IGV1 variceal
bleeding Because in most cases drug therapy is
started before diagnostic endoscopy (and therefore
before the identi1047297cation of the gastric variceal origin
of bleeding) it seems the most rational approach is to
combine drug therapy plus endoscopic treatment
(preferably tissue adhesives) in patients with acute GV
bleeding
In massive bleeding with hemodynamic instabilityballoon tamponade can be used as a temporary ldquobridgerdquo
(for a maximum of 24 hours) until de1047297nitive treatment
can be instituted Tamponade may achieve hemostasis
in up to 80 of the patients although more than 50
of the cases rebleed af ter balloon de1047298ation A single
study from Teres et al18 comparing the LintonndashNachlas
vs the SengstakenndashBlakemore tube demonstrated that
LintonndashNachlas tube was more effective in fundal var-
iceal bleeding because of the large volume (600 mL) of
its single gastric balloon allowing an appropriate
compression of the fundal varices Nevertheless if the
Lintonndash
Nachlas balloon is not available compressionwith the gastric balloon of a SengstakenndashBlakemore
tube maximally in1047298ated may be appropriate
TIPS is considered the treatment of choice in patients
bleeding from GOV2 or IGV1 after failure to control initial
bleeding or rebleeding with combination therapy1920
Contrary to what is suggested in esophageal variceal
bleeding a second-attempt endoscopic therapy is
usually not considered Embolization of collaterals
feeding GV has been proposed to increase the ef 1047297cacy of
the TIPS procedure Two retrospective studies analyzed
the ef 1047297cacy of embolization combined with TIPS in acute
variceal bleeding Few patient s with cardiofundal
variceal bleeding (2121 and 3122 respectively) were
Table 1 Results of Published Studies on Endoscopic Treatment of Acute Bleeding From GV
First author year (reference) Design n
Treatmentreceived (n)
Initial control ( )overall (according
to treatment)
Mortality ( )overall (according to
treatment)Follow-up a
( mo )
Ogawa 199969 Retros 33 EIS (21) vs glue (12) 67 (53 vs 100) NR mdash
Kind 200070 Obs 174 Glue 97 64 36Huang 200071 Obs 90 Glue 100 40 36
Akahoshi 200272 Obs 52 Glue 96 30 12Rengstorff 200473 Pilot 25 Glue 100 12 11Mahadeva 200323 Obs 43 TIPS (20) vs
glue (23)93 (90 vs 96) 20 (25 vs 15) 6
Cheng 200730 Obs 146 Glue 95 10 36Mumtaz 200774 Obs 50 Glue 100 12 In-hospitalMarques 200828 Obs 48 Glue 88 44 18Paik 200875 Obs 121 Glue 91 12 1Procaccini 200944 Retros 105 TIPS (61) vs
glue (44)91 (90 vs 93) NR mdash
Monsanto 201276 Obs 97 Glue 96 9 In-hospitalOho 19959 RCT 53 EIS (24) vs
glue (29)81 (50 vs 88) 53 (67 vs 38) mdash
Lo 20018 RCT 26 EBL (11) vs glue (15) 69 (45 vs 87) 42 (48 vs 29) 24Sarin 200210 RCT 17 EIS (8) vs
glue (9)59 (38 vs 78) 18 (25 vs 11) 16
Tan 20067 RCT 97 EBL (48) vsglue (49)
93 (93 vs 93) 64 (63 vs 65) 36
Hou 200977 RCT 91 Glue (05 vs10 mL)
88 NR mdash
NOTE All the studies included IGV1 GOV1 and GOV2Obs observational study Retros retrospective comparative study aMedian
June 2014 Management of Gastric Varices 921
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 411
included No 1047297rm conclusions can be drawn from these
small studies However although evidence on the target
portal pressure gradient to be reached to prevent
rebleeding from fundal GV is not clear and it has been
suggested that fundal varices may rebleed despite a
portal pressure gradient slightly below 12 mm Hg the
small previous studies suggest that there is not a clear
rationale to perform embolization particularly if theportal pressure gradient after TIPS is reduced below 12
mm Hg
There is no RCT evaluating the use of TIPS as the
initial treatment to achieve hemostasis in patients with
IGV1 a cohort study suggested that it is highly effective
in achieving initial hemostasis in GOV1 and GOV2 vari-
ces23 A recent RCT showed that early (72 hours from
bleeding) polytetra1047298uoroethylene-coated TIPS can be
considered as a 1047297rst-line treatment in patients with
esophageal variceal bleeding at high risk of treatment
failure (de1047297ned by Child class C less than 14 points or
Child class B with active bleeding) because it reduces the
risk of treatment failure and improves survival in com-
parison with convent ional treatment with drugs plus
endoscopic therapy24 Although patients with GV were
excluded in the study it is likely that the bene1047297t of the
use of early TIPS may also apply to patients with GV and
the same high-risk criteria however this needs to be
studied further
Secondary Prophylaxis
Rebleeding rates after an acute GV bleeding episode
treated with tissue adhesives (mainly CA) range from7ndash65 with most of the large series reporting rates
below 15 Thus after initial hemostasis with tissue
adhesives repeated sessions are performed on a 2- to
4-week basis until endoscopic obliteration is achieved
Several case series and controlled studies have specif-
ically evaluated the effect of long-term injections
of tissue adhesives (mainly CA) to prevent GV
rebleeding1725ndash30 (Table 2) In most of these studies
eradication is achieved with 2ndash4 injections with a
volume ranging from 1ndash2 mL per session
Similar to what occurs with initial hemostasis CA
has been shown to be superior to both sclerotherapy
and band ligation for secondary prophylaxis On the
contrary comparison with nonselective beta-blockers
offers con1047298icting results In a small randomized study
41 patients who bled from esophageal (n frac14 31) or GV
(GOV 1 and GOV 2) (n frac14 10) treated initially with CA
were randomized to repeated CA injections (n frac14 21) or
propranolol (80ndash160 mg) (n frac14 20)31 No signi1047297cant
differences were observed between the 2 groups in theincidence of variceal rebleeding and death The inci-
dence of complications was higher in the CA group
(47 vs 10) A major limitation of the study was the
small number of patients with GV31 In a more recent
RCT 64 patients who bled from GV (54 GOV 2 and
10 IGV1) were allocated to receive either repeated CA
(n frac14 33) or propranolol (n frac14 34) for secondary pro-
phylaxis32 Rebleeding in the CA group was signi1047297cantly
lower than in the beta-blocker group (15 vs 55
P frac14 004) and after a 26-month follow-up the mortality
rate was lower as well (3 vs 25 P frac14 026) The rate
of complications in the CA group was 3
A recent report indicates that endoscopic ultraso-
nography (EUS)ndashguided therapy for fundal GV (IGV1 and
GOV2) with CA and 1047297bered coils may improve the ef 1047297-
cacy of this technique33 In this study 30 patients un-
derwent successful transesophageal EUS-guided therapy
of IGV1 and GOV2 The mean number of GV treated was
13 per patient and the mean volume of CA injected was
14 mL per varix GV were obliterated after a single
treatment session in the vast majority of patients (96)
who underwent follow-up endoscopy Rebleeding
occurred in 1 patient who was successfully treated with
a second session There were no procedure-related
complications Although this is a small series EUS-guidedtherapy seems to be a promising approach in selected
cases however more data are needed to consider it a
routine tool for the management of GV
Finally in a recent study 95 patients with GV (GOV2
n frac14 77 IGV1 n frac14 18) who bled and were successfully
treated with CA were assigned to receive treatment with
beta-blockers plus repeated CA (every 3ndash4 weeks until
the varices were obliterated) or repeated CA injections
alone34 After a mean follow-up of 19 months the overall
rebleeding (22 vs 26 patients P frac14 336) and survival
rates (22 vs 20 P frac14 936) were not different between the
2 groups One-year rebleeding free survival was also
Table 2 Results of Published Studies on Long-term Injection of Tissue Adhesives in the Prevention of GV Rebleeding
First author year (reference) n Eradicationhemostasis ( ) Rebleeding ( )
Follow-up(median) Survival ( ) Complications ( )
Rajoriya 201125 31 90 10 4 y 65 (1 y) 64Mishra 201032 33 100 10 26 mo 90 (2 y) 3Choudhuri 201026 108 89 10 307 thorn 172 mo NA NA Belletrutti 200827 34 84 12 11 mo 82 (1 y) 3Marqueacutes 200828 48 87 20 18 mo 56 (NA) 6Cheng 200730 613 77 8 25 mo 95 (1 y) 5Joo 200717 85 98 29 24 mo NA 35
922 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 511
similar (77 vs 765) The results of this study suggest
that contrary to what has been demonstrated for
esophageal variceal bleeding adding beta-blocker ther-
apy to repeated sessions of CA provides no important
bene1047297t for prevention of rebleeding and mortality in
patients with GV bleeding Despite these 1047297ndings and
because nonselective beta-blockers are effective in pa-
tients with concomitant esophageal varices until largerstudies with longer follow-up are available we still
recommend the use of nonselective beta-blockers as an
adjunct to endoscopic therapy in the prevention of GV
rebleeding
Other Endoscopic Therapies
Other endoscopic treatments have also been used to
prevent rebleeding Sclerotherapy has been abandoned
because of high rebleeding rates (50ndash90) Variceal
band ligation may be used for those patients with GOV1
and in some cases of small GOV2 and it is generallyperformed every 2 weeks until apparent endoscopic
obliteration However band ligation is limited by the fact
that it cannot be used in large GOV2 or IGV17 Detachable
loop snares to treat large GV (gt2 cm) along with pro-
pranolol have resulted in low rebleeding rates however
data are very scarce and the procedure is labor inten-
sive This approach has not been further evaluated and
has not been compared with other modalities and thus
cannot be routinely recommended
Thrombin
Thrombin converts 1047297brinogen to a 1047297brin clot thus
forming a clot inside the GV and occluding blood 1047298ow
The use of bovine thrombin was banned because of the
risk of potential prion transmission This is not the case
when using commercially available human thrombin
Each vial is reconstituted with 5 mL distilled water for a
concentration of 250 UmL35 The average dose of
injected thrombin ranges between 1500 and 2000 U
Available data indicate that thrombin is safe and effective
in the treatment of acute GV bleeding with hemostasis
rates of 70ndash100 however rebleeding rates may
range from 7ndash
5036ndash41
There are scarce data inregard to follow-up and eradication rates After initial
hemostasis repeated thrombin injections are
performed every 2ndash3 weeks until eradication Because
of the paucity of data mostly coming from case series
the routine use of thrombin cannot be routinely
recommended
Transjugular Intrahepatic PortosystemicShunt
The role of TIPS vs CA in preventing GV bleeding has
been evaluated in 3 small studies (2 retrospective
observational studies and 1 prospective) Remarkablyin all
3 studies most patients included had GOV1a fewGOV2 and
only anecdotal IGV1 varices In addition the stents used
were uncoated which hasbeen shownto be associatedwith
lower TIPS patency ef 1047297cacy and survival than coated
stents42 Two of these studies2343 showed a higher
rebleeding rate in the CA group (30 and 59) vs the
TIPS group (15 and 40) (Supplementary Table 1)Frequency of complications was similar in the 2 groups
but TIPS-treated patients showed a higher incidence of
hepatic encephalopathy234344 and long-term morbidity
requiring hospitalization44 than endoscopically treated
patients The studies found no signi1047297cant differences in
survival Mahadeva et al23 analyzed the costs after 6
months of therapy and found that CA injections were
more cost-effective than TIPS in a small group of 43
patients with GV bleeding In summary TIPS is a very
effective therapy to prevent GV rebleeding Nevertheless
because of the previously mentioned drawbacks more
data are needed to clarify the role of TIPS in the
secondary prophylaxis of GV bleeding and determine
whether this therapy must be universally applied or
reserved as a rescue therapy after failure of more
conservative approaches
Surgery
Surgery has currently fallen out of favor for patients
with portal hypertension because of the wide avail-
ability of less invasive techniques such as endoscopy
and interventional radiology In selected cases pa-
tients with GV and segmentalleft-sided portal hyper-
tension that is due to isolated splenic vein thrombosis
may be candidates for splenectomy or splenic emboli-
zation as a means of de1047297nitive therapy however data
are scarce
Balloon-occluded RetrogradeTransvenous Obliteration
Balloon-occluded retrograde transvenous obliteration
(BRTO) has been introduced as a treatment method that
aims to directly oblit erate the GV Since its introduction
by Kanagawa et al
45
BRTO has become widely acceptedin Japan and in some centers in the United States as a
minimally invasive and highly effective treatment for GV
The technical dif 1047297culty of BRTO relies on the anatomy of
the afferent and draining veins of the GV Accurate
assessment which is mainly based on imaging studies of
the variceal hemodynamic pattern is the most important
factor in ensuring successful treatment This anatomy
and how it alters the approach have been t horoughly
reviewed by Hirota et al46 Kiyosue et al4748 and
Al-Osaimi et al49
In most cases there is a gastrorenal or gastrocaval
shunt In this situation under 1047298uoroscopic guidance a
balloon catheter is inserted into the outlet of the
June 2014 Management of Gastric Varices 923
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 611
gastrorenal or gastrocaval shunt through a sheath placed
in the right femoral vein Immediately afterward
venography is performed with an injection of 10ndash15 mL
contrast medium via the in1047298ated balloon catheter and
GV are slowly intermitt ently and completely 1047297lled with
a sclerosant (Figure 3)454650ndash63 Thirty to 50 minutes
after the injection as much of the remaining sclerosant
as possible is aspirated via the catheter Finally the
balloon is de1047298ated and the catheter is withdrawn
Ethanolamine oleate is the predominant and traditional
sclerosant agent used in the BRTO procedure
particularly in Asia454650ndash60 Detergent sclerosants in a
foam or frot h have also been studied in both Japan
(polidocanol)6162 and the United States (3 STS)63
Figure 3 ( A ) Basic porto-systemic venous anatomyof GV with the classic gas-trorenal or splenorenalshunts ( B ) ConventionalBRTO procedure throughtransfemoral approach withballoon in the gastrorenalshunt IVC inferior venacava LGV left gastric veinLRV left renal vein MV
mesenteric vein PGVposterior gastric vein(s)PV main portal vein SGVshort gastric vein(s) SVsplenic vein Afferent vein( thin arrows ) Drainage vein( thick arrow )
924 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 711
The advantage of foam is that it reduces the sclerosant-
to-volume ratio requiring less sclerosant per procedure
In cases that involve complex types of afferent or
draining veins the use of additional techniques is required
for successful treatment These techniques include step-wise injection of the sclerosing agent selective injection of
the agent via a microcatheter coil embolization of the
afferent gastric veins double-balloon catheterization and
BRTO performed with percutaneous transhepatic portal
venous access or transileocolic venous access48
Epigastric and back pain (76)56 fever (26)5660
and transient hematuria (53) are the most common
complications of BRTO Bacterial peritonitis was found in
8 of patients in one study but t hese patients recovered
after only conservative therapy45 and this complication is
otherwise rarely mentioned in the literature Portal
