2012-566 medical bcbsal health plan booklet 566-jeffersonville
DESCRIPTION
BlueCard PPO Group 49992 Division 566 Only - Jeffersonville Effective January 1, 2012TRANSCRIPT
TMSi 80/20 Plan
BlueCard PPO Group 49992 Division 566 Only - Jeffersonville
Effective January 1, 2012
Page 1
TMSi BlueCard PPO
Effective January 1, 2012 BENEFIT IN-NETWORK OUT-OF-NETWORK
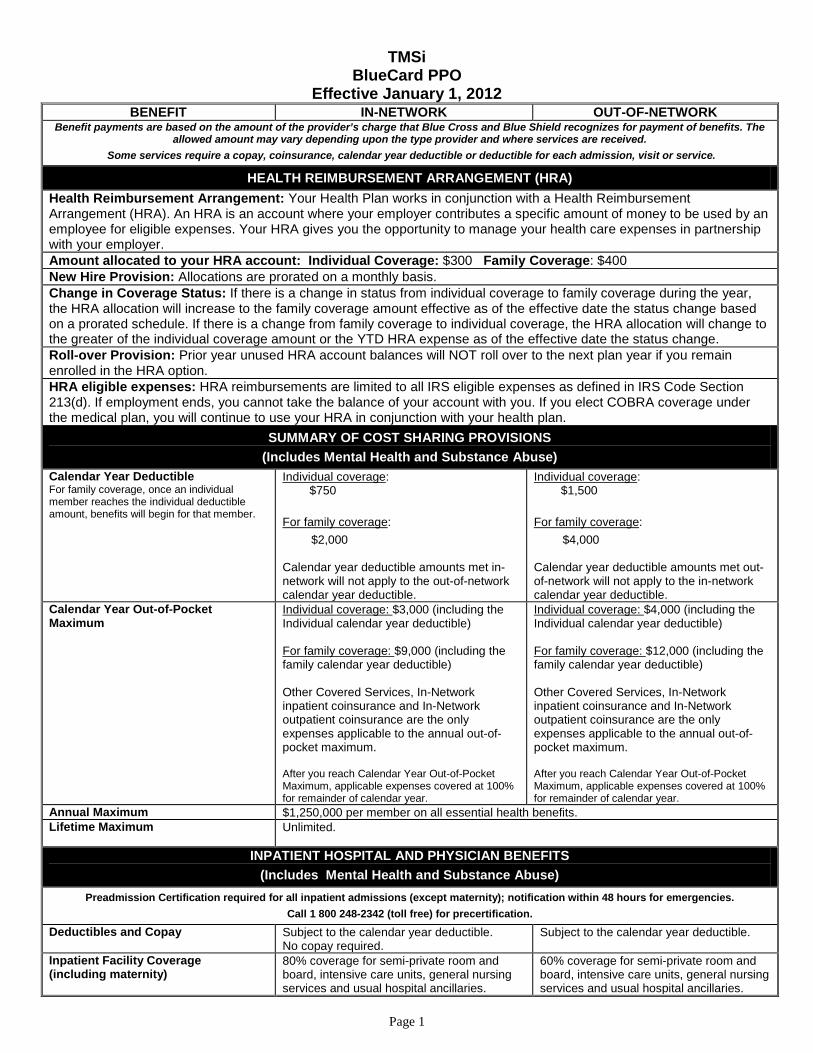
Benefit payments are based on the amount of the provider’s charge that Blue Cross and Blue Shield recognizes for payment of benefits. The allowed amount may vary depending upon the type provider and where services are received.
Some services require a copay, coinsurance, calendar year deductible or deductible for each admission, visit or service.
HEALTH REIMBURSEMENT ARRANGEMENT (HRA) Health Reimbursement Arrangement: Your Health Plan works in conjunction with a Health Reimbursement Arrangement (HRA). An HRA is an account where your employer contributes a specific amount of money to be used by an employee for eligible expenses. Your HRA gives you the opportunity to manage your health care expenses in partnership with your employer. Amount allocated to your HRA account: Individual Coverage: $300 Family Coverage: $400 New Hire Provision: Allocations are prorated on a monthly basis. Change in Coverage Status: If there is a change in status from individual coverage to family coverage during the year, the HRA allocation will increase to the family coverage amount effective as of the effective date the status change based on a prorated schedule. If there is a change from family coverage to individual coverage, the HRA allocation will change to the greater of the individual coverage amount or the YTD HRA expense as of the effective date the status change. Roll-over Provision: Prior year unused HRA account balances will NOT roll over to the next plan year if you remain enrolled in the HRA option. HRA eligible expenses: HRA reimbursements are limited to all IRS eligible expenses as defined in IRS Code Section 213(d). If employment ends, you cannot take the balance of your account with you. If you elect COBRA coverage under the medical plan, you will continue to use your HRA in conjunction with your health plan.
