14 pregnancy in women on haemodialysis and peritoneal dialysis
TRANSCRIPT

14
Pregnancy in women on haemodialysis and peritoneal dialysis
SUSAN H. HOU
Pregnancy is unusual in women with moderate renal insufficiency and very rare in women with end-stage renal disease (ESRD) treated with peritoneal dialysis or haemodialysis. However, as the length of survival on dialysis increases and the quality of life for women with chronic renal failure improves, decreased fertility and fetal loss continue to bar women with renal failure from child bearing and parenthood at a time when adoption by a woman with a serious medical illness is all but impossible. The first three sections of this chapter will review the literature describing the experience with pregnancy in dialysis patients. The fourth will address specific manage- ment issues.
FREQUENCY AND OUTCOME OF PREGNANCY IN DIALYSIS PATIENTS
As of the summer of 1993, there are at least 68 case reports of women dialysed for renal failure during pregnancy (Herwig et al, 1965; Orme et al, 1968; Mitra et al, 1970; Confortini et al, 1971; Unzelman et al, 1973; Ackrill et al, 1975; Marwood et al, 1977; Nemoto et al, 1977; Leader et al, 1978; Lindley et al, 1978; Ringenbach et al, 1978; Sanchez-Casajus et al, 1978; Sheriff et al, 1978; Thompson et al, 1978; Johnson et al, 1979; Naik et al, 1979; Kobayashi et al, 1981; Lee et al, 1981; Savdie et al, 1982; Cattran and Benzie, 1983; David et al, 1983; Kioko et al, 1983; Rotellar, 1983; Harum et al, 1987; Redrow et al, 1988; Brem et al, 1988; Nageotte and Grundy, 1988; Cohen et al, 1988; Yasin and Beydoun, 1988; Fujimi et al, 1990; Amoah and Arab, 1991; Barri et al, 1991; McGregor et al, 1991; Alcalay et al, 1992; Dolkart et al, 1992; Gadallah et al, 1992; Jakobi et al, 1992; Lew and Watson, 1992; Wadhwa et al, 1992; Yousri et al, 1992; Hou et al, 1993; D. Latos, personal communication).
Case reports are skewed toward reporting successful outcomes and only a handful describe unsuccessful outcomes. Estimates of the likelihood of successful pregnancy are based on four surveys (Registration Committee of the European Dialysis and Transplant Association, 1980; Roxe and Parker 1985; Souqiyyeh et al, 1992; Hou, 1993).
Baillibre' s Clinical Obstetrics and Gynaecology-- 481 Vol. 8, No. 2, June 1994 Copyright © 1994, by Bailli~re Tindall ISBN 0-7020-1861-9 All rights of reproduction in any form reserved

482 s .H. HOU
In 1980, 115 pregnancies were reported in the 13000 women of child- bearing age followed by the European Dialysis and Transplant Association. Forty-five women had therapeutic abortions, and of the remaining 70 women, 16 carried their pregnancies to viability (23%). Roxe and Parker reported 43 pregnancies in 35 women who became pregnant after starting dialysis. These pregnancies led to six live births (19%) (one set of twins). Souqiyyeh and colleagues report a 30% incidence of live births in women who became pregnant on dialysis in Saudia Arabia. In 1994, Hou reported the frequency and outcome of pregnancy in 10% of the dialysis units in the USA. These units reported 60 pregnancies, 20 during the survey period, 1990-1991. These 20 pregnancies occurred in 1281 women between the ages of 18 and 44 years dialysed in these units during the survey period (1.5%). The frequency of conception was approximately one-eigth the general United States population. The overall success rate in these 60 pregnancies was 37% but in pregnancies occurring during and after 1990, 52% of the infants survived. In Hou's Survey, pregnancy was most common in women who started dialysis after conception or who had been on dialysis 1 year or less. However, 21% of pregnancies occurred in women who had been on dialysis more than 10 years. While fertility is decreased in dialysis patients, it is common enough that contraceptive counselling should be provided to women of childbearing age with ESRD.
The diagnosis of pregnancy in dialysis patients can be difficult and, as a result, pregnancy is usually diagnosed at a late stage. Often the symptom leading to diagnosis is increase in abdominal girth or abdominal pain. The more common symptoms of pregnancy, nausea and amenorrhoea, are commonly attributed to other conditions. A high index of suspicion is necessary to exclude pregnancy before embarking on extensive radiographic examinations to evaluate gastrointestinal symptoms.
Urine pregnancy tests are not helpful in making the diagnosis even when residual urine output is present and measurements of serum levels of the [3 subunit of human chorionic gonadotropin (hCG) can be deceptive. Small amounts of hCG are produced by all cells, and because hCG is excreted by the kidney, its level can be borderline high in dialysis patients even when they are not pregnant (Schwartz et al, 1985). During pregnancy, hCG levels may be higher than expected for the stage of gestation. Serial hCG measure- ments which show a rising trend indicate pregnancy. Once the diagnosis of pregnancy is made, ultrasonography is necessary to assess gestational age.
MATERNAL RISKS
There have been no maternal deaths reported in women who were dialysed during pregnancy; however, bleeding and hypertension, which are common complications of pregnancy in dialysis patients, constitute a risk which could result in maternal death if extreme vigilance is not employed. Malignant hypertension with seizures and coma, respiratory failure, disseminated intravascular coagulation, pulmonary oedema and diabetic ketoacidosis are among the life-threatening complications which have been reported.

