1-s2.0-s0026049514003126-main
DESCRIPTION
ckdTRANSCRIPT
M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Metabolismwww.metabo l i sm jou rna l . com
Effect of lifestyle intervention in patients with type 2
diabetes: A meta-analysisLiang Chen⁎, Jian-Hao Pei, Jian Kuang, Hong-Mei Chen, Zhong Chen,Zhong-Wen Li, Hua-Zhang YangThe First Division in Department of Endocrinology, Guangdong General Hospital, Guangdong Academy of Medical Sciences,106th of Zhongshan Er Road, Guangzhou 510080, China
A R T I C L E I N F O
Abbreviations: BMI, body mass index; HbAhigh-density lipoprotein cholesterol; LDL-c, l⁎ Corresponding author. Tel.: +86 1353878549
E-mail address: [email protected] (
http://dx.doi.org/10.1016/j.metabol.2014.10.010026-0495/© 2015 The Authors. PublishedbyEorg/licenses/by-nc-nd/3.0/).
A B S T R A C T
Article history:Received 16 June 2014Accepted 19 October 2014
Objective. The effect of lifestyle intervention on clinical risk factors in patients with type2 diabetes is unclear. The aim of this meta-analysis was to evaluate the effects ofcomprehensive lifestyle change, such as diet, exercise, and education, on clinical markersthat are risk-factors for cardiovascular disease in patients with type 2 diabetes.
Methods. We searched Medline, Cochrane, EMBASE, and Google Scholar (up to August 31,2013) for randomized controlled trials that compared standard of care (control group) withtreatment regimens that included changes in lifestyle (intervention group). The primaryoutcome was reduction in risk factors of cardiovascular disease including body mass index(BMI), glycatedhemoglobin (HbA1c), systolic bloodpressure (SBP), diastolic bloodpressure (DBP),high-density lipoprotein cholesterol (HDL-c), and low-density lipoprotein cholesterol (LDL-c).
Results. A total of 16 studieswere included in themeta-analysis. The standardizeddifferencein means of change from baseline significantly favored the intervention compared with thecontrol group inBMI (−0.29; 95%CI,−0.52 to−0.06,P = 0.014),HbA1c (−0.37; 95%CI,−0.59 to−0.14,P = 0.001), SBP (−0.16: 95% CI, −0.29 to −0.03, P = 0.016), DBP (−0.27, 95% CI = −0.41 to −0.12,P < 0.001). There was no difference between the intervention and control groups in HDL-c (0.05;95% CI, −0.10 to 0.21; P = 0.503) and LDL-c (−0.14; 95% CI, −0.29 to 0.02; P = 0.092).
Conclusions. The meta-analysis found that lifestyle intervention showed significantbenefit in risk factors that are known to be associated with development of cardiovasculardisease in patients with type 2 diabetes.© 2015 The Authors. PublishedbyElsevier Inc.This isanopenaccessarticleunder theCCBY-NC-
ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/).
Keywords:LifestyleInterventionType 2 diabetesMeta-analysis
1. Introduction
The proportion of people with type 2 diabetes is on the riseand is a major cause of death world-wide. Type 2 diabetes is amajor risk factor for vascular disease with 65% of all diabeticdeaths being due to cardiovascular disease [1].
Lifestyle characteristics, such as physical activity, diet, andstress are important factors that influence development and
1c, glycated hemoglobin;ow-density lipoprotein ch1.L. Chen).
8lsevier Inc. This is anopen
prognosis of type 2 diabetes [2]. Changes in diet and increasein physical activity (walking, etc.) and exercise (running,cycling, etc.) are key components of the management of type2 diabetes [3], and guidelines recommend changes in theselifestyle characteristics for both prevention and managementof the disease [4].
Several systematic reviews and meta-analyses have report-ed the benefit of interventions aimed at improving lifestyle
SBP, systolic blood pressure; DBP, diastolic blood pressure; HDL-c,olesterol.
accessarticleunder theCCBY-NC-ND license (http://creativecommons.

339M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
behaviors on disease progression and development of co-morbidities (eg, vascular disease) in patients with type 2diabetes [5–13]. However, the benefit of lifestyle changes inreducing all-cause mortality or cardiovascular disease is lessclear as the findings from these analyses are inconsistent or thedata are inconclusive [5–13]. To our knowledge, there have beennometa-analyses that evaluated the effect of interventions thatresult in multiple lifestyle changes on risk factors for cardio-vascular disease inpatientswith type2diabetes. The aimof thismeta-analysis was to evaluate the effects of changes in lifestylethat includeddietarybehavior, exercise, orphysical activities onclinical markers of cardiovascular disease in patients with type2 diabetes.
2. Materials and methods
2.1. Search strategy
We searched Medline, Cochrane, EMBASE, and Google Scholarfor randomized controlled trials that compared standard carewith interventions that involved changes in lifestyle. Thefollowing terms were used in the search: diabetes, cardiovas-cular risk, lifestyle, health education, dietary, exercise/physicalactivities, and behavioral intervention. Articles up to August 31,2013 were included. Studies were excluded if they were notpublished in English, were not prospective randomized trials,did not enroll patients with type 2 diabetes, or did notinvestigate lifestyle or education programs relating to dietarybehavior, exercise, or physical activities. All possibly relevantstudies were also hand-searched by 2 independent reviewersand both reviewers had to agree for the study to be included. Ifthere was disagreement, it was resolved by a third reviewer.
2.2. Data extraction
The following information or data were extracted from theincluded studies: the name of the first author, year of publica-tion, study design, number of participants in each treatmentgroup, participants' age and gender, diagnostic criteria, inter-vention regiment for study/control group, and results.