SUMMARY OF COST SHARING PROVISIONS (Includes Mental Health and Substance Abuse)
Calendar Year Deductible For family coverage, once an individual member reaches the individual deductible amount, benefits will begin for that member.
Individual coverage: $750
For family coverage:
$2,000
Calendar year deductible amounts met in-network will not apply to the out-of-network calendar year deductible.
Individual coverage: $1,500
For family coverage:
$4,000
Calendar year deductible amounts met out-of-network will not apply to the in-network calendar year deductible.
Calendar Year Out-of-Pocket Maximum
Individual coverage: $3,000 (including the Individual calendar year deductible) For family coverage: $9,000 (including the family calendar year deductible) Other Covered Services, In-Network inpatient coinsurance and In-Network outpatient coinsurance are the only expenses applicable to the annual out-of-pocket maximum. After you reach Calendar Year Out-of-Pocket Maximum, applicable expenses covered at 100% for remainder of calendar year.
Individual coverage: $4,000 (including the Individual calendar year deductible) For family coverage: $12,000 (including the family calendar year deductible) Other Covered Services, In-Network inpatient coinsurance and In-Network outpatient coinsurance are the only expenses applicable to the annual out-of-pocket maximum. After you reach Calendar Year Out-of-Pocket Maximum, applicable expenses covered at 100% for remainder of calendar year.
Annual Maximum $1,250,000 per member on all essential health benefits. Lifetime Maximum
Unlimited.
INPATIENT HOSPITAL AND PHYSICIAN BENEFITS (Includes Mental Health and Substance Abuse)
Preadmission Certification required for all inpatient admissions (except maternity); notification within 48 hours for emergencies. Call 1 800 248-2342 (toll free) for precertification.
Deductibles and Copay Subject to the calendar year deductible. No copay required.
Subject to the calendar year deductible.
Inpatient Facility Coverage (including maternity)
80% coverage for semi-private room and board, intensive care units, general nursing services and usual hospital ancillaries.
60% coverage for semi-private room and board, intensive care units, general nursing services and usual hospital ancillaries.
Page 2
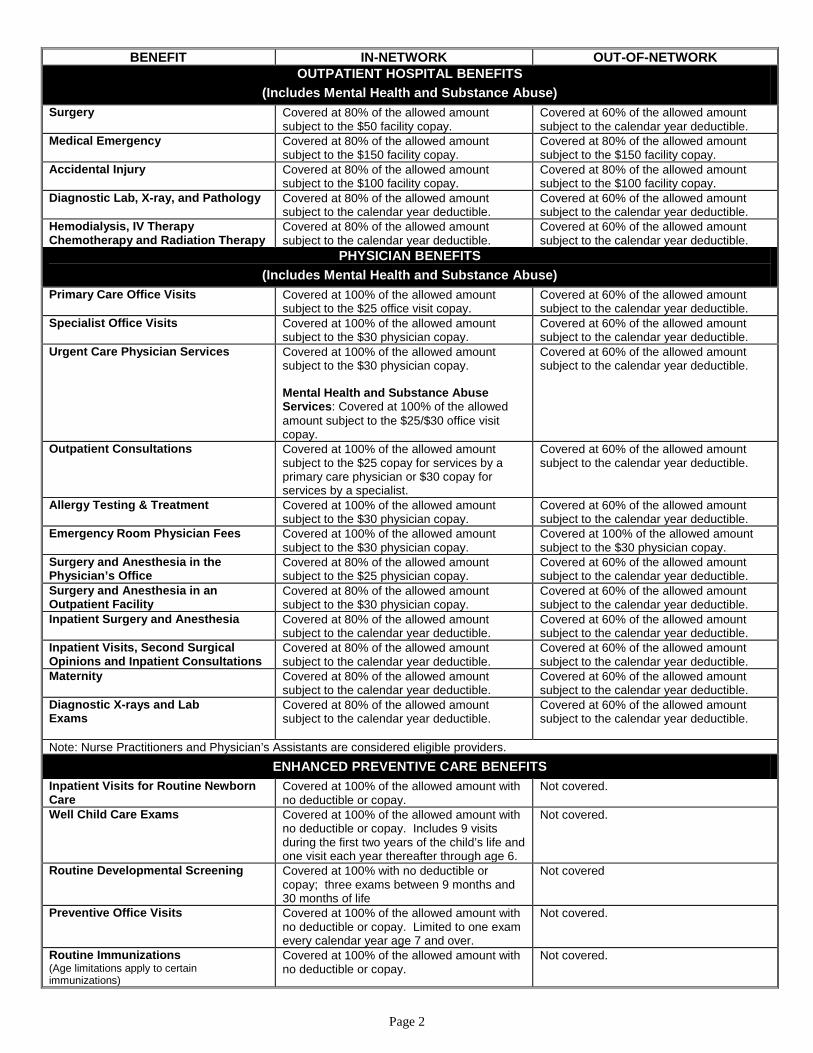
BENEFIT IN-NETWORK OUT-OF-NETWORK OUTPATIENT HOSPITAL BENEFITS
(Includes Mental Health and Substance Abuse) Surgery Covered at 80% of the allowed amount
subject to the $50 facility copay. Covered at 60% of the allowed amount subject to the calendar year deductible.
