1-s2.0-s2212267213005182-main
DESCRIPTION
cortoTRANSCRIPT
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 19
RESEARCHResearch and Practice Innovations
An Overview of Short Bowel Syndrome Management
Adherence Adaptation and PracticalRecommendationsElizabeth A Wall MS RD LDN
ARTICLE INFORMATION
Article historyAccepted 30 April 2013Available online 3 July 2013
KeywordsPathophysiology of short bowel syndromeMedical nutrition therapy
Clinical management of patients with short bowelsyndrome
Copyright ordf 2013 by the Academy of Nutritionand Dietetics2212-2672$3600doi101016jjand201305001
ABSTRACTShort bowel syndrome (SBS) refers to the clinical consequences resulting from loss of small bowel absorptive surface area due to surgical resection or bypass The syndrome ischaracterized by maldigestion malabsorption and malnutrition Survival of patientswith SBS is dependent on adaptation in the remaining bowel and a combination of pharmacologic and nutrition therapies Individual plans of care are developed based onthe length and sites of remaining bowel the degree of intestinal adaptation and the
patientrsquos ability to adhere to the medication and dietary regimens Antisecretory andantidiarrheal medications are prescribed to slow intestinal transit times and optimize1047298uid and nutrient absorption Based on postsurgical anatomy enteral feedings paren-teral infusions complex diet plans and vitamin and mineral supplementation are usedin various combinations to nourish patients with SBS In the acute care setting regis-tered dietitians (RDs) assist with infusion therapy diet education and discharge plan-ning Long-term as the small intestine adapts RDs revise the nutrition care plan andmonitor for nutrient de1047297ciencies metabolic bone disease and anemia The frequentmonitoring and revision of care plans plus the appreciable bene1047297ts from propermedical nutrition therapy make this patient population extremely challenging andrewarding for RDs to manage This article provides a brief case study-based overview of the medical and nutrition management of SBSJ Acad Nutr Diet 20131131200-1208
SHORT BOWEL SYNDROME (SBS) REFERS TO THEclinical consequences resulting from loss of smallbowel absorptive surface area due to surgical resec-tion or bypass The syndrome is characterized by
maldigestion malabsorption and malnutrition The mostcommon causes of SBS in adults are small bowel resectionsfrom strangulated bowel Crohnrsquos disease ischemia traumaor malabsorptive weight loss surgery1 The metabolic conse-quences of removing the small intestine are variable anddepend on a number of factors including the length condi-tion and sites of remaining small bowel23 Survival of a pa-
tient with SBS is dependent on adaptation in the remainingbowel and a combination of pharmacologic and nutritiontherapies This overview covers the pathophysiology of SBSmedical and nutrition management and provides practicaladvice for clinicians who encounter patients with SBS
PATHOPHYSIOLOGYNormal length of the small intestine varies from 300 to 600cm approximately half of the upper intestine (jejunum) canbe removed without signi1047297cant problems Patients with lt100cm of small intestine will have severe malabsorption whichwill result in malnutrition if untreated There are two clini-cally useful categories of patients with SBS those with a
colon in continuity with the remaining small bowel and thosewith a small bowel ostomy The presence of the ilealcecalvalve and colon even with as little as 50 cm of small bowelmarkedly improves 1047298uid and electrolyte absorption as well asuptake of short-chain fatty acids and often allows for survivalwithout arti1047297cial nutrition support4 When the small bowelis lt100 cm to an end jejunostomy or ileostomy parenteralnutrition (PN) and hydration will likely be needed forsurvival45
Consideration of the site of small bowel resection isimportant in determining the extent of metabolic conse-
quences The duodenum and jejunum are the primary sites of protein carbohydrate fat water-soluble vitamin and mineralabsorption (particularly calcium iron and folate) as well asthe mixing site of pancreatic and biliary secretions Resectionof the ileum particularly the terminal ileum is more detri-mental than loss of jejunum because it is the only site forabsorption of intrinsic factor-bound B-12 and bile salts If gt100 cm of distal ileum is removed then enterohepatic cir-culation of bile salts is disrupted resulting in severe fatmalabsorption and steatorrhea6 The distal ileum is also animportant regulator of gastric emptying and small boweltransit time7 Loss leads to rapid gastric emptying and rapidsmall bowel transit similar to the dumping syndrome
1200 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS ordf 2013 by the Academy of Nutrition and Dietetics
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 29
After surgical resection the remaining small bowel un-dergoes an adaptation process that involves morphologic andfunctional changes8 The small bowel dilates and the villiheight and crypt depth increase expanding the absorptivesurface area of the small bowel without change in length9
The mechanism of adaption is not fully understood Impor-tant factors include hormonal growth factors nutrients
(particularly complex macronutrients) bile and pancreaticsecretions and local intestinal hormones such as glucagon-like peptide 210 Adaptation begins soon after intestinalresection and may continue for 2 years11 Because oral nu-trients stimulate intestinal adaptation it is important toinitiate an oral diet or enteral feedings as soon as possibleafter surgery12
MANAGEMENT OF SBSThe goal of therapy is to maximize small bowel absorption of 1047298uids and nutrients to prevent de1047297ciencies and dehydration12
This is accomplished by controlling the rate at which nutri-ents and 1047298uids move through the intestinal tract with the useof medications and diet therapy In some cases infusiontherapy (enteral andor parenteral) with nutrients and 1047298uidmay be required either temporarily after surgery or lifelong1
PharmacotherapyThe common categories of medications used to manage SBSinclude antimotility agents antisecretory agents and paren-teral infusion therapy (intravenous [IV] 1047298uids andor PN)1
Antimotility medications (the most common are loperamidediphenoxylate and atropine codeine and deodorized tinctureof opium [DTO]) are used to slow peristalsis and improve ab-sorption of 1047298uid electrolytes and nutrients13 These medica-tions are usually taken as needed after a loose bowelmovement but for patients with SBS the dose is given
routinely 30 minutes before meals and at bedtime Often pa-tients with SBS have to adjust the timing and titrate the dose of antimotility agents based on meal composition daily activitiesand degree of bowel adaptation Patients taking opiate-basedmedications to control 1047298uid and electrolyte losses (codeineand DTO) must be closely monitored for side effects includingimpaired mental or physical alertness as well as symptoms of withdrawal if the medications are abruptly discontinued afterprolonged use14 Clonidine an a2-adrenergic agonist has beenshown to increase intestinal transit time and decrease fecalweight in patients with SBS15-17 It can be administered by oralmedication or transdermal patch which is an effective alter-native for patients with reduced small bowel absorptionClonidine is commonly used to treat hypertension so bloodpressure should be monitored closely when starting thismedication Patients with severe coronary heart diseasechronic renal insuf 1047297ciency and hemodynamic instability maynot be good candidates for clonidine therapy14
Hypersecretion of gastrin and gastric acid occurs in pa-tients after extensive small bowel resection18 Histamine H2
antagonists (ie H2 blockers) and the more potent protonpump inhibitors (PPIs) are used in SBS to decrease gastric acidsecretion diarrheal losses and risk for peptic ulcer diseaseand its complications The H2 blockers inhibit histamine atthe histamine H2 receptors of gastric parietal cells thusreducing gastric acid secretion whereas PPIs directly inhibithydrogen potassium ATPase pump of parietal cells effectively
stopping acid secretion14 Somatostatin analogues inhibit therelease of gastrointestinal hormones and reduce secretion of intestinal and pancreatic 1047298uids which reduces diarrhea inpatients with SBS14
In some cases pancreatic enzyme replacement and bile acidsequestrants may be used to control maldigestion and diar-rhea13 Exogenous pancreatic enzyme mixing with food in the
stomach can increase nutrient absorption in patients withrapid small bowel transit and poor intestinal mixing of chymewith pancreatic secretions Bile acid sequestrants can helpalleviate choleretic diarrhea that occurs when distal ilealresection disrupts enterohepatic circulation of bile salts1
Small bowel bacterial overgrowth can occur in conjunctionwith SBS and is related to alterations of intestinal anatomymotility and gastric acid suppression1920 Bacteria in thesmall bowel can deconjugate bile acids which may worsendiarrhea and malabsorption20-22 Treatments for bacterialovergrowth include antibiotics probiotics and bile acidsequestrants23 Often broad spectrum antibiotics are cycled(alternating 1 or 2 weeks of treatment with an antibiotic withseveral weeks off antibiotic therapy) to prevent or delay
antibiotic resistanceParenteral infusion therapy is often needed immediately
after surgery to maintain 1047298uid and electrolyte balance asbowel function returns12 IV support can vary from saline orlactated ringerrsquos infusions to full PN support (IV 1047298uids thatcontain both macro- and micronutrients) The degree of bowel adaptation will dictate the length of IV therapy A goodguideline is that patients with SBS with gt15 L stool outputand lt800 mL urine output in 24 hours will have dif 1047297cultymaintaining hydration and electrolyte balance without someIV 1047298uid support3
Medical Nutrition Therapy
The macronutrient distribution of diets for SBS will varydepending upon the sites and length of remaining bowel(Figure 1) In small clinical studies patients with end jeju-nostomies have improved energy absorption and similar stoollosses with moderately high amounts of fats and dietary 1047297berwhen compared with diets high in complex carbohydrates(CHO) alone24-27 The optimal diet includes generous amountsof complex CHO and fats with a macronutrient distribution of approximately (50 CHO 20 to 30 protein and40 fat)28
Foods rich in water-soluble 1047297ber can slow both gastricemptying and intestinal transit time thicken ostomy ef 1047298uentand promote intestinal adaptation2429 It is best to minimize1047298uid intake with solid food meals beverages should be sippedcontinuously between meals3031 Avoidance of foods andbeverages high in simple sugars may alleviate dumping of hypertonic chyme into the intestine Patients should eat fourto six small meals a day Another important goal for patientswith SBS and jejunostomies is to maximize 1047298uid uptake by thesmall intestine This is best achieved by utilizing the sodium-glucose cotransport system to pull water across the epitheliallining32-35 Liberal use of salt on food and sipping oral rehy-dration solutions (ORS) between meals (1 to 2 Lday) haveshown to be bene1047297cial332
Patients with an intact colon bene1047297t from a diet higher incomplex CHO and moderate in fat (50 to 60 CHO 20 to30 protein and 20 to 30 fat) divided into three smallmeals plus two to three snacks per day2729 The rationale for
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1201
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 39
emphasizing complex CHO and less fat is twofold Firstcolonic bacteria can metabolize undigested CHO includingdietary 1047297ber to short-chain fatty acids leading to salvageabsorption and net increase energy sodium and water up-take2533 Second steatorrhea from poorly absorbed dietaryfats and increased risk of oxalate absorption in the colon mayresult in calcium oxalate kidney stone formation436 A dietlow in fat and oxalate along with calcium supplementationat meals can reduce the risk of kidney stone formationConsumption of salty foods and ORS is not as important forpatients with SBS who have an intact colon as long as foodand 1047298uid intake is spread throughout the day24
Enteral nutrition (EN) support alone or in combinationwith an oral diet has proven to increase absorption of mac-ronutrients in patients with and without colonic continuity Joly and colleagues37 demonstrated that continuous naso-gastric feedings with a polymeric formula in patients withSBS signi1047297cantly (P lt0001) increased absorption of proteinsfats and energy compared with an isocaloric oral diet This
enhanced nutrient absorption may be related to continuousinfusion of isotonic nutrients which is better tolerated withaltered gut anatomy when compared with bolus infusion of feedings or food The continuous bathing of the gut withmacronutrients may promote release of pancreatic and in-testinal enzymes as well as intestinal hormones that enhancebowel adaptation and overall absorption EN is less expensiveand presents lower overall risks than PN In SBS the use of ENcan facilitate reduction in the number of PN infusions eachweek andor complete weaning from PN therapy altogether
Micronutrient requirements will vary among patientsdepending upon the sites of remaining intestine All patientswith SBS should take a daily multivitamin with minerals bymouth (preferably chewable or liquid) or IV Routine moni-
toring of serum vitamin B-12 and methylmalonic acid (amarker of vitamin B-12 status) levels is required for any pa-tient with a distal ileum resection or small bowel bacterialovergrowth supplementation may be required2138-40 Diva-lent cations mainly calcium magnesium and zinc can bede1047297cient in patients with SBS and many will require sup-plementation1 This may be related to lack of absorptivesurface rapid transit time and binding with unabsorbed fatin the intestinal lumen Cautious supplementation of mag-nesium is advisable because oral magnesium preparationsare dif 1047297cult to absorb and therefore have cathartic effectsSlow-release magnesium chloride magnesium gluconate ormagnesium lactate preparations can reduce some of thegastrointestinal symptoms related to oral magnesium inges-
tion13 Practitioners should be cognizant that osteoporosisanemia and fat-soluble vitamin de1047297ciencies are common inpatients with SBS and long-term monitoring is necessaryIndividual vitamin and mineral supplements should be pre-scribed as needed38 The following case highlights theimportance of comprehensive medical management of pa-tients with SBS and provides an opportunity to discusspractical clinical applications
PATIENT PROFILEThe patient is a 72-year-old woman with a past medicalhistory of colon cancer that was treated by partial colectomyand chemotherapy Recurrent colon cancer was diagnosed 11years later requiring a complete colectomy with end ileos-tomy Postoperative Day 3 she developed severe abdominalpain and blood-tinged ostomy ef 1047298uent re-exploration sur-gery demonstrated extensive distal small bowel necrosis Thenecrotic bowel was resected leaving an estimated 105 cm of proximal small bowel to an end jejunostomy The patient rsquosrecovery was uneventful she was discharged from the hos-pital on a regular diet
During the 1047297rst month after discharge from the hospitalthe patient had multiple admissions for dehydration andweight loss During one such hospitalization a double-lumenperipherally inserted central catheter (PICC) was placed andPN initiated Soon after the start of therapy she developed an
Nutrient
Small bowel
ostomy
Colonic
continuity
Carbohydrates 50 of total
energy complex
carbohydrates
including soluble
1047297ber limit simple
sugars
50-60 of total
energy complex
carbohydrates
including soluble
1047297ber
Proteins 20-30 of total
energy
20-30 of total
energy
Fats 40 of total
energy
20-30 of total
energy
Fluids ORSb important
minimize 1047298uids
with meals
sipping of 1047298uids
between meals
Minimize 1047298uids
with meals
sipping of 1047298uids
between meals
Vitamins Daily multiple
vitamin with
minerals monthly
B-12 possibly
vitamins A Dc
and E
supplements
Daily multiple
vitamin with
minerals possibly
B-12 possibly
vitamins A D and
E supplements
Minerals Generous use of
sodium chloride
on food calcium
1000-1500 mg
daily possibly
iron magnesium
and zinc
supplements
400-600 mg
calcium with
meals possibly
iron magnesium
and zinc
supplements
reduced oxalate
Meals 4-6 small meals 3 small meals plus
2-3 snacks
aBased on references 24 47 and 60bORSfrac14oral rehydration solutionc25-hydroxy vitamin D
Figure 1 Medical nutrition therapy for short bowel syndromea
RESEARCH
1202 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 49
upper extremity deep vein thrombosis originating at the PICCinsertion site anticoagulation therapy was started Duringthe same hospitalization she developed fevers due to acatheter-related blood infection hypotension hypokalemiaand increased liver function tests On Hospital Day 17 thepatient was transferred to a tertiary care hospital for man-agement of SBS
TERTIARY CARE CENTER COURSEThe PICC was pulled and the patient was given a central lineholiday while antibiotic therapy was completed PeripheralPN (1 L 50-g dextrose and 20-g amino acids without lipidemulsion due to an egg allergy) was initiated along withantisecretory (ie PPI) and antimotility (ie DTO) medicationsHer diet was changed to six small meals with sipping of ORSbetween meals On Hospital Day 9 a tunneled central cath-eter was placed and the PN formulation was increased to 50 gdextrose 80 g amino acids infusing over 10 hours each night(490 kcalday) After intensive diet and infusion therapy ed-ucation the patient was discharged to home with the samePN formula diet and medications
AT HOMEAt home the patientrsquos oral intake increased with subsequentincrease in jejunostomy output necessitating adjustment of the PN volume to 15 L infused over 12 hours and titration of the DTO dose to 1 mL four times a day Six months afterdischarge PN she had stable serum chemistry valuesadequate hydration and she was slowly losing weight thePN infusion was changed to every other day and the anti-coagulation therapy was discontinued Subsequent serumchemistry results suggested negative 1047298uid balance and thepatient complained of extreme thirst and fatigue A 24-hoururine collection during an off day from PN resulted in only
400 mL urine The PN volume was increased to 24L over 12hours every other day and the patient was instructed tostrictly adhere to the diet and ORS therapy The patient hadimproved hydration on noninfusion days and the repeat 24-hour urine collection yielded 850 mL
The patient remains on every-other-day IV infusions for1047298uid vitamins minerals and electrolytes her weight hasstabilized at 86 kg (body mass index 307) Four years afterdischarge on PN her insurance provider mandated a switchedto noneamino acid-containing IV 1047298uid (Table) She continuesto strictly adhere to the diet regimen but has ceased usingORS because she no longer appreciates hydration bene1047297tsfrom the therapy Repeat chemistry data including normalvitamin levels and triene to tetraene ratio (an indication of
adequate absorption of essential fatty acids) plus stable bodymass index suggest adequate hydration and nutrient uptakewith the current management
DISCUSSIONHistorically loss of a signi1047297cant portion of the intestine wasphysically devastating and often a death sentence During thepast 50 years with the advent of PN and a better under-standing of small bowel physiology most patients with SBSrecover and live without signi1047297cant reduction in quality of life41-44 The case of the patient provided is an excellentexample of the metabolic consequences of massive smallbowel resection and the complications of infusion therapy
Per the Nutrition Care Process this patient had alteredgastrointestinal function due to extensive intestinal resectionas evidenced by inability to maintain hydration on an oraldiet Through aggressive medical management strict dietaryadherence and appreciable bowel adaptation she hasreduced her dependence on IV support and ORS by approx-imately 80 The dietary key to her success was the transition
from eating two large meals a day and drinking large volumesof sugar-containing beverages to separating food and 1047298uidingestion eating four small meals daily limiting simple sugarintake and sipping ORS daily Through trial and error thepatient has re1047297ned her schedule for antisecretory and anti-motility medications to maximize 1047298uid and electrolyte ab-sorption With remnant bowel length of only 105 cm it isunlikely she will ever completely wean from infusion ther-apy but with the conversion to every-other-day IV infusiontherapy she reports improved quality of life
Like many patients receiving home PN this patient hashad complications related to infusion therapy including athrombosis around a PICC catheter-related blood infectionsand liver function abnormalities The incidence of catheter-
related complications has been minimized by using singlelumen tunneled catheters to minimize the diameter of thecatheter and reduce the risk of clot formation limiting accessfor bacterial introduction with a single lumen and by re-education in aseptic technique Her liver function hasreturned to normal with the reduction of PN support andfewer central line infections (a frequent cause of abnormalliver tests) She will require lifelong monitoring of overallhealth and nutrition parameters vitamin levels and tracemineral levels as well as bone and vital organ health Every6 months the patient returns to clinic for monitoring She hasdual-energy x-ray absorptiometry scans every 2 years toassess her risk of metabolic bone disease (postmenopausaland SBS-related) Her overall prognosis is excellent given her
signi1047297cant small bowel adaptation the low rate of central linecomplications and reduced dependence on IV support
PRACTICE APPLICATIONSManagement of patients with SBS requires a thorough un-derstanding of intestinal physiology knowledge of pharma-conutrition therapy (ie the use of nutrients for therapeuticbene1047297t) close attention to detail and patience Each SBSpatient presents with unique nutrient requirements based onthe length site and health of their remaining intestineWhen caring for a patient with SBS a registered dietitian(RD) must know the exact intestinal anatomy so that a plan of care is developed to optimize bowel function and nourish thepatient If the operative report is unavailable or there isquestion as to the length or health of the remaining bowel anupper gastrointestinal with small bowel follow-throughbarium study provides vital information on the length andcondition of intestine remaining as well as transit time45 Inaddition RDs must have accurate intake and output data toassess 1047298uid balance awareness of all prescribed medicationsand supplements knowledge of IV access including cathetertip location weight history and laboratory data
Before hospital discharge there are many details RDsmust ensure are in place for patients with SBS (Figure 2)First the patient must understand the proper diet and oralhydration guidelines as well as the dosage and timing of
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1203
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 59
Table Data for a 72-year-old female patient from hospital admission to 4 y after massive small bowel resection
Patient data
Transfer to
tertiary
care center
Time After Discharge
3 wk 55 mo 6 mo 65 mo 75 mo 4 y
Body mass index 353 350 325 325 315 307 307
Laboratory dataa
Glucose (65-110 mgdL)b 169 148 115 122 100 119 89
Sodium (136-144 mEqL) 138 137 138 144 140 140 141
Potassium (36-51 mEqL) 33 44 42 42 42 38 42
Chloride (101-111 mEqL) 95 103 105 102 103 105 105
Bicarbonate (22-32 mEqL) 35 26 26 29 33 30 29
Blood urea nitrogen (7-19 mgdL)c 22 37 28 22 26 22 21
Creatinine (050-15 mgdL)d 10 08 10 13 12 10 096
Calcium (86-106 mgdL)e 77 93 89 95 92 87 95
Phosphorus (24-47 mgdL)f 38 39 40 38 42 36 35
Magnesium (18-25 mgdL)g 19 22 22 21 22 22 23
Total protein (gdL)h 60 78 79 76 67 76
Albumin (gdL)i 29 33 45 40 39 40
Total bilirubin (0-13 mgdL) j 16 095 09 129 097 08
Alkaline phosphatase (38-126 IUL) 239 204 320 217 163 95
24-h urine volume (mL)k 400 850
Measured energy expenditure (kcald) 1794
Respiratory quotient 069
Medications
Warfarin (mg) 4 4 0 0 0 0 0
Proton pump inhibitor (mgd) 40 40 40 40 40 40 30Deoderized tincture of opium (mLday) 12 3 3 3 3 3 4
Oral multivitamin 0 0 0 1l 1l 1l 1l
Vitamin D-3 (IUd) 0 0 0 0 0 0 1000
Calcium carbonate (mgd) 0 0 0 0 0 0 500
Oral rehydration solution (Ld) 1 1 1 1 1 1 0
Parenteral nutrition volume (Ld) 1 15 15 2m 24m 24m 24m
Parenteral nutrition energy (kcald) 490 490 490 410m 410m 410m 170m
