1 skeletal class iii malocclusion: a case report · skeletal class iii malocclusion: a case report...
TRANSCRIPT

1
ORTHODONTIC COMPENSATION INSKELETAL CLASS III MALOCCLUSION:A CASE REPORT
Aim: To describe the dentoskeletal changes occurring during treat-ment of a patient with a skeletal Class III malocclusion treated fororthodontic compensation at 10 years 4 months of age. Methods:Rapid maxillary expansion was performed with a Hyrax appliance,Petit orthopedic face mask, high-pull chin cap, and bioprogressivefixed mechanics. Results: The mechanics employed yielded down-ward and backward mandibular rotation (3 degrees of opening of thefacial axis), advancement of the maxillary incisors, and retraction ofthe mandibular incisors. The result was satisfactory from bothesthetic and functional standpoints, providing adequate overjet andoverbite, and with stability at 5 years posttreatment. Conclusion: Theoption for compensatory treatment of the skeletal Class III malocclu-sion without extractions and without orthognathic surgery might be agood option for young patients with good compliance, convergentfacial pattern (brachyfacial), and with deep bite, since such occlusalcharacteristics allow the downward and backward mandibular rota-tion that is necessary for correction of this problem. World J Orthod2007;8:xx–xx.
Márcio Antonio deFigueiredo, MSc1
Danilo Furquim Siqueira,PhD2
Silvana Bommarito, PhD3
Marco Antonio Scanavini,PhD4
Class III malocclusions may be classi-fied into 2 types: pseudo Class III
and true Class III. According to Gianellyet al,1 pseudo Class III involves anteriorcrossbite in maximum intercuspation;however, in centric relation, there isClass I malocclusion with an orthog-nathic facial profile. According to Benchet al,2 pseudo Class III may be causedby inadequate positioning of the maxil-lary incisors (crowding, ectopic eruption,trauma, early loss of primary or perma-nent teeth), which inter feres withmandibular closure, displacing it anteri-orly; in general, the problem is solvedafter removal of the interference. Thetrue Class III involves a skeletal Class IIIpattern in centric relation.1 As men-tioned by Bench et al,2 the true Class IIIshows a genetic trend toward extremeupward and backward condylar growth,
anterior crossbite, null overbite or openbite, and dolichofacial pattern, whichcontraindicates its correction by down-ward and backward mandibular rotation.The clinician should determine if there isanother family member with the samemalocclusion to help in the diagnosis.
According to Bench et al2 and Fränkeland Fränkel,3 the anterior crossbitecaused by interferences (pseudo ClassIII) may lead to upward and backwardcondylar growth with downward and for-ward mandibular displacement, givingrise to a true Class III because of inade-quate growth stimulus. Gianelly et al1
stated that even though this relationshipmay not be clear, it is advisable to adoptthe idea that prevention would be thebest option and thus perform early cor-rection of the crossbite.
1Resident, Department of Orthodon-tics, Methodist University of SãoPaulo, Brazil.
2Professor, Postgraduate Program inDentistry, Department of Orthodon-tics, Methodist University of SãoPaulo; Professor, Discipline of ChildClinic, Dental School, Methodist University of São Paulo, Brazil.
3Professor, Human CommunicationDisturbances, University Federal ofSão Paulo (UNIFESP); Chair and Professor, Postgraduate Program inDentistry, Department of Orthodon-tics, Methodist University of SãoPaulo, Brazil.
4Coordinator, Postgraduate Programin Dentistry, Department of Ortho-dontics, Methodist University of SãoPaulo, Brazil.
CORRESPONDENCEDr Márcio Antonio de FigueiredoRua Capitão Nascimento Filho,131–VergueiroCep.18030-123Sorocaba, SPBrazilE-mail:[email protected]

