11th international conference on medical regulation · 11th international conference . on medical...
TRANSCRIPT

11th international conference on medical regulation
Medical regulation – evaluating risk and reducing harm to patients
9–12 September 2014London
Conference posters
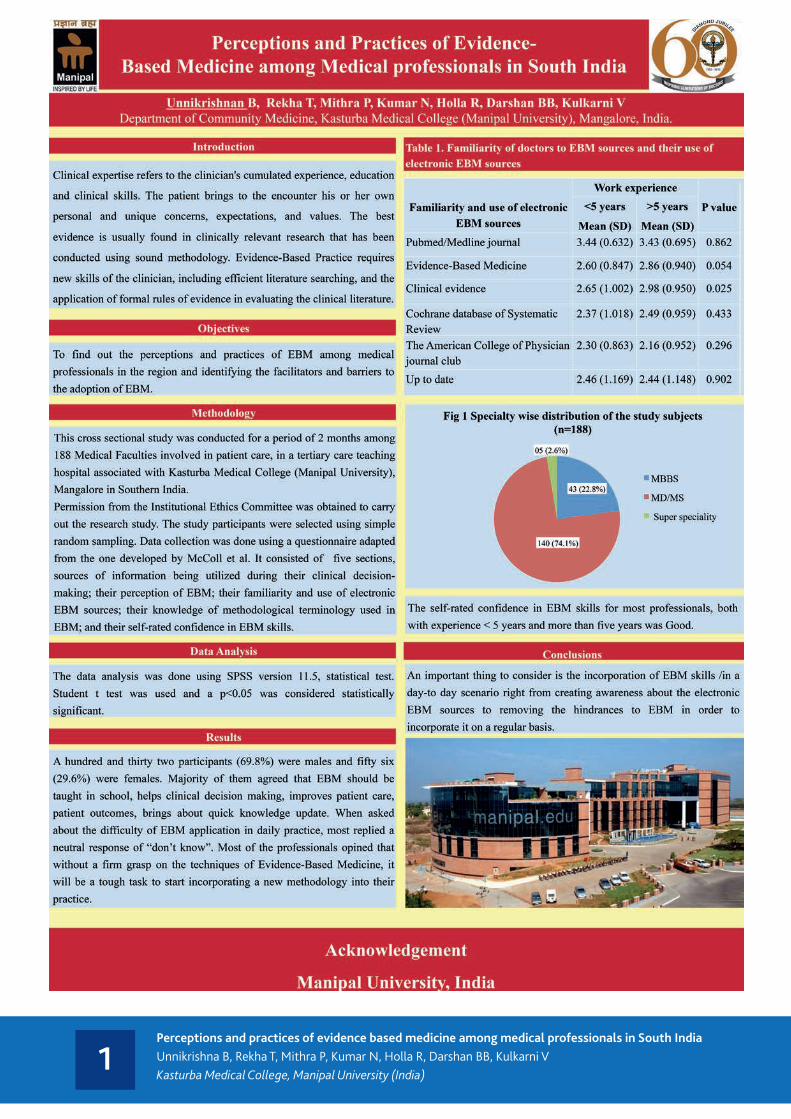
1Perceptions and practices of evidence based medicine among medical professionals in South IndiaUnnikrishna B, Rekha T, Mithra P, Kumar N, Holla R, Darshan BB, Kulkarni VKasturba Medical College, Manipal University (India)

2Tracking doctors’ knowledge and attitudes towards the statutory duty to maintain professional competence: a Medical Council survey of doctors in IrelandGráinne Behan, Fergal McNally, Medical Council of Ireland
TRACKING DOCTORS’ KNOWLEDGE AND ATTITUDES !TOWARDS THE STATUTORY DUTY TO!
MAINTAIN PROFESSIONAL COMPETENCE:!A MEDICAL COUNCIL SURVEY OF DOCTORS IN IRELAND!
!
Gráinne Behan, Fergal McNally!Medical Council of Ireland!
Background:!!In May 2011, the scope of professional medical regulation in Ireland was extended to include a legal duty on all doctors to maintain their professional competence. !!The Medical Council sought to better understand and track doctors’ attitudes and knowledge towards this new duty and determine if Council’s support to doctors in meeting this statutory duty was effective. !
!Results:!!Doctors’ awareness of the detailed requirements of the statutory duty increased year on year; rising from 42% of doctors being aware of requirements at T1, to 94% in T3. (Figure 1). !!Doctors’ self-confidence in their ability to meet the requirements of the new statutory duty fell between T1 and T2 (suggesting that for some doctors the new duties were harder to meet than they anticipated) before rising at T3. (Figure 2). !
!!The number of doctors stating that structural factors supported them in pursuing requirements for the maintenance of professional competence increased over time. For example, at T2, 47% of doctors felt there was access to tools, documents and guides to support them maintaining professional competence compared to 61% at T3. (Figure 3).!
Acknowledgements:!We thank the doctors who participated in the surveys. Postgraduate training bodies play a key role in providing advice to doctors in relation to professional competence requirements and we are grateful for their support. !The studies were directed and overseen by the Medical Council’s former Professional Competence Committee and we would like to thank the past members and former Chair, Dr David O’Keeffe for advice and encouragement. Finally we would like to thank Dr Paul Kavanagh, Director of Professional Development and Practice and Mr Simon O’ Hare, Research Manager for their assistance.!
!!!
!Approach:!!A random, independent, sample of 1000 doctors from the Medical Council’s register of medical practitioners were asked to complete a web-based survey before (in November 2010 = T1) and after (in September 2011 = T2) the introduction of the new regulatory arrangements. !!A similar survey was conducted in June 2013 (T3) to help identify changing trends in doctors’ awareness, attitudes and knowledge towards this duty.!
Figure 1: !• Participants in the 2013 survey were more aware in the types and amounts of
activities required to maintain professional competence. !!!!!!!!!
!!!!!!!!Figure 2: !!
• The survey reported a decrease in confidence in meeting professional competence requirements in T2 before rising again in T3.!
!!!!!!!!!!!!!
Figure 1: !I am aware of the types and amounts of activities that I am required to do to maintain my professional competence. !
42%
58%
Yes No
(T1) Survey 1: 2010
94%
6%
Yes No
(T3) Survey 2: 2013
97%
91%
95%
80%
90%
100%
T1 (2010) T2 (2011) T3 (2013)
Strongly Agree/Agree Figure 2: !I am confident that I can meet requirements to maintain my professional competence.!
Figure 3:!• An increase in participants in T3 agreed that there was access to a range of
support mechanisms to support doctors to maintain professional competence. !
Figure 3: !There is access to tools, documents and guides to support me to pursue standards for maintenance of professional competence !
Conclusions: !Doctors’ awareness of the duty to maintain professional competence improved post introduction of regulatory arrangements.!!Although confidence to maintain competence fell post inception, this then increased and results suggest that support from Medical Council and Postgraduate Training Bodies was effective in helping doctors maintain professional competence. !
47%
61%
T2 (2011) T3 (2013) 10%
20%
30%
40%
50%
60%
70% Strongly Agree/Agree

3Choosing the right path to improve patient safety in Ireland – Medical Council strategy developmentLorna Farren, Caroline SpillaneMedical Council of Ireland
Choosing the right path to improve patient safety in Ireland - Medical Council strategy development
Authors: Lorna Farren, Caroline Spillane Medical Council of Ireland
Background: A clear and coherent strategy is essential in underpinning the work of an effective regulator. The Medical Council developed its first formal statement of strategy for implementation between 2010-2013. For its second strategy, for the period 2014-2018, the objective was to ensure the creation of an effective five year plan for the organisation that enhanced patient safety by drawing on the views and experience of the public, the medical profession and partner organisations.
Results: The Medical Council’s statement of strategy for 2014 to 2018 was launched in March and has been operationalised through the 2014 business plan. The need for leadership within the Irish health system was a key theme emerging from the consultation process. The Council’s vision is: “Providing leadership to doctors in enhancing good professional practice in the interests of patient safety” Six strategic objectives have been set, reflecting the key issues which emerged from internal and external consultation processes. To ensure confidence of all partners in the Council’s work, a detailed programme of metrics have been established which will measure progress over the next five years.
Acknowledgements: The Medical Council would like to thank the 700 doctors, 1,000 members of the public and representatives of over 40 partner organisations who informed the development of the strategy by providing open and honest feedback.
Approach: The development of the statement of strategy followed internal consultation with staff, former and current Council members. To ensure the views of external audiences were captured, research was conducted with approximately 1,000 members of the public and 700 doctors. A detailed consultation plan was also implemented to measure feedback from over 40 partner organisations.
Conclusions: To enhance patient safety and reduce risk, an effective strategy is pivotal. The process focused on transparency and engagement, principles that are fundamental to an effective regulator. The relationships built during the process will assist in the implementation of the strategy as it addresses many of the issues raised by partner organisations, patients and doctors.
Figure 2: Medical Council Values
Figure 1: The Medical Council’s Strategy Wheel

4Caring for others more than for themselves? Doctors’ health experiences in IrelandDr Paul Kavanagh, Caroline Spillane, Simon O’Hare, Lorna Farren, Medical Council of IrelandProf Hannah McGee, Dr Mary Clarke, Royal College of Surgeons (Ireland)

5Medical Workforce Intelligence – the start and end point for medical education and training in Ireland?Dr Paul Kavanagh, Lorna Farren, Caroline SpillaneMedical Council of Ireland
Medical Workforce Intelligence – the start and end point for medical education and training in Ireland? Authors: Paul Kavanagh, Lorna Farren and Caroline Spillane Medical Council of Ireland
Background: The medical workforce is a cornerstone of a strong health system. High quality intelligence is necessary to continually plan, develop and maintain a medical workforce to meet health system needs. Understanding the medical workforce can help better inform the work of the medical regulator; it can also enable the medical regulator to inform health system design in favour of good professional practice and patient safety. To address this, the Medical Council has re-used data from its annual registration retention process to develop medical workforce intelligence for Ireland.
Results: The number and age-profile of the medical workforce in Ireland appear sustainable. However, deeper analyse highlights some challenges: • Age-patterning of outflows underlines the
challenge Ireland faces in retaining domestically trained doctors (Figure 1).
• The high dependence on international medical graduates raises questions about sustainability and equity of workforce planning (Figure 2).
• Skill-mix varies significantly across practice areas and specialisation is growing in the absence of a clear strategic policy framework (Figure 3).
• The feminisation of the medical workforce and variation in work practice are important developments which require a response to ensure all doctors are enables to contribute equitably to the health system (Figure 4).
Acknowledgements: Emma Cassidy and Sarah Lane who contributed to the analysis of data and development of this report. Philip Brady, Head of Registration, led the Medical Council team that managed the annual application retention process.
Approach: The Medical Council maintains a register of doctors who are legally entitled to practise medicine in Ireland. Each year it invites doctors to apply to retain registration. In response to a need to monitor maintenance of competence and ensure continuing fitness to practice, in 2012, this process was comprehensively re-designed to collect data about doctors current practise. Responses were linked with registration data and the final dataset was analysed to identify current number, inflows, outflows and key trends in the medical workforce in Ireland.
Figure 1: Exit rate 2012 per age group (doctors who graduated from Irish medical schools only)
Figure 2: Trend in proportion of doctors registered, Irish versus other medical schools, 2008-2012
Conclusions: Routine administrative data collected from registration processes can be innovatively re-used to directly and indirectly enhance medical regulation. This project provided the Medical Council with a clear and comprehensive view of the medical workforce which it regulates. This better informs strategic policy in education and training, registration and maintenance of competence. It also provides the Medical Council with a platform to engage with the health system to ensure that medical workforce planning and management fosters good practice and promotes patient safety. The response to the report was positive and annual reports are now underway.
Figure 3: Proportion of doctors registered in the Specialist division at year end, 2008-2012
Figure 4: Proportion of female doctors in each age group
6“Your training counts” A national trainee experience survey of doctors in IrelandSimon O’Hare, Paul Lyons, Dr Paul KavanaghMedical Council of Ireland
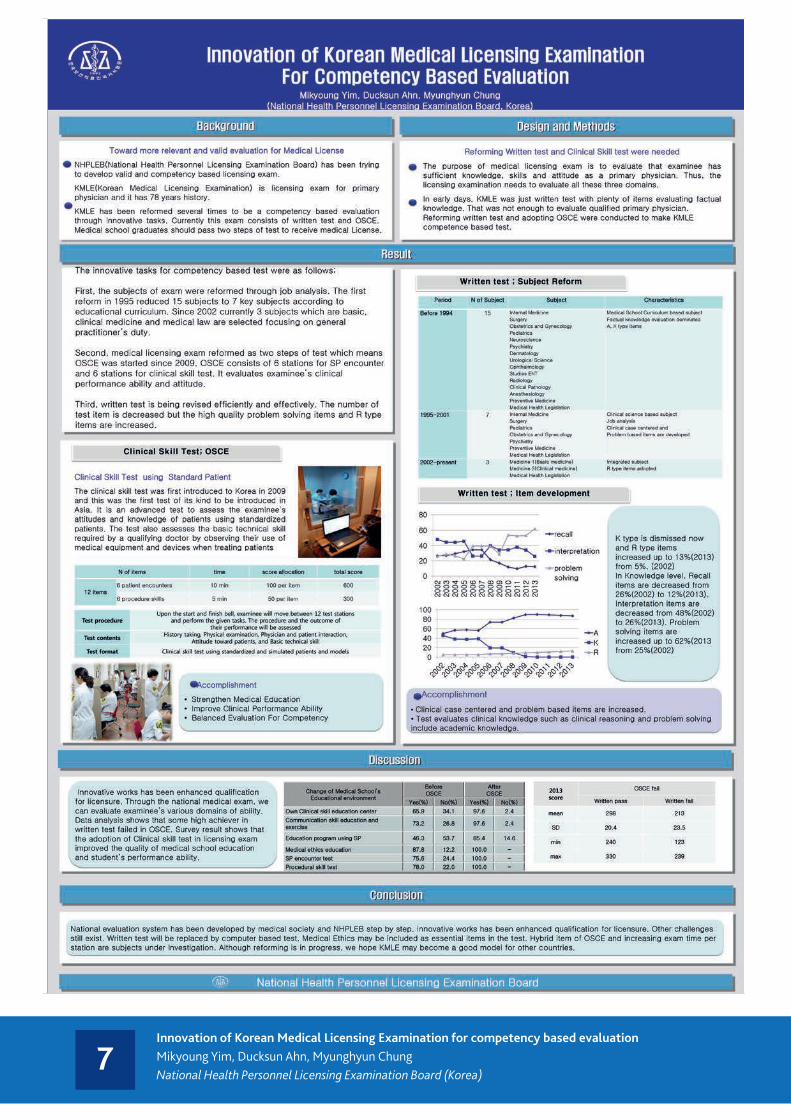
7Innovation of Korean Medical Licensing Examination for competency based evaluationMikyoung Yim, Ducksun Ahn, Myunghyun ChungNational Health Personnel Licensing Examination Board (Korea)

8The Medical Board of Trinidad and Tobago...Challenges even after 200 YEARSProf Samual Ramsewak, Prof Hariharan SeetharamaMedical Board of Trinidad and Tobago
THE
MED
ICAL
BO
ARD
OF
TRIN
IDAD
AN
D TO
BAGO
…
C
halle
nges
eve
n a:
er 2
00 Y
EARS
Alth
ough
two-‐
hund
red
year
s old
, MBT
T is
sIll
evol
ving
as i
t aim
s to
intr
oduc
e an
d m
aint
ain
acce
ptab
le in
tern
aIon
al st
anda
rds i
n re
gula
Ing
the
med
ical
pro
fess
ion.
Muc
h ha
s hap
pene
d sin
ce 1
814
and
the
exisI
ng M
edic
al B
oard
Act
(196
0) w
ith ru
les
and
regu
laIo
ns a
s sIp
ulat
ed in
this
Act a
nd a
s en
acte
d by
Par
liam
ent.
The
maj
or c
halle
nges
cur
rent
ly fa
cing
the
MBT
T ar
e:
• In
trod
ucin
g m
anda
tory
Con
Inui
ng P
rofe
ssio
nal D
evel
opm
ent (
CPD)
for
licen
ce re
new
al in
acc
orda
nce
with
a p
ropo
sed
amen
dmen
t of t
he M
BTT
Act.
This
is ou
tsta
ndin
g de
spite
the
fact
that
CPD
for c
onIn
uing
regi
stra
Ion
has b
een
prop
osed
sinc
e 19
96.
• D
ereg
istra
Ion
of m
edic
al p
racI
Ione
rs w
ho h
ave
not p
aid
thei
r ann
ual
rete
nIon
fees
. The
tota
l num
ber o
f reg
ister
ed m
edic
al p
racI
Ione
rs is
312
1 of
w
hich
onl
y 22
45 (7
2%) a
re in
fina
ncia
l goo
d st
andi
ng w
hile
876
( 28%
) hav
e no
t pai
d bu
t leg
ally
may
con
Inue
to p
racI
ce.
• F
inan
cing
of l
egal
resp
onse
s to
ensu
re a
dequ
ate
repr
esen
taIo
n in
ad
dres
sing
com
plai
nts a
gain
st d
octo
rs, p
arIc
ular
ly si
nce
the
inco
me
of M
BTT
deriv
es so
lely
from
regi
stra
Ion
fees
.