(43) and renal vein thrombosis (5) can be found in asmall number of patients and bot h are usually clinically
silent465059 Pulmonary embolism59 pulmonary edema61
coil migration46 and anaphylaxis to ethanolamine oleate46
have also been reported
Technical success de1047297ned by complete obliteration of
the GV with sclerosant occurs in 77ndash100 of pa-
tients64 In some studies repeat BRTO was necessary to
achieve such high percentages465260 GV bleeding af t er a
successful BRTO ranges from 0ndash15465052555659ndash6165
or from 0ndash31666 when factoring in an intent-to-treat
basis (including technical failures) Some authors suggest
that BRTO might be better than TIPS67 or glue65 in the
prevention of GV bleeding However the fact that in
most patients treatment was administered as primary
prophylaxis for high-risk GV the studies had a small
sample size and the ef 1047297cacy of the comparative groups
(either TIPS or glue therapy) was poorer than expected
precludes de1047297nitive conclusions There is only a smallstudy54 that randomized 15 patients with acute GV
bleeding to receive TIPS (n frac14 7) or BRTO (n frac14 8)
without observing signi1047297cant differences in rebleeding
hepatic encephalopathy or survival
BRTO has the potential advantage of increasing portal
blood 1047298ow and potentially improving liver function525457
Therefore it may represent an alternative in patients who
may otherwise not tolerate TIPS59 In that regard in 4
studies including patients with hepatic encephalopathy
there was resolution or signi1047297cant reduction in
encephalopathy in all patients after BRTO46505158 By
contrast BRTO obliterates a spontaneous portosystemicshunt and therefore aggravates portal hypertension and
its related complications An increase in the size of
esophageal varices and the risk of esophageal variceal
bleeding after BRTO has been reported (between 73
and 27 after 1 year)525556 Other complications related
to the increase of portal hypertension after BRTO are the
development of portal hypertensive gastropathy (in 5ndash
13 of cases) ascites (0ndash44)65 and hydrothorax
pleural effusion (0ndash72) As a consequence of the
worsening of portal hypertension in some cases TIPS has
been performed after BRTO68
In conclusion although BRTO seems to be a feasible
technique that is able to successfully control and prevent
Figure 4 Suggested algo-rithm for management of GV EBL in small GV if tissue adhesives notavailable HE hepaticencephalopathy
June 2014 Management of Gastric Varices 925
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 811
GV bleeding there is a lack of good quality data to
routinely recommend BRTO in the management of GV In
our opinion BRTO could be considered in patients with
GV bleeding and large gastrorenal shunts in whom TIPS
may be contraindicated (such as those with refractory
hepatic encephalopathy or elderly patients)
Summary
The best management strategy for GV has not been
completely established because of a paucity of data of
RCTs in this area Speci1047297c treatments such as CA injec-
tion and BRTO are not widely available in all centers
Another limitation is the fact that tissue adhesives such
as CA are not approved by the Food and Drug Adminis-
tration in the United States and thus recommendations
arising from published studies guidelines and expert
opinion cannot be extrapolated to routine practice We
recommend a stepped care approach to the management
of GV as described in Figure 4 There are scarce data onthe role of CA or beta-blockers for primary prophylaxis
of GV bleeding and thus speci1047297c recommendations
cannot be made however patients should receive beta-
blockers if they have concomitant esophageal varices
After initial resuscitation and implementation of vaso-
constrictors and antibiotics endoscopic therapy with CA
should be the 1047297rst line of therapy if available After the
acute episode patients should receive beta-blockers
along with repeated sessions of CA injection if available
TIPS is very effective in controlling active GV bleeding
and for secondary prophylaxis However it carries a risk
of hepatic encephalopathy TIPS is the best treatment
strategy for patients who fail endoscopic therapy
Supplementary Material
Note To access the supplementary materials accom-
panying this article visit the online version of Clinical
Gastroenterology and Hepatology at wwwcghjournalorg
and at httpdxdoiorg101016jcgh201307015
References1 Sarin SK Lahoti D Saxena SP et al Prevalence classi1047297cation
and natural history of gastric varices a long-term follow-upstudy in 568 portal hypertension patients Hepatology 1992161343ndash1349
2 Kim T Shijo H Kokawa H et al Risk factors for hemorrhagefrom gastric fundal varices Hepatology 199725307ndash312
3 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric variceal bleeding comparing cyanoacrylate injection andbeta-blockers a randomized controlled trial J Hepatol 2011541161ndash1167
4 de Franchis R Revising consensus in portal hypertensionreport of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension J Hepatol 201053762ndash768
5 Garcia-Tsao G Sanyal AJ Grace ND et al Prevention andmanagement of gastroesophageal varices and variceal hemor-
rhage in cirrhosis Hepatology 200746922ndash938
6 Escorsell A Abraldes JG Pipa-Muntildeiz M et al Prognosis of acute bleeding from isolated fundal varices in patients withcirrhosis a European cohort Hepatology 201256(Suppl)748A
7 Tan PC Hou MC Lin HC et al A randomized trial of endoscopictreatment of acute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus band ligation Hepatology 200643690ndash697
8 Lo GH Lai KH Cheng JS et al A prospective randomized trial
of butyl cyanoacrylate injection versus band ligation in themanagement of bleeding gastric varices Hepatology 2001331060ndash1064
9 Oho K Iwao T Sumino M et al Ethanolamine oleate versusbutyl cyanoacrylate for bleeding gastric varices a non-randomized study Endoscopy 199527349ndash354
10 Sarin SK Jain AK Jain M et al A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolatedfundic varices Am J Gastroenterol 2002971010ndash1015
11 Lo GH Lai KH Should GOV1 be treated as for esophagealvarices Gastroenterology 20041271014ndash1015
12 Greenwald BD Caldwell SH Hespenheide EE et al N-2-butyl-cyanoacrylate for bleeding gastric varices a United States pilot
studyand cost analysis Am J Gastroenterol 2003981982ndash1988
13 Caldwell SH Hespenheide EE Greenwald BD et al Enbucrilatefor gastric varices extended experience in 92 patients AlimentPharmacol Ther 20072649ndash59
14 Seewald S Ang TL Imazu H et al A standardized injectiontechnique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundalvarices (with videos) Gastrointest Endosc 200868447ndash454
15 Wang YM Cheng LF Li N et al Study of glue extrusion after endoscopic N-butyl-2-cyanoacrylate injection on gastric vari-ceal bleeding World J Gastroenterol 2009154945ndash4951
16 Cheng LF Wang ZQ Li CZ et al Low incidence of complica-tions from endoscopic gastric variceal obturation with butyl
cyanoacrylate Clin Gastroenterol Hepatol 20108760ndash766
17 Joo HS Jang JY Eun SH et al [Long-term results of endo-scopic histoacryl (N-butyl-2-cyanoacrylate) injection for treat-ment of gastric varices a 10-year experience] Korean JGastroenterol 200749320ndash326
18 Teres J Cecilia A Bordas JM et al Esophageal tamponadefor bleeding varices controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube Gastroenterology197875566ndash569
19 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepatic portosystemic shunts gastric fundal compared withesophageal variceal bleeding Gastroenterology 1998114981ndash987
20 Azoulay D Castaing D Majno P et al Salvage transjugular intrahepatic portosystemic shunt for uncontrolled varicealbleeding in patients with decompensated cirrhosis J Hepatol200135590ndash597
21 Gaba RC Bui JT Cotler SJ et al Rebleeding rates followingTIPS forvariceal hemorrhage in the Viatorr era TIPS alone versusTIPS with variceal embolization Hepatol Int 20104749ndash756
22 Xiao T Chen L Chen W et al Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone versus TIPScombined with embolotherapy in advanced cirrhosis a retro-spective study J Clin Gastroenterol 201145643ndash650
23 Mahadeva S Bellamy MC Kessel D et al Cost-effectivenessof N-butyl-2-cyanoacrylate (histoacryl) glue injections versus trans-
jugular intrahepatic portosystemic shunt in the management of
926 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
Edso nGuzman FirmadodigitalmenteporEdso nGuzmanNombredereconocimiento(D N)cn=EdsonGuzmanoou=HNERMemail=e dson_guzmanhotmailcomc=PEFecha20140526200159-050 0
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 311
ligation seems to have some bene1047297t in small GOV2 varices
However no speci1047297c studies have evaluated this issue5
The standard protocol uses CA and lipiodol in 11ratio injecting with no more than 1 mL at the varix each
time14 (Supplementary Video) In most cases CA is
usually extruded into t he stomach lumen within 1ndash3
months after injection15 Multiple complications from CA
injection have been reported among published studies A
recent report of 753 patients indicated that most com-
plications occurred from rebleeding that was due to
extrusion of the glue cast (44) sepsis (13) distant
emboli (pulmonary cerebral splenic 07) gastric ulcer
formation (01) major gastric variceal bleeding (01)
and mesenteric hematoma associated with hemoper-
itoneum and bacterial peritonitis (01) The complica-tion-related mortality was 0516 Other studies have
reported a higher incidence of embolism that may occur
in up to 2ndash3 of cases1317
Combination therapy of endoscopy and pharmaco-
logic therapy is considered the st andard of care in acute
esophageal variceal bleeding45 However because of
the paucity of data it is unknown whether this
recommendation also applies to GOV2 or IGV1 variceal
bleeding Because in most cases drug therapy is
started before diagnostic endoscopy (and therefore
before the identi1047297cation of the gastric variceal origin
of bleeding) it seems the most rational approach is to
combine drug therapy plus endoscopic treatment
(preferably tissue adhesives) in patients with acute GV
bleeding
In massive bleeding with hemodynamic instabilityballoon tamponade can be used as a temporary ldquobridgerdquo
(for a maximum of 24 hours) until de1047297nitive treatment
can be instituted Tamponade may achieve hemostasis
in up to 80 of the patients although more than 50
of the cases rebleed af ter balloon de1047298ation A single
study from Teres et al18 comparing the LintonndashNachlas
vs the SengstakenndashBlakemore tube demonstrated that
LintonndashNachlas tube was more effective in fundal var-
iceal bleeding because of the large volume (600 mL) of
its single gastric balloon allowing an appropriate
compression of the fundal varices Nevertheless if the
Lintonndash
Nachlas balloon is not available compressionwith the gastric balloon of a SengstakenndashBlakemore
tube maximally in1047298ated may be appropriate
TIPS is considered the treatment of choice in patients
bleeding from GOV2 or IGV1 after failure to control initial
bleeding or rebleeding with combination therapy1920
Contrary to what is suggested in esophageal variceal
bleeding a second-attempt endoscopic therapy is
usually not considered Embolization of collaterals
feeding GV has been proposed to increase the ef 1047297cacy of
the TIPS procedure Two retrospective studies analyzed
the ef 1047297cacy of embolization combined with TIPS in acute
variceal bleeding Few patient s with cardiofundal
variceal bleeding (2121 and 3122 respectively) were
Table 1 Results of Published Studies on Endoscopic Treatment of Acute Bleeding From GV
First author year (reference) Design n
Treatmentreceived (n)
Initial control ( )overall (according
to treatment)
Mortality ( )overall (according to
treatment)Follow-up a
( mo )
Ogawa 199969 Retros 33 EIS (21) vs glue (12) 67 (53 vs 100) NR mdash
Kind 200070 Obs 174 Glue 97 64 36Huang 200071 Obs 90 Glue 100 40 36
Akahoshi 200272 Obs 52 Glue 96 30 12Rengstorff 200473 Pilot 25 Glue 100 12 11Mahadeva 200323 Obs 43 TIPS (20) vs
glue (23)93 (90 vs 96) 20 (25 vs 15) 6
Cheng 200730 Obs 146 Glue 95 10 36Mumtaz 200774 Obs 50 Glue 100 12 In-hospitalMarques 200828 Obs 48 Glue 88 44 18Paik 200875 Obs 121 Glue 91 12 1Procaccini 200944 Retros 105 TIPS (61) vs
glue (44)91 (90 vs 93) NR mdash
Monsanto 201276 Obs 97 Glue 96 9 In-hospitalOho 19959 RCT 53 EIS (24) vs
glue (29)81 (50 vs 88) 53 (67 vs 38) mdash
Lo 20018 RCT 26 EBL (11) vs glue (15) 69 (45 vs 87) 42 (48 vs 29) 24Sarin 200210 RCT 17 EIS (8) vs
glue (9)59 (38 vs 78) 18 (25 vs 11) 16
Tan 20067 RCT 97 EBL (48) vsglue (49)
93 (93 vs 93) 64 (63 vs 65) 36
Hou 200977 RCT 91 Glue (05 vs10 mL)
88 NR mdash
NOTE All the studies included IGV1 GOV1 and GOV2Obs observational study Retros retrospective comparative study aMedian
June 2014 Management of Gastric Varices 921
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 411
included No 1047297rm conclusions can be drawn from these
small studies However although evidence on the target
portal pressure gradient to be reached to prevent
rebleeding from fundal GV is not clear and it has been
suggested that fundal varices may rebleed despite a
portal pressure gradient slightly below 12 mm Hg the
small previous studies suggest that there is not a clear
rationale to perform embolization particularly if theportal pressure gradient after TIPS is reduced below 12
mm Hg
There is no RCT evaluating the use of TIPS as the
initial treatment to achieve hemostasis in patients with
IGV1 a cohort study suggested that it is highly effective
in achieving initial hemostasis in GOV1 and GOV2 vari-
ces23 A recent RCT showed that early (72 hours from
bleeding) polytetra1047298uoroethylene-coated TIPS can be
considered as a 1047297rst-line treatment in patients with
esophageal variceal bleeding at high risk of treatment
failure (de1047297ned by Child class C less than 14 points or
Child class B with active bleeding) because it reduces the
risk of treatment failure and improves survival in com-
parison with convent ional treatment with drugs plus
endoscopic therapy24 Although patients with GV were
excluded in the study it is likely that the bene1047297t of the
use of early TIPS may also apply to patients with GV and
the same high-risk criteria however this needs to be
studied further
Secondary Prophylaxis
Rebleeding rates after an acute GV bleeding episode
treated with tissue adhesives (mainly CA) range from7ndash65 with most of the large series reporting rates
below 15 Thus after initial hemostasis with tissue
adhesives repeated sessions are performed on a 2- to
4-week basis until endoscopic obliteration is achieved
Several case series and controlled studies have specif-
ically evaluated the effect of long-term injections
of tissue adhesives (mainly CA) to prevent GV
rebleeding1725ndash30 (Table 2) In most of these studies
eradication is achieved with 2ndash4 injections with a
volume ranging from 1ndash2 mL per session
Similar to what occurs with initial hemostasis CA
has been shown to be superior to both sclerotherapy
and band ligation for secondary prophylaxis On the
contrary comparison with nonselective beta-blockers
offers con1047298icting results In a small randomized study
41 patients who bled from esophageal (n frac14 31) or GV
(GOV 1 and GOV 2) (n frac14 10) treated initially with CA
were randomized to repeated CA injections (n frac14 21) or
propranolol (80ndash160 mg) (n frac14 20)31 No signi1047297cant
differences were observed between the 2 groups in theincidence of variceal rebleeding and death The inci-