The true Class III malocclusion mayalso be called skeletal due to the involve-ment of skeletal structures; it may becaused by maxillary retrusion, mandibu-lar protrusion, or a combination ofboth.1,4–6 Frequently, there is also maxil-lary constriction,1,2 represented by poste-rior crossbite.
There are 3 options for the treatmentof skeletal Class III malocclusion: ortho-pedic, compensatory, or surgical. Selec-tion of treatment type is based on thediagnosis, especially the indication ofheredity, facial pattern, age, gender,severity of the problem, and patient com-pliance.
Turpin7 and Campbell8 mentioned pos-itive and negative factors for the intercep-tive treatment of Class III malocclusion.Positive factors are convergent facial pat-tern (brachyfacial), anterior functionaldeviation (difference between centricrelation and maximum intercuspation),symmetric condylar growth, growing sta-tus, ANB angle less than or equal to –2degrees, expectation of good compli-
ance, absence of hereditary involvement,and good facial esthetics. Negative fac-tors include divergent facial type(dolichofacial), absence of anterior func-tional deviation, asymmetric growth, non-growing status, ANB angle larger than –2degrees, expectation of poor compliance,familial history, and unpleasant facialesthetics.
According to Langlade,9 during normalgrowth, the amount of growth of the cra-nial base is nearly equivalent to that ofthe mandibular body; in the surgicalClass III syndrome there is hypodevelop-ment of the cranial base, exaggeratedmandibular growth (3.5 mm per year, asanalyzed by the facial axis). In addition tothis growth, the patient with a Class IIImalocclusion may be in a growth periodfor up to 16 years for females and 20years for males.
As mentioned by Gianelly et al,1 ortho-pedic treatment of Class III malocclusionin the permanent dentition is more diffi-cult. Thus, treatment should be per-formed early whenever possible.
2
Figueiredo et al WORLD JOURNAL OF ORTHODONTICS
Fig 1 Initial photographs taken onDecember 1992. (a,b) Frontal and lat-eral views of the face. (c to e) Posteriorand anterior crossbite.
a b
c d e

3
VOLUME 8, NUMBER 1, 2007 Author et al
CASE REPORT
Patient LRJ, a male 13 years of age,requested treatment at the authors’clinic, with referral to facial orthopedictreatment. He and his parents broughtrecords taken 2.5 years earlier (cephalo-metric radiograph, panoramic radio-graph, dental casts, extraoral and intrao-ral photographs). Anamnesis revealedthat the patient was being treated with aFränkel appliance (FR-3)3; the initialrecords of the patient showed a skeletalClass III malocclusion, as observed on
the extraoral and intraoral photographs,dental casts (Figs 1 and 2), and thecephalometric analysis (Figs 3 and 4,Table 1).
The patient was asked to interrupt useof the Fränkel appliance and obtain newrecords for reevaluation of the case.These records revealed lack of space forthe maxillary right canine, which wasunerupted and impacted (Fig 5), and thepresence of a skeletal Class III malocclu-sion with an anterior edge-to-edge rela-tionship and posterior open bite (Fig 6).
Fig 2 Initial dental casts.
Fig 3 Initial cephalometric radiograph.
Fig 4 Initial cephalometric analysis,using Ricketts method.

4
Figueiredo et al WORLD JOURNAL OF ORTHODONTICS
Fig 5 Panoramic radiograph confirming presence of the maxillaryright canine, unerupted and impacted.
Table 1 Cephalometric analysis
Patient Normative value
SNA (degrees) 85 82SNB (degrees) 101 80ANB (degrees) 5 2Cranial deflection (degrees) 31 27Anterior cranial base (mm) 54 55Posterior cranial length (mm) 27 41Mandibular body length (mm) 72 64.2Facial depth (degrees) 100 86.7Convexity (mm) 5 0.1Facial axis (degrees) 96 93Growth pattern Brachyfacial
Fig 6 Photographs taken on October 1995, when treatment was initiated with fixed orthodontics. (a to c) Frontal, smiling,and lateral views of the face. (d to f) Anterior edge-to-edge bite and posterior open bite.
d
a b
e
c
f