2.3. Quality assessment
The included studies were assessed for risk bias using the ‘Riskof Bias’ assessment tool, Review Manager 5.1, and recommen-dations for judging risk of bias provided in Chapter 8 of theCochrane Handbook for Systematic Reviews Interventions [14].
2.4. Statistical analysis
The primary outcome was reduction in any risk factor ofcardiovascular disease including body mass index (BMI),HbA1c, systolic blood pressure (SBP), diastolic blood pressure(DBP), high-density lipoprotein-c (HDL-c), and low-densitylipoprotein-c (LDL-c). BMI, HbA1c, SBP, DBP, HDL-c, and LDL-cwere compared between participants having intensive life-style intervention (intervention group) and conventionalintervention (control group). A χ2 based test of homogeneitywas performed using Cochran's Q statistic and I2. I2 illustrates
the percentage of the total variability in effect estimatesamong trials resulting from heterogeneity rather than chance.Random-effects models of analysis were used if heterogeneitywas detected (I2 > 50%). Otherwise, fixed-effects models wereused. For each risk factor measure, standardized difference inmeans with corresponding 95% confidence intervals (CIs) wascalculated for between groups and among studies. A two-sided P value <0.05 indicated statistical significance for onecomparison group over the other. Sensitivity analysis wascarried out for the risk factors BMI and HbA1c using the leaveone-out approach. A funnel plot, the fail-safe N (whichindicates whether the observed significance is spurious ornot), and Egger's test (which detects whether the observedstudies is asymmetric or not) were used to assess possiblepublication bias. All analyses were performed using Compre-hensive Meta-Analysis statistical software, version 2.0 (Biostat,Englewood, NJ).
3. Results
3.1. Characteristics of included studies
Eighty-fivepossible studieswere identifiedand18wereexcludedowing to not being relevant to this analysis (Fig. 1). Of the 67remaining studies, 51 were excluded due to being redundantwith an included study, not presenting outcomes of interest,having an intervention period of <6 months, not using behavioror exercise programs, only having one gender in the study, orhaving >2 treatment arms. One study [15] met the inclusioncriteria but was excluded because its findings, in regard to BMI,LDL-c and HDL-c changes, were not in concordance with theincluded studies. The inclusion of this studywould have skewedthe meta-analysis by increasing the discrepancy in bothsensitivity and publication bias analyses (Fig. 1). A total of 16studies were included in the meta-analysis [16–31].
The number of patients per study ranged from 23 to 2575(Table 1). The mean (SD) age was similar across studies(range, 51.3 [1.8] to 67.3 [19]) and between the interventional andcontrol groups (Table 1). The proportion of patients that weremale ranged from 34.8% to 98%, and the lengths of the studyranged from 6 months to 8 years (Table 1). SupplementaryTable S1 summarizes the change from baseline of key riskfactors for all included studies.
Quality assessment indicated that all 16 studies had a highrisk of performance bias due to the studies not havingadequate blinding of the participants and personnel (Fig. 2Aand B). Six studies had high risk of bias due to risk factorassessments not being blinded (Fig. 2B) [16,22–24,30,31].
3.2. Body mass index
Eleven of the included studies reported change from baselinein BMI [18–20,22–25,27,28,30,31]. There was heterogeneityfor BMI across studies (Q statistic = 71.93, I2 = 86.10%,P < 0.001); hence, a random effects analysis was applied. Thestandardized difference in means of change from baselinein BMI significantly favored the intervention group over thecontrol group (standardized difference in means, −0.29; 95%CI, −0.52 to −0.06, P = 0.014) (Fig. 3).
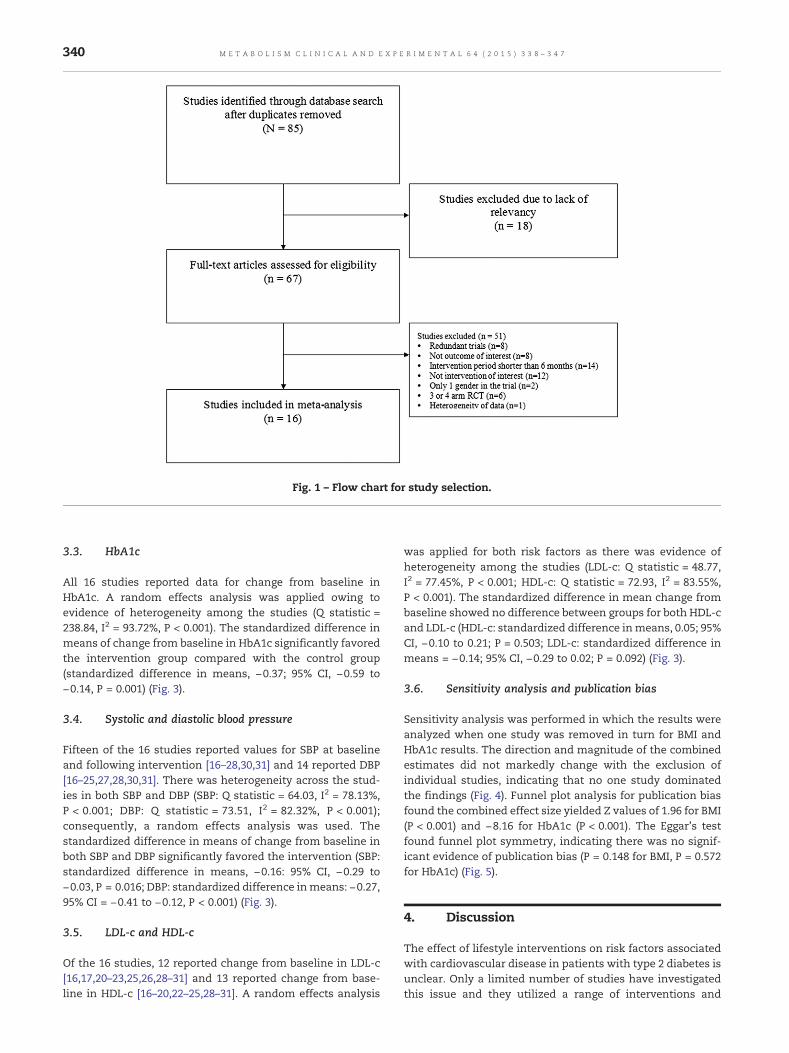
Fig. 1 – Flow chart for study selection.