dence of complications was higher in the CA group
(47 vs 10) A major limitation of the study was the
small number of patients with GV31 In a more recent
RCT 64 patients who bled from GV (54 GOV 2 and
10 IGV1) were allocated to receive either repeated CA
(n frac14 33) or propranolol (n frac14 34) for secondary pro-
phylaxis32 Rebleeding in the CA group was signi1047297cantly
lower than in the beta-blocker group (15 vs 55
P frac14 004) and after a 26-month follow-up the mortality
rate was lower as well (3 vs 25 P frac14 026) The rate
of complications in the CA group was 3
A recent report indicates that endoscopic ultraso-
nography (EUS)ndashguided therapy for fundal GV (IGV1 and
GOV2) with CA and 1047297bered coils may improve the ef 1047297-
cacy of this technique33 In this study 30 patients un-
derwent successful transesophageal EUS-guided therapy
of IGV1 and GOV2 The mean number of GV treated was
13 per patient and the mean volume of CA injected was
14 mL per varix GV were obliterated after a single
treatment session in the vast majority of patients (96)
who underwent follow-up endoscopy Rebleeding
occurred in 1 patient who was successfully treated with
a second session There were no procedure-related
complications Although this is a small series EUS-guidedtherapy seems to be a promising approach in selected
cases however more data are needed to consider it a
routine tool for the management of GV
Finally in a recent study 95 patients with GV (GOV2
n frac14 77 IGV1 n frac14 18) who bled and were successfully
treated with CA were assigned to receive treatment with
beta-blockers plus repeated CA (every 3ndash4 weeks until
the varices were obliterated) or repeated CA injections
alone34 After a mean follow-up of 19 months the overall
rebleeding (22 vs 26 patients P frac14 336) and survival
rates (22 vs 20 P frac14 936) were not different between the
2 groups One-year rebleeding free survival was also
Table 2 Results of Published Studies on Long-term Injection of Tissue Adhesives in the Prevention of GV Rebleeding
First author year (reference) n Eradicationhemostasis ( ) Rebleeding ( )
Follow-up(median) Survival ( ) Complications ( )
Rajoriya 201125 31 90 10 4 y 65 (1 y) 64Mishra 201032 33 100 10 26 mo 90 (2 y) 3Choudhuri 201026 108 89 10 307 thorn 172 mo NA NA Belletrutti 200827 34 84 12 11 mo 82 (1 y) 3Marqueacutes 200828 48 87 20 18 mo 56 (NA) 6Cheng 200730 613 77 8 25 mo 95 (1 y) 5Joo 200717 85 98 29 24 mo NA 35
922 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 511
similar (77 vs 765) The results of this study suggest
that contrary to what has been demonstrated for
esophageal variceal bleeding adding beta-blocker ther-
apy to repeated sessions of CA provides no important
bene1047297t for prevention of rebleeding and mortality in
patients with GV bleeding Despite these 1047297ndings and
because nonselective beta-blockers are effective in pa-
tients with concomitant esophageal varices until largerstudies with longer follow-up are available we still
recommend the use of nonselective beta-blockers as an
adjunct to endoscopic therapy in the prevention of GV
rebleeding
Other Endoscopic Therapies
Other endoscopic treatments have also been used to
prevent rebleeding Sclerotherapy has been abandoned
because of high rebleeding rates (50ndash90) Variceal
band ligation may be used for those patients with GOV1
and in some cases of small GOV2 and it is generallyperformed every 2 weeks until apparent endoscopic
obliteration However band ligation is limited by the fact
that it cannot be used in large GOV2 or IGV17 Detachable
loop snares to treat large GV (gt2 cm) along with pro-
pranolol have resulted in low rebleeding rates however
data are very scarce and the procedure is labor inten-
sive This approach has not been further evaluated and
has not been compared with other modalities and thus
cannot be routinely recommended
Thrombin
Thrombin converts 1047297brinogen to a 1047297brin clot thus
forming a clot inside the GV and occluding blood 1047298ow
The use of bovine thrombin was banned because of the
risk of potential prion transmission This is not the case
when using commercially available human thrombin
Each vial is reconstituted with 5 mL distilled water for a
concentration of 250 UmL35 The average dose of
injected thrombin ranges between 1500 and 2000 U
Available data indicate that thrombin is safe and effective
in the treatment of acute GV bleeding with hemostasis
rates of 70ndash100 however rebleeding rates may
range from 7ndash
5036ndash41
There are scarce data inregard to follow-up and eradication rates After initial
hemostasis repeated thrombin injections are
performed every 2ndash3 weeks until eradication Because
of the paucity of data mostly coming from case series
the routine use of thrombin cannot be routinely
recommended
Transjugular Intrahepatic PortosystemicShunt
The role of TIPS vs CA in preventing GV bleeding has
been evaluated in 3 small studies (2 retrospective
observational studies and 1 prospective) Remarkablyin all
3 studies most patients included had GOV1a fewGOV2 and
only anecdotal IGV1 varices In addition the stents used
were uncoated which hasbeen shownto be associatedwith
lower TIPS patency ef 1047297cacy and survival than coated
stents42 Two of these studies2343 showed a higher
rebleeding rate in the CA group (30 and 59) vs the
TIPS group (15 and 40) (Supplementary Table 1)Frequency of complications was similar in the 2 groups
but TIPS-treated patients showed a higher incidence of
hepatic encephalopathy234344 and long-term morbidity
requiring hospitalization44 than endoscopically treated
patients The studies found no signi1047297cant differences in
survival Mahadeva et al23 analyzed the costs after 6
months of therapy and found that CA injections were
more cost-effective than TIPS in a small group of 43
patients with GV bleeding In summary TIPS is a very
effective therapy to prevent GV rebleeding Nevertheless
because of the previously mentioned drawbacks more
data are needed to clarify the role of TIPS in the
secondary prophylaxis of GV bleeding and determine
whether this therapy must be universally applied or
reserved as a rescue therapy after failure of more
conservative approaches
Surgery
Surgery has currently fallen out of favor for patients
with portal hypertension because of the wide avail-
ability of less invasive techniques such as endoscopy
and interventional radiology In selected cases pa-
tients with GV and segmentalleft-sided portal hyper-
tension that is due to isolated splenic vein thrombosis
may be candidates for splenectomy or splenic emboli-
zation as a means of de1047297nitive therapy however data
are scarce
Balloon-occluded RetrogradeTransvenous Obliteration
Balloon-occluded retrograde transvenous obliteration
(BRTO) has been introduced as a treatment method that
aims to directly oblit erate the GV Since its introduction
by Kanagawa et al
45
BRTO has become widely acceptedin Japan and in some centers in the United States as a
minimally invasive and highly effective treatment for GV
The technical dif 1047297culty of BRTO relies on the anatomy of
the afferent and draining veins of the GV Accurate
assessment which is mainly based on imaging studies of
the variceal hemodynamic pattern is the most important
factor in ensuring successful treatment This anatomy
and how it alters the approach have been t horoughly
reviewed by Hirota et al46 Kiyosue et al4748 and
Al-Osaimi et al49
In most cases there is a gastrorenal or gastrocaval
shunt In this situation under 1047298uoroscopic guidance a
balloon catheter is inserted into the outlet of the
June 2014 Management of Gastric Varices 923
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 611
gastrorenal or gastrocaval shunt through a sheath placed
in the right femoral vein Immediately afterward
venography is performed with an injection of 10ndash15 mL
contrast medium via the in1047298ated balloon catheter and
GV are slowly intermitt ently and completely 1047297lled with
a sclerosant (Figure 3)454650ndash63 Thirty to 50 minutes
after the injection as much of the remaining sclerosant
as possible is aspirated via the catheter Finally the
balloon is de1047298ated and the catheter is withdrawn
Ethanolamine oleate is the predominant and traditional
sclerosant agent used in the BRTO procedure
particularly in Asia454650ndash60 Detergent sclerosants in a
foam or frot h have also been studied in both Japan
(polidocanol)6162 and the United States (3 STS)63
Figure 3 ( A ) Basic porto-systemic venous anatomyof GV with the classic gas-trorenal or splenorenalshunts ( B ) ConventionalBRTO procedure throughtransfemoral approach withballoon in the gastrorenalshunt IVC inferior venacava LGV left gastric veinLRV left renal vein MV
mesenteric vein PGVposterior gastric vein(s)PV main portal vein SGVshort gastric vein(s) SVsplenic vein Afferent vein( thin arrows ) Drainage vein( thick arrow )
924 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 711
The advantage of foam is that it reduces the sclerosant-
to-volume ratio requiring less sclerosant per procedure
In cases that involve complex types of afferent or
draining veins the use of additional techniques is required
for successful treatment These techniques include step-wise injection of the sclerosing agent selective injection of
the agent via a microcatheter coil embolization of the
afferent gastric veins double-balloon catheterization and
BRTO performed with percutaneous transhepatic portal
venous access or transileocolic venous access48
Epigastric and back pain (76)56 fever (26)5660
and transient hematuria (53) are the most common
complications of BRTO Bacterial peritonitis was found in
8 of patients in one study but t hese patients recovered
after only conservative therapy45 and this complication is
otherwise rarely mentioned in the literature Portal
(43) and renal vein thrombosis (5) can be found in asmall number of patients and bot h are usually clinically
silent465059 Pulmonary embolism59 pulmonary edema61
coil migration46 and anaphylaxis to ethanolamine oleate46
have also been reported
Technical success de1047297ned by complete obliteration of
the GV with sclerosant occurs in 77ndash100 of pa-
tients64 In some studies repeat BRTO was necessary to
achieve such high percentages465260 GV bleeding af t er a
successful BRTO ranges from 0ndash15465052555659ndash6165
or from 0ndash31666 when factoring in an intent-to-treat
basis (including technical failures) Some authors suggest
that BRTO might be better than TIPS67 or glue65 in the
prevention of GV bleeding However the fact that in
most patients treatment was administered as primary
prophylaxis for high-risk GV the studies had a small
sample size and the ef 1047297cacy of the comparative groups
(either TIPS or glue therapy) was poorer than expected
precludes de1047297nitive conclusions There is only a smallstudy54 that randomized 15 patients with acute GV
bleeding to receive TIPS (n frac14 7) or BRTO (n frac14 8)
without observing signi1047297cant differences in rebleeding
hepatic encephalopathy or survival
BRTO has the potential advantage of increasing portal
blood 1047298ow and potentially improving liver function525457
Therefore it may represent an alternative in patients who
may otherwise not tolerate TIPS59 In that regard in 4
studies including patients with hepatic encephalopathy
there was resolution or signi1047297cant reduction in
encephalopathy in all patients after BRTO46505158 By
contrast BRTO obliterates a spontaneous portosystemicshunt and therefore aggravates portal hypertension and
its related complications An increase in the size of
esophageal varices and the risk of esophageal variceal
bleeding after BRTO has been reported (between 73
and 27 after 1 year)525556 Other complications related
to the increase of portal hypertension after BRTO are the
development of portal hypertensive gastropathy (in 5ndash
13 of cases) ascites (0ndash44)65 and hydrothorax
pleural effusion (0ndash72) As a consequence of the
worsening of portal hypertension in some cases TIPS has
been performed after BRTO68
In conclusion although BRTO seems to be a feasible
technique that is able to successfully control and prevent
Figure 4 Suggested algo-rithm for management of GV EBL in small GV if tissue adhesives notavailable HE hepaticencephalopathy
June 2014 Management of Gastric Varices 925
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 811
GV bleeding there is a lack of good quality data to
routinely recommend BRTO in the management of GV In
our opinion BRTO could be considered in patients with
GV bleeding and large gastrorenal shunts in whom TIPS
may be contraindicated (such as those with refractory
hepatic encephalopathy or elderly patients)
Summary
The best management strategy for GV has not been
completely established because of a paucity of data of
RCTs in this area Speci1047297c treatments such as CA injec-
tion and BRTO are not widely available in all centers
Another limitation is the fact that tissue adhesives such
as CA are not approved by the Food and Drug Adminis-
tration in the United States and thus recommendations
arising from published studies guidelines and expert
opinion cannot be extrapolated to routine practice We
recommend a stepped care approach to the management
of GV as described in Figure 4 There are scarce data onthe role of CA or beta-blockers for primary prophylaxis
of GV bleeding and thus speci1047297c recommendations
cannot be made however patients should receive beta-
blockers if they have concomitant esophageal varices
After initial resuscitation and implementation of vaso-
constrictors and antibiotics endoscopic therapy with CA
should be the 1047297rst line of therapy if available After the
acute episode patients should receive beta-blockers
along with repeated sessions of CA injection if available
TIPS is very effective in controlling active GV bleeding
and for secondary prophylaxis However it carries a risk
of hepatic encephalopathy TIPS is the best treatment
strategy for patients who fail endoscopic therapy
Supplementary Material
Note To access the supplementary materials accom-
panying this article visit the online version of Clinical
Gastroenterology and Hepatology at wwwcghjournalorg
and at httpdxdoiorg101016jcgh201307015
References1 Sarin SK Lahoti D Saxena SP et al Prevalence classi1047297cation
and natural history of gastric varices a long-term follow-upstudy in 568 portal hypertension patients Hepatology 1992161343ndash1349
2 Kim T Shijo H Kokawa H et al Risk factors for hemorrhagefrom gastric fundal varices Hepatology 199725307ndash312
3 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric variceal bleeding comparing cyanoacrylate injection andbeta-blockers a randomized controlled trial J Hepatol 2011541161ndash1167
4 de Franchis R Revising consensus in portal hypertensionreport of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension J Hepatol 201053762ndash768
5 Garcia-Tsao G Sanyal AJ Grace ND et al Prevention andmanagement of gastroesophageal varices and variceal hemor-
rhage in cirrhosis Hepatology 200746922ndash938
6 Escorsell A Abraldes JG Pipa-Muntildeiz M et al Prognosis of acute bleeding from isolated fundal varices in patients withcirrhosis a European cohort Hepatology 201256(Suppl)748A
7 Tan PC Hou MC Lin HC et al A randomized trial of endoscopictreatment of acute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus band ligation Hepatology 200643690ndash697
8 Lo GH Lai KH Cheng JS et al A prospective randomized trial
of butyl cyanoacrylate injection versus band ligation in themanagement of bleeding gastric varices Hepatology 2001331060ndash1064