Medical Emergency
Covered at 80% of the allowed amount subject to the $150 facility copay.
Covered at 80% of the allowed amount subject to the $150 facility copay.
Accidental Injury Covered at 80% of the allowed amount subject to the $100 facility copay.
Covered at 80% of the allowed amount subject to the $100 facility copay.
Diagnostic Lab, X-ray, and Pathology Covered at 80% of the allowed amount subject to the calendar year deductible.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Hemodialysis, IV Therapy Chemotherapy and Radiation Therapy
Covered at 80% of the allowed amount subject to the calendar year deductible.
Covered at 60% of the allowed amount subject to the calendar year deductible.
PHYSICIAN BENEFITS (Includes Mental Health and Substance Abuse)
Primary Care Office Visits Covered at 100% of the allowed amount subject to the $25 office visit copay.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Specialist Office Visits Covered at 100% of the allowed amount subject to the $30 physician copay.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Urgent Care Physician Services Covered at 100% of the allowed amount subject to the $30 physician copay. Mental Health and Substance Abuse Services: Covered at 100% of the allowed amount subject to the $25/$30 office visit copay.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Outpatient Consultations Covered at 100% of the allowed amount subject to the $25 copay for services by a primary care physician or $30 copay for services by a specialist.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Allergy Testing & Treatment Covered at 100% of the allowed amount subject to the $30 physician copay.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Emergency Room Physician Fees Covered at 100% of the allowed amount subject to the $30 physician copay.
Covered at 100% of the allowed amount subject to the $30 physician copay.
Surgery and Anesthesia in the Physician’s Office
Covered at 80% of the allowed amount subject to the $25 physician copay.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Surgery and Anesthesia in an Outpatient Facility
Covered at 80% of the allowed amount subject to the $30 physician copay.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Inpatient Surgery and Anesthesia Covered at 80% of the allowed amount subject to the calendar year deductible.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Inpatient Visits, Second Surgical Opinions and Inpatient Consultations
Covered at 80% of the allowed amount subject to the calendar year deductible.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Maternity Covered at 80% of the allowed amount subject to the calendar year deductible.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Diagnostic X-rays and Lab Exams
Covered at 80% of the allowed amount subject to the calendar year deductible.
Covered at 60% of the allowed amount subject to the calendar year deductible.
Note: Nurse Practitioners and Physician’s Assistants are considered eligible providers. ENHANCED PREVENTIVE CARE BENEFITS
Inpatient Visits for Routine Newborn Care
Covered at 100% of the allowed amount with no deductible or copay.
Not covered.
Well Child Care Exams Covered at 100% of the allowed amount with no deductible or copay. Includes 9 visits during the first two years of the child’s life and one visit each year thereafter through age 6.
Not covered.
Routine Developmental Screening
Covered at 100% with no deductible or copay; three exams between 9 months and 30 months of life
Not covered
Preventive Office Visits Covered at 100% of the allowed amount with no deductible or copay. Limited to one exam every calendar year age 7 and over.
Not covered.
Routine Immunizations (Age limitations apply to certain immunizations)
Covered at 100% of the allowed amount with no deductible or copay.
Not covered.