340 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
3.3. HbA1c
All 16 studies reported data for change from baseline inHbA1c. A random effects analysis was applied owing toevidence of heterogeneity among the studies (Q statistic =238.84, I2 = 93.72%, P < 0.001). The standardized difference inmeans of change from baseline in HbA1c significantly favoredthe intervention group compared with the control group(standardized difference in means, −0.37; 95% CI, −0.59 to−0.14, P = 0.001) (Fig. 3).
3.4. Systolic and diastolic blood pressure
Fifteen of the 16 studies reported values for SBP at baselineand following intervention [16–28,30,31] and 14 reported DBP[16–25,27,28,30,31]. There was heterogeneity across the stud-ies in both SBP and DBP (SBP: Q statistic = 64.03, I2 = 78.13%,P < 0.001; DBP: Q statistic = 73.51, I2 = 82.32%, P < 0.001);consequently, a random effects analysis was used. Thestandardized difference in means of change from baseline inboth SBP and DBP significantly favored the intervention (SBP:standardized difference in means, −0.16: 95% CI, −0.29 to−0.03, P = 0.016; DBP: standardized difference inmeans: −0.27,95% CI = −0.41 to −0.12, P < 0.001) (Fig. 3).
3.5. LDL-c and HDL-c
Of the 16 studies, 12 reported change from baseline in LDL-c[16,17,20–23,25,26,28–31] and 13 reported change from base-line in HDL-c [16–20,22–25,28–31]. A random effects analysis
was applied for both risk factors as there was evidence ofheterogeneity among the studies (LDL-c: Q statistic = 48.77,I2 = 77.45%, P < 0.001; HDL-c: Q statistic = 72.93, I2 = 83.55%,P < 0.001). The standardized difference in mean change frombaseline showed no difference between groups for both HDL-cand LDL-c (HDL-c: standardized difference inmeans, 0.05; 95%CI, −0.10 to 0.21; P = 0.503; LDL-c: standardized difference inmeans = −0.14; 95% CI, −0.29 to 0.02; P = 0.092) (Fig. 3).
3.6. Sensitivity analysis and publication bias
Sensitivity analysis was performed in which the results wereanalyzed when one study was removed in turn for BMI andHbA1c results. The direction and magnitude of the combinedestimates did not markedly change with the exclusion ofindividual studies, indicating that no one study dominatedthe findings (Fig. 4). Funnel plot analysis for publication biasfound the combined effect size yielded Z values of 1.96 for BMI(P < 0.001) and −8.16 for HbA1c (P < 0.001). The Eggar's testfound funnel plot symmetry, indicating there was no signif-icant evidence of publication bias (P = 0.148 for BMI, P = 0.572for HbA1c) (Fig. 5).
4. Discussion
The effect of lifestyle interventions on risk factors associatedwith cardiovascular disease in patients with type 2 diabetes isunclear. Only a limited number of studies have investigatedthis issue and they utilized a range of interventions and
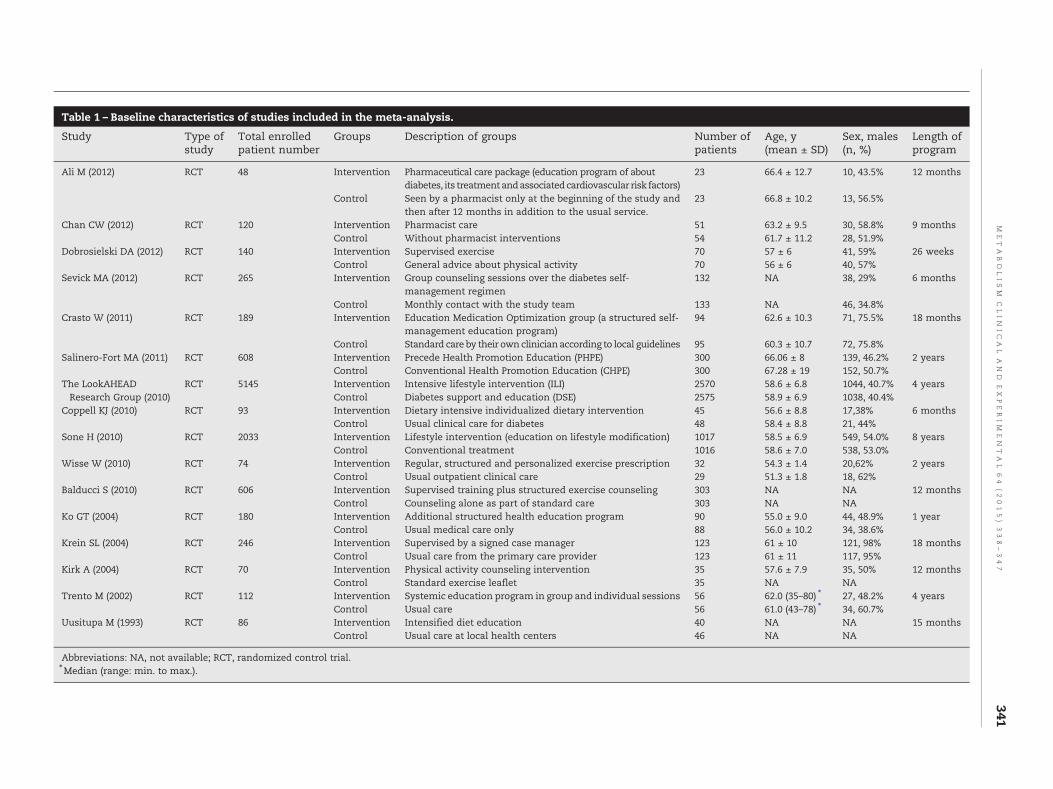
T le 1 – Baseline characteristics of studies included in the meta-analysis.