HAEMODIALYSIS AND PERITONEAL DIALYSIS 483
Decline in renal function
Many of the women who were dialysed during pregnancy started dialysis during pregnancy conceived prior to the initiation of dialysis. In this group, worsening renal function may have resulted from pregnancy. In 1985, we reported on a group of 23 women with moderate renal insufficiency (serum creatinine > 1.4 mg d1-1) who became pregnant (Hou et al, 1985). A third of these women experienced a decline in renal function that was faster than would have been expected from the natural history of the renal disease. These deteriorations in renal function did not reverse and generally pro- gressed after delivery. Surian et al (1984), using the reciprocal of the slope of the serum creatinine to define more precisely the natural history of the disease, confirmed our findings. Becker et al (1986) reported a rapid deterioration in renal function in six women with reflux nephropathy and moderate renal insufficiency who became pregnant. They were compared to ten control women who had reflux nephropathy but did not become preg- nant. Decline in renal function was significantly slower in the control group. More recently, Purdy et al (1993) demonstrated an acceleration in the decline in renal function during nine of 14 pregnancies in 11 women with type I diabetes with serum creatinine > 1.4 mg d1-1.
Hypertension
Of the 68 pregnant dialysis patients described in the literature, 40 were noted to be hypertensive, as defined by a diastolic blood pressure of 90 mmHg or greater, or by the use of antihypertensive medications. In 14 of these women, diastolic blood pressure rose to 110 mmHg or greater. In four, it was greater than 130 mmHg. Blood pressure was noted to be normal in 17 women and no mention was made of blood pressure in 11 cases (Table 1). A wide range of medication was used to control blood pressure, including methyldopa, hydralazine, clonidine, propranotol, metoprolol, reserpine, prazosin, labetalol and nifedipine.
Anaemia and bleeding
Haemorrhage and abruptio placentae appear to be more common in dialysis patients than in the general population. The anaemia associated with renal
Table 1. Highest blood pressure measurements in 68 preg- nant dialysis patients.
Highest blood pressure (mm/Hg) No. %
_< 140/90 17 25 > 140/90 but < 170/110 21 31 -> 170/110 but < 1701130 10 15 > 170/130 4 6 Taking antihypertensive medication,
blood pressure not mentioned 5 7 Blood pressure not mentioned 11 16
484 s.H. HOU
failure increases the danger associated with bleeding from obstetric prob- lems. In women with renal failure, the haematocrit drops during pregnancy, even without evident blood loss, as it appears that plasma volume increases while red cell mass does not. The drop in haematocrit has been observed even in women treated with human recombinant erythropoietin (EPO) (Hou et al, 1994). Twenty-three case reports mention that transfusion was required either for progressive anaemia or for bleeding episodes. It was initially hoped that continuous ambulatory peritoneal dialysis (CAPD), which is performed without the use of heparin, would decrease such prob- lems as bleeding and abruptio placentae but two severe bleeding episodes have been noted in reports of women treated exclusively with CAPD.
Other maternal problems
Problems with clotting of vascular access have been noted in a number of pregnancies (Redrow et al, 1988). In some, it is possible that the hyper- coagulable state that accompanies gestation may have played a role. Since dialysis is frequently begun earlier in the course of renal disease than it would be were the patient not pregnant, and the frequency of dialysis is often increased in women already treated with dialysis, the effect of uraemia on platelet function is minimal in these women. In essence, normalization of the bleeding time may actually make access thrombosis more likely.
The effect of pregnancy and fetal calcium requirements on maternal osteodystrophy has not been systematically studied. In one case report, maternal bone disease worsened during pregnancy and fetal skeletal calci- fication was less complete than expected for gestational age (Pepperell et al, 1970). In another, note is made of congenital rickets in the infant (Savdie et al, 1982).
Pregnancy is a recognized cause of sensitization to transplant antigens and may make it more difficult to find a donor kidney with a negative crossmatch (Sanfilippo et al, 1982). Once pregnancy occurs, it is not clear whether termination of the pregnancy will prevent sensitization.
Pregnancy" in a dialysis patient carries the risk of severe emotional stress. Often the pregnancy occurs after years of infertility and the patient is asked to undertake a time-consuming regimen of increased dialysis and blood pressure monitoring with but a small chance of success. More than half of fetal losses are accounted for by second trimester spontaneous abortion, stillbirth and neonatal death, which are all more difficult to accept than early losses.
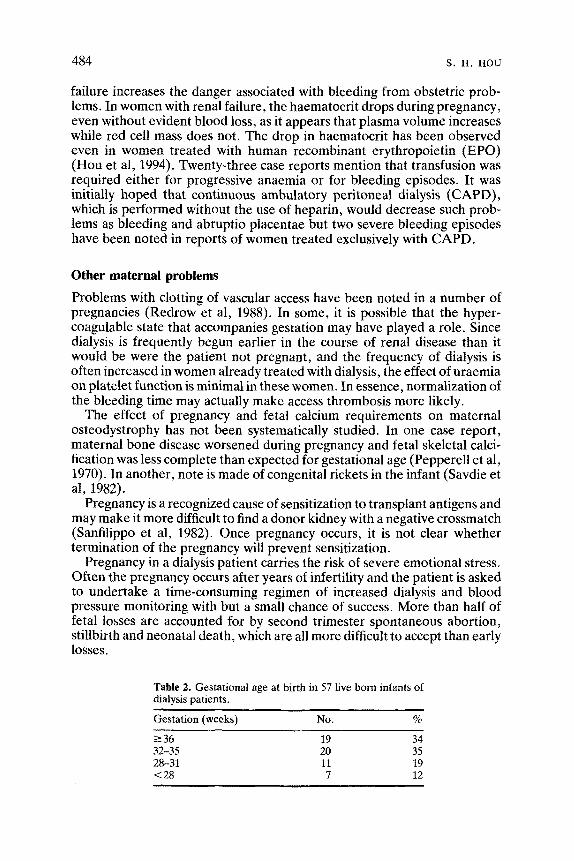
Table 2. Gestational age at birth in 57 live born infants of dialysis patients.
Gestation (weeks) No. %
-> 36 19 34 32-35 20 35 28-31 11 19 < 28 7 12

HAEMODIALYSIS AND PERITONEAL DIALYSIS 485
Systemic lupus erythematosus (SLE) and diabetes are common causes of renal failure among women of childbearing age and pregnancy can be complicated by problems associated with these conditions as well as by renal failure. In the cases reported to date, six women had ESRD as a result of diabetes and seven had ESRD as a result of SLE.
RISKS TO THE FETUS AND NEONATE
Fetal or neonatal death
Pregnancy loss can occur at any time during the pregnancy. First trimester losses are probably underestimated because diagnosis is frequently made late. Placental insufficiency occurs late in gestation. Abnormalities found in the placenta include abruptio, infarction and microscopic areas of fibrosis. Neonatal deaths secondary to prematurity are common.
Prematurity
Prematurity is common as 38 of the 57 live born infants for whom informa- tion is available were born before 36 weeks gestation. The distribution of gestational age is summarized in Table 2. The most common reason for early delivery was premature labour, which accounted for 20 of the premature deliveries (see Table 3). Transient contractions were common during dialy- sis and following placement of a peritoneal catheter. Polyhydramnios was common in pregnant dialysis patients, perhaps as a result of an osmotic diuresis by the fetus with normal kidneys presented with an increased urea load, and it may have contributed to premature labour in some cases. Other causes of premature delivery include fetal distress, abruptio placentae, other bleeding problems, premature rupture of membranes, hypertension and intrauterine growth retardation. In some premature deliveries several factors were causative.
In many instances, premature labour began during dialysis, but it was unclear whether dialysis itself precipitated premature labour. Premature labour occurs in women with renal insufficiency who are not on dialysis (Hou et al, 1985), and has been noted in CAPD patients as well as haemodialysis patients. However , haemodialysis is accompanied by a decrease in serum
Table 3. Causes for premature delivery in 38 live births.
Cause No. %
Premature labour 20 50 Fetal distress 7 18 Haemorrhage/abruptio placentae 4 10 Intrauterine growth retardation 3 8 Hypertension 3 8 Prolapsed cord 1 3 Elective 1 3

progesterone levels of about 10% and this drop may precipitate labour (Johnson et al, 1979).
Growth retardation
.=
.£: .t2~ 03
The weights of infants born at various gestational ages are reported in Figure 1. Twenty-one of the infants were below the 10th percentile at birth, with an additional six at the 10th percentile. Of the infants who were small for gestational age, nine were exposed to severe hypertension (diastolic blood pressure 110 mmHg or greater).
5OOO 4750 4500 4250 4000 3750 3500 3250 3000 2750 2500 2250 2000 1750 1500 1250 1000 750 500
486 s. H, HOU
24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
Weeks of gestation Preterm ~ Term ~ Postterm -1
Large for gestationat age
90th%
Appropriate for gestational age
10th%
Small for gestational age
Figure 1. Weight versus gestational; age in 54 infants of dialysis patients. 0 , Infants of haemodialysis patients who survived; A stillbirths and neonatal deaths in infants of haemo- dialysis patients; O, infants of CAPD patients who survived; A, stillbirths or neonatal deaths in infants of CAPD patients.
Other neonatal complications
Most of the neonatal problems experienced by the infants were the result of prematurity, including jaundice and respiratory distress. In all infants in whom serum urea nitrogen and creatinine were measured, cord levels approached maternal concentrations at birth. Infants born to women with renal failure experience an osmotic diuresis at birth which leads to rapid volume contraction if losses are not replaced.
Additionally, one infant was born with a poorly calcified skeleton and a second was born with congenital rickets; both problems were felt to be the result of the derangement in maternal calcium and phosphorus metabolism (Pepperell et al, 1970; Savdie et al, 1982).