Parenteral nutrition amino acids (gd) 80 60 60 60m 60m 60m 0
aRanges shown in parentheses are reference rangesb To convert mgdL glucose to mmolL multiply mgdL by 00555 To convert mmolL glucose to mgdL multiply mmolL by 1801 Glucose of 65 mgdLfrac14361 mmolLc To convert mgdL blood urea nitrogen to mmolL multiply mgdL by 0357 To convert mmolL blood urea nitrogen to m gdL multiply mmolL by 280 Blood urea nitrogen of 7 mg
dLfrac14250 mmolLd To convert mgdL creatinine to mmolL multiply mgdL by 884 To convert mmolL creatinine to mgdL multiply mmolL by 001 Creatinine of 05 mgdLfrac14442 mmolLe To convert mgdL calcium to mmolL multiply mgdL by 025 To convert mmolL calcium to mgdL multiply mmolL by 4 Calcium of 86 mgdLfrac14215 mmolLf To convert mgdL phosphorous to mmolL multiply mgdL by 0323 To convert mmolL phosphorous to mgdL multiply mmolL by 309 Phosphorous of 24 mgdLfrac14078 mmolLg To convert mgdL magnesium to mmolL multiply mgdL by 0411 To convert mmolL magnesium to mgdL multiply mmolL by 243 Magnesium of 18 mgdLfrac1474 mmolLh To convert gdL total protein to gL multiply gdL by 10 To convert gL total protein to gdL multiply gL by 01 Total protein of 60 gdLfrac1460 gLi To convert gdL albumin to gL multiply gdL by 10 To convert gL albumin to gdL multiply gL by 01 Albumin of 29 gdLfrac1429 gL j To convert mgdL total bilirubin to mmolL multiply mgdL by 171 To convert mmolL total bilirubin to mgdL multiply mmolL by 058 Total bilirubin of 16 mgdLfrac142737 mmolLk 24-h urine volume collected on a day without parenteral nutrition infusionlOff parenteral nutrition daymEvery other day
RESEARCH
1204 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 69
antimotility and acid-blocking medications46 In additionthe patient should be aware that the dosage of the medi-cations may change once he or she is home and eatingmore food Emphasis should be placed on proper eatingtechniques for example eating slowly resting after eatingminimal 1047298uid intake with the meal and sipping of 1047298uidsbetween meals47 If an ORS is required recipes to preparethe solution or information on where to purchase ORSmust be given to the patient The RD may have to reinforcethis information repeatedly before and after dischargeAdults in particular have dif 1047297culty changing their eatinghabits and may 1047297nd it challenging to adhere to the newguidelines until they begin to see reduction in stool outputand improved overall sense of well-being Also the patient
must have prescriptions for antisecretory therapy (eitherPPI or H2 blocker) and vitamin and mineral supplements if needed For those discharged on PN the patient and familyrequire education on catheter care and aseptic techniquefor infusion therapy before discharge4849 Patient moni-toring of oral intake stool and urine output as well asweight in the early period after hospital discharge willfacilitate decisions regarding medication adjustments andpossibly weaning of EN or PN support The patient andfamily may require education on proper techniques formeasuring body 1047298uid output at home48 Nursing support inthe home can help to reinforce the concepts of SBS man-agement and provide RDs essential insight to the homeenvironment
Checklist item Acute care setting Home care setting
Diet education Educate and reinforce as diet is advanced
in the hospital
Reinforce and adjust diet as bowel adapts
Laboratory data Daily chemistry panel including magnesium
and blood count
Twice weekly liver function testsBaseline vitamin and trace mineral
levels (A E Db folate B-12 iron zinc
copper and selenium) before discharge
Weekly comprehensive metabolic panel
including magnesium until stable then monthly
Annually vitamin and trace mineral levels
Weights and IOc
data
Daily weight
Daily IO data
Weekly weight
Once weekly IO data until stable then monthly
(more frequently if change in medical
management or status)
Medications Antimotility agent
PPId or H2 blockere
Multivitamin and mineral supplements
Antimotility agent
PPI or H2 blocker
Multivitamin and mineral supplements
Possibly pancreatic enzyme replacement or bile
acid sequestrant
Nutrition support If on enteral nutrition then know the
type of tube and enteral formula
If parenteral nutrition know the type of
catheter the position of the catheter
tip and the formula
Note any additional intravenous 1047298uids
Talk to the patient andor caregiver
Communicate with the home care company any
changes in enteral or parenteral formulas
Obtain report from home nurse
Monitoring frequency Daily Weekly until stable then reduce frequency
as appropriate
Other Know the exact post-operative intestinal
anatomyCommunicate long-term plan with the
primary care physician prior to discharge
Monitor for bowel adaptation and make
alterations in MNT
f
as possibleScreen for bone disease and anemia
aBased on references 46 and 59b25-hydroxy vitamin DcIOfrac14intake and output Includes oral enteral and parenteral intake plus urine stool and drain outputdPPIfrac14proton pump inhibitoreH2frac14histamine 2 antagonistf MNT frac14medical nutrition therapy
Figure 2 Checklist for registered dietitian management of patients with short bowel syndromea
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1205
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 79
After hospital discharge patients with SBS are best servedby frequent follow-up appointments with all members of thenutrition support team in particular the managing physicianand RD The primary goals of these appointments are toassess adherence to the prescribed therapies monitor 1047298uidelectrolyte hydration and nutritional status reinforce theprinciples of nutrition therapy and adjust the therapies as
necessary
50
Periodic weights and blood chemistry levels(including liver function tests) will help to determine theextent of bowel adaptation liver-related complications of PNand the possibility of weaning from EN or PN48 If a patientdevelops PN-related liver disease the workup should assessfor small bowel bacterial overgrowth blood infection and re-evaluate IV fat emulsion deliverymdashall of which can alter liverfunction51 Treatment may include a reduction in the amountand frequency of IV fat emulsion infusions (lt1 gkgday asinfrequently as once a week) with periodic monitoring foressential fatty acid de1047297ciency52
Baseline vitamin (eg folate B-12 and vitamins A D E)mineral (eg iron calcium and magnesium) and trace mineral(eg zinc copper and selenium and chromium and manganese
for PN patients) levels and dual-energy x-ray absorptiometryscan are required for comparison purposes in long-term followup53 The standard parenteral multivitamin and trace mineraladditives may not meet a patientrsquos exact requirements and cancause de1047297ciency or toxicity states over time54 For exampledaily trace mineralinfusions of 03 mg manganese over timecanlead to deposits in the brain55 and chronic standard multivi-tamin dosing of 200 IU vitamin D can cause insuf 1047297ciency orde1047297ciency states56 Further complicating the issue of moni-toring micronutrient levels of patients dependent on PN are theongoing product shortages These shortages have led to omis-sion or rationing of certain nutrients that can cause life-threatening de1047297ciency states505758 These levels should becheckedno less than every 6 to 12 months or more frequently if
abnormal levels are identi1047297ed5859 With time as a patient sta-bilizes and thrives at home the length of time between clinicvisits can be extended For patients with stable chronic SBS theminimum follow-up should occur every 6 to 12 months As withthe patientpro1047297le provided bowel adaptation can occur slowlyIt can take more than 2 years before adaptation has fullyoccurred to change the treatment plan and wean arti1047297cialnutrition support11
CONCLUSIONSManagement of SBS is complex and requires a concert of medical nutrition and pharmaceutical therapies to optimize1047298uid and nutrient absorption for survival Each patientrsquos
unique care plan depends on the amount and site of remaining intestine and the patientrsquos ability to adhere to themedical and nutrition therapies Some patients will be able tosurvive with antisecretory and anti-motility agents alongwith strict diet adherence alone whereas other patients willrequire lifelong infusion therapy In either case patients withSBS must have close follow-up with a specialized medicalteam to monitor for nutrient de1047297ciencies and potentialcomplications of SBS The most common long-term compli-cations include metabolic bone disease PN-related liver dis-ease nephrolithiasis anemia central line infection centralaccess problems (thrombosis and superior vena cava syn-drome due to vein stenosis) and vitamin and trace mineral
de1047297ciencies62738 Patients with SBS are medically complexand require long-term monitoring and revisions of the careplan The substantial bene1047297t of medical nutrition therapy iswhat makes these patients both challenging and extremelyrewarding for RDs to manage
References
1 Semrad CE Approach to the patient with diarrhea and malabsorp-tion In Goldmanrsquo s Cecil Medicine 24th ed Philadelphia PA ElsevierSaunders 2012895-913
2 OrsquoKeefe SJD Buchman AL Fishbein TM Jeejeebhoy KN Jeppesen PBShaffer J Short bowel syndrome and intestinal failure Consensus def-initions and overview Clin Gastroenterol Hepatol 20064(1)6-10
3 Nightingale J Woodward JM Guidelines for management of patientswith short bowel Gut 200655(suppl IV)iv1-iv12
4 Nightingale JMD Lennard-Jones JE Gertner DJ Wood SRBartram CI Colonic preservation reduces need for parenteral ther-apy increases incidence of renal stones but does not change highprevalence of gallstones in patients with a short bowel Gut 199233(11)1493-1497
5 Messing B Crenn P Beau P Boutron-Ruault MC Rambaud J-CMatuchansky C Long-term survival and parenteral nutritiondependence in adult patients with the short bowel syndrome
Gastroenterology 1999117(5)1043-10506 Jeejeebhoy KN Short bowel syndrome A nutritional and medical
approach Can Med Assoc J 2002166(10)1297-1302
7 Welch IM Cunningham KM Read NW Regulation of gastric emptyingby ileal nutrients in humans Gastroenterology 19 8894(2)401-404
8 Bines JE Intestinal failure A new era in clinical management J Gastroenterol Hepatol 200924(suppl 3)S86-S92
9 Bines JE Taylor RG Justice F et al Diet following small bowelresection In1047298uence of diet complexity on intestinal adaptationfollowing massive small bowel resection in a preclinical model
J Gastroenterol Hepatol 200217(11)1170-1179
10 Jeppesen PB Mortensen PB Enhancing bowel adaptation in shortbowel syndrome Curr Gastroenterol Rep 20024(4)338-347
11 Gouttebel MC Saint Aubert B ColetteC Astre C Monnier LHJoyeuxHIntestinal adaptation in patients with short bowel syndrome mea-surement by calcium absorption Dig Dis 198934(5)709-715
12 Buchman AL Etiology and initial management of short bowel syn-drome Gastroenterology 2006130(suppl)S5-S15
13 Parekh NR Steiger E Short bowel syndrome Curr Treat OptionsGastroenterol 200710(1)10-23
14 Lacy CF Armstrong LL Goldman MP Lance LL Drug InformationHandbook A Comprehensive Resource for All Clinicians and HealthcareProfessionals 19th ed Hudson OH Lexi-Comp 2010
15 Rubinoff MJ Piccione PR Holt PR Clonidine prolongs human intes-tine transit time Use of the lactulose-breath hydrogen test Am J Gastroenterol 198984(4)372-374
16 Buchman AL Fryer J Wallin A Ahn CW Polensky S Zaremba KClonidine reduces diarrhea and sodium loss in patients with prox-imal jejunostomy A controlled study JPEN J Parenter Enteral Nutr 200630(6)487-491
17 McDoniel K Taylor B Huey W et al Use of clonidine to decreaseintestinal 1047298uid losses in patients with high-output short-bowel
syndrome JPEN J Parenter Enteral Nutr 200428(4)265-268
18 Williams NS Evans P King RFGJ Gastric acid secretion andgastrin production in the short bowel syndrome Gut 198526(9)914-919
19 Quigley EMM Quera R Small intestinal bacterial overgrowthRoles of antibiotics prebiotics and probiotics Gastroenterology2006130(2 suppl 1)S78-S90
20 Gracey M The contaminated small bowel syndrome Pathogenesisdiagnosis and treatment Am J Clin Nutr 197932(1)234-243
21 Giannella RA Broitman SA Zamcheck N Vitamin B12 uptake byintestinal microorganisms Mechanism and relevance to syn-dromes of intestinal bacterial overgrowth J Clin Invest 197150(5)1100-1107
22 Bala L Ghoshal UC Ghoshal U et al Malabsorption syndrome withand without small intestinal bacterial overgrowth A study on
RESEARCH
1206 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 89
upper-gut aspirates using 1H NMR spectroscopy Magn Reson Med200656(4)738-744
23 Ziegler TR Cole CR Small bowel bacterial overgrowth in adults Apotential contributor to intestinal failure Curr Gastroenterol Rep20079(6)463-467
24 Byrne T Veglia L Camelio M et al Beyond the prescription Opti-mizing the diet of patients with short bowel syndrome Nutr ClinPract 200015(6)306-311
25 Nordgaard I Hansen BS Mortensen PB Colon as a digestive organ inpatientswith short bowel syndromeLancet 1994343(8894)373-376
26 Lykins TC Stockwell J Comprehensive modi1047297ed diet simpli1047297esnutrition management of adults with short bowel syndrome J AmDiet Assoc 199898(3)309-315
27 Matarese LE Steiger E Dietary and medical management of shortbowel syndrome in adult patients J Clin Gastroenterol 200640(suppl2)S85-S93
28 Woolf GM Miller C Kurian R Jeejeebhoy KN Diet for patients with ashort bowel High fat or high carbohydrate Gastroenterology198384(4)823-828
29 Atia A Girard-Pipau F Hebuterne X et al Macronutrient absorptioncharacteristics in human short bowel syndrome and jejunocolonicanastamosis Starch is the most important carbohydrate substratealthough pectin supplementation may modestly enhance short chainfatty acid production and 1047298uid absorption JPEN J Parenter EnteralNutr 201135(2)229-240
30 Tilg H Short bowel syndrome Searching for the proper diet Euro- pean J Gastroenterol Hepatol 200820(11)1061-1063
31 Shatnawei A Parekh NR Rhoda KM et al Intestinal failure man-agement at the Cleveland Clinic Arch Surg 2010145(6)521-527
32 Atia AN Buchman AL Oral rehydration solutions in non-choleradiarrhea A review Am J Gastroenterol 2009104(10)2596-2604
33 Kles KA Chang EB Short-chain fatty acids impact on intestinaladaptation in1047298ammation carcinoma and failure Gastroenterology2006130(suppl 2)S100-S105
34 Banks MR Farthing MJG Fluid and electrolyte transport in the smallintestine Curr Opin Gastroenterol 200218(2)176-181
35 Alam NH Bhatnagar S Chea-Woo E et al Multicenter randomizeddouble-blind clinical trial to evaluate the ef 1047297cacy and safety of areduced osmolarity oral hydration salt solution in children withwatery diarrhea Pediatrics 2001107(4)613-618
36 Rudman D Dedonis JL Fountain MT et al Hypocitraturia in patientswith gastrointestinal malabsorption N Engl J Med 1980303(12)657-661
37 Joly F Dray X Corcos O Barbot L Kapel N Messing B Tube feedingimproves intestinal absorption in short bowel syndrome patientsGastroenterology 2009136(3)824-831
38 Mziray-Andrew CH Sentongo TA Nutritional de1047297ciencies in intes-tinal failure Pediatr Clin North Am 200956(5)1185-1200
39 Okuda K Discovery of vitamin B12 in the liver and its absorptionfactor in the stomach A historical review J Gastroenterol Hepatol199914(4)301-308
40 Green R Indicators for assessing folate and vitamin B12 status and formonitoring the ef 1047297cacy of intervention strategies Food Nutr Bull200829(2 suppl)S52-S63
41 Malone M Longitudinal assessment of outcome health statusand changes in lifestyle associated with long-term home parenteraland enteral nutrition JPEN J Parenter Enteral Nutr 200226164-168
42 Baxter JP Fayers PM McKinlay AW A review of the quality of life of adult patients treated with long-term parenteral nutrition Clin Nutr 200625543-553
43 Huisman-de Waal G Schoonhoven L Jansen J Wanten G vanAchterberg T The impact of home parenteral nutrition on daily lifemdashA review Clin Nutr 200726275-288
44 Dudrick SJ Palesty JA Historical highlights of the development of total parenteral nutrition Surg Clin N Am 201191693-717
45 Shatari T Clark MA Lee JR Keighley MRB Reliability of radiographicmeasurement of small intestine length Colorectal Dis 20036(65)327-329
46 Kovacevich DS Frederick A Kelly D Nishikawa R Young L Standardsfor specialized nutrition support Home care patients Nutr Clin Pract 200520579-590
47 Matarese LE OrsquoKeefe SJ Kandie HM et al Short bowel syndromeClinical guidelines for nutrition management Nutr Clin Pract 200520(5)493-502
48 Kovacevich DS Orr ME Considerations for home nutrition supportIn The ASPEN Nutrition Support Practice Manual 2nd ed SilverSpring MD American Society of Parenteral and Enteral Nutrition2005371-377
49 Kumpf VJ Tillman EM Home parenteral nutrition Safe transitionfrom hospital to home Nutr Clin Pract 201227749-757
50 WinklerM Hagan E Albin J Homenutrition support In ASPEN Adult Nutrition Support Core Curriculum 2nded Silver Spring MD AmericanSociety of Parenteral and Enteral Nutrition 2012639-655
51 Kumpf VJ Parenteral nutrition-associated liver disease in adult andpediatric patients Nutr Clin Pract 200621279-290
52 Kumpf VJ Gervasio J Complications of parenteral nutrition In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver SpringMD American Society of Parenteral and Enteral Nutrition 2012384e297
53 Dreesen M Foulon V Vanhaecht K et al Guidelines recommenda-tions on care of adult patients receiving home parenteral nutritionA systematic review of global practices Clin Nutr 201231602-608
54 Howard L Ashley C Lyon D Shenkin A Autopsy tissue trace ele-ments in 8 long-term parenteral nutrition patients who receive thecurrent US Food and Drug Administration formulation JPEN J Parenter Enteral Nutr 200731(5)388-396
55 Reynolds N Blumsohn A Baxter JP Houston G Pennington CRManganese requirement and toxicity in patients on home parenteralnutrition Clin Nutr 199817(5)227-230
56 Thompson P Dueksen DV Vitamin D de1047297ciency in patients receivinghome parenteral nutrition JPEN J Parenter Enteral Nutr 201135(4)499-504
57 Yusuf SW Rehman Q Casscells W Cardiomyopathy in associationwith selenium de1047297ciency A case report JPEN J Parenter Enteral Nutr 200226(1)63-66
58 Mirtallo JM Holcombe B Kochevar M Guenter P Parenteral nutri-tion product shortages The ASPEN strategy Nutr Clin Pract 201227(3)385-391
59 Gillanders L Angstmann K Ball P et al AuSPEN clinical practiceguidelines for home parenteral nutrition patient in Australia andNew Zealand Nutrition 200824998-1012
60 Tarleton S DiBaise JK Short bowel syndrome In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver Spring MDASPEN 2012511-522
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1207
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9

7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 29
After surgical resection the remaining small bowel un-dergoes an adaptation process that involves morphologic andfunctional changes8 The small bowel dilates and the villiheight and crypt depth increase expanding the absorptivesurface area of the small bowel without change in length9
The mechanism of adaption is not fully understood Impor-tant factors include hormonal growth factors nutrients
(particularly complex macronutrients) bile and pancreaticsecretions and local intestinal hormones such as glucagon-like peptide 210 Adaptation begins soon after intestinalresection and may continue for 2 years11 Because oral nu-trients stimulate intestinal adaptation it is important toinitiate an oral diet or enteral feedings as soon as possibleafter surgery12
MANAGEMENT OF SBSThe goal of therapy is to maximize small bowel absorption of 1047298uids and nutrients to prevent de1047297ciencies and dehydration12
This is accomplished by controlling the rate at which nutri-ents and 1047298uids move through the intestinal tract with the useof medications and diet therapy In some cases infusiontherapy (enteral andor parenteral) with nutrients and 1047298uidmay be required either temporarily after surgery or lifelong1
PharmacotherapyThe common categories of medications used to manage SBSinclude antimotility agents antisecretory agents and paren-teral infusion therapy (intravenous [IV] 1047298uids andor PN)1
Antimotility medications (the most common are loperamidediphenoxylate and atropine codeine and deodorized tinctureof opium [DTO]) are used to slow peristalsis and improve ab-sorption of 1047298uid electrolytes and nutrients13 These medica-tions are usually taken as needed after a loose bowelmovement but for patients with SBS the dose is given
routinely 30 minutes before meals and at bedtime Often pa-tients with SBS have to adjust the timing and titrate the dose of antimotility agents based on meal composition daily activitiesand degree of bowel adaptation Patients taking opiate-basedmedications to control 1047298uid and electrolyte losses (codeineand DTO) must be closely monitored for side effects includingimpaired mental or physical alertness as well as symptoms of withdrawal if the medications are abruptly discontinued afterprolonged use14 Clonidine an a2-adrenergic agonist has beenshown to increase intestinal transit time and decrease fecalweight in patients with SBS15-17 It can be administered by oralmedication or transdermal patch which is an effective alter-native for patients with reduced small bowel absorptionClonidine is commonly used to treat hypertension so bloodpressure should be monitored closely when starting thismedication Patients with severe coronary heart diseasechronic renal insuf 1047297ciency and hemodynamic instability maynot be good candidates for clonidine therapy14
Hypersecretion of gastrin and gastric acid occurs in pa-tients after extensive small bowel resection18 Histamine H2
antagonists (ie H2 blockers) and the more potent protonpump inhibitors (PPIs) are used in SBS to decrease gastric acidsecretion diarrheal losses and risk for peptic ulcer diseaseand its complications The H2 blockers inhibit histamine atthe histamine H2 receptors of gastric parietal cells thusreducing gastric acid secretion whereas PPIs directly inhibithydrogen potassium ATPase pump of parietal cells effectively
stopping acid secretion14 Somatostatin analogues inhibit therelease of gastrointestinal hormones and reduce secretion of intestinal and pancreatic 1047298uids which reduces diarrhea inpatients with SBS14
In some cases pancreatic enzyme replacement and bile acidsequestrants may be used to control maldigestion and diar-rhea13 Exogenous pancreatic enzyme mixing with food in the
stomach can increase nutrient absorption in patients withrapid small bowel transit and poor intestinal mixing of chymewith pancreatic secretions Bile acid sequestrants can helpalleviate choleretic diarrhea that occurs when distal ilealresection disrupts enterohepatic circulation of bile salts1
Small bowel bacterial overgrowth can occur in conjunctionwith SBS and is related to alterations of intestinal anatomymotility and gastric acid suppression1920 Bacteria in thesmall bowel can deconjugate bile acids which may worsendiarrhea and malabsorption20-22 Treatments for bacterialovergrowth include antibiotics probiotics and bile acidsequestrants23 Often broad spectrum antibiotics are cycled(alternating 1 or 2 weeks of treatment with an antibiotic withseveral weeks off antibiotic therapy) to prevent or delay
antibiotic resistanceParenteral infusion therapy is often needed immediately
after surgery to maintain 1047298uid and electrolyte balance asbowel function returns12 IV support can vary from saline orlactated ringerrsquos infusions to full PN support (IV 1047298uids thatcontain both macro- and micronutrients) The degree of bowel adaptation will dictate the length of IV therapy A goodguideline is that patients with SBS with gt15 L stool outputand lt800 mL urine output in 24 hours will have dif 1047297cultymaintaining hydration and electrolyte balance without someIV 1047298uid support3
Medical Nutrition Therapy
The macronutrient distribution of diets for SBS will varydepending upon the sites and length of remaining bowel(Figure 1) In small clinical studies patients with end jeju-nostomies have improved energy absorption and similar stoollosses with moderately high amounts of fats and dietary 1047297berwhen compared with diets high in complex carbohydrates(CHO) alone24-27 The optimal diet includes generous amountsof complex CHO and fats with a macronutrient distribution of approximately (50 CHO 20 to 30 protein and40 fat)28
Foods rich in water-soluble 1047297ber can slow both gastricemptying and intestinal transit time thicken ostomy ef 1047298uentand promote intestinal adaptation2429 It is best to minimize1047298uid intake with solid food meals beverages should be sippedcontinuously between meals3031 Avoidance of foods andbeverages high in simple sugars may alleviate dumping of hypertonic chyme into the intestine Patients should eat fourto six small meals a day Another important goal for patientswith SBS and jejunostomies is to maximize 1047298uid uptake by thesmall intestine This is best achieved by utilizing the sodium-glucose cotransport system to pull water across the epitheliallining32-35 Liberal use of salt on food and sipping oral rehy-dration solutions (ORS) between meals (1 to 2 Lday) haveshown to be bene1047297cial332