S dy Type ofstudy
Total enrolledpatient number
Groups Description of groups Num r ofpat s
Age, y(mean ± SD)
Sex, males(n, %)
Length ofprogram
A (2012) RCT 48 Intervention Pharmaceutical care package (education program of aboutdiabetes, its treatmentandassociatedcardiovascular risk factors)
23 66.4 ± 12.7 10, 43.5% 12 months
Control Seen by a pharmacist only at the beginning of the study andthen after 12 months in addition to the usual service.
23 66.8 ± 10.2 13, 56.5%
C n CW (2012) RCT 120 Intervention Pharmacist care 51 63.2 ± 9.5 30, 58.8% 9 monthsControl Without pharmacist interventions 54 61.7 ± 11.2 28, 51.9%
D rosielski DA (2012) RCT 140 Intervention Supervised exercise 70 57 ± 6 41, 59% 26 weeksControl General advice about physical activity 70 56 ± 6 40, 57%
S ick MA (2012) RCT 265 Intervention Group counseling sessions over the diabetes self-management regimen
132 NA 38, 29% 6 months
Control Monthly contact with the study team 133 NA 46, 34.8%C to W (2011) RCT 189 Intervention Education Medication Optimization group (a structured self-
management education program)94 62.6 ± 10.3 71, 75.5% 18 months
Control Standard care by their own clinician according to local guidelines 95 60.3 ± 10.7 72, 75.8%S nero-Fort MA (2011) RCT 608 Intervention Precede Health Promotion Education (PHPE) 300 66.06 ± 8 139, 46.2% 2 years
Control Conventional Health Promotion Education (CHPE) 300 67.28 ± 19 152, 50.7%T LookAHEAD
search Group (2010)RCT 5145 Intervention Intensive lifestyle intervention (ILI) 2570 58.6 ± 6.8 1044, 40.7% 4 years
Control Diabetes support and education (DSE) 2575 58.9 ± 6.9 1038, 40.4%C pell KJ (2010) RCT 93 Intervention Dietary intensive individualized dietary intervention 45 56.6 ± 8.8 17,38% 6 months
Control Usual clinical care for diabetes 48 58.4 ± 8.8 21, 44%S e H (2010) RCT 2033 Intervention Lifestyle intervention (education on lifestyle modification) 1017 58.5 ± 6.9 549, 54.0% 8 years
Control Conventional treatment 1016 58.6 ± 7.0 538, 53.0%W se W (2010) RCT 74 Intervention Regular, structured and personalized exercise prescription 32 54.3 ± 1.4 20,62% 2 years
Control Usual outpatient clinical care 29 51.3 ± 1.8 18, 62%B ucci S (2010) RCT 606 Intervention Supervised training plus structured exercise counseling 303 NA NA 12 months
Control Counseling alone as part of standard care 303 NA NAK T (2004) RCT 180 Intervention Additional structured health education program 90 55.0 ± 9.0 44, 48.9% 1 year
Control Usual medical care only 88 56.0 ± 10.2 34, 38.6%K n SL (2004) RCT 246 Intervention Supervised by a signed case manager 123 61 ± 10 121, 98% 18 months
Control Usual care from the primary care provider 123 61 ± 11 117, 95%K A (2004) RCT 70 Intervention Physical activity counseling intervention 35 57.6 ± 7.9 35, 50% 12 months
Control Standard exercise leaflet 35 NA NAT to M (2002) RCT 112 Intervention Systemic education program in group and individual sessions 56 62.0 (35–80) ⁎ 27, 48.2% 4 years
Control Usual care 56 61.0 (43–78) ⁎ 34, 60.7%U itupa M (1993) RCT 86 Intervention Intensified diet education 40 NA NA 15 months
Control Usual care at local health centers 46 NA NA
A reviations: NA, not available; RCT, randomized control trial.⁎M dian (range: min. to max.).