9 Oho K Iwao T Sumino M et al Ethanolamine oleate versusbutyl cyanoacrylate for bleeding gastric varices a non-randomized study Endoscopy 199527349ndash354
10 Sarin SK Jain AK Jain M et al A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolatedfundic varices Am J Gastroenterol 2002971010ndash1015
11 Lo GH Lai KH Should GOV1 be treated as for esophagealvarices Gastroenterology 20041271014ndash1015
12 Greenwald BD Caldwell SH Hespenheide EE et al N-2-butyl-cyanoacrylate for bleeding gastric varices a United States pilot
studyand cost analysis Am J Gastroenterol 2003981982ndash1988
13 Caldwell SH Hespenheide EE Greenwald BD et al Enbucrilatefor gastric varices extended experience in 92 patients AlimentPharmacol Ther 20072649ndash59
14 Seewald S Ang TL Imazu H et al A standardized injectiontechnique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundalvarices (with videos) Gastrointest Endosc 200868447ndash454
15 Wang YM Cheng LF Li N et al Study of glue extrusion after endoscopic N-butyl-2-cyanoacrylate injection on gastric vari-ceal bleeding World J Gastroenterol 2009154945ndash4951
16 Cheng LF Wang ZQ Li CZ et al Low incidence of complica-tions from endoscopic gastric variceal obturation with butyl
cyanoacrylate Clin Gastroenterol Hepatol 20108760ndash766
17 Joo HS Jang JY Eun SH et al [Long-term results of endo-scopic histoacryl (N-butyl-2-cyanoacrylate) injection for treat-ment of gastric varices a 10-year experience] Korean JGastroenterol 200749320ndash326
18 Teres J Cecilia A Bordas JM et al Esophageal tamponadefor bleeding varices controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube Gastroenterology197875566ndash569
19 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepatic portosystemic shunts gastric fundal compared withesophageal variceal bleeding Gastroenterology 1998114981ndash987
20 Azoulay D Castaing D Majno P et al Salvage transjugular intrahepatic portosystemic shunt for uncontrolled varicealbleeding in patients with decompensated cirrhosis J Hepatol200135590ndash597
21 Gaba RC Bui JT Cotler SJ et al Rebleeding rates followingTIPS forvariceal hemorrhage in the Viatorr era TIPS alone versusTIPS with variceal embolization Hepatol Int 20104749ndash756
22 Xiao T Chen L Chen W et al Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone versus TIPScombined with embolotherapy in advanced cirrhosis a retro-spective study J Clin Gastroenterol 201145643ndash650
23 Mahadeva S Bellamy MC Kessel D et al Cost-effectivenessof N-butyl-2-cyanoacrylate (histoacryl) glue injections versus trans-
jugular intrahepatic portosystemic shunt in the management of
926 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
Edso nGuzman FirmadodigitalmenteporEdso nGuzmanNombredereconocimiento(D N)cn=EdsonGuzmanoou=HNERMemail=e dson_guzmanhotmailcomc=PEFecha20140526200159-050 0
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 411
included No 1047297rm conclusions can be drawn from these
small studies However although evidence on the target
portal pressure gradient to be reached to prevent
rebleeding from fundal GV is not clear and it has been
suggested that fundal varices may rebleed despite a
portal pressure gradient slightly below 12 mm Hg the
small previous studies suggest that there is not a clear
rationale to perform embolization particularly if theportal pressure gradient after TIPS is reduced below 12
mm Hg
There is no RCT evaluating the use of TIPS as the
initial treatment to achieve hemostasis in patients with
IGV1 a cohort study suggested that it is highly effective
in achieving initial hemostasis in GOV1 and GOV2 vari-
ces23 A recent RCT showed that early (72 hours from
bleeding) polytetra1047298uoroethylene-coated TIPS can be
considered as a 1047297rst-line treatment in patients with
esophageal variceal bleeding at high risk of treatment
failure (de1047297ned by Child class C less than 14 points or
Child class B with active bleeding) because it reduces the
risk of treatment failure and improves survival in com-
parison with convent ional treatment with drugs plus
endoscopic therapy24 Although patients with GV were
excluded in the study it is likely that the bene1047297t of the
use of early TIPS may also apply to patients with GV and
the same high-risk criteria however this needs to be
studied further
Secondary Prophylaxis
Rebleeding rates after an acute GV bleeding episode
treated with tissue adhesives (mainly CA) range from7ndash65 with most of the large series reporting rates
below 15 Thus after initial hemostasis with tissue
adhesives repeated sessions are performed on a 2- to
4-week basis until endoscopic obliteration is achieved
Several case series and controlled studies have specif-
ically evaluated the effect of long-term injections
of tissue adhesives (mainly CA) to prevent GV
rebleeding1725ndash30 (Table 2) In most of these studies
eradication is achieved with 2ndash4 injections with a
volume ranging from 1ndash2 mL per session
Similar to what occurs with initial hemostasis CA
has been shown to be superior to both sclerotherapy
and band ligation for secondary prophylaxis On the
contrary comparison with nonselective beta-blockers
offers con1047298icting results In a small randomized study
41 patients who bled from esophageal (n frac14 31) or GV
(GOV 1 and GOV 2) (n frac14 10) treated initially with CA
were randomized to repeated CA injections (n frac14 21) or
propranolol (80ndash160 mg) (n frac14 20)31 No signi1047297cant
differences were observed between the 2 groups in theincidence of variceal rebleeding and death The inci-
dence of complications was higher in the CA group
(47 vs 10) A major limitation of the study was the
small number of patients with GV31 In a more recent
RCT 64 patients who bled from GV (54 GOV 2 and
10 IGV1) were allocated to receive either repeated CA
(n frac14 33) or propranolol (n frac14 34) for secondary pro-
phylaxis32 Rebleeding in the CA group was signi1047297cantly
lower than in the beta-blocker group (15 vs 55
P frac14 004) and after a 26-month follow-up the mortality
rate was lower as well (3 vs 25 P frac14 026) The rate
of complications in the CA group was 3
A recent report indicates that endoscopic ultraso-
nography (EUS)ndashguided therapy for fundal GV (IGV1 and
GOV2) with CA and 1047297bered coils may improve the ef 1047297-
cacy of this technique33 In this study 30 patients un-
derwent successful transesophageal EUS-guided therapy
of IGV1 and GOV2 The mean number of GV treated was
13 per patient and the mean volume of CA injected was
14 mL per varix GV were obliterated after a single
treatment session in the vast majority of patients (96)
who underwent follow-up endoscopy Rebleeding
occurred in 1 patient who was successfully treated with
a second session There were no procedure-related
complications Although this is a small series EUS-guidedtherapy seems to be a promising approach in selected
cases however more data are needed to consider it a
routine tool for the management of GV
Finally in a recent study 95 patients with GV (GOV2
n frac14 77 IGV1 n frac14 18) who bled and were successfully
treated with CA were assigned to receive treatment with
beta-blockers plus repeated CA (every 3ndash4 weeks until
the varices were obliterated) or repeated CA injections
alone34 After a mean follow-up of 19 months the overall
rebleeding (22 vs 26 patients P frac14 336) and survival
rates (22 vs 20 P frac14 936) were not different between the
2 groups One-year rebleeding free survival was also
Table 2 Results of Published Studies on Long-term Injection of Tissue Adhesives in the Prevention of GV Rebleeding
First author year (reference) n Eradicationhemostasis ( ) Rebleeding ( )
Follow-up(median) Survival ( ) Complications ( )
Rajoriya 201125 31 90 10 4 y 65 (1 y) 64Mishra 201032 33 100 10 26 mo 90 (2 y) 3Choudhuri 201026 108 89 10 307 thorn 172 mo NA NA Belletrutti 200827 34 84 12 11 mo 82 (1 y) 3Marqueacutes 200828 48 87 20 18 mo 56 (NA) 6Cheng 200730 613 77 8 25 mo 95 (1 y) 5Joo 200717 85 98 29 24 mo NA 35
922 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 511
similar (77 vs 765) The results of this study suggest
that contrary to what has been demonstrated for
esophageal variceal bleeding adding beta-blocker ther-
apy to repeated sessions of CA provides no important
bene1047297t for prevention of rebleeding and mortality in
patients with GV bleeding Despite these 1047297ndings and
because nonselective beta-blockers are effective in pa-
tients with concomitant esophageal varices until largerstudies with longer follow-up are available we still
recommend the use of nonselective beta-blockers as an
adjunct to endoscopic therapy in the prevention of GV
rebleeding
Other Endoscopic Therapies
Other endoscopic treatments have also been used to
prevent rebleeding Sclerotherapy has been abandoned
because of high rebleeding rates (50ndash90) Variceal
band ligation may be used for those patients with GOV1
and in some cases of small GOV2 and it is generallyperformed every 2 weeks until apparent endoscopic
obliteration However band ligation is limited by the fact
that it cannot be used in large GOV2 or IGV17 Detachable
loop snares to treat large GV (gt2 cm) along with pro-
pranolol have resulted in low rebleeding rates however
data are very scarce and the procedure is labor inten-
sive This approach has not been further evaluated and
has not been compared with other modalities and thus
cannot be routinely recommended
Thrombin
Thrombin converts 1047297brinogen to a 1047297brin clot thus
forming a clot inside the GV and occluding blood 1047298ow
The use of bovine thrombin was banned because of the
risk of potential prion transmission This is not the case
when using commercially available human thrombin
Each vial is reconstituted with 5 mL distilled water for a
concentration of 250 UmL35 The average dose of
injected thrombin ranges between 1500 and 2000 U
Available data indicate that thrombin is safe and effective
in the treatment of acute GV bleeding with hemostasis
rates of 70ndash100 however rebleeding rates may
range from 7ndash
5036ndash41
There are scarce data inregard to follow-up and eradication rates After initial
hemostasis repeated thrombin injections are
performed every 2ndash3 weeks until eradication Because
of the paucity of data mostly coming from case series
the routine use of thrombin cannot be routinely
recommended
Transjugular Intrahepatic PortosystemicShunt
The role of TIPS vs CA in preventing GV bleeding has
been evaluated in 3 small studies (2 retrospective
observational studies and 1 prospective) Remarkablyin all
3 studies most patients included had GOV1a fewGOV2 and
only anecdotal IGV1 varices In addition the stents used
were uncoated which hasbeen shownto be associatedwith
lower TIPS patency ef 1047297cacy and survival than coated
stents42 Two of these studies2343 showed a higher
rebleeding rate in the CA group (30 and 59) vs the
TIPS group (15 and 40) (Supplementary Table 1)Frequency of complications was similar in the 2 groups
but TIPS-treated patients showed a higher incidence of
hepatic encephalopathy234344 and long-term morbidity
requiring hospitalization44 than endoscopically treated
patients The studies found no signi1047297cant differences in
survival Mahadeva et al23 analyzed the costs after 6
months of therapy and found that CA injections were
more cost-effective than TIPS in a small group of 43
patients with GV bleeding In summary TIPS is a very
effective therapy to prevent GV rebleeding Nevertheless
because of the previously mentioned drawbacks more
data are needed to clarify the role of TIPS in the
secondary prophylaxis of GV bleeding and determine
whether this therapy must be universally applied or
reserved as a rescue therapy after failure of more
conservative approaches
Surgery
Surgery has currently fallen out of favor for patients
with portal hypertension because of the wide avail-
ability of less invasive techniques such as endoscopy
and interventional radiology In selected cases pa-
tients with GV and segmentalleft-sided portal hyper-
tension that is due to isolated splenic vein thrombosis
may be candidates for splenectomy or splenic emboli-
zation as a means of de1047297nitive therapy however data
are scarce
Balloon-occluded RetrogradeTransvenous Obliteration
Balloon-occluded retrograde transvenous obliteration
(BRTO) has been introduced as a treatment method that
aims to directly oblit erate the GV Since its introduction
by Kanagawa et al
45
BRTO has become widely acceptedin Japan and in some centers in the United States as a
minimally invasive and highly effective treatment for GV
The technical dif 1047297culty of BRTO relies on the anatomy of
the afferent and draining veins of the GV Accurate
assessment which is mainly based on imaging studies of
the variceal hemodynamic pattern is the most important
factor in ensuring successful treatment This anatomy
and how it alters the approach have been t horoughly
reviewed by Hirota et al46 Kiyosue et al4748 and
Al-Osaimi et al49
In most cases there is a gastrorenal or gastrocaval
shunt In this situation under 1047298uoroscopic guidance a
balloon catheter is inserted into the outlet of the
June 2014 Management of Gastric Varices 923
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 611
gastrorenal or gastrocaval shunt through a sheath placed
in the right femoral vein Immediately afterward
venography is performed with an injection of 10ndash15 mL
contrast medium via the in1047298ated balloon catheter and
GV are slowly intermitt ently and completely 1047297lled with
a sclerosant (Figure 3)454650ndash63 Thirty to 50 minutes
after the injection as much of the remaining sclerosant
as possible is aspirated via the catheter Finally the
balloon is de1047298ated and the catheter is withdrawn
Ethanolamine oleate is the predominant and traditional
sclerosant agent used in the BRTO procedure
particularly in Asia454650ndash60 Detergent sclerosants in a
foam or frot h have also been studied in both Japan
(polidocanol)6162 and the United States (3 STS)63
Figure 3 ( A ) Basic porto-systemic venous anatomyof GV with the classic gas-trorenal or splenorenalshunts ( B ) ConventionalBRTO procedure throughtransfemoral approach withballoon in the gastrorenalshunt IVC inferior venacava LGV left gastric veinLRV left renal vein MV
mesenteric vein PGVposterior gastric vein(s)PV main portal vein SGVshort gastric vein(s) SVsplenic vein Afferent vein( thin arrows ) Drainage vein( thick arrow )
924 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 711
The advantage of foam is that it reduces the sclerosant-
to-volume ratio requiring less sclerosant per procedure
In cases that involve complex types of afferent or
draining veins the use of additional techniques is required
for successful treatment These techniques include step-wise injection of the sclerosing agent selective injection of
the agent via a microcatheter coil embolization of the
afferent gastric veins double-balloon catheterization and
BRTO performed with percutaneous transhepatic portal
venous access or transileocolic venous access48
Epigastric and back pain (76)56 fever (26)5660
and transient hematuria (53) are the most common
complications of BRTO Bacterial peritonitis was found in
8 of patients in one study but t hese patients recovered
after only conservative therapy45 and this complication is
otherwise rarely mentioned in the literature Portal
(43) and renal vein thrombosis (5) can be found in asmall number of patients and bot h are usually clinically
silent465059 Pulmonary embolism59 pulmonary edema61
coil migration46 and anaphylaxis to ethanolamine oleate46
have also been reported
Technical success de1047297ned by complete obliteration of
