1hypersensitivity08 by akram.ppt - mymensingh medical college file/hypersensitivity-1by...
TRANSCRIPT
Hypersensitivity
Prof. Md. Akram Hossain
1/1/20141Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Working Definition of Working Definition of Hypersensitivity
Adverse clinical reaction to the antigen or,“when the immune system does something“when the immune system does something
bad to the host, i.e. tissue damage”
1/1/20142Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Other definitions
� Classical definition� Inappropriate or excessive immune
response in pre-sensitized host leadingto tissue damage.
� But recent opinion-Hypersensitivity can also arise from direct
interaction of the inciting agent with elementsof the innate immune system withoutintervention by acquired responses. (Roitt2006 11th edition)1/1/20143
Prof. Muhammad Akram Hossain, Hypersensitivity-1

Historical background of hypersensitivity
� Charles Robert Richet & Paul Portier in 1902� Experiment
� Injected toxin to Dogs, when 2nd dose given after 1 week, instead of protection, dogs become ill (excessive salivation,defecation, difficulty respiration, (excessive salivation,defecation, difficulty respiration, death) within minutes.
� So they named this phenomenon as anaphylaxis, Greek ana- means away from, phylaxis means Protection
� This is first example that immune system can cause harm.
1/1/20144Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Charles Robert Richet(August 25, 1850 – December4, 1935) was a Frenchphysiologistphysiologist
Won Nobel Prize forPhysiology or Medicine in1913.
1/1/20145Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Classification
A. On the basis of onset of action
B. On the basis of mechanism of action B. On the basis of mechanism of action
C. Coomb’s and Gel classification
(Combined)
1/1/20146Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Classification..
1. Based on onset of action
Immediate hypersensitivities
Delayed hypersensitivities
2. Based on mechanism of actionAntibody mediated: Type I, II, III & VCell mediated: Type IV
1/1/20147Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Classification…
3. Coombs & Gel - - In the early 1970s, P.G.H. Gell and R.A.
Coombs proposed following method of classification
of hypersensitivity.
Type-1 or anaphylactic hypersensitivity
Type-II or cytotoxic hypersensitivity
Type-III or immune complex hypersensitivity
Type-IV or Delayed or Cell mediated hypersensitivity
Type-V or Stimulatory hypersensitivity (Later added)
1/1/20148Prof. Muhammad Akram Hossain,
Hypersensitivity-1
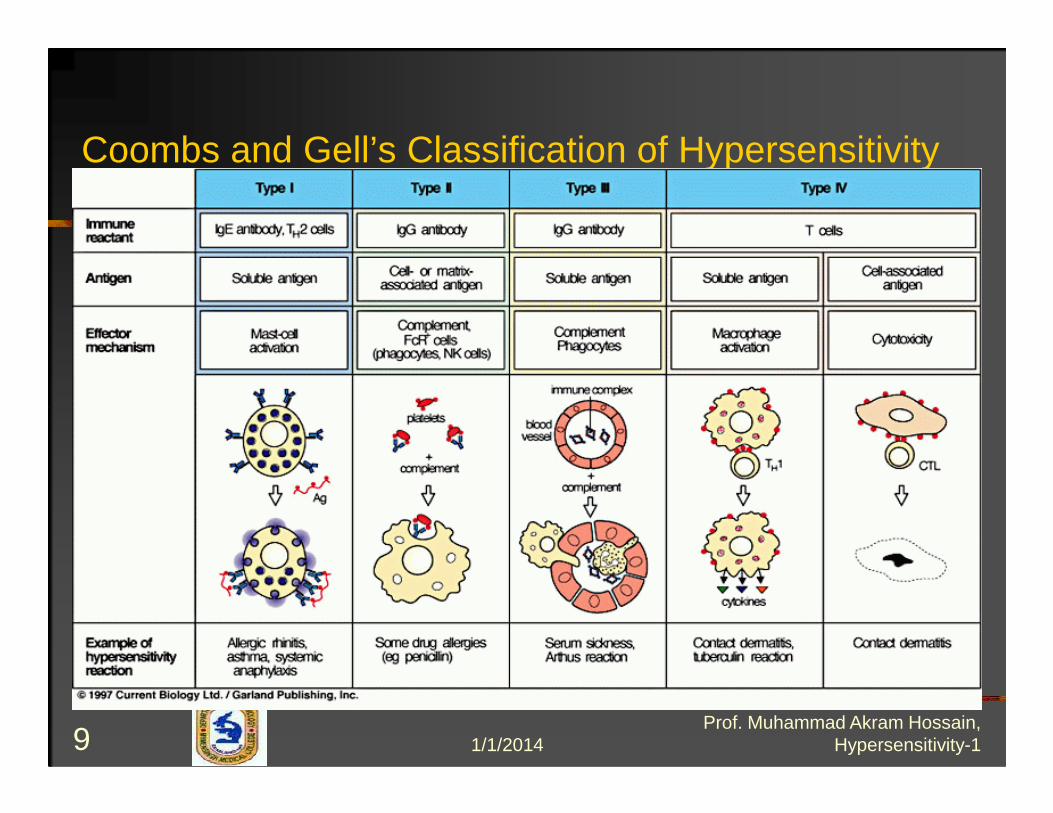
Coombs and Gell’s Classification of Hypersensitivity
1/1/20149Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Type I Hypersensitivity
� Also known as:� Immediate
hypersensitivityhypersensitivity� Allergy� Anaphylaxis� IgE-associated
immune responses
1/1/201410Prof. Muhammad Akram Hossain,
Hypersensitivity-1

What is an Allergy?
� Allergy: a biological hypersensitivity in certainindividuals to substances which, in similar amountsand circumstances, do not have an effect on others.
In other words, an allergy is an unusual or exaggeratedresponse to certain substances.
� Allergen: a substance capable of producing an allergicreaction. (can be anything!)
� “One person’s food in another person’s poison.”-- Hippocrates (460–377 BC)
1/1/201411Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Where does the term “allergy” come from?
� Term “allergy” was coined in 1906 byAustrian pediatrician Clements VonPirquet (1874-1929)
Clemens Peter Freiherr von Pirquet was an Austrian scientist In 1906 henoticed that patients who had previously received injections of horse serum orsmallpox vaccine had quicker, more severe reactions to a second injection. He,along with Bela Schick, coined the word allergy (from the Greek allos meaning"other" and ergon meaning "reaction") to describe this hypersensitivity reaction
1/1/201412Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Two Types of Allergies
ACTIVE Allergies…
Cause very visible, uncomfortable allergic reactions includinghives, rashes, swelling, wheezing, runny eyes, runny nose, etc.
HIDDEN Allergies…
Cause few visible allergic reactions.
Patients complain of poor function of body and/or mind including fatigue, anxiety, nose, etc. including fatigue, anxiety, mental fogginess, back pain, arthritis, malaise, etc. and don’t know the reason why.