HAEMODIALYSIS AND PERITONEAL DIALYSIS 487
Detailed follow-up of intellectual and physical development in these infants who have been exposed to an azotaemic intrauterine environment has not been carried out. Brem et al (1988) found delayed motor develop- ment in one such infant at 11.5 months and normal development in another at age 15 months. It is difficult to separate the effects of azotaemia from the effects of prematurity and of other diseases such as SLE and diabetes. Apgar scores were recorded in 42 babies. Fifteen had 1-min Apgar scores of 5 or less, while five had scores of 5 or less at 5 min. Only one baby with an Apgar score of 5 or less at 5 rain survived. Congenital anomalies did not appear to be increased.
MANAGEMENT
Deterioration in renal function
Almost one-half of the patients dialysed during pregnancy did not require dialysis prior to pregnancy. When a women with renal insufficiency experi- ences a decline in renal function during pregnancy, she needs to be assessed for reversible causes of renal failure. Nephrotoxic drugs should be avoided, although the use of indomethacin is sometimes required for control of premature labour. Several cases of reversible obstruction by the pregnant uterus have been described (Homans et al, 1981). Polyhydramnios, single kidney and renal transplant are risk factors for obstruction. When obstruction is caused by the pregnancy, it may be relieved by turning the patient on the side opposite the single kidney or, when polyhydramnios is present, by indomethacin or periodic removal of amniotic fluid. If obstruction occurs secondary to other causes, percutaneous nephrostomy tubes or ureteral stents can be placed by a urologist experienced in doing these procedures in pregnant women. Pre-eclampsia is probably the most common cause of reversible renal failure in pregnant women. Diagnosis can be difficult as most of the parameters followed to diagnose pre-eclampsia are distorted by underlying renal disease. It is rarely necessary to do a biopsy to distinguish between pre-eclampsia and other causes of worsening renal function. The decision as to whether to terminate the pregnancy can usually be decided on the basis of whether or not the blood pressure can be controlled.
Standard practice in the past was to recommend termination of pregnancy when renal function deteriorated, with the hope that deterioration could be reversed. Our experience has been that once a decline in renal function occurs, it may progress or at best stabilize after the termination of preg- nancy. The decision as to whether to terminate pregnancy is best made before the decline in renal function. Once the decline in renal function occurs, the patient cannot be assured that renal function will improve and that the delivery of a previable infant is justified. Often the underlying disease is one that is destined to progress and pregnancy merely hastens the need for dialysis. The outcome of pregnancy in women who start dialysis after conception is better than for dialysis patients as a whole (over 80% live births in patients we have cared for) and since a successful renal transplant

488 s.H. HOU
cannot be guaranteed, the pregnancy may represent the woman's best chance for successful pregnancy. If renal function worsens later than 32 weeks gestation, when fetal survival without long-term sequelae is likely, it is reasonable to deliver the baby early for combined maternal and fetal reasons.
Prophylactic or intensified dialysis
It is common practice to begin dialysis in pregnant women before it becomes necessary for the health of the mother. In women who conceive while on dialysis, the frequency of dialysis is usually increased. Unless pregnancy in dialysis patients becomes more common, this practice will not be subjected to prospective randomized studies. Although few reports deal with the management of unsuccessful pregnancies, in at least some of those patients the frequency of dialysis has been increased (Redrow et al, 1988). By the same token, there are case reports of successful pregnancy in women with severe azotaemia who were not dialysed during pregnancy (Naranjo et al, 1978). However, there are several arguments in favour of starting dialysis early and increasing its frequency. We know that fetal outcome is poor on regimens that merely keep the mother free of uraemic symptoms, and that success is more common in women with residual renal function. It is reason- able to hypothesize that the baby's chance of survival will improve if the intrauterine environment is made less azotaemic, even though it is unclear whether it is azotaemia or the absence of some as yet unidentified hormonal factor produced by the kidney that leads to premature labour and stillbirth. In many instances, the initiation of dialysis makes blood pressure easier to control as hypertension in women with renal failure often has a component that it is caused by hypervolaemia. Daily dialysis allows a more liberal diet. The amount of fluid that needs to be removed with each treatment is smaller, so the risk of hypovolaemia is lower. If the elevated maternal blood urea nitrogen leads to an osmotic diuresis by the fetus which contributes to the development of polyhydramnios, intensive dialysis may decrease this prob- lem.
There are only a few observations that suggest that haemodialysis is harmful to the baby. Fetal monitoring has been described during dialysis. Sanchez-Casajus et al (1978) described fetal monitoring during haemodialy- sis. During one treatment, fetal distress developed during an episode of maternal hypotension. A second patient described by Redrow et al (1988) was dialysed 3-4 times a week from 26 to 38 weeks gestation. Fetal moni- toring done during each dialysis showed a single episode of fetal distress which was not associated with maternal hypotension. We generally start dialysis when the serum urea nitrogen (SUN) is 60-70 mg d1-1 and the serum creatinine is 6-7 mg d1-1. Once dialysis is initiated, we have arbitrarily tried to keep the SUN below 50 mg d1-1. This goal may be difficult to attain in women who have no residual renal function, who often need daily dialysis to keep the SUN below 50mg d1-1. Most nephrologists have found that the SUN increases in the third trimester, requiring an increase in dialysis time (Confortini et al, 1971).