341M
ET
ABO
LISM
CLIN
IC
AL
AN
DEX
PER
IM
EN
TA
L64
(2015)
338–347
ab
tu
li M
ha
ob
ev
ras
ali
heReop
on
is
ald
o G
rei
irk
ren
us
bbe
beient
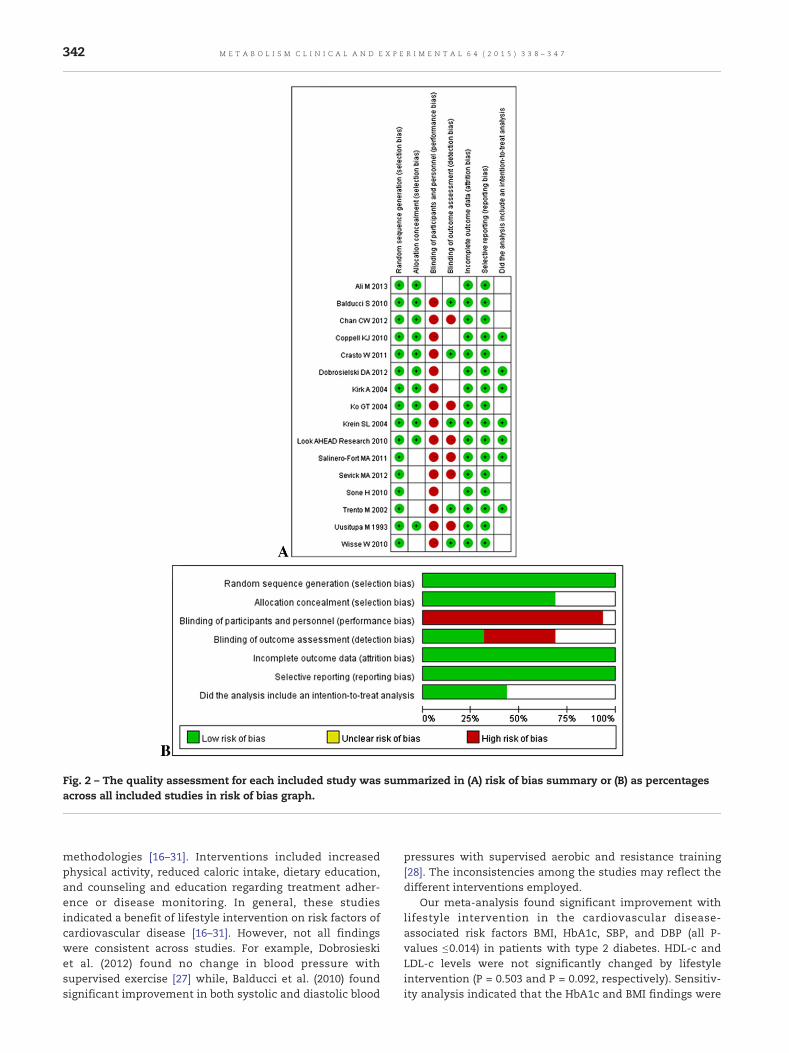
Fig. 2 – The quality assessment for each included study was summarized in (A) risk of bias summary or (B) as percentagesacross all included studies in risk of bias graph.
342 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
methodologies [16–31]. Interventions included increasedphysical activity, reduced caloric intake, dietary education,and counseling and education regarding treatment adher-ence or disease monitoring. In general, these studiesindicated a benefit of lifestyle intervention on risk factors ofcardiovascular disease [16–31]. However, not all findingswere consistent across studies. For example, Dobrosieskiet al. (2012) found no change in blood pressure withsupervised exercise [27] while, Balducci et al. (2010) foundsignificant improvement in both systolic and diastolic blood
pressures with supervised aerobic and resistance training[28]. The inconsistencies among the studies may reflect thedifferent interventions employed.
Our meta-analysis found significant improvement withlifestyle intervention in the cardiovascular disease-associated risk factors BMI, HbA1c, SBP, and DBP (all P-values ≤0.014) in patients with type 2 diabetes. HDL-c andLDL-c levels were not significantly changed by lifestyleintervention (P = 0.503 and P = 0.092, respectively). Sensitiv-ity analysis indicated that the HbA1c and BMI findings were
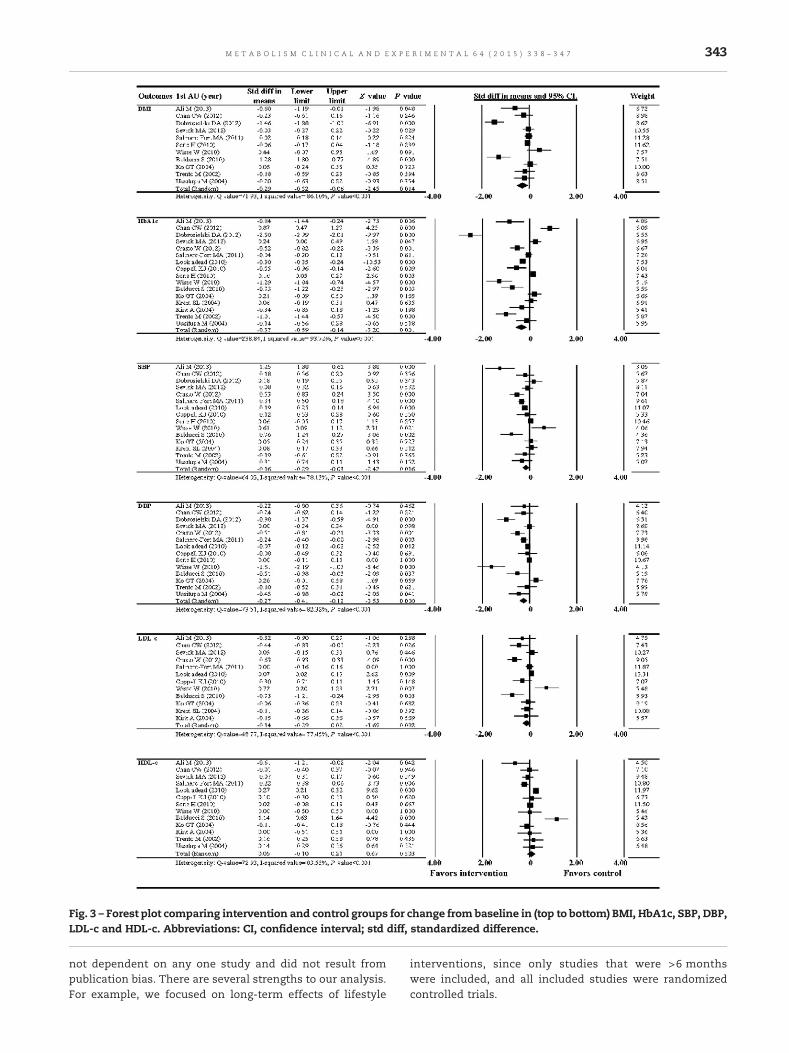
Fig. 3 – Forest plot comparing intervention and control groups for change from baseline in (top to bottom) BMI, HbA1c, SBP, DBP,LDL-c and HDL-c. Abbreviations: CI, confidence interval; std diff, standardized difference.