FACT: Most allergy sufferers have both types.1/1/201413
Prof. Muhammad Akram Hossain, Hypersensitivity-1
Allergen
� Allergen: are antigens that induce production of specific IgE AB
� Examples- protein- polypeptide- polysaccharide- nucleic acid- low M.W chemicals
1/1/201414Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Charecteristic of Allergen
1. Low M.W : < 40 kD1. Low M.W : < 40 kD
2. Water soluble
3. Stability
1/1/201415Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Route of Allergen Entry
- Skin
- Respiratory tract
- GI tract
- Eye
1/1/201416Prof. Muhammad Akram Hossain,
Hypersensitivity-1

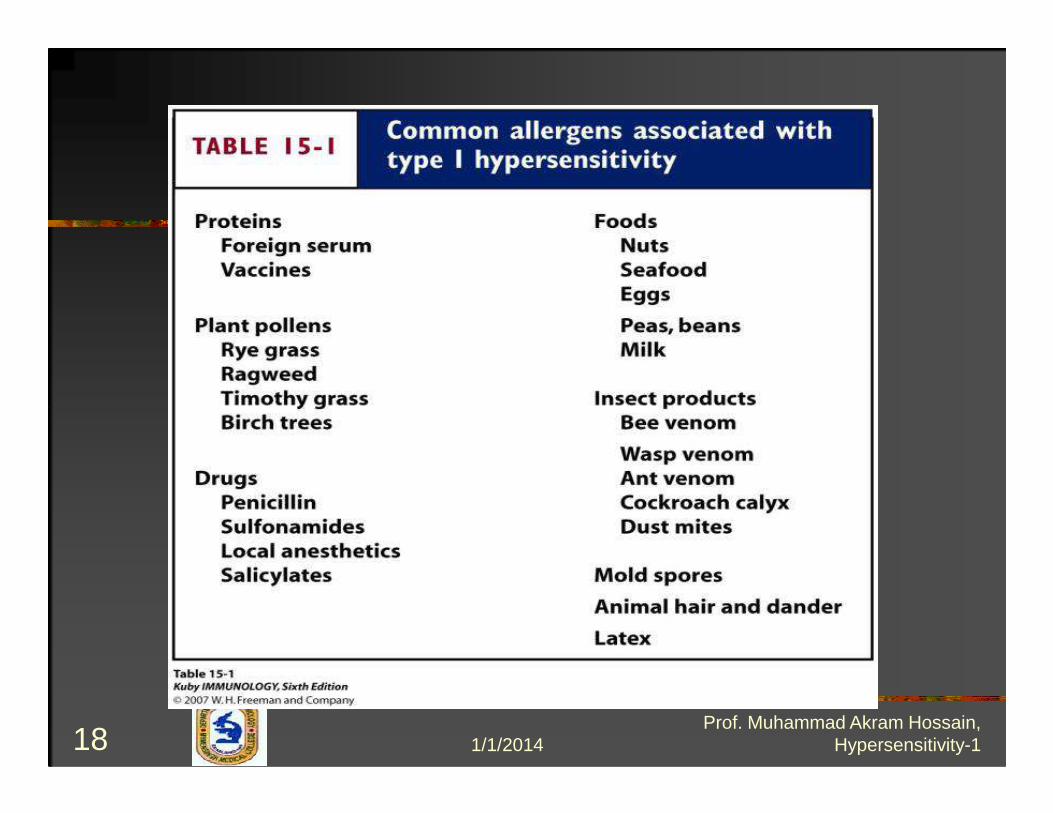
Common Allergens :- House dust : mite
- Pollen
- Animal dander
- Microorganisms
- Serum protein/Animal protein
- Antibiotic ( penicillin, streptomycin )
- Insect poison1/1/201417
Prof. Muhammad Akram Hossain, Hypersensitivity-1
1/1/201418Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Atopy
� Atopy: Describes individuals that produce IgEAb in response to various environmental Ag anddevelop immediate hypersensitivity (Type I)responses.(Asthma, eczema, hay fever, andresponses.(Asthma, eczema, hay fever, andurticaria)
� These individuals normally have a strong familyhistory (autosomal transmission of atopy)
1/1/201419Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Atopy
