©2012 mfmer | 3188678-1 adni clinical core paul aisen ron petersen michael donohue jennifer salazar
TRANSCRIPT
©2012 MFMER | 3188678-1
ADNI Clinical Core
Paul Aisen
Ron Petersen
Michael Donohue
Jennifer Salazar
ADNI 2 Enrollment Update
• ADNI2 enrollment closed - July 1, 2013
• New ADNI2 subjects enrolled: 767 (not including baseline fails)
• ADNI 1 continuations to ADNI 2: 276
• ADNI GO continuations to ADNI 2: 120
• Total Enrolled in ADNI 2: 1,033 ((767 totaled enrolled in ADNI2 - 130 reported discontinuations) + 276 ADNI1 rollovers + 120 ADNIGO rollovers)
©2012 MFMER | 3188678-2
©2012 MFMER | 3188678-3
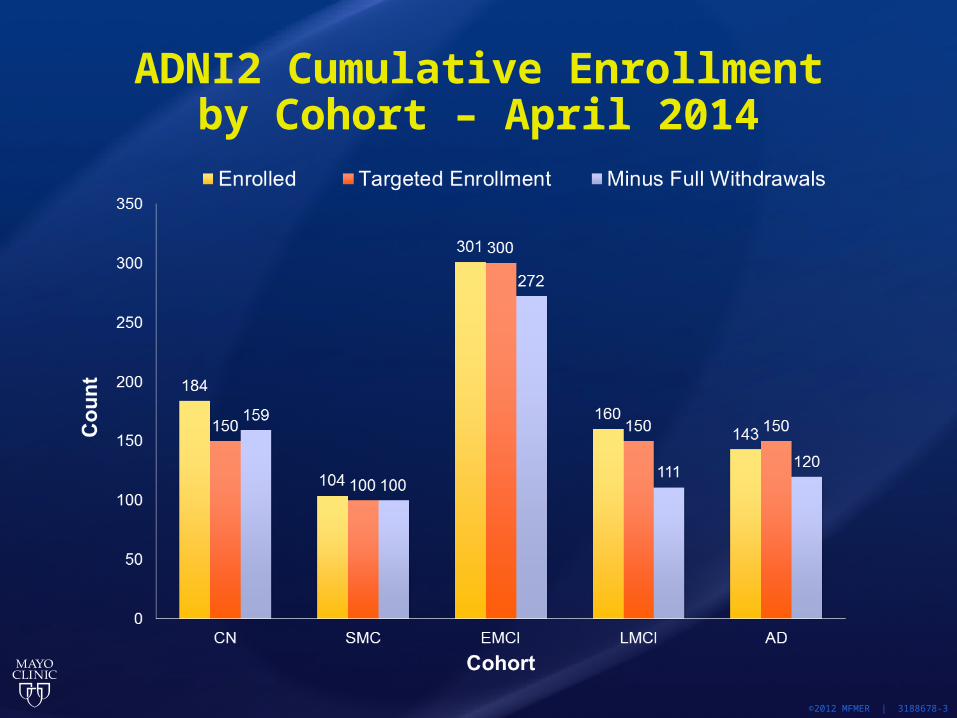
ADNI2 Cumulative Enrollmentby Cohort – April 2014
©2012 MFMER | 3188678-4
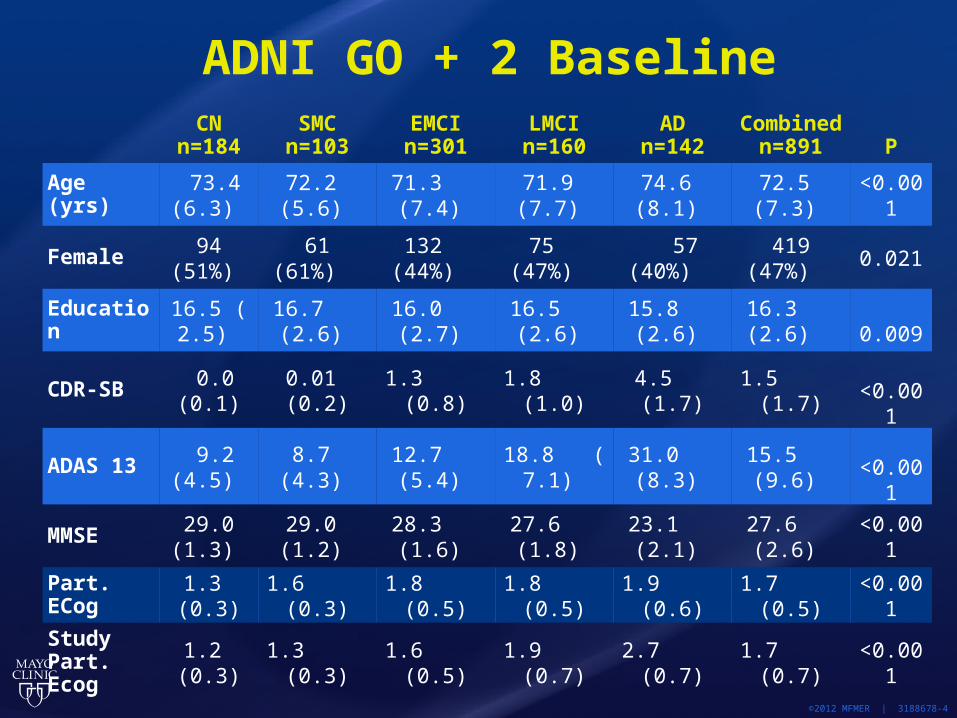
CN
n=184SMC
n=103EMCIn=301
LMCIn=160
ADn=142
Combinedn=891 P
Age (yrs) 73.4 (6.3)
72.2 (5.6)