Patients with an intact colon bene1047297t from a diet higher incomplex CHO and moderate in fat (50 to 60 CHO 20 to30 protein and 20 to 30 fat) divided into three smallmeals plus two to three snacks per day2729 The rationale for
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1201
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 39
emphasizing complex CHO and less fat is twofold Firstcolonic bacteria can metabolize undigested CHO includingdietary 1047297ber to short-chain fatty acids leading to salvageabsorption and net increase energy sodium and water up-take2533 Second steatorrhea from poorly absorbed dietaryfats and increased risk of oxalate absorption in the colon mayresult in calcium oxalate kidney stone formation436 A dietlow in fat and oxalate along with calcium supplementationat meals can reduce the risk of kidney stone formationConsumption of salty foods and ORS is not as important forpatients with SBS who have an intact colon as long as foodand 1047298uid intake is spread throughout the day24
Enteral nutrition (EN) support alone or in combinationwith an oral diet has proven to increase absorption of mac-ronutrients in patients with and without colonic continuity Joly and colleagues37 demonstrated that continuous naso-gastric feedings with a polymeric formula in patients withSBS signi1047297cantly (P lt0001) increased absorption of proteinsfats and energy compared with an isocaloric oral diet This
enhanced nutrient absorption may be related to continuousinfusion of isotonic nutrients which is better tolerated withaltered gut anatomy when compared with bolus infusion of feedings or food The continuous bathing of the gut withmacronutrients may promote release of pancreatic and in-testinal enzymes as well as intestinal hormones that enhancebowel adaptation and overall absorption EN is less expensiveand presents lower overall risks than PN In SBS the use of ENcan facilitate reduction in the number of PN infusions eachweek andor complete weaning from PN therapy altogether
Micronutrient requirements will vary among patientsdepending upon the sites of remaining intestine All patientswith SBS should take a daily multivitamin with minerals bymouth (preferably chewable or liquid) or IV Routine moni-
toring of serum vitamin B-12 and methylmalonic acid (amarker of vitamin B-12 status) levels is required for any pa-tient with a distal ileum resection or small bowel bacterialovergrowth supplementation may be required2138-40 Diva-lent cations mainly calcium magnesium and zinc can bede1047297cient in patients with SBS and many will require sup-plementation1 This may be related to lack of absorptivesurface rapid transit time and binding with unabsorbed fatin the intestinal lumen Cautious supplementation of mag-nesium is advisable because oral magnesium preparationsare dif 1047297cult to absorb and therefore have cathartic effectsSlow-release magnesium chloride magnesium gluconate ormagnesium lactate preparations can reduce some of thegastrointestinal symptoms related to oral magnesium inges-
tion13 Practitioners should be cognizant that osteoporosisanemia and fat-soluble vitamin de1047297ciencies are common inpatients with SBS and long-term monitoring is necessaryIndividual vitamin and mineral supplements should be pre-scribed as needed38 The following case highlights theimportance of comprehensive medical management of pa-tients with SBS and provides an opportunity to discusspractical clinical applications
PATIENT PROFILEThe patient is a 72-year-old woman with a past medicalhistory of colon cancer that was treated by partial colectomyand chemotherapy Recurrent colon cancer was diagnosed 11years later requiring a complete colectomy with end ileos-tomy Postoperative Day 3 she developed severe abdominalpain and blood-tinged ostomy ef 1047298uent re-exploration sur-gery demonstrated extensive distal small bowel necrosis Thenecrotic bowel was resected leaving an estimated 105 cm of proximal small bowel to an end jejunostomy The patient rsquosrecovery was uneventful she was discharged from the hos-pital on a regular diet
During the 1047297rst month after discharge from the hospitalthe patient had multiple admissions for dehydration andweight loss During one such hospitalization a double-lumenperipherally inserted central catheter (PICC) was placed andPN initiated Soon after the start of therapy she developed an
Nutrient
Small bowel
ostomy
Colonic
continuity
Carbohydrates 50 of total
energy complex
carbohydrates
including soluble
1047297ber limit simple
sugars
50-60 of total
energy complex
carbohydrates
including soluble
1047297ber
Proteins 20-30 of total
energy
20-30 of total
energy
Fats 40 of total
energy
20-30 of total
energy
Fluids ORSb important
minimize 1047298uids
with meals
sipping of 1047298uids
between meals
Minimize 1047298uids
with meals
sipping of 1047298uids
between meals
Vitamins Daily multiple
vitamin with
minerals monthly
B-12 possibly
vitamins A Dc
and E
supplements
Daily multiple
vitamin with
minerals possibly
B-12 possibly
vitamins A D and
E supplements
Minerals Generous use of
sodium chloride
on food calcium
1000-1500 mg
daily possibly
iron magnesium
and zinc
supplements
400-600 mg
calcium with
meals possibly
iron magnesium
and zinc
supplements
reduced oxalate
Meals 4-6 small meals 3 small meals plus
2-3 snacks
aBased on references 24 47 and 60bORSfrac14oral rehydration solutionc25-hydroxy vitamin D
Figure 1 Medical nutrition therapy for short bowel syndromea
RESEARCH
1202 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 49
upper extremity deep vein thrombosis originating at the PICCinsertion site anticoagulation therapy was started Duringthe same hospitalization she developed fevers due to acatheter-related blood infection hypotension hypokalemiaand increased liver function tests On Hospital Day 17 thepatient was transferred to a tertiary care hospital for man-agement of SBS
TERTIARY CARE CENTER COURSEThe PICC was pulled and the patient was given a central lineholiday while antibiotic therapy was completed PeripheralPN (1 L 50-g dextrose and 20-g amino acids without lipidemulsion due to an egg allergy) was initiated along withantisecretory (ie PPI) and antimotility (ie DTO) medicationsHer diet was changed to six small meals with sipping of ORSbetween meals On Hospital Day 9 a tunneled central cath-eter was placed and the PN formulation was increased to 50 gdextrose 80 g amino acids infusing over 10 hours each night(490 kcalday) After intensive diet and infusion therapy ed-ucation the patient was discharged to home with the samePN formula diet and medications
AT HOMEAt home the patientrsquos oral intake increased with subsequentincrease in jejunostomy output necessitating adjustment of the PN volume to 15 L infused over 12 hours and titration of the DTO dose to 1 mL four times a day Six months afterdischarge PN she had stable serum chemistry valuesadequate hydration and she was slowly losing weight thePN infusion was changed to every other day and the anti-coagulation therapy was discontinued Subsequent serumchemistry results suggested negative 1047298uid balance and thepatient complained of extreme thirst and fatigue A 24-hoururine collection during an off day from PN resulted in only
400 mL urine The PN volume was increased to 24L over 12hours every other day and the patient was instructed tostrictly adhere to the diet and ORS therapy The patient hadimproved hydration on noninfusion days and the repeat 24-hour urine collection yielded 850 mL
The patient remains on every-other-day IV infusions for1047298uid vitamins minerals and electrolytes her weight hasstabilized at 86 kg (body mass index 307) Four years afterdischarge on PN her insurance provider mandated a switchedto noneamino acid-containing IV 1047298uid (Table) She continuesto strictly adhere to the diet regimen but has ceased usingORS because she no longer appreciates hydration bene1047297tsfrom the therapy Repeat chemistry data including normalvitamin levels and triene to tetraene ratio (an indication of
adequate absorption of essential fatty acids) plus stable bodymass index suggest adequate hydration and nutrient uptakewith the current management
DISCUSSIONHistorically loss of a signi1047297cant portion of the intestine wasphysically devastating and often a death sentence During thepast 50 years with the advent of PN and a better under-standing of small bowel physiology most patients with SBSrecover and live without signi1047297cant reduction in quality of life41-44 The case of the patient provided is an excellentexample of the metabolic consequences of massive smallbowel resection and the complications of infusion therapy
Per the Nutrition Care Process this patient had alteredgastrointestinal function due to extensive intestinal resectionas evidenced by inability to maintain hydration on an oraldiet Through aggressive medical management strict dietaryadherence and appreciable bowel adaptation she hasreduced her dependence on IV support and ORS by approx-imately 80 The dietary key to her success was the transition
from eating two large meals a day and drinking large volumesof sugar-containing beverages to separating food and 1047298uidingestion eating four small meals daily limiting simple sugarintake and sipping ORS daily Through trial and error thepatient has re1047297ned her schedule for antisecretory and anti-motility medications to maximize 1047298uid and electrolyte ab-sorption With remnant bowel length of only 105 cm it isunlikely she will ever completely wean from infusion ther-apy but with the conversion to every-other-day IV infusiontherapy she reports improved quality of life
Like many patients receiving home PN this patient hashad complications related to infusion therapy including athrombosis around a PICC catheter-related blood infectionsand liver function abnormalities The incidence of catheter-
related complications has been minimized by using singlelumen tunneled catheters to minimize the diameter of thecatheter and reduce the risk of clot formation limiting accessfor bacterial introduction with a single lumen and by re-education in aseptic technique Her liver function hasreturned to normal with the reduction of PN support andfewer central line infections (a frequent cause of abnormalliver tests) She will require lifelong monitoring of overallhealth and nutrition parameters vitamin levels and tracemineral levels as well as bone and vital organ health Every6 months the patient returns to clinic for monitoring She hasdual-energy x-ray absorptiometry scans every 2 years toassess her risk of metabolic bone disease (postmenopausaland SBS-related) Her overall prognosis is excellent given her
signi1047297cant small bowel adaptation the low rate of central linecomplications and reduced dependence on IV support
PRACTICE APPLICATIONSManagement of patients with SBS requires a thorough un-derstanding of intestinal physiology knowledge of pharma-conutrition therapy (ie the use of nutrients for therapeuticbene1047297t) close attention to detail and patience Each SBSpatient presents with unique nutrient requirements based onthe length site and health of their remaining intestineWhen caring for a patient with SBS a registered dietitian(RD) must know the exact intestinal anatomy so that a plan of care is developed to optimize bowel function and nourish thepatient If the operative report is unavailable or there isquestion as to the length or health of the remaining bowel anupper gastrointestinal with small bowel follow-throughbarium study provides vital information on the length andcondition of intestine remaining as well as transit time45 Inaddition RDs must have accurate intake and output data toassess 1047298uid balance awareness of all prescribed medicationsand supplements knowledge of IV access including cathetertip location weight history and laboratory data
Before hospital discharge there are many details RDsmust ensure are in place for patients with SBS (Figure 2)First the patient must understand the proper diet and oralhydration guidelines as well as the dosage and timing of
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1203
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 59
Table Data for a 72-year-old female patient from hospital admission to 4 y after massive small bowel resection
Patient data
Transfer to
tertiary
care center
Time After Discharge
3 wk 55 mo 6 mo 65 mo 75 mo 4 y
Body mass index 353 350 325 325 315 307 307
Laboratory dataa
Glucose (65-110 mgdL)b 169 148 115 122 100 119 89
Sodium (136-144 mEqL) 138 137 138 144 140 140 141
Potassium (36-51 mEqL) 33 44 42 42 42 38 42
Chloride (101-111 mEqL) 95 103 105 102 103 105 105
Bicarbonate (22-32 mEqL) 35 26 26 29 33 30 29
Blood urea nitrogen (7-19 mgdL)c 22 37 28 22 26 22 21
Creatinine (050-15 mgdL)d 10 08 10 13 12 10 096
Calcium (86-106 mgdL)e 77 93 89 95 92 87 95
Phosphorus (24-47 mgdL)f 38 39 40 38 42 36 35
Magnesium (18-25 mgdL)g 19 22 22 21 22 22 23
Total protein (gdL)h 60 78 79 76 67 76
Albumin (gdL)i 29 33 45 40 39 40
Total bilirubin (0-13 mgdL) j 16 095 09 129 097 08
Alkaline phosphatase (38-126 IUL) 239 204 320 217 163 95
24-h urine volume (mL)k 400 850
Measured energy expenditure (kcald) 1794
Respiratory quotient 069
Medications
Warfarin (mg) 4 4 0 0 0 0 0
Proton pump inhibitor (mgd) 40 40 40 40 40 40 30Deoderized tincture of opium (mLday) 12 3 3 3 3 3 4
Oral multivitamin 0 0 0 1l 1l 1l 1l
Vitamin D-3 (IUd) 0 0 0 0 0 0 1000
Calcium carbonate (mgd) 0 0 0 0 0 0 500
Oral rehydration solution (Ld) 1 1 1 1 1 1 0
Parenteral nutrition volume (Ld) 1 15 15 2m 24m 24m 24m
Parenteral nutrition energy (kcald) 490 490 490 410m 410m 410m 170m
Parenteral nutrition amino acids (gd) 80 60 60 60m 60m 60m 0
aRanges shown in parentheses are reference rangesb To convert mgdL glucose to mmolL multiply mgdL by 00555 To convert mmolL glucose to mgdL multiply mmolL by 1801 Glucose of 65 mgdLfrac14361 mmolLc To convert mgdL blood urea nitrogen to mmolL multiply mgdL by 0357 To convert mmolL blood urea nitrogen to m gdL multiply mmolL by 280 Blood urea nitrogen of 7 mg
dLfrac14250 mmolLd To convert mgdL creatinine to mmolL multiply mgdL by 884 To convert mmolL creatinine to mgdL multiply mmolL by 001 Creatinine of 05 mgdLfrac14442 mmolLe To convert mgdL calcium to mmolL multiply mgdL by 025 To convert mmolL calcium to mgdL multiply mmolL by 4 Calcium of 86 mgdLfrac14215 mmolLf To convert mgdL phosphorous to mmolL multiply mgdL by 0323 To convert mmolL phosphorous to mgdL multiply mmolL by 309 Phosphorous of 24 mgdLfrac14078 mmolLg To convert mgdL magnesium to mmolL multiply mgdL by 0411 To convert mmolL magnesium to mgdL multiply mmolL by 243 Magnesium of 18 mgdLfrac1474 mmolLh To convert gdL total protein to gL multiply gdL by 10 To convert gL total protein to gdL multiply gL by 01 Total protein of 60 gdLfrac1460 gLi To convert gdL albumin to gL multiply gdL by 10 To convert gL albumin to gdL multiply gL by 01 Albumin of 29 gdLfrac1429 gL j To convert mgdL total bilirubin to mmolL multiply mgdL by 171 To convert mmolL total bilirubin to mgdL multiply mmolL by 058 Total bilirubin of 16 mgdLfrac142737 mmolLk 24-h urine volume collected on a day without parenteral nutrition infusionlOff parenteral nutrition daymEvery other day
RESEARCH
1204 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 69
antimotility and acid-blocking medications46 In additionthe patient should be aware that the dosage of the medi-cations may change once he or she is home and eatingmore food Emphasis should be placed on proper eatingtechniques for example eating slowly resting after eatingminimal 1047298uid intake with the meal and sipping of 1047298uidsbetween meals47 If an ORS is required recipes to preparethe solution or information on where to purchase ORSmust be given to the patient The RD may have to reinforcethis information repeatedly before and after dischargeAdults in particular have dif 1047297culty changing their eatinghabits and may 1047297nd it challenging to adhere to the newguidelines until they begin to see reduction in stool outputand improved overall sense of well-being Also the patient
must have prescriptions for antisecretory therapy (eitherPPI or H2 blocker) and vitamin and mineral supplements if needed For those discharged on PN the patient and familyrequire education on catheter care and aseptic techniquefor infusion therapy before discharge4849 Patient moni-toring of oral intake stool and urine output as well asweight in the early period after hospital discharge willfacilitate decisions regarding medication adjustments andpossibly weaning of EN or PN support The patient andfamily may require education on proper techniques formeasuring body 1047298uid output at home48 Nursing support inthe home can help to reinforce the concepts of SBS man-agement and provide RDs essential insight to the homeenvironment
Checklist item Acute care setting Home care setting
Diet education Educate and reinforce as diet is advanced
in the hospital
Reinforce and adjust diet as bowel adapts
Laboratory data Daily chemistry panel including magnesium
and blood count
Twice weekly liver function testsBaseline vitamin and trace mineral
levels (A E Db folate B-12 iron zinc
copper and selenium) before discharge
Weekly comprehensive metabolic panel
including magnesium until stable then monthly
Annually vitamin and trace mineral levels
Weights and IOc
data
Daily weight
Daily IO data
Weekly weight
Once weekly IO data until stable then monthly
(more frequently if change in medical
management or status)
Medications Antimotility agent
PPId or H2 blockere
Multivitamin and mineral supplements
Antimotility agent
PPI or H2 blocker
Multivitamin and mineral supplements
Possibly pancreatic enzyme replacement or bile
acid sequestrant
Nutrition support If on enteral nutrition then know the
type of tube and enteral formula
If parenteral nutrition know the type of
catheter the position of the catheter
tip and the formula
Note any additional intravenous 1047298uids
Talk to the patient andor caregiver
Communicate with the home care company any
changes in enteral or parenteral formulas
Obtain report from home nurse
Monitoring frequency Daily Weekly until stable then reduce frequency
as appropriate
Other Know the exact post-operative intestinal
anatomyCommunicate long-term plan with the
primary care physician prior to discharge
Monitor for bowel adaptation and make
alterations in MNT
f
as possibleScreen for bone disease and anemia
aBased on references 46 and 59b25-hydroxy vitamin DcIOfrac14intake and output Includes oral enteral and parenteral intake plus urine stool and drain outputdPPIfrac14proton pump inhibitoreH2frac14histamine 2 antagonistf MNT frac14medical nutrition therapy
Figure 2 Checklist for registered dietitian management of patients with short bowel syndromea
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1205
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 79
After hospital discharge patients with SBS are best servedby frequent follow-up appointments with all members of thenutrition support team in particular the managing physicianand RD The primary goals of these appointments are toassess adherence to the prescribed therapies monitor 1047298uidelectrolyte hydration and nutritional status reinforce theprinciples of nutrition therapy and adjust the therapies as
necessary
50
Periodic weights and blood chemistry levels(including liver function tests) will help to determine theextent of bowel adaptation liver-related complications of PNand the possibility of weaning from EN or PN48 If a patientdevelops PN-related liver disease the workup should assessfor small bowel bacterial overgrowth blood infection and re-evaluate IV fat emulsion deliverymdashall of which can alter liverfunction51 Treatment may include a reduction in the amountand frequency of IV fat emulsion infusions (lt1 gkgday asinfrequently as once a week) with periodic monitoring foressential fatty acid de1047297ciency52
Baseline vitamin (eg folate B-12 and vitamins A D E)mineral (eg iron calcium and magnesium) and trace mineral(eg zinc copper and selenium and chromium and manganese
for PN patients) levels and dual-energy x-ray absorptiometryscan are required for comparison purposes in long-term followup53 The standard parenteral multivitamin and trace mineraladditives may not meet a patientrsquos exact requirements and cancause de1047297ciency or toxicity states over time54 For exampledaily trace mineralinfusions of 03 mg manganese over timecanlead to deposits in the brain55 and chronic standard multivi-tamin dosing of 200 IU vitamin D can cause insuf 1047297ciency orde1047297ciency states56 Further complicating the issue of moni-toring micronutrient levels of patients dependent on PN are theongoing product shortages These shortages have led to omis-sion or rationing of certain nutrients that can cause life-threatening de1047297ciency states505758 These levels should becheckedno less than every 6 to 12 months or more frequently if
abnormal levels are identi1047297ed5859 With time as a patient sta-bilizes and thrives at home the length of time between clinicvisits can be extended For patients with stable chronic SBS theminimum follow-up should occur every 6 to 12 months As withthe patientpro1047297le provided bowel adaptation can occur slowlyIt can take more than 2 years before adaptation has fullyoccurred to change the treatment plan and wean arti1047297cialnutrition support11
CONCLUSIONSManagement of SBS is complex and requires a concert of medical nutrition and pharmaceutical therapies to optimize1047298uid and nutrient absorption for survival Each patientrsquos
unique care plan depends on the amount and site of remaining intestine and the patientrsquos ability to adhere to themedical and nutrition therapies Some patients will be able tosurvive with antisecretory and anti-motility agents alongwith strict diet adherence alone whereas other patients willrequire lifelong infusion therapy In either case patients withSBS must have close follow-up with a specialized medicalteam to monitor for nutrient de1047297ciencies and potentialcomplications of SBS The most common long-term compli-cations include metabolic bone disease PN-related liver dis-ease nephrolithiasis anemia central line infection centralaccess problems (thrombosis and superior vena cava syn-drome due to vein stenosis) and vitamin and trace mineral
de1047297ciencies62738 Patients with SBS are medically complexand require long-term monitoring and revisions of the careplan The substantial bene1047297t of medical nutrition therapy iswhat makes these patients both challenging and extremelyrewarding for RDs to manage
References
1 Semrad CE Approach to the patient with diarrhea and malabsorp-tion In Goldmanrsquo s Cecil Medicine 24th ed Philadelphia PA ElsevierSaunders 2012895-913
2 OrsquoKeefe SJD Buchman AL Fishbein TM Jeejeebhoy KN Jeppesen PBShaffer J Short bowel syndrome and intestinal failure Consensus def-initions and overview Clin Gastroenterol Hepatol 20064(1)6-10
3 Nightingale J Woodward JM Guidelines for management of patientswith short bowel Gut 200655(suppl IV)iv1-iv12
4 Nightingale JMD Lennard-Jones JE Gertner DJ Wood SRBartram CI Colonic preservation reduces need for parenteral ther-apy increases incidence of renal stones but does not change highprevalence of gallstones in patients with a short bowel Gut 199233(11)1493-1497
5 Messing B Crenn P Beau P Boutron-Ruault MC Rambaud J-CMatuchansky C Long-term survival and parenteral nutritiondependence in adult patients with the short bowel syndrome
Gastroenterology 1999117(5)1043-10506 Jeejeebhoy KN Short bowel syndrome A nutritional and medical
approach Can Med Assoc J 2002166(10)1297-1302
7 Welch IM Cunningham KM Read NW Regulation of gastric emptyingby ileal nutrients in humans Gastroenterology 19 8894(2)401-404
8 Bines JE Intestinal failure A new era in clinical management J Gastroenterol Hepatol 200924(suppl 3)S86-S92
9 Bines JE Taylor RG Justice F et al Diet following small bowelresection In1047298uence of diet complexity on intestinal adaptationfollowing massive small bowel resection in a preclinical model
J Gastroenterol Hepatol 200217(11)1170-1179
10 Jeppesen PB Mortensen PB Enhancing bowel adaptation in shortbowel syndrome Curr Gastroenterol Rep 20024(4)338-347
11 Gouttebel MC Saint Aubert B ColetteC Astre C Monnier LHJoyeuxHIntestinal adaptation in patients with short bowel syndrome mea-surement by calcium absorption Dig Dis 198934(5)709-715
12 Buchman AL Etiology and initial management of short bowel syn-drome Gastroenterology 2006130(suppl)S5-S15
13 Parekh NR Steiger E Short bowel syndrome Curr Treat OptionsGastroenterol 200710(1)10-23