� HLA vs. Allergen Responsiveness-Some allergens response have a relationship to HLA-HLA-DR2 and HLA-A2: high responder to low dos of ragweed-HLA-B8: high responder to ragweed and also associated to other forms of hyperimmunity (autoimmunity)
1/1/201420Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Risk of Allergy
Parents – both = 50 %
one = 30 %
none = 15 % ( 30 % )
1/1/201421Prof. Muhammad Akram Hossain,
Hypersensitivity-1

IgE
� IgE blood concentrations are oftenincreased in allergic disease and aregrossly elevated in parasitic infectionsgrossly elevated in parasitic infections
� IL-4: promote B-cells to differentiate intoIgE-producing specific cells
1/1/201422Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Fig 15.10 Risk factors for allergy
1/1/201423Prof. Muhammad Akram Hossain,
Hypersensitivity-1

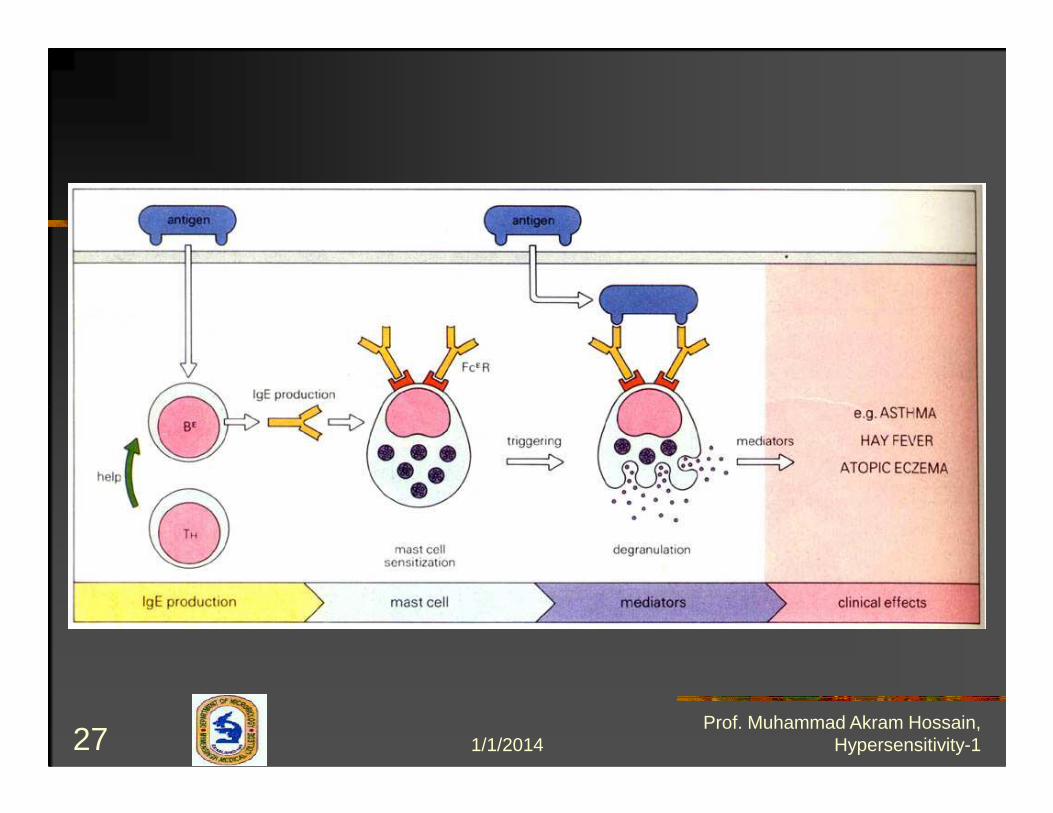
Phases of Type -1Hypersensitivity Phases of Type -1Hypersensitivity
1/1/201424Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Sensitization
1/1/201425Prof. Muhammad Akram Hossain,
Hypersensitivity-1
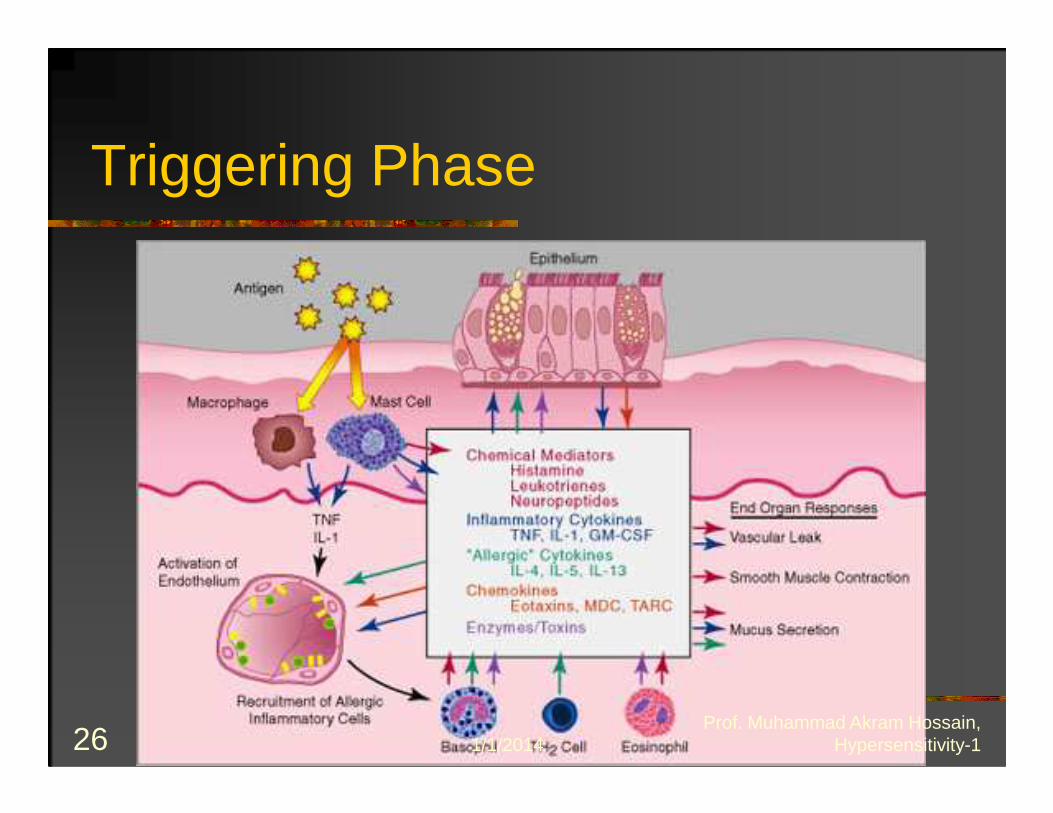
Triggering Phase
1/1/201426Prof. Muhammad Akram Hossain,
Hypersensitivity-1
1/1/201427Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Type-I Hypersensitivity: Animation IProduction of IgE in Response to an Allergen
1/1/201428Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Type-I Hypersensitivity: Animation II
Allergen Interaction with IgE on the Surface of Mast Cells triggers the Release of Inflammatory Mediators
1/1/201429Prof. Muhammad Akram Hossain,