9The impact and relevance of Occupational English Test (OET) for the medical and nursing workplaceDr Ivana VidakovicCambridge English Language Assessment (UK)
1. About OET• It is a screening test of English communication skills for doctors and nurses.
• It is recognised by over 30 regulatory healthcare bodies and councils internationally and has been used for medical registration in Australia since the 1980s. It is available in 28 countries around the world, up to 10 times a year (rising to 12 times a year in 2 time zones from 2015), see www.occupationalenglishtest.org
• As a result of extensive and in-depth research into the linguistic needs and practices of doctors and nurses:
• OET is a test of English for Specific Purposes (ESP) designed to meet the specific needs of doctors and nurses.
• OET Speaking and Writing tests are profession-specific.
• OET Reading and Listening tests are not profession-specific, but are firmly grounded in the healthcare domain.
The impact and relevance of the Occupational English Test (OET) for the medical and nursing workplace
www.occupationalenglishtest.org
4. Summary• Preparing for OET has a positive effect on OET test-takers’ language ability and
confidence.
• OET successfully simulates many relevant aspects of the medical and nursing workplaces for which it is used as an entry requirement. Its validity for these contexts is confirmed in the eyes of test-takers, their workplace supervisors and the interviewed healthcare regulatory bodies.
• OET test-takers are perceived as effective communicators who can communicate on both technical and emotional matters and be easily understood by patients.
1. Preparation for OET impacts positively on OET test-takers’ language ability and on their confidence in using English.
2. Research questions and a mixed methods design
3. Key findings
1. What is the intended impact of using an ESP test, i.e. OET, when assessing the language ability of healthcare professionals?
2. Is OET an appropriate language examination for the health sector in terms of its construct validity (i.e. content, skills/abilities assessed)?
3. Are OET test-takers perceived as ready for the workplace in terms of their English language ability and their confidence in using English in a healthcare context?
The research participants: 603 past OET test takers, 51 colleagues/supervisors, 2 representatives of the healthcare regulatory bodies in Australia.
5. Looking forwardOET rests on a large body of research and an up-to-date research agenda. As part of continuous improvement, a programme of OET revision is being established. The following revisions are already taking place:
• The Speaking test construct has been expanded to bring it in line with the best practice in clinical communication, as encapsulated in the Calgary-Cambridge Guides. The speaking assessment criteria have been enhanced and are currently at the trialling stage, but OET is not intended to replace tests of clinical skills.
• The Listening test will include more representation of professional-professional communication to complement the current emphasis on professional-patient communication. New task types and item writer guidelines are at the development stage.
Test-takers’ perspectivesAs a test relevant to specific healthcare professions, OET has a positive impact on its test-takers. OET test-takers believe that:
a) Preparation for OET prepares them for language-mediated tasks in their profession.
b) Interesting and relevant topics in OET allow them to engage more with test preparation and OET tasks.
c) Familiarity with terminology and content reduces their anxiety during written and spoken tasks.
Perspectives from the workplaceOn the task of writing a letter using case notes as input:‘We do those all day every day.’ (A senior doctor)Writing a discharge letter is ‘very very appropriate.’ (A senior nurse)
On a Listening task: ‘The dialogue is actually very, very relevant.’ (A senior doctor)
The perspectives of the interviewed regulatory healthcare bodies‘Speaking as an employer, sure you would have to have more confidence in someone who could pass the English language test that was related to the industry in which they were going to go and work.’
‘…If testing is congruent with practice, that’s terrific.’
On Speaking tasks: ‘They are relevant. I think they are appropriate.’
3. OET test-takers are able and effective users of English in their workplace.
Test-takers’ perspectives‘As an employee (nurse) in a hospital you are expected to function almost at a hundred percent from day one, meaning that you are expected to understand both patients and staff, the latter often speaking very fast and with lots of abbreviations. Preparing for the OET helped a lot.’ (A nurse)
‘It helped me to communicate with patients and workmates effectively and correctly, because I have gained a lot of good communication styles in a very professional and elegant way.’ (A physician)
‘OET helped me in gaining communication skills with patients and other health professionals. Now I can use some expressions in calming patients and showing empathy, which I knew but never used before.’ (A nurse)
Perspectives from the workplaceThe employees/colleagues who have taken OET… Percentage
agreement
… use English effectively in their health-related workplace. 93%
… communicate well with their patients. 68%
… communicate well with their colleagues. 83%
… understand well what they are told by their colleagues. 83%
… understand well what they are told by their patients. 65%*
… perform well at the writing tasks in their health-related workplace. 83%
… understand well what they read in their health-related workplace. 80%
*The most common feedback focuses on employees’ ability to understand idioms and slang.
Quantitative data collection
InstrumentsQuestionnaires for past test takers(N=585) and employers (N=40)
Qualitative data collection
InstrumentsOpen-ended comments in questionnaires Semi-structured interviews with past test takers (N=18), employers (N=11) and regulatory bodies (N=2)
Quantitative data analysis
ProceduresDescriptive statistics
ProductsFrequency (count and %)
Merge results and provide interpretation
ProcedureConsider how merged results produce better
understanding and confirm findings
ProductDiscussion
Qualitative data collection
ProceduresThematic analysis
ProductsMajor themes
35%
30%
25%
20%
15%
10%
55%
0%...improved a lot ...improved
moderately...improved
slightly...not changed Not sure
70%
80%
60%
50%
40%
30%
20%
10%
0%...using English in my chosen
profession.
...communicatingeffectively with
patients andcarers.
...communicatingeffectively withmy colleagues.
...reading inEnglish in my
chosenprofession.
...writing inEnglish in my
chosenprofession.
Strongly agree/Agree Strongly disagree/Disagree Not sure
70%
80%
90%
60%
50%
40%
30%
20%
10%
0%OET is well designed for
testing the ability ofhealth-care professionals
to use English in my health-related context.
OET assesses anappropriate range of
language relevant for myhealth-related workplace.
The topics in OET arerelevant for my
health-related workplace.
Strongly agree/Agree Strongly disagree/Disagree Not sure
Preparing for OET has made me feel confident about…
2. In the eyes of test-takers, employers and healthcare regulatory bodies, the major strength of OET is its relevance for the healthcare (medical and nursing) context in terms of topics, language, tasks, scenarios and the language ability/skills required to address tasks.
As a result of preparing for OET, my ability to use English in my health-
related context has…
CE_3025_4Y08_P_OET IAMRA 2014 conference poster_JB.indd 1 30/07/2014 12:23
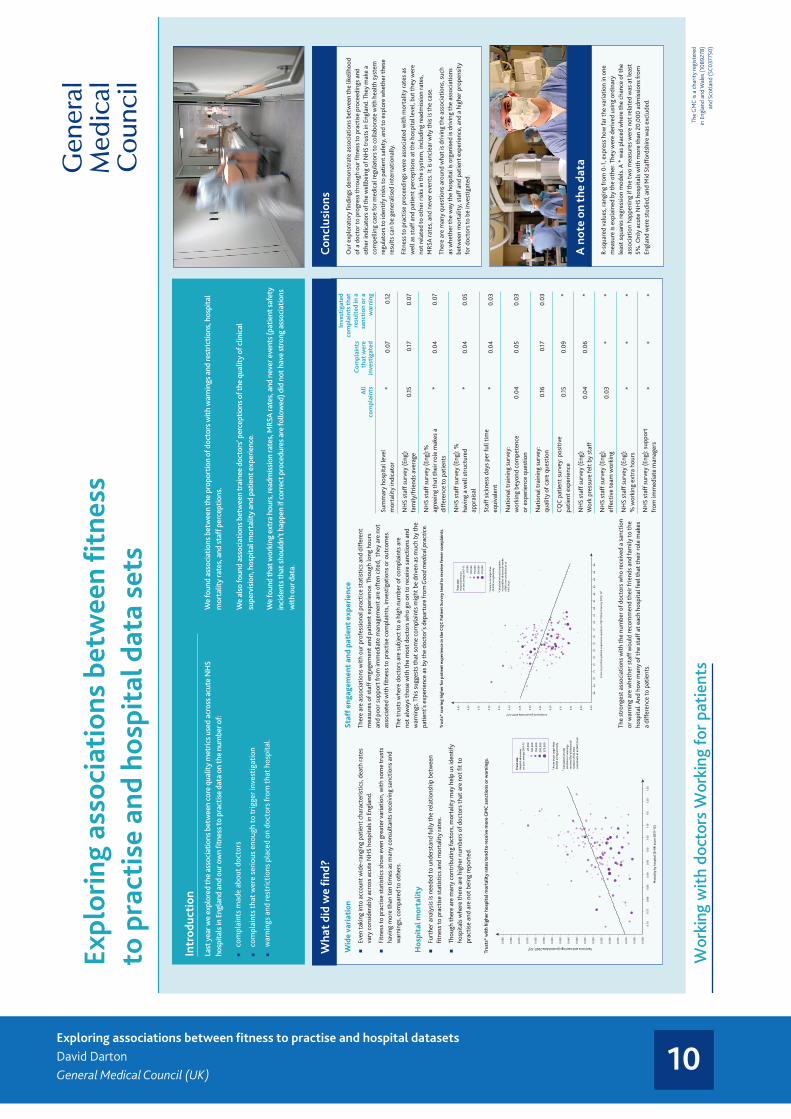
10Exploring associations between fitness to practise and hospital datasetsDavid DartonGeneral Medical Council (UK)
Expl
orin
g as
soci
atio
ns b
etw
een
fitne
ss
to p
ract
ise
and
hosp
ital
dat
a se
ts
The
GM
C is
a c
harit
y re
gist
ered
in
Eng
land
and
Wal
es (1
0892
78)
and
Scot
land
(SC0
3775
0)
Intr
oduc
tion
Last
yea
r we
expl
ored
the
asso
ciat
ions
bet
wee
n co
re q
ualit
y m
etric
s use
d ac
ross
acu
te N
HS
hosp
itals
in E
ngla
nd a
nd o
ur o
wn
fitne
ss to
pra
ctis
e da
ta o
n th
e nu
mbe
r of:
■■
com
plai
nts
mad
e ab
out d
octo
rs
■■
com
plai
nts t
hat w
ere
serio
us e
noug
h to
trig
ger i
nves
tigat
ion
■■
war
ning
s an
d re
stric
tions
pla
ced
on d
octo
rs fr
om th
at h
ospi
tal.
We
foun
d as
soci
atio
ns b
etw
een
the
prop
ortio
n of
doc
tors
with
war
ning
s and
rest
rictio
ns, h
ospi
tal
mor
talit
y ra
tes,
and
staf
f per
cept
ions
.
We
also
foun
d as
soci
atio
ns b
etw
een
trai
nee
doct
ors’
perc
eptio
ns o
f the
qua
lity
of c
linic
al
supe
rvis
ion,
hos
pita
l mor
talit
y an
d pa
tient
exp
erie
nce.
We
foun
d th
at w
orki
ng e
xtra
hou
rs, r
eadm
issi
on ra
tes,
MRS
A ra
tes,
and
nev
er e
vent
s (pa
tient
safe
ty
inci
dent
s tha
t sho
uldn
’t ha
ppen
if c
orre
ct p
roce
dure
s are
follo
wed
) did
not
hav
e st
rong
ass
ocia
tions
w
ith o
ur d
ata.
Wid
e va
riat
ion
■■
Even
taki
ng in
to a
ccou
nt w
ide-
rang
ing
patie
nt c
hara
cter
istic
s, d
eath
rate
s va
ry c
onsi
dera
bly
acro
ss a
cute
NH
S ho
spita
ls in
Eng
land
.
■■
Fitn
ess t
o pr
actis
e st
atis
tics
show
eve
n gr
eate
r var
iatio
n, w
ith s
ome
trus
ts
havi
ng m
ore
than
ten
times
as
man
y co
nsul
tant
s re
ceiv
ing
sanc
tions
and
w
arni
ngs,
com
pare
d to
oth
ers.
Hos
pita
l mor
talit
y■
■Fu
rthe
r ana
lysi
s is
nee
ded
to u
nder
stan
d fu
lly th
e re
latio
nshi
p be
twee
n fit
ness
to p
ract
ise
stat
istic
s an
d m
orta
lity
rate
s.
■■
Thou
gh th
ere
are
man
y co
ntrib
utin
g fa
ctor
s, m
orta
lity
may
hel
p us
iden
tify
hosp
itals
whe
re th
ere
are
high
er n
umbe
rs o
f doc
tors
that
are
not
fit t
o pr
actis
e an
d ar
e no
t bei
ng re
port
ed.
Staf
f eng
agem
ent
and
pati
ent
expe
rien
ceTh
ere
are
asso
ciat
ions
with
our
pro
fess
iona
l pra
ctic
e st
atis
tics
and
diff
eren
t m
easu
res o
f sta
ff e
ngag
emen
t and
pat
ient
exp
erie
nce.
Tho
ugh
long
hou
rs
and
poor
sup
port
from
imm
edia
te m
anag
emen
t are
oft
en c
ited,
the
y ar
e no
t as
soci
ated
with
fitn
ess t
o pr
actis
e co
mpl
aint
s, in
vest
igat
ions
or o
utco
mes
.
The
trus
ts w
here
doc
tors
are
sub
ject
to a
hig
h nu
mbe
r of c
ompl
aint
s ar
e no
t alw
ays t
hose
with
the
mos
t doc
tors
who
go
on to
rece
ive
sanc
tions
and
w
arni
ngs.
Thi
s su
gges
ts th
at s
ome
com
plai
nts
mig
ht b
e dr
iven
as
muc
h by
the
patie
nt’s
expe
rienc
e as
by
the
doct
or’s
depa
rtur
e fr
om G
ood
med
ical
pra
ctic
e.
The
stro
nges
t ass
ocia
tions
with
the
num
ber o
f doc
tors
who
rece
ived
a s
anct
ion
or w
arni
ng a
re w
heth
er s
taff
wou
ld re
com
men
d th
eir f
riend
s an
d fa
mily
to th
e ho
spita
l. A
nd h
ow m
any
of th
e st
aff a
t eac
h ho
spita
l fee
l tha
t the
ir ro
le m
akes
a
diff
eren
ce to
pat
ient
s.
Wha
t did
we
find?
0.06
5
0.06
0
0.05
5
0.05
0
0.04
5
0.04
0
0.03
5
0.03
0
0.02
5
0.02
0
0.01
5
0.01
0
0.00
5
0.00
0
0.07
0
0.07
5
0.08
0
0.08
5
0.70
0.75
0.80
0.85
0.90
0.95
1.00
1.05
1.10
1.15
1.20
1.25
Sanc
tion
s as
soci
ated
wit
h ho
spit
al m
orta
lity
Trus
ts*
with
hig
her h
ospi
tal m
orta
lity
rate
s ten
d to
rece
ive
prop
ortio
nally
mor
e G
MC
san
ctio
ns o
r war
ning
s
Sanctions and warnings (pooled data 2007–12)†
Mor
talit
y by
hos
pita
l (SH
MI s
core
201
1–12
)
† C
alcu
late
d as
tota
l
sanc
tions
or w
arni
ngs
re
ceiv
ed (f
or a
ll do
ctor
s)/
nu
mbe
r of f
ull-
time
co
nsul
tant
s at
an
NH
S tr
ust.
* A
cute
trus
ts la
rger
than
2
0,00
0 in
Eng
land
onl
y.
Trus
t si
zeH
ospi
tal a
dmis
sion
s pe
r yea
r, av
erag
e 20
07–1
2
20,0
0010
0,00
015
0,00
020
0,00
027
5,00
0
Trus
ts*
wit
h hi
gher
hos
pita
l mor
talit
y ra
tes
tend
to re
ceiv
e m
ore
GM
C s
anct
ions
or w
arni
ngs.
Our
exp
lora
tory
find
ings
dem
onst
rate
ass
ocia
tions
bet
wee
n th
e lik
elih
ood
of a
doc
tor t
o pr
ogre
ss th
roug
h ou
r fitn
ess t
o pr
actis
e pr
ocee
ding
s an
d ot
her i
ndic
ator
s of t
he w
ellb
eing
of N
HS
trus
ts in
Eng
land
. The
y m
ake
a co
mpe
lling
cas
e fo
r med
ical
regu
lato
rs to
col
labo
rate
with
hea
lth
syst
em
regu
lato
rs to
iden
tify
risks
to p
atie
nt s
afet
y, a
nd to
exp
lore
whe
ther
thes
e re
sult
s ca
n be
gen
eral
ised
inte
rnat
iona
lly.
Fitn
ess t
o pr
actis
e pr
ocee
ding
s w
ere
asso
ciat
ed w
ith m
orta
lity
rate
s as
w
ell a
s st
aff a
nd p
atie
nt p
erce
ptio
ns a
t the
hos
pita
l lev
el, b
ut th
ey w
ere
not r
elat
ed to
oth
er ri
sks
in th
e sy
stem
, inc
ludi
ng re
adm
issi
on ra
tes,
M
RSA
rate
s, a
nd n
ever
eve
nts.
It is
unc
lear
why
this
is th
e ca
se.
Ther
e ar
e m
any
ques
tions
aro
und
wha
t is d
rivin
g th
e as
soci
atio
ns, s
uch
as w
heth
er th
e w
ay th
e ho
spita
l is o
rgan
ised
is d
rivin
g th
e as
soci
atio
ns
betw
een
mor
talit
y, s
taff
and
pat
ient
exp
erie
nce,
and
a h
ighe
r pro
pens
ity
for d
octo
rs to
be
inve
stig
ated
.
Con
clus
ions
R-sq
uare
d va
lues
, ran
ging
from
0-1
, exp
ress
how
far t
he v
aria
tion
in o
ne
mea
sure
is e
xpla
ined
by
the
othe
r. Th
ey w
ere
deriv
ed u
sing
ord
inar
y le
ast s
quar
es re
gres
sion
mod
els.
A *
was
pla
ced
whe
re th
e ch
ance
of t
he
asso
ciat
ion
happ
enin
g if
the
two
mea
sure
s w
ere
not r
elat
ed w
as a
t lea
st
5%. O
nly
acut
e N
HS
hosp
itals
with
mor
e th
an 2
0,00
0 ad
mis
sion
s fro
m
Engl
and
wer
e st
udie
d, a
nd M
id S
taff
ords
hire
was
exc
lude
d.
A n
ote
on th
e da
ta
0.65
0.60
0.55
0.50
0.45
0.40
0.35
0.30
0.25
0.20
0.15
0.10
0.05
0.00
6869
7071
7273
7475
7677
7879
8081
8283
8485
86
Ass
ocia
tion
bet
wee
n ov
eral
l num
ber
of c
ompl
aint
s an
d pa
tien
t ex
peri
ence
Trus
ts*
scor
ing
high
er fo
r pat
ient
exp
erie
nce
in th
e C
QC
Pat
ient
Sur
vey
tend
to re
ceiv
e pr
opor
tiona
lly fe
wer
GM
C c
ompl
aint
s
Scor
e on
pos
itive
pat
ient
exp
erie
nce
ques
tion,
CQ
C P
atie
nt S
urve
y 20
12, %
†
Complaints (pooled data 2007–12)†
Trus
t si
zeH
ospi
tal a
dmis
sion
s pe
r yea
r, av
erag
e 20
07–1
2
20,0
0010
0,00
015
0,00
020
0,00
027
5,00
0
† C
alcu
late
d as
tota
l com
plai
nts
re
ceiv
ed (f
or a
ll do
ctor
s)/n
umbe
r
of fu
ll-tim
e co
nsul
tant
s at
an
N
HS
trus
t.
* A
cute
trus
ts la
rger
than
2
0,00
0 in
Eng
land
onl
y.
Trus
ts*
scor
ing
high
er fo
r pat
ient
exp
erie
nce
in th
e C
QC
Pat
ient
Sur
vey
tend
to re
ceiv
e fe
wer
com
plai
nts.
All
com
plai
nts
Com
plai
nts
that
wer
e in
vest
igat
ed
Inve
stig
ated
co
mpl
aint
s th
at
resu
lted
in a
sa
ncti
on o
r a
war
ning
Sum
mar
y ho
spita
l lev
el
mor
talit
y in
dica
tor
*0.
070.
12
NH
S st
aff s
urve
y (E
ng):
fa
mily
/frie
nds
aver
age
0.15
0.17
0.
07
NH
S st
aff s
urve
y (E
ng):%
ag
reei
ng th
at th
eir r
ole
mak
es a
di
ffer
ence
to p
atie
nts
*0.
040.
07
NH
S st
aff s
urve
y (E
ng):
%
havi
ng a
wel
l str
uctu
red
appr
aisa
l*
0.04
0.05
Staf
f sic
knes
s day
s pe
r ful
l tim
e eq
uiva
lent
*0.
040.
03
Nat
iona
l tra
inin
g su
rvey
: w
orki
ng b
eyon
d co
mpe
tenc
e
or e
xper
ienc
e qu
estio
n0.
040.
050.
03
Nat
iona
l tra
inin
g su
rvey
: qu
ality
of c
are
ques
tion
0.16
0.17
0.03
CQ
C p
atie
nt s
urve
y: p
ositi
ve
patie
nt e
xper
ienc
e0.
150.
09*
NH
S st
aff s
urve
y (E
ng):
W
ork
pres
sure
felt
by
staf
f0.
040.
06*
NH
S st
aff s
urve
y (E
ng):
ef
fect
ive
team
wor
king
0.03
**
NH
S st
aff s
urve
y (E
ng):
%
wor
king
ext
ra h
ours
**
*
NH
S st
aff s
urve
y (E
ng):
supp
ort
from
imm
edia
te m
anag
ers
**
*
11Bridging the gap: local support for medical regulation in the UKEmployer Liaison Service, Devolved Offices team, Regional Liaison ServiceGeneral Medical Council (UK)
As
wel
l as f
eedb
ack
on o
ur in
tern
al p
roce
sses
an
d ke
y fu
nctio
ns, t
he s
ervi
ce h
as a
lso
led
to
new
opp
ortu
nitie
s to
cont
ribut
e to
wid
er p
atie
nt
safe
ty d
ebat
es a
nd in
itiat
ives
acr
oss
heal
thca
re.
We
wor
k w
ith p
artn
er o
rgan
isat
ions
thro
ugh
activ
e pa
rtic
ipat
ion
in lo
cal a
nd re
gion
al fo
rum
s.
This
giv
es th
e he
alth
sys
tem
a s
hare
d vi
ew o
f ris
ks
to q
ualit
y th
roug
h sh
arin
g in
form
atio
n, e
arly
w
arni
ngs w
here
risk
s of p
oor q
ualit
y ar
e id
entifi
ed
and
cons
eque
nt o
ppor
tuni
ties t
o w
ork
toge
ther
to
driv
e im
prov
emen
t.
Our
Em
ploy
er L
iais
on S
ervi
ce le
ts u
s co
ntrib
ute
to th
e de
liver
y of
hig
h qu
ality
car
e an
d pa
tient
sa
fety
. Thi
s is
bec
ause
of c
lose
par
tner
ship
w
orki
ng, s
harin
g in
form
atio
n ap
prop
riate
ly, u
sing
th
e in
form
atio
n of
oth
ers t
o en
hanc
e ou
r ow
n un
ders
tand
ing
and,
on
occa
sion
, fol
low
ing
up o
n G
MC-
rela
ted
conc
erns
.
The
chal
leng
e in
brid
ging
the
gap
betw
een
loca
l de
liver
y an
d ov
ersi
ght i
s es
peci
ally
evi
dent
whe
n co
ncer
ns a
re ra
ised
abo
ut a
doc
tor a
nd th
eir fi
tnes
s to
pra
ctis
e is
inve
stig
ated
. In
2006
, fol
low
ing
a nu
mbe
r of h
igh
profi
le m
edic
al e
vent
s in
the
UK,
the
Chie
f Med
ical
Offi
cer r
ecom
men
ded
that
we
esta
blish
a
mec
hani
sm to
impr
ove
info
rmat
ion
shar
ing
betw
een
syst
ems o
f loc
al m
anag
emen
t and
nat
iona
l re
gula
tion.
The
wor
k th
at fo
llow
ed te
sted
and
refin
ed
an a
ppro
ach
that
wou
ld e
vent
ually
be
rolle
d ou
t ac
ross
the
UK
as th
e Em
ploy
er L
iais
on S
ervi
ce.
The
Empl
oyer
Lia
ison
Ser
vice
faci
litat
es c
lose
r w
orki
ng b
etw
een
ours
elve
s an
d he
alth
care
pr
ovid
ers,
pre
dom
inat
ely
arou
nd fi
tnes
s to
prac
tise
and
reva
lidat
ion.
Spe
cific
ally
, we
aim
to w
ork
with
he
alth
care
pro
vide
rs to
impr
ove
patie
nt s
afet
y an
d en
sure
hig
her s
tand
ards
of m
edic
al p
ract
ice.
W
e do
this
by:
■■
impr
ovin
g th
e un
ders
tand
ing
of o
ur fi
tnes
s to
prac
tise
proc
edur
es, i
nclu
ding
rais
ing
awar
enes
s
of p
atie
nt s
afet
y is
sues
and
our
thre
shol
ds
for r
efer
ral
■■
impr
ovin
g th
e qu
ality
of r
efer
rals
and
sup
port
ing
evid
ence
giv
en to
us
whe
n co
ncer
ns a
re ra
ised
ab
out a
doc
tor
■■
enco
urag
ing
thor
ough
loca
l inv
estig
atio
n,
perf
orm
ance
man
agem
ent a
nd c
linic
al
gove
rnan
ce in
the
hand
ling
of u
nder
perf
orm
ing
doct
ors,
in o
rder
to s
uppo
rt lo
w le
vel c
once
rns
to b
e re
solv
ed lo
cally
■■
prov
idin
g ad
vice
and
sup
port
on
reva
lidat
ion
■■
wor
king
with
oth
er a
genc
ies,
incl
udin
g sy
stem
s re
gula
tors
, on
qual
ity in
itiat
ives
to d
evel
op a
m
utua
l und
erst
andi
ng a
roun
d ke
y th
emes
and
em
ergi
ng tr
ends
in p
oor p
erfo
rman
ce.
The
succ
ess o
f the
Em
ploy
er L
iais
on S
ervi
ce g
oes
beyo
nd is
sues
aff
ectin
g th
e in
divi
dual
doc
tor.
Addi
tiona
l ben
efits
, bot
h op
erat
iona
l and
str
ateg
ic,
have
em
erge
d fr
om th
is m
odel
of p
roac
tivel
y w
orki
ng w
ith h
ealt
hcar
e pr
ovid
ers.
Our
dev
olve
d of
fices
mak
e su
re th
at w
e fu
lfil o
ur s
tatu
tory
role
as
a U
K-w
ide
regu
lato
r, an
d co
ntin
ue to
be
a re
leva
nt,
phys
ical
pre
senc
e in
Nor
ther
n Ire
land
, Sco
tlan
d an
d W
ales
. Tea
ms
are
base
d in
Bel
fast
, Edi
nbur
gh a
nd
Car
diff
and
pro
mot
e ou
r wor
k to
key
inte
rest
gro
ups
in e
ach
coun
try.
The
y w
ere
set u
p be
twee
n 20
03 a
nd 2
005
to
hel
p us
resp
ond
to p
oliti
cal d
evol
utio
n in
the
UK
– en
surin
g ou
r app
roac
h to
regu
latio
n re
mai
ns a
ppro
pria
te
in a
ll fo
ur c
ount
ries,
whi
ch in
crea
sing
ly h
ave
diff
eren
t hea
lth
polic
ies
and
stru
ctur
es.
The
offic
es p
rovi
de u
s w
ith u
p-to
-dat
e, re
leva
nt, i
ntel
ligen
ce a
nd g
uida
nce
on lo
cal s
ensi
tiviti
es, w
hich
hel
ps u
s
to s
hape
our
regu
lato
ry a
ctio
ns a
ppro
pria
tely
. The
offi
ces
also
incr
ease
the
awar
enes
s of t
he p
rofe
ssio
nal
stan
dard
s an
d gu
idan
ce w
e pr
oduc
e am
ong
the
prof
essi
on a
nd p
atie
nts
in e
ach
coun
try.
Key
inte
rest
gro
ups
get a
sin
gle
poin
t of l
ocal
con
tact
, com
mun
icat
ions
that
are
tailo
red
to th
eir n
eeds
, th
e ch
ance
to in
fluen
ce o
ur w
ork
and
an o
ppor
tuni
ty to
eng
age
with
on
us o
n lo
cal j
oint
wor
king
opp
ortu
nitie
s.
Brid
ging
the
gap:
loca
l sup
port
for m
edic
al re
gula
tion
in th
e U
K
The
GM
C is
a c
harit
y re
gist
ered
in
Eng
land
and
Wal
es (1
0892
78)
and
Scot
land
(SC0
3775
0)
GM
C li
aiso
n se
rvic
esO
ur li
aiso
n se
rvic
es c
over
the
four
cou
ntrie
s of t
he U
K. To
geth
er, t
hey
help
us i
mpr
ove
how
we
wor
k w
ith o
ur k
ey in
tere
st g
roup
s – in
par
ticul
ar p
atie
nts,
the
med
ical
pro
fess
ion,
med
ial e
duca
tors
and
he
alth
org
anis
atio
ns –
and
incr
ease
thei
r und
erst
andi
ng o
f our
wor
k an
d its
val
ue. T
he fe
edba
ck
we
rece
ive
thro
ugh
thes
e te
ams c
an a
lert
us t
o tr
ends
, goo
d pr
actic
e an
d co
ncer
ns re
latin
g to
pr
ofes
sion
al p
ract
ise
and
patie
nt sa
fety
. It c
an a
lso
help
us t
o sh
ape
our p
olic
y an
d pr
oces
ses t
o th
e ra
pidl
y ch
angi
ng a
nd c
ompl
ex w
orld
of h
ealt
hcar
e de
liver
y ac
ross
the
UK.
The
serv
ices
ena
ble
loca
l dec
isio
n m
akin
g an
d re
latio
nshi
p bu
ildin
g an
d ar
e pa
rt o
f our
com
mitm
ent
to b
eing
bot
h a
proa
ctiv
e, li
sten
ing
orga
nisa
tion
and
rele
vant
to th
e do
ctor
s and
env
ironm
ents
we
regu
late
– a
s wel
l as t
o th
e pa
tient
s in
who
se in
tere
st w
e re
gula
te.
Thes
e lo
cal s
ervi
ces a
lso
prov
ide
supp
ort a
nd in
sigh
t to
our o
ffice
-bas
ed c
olle
ague
s whi
ch c
an e
nabl
e us
to in
terv
ene
at a
n ea
rlier
stag
e –
befo
re p
anel
hea
rings
or s
erio
us sa
nctio
ns a
gain
st d
octo
rs o
r fo
rmal
regu
lato
ry a
ctio
n to
add
ress
con
cern
s abo
ut th
e tr
aini
ng o
f doc
tors
are
nee
ded.
See
bel
ow to
fin
d ou
t mor
e ab
out o
ur th
ree
loca
l lia
ison
serv
ices
.
Empl
oyer
Lia
ison
Ser
vice
Our
Reg
iona
l Lia
ison
Ser
vice
was
set
up
to g
ive
us g
reat
er u
nder
stan
ding
of
and
con
tact
with
loca
l int
eres
t gro
ups
with
in E
ngla
nd, b
uild
ing
on th
e su
cces
sful
mod
el o
f loc
al e
ngag
emen
t dev
elop
ed b
y ou
r dev
olve
d of
fices
. Th
e te
am o
f eig
ht re
gion
al li
aiso
n ad
vise
rs d
edic
ate
thei
r tim
e to
wor
king
w
ith g
roup
s of d
octo
rs, m
edic
al st
uden
ts, e
duca
tors
and
pat
ient
gro
ups t
o:
■■
prom
ote
the
GM
C, i
ncre
asin
g pa
rtne
rs u
nder
stan
ding
of o
ur w
ork
■■
prom
ote
and
expl
ain
the
ethi
cal s
tand
ards
and
gui
danc
e fo
r pr
ofes
sion
al p
ract
ise
we
prod
uce
■■
Impr
ove
the
GM
C’s
unde
rsta
ndin
g of
the
conc
erns
and
nee
ds o
f do
ctor
s, p
atie
nts
and
med
ical
stu
dent
s
■■
cons
ult o
n ch
ange
s to
GM
C p
olic
ies
and
proc
esse
s.
The
team
is re
mot
ely
base
d ac
ross
Eng
land
and
wor
ks c
lose
ly w
ith o
ur
Empl
oyer
Lia
ison
Ser
vice
col
leag
ues t
o pr
ovid
e ou
trea
ch s
ervi
ces t
o he
alth
care
Env
ironm
ents
in E
ngla
nd –
be
that
the
hosp
ital,
GP
surg
ery
or
educ
atio
n en
viro
nmen
ts.
The
team
has
rece
ived
str
ong
feed
back
from
doc
tors
and
med
ical
ed
ucat
ors t
hat s
ugge
sts o
ur e
xpla
natio
n of
sta
ndar
ds a
nd g
uida
nce
is
help
ing
them
to re
flect
on
thei
r pra
ctic
e an
d ch
ange
it w
hen
they
nee
d to
. Sin
ce it
s la
unch
in 2
013,
the
Regi
onal
Lia
ison
Ser
vice
has
met
with
ov
er 2
5,00
0 do
ctor
s, 1
5,00
0 m
edic
al s
tude
nts.
Mea
nwhi
le, w
e’ve
als
o w
orke
d di
rect
ly w
ith lo
cal p
atie
nt g
roup
s, to
exp
lain
the
role
of t
he G
MC
–
part
icul
arly
our
wor
k on
set
ting
stan
dard
s an
d ha
ndlin
g co
mpl
aint
s.
We’
ve s
pent
a lo
t of t
ime
expl
aini
ng re
valid
atio
n an
d re
flect
ive
prac
tice,
bu
t hav
e al
so b
een
able
to fa
cilit
ate
lear
ning
on
ethi
cal i
ssue
s su
ch a
s en
d of
life
car
e, u
se o
f soc
ial m
edia
, how
to ra
ise
conc
erns
as
wel
l as
core
to
pics
like
con
sent
, con
fiden
tialit
y an
d go
od m
edic
al p
ract
ice.
Regi
onal
Lia
ison
Ser
vice
Dev
olve
d na
tion
offi
ces
Wal
es
Nor
ther
nIre
land
East
of E
ngla
ndW
est M
idla
nds
East
Mid
land
s
Nor
th E
ast a
nd C
umbr
ia
Che
shire
and
N
orth
Sta
ffor
dshi
re
Lond
on
Sout
h Ea
st
York
shire
and
the
Hum
ber
Sout
h Ce
ntra
l
Sout
h W
est C
oast
Scot
land
Sout
h W
est
Nor
th W
est
3,97
7 Ad
-hoc
con
tact
s se
ekin
g
advi
ce a
nd s
uppo
rt.
847
Hea
lthc
are
orga
nisa
tions
lin
king
to th
e se
rvic
e.
3,53
3M
eetin
gs w
ith li
nked
or
gani
satio
ns.
18 Empl
oyer
liai
son
advi
sers
su
ppor
ted
by a
cen
tral
ised
11
str
ong
supp
ort t
eam
.
Rach
el W
ooda
llN
orth
Eas
t, C
umbr
ia, N
orth
and
Ea
st Y
orks
hire
and
Hul
l Em
ail:
RWoo
dall@
gmc-
uk.o
rg
Jo W
ren
East
of E
ngla
nd a
nd
Tham
es V
alle
y Em
ail:
JWre
n@gm
c-uk
.org
Tist
a C
hakr
avar
ty-G
anno
nN
orth
Wes
t, N
orth
Der
bysh
ire a
ndYo
rksh
ire (M
id, S
outh
and
Wes
t)
Emai
l: TC
Gan
non@
gmc-
uk.o
rg
Dar
ren
Mer
ciec
aTh
e M
idla
nds
Emai
l: D
Mer
ciec
a@gm
c-uk
.org
Sabi
na K
han
Sout
h W
est
Emai
l: SK
han4
@gm
c-uk
.org
How
ard
Lew
isSo
uth
East
coa
st
Emai
l: H
Lew
is2@
gmc-
uk.o
rg
Kim
Tol
ley
Sout
h Lo
ndon
Em
ail:
KTol
ley@
gmc-
uk.o
rg
Ian
McN
eill
Nor
th L
ondo
n Em
ail:
IMcn
eill@
gmc-
uk.o
rg
96%
of
doc
tors
sai
d w
orki
ng
with
the
Regi
onal
Lia
ison
Se
rvic
e to
und
erst
and
GM
C
stan
dard
s an
d gu
idan
ce
help
ed th
em to
refle
ct o
n th
eir p
ract
ices
.
77%
of
doc
tors
sai
d af
ter a
Re
gion
al L
iais
on S
ervi
ce
sess
ion
they
wou
ld c
hang
e th
eir p
ract
ice.
187
169
148
144
139
Reva
lidat
ion
Goo
d m
edic
alpr
actic
e
Soci
al m
edia
Rais
ing
conc
erns
The
stat
e of
med
ical
edu
catio
n a
nd p
ract
ice
in th
e U
K
Regi
onal
Lia
ison
Se
rvic
e se
ssio
n to
pics
in 2
013
Scot
land
Wal
es
Nor
ther
n Ir
elan
d
Dev
olve
d na
tion
offi
ces:
key
inte
rest
gro
ups w
e w
ork
with
Gov
ernm
ent
Doc
tors
Patie
nts
and
the
publ
ic
Med
ical
stu
dent
s
Hea
lthc
are
regu
lato
rsOm
buds
men
Med
ical
edu
cato
rsan
d tr
aine
rsParli
amen
ts/
Asse
mbl
ies
Syst
emre
gula
tors

