2009 hrg4 road shows finance & costing break out session reference costs 2008/09 payment by...
TRANSCRIPT

2009 HRG4 Road ShowsFinance & Costing Break Out SessionReference Costs 2008/09
Payment by Results – Operations
2007/08 Data
• THANKS!!
• Data collected from over 400 organisations
• Total quantum of approx £44bn
• Analysis and Data Quality
• Data published on DH website and Unify2 tool by end of March ’09 (Unify2 replaces DVD)

2008/09 Timescales• HRG4 Ref Costs Grouper out 13 Feb• Ref Cost Guidance / Costing Manual published early March
• Collection Timescales back to prior year timescales
• New structure to 2007-08 Timescales:– 3 week submission (Jun 8 – Jun 26)– 2 week analysis period (Jun 29 – Jul 10)– 4 week resubmission (Jul 13 – Aug 7)
• All designed around ensuring data quality (getting it right first time should always be the priority)

2008/09 Guidance • No fundamental change (currency / collection system)
• Refinement and Improvement– Further clarification – Changes to further align with PbR Tariff development
• Interventional Radiology – no longer unbundled
• Diagnostic Imaging – APC no longer unbundled
• Critical Care – Adult– Paediatrics / Neonatal
• Community– Consistency with community work (Development Sites)

2008/09 Collection System• As per 2007/08 – Unify2
• User Accounts – still active from 2007/08– SHA Leads first port of call for new accounts
• Concise / Updated Guidance (summary + detailed)
• Involving Software Suppliers in update – workbooks/validations
• We advise NHS users re-familiarise themselves with system in advance of collection
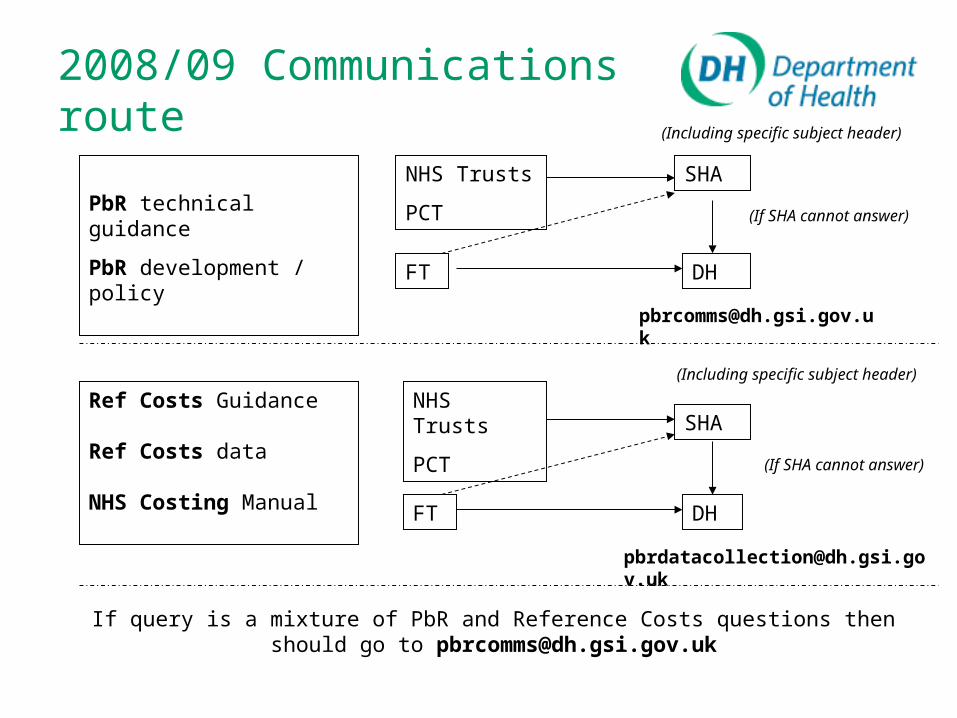
2008/09 Communications route
PbR technical guidance
PbR development / policy
Ref Costs Guidance
Ref Costs data
NHS Costing Manual
If query is a mixture of PbR and Reference Costs questions then should go to [email protected]
NHS Trusts
PCT
FT
SHA
DH
(Including specific subject header)
(If SHA cannot answer)
NHS Trusts
PCT
FT
SHA
DH
(If SHA cannot answer)
(Including specific subject header)

Key Messages• Timetable back in-line with previous years
– “Business as usual”
• No major change to collection requirements in 2008/09– No new currency– No new collection system (see below)
• Unify2 continues to be the collection tool
• Refinement and improvement of Guidance
A year of stability and driving up the data quality

For info – SHA Leads
Q30 North East [email protected]
Q31 North West [email protected]
Q32 Yorkshire & Humber [email protected]
Q33 East Midlands [email protected]
Q34 West Midlandshelen.o’[email protected]
Q35 East of England [email protected]
Q36 London [email protected]
Q37 South East Coast [email protected]
Q38 South Central [email protected]
Q39 South West [email protected]