71.3 (7.4)
71.9 (7.7)
74.6 (8.1)
72.5 (7.3)
<0.001
Female 94 (51%)
61 (61%)
132 (44%)
75 (47%)
57 (40%)
419 (47%)
0.021
Education 16.5 ( 2.5)
16.7 (2.6)
16.0 (2.7)
16.5 (2.6)
15.8 (2.6)
16.3 (2.6)
0.009
CDR-SB 0.0 (0.1)
0.01 (0.2)
1.3 (0.8)
1.8 (1.0)
4.5 (1.7)
1.5 (1.7)
<0.001
ADAS 13 9.2 (4.5)
8.7 (4.3)
12.7 (5.4)
18.8 ( 7.1)
31.0 (8.3)
15.5 (9.6)
<0.001
MMSE 29.0 (1.3)
29.0 (1.2)
28.3 (1.6)
27.6 (1.8)
23.1 (2.1)
27.6 (2.6)
<0.001
Part. ECog
1.3 (0.3)
1.6 (0.3)
1.8 (0.5)
1.8 (0.5)
1.9 (0.6)
1.7 (0.5)
<0.001
Study Part. Ecog
1.2 (0.3)
1.3 (0.3)
1.6 (0.5)
1.9 (0.7)
2.7 (0.7)
1.7 (0.7)
<0.001
ADNI GO + 2 Baseline
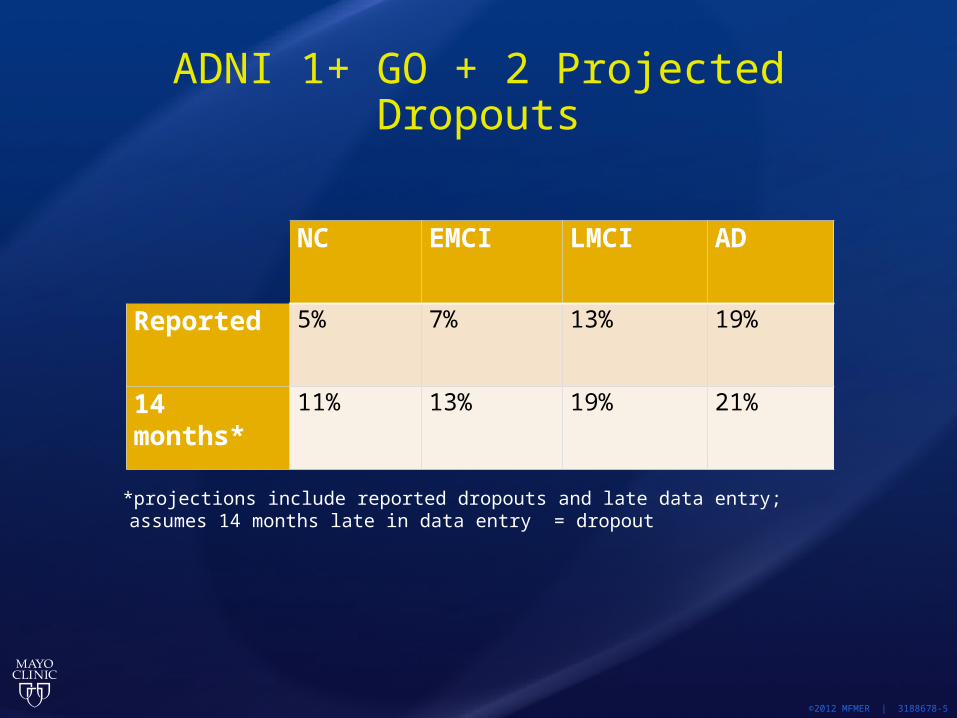
ADNI 1+ GO + 2 Projected Dropouts
©2012 MFMER | 3188678-5
NC EMCI LMCI AD
Reported 5% 7% 13% 19%
14 months* 11% 13% 19% 21%
*projections include reported dropouts and late data entry; assumes 14 months late in data entry = dropout