12Making sure all doctors have the necessary knowledge of English to practise safely in the UKJo Nicholas, Sara Kovach ClarkeGeneral Medical Council (UK)
Mak
ing
sure
all
doct
ors
have
the
nece
ssar
y kn
owle
dge
of
Eng
lish
to p
ract
ise
safe
ly in
the
UK
The
GM
C is
a c
harit
y re
gist
ered
in
Eng
land
and
Wal
es (1
0892
78)
and
Scot
land
(SC0
3775
0)
Voi
cing
our
con
cern
sIn
201
0 w
e be
gan
voic
ing
our c
once
rns
that
Eur
opea
n do
ctor
s w
ere
allo
wed
to re
gist
er w
ith
a lic
ence
to p
ract
ise
med
icin
e in
the
UK
wit
hout
bei
ng a
sked
for e
vide
nce
of th
eir E
nglis
h la
ngua
ge k
now
ledg
e. T
his
has
been
a lo
ng-s
tand
ing
requ
irem
ent f
or d
octo
rs tr
aine
d ou
tsid
e th
e Eu
rope
an U
nion
.
In 2
013
the
UK
Gov
ernm
ent c
onsu
lted
on
new
pow
ers
for t
he G
MC
. Thi
s ye
ar w
e im
plem
ente
d th
ese
legi
slat
ive
chan
ges
acro
ss th
e or
gani
sati
on to
mak
e su
re th
at a
ll do
ctor
s ha
ve th
e ne
cess
ary
know
ledg
e of
Eng
lish
to p
ract
ise
safe
ly in
the
UK.
‘Thi
s is a
n im
port
ant m
ilest
one
in cr
eatin
g be
tter
, saf
er ca
re fo
r pat
ient
s. E
very
one
has a
rig
ht to
exp
ect t
o be
trea
ted
by d
octo
rs w
ho ca
n co
mm
unic
ate
effe
ctiv
ely
in E
nglis
h an
d th
is w
ill h
elp
us a
chie
ve th
is. E
urop
ean
law
doe
s not
yet
allo
w u
s to
chec
k ev
ery d
octo
r but
th
at re
form
will
com
e and
this
is a v
ital fi
rst s
tep.
’
Nia
ll D
icks
on, C
hief
Exe
cutiv
e of
the
GM
C
‘For
the
first
tim
e ev
er, w
e ha
ve a
full
syst
em o
f che
cks i
n pl
ace t
o pr
even
t doc
tors
wor
king
in
the
NH
S w
ho d
o no
t hav
e the
nec
essa
ry k
now
ledg
e of E
nglis
h fr
om tr
eatin
g pa
tient
s.
This
is a
huge
step
forw
ard
for p
atie
nt sa
fety
. I a
m p
leas
ed to
hav
e pl
ayed
my
part
in
mak
ing
this
happ
en.’
D
r Dan
Pou
lter
, Hea
lth
Min
iste
r
Top
five
Euro
pean
cou
ntri
es o
f med
ical
qu
alifi
cati
on fo
r doc
tors
regi
ster
ed
wit
h th
e G
MC
Irel
and
4,03
8G
erm
any
3,24
3G
reec
e3,
290
Ital
y3,
239
Rom
ania
2,25
6
The
know
ledg
e of
Eng
lish
to p
ract
ise
safe
ly in
the
UK
Seek
ing
evid
ence
that
a E
urop
ean
doct
or is
abl
e to
co
mm
unic
ate
in E
nglis
h be
fore
gra
ntin
g a
licen
cePr
evio
usly
, if E
urop
ean
doct
ors
had
a re
cogn
ised
med
ical
qua
lifica
tion
from
a
med
ical
sch
ool b
ased
in a
mem
ber s
tate
of t
he E
urop
ean
Econ
omic
Are
a or
Sw
itzer
land
, we
wer
e re
quire
d by
law
to g
rant
regi
stra
tion
and
a lic
ence
to
prac
tise.
We
wer
en’t
allo
wed
to d
o an
y fu
rthe
r ass
essm
ent o
r tes
ting,
or a
sk
thes
e do
ctor
s for
any
evi
denc
e of
thei
r lan
guag
e sk
ills.
This
cha
nge
mea
ns th
at:
■■
we
can
ask
for e
vide
nce
of a
Eur
opea
n do
ctor
’s ab
ility
to c
omm
unic
ate
in
Engl
ish
if co
ncer
ns a
bout
this
em
erge
dur
ing
the
regi
stra
tion
proc
ess
■■
we
will
refu
se to
gra
nt a
lice
nce
if a
doct
or is
una
ble
to d
emon
stra
te th
at
they
hav
e th
e ne
cess
ary
know
ledg
e of
Eng
lish
■■
we
will
reco
gnis
e th
eir q
ualifi
catio
ns b
y co
ntin
uing
to g
rant
regi
stra
tion.
Our
evi
denc
e re
quire
men
tsW
e w
ill c
onsi
der e
vide
nce
of k
now
ledg
e of
Eng
lish
only
if it
:
■■
is re
cent
(les
s tha
n tw
o ye
ars o
ld a
t the
poi
nt o
f app
licat
ion)
■■
clea
rly s
how
s the
doc
tor c
an re
ad, w
rite
and
inte
ract
with
pat
ient
s,
rela
tives
and
hea
lthc
are
prof
essi
onal
s in
Eng
lish
■■
can
be v
erifi
ed b
y us
thro
ugh
cont
act w
ith re
cogn
ised
med
ical
inst
itutio
ns,
regu
lato
rs o
r oth
er o
ffici
al b
odie
s.
We
rout
inel
y ac
cept
:
■■
a va
lid In
tern
atio
nal E
nglis
h La
ngua
ge T
estin
g Sy
stem
cer
tifica
te th
at m
eets
ou
r crit
eria
■■
a le
tter
or c
ertifi
cate
from
the
inst
itutio
n w
here
the
doct
or q
ualifi
ed th
at
confi
rms
all o
f the
cou
rse,
incl
udin
g cl
inic
al a
ctiv
ities
, wer
e ta
ught
and
ex
amin
ed s
olel
y in
Eng
lish,
and
at l
east
75%
of a
ny c
linic
al in
tera
ctio
n w
as
cond
ucte
d in
Eng
lish
(if th
e pr
imar
y m
edic
al q
ualifi
catio
n is
mor
e th
an tw
o ye
ars o
ld a
t the
poi
nt o
f app
licat
ion
we
also
nee
d em
ploy
er re
fere
nces
).
Dea
ling
wit
h co
ncer
ns a
bout
a d
octo
r’s
know
ledg
e of
Eng
lish
Prev
ious
ly, s
erio
us c
ompl
aint
s ab
out a
doc
tor’s
com
mun
icat
ion
skill
s, in
clud
ing
know
ledg
e of
Eng
lish,
hav
e be
en c
ateg
oris
ed a
s pe
rfor
man
ce c
once
rns.
This
cha
nge
mea
ns th
at:
■■
whe
re a
doc
tor’s
inab
ility
to s
peak
, writ
e, re
ad o
r und
erst
and
Engl
ish
mea
ns
they
are
una
ble
to tr
eat p
atie
nts
safe
ly, w
e ca
n cl
early
sta
te th
is a
s the
re
ason
thei
r fitn
ess t
o pr
actis
e is
impa
ired
■■
as p
art o
f the
info
rmat
ion
gath
erin
g pr
oces
s, th
e re
gist
rar a
nd p
anel
s w
ill
have
a n
ew p
ower
to re
quire
doc
tors
to u
nder
go a
lang
uage
ass
essm
ent i
f w
e ne
ed e
vide
nce
of th
eir l
angu
age
skill
s for
us t
o m
ake
a de
cisi
on a
bout
th
eir fi
tnes
s to
prac
tise
med
icin
e in
the
UK
■■
if a
doct
or’s
lang
uage
ski
lls d
o no
t im
prov
e su
ffici
entl
y or
they
are
unw
illin
g to
agr
ee th
e ne
cess
ary
actio
n, th
e ca
se m
ay b
e re
ferr
ed to
a fi
tnes
s to
prac
tise
pane
l to
cons
ider
if a
ctio
n is
nec
essa
ry to
pro
tect
the
publ
ic.
In s
uch
case
s, in
defin
ite s
uspe
nsio
n w
ould
be
the
mos
t ser
ious
out
com
e av
aila
ble
to u
s in
dea
ling
with
con
cern
s ab
out a
doc
tor t
hat r
elat
e so
lely
to
thei
r kno
wle
dge
of E
nglis
h.
Resp
onsi
bilit
ies
of h
ealt
hcar
e or
gani
sati
ons
and
resp
onsi
ble
offic
ers
Hea
lthc
are
orga
nisa
tions
hav
e al
way
s ha
d re
spon
sibi
litie
s to
mak
e su
re th
at
the
doct
ors
who
wor
k fo
r the
m a
re c
ompe
tent
for t
heir
role
. Thi
s in
clud
es
bein
g as
sure
d of
a d
octo
r’s E
nglis
h la
ngua
ge a
bilit
y.
In A
pril
2013
thes
e re
spon
sibi
litie
s w
ere
mad
e ex
plic
it in
legi
slat
ion
for
resp
onsi
ble
offic
ers
base
d in
Eng
land
. Loc
al a
rran
gem
ents
are
als
o in
pla
ce in
N
orth
ern
Irela
nd, S
cotl
and
and
Wal
es.
Thes
e re
spon
sibi
litie
s w
ill c
ontin
ue to
exi
st in
futu
re, b
ut w
ill b
e st
reng
then
ed
by o
ur a
bilit
y to
ask
for e
vide
nce
of E
urop
ean
doct
ors’
Eng
lish
lang
uage
abi
lity
whe
n co
ncer
ns a
rise
durin
g ou
r reg
istr
atio
n pr
oces
s.
Key
chan
ges
we
intr
oduc
ed
in s
umm
er 2
014
■■
We
intr
oduc
ed a
refe
renc
e to
Eng
lish
know
ledg
e in
our
cor
e gu
idan
ce
Goo
d m
edic
al p
ract
ice.
■■
We
incr
ease
d th
e m
inim
um s
core
acc
epte
d on
a re
cogn
ised
aca
dem
ic
Engl
ish
lang
uage
test
.
■■
We
chan
ged
the
law
so
that
we
can
refu
se to
gra
nt a
lice
nce
to
any
doct
or u
nabl
e to
dem
onst
rate
that
they
hav
e th
e ne
cess
ary
know
ledg
e of
Eng
lish.
■■
We
esta
blis
hed
a ne
w g
roun
d of
‘im
pairm
ent’
whe
re th
ere
are
issu
es
with
a d
octo
r’s a
bilit
y to
spe
ak, r
ead,
writ
e or
und
erst
and
Engl
ish,
and
in
trod
uced
Eng
lish
lang
uage
ass
essm
ents
into
our
inve
stig
atio
ns o
f th
ese
conc
erns
.
Impl
emen
tati
on tr
ends
2013
2014
MAY JUNE
710
897
981
1,41
5
We
rece
ived
an
incr
ease
in a
pplic
atio
ns fo
r reg
istr
atio
n w
ith a
lice
nce
to p
ract
ise
from
Eur
opea
n do
ctor
s in
the
two
mon
ths
befo
re o
ur
chan
ges w
ere
impl
emen
ted.