the GV with sclerosant occurs in 77ndash100 of pa-
tients64 In some studies repeat BRTO was necessary to
achieve such high percentages465260 GV bleeding af t er a
successful BRTO ranges from 0ndash15465052555659ndash6165
or from 0ndash31666 when factoring in an intent-to-treat
basis (including technical failures) Some authors suggest
that BRTO might be better than TIPS67 or glue65 in the
prevention of GV bleeding However the fact that in
most patients treatment was administered as primary
prophylaxis for high-risk GV the studies had a small
sample size and the ef 1047297cacy of the comparative groups
(either TIPS or glue therapy) was poorer than expected
precludes de1047297nitive conclusions There is only a smallstudy54 that randomized 15 patients with acute GV
bleeding to receive TIPS (n frac14 7) or BRTO (n frac14 8)
without observing signi1047297cant differences in rebleeding
hepatic encephalopathy or survival
BRTO has the potential advantage of increasing portal
blood 1047298ow and potentially improving liver function525457
Therefore it may represent an alternative in patients who
may otherwise not tolerate TIPS59 In that regard in 4
studies including patients with hepatic encephalopathy
there was resolution or signi1047297cant reduction in
encephalopathy in all patients after BRTO46505158 By
contrast BRTO obliterates a spontaneous portosystemicshunt and therefore aggravates portal hypertension and
its related complications An increase in the size of
esophageal varices and the risk of esophageal variceal
bleeding after BRTO has been reported (between 73
and 27 after 1 year)525556 Other complications related
to the increase of portal hypertension after BRTO are the
development of portal hypertensive gastropathy (in 5ndash
13 of cases) ascites (0ndash44)65 and hydrothorax
pleural effusion (0ndash72) As a consequence of the
worsening of portal hypertension in some cases TIPS has
been performed after BRTO68
In conclusion although BRTO seems to be a feasible
technique that is able to successfully control and prevent
Figure 4 Suggested algo-rithm for management of GV EBL in small GV if tissue adhesives notavailable HE hepaticencephalopathy
June 2014 Management of Gastric Varices 925
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 811
GV bleeding there is a lack of good quality data to
routinely recommend BRTO in the management of GV In
our opinion BRTO could be considered in patients with
GV bleeding and large gastrorenal shunts in whom TIPS
may be contraindicated (such as those with refractory
hepatic encephalopathy or elderly patients)
Summary
The best management strategy for GV has not been
completely established because of a paucity of data of
RCTs in this area Speci1047297c treatments such as CA injec-
tion and BRTO are not widely available in all centers
Another limitation is the fact that tissue adhesives such
as CA are not approved by the Food and Drug Adminis-
tration in the United States and thus recommendations
arising from published studies guidelines and expert
opinion cannot be extrapolated to routine practice We
recommend a stepped care approach to the management
of GV as described in Figure 4 There are scarce data onthe role of CA or beta-blockers for primary prophylaxis
of GV bleeding and thus speci1047297c recommendations
cannot be made however patients should receive beta-
blockers if they have concomitant esophageal varices
After initial resuscitation and implementation of vaso-
constrictors and antibiotics endoscopic therapy with CA
should be the 1047297rst line of therapy if available After the
acute episode patients should receive beta-blockers
along with repeated sessions of CA injection if available
TIPS is very effective in controlling active GV bleeding
and for secondary prophylaxis However it carries a risk
of hepatic encephalopathy TIPS is the best treatment
strategy for patients who fail endoscopic therapy
Supplementary Material
Note To access the supplementary materials accom-
panying this article visit the online version of Clinical
Gastroenterology and Hepatology at wwwcghjournalorg
and at httpdxdoiorg101016jcgh201307015
References1 Sarin SK Lahoti D Saxena SP et al Prevalence classi1047297cation
and natural history of gastric varices a long-term follow-upstudy in 568 portal hypertension patients Hepatology 1992161343ndash1349
2 Kim T Shijo H Kokawa H et al Risk factors for hemorrhagefrom gastric fundal varices Hepatology 199725307ndash312
3 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric variceal bleeding comparing cyanoacrylate injection andbeta-blockers a randomized controlled trial J Hepatol 2011541161ndash1167
4 de Franchis R Revising consensus in portal hypertensionreport of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension J Hepatol 201053762ndash768
5 Garcia-Tsao G Sanyal AJ Grace ND et al Prevention andmanagement of gastroesophageal varices and variceal hemor-
rhage in cirrhosis Hepatology 200746922ndash938
6 Escorsell A Abraldes JG Pipa-Muntildeiz M et al Prognosis of acute bleeding from isolated fundal varices in patients withcirrhosis a European cohort Hepatology 201256(Suppl)748A
7 Tan PC Hou MC Lin HC et al A randomized trial of endoscopictreatment of acute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus band ligation Hepatology 200643690ndash697
8 Lo GH Lai KH Cheng JS et al A prospective randomized trial
of butyl cyanoacrylate injection versus band ligation in themanagement of bleeding gastric varices Hepatology 2001331060ndash1064
9 Oho K Iwao T Sumino M et al Ethanolamine oleate versusbutyl cyanoacrylate for bleeding gastric varices a non-randomized study Endoscopy 199527349ndash354
10 Sarin SK Jain AK Jain M et al A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolatedfundic varices Am J Gastroenterol 2002971010ndash1015
11 Lo GH Lai KH Should GOV1 be treated as for esophagealvarices Gastroenterology 20041271014ndash1015
12 Greenwald BD Caldwell SH Hespenheide EE et al N-2-butyl-cyanoacrylate for bleeding gastric varices a United States pilot
studyand cost analysis Am J Gastroenterol 2003981982ndash1988
13 Caldwell SH Hespenheide EE Greenwald BD et al Enbucrilatefor gastric varices extended experience in 92 patients AlimentPharmacol Ther 20072649ndash59
14 Seewald S Ang TL Imazu H et al A standardized injectiontechnique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundalvarices (with videos) Gastrointest Endosc 200868447ndash454
15 Wang YM Cheng LF Li N et al Study of glue extrusion after endoscopic N-butyl-2-cyanoacrylate injection on gastric vari-ceal bleeding World J Gastroenterol 2009154945ndash4951
16 Cheng LF Wang ZQ Li CZ et al Low incidence of complica-tions from endoscopic gastric variceal obturation with butyl
cyanoacrylate Clin Gastroenterol Hepatol 20108760ndash766
17 Joo HS Jang JY Eun SH et al [Long-term results of endo-scopic histoacryl (N-butyl-2-cyanoacrylate) injection for treat-ment of gastric varices a 10-year experience] Korean JGastroenterol 200749320ndash326
18 Teres J Cecilia A Bordas JM et al Esophageal tamponadefor bleeding varices controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube Gastroenterology197875566ndash569
19 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepatic portosystemic shunts gastric fundal compared withesophageal variceal bleeding Gastroenterology 1998114981ndash987
20 Azoulay D Castaing D Majno P et al Salvage transjugular intrahepatic portosystemic shunt for uncontrolled varicealbleeding in patients with decompensated cirrhosis J Hepatol200135590ndash597
21 Gaba RC Bui JT Cotler SJ et al Rebleeding rates followingTIPS forvariceal hemorrhage in the Viatorr era TIPS alone versusTIPS with variceal embolization Hepatol Int 20104749ndash756
22 Xiao T Chen L Chen W et al Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone versus TIPScombined with embolotherapy in advanced cirrhosis a retro-spective study J Clin Gastroenterol 201145643ndash650
23 Mahadeva S Bellamy MC Kessel D et al Cost-effectivenessof N-butyl-2-cyanoacrylate (histoacryl) glue injections versus trans-
jugular intrahepatic portosystemic shunt in the management of
926 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
Edso nGuzman FirmadodigitalmenteporEdso nGuzmanNombredereconocimiento(D N)cn=EdsonGuzmanoou=HNERMemail=e dson_guzmanhotmailcomc=PEFecha20140526200159-050 0
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 511
similar (77 vs 765) The results of this study suggest
that contrary to what has been demonstrated for
esophageal variceal bleeding adding beta-blocker ther-
apy to repeated sessions of CA provides no important
bene1047297t for prevention of rebleeding and mortality in
patients with GV bleeding Despite these 1047297ndings and
because nonselective beta-blockers are effective in pa-
tients with concomitant esophageal varices until largerstudies with longer follow-up are available we still
recommend the use of nonselective beta-blockers as an
adjunct to endoscopic therapy in the prevention of GV
rebleeding
Other Endoscopic Therapies
Other endoscopic treatments have also been used to
prevent rebleeding Sclerotherapy has been abandoned
because of high rebleeding rates (50ndash90) Variceal
band ligation may be used for those patients with GOV1
and in some cases of small GOV2 and it is generallyperformed every 2 weeks until apparent endoscopic
obliteration However band ligation is limited by the fact
that it cannot be used in large GOV2 or IGV17 Detachable
loop snares to treat large GV (gt2 cm) along with pro-
pranolol have resulted in low rebleeding rates however
data are very scarce and the procedure is labor inten-
sive This approach has not been further evaluated and
has not been compared with other modalities and thus
cannot be routinely recommended
Thrombin
Thrombin converts 1047297brinogen to a 1047297brin clot thus
forming a clot inside the GV and occluding blood 1047298ow
The use of bovine thrombin was banned because of the
risk of potential prion transmission This is not the case
when using commercially available human thrombin
Each vial is reconstituted with 5 mL distilled water for a
concentration of 250 UmL35 The average dose of
injected thrombin ranges between 1500 and 2000 U
Available data indicate that thrombin is safe and effective
in the treatment of acute GV bleeding with hemostasis
rates of 70ndash100 however rebleeding rates may
range from 7ndash
5036ndash41
There are scarce data inregard to follow-up and eradication rates After initial
hemostasis repeated thrombin injections are
performed every 2ndash3 weeks until eradication Because
of the paucity of data mostly coming from case series
the routine use of thrombin cannot be routinely
recommended
Transjugular Intrahepatic PortosystemicShunt
The role of TIPS vs CA in preventing GV bleeding has
been evaluated in 3 small studies (2 retrospective
observational studies and 1 prospective) Remarkablyin all
3 studies most patients included had GOV1a fewGOV2 and
only anecdotal IGV1 varices In addition the stents used
were uncoated which hasbeen shownto be associatedwith
lower TIPS patency ef 1047297cacy and survival than coated
stents42 Two of these studies2343 showed a higher
rebleeding rate in the CA group (30 and 59) vs the
TIPS group (15 and 40) (Supplementary Table 1)Frequency of complications was similar in the 2 groups
but TIPS-treated patients showed a higher incidence of
hepatic encephalopathy234344 and long-term morbidity
requiring hospitalization44 than endoscopically treated
patients The studies found no signi1047297cant differences in
survival Mahadeva et al23 analyzed the costs after 6
months of therapy and found that CA injections were
more cost-effective than TIPS in a small group of 43
patients with GV bleeding In summary TIPS is a very
effective therapy to prevent GV rebleeding Nevertheless
because of the previously mentioned drawbacks more
data are needed to clarify the role of TIPS in the
secondary prophylaxis of GV bleeding and determine
whether this therapy must be universally applied or
reserved as a rescue therapy after failure of more
conservative approaches
Surgery
Surgery has currently fallen out of favor for patients
with portal hypertension because of the wide avail-
ability of less invasive techniques such as endoscopy
and interventional radiology In selected cases pa-
tients with GV and segmentalleft-sided portal hyper-
tension that is due to isolated splenic vein thrombosis
may be candidates for splenectomy or splenic emboli-
zation as a means of de1047297nitive therapy however data
are scarce
Balloon-occluded RetrogradeTransvenous Obliteration
Balloon-occluded retrograde transvenous obliteration
(BRTO) has been introduced as a treatment method that
aims to directly oblit erate the GV Since its introduction
by Kanagawa et al
45
BRTO has become widely acceptedin Japan and in some centers in the United States as a
minimally invasive and highly effective treatment for GV
The technical dif 1047297culty of BRTO relies on the anatomy of
the afferent and draining veins of the GV Accurate
assessment which is mainly based on imaging studies of
the variceal hemodynamic pattern is the most important
factor in ensuring successful treatment This anatomy
and how it alters the approach have been t horoughly
reviewed by Hirota et al46 Kiyosue et al4748 and
Al-Osaimi et al49
In most cases there is a gastrorenal or gastrocaval
shunt In this situation under 1047298uoroscopic guidance a
balloon catheter is inserted into the outlet of the
June 2014 Management of Gastric Varices 923
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 611
gastrorenal or gastrocaval shunt through a sheath placed
in the right femoral vein Immediately afterward
venography is performed with an injection of 10ndash15 mL
contrast medium via the in1047298ated balloon catheter and
GV are slowly intermitt ently and completely 1047297lled with
a sclerosant (Figure 3)454650ndash63 Thirty to 50 minutes
after the injection as much of the remaining sclerosant
as possible is aspirated via the catheter Finally the
balloon is de1047298ated and the catheter is withdrawn
Ethanolamine oleate is the predominant and traditional
sclerosant agent used in the BRTO procedure
particularly in Asia454650ndash60 Detergent sclerosants in a
foam or frot h have also been studied in both Japan
(polidocanol)6162 and the United States (3 STS)63
Figure 3 ( A ) Basic porto-systemic venous anatomyof GV with the classic gas-trorenal or splenorenalshunts ( B ) ConventionalBRTO procedure throughtransfemoral approach withballoon in the gastrorenalshunt IVC inferior venacava LGV left gastric veinLRV left renal vein MV
mesenteric vein PGVposterior gastric vein(s)PV main portal vein SGVshort gastric vein(s) SVsplenic vein Afferent vein( thin arrows ) Drainage vein( thick arrow )
924 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 711
The advantage of foam is that it reduces the sclerosant-
to-volume ratio requiring less sclerosant per procedure
In cases that involve complex types of afferent or
draining veins the use of additional techniques is required
for successful treatment These techniques include step-wise injection of the sclerosing agent selective injection of
the agent via a microcatheter coil embolization of the
afferent gastric veins double-balloon catheterization and
BRTO performed with percutaneous transhepatic portal
venous access or transileocolic venous access48
Epigastric and back pain (76)56 fever (26)5660
and transient hematuria (53) are the most common
complications of BRTO Bacterial peritonitis was found in
8 of patients in one study but t hese patients recovered
after only conservative therapy45 and this complication is