14 Lacy CF Armstrong LL Goldman MP Lance LL Drug InformationHandbook A Comprehensive Resource for All Clinicians and HealthcareProfessionals 19th ed Hudson OH Lexi-Comp 2010
15 Rubinoff MJ Piccione PR Holt PR Clonidine prolongs human intes-tine transit time Use of the lactulose-breath hydrogen test Am J Gastroenterol 198984(4)372-374
16 Buchman AL Fryer J Wallin A Ahn CW Polensky S Zaremba KClonidine reduces diarrhea and sodium loss in patients with prox-imal jejunostomy A controlled study JPEN J Parenter Enteral Nutr 200630(6)487-491
17 McDoniel K Taylor B Huey W et al Use of clonidine to decreaseintestinal 1047298uid losses in patients with high-output short-bowel
syndrome JPEN J Parenter Enteral Nutr 200428(4)265-268
18 Williams NS Evans P King RFGJ Gastric acid secretion andgastrin production in the short bowel syndrome Gut 198526(9)914-919
19 Quigley EMM Quera R Small intestinal bacterial overgrowthRoles of antibiotics prebiotics and probiotics Gastroenterology2006130(2 suppl 1)S78-S90
20 Gracey M The contaminated small bowel syndrome Pathogenesisdiagnosis and treatment Am J Clin Nutr 197932(1)234-243
21 Giannella RA Broitman SA Zamcheck N Vitamin B12 uptake byintestinal microorganisms Mechanism and relevance to syn-dromes of intestinal bacterial overgrowth J Clin Invest 197150(5)1100-1107
22 Bala L Ghoshal UC Ghoshal U et al Malabsorption syndrome withand without small intestinal bacterial overgrowth A study on
RESEARCH
1206 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 89
upper-gut aspirates using 1H NMR spectroscopy Magn Reson Med200656(4)738-744
23 Ziegler TR Cole CR Small bowel bacterial overgrowth in adults Apotential contributor to intestinal failure Curr Gastroenterol Rep20079(6)463-467
24 Byrne T Veglia L Camelio M et al Beyond the prescription Opti-mizing the diet of patients with short bowel syndrome Nutr ClinPract 200015(6)306-311
25 Nordgaard I Hansen BS Mortensen PB Colon as a digestive organ inpatientswith short bowel syndromeLancet 1994343(8894)373-376
26 Lykins TC Stockwell J Comprehensive modi1047297ed diet simpli1047297esnutrition management of adults with short bowel syndrome J AmDiet Assoc 199898(3)309-315
27 Matarese LE Steiger E Dietary and medical management of shortbowel syndrome in adult patients J Clin Gastroenterol 200640(suppl2)S85-S93
28 Woolf GM Miller C Kurian R Jeejeebhoy KN Diet for patients with ashort bowel High fat or high carbohydrate Gastroenterology198384(4)823-828
29 Atia A Girard-Pipau F Hebuterne X et al Macronutrient absorptioncharacteristics in human short bowel syndrome and jejunocolonicanastamosis Starch is the most important carbohydrate substratealthough pectin supplementation may modestly enhance short chainfatty acid production and 1047298uid absorption JPEN J Parenter EnteralNutr 201135(2)229-240
30 Tilg H Short bowel syndrome Searching for the proper diet Euro- pean J Gastroenterol Hepatol 200820(11)1061-1063
31 Shatnawei A Parekh NR Rhoda KM et al Intestinal failure man-agement at the Cleveland Clinic Arch Surg 2010145(6)521-527
32 Atia AN Buchman AL Oral rehydration solutions in non-choleradiarrhea A review Am J Gastroenterol 2009104(10)2596-2604
33 Kles KA Chang EB Short-chain fatty acids impact on intestinaladaptation in1047298ammation carcinoma and failure Gastroenterology2006130(suppl 2)S100-S105
34 Banks MR Farthing MJG Fluid and electrolyte transport in the smallintestine Curr Opin Gastroenterol 200218(2)176-181
35 Alam NH Bhatnagar S Chea-Woo E et al Multicenter randomizeddouble-blind clinical trial to evaluate the ef 1047297cacy and safety of areduced osmolarity oral hydration salt solution in children withwatery diarrhea Pediatrics 2001107(4)613-618
36 Rudman D Dedonis JL Fountain MT et al Hypocitraturia in patientswith gastrointestinal malabsorption N Engl J Med 1980303(12)657-661
37 Joly F Dray X Corcos O Barbot L Kapel N Messing B Tube feedingimproves intestinal absorption in short bowel syndrome patientsGastroenterology 2009136(3)824-831
38 Mziray-Andrew CH Sentongo TA Nutritional de1047297ciencies in intes-tinal failure Pediatr Clin North Am 200956(5)1185-1200
39 Okuda K Discovery of vitamin B12 in the liver and its absorptionfactor in the stomach A historical review J Gastroenterol Hepatol199914(4)301-308
40 Green R Indicators for assessing folate and vitamin B12 status and formonitoring the ef 1047297cacy of intervention strategies Food Nutr Bull200829(2 suppl)S52-S63
41 Malone M Longitudinal assessment of outcome health statusand changes in lifestyle associated with long-term home parenteraland enteral nutrition JPEN J Parenter Enteral Nutr 200226164-168
42 Baxter JP Fayers PM McKinlay AW A review of the quality of life of adult patients treated with long-term parenteral nutrition Clin Nutr 200625543-553
43 Huisman-de Waal G Schoonhoven L Jansen J Wanten G vanAchterberg T The impact of home parenteral nutrition on daily lifemdashA review Clin Nutr 200726275-288
44 Dudrick SJ Palesty JA Historical highlights of the development of total parenteral nutrition Surg Clin N Am 201191693-717
45 Shatari T Clark MA Lee JR Keighley MRB Reliability of radiographicmeasurement of small intestine length Colorectal Dis 20036(65)327-329
46 Kovacevich DS Frederick A Kelly D Nishikawa R Young L Standardsfor specialized nutrition support Home care patients Nutr Clin Pract 200520579-590
47 Matarese LE OrsquoKeefe SJ Kandie HM et al Short bowel syndromeClinical guidelines for nutrition management Nutr Clin Pract 200520(5)493-502
48 Kovacevich DS Orr ME Considerations for home nutrition supportIn The ASPEN Nutrition Support Practice Manual 2nd ed SilverSpring MD American Society of Parenteral and Enteral Nutrition2005371-377
49 Kumpf VJ Tillman EM Home parenteral nutrition Safe transitionfrom hospital to home Nutr Clin Pract 201227749-757
50 WinklerM Hagan E Albin J Homenutrition support In ASPEN Adult Nutrition Support Core Curriculum 2nded Silver Spring MD AmericanSociety of Parenteral and Enteral Nutrition 2012639-655
51 Kumpf VJ Parenteral nutrition-associated liver disease in adult andpediatric patients Nutr Clin Pract 200621279-290
52 Kumpf VJ Gervasio J Complications of parenteral nutrition In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver SpringMD American Society of Parenteral and Enteral Nutrition 2012384e297
53 Dreesen M Foulon V Vanhaecht K et al Guidelines recommenda-tions on care of adult patients receiving home parenteral nutritionA systematic review of global practices Clin Nutr 201231602-608
54 Howard L Ashley C Lyon D Shenkin A Autopsy tissue trace ele-ments in 8 long-term parenteral nutrition patients who receive thecurrent US Food and Drug Administration formulation JPEN J Parenter Enteral Nutr 200731(5)388-396
55 Reynolds N Blumsohn A Baxter JP Houston G Pennington CRManganese requirement and toxicity in patients on home parenteralnutrition Clin Nutr 199817(5)227-230
56 Thompson P Dueksen DV Vitamin D de1047297ciency in patients receivinghome parenteral nutrition JPEN J Parenter Enteral Nutr 201135(4)499-504
57 Yusuf SW Rehman Q Casscells W Cardiomyopathy in associationwith selenium de1047297ciency A case report JPEN J Parenter Enteral Nutr 200226(1)63-66
58 Mirtallo JM Holcombe B Kochevar M Guenter P Parenteral nutri-tion product shortages The ASPEN strategy Nutr Clin Pract 201227(3)385-391
59 Gillanders L Angstmann K Ball P et al AuSPEN clinical practiceguidelines for home parenteral nutrition patient in Australia andNew Zealand Nutrition 200824998-1012
60 Tarleton S DiBaise JK Short bowel syndrome In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver Spring MDASPEN 2012511-522
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1207
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
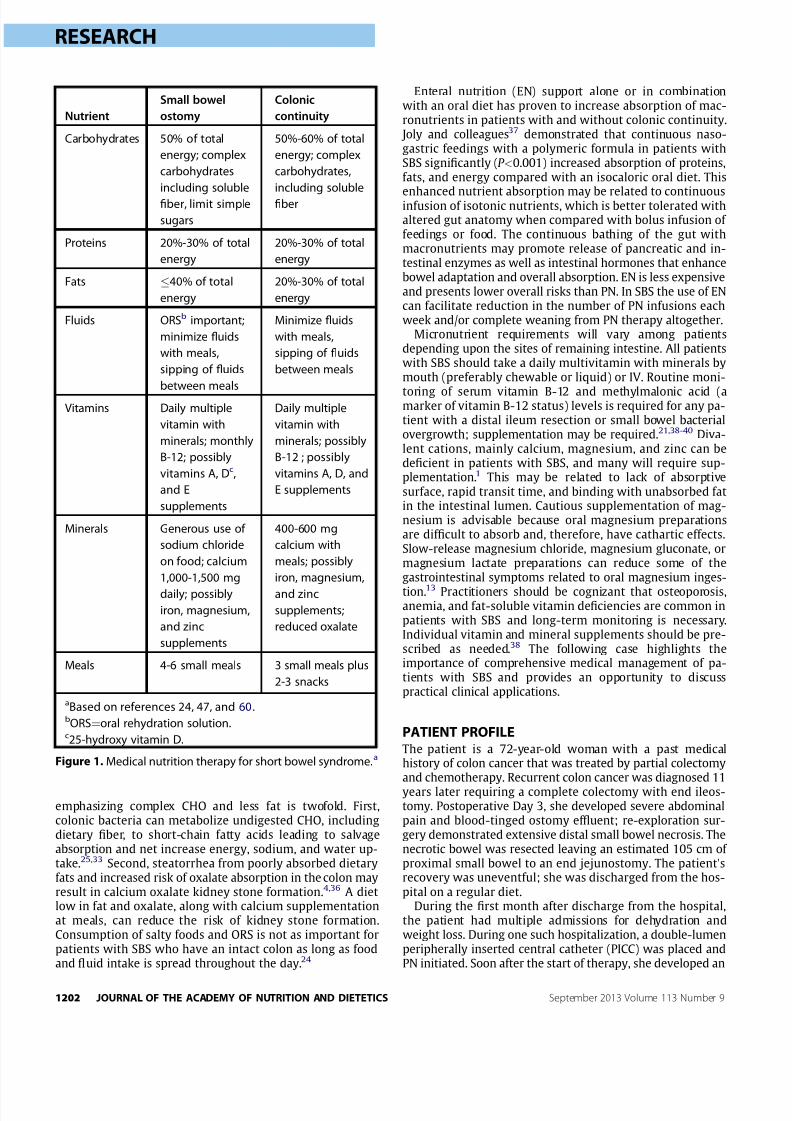
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 39
emphasizing complex CHO and less fat is twofold Firstcolonic bacteria can metabolize undigested CHO includingdietary 1047297ber to short-chain fatty acids leading to salvageabsorption and net increase energy sodium and water up-take2533 Second steatorrhea from poorly absorbed dietaryfats and increased risk of oxalate absorption in the colon mayresult in calcium oxalate kidney stone formation436 A dietlow in fat and oxalate along with calcium supplementationat meals can reduce the risk of kidney stone formationConsumption of salty foods and ORS is not as important forpatients with SBS who have an intact colon as long as foodand 1047298uid intake is spread throughout the day24
Enteral nutrition (EN) support alone or in combinationwith an oral diet has proven to increase absorption of mac-ronutrients in patients with and without colonic continuity Joly and colleagues37 demonstrated that continuous naso-gastric feedings with a polymeric formula in patients withSBS signi1047297cantly (P lt0001) increased absorption of proteinsfats and energy compared with an isocaloric oral diet This
enhanced nutrient absorption may be related to continuousinfusion of isotonic nutrients which is better tolerated withaltered gut anatomy when compared with bolus infusion of feedings or food The continuous bathing of the gut withmacronutrients may promote release of pancreatic and in-testinal enzymes as well as intestinal hormones that enhancebowel adaptation and overall absorption EN is less expensiveand presents lower overall risks than PN In SBS the use of ENcan facilitate reduction in the number of PN infusions eachweek andor complete weaning from PN therapy altogether
Micronutrient requirements will vary among patientsdepending upon the sites of remaining intestine All patientswith SBS should take a daily multivitamin with minerals bymouth (preferably chewable or liquid) or IV Routine moni-
toring of serum vitamin B-12 and methylmalonic acid (amarker of vitamin B-12 status) levels is required for any pa-tient with a distal ileum resection or small bowel bacterialovergrowth supplementation may be required2138-40 Diva-lent cations mainly calcium magnesium and zinc can bede1047297cient in patients with SBS and many will require sup-plementation1 This may be related to lack of absorptivesurface rapid transit time and binding with unabsorbed fatin the intestinal lumen Cautious supplementation of mag-nesium is advisable because oral magnesium preparationsare dif 1047297cult to absorb and therefore have cathartic effectsSlow-release magnesium chloride magnesium gluconate ormagnesium lactate preparations can reduce some of thegastrointestinal symptoms related to oral magnesium inges-
tion13 Practitioners should be cognizant that osteoporosisanemia and fat-soluble vitamin de1047297ciencies are common inpatients with SBS and long-term monitoring is necessaryIndividual vitamin and mineral supplements should be pre-scribed as needed38 The following case highlights theimportance of comprehensive medical management of pa-tients with SBS and provides an opportunity to discusspractical clinical applications
PATIENT PROFILEThe patient is a 72-year-old woman with a past medicalhistory of colon cancer that was treated by partial colectomyand chemotherapy Recurrent colon cancer was diagnosed 11years later requiring a complete colectomy with end ileos-tomy Postoperative Day 3 she developed severe abdominalpain and blood-tinged ostomy ef 1047298uent re-exploration sur-gery demonstrated extensive distal small bowel necrosis Thenecrotic bowel was resected leaving an estimated 105 cm of proximal small bowel to an end jejunostomy The patient rsquosrecovery was uneventful she was discharged from the hos-pital on a regular diet
During the 1047297rst month after discharge from the hospitalthe patient had multiple admissions for dehydration andweight loss During one such hospitalization a double-lumenperipherally inserted central catheter (PICC) was placed andPN initiated Soon after the start of therapy she developed an
Nutrient
Small bowel
ostomy
Colonic
continuity
Carbohydrates 50 of total
energy complex
carbohydrates
including soluble
1047297ber limit simple
sugars
50-60 of total
energy complex
carbohydrates
including soluble
1047297ber
Proteins 20-30 of total
energy
20-30 of total
energy
Fats 40 of total
energy
20-30 of total
energy
Fluids ORSb important
minimize 1047298uids
with meals
sipping of 1047298uids
between meals
Minimize 1047298uids
with meals
sipping of 1047298uids
between meals
Vitamins Daily multiple
vitamin with
minerals monthly
B-12 possibly
vitamins A Dc
and E
supplements
Daily multiple
vitamin with
minerals possibly
B-12 possibly
vitamins A D and
E supplements
Minerals Generous use of
sodium chloride
on food calcium
1000-1500 mg
daily possibly
iron magnesium
and zinc
supplements
400-600 mg
calcium with
meals possibly
iron magnesium
and zinc
supplements
reduced oxalate
Meals 4-6 small meals 3 small meals plus
2-3 snacks
aBased on references 24 47 and 60bORSfrac14oral rehydration solutionc25-hydroxy vitamin D
Figure 1 Medical nutrition therapy for short bowel syndromea
RESEARCH
1202 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 49
upper extremity deep vein thrombosis originating at the PICCinsertion site anticoagulation therapy was started Duringthe same hospitalization she developed fevers due to acatheter-related blood infection hypotension hypokalemiaand increased liver function tests On Hospital Day 17 thepatient was transferred to a tertiary care hospital for man-agement of SBS
TERTIARY CARE CENTER COURSEThe PICC was pulled and the patient was given a central lineholiday while antibiotic therapy was completed PeripheralPN (1 L 50-g dextrose and 20-g amino acids without lipidemulsion due to an egg allergy) was initiated along withantisecretory (ie PPI) and antimotility (ie DTO) medicationsHer diet was changed to six small meals with sipping of ORSbetween meals On Hospital Day 9 a tunneled central cath-eter was placed and the PN formulation was increased to 50 gdextrose 80 g amino acids infusing over 10 hours each night(490 kcalday) After intensive diet and infusion therapy ed-ucation the patient was discharged to home with the samePN formula diet and medications
AT HOMEAt home the patientrsquos oral intake increased with subsequentincrease in jejunostomy output necessitating adjustment of the PN volume to 15 L infused over 12 hours and titration of the DTO dose to 1 mL four times a day Six months afterdischarge PN she had stable serum chemistry valuesadequate hydration and she was slowly losing weight thePN infusion was changed to every other day and the anti-coagulation therapy was discontinued Subsequent serumchemistry results suggested negative 1047298uid balance and thepatient complained of extreme thirst and fatigue A 24-hoururine collection during an off day from PN resulted in only
400 mL urine The PN volume was increased to 24L over 12hours every other day and the patient was instructed tostrictly adhere to the diet and ORS therapy The patient hadimproved hydration on noninfusion days and the repeat 24-hour urine collection yielded 850 mL
The patient remains on every-other-day IV infusions for1047298uid vitamins minerals and electrolytes her weight hasstabilized at 86 kg (body mass index 307) Four years afterdischarge on PN her insurance provider mandated a switchedto noneamino acid-containing IV 1047298uid (Table) She continuesto strictly adhere to the diet regimen but has ceased usingORS because she no longer appreciates hydration bene1047297tsfrom the therapy Repeat chemistry data including normalvitamin levels and triene to tetraene ratio (an indication of
adequate absorption of essential fatty acids) plus stable bodymass index suggest adequate hydration and nutrient uptakewith the current management
DISCUSSIONHistorically loss of a signi1047297cant portion of the intestine wasphysically devastating and often a death sentence During thepast 50 years with the advent of PN and a better under-standing of small bowel physiology most patients with SBSrecover and live without signi1047297cant reduction in quality of life41-44 The case of the patient provided is an excellentexample of the metabolic consequences of massive smallbowel resection and the complications of infusion therapy
Per the Nutrition Care Process this patient had alteredgastrointestinal function due to extensive intestinal resectionas evidenced by inability to maintain hydration on an oraldiet Through aggressive medical management strict dietaryadherence and appreciable bowel adaptation she hasreduced her dependence on IV support and ORS by approx-imately 80 The dietary key to her success was the transition
from eating two large meals a day and drinking large volumesof sugar-containing beverages to separating food and 1047298uidingestion eating four small meals daily limiting simple sugarintake and sipping ORS daily Through trial and error thepatient has re1047297ned her schedule for antisecretory and anti-motility medications to maximize 1047298uid and electrolyte ab-sorption With remnant bowel length of only 105 cm it isunlikely she will ever completely wean from infusion ther-apy but with the conversion to every-other-day IV infusiontherapy she reports improved quality of life
Like many patients receiving home PN this patient hashad complications related to infusion therapy including athrombosis around a PICC catheter-related blood infectionsand liver function abnormalities The incidence of catheter-
related complications has been minimized by using singlelumen tunneled catheters to minimize the diameter of thecatheter and reduce the risk of clot formation limiting accessfor bacterial introduction with a single lumen and by re-education in aseptic technique Her liver function hasreturned to normal with the reduction of PN support andfewer central line infections (a frequent cause of abnormalliver tests) She will require lifelong monitoring of overallhealth and nutrition parameters vitamin levels and tracemineral levels as well as bone and vital organ health Every6 months the patient returns to clinic for monitoring She hasdual-energy x-ray absorptiometry scans every 2 years toassess her risk of metabolic bone disease (postmenopausaland SBS-related) Her overall prognosis is excellent given her
signi1047297cant small bowel adaptation the low rate of central linecomplications and reduced dependence on IV support
PRACTICE APPLICATIONSManagement of patients with SBS requires a thorough un-derstanding of intestinal physiology knowledge of pharma-conutrition therapy (ie the use of nutrients for therapeuticbene1047297t) close attention to detail and patience Each SBSpatient presents with unique nutrient requirements based onthe length site and health of their remaining intestineWhen caring for a patient with SBS a registered dietitian(RD) must know the exact intestinal anatomy so that a plan of care is developed to optimize bowel function and nourish thepatient If the operative report is unavailable or there isquestion as to the length or health of the remaining bowel anupper gastrointestinal with small bowel follow-throughbarium study provides vital information on the length andcondition of intestine remaining as well as transit time45 Inaddition RDs must have accurate intake and output data toassess 1047298uid balance awareness of all prescribed medicationsand supplements knowledge of IV access including cathetertip location weight history and laboratory data
Before hospital discharge there are many details RDsmust ensure are in place for patients with SBS (Figure 2)First the patient must understand the proper diet and oralhydration guidelines as well as the dosage and timing of
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1203
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 59
Table Data for a 72-year-old female patient from hospital admission to 4 y after massive small bowel resection
Patient data
Transfer to
tertiary
care center
Time After Discharge
3 wk 55 mo 6 mo 65 mo 75 mo 4 y
Body mass index 353 350 325 325 315 307 307
Laboratory dataa
Glucose (65-110 mgdL)b 169 148 115 122 100 119 89
Sodium (136-144 mEqL) 138 137 138 144 140 140 141
Potassium (36-51 mEqL) 33 44 42 42 42 38 42
Chloride (101-111 mEqL) 95 103 105 102 103 105 105
Bicarbonate (22-32 mEqL) 35 26 26 29 33 30 29
Blood urea nitrogen (7-19 mgdL)c 22 37 28 22 26 22 21
Creatinine (050-15 mgdL)d 10 08 10 13 12 10 096
Calcium (86-106 mgdL)e 77 93 89 95 92 87 95
Phosphorus (24-47 mgdL)f 38 39 40 38 42 36 35
Magnesium (18-25 mgdL)g 19 22 22 21 22 22 23
Total protein (gdL)h 60 78 79 76 67 76
Albumin (gdL)i 29 33 45 40 39 40
Total bilirubin (0-13 mgdL) j 16 095 09 129 097 08
Alkaline phosphatase (38-126 IUL) 239 204 320 217 163 95
24-h urine volume (mL)k 400 850
Measured energy expenditure (kcald) 1794
Respiratory quotient 069
Medications
Warfarin (mg) 4 4 0 0 0 0 0
Proton pump inhibitor (mgd) 40 40 40 40 40 40 30Deoderized tincture of opium (mLday) 12 3 3 3 3 3 4
Oral multivitamin 0 0 0 1l 1l 1l 1l
Vitamin D-3 (IUd) 0 0 0 0 0 0 1000
Calcium carbonate (mgd) 0 0 0 0 0 0 500
Oral rehydration solution (Ld) 1 1 1 1 1 1 0
Parenteral nutrition volume (Ld) 1 15 15 2m 24m 24m 24m
Parenteral nutrition energy (kcald) 490 490 490 410m 410m 410m 170m
Parenteral nutrition amino acids (gd) 80 60 60 60m 60m 60m 0
aRanges shown in parentheses are reference rangesb To convert mgdL glucose to mmolL multiply mgdL by 00555 To convert mmolL glucose to mgdL multiply mmolL by 1801 Glucose of 65 mgdLfrac14361 mmolLc To convert mgdL blood urea nitrogen to mmolL multiply mgdL by 0357 To convert mmolL blood urea nitrogen to m gdL multiply mmolL by 280 Blood urea nitrogen of 7 mg
dLfrac14250 mmolLd To convert mgdL creatinine to mmolL multiply mgdL by 884 To convert mmolL creatinine to mgdL multiply mmolL by 001 Creatinine of 05 mgdLfrac14442 mmolLe To convert mgdL calcium to mmolL multiply mgdL by 025 To convert mmolL calcium to mgdL multiply mmolL by 4 Calcium of 86 mgdLfrac14215 mmolLf To convert mgdL phosphorous to mmolL multiply mgdL by 0323 To convert mmolL phosphorous to mgdL multiply mmolL by 309 Phosphorous of 24 mgdLfrac14078 mmolLg To convert mgdL magnesium to mmolL multiply mgdL by 0411 To convert mmolL magnesium to mgdL multiply mmolL by 243 Magnesium of 18 mgdLfrac1474 mmolLh To convert gdL total protein to gL multiply gdL by 10 To convert gL total protein to gdL multiply gL by 01 Total protein of 60 gdLfrac1460 gLi To convert gdL albumin to gL multiply gdL by 10 To convert gL albumin to gdL multiply gL by 01 Albumin of 29 gdLfrac1429 gL j To convert mgdL total bilirubin to mmolL multiply mgdL by 171 To convert mmolL total bilirubin to mgdL multiply mmolL by 058 Total bilirubin of 16 mgdLfrac142737 mmolLk 24-h urine volume collected on a day without parenteral nutrition infusionlOff parenteral nutrition daymEvery other day
RESEARCH
1204 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 69
antimotility and acid-blocking medications46 In additionthe patient should be aware that the dosage of the medi-cations may change once he or she is home and eatingmore food Emphasis should be placed on proper eatingtechniques for example eating slowly resting after eatingminimal 1047298uid intake with the meal and sipping of 1047298uidsbetween meals47 If an ORS is required recipes to preparethe solution or information on where to purchase ORSmust be given to the patient The RD may have to reinforcethis information repeatedly before and after dischargeAdults in particular have dif 1047297culty changing their eatinghabits and may 1047297nd it challenging to adhere to the newguidelines until they begin to see reduction in stool outputand improved overall sense of well-being Also the patient
must have prescriptions for antisecretory therapy (eitherPPI or H2 blocker) and vitamin and mineral supplements if needed For those discharged on PN the patient and familyrequire education on catheter care and aseptic techniquefor infusion therapy before discharge4849 Patient moni-toring of oral intake stool and urine output as well asweight in the early period after hospital discharge willfacilitate decisions regarding medication adjustments andpossibly weaning of EN or PN support The patient andfamily may require education on proper techniques formeasuring body 1047298uid output at home48 Nursing support inthe home can help to reinforce the concepts of SBS man-agement and provide RDs essential insight to the homeenvironment
Checklist item Acute care setting Home care setting
Diet education Educate and reinforce as diet is advanced
in the hospital
Reinforce and adjust diet as bowel adapts
Laboratory data Daily chemistry panel including magnesium
and blood count
Twice weekly liver function testsBaseline vitamin and trace mineral
levels (A E Db folate B-12 iron zinc
copper and selenium) before discharge
Weekly comprehensive metabolic panel
including magnesium until stable then monthly
Annually vitamin and trace mineral levels
Weights and IOc
data
Daily weight
Daily IO data
Weekly weight
Once weekly IO data until stable then monthly
(more frequently if change in medical
management or status)