13Engaging patients during a fitness to practise investigationRachel Procter (author), Patient Meetings Pilot team: Rachel Procter and Cristina Diaz (Patient Information Officers), Lyndsey Dodd and Eleanor Davy (project team), Anna Rowland (project sponsor), General Medical Council (UK)
Enga
ging
pat
ient
s du
ring
a fi
tnes
s to
pra
ctis
e in
vest
igat
ion
The
GM
C is
a c
harit
y re
gist
ered
in
Eng
land
and
Wal
es (1
0892
78)
and
Scot
land
(SC0
3775
0)
Back
grou
ndW
e la
unch
ed o
ur P
atie
nt In
form
atio
n Se
rvic
e pi
lot i
n 20
12 w
ith th
e ai
m o
f pro
vidi
ng im
prov
ed
com
mun
icat
ion
wit
h pa
tien
ts, t
heir
rela
tive
s or
oth
er m
embe
rs o
f the
pub
lic w
ho h
ave
rais
ed a
co
mpl
aint
abo
ut a
doc
tor’s
fitn
ess
to p
ract
ise
med
icin
e.
Aim
The
obje
ctiv
e of
the
pilo
t was
to fa
cilit
ate
com
mun
icat
ion
wit
h pa
tien
ts to
impr
ove
our
unde
rsta
ndin
g of
con
cern
s an
d th
eir u
nder
stan
ding
of t
he in
vest
igat
ion
proc
ess.
Pilo
t tar
get
The
pilo
t was
des
igne
d to
invo
lve
100
face
-to-
face
mee
ting
s w
ith
pati
ents
, to
prov
ide
suffi
cien
t dat
a fo
r mea
ning
ful e
valu
atio
n. T
his
targ
et w
as re
ache
d in
Mar
ch 2
014
and
a de
cisi
on w
as m
ade
to c
onti
nue
hold
ing
mee
ting
s un
til t
he fi
nal r
epor
t fro
m th
e in
depe
nden
t ev
alua
tors
was
rece
ived
in Ju
ly 2
014.
Loca
tion
We
have
offi
ces
in b
oth
Man
ches
ter a
nd L
ondo
n w
ith
a Pa
tien
t Inf
orm
atio
n O
ffice
r bas
ed in
ea
ch o
ffice
. Pat
ient
s w
ho li
ve in
the
Nor
th W
est a
nd G
reat
er L
ondo
n re
gion
s of
the
UK
wer
e in
vite
d to
par
tici
pate
in th
e pi
lot.
A te
leph
one
mee
ting
was
off
ered
to th
ose
unab
le to
trav
el to
th
e of
fices
Two
type
s of m
eetin
g ar
e of
fere
d:
■■
an in
itial
sta
ge m
eetin
g he
ld s
oon
afte
r the
inve
stig
atio
n ha
s ope
ned,
and
■■
an e
nd s
tage
mee
ting
held
follo
win
g th
e co
nclu
sion
of t
he in
vest
igat
ion
or a
fter
a p
anel
hea
ring
has t
aken
pla
ce.
The
mee
tings
are
an
oppo
rtun
ity to
:
■■
ensu
re th
at w
e ha
ve fu
lly u
nder
stoo
d th
e m
atte
r the
per
son
is c
ompl
aini
ng a
bout
■■
impr
ove
the
publ
ic’s
unde
rsta
ndin
g of
our
role
and
func
tion
■■
expl
ain
our p
roce
sses
of i
nves
tigat
ion
and
wha
t the
y ca
n ex
pect
■■
expl
ain
the
poss
ible
out
com
es th
at w
e ca
n re
ach
at th
e en
d of
our
inve
stig
atio
n
■■
prov
ide
info
rmat
ion
abou
t oth
er o
rgan
isat
ions
that
may
be
able
to a
ssis
t.
The
mee
ting
s
AS
OF
JUN
E 20
14 W
E H
AVE
HEL
D:
Init
ial s
tage
mee
ting
s
167
92
in
per
son
via
phon
e
End
stag
e m
eeti
ngs
64
35
in p
erso
n
via
ph
one
■■
Arr
angi
ng, f
acili
tatin
g an
d
cond
uctin
g th
e m
eetin
gs.
■■
Liai
sing
with
Inve
stig
atio
n st
aff
befo
re a
nd a
fter
the
mee
tings
.
■■
Writ
ing
to th
e pa
tient
aft
er th
e m
eetin
g
to e
nsur
e th
ey k
now
wha
t to
expe
ct.
■■
Ans
wer
ing
inte
rnal
and
ext
erna
l qu
erie
s ab
out t
he m
eetin
gs.
Role
of t
he P
atie
nt In
form
atio
n O
ffice
r
The
eval
uatio
n re
port
sho
ws t
hat t
he v
ast m
ajor
ity o
f fee
dbac
k in
rela
tion
to p
atie
nt m
eetin
gs is
pos
itive
.
■■
Com
plai
nant
s w
ere
posi
tive
abou
t the
opp
ortu
nity
to m
eet w
ith u
s.
■■
It is
cle
ar fr
om c
omm
ents
rece
ived
that
the
mee
tings
bui
ld ra
ppor
t with
com
plai
nant
s an
d re
duce
th
eir f
eelin
g of
isol
atio
n. T
he m
eetin
gs h
elp
com
plai
nant
s to
unde
rsta
nd o
ur ro
le a
nd p
urpo
se
and
our i
nves
tigat
ion
proc
ess.
■■
Som
e co
mpl
aina
nts
rais
ed c
once
rns
abou
t the
end
sta
ge m
eetin
gs th
at s
eem
s to
aris
e la
rgel
y fr
om
thei
r unh
appi
ness
with
our
dec
isio
n on
the
case
, rat
her t
han
from
the
mee
tings
them
selv
es,
alth
ough
we
are
look
ing
at w
ays t
o im
prov
e th
is p
art o
f the
pro
cess
.
Feed
back
from
the
inde
pend
ent
eval
uati
on
Ass
ess
case
Doc
tors
disc
losu
re
Ope
n in
vest
igat
ion
Seek
co
nsen
t fr
om c
ompl
aina
nt
to d
iscl
ose
Init
ial s
tage
Pati
ent
mee
ting
invi
tati
on s
ent
Colle
ctio
n of
info
rmat
ion
Empl
oyer
disc
losu
re
Dec
isio
nEn
d st
age
Pati
ent
mee
ting
invi
tati
on s
ent