H A E M O D I A L Y S I S A N D P E R I T O N E A L DIALYSIS 489
Modifications of the haemodialysis prescription
Based on the rationale detailed above, we increase dialysis as needed to achieve a predialysis SUN of <50mgd1-1, and daily dialysis may be required. With the use of daily dialysis, the patient may become hypo- kalaemic and the dialysate potassium concentration may have to be increased to 3-3.5 mmol1-1. We monitor serum electrolytes weekly and increase dialysate potassium accordingly. Serum sodium is decreased in normal pregnancy and we dialyse patients with a bath containing 134 mmol 1- ~ sodium.
Daily dialysis results in the uptake of more alkali than required to offset daily acid production. The respiratory alkalosis associated with pregnancy results in a serum bicarbonate level of 18-22 mmol 1-1 in women with normal renal function. Low bicarbonate dialysate is not widely available and if it is not possible to lower dialysate bicarbonate in women on daily dialysis, they should be monitored for extremes of alkalaemia. There is little information on the metabolism of acetate by pregnant women and we recommend using bicarbonate dialysate.
The effects of pregnancy on calcium and phosphorus metabolism in dialysis patients are not known. There is some production of 1,25- dihydroxycholecalciferol (1,25(OHz)D3) by the fetus and placenta but it is not clear how much intestinal calcium absorption is increased (Weisman et al, 1978). When the dialysis bath contains 3.5 mmol 1-1 calcium the net influx of calcium into the patient is almost 1 g per treatment (Hou et al, 1991), and thus the net influx of calcium from dialysis exceeds the 25-30 g calcium required for calcification of the fetal skeleton. At present, we prescribe no calcium over and above phosphate binders for women dialysed with a 3.5 mmol 1-1 calcium bath. In the patient dialysed with a bath containing 2.5 mmol 1-1, we prescribe 1-2g additional calcium in the form of calcium carbonate daily over and above what is contained in phosphate binders. We monitor pre- and post-dialysis calcium weekly to detect either hypercal- caemia or hypocalcaemia. We recommend measuring 1,25(OHa)D3 levels each trimester, and giving supplements if the level is low. Primary hyper- parathyroidism is associated with a high rate of fetal loss (Kristofferson et al, 1985), but it is unclear whether this results from abnormalities of calcium and phosphorus metabolism or from the toxic effects of parathyroid hormone itself; whether or not parathyroid hormone plays a role in fetal loss in women with renal failure remains to be investigated.
Hypotension during dialysis should be avoided since it has been associ- ated with fetal distress. The use of daily dialysis reduces the amount of volume that needs to be removed during each treatment. Blood pressure should be supported with saline administration as usual. If volume overload ensues despite daily dialysis, isolated ultrafiltration should be used liberally.
In the past, we have advocated minimizing the use of heparin during haemodialysis. Recent literature suggests that the morbidity associated with heparin during pregnancy can be attributed to the underlying condition for which heparin is being given rather than to heparin itself, which does not cross the placenta (Ginsberg et al, 1989). Our experience since the first

490 s . n . Hou
publication of this symposium has been that attempts to limit heparin dose drastically are associated with inordinate blood loss from clotting of the extracorporeal circuit and frequent episodes of dotting in grafts and temporary lines. We now use the usual doses of heparin for dialysis unless the patient has active vaginal bleeding.
The ideal KT/V (clearance x time/volume) and the benefits of high flux dialysis have not been established for pregnant women.
Mode of dialysis: CAPD in pregnancy
Since 1976, CAPD has become a major form of treatment for ESRD, accounting for 19% of dialysis in American patients between the ages of 20 and 44 (United States Renal Data System, 1993). This type of dialysis combines the established technique of instilling dialysate through a per- manent indwelling peritoneal catheter with prolonged dwell times. With this technique, 1.5-3 litres of dialysate are instilled through the catheter four or more times daily and left for 4-8 h, after which time the fluid is removed and replaced by fresh dialysate. Urea and other waste products are removed by diffusion into the dialysate. Volume removal is achieved by including glu- cose in different concentrations as the osmotically active substance that pulls fluid into the peritoneal cavity to be discarded with the spent dialysate.
There are 18 reported pregnancies in 17 CAPD patients (Cattran and Benzie, 1983; Kioko et al, 1983; Redrow et al, 1988; Gadallah et al, 1992; Jakobi et al, 1992; Lew and Watson, 1992; Hou et al, 1993; D. Latos, personal communication). Twelve of those pregnancies resulted in an infant who survived the neonatal period. The first series of patients treated with CAPD (Redrow et al, 1988) suggested that the outcome for CAPD patients was better than for haemodialysis patients. This series included six patients who represented all the CAPD patients who had become pregnant in Phoenix, Arizona prior to the time of writing the article so that selection bias was eliminated. However, the series was very small. A recent survey looking at the results of pregnancy in all women of childbearing age in 206 dialysis units in the USA showed a 42% success rate for haemodialysis patients and 83% for CAPD patients, again favouring CAPD; however, the number is still too small to be significant (Hou, 1994). Moreover, the majority of these pregnancies took place at a time when the overall success rate of pregnancies was improving. At present, it is reasonable to start pregnant patients new to dialysis on CAPD but not to switch haemodialysis patients to CAPD.
In the case reports available, 11 catheters were placed in eight women. The stage of gestation ranged from 4 to 29 weeks. Three catheters were placed between 17 and 19 weeks gestation in one patient and all were removed for failure to drain. Outflow obstruction ultimately resulted in switching the patient from peritoneal to haemodialysis. Despite increased abdominal pressure, a dialysate leak was noted in only one patient and a subcutaneous fluid collection was noted in another.
The possibility of peritonitis has raised concern when peritoneal dialysis has been considered. In the publications to date, three episodes of peritonitis have been reported. Labour and delivery occurred shortly after the onset of

HAEMODIALYSIS AND PERITONEAL DIALYSIS 491
peritonitis in two patients. One baby was born at 34 weeks gestation and did well. The second was stillborn at 24 weeks gestation. Most penicillins and cephalosporins can be used in pregnancy. There is little experience with vancomycin. Aminoglycosides have been associated with fetal ototoxicity.
Bloody peritoneal dialysate can indicate serious problems in pregnant CAPD patients, including abruptio placentae, bleeding from uterine vessels or impending spontaneous abortion. Women with bloody dialysate should be hospitalized for observation and undergo ultrasonographic examination to look for placental separation.
Hypertension, anaemia and premature labour were problems in CAPD patients, as they were in haemodialysis patients. Nine pregnancies were complicated by premature labour and only one baby was born at term.
Toward term, the peritoneal dialysis regimen may have to be modified because of discomfort from abdominal fullness. Exchange volume may be decreased and exchange frequency increased. Sometimes a cycler is neces- sary to achieve a target SUN of 50 mg d1-1. In the single instance when peritoneal equilibrium testing (PET) was done during pregnancy, there was no evidence of change in peritoneal membrane permeability (Lew and Watson, 1992).
Six of the live born infants were delivered by caesarian section. Surgical delivery did not require the removal of the peritoneal catheter and in only one instance was haemodialysis used postoperatively. The most common approach was to hold dialysis for 24-72 h after surgery and then to restart CAPD, initially with 1 litre exchanges, gradually increasing to 2 litres.
Treatment of hypertension
In a woman whose renal failure is severe enough to require dialysis, blood pressure should be treated early and aggressively, recognizing that this group has a substantial risk of developing life-threatening blood pressure elevations. We recommend teaching the patient to take her own blood pressure at home, as abrupt increases may occur, and treating with medi- cation any blood pressure over 140/90mmHg that does not respond promptly to fluid removal during dialysis.
Methyldopa has been used for over 30 years in pregnant women and long-term ill effects have not been described. Ounsted and her colleagues (1980) did careful follow-up testing of children whose mothers took methyl- dopa during pregnancy and compared them with the children of normoten- sive and untreated hypertensive controls. In most areas the children whose mothers had been treated with methyldopa were not significantly different from controls. In the few areas where the difference was significant, the children of mothers treated with methyldopa performed slightly less well than the children of normal mothers and slightly better than the children of mothers with untreated hypertension. However, methyldopa frequently causes central nervous system side-effects such as fatigue and depression in the mother. Moreover, since methyldopa causes hepatitis in a small percent- age of patients, its use can make assessment of third trimester transaminase elevations more difficult. None the less, methyldopa still represents the