5
VOLUME 8, NUMBER 4, 2007 Figueiredo et al
The lateral cephalogram (Figs 7 and 8)was taken with the patient in the edge-to-edge position, which masked somecephalometric measurements (SNB, 86degrees; ANB, 1 degree; facial depth, 96degrees; convexity, 1 mm; facial axis, 90degrees) because of the downward andbackward mandibular rotation; however,the internal structures revealed signs of aClass III malocclusion, according toLanglade,9 including increased cranialdeflection (32 degrees), reduced poste-r ior cranial length (30 mm), andincreased mandibular body length (81mm). This information confirmed thepresence of a skeletal Class III malocclu-sion and the brachyfacial growth pattern.
Evaluation of the linear measure-ments, using the McNamara10 analysis,revealed the presence of a Class III mal-occlusion with mild maxillary retrog-nathism and mandibular prognathism.
Analysis of the mandibular dentalcasts was done according to Ricketts.11
Even though the measurements wereincreased when compared to normativevalues, they were considered normal, dueto the patient’s large tooth size.
Treatment plan
There were 2 treatment options for theskeletal problem: (1) orthodontic treat-ment with orthognathic surgery and (2)compensatory orthodontic treatment.Orthodontic compensation was selectedby consensus between parents and ortho-dontist, especially due to the patient’sage, which contraindicated surgery.According to Gianelly et al,1 an orthopedicapproach is the first option until pubertyis reached. Pinho et al12 mentioned costreduction and potential risk associatedwith orthognathic surgery as advantagesto the orthopedic approach [AU: editokay?], and the involvement of estheticappearance and potential of occlusalinstability as disadvantages. McNamaraand Brudon5 highlighted that early correc-tion of the Class III malocclusion mightlead to the need for surgical correctionlater, and that a careful specialist shouldnever guarantee the Class III correction,since the individual long-term result ofsuch treatment is difficult to forecast.
The lack of space for eruption of themaxillary right canine led to 3 treatmentoptions: (1) extraction of the impactedcanine; (2) extraction of 1 premolar onthe same side, to achieve space fororthodontic extrusion of the canine; or(3) orthodontic space opening. The thirdoption was selected because the skeletalClass III malocclusion may be worsenedby the extraction of a maxillary tooth.
Fig 7 Cephalometric radiographtaken on August 1995.
Fig 8 Cephalometric analysis, byRicketts method, done beforeonset of treatment with fixedorthodontics.

Treatment
Treatment was performed within the prin-ciples of Ricketts’ bioprogressive therapy,with use of the following appliances:Hyrax rapid maxillary expander (Fig 9),Petit face mask, mandibular bite block torelease the occlusion, chin cap, utilityarches, segmented arches (Fig 10), andideal arches.
The expander was activated 10 turns(nearly 1 cm per turn [AU: correct?]). Theface mask was placed immediately after final-ization of rapid maxillary expansion, deliver-ing nearly 900 kgf with 2 elastics 5/16-inch(8 oz) placed on each side of the mask.
The chin cap was worn by the patientduring sleep, throughout the treatmentand follow-up years until he reached 20years of age, with a force of 250 kgf. Useof the chin cap may have helped in themandibular posterior positioning in thetemporal fossa, followed by downwardand backward rotation. According toGianelly et al,1 mandibular posteriorrepositioning and rotation are importantcomponents of the response to Class IIItreatment, and a successful treatment israrely achieved if such repositioning doesnot occur. The final result is shown inFigs 11 and 12.
6
Figueiredo et al WORLD JOURNAL OF ORTHODONTICS
Fig 9 (a,b) Occlusal view of the maxilla before and soon after rapid expansion. (c) Intraoral frontal view after rapid maxillaryexpansion; maxillary left central and lateral incisors connected to the Hyrax with a ligature wire 0.25 inches, so that the transep-tal fibers would allow closure of the anterior diastemas for correction of the midline and space opening for the maxillary right[AU: Should this be left?] canine.
Fig 10 (a to c) Right, frontal, and leftintraoral view of the patient with thedouble-T segmented arch for levelingand expansion of mandibular premo-lars. (d) Triple-T segmented arch forleveling of the maxillary right first andsecond premolars and first molar andextrusion of the maxillary right canine.
a b c
a b
c d

7
VOLUME 8, NUMBER 4, 2007 Figueiredo et al
Fig 11 Final intraoral and extraoralphotographs following removal of theappliances on December 18, 1998(patient was 16 years 3 months of age).
Fig 12 Final panoramic radiograph reveals normality (mandibular third molarswere extracted during the treatment).