14Continuously improving our regulatory functions and operations: the journey so farRegistration and Revalidation business improvement team, Resources and Quality Assurance finance improvement team, Fitness to Practise Lean review team, Communications team, General Medical Council (UK)
Con
tinu
ousl
y im
prov
ing
our r
egul
ator
y fu
ncti
ons
and
oper
atio
ns: t
he jo
urne
y so
far
The
GM
C is
a c
harit
y re
gist
ered
in
Eng
land
and
Wal
es (1
0892
78)
and
Scot
land
(SC0
3775
0)
Find
ing
way
s to
impr
ove
our w
ork
As
an o
rgan
isat
ion,
we
cons
tant
ly n
eed
to c
hang
e. C
ontin
uous
im
prov
emen
t is
abou
t sup
port
ing
our s
taff
to d
eliv
er a
bet
ter
and
mor
e ef
ficie
nt s
ervi
ce fo
r pat
ient
s, d
octo
rs a
nd o
ther
s w
ho re
ly o
n us
and
the
wor
k w
e do
.
We
intr
oduc
ed o
ur c
ontin
uous
impr
ovem
ent p
rogr
amm
e in
200
4 fo
llow
ing
the
Ship
man
and
Nea
l pub
lic e
nqui
ries,
w
hen
we
face
d in
crea
sed
scru
tiny
abou
t our
role
in p
rote
ctin
g pa
tient
s. T
he a
im w
as to
con
stan
tly
ques
tion
our p
roce
sses
an
d to
find
way
s to
impr
ove
them
.
Why
do
we
need
con
tinu
ous
impr
ovem
ent
in th
e G
MC
?■
■W
e ow
e it
to th
e pu
blic
to d
o th
e be
st jo
b w
e ca
n.
■■
We
owe
it to
doc
tors
to u
se th
eir f
ees
effic
ient
ly a
nd
effe
ctiv
ely.
■■
We
wan
t to
do m
ore
with
wha
t we’
ve g
ot (o
r with
less
).
■■
We
need
to k
eep
up w
ith d
eman
d fo
r our
ser
vice
s.
Our
app
roac
h to
con
tinu
ous
impr
ovem
ent
■■
Our
impr
ovem
ent t
eam
s w
ork
acro
ss te
ams
and
dire
ctor
ates
, with
sup
port
from
sen
ior m
anag
emen
t.
■■
We’
ve in
trod
uced
a s
ugge
stio
n sc
hem
e so
that
any
one
can
high
light
impr
ovem
ent o
ppor
tuni
ties.
■■
We’
re tr
aini
ng, c
oach
ing
and
men
torin
g st
aff m
embe
rs.
Con
tinu
ous
impr
ovem
ent t
imel
ine
■■
Incr
ease
d sc
rutin
y an
d pr
essu
re o
n th
e G
MC
to
impr
ove
perf
orm
ance
fo
llow
ing
publ
ic e
nqui
ries
(Shi
pman
, Nea
l).
■■
Lim
ited
qual
ity a
ssur
ance
.
■■
Ove
r-re
liant
on
pape
r.
2004
2005 ■
■Fi
tnes
s to
Prac
tise
and
Regi
stra
tion
dire
ctor
ates
in
trod
uce
Qua
lity
Ass
uran
ce
and
Proj
ect M
anag
emen
t te
ams.
■■
Cha
nge
Man
agem
ent a
nd
Busi
ness
Impr
ovem
ent
team
s se
t up.
2006
■■
We
adop
t Lea
n/Si
x Si
gma/
Tota
l Qua
lity
Man
agem
ent a
ppro
ach
to c
ontin
uous
im
prov
emen
t.
■■
Dire
ctor
of R
esou
rces
com
mis
sion
s a
five
day
cour
se to
trai
n a
grou
p of
sta
ff in
co
ntin
uous
impr
ovem
ent.
2007
2008
2009
2010
2011
2012
2013
■■
Regi
stra
tion
and
Reso
urce
s la
unch
its
dire
ctor
ate-
wid
e pr
ogra
mm
e an
d ro
ll ou
t a b
espo
ke c
ours
e to
trai
n st
aff i
n co
ntin
uous
im
prov
emen
t.
■■
Ove
r 250
sta
ff h
ave
rece
ived
ba
sic
trai
ning
and
ove
r 50
proj
ect
lead
ers
have
bee
n tr
aine
d.
■■
Focu
s on
the
cust
omer
, aut
omat
ion
and
impr
ovin
g ou
r onl
ine
capa
bilit
y.
■■
Impl
emen
t a n
umbe
r of c
ontin
uous
impr
ovem
ent p
roje
cts,
del
iver
ing
in
exce
ss o
f £10
0,00
0 sa
ving
s.
■■
Com
plet
e m
erge
r with
the
Post
grad
uate
Med
ical
Edu
catio
n Tr
aini
ng B
oard
.
■■
Intr
oduc
e th
e lic
ence
to p
ract
ise.
■■
Fitn
ess t
o Pr
actis
e di
rect
orat
e la
unch
es th
eir d
irect
orat
e-w
ide
impr
ovem
ent p
rogr
amm
e an
d a
loca
l con
tinuo
us im
prov
emen
t fr
amew
ork
– st
artin
g w
ith a
n ov
eral
l re
view
of t
he fi
tnes
s to
prac
tise
proc
ess.
■■
Five
pro
ject
s ha
ve b
een
com
plet
ed
so fa
r, w
ith a
roun
d £1
00,0
00-w
orth
of
sta
ff ti
me
save
d.
■■
Regi
stra
tion
and
Reva
lidat
ion
dire
ctor
ate
star
t a s
ervi
ce re
view
pr
ogra
mm
e to
pro
vide
ass
uran
ce
that
team
s ar
e do
ing
the
right
th
ings
, for
the
right
reas
ons
and
then
add
ress
the
gaps
.
■■
Impr
ovem
ent a
ppro
ache
s co
ntin
ue to
dev
elop
acr
oss
th
e or
gani
satio
n.
2014
■■
We’
ll re
bran
d ou
r sug
gest
ion
sche
me
to T
ell u
s you
r pro
blem
–
to h
elp
us to
get
at r
oot c
ause
s.
■■
We’
ll lo
ok a
t get
ting
accr
edita
tion
agai
nst a
n in
tern
atio
nal
qual
ity s
tand
ard.
■■
We’
ll co
ntin
ue to
roll
out t
he p
rogr
amm
e ac
ross
the
orga
nisa
tion.
So
me
lead
ing
orga
nisa
tions
in th
is fi
eld
have
bee
n on
thei
r co
ntin
uous
impr
ovem
ent j
ourn
ey fo
r ove
r 40
year
s. W
e ha
ve a
way
to
go!
Whe
re n
ext?
Staf
f mem
bers
on
the
first
Con
tinuo
us Im
prov
emen
t Pro
ject
Lea
ders
cou
rse,
Nov
embe
r 200
8.
Loca
l pro
cess
impr
ovem
ents
to in
crea
se o
ur e
ffici
ency
an
d im
prov
e th
e qu
alit
y of
our
ser
vice
s.
For e
xam
ple,
rede
sign
ing
our d
irect
deb
it fo
rm u
sed
by
doct
ors t
o pa
y th
eir a
nnua
l ret
entio
n fe
e, h
ad th
e
follo
win
g im
pact
.
■■
We
relo
cate
d ou
r adj
udic
atio
n an
d ce
rtifi
catio
n fu
nctio
ns fr
om L
ondo
n to
Man
ches
ter.
■■
We
cut t
he a
nnua
l ret
entio
n fe
e fr
om £
420
in M
arch
20
12 to
£39
0 no
w.
■■
We’
ve c
ut d
own
the
amou
nt o
f pap
er w
e us
e by
usi
ng
mor
e el
ectr
onic
com
mun
icat
ion
met
hods
.
■■
We’
ve b
ecom
e be
tter
at u
sing
tech
nolo
gy –
for e
xam
ple,
by
dig
itally
reco
rdin
g he
arin
gs.
■■
We’
ve in
trod
uced
vis
ual m
anag
emen
t to
keep
sta
ff
info
rmed
– fo
r exa
mpl
e by
sho
win
g th
e nu
mbe
r of
cur
rent
fitn
ess t
o pr
actis
e he
arin
gs o
n a
digi
tal
dash
boar
d.
■■
We’
ve m
ade
£17.6
mill
ion
of e
ffici
ency
sav
ings
.
■■
We’
ve w
orke
d to
sim
plify
and
sta
ndar
dise
our
pr
oced
ures
.■
■W
e in
trod
uced
flow
cha
rts t
o gi
ve s
taff
acr
oss t
eam
s a
bett
er u
nder
stan
ding
of o
ur p
roce
sses
. The
exa
mpl
e be
low
sho
ws o
ur p
roce
ss fo
r rev
iew
ing
fitne
ss to
pr
actis
e re
stric
tions
.
Som
e ex
ampl
es o
f our
con
tinu
ous
impr
ovem
ent
proj
ects
July
200
5 Ju
ly 2
006
2418
20%
3117
41%
Aug
ust 2
005
Aug
ust 2
006
Rest
rictio
ns
impo
sed
by a
pa
nel o
f cas
e ex
amin
er
Cas
e tr
ansf
erre
d to
C
ase
Revi
ew
Team
Cas
e Re
view
Tea
m
mon
itor d
octo
r’s
com
plia
nce
with
re
stric
tions
Revi
ew h
earin
g/
case
exa
min
er
revi
ew
Prep
are
for r
evie
w
hear
ing
proc
ess
Rest
rictio
ns
lifte
d?
Doc
tor r
etur
ns
to u
nres
tric
ted
prac
tice
Doc
tor
rem
ains
und
er
rest
rictio
ns
YES
NO
Adve
rse
info
rmat
ion
rece
ived
? Ad
vers
e in
fo p
roce
ss
Num
ber a
nd p
erce
ntag
e of
fees
ca
lls to
our
Con
tact
Cen
tre
Dire
ctor
of R
esou
rces
and
Qua
lity
Assu
ranc
e, N
eil R
ober
ts, a
war
ds a
mem
ber o
f sta
ff h
is co
mpl
etio
n ce
rtifi
cate
at a
rece
nt
Cont
inuo
us Im
prov
emen
t Pro
ject
Lea
ders
cou
rse.