Hypersensitivity-1
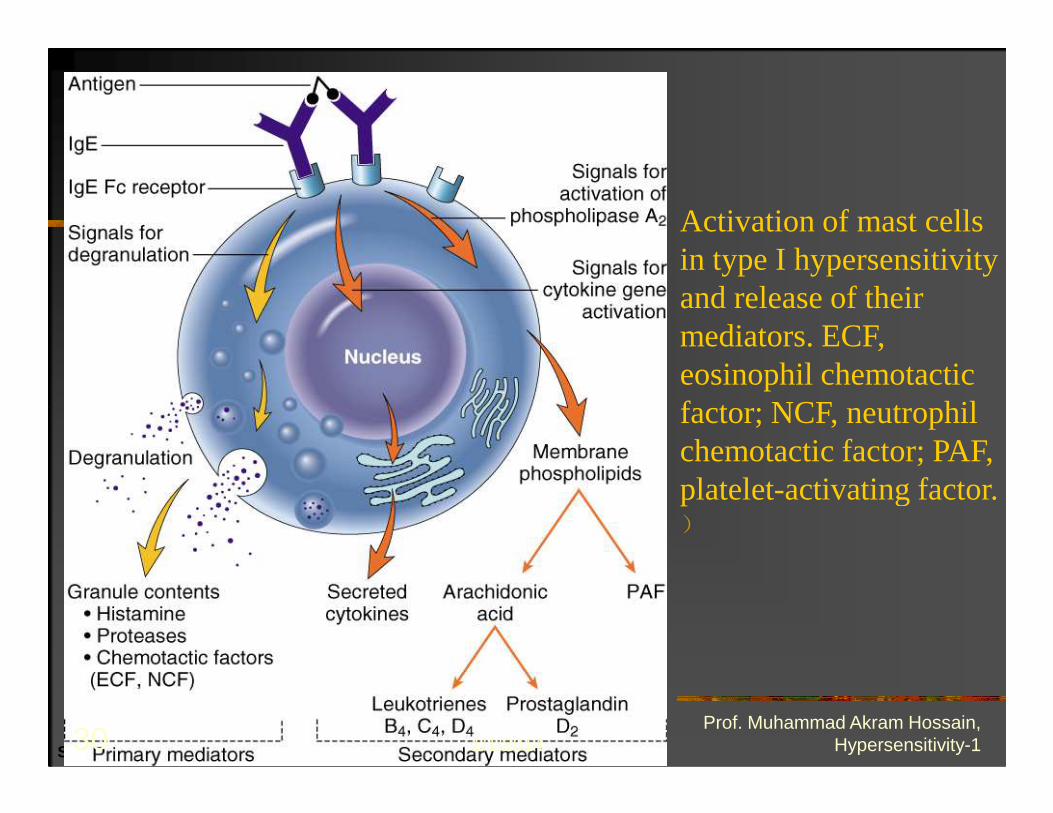
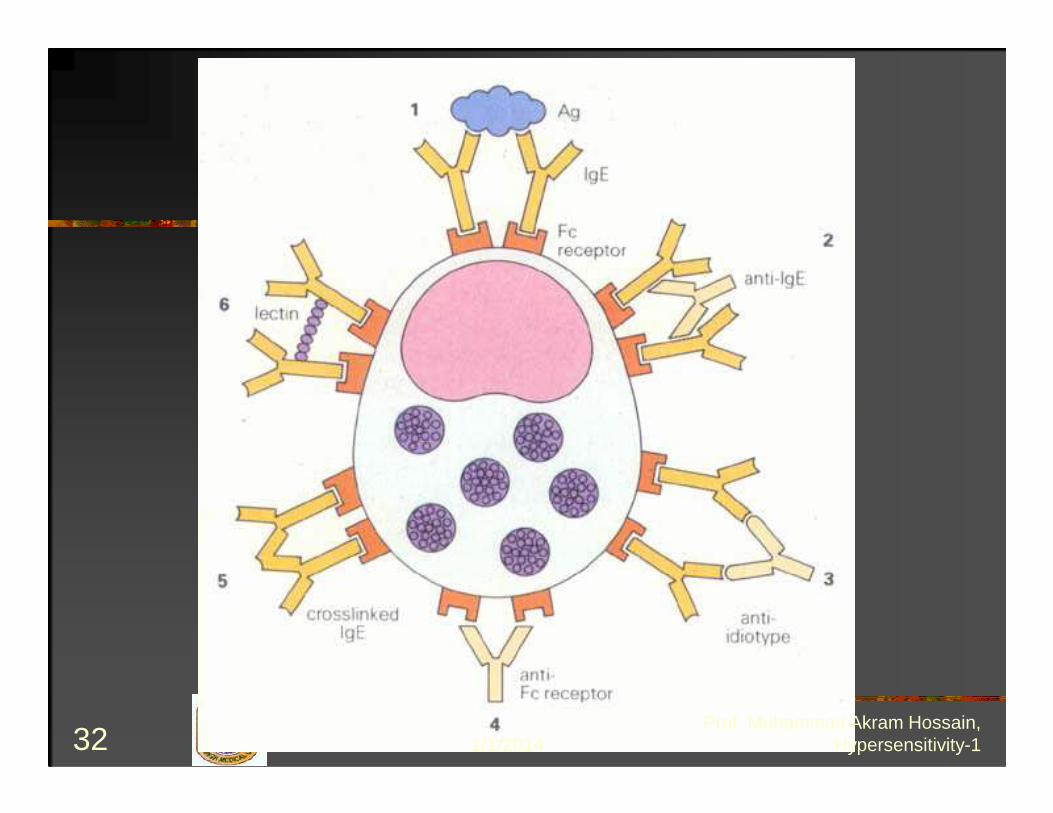
Activation of mast cells in type I hypersensitivity and release of their mediators. ECF, eosinophil chemotactic factor; NCF, neutrophil
Slide 7.9
factor; NCF, neutrophil chemotactic factor; PAF, platelet-activating factor. )
1/1/201430Prof. Muhammad Akram Hossain,
Hypersensitivity-1
1/1/201431Prof. Muhammad Akram Hossain,
Hypersensitivity-1
1/1/201432Prof. Muhammad Akram Hossain,
Hypersensitivity-1
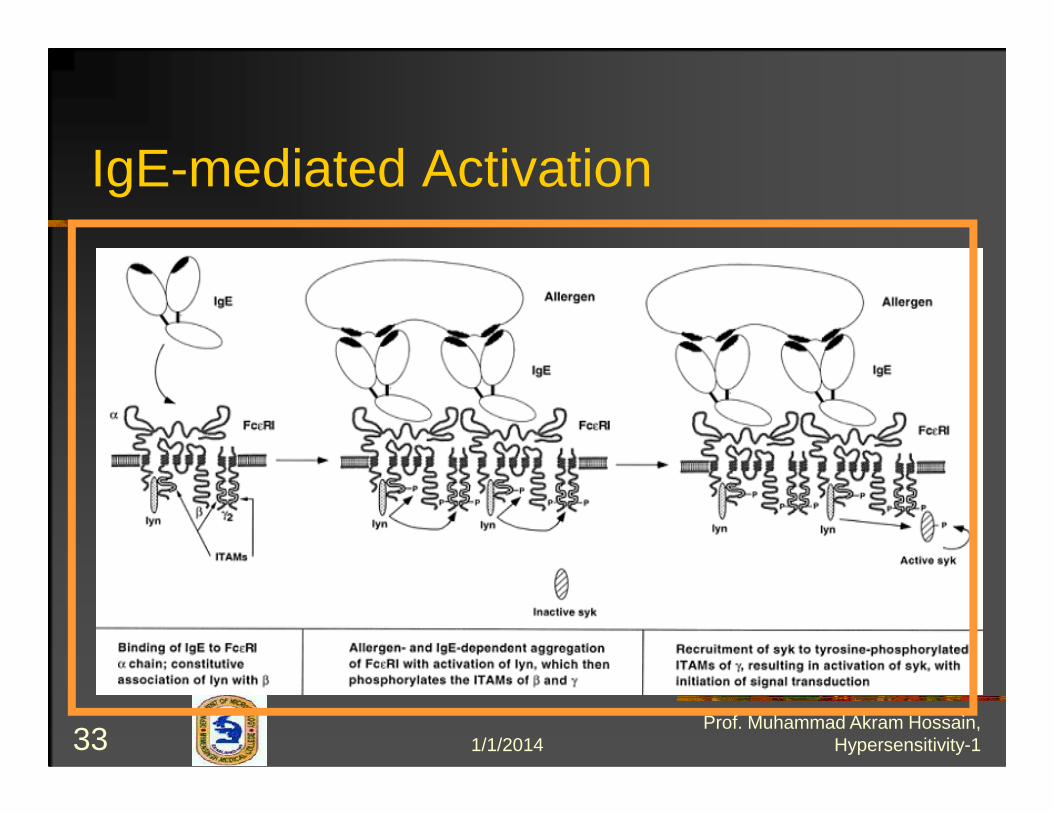
IgE-mediated Activation
1/1/201433Prof. Muhammad Akram Hossain,
Hypersensitivity-1
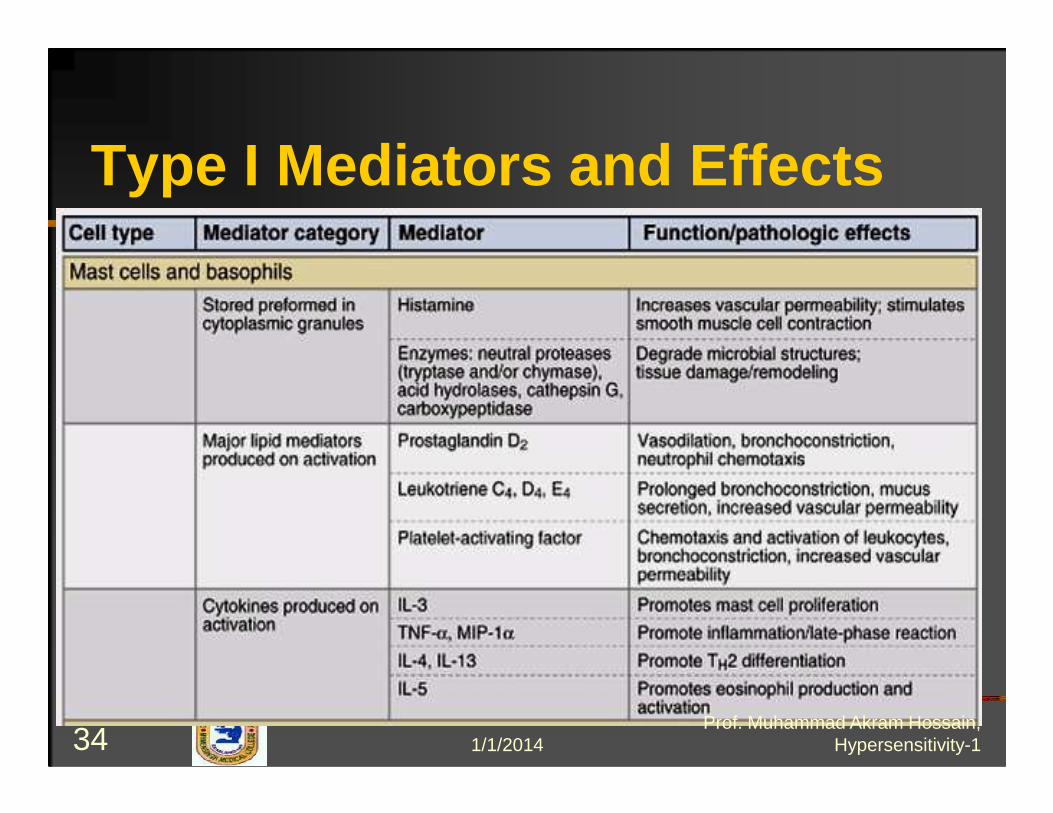
Type I Mediators and Effects
1/1/201434Prof. Muhammad Akram Hossain,
Hypersensitivity-1
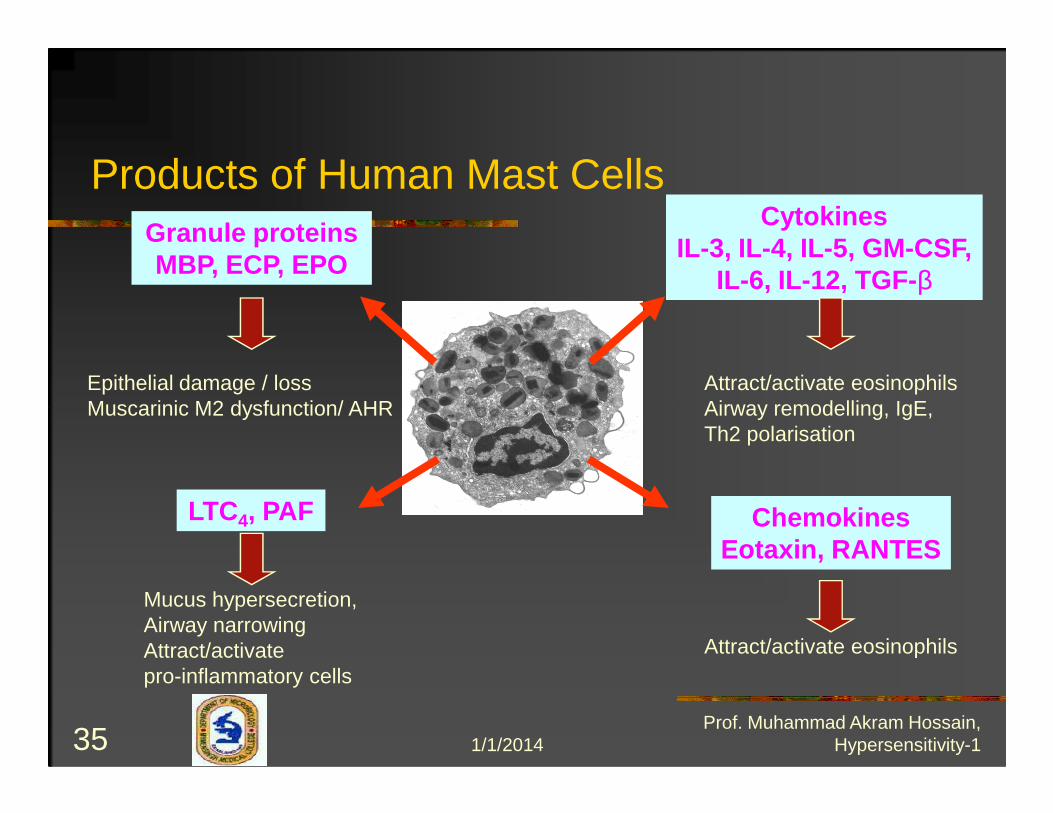
Granule proteinsMBP, ECP, EPO
CytokinesIL-3, IL-4, IL-5, GM -CSF,
IL-6, IL-12, TGF-β
Epithelial damage / loss Muscarinic M2 dysfunction/ AHR
Attract/activate eosinophilsAirway remodelling, IgE,
Products of Human Mast Cells
LTC4, PAF ChemokinesEotaxin, RANTES
Muscarinic M2 dysfunction/ AHR Airway remodelling, IgE, Th2 polarisation
Attract/activate eosinophils
Mucus hypersecretion,Airway narrowingAttract/activate pro-inflammatory cells
1/1/201435Prof. Muhammad Akram Hossain,
Hypersensitivity-1
1. Early phase: 2-3 min. to 6 hr.
- histamine
- eosinophil chemotactic facter ( ECF )
Time of Chemical Mediator Release
- neutrophil chemotactic factor ( NCF ) etc.