DISCUSSION
Analysis of the results through cephalo-metric analysis (Figs 13 and 14) reveal
skeletal and dentoalveolar alterationsthat can be described by the superimpo-sition method of Ricketts.13
8
Figueiredo et al WORLD JOURNAL OF ORTHODONTICS
Fig 13 Final cephalometric radio-graph.
Fig 14 Final cephalometric analysis,using Ricketts method.
Fig 15 (a to c) Cephalometric superimposition using the basion-nasion plane with center in point Cc (T1, yellow; T2, orange;T3, green).
Fig 16 (a to c) Basion-nasion-point A superimposition with center in nasion.
a b c
a b c

9
VOLUME 8, NUMBER 4, 2007 Figueiredo et al
Evaluation of skeletal and dentoalveolar changes
The skeletal and dentoalveolar changesdiscussed below occurred betweenDecember 1992 (T1, treatment withFränkel FR-3), July 1995 (T2, treatmentonset), and January 1999 (T3, treatmentcompletion).
Basion-nasion plane with center inpoint Cc (Fig 15). The facial axis wasopened 6 degrees (downward and back-ward mandibular rotation) between T1and T2, and was closed 3 degreesbetween T2 and T3, yielding an openingof 3 degrees in the period between T1and T3. Analysis of these data revealsthat the Fränkel FR-3 appliance yieldeddownward and backward mandibularrotation; after interruption of the FR-3use, the mandible showed upward andforward rotation, despite the use of extru-sion mechanics (Hyrax, Petit face mask).This effect, to a large extent, may be dueto the brachyfacial pattern.
Finally, this result (opening of thefacial axis) helped in the correction of theClass III malocclusion, yielding downwardand backward mandibular rotation.According to Gianelly et al,1 when there isa deep bite, the occlusal complex mayshow the effect of bite opening resultingfrom mandibular rotation. Therefore,these mechanics may be successfullyemployed in brachyfacial patients withClass III malocclusion since, when themandible is rotated in a downward andbackward direction and the anterior openbite is corrected, a favorable overbite isachieved, increasing the outcome stabil-ity. On the other hand, dolichofacialpatients do not have a favorableresponse, since this downward and back-ward mandibular rotation gives rise toanterior open bite, which is not ideal forthe esthetics and function of the patient.1
Basion-nasion-point A with center innasion (Fig 16). During the period fromT1 to T2 and T1 to T3, there was onlymild anterior maxillary displacement,which may have occurred due to the stim-ulation of maxillary development pro-vided by the Fränkel FR-3 appliance3 orby normal growth itself since, as shownby Baik et al,14 the orthopedic effects inthe maxilla with use of the Fränkel FR-3appliance are mild.
Between T2 and T3, there was noalteration in horizontal maxillary position-ing, even though the Petit face mask wasapplied with orthopedic force. This maybe explained by the bone maturation ofthe patient, which reduced the skeletaloutcomes.
The rhythm of maxillary vertical growthwas more remarkable in the period dur-ing which the patient was treated withthe Fränkel appliance (T1 and T2). Thiswas reduced when treatment was per-formed with fixed appliances (T2 and T3),thus keeping normal values (1.16 mmper year), as shown in the periodbetween T1 and T3.
Palatal plane with center in anteriornasal spine (Fig 17). Between T1 andT2, the maxillary incisors were retruded(1 mm) and extruded (0.5 mm). Thisalteration in positioning of the incisorswas not favorable for the Class III treat-ment, since it worsened the overjet.Between T2 and T3, the incisors wereadvanced 4 mm and intruded 1 mm.Analysis of this period reveals that thisadvancement had a favorable effect ofcompensatory treatment of the skeletalClass III malocclusion. In the periodbetween T1 and T3, there was 3 mm ofadvancement and 0.5 mm of intrusion.
The maxillary molars were extruded 4mm between T1 and T2 and did not showmesial movement, which are both unfa-vorable treatment sequelae for the cor-
Fig 17 (a to c) Superimposi-tion on the palatal plane (ENA-ENP) with center in the ante-rior nasal spine.
a cb