15Welcome to UK practice: an introduction to the guidance and support we give to doctors new to the medical register
Kim Tolley, Sunil Kapur, Ian McNeill, Mary Morgan-Hyland, Nico Kirkpatrick, Maria Walsh and Gareth Williams General Medical Council (UK)
Wel
com
e to
UK
pra
ctic
e: a
n in
trod
ucti
on to
the
guid
ance
an
d su
ppor
t we
give
to d
octo
rs n
ew to
the
med
ical
regi
ster
The
GM
C is
a c
harit
y re
gist
ered
in
Eng
land
and
Wal
es (1
0892
78)
and
Scot
land
(SC0
3775
0)
Why
is th
e pr
ogra
mm
e ne
eded
?W
e de
velo
ped
the
Wel
com
e to
UK
prac
tice
prog
ram
me
in
resp
onse
to o
ur re
port
The
stat
e of m
edic
al e
duca
tion
and
prac
tice
in th
e UK
201
1 . I
t fou
nd:
‘A va
riatio
n in
the
stan
dard
s of m
edic
al p
ract
ice d
ispla
yed
by
doct
ors n
ew th
e pr
actic
e in
the U
K. R
esea
rch
unde
rtak
en o
n be
half
of th
e GM
C an
d ev
iden
ce g
athe
red
also
sugg
ests
varia
tion
in th
e ap
plic
atio
n of
lega
l, et
hica
l and
pro
fess
iona
l sta
ndar
ds as
set o
ut
in G
ood
med
ical
pra
ctic
e. Th
ese
stan
dard
s inc
lude
, but
are
not l
imite
d to
com
mun
icat
ion,
team
wor
k and
und
erst
andi
ng
prof
essio
nal r
elat
ions
hips
’.
A re
cent
stud
y by
Bha
t, Aj
az a
nd Z
aman
(201
4) su
ppor
ts th
ese
conc
erns
. It
says
that
doc
tors
in tr
aini
ng re
port
ed th
at:
‘Indu
ctio
ns co
nduc
ted
at th
eir i
ndiv
idua
l tru
sts w
ere g
ener
ic an
d no
t tai
lore
d to
supp
ort t
heir
part
icul
ar n
eeds
, and
ther
e was
an
expe
ctat
ion
that
doc
tors
wer
e alre
ady
fam
iliar
with
the o
vera
ll he
alth
care
syst
em in
the U
nite
d Ki
ngdo
m an
d ho
w th
e diff
eren
t se
rvic
es w
ere
inte
grat
ed’.
Stag
es o
f dev
elop
men
t of t
he W
elco
me
to U
K p
ract
ice
prog
ram
me
Earl
y 20
12
Surv
ey s
ent t
o 78
or
gani
satio
ns fo
r the
ir vi
ews o
n in
duct
ion.
Late
201
2
Iden
tified
ten
them
es fr
om th
e su
rvey
.
■■
Rais
ing
conc
erns
.
■■
Team
rela
tions
hips
.
■■
Prof
essi
onal
exp
ecta
tions
and
pre
ssur
es.
■■
Und
erst
andi
ng th
e w
ider
hea
lth
syst
em.
■■
Ong
oing
lear
ning
and
mai
ntai
ning
pr
ofes
sion
al p
erfo
rman
ce.
■■
App
lyin
g kn
owle
dge
and
expe
rienc
e to
pr
actic
ing
as a
doc
tor i
n th
e U
K.
■■
Ensu
ring
equa
l acc
ess t
o
non-
disc
rimin
ator
y ca
re.
■■
Resp
ect f
or p
atie
nts.
■■
Issu
es o
f con
fiden
tialit
y.
■■
Und
erst
andi
ng h
ow to
com
mun
icat
e ef
fect
ivel
y as
a d
octo
r in
the
UK.
Earl
y 20
13
Them
es w
ere
used
to d
evel
op le
arni
ng to
ols.
■■
Onl
ine
scen
ario
-bas
ed to
ol.
■■
Seve
n et
hica
l sce
nario
vid
eos.
■■
Thin
gs I w
ish I’
d ha
ve k
now
n w
hen
I s
tart
ed p
ract
ice
in th
e U
K vi
deo.
Late
201
3
Seve
n pi
lot e
vent
s ac
ross
the
UK,
w
hich
incl
uded
:
■■
over
view
of t
he G
MC
■■
Thin
gs I w
ish I’
d ha
ve k
now
n w
hen
I sta
rted
pra
ctic
e in
the
UK
■■
ethi
cal s
cena
rio v
ideo
s
and
disc
ussi
on
■■
com
mun
icat
ions
exe
rcis
es.
Onl
ine
scen
ario
-bas
ed to
ol
Our
ano
nym
ous o
n-lin
e se
lf-as
sess
men
t sce
nario
-bas
ed to
ol is
des
igne
d to
he
lp d
octo
rs c
heck
thei
r kno
wle
dge
of o
ur c
ore
guid
ance
Goo
d m
edic
al p
ract
ice
and
see
how
they
app
ly it
to re
al s
ituat
ions
. It
als
o sh
ows
whe
re to
find
furt
her
info
rmat
ion
and
advi
ce. T
he to
ol c
onta
ins
16 c
ase
stud
ies t
hat e
xplo
re e
thic
al
chal
leng
es in
diff
eren
t clin
ical
sce
nario
s.
The
onlin
e to
ol h
as b
een
visi
ted
5,00
0 tim
es s
ince
its
laun
ch b
y do
ctor
s fro
m
19 c
ount
ries
and
has
had
posi
tive
feed
back
.
Test
ing
the
Wel
com
e to
UK
pra
ctic
e ev
ents
We
deliv
ered
sev
en p
ilot e
vent
s to
320
doct
ors
in la
te 2
013.
The
aim
of t
hese
pi
lots
was
to u
nder
stan
d ho
w w
e ca
n de
velo
p th
e pr
ogra
mm
e to
del
iver
our
m
essa
ges t
o do
ctor
s ne
w to
pra
ctic
e.
The
first
pha
se o
f the
pilo
ts s
how
ed u
s tha
t the
orig
inal
inte
ract
ive
vide
os
wor
ked
wel
l. Th
e se
cond
pha
se a
llow
ed u
s to
test
our
new
idea
s an
d id
entif
y w
ays t
o m
axim
ise
the
impa
ct o
f the
se e
vent
s w
ith th
e m
ost d
octo
rs.
Dur
ing
the
pilo
t eve
nts
we
show
ed th
e fil
m, T
hing
s I w
ish I
had
know
n w
hen
I sta
rted
pra
ctic
e in
the
UK,
whi
ch s
how
s doc
tors
sha
ring
thei
r per
sona
l ch
alle
nges
and
exp
erie
nces
of s
tart
ing
prac
tice
in th
e U
K.
We
also
use
d et
hica
l sce
nario
vid
eos,
whi
ch e
xplo
re k
ey e
lem
ents
of o
ur
stan
dard
s an
d ex
plan
ator
y gu
idan
ce.
Each
sce
nario
sho
ws
a cl
inic
al s
ituat
ion
whi
ch w
as th
en d
iscu
ssed
by
the
grou
p.
Dur
ing
the
disc
ussi
ons t
he
grou
p w
as s
how
n ho
w th
e
rele
vant
par
ts o
f our
gui
danc
e ap
plie
d to
the
clin
ical
situ
atio
n.
Each
of t
he e
thic
al s
cena
rio v
ideo
s
has
a se
cond
par
t, w
hich
giv
es
a su
gges
ted
outc
ome.
All
of th
ese
lear
ning
tool
s
aim
to b
e in
tera
ctiv
e an
d
seek
to b
ring
our g
uida
nce
to li
fe.
Wha
t ne
xt fo
r the
pro
gram
me?
We
are
wor
king
with
par
tner
s to
hold
furt
her p
ilot e
vent
s ac
ross
the
UK,
as
wel
l as
look
ing
at h
ow m
any
orga
nisa
tions
mig
ht w
ant t
o us
e th
e pr
ogra
mm
e an
d ho
w it
mig
ht b
e pr
ogre
ssed
in th
e fu
ture
.
If yo
u ha
ve a
ny q
uest
ions
abo
ut th
e W
elco
me
to U
K pr
actic
e
prog
ram
me
or w
ould
like
to b
e in
volv
ed, p
leas
e co
ntac
t the
team
at
Wel
com
eUK
@gm
c-uk
.org
.
At t
he e
nd o
f the
pilo
t ev
ents
doc
tors
w
ere
aske
d if
the
day
had
‘impr
oved
th
eir a
war
enes
s of
issu
es re
late
d
to th
e G
MC
eth
ical
gui
danc
e?’
stro
ngly
agr
ee69
.1%
agre
e28
.7%
1.
8%
neith
er a
gree
or
dis
agre
e
0.4%
di
sagr
ee
A b
rillia
nt to
ol in
bet
ter u
nder
stan
ding
G
ood
med
ical
pra
ctic
e in
act
ion
and
it ha
s be
en a
ver
y in
form
ativ
e ex
perie
nce
goin
g th
roug
h al
l the
them
es.
A g
reat
way
to m
eet
othe
r doc
tors
and
lear
n fr
om th
eir e
xper
ienc
es.
I will
use
the
GM
C
reso
urce
s if
I hav
e qu
estio
ns re
gard
ing
the
topi
cs p
rese
nted
toda
y.
I thi
nk th
e G
MC
sho
uld
cont
inue
off
erin
g th
is d
ay.
It h
as b
een
one
of th
e m
ost i
nter
estin
g co
urse
s/ed
ucat
iona
l day
s I h
ave
ever
att
ende
d.

16The national training surveys – driving our quality assurance of medical education and trainingKirsty White, Paul Clayton and Nick di PaoloGeneral Medical Council (UK)
In 2
014,
53,
077
doct
ors
in tr
aini
ng c
ompl
eted
the
su
rvey
out
of 5
4,06
8 w
ho
wer
e el
igib
le, g
ivin
g a
resp
onse
ra
te o
f 98.
2%.
The
doct
ors
in tr
aini
ng s
urve
yed
wer
e:
■■
doct
ors
in tr
aini
ng in
the
first
(F1)
an
d se
cond
(F2)
yea
r of t
he
Foun
datio
n Pr
ogra
mm
e
■■
core
doc
tors
in tr
aini
ng
■■
high
er s
peci
alty
doc
tors
in
trai
ning
, inc
ludi
ng s
peci
alis
t re
gist
rar a
nd g
ener
al
prac
titio
ner d
octo
rs in
trai
ning
■■
fixed
term
spe
cial
ty tr
aini
ng
appo
intm
ent d
octo
rs in
trai
ning
.
The
surv
ey id
entifi
ed v
aria
tion
acro
ss tr
aini
ng p
osts
, for
exa
mpl
e, in
the
over
all s
atis
fact
ion
of tr
aini
ng, w
ith g
ener
al p
ract
ice
post
s (in
clud
ing
Foun
datio
n do
ctor
s) h
avin
g th
e hi
ghes
t av
erag
e sc
ore
of 8
8.6,
and
sur
gica
l pos
ts (i
nclu
ding
Fou
ndat
ion
doct
ors)
with
the
low
est
with
a s
core
of 7
7.1.
C
T1/S
T1C
T2/S
T2ST
3ST
4ST
5ST
6ST
7ST
8To
tal
Core
795
813
Car
diot
hora
cic
5829
1510
75
124
Gen
eral
210
337
280
237
235
206
137
1,44
4
Ora
l and
m
axill
ofac
ial s
urge
ry
39
3524
3510
14
3
Ear,
nose
and
thro
at
10
170
7656
4329
375
Paed
iatr
ic4
529
1832
2115
1213
6
Trau
ma
and
orth
opae
dic
3945
301
183
183
213
186
122
1,27
2
Uro
logy
103
6967
6056
35
5
Tota
l84
187
51,
052
727
704
701
588
328
5,81
6
Nat
iona
l tra
inin
g su
rvey
s: o
ur a
nnua
l sur
vey
of
doc
tors
in tr
aini
ng
The
GM
C is
a c
harit
y re
gist
ered
in
Eng
land
and
Wal
es (1
0892
78)
and
Scot
land
(SC0
3775
0)
Why
do
we
surv
ey d
octo
rs in
trai
ning
?W
e re
gist
er d
octo
rs to
pra
ctis
e m
edic
ine
in th
e U
K. W
e pr
otec
t, pr
omot
e an
d m
aint
ain
the
heal
th
and
safe
ty o
f the
pub
lic b
y en
surin
g pr
oper
stan
dard
s in
the
prac
tice
of m
edic
ine
and
in m
edic
al
educ
atio
n an
d tr
aini
ng.
Each
yea
r, w
e ru
n a
surv
ey o
f all
doct
ors i
n po
stgr
adua
te m
edic
al tr
aini
ng in
the
UK
(aro
und
55,0
00
doct
ors,
with
a re
spon
se ra
te o
f ove
r 95%
sinc
e 20
12).
The
resu
lts o
f the
surv
ey g
ive
us a
relia
ble
sour
ce o
f evi
denc
e th
e pe
rspe
ctiv
e th
at d
octo
rs in
trai
ning
hav
e of
thei
r tra
inin
g en
viro
nmen
t and
th
e qu
ality
of t
heir
trai
ning
.
The
surv
ey g
ives
a sn
apsh
ot o
f the
qua
lity
of m
edic
al e
duca
tion
and
trai
ning
at a
nat
iona
l lev
el.
The
surv
ey a
lso
gene
rate
s a u
niqu
e da
tase
t of t
he tr
aini
ng p
athw
ay a
nd p
rogr
essi
on o
f UK
doct
ors
in tr
aini
ng.
Resp
onde
nts
com
plet
e th
e su
rvey
onl
ine.
The
ir an
swer
s ar
e lo
gged
on
our i
n-ho
use
syst
ems,
whi
ch a
llow
s su
rvey
re
spon
ses t
o be
aut
omat
ical
ly s
tore
d ag
ains
t the
doc
tors
’ rec
ords
hel
d by
the
GM
C.
We
calc
ulat
e sc
ores
for e
very
med
ical
trai
ning
pro
vide
r in
the
UK
for 1
2 di
ffer
ent a
reas
, inc
ludi
ng o
vera
ll sa
tisfa
ctio
n,
clin
ical
sup
ervi
sion
, ind
uctio
n, a
nd h
ando
ver.
The
2014
sur
vey
invo
lved
the
follo
win
g ke
y st
ages
.
■■
We
colle
ct d
ata
from
pos
tgra
duat
e de
ans o
n do
ctor
s in
trai
ning
and
thei
r tra
inin
g lo
catio
n. W
e al
so c
heck
to m
ake
sure
that
all
loca
tions
are
app
rove
d tr
aini
ng s
ites.
■■
Doc
tors
in tr
aini
ng c
onfir
m th
eir t
rain
ing
info
rmat
ion
and
com
plet
e th
e su
rvey
. Thi
s yea
r, th
ey c
ould
do
this
ove
r a
seve
n w
eek
perio
d, b
egin
ning
from
26
Mar
ch 2
014.
■■
We
rele
as th
e su
rvey
resu
lts t
o po
stgr
adua
te d
eans
and
med
ical
roya
l col
lege
s us
ing
our w
eb-b
ased
repo
rtin
g to
ol.
The
resu
lts
pass
wor
d pr
otec
ted
– de
ans
and
roya
l col
lege
s co
uld
see
the
resu
lts o
ne m
onth
bef
ore
they
wer
e re
leas
ed
to th
e pu
blic
, so
they
cou
ld in
vest
igat
e co
ncer
ns lo
cally
.
■■
We
publ
ish
the
surv
ey re
sult
s on
our w
ebsi
te, a
ppro
xim
atel
y ei
ght w
eeks
aft
er th
e su
rvey
clo
ses.
The
resu
lts
can
be
view
ed b
y tr
aini
ng p
rogr
amm
e an
d by
trai
ning
pro
vide
r.
This
was
the
third
yea
r tha
t we
had
run
the
surv
ey o
urse
lves
. It m
eant
that
we’
ve b
een
able
to o
ffer
mor
e us
eful
repo
rts
than
eve
r bef
ore.
■■
Our
onl
ine
tool
incl
udes
agg
rega
ted
repo
rts,
whi
ch c
ombi
ne u
p to
thre
e ye
ars o
f sur
vey
resu
lts.
The
y ar
e de
sign
ed fo
r si
tes
and
spec
ialt
ies t
hat d
o no
t gen
erat
e re
port
s ea
ch y
ear b
ecau
se th
ere
are
less
than
thre
e do
ctor
s in
the
trai
ning
po
sts
at o
ne ti
me.
■■
Our
tren
d re
port
s, w
hich
sho
w th
ree
year
s of r
esul
ts s
ide
by s
ide,
to g
ive
an o
verv
iew
of h
ow p
erce
ptio
ns o
f tra
inin
g ha
ve im
prov
ed, d
eter
iora
ted
or re
mai
ned
cons
tant
ove
r tim
e. T
hey
let p
ostg
radu
ate
dean
s se
e w
here
thei
r qua
lity
impr
ovem
ent s
trat
egie
s ar
e w
orki
ng a
nd w
hich
are
as n
eed
furt
her w
ork.
We
have
iden
tified
the
site
s w
ith th
ree
year
s of
poo
r res
ults
and
are
wor
king
with
pos
tgra
duat
e de
ans t
o in
vest
igat
e th
em a
nd ta
ke a
ctio
n.
■■
The
surv
ey a
lso
give
s doc
tors
in tr
aini
ng th
e ch
ance
to ra
ise
any
conc
erns
they
hav
e ab
out p
atie
nt s
afet
y.
How
doe
s th
e su
rvey
wor
k?
Wha
t the
sur
vey
show
s
Our
201
4 su
rvey
had
one
of t
he h
ighe
st re
spon
se ra
tes o
f any
of o
ur p
revi
ous
surv
eys o
f doc
tors
in
trai
ning
. The
resu
lts
wer
e sh
ared
with
pos
tgra
duat
e de
ans
and
med
ical
roya
l col
lege
s to
take
act
ion
only
four
wee
ks a
fter
the
surv
ey c
lose
d.
The
surv
ey is
wel
l est
ablis
hed
and
deep
ly e
mbe
dded
in th
e qu
ality
ass
uran
ce s
yste
ms o
f reg
iona
l (P
ostg
radu
ate
Dea
ns) a
nd lo
cal (
trus
ts, b
oard
s, h
ospi
tals
, pra
ctic
es) t
rain
ing
prov
ider
s. P
ostg
radu
ate
Dea
ns a
re re
quire
d to
resp
ond
to th
e re
sult
s ea
ch y
ear,
and
to p
ublis
h ac
tion
plan
s w
here
poo
r re
sult
s in
dica
te p
robl
ems.
Con
clus
ion
In a
utum
n 20
14 w
e w
ill p
ilot a
sur
vey
of tr
aine
rs, w
hich
will
pro
vide
evi
denc
e on
whe
ther
they
thin
k th
e tr
aini
ng e
nviro
nmen
ts s
uppo
rt th
em in
thei
r tra
iner
role
. We’
ve b
een
wor
king
for s
ome
time
to
incr
ease
the
reco
gniti
on a
nd s
uppo
rt fo
r doc
tors
who
mak
e a
sign
ifica
nt c
ontr
ibut
ion
to m
edic
al
trai
ning
as
part
of t
heir
prof
essi
onal
role
. In
2012
, fol
low
ing
cons
ulta
tion,
we
publ
ishe
d Re
cogn
ising
an
d ap
prov
ing
trai
ners
: the
impl
emen
tatio
n pl
an w
hich
det
ails
arr
ange
men
ts a
nd a
tim
etab
le fo
r re
cogn
isin
g un
derg
radu
ate
and
post
grad
uate
trai
ners
. Ove
r tim
e, th
e su
rvey
of t
rain
ers
will
hel
p us
un
ders
tand
how
the
impl
emen
tatio
n pl
an h
as b
een
deliv
ered
acr
oss t
he U
K.
Nex
t st
eps:
und
erst
andi
ng th
e pe
rspe
ctiv
e
of tr
aine
rs
98.2
%
of d
octo
rs in
trai
ning
re
spon
ded
to th
e
2014
sur
vey
100 80 4060 20 0
Ove
rall
satis
fact
ion
Clin
ical
sup
ervi
sion
Han
dove
rIn
duct
ion
Ade
quat
e ex
perie
nce
Wor
kloa
dEd
ucat
iona
l sup
ervi
sion
Acc
ess t
o ed
ucat
iona
l res
ourc
esFe
edba
ckLo
cal t
each
ing
Regi
onal
teac
hing
Stud
y le
ave
Upp
er q
uart
ileIn
terq
uart
ile ra
nge
Low
er q
uart
ileN
atio
nal m
ean
Nat
iona
l ind
icat
or s
core
s 20
14
Wal
es
Nor
ther
nIre
land
East
of E
ngla
ndW
est M
idla
nds
East
Mid
land
s
Nor
th E
ast
Nor
th W
est
Lond
on
Kent
, Sur
rey
and
Suss
ex
York
shire
and
the
Hum
ber
Wes
sex
Sout
h W
est
Peni
nsul
a
Scot
land
(Wes
t Reg
ion)
Seve
rn
Oxf
ord
Mer
sey
Scot
land
(Nor
th R
egio
n)
Scot
land
(Eas
t Reg
ion)
Scot
land
(Sou
th-E
ast R
egio
n)
9,667
4,704
4,4153,651
3,420
3,247
3,141
2,619
2,555
2,417
2,354
2,002
2,051
1,739
1,639
1,435
1,25
7
716
528
Num
bers
of d
octo
rs in
trai
ning
by
regi
on
All
UK
sur
gery
doc
tors
in tr
aini
ng b
y tr
aini
ng le
vel
CT=
Cor
e tr
aini
ng, S
T= S
peci
alit
y tr
aini
ng
Aut
hors
: Kirs
ty W
hite
, Hea
d of
Pla
nnin
g, R
esea
rch
and
Dev
elop
men
t,Pa
ul C
layt
on, S
urve
y D
evel
opm
ent M
anag
er, N
ick
di P
aolo
, Sur
vey
Ana
lyst
(GM
C S
urve
ys T
eam
).
17‘Coaching and Mentoring’ – a prerequisite for the doctor of today and tomorrowDr Rebecca Viney, Prof John Howard, Health Education East of EnglandBeryl Da Souza, Medical Womens Federation
‘Coaching and Mentoring’
-‐ a prerequisite for the doctor of today and tomorrow
Dr Rebecca Viney, Professor John Howard, Ms Beryl De Souza,
Coaching and Mentoring In addition to increasing depth and knowledge needed to work in their chosen specialty. It is becoming more important that the skills of mentoring and coaching are needed in the everyday life of a doctor. This concept is endorsed by the GMC as important for doctors to deliver safe, effective and efficient care to patients as soon as they start a new job. Coaching and mentoring have been used in the commercial sector for many years and are increasingly being used in the NHS with patients, colleagues, teams, in management and for leadership. The development of local and national schemes to train mentors and coaches for health care professionals is supported by the National Health Service by initiatives such as the London Deanery Coaching and Mentoring Service.
Defining coaching and mentoring When defining coaching and mentoring the terms should be differentiated from other development roles such as patronage, appraisal, educational supervision or line management. It is not teaching, telling, advising or instructing. Neither is it counselling or therapy although the process of coaching and mentoring may identify the need for this. The precise definitions and use of the terms coaching and mentoring vary. However those offering will need to demonstrate a common set of core skills and qualities.
Core skills needed to be a coach or mentor [1] Observation The person being coached or mentored will at times display much of what they are thinking or feeling through body language. It is therefore essential that the coach or mentor is able to notice this and in particular to react appropriately when there is a mismatch between what is being said and the non-verbal cues that are being displayed. Questioning This is the ability to use questions to help the person being coached or mentored to develop their thinking and to explore the issue or topic in depth. Challenge The coach or mentor needs to be able to challenge the thinking of the person being coached or mentored, and this may be done through questioning but also through observation and comment. Feedback Providing specific and constructive feedback is a necessary part of helping the person being coached or mentored to develop. Reflection The coach or mentor needs to practise reflection and to foster a reflective perspective in the person being coached or mentored. Mentoring and Coaching We recommend to allow for resilience and sustaining of the working life of a doctor there should be coaching and mentoring training embedded at medical school and throughout the training grades. Reference [1] Viney R, Harris D. Coaching and mentoring. In: Bhugra D, Ruiz P, Gupta S, eds. Leadership in psychiatry. Wiley-Blackwell, 2013:126-36.
Qualities needed in a coach or mentor [1] • High level of self awareness
• Genuine interest in others
• Open and approachable style
• Humility
• Integrity
• Confidentiality
Active listening This is the ability to engage with and respond to what the person being coached or mentored is saying, attending to what is being said, and managing distractions.
Dr Rebecca Viney: [email protected] | Beryl De Souza: [email protected]
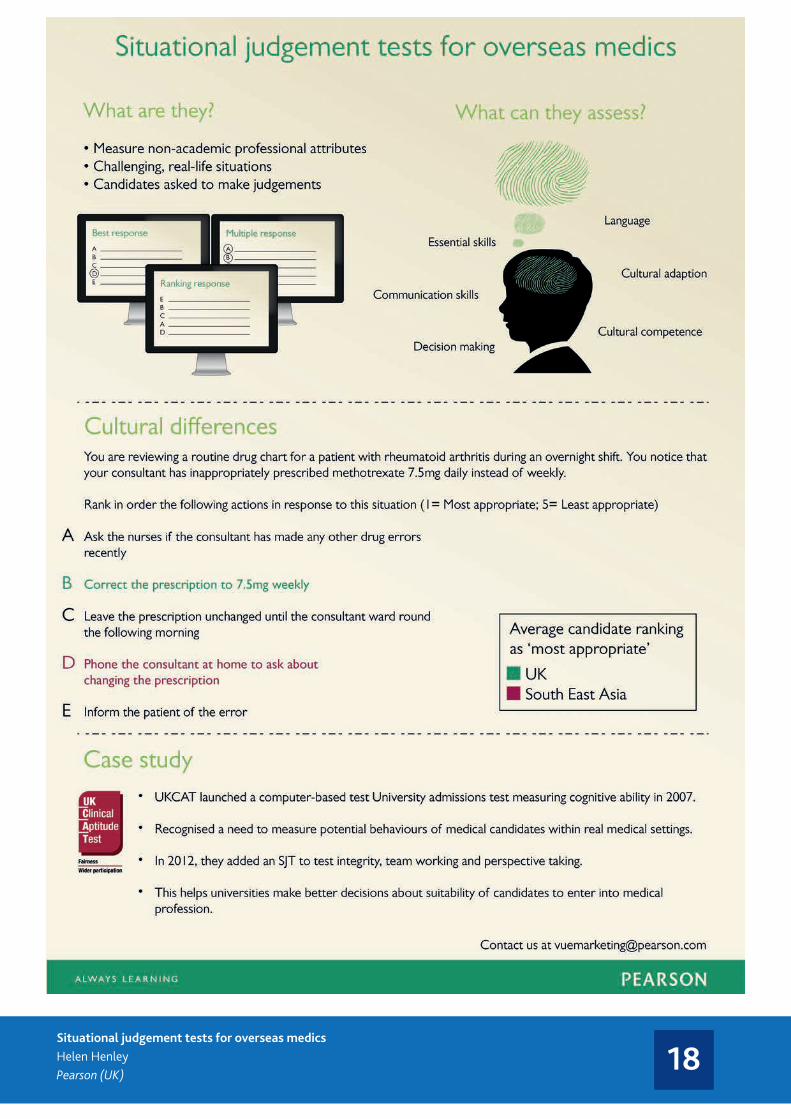
18Situational judgement tests for overseas medicsHelen HenleyPearson (UK)