2. Late phase: > 6 hr. - 24 hr.
- SRS-A ( Leukotrienes )
- PAF ( platelet activating factor )
- vasoactive amine
1/1/201436Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Spasmogens:
- Histamine -Bronchial smooth
- Prostaglandin muscle contraction
- Leukotriene-C4 -Mucosal edema
- Leukotriene-D4 - Mucus secretion
1/1/201437Prof. Muhammad Akram Hossain,
Hypersensitivity-1

• Bronchial asthma
• Allergic rhinitis
Example of Type -1diseases
• Urticaria
• Anaphylactic shock
• Food allergy
• Eczema• Hay fever
1/1/201438Prof. Muhammad Akram Hossain,
Hypersensitivity-1

IgE-Mediated Allergic Reactions
1/1/201439Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Type I Mediators and Effects
1/1/201440Prof. Muhammad Akram Hossain,
Hypersensitivity-1

1/1/201441Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Vasculature
Skin
Upper respiratoryrespiratory
Lower respiratory
GI Tract
1/1/201442Prof. Muhammad Akram Hossain,
Hypersensitivity-1
1. Skin test ( Prick test )
2. Histamine determination
Laboratory Testing
3. IgElavel - RIA
4. Eosinophil count = 10-20 %
1/1/201443Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Skin Prick TestIn this test a small needle is used togently prick the skin through a dropof fluid containing a known allergen.It is usually done on the forearm,although with young children it maybe done on the back so they don'tbe done on the back so they don'thave to see what is happening.A negative reaction means that youdo not have an allergy to thatparticular allergen.
1/1/201444Prof. Muhammad Akram Hossain,
Hypersensitivity-1

1/1/201445Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Roles of Mast Cells
� Part of connective tissue (contains granules ofhistamine and heparin)
� Allergic diseases (asthma,eczema,itch)� Anaphylaxis (systemic shock to allergens such� Anaphylaxis (systemic shock to allergens such
as bee sting,nuts,drugs)� Autoimmune disorders/Acute or chronic
inflammation (MS, Rheumatoid arthritis)� Wound healing� Innate response for clearing bacteria and
viruses
1/1/201446Prof. Muhammad Akram Hossain,
Hypersensitivity-1

BasophilMast Cell
1/1/201447Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Mediator Release from Mast Cells1/1/201448
Prof. Muhammad Akram Hossain, Hypersensitivity-1
Two Types of Mast Cells