rection of the Class III malocclusion.Between T2 and T3, the maxillary molarsshowed 1 mm of mesial movement and 1mm of extrusion. Between T1 and T3, themaxillary first molars did not show mesialmovement; since this is a Class III maloc-clusion, this is not a good result, yet itshould be highlighted that at treatmentonset there was lack of space for eruptionof the right maxillary canine, which requiredblockage of the maxillary first molars forachievement of space for eruption. Themaxillary first molars also erupted 5 mm.
Plane Xi-Pm [AU: What is this plane?Please spell out, as abbreviations arenot familiar ones] with center in Pm,
supra-pogonion (Fig 18). During theperiod from T1 to T2, the mandibular firstmolars had 4 mm of extrusion and 1.5mm of uprighting, a favorable alterationfor Class III treatment. Between T2 andT3, the molars had nearly no movement,as observed in Fig 18b. This blockageoccurred due to the mechanics employed(utility arches), since in normal conditionsthese teeth erupt 0.5 mm per year. Inves-t igation of the changes occurringbetween T1 and T3 reveal 4 mm of extru-sion, a normal amount for the 6-yearperiod. The same first molars presented2 mm of uprighting, which was beneficialfor the treatment.
10
Figueiredo et al WORLD JOURNAL OF ORTHODONTICS
Fig 19 (a to c) Superimposition on intersection of the esthetic plane with the functional occlusal plane.
Fig 18 (a to c) Superimposition on Plane Xi–Pm (supra-pogonion) with center in point Pm.
cba
a b c
11
VOLUME 8, NUMBER 4, 2007 Figueiredo et al
The mandibular incisors wereextruded 3 mm and advanced 1 mm inthe period between T1 and T2, whichwas not favorable, since it worsens theoverjet and overbite. Between T2 and T3,the incisors were retracted 1 mm andblocked in vertically. Between T1 and T3,the incisors moved distally 2 mm and 3mm vertically. This movement was proba-bly related to the effect of the compen-satory treatment performed.
Esthetic plane (E) in intersectionwith the occlusal plane (Fig 19). Duringthe period T1 to T2, the lower lip was low-ered and there was mild posterior reposi-tioning due to the downward and back-
ward mandibular rotation; the upper lipwas advanced, probably due to the effectof the Fränkel FR-3 appliance. These mildchanges favored an improvement in thesoft-tissue profile.
Between T2 and T3, the lower lip wasmildly displaced backward and downwardbecause of retraction of the mandibularincisors, whereas the upper lip showedonly downward movement. These mildchanges improved the soft-tissue profile,as can be seen in Fig 19b.
Between T1 and T3, the changes aremore evident: The upper and lower lipsshow downward displacement becauseof opening of the facial axis (downward
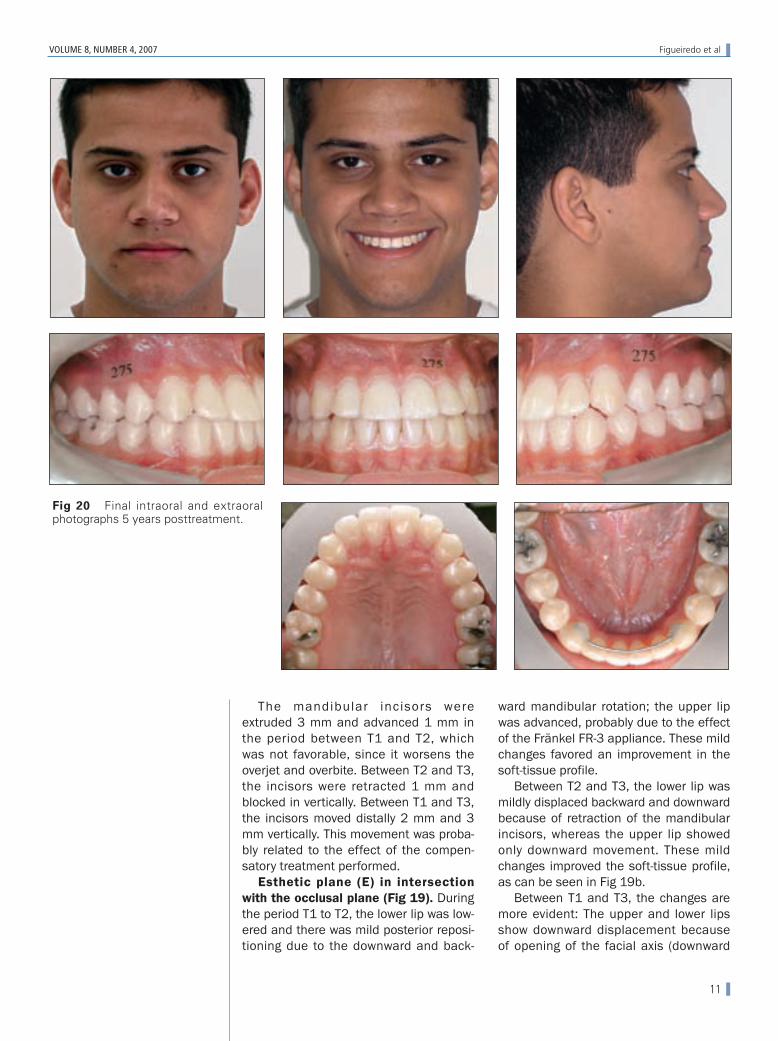
Fig 20 Final intraoral and extraoralphotographs 5 years posttreatment.