otherwise rarely mentioned in the literature Portal
(43) and renal vein thrombosis (5) can be found in asmall number of patients and bot h are usually clinically
silent465059 Pulmonary embolism59 pulmonary edema61
coil migration46 and anaphylaxis to ethanolamine oleate46
have also been reported
Technical success de1047297ned by complete obliteration of
the GV with sclerosant occurs in 77ndash100 of pa-
tients64 In some studies repeat BRTO was necessary to
achieve such high percentages465260 GV bleeding af t er a
successful BRTO ranges from 0ndash15465052555659ndash6165
or from 0ndash31666 when factoring in an intent-to-treat
basis (including technical failures) Some authors suggest
that BRTO might be better than TIPS67 or glue65 in the
prevention of GV bleeding However the fact that in
most patients treatment was administered as primary
prophylaxis for high-risk GV the studies had a small
sample size and the ef 1047297cacy of the comparative groups
(either TIPS or glue therapy) was poorer than expected
precludes de1047297nitive conclusions There is only a smallstudy54 that randomized 15 patients with acute GV
bleeding to receive TIPS (n frac14 7) or BRTO (n frac14 8)
without observing signi1047297cant differences in rebleeding
hepatic encephalopathy or survival
BRTO has the potential advantage of increasing portal
blood 1047298ow and potentially improving liver function525457
Therefore it may represent an alternative in patients who
may otherwise not tolerate TIPS59 In that regard in 4
studies including patients with hepatic encephalopathy
there was resolution or signi1047297cant reduction in
encephalopathy in all patients after BRTO46505158 By
contrast BRTO obliterates a spontaneous portosystemicshunt and therefore aggravates portal hypertension and
its related complications An increase in the size of
esophageal varices and the risk of esophageal variceal
bleeding after BRTO has been reported (between 73
and 27 after 1 year)525556 Other complications related
to the increase of portal hypertension after BRTO are the
development of portal hypertensive gastropathy (in 5ndash
13 of cases) ascites (0ndash44)65 and hydrothorax
pleural effusion (0ndash72) As a consequence of the
worsening of portal hypertension in some cases TIPS has
been performed after BRTO68
In conclusion although BRTO seems to be a feasible
technique that is able to successfully control and prevent
Figure 4 Suggested algo-rithm for management of GV EBL in small GV if tissue adhesives notavailable HE hepaticencephalopathy
June 2014 Management of Gastric Varices 925
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 811
GV bleeding there is a lack of good quality data to
routinely recommend BRTO in the management of GV In
our opinion BRTO could be considered in patients with
GV bleeding and large gastrorenal shunts in whom TIPS
may be contraindicated (such as those with refractory
hepatic encephalopathy or elderly patients)
Summary
The best management strategy for GV has not been
completely established because of a paucity of data of
RCTs in this area Speci1047297c treatments such as CA injec-
tion and BRTO are not widely available in all centers
Another limitation is the fact that tissue adhesives such
as CA are not approved by the Food and Drug Adminis-
tration in the United States and thus recommendations
arising from published studies guidelines and expert
opinion cannot be extrapolated to routine practice We
recommend a stepped care approach to the management
of GV as described in Figure 4 There are scarce data onthe role of CA or beta-blockers for primary prophylaxis
of GV bleeding and thus speci1047297c recommendations
cannot be made however patients should receive beta-
blockers if they have concomitant esophageal varices
After initial resuscitation and implementation of vaso-
constrictors and antibiotics endoscopic therapy with CA
should be the 1047297rst line of therapy if available After the
acute episode patients should receive beta-blockers
along with repeated sessions of CA injection if available
TIPS is very effective in controlling active GV bleeding
and for secondary prophylaxis However it carries a risk
of hepatic encephalopathy TIPS is the best treatment
strategy for patients who fail endoscopic therapy
Supplementary Material
Note To access the supplementary materials accom-
panying this article visit the online version of Clinical
Gastroenterology and Hepatology at wwwcghjournalorg
and at httpdxdoiorg101016jcgh201307015
References1 Sarin SK Lahoti D Saxena SP et al Prevalence classi1047297cation
and natural history of gastric varices a long-term follow-upstudy in 568 portal hypertension patients Hepatology 1992161343ndash1349
2 Kim T Shijo H Kokawa H et al Risk factors for hemorrhagefrom gastric fundal varices Hepatology 199725307ndash312
3 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric variceal bleeding comparing cyanoacrylate injection andbeta-blockers a randomized controlled trial J Hepatol 2011541161ndash1167
4 de Franchis R Revising consensus in portal hypertensionreport of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension J Hepatol 201053762ndash768
5 Garcia-Tsao G Sanyal AJ Grace ND et al Prevention andmanagement of gastroesophageal varices and variceal hemor-
rhage in cirrhosis Hepatology 200746922ndash938
6 Escorsell A Abraldes JG Pipa-Muntildeiz M et al Prognosis of acute bleeding from isolated fundal varices in patients withcirrhosis a European cohort Hepatology 201256(Suppl)748A
7 Tan PC Hou MC Lin HC et al A randomized trial of endoscopictreatment of acute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus band ligation Hepatology 200643690ndash697
8 Lo GH Lai KH Cheng JS et al A prospective randomized trial
of butyl cyanoacrylate injection versus band ligation in themanagement of bleeding gastric varices Hepatology 2001331060ndash1064
9 Oho K Iwao T Sumino M et al Ethanolamine oleate versusbutyl cyanoacrylate for bleeding gastric varices a non-randomized study Endoscopy 199527349ndash354
10 Sarin SK Jain AK Jain M et al A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolatedfundic varices Am J Gastroenterol 2002971010ndash1015
11 Lo GH Lai KH Should GOV1 be treated as for esophagealvarices Gastroenterology 20041271014ndash1015
12 Greenwald BD Caldwell SH Hespenheide EE et al N-2-butyl-cyanoacrylate for bleeding gastric varices a United States pilot
studyand cost analysis Am J Gastroenterol 2003981982ndash1988
13 Caldwell SH Hespenheide EE Greenwald BD et al Enbucrilatefor gastric varices extended experience in 92 patients AlimentPharmacol Ther 20072649ndash59
14 Seewald S Ang TL Imazu H et al A standardized injectiontechnique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundalvarices (with videos) Gastrointest Endosc 200868447ndash454
15 Wang YM Cheng LF Li N et al Study of glue extrusion after endoscopic N-butyl-2-cyanoacrylate injection on gastric vari-ceal bleeding World J Gastroenterol 2009154945ndash4951
16 Cheng LF Wang ZQ Li CZ et al Low incidence of complica-tions from endoscopic gastric variceal obturation with butyl
cyanoacrylate Clin Gastroenterol Hepatol 20108760ndash766
17 Joo HS Jang JY Eun SH et al [Long-term results of endo-scopic histoacryl (N-butyl-2-cyanoacrylate) injection for treat-ment of gastric varices a 10-year experience] Korean JGastroenterol 200749320ndash326
18 Teres J Cecilia A Bordas JM et al Esophageal tamponadefor bleeding varices controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube Gastroenterology197875566ndash569
19 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepatic portosystemic shunts gastric fundal compared withesophageal variceal bleeding Gastroenterology 1998114981ndash987
20 Azoulay D Castaing D Majno P et al Salvage transjugular intrahepatic portosystemic shunt for uncontrolled varicealbleeding in patients with decompensated cirrhosis J Hepatol200135590ndash597
21 Gaba RC Bui JT Cotler SJ et al Rebleeding rates followingTIPS forvariceal hemorrhage in the Viatorr era TIPS alone versusTIPS with variceal embolization Hepatol Int 20104749ndash756
22 Xiao T Chen L Chen W et al Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone versus TIPScombined with embolotherapy in advanced cirrhosis a retro-spective study J Clin Gastroenterol 201145643ndash650
23 Mahadeva S Bellamy MC Kessel D et al Cost-effectivenessof N-butyl-2-cyanoacrylate (histoacryl) glue injections versus trans-
jugular intrahepatic portosystemic shunt in the management of
926 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
Edso nGuzman FirmadodigitalmenteporEdso nGuzmanNombredereconocimiento(D N)cn=EdsonGuzmanoou=HNERMemail=e dson_guzmanhotmailcomc=PEFecha20140526200159-050 0
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 611
gastrorenal or gastrocaval shunt through a sheath placed
in the right femoral vein Immediately afterward
venography is performed with an injection of 10ndash15 mL
contrast medium via the in1047298ated balloon catheter and
GV are slowly intermitt ently and completely 1047297lled with
a sclerosant (Figure 3)454650ndash63 Thirty to 50 minutes
after the injection as much of the remaining sclerosant
as possible is aspirated via the catheter Finally the
balloon is de1047298ated and the catheter is withdrawn
Ethanolamine oleate is the predominant and traditional
sclerosant agent used in the BRTO procedure
particularly in Asia454650ndash60 Detergent sclerosants in a
foam or frot h have also been studied in both Japan
(polidocanol)6162 and the United States (3 STS)63
Figure 3 ( A ) Basic porto-systemic venous anatomyof GV with the classic gas-trorenal or splenorenalshunts ( B ) ConventionalBRTO procedure throughtransfemoral approach withballoon in the gastrorenalshunt IVC inferior venacava LGV left gastric veinLRV left renal vein MV
mesenteric vein PGVposterior gastric vein(s)PV main portal vein SGVshort gastric vein(s) SVsplenic vein Afferent vein( thin arrows ) Drainage vein( thick arrow )
924 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 711
The advantage of foam is that it reduces the sclerosant-
to-volume ratio requiring less sclerosant per procedure
In cases that involve complex types of afferent or
draining veins the use of additional techniques is required
for successful treatment These techniques include step-wise injection of the sclerosing agent selective injection of
the agent via a microcatheter coil embolization of the
afferent gastric veins double-balloon catheterization and
BRTO performed with percutaneous transhepatic portal
venous access or transileocolic venous access48
Epigastric and back pain (76)56 fever (26)5660
and transient hematuria (53) are the most common
complications of BRTO Bacterial peritonitis was found in
8 of patients in one study but t hese patients recovered
after only conservative therapy45 and this complication is
otherwise rarely mentioned in the literature Portal
(43) and renal vein thrombosis (5) can be found in asmall number of patients and bot h are usually clinically
silent465059 Pulmonary embolism59 pulmonary edema61
coil migration46 and anaphylaxis to ethanolamine oleate46
have also been reported
Technical success de1047297ned by complete obliteration of
the GV with sclerosant occurs in 77ndash100 of pa-
tients64 In some studies repeat BRTO was necessary to
achieve such high percentages465260 GV bleeding af t er a
successful BRTO ranges from 0ndash15465052555659ndash6165
or from 0ndash31666 when factoring in an intent-to-treat
basis (including technical failures) Some authors suggest
that BRTO might be better than TIPS67 or glue65 in the
prevention of GV bleeding However the fact that in
most patients treatment was administered as primary
prophylaxis for high-risk GV the studies had a small
sample size and the ef 1047297cacy of the comparative groups
(either TIPS or glue therapy) was poorer than expected
precludes de1047297nitive conclusions There is only a smallstudy54 that randomized 15 patients with acute GV
bleeding to receive TIPS (n frac14 7) or BRTO (n frac14 8)
without observing signi1047297cant differences in rebleeding
hepatic encephalopathy or survival
BRTO has the potential advantage of increasing portal
blood 1047298ow and potentially improving liver function525457
Therefore it may represent an alternative in patients who
may otherwise not tolerate TIPS59 In that regard in 4
studies including patients with hepatic encephalopathy
there was resolution or signi1047297cant reduction in
encephalopathy in all patients after BRTO46505158 By
contrast BRTO obliterates a spontaneous portosystemicshunt and therefore aggravates portal hypertension and
its related complications An increase in the size of
esophageal varices and the risk of esophageal variceal
bleeding after BRTO has been reported (between 73
and 27 after 1 year)525556 Other complications related
to the increase of portal hypertension after BRTO are the
development of portal hypertensive gastropathy (in 5ndash
13 of cases) ascites (0ndash44)65 and hydrothorax
pleural effusion (0ndash72) As a consequence of the
worsening of portal hypertension in some cases TIPS has
been performed after BRTO68
In conclusion although BRTO seems to be a feasible
technique that is able to successfully control and prevent
Figure 4 Suggested algo-rithm for management of GV EBL in small GV if tissue adhesives notavailable HE hepaticencephalopathy
June 2014 Management of Gastric Varices 925
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 811
GV bleeding there is a lack of good quality data to
routinely recommend BRTO in the management of GV In
our opinion BRTO could be considered in patients with
GV bleeding and large gastrorenal shunts in whom TIPS
may be contraindicated (such as those with refractory
hepatic encephalopathy or elderly patients)
Summary
The best management strategy for GV has not been
completely established because of a paucity of data of
RCTs in this area Speci1047297c treatments such as CA injec-
tion and BRTO are not widely available in all centers
Another limitation is the fact that tissue adhesives such
as CA are not approved by the Food and Drug Adminis-
tration in the United States and thus recommendations
arising from published studies guidelines and expert
opinion cannot be extrapolated to routine practice We
recommend a stepped care approach to the management
of GV as described in Figure 4 There are scarce data onthe role of CA or beta-blockers for primary prophylaxis
of GV bleeding and thus speci1047297c recommendations
cannot be made however patients should receive beta-
blockers if they have concomitant esophageal varices
After initial resuscitation and implementation of vaso-
constrictors and antibiotics endoscopic therapy with CA
should be the 1047297rst line of therapy if available After the
acute episode patients should receive beta-blockers
along with repeated sessions of CA injection if available
TIPS is very effective in controlling active GV bleeding
and for secondary prophylaxis However it carries a risk
of hepatic encephalopathy TIPS is the best treatment
strategy for patients who fail endoscopic therapy
Supplementary Material
Note To access the supplementary materials accom-
panying this article visit the online version of Clinical
Gastroenterology and Hepatology at wwwcghjournalorg
and at httpdxdoiorg101016jcgh201307015
References1 Sarin SK Lahoti D Saxena SP et al Prevalence classi1047297cation
and natural history of gastric varices a long-term follow-upstudy in 568 portal hypertension patients Hepatology 1992161343ndash1349
2 Kim T Shijo H Kokawa H et al Risk factors for hemorrhagefrom gastric fundal varices Hepatology 199725307ndash312