19One size does not fit all – a right-touch approach to assuring continuing fitness to practiseDinah GodfreeProfessional Standards Authority for Health and Social Care (UK)
� Determining what level of risk you should and can mitigate You should determine the extent to which you are willing to compromise on the reliability of your mechanisms for determining whether a practitioner continues to be fit to practise, based on an assessment of the level and type of risk you feel you can and should be mitigating – and what risks you are prepared to tolerate. Reliability can be improved by reducing the numbers of false negatives (incorrect ‘fails’) and false positives (incorrect ‘passes’).
� Developing a response that is proportionate to the level of risk you want to mitigate The severity and prevalence of a risk, and your decisions about what risks you are prepared to tolerate should guide decisions about the regulatory force that is needed. We find it helpful to think of the range of possible responses as sitting on a risk-based continuum (fig. 2).
� Targeting your response You can use the information derived from identifying risks to develop mechanisms that focus on the higher risk practice areas or groups.
� Developing a response that addresses the type of risk, for example:
� Tailoring evidence requirements to collect information on a specific area of practice or conduct, and to improve practice in these areas (e.g. gathering information on how one-to-one consultations are carried out to identify and root out sub-standard practice)
� Using evidence collection or assessment methods that address identified risks (e.g. requiring peer review of performance to address problem of isolated practice).
Applying right-touch regulation principles to continuing fitness to practise � Understanding the risks
This involves looking at the factors that might be associated with professional failings in continuing practise in terms of context and activity, and possible impact on conduct and competence.
Table 1: Some risk factors associated with continuing fitness to practise for health and care professionals
Risk factor (source) Authority’s interpretation
Context
Effectiveness of clinical governance mechanisms (GOC)
What measures are in place to manage risk and learn from mistakes
Effectiveness of qualifying training (HCPC) How well the course has taught skills, knowledge and professionalism Frequency of practise (PSNI, TAS) If practitioner is well-versed in his/her field, e.g. returners to practise, practitioners in
predominantly management roles Level of autonomy (TAS) Extent to which practice is monitored and practitioners able to practise independently Level of isolation (GOC) Level of interaction with other practitioners (linked to practice context) Level of support (PSNI) Quantity and quality of appraisals, learning opportunities, etc to which registrant has
access Practice context (GOC, GOsC, TAS) Whether in private practice, NHS or non-NHS managed environments, or domiciliary Time since qualification (GOC, NCAS, TAS) Length of time since practitioner qualified Workload (PSNI) Pressure on practitioners to become more efficient; increased stress
Activity
Complexity of task (GOC, TAS) Complexity of diagnosis, procedure or treatment; including management of issues related to the service user such as compliance with treatment
Emotional and psychological engagement (PSA)
Extent to which intervention poses an emotional and/or psychological risk to the service user
Level of responsibility (TAS) Whether responsible for service user safety, how many responsible for; vulnerability and/or severity of condition
Likelihood and severity of treatments side-effects (GCC)
Extent to which practitioner manages risky side-effects
Medical invasiveness (TAS) Whether the intervention requires invasive medical treatment Rate of evolution of techniques (GOC) Level of need for ongoing training and learning Sexual invasiveness (GOsC) Whether the intervention requires undressing and/or contact with intimate areas
What is right-touch regulation?
A set of principles for developing regulatory policy Regulation should: � be proportionate, consistent, targeted, transparent,
accountable, agile, and outcome-focused � be based on a sound understanding of the risks it needs to
address � share the risks with other agencies: people, professionals,
employers, commissioners, the law, and other regulators � look for existing solutions before introducing new ones � apply the appropriate level of regulatory force.
Figure 1: The concept of regulatory force
Professional Standards Authority, August 2010. Right-touch regulation.
One size does not fit all – a right-touch approach to assuring continuing fitness to practise Dinah Godfree, Policy Adviser IAMRA Conference 2014
Abstract With the UK General Medical Council’s recent introduction of revalidation for doctors in the UK, the question of how a professional regulator can assure the continuing fitness to practise (FtP) of its registrants is a live debate both within the UK and internationally. At the Professional Standards Authority, we have applied the principles set out in our landmark paper Right-touch regulation to this question. This poster explains how an intelligent and proportionate continuing fitness to practise model should be based on a sound understanding of the type and prevalence of a range of risk factors connected to the professional group in question.
What is continuing fitness to practise?
Regulators should be able to provide assurances of the continuing fitness to practise of their registrants
All the regulatory functions contribute to these aims
How do I know that my healthcare professional is up-to-date and fit to practise?
Focus on the outcome: compliance with the regulator’s core
standards of competence and conduct
Quality control vs. quality improvement It is important to be clear about the purpose of assuring continuing fitness to practise. For regulators to be able to answer the patient’s question above, they must have some means of checking their registrants’ compliance with core standards – you could call this outcome-focused ‘quality control’. However, this does not preclude the pursuit of quality improvement, which can be achieved through the intelligent application of quality control mechanisms. The primary role of continuing fitness to practise should be to reaffirm that registrants continue to meet the core standards of competence and behaviour.
Be clear about the purpose: periodic re-affirmation of continued
fitness to practise
too little: ineffective
too much: wasted effort
right-touch regulation
standards QA of education registration continuing FtP FtP
Some examples from the UK
In conclusion � There are many possible responses to the challenge of assuring continuing fitness to
practise, revalidation is just one of them. � Continuing fitness to practise mechanisms should enable a regulator to reaffirm
periodically its registrants’ continued fitness to practise, in relation to both conduct and competence.
� Compliance with CPD requirements is not in itself a demonstration of continuing fitness to practise.
� Regulators need to know the types, severity and prevalence of the risks presented by the professions they regulate in order to develop measures that are proportionate and targeted. They should consider risk factors linked with context as well as activity.
� Regulators also need to make a judgment about the levels of risk they can and should respond to and what they are prepared to tolerate.
� Approaches taken should be both intelligent and agile, making use of existing mechanisms where possible, and adapting in response to intelligence about their effectiveness and impact.
continuing fitness to practise
CHRE: although it did not feature in any of the literature reviewed, this risk factor has been added by the authors, on the basis that if medical and sexual invasiveness can be said to result in heightened risks for service users, so too can psychological or emotional ‘invasiveness’. GCC: Europe Economics, February 2010. Report to the General Chiropractic Council. General Chiropractic Council. GOC: Europe Economics, March 2010. Risks in the Optical Profession, Final Report. General Optical Council. GOsC: KPMG, 2011. How do osteopaths practise? Executive summary. General Osteopathic Council.
HCPC (then HPC): Health Professions Council, October 2008. Continuing Fitness to Practise, Towards an evidence–based approach to revalidation. Health Professions Council. NCAS: National Clinical Assessment Service, September 2009. NCAS Casework, The first eight years. National Clinical Assessment Service. PSNI: University of Manchester, June 2011. Assessing Risk Associated with Contemporary Pharmacy Practice in Northern Ireland, Executive Summary of the Final Report. Pharmaceutical Society of Northern Ireland TAS: HM Government, February 2007. Trust, Assurance and Safety – The Regulation of Health Professionals in
st
Low High
High
Figure 2: How levels of risk drive levels of assurance
Level of assurance/ reliability of measurement
Level of risk
regulatory force
target risk
General Medical Council (introduced 2012) � Five year cycle � Based on regular appraisals against core guidance, Good
medical practice including reflection and discussion of: 1. Continuing professional development (CPD) 2. Quality improvement activity 3. Significant events 4. Feedback from colleagues 5. Feedback from patients 6. Review of complaints and compliments.
� GMC decision to revalidate based on: - a recommendation from a ‘responsible officer’
(usually medical director) that the doctor is up to date and fit to practise based on a doctor’s appraisals over the last five years and other information drawn from their organisation’s clinical governance systems
- further checks by the GMC to ensure there are no other concerns.
General Osteopathic Council (draft framework)
Three year cycle with 90 hours of CPD (including 45 hours of learning with others).Three mandatory elements: � objective activity to inform CPD and
practice (e.g. patient feedback), peer observation, clinical audit or case-based discussion
� CPD in communication and consent � CPD in all four themes of the
Osteopathic Practice Standards (communication and patient partnership, knowledge, skills and performance, safety and quality).
Cycle completed by ‘Peer Discussion Review’ of CPD, practice, and patient care; compliance with the scheme.
General Optical Council (introduced 2013)
� Three year cycle � Points-based requirements – minimum per cycle. Points reflect:
- the level of engagement with peers or experts, and - the extent to which the activity supports reflection (e.g. peer discussion and clinical skills Continuing
Education and Training (CET) carry more points than attendance at lectures. � Registrants expected to spread their CET activity throughout 3 year cycle with a min of 6 points / year (the
points requirement is calculated pro rata for registrants who join mid-year) � A minimum of half the points must be achieved through interactive CET.
� Fitness to practise data suggests that conduct breaches arise in a large proportion of fitness to practise cases: - GMC: in 2012, 46% of complaints were neither
about clinical care, nor about clinical care combined with communication. Complaints concerning probity almost always reached the threshold for investigation.1
- GDC: 1/3 of issues considered by its fitness to practise committees in 2013 related to conduct.2
1 General Medical Council, 2014. The State of Medical Education and Practice in the UK, 2013. 2 General Dental Council, 2014. Annual report and accounts 2013.
� Compliance with CPD requirements may be necessary but is not in itself a demonstration of continuing fitness to practise.
For the full report, An approach to assuring continuing fitness to practise based on right-touch regulation principles, and references, please visit:
www.professionalstandards.org.uk © Professional standards Authority for Health and Social Care, September 2014

20Let’s talk about end of life careKevin Stewart, Janet Husk, Royal College of Physicians of London (UK) John Ellershaw, Helen Mulholland, Marie Curie Palliative Care Institute Liverpool

21Standards for the structure and content of clinical incident reportsAlexis Lewis, John Williams, Harold ThimblebySwansea University (UK)
Methods applied
Systema0c literature review
Comparison of current repor0ng forms
Interviews with staff
Workshops with staff and pa0ents
Well documented barriers to clinical incident repor0ng
Forms are long, diverse, complicated and do not match na0onal requirements
“By the 0me you get to the boDom of the form you are losing the will to live!”
The development of a simplified content for the report form A single repor0ng process is in
development which will conform to the Academy of Medical Royal Colleges' standards for the structure and content of pa0ent records.
Alexis Lewis, John Williams and Harold Thimbleby
Repor0ng requirements
Diversity in local and na0onal requirements for inves0ga0on and analysis