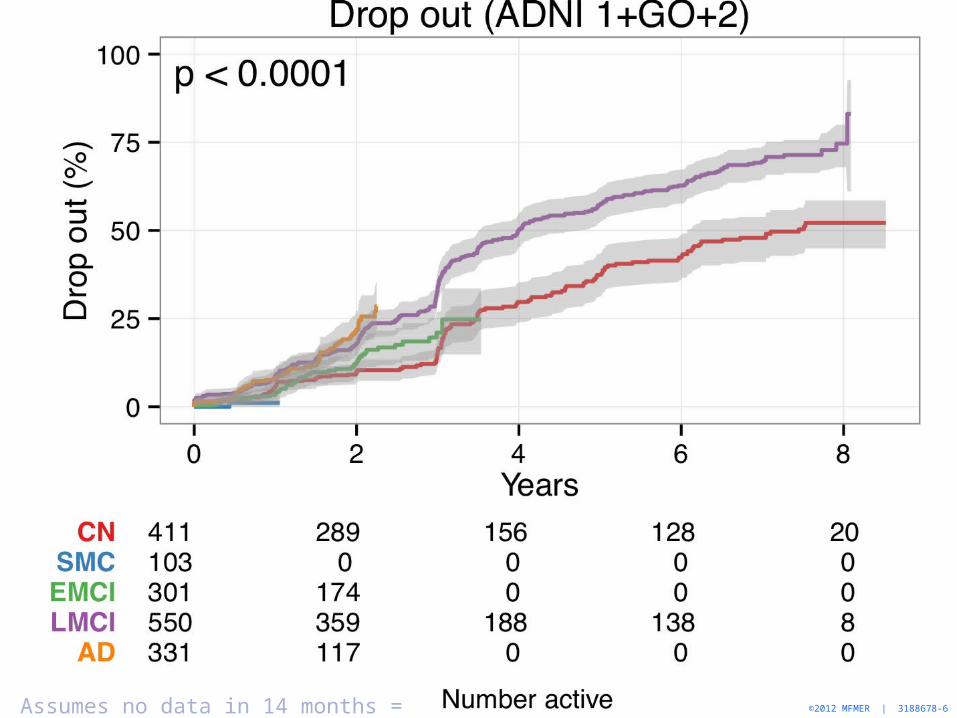
©2012 MFMER | 3188678-6Assumes no data in 14 months = dropout

©2012 MFMER | 3188678-7Assumes no data in 14 months = dropout
©2014 MFMER | 3343740-8
Dx
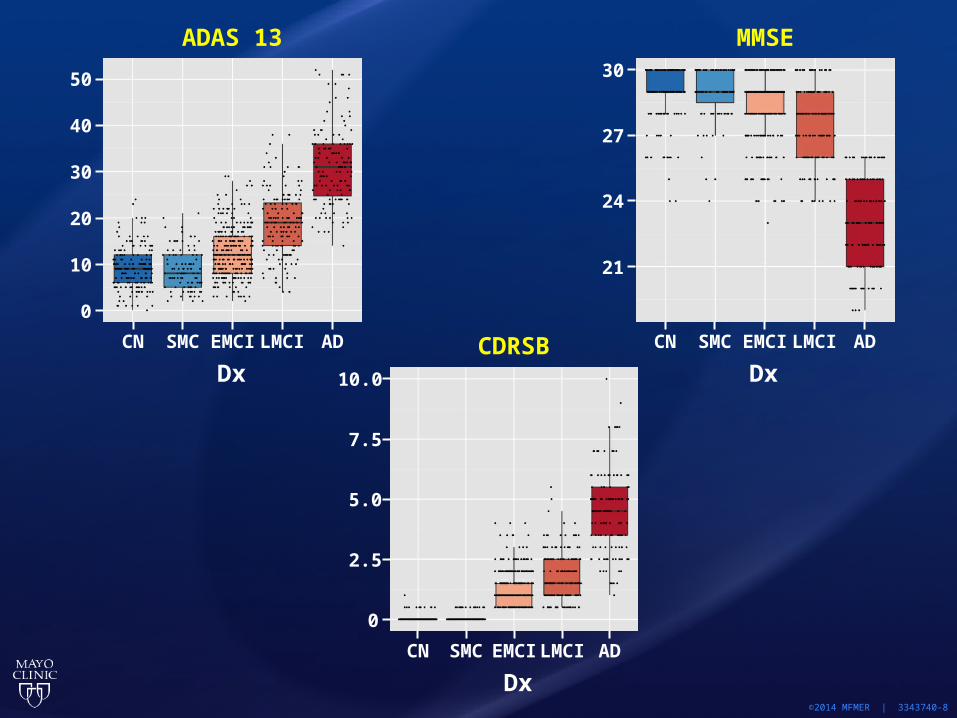
ADAS 13
50
40
30
20
10
0
CN SMC EMCI LMCI AD
MMSE
Dx
21
CN SMC EMCI LMCI AD
24
27
30
CDRSB
Dx
0
CN SMC EMCILMCI AD
2.5
5.0
7.5
10.0
©2014 MFMER | 3343740-9
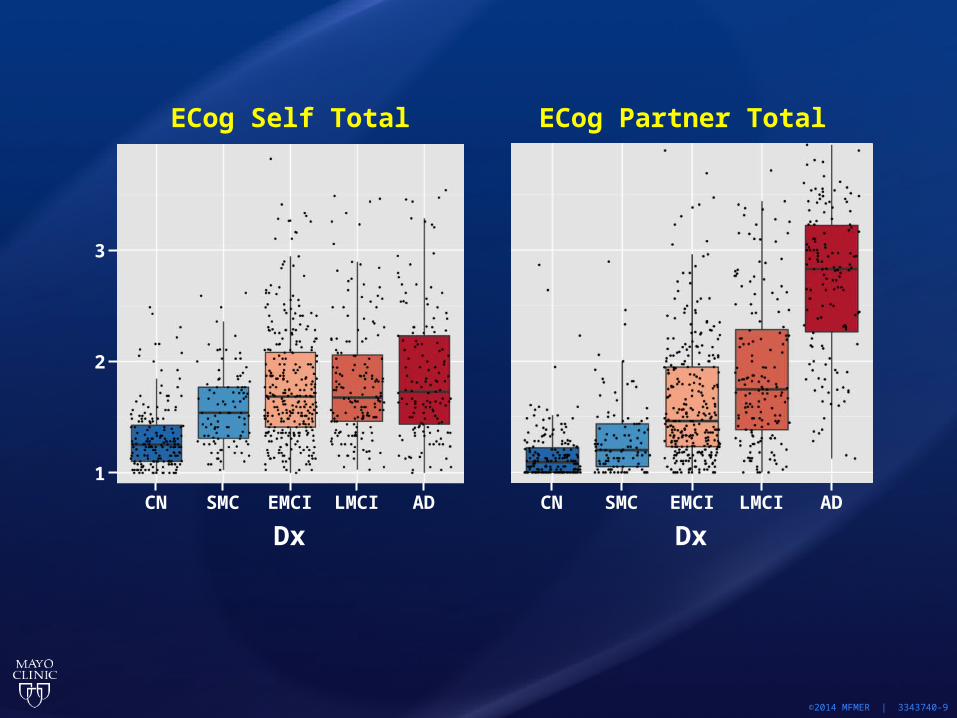
ECog Self Total
DxCN SMC EMCI LMCI AD
1
2
3
DxCN SMC EMCI LMCI AD
ECog Partner Total
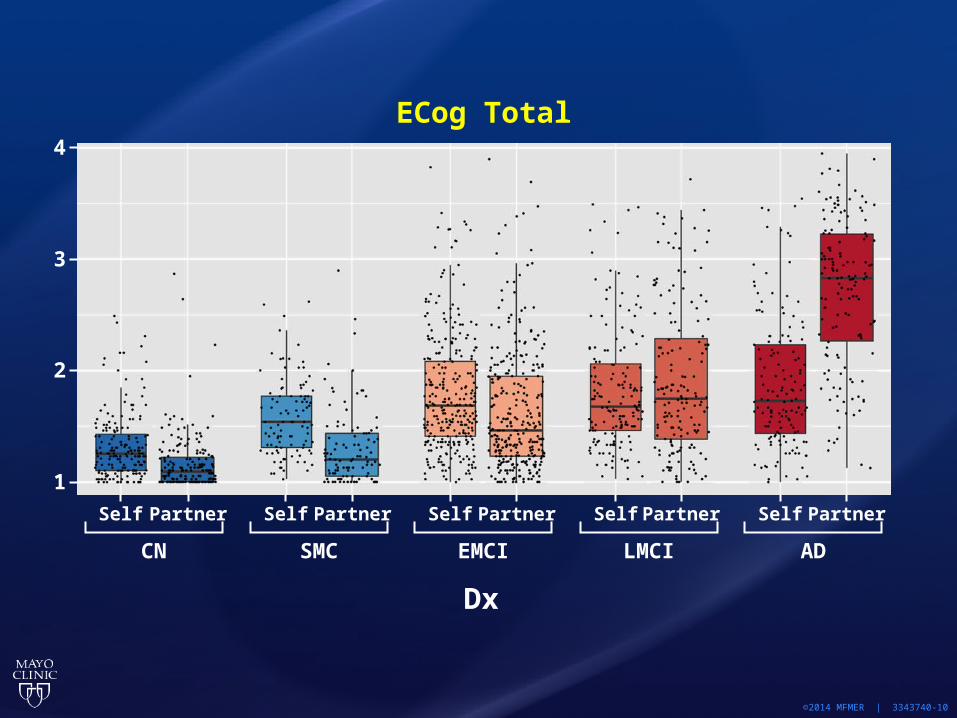
©2014 MFMER | 3343740-10
ECog Total
Dx
Self
1
2
3
Partner
CN
Self Partner
SMC
Self Partner
EMCI
Self Partner
LMCI
Self Partner
AD
4
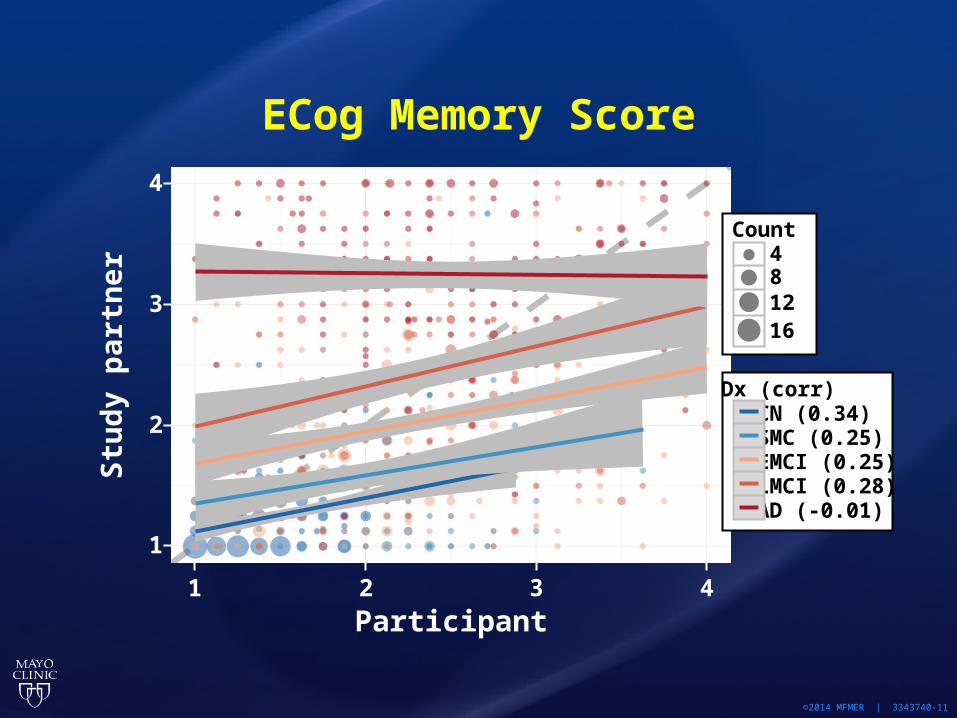
©2014 MFMER | 3343740-11
Participant
1
1
2
3
4
2 3 4
Stu
dy
par
tner
ECog Memory Score
Count481216