343M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
not dependent on any one study and did not result frompublication bias. There are several strengths to our analysis.For example, we focused on long-term effects of lifestyle
interventions, since only studies that were >6 monthswere included, and all included studies were randomizedcontrolled trials.
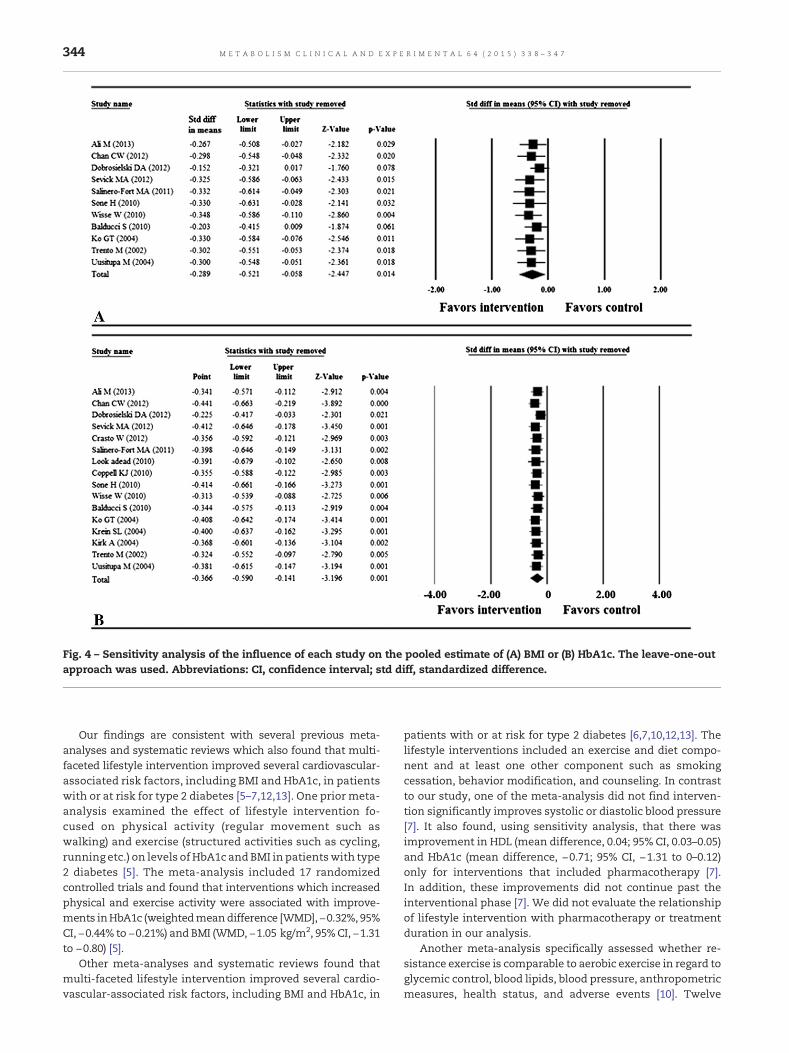
Fig. 4 – Sensitivity analysis of the influence of each study on the pooled estimate of (A) BMI or (B) HbA1c. The leave-one-outapproach was used. Abbreviations: CI, confidence interval; std diff, standardized difference.
344 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
Our findings are consistent with several previous meta-analyses and systematic reviews which also found that multi-faceted lifestyle intervention improved several cardiovascular-associated risk factors, including BMI and HbA1c, in patientswith or at risk for type 2 diabetes [5–7,12,13]. One prior meta-analysis examined the effect of lifestyle intervention fo-cused on physical activity (regular movement such aswalking) and exercise (structured activities such as cycling,running etc.) on levels of HbA1c andBMI in patientswith type2 diabetes [5]. The meta-analysis included 17 randomizedcontrolled trials and found that interventions which increasedphysical and exercise activity were associated with improve-ments inHbA1c (weightedmeandifference [WMD],−0.32%, 95%CI, −0.44% to −0.21%) and BMI (WMD, −1.05 kg/m2, 95%CI, −1.31to −0.80) [5].
Other meta-analyses and systematic reviews found thatmulti-faceted lifestyle intervention improved several cardio-vascular-associated risk factors, including BMI and HbA1c, in
patients with or at risk for type 2 diabetes [6,7,10,12,13]. Thelifestyle interventions included an exercise and diet compo-nent and at least one other component such as smokingcessation, behavior modification, and counseling. In contrastto our study, one of the meta-analysis did not find interven-tion significantly improves systolic or diastolic blood pressure[7]. It also found, using sensitivity analysis, that there wasimprovement in HDL (mean difference, 0.04; 95% CI, 0.03–0.05)and HbA1c (mean difference, −0.71; 95% CI, −1.31 to 0–0.12)only for interventions that included pharmacotherapy [7].In addition, these improvements did not continue past theinterventional phase [7]. We did not evaluate the relationshipof lifestyle intervention with pharmacotherapy or treatmentduration in our analysis.