492 s .H. HOU
standard against which other antihypertensive medications should be measured.
[3-Adrenergic antagonists have enjoyed widespread popularity in the treatment of hypertension. Initial use of them in the newborn led to reports of bradycardia, apnoea and hypoglycaemia (Gladstone et al, t975). Intrauterine growth retardation was noted by Pruyn et al (979) and there has been concern, based on animal work, that these drugs interfere with the ability of the fetus to withstand anoxic stress (Cottle et al, 1983). Since many of the diseases treated with t3-blockers are associated with fetal distress and intrauterine growth retardation, it is difficult to assess whether these are truly adverse effects of the drugs, except in prospective randomized trials. Gallery et al (1979) carried out a randomized comparison of the 13-adrener- gic blocking drug, oxyprenolol, with methyldopa and found no difference in fetal loss. They did note, however, that infants born to mothers treated with oxyprenolol were significantly heavier than infants born to mothers treated with methyldopa. The Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (1990) gives tentative approval to the use of 13-blockers in pregnancy.
Limited studies have been carried out with labetolol (Jouppila et al, 1986) and no fetal problems were found. Hydralazine has been used both orally and intravenously without adverse effects. Oral hydralazine can be added to a sympatholytic agent if blood pressure control with a single drug is inadequate.
Calcium channel blockers have become popular in the treatment of hypertension in the general population. Nifedipine has been used both acutely and chronically for hypertension in pregnant women without serious ill effects (Waiters and Redman, 1984). Experience with its use in early pregnancy is limited. It is often effective in hypertension that is refractory to the combination of a sympatholytic agent and hydralazine.
Angiotensin converting enzymes are among the most commonly used drugs in patients with renal failure. Patients who conceive before they require dialysis will almost certainly be treated with angiotensin converting enzyme inhibitors because of the growing evidence that they slow the progression of renal failure. However, angiotensin converting enzyme inhibitors are strongly contraindicated in pregnancy. Animal data in rabbits demonstrate that captopril decreases placental prostaglandin production and blood flow (Ferris and Weir, 1983). When rabbits were treated 2.5 mg kg-lday -1 of captopril, only 20% of fetuses survived, and when the dose was increased to 5 mg kg-lday -1, only 7.5% of fetuses survived. There are 85 reported uses of angiotensin converting enzyme inhibitors in human pregnancy (Hanssens et al, 1991). Their use was commonly complicated by oligohydramnios, which contributed to fatal pulmonary hypoplasia in three cases. There were nine episodes of neonatal anuria, six associated with oligohydramnios. Four infants died and five required dialysis from 3 to 9 days. Eleven of the 68 infants for whom the outcome was known were either stillborn or did not survive the neonatal period.
In summary, our approach to hypertension when medication is needed to begin treatment with 1 g methyldopa divided into two daily doses. If a large

HAEMODIALYSIS AND PERITONEAL DIALYSIS 493
dose is not tolerated, the drug can be divided into four daily doses. 13-Adrenergic blocking agents and labetalol (a combination a- and 13-antagonist) are acceptable alternatives. Methyldopa can be increased to a total of 3 g daily. If blood pressure remains elevated, hydralazine can be added in daily doses of 200 mg, and even up to 400 mg, although there is a 10% incidence of drug induced lupus at the higher dose. If blood pressure control is still unsatisfactory, long-acting nifedipine starting in doses of 30mg and gradually increasing to 90rag a day can be used in place of hydralazine, while continuing the first line drug.
When the patient develops a hypertensive crisis, seizures or diastolic blood pressure over 110 mmHg when taking maximum oral medication and dialysed to ideal weight, the pregnancy should be terminated. The patient can be treated with intravenous hydralazine while preparing for delivery. If there is an inadequate response to 10-30 mg intravenous hydralazine, short- acting nifedipine in doses of 10-30 mg can be used. Intravenous labetalol has been used as an alternative to hydralazine. If there is inadequate response to hydralazine, nifedipine and labetalol, diazoxide can be used in successive doses of 30 mg given by intravenous push. Nitroprusside is to be avoided because of the risk of fetal cyanide toxicity, a risk which is higher in dialysis patients. Termination of the pregnancy will almost invariably make the blood pressure easier to control, but the patient should be followed vigi- lantly for at least 6 weeks postpartum since hypertensive crisis has been described during the first postpartum weeks. Benzodiazapine and pheno- barbitol are preferable to magnesium for the prevention of seizures since magnesium can be removed only by dialysis if magnesium toxicity occurs.
Treatment of premature labour
Premature labour is the single most frequent cause of premature birth in dialysis patients. Thirty-four pregnancies were complicated by premature labour. In 20, it led to birth before 36 weeks gestation. Fourteen women were treated for their premature labour with various medications, and in 12 delivery was delayed between 1 and 11 weeks. Twenty were not treated, and delivery was delayed in seven for between half a week and 9 weeks. The onset of premature labour in the treated group ranged from 23 to 31 weeks. Ten were delivered over 32 weeks. In the untreated group, the onset of premature labour was between 21 and 35 weeks. Fourteen were delivered before 32 weeks. In six reports polyhydramnios was specifically mentioned. It was also present in five patients who did not experience premature labour, four of whom were delivered very early for other indications. In two, labour was precipitated by peritonitis. Four patients suffered abruptio placentae, leading to one spontaneous abortion, one premature delivery before the onset of labour and two instances of premature labour. The first step in evaluation and treatment of a dialysis patient with premature labour is to evaluate the patient for premature placental separation by ultrasonography.
After institution of bed rest, correction of any volume contraction and treatment of any peritonitis, a number of drugs can be used. [3-Agonists have

494 s.H. HOU
been the first line of therapy in patients in whom they are not contra- indicated because of hypertension or heart disease. We have found them to be of limited use, although in case reports they were the mostly commonly used treatment.
Redrow et al (1988) used intraperitoneal magnesium to treat CAPD patients with premature labour. They gave a loading dose of magnesium intravenously and added magnesium to the dialysate to give a dialysate magnesium level of 5 mg dl-1. If serum concentration exceeded 5 mg dl-1, it was lost in the dialysate, preventing dangerous levels. Despite the safety and ease of treatment found by Redrow et al, we discourage the use of mag- nesium. We have found that there is a high risk of the patient receiving standard obstetric doses of magnesium, particularly when many physicians are involved in the care of the patient, and we have seen one episode of pulmonary oedema resulting from magnesium toxicity. Some obstetric investigators question its efficacy in women with normal renal function and discourage its use (Higby et al, 1993).
Nifedipine has been used to stop premature labour and its use is fairly safe but our experience with it has been too limited for us to advocate its use. The combination of magnesium and nifedipine can cause profound hypotension and the two should not be used together.
To date, our greatest success with the treatment of premature labour has been with the use of indomethacin (Hou et al, 1993). The patients must be monitored for the development of oligohydramnios, but in those who have polyhydramnios, the reduction in amniotic fluid volume may remove the underlying cause for premature labour. Women with renal failure generally need treatment for longer than the recommended 72 h. The infant requires monitoring by ultrasonography for any evidence of right heart failure. In women with residual renal function, indomethacin may eliminate that residual renal function and the patient may require greater potassium restriction and more frequent dialysis.
Although the usefulness of home contraction monitors has been ques- tioned, our current practice is to begin using them at 20 weeks gestation.
Correction of anaemia
The anaemia of renal failure usually worsens during pregnancy as plasma volume increases without an increase in red cell mass. Forty-eight case reports specified that the mother was anaemic. In 23 women transfusions were required, in some instances as many as 15 units during the pregnancy. Controversy exists regarding the impact of anaemia on the mother and fetus. There is a consensus that a haemoglobin of less than 6 g d1-1 is associated with increased perinatal mortality and with maternal high output failure (Beischer, 1971). Other studies suggest that the rates of prematurity are doubled in women with a haemoglobin less than 10 g d1-1, although such studies did not adequately control for other risk factors (Klein, 1961; Kaltreider and Johnson, 1976). In view of the high risk of prematurity and bleedin~ in dialysis patients, we recommend a target haemoglobin of 10 g dl -~ or higher.