Dx (corr)CN (0.34)SMC (0.25)EMCI (0.25)LMCI (0.28)AD (-0.01)
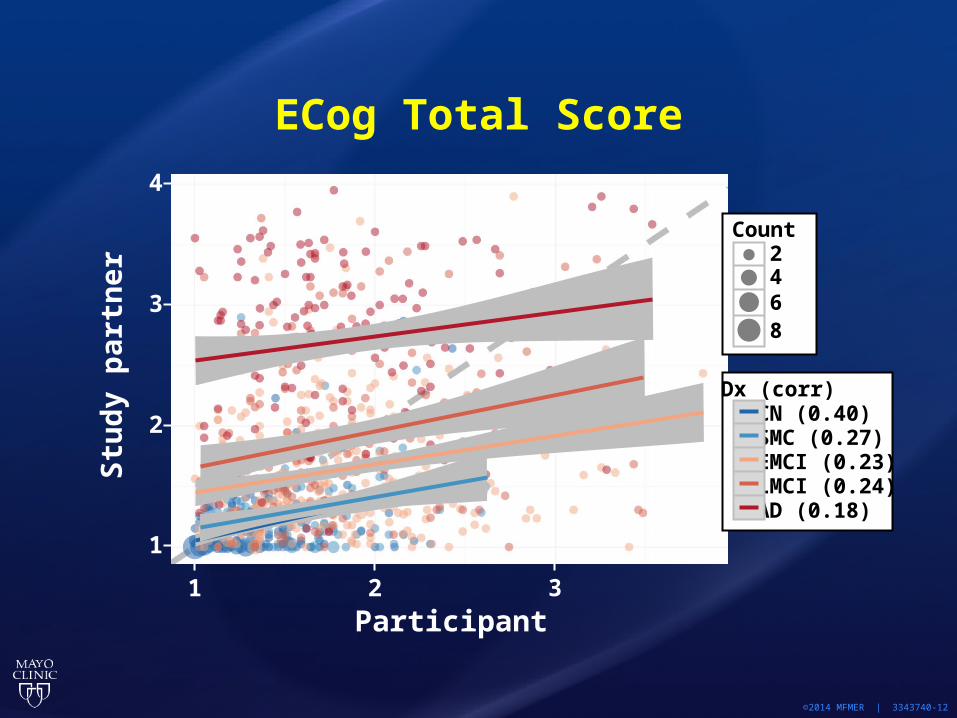
©2014 MFMER | 3343740-12
Stu
dy
par
tner
Participant
1
1
2
3
4
2 3
ECog Total Score
Count2468
Dx (corr)CN (0.40)SMC (0.27)EMCI (0.23)LMCI (0.24)AD (0.18)
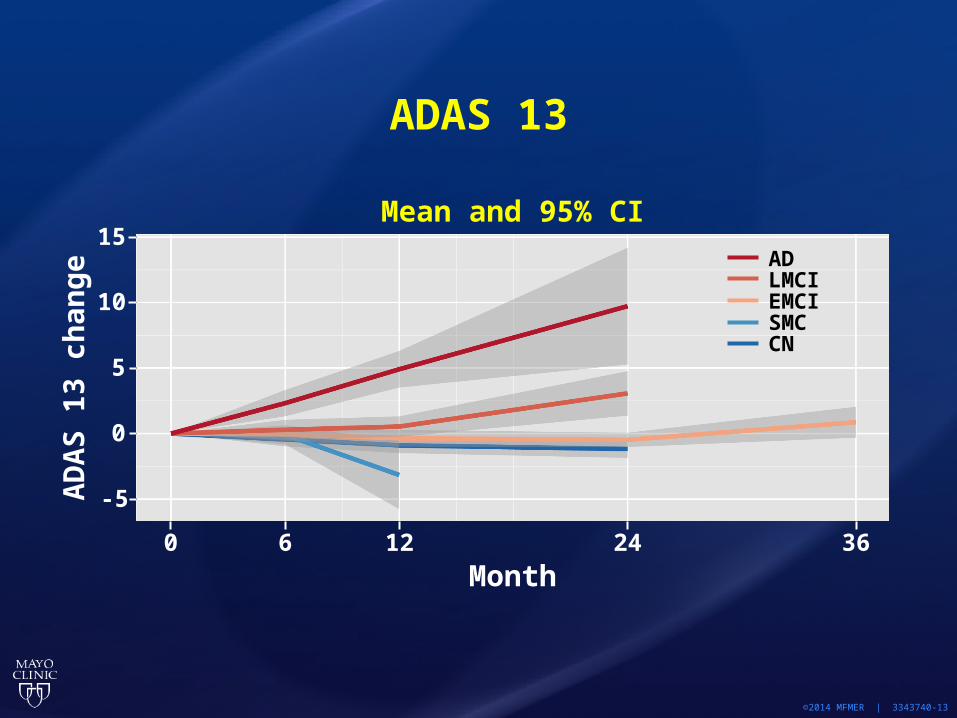
©2014 MFMER | 3343740-13
ADAS 13A
DA
S 1
3 ch
ang
e
Month
-5
0
Mean and 95% CI
0
5
10
15
6 12 24 36
ADLMCIEMCISMCCN
©2014 MFMER | 3343740-14
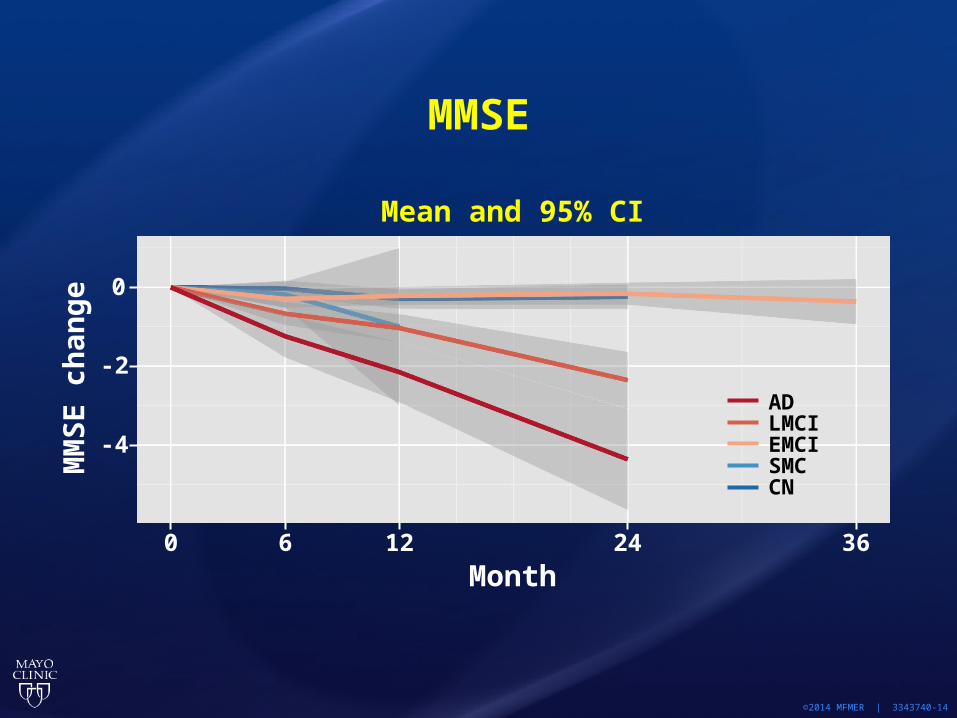
MMSEM
MS
E c
han
ge
Month
-2
0
Mean and 95% CI
0
6 12 24 36
-4
ADLMCIEMCISMCCN

NL to MCI (1+GO+2)*
©2012 MFMER | 3188678-15* Imputed baseline AV45 where not observed
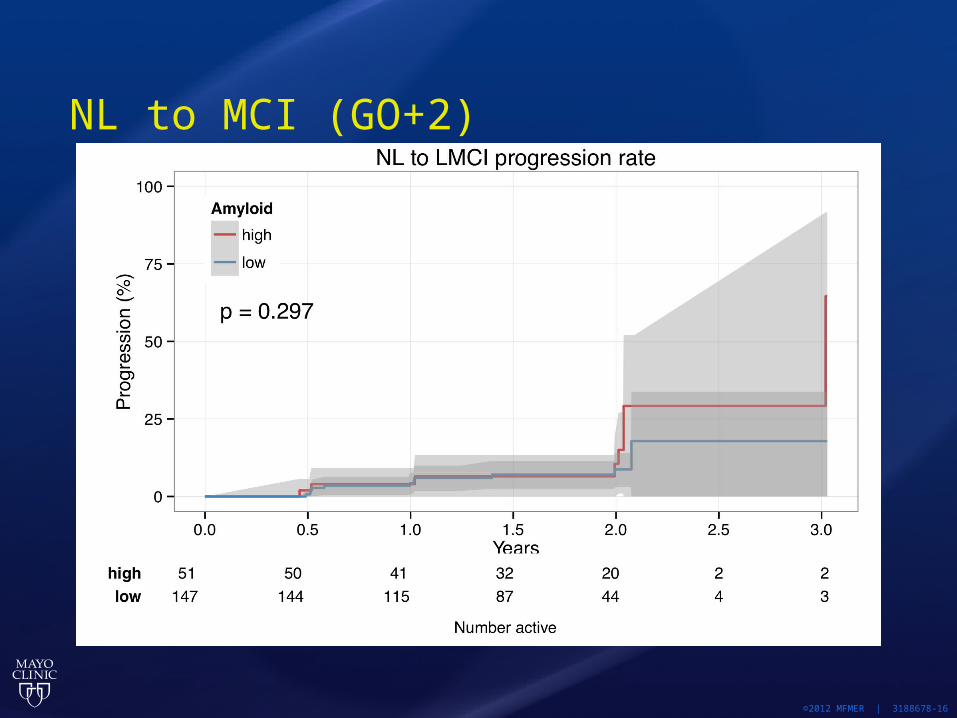
NL to MCI (GO+2)
©2012 MFMER | 3188678-16
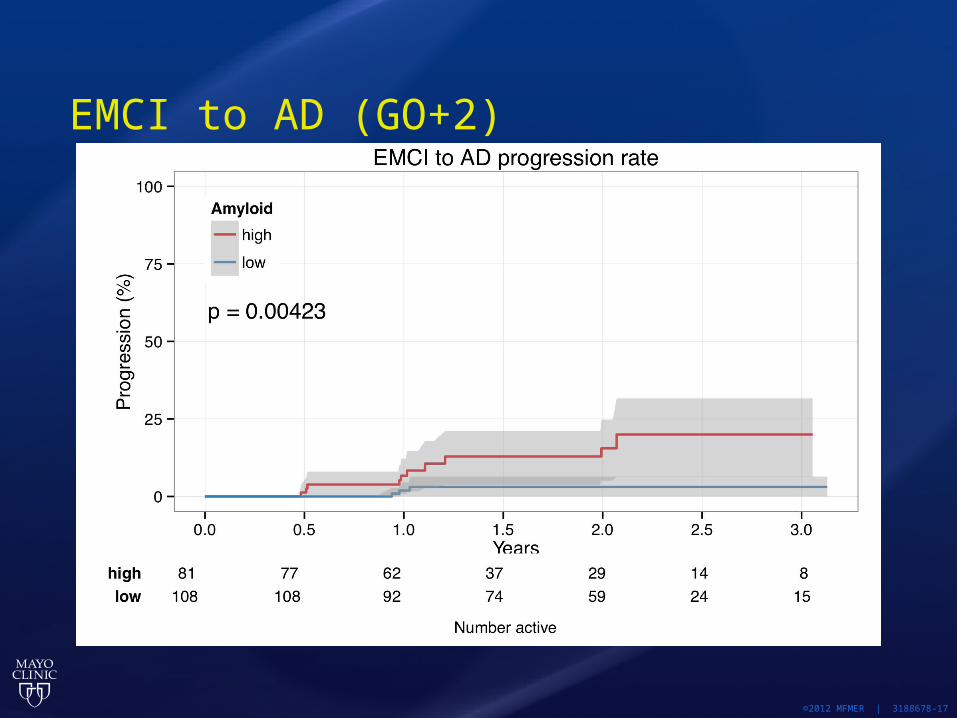
EMCI to AD (GO+2)
©2012 MFMER | 3188678-17

LMCI to AD (1+GO+2)
©2012 MFMER | 3188678-18