Another meta-analysis specifically assessed whether re-sistance exercise is comparable to aerobic exercise in regard toglycemic control, blood lipids, blood pressure, anthropometricmeasures, health status, and adverse events [10]. Twelve
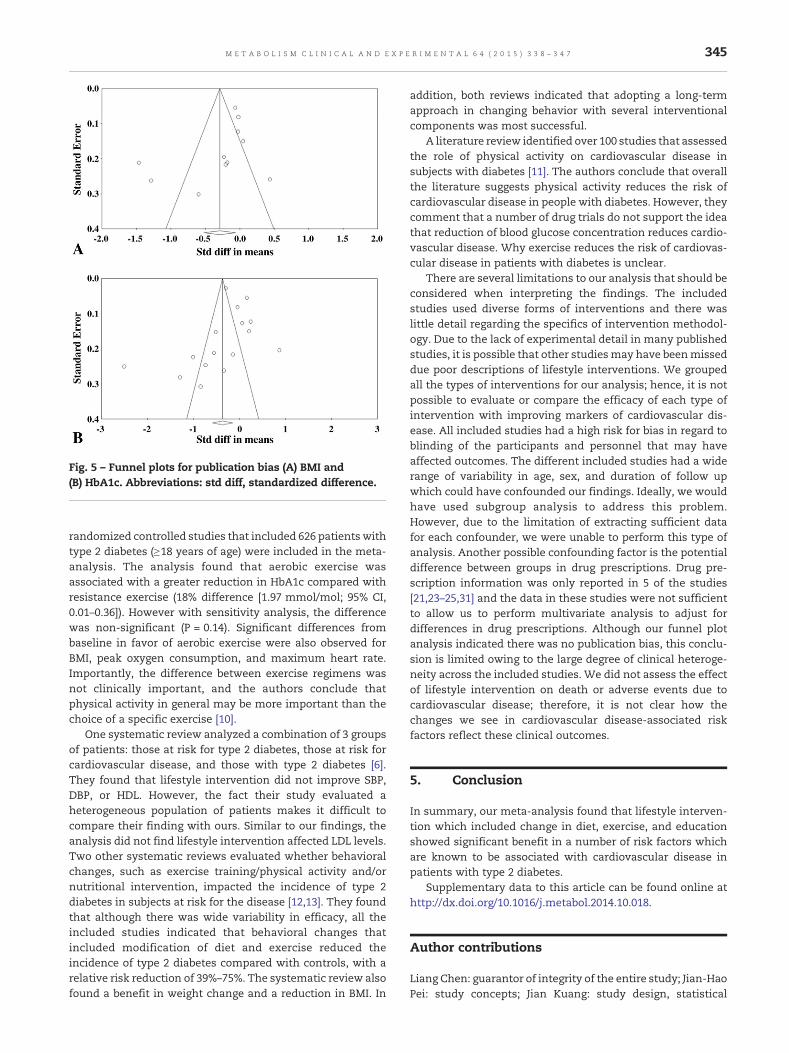
Fig. 5 – Funnel plots for publication bias (A) BMI and(B) HbA1c. Abbreviations: std diff, standardized difference.
345M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
randomized controlled studies that included 626 patients withtype 2 diabetes (≥18 years of age) were included in the meta-analysis. The analysis found that aerobic exercise wasassociated with a greater reduction in HbA1c compared withresistance exercise (18% difference [1.97 mmol/mol; 95% CI,0.01–0.36]). However with sensitivity analysis, the differencewas non-significant (P = 0.14). Significant differences frombaseline in favor of aerobic exercise were also observed forBMI, peak oxygen consumption, and maximum heart rate.Importantly, the difference between exercise regimens wasnot clinically important, and the authors conclude thatphysical activity in general may be more important than thechoice of a specific exercise [10].
One systematic review analyzed a combination of 3 groupsof patients: those at risk for type 2 diabetes, those at risk forcardiovascular disease, and those with type 2 diabetes [6].They found that lifestyle intervention did not improve SBP,DBP, or HDL. However, the fact their study evaluated aheterogeneous population of patients makes it difficult tocompare their finding with ours. Similar to our findings, theanalysis did not find lifestyle intervention affected LDL levels.Two other systematic reviews evaluated whether behavioralchanges, such as exercise training/physical activity and/ornutritional intervention, impacted the incidence of type 2diabetes in subjects at risk for the disease [12,13]. They foundthat although there was wide variability in efficacy, all theincluded studies indicated that behavioral changes thatincluded modification of diet and exercise reduced theincidence of type 2 diabetes compared with controls, with arelative risk reduction of 39%–75%. The systematic review alsofound a benefit in weight change and a reduction in BMI. In
addition, both reviews indicated that adopting a long-termapproach in changing behavior with several interventionalcomponents was most successful.
A literature review identified over 100 studies that assessedthe role of physical activity on cardiovascular disease insubjects with diabetes [11]. The authors conclude that overallthe literature suggests physical activity reduces the risk ofcardiovascular disease in people with diabetes. However, theycomment that a number of drug trials do not support the ideathat reduction of blood glucose concentration reduces cardio-vascular disease. Why exercise reduces the risk of cardiovas-cular disease in patients with diabetes is unclear.
There are several limitations to our analysis that should beconsidered when interpreting the findings. The includedstudies used diverse forms of interventions and there waslittle detail regarding the specifics of intervention methodol-ogy. Due to the lack of experimental detail in many publishedstudies, it is possible that other studiesmay have beenmisseddue poor descriptions of lifestyle interventions. We groupedall the types of interventions for our analysis; hence, it is notpossible to evaluate or compare the efficacy of each type ofintervention with improving markers of cardiovascular dis-ease. All included studies had a high risk for bias in regard toblinding of the participants and personnel that may haveaffected outcomes. The different included studies had a widerange of variability in age, sex, and duration of follow upwhich could have confounded our findings. Ideally, we wouldhave used subgroup analysis to address this problem.However, due to the limitation of extracting sufficient datafor each confounder, we were unable to perform this type ofanalysis. Another possible confounding factor is the potentialdifference between groups in drug prescriptions. Drug pre-scription information was only reported in 5 of the studies[21,23–25,31] and the data in these studies were not sufficientto allow us to perform multivariate analysis to adjust fordifferences in drug prescriptions. Although our funnel plotanalysis indicated there was no publication bias, this conclu-sion is limited owing to the large degree of clinical heteroge-neity across the included studies. We did not assess the effectof lifestyle intervention on death or adverse events due tocardiovascular disease; therefore, it is not clear how thechanges we see in cardiovascular disease-associated riskfactors reflect these clinical outcomes.