1) Connective tissue mast cells (CTMCs)2) Mucosal mast cells (MMC)2) Mucosal mast cells (MMC)
1/1/201449Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Type I: Mast Cells� Type I reaction is dependent upon the specific
triggering of IgE-sensitized mast-cells byallergen (Ag)
� Ag enter via mucosal surfaces and are taken upby APCby APC
� Th2 cells release IL-4 to facilitate the B-cellproliferation and differentiation, producing IgEspecific for the allergen
� REMEMBER: THIS IS A TH2 RESPONSE!
1/1/201450Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Connective Tissue Mass Cells
� CTMCs are found most in blood vesselsbut vary in size and number of granules atdifferent regions of the bodydifferent regions of the body
� Diseases such as Crohn’s disease,ulcerative colitis, and RA all present withincrease in CTMCs
1/1/201451Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Mast-Cells: Cytokines
� IL-3: Promote mast cell proliferation� IL-4, IL-5: Promote Th2 differentiation and
IgE AB productionIgE AB production� TNF-α, MIP-1α : Enhance inflammatory
reaction
1/1/201452Prof. Muhammad Akram Hossain,
Hypersensitivity-1

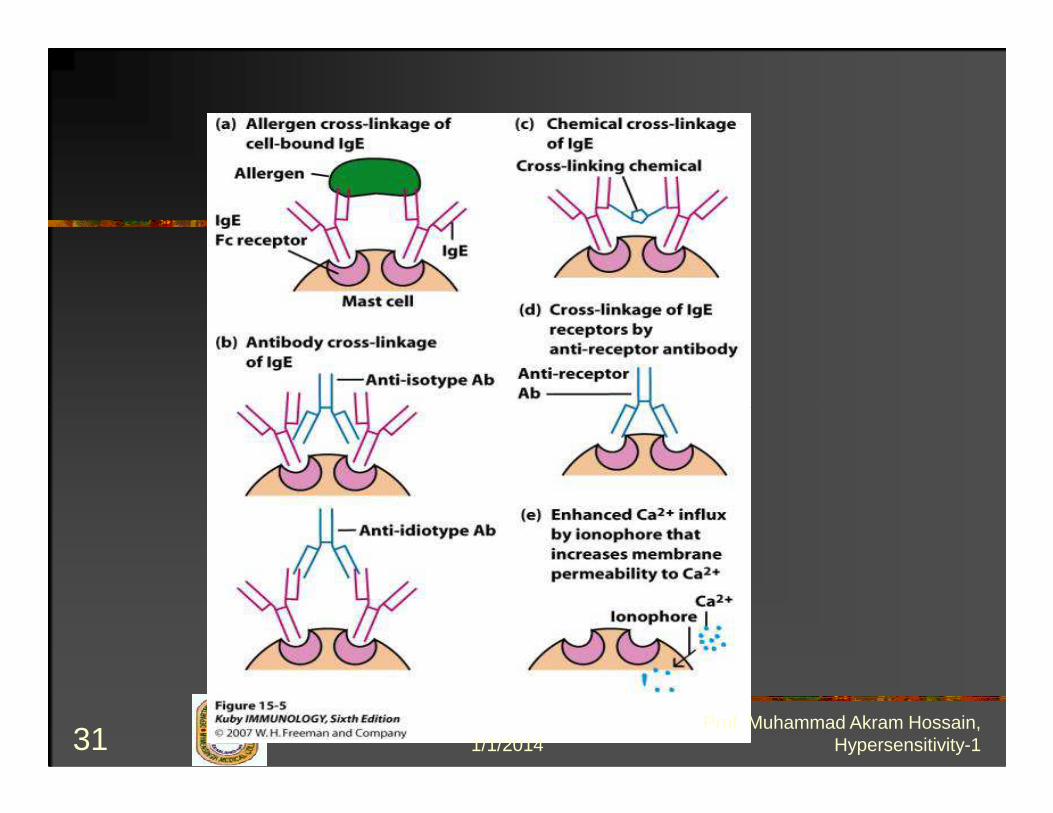
Activation of Mast Cells
� IgE from B-cells binds to FcεRI on mast-cells-ε is the heavy chain responsible for IgE -ε is the heavy chain responsible for IgE isotype switching
� FcεRI on mast-cells cross-links with Ag-bounded IgE and induces degranulation of mediators
1/1/201453Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Mast Cells Activation
� Cross-linking can be artificially inducedwith lectins such as PHA(Polyhydroxyaldehyde) and ConAThese carbohydrates cross-link with IgE� These carbohydrates cross-link with IgEand cause degranulation
� This explains urticaria in individualsallergic to fruits (ie strawberries-containlarge amt of lectin
1/1/201454Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Degranulation
� C’ products of C3a and C5a are veryactive in degranulating mast cells
� Compounds that affect Ca+2 influx into� Compounds that affect Ca influx intomast cells can induce degranulation
� Drugs such as morphine, codeine,synthetic ACTH can create clinicalmanifestations related to mast cells
1/1/201455Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Eosinophil