Medications Antimotility agent
PPId or H2 blockere
Multivitamin and mineral supplements
Antimotility agent
PPI or H2 blocker
Multivitamin and mineral supplements
Possibly pancreatic enzyme replacement or bile
acid sequestrant
Nutrition support If on enteral nutrition then know the
type of tube and enteral formula
If parenteral nutrition know the type of
catheter the position of the catheter
tip and the formula
Note any additional intravenous 1047298uids
Talk to the patient andor caregiver
Communicate with the home care company any
changes in enteral or parenteral formulas
Obtain report from home nurse
Monitoring frequency Daily Weekly until stable then reduce frequency
as appropriate
Other Know the exact post-operative intestinal
anatomyCommunicate long-term plan with the
primary care physician prior to discharge
Monitor for bowel adaptation and make
alterations in MNT
f
as possibleScreen for bone disease and anemia
aBased on references 46 and 59b25-hydroxy vitamin DcIOfrac14intake and output Includes oral enteral and parenteral intake plus urine stool and drain outputdPPIfrac14proton pump inhibitoreH2frac14histamine 2 antagonistf MNT frac14medical nutrition therapy
Figure 2 Checklist for registered dietitian management of patients with short bowel syndromea
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1205
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 79
After hospital discharge patients with SBS are best servedby frequent follow-up appointments with all members of thenutrition support team in particular the managing physicianand RD The primary goals of these appointments are toassess adherence to the prescribed therapies monitor 1047298uidelectrolyte hydration and nutritional status reinforce theprinciples of nutrition therapy and adjust the therapies as
necessary
50
Periodic weights and blood chemistry levels(including liver function tests) will help to determine theextent of bowel adaptation liver-related complications of PNand the possibility of weaning from EN or PN48 If a patientdevelops PN-related liver disease the workup should assessfor small bowel bacterial overgrowth blood infection and re-evaluate IV fat emulsion deliverymdashall of which can alter liverfunction51 Treatment may include a reduction in the amountand frequency of IV fat emulsion infusions (lt1 gkgday asinfrequently as once a week) with periodic monitoring foressential fatty acid de1047297ciency52
Baseline vitamin (eg folate B-12 and vitamins A D E)mineral (eg iron calcium and magnesium) and trace mineral(eg zinc copper and selenium and chromium and manganese
for PN patients) levels and dual-energy x-ray absorptiometryscan are required for comparison purposes in long-term followup53 The standard parenteral multivitamin and trace mineraladditives may not meet a patientrsquos exact requirements and cancause de1047297ciency or toxicity states over time54 For exampledaily trace mineralinfusions of 03 mg manganese over timecanlead to deposits in the brain55 and chronic standard multivi-tamin dosing of 200 IU vitamin D can cause insuf 1047297ciency orde1047297ciency states56 Further complicating the issue of moni-toring micronutrient levels of patients dependent on PN are theongoing product shortages These shortages have led to omis-sion or rationing of certain nutrients that can cause life-threatening de1047297ciency states505758 These levels should becheckedno less than every 6 to 12 months or more frequently if
abnormal levels are identi1047297ed5859 With time as a patient sta-bilizes and thrives at home the length of time between clinicvisits can be extended For patients with stable chronic SBS theminimum follow-up should occur every 6 to 12 months As withthe patientpro1047297le provided bowel adaptation can occur slowlyIt can take more than 2 years before adaptation has fullyoccurred to change the treatment plan and wean arti1047297cialnutrition support11
CONCLUSIONSManagement of SBS is complex and requires a concert of medical nutrition and pharmaceutical therapies to optimize1047298uid and nutrient absorption for survival Each patientrsquos
unique care plan depends on the amount and site of remaining intestine and the patientrsquos ability to adhere to themedical and nutrition therapies Some patients will be able tosurvive with antisecretory and anti-motility agents alongwith strict diet adherence alone whereas other patients willrequire lifelong infusion therapy In either case patients withSBS must have close follow-up with a specialized medicalteam to monitor for nutrient de1047297ciencies and potentialcomplications of SBS The most common long-term compli-cations include metabolic bone disease PN-related liver dis-ease nephrolithiasis anemia central line infection centralaccess problems (thrombosis and superior vena cava syn-drome due to vein stenosis) and vitamin and trace mineral
de1047297ciencies62738 Patients with SBS are medically complexand require long-term monitoring and revisions of the careplan The substantial bene1047297t of medical nutrition therapy iswhat makes these patients both challenging and extremelyrewarding for RDs to manage
References
1 Semrad CE Approach to the patient with diarrhea and malabsorp-tion In Goldmanrsquo s Cecil Medicine 24th ed Philadelphia PA ElsevierSaunders 2012895-913
2 OrsquoKeefe SJD Buchman AL Fishbein TM Jeejeebhoy KN Jeppesen PBShaffer J Short bowel syndrome and intestinal failure Consensus def-initions and overview Clin Gastroenterol Hepatol 20064(1)6-10
3 Nightingale J Woodward JM Guidelines for management of patientswith short bowel Gut 200655(suppl IV)iv1-iv12
4 Nightingale JMD Lennard-Jones JE Gertner DJ Wood SRBartram CI Colonic preservation reduces need for parenteral ther-apy increases incidence of renal stones but does not change highprevalence of gallstones in patients with a short bowel Gut 199233(11)1493-1497
5 Messing B Crenn P Beau P Boutron-Ruault MC Rambaud J-CMatuchansky C Long-term survival and parenteral nutritiondependence in adult patients with the short bowel syndrome
Gastroenterology 1999117(5)1043-10506 Jeejeebhoy KN Short bowel syndrome A nutritional and medical
approach Can Med Assoc J 2002166(10)1297-1302
7 Welch IM Cunningham KM Read NW Regulation of gastric emptyingby ileal nutrients in humans Gastroenterology 19 8894(2)401-404
8 Bines JE Intestinal failure A new era in clinical management J Gastroenterol Hepatol 200924(suppl 3)S86-S92
9 Bines JE Taylor RG Justice F et al Diet following small bowelresection In1047298uence of diet complexity on intestinal adaptationfollowing massive small bowel resection in a preclinical model
J Gastroenterol Hepatol 200217(11)1170-1179
10 Jeppesen PB Mortensen PB Enhancing bowel adaptation in shortbowel syndrome Curr Gastroenterol Rep 20024(4)338-347
11 Gouttebel MC Saint Aubert B ColetteC Astre C Monnier LHJoyeuxHIntestinal adaptation in patients with short bowel syndrome mea-surement by calcium absorption Dig Dis 198934(5)709-715
12 Buchman AL Etiology and initial management of short bowel syn-drome Gastroenterology 2006130(suppl)S5-S15
13 Parekh NR Steiger E Short bowel syndrome Curr Treat OptionsGastroenterol 200710(1)10-23
14 Lacy CF Armstrong LL Goldman MP Lance LL Drug InformationHandbook A Comprehensive Resource for All Clinicians and HealthcareProfessionals 19th ed Hudson OH Lexi-Comp 2010
15 Rubinoff MJ Piccione PR Holt PR Clonidine prolongs human intes-tine transit time Use of the lactulose-breath hydrogen test Am J Gastroenterol 198984(4)372-374
16 Buchman AL Fryer J Wallin A Ahn CW Polensky S Zaremba KClonidine reduces diarrhea and sodium loss in patients with prox-imal jejunostomy A controlled study JPEN J Parenter Enteral Nutr 200630(6)487-491
17 McDoniel K Taylor B Huey W et al Use of clonidine to decreaseintestinal 1047298uid losses in patients with high-output short-bowel
syndrome JPEN J Parenter Enteral Nutr 200428(4)265-268
18 Williams NS Evans P King RFGJ Gastric acid secretion andgastrin production in the short bowel syndrome Gut 198526(9)914-919
19 Quigley EMM Quera R Small intestinal bacterial overgrowthRoles of antibiotics prebiotics and probiotics Gastroenterology2006130(2 suppl 1)S78-S90
20 Gracey M The contaminated small bowel syndrome Pathogenesisdiagnosis and treatment Am J Clin Nutr 197932(1)234-243
21 Giannella RA Broitman SA Zamcheck N Vitamin B12 uptake byintestinal microorganisms Mechanism and relevance to syn-dromes of intestinal bacterial overgrowth J Clin Invest 197150(5)1100-1107
22 Bala L Ghoshal UC Ghoshal U et al Malabsorption syndrome withand without small intestinal bacterial overgrowth A study on
RESEARCH
1206 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 89
upper-gut aspirates using 1H NMR spectroscopy Magn Reson Med200656(4)738-744
23 Ziegler TR Cole CR Small bowel bacterial overgrowth in adults Apotential contributor to intestinal failure Curr Gastroenterol Rep20079(6)463-467
24 Byrne T Veglia L Camelio M et al Beyond the prescription Opti-mizing the diet of patients with short bowel syndrome Nutr ClinPract 200015(6)306-311
25 Nordgaard I Hansen BS Mortensen PB Colon as a digestive organ inpatientswith short bowel syndromeLancet 1994343(8894)373-376
26 Lykins TC Stockwell J Comprehensive modi1047297ed diet simpli1047297esnutrition management of adults with short bowel syndrome J AmDiet Assoc 199898(3)309-315
27 Matarese LE Steiger E Dietary and medical management of shortbowel syndrome in adult patients J Clin Gastroenterol 200640(suppl2)S85-S93
28 Woolf GM Miller C Kurian R Jeejeebhoy KN Diet for patients with ashort bowel High fat or high carbohydrate Gastroenterology198384(4)823-828
29 Atia A Girard-Pipau F Hebuterne X et al Macronutrient absorptioncharacteristics in human short bowel syndrome and jejunocolonicanastamosis Starch is the most important carbohydrate substratealthough pectin supplementation may modestly enhance short chainfatty acid production and 1047298uid absorption JPEN J Parenter EnteralNutr 201135(2)229-240
30 Tilg H Short bowel syndrome Searching for the proper diet Euro- pean J Gastroenterol Hepatol 200820(11)1061-1063
31 Shatnawei A Parekh NR Rhoda KM et al Intestinal failure man-agement at the Cleveland Clinic Arch Surg 2010145(6)521-527
32 Atia AN Buchman AL Oral rehydration solutions in non-choleradiarrhea A review Am J Gastroenterol 2009104(10)2596-2604
33 Kles KA Chang EB Short-chain fatty acids impact on intestinaladaptation in1047298ammation carcinoma and failure Gastroenterology2006130(suppl 2)S100-S105
34 Banks MR Farthing MJG Fluid and electrolyte transport in the smallintestine Curr Opin Gastroenterol 200218(2)176-181
35 Alam NH Bhatnagar S Chea-Woo E et al Multicenter randomizeddouble-blind clinical trial to evaluate the ef 1047297cacy and safety of areduced osmolarity oral hydration salt solution in children withwatery diarrhea Pediatrics 2001107(4)613-618
36 Rudman D Dedonis JL Fountain MT et al Hypocitraturia in patientswith gastrointestinal malabsorption N Engl J Med 1980303(12)657-661
37 Joly F Dray X Corcos O Barbot L Kapel N Messing B Tube feedingimproves intestinal absorption in short bowel syndrome patientsGastroenterology 2009136(3)824-831
38 Mziray-Andrew CH Sentongo TA Nutritional de1047297ciencies in intes-tinal failure Pediatr Clin North Am 200956(5)1185-1200
39 Okuda K Discovery of vitamin B12 in the liver and its absorptionfactor in the stomach A historical review J Gastroenterol Hepatol199914(4)301-308
40 Green R Indicators for assessing folate and vitamin B12 status and formonitoring the ef 1047297cacy of intervention strategies Food Nutr Bull200829(2 suppl)S52-S63
41 Malone M Longitudinal assessment of outcome health statusand changes in lifestyle associated with long-term home parenteraland enteral nutrition JPEN J Parenter Enteral Nutr 200226164-168
42 Baxter JP Fayers PM McKinlay AW A review of the quality of life of adult patients treated with long-term parenteral nutrition Clin Nutr 200625543-553
43 Huisman-de Waal G Schoonhoven L Jansen J Wanten G vanAchterberg T The impact of home parenteral nutrition on daily lifemdashA review Clin Nutr 200726275-288
44 Dudrick SJ Palesty JA Historical highlights of the development of total parenteral nutrition Surg Clin N Am 201191693-717
45 Shatari T Clark MA Lee JR Keighley MRB Reliability of radiographicmeasurement of small intestine length Colorectal Dis 20036(65)327-329
46 Kovacevich DS Frederick A Kelly D Nishikawa R Young L Standardsfor specialized nutrition support Home care patients Nutr Clin Pract 200520579-590
47 Matarese LE OrsquoKeefe SJ Kandie HM et al Short bowel syndromeClinical guidelines for nutrition management Nutr Clin Pract 200520(5)493-502
48 Kovacevich DS Orr ME Considerations for home nutrition supportIn The ASPEN Nutrition Support Practice Manual 2nd ed SilverSpring MD American Society of Parenteral and Enteral Nutrition2005371-377
49 Kumpf VJ Tillman EM Home parenteral nutrition Safe transitionfrom hospital to home Nutr Clin Pract 201227749-757
50 WinklerM Hagan E Albin J Homenutrition support In ASPEN Adult Nutrition Support Core Curriculum 2nded Silver Spring MD AmericanSociety of Parenteral and Enteral Nutrition 2012639-655
51 Kumpf VJ Parenteral nutrition-associated liver disease in adult andpediatric patients Nutr Clin Pract 200621279-290
52 Kumpf VJ Gervasio J Complications of parenteral nutrition In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver SpringMD American Society of Parenteral and Enteral Nutrition 2012384e297
53 Dreesen M Foulon V Vanhaecht K et al Guidelines recommenda-tions on care of adult patients receiving home parenteral nutritionA systematic review of global practices Clin Nutr 201231602-608
54 Howard L Ashley C Lyon D Shenkin A Autopsy tissue trace ele-ments in 8 long-term parenteral nutrition patients who receive thecurrent US Food and Drug Administration formulation JPEN J Parenter Enteral Nutr 200731(5)388-396
55 Reynolds N Blumsohn A Baxter JP Houston G Pennington CRManganese requirement and toxicity in patients on home parenteralnutrition Clin Nutr 199817(5)227-230
56 Thompson P Dueksen DV Vitamin D de1047297ciency in patients receivinghome parenteral nutrition JPEN J Parenter Enteral Nutr 201135(4)499-504
57 Yusuf SW Rehman Q Casscells W Cardiomyopathy in associationwith selenium de1047297ciency A case report JPEN J Parenter Enteral Nutr 200226(1)63-66
58 Mirtallo JM Holcombe B Kochevar M Guenter P Parenteral nutri-tion product shortages The ASPEN strategy Nutr Clin Pract 201227(3)385-391
59 Gillanders L Angstmann K Ball P et al AuSPEN clinical practiceguidelines for home parenteral nutrition patient in Australia andNew Zealand Nutrition 200824998-1012
60 Tarleton S DiBaise JK Short bowel syndrome In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver Spring MDASPEN 2012511-522
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1207
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9

7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 49
upper extremity deep vein thrombosis originating at the PICCinsertion site anticoagulation therapy was started Duringthe same hospitalization she developed fevers due to acatheter-related blood infection hypotension hypokalemiaand increased liver function tests On Hospital Day 17 thepatient was transferred to a tertiary care hospital for man-agement of SBS
TERTIARY CARE CENTER COURSEThe PICC was pulled and the patient was given a central lineholiday while antibiotic therapy was completed PeripheralPN (1 L 50-g dextrose and 20-g amino acids without lipidemulsion due to an egg allergy) was initiated along withantisecretory (ie PPI) and antimotility (ie DTO) medicationsHer diet was changed to six small meals with sipping of ORSbetween meals On Hospital Day 9 a tunneled central cath-eter was placed and the PN formulation was increased to 50 gdextrose 80 g amino acids infusing over 10 hours each night(490 kcalday) After intensive diet and infusion therapy ed-ucation the patient was discharged to home with the samePN formula diet and medications
AT HOMEAt home the patientrsquos oral intake increased with subsequentincrease in jejunostomy output necessitating adjustment of the PN volume to 15 L infused over 12 hours and titration of the DTO dose to 1 mL four times a day Six months afterdischarge PN she had stable serum chemistry valuesadequate hydration and she was slowly losing weight thePN infusion was changed to every other day and the anti-coagulation therapy was discontinued Subsequent serumchemistry results suggested negative 1047298uid balance and thepatient complained of extreme thirst and fatigue A 24-hoururine collection during an off day from PN resulted in only
400 mL urine The PN volume was increased to 24L over 12hours every other day and the patient was instructed tostrictly adhere to the diet and ORS therapy The patient hadimproved hydration on noninfusion days and the repeat 24-hour urine collection yielded 850 mL
The patient remains on every-other-day IV infusions for1047298uid vitamins minerals and electrolytes her weight hasstabilized at 86 kg (body mass index 307) Four years afterdischarge on PN her insurance provider mandated a switchedto noneamino acid-containing IV 1047298uid (Table) She continuesto strictly adhere to the diet regimen but has ceased usingORS because she no longer appreciates hydration bene1047297tsfrom the therapy Repeat chemistry data including normalvitamin levels and triene to tetraene ratio (an indication of
adequate absorption of essential fatty acids) plus stable bodymass index suggest adequate hydration and nutrient uptakewith the current management
DISCUSSIONHistorically loss of a signi1047297cant portion of the intestine wasphysically devastating and often a death sentence During thepast 50 years with the advent of PN and a better under-standing of small bowel physiology most patients with SBSrecover and live without signi1047297cant reduction in quality of life41-44 The case of the patient provided is an excellentexample of the metabolic consequences of massive smallbowel resection and the complications of infusion therapy
Per the Nutrition Care Process this patient had alteredgastrointestinal function due to extensive intestinal resectionas evidenced by inability to maintain hydration on an oraldiet Through aggressive medical management strict dietaryadherence and appreciable bowel adaptation she hasreduced her dependence on IV support and ORS by approx-imately 80 The dietary key to her success was the transition
from eating two large meals a day and drinking large volumesof sugar-containing beverages to separating food and 1047298uidingestion eating four small meals daily limiting simple sugarintake and sipping ORS daily Through trial and error thepatient has re1047297ned her schedule for antisecretory and anti-motility medications to maximize 1047298uid and electrolyte ab-sorption With remnant bowel length of only 105 cm it isunlikely she will ever completely wean from infusion ther-apy but with the conversion to every-other-day IV infusiontherapy she reports improved quality of life
Like many patients receiving home PN this patient hashad complications related to infusion therapy including athrombosis around a PICC catheter-related blood infectionsand liver function abnormalities The incidence of catheter-
related complications has been minimized by using singlelumen tunneled catheters to minimize the diameter of thecatheter and reduce the risk of clot formation limiting accessfor bacterial introduction with a single lumen and by re-education in aseptic technique Her liver function hasreturned to normal with the reduction of PN support andfewer central line infections (a frequent cause of abnormalliver tests) She will require lifelong monitoring of overallhealth and nutrition parameters vitamin levels and tracemineral levels as well as bone and vital organ health Every6 months the patient returns to clinic for monitoring She hasdual-energy x-ray absorptiometry scans every 2 years toassess her risk of metabolic bone disease (postmenopausaland SBS-related) Her overall prognosis is excellent given her
signi1047297cant small bowel adaptation the low rate of central linecomplications and reduced dependence on IV support
PRACTICE APPLICATIONSManagement of patients with SBS requires a thorough un-derstanding of intestinal physiology knowledge of pharma-conutrition therapy (ie the use of nutrients for therapeuticbene1047297t) close attention to detail and patience Each SBSpatient presents with unique nutrient requirements based onthe length site and health of their remaining intestineWhen caring for a patient with SBS a registered dietitian(RD) must know the exact intestinal anatomy so that a plan of care is developed to optimize bowel function and nourish thepatient If the operative report is unavailable or there isquestion as to the length or health of the remaining bowel anupper gastrointestinal with small bowel follow-throughbarium study provides vital information on the length andcondition of intestine remaining as well as transit time45 Inaddition RDs must have accurate intake and output data toassess 1047298uid balance awareness of all prescribed medicationsand supplements knowledge of IV access including cathetertip location weight history and laboratory data
Before hospital discharge there are many details RDsmust ensure are in place for patients with SBS (Figure 2)First the patient must understand the proper diet and oralhydration guidelines as well as the dosage and timing of
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1203
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 59
Table Data for a 72-year-old female patient from hospital admission to 4 y after massive small bowel resection
Patient data
Transfer to
tertiary
care center
Time After Discharge
3 wk 55 mo 6 mo 65 mo 75 mo 4 y
Body mass index 353 350 325 325 315 307 307
Laboratory dataa
Glucose (65-110 mgdL)b 169 148 115 122 100 119 89
Sodium (136-144 mEqL) 138 137 138 144 140 140 141
Potassium (36-51 mEqL) 33 44 42 42 42 38 42
Chloride (101-111 mEqL) 95 103 105 102 103 105 105
Bicarbonate (22-32 mEqL) 35 26 26 29 33 30 29
Blood urea nitrogen (7-19 mgdL)c 22 37 28 22 26 22 21
Creatinine (050-15 mgdL)d 10 08 10 13 12 10 096
Calcium (86-106 mgdL)e 77 93 89 95 92 87 95
Phosphorus (24-47 mgdL)f 38 39 40 38 42 36 35
Magnesium (18-25 mgdL)g 19 22 22 21 22 22 23
Total protein (gdL)h 60 78 79 76 67 76
Albumin (gdL)i 29 33 45 40 39 40
Total bilirubin (0-13 mgdL) j 16 095 09 129 097 08
Alkaline phosphatase (38-126 IUL) 239 204 320 217 163 95
24-h urine volume (mL)k 400 850
Measured energy expenditure (kcald) 1794
Respiratory quotient 069
Medications
Warfarin (mg) 4 4 0 0 0 0 0
Proton pump inhibitor (mgd) 40 40 40 40 40 40 30Deoderized tincture of opium (mLday) 12 3 3 3 3 3 4
Oral multivitamin 0 0 0 1l 1l 1l 1l
Vitamin D-3 (IUd) 0 0 0 0 0 0 1000
Calcium carbonate (mgd) 0 0 0 0 0 0 500
Oral rehydration solution (Ld) 1 1 1 1 1 1 0
Parenteral nutrition volume (Ld) 1 15 15 2m 24m 24m 24m
Parenteral nutrition energy (kcald) 490 490 490 410m 410m 410m 170m
Parenteral nutrition amino acids (gd) 80 60 60 60m 60m 60m 0
aRanges shown in parentheses are reference rangesb To convert mgdL glucose to mmolL multiply mgdL by 00555 To convert mmolL glucose to mgdL multiply mmolL by 1801 Glucose of 65 mgdLfrac14361 mmolLc To convert mgdL blood urea nitrogen to mmolL multiply mgdL by 0357 To convert mmolL blood urea nitrogen to m gdL multiply mmolL by 280 Blood urea nitrogen of 7 mg
dLfrac14250 mmolLd To convert mgdL creatinine to mmolL multiply mgdL by 884 To convert mmolL creatinine to mgdL multiply mmolL by 001 Creatinine of 05 mgdLfrac14442 mmolLe To convert mgdL calcium to mmolL multiply mgdL by 025 To convert mmolL calcium to mgdL multiply mmolL by 4 Calcium of 86 mgdLfrac14215 mmolLf To convert mgdL phosphorous to mmolL multiply mgdL by 0323 To convert mmolL phosphorous to mgdL multiply mmolL by 309 Phosphorous of 24 mgdLfrac14078 mmolLg To convert mgdL magnesium to mmolL multiply mgdL by 0411 To convert mmolL magnesium to mgdL multiply mmolL by 243 Magnesium of 18 mgdLfrac1474 mmolLh To convert gdL total protein to gL multiply gdL by 10 To convert gL total protein to gdL multiply gL by 01 Total protein of 60 gdLfrac1460 gLi To convert gdL albumin to gL multiply gdL by 10 To convert gL albumin to gdL multiply gL by 01 Albumin of 29 gdLfrac1429 gL j To convert mgdL total bilirubin to mmolL multiply mgdL by 171 To convert mmolL total bilirubin to mgdL multiply mmolL by 058 Total bilirubin of 16 mgdLfrac142737 mmolLk 24-h urine volume collected on a day without parenteral nutrition infusionlOff parenteral nutrition daymEvery other day
RESEARCH
1204 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 69