HAEMODIALYSIS AND PERITONEAL DIALYSIS 495
Eleven women were treated with erythropoietin during pregnancy (Fujimi et al, 1990; Barri et al, 1991; McGregor et al, 1991, Gadallah et al, 1992; Jakobi et al, 1992; Wadhwa et al, 1992; Hou et al, 1993). Three required transfusions during pregnancy and one was transfused for a postpartum bleed. Seven patients were hypertensive, but in only one was it a severe problem. In the others hypertension was no more difficult to control than it had been prior to pregnancy. In patients who had a stable haemato- crit when receiving erythropoietin prior to pregnancy, haematocrit dropped during pregnancy and erythropoietin requirements increased. The drop in haematocrit occurred even when iron deficiency was not present or when it was treated. There were no congenital anomalies among infants whose mothers were treated with erythropoietin during organogenesis, and cord blood erythropoietin levels showed no evidence that erythropoietin crossed the placenta. The recent survey of American dialysis units (Hou, 1994) showed no improvement in infant survival with the use of erythropoietin; however, in view of the morbidity associated with maternal transfusions, we have elected to continue erythropoietin use during pregnancy. We now increase erythropoietin dose by 50% as soon as pregnancy is recognized, in the hope that the haematocrit will not drop and the need for transfusion can be avoided. Further experience will be needed before the ideal increase in the dose of erythropoietin can be determined.
Like other pregnant women, dialysis patients should receive 1 mg folate daily over and above their usual supplement. Iron, total iron binding capacity and ferritin should be monitored monthly and the patient treated with intravenous iron as needed.
Infection
Infection is a common problem in pregnant dialysis patients, as it is in all dialysis patients. The early initiation of dialysis may necessitate the use of temporary access with its associated risk of infection; even with well- established haemo and peritoneal access, infection remains a problem. The first priority in the treatment of infection is the protection of the mother, but the fetus should be protected as far as is possible without endangering the mother.
Experience with infection in pregnancy has shown penicillins and cephalosporins to have the best track record for safety. Aztreonam has also proved safe for treatment of Gram-negative infections. There are few data on vancomycin, which is commonly used in dialysis patients because of its convenience rather than superior efficacy. For treatment of Gram-positive infections, penicillins or cephalosporins should be used. Broad-spectrum cephalosporins or aztreonam should be used for Gram-negative infections. Aminoglycosides are still occasionally required but carry the risk of fetal ototoxicity and, in rare cases, fetal renal damage. While trimethoprim sulphamethoxazole has not been associated with fetal problems, its use is usually avoided because of the theoretical risk of using folic acid antagonists in a developing fetus and because of the risk of using sulphonamides in a fetus that may be at risk for glucose 6-phosphate dehydrogenase deficiency.

496 s .H. IJov
Because metronidazole has been found to cause mutagenesis in animals, its use is avoided in the first trimester. Ciprofloxacin is currently part of the initial treatment of peritonitis in CAPD patients, but it has been associated with defective cartilage development. Aztreonam or a cephalosporin should be used as an alternative.
Diet
Our approach is to dispense with any dietary protein restriction and increase dialysis to deal with the increased azotaemia. Haemodialysis patients should take in l gkg- lday -1 protein plus an additional 20g for the pregnancy. CAPD patients should add 20g to a baseline intake of 1.5gkg-~day -1. Patients should receive a supplement containing 15 mg day -1 of zinc. Water- soluble vitamins should be supplemented over and above the usual supplement for dialysis patients. This should be accomplished by increasing the standard renal supplement rather than by prenatal vitamins, which should be avoided because they carry the risk of vitamin A toxicity. It is difficult to prescribe a specific weight gain for pregnant dialysis patients. They should undergo physical examination weekly to evaluate volume status, and dialysis fluid removal should be adjusted accordingly. Such evaluations are imprecise and do not fully avoid the problems of fluid overload or hypotension, but we have found it almost impossible to pre- scribe a specific weight gain.
Antenatal monitoring
Because of the risk of growth retardation and stillbirth, close monitoring of the fetus is necessary. Fetal growth can be monitored by ultrasonography every 2 weeks. Monitoring of fetal wellbeing should start at 26 weeks gestation when the fetus begins to have a reasonable chance of survival outside the uterus. Non-stress testing is both simple and safe, but it may be difficult to interpret at 26 weeks. When the non-stress test is non-reactive, a biophysical profile can be done. Oxytocin challenge testing may precipitate premature labour and should be avoided. Because there has been at least one report of a stillbirth within a week of a reassuring non-stress test, the test should be performed twice weekly. In a woman taking [3-adrenergic blocking agents, fetal bradycardia may be present without fetal distress. It is not yet known whether antenatal testing developed in the setting of diseases where fetal compromise develops slowly will consistently identify a fetus at risk of stillbirth in a pregnant dialysis patient. The cause of stillbirth in the infants of dialysis patients is not known. If it is related to electrolyte abnormalities it may occur without warning. The uncertainty about our ability to assess fetal weltbeing has led to the practice by some of elective delivery at 36 weeks if amniocentesis shows fetal lung maturity. Practically, it is more common for an indication for delivery to appear before 36 weeks gestation.