� Th2 produce IL-5: Promotes the synthesisand secretion of IgA from B-cells and alsoimportant in stimulating eosinophilimportant in stimulating eosinophildevelopment and activation
� IL-4 and IL-5 production by Th2 cells mayaccount for the eosinophilia seen in type Ihypersensitivity and parasitemia
1/1/201456Prof. Muhammad Akram Hossain,
Hypersensitivity-1
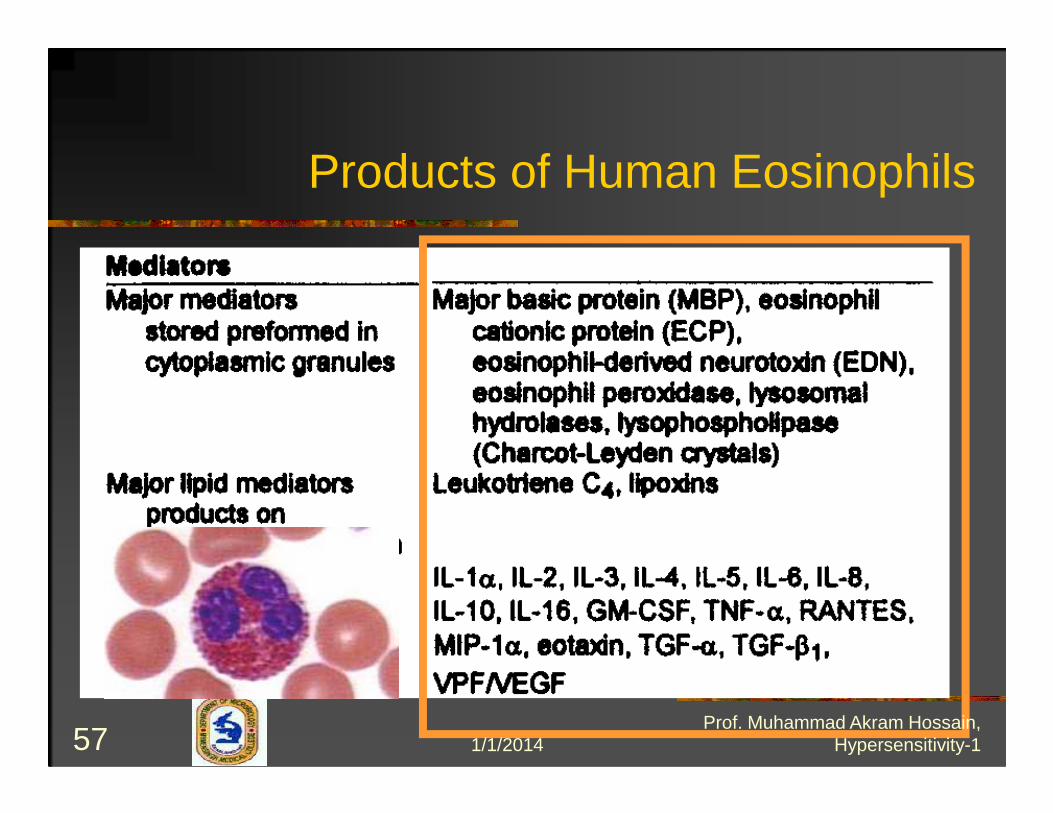
Products of Human Eosinophils
1/1/201457Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Types of Fc Receptors for IgE
� There are two types of receptors for IgE1) FcεRI (high affinity): Expressed on mastcells and basophilscells and basophils2) FcεRII (low affinity): Expressed bylymphocytes
1/1/201458Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Anaphylactic-type Degranulation of a Mast Cell
1/1/201459Prof. Muhammad Akram Hossain,
Hypersensitivity-1
vity Reaction
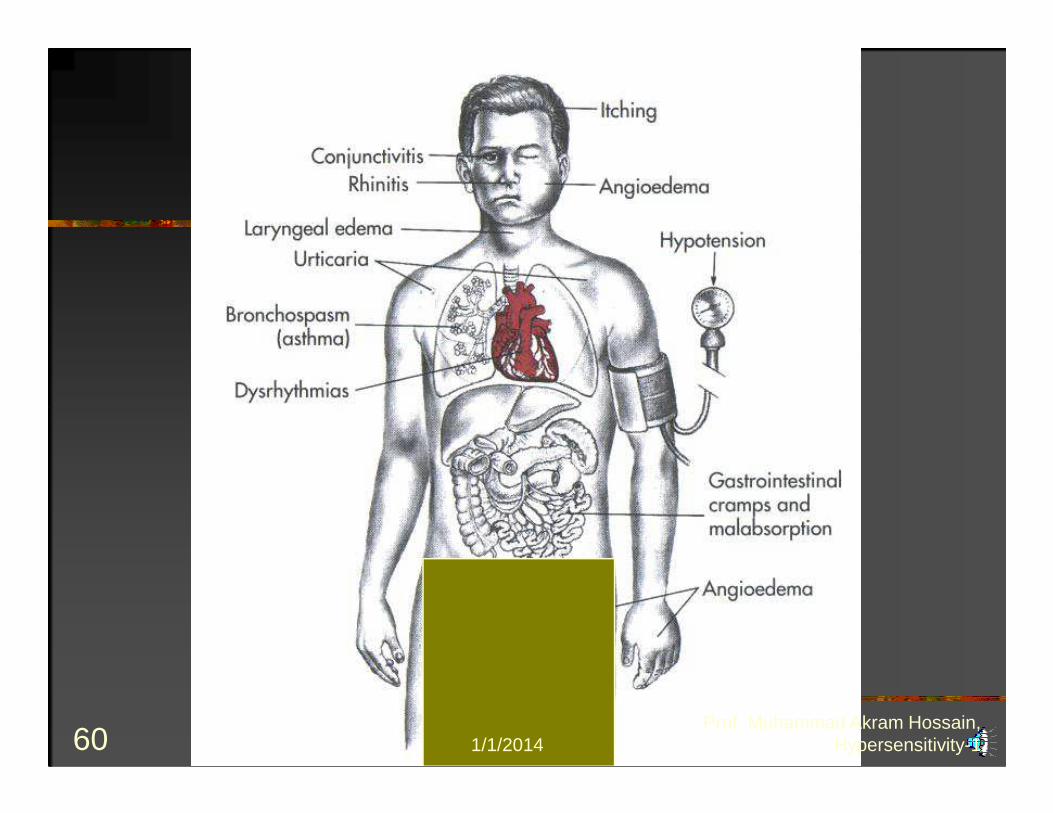
Type I Hypersensitivity
1/1/201460Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Treatment & Prevention
1/1/201461Prof. Muhammad Akram Hossain,
Hypersensitivity-1
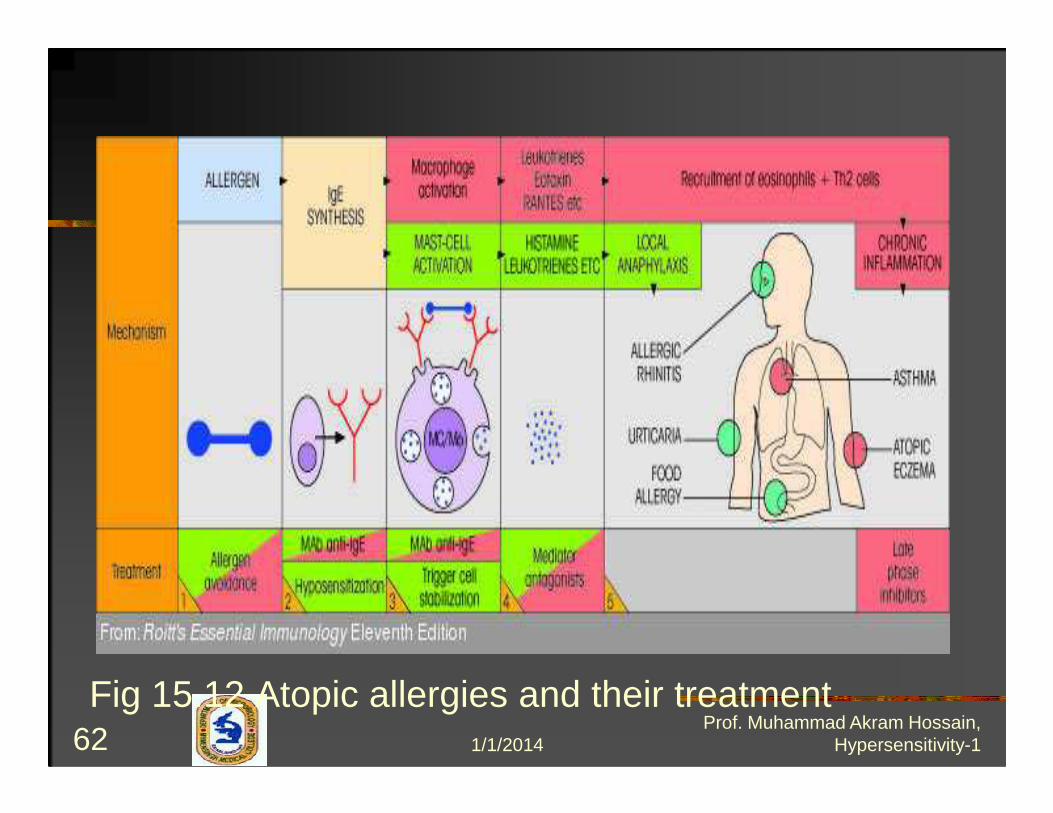
Fig 15.12 Atopic allergies and their treatment1/1/201462
Prof. Muhammad Akram Hossain, Hypersensitivity-1

Treatment & Prevention…1.Allergen avoidance
- Environmental control
2. IgE removement2. IgE removement
2.1 Hyposensitization ( Desensitization )
Allergen i.d Blocking IgG
1/1/201463Prof. Muhammad Akram Hossain,
Hypersensitivity-1
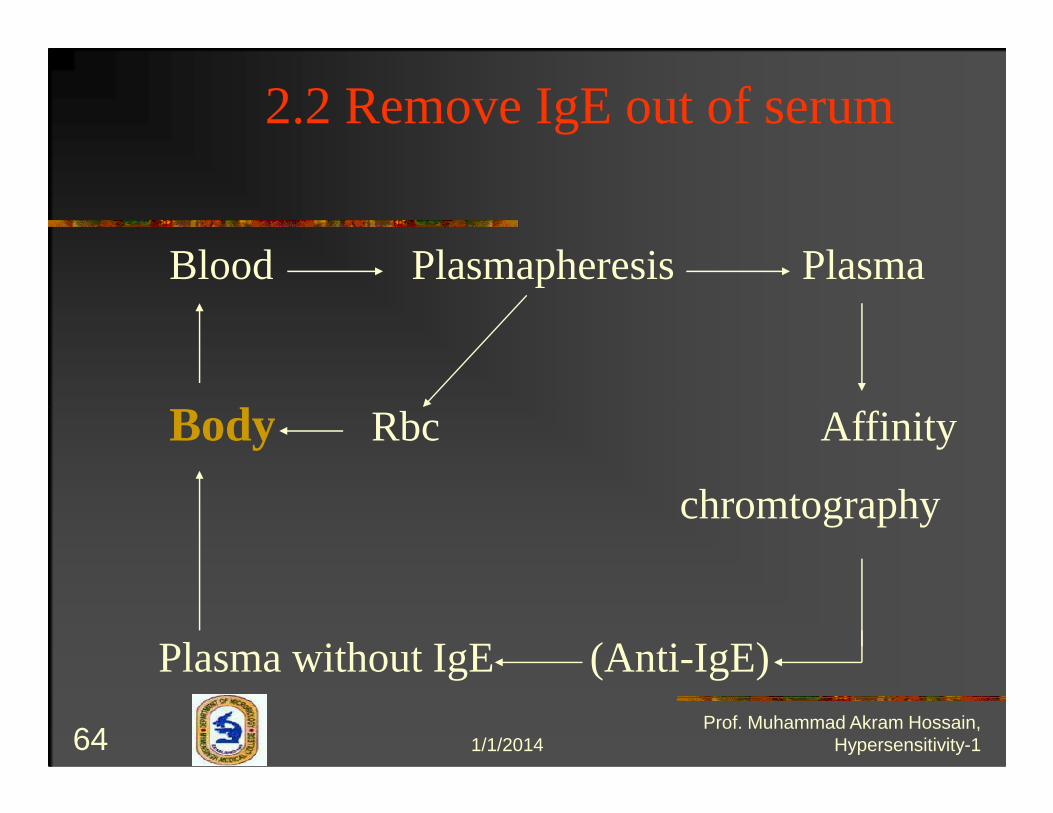
2.2 Remove IgE out of serum
Blood Plasmapheresis Plasma
Body Rbc AffinityBody Rbc Affinity
chromtography
Plasma without IgE (Anti-IgE)
1/1/201464Prof. Muhammad Akram Hossain,
Hypersensitivity-1
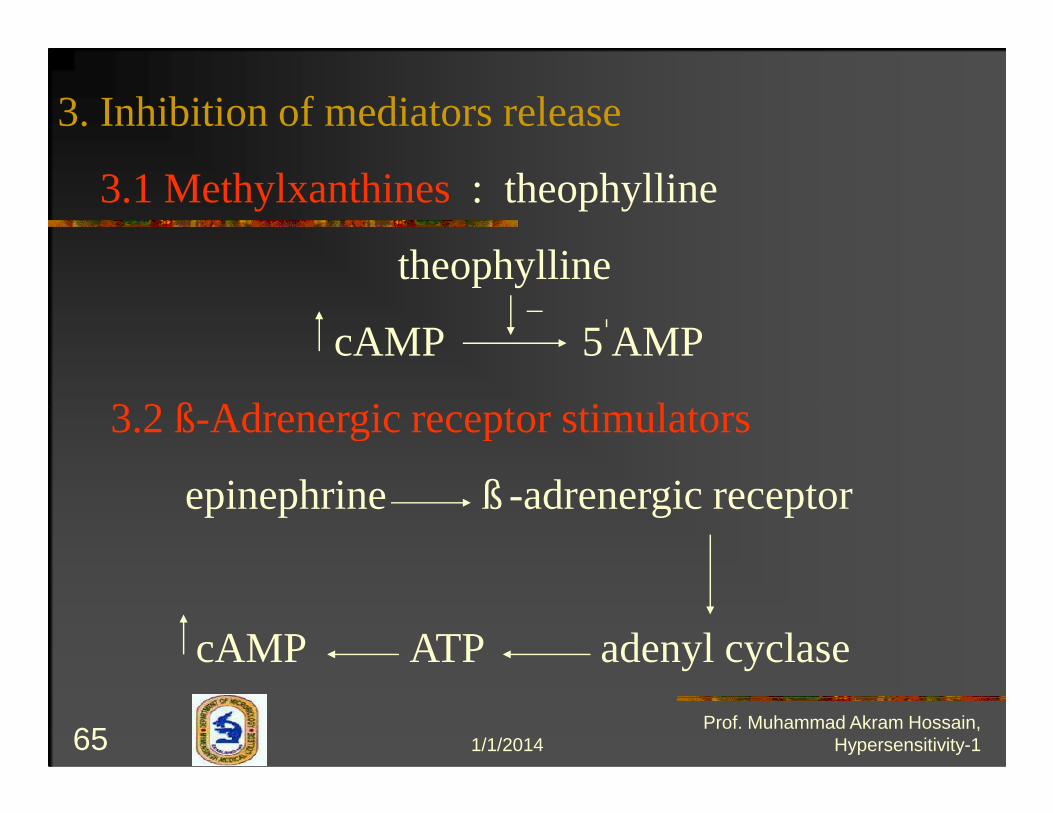
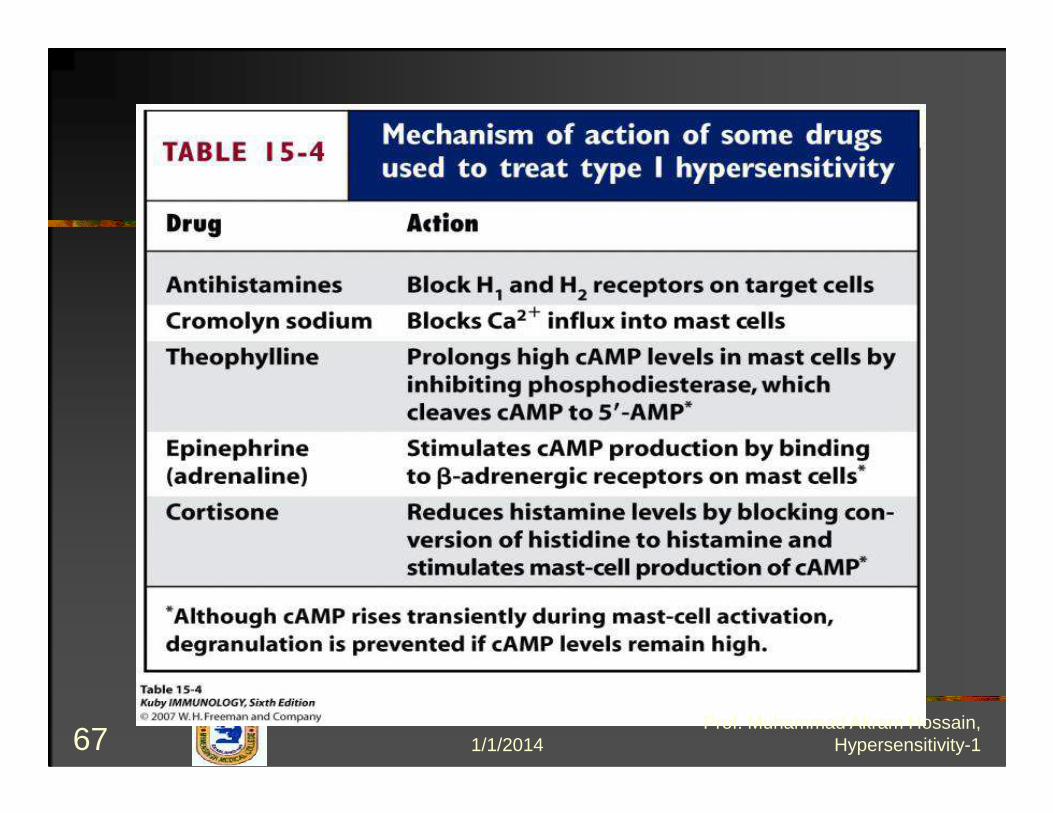
3. Inhibition of mediators release
3.1 Methylxanthines: theophylline
theophylline
cAMP 5 AMP
3.2 ß-Adrenergic receptor stimulators3.2 ß-Adrenergic receptor stimulators
epinephrine ß -adrenergic receptor
cAMP ATP adenyl cyclase
1/1/201465Prof. Muhammad Akram Hossain,
Hypersensitivity-1
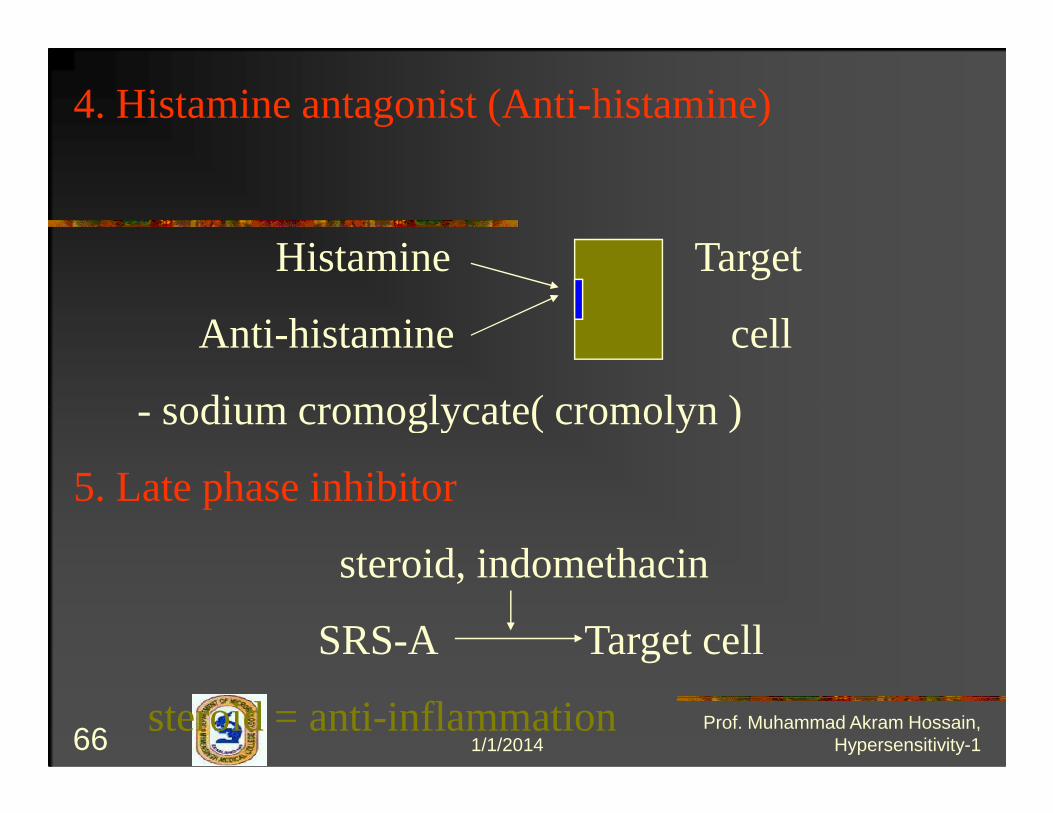
4. Histamine antagonist (Anti-histamine)
Histamine Target
Anti-histamine cell
- sodium cromoglycate( cromolyn )- sodium cromoglycate( cromolyn )
5. Late phase inhibitor
steroid, indomethacin
SRS-A Target cell
steroid = anti-inflammation1/1/201466