3 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric variceal bleeding comparing cyanoacrylate injection andbeta-blockers a randomized controlled trial J Hepatol 2011541161ndash1167
4 de Franchis R Revising consensus in portal hypertensionreport of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension J Hepatol 201053762ndash768
5 Garcia-Tsao G Sanyal AJ Grace ND et al Prevention andmanagement of gastroesophageal varices and variceal hemor-
rhage in cirrhosis Hepatology 200746922ndash938
6 Escorsell A Abraldes JG Pipa-Muntildeiz M et al Prognosis of acute bleeding from isolated fundal varices in patients withcirrhosis a European cohort Hepatology 201256(Suppl)748A
7 Tan PC Hou MC Lin HC et al A randomized trial of endoscopictreatment of acute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus band ligation Hepatology 200643690ndash697
8 Lo GH Lai KH Cheng JS et al A prospective randomized trial
of butyl cyanoacrylate injection versus band ligation in themanagement of bleeding gastric varices Hepatology 2001331060ndash1064
9 Oho K Iwao T Sumino M et al Ethanolamine oleate versusbutyl cyanoacrylate for bleeding gastric varices a non-randomized study Endoscopy 199527349ndash354
10 Sarin SK Jain AK Jain M et al A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolatedfundic varices Am J Gastroenterol 2002971010ndash1015
11 Lo GH Lai KH Should GOV1 be treated as for esophagealvarices Gastroenterology 20041271014ndash1015
12 Greenwald BD Caldwell SH Hespenheide EE et al N-2-butyl-cyanoacrylate for bleeding gastric varices a United States pilot
studyand cost analysis Am J Gastroenterol 2003981982ndash1988
13 Caldwell SH Hespenheide EE Greenwald BD et al Enbucrilatefor gastric varices extended experience in 92 patients AlimentPharmacol Ther 20072649ndash59
14 Seewald S Ang TL Imazu H et al A standardized injectiontechnique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundalvarices (with videos) Gastrointest Endosc 200868447ndash454
15 Wang YM Cheng LF Li N et al Study of glue extrusion after endoscopic N-butyl-2-cyanoacrylate injection on gastric vari-ceal bleeding World J Gastroenterol 2009154945ndash4951
16 Cheng LF Wang ZQ Li CZ et al Low incidence of complica-tions from endoscopic gastric variceal obturation with butyl
cyanoacrylate Clin Gastroenterol Hepatol 20108760ndash766
17 Joo HS Jang JY Eun SH et al [Long-term results of endo-scopic histoacryl (N-butyl-2-cyanoacrylate) injection for treat-ment of gastric varices a 10-year experience] Korean JGastroenterol 200749320ndash326
18 Teres J Cecilia A Bordas JM et al Esophageal tamponadefor bleeding varices controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube Gastroenterology197875566ndash569
19 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepatic portosystemic shunts gastric fundal compared withesophageal variceal bleeding Gastroenterology 1998114981ndash987
20 Azoulay D Castaing D Majno P et al Salvage transjugular intrahepatic portosystemic shunt for uncontrolled varicealbleeding in patients with decompensated cirrhosis J Hepatol200135590ndash597
21 Gaba RC Bui JT Cotler SJ et al Rebleeding rates followingTIPS forvariceal hemorrhage in the Viatorr era TIPS alone versusTIPS with variceal embolization Hepatol Int 20104749ndash756
22 Xiao T Chen L Chen W et al Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone versus TIPScombined with embolotherapy in advanced cirrhosis a retro-spective study J Clin Gastroenterol 201145643ndash650
23 Mahadeva S Bellamy MC Kessel D et al Cost-effectivenessof N-butyl-2-cyanoacrylate (histoacryl) glue injections versus trans-
jugular intrahepatic portosystemic shunt in the management of
926 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
Edso nGuzman FirmadodigitalmenteporEdso nGuzmanNombredereconocimiento(D N)cn=EdsonGuzmanoou=HNERMemail=e dson_guzmanhotmailcomc=PEFecha20140526200159-050 0
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1
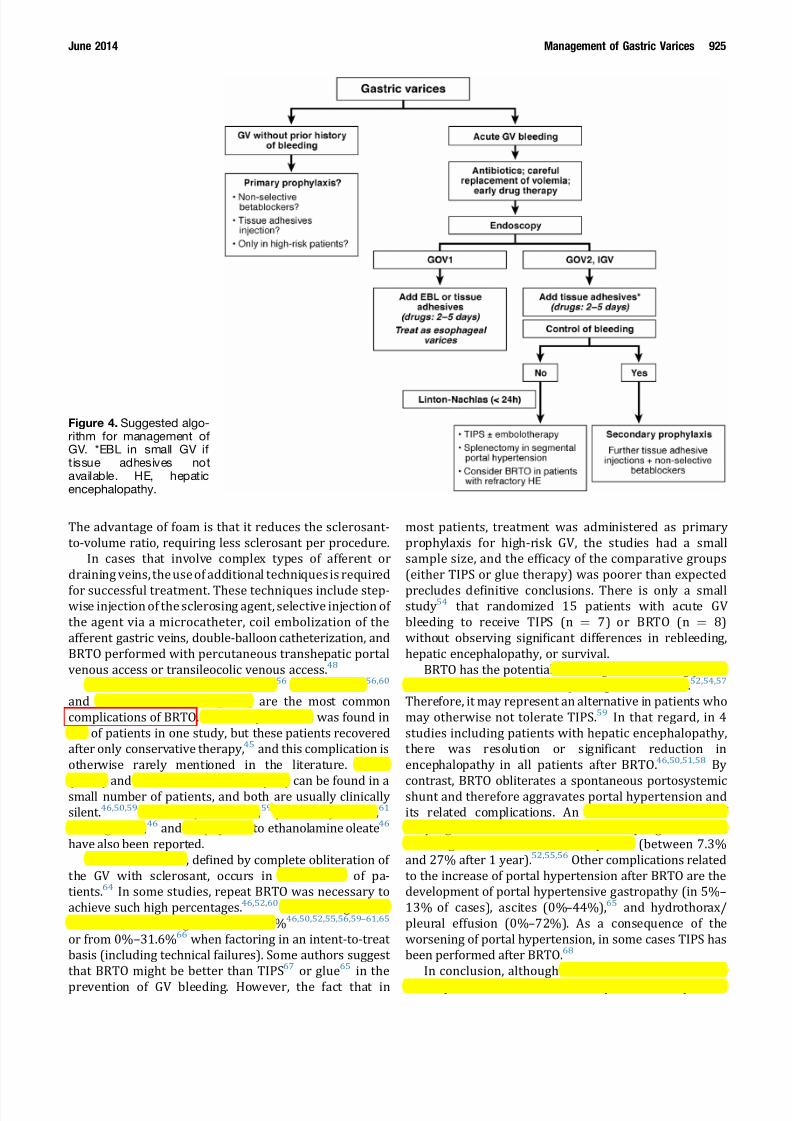
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 711
The advantage of foam is that it reduces the sclerosant-
to-volume ratio requiring less sclerosant per procedure
In cases that involve complex types of afferent or
draining veins the use of additional techniques is required
for successful treatment These techniques include step-wise injection of the sclerosing agent selective injection of
the agent via a microcatheter coil embolization of the
afferent gastric veins double-balloon catheterization and
BRTO performed with percutaneous transhepatic portal
venous access or transileocolic venous access48
Epigastric and back pain (76)56 fever (26)5660
and transient hematuria (53) are the most common
complications of BRTO Bacterial peritonitis was found in
8 of patients in one study but t hese patients recovered
after only conservative therapy45 and this complication is
otherwise rarely mentioned in the literature Portal
(43) and renal vein thrombosis (5) can be found in asmall number of patients and bot h are usually clinically
silent465059 Pulmonary embolism59 pulmonary edema61
coil migration46 and anaphylaxis to ethanolamine oleate46
have also been reported
Technical success de1047297ned by complete obliteration of
the GV with sclerosant occurs in 77ndash100 of pa-
tients64 In some studies repeat BRTO was necessary to
achieve such high percentages465260 GV bleeding af t er a
successful BRTO ranges from 0ndash15465052555659ndash6165
or from 0ndash31666 when factoring in an intent-to-treat
basis (including technical failures) Some authors suggest
that BRTO might be better than TIPS67 or glue65 in the
prevention of GV bleeding However the fact that in
most patients treatment was administered as primary
prophylaxis for high-risk GV the studies had a small
sample size and the ef 1047297cacy of the comparative groups
(either TIPS or glue therapy) was poorer than expected
precludes de1047297nitive conclusions There is only a smallstudy54 that randomized 15 patients with acute GV
bleeding to receive TIPS (n frac14 7) or BRTO (n frac14 8)
without observing signi1047297cant differences in rebleeding
hepatic encephalopathy or survival
BRTO has the potential advantage of increasing portal
blood 1047298ow and potentially improving liver function525457
Therefore it may represent an alternative in patients who
may otherwise not tolerate TIPS59 In that regard in 4
studies including patients with hepatic encephalopathy
there was resolution or signi1047297cant reduction in
encephalopathy in all patients after BRTO46505158 By
contrast BRTO obliterates a spontaneous portosystemicshunt and therefore aggravates portal hypertension and
its related complications An increase in the size of
esophageal varices and the risk of esophageal variceal
bleeding after BRTO has been reported (between 73
and 27 after 1 year)525556 Other complications related
to the increase of portal hypertension after BRTO are the
development of portal hypertensive gastropathy (in 5ndash
13 of cases) ascites (0ndash44)65 and hydrothorax
pleural effusion (0ndash72) As a consequence of the
worsening of portal hypertension in some cases TIPS has
been performed after BRTO68
In conclusion although BRTO seems to be a feasible
technique that is able to successfully control and prevent
Figure 4 Suggested algo-rithm for management of GV EBL in small GV if tissue adhesives notavailable HE hepaticencephalopathy
June 2014 Management of Gastric Varices 925
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 811
GV bleeding there is a lack of good quality data to
routinely recommend BRTO in the management of GV In
our opinion BRTO could be considered in patients with
GV bleeding and large gastrorenal shunts in whom TIPS
may be contraindicated (such as those with refractory
hepatic encephalopathy or elderly patients)
Summary
The best management strategy for GV has not been
completely established because of a paucity of data of
RCTs in this area Speci1047297c treatments such as CA injec-
tion and BRTO are not widely available in all centers
Another limitation is the fact that tissue adhesives such
as CA are not approved by the Food and Drug Adminis-
tration in the United States and thus recommendations
arising from published studies guidelines and expert
opinion cannot be extrapolated to routine practice We
recommend a stepped care approach to the management
of GV as described in Figure 4 There are scarce data onthe role of CA or beta-blockers for primary prophylaxis
of GV bleeding and thus speci1047297c recommendations
cannot be made however patients should receive beta-
blockers if they have concomitant esophageal varices
After initial resuscitation and implementation of vaso-
constrictors and antibiotics endoscopic therapy with CA
should be the 1047297rst line of therapy if available After the
acute episode patients should receive beta-blockers
along with repeated sessions of CA injection if available
TIPS is very effective in controlling active GV bleeding
and for secondary prophylaxis However it carries a risk
of hepatic encephalopathy TIPS is the best treatment
strategy for patients who fail endoscopic therapy
Supplementary Material
Note To access the supplementary materials accom-
panying this article visit the online version of Clinical
Gastroenterology and Hepatology at wwwcghjournalorg
and at httpdxdoiorg101016jcgh201307015
References1 Sarin SK Lahoti D Saxena SP et al Prevalence classi1047297cation
and natural history of gastric varices a long-term follow-upstudy in 568 portal hypertension patients Hepatology 1992161343ndash1349
2 Kim T Shijo H Kokawa H et al Risk factors for hemorrhagefrom gastric fundal varices Hepatology 199725307ndash312
3 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric variceal bleeding comparing cyanoacrylate injection andbeta-blockers a randomized controlled trial J Hepatol 2011541161ndash1167
4 de Franchis R Revising consensus in portal hypertensionreport of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension J Hepatol 201053762ndash768
5 Garcia-Tsao G Sanyal AJ Grace ND et al Prevention andmanagement of gastroesophageal varices and variceal hemor-
rhage in cirrhosis Hepatology 200746922ndash938
6 Escorsell A Abraldes JG Pipa-Muntildeiz M et al Prognosis of acute bleeding from isolated fundal varices in patients withcirrhosis a European cohort Hepatology 201256(Suppl)748A
7 Tan PC Hou MC Lin HC et al A randomized trial of endoscopictreatment of acute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus band ligation Hepatology 200643690ndash697
8 Lo GH Lai KH Cheng JS et al A prospective randomized trial
of butyl cyanoacrylate injection versus band ligation in themanagement of bleeding gastric varices Hepatology 2001331060ndash1064
9 Oho K Iwao T Sumino M et al Ethanolamine oleate versusbutyl cyanoacrylate for bleeding gastric varices a non-randomized study Endoscopy 199527349ndash354
10 Sarin SK Jain AK Jain M et al A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolatedfundic varices Am J Gastroenterol 2002971010ndash1015
11 Lo GH Lai KH Should GOV1 be treated as for esophagealvarices Gastroenterology 20041271014ndash1015
12 Greenwald BD Caldwell SH Hespenheide EE et al N-2-butyl-cyanoacrylate for bleeding gastric varices a United States pilot
studyand cost analysis Am J Gastroenterol 2003981982ndash1988
13 Caldwell SH Hespenheide EE Greenwald BD et al Enbucrilatefor gastric varices extended experience in 92 patients AlimentPharmacol Ther 20072649ndash59
14 Seewald S Ang TL Imazu H et al A standardized injectiontechnique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundalvarices (with videos) Gastrointest Endosc 200868447ndash454
15 Wang YM Cheng LF Li N et al Study of glue extrusion after endoscopic N-butyl-2-cyanoacrylate injection on gastric vari-ceal bleeding World J Gastroenterol 2009154945ndash4951
16 Cheng LF Wang ZQ Li CZ et al Low incidence of complica-tions from endoscopic gastric variceal obturation with butyl
cyanoacrylate Clin Gastroenterol Hepatol 20108760ndash766
17 Joo HS Jang JY Eun SH et al [Long-term results of endo-scopic histoacryl (N-butyl-2-cyanoacrylate) injection for treat-ment of gastric varices a 10-year experience] Korean JGastroenterol 200749320ndash326
18 Teres J Cecilia A Bordas JM et al Esophageal tamponadefor bleeding varices controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube Gastroenterology197875566ndash569
19 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepatic portosystemic shunts gastric fundal compared withesophageal variceal bleeding Gastroenterology 1998114981ndash987
20 Azoulay D Castaing D Majno P et al Salvage transjugular intrahepatic portosystemic shunt for uncontrolled varicealbleeding in patients with decompensated cirrhosis J Hepatol200135590ndash597
21 Gaba RC Bui JT Cotler SJ et al Rebleeding rates followingTIPS forvariceal hemorrhage in the Viatorr era TIPS alone versusTIPS with variceal embolization Hepatol Int 20104749ndash756
22 Xiao T Chen L Chen W et al Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone versus TIPScombined with embolotherapy in advanced cirrhosis a retro-spective study J Clin Gastroenterol 201145643ndash650
23 Mahadeva S Bellamy MC Kessel D et al Cost-effectivenessof N-butyl-2-cyanoacrylate (histoacryl) glue injections versus trans-
jugular intrahepatic portosystemic shunt in the management of
926 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
Edso nGuzman FirmadodigitalmenteporEdso nGuzmanNombredereconocimiento(D N)cn=EdsonGuzmanoou=HNERMemail=e dson_guzmanhotmailcomc=PEFecha20140526200159-050 0
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 811
GV bleeding there is a lack of good quality data to
routinely recommend BRTO in the management of GV In
our opinion BRTO could be considered in patients with
GV bleeding and large gastrorenal shunts in whom TIPS
may be contraindicated (such as those with refractory
hepatic encephalopathy or elderly patients)
Summary
The best management strategy for GV has not been
completely established because of a paucity of data of
RCTs in this area Speci1047297c treatments such as CA injec-
tion and BRTO are not widely available in all centers
Another limitation is the fact that tissue adhesives such
as CA are not approved by the Food and Drug Adminis-
tration in the United States and thus recommendations
arising from published studies guidelines and expert
opinion cannot be extrapolated to routine practice We
recommend a stepped care approach to the management
of GV as described in Figure 4 There are scarce data onthe role of CA or beta-blockers for primary prophylaxis
of GV bleeding and thus speci1047297c recommendations
cannot be made however patients should receive beta-
blockers if they have concomitant esophageal varices
After initial resuscitation and implementation of vaso-
constrictors and antibiotics endoscopic therapy with CA
should be the 1047297rst line of therapy if available After the
acute episode patients should receive beta-blockers
along with repeated sessions of CA injection if available
TIPS is very effective in controlling active GV bleeding
and for secondary prophylaxis However it carries a risk
of hepatic encephalopathy TIPS is the best treatment
strategy for patients who fail endoscopic therapy
Supplementary Material
Note To access the supplementary materials accom-
panying this article visit the online version of Clinical
Gastroenterology and Hepatology at wwwcghjournalorg
and at httpdxdoiorg101016jcgh201307015
References1 Sarin SK Lahoti D Saxena SP et al Prevalence classi1047297cation
and natural history of gastric varices a long-term follow-upstudy in 568 portal hypertension patients Hepatology 1992161343ndash1349