Page 3
BENEFIT IN-NETWORK OUT-OF-NETWORK Routine Pap Smears Covered at 100% of the allowed amount with
no deductible or copay. Limited to one per year.
Not covered.
Routine Human Papillomavirus (HPV) Testing
Covered at 100% of the allowed amount with no deductible or copay; one routine test every three calendar years for females ages 30 and over.
Not covered.
Routine Chlamydia Screening
Covered at 100% with no deductible or copay; one per calendar year for females ages 15-24
Not covered
Routine Mammograms Covered at 100% of the allowed amount with no deductible or copay. Limited to one exam for females between the ages of 35-39 and one per year for females age 40 and above.
Not covered.
Routine Prostate Specific Antigen (includes digital rectal exam)
Covered at 100% of the allowed amount with no deductible or copay. Limited to one per year for males age 40 and over.
Not covered.
Routine Colonoscopy Covered at 100% of the allowed amount with no deductible or copay for members over 50 once every three calendar years.
Not covered.
Other Routine Screening Covered at 100% of the allowed amount with no deductible or copay. Includes the following: Urinalysis and CBC (when necessary), TB skin testing (when necessary) , Cholesterol Screening (once every year), Lipid panel (once every year), Hemocult (annually, ages 50 and over), Sigmoidoscopy (every 3 years, ages 50 and over).
Not covered.
Note: In case of illness or family history of cancer, services generally are not considered preventive and may be covered by other plan provisions
ROUTINE VISION BENEFITS Eye Exam (one eye exam per person every 12 months)
Covered at 100% of the allowed amount subject to the $10 physician copay.
Covered at 100% of the allowed amount subject to the $35 physician copay.
Lenses, Contact Lenses and Frames
Covered at 100% of the allowed amount up to a combined $200 maximum per person each calendar year.
PRESCRIPTION DRUG BENEFITS (Includes Mental Health and Substance Abuse)
Prepaid Drug Card Preferred Rx Products • Non-maintenance – up to 30 day
supply at retail • Blue Cross Maintenance Drug List –
up to a 60 day supply Diabetic Supplies (copays apply) • Diabetic supplies are covered only
through the Prescription Drug Card Program.
• Copays are combined for some
products if purchased on the same day.
Participating Pharmacy: Prescription drugs will be covered at 100% subject to the following copays: Generic Drugs: $5 copay per prescription Preferred Brand Name Drugs: $35 copay per prescription Other Brand Name Drugs: $75 copay per prescription • Insulin, insulin needles and syringes
purchased on the same day will require only one copay.
• Blood glucose strips and lancets purchased on the same day will require only one copay.
• Glucose monitors will always require a separate copay.
Non-Participating Pharmacy: There are no benefits available for prescription drugs purchased from a non-Participating Pharmacy.
Page 4
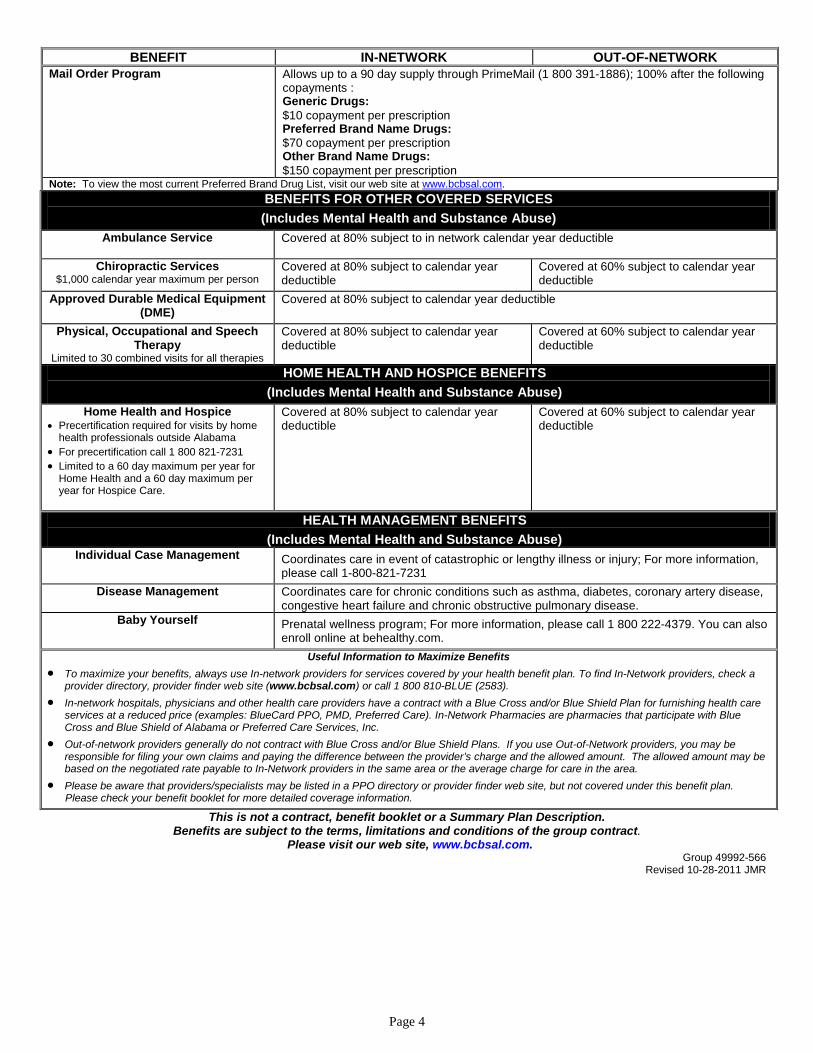
BENEFIT IN-NETWORK OUT-OF-NETWORK Mail Order Program Allows up to a 90 day supply through PrimeMail (1 800 391-1886); 100% after the following
copayments : Generic Drugs: $10 copayment per prescription Preferred Brand Name Drugs: $70 copayment per prescription Other Brand Name Drugs: $150 copayment per prescription