antimotility and acid-blocking medications46 In additionthe patient should be aware that the dosage of the medi-cations may change once he or she is home and eatingmore food Emphasis should be placed on proper eatingtechniques for example eating slowly resting after eatingminimal 1047298uid intake with the meal and sipping of 1047298uidsbetween meals47 If an ORS is required recipes to preparethe solution or information on where to purchase ORSmust be given to the patient The RD may have to reinforcethis information repeatedly before and after dischargeAdults in particular have dif 1047297culty changing their eatinghabits and may 1047297nd it challenging to adhere to the newguidelines until they begin to see reduction in stool outputand improved overall sense of well-being Also the patient
must have prescriptions for antisecretory therapy (eitherPPI or H2 blocker) and vitamin and mineral supplements if needed For those discharged on PN the patient and familyrequire education on catheter care and aseptic techniquefor infusion therapy before discharge4849 Patient moni-toring of oral intake stool and urine output as well asweight in the early period after hospital discharge willfacilitate decisions regarding medication adjustments andpossibly weaning of EN or PN support The patient andfamily may require education on proper techniques formeasuring body 1047298uid output at home48 Nursing support inthe home can help to reinforce the concepts of SBS man-agement and provide RDs essential insight to the homeenvironment
Checklist item Acute care setting Home care setting
Diet education Educate and reinforce as diet is advanced
in the hospital
Reinforce and adjust diet as bowel adapts
Laboratory data Daily chemistry panel including magnesium
and blood count
Twice weekly liver function testsBaseline vitamin and trace mineral
levels (A E Db folate B-12 iron zinc
copper and selenium) before discharge
Weekly comprehensive metabolic panel
including magnesium until stable then monthly
Annually vitamin and trace mineral levels
Weights and IOc
data
Daily weight
Daily IO data
Weekly weight
Once weekly IO data until stable then monthly
(more frequently if change in medical
management or status)
Medications Antimotility agent
PPId or H2 blockere
Multivitamin and mineral supplements
Antimotility agent
PPI or H2 blocker
Multivitamin and mineral supplements
Possibly pancreatic enzyme replacement or bile
acid sequestrant
Nutrition support If on enteral nutrition then know the
type of tube and enteral formula
If parenteral nutrition know the type of
catheter the position of the catheter
tip and the formula
Note any additional intravenous 1047298uids
Talk to the patient andor caregiver
Communicate with the home care company any
changes in enteral or parenteral formulas
Obtain report from home nurse
Monitoring frequency Daily Weekly until stable then reduce frequency
as appropriate
Other Know the exact post-operative intestinal
anatomyCommunicate long-term plan with the
primary care physician prior to discharge
Monitor for bowel adaptation and make
alterations in MNT
f
as possibleScreen for bone disease and anemia
aBased on references 46 and 59b25-hydroxy vitamin DcIOfrac14intake and output Includes oral enteral and parenteral intake plus urine stool and drain outputdPPIfrac14proton pump inhibitoreH2frac14histamine 2 antagonistf MNT frac14medical nutrition therapy
Figure 2 Checklist for registered dietitian management of patients with short bowel syndromea
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1205
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 79
After hospital discharge patients with SBS are best servedby frequent follow-up appointments with all members of thenutrition support team in particular the managing physicianand RD The primary goals of these appointments are toassess adherence to the prescribed therapies monitor 1047298uidelectrolyte hydration and nutritional status reinforce theprinciples of nutrition therapy and adjust the therapies as
necessary
50
Periodic weights and blood chemistry levels(including liver function tests) will help to determine theextent of bowel adaptation liver-related complications of PNand the possibility of weaning from EN or PN48 If a patientdevelops PN-related liver disease the workup should assessfor small bowel bacterial overgrowth blood infection and re-evaluate IV fat emulsion deliverymdashall of which can alter liverfunction51 Treatment may include a reduction in the amountand frequency of IV fat emulsion infusions (lt1 gkgday asinfrequently as once a week) with periodic monitoring foressential fatty acid de1047297ciency52
Baseline vitamin (eg folate B-12 and vitamins A D E)mineral (eg iron calcium and magnesium) and trace mineral(eg zinc copper and selenium and chromium and manganese
for PN patients) levels and dual-energy x-ray absorptiometryscan are required for comparison purposes in long-term followup53 The standard parenteral multivitamin and trace mineraladditives may not meet a patientrsquos exact requirements and cancause de1047297ciency or toxicity states over time54 For exampledaily trace mineralinfusions of 03 mg manganese over timecanlead to deposits in the brain55 and chronic standard multivi-tamin dosing of 200 IU vitamin D can cause insuf 1047297ciency orde1047297ciency states56 Further complicating the issue of moni-toring micronutrient levels of patients dependent on PN are theongoing product shortages These shortages have led to omis-sion or rationing of certain nutrients that can cause life-threatening de1047297ciency states505758 These levels should becheckedno less than every 6 to 12 months or more frequently if
abnormal levels are identi1047297ed5859 With time as a patient sta-bilizes and thrives at home the length of time between clinicvisits can be extended For patients with stable chronic SBS theminimum follow-up should occur every 6 to 12 months As withthe patientpro1047297le provided bowel adaptation can occur slowlyIt can take more than 2 years before adaptation has fullyoccurred to change the treatment plan and wean arti1047297cialnutrition support11
CONCLUSIONSManagement of SBS is complex and requires a concert of medical nutrition and pharmaceutical therapies to optimize1047298uid and nutrient absorption for survival Each patientrsquos
unique care plan depends on the amount and site of remaining intestine and the patientrsquos ability to adhere to themedical and nutrition therapies Some patients will be able tosurvive with antisecretory and anti-motility agents alongwith strict diet adherence alone whereas other patients willrequire lifelong infusion therapy In either case patients withSBS must have close follow-up with a specialized medicalteam to monitor for nutrient de1047297ciencies and potentialcomplications of SBS The most common long-term compli-cations include metabolic bone disease PN-related liver dis-ease nephrolithiasis anemia central line infection centralaccess problems (thrombosis and superior vena cava syn-drome due to vein stenosis) and vitamin and trace mineral
de1047297ciencies62738 Patients with SBS are medically complexand require long-term monitoring and revisions of the careplan The substantial bene1047297t of medical nutrition therapy iswhat makes these patients both challenging and extremelyrewarding for RDs to manage
References
1 Semrad CE Approach to the patient with diarrhea and malabsorp-tion In Goldmanrsquo s Cecil Medicine 24th ed Philadelphia PA ElsevierSaunders 2012895-913
2 OrsquoKeefe SJD Buchman AL Fishbein TM Jeejeebhoy KN Jeppesen PBShaffer J Short bowel syndrome and intestinal failure Consensus def-initions and overview Clin Gastroenterol Hepatol 20064(1)6-10
3 Nightingale J Woodward JM Guidelines for management of patientswith short bowel Gut 200655(suppl IV)iv1-iv12
4 Nightingale JMD Lennard-Jones JE Gertner DJ Wood SRBartram CI Colonic preservation reduces need for parenteral ther-apy increases incidence of renal stones but does not change highprevalence of gallstones in patients with a short bowel Gut 199233(11)1493-1497
5 Messing B Crenn P Beau P Boutron-Ruault MC Rambaud J-CMatuchansky C Long-term survival and parenteral nutritiondependence in adult patients with the short bowel syndrome
Gastroenterology 1999117(5)1043-10506 Jeejeebhoy KN Short bowel syndrome A nutritional and medical
approach Can Med Assoc J 2002166(10)1297-1302
7 Welch IM Cunningham KM Read NW Regulation of gastric emptyingby ileal nutrients in humans Gastroenterology 19 8894(2)401-404
8 Bines JE Intestinal failure A new era in clinical management J Gastroenterol Hepatol 200924(suppl 3)S86-S92
9 Bines JE Taylor RG Justice F et al Diet following small bowelresection In1047298uence of diet complexity on intestinal adaptationfollowing massive small bowel resection in a preclinical model
J Gastroenterol Hepatol 200217(11)1170-1179
10 Jeppesen PB Mortensen PB Enhancing bowel adaptation in shortbowel syndrome Curr Gastroenterol Rep 20024(4)338-347
11 Gouttebel MC Saint Aubert B ColetteC Astre C Monnier LHJoyeuxHIntestinal adaptation in patients with short bowel syndrome mea-surement by calcium absorption Dig Dis 198934(5)709-715
12 Buchman AL Etiology and initial management of short bowel syn-drome Gastroenterology 2006130(suppl)S5-S15
13 Parekh NR Steiger E Short bowel syndrome Curr Treat OptionsGastroenterol 200710(1)10-23
14 Lacy CF Armstrong LL Goldman MP Lance LL Drug InformationHandbook A Comprehensive Resource for All Clinicians and HealthcareProfessionals 19th ed Hudson OH Lexi-Comp 2010
15 Rubinoff MJ Piccione PR Holt PR Clonidine prolongs human intes-tine transit time Use of the lactulose-breath hydrogen test Am J Gastroenterol 198984(4)372-374
16 Buchman AL Fryer J Wallin A Ahn CW Polensky S Zaremba KClonidine reduces diarrhea and sodium loss in patients with prox-imal jejunostomy A controlled study JPEN J Parenter Enteral Nutr 200630(6)487-491
17 McDoniel K Taylor B Huey W et al Use of clonidine to decreaseintestinal 1047298uid losses in patients with high-output short-bowel
syndrome JPEN J Parenter Enteral Nutr 200428(4)265-268
18 Williams NS Evans P King RFGJ Gastric acid secretion andgastrin production in the short bowel syndrome Gut 198526(9)914-919
19 Quigley EMM Quera R Small intestinal bacterial overgrowthRoles of antibiotics prebiotics and probiotics Gastroenterology2006130(2 suppl 1)S78-S90
20 Gracey M The contaminated small bowel syndrome Pathogenesisdiagnosis and treatment Am J Clin Nutr 197932(1)234-243
21 Giannella RA Broitman SA Zamcheck N Vitamin B12 uptake byintestinal microorganisms Mechanism and relevance to syn-dromes of intestinal bacterial overgrowth J Clin Invest 197150(5)1100-1107
22 Bala L Ghoshal UC Ghoshal U et al Malabsorption syndrome withand without small intestinal bacterial overgrowth A study on
RESEARCH
1206 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 89
upper-gut aspirates using 1H NMR spectroscopy Magn Reson Med200656(4)738-744
23 Ziegler TR Cole CR Small bowel bacterial overgrowth in adults Apotential contributor to intestinal failure Curr Gastroenterol Rep20079(6)463-467
24 Byrne T Veglia L Camelio M et al Beyond the prescription Opti-mizing the diet of patients with short bowel syndrome Nutr ClinPract 200015(6)306-311
25 Nordgaard I Hansen BS Mortensen PB Colon as a digestive organ inpatientswith short bowel syndromeLancet 1994343(8894)373-376
26 Lykins TC Stockwell J Comprehensive modi1047297ed diet simpli1047297esnutrition management of adults with short bowel syndrome J AmDiet Assoc 199898(3)309-315
27 Matarese LE Steiger E Dietary and medical management of shortbowel syndrome in adult patients J Clin Gastroenterol 200640(suppl2)S85-S93
28 Woolf GM Miller C Kurian R Jeejeebhoy KN Diet for patients with ashort bowel High fat or high carbohydrate Gastroenterology198384(4)823-828
29 Atia A Girard-Pipau F Hebuterne X et al Macronutrient absorptioncharacteristics in human short bowel syndrome and jejunocolonicanastamosis Starch is the most important carbohydrate substratealthough pectin supplementation may modestly enhance short chainfatty acid production and 1047298uid absorption JPEN J Parenter EnteralNutr 201135(2)229-240
30 Tilg H Short bowel syndrome Searching for the proper diet Euro- pean J Gastroenterol Hepatol 200820(11)1061-1063
31 Shatnawei A Parekh NR Rhoda KM et al Intestinal failure man-agement at the Cleveland Clinic Arch Surg 2010145(6)521-527
32 Atia AN Buchman AL Oral rehydration solutions in non-choleradiarrhea A review Am J Gastroenterol 2009104(10)2596-2604
33 Kles KA Chang EB Short-chain fatty acids impact on intestinaladaptation in1047298ammation carcinoma and failure Gastroenterology2006130(suppl 2)S100-S105
34 Banks MR Farthing MJG Fluid and electrolyte transport in the smallintestine Curr Opin Gastroenterol 200218(2)176-181
35 Alam NH Bhatnagar S Chea-Woo E et al Multicenter randomizeddouble-blind clinical trial to evaluate the ef 1047297cacy and safety of areduced osmolarity oral hydration salt solution in children withwatery diarrhea Pediatrics 2001107(4)613-618
36 Rudman D Dedonis JL Fountain MT et al Hypocitraturia in patientswith gastrointestinal malabsorption N Engl J Med 1980303(12)657-661
37 Joly F Dray X Corcos O Barbot L Kapel N Messing B Tube feedingimproves intestinal absorption in short bowel syndrome patientsGastroenterology 2009136(3)824-831
38 Mziray-Andrew CH Sentongo TA Nutritional de1047297ciencies in intes-tinal failure Pediatr Clin North Am 200956(5)1185-1200
39 Okuda K Discovery of vitamin B12 in the liver and its absorptionfactor in the stomach A historical review J Gastroenterol Hepatol199914(4)301-308
40 Green R Indicators for assessing folate and vitamin B12 status and formonitoring the ef 1047297cacy of intervention strategies Food Nutr Bull200829(2 suppl)S52-S63
41 Malone M Longitudinal assessment of outcome health statusand changes in lifestyle associated with long-term home parenteraland enteral nutrition JPEN J Parenter Enteral Nutr 200226164-168
42 Baxter JP Fayers PM McKinlay AW A review of the quality of life of adult patients treated with long-term parenteral nutrition Clin Nutr 200625543-553
43 Huisman-de Waal G Schoonhoven L Jansen J Wanten G vanAchterberg T The impact of home parenteral nutrition on daily lifemdashA review Clin Nutr 200726275-288
44 Dudrick SJ Palesty JA Historical highlights of the development of total parenteral nutrition Surg Clin N Am 201191693-717
45 Shatari T Clark MA Lee JR Keighley MRB Reliability of radiographicmeasurement of small intestine length Colorectal Dis 20036(65)327-329
46 Kovacevich DS Frederick A Kelly D Nishikawa R Young L Standardsfor specialized nutrition support Home care patients Nutr Clin Pract 200520579-590
47 Matarese LE OrsquoKeefe SJ Kandie HM et al Short bowel syndromeClinical guidelines for nutrition management Nutr Clin Pract 200520(5)493-502
48 Kovacevich DS Orr ME Considerations for home nutrition supportIn The ASPEN Nutrition Support Practice Manual 2nd ed SilverSpring MD American Society of Parenteral and Enteral Nutrition2005371-377
49 Kumpf VJ Tillman EM Home parenteral nutrition Safe transitionfrom hospital to home Nutr Clin Pract 201227749-757
50 WinklerM Hagan E Albin J Homenutrition support In ASPEN Adult Nutrition Support Core Curriculum 2nded Silver Spring MD AmericanSociety of Parenteral and Enteral Nutrition 2012639-655
51 Kumpf VJ Parenteral nutrition-associated liver disease in adult andpediatric patients Nutr Clin Pract 200621279-290
52 Kumpf VJ Gervasio J Complications of parenteral nutrition In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver SpringMD American Society of Parenteral and Enteral Nutrition 2012384e297
53 Dreesen M Foulon V Vanhaecht K et al Guidelines recommenda-tions on care of adult patients receiving home parenteral nutritionA systematic review of global practices Clin Nutr 201231602-608
54 Howard L Ashley C Lyon D Shenkin A Autopsy tissue trace ele-ments in 8 long-term parenteral nutrition patients who receive thecurrent US Food and Drug Administration formulation JPEN J Parenter Enteral Nutr 200731(5)388-396
55 Reynolds N Blumsohn A Baxter JP Houston G Pennington CRManganese requirement and toxicity in patients on home parenteralnutrition Clin Nutr 199817(5)227-230
56 Thompson P Dueksen DV Vitamin D de1047297ciency in patients receivinghome parenteral nutrition JPEN J Parenter Enteral Nutr 201135(4)499-504
57 Yusuf SW Rehman Q Casscells W Cardiomyopathy in associationwith selenium de1047297ciency A case report JPEN J Parenter Enteral Nutr 200226(1)63-66
58 Mirtallo JM Holcombe B Kochevar M Guenter P Parenteral nutri-tion product shortages The ASPEN strategy Nutr Clin Pract 201227(3)385-391
59 Gillanders L Angstmann K Ball P et al AuSPEN clinical practiceguidelines for home parenteral nutrition patient in Australia andNew Zealand Nutrition 200824998-1012
60 Tarleton S DiBaise JK Short bowel syndrome In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver Spring MDASPEN 2012511-522
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1207
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
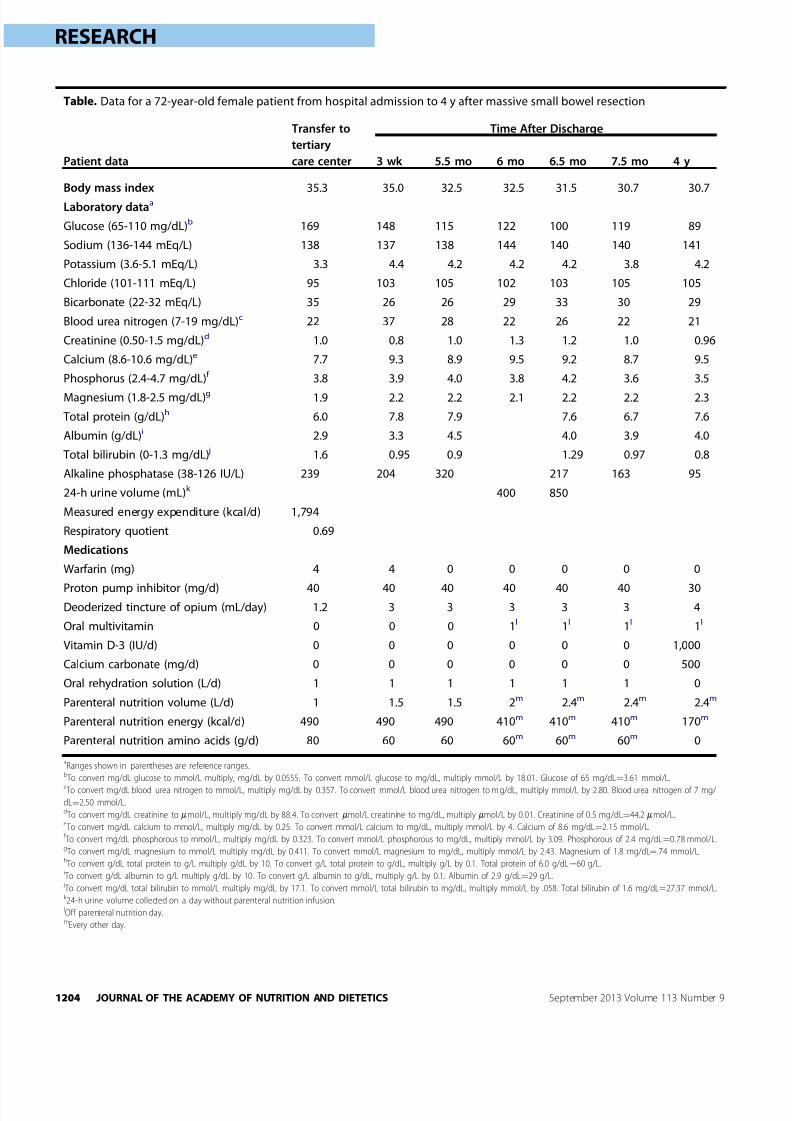
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 59
Table Data for a 72-year-old female patient from hospital admission to 4 y after massive small bowel resection
Patient data
Transfer to
tertiary
care center
Time After Discharge
3 wk 55 mo 6 mo 65 mo 75 mo 4 y
Body mass index 353 350 325 325 315 307 307
Laboratory dataa
Glucose (65-110 mgdL)b 169 148 115 122 100 119 89
Sodium (136-144 mEqL) 138 137 138 144 140 140 141
Potassium (36-51 mEqL) 33 44 42 42 42 38 42
Chloride (101-111 mEqL) 95 103 105 102 103 105 105
Bicarbonate (22-32 mEqL) 35 26 26 29 33 30 29
Blood urea nitrogen (7-19 mgdL)c 22 37 28 22 26 22 21
Creatinine (050-15 mgdL)d 10 08 10 13 12 10 096
Calcium (86-106 mgdL)e 77 93 89 95 92 87 95
Phosphorus (24-47 mgdL)f 38 39 40 38 42 36 35
Magnesium (18-25 mgdL)g 19 22 22 21 22 22 23
Total protein (gdL)h 60 78 79 76 67 76
Albumin (gdL)i 29 33 45 40 39 40
Total bilirubin (0-13 mgdL) j 16 095 09 129 097 08
Alkaline phosphatase (38-126 IUL) 239 204 320 217 163 95
24-h urine volume (mL)k 400 850
Measured energy expenditure (kcald) 1794
Respiratory quotient 069
Medications
Warfarin (mg) 4 4 0 0 0 0 0
Proton pump inhibitor (mgd) 40 40 40 40 40 40 30Deoderized tincture of opium (mLday) 12 3 3 3 3 3 4
Oral multivitamin 0 0 0 1l 1l 1l 1l
Vitamin D-3 (IUd) 0 0 0 0 0 0 1000
Calcium carbonate (mgd) 0 0 0 0 0 0 500
Oral rehydration solution (Ld) 1 1 1 1 1 1 0
Parenteral nutrition volume (Ld) 1 15 15 2m 24m 24m 24m
Parenteral nutrition energy (kcald) 490 490 490 410m 410m 410m 170m
Parenteral nutrition amino acids (gd) 80 60 60 60m 60m 60m 0
aRanges shown in parentheses are reference rangesb To convert mgdL glucose to mmolL multiply mgdL by 00555 To convert mmolL glucose to mgdL multiply mmolL by 1801 Glucose of 65 mgdLfrac14361 mmolLc To convert mgdL blood urea nitrogen to mmolL multiply mgdL by 0357 To convert mmolL blood urea nitrogen to m gdL multiply mmolL by 280 Blood urea nitrogen of 7 mg
dLfrac14250 mmolLd To convert mgdL creatinine to mmolL multiply mgdL by 884 To convert mmolL creatinine to mgdL multiply mmolL by 001 Creatinine of 05 mgdLfrac14442 mmolLe To convert mgdL calcium to mmolL multiply mgdL by 025 To convert mmolL calcium to mgdL multiply mmolL by 4 Calcium of 86 mgdLfrac14215 mmolLf To convert mgdL phosphorous to mmolL multiply mgdL by 0323 To convert mmolL phosphorous to mgdL multiply mmolL by 309 Phosphorous of 24 mgdLfrac14078 mmolLg To convert mgdL magnesium to mmolL multiply mgdL by 0411 To convert mmolL magnesium to mgdL multiply mmolL by 243 Magnesium of 18 mgdLfrac1474 mmolLh To convert gdL total protein to gL multiply gdL by 10 To convert gL total protein to gdL multiply gL by 01 Total protein of 60 gdLfrac1460 gLi To convert gdL albumin to gL multiply gdL by 10 To convert gL albumin to gdL multiply gL by 01 Albumin of 29 gdLfrac1429 gL j To convert mgdL total bilirubin to mmolL multiply mgdL by 171 To convert mmolL total bilirubin to mgdL multiply mmolL by 058 Total bilirubin of 16 mgdLfrac142737 mmolLk 24-h urine volume collected on a day without parenteral nutrition infusionlOff parenteral nutrition daymEvery other day
RESEARCH
1204 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 69
antimotility and acid-blocking medications46 In additionthe patient should be aware that the dosage of the medi-cations may change once he or she is home and eatingmore food Emphasis should be placed on proper eatingtechniques for example eating slowly resting after eatingminimal 1047298uid intake with the meal and sipping of 1047298uidsbetween meals47 If an ORS is required recipes to preparethe solution or information on where to purchase ORSmust be given to the patient The RD may have to reinforcethis information repeatedly before and after dischargeAdults in particular have dif 1047297culty changing their eatinghabits and may 1047297nd it challenging to adhere to the newguidelines until they begin to see reduction in stool outputand improved overall sense of well-being Also the patient
must have prescriptions for antisecretory therapy (eitherPPI or H2 blocker) and vitamin and mineral supplements if needed For those discharged on PN the patient and familyrequire education on catheter care and aseptic techniquefor infusion therapy before discharge4849 Patient moni-toring of oral intake stool and urine output as well asweight in the early period after hospital discharge willfacilitate decisions regarding medication adjustments andpossibly weaning of EN or PN support The patient andfamily may require education on proper techniques formeasuring body 1047298uid output at home48 Nursing support inthe home can help to reinforce the concepts of SBS man-agement and provide RDs essential insight to the homeenvironment
Checklist item Acute care setting Home care setting
Diet education Educate and reinforce as diet is advanced
in the hospital
Reinforce and adjust diet as bowel adapts
Laboratory data Daily chemistry panel including magnesium
and blood count
Twice weekly liver function testsBaseline vitamin and trace mineral
levels (A E Db folate B-12 iron zinc
copper and selenium) before discharge
Weekly comprehensive metabolic panel
including magnesium until stable then monthly
Annually vitamin and trace mineral levels
Weights and IOc
data
Daily weight
Daily IO data
Weekly weight
Once weekly IO data until stable then monthly
(more frequently if change in medical
management or status)
Medications Antimotility agent
PPId or H2 blockere
Multivitamin and mineral supplements
Antimotility agent
PPI or H2 blocker
Multivitamin and mineral supplements
Possibly pancreatic enzyme replacement or bile
acid sequestrant
Nutrition support If on enteral nutrition then know the
type of tube and enteral formula
If parenteral nutrition know the type of
catheter the position of the catheter
tip and the formula
Note any additional intravenous 1047298uids
Talk to the patient andor caregiver
Communicate with the home care company any
changes in enteral or parenteral formulas
Obtain report from home nurse
Monitoring frequency Daily Weekly until stable then reduce frequency
as appropriate
Other Know the exact post-operative intestinal
anatomyCommunicate long-term plan with the
primary care physician prior to discharge
Monitor for bowel adaptation and make
alterations in MNT
f
as possibleScreen for bone disease and anemia
aBased on references 46 and 59b25-hydroxy vitamin DcIOfrac14intake and output Includes oral enteral and parenteral intake plus urine stool and drain outputdPPIfrac14proton pump inhibitoreH2frac14histamine 2 antagonistf MNT frac14medical nutrition therapy
Figure 2 Checklist for registered dietitian management of patients with short bowel syndromea
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1205
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 79
After hospital discharge patients with SBS are best servedby frequent follow-up appointments with all members of thenutrition support team in particular the managing physicianand RD The primary goals of these appointments are toassess adherence to the prescribed therapies monitor 1047298uidelectrolyte hydration and nutritional status reinforce theprinciples of nutrition therapy and adjust the therapies as
necessary
50
Periodic weights and blood chemistry levels(including liver function tests) will help to determine theextent of bowel adaptation liver-related complications of PNand the possibility of weaning from EN or PN48 If a patientdevelops PN-related liver disease the workup should assessfor small bowel bacterial overgrowth blood infection and re-evaluate IV fat emulsion deliverymdashall of which can alter liverfunction51 Treatment may include a reduction in the amountand frequency of IV fat emulsion infusions (lt1 gkgday asinfrequently as once a week) with periodic monitoring foressential fatty acid de1047297ciency52
Baseline vitamin (eg folate B-12 and vitamins A D E)mineral (eg iron calcium and magnesium) and trace mineral(eg zinc copper and selenium and chromium and manganese