Prof. Muhammad Akram Hossain, Hypersensitivity-1
1/1/201467Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Immunological interventions
Desensitisation
� Acute desensitisation –
� Very small amounts of Ag at 15 min intervals to formAg-IgE complex on small scale which will notdegranulate mast cell.degranulate mast cell.
� Chronic desensitisation -
� Small doses of allergens are injected at weeklyintervals where IgG antibody is produced whichblocks the Ag by binding with it and does not allowthe Ag to reach the mast cell bound IgE .
1/1/201468Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Desensitization..Severity may be reduced by desensitization shots (allergy
shots). It is thought that when very dilute allergen is given
by injection, it stimulates the production of IgG and IgA. IgG
and IgA then act as blocking antibodies to bind and
neutralize much of the allergen in secretions before it canneutralize much of the allergen in secretions before it can
bind to the deeper cell-bound IgE on the mast cells in the
connective tissue. The shots also appear to suppress
production of IgE by inducing tolerance and/or by activating
T8-suppressor cells.
1/1/201469Prof. Muhammad Akram Hossain,
Hypersensitivity-1
Desensitization…A new experimental approach to treating and preventing Type-I
hypersensitivity involves giving the person with allergies
injections of monoclonal antibodies that have been made
against the Fc portion of human IgE .
This, in turn, blocks the attachment of the IgE to the FcThis, in turn, blocks the attachment of the IgE to the Fc
receptors on mast cells and basophils and the subsequent
release of histamine by those cells upon exposure to
allergen.
In addition, the anti-IgE binds to IgE-producing B-lymphocytes
causing apoptosis .
1/1/201470Prof. Muhammad Akram Hossain,
Hypersensitivity-1
The monoclonal antibody is a humanizedhybrid molecule consisting of a mousebinding (Fab) portion attached to a humanbinding (Fab) portion attached to a humanconstant (Fc) portion and is known asrhuMab (recombinant human monoclonalantibody).
1/1/201471Prof. Muhammad Akram Hossain,
Hypersensitivity-1

Intervention for Type I Hypersensitivity
Animation: Treatment with monoclonal anti-IgE antibody1/1/201472
Prof. Muhammad Akram Hossain, Hypersensitivity-1