HRG4 2008/09 Reference Costs Grouper
– HRG4 changes from 2007/08

HRG4 changes summary
•Design changes - Concepts
•Design changes - Tweaks
•Design changes - Logic
•Datasets and Software
•Key messages

Grouper design changes – Concepts
Removal of sub-chapter and HRGs• Known areas of difficulty
• Sub-chapter RB (Interventional Radiology) removed
Differential between shoulder and elbow surgery• Better split of anatomical sites
Creation of new sub-chapters• Traumatic or non traumatic HRGs?
• Sub-chapter HR (Orthopaedic Reconstructions) created

Grouper design changes – Tweaks
Creation of new HRGs:•New technology, greater granularity or specificity
•FZ42Z Wireless Capsule Endoscopy
Reallocate OPCS/ICD10 codes to HRGs:•Different resource usage identified
•Remap N390 (Urinary tract infection site not specified) from PA18 (Minor infections) to PA17 (Intermediate infections)
Label changes:•Amendments to description and purpose of a sub-chapter
•Sub-chapter SA - Haematological Procedures and Disorders
Grouper design changes – Logic
Age splits amended:• Orthopaedics (added to specific HRGs)• Obstetrics (between 16 and 40 / under 16 or over 40)
Length of Stay splits amended:• To group off diagnosis rather than “incidental” procedures
• Insertion of catheters, ECGs
Complications and Co-morbidities (CCs):• PA02 Epilepsy syndrome (added)• N390 Urinary tract infection added as a CC to Chapter M
(Gynaecology)
Datasets and Software
• Inclusion of Paediatric Critical Care and Neonatal Critical Care datasets
• Updated data quality report
• Multiple HRG4 Groupers can now be loaded onto the same PC. Currently, installation of a new HRG4 grouper removes any previous versions.
Key messages
• Understand the changes from previous years
• Double check that you are using the correct version of the Grouper
• Make use of the Casemix helpdesk!– [email protected]
Further information
• www.ic.nhs.uk/casemix/prepare– Introduction to HRG4– HRG4 Concepts– HRG Coding Validation– HRG4 Chapter Summaries, Definitions &
Comparative Analysis– HRG4 Code to Group [what goes where and
how]– Guide to Data Field validation– Top 10 Tips / FAQs

2009 HRG4 Road ShowsPLICS & Acute Health Clinical Costing Standards - Quality in Costing
Peter Donnelly, Suzanne Ibbotson Department of Health

PLICS & Costing Standards
Summary
• PLICS
• Acute Health Clinical Costing Standards
• Collection

PLICS
• What is PLICS?
Patient Level Information & Costing Systems– Records individual interactions and events which are
connected directly with a patient’s care from the time of admission until the time of discharge.
– Ascribes to the patient the direct and indirect cost of the resources used during those interactions
– The more detailed the record of what happens to the patient, the better the costing can be
PLICS - Benefits
• Better quality costing• Allows an organisation to understand their costs better –
highlighting inefficiencies and cost drivers• Improved transparency, time, costs etc• Improved costing of clinical activity allows meaningful
comparison and dialogue with clinicians, including care pathways and treatment of similar patients and links to quality
• Better quality data to inform tariff

Costing Standards Background
• Why have Standards?
• What are they ?
• Who developed them ?
• How to use?
• Quality
• Extension to other areas

Costing Standards - Why?
• Evolve : what was good enough yesterday will not be good enough tomorrow
• Economic downturn will put extra pressure on getting the tariff right and maximising efficiency.
• Need to maximise the benefit /cost equation of better data quality.

What are they?
• A set of guidelines for excellent practice
• Designed to improve costing of services within NHS
• Will provide a basis for benchmarking
• Will provide a platform for continuous development in line with international best practice
Development
• Starting point Australian Costing Standards, adapted and revised for England
• Drafting Committee:
- 12 practitioners from Acute hospitals
- 3 from DH
- 1 from Audit Commission
• Consultation with major stakeholders
How to use?
• Acute Clinical Costing Standards should be used by all PLICS users & those seeking to implement PLICS
• Provides consistent methodologies for allocating costs, and sets out best practice guidelines – shows real costs
• Still need NHS Costing Manual & Reference Cost Guidance for cost collection
• Standards seek to promote improved costing within NHS not directly to support cost collection
Quality
• Quality of data
- Need good quality information as well as cost data
• Concept
- Materiality of the amount allocated and how accurately the allocation is done
• Application
- MAQS score (self assessment)

Extension of Standards
• Mental Health: Out for Consultation
• Cystic Fibrosis: In Action, use by PbR Development Sites

Next Steps/Collection• Direction of travel towards PLICS & use of PLICS to help inform tariff –
focus on improving and proving quality first
• Review 2007/08 PLICS data from small sample of hospitals (drafting committee members)
• Review of Cost Collection commencing this year
– Reference Costs still mandatory for all NHS providers
• Approximately 60 organisations reported using PLICS for 2009/10 and having data available
• Additional 60 - 80 organisations planning on implementing PLICS during 2009/10

Feedback & Questions
PLICS @ dh.gsi.gov.uk
www.dh.gov.uk/pbr
(PLICS/Costing Standards)