for PN patients) levels and dual-energy x-ray absorptiometryscan are required for comparison purposes in long-term followup53 The standard parenteral multivitamin and trace mineraladditives may not meet a patientrsquos exact requirements and cancause de1047297ciency or toxicity states over time54 For exampledaily trace mineralinfusions of 03 mg manganese over timecanlead to deposits in the brain55 and chronic standard multivi-tamin dosing of 200 IU vitamin D can cause insuf 1047297ciency orde1047297ciency states56 Further complicating the issue of moni-toring micronutrient levels of patients dependent on PN are theongoing product shortages These shortages have led to omis-sion or rationing of certain nutrients that can cause life-threatening de1047297ciency states505758 These levels should becheckedno less than every 6 to 12 months or more frequently if
abnormal levels are identi1047297ed5859 With time as a patient sta-bilizes and thrives at home the length of time between clinicvisits can be extended For patients with stable chronic SBS theminimum follow-up should occur every 6 to 12 months As withthe patientpro1047297le provided bowel adaptation can occur slowlyIt can take more than 2 years before adaptation has fullyoccurred to change the treatment plan and wean arti1047297cialnutrition support11
CONCLUSIONSManagement of SBS is complex and requires a concert of medical nutrition and pharmaceutical therapies to optimize1047298uid and nutrient absorption for survival Each patientrsquos
unique care plan depends on the amount and site of remaining intestine and the patientrsquos ability to adhere to themedical and nutrition therapies Some patients will be able tosurvive with antisecretory and anti-motility agents alongwith strict diet adherence alone whereas other patients willrequire lifelong infusion therapy In either case patients withSBS must have close follow-up with a specialized medicalteam to monitor for nutrient de1047297ciencies and potentialcomplications of SBS The most common long-term compli-cations include metabolic bone disease PN-related liver dis-ease nephrolithiasis anemia central line infection centralaccess problems (thrombosis and superior vena cava syn-drome due to vein stenosis) and vitamin and trace mineral
de1047297ciencies62738 Patients with SBS are medically complexand require long-term monitoring and revisions of the careplan The substantial bene1047297t of medical nutrition therapy iswhat makes these patients both challenging and extremelyrewarding for RDs to manage
References
1 Semrad CE Approach to the patient with diarrhea and malabsorp-tion In Goldmanrsquo s Cecil Medicine 24th ed Philadelphia PA ElsevierSaunders 2012895-913
2 OrsquoKeefe SJD Buchman AL Fishbein TM Jeejeebhoy KN Jeppesen PBShaffer J Short bowel syndrome and intestinal failure Consensus def-initions and overview Clin Gastroenterol Hepatol 20064(1)6-10
3 Nightingale J Woodward JM Guidelines for management of patientswith short bowel Gut 200655(suppl IV)iv1-iv12
4 Nightingale JMD Lennard-Jones JE Gertner DJ Wood SRBartram CI Colonic preservation reduces need for parenteral ther-apy increases incidence of renal stones but does not change highprevalence of gallstones in patients with a short bowel Gut 199233(11)1493-1497
5 Messing B Crenn P Beau P Boutron-Ruault MC Rambaud J-CMatuchansky C Long-term survival and parenteral nutritiondependence in adult patients with the short bowel syndrome
Gastroenterology 1999117(5)1043-10506 Jeejeebhoy KN Short bowel syndrome A nutritional and medical
approach Can Med Assoc J 2002166(10)1297-1302
7 Welch IM Cunningham KM Read NW Regulation of gastric emptyingby ileal nutrients in humans Gastroenterology 19 8894(2)401-404
8 Bines JE Intestinal failure A new era in clinical management J Gastroenterol Hepatol 200924(suppl 3)S86-S92
9 Bines JE Taylor RG Justice F et al Diet following small bowelresection In1047298uence of diet complexity on intestinal adaptationfollowing massive small bowel resection in a preclinical model
J Gastroenterol Hepatol 200217(11)1170-1179
10 Jeppesen PB Mortensen PB Enhancing bowel adaptation in shortbowel syndrome Curr Gastroenterol Rep 20024(4)338-347
11 Gouttebel MC Saint Aubert B ColetteC Astre C Monnier LHJoyeuxHIntestinal adaptation in patients with short bowel syndrome mea-surement by calcium absorption Dig Dis 198934(5)709-715
12 Buchman AL Etiology and initial management of short bowel syn-drome Gastroenterology 2006130(suppl)S5-S15
13 Parekh NR Steiger E Short bowel syndrome Curr Treat OptionsGastroenterol 200710(1)10-23
14 Lacy CF Armstrong LL Goldman MP Lance LL Drug InformationHandbook A Comprehensive Resource for All Clinicians and HealthcareProfessionals 19th ed Hudson OH Lexi-Comp 2010
15 Rubinoff MJ Piccione PR Holt PR Clonidine prolongs human intes-tine transit time Use of the lactulose-breath hydrogen test Am J Gastroenterol 198984(4)372-374
16 Buchman AL Fryer J Wallin A Ahn CW Polensky S Zaremba KClonidine reduces diarrhea and sodium loss in patients with prox-imal jejunostomy A controlled study JPEN J Parenter Enteral Nutr 200630(6)487-491
17 McDoniel K Taylor B Huey W et al Use of clonidine to decreaseintestinal 1047298uid losses in patients with high-output short-bowel
syndrome JPEN J Parenter Enteral Nutr 200428(4)265-268
18 Williams NS Evans P King RFGJ Gastric acid secretion andgastrin production in the short bowel syndrome Gut 198526(9)914-919
19 Quigley EMM Quera R Small intestinal bacterial overgrowthRoles of antibiotics prebiotics and probiotics Gastroenterology2006130(2 suppl 1)S78-S90
20 Gracey M The contaminated small bowel syndrome Pathogenesisdiagnosis and treatment Am J Clin Nutr 197932(1)234-243
21 Giannella RA Broitman SA Zamcheck N Vitamin B12 uptake byintestinal microorganisms Mechanism and relevance to syn-dromes of intestinal bacterial overgrowth J Clin Invest 197150(5)1100-1107
22 Bala L Ghoshal UC Ghoshal U et al Malabsorption syndrome withand without small intestinal bacterial overgrowth A study on
RESEARCH
1206 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 89
upper-gut aspirates using 1H NMR spectroscopy Magn Reson Med200656(4)738-744
23 Ziegler TR Cole CR Small bowel bacterial overgrowth in adults Apotential contributor to intestinal failure Curr Gastroenterol Rep20079(6)463-467
24 Byrne T Veglia L Camelio M et al Beyond the prescription Opti-mizing the diet of patients with short bowel syndrome Nutr ClinPract 200015(6)306-311
25 Nordgaard I Hansen BS Mortensen PB Colon as a digestive organ inpatientswith short bowel syndromeLancet 1994343(8894)373-376
26 Lykins TC Stockwell J Comprehensive modi1047297ed diet simpli1047297esnutrition management of adults with short bowel syndrome J AmDiet Assoc 199898(3)309-315
27 Matarese LE Steiger E Dietary and medical management of shortbowel syndrome in adult patients J Clin Gastroenterol 200640(suppl2)S85-S93
28 Woolf GM Miller C Kurian R Jeejeebhoy KN Diet for patients with ashort bowel High fat or high carbohydrate Gastroenterology198384(4)823-828
29 Atia A Girard-Pipau F Hebuterne X et al Macronutrient absorptioncharacteristics in human short bowel syndrome and jejunocolonicanastamosis Starch is the most important carbohydrate substratealthough pectin supplementation may modestly enhance short chainfatty acid production and 1047298uid absorption JPEN J Parenter EnteralNutr 201135(2)229-240
30 Tilg H Short bowel syndrome Searching for the proper diet Euro- pean J Gastroenterol Hepatol 200820(11)1061-1063
31 Shatnawei A Parekh NR Rhoda KM et al Intestinal failure man-agement at the Cleveland Clinic Arch Surg 2010145(6)521-527
32 Atia AN Buchman AL Oral rehydration solutions in non-choleradiarrhea A review Am J Gastroenterol 2009104(10)2596-2604
33 Kles KA Chang EB Short-chain fatty acids impact on intestinaladaptation in1047298ammation carcinoma and failure Gastroenterology2006130(suppl 2)S100-S105
34 Banks MR Farthing MJG Fluid and electrolyte transport in the smallintestine Curr Opin Gastroenterol 200218(2)176-181
35 Alam NH Bhatnagar S Chea-Woo E et al Multicenter randomizeddouble-blind clinical trial to evaluate the ef 1047297cacy and safety of areduced osmolarity oral hydration salt solution in children withwatery diarrhea Pediatrics 2001107(4)613-618
36 Rudman D Dedonis JL Fountain MT et al Hypocitraturia in patientswith gastrointestinal malabsorption N Engl J Med 1980303(12)657-661
37 Joly F Dray X Corcos O Barbot L Kapel N Messing B Tube feedingimproves intestinal absorption in short bowel syndrome patientsGastroenterology 2009136(3)824-831
38 Mziray-Andrew CH Sentongo TA Nutritional de1047297ciencies in intes-tinal failure Pediatr Clin North Am 200956(5)1185-1200
39 Okuda K Discovery of vitamin B12 in the liver and its absorptionfactor in the stomach A historical review J Gastroenterol Hepatol199914(4)301-308
40 Green R Indicators for assessing folate and vitamin B12 status and formonitoring the ef 1047297cacy of intervention strategies Food Nutr Bull200829(2 suppl)S52-S63
41 Malone M Longitudinal assessment of outcome health statusand changes in lifestyle associated with long-term home parenteraland enteral nutrition JPEN J Parenter Enteral Nutr 200226164-168
42 Baxter JP Fayers PM McKinlay AW A review of the quality of life of adult patients treated with long-term parenteral nutrition Clin Nutr 200625543-553
43 Huisman-de Waal G Schoonhoven L Jansen J Wanten G vanAchterberg T The impact of home parenteral nutrition on daily lifemdashA review Clin Nutr 200726275-288
44 Dudrick SJ Palesty JA Historical highlights of the development of total parenteral nutrition Surg Clin N Am 201191693-717
45 Shatari T Clark MA Lee JR Keighley MRB Reliability of radiographicmeasurement of small intestine length Colorectal Dis 20036(65)327-329
46 Kovacevich DS Frederick A Kelly D Nishikawa R Young L Standardsfor specialized nutrition support Home care patients Nutr Clin Pract 200520579-590
47 Matarese LE OrsquoKeefe SJ Kandie HM et al Short bowel syndromeClinical guidelines for nutrition management Nutr Clin Pract 200520(5)493-502
48 Kovacevich DS Orr ME Considerations for home nutrition supportIn The ASPEN Nutrition Support Practice Manual 2nd ed SilverSpring MD American Society of Parenteral and Enteral Nutrition2005371-377
49 Kumpf VJ Tillman EM Home parenteral nutrition Safe transitionfrom hospital to home Nutr Clin Pract 201227749-757
50 WinklerM Hagan E Albin J Homenutrition support In ASPEN Adult Nutrition Support Core Curriculum 2nded Silver Spring MD AmericanSociety of Parenteral and Enteral Nutrition 2012639-655
51 Kumpf VJ Parenteral nutrition-associated liver disease in adult andpediatric patients Nutr Clin Pract 200621279-290
52 Kumpf VJ Gervasio J Complications of parenteral nutrition In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver SpringMD American Society of Parenteral and Enteral Nutrition 2012384e297
53 Dreesen M Foulon V Vanhaecht K et al Guidelines recommenda-tions on care of adult patients receiving home parenteral nutritionA systematic review of global practices Clin Nutr 201231602-608
54 Howard L Ashley C Lyon D Shenkin A Autopsy tissue trace ele-ments in 8 long-term parenteral nutrition patients who receive thecurrent US Food and Drug Administration formulation JPEN J Parenter Enteral Nutr 200731(5)388-396
55 Reynolds N Blumsohn A Baxter JP Houston G Pennington CRManganese requirement and toxicity in patients on home parenteralnutrition Clin Nutr 199817(5)227-230
56 Thompson P Dueksen DV Vitamin D de1047297ciency in patients receivinghome parenteral nutrition JPEN J Parenter Enteral Nutr 201135(4)499-504
57 Yusuf SW Rehman Q Casscells W Cardiomyopathy in associationwith selenium de1047297ciency A case report JPEN J Parenter Enteral Nutr 200226(1)63-66
58 Mirtallo JM Holcombe B Kochevar M Guenter P Parenteral nutri-tion product shortages The ASPEN strategy Nutr Clin Pract 201227(3)385-391
59 Gillanders L Angstmann K Ball P et al AuSPEN clinical practiceguidelines for home parenteral nutrition patient in Australia andNew Zealand Nutrition 200824998-1012
60 Tarleton S DiBaise JK Short bowel syndrome In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver Spring MDASPEN 2012511-522
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1207
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
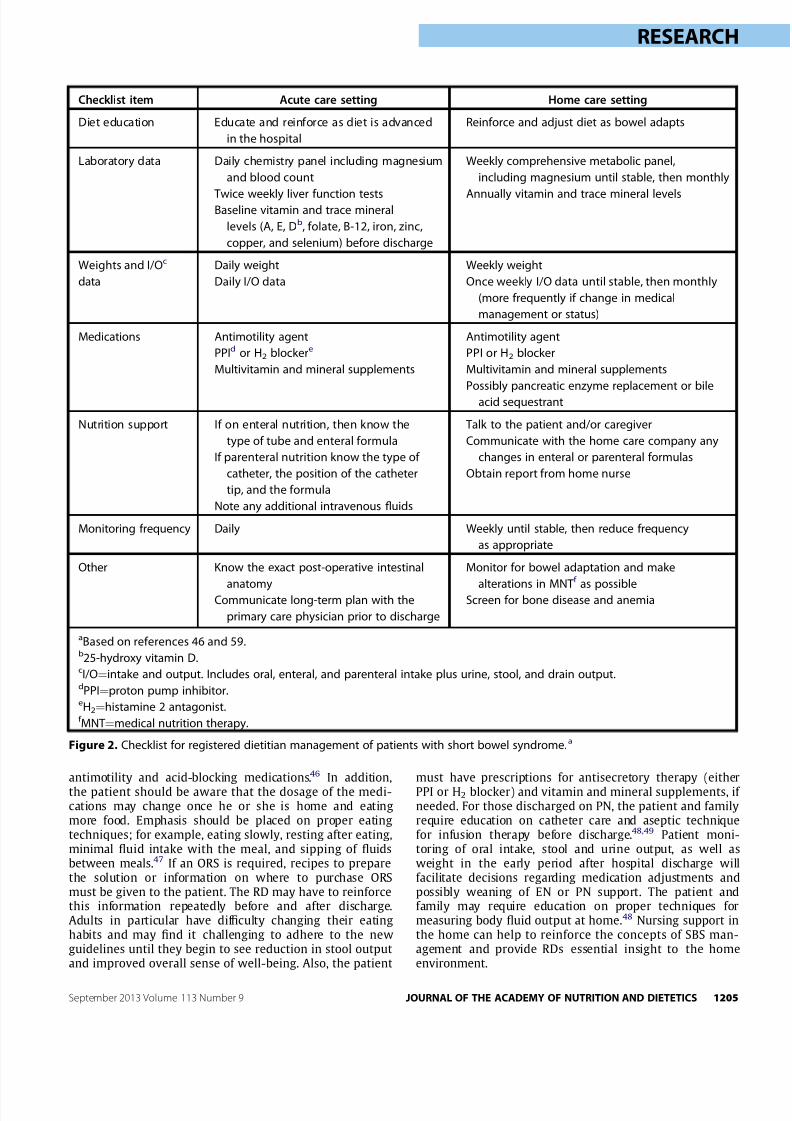
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 69
antimotility and acid-blocking medications46 In additionthe patient should be aware that the dosage of the medi-cations may change once he or she is home and eatingmore food Emphasis should be placed on proper eatingtechniques for example eating slowly resting after eatingminimal 1047298uid intake with the meal and sipping of 1047298uidsbetween meals47 If an ORS is required recipes to preparethe solution or information on where to purchase ORSmust be given to the patient The RD may have to reinforcethis information repeatedly before and after dischargeAdults in particular have dif 1047297culty changing their eatinghabits and may 1047297nd it challenging to adhere to the newguidelines until they begin to see reduction in stool outputand improved overall sense of well-being Also the patient
must have prescriptions for antisecretory therapy (eitherPPI or H2 blocker) and vitamin and mineral supplements if needed For those discharged on PN the patient and familyrequire education on catheter care and aseptic techniquefor infusion therapy before discharge4849 Patient moni-toring of oral intake stool and urine output as well asweight in the early period after hospital discharge willfacilitate decisions regarding medication adjustments andpossibly weaning of EN or PN support The patient andfamily may require education on proper techniques formeasuring body 1047298uid output at home48 Nursing support inthe home can help to reinforce the concepts of SBS man-agement and provide RDs essential insight to the homeenvironment
Checklist item Acute care setting Home care setting
Diet education Educate and reinforce as diet is advanced
in the hospital
Reinforce and adjust diet as bowel adapts
Laboratory data Daily chemistry panel including magnesium
and blood count
Twice weekly liver function testsBaseline vitamin and trace mineral
levels (A E Db folate B-12 iron zinc
copper and selenium) before discharge
Weekly comprehensive metabolic panel
including magnesium until stable then monthly
Annually vitamin and trace mineral levels
Weights and IOc
data
Daily weight
Daily IO data
Weekly weight
Once weekly IO data until stable then monthly
(more frequently if change in medical
management or status)
Medications Antimotility agent
PPId or H2 blockere
Multivitamin and mineral supplements
Antimotility agent
PPI or H2 blocker
Multivitamin and mineral supplements
Possibly pancreatic enzyme replacement or bile
acid sequestrant
Nutrition support If on enteral nutrition then know the
type of tube and enteral formula
If parenteral nutrition know the type of
catheter the position of the catheter
tip and the formula
Note any additional intravenous 1047298uids
Talk to the patient andor caregiver
Communicate with the home care company any
changes in enteral or parenteral formulas
Obtain report from home nurse
Monitoring frequency Daily Weekly until stable then reduce frequency
as appropriate
Other Know the exact post-operative intestinal
anatomyCommunicate long-term plan with the
primary care physician prior to discharge
Monitor for bowel adaptation and make
alterations in MNT
f
as possibleScreen for bone disease and anemia
aBased on references 46 and 59b25-hydroxy vitamin DcIOfrac14intake and output Includes oral enteral and parenteral intake plus urine stool and drain outputdPPIfrac14proton pump inhibitoreH2frac14histamine 2 antagonistf MNT frac14medical nutrition therapy
Figure 2 Checklist for registered dietitian management of patients with short bowel syndromea
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1205
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 79
After hospital discharge patients with SBS are best servedby frequent follow-up appointments with all members of thenutrition support team in particular the managing physicianand RD The primary goals of these appointments are toassess adherence to the prescribed therapies monitor 1047298uidelectrolyte hydration and nutritional status reinforce theprinciples of nutrition therapy and adjust the therapies as
necessary
50
Periodic weights and blood chemistry levels(including liver function tests) will help to determine theextent of bowel adaptation liver-related complications of PNand the possibility of weaning from EN or PN48 If a patientdevelops PN-related liver disease the workup should assessfor small bowel bacterial overgrowth blood infection and re-evaluate IV fat emulsion deliverymdashall of which can alter liverfunction51 Treatment may include a reduction in the amountand frequency of IV fat emulsion infusions (lt1 gkgday asinfrequently as once a week) with periodic monitoring foressential fatty acid de1047297ciency52
Baseline vitamin (eg folate B-12 and vitamins A D E)mineral (eg iron calcium and magnesium) and trace mineral(eg zinc copper and selenium and chromium and manganese
for PN patients) levels and dual-energy x-ray absorptiometryscan are required for comparison purposes in long-term followup53 The standard parenteral multivitamin and trace mineraladditives may not meet a patientrsquos exact requirements and cancause de1047297ciency or toxicity states over time54 For exampledaily trace mineralinfusions of 03 mg manganese over timecanlead to deposits in the brain55 and chronic standard multivi-tamin dosing of 200 IU vitamin D can cause insuf 1047297ciency orde1047297ciency states56 Further complicating the issue of moni-toring micronutrient levels of patients dependent on PN are theongoing product shortages These shortages have led to omis-sion or rationing of certain nutrients that can cause life-threatening de1047297ciency states505758 These levels should becheckedno less than every 6 to 12 months or more frequently if
abnormal levels are identi1047297ed5859 With time as a patient sta-bilizes and thrives at home the length of time between clinicvisits can be extended For patients with stable chronic SBS theminimum follow-up should occur every 6 to 12 months As withthe patientpro1047297le provided bowel adaptation can occur slowlyIt can take more than 2 years before adaptation has fullyoccurred to change the treatment plan and wean arti1047297cialnutrition support11
CONCLUSIONSManagement of SBS is complex and requires a concert of medical nutrition and pharmaceutical therapies to optimize1047298uid and nutrient absorption for survival Each patientrsquos
unique care plan depends on the amount and site of remaining intestine and the patientrsquos ability to adhere to themedical and nutrition therapies Some patients will be able tosurvive with antisecretory and anti-motility agents alongwith strict diet adherence alone whereas other patients willrequire lifelong infusion therapy In either case patients withSBS must have close follow-up with a specialized medicalteam to monitor for nutrient de1047297ciencies and potentialcomplications of SBS The most common long-term compli-cations include metabolic bone disease PN-related liver dis-ease nephrolithiasis anemia central line infection centralaccess problems (thrombosis and superior vena cava syn-drome due to vein stenosis) and vitamin and trace mineral
de1047297ciencies62738 Patients with SBS are medically complexand require long-term monitoring and revisions of the careplan The substantial bene1047297t of medical nutrition therapy iswhat makes these patients both challenging and extremelyrewarding for RDs to manage
References
1 Semrad CE Approach to the patient with diarrhea and malabsorp-tion In Goldmanrsquo s Cecil Medicine 24th ed Philadelphia PA ElsevierSaunders 2012895-913
2 OrsquoKeefe SJD Buchman AL Fishbein TM Jeejeebhoy KN Jeppesen PBShaffer J Short bowel syndrome and intestinal failure Consensus def-initions and overview Clin Gastroenterol Hepatol 20064(1)6-10
3 Nightingale J Woodward JM Guidelines for management of patientswith short bowel Gut 200655(suppl IV)iv1-iv12
4 Nightingale JMD Lennard-Jones JE Gertner DJ Wood SRBartram CI Colonic preservation reduces need for parenteral ther-apy increases incidence of renal stones but does not change highprevalence of gallstones in patients with a short bowel Gut 199233(11)1493-1497
5 Messing B Crenn P Beau P Boutron-Ruault MC Rambaud J-CMatuchansky C Long-term survival and parenteral nutritiondependence in adult patients with the short bowel syndrome
Gastroenterology 1999117(5)1043-10506 Jeejeebhoy KN Short bowel syndrome A nutritional and medical
approach Can Med Assoc J 2002166(10)1297-1302
7 Welch IM Cunningham KM Read NW Regulation of gastric emptyingby ileal nutrients in humans Gastroenterology 19 8894(2)401-404
8 Bines JE Intestinal failure A new era in clinical management J Gastroenterol Hepatol 200924(suppl 3)S86-S92
9 Bines JE Taylor RG Justice F et al Diet following small bowelresection In1047298uence of diet complexity on intestinal adaptationfollowing massive small bowel resection in a preclinical model
J Gastroenterol Hepatol 200217(11)1170-1179
10 Jeppesen PB Mortensen PB Enhancing bowel adaptation in shortbowel syndrome Curr Gastroenterol Rep 20024(4)338-347
11 Gouttebel MC Saint Aubert B ColetteC Astre C Monnier LHJoyeuxHIntestinal adaptation in patients with short bowel syndrome mea-surement by calcium absorption Dig Dis 198934(5)709-715
12 Buchman AL Etiology and initial management of short bowel syn-drome Gastroenterology 2006130(suppl)S5-S15
13 Parekh NR Steiger E Short bowel syndrome Curr Treat OptionsGastroenterol 200710(1)10-23
14 Lacy CF Armstrong LL Goldman MP Lance LL Drug InformationHandbook A Comprehensive Resource for All Clinicians and HealthcareProfessionals 19th ed Hudson OH Lexi-Comp 2010
15 Rubinoff MJ Piccione PR Holt PR Clonidine prolongs human intes-tine transit time Use of the lactulose-breath hydrogen test Am J Gastroenterol 198984(4)372-374
16 Buchman AL Fryer J Wallin A Ahn CW Polensky S Zaremba KClonidine reduces diarrhea and sodium loss in patients with prox-imal jejunostomy A controlled study JPEN J Parenter Enteral Nutr 200630(6)487-491
17 McDoniel K Taylor B Huey W et al Use of clonidine to decreaseintestinal 1047298uid losses in patients with high-output short-bowel
syndrome JPEN J Parenter Enteral Nutr 200428(4)265-268
18 Williams NS Evans P King RFGJ Gastric acid secretion andgastrin production in the short bowel syndrome Gut 198526(9)914-919
19 Quigley EMM Quera R Small intestinal bacterial overgrowthRoles of antibiotics prebiotics and probiotics Gastroenterology2006130(2 suppl 1)S78-S90
20 Gracey M The contaminated small bowel syndrome Pathogenesisdiagnosis and treatment Am J Clin Nutr 197932(1)234-243
21 Giannella RA Broitman SA Zamcheck N Vitamin B12 uptake byintestinal microorganisms Mechanism and relevance to syn-dromes of intestinal bacterial overgrowth J Clin Invest 197150(5)1100-1107
22 Bala L Ghoshal UC Ghoshal U et al Malabsorption syndrome withand without small intestinal bacterial overgrowth A study on
RESEARCH
1206 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 89
upper-gut aspirates using 1H NMR spectroscopy Magn Reson Med200656(4)738-744
23 Ziegler TR Cole CR Small bowel bacterial overgrowth in adults Apotential contributor to intestinal failure Curr Gastroenterol Rep20079(6)463-467
24 Byrne T Veglia L Camelio M et al Beyond the prescription Opti-mizing the diet of patients with short bowel syndrome Nutr ClinPract 200015(6)306-311
25 Nordgaard I Hansen BS Mortensen PB Colon as a digestive organ inpatientswith short bowel syndromeLancet 1994343(8894)373-376
26 Lykins TC Stockwell J Comprehensive modi1047297ed diet simpli1047297esnutrition management of adults with short bowel syndrome J AmDiet Assoc 199898(3)309-315
27 Matarese LE Steiger E Dietary and medical management of shortbowel syndrome in adult patients J Clin Gastroenterol 200640(suppl2)S85-S93
28 Woolf GM Miller C Kurian R Jeejeebhoy KN Diet for patients with ashort bowel High fat or high carbohydrate Gastroenterology198384(4)823-828
29 Atia A Girard-Pipau F Hebuterne X et al Macronutrient absorptioncharacteristics in human short bowel syndrome and jejunocolonicanastamosis Starch is the most important carbohydrate substratealthough pectin supplementation may modestly enhance short chainfatty acid production and 1047298uid absorption JPEN J Parenter EnteralNutr 201135(2)229-240
30 Tilg H Short bowel syndrome Searching for the proper diet Euro- pean J Gastroenterol Hepatol 200820(11)1061-1063
31 Shatnawei A Parekh NR Rhoda KM et al Intestinal failure man-agement at the Cleveland Clinic Arch Surg 2010145(6)521-527
32 Atia AN Buchman AL Oral rehydration solutions in non-choleradiarrhea A review Am J Gastroenterol 2009104(10)2596-2604
33 Kles KA Chang EB Short-chain fatty acids impact on intestinaladaptation in1047298ammation carcinoma and failure Gastroenterology2006130(suppl 2)S100-S105
34 Banks MR Farthing MJG Fluid and electrolyte transport in the smallintestine Curr Opin Gastroenterol 200218(2)176-181