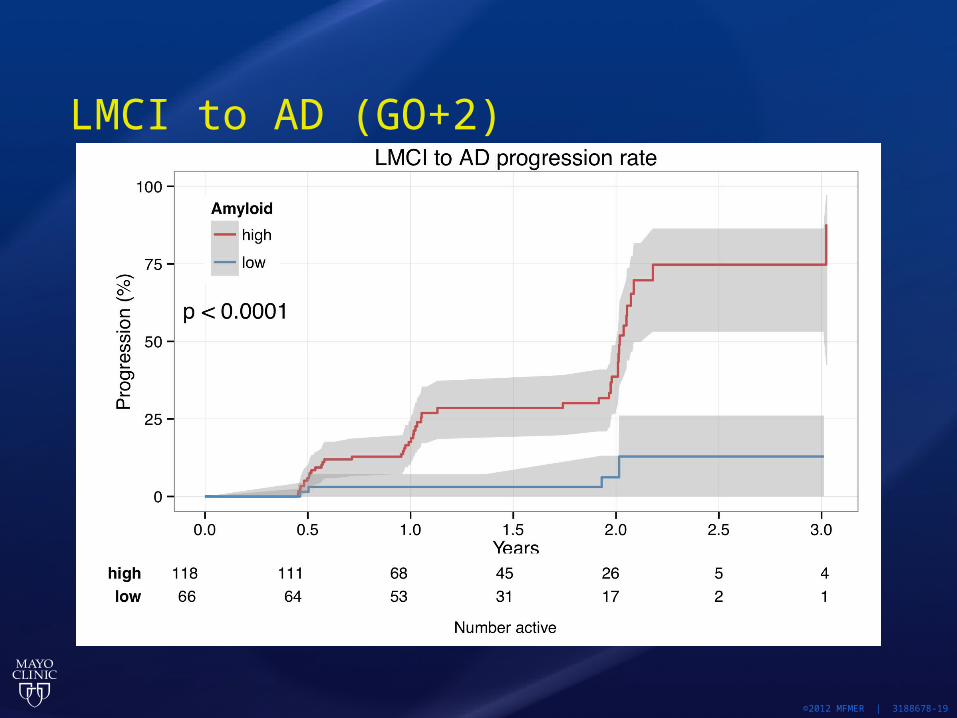
LMCI to AD (GO+2)
©2012 MFMER | 3188678-19

ADNI3 CLINICAL CORE
Paul AisenRon PetersenMike DonohueMike Weiner
ADNI3 Primary Aim
Validate biomarkers for clinical trials
To guide ADNI3, we need to reach consensus on the direction of future AD trials
ADNI3 additional goals
Address gaps in our understanding of the clinical spectrum of AD
Utilize biomarker advances (eg tau PET) to further elucidate AD neurobiology
Evaluate outcome measures, including computerized cognitive assessments
Facilitate new and promising trial designs
Focus on early stage disease? Biggest gaps are early Very early trials may be optimal for
disease-modification. The likelihood of major, useful advances in AD dementia trials may be small. There is certainly a need for drug