22The science of bespoke testingDr Clare Wadlow, Dr Eleana Ntatsaki, Dr Alison Sturrock, Prof Jane DacreUniversity College London (UK)
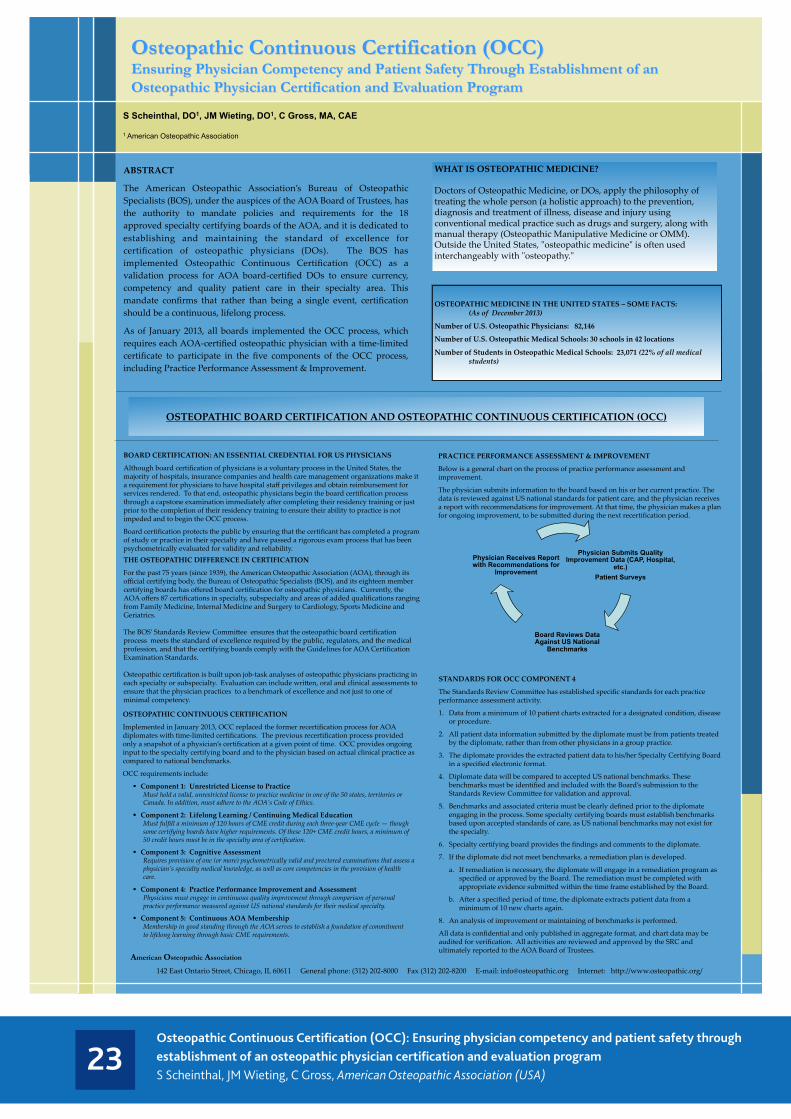
23Osteopathic Continuous Certification (OCC): Ensuring physician competency and patient safety through establishment of an osteopathic physician certification and evaluation programS Scheinthal, JM Wieting, C Gross, American Osteopathic Association (USA)
S Scheinthal, DO1, JM Wieting, DO1, C Gross, MA, CAE 1 American Osteopathic Association
ABSTRACT
The American Osteopathic Association’s Bureau of Osteopathic Specialists (BOS), under the auspices of the AOA Board of Trustees, has the authority to mandate policies and requirements for the 18 approved specialty certifying boards of the AOA, and it is dedicated to establishing and maintaining the standard of excellence for certification of osteopathic physicians (DOs). The BOS has implemented Osteopathic Continuous Certification (OCC) as a validation process for AOA board-‐‑certified DOs to ensure currency, competency and quality patient care in their specialty area. This mandate confirms that rather than being a single event, certification should be a continuous, lifelong process.
As of January 2013, all boards implemented the OCC process, which requires each AOA-‐‑certified osteopathic physician with a time-‐‑limited certificate to participate in the five components of the OCC process, including Practice Performance Assessment & Improvement.
Osteopathic Continuous Certification (OCC) Ensuring Physician Competency and Patient Safety Through Establishment of an Osteopathic Physician Certification and Evaluation Program
WHAT IS OSTEOPATHIC MEDICINE? Doctors of Osteopathic Medicine, or DOs, apply the philosophy of treating the whole person (a holistic approach) to the prevention, diagnosis and treatment of illness, disease and injury using conventional medical practice such as drugs and surgery, along with manual therapy (Osteopathic Manipulative Medicine or OMM). Outside the United States, "ʺosteopathic medicine"ʺ is often used interchangeably with "ʺosteopathy."ʺ
BOARD CERTIFICATION: AN ESSENTIAL CREDENTIAL FOR US PHYSICIANS
Although board certification of physicians is a voluntary process in the United States, the majority of hospitals, insurance companies and health care management organizations make it a requirement for physicians to have hospital staff privileges and obtain reimbursement for services rendered. To that end, osteopathic physicians begin the board certification process through a capstone examination immediately after completing their residency training or just prior to the completion of their residency training to ensure their ability to practice is not impeded and to begin the OCC process.
Board certification protects the public by ensuring that the certificant has completed a program of study or practice in their specialty and have passed a rigorous exam process that has been psychometrically evaluated for validity and reliability.
OSTEOPATHIC BOARD CERTIFICATION AND OSTEOPATHIC CONTINUOUS CERTIFICATION (OCC)
OSTEOPATHIC MEDICINE IN THE UNITED STATES – SOME FACTS: (As of December 2013)
Number of U.S. Osteopathic Physicians: 82,146
Number of U.S. Osteopathic Medical Schools: 30 schools in 42 locations
Number of Students in Osteopathic Medical Schools: 23,071 (22% of all medical students)
American Osteopathic Association
142 East Ontario Street, Chicago, IL 60611 General phone: (312) 202-‐‑8000 Fax (312) 202-‐‑8200 E-‐‑mail: [email protected] Internet: h`p://www.osteopathic.org/
PRACTICE PERFORMANCE ASSESSMENT & IMPROVEMENT
Below is a general chart on the process of practice performance assessment and improvement.
The physician submits information to the board based on his or her current practice. The data is reviewed against US national standards for patient care, and the physician receives a report with recommendations for improvement. At that time, the physician makes a plan for ongoing improvement, to be submi`ed during the next recertification period.
OSTEOPATHIC CONTINUOUS CERTIFICATION
Implemented in January 2013, OCC replaced the former recertification process for AOA diplomates with time-‐‑limited certifications. The previous recertification process provided only a snapshot of a physician’s certification at a given point of time. OCC provides ongoing input to the specialty certifying board and to the physician based on actual clinical practice as compared to national benchmarks.
OCC requirements include:
§ Component 1: Unrestricted License to Practice Must hold a valid, unrestricted license to practice medicine in one of the 50 states, territories or Canada. In addition, must adhere to the AOA’s Code of Ethics.
§ Component 2: Lifelong Learning / Continuing Medical Education Must fulfill a minimum of 120 hours of CME credit during each three-‐‑year CME cycle — though some certifying boards have higher requirements. Of these 120+ CME credit hours, a minimum of 50 credit hours must be in the specialty area of certification.
§ Component 3: Cognitive Assessment Requires provision of one (or more) psychometrically valid and proctored examinations that assess a physician’s specialty medical knowledge, as well as core competencies in the provision of health care.
§ Component 4: Practice Performance Improvement and Assessment Physicians must engage in continuous quality improvement through comparison of personal practice performance measured against US national standards for their medical specialty.
§ Component 5: Continuous AOA Membership Membership in good standing through the AOA serves to establish a foundation of commitment to lifelong learning through basic CME requirements.
THE OSTEOPATHIC DIFFERENCE IN CERTIFICATION
For the past 75 years (since 1939), the American Osteopathic Association (AOA), through its official certifying body, the Bureau of Osteopathic Specialists (BOS), and its eighteen member certifying boards has offered board certification for osteopathic physicians. Currently, the AOA offers 87 certifications in specialty, subspecialty and areas of added qualifications ranging from Family Medicine, Internal Medicine and Surgery to Cardiology, Sports Medicine and Geriatrics. The BOS’ Standards Review Commi`ee ensures that the osteopathic board certification process meets the standard of excellence required by the public, regulators, and the medical profession, and that the certifying boards comply with the Guidelines for AOA Certification Examination Standards. Osteopathic certification is built upon job-‐‑task analyses of osteopathic physicians practicing in each specialty or subspecialty. Evaluation can include wri`en, oral and clinical assessments to ensure that the physician practices to a benchmark of excellence and not just to one of minimal competency.
Physician Submits Quality Improvement Data (CAP, Hospital,
etc.) Patient Surveys
Board Reviews Data Against US National
Benchmarks
Physician Receives Report with Recommendations for
Improvement
STANDARDS FOR OCC COMPONENT 4
The Standards Review Commi`ee has established specific standards for each practice performance assessment activity.
1. Data from a minimum of 10 patient charts extracted for a designated condition, disease or procedure.
2. All patient data information submi`ed by the diplomate must be from patients treated by the diplomate, rather than from other physicians in a group practice.
3. The diplomate provides the extracted patient data to his/her Specialty Certifying Board in a specified electronic format.
4. Diplomate data will be compared to accepted US national benchmarks. These benchmarks must be identified and included with the Board’s submission to the Standards Review Commi`ee for validation and approval.
5. Benchmarks and associated criteria must be clearly defined prior to the diplomate engaging in the process. Some specialty certifying boards must establish benchmarks based upon accepted standards of care, as US national benchmarks may not exist for the specialty.
6. Specialty certifying board provides the findings and comments to the diplomate.
7. If the diplomate did not meet benchmarks, a remediation plan is developed.
a. If remediation is necessary, the diplomate will engage in a remediation program as specified or approved by the Board. The remediation must be completed with appropriate evidence submi`ed within the time frame established by the Board.
b. After a specified period of time, the diplomate extracts patient data from a minimum of 10 new charts again.
8. An analysis of improvement or maintaining of benchmarks is performed.
All data is confidential and only published in aggregate format, and chart data may be audited for verification. All activities are reviewed and approved by the SRC and ultimately reported to the AOA Board of Trustees.

24Pathway to medical practice in the US.Dr Humayun Chaudhry, Mike Dugan, Kevin Caldwell, David Hooper, Amy GeraldFederation of State Medical Boards (USA)
Before the End of U.S. Residency/Fellowship
• Begin to apply for employment or make plans for independent practice
• Apply for full and unrestricted state medical license(s)6
• Apply with FCVS (may be required) • Apply with Uniform Application
(available in many states)• Apply with individual state medical
board(s) (if applicable)If indicated:
• Apply for ABMS /AOA Specialty Board Certifi cation Exam
• Apply for hospital privileges• Apply for provider status with health
insurance companies• Apply for DEA Registration• Obtain Medicare/Medicaid privileges
U.S. Pre-Medical• Register for MCAT• Apply with AMCAS
and/or AACOMAS
U.S. Medical School1st Year
U.S. Medical School 2nd Year• USMLE Step 1• COMLEX-USA
Level 11
U.S. Medical School 4th Year• Register for ERAS• Register for NRMP2
• Register for AOA Match• Obtain MD or DO degree
U.S. Medical School 3rd Year
• USMLE Step 2 CK• USMLE Step 2 CS• COMLEX-USA Level 2 CE1
• COMLEX-USA Level 2 PE1
After the Start of U.S. Residency• USMLE Step 34
• COMLEX-USA Level 31,4
• Apply for state training license5, if indicated, or full and unrestricted state medical license, if eligible6
Ongoing Medical Practice• State licensure renewal7 (Maintenance
of Licensure), including state-specifi c requirements
• Continuing Medical Education8
• Maintenance of Certifi cation and/or Osteopathic Continuous Certifi cation, if indicated
MD DO IMG ALL
1U.S. DOs are also eligible to take the USMLE Examination.2U.S. DOs are also eligible to register for the NRMP.3IMGs are eligible at this time to train in ACGME-accredited
GME programs only.4Medical school graduates may be able to sit for this exam
before residency training.
5Training licensure requirements vary from state to state (41
state boards issue a resident/training license). 6Licensure eligibility differs from state to state.7State licensure renewals vary from 1- to 3-year cycles.8CME is usually accredited by the ACCME, AMA, AAFP and AOA.
LegendAACOMAS: American Association of Colleges of Osteopathic Medicine
Application Service
AAFP: American Academy of Family Physicians
ABMS: American Board of Medical Specialties
ACCME: Accreditation Council for Continuing Medical Education
ACGME: Accreditation Council for Graduate Medical Education
AMA: American Medical Association
AMCAS: American Medical College Application Service
AOA: American Osteopathic Association
CE: Cognitive Evaluation
CK: Clinical Knowledge
COMLEX-USA: Comprehensive Osteopathic Medical Licensing Examination
CS: Clinical Skills
DEA: Drug Enforcement Administration
DO: Doctor of Osteopathic Medicine
ECFMG: Educational Commission for Foreign Medical Graduates
ERAS: Electronic Residency Application Service
FCVS: Federation Credentials Verifi cation Service
GME: Graduate Medical Education
IMG: International Medical Graduate
MCAT: Medical College Admission Test
MD: Doctor of Medicine
NRMP: National Resident Matching Program
PE: Performance Evaluation
USMLE: United States Medical Licensing Examination
PATHWAY TO MEDICAL PRACTICE IN THE U.S.
IMG Registration for U.S. Residency• USMLE Step 1• USMLE Step 2 CK, USMLE Step 2 CS• Obtain MD degree or equivalent• Obtain ECFMG certifi cation• Obtain Visa, if indicated
25Training the global physicians: The SGU School of Medicine approachCalum N. L. MacphersonSt George’s University, Grenada (West Indies)
26Decentralisation of internship by the Medical and Dental Practitioners’ Council of ZimbabweJosephine MwakutuyaMedical and Dental Practitioners Council of Zimbabwe
DECENTRALISATION OF INTERNSHIP BY THE MEDICAL AND DENTAL PRACTITIONERS’ COUNCIL OF ZIMBABWE (MDPCZ) Josephine Mwakutuya BMGT (HR) MBA The Medical and Dental Practitioners Council of Zimbabwe whose tenure has been from 2010 and ending in 2015 was faced with an increasing number of junior resident medical officers from the College of Health Sciences as its throughput increased over the years. The increased residents had to be absorbed somehow. The Council resolved to identify and upgrade five Provisional and District hospitals from ten Provinces where these Junior Resident Medical Officers (JRMOs) could undertake their internship away from the traditional Teaching Units (TUs) which were becoming congested. The strategy was to: Broadly to reduce harm to patients as is the theme of the 11th biennial
edition of the conference Specifically enhance quality of medical standards Meet the growing output of medical graduates Guaranteeing best practice in a growth background
The background of the challenges on the scene included: Shrinking space at traditional Teaching Units (TUs) General resource constraints with the associated negative impact on the
limited Designated Health Institutions (DHIs) “Unbaked” products of internship Distorted population ratios per medical practitioner The growing patient population and the burden of the same The structure of traditional Teaching Units (TUs) assumed the following
organogram:
Consultant Senior Registrar (SR) , Masters in Medicine (MMED) students
Senior House Officer (SHO) Junior Resident Medical Officer (JRMO) (Medical Students)
Challenges on the JRMO training included: Overcrowded 10-15 JRMOs per unit The ideal setup is 4 JRMOs per unit There was then compromise on the quality of the JRMO produced
alongside virtues of excellence , motivation and best practice In the year 2000 the throughput was 150 JRMOs and in 2013 it shot up
to 299 This is against a background that another faculty has since been
established in the country
The Medical and Dental Practitioners’ Council of Zimbabwe has since responded to these challenges in the increase of JRMOs by: Adopting a concept of decentralisation of internship By identifying and accrediting suitable peripheral institutions Five such institutions equipped with optimal material and human capital
resources were found in 10 Provinces. The limitation however was that complete rotations in all disciplines were
not possible. Therefore twinning arrangements were put into place It is also envisaged that experiences from the five units be shared at a
consultative forum Inter-alia here and there teething problems have necessitated
“re-strategy”
The new model which is co-existing with the traditional Teaching Units (TUs) still offers comprehensive services that include: Acute intake rota, medicine and psychiatry. Post take rounds. Grand rounds. Emergency and electric surgical/orthopaedic lists Gynaecology and Obstetrics Anaesthesia Internal Medicine
CO-EXISTING NEW MODEL Consultant
Middle level Government Medical Officer Special (GMO)
“Train the Trainer”
JRMO
The monitoring and evaluation is being achieved through: Interval and Adhoc inspections in loco by sub-committees of the
Education and Liason Committee (ECL). Pilot assessment forms are in place. Log books are universal for all interns. Feedback forms are in place. Inter-alia there is always room for systems improvement.
The benefits of this exercise include: Decongestion achieved at traditional Teaching Units. Mentees report good exposure as they are apprenticed. Invariably senior surgeons in the outskirts are apparently versatile. The majority of folk who are rural are served. Professionalism and ethics not only prevail comparably but also are
maintained.
The government medical officer featured in the decentralisation programme since 2011. This is a medical cadre who would have completed a 2 year general medical education programme and rotated sufficiently in surgery obstetrics and gynaecology and in some cases anaesthesia. In other words the medical practitioner is a graduate “train the trainer”. They are: Generally effective mentors for mentees Complimenting Consultants effectively In the majority posted to Provisional and District hospitals Are good candidates for specialisation later From the 10 Provinces they are five Teaching Units (TUs) accommodating 140 JRMOs.
In conclusion MDPCZ is satisfied with the paradigm shift which it is happy to share with those in similar settings as theirs. Besides there is indication that there is less harm to patients. And indeed the quality of public health delivery is enhanced. Against this background of success, Council has resolved to copying and pasting the same programme on the SHO (MMED) graduate deployment.

HOSTED BY
Email: [email protected] GMC website: www.gmc-uk.orgIAMRA website: www.iamra.com
Join the conversation
#IAMRA2014
Published September 2014
The GMC is a charity registered in England and Wales (1089278) and Scotland (SC037750)
GMC/IAMRACG/0914