35 Alam NH Bhatnagar S Chea-Woo E et al Multicenter randomizeddouble-blind clinical trial to evaluate the ef 1047297cacy and safety of areduced osmolarity oral hydration salt solution in children withwatery diarrhea Pediatrics 2001107(4)613-618
36 Rudman D Dedonis JL Fountain MT et al Hypocitraturia in patientswith gastrointestinal malabsorption N Engl J Med 1980303(12)657-661
37 Joly F Dray X Corcos O Barbot L Kapel N Messing B Tube feedingimproves intestinal absorption in short bowel syndrome patientsGastroenterology 2009136(3)824-831
38 Mziray-Andrew CH Sentongo TA Nutritional de1047297ciencies in intes-tinal failure Pediatr Clin North Am 200956(5)1185-1200
39 Okuda K Discovery of vitamin B12 in the liver and its absorptionfactor in the stomach A historical review J Gastroenterol Hepatol199914(4)301-308
40 Green R Indicators for assessing folate and vitamin B12 status and formonitoring the ef 1047297cacy of intervention strategies Food Nutr Bull200829(2 suppl)S52-S63
41 Malone M Longitudinal assessment of outcome health statusand changes in lifestyle associated with long-term home parenteraland enteral nutrition JPEN J Parenter Enteral Nutr 200226164-168
42 Baxter JP Fayers PM McKinlay AW A review of the quality of life of adult patients treated with long-term parenteral nutrition Clin Nutr 200625543-553
43 Huisman-de Waal G Schoonhoven L Jansen J Wanten G vanAchterberg T The impact of home parenteral nutrition on daily lifemdashA review Clin Nutr 200726275-288
44 Dudrick SJ Palesty JA Historical highlights of the development of total parenteral nutrition Surg Clin N Am 201191693-717
45 Shatari T Clark MA Lee JR Keighley MRB Reliability of radiographicmeasurement of small intestine length Colorectal Dis 20036(65)327-329
46 Kovacevich DS Frederick A Kelly D Nishikawa R Young L Standardsfor specialized nutrition support Home care patients Nutr Clin Pract 200520579-590
47 Matarese LE OrsquoKeefe SJ Kandie HM et al Short bowel syndromeClinical guidelines for nutrition management Nutr Clin Pract 200520(5)493-502
48 Kovacevich DS Orr ME Considerations for home nutrition supportIn The ASPEN Nutrition Support Practice Manual 2nd ed SilverSpring MD American Society of Parenteral and Enteral Nutrition2005371-377
49 Kumpf VJ Tillman EM Home parenteral nutrition Safe transitionfrom hospital to home Nutr Clin Pract 201227749-757
50 WinklerM Hagan E Albin J Homenutrition support In ASPEN Adult Nutrition Support Core Curriculum 2nded Silver Spring MD AmericanSociety of Parenteral and Enteral Nutrition 2012639-655
51 Kumpf VJ Parenteral nutrition-associated liver disease in adult andpediatric patients Nutr Clin Pract 200621279-290
52 Kumpf VJ Gervasio J Complications of parenteral nutrition In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver SpringMD American Society of Parenteral and Enteral Nutrition 2012384e297
53 Dreesen M Foulon V Vanhaecht K et al Guidelines recommenda-tions on care of adult patients receiving home parenteral nutritionA systematic review of global practices Clin Nutr 201231602-608
54 Howard L Ashley C Lyon D Shenkin A Autopsy tissue trace ele-ments in 8 long-term parenteral nutrition patients who receive thecurrent US Food and Drug Administration formulation JPEN J Parenter Enteral Nutr 200731(5)388-396
55 Reynolds N Blumsohn A Baxter JP Houston G Pennington CRManganese requirement and toxicity in patients on home parenteralnutrition Clin Nutr 199817(5)227-230
56 Thompson P Dueksen DV Vitamin D de1047297ciency in patients receivinghome parenteral nutrition JPEN J Parenter Enteral Nutr 201135(4)499-504
57 Yusuf SW Rehman Q Casscells W Cardiomyopathy in associationwith selenium de1047297ciency A case report JPEN J Parenter Enteral Nutr 200226(1)63-66
58 Mirtallo JM Holcombe B Kochevar M Guenter P Parenteral nutri-tion product shortages The ASPEN strategy Nutr Clin Pract 201227(3)385-391
59 Gillanders L Angstmann K Ball P et al AuSPEN clinical practiceguidelines for home parenteral nutrition patient in Australia andNew Zealand Nutrition 200824998-1012
60 Tarleton S DiBaise JK Short bowel syndrome In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver Spring MDASPEN 2012511-522
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1207
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9

7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 79
After hospital discharge patients with SBS are best servedby frequent follow-up appointments with all members of thenutrition support team in particular the managing physicianand RD The primary goals of these appointments are toassess adherence to the prescribed therapies monitor 1047298uidelectrolyte hydration and nutritional status reinforce theprinciples of nutrition therapy and adjust the therapies as
necessary
50
Periodic weights and blood chemistry levels(including liver function tests) will help to determine theextent of bowel adaptation liver-related complications of PNand the possibility of weaning from EN or PN48 If a patientdevelops PN-related liver disease the workup should assessfor small bowel bacterial overgrowth blood infection and re-evaluate IV fat emulsion deliverymdashall of which can alter liverfunction51 Treatment may include a reduction in the amountand frequency of IV fat emulsion infusions (lt1 gkgday asinfrequently as once a week) with periodic monitoring foressential fatty acid de1047297ciency52
Baseline vitamin (eg folate B-12 and vitamins A D E)mineral (eg iron calcium and magnesium) and trace mineral(eg zinc copper and selenium and chromium and manganese
for PN patients) levels and dual-energy x-ray absorptiometryscan are required for comparison purposes in long-term followup53 The standard parenteral multivitamin and trace mineraladditives may not meet a patientrsquos exact requirements and cancause de1047297ciency or toxicity states over time54 For exampledaily trace mineralinfusions of 03 mg manganese over timecanlead to deposits in the brain55 and chronic standard multivi-tamin dosing of 200 IU vitamin D can cause insuf 1047297ciency orde1047297ciency states56 Further complicating the issue of moni-toring micronutrient levels of patients dependent on PN are theongoing product shortages These shortages have led to omis-sion or rationing of certain nutrients that can cause life-threatening de1047297ciency states505758 These levels should becheckedno less than every 6 to 12 months or more frequently if
abnormal levels are identi1047297ed5859 With time as a patient sta-bilizes and thrives at home the length of time between clinicvisits can be extended For patients with stable chronic SBS theminimum follow-up should occur every 6 to 12 months As withthe patientpro1047297le provided bowel adaptation can occur slowlyIt can take more than 2 years before adaptation has fullyoccurred to change the treatment plan and wean arti1047297cialnutrition support11
CONCLUSIONSManagement of SBS is complex and requires a concert of medical nutrition and pharmaceutical therapies to optimize1047298uid and nutrient absorption for survival Each patientrsquos
unique care plan depends on the amount and site of remaining intestine and the patientrsquos ability to adhere to themedical and nutrition therapies Some patients will be able tosurvive with antisecretory and anti-motility agents alongwith strict diet adherence alone whereas other patients willrequire lifelong infusion therapy In either case patients withSBS must have close follow-up with a specialized medicalteam to monitor for nutrient de1047297ciencies and potentialcomplications of SBS The most common long-term compli-cations include metabolic bone disease PN-related liver dis-ease nephrolithiasis anemia central line infection centralaccess problems (thrombosis and superior vena cava syn-drome due to vein stenosis) and vitamin and trace mineral
de1047297ciencies62738 Patients with SBS are medically complexand require long-term monitoring and revisions of the careplan The substantial bene1047297t of medical nutrition therapy iswhat makes these patients both challenging and extremelyrewarding for RDs to manage
References
1 Semrad CE Approach to the patient with diarrhea and malabsorp-tion In Goldmanrsquo s Cecil Medicine 24th ed Philadelphia PA ElsevierSaunders 2012895-913
2 OrsquoKeefe SJD Buchman AL Fishbein TM Jeejeebhoy KN Jeppesen PBShaffer J Short bowel syndrome and intestinal failure Consensus def-initions and overview Clin Gastroenterol Hepatol 20064(1)6-10
3 Nightingale J Woodward JM Guidelines for management of patientswith short bowel Gut 200655(suppl IV)iv1-iv12
4 Nightingale JMD Lennard-Jones JE Gertner DJ Wood SRBartram CI Colonic preservation reduces need for parenteral ther-apy increases incidence of renal stones but does not change highprevalence of gallstones in patients with a short bowel Gut 199233(11)1493-1497
5 Messing B Crenn P Beau P Boutron-Ruault MC Rambaud J-CMatuchansky C Long-term survival and parenteral nutritiondependence in adult patients with the short bowel syndrome
Gastroenterology 1999117(5)1043-10506 Jeejeebhoy KN Short bowel syndrome A nutritional and medical
approach Can Med Assoc J 2002166(10)1297-1302
7 Welch IM Cunningham KM Read NW Regulation of gastric emptyingby ileal nutrients in humans Gastroenterology 19 8894(2)401-404
8 Bines JE Intestinal failure A new era in clinical management J Gastroenterol Hepatol 200924(suppl 3)S86-S92
9 Bines JE Taylor RG Justice F et al Diet following small bowelresection In1047298uence of diet complexity on intestinal adaptationfollowing massive small bowel resection in a preclinical model
J Gastroenterol Hepatol 200217(11)1170-1179
10 Jeppesen PB Mortensen PB Enhancing bowel adaptation in shortbowel syndrome Curr Gastroenterol Rep 20024(4)338-347
11 Gouttebel MC Saint Aubert B ColetteC Astre C Monnier LHJoyeuxHIntestinal adaptation in patients with short bowel syndrome mea-surement by calcium absorption Dig Dis 198934(5)709-715
12 Buchman AL Etiology and initial management of short bowel syn-drome Gastroenterology 2006130(suppl)S5-S15
13 Parekh NR Steiger E Short bowel syndrome Curr Treat OptionsGastroenterol 200710(1)10-23
14 Lacy CF Armstrong LL Goldman MP Lance LL Drug InformationHandbook A Comprehensive Resource for All Clinicians and HealthcareProfessionals 19th ed Hudson OH Lexi-Comp 2010
15 Rubinoff MJ Piccione PR Holt PR Clonidine prolongs human intes-tine transit time Use of the lactulose-breath hydrogen test Am J Gastroenterol 198984(4)372-374
16 Buchman AL Fryer J Wallin A Ahn CW Polensky S Zaremba KClonidine reduces diarrhea and sodium loss in patients with prox-imal jejunostomy A controlled study JPEN J Parenter Enteral Nutr 200630(6)487-491
17 McDoniel K Taylor B Huey W et al Use of clonidine to decreaseintestinal 1047298uid losses in patients with high-output short-bowel
syndrome JPEN J Parenter Enteral Nutr 200428(4)265-268
18 Williams NS Evans P King RFGJ Gastric acid secretion andgastrin production in the short bowel syndrome Gut 198526(9)914-919
19 Quigley EMM Quera R Small intestinal bacterial overgrowthRoles of antibiotics prebiotics and probiotics Gastroenterology2006130(2 suppl 1)S78-S90
20 Gracey M The contaminated small bowel syndrome Pathogenesisdiagnosis and treatment Am J Clin Nutr 197932(1)234-243
21 Giannella RA Broitman SA Zamcheck N Vitamin B12 uptake byintestinal microorganisms Mechanism and relevance to syn-dromes of intestinal bacterial overgrowth J Clin Invest 197150(5)1100-1107
22 Bala L Ghoshal UC Ghoshal U et al Malabsorption syndrome withand without small intestinal bacterial overgrowth A study on
RESEARCH
1206 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 89
upper-gut aspirates using 1H NMR spectroscopy Magn Reson Med200656(4)738-744
23 Ziegler TR Cole CR Small bowel bacterial overgrowth in adults Apotential contributor to intestinal failure Curr Gastroenterol Rep20079(6)463-467
24 Byrne T Veglia L Camelio M et al Beyond the prescription Opti-mizing the diet of patients with short bowel syndrome Nutr ClinPract 200015(6)306-311
25 Nordgaard I Hansen BS Mortensen PB Colon as a digestive organ inpatientswith short bowel syndromeLancet 1994343(8894)373-376
26 Lykins TC Stockwell J Comprehensive modi1047297ed diet simpli1047297esnutrition management of adults with short bowel syndrome J AmDiet Assoc 199898(3)309-315
27 Matarese LE Steiger E Dietary and medical management of shortbowel syndrome in adult patients J Clin Gastroenterol 200640(suppl2)S85-S93
28 Woolf GM Miller C Kurian R Jeejeebhoy KN Diet for patients with ashort bowel High fat or high carbohydrate Gastroenterology198384(4)823-828
29 Atia A Girard-Pipau F Hebuterne X et al Macronutrient absorptioncharacteristics in human short bowel syndrome and jejunocolonicanastamosis Starch is the most important carbohydrate substratealthough pectin supplementation may modestly enhance short chainfatty acid production and 1047298uid absorption JPEN J Parenter EnteralNutr 201135(2)229-240
30 Tilg H Short bowel syndrome Searching for the proper diet Euro- pean J Gastroenterol Hepatol 200820(11)1061-1063
31 Shatnawei A Parekh NR Rhoda KM et al Intestinal failure man-agement at the Cleveland Clinic Arch Surg 2010145(6)521-527
32 Atia AN Buchman AL Oral rehydration solutions in non-choleradiarrhea A review Am J Gastroenterol 2009104(10)2596-2604
33 Kles KA Chang EB Short-chain fatty acids impact on intestinaladaptation in1047298ammation carcinoma and failure Gastroenterology2006130(suppl 2)S100-S105
34 Banks MR Farthing MJG Fluid and electrolyte transport in the smallintestine Curr Opin Gastroenterol 200218(2)176-181
35 Alam NH Bhatnagar S Chea-Woo E et al Multicenter randomizeddouble-blind clinical trial to evaluate the ef 1047297cacy and safety of areduced osmolarity oral hydration salt solution in children withwatery diarrhea Pediatrics 2001107(4)613-618
36 Rudman D Dedonis JL Fountain MT et al Hypocitraturia in patientswith gastrointestinal malabsorption N Engl J Med 1980303(12)657-661
37 Joly F Dray X Corcos O Barbot L Kapel N Messing B Tube feedingimproves intestinal absorption in short bowel syndrome patientsGastroenterology 2009136(3)824-831
38 Mziray-Andrew CH Sentongo TA Nutritional de1047297ciencies in intes-tinal failure Pediatr Clin North Am 200956(5)1185-1200
39 Okuda K Discovery of vitamin B12 in the liver and its absorptionfactor in the stomach A historical review J Gastroenterol Hepatol199914(4)301-308
40 Green R Indicators for assessing folate and vitamin B12 status and formonitoring the ef 1047297cacy of intervention strategies Food Nutr Bull200829(2 suppl)S52-S63
41 Malone M Longitudinal assessment of outcome health statusand changes in lifestyle associated with long-term home parenteraland enteral nutrition JPEN J Parenter Enteral Nutr 200226164-168
42 Baxter JP Fayers PM McKinlay AW A review of the quality of life of adult patients treated with long-term parenteral nutrition Clin Nutr 200625543-553
43 Huisman-de Waal G Schoonhoven L Jansen J Wanten G vanAchterberg T The impact of home parenteral nutrition on daily lifemdashA review Clin Nutr 200726275-288
44 Dudrick SJ Palesty JA Historical highlights of the development of total parenteral nutrition Surg Clin N Am 201191693-717
45 Shatari T Clark MA Lee JR Keighley MRB Reliability of radiographicmeasurement of small intestine length Colorectal Dis 20036(65)327-329
46 Kovacevich DS Frederick A Kelly D Nishikawa R Young L Standardsfor specialized nutrition support Home care patients Nutr Clin Pract 200520579-590
47 Matarese LE OrsquoKeefe SJ Kandie HM et al Short bowel syndromeClinical guidelines for nutrition management Nutr Clin Pract 200520(5)493-502
48 Kovacevich DS Orr ME Considerations for home nutrition supportIn The ASPEN Nutrition Support Practice Manual 2nd ed SilverSpring MD American Society of Parenteral and Enteral Nutrition2005371-377
49 Kumpf VJ Tillman EM Home parenteral nutrition Safe transitionfrom hospital to home Nutr Clin Pract 201227749-757
50 WinklerM Hagan E Albin J Homenutrition support In ASPEN Adult Nutrition Support Core Curriculum 2nded Silver Spring MD AmericanSociety of Parenteral and Enteral Nutrition 2012639-655
51 Kumpf VJ Parenteral nutrition-associated liver disease in adult andpediatric patients Nutr Clin Pract 200621279-290
52 Kumpf VJ Gervasio J Complications of parenteral nutrition In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver SpringMD American Society of Parenteral and Enteral Nutrition 2012384e297
53 Dreesen M Foulon V Vanhaecht K et al Guidelines recommenda-tions on care of adult patients receiving home parenteral nutritionA systematic review of global practices Clin Nutr 201231602-608
54 Howard L Ashley C Lyon D Shenkin A Autopsy tissue trace ele-ments in 8 long-term parenteral nutrition patients who receive thecurrent US Food and Drug Administration formulation JPEN J Parenter Enteral Nutr 200731(5)388-396
55 Reynolds N Blumsohn A Baxter JP Houston G Pennington CRManganese requirement and toxicity in patients on home parenteralnutrition Clin Nutr 199817(5)227-230
56 Thompson P Dueksen DV Vitamin D de1047297ciency in patients receivinghome parenteral nutrition JPEN J Parenter Enteral Nutr 201135(4)499-504
57 Yusuf SW Rehman Q Casscells W Cardiomyopathy in associationwith selenium de1047297ciency A case report JPEN J Parenter Enteral Nutr 200226(1)63-66
58 Mirtallo JM Holcombe B Kochevar M Guenter P Parenteral nutri-tion product shortages The ASPEN strategy Nutr Clin Pract 201227(3)385-391
59 Gillanders L Angstmann K Ball P et al AuSPEN clinical practiceguidelines for home parenteral nutrition patient in Australia andNew Zealand Nutrition 200824998-1012
60 Tarleton S DiBaise JK Short bowel syndrome In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver Spring MDASPEN 2012511-522
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1207
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 89
upper-gut aspirates using 1H NMR spectroscopy Magn Reson Med200656(4)738-744
23 Ziegler TR Cole CR Small bowel bacterial overgrowth in adults Apotential contributor to intestinal failure Curr Gastroenterol Rep20079(6)463-467
24 Byrne T Veglia L Camelio M et al Beyond the prescription Opti-mizing the diet of patients with short bowel syndrome Nutr ClinPract 200015(6)306-311
25 Nordgaard I Hansen BS Mortensen PB Colon as a digestive organ inpatientswith short bowel syndromeLancet 1994343(8894)373-376
26 Lykins TC Stockwell J Comprehensive modi1047297ed diet simpli1047297esnutrition management of adults with short bowel syndrome J AmDiet Assoc 199898(3)309-315
27 Matarese LE Steiger E Dietary and medical management of shortbowel syndrome in adult patients J Clin Gastroenterol 200640(suppl2)S85-S93
28 Woolf GM Miller C Kurian R Jeejeebhoy KN Diet for patients with ashort bowel High fat or high carbohydrate Gastroenterology198384(4)823-828
29 Atia A Girard-Pipau F Hebuterne X et al Macronutrient absorptioncharacteristics in human short bowel syndrome and jejunocolonicanastamosis Starch is the most important carbohydrate substratealthough pectin supplementation may modestly enhance short chainfatty acid production and 1047298uid absorption JPEN J Parenter EnteralNutr 201135(2)229-240
30 Tilg H Short bowel syndrome Searching for the proper diet Euro- pean J Gastroenterol Hepatol 200820(11)1061-1063
31 Shatnawei A Parekh NR Rhoda KM et al Intestinal failure man-agement at the Cleveland Clinic Arch Surg 2010145(6)521-527
32 Atia AN Buchman AL Oral rehydration solutions in non-choleradiarrhea A review Am J Gastroenterol 2009104(10)2596-2604
33 Kles KA Chang EB Short-chain fatty acids impact on intestinaladaptation in1047298ammation carcinoma and failure Gastroenterology2006130(suppl 2)S100-S105
34 Banks MR Farthing MJG Fluid and electrolyte transport in the smallintestine Curr Opin Gastroenterol 200218(2)176-181
35 Alam NH Bhatnagar S Chea-Woo E et al Multicenter randomizeddouble-blind clinical trial to evaluate the ef 1047297cacy and safety of areduced osmolarity oral hydration salt solution in children withwatery diarrhea Pediatrics 2001107(4)613-618
36 Rudman D Dedonis JL Fountain MT et al Hypocitraturia in patientswith gastrointestinal malabsorption N Engl J Med 1980303(12)657-661
37 Joly F Dray X Corcos O Barbot L Kapel N Messing B Tube feedingimproves intestinal absorption in short bowel syndrome patientsGastroenterology 2009136(3)824-831
38 Mziray-Andrew CH Sentongo TA Nutritional de1047297ciencies in intes-tinal failure Pediatr Clin North Am 200956(5)1185-1200
39 Okuda K Discovery of vitamin B12 in the liver and its absorptionfactor in the stomach A historical review J Gastroenterol Hepatol199914(4)301-308
40 Green R Indicators for assessing folate and vitamin B12 status and formonitoring the ef 1047297cacy of intervention strategies Food Nutr Bull200829(2 suppl)S52-S63
41 Malone M Longitudinal assessment of outcome health statusand changes in lifestyle associated with long-term home parenteraland enteral nutrition JPEN J Parenter Enteral Nutr 200226164-168
42 Baxter JP Fayers PM McKinlay AW A review of the quality of life of adult patients treated with long-term parenteral nutrition Clin Nutr 200625543-553
43 Huisman-de Waal G Schoonhoven L Jansen J Wanten G vanAchterberg T The impact of home parenteral nutrition on daily lifemdashA review Clin Nutr 200726275-288
44 Dudrick SJ Palesty JA Historical highlights of the development of total parenteral nutrition Surg Clin N Am 201191693-717
45 Shatari T Clark MA Lee JR Keighley MRB Reliability of radiographicmeasurement of small intestine length Colorectal Dis 20036(65)327-329
46 Kovacevich DS Frederick A Kelly D Nishikawa R Young L Standardsfor specialized nutrition support Home care patients Nutr Clin Pract 200520579-590
47 Matarese LE OrsquoKeefe SJ Kandie HM et al Short bowel syndromeClinical guidelines for nutrition management Nutr Clin Pract 200520(5)493-502
48 Kovacevich DS Orr ME Considerations for home nutrition supportIn The ASPEN Nutrition Support Practice Manual 2nd ed SilverSpring MD American Society of Parenteral and Enteral Nutrition2005371-377
49 Kumpf VJ Tillman EM Home parenteral nutrition Safe transitionfrom hospital to home Nutr Clin Pract 201227749-757
50 WinklerM Hagan E Albin J Homenutrition support In ASPEN Adult Nutrition Support Core Curriculum 2nded Silver Spring MD AmericanSociety of Parenteral and Enteral Nutrition 2012639-655
51 Kumpf VJ Parenteral nutrition-associated liver disease in adult andpediatric patients Nutr Clin Pract 200621279-290
52 Kumpf VJ Gervasio J Complications of parenteral nutrition In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver SpringMD American Society of Parenteral and Enteral Nutrition 2012384e297
53 Dreesen M Foulon V Vanhaecht K et al Guidelines recommenda-tions on care of adult patients receiving home parenteral nutritionA systematic review of global practices Clin Nutr 201231602-608
54 Howard L Ashley C Lyon D Shenkin A Autopsy tissue trace ele-ments in 8 long-term parenteral nutrition patients who receive thecurrent US Food and Drug Administration formulation JPEN J Parenter Enteral Nutr 200731(5)388-396
55 Reynolds N Blumsohn A Baxter JP Houston G Pennington CRManganese requirement and toxicity in patients on home parenteralnutrition Clin Nutr 199817(5)227-230
56 Thompson P Dueksen DV Vitamin D de1047297ciency in patients receivinghome parenteral nutrition JPEN J Parenter Enteral Nutr 201135(4)499-504
57 Yusuf SW Rehman Q Casscells W Cardiomyopathy in associationwith selenium de1047297ciency A case report JPEN J Parenter Enteral Nutr 200226(1)63-66
58 Mirtallo JM Holcombe B Kochevar M Guenter P Parenteral nutri-tion product shortages The ASPEN strategy Nutr Clin Pract 201227(3)385-391
59 Gillanders L Angstmann K Ball P et al AuSPEN clinical practiceguidelines for home parenteral nutrition patient in Australia andNew Zealand Nutrition 200824998-1012
60 Tarleton S DiBaise JK Short bowel syndrome In ASPEN Adult Nutrition Support Core Curriculum 2nd ed Silver Spring MDASPEN 2012511-522
RESEARCH
September 2013 Volume 113 Number 9 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1207
7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9

7172019 1-s20-S2212267213005182-main
httpslidepdfcomreaderfull1-s20-s2212267213005182-main 99
AUTHOR INFORMATIONE A Wall is a nutrition support dietitian The University of Chicago Medicine Chicago IL
Address correspondence to Elizabeth A Wall MS RD LDN The University of Chicago Medicine 5841 S Maryland Ave MC 4080 ChicagoIL 60637 E-mail elizabethwalluchospitalsedu
STATEMENT OF POTENTIAL CONFLICT OF INTEREST
No potential con1047298ict of interest was reported by the author
ACKNOWLEDGEMENTS
The author thanks Patricia Sheean PhD RD for the invitation to write this article and for her guidance with respect to the content The authoralso thanks Carol E Semrad MD for her expert review of this articlersquos content as well as Linda Trumbore MS RD and Scott Lozano PharmD forproviding editorial assistance
RESEARCH
1208 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS September 2013 Volume 113 Number 9