HAEMODIALYSIS AND PERITONEAL DIALYSIS 497
SUMMARY
Pregnancy in women with renal insufficiency and end-stage renal disease, while uncommon, is definitely possible, and such women should not assume they are infertile. Contraception should be prescribed for those who do not want to conceive. For the woman who is dialysed during pregnancy, the risks can be minimized by aggressive blood pressure control and prompt diagnosis and treatment of bleeding episodes; however, no degree of vigilance can guarantee that a woman will not suffer any of the severe complications that have been described in pregnant dialysis patients. Intensive dialysis should be undertaken to maintain chemistries that are as nearly normal as possible, and premature labour should be treated with indomethacin. Our current state of knowledge suggests that the success rate of pregnancy in dialysis patients is no better than 52%. It remains to be seen whether CAPD and erythropoietin improve the currently poor outcome.
While transplantation offers the best chance of child bearing for women with end-stage renal disease, transplantation is not always possible. Thus we no longer discourage women on dialysis from becoming pregnant as long as they understand that the likelihood of success is small and that serious risks are involved, and as long as they are willing to follow the time-consuming regimen we think it is necessary for their safety. We hope that, in time, increased experience with pregnant dialysis patients will lead to more successful outcomes and that the possibility of parenthood will be added to the improved quality of life in these women.
REFERENCES
Ackrill P, Goodwin FJ, Marsh FP, Stratton D & Wagman H (1975) Successful pregnancy in a patient on regular dialysis. BMJ 2: 172-174.
Alcalay M, Blau A, Barkai G, Lipitz S, Maschiach S & Eliahou HE (1992) Successful pregnancy in a patient with potycystic kidney disease and advanced renal failure. The use of prophylactic dialysis. American Journal of Kidney Diseases 19: 382-384.
Amoah E & Arab H (1991) Pregnancy in a hemodialysis patient with no residual renal function. American Journal of Kidney Diseases 17: 585-587.
Barri YM, A1-Furayh O, Qunibi WY & Rahman F (1991) Pregnancy in women on regular hemodialysis. Dialysis and Transplantation 20: 652-656.
Becker GJ, thie B, Fairley K, Bastos M & Kincaid-Smith P (1986) Effect of pregnancy on moderate renal failure in reflux nephropathy. BMJ 292: 796-798.
Beischer NA (1971) The effects of maternal anemia upon the fetus. Journal of Reproductive Medicine 6: 262-265.
Brem AS, Singer D, Anderson L, Lester B & Abuelo JG (1988) Infants of azotemic mothers: a report of three live births. American Journal of Kidney Diseases 12: 299-303.
Cattran DC & Benzie RJ (1983) Pregnancy in a continuous ambulatory peritoneal dialysis patient. Peritoneal Dialysis Bulletin 3: 13-14.
Cohen D, Frenkel Y, Maschiach S & Eliahou HE (1988) Dialysis during pregnancy in advanced chronic renal failure patients: outcome and progression. Clinical Nephrology 29: 144-148.
Confortini P, Galanti G, Ancona G e t al (1971) Full term pregnancy and successful delivery in a patient on chronic haemodialysis. Proceedings of the European Dialysis and Transplant Association 8: 74-80.
Cottle MKW, Van Petten & van Muyden P (1983) Maternal and fetal cardiovascular indices

498 s . H . HOU
during fetal hypoxia due to cord compression in chronically cannulated sheep. American Journal of Obstetrics and Gynecology 146: 678--685.
David AS, Newling DWW & Farr MJ (1983) Successful pregnancy following haemodialysis and pyeloplasty. Nephron 34: 64-66.
Dolkart LA, Eshwar KP & Reimers FT (1992) Indomethacin therapy and chronic hemodialysis during pregnancy. Journal of Reproductive Medicine 37: 181-183.
Ferris TF & Weir EK (1983) Effect of captopril on uterine blood flow and prostaglandin E synthesis in the pregnant rabbit. Journal of Clinical Investigation 71: 809-815.
Fujimi S, Hori K, Miijima C & Shigametsu M (1990) Successful pregnancy and delivery in a patient following rHuEPO therapy and on long-term dialysis. Journal of the American Society of Nephrology 1: 397.
Gadallah MF, Ahmad B, Karubian F & Campese VM (1992) Pregnancy in patients on chronic ambulatory peritoneal dialysis. American Journal of Kidney Diseases 20: 407-410.
Gallery EDM, Saunders DM, Hunyor SN & Gyory AZ (1979) Randomized comparison of methyldopa and oxyprenolol for treatment of hypertension in pregnancy. BMJ 1: 1591- 1594.
Ginsberg JS, Kowalchuk G, Hirsh J, Brill-Edwards P & Burrow R (1989) Heparin therapy during pregnancy. Archives of Internal Medicine 149: 2233-2236.
Gladstone GR, Hordof A & Gersony WM (1975) Propranolol administration during preg- nancy: effects on the fetus. Pediatrics 86: 962-964.
Hanssens M, Keirse MJNC, Vankelecom F & Van Assche FA (1991) Fetal and neonatal effects of treatment with angiotensin converting enzyme inhibitors in pregnancy. Obstetrics and Gynecology 78: 128-135.
Harum P, de Velasco R, Pellegrini E, Garcia Estrada H & Robbins ML (1987) Nutrition in a pregnant dialysis patient. CRN Quarterly 2: 10-14.
Herwig KR, Merrill JP, Jackson RL & Okon DE (1965) Chronic renal disease and pregnancy. American Journal of Obstetrics and Gynecology 92: 1117-1121.
Higby K, Xenakis EMJ & Pauerstein CJ (1993) Do tocolytic agents stop preterm labor? A critical and comprehensive review of efficacy and safety. American Journal of Obstetrics and Gynecology 168: 1247-1259.
Homans DC, Blake GD, Harrington JT & Cetrullo CL (1981) Acute renal failure caused by ureteral obstruction by a gravid uterus. JAMA 246: 1230-1231.
Hou S (1994) Frequency and outcome of pregnancy in women on dialysis. American Journal of Kidney Diseases 23: 60--63.
Hou S, Grossman S & Madias N (1985) Pregnancy in women with renal disease and moderate renal insufficiency. American Journal of Medicine 78: 185-194.
Hou S, Orlowski J, Pahl M e t al (1993) Pregnancy in women with end-stage renal disease: treatment of anemia and premature labor. American Journal of Kidney Diseases 21" 16-22.
Jakobi P, Ohel G, Szylman P e t al (1992) Continuous ambulatory peritoneal dialysis as the primary approach in the management of severe renal insufficiency in pregnancy. Obstetrics and Gynecology 79: 808-810.
Johnson TR, Lorenz RP, Menon KMJ & Nola GH (1979) Successful outcome of a pregnancy requiring dialysis. Journal of Reproductive Medicine 22: 217-218.
Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (1990) National high blood pressure education program working group report on high blood pressure in pregnancy. American Journal of Obstetrics and Gynecology 163: 1689-1712.
Jouppila P, Kirkinen P, Koivula A & Ylikorkaloa O (1986) Labetolol does not alter the placental and fetal blood flow or maternal prostanoids in pre-eclampsia. British Journal of Obstetrics and Gynecology 93: 543-547.
Kaltreider D & Johnson JW (1976) Patients at high risk for low birth weight delivery. American Journal of Obstetrics and Gynecology 124: 251-256.
Kioko EM, Shaw KM, Clarke AD & Warren DJ (1983) Successful pregnancy in a diabetic patient treated with continuous ambulatory peritoneal dialysis. Diabetes Care 6: 298-300.
Klein L (1961) Premature birth and maternal prenatal anemia. American Journal of Obstetrics and Gynecology 83: 588-590.
Kobayashi H, Matsumoto Y, Otsubo O, Otsubo K & Naito T (1981) Successful pregnancy in a patient undergoing chronic hemodialysis. Obstetrics and Gynecology 57: 382-386.
Kristoffersson A, Dahlgren S, Lithner F & Jarhult J (1985) Primary hyperparathyroidism in pregnancy. Surgery 97: 326-330.