2 Kim T Shijo H Kokawa H et al Risk factors for hemorrhagefrom gastric fundal varices Hepatology 199725307ndash312
3 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric variceal bleeding comparing cyanoacrylate injection andbeta-blockers a randomized controlled trial J Hepatol 2011541161ndash1167
4 de Franchis R Revising consensus in portal hypertensionreport of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension J Hepatol 201053762ndash768
5 Garcia-Tsao G Sanyal AJ Grace ND et al Prevention andmanagement of gastroesophageal varices and variceal hemor-
rhage in cirrhosis Hepatology 200746922ndash938
6 Escorsell A Abraldes JG Pipa-Muntildeiz M et al Prognosis of acute bleeding from isolated fundal varices in patients withcirrhosis a European cohort Hepatology 201256(Suppl)748A
7 Tan PC Hou MC Lin HC et al A randomized trial of endoscopictreatment of acute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus band ligation Hepatology 200643690ndash697
8 Lo GH Lai KH Cheng JS et al A prospective randomized trial
of butyl cyanoacrylate injection versus band ligation in themanagement of bleeding gastric varices Hepatology 2001331060ndash1064
9 Oho K Iwao T Sumino M et al Ethanolamine oleate versusbutyl cyanoacrylate for bleeding gastric varices a non-randomized study Endoscopy 199527349ndash354
10 Sarin SK Jain AK Jain M et al A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolatedfundic varices Am J Gastroenterol 2002971010ndash1015
11 Lo GH Lai KH Should GOV1 be treated as for esophagealvarices Gastroenterology 20041271014ndash1015
12 Greenwald BD Caldwell SH Hespenheide EE et al N-2-butyl-cyanoacrylate for bleeding gastric varices a United States pilot
studyand cost analysis Am J Gastroenterol 2003981982ndash1988
13 Caldwell SH Hespenheide EE Greenwald BD et al Enbucrilatefor gastric varices extended experience in 92 patients AlimentPharmacol Ther 20072649ndash59
14 Seewald S Ang TL Imazu H et al A standardized injectiontechnique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundalvarices (with videos) Gastrointest Endosc 200868447ndash454
15 Wang YM Cheng LF Li N et al Study of glue extrusion after endoscopic N-butyl-2-cyanoacrylate injection on gastric vari-ceal bleeding World J Gastroenterol 2009154945ndash4951
16 Cheng LF Wang ZQ Li CZ et al Low incidence of complica-tions from endoscopic gastric variceal obturation with butyl
cyanoacrylate Clin Gastroenterol Hepatol 20108760ndash766
17 Joo HS Jang JY Eun SH et al [Long-term results of endo-scopic histoacryl (N-butyl-2-cyanoacrylate) injection for treat-ment of gastric varices a 10-year experience] Korean JGastroenterol 200749320ndash326
18 Teres J Cecilia A Bordas JM et al Esophageal tamponadefor bleeding varices controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube Gastroenterology197875566ndash569
19 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepatic portosystemic shunts gastric fundal compared withesophageal variceal bleeding Gastroenterology 1998114981ndash987
20 Azoulay D Castaing D Majno P et al Salvage transjugular intrahepatic portosystemic shunt for uncontrolled varicealbleeding in patients with decompensated cirrhosis J Hepatol200135590ndash597
21 Gaba RC Bui JT Cotler SJ et al Rebleeding rates followingTIPS forvariceal hemorrhage in the Viatorr era TIPS alone versusTIPS with variceal embolization Hepatol Int 20104749ndash756
22 Xiao T Chen L Chen W et al Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone versus TIPScombined with embolotherapy in advanced cirrhosis a retro-spective study J Clin Gastroenterol 201145643ndash650
23 Mahadeva S Bellamy MC Kessel D et al Cost-effectivenessof N-butyl-2-cyanoacrylate (histoacryl) glue injections versus trans-
jugular intrahepatic portosystemic shunt in the management of
926 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
Edso nGuzman FirmadodigitalmenteporEdso nGuzmanNombredereconocimiento(D N)cn=EdsonGuzmanoou=HNERMemail=e dson_guzmanhotmailcomc=PEFecha20140526200159-050 0
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 911
acute gastric variceal bleeding Am J Gastroenterol 2003982688ndash2693
24 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS inpatients with cirrhosis and variceal bleeding N Engl J Med 20103622370ndash2379
25 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic Histoacryl glue injection for the management of gastric variceal bleeding QJM 201110441ndash47
26 Choudhuri G Chetri K Bhat G et al Long-term ef 1047297cacy andsafety of N-butylcyanoacrylate in endoscopic treatment of gastric varices Trop Gastroenterol 201031155ndash164
27 Belletrutti PJ Romagnuolo J Hilsden RJ et al Endoscopicmanagement of gastric varices ef 1047297cacy and outcomes of gluingwith N-butyl-2-cyanoacrylate in a North American patient pop-ulation Can J Gastroenterol 200822931ndash936
28 Marques P Maluf-Filho F Kumar A et al Long-term outcomesof acute gastric variceal bleeding in 48 patients followingtreatment with cyanoacrylate Dig Dis Sci 200853544ndash550
29 Fry LC Neumann H Olano C et al Ef 1047297cacy complications andclinical outcomes of endoscopic sclerotherapy with N-butyl-2-cyanoacrylate for bleeding gastric varices Dig Dis 200826
300ndash30330 Cheng LF Wang ZQ Li CZ et al Treatment of gastric varices by
endoscopic sclerotherapy using butyl cyanoacrylate 10 yearsrsquoexperience of 635 cases Chin Med J (Engl) 20071202081ndash2085
31 Evrard S Dumonceau JM Delhaye M et al Endoscopic histo-acryl obliteration vs propranolol in the prevention of esoph-agogastric variceal rebleeding a randomized trial Endoscopy200335729ndash735
32 Mishra SR Chander SB Kumar A et al Endoscopic cyanoac-rylate injection versus beta-blocker for secondary prophylaxis of gastric variceal bleed a randomised controlled trial Gut 201059729ndash735
33 Binmoeller KF Weilert F Shah JN et al EUS-guided trans-esophageal treatment of gastric fundal varices with combinedcoiling and cyanoacrylate glue injection (with videos) Gastro-intest Endosc 2011741019ndash1025
34 Hung HH Chang CJ Hou MC et al Ef 1047297cacy of non-selectivebeta-blockers as adjunct to endoscopic prophylactic treatment for gastric variceal bleeding a randomized controlled trial J Hepatol2012561025ndash1032
35 McAvoy NC Plevris JN Hayes PC Human thrombin for thetreatment of gastric and ectopic varices World J Gastroenterol2012185912ndash5917
36 Krystallis C McAvoy NC Wilson J et al EUS-assisted thrombininjection for ectopic bleeding varices a case report and review
of the literature QJM 2012105355ndash
35837 Ramesh J Limdi JK Sharma V et al The use of thrombininjections in the management of bleeding gastric varices a single-center experience Gastrointest Endosc 200868877ndash882
38 Heneghan MA Byrne A Harrison PM An open pilot study of theeffects of a human 1047297brin glue for endoscopic treatment of pa-tients with acute bleeding from gastric varices GastrointestEndosc 200256422ndash426
39 Yang WL Tripathi D Therapondos G et al Endoscopic use of human thrombin in bleeding gastric varices Am J Gastroenterol2002971381ndash1385
40 Przemioslo RT McNair A Williams R Thrombin is effective inarresting bleeding from gastric variceal hemorrhage Dig Dis Sci199944778ndash781
41 Williams SG Peters RA Westaby D Thrombin an effectivetreatment for gastric variceal haemorrhage Gut 1994351287ndash1289
42 Yang Z Han G Wu Q et al Patency and clinical outcomesof transjugular intrahepatic portosystemic shunt with poly-tetra1047298uoroethylene-covered stents versus bare stents a meta-analysis J Gastroenterol Hepatol 2010251718ndash1725
43 Lo GH Liang HL Chen WC et al A prospective randomized
controlled trial of transjugular intrahepatic portosystemic shuntversus cyanoacrylate injection in the prevention of gastric vari-ceal rebleeding Endoscopy 200739679ndash685
44 Procaccini NJ Al-Osaimi AM Northup P et al Endoscopiccyanoacrylate versus transjugular intrahepatic portosystemicshunt for gastric variceal bleeding a single-center US analysisGastrointest Endosc 200970881ndash887
45 Kanagawa H Mima S Kouyama H et al Treatment of gastricfundal varices by balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 19961151ndash58
46 Hirota S Matsumoto S Tomita M et al Retrograde transvenousobliteration of gastric varices Radiology 1999211349ndash356
47 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-
tion of gastric varices part 2mdashstrategy and techniques basedon hemodynamic features Radiographics 200323921ndash937
48 Kiyosue H Mori H Matsumoto S et al Transcatheter oblitera-tion of gastric varices part 1mdashanatomic classi1047297cation Radio-graphics 200323911ndash920
49 Al-Osaimi AM Sabri SS Caldwell SH Balloon-occluded retro-grade transvenous obliteration (BRTO) preprocedural evalua-tion and imaging Semin Intervent Radiol 201128288ndash295
50 Cho SK Shin SW Lee IH et al Balloon-occluded retrogradetransvenous obliteration of gastric varices outcomes andcomplications in 49 patients AJR Am J Roentgenol 2007189W365ndashW372
51 Sonomura T Sato M Kishi K et al Balloon-occluded retrograde
transvenous obliteration for gastric varices a feasibility studyCardiovasc Intervent Radiol 19982127ndash30
52 Fukuda T Hirota S Sugimura K Long-term results of balloon-occluded retrograde transvenous obliteration for the treatmentof gastric varices and hepatic encephalopathy J Vasc IntervRadiol 200112327ndash336
53 Kitamoto M Imamura M Kamada K et al Balloon-occludedretrograde transvenous obliteration of gastric fundal varices withhemorrhage AJR Am J Roentgenol 20021781167ndash1174
54 Choi YH Yoon CJ Park JH et al Balloon-occluded retrogradetransvenous obliteration for gastric variceal bleeding its feasi-bility compared with transjugular intrahepatic portosystemicshunt Korean J Radiol 20034109ndash116
55 Ninoi T Nishida N Kaminou T et al Balloon-occluded retro-grade transvenous obliteration of gastric varices with gastro-renal shunt long-term follow-up in 78 patients AJR Am JRoentgenol 20051841340ndash1346
56 Hiraga N Aikata H Takaki S et al The long-term outcome of patients with bleeding gastric varices after balloon-occludedretrograde transvenous obliteration J Gastroenterol 200742663ndash672
57 Akahoshi T Hashizume M Tomikawa M et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices a 10-year experience J Gastroenterol Hepatol 2008231702ndash1709
58 Kumamoto M Toyonaga A Inoue H et al Long-term resultsof balloon-occluded retrograde transvenous obliteration for
June 2014 Management of Gastric Varices 927
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1011
gastric fundal varices hepatic deterioration links to portosys-temic shunt syndrome J Gastroenterol Hepatol 2010251129ndash1135
59 Sabri SS Swee W Turba UC et al Bleeding gastric varicesobliteration with balloon-occluded retrograde transvenousobliteration using sodium tetradecyl sulfate foam J Vasc IntervRadiol 201122309ndash316
60 Akahoshi T Tomikawa M Kamori M et al Impact of balloon-
occluded retrograde transvenous obliteration on managementof isolated fundal gastric variceal bleeding Hepatol Res 201242385ndash393
61 Choi SY Won JY Kim KA et al Foam sclerotherapy usingpolidocanol for balloon-occluded retrograde transvenous oblit-eration (BRTO) Eur Radiol 201121122ndash129
62 Clements W Cavanagh K Ali F et al Variant treatment for gastric varices with polidocanol foam using balloon-occludedretrograde transvenous obliteration a pilot study J Med Imag-ing Radiat Oncol 201256599ndash605
63 Saad WE The history and evolution of balloon-occludedretrograde transvenous obliteration (BRTO) from the UnitedStates to Japan and back Semin Intervent Radiol 201128
283ndash28764 Patel A Fischman AM Saad WE Balloon-occluded retrograde
transvenous obliteration of gastric varices AJR Am J Roent-genol 2012199721ndash729
65 Hong CH Kim HJ Park JH et al Treatment of patients withgastric variceal hemorrhage endoscopic N-butyl-2-cyanoacry-late injection versus balloon-occluded retrograde transvenousobliteration J Gastroenterol Hepatol 200924372ndash378
66 Saad WE Sabri SS Balloon-occluded retrograde transvenousobliteration (BRTO) technical results and outcomes SeminIntervent Radiol 201128333ndash338
67 Ninoi T Nakamura K Kaminou T et al TIPS versus trans-catheter sclerotherapy for gastric varices AJR Am J Roentgenol
2004183369ndash
37668 Saad WE Al-Osaimi AM Caldwell SH Pre- and post-balloon-
occluded retrograde transvenous obliteration clinical evalua-tion management and imaging indications managementprotocols and follow-up Tech Vasc Interv Radiol 201215165ndash202
69 Ogawa K Ishikawa S Naritaka Y et al Clinical evaluation of endo-scopic injection sclerotherapy using n-butyl-2-cyanoacrylate for gastric variceal bleedingJ Gastroenterol Hepatol 199914245ndash250
70 Kind R Guglielmi A Rodella L et al Bucrylate treatment of bleeding gastric varices 12 yearsrsquo experience Endoscopy 200032512ndash519
71 Huang YH Yeh HZ Chen GH et al Endoscopic treatment of bleeding gastric varices by N-butyl-2- cyanoacrylate (Histoacryl)
injection long-term ef 1047297cacy and safety Gastrointest Endosc200052160ndash167
72 Akahoshi T Hashizume M Shimabukuro R et al Long-termresults of endoscopic Histoacryl injection sclerotherapy for gastric variceal bleeding a 10-year experience Surgery 2002131(Suppl)S176ndashS181
73 Rengstorff DS Binmoeller KF A pilot study of 2-octyl cyano-acrylate injection for treatment of gastric fundal varices inhumans Gastrointest Endosc 200459553ndash558
74 Mumtaz K Majid S Shah H et al Prevalence of gastric varicesand results of sclerotherapy with N-butyl 2 cyanoacrylate for controlling acute gastric variceal bleeding World J Gastro-enterol 2007131247ndash1251
75 Paik CN Kim SW Lee IS et al The therapeutic effect of cyanoacrylate on gastric variceal bleeding and factors related toclinical outcome J Clin Gastroenterol 200842916ndash922
76 Monsanto P Almeida N Rosa A et al Endoscopic treatment of bleeding gastric varices with histoacryl (N-butyl-2-cyanoacry-late) a South European single center experience Indian JGastroenterol 201232227ndash231
77 Hou MC Lin HC Lee HS et al A randomized trial of endoscopiccyanoacrylate injection for acute gastric variceal bleeding 05 mLversus 10 mL Gastrointest Endosc 200970668ndash675
Reprint requests Address requests for reprints to Juan Carlos Garcia-Pagaacuten MD HepaticHemodynamic Laboratory Liver Unit Hospital Clinic Villarroel 170 08036Barcelona Spain e-mail jcgarciaclinicubes fax 34-93-227-98-56
Con1047298icts of interestThese authors disclose the following Juan Garcia-Pagaacuten received grant sup-port from GORE Andres Cardenas has been a consultant to Limmedx LLCFrontier Medex and BMJ Publishing Group The remaining authors disclose nocon1047298icts
928 GarciandashPaga n et al Clinical Gastroenterology and Hepatology Vol 12 No 6
8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1

8102019 2014 06 Manejo de Las Varices Gastricas
httpslidepdfcomreaderfull2014-06-manejo-de-las-varices-gastricas 1111
Supplementary Table 1 Studies That Used TIPS or CA in Bleeding GV
First authoryear (reference) Design n
Treatmentreceived (n)
Initialcontrol ( ) Mortality ( )
Any sourceof rebleeding ( )
Follow-up ( mo )
Mahadeva 200323 Cohorts retrospective(GOV1 and GOV2)
43 TIPS (20)vs glue (23)
TIPS (90)vs glue (96)
At 6 monthsTIPS (25) vsglue (15)
At 6 months TIPS (15)vs glue (30)
6
Lo 200743 Randomized prospective(mostly GOV1 andGOV2 and few IGV1)
72 TIPS (35)vs glue (37)
NA TIPS (30) vsglue (17)
TIPS (43) vs glue (59) 33
Procaccini 200944 Cohorts retrospective(GV type not speci1047297ed)
105 TIPS (44)vs glue (61)
NA At 1 yearTIPS (33) vsglue (28)
At 1 year TIPS(25) vs glue (10)
TIPS (48)glue (74)
June 2014 Management of Gastric Varices 928e1