development in AD dementia, including disease-modifiers, cognitive enhancers and behavioral therapies. But such trials are based on clinical/cognitive/behavioral measures that are fairly well established.
ADNI2 cohorts
Normal: CDR=0, no subjective complaints, LogMem nl, MMSE 24-30, age>=65 or 70 (adjusted periodically, wider range for minorities)
SMC: CDR=0, subjective complaints, LogMem nl, MMSE 24-30, age>=65 or 70 (adjusted periodically)
EMCI: CDR=.5, LogMem 1sd below norm, MMSE 24-30, age 55-90
LMCI: CDR=.5, LogMem 1.5sd below norm, MMSE 24-30, age 55-90
Mild AD: CDR=.5-1, dementia, LogMem 1.5sd below norm, MMSE 20-26, age 55-90
ADNI3 clinical trial aims
Study the utility of imaging and biochemical markers in prodromal and preclinical AD trials
Optimize cognitive and PRO-type measures in prodromal and preclinical AD trials
Facilitate primary prevention trials (?), ie, treatment before brain amyloid is elevated This would be new territory and somewhat risky In favor: primary prevention is the ultimate goal, and
ADNI must lead the way Against: Is industry interested? Can we find an efficient
way to study individuals not yet at the preclinical stage?

These aims suggest: Drop AD dementia from ADNI? Continue indefinite follow-up of other existing ADNI2
cohorts Add new biomarkers (tau PET) Manage overall subject burden (drop FDG PET?) Include: cognitive measures optimized for clinically
normal subjects, computerized assessments, PROs, possibly explore functional performance testing
Reduce lower age limit (?) Consider ways to enrich young normal for risk of AD
(FHx, APOE, vascular risk, subjective concerns …)
Specific ideas for ADNI3
Drop AD dementia Combine LMCI, EMCI Reduce lower age limit on normal, but
with enrichment based on risk
Focus on intermediate amyloid PET suvr group?

Example: new subjects for ADNI3Age CDR Memor
y concerns
Risk
Young normal at risk
50-60 0 + or - E4 carrieror known amyloid PET positive or CSF positive or strongly positive family history
Normals 60-90 0 + or -
MCI 50-90 0.5 +
continue ADNI2 normal, SMC, EMCI, (LMCI?) drop ADNI2 AD cohort, subjects that have converted to AD dementia
Do we need younger subjects? Perhaps: primary prevention will target
middle age Or: why not study transition to amyloid
positivity in older individuals?
ADNI3 schedule, new and carry-over Semiannual: mail-in assessments Annual: MRI, blood, NP tests,
computerized tests, PROs Biennial: amyloid PET, tau PET, LP
Other ideas
Mild BehavioraI Impairment (Jesse Cedarbaum)
New biomarker approaches (ophthalmologic?)
Web-based recruitment/testing Home-based (snail mail?) assessments Utilize 23 and me data