HAEMODIALYSIS AND PERITONEAL DIALYSIS 499
Leader L, Strasburg ER, Baillie P & Keeton RD (1978) Hemodialysis in pregnancy. South African Medical Journal 53: 871-872.
Lee SH, Wang TC, Lee TY, Chen FY & Chien TY (1981) Successful pregnancy in a patient on hemodialysis. Journal of the Formosan Medical Association 80: 136-140.
Lew SQ & Watson JA (1992) Urea and creatinine generation and removalin a pregnant patient receiving peritoneal dialysis. Advances in Peritoneal Dialysis 8: 131-135.
Lindley JD, Beathard GA, Moncrief JW, Decherd JF, Baker J, Sharp E & Broadrick LJ (1978) Successful pregnancy in the long term hemodialysis patient. Kidney International 14:679 (abstract).
McGregor E, Stewart G, Junor BJR & Rodger RSC (1991) Successful use of recombinant human erythropoietin in pregnancy. Nephrology, Dialysis, Transplantation 6: 292-293.
Marwood RP, Ogg CS, Coltart TM & Klopper AI (1977) Plasma oestrogens in a pregnancy associated with chronic haemodialysis. British Journal of Obstetrics and Gynaecology 84: 613-617.
Mitra S, Vertes V, Roza O & Berman LB (1970) Periodic hemodialysis in pregnancy. American Journal of Medical Sciences 259: 333-339.
Nageotte MP & Grundy HO (1988) Pregnancy outcome in women requiring chronic hemo- dialysis. Obstetrics and Gynecology 72: 456-459.
Naik RB, Clark AD & Warren DJ (1979) Acute proliferative glomerulonephritis with crescents and renal failure in pregnancy successfully managed by intermittent haemodialysis. British Journal of Obstetrics and Gynaecology 86: 819-822.
Naranjo P, Prats D & Rodrigo A (1978) Insuiciencia renal avanzada embarazo. Revista Clinica Espanola 149: 509-512.
Nemoto R, Sugiyama Y, Kuwahara M, Kato T & Tsuchida S (1977) Successful delivery of a patient on hemodialysis for acute renal failure. A case report and review of the literature. Journal of Urology 118: 673-674.
Orme BM, Ueland K, Simpson DP & Scribner BH (1968) The effect of hemodialysis on fetal survival and renal function in pregnancy. Transactions of the American Society for Artificial Internal Organs 14: 402-404.
Ounsted MK, Moar VA, Good FJ & Redman CWG (1980) Hypertension during pregnancy with and without specific treatment: the development of the children at the age of four years. British Journal of Obstetrics and Gynaecology 87: 19-24.
Pepperell ILl, Adam WR & Dawborn JK (1970) Hemodialysis in the management of chronic renal failure during pregnancy. Australian and New Zealand Journal of Obstetrics and Gynecology 10: 180-186.
Pruyn SC, Phelan JP & Buchanan GC (1979) Long term propranolol therapy in pregnancy: maternal and fetal outcome. American Journal of Obstetrics and Gynecology 135: 485-489.
Purdy L, Hantsch C, Molitch ME, Metzger BE, Phelps R, Dooley S, Socol M & Hou S (1993) Effect of pregnancy on the course of renal function in patients with established diabetic nephropathy. Proceedings of the Xllth International Congress of Nephrology, June 1993, p 598 (abstract).
Redrow M, Cherem L, Elliott J e t al (1988) Dialysis in the management of pregnant patients with renal insufficiency. Medicine 67: 199-208.
Registration Committee of the European Dialysis and Transplant Association (1980) Success- ful pregnancy in women treated by dialysis and kidney transplantation. British Journal of Obstetrics and Gynaecology 87: 839-845.
Ringenbach M, Renger B, Beauvais P e t al (1978) Grossesse et accouchement d'un enfant vivant chez une patiente traitre par hrmodialyse itrrative. Journal d'Urologie et de N~phrologie 84: 360-366.
Rotellar C, Ferragut A & Borrull J (1983) Pregnancy in a patient on regular hemodialysis. Nephron 35: 66457.
Roxe DM & Parker J (1985) Reports of a survey of reproductive function in female hemo- dialysis patients. Proceedings of the American Nephrology Nursing Association, National Meeting, New Orleans.
Sanchez-Casajus A, Ramos I & Santos M (1978) Monitorizacirn fetal en el transcurso de hemodi~lysis durante el embarazo. Revista Clinica Espanola 149: 187-188.
SanfiUippo F, Vaughn WK, Bollinger RP & Spoto EK (1982) Comparative effects of preg- nancy, transfusion and prior graft rejection on sensitization and renal transplant results. Transplantation 34: 360-366.
500 S . H . HOU
Savdie E, Caterson RJ, Mahoney JF et al (1982) Successful pregnancies in women treated by haemodialysis. Medical Journal of Australia 2: 9.
Schwartz A, Post KG, Keller F & Molzahn M (1985) Value of human chronic gonadotropin measurements in blood as a pregnancy test in women on maintenance hemodialysis. Nephron 39: 341-343.
Sheriff MHR, Hardman M, Lamont CAR, Shepherd R & Warren DJ (1978) Successful pregnancy in a 44-year-old haemodialysis patient. British Journal of Obstetrics and Gynaecology 85: 386--389.
Souqiyyeh MZ, Huraib SO, Saleh AGM & Aswad S (1992) Pregnancy in chronic hemodialysis patients in the Kingdom of Saudi Arabia. American Journal of Kidney Diseases 19: 235-238.
Surian M, Imbasciatti E, Cosci P e t al (1984) Glomerular disease in pregnancy. Nephron 36" 101-105.
Thompson NM, Rigby RJ & Atkins RC (1978) Successful pregnancy in a woman on recurrent hemodialysis. Australian and New Zealand Journal of Medicine 8: 243.
United States Renal Data System (1993) Annual Data Report. Bethesda MD: National Insti- tute of Health, National Institute of Diabetes and Digestive and Kidney Diseases.
Unzelman RF, Alderfer GR & Chojnacki RE (1973) Pregnancy and chronic hemodialysis. Transactions of the American Society for Artificial Internal Organs 19: 144-149.
Wadhwa NK, Heesuck S, Latta R, Cashin MJ & Danko H (1992) Use of epoetin alpha in a pregnant diabetic with end stage renal disease. Journal of the American Society of Nephrology 3:432 (abstract).
Waiters BNJ & Redman CWG (1984) Treatment of severe pregnancy-associated hypertension with the calcium antagonist nifedipine. British Journal of Obstetrics and Gynaecology 91: 330-336.
Weisman Y, Vargas A, Duckett G, Reiter E & Root AW (1978) Synthesis of 1,25-dihydroxy- vitamin D3 in the nephrectomized pregnant rat. Endocrinology 103: 1992-1996.
Yasin SY & Beydoun SN (1988) Hemodialysis in pregnancy. Obstetrical and Gynecological Survey 43: 655-668.
Yousri BM, Al-Furayh D, Quribi WY & Rahman F (1991) Pregnancy in women on regular haemodialysis. Transplantation 20: 652-656, 695.