Note: To view the most current Preferred Brand Drug List, visit our web site at www.bcbsal.com. BENEFITS FOR OTHER COVERED SERVICES (Includes Mental Health and Substance Abuse)
Ambulance Service Covered at 80% subject to in network calendar year deductible
Chiropractic Services $1,000 calendar year maximum per person
Covered at 80% subject to calendar year deductible
Covered at 60% subject to calendar year deductible
Approved Durable Medical Equipment (DME)
Covered at 80% subject to calendar year deductible
Physical, Occupational and Speech Therapy
Limited to 30 combined visits for all therapies
Covered at 80% subject to calendar year deductible
Covered at 60% subject to calendar year deductible
HOME HEALTH AND HOSPICE BENEFITS (Includes Mental Health and Substance Abuse)
Home Health and Hospice • Precertification required for visits by home
health professionals outside Alabama • For precertification call 1 800 821-7231 • Limited to a 60 day maximum per year for
Home Health and a 60 day maximum per year for Hospice Care.
Covered at 80% subject to calendar year deductible
Covered at 60% subject to calendar year deductible
HEALTH MANAGEMENT BENEFITS (Includes Mental Health and Substance Abuse)
Individual Case Management
Coordinates care in event of catastrophic or lengthy illness or injury; For more information, please call 1-800-821-7231
Disease Management Coordinates care for chronic conditions such as asthma, diabetes, coronary artery disease, congestive heart failure and chronic obstructive pulmonary disease.
Baby Yourself
Prenatal wellness program; For more information, please call 1 800 222-4379. You can also enroll online at behealthy.com.
Useful Information to Maximize Benefits • To maximize your benefits, always use In-network providers for services covered by your health benefit plan. To find In-Network providers, check a
provider directory, provider finder web site (www.bcbsal.com) or call 1 800 810-BLUE (2583). • In-network hospitals, physicians and other health care providers have a contract with a Blue Cross and/or Blue Shield Plan for furnishing health care
services at a reduced price (examples: BlueCard PPO, PMD, Preferred Care). In-Network Pharmacies are pharmacies that participate with Blue Cross and Blue Shield of Alabama or Preferred Care Services, Inc.
• Out-of-network providers generally do not contract with Blue Cross and/or Blue Shield Plans. If you use Out-of-Network providers, you may be responsible for filing your own claims and paying the difference between the provider’s charge and the allowed amount. The allowed amount may be based on the negotiated rate payable to In-Network providers in the same area or the average charge for care in the area.
• Please be aware that providers/specialists may be listed in a PPO directory or provider finder web site, but not covered under this benefit plan. Please check your benefit booklet for more detailed coverage information.
This is not a contract, benefit booklet or a Summary Plan Description. Benefits are subject to the terms, limitations and conditions of the group contract.
Please visit our web site, www.bcbsal.com. Group 49992-566
Revised 10-28-2011 JMR