and backward mandibular rotation). Theupper lip was advanced and the lower lipwas retruded, following the movement ofthe incisors, resulting in an improvedsoft-tissue profile.
The stability of the compensatorytreatment, as well as the adequateesthetics from both facial and dentalviewpoints, can be seen in Fig 20, taken5 years after treatment completion.
CONCLUSION
This article investigated the dentoskele-tal and soft-tissue alterations occurringduring compensatory treatment of ClassIII malocclusion, by the superimpositionmethod of Ricketts.13 These alterationsincluded downward and backwardmandibular rotation (opening of facialaxis, 3 degrees), mild maxillary advance-ment (1.5 degree increase in the angleBa-Na-A), advancement of maxillaryincisors, retraction of mandibularincisors, and uprighting of the mandibu-lar first molars.
Selection of the compensatory treat-ment (orthodontic camouflage) was satis-factory based on the final outcome, fromboth functional and esthetic standpoints,and the treatment stability at 5 yearsposttreatment.
REFERENCES
1. Gianelly AA, Bednar J, Cociani S, Giancotti F,Maino G, Richter O. Bidimensional technique:Theory and practice. Islandia, NY: GAC Interna-tional, 2000:128–141.
2. Bench RW, Gugino CF, Hilgers JJ. Bioprogressivetherapy part 8: Bioprogressive mixed dentitiontreatment. J Clin Orthod 1978;12:279–298.
3. Fränkel R, Fränkel C. Orofacial orthopedics withthe function regulator. Basel: Karger, 1989:36–38, 190–211.
4. Guyer EC, Ellis EW, McNamara JA Jr, BehrentsRG. Components of Class III malocclusion injuveniles and adolescents. Angle Orthod 1986;56:7–31.
5. McNamara JA Jr, Brudon WL. Tratamientoortodóncico y ortopédico en la dentición. AnnArbor: Needham, 1995:121–133.
6. Seher GA, Jalan DK, Sedat B. Correction of asevere Class III malocclusion. Am J OrthodDentofacial Orthop 2004;126:237–244.
7. Turpin DL. Early Class III treatment. [unpub-lished thesis]. Presented at 81st session of theAmerican Association of Orthodontists, SanFrancisco, 1981.
8. Campbell PM. The dilemma of Class III treat-ment. Angle Orthod 1983;53:175–191.
9. Langlade M. Diagnostic orthodontique. Paris:Maloine, 1981:245–301, 696–714.
10. McNamara JA Jr. A method of cephalometricevaluation. Am J Orthod 1984;86:449–469.
11. Ricketts RM. Provocations and perceptions incraniofacial orthopedics. Glendora, CA: RMO,1989:735, 817–818.
12. Pinho TMC, Torrent JMU, Pinto JGRC. Orthodon-tic camouflage in the case of a skeletal Class IIImalocclusion. World J Orthod 2004;5:213–223.
13. Ricketts RM. A four-step method to distinguishorthodontic changes from natural growth. J ClinOrthod 1975;9:208–228.
14. Baik HS, Jee SH, Lee KJ, Oh TK. Treatmenteffects of Fränkel functional regulator III in chil-dren with Class III malocclusions. Am J OrthodDentofacial Orthop 2004;125:294–301.
12
Figueiredo et al WORLD JOURNAL OF ORTHODONTICS