5. Conclusion
In summary, our meta-analysis found that lifestyle interven-tion which included change in diet, exercise, and educationshowed significant benefit in a number of risk factors whichare known to be associated with cardiovascular disease inpatients with type 2 diabetes.
Supplementary data to this article can be found online athttp://dx.doi.org/10.1016/j.metabol.2014.10.018.
Author contributions
Liang Chen: guarantor of integrity of the entire study; Jian-HaoPei: study concepts; Jian Kuang: study design, statistical
346 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
analysis; Hong-Mei Chen: data analysis; Zhong Chen:manuscript preparation; Zhong-Wen Li: manuscript editing;Hua-Zhang Yang: manuscript review.
Acknowledgments
None.
Conflict of interest
None.
R E F E R E N C E S
[1] Lloyd-Jones D, Adams R, Carnethon M, De Simone G,Ferguson TB, Flegal K, et al. Heart disease and strokestatistics–2009 update: a report from the American HeartAssociation Statistics Committee and Stroke StatisticsSubcommittee. Circulation 2009;119:e21-181.
[2] Deshpande AD, Harris-Hayes M, Schootman M. Epidemiologyof diabetes and diabetes-related complications. Phys Ther2008;88:1254–64.
[3] Boule NG, Haddad E, Kenny GP, Wells GA, Sigal RJ. Effects ofexercise on glycemic control and bodymass in type 2 diabetesmellitus: a meta-analysis of controlled clinical trials. JAMA2001;286:1218–27.
[4] American Diabetes A. Standards of medical care indiabetes–2013. Diabetes Care 2013;36(Suppl. 1):S11–66.
[5] Avery L, Flynn D, van Wersch A, Sniehotta FF, Trenell MI.Changing physical activity behavior in type 2 diabetes: asystematic review and meta-analysis of behavioralinterventions. Diabetes Care 2012;35:2681–9.
[6] Angermayr L, Melchart D, Linde K. Multifactorial lifestyleinterventions in the primary and secondary prevention ofcardiovascular disease and type 2 diabetes mellitus—asystematic review of randomized controlled trials. Ann BehavMed 2010;40:49–64.
[7] Schellenberg ES, DrydenDM, Vandermeer B, HaC, KorownykC.Lifestyle interventions for patients with and at risk for type 2diabetes: a systematic review and meta-analysis. Ann InternMed 2013;159:543–51.
[8] Yuen A, Sugeng Y, Weiland TJ, Jelinek GA. Lifestyle andmedication interventions for the prevention or delay of type 2diabetes mellitus in prediabetes: a systematic review ofrandomised controlled trials. Aust N Z J Public Health 2010;34:172–8.
[9] Brand T, Pischke CR, Steenbock B, Schoenbach J, Poettgen S,Samkange-Zeeb F, et al. What works in community-basedinterventions promoting physical activity and healthyeating? A review of reviews. Int J Environ Res Public Health2014;11(6):5866–88.
[10] Yang Z, Scott CA, Mao C, Tang J, Farmer AJ. Resistance exerciseversus aerobic exercise for type 2 diabetes: a systematic reviewand meta-analysis. Sports Med 2014;44(4):487–99.
[11] Koivula RW, Tornberg AB, Franks PW. Exercise anddiabetes-related cardiovascular disease: systematic review ofpublished evidence from observational studies and clinicaltrials. Curr Diab Rep 2013;13(3):372–80.
[12] Norris SL, Zhang X, Avenell A, Gregg E, Schmid CH, Lau J.Long-term non-pharmacological weight loss interventionsfor adults with prediabetes. Cochrane Database Syst Rev 2005(2):CD005270.
[13] Baker MK, Simpson K, Lloyd B, Bauman AE, Singh MA.Behavioral strategies in diabetes prevention programs: asystematic review of randomized controlled trials. DiabetesRes Clin Pract 2011;91(1):1–12.
[14] Cochrane Handbook for Systematic Reviews of InterventionsVersion 5.1.0. [updated March 2011] , In: Higgens JPT, GreenLA, editors. The Cochrane Collaboration; 2011.
[15] KadoglouNP, Iliadis F,AngelopoulouN, PerreaD,AmpatzidisG,Liapis CD, et al. The anti-inflammatory effects of exercisetraining in patients with type 2 diabetes mellitus. Eur JCardiovasc Prev Rehabil 2007;14:837–43.
[16] Look ARG, Wing RR. Long-term effects of a lifestyleintervention on weight and cardiovascular risk factors inindividuals with type 2 diabetes mellitus: four-year results ofthe Look AHEAD trial. Arch Intern Med 2010;170:1566–75.
[17] Coppell KJ, Kataoka M, Williams SM, Chisholm AW,Vorgers SM, Mann JI. Nutritional intervention in patientswith type 2 diabetes who are hyperglycaemic despiteoptimised drug treatment–Lifestyle Over and Above Drugsin Diabetes (LOADD) study: randomised controlled trial.BMJ 2010;341:c3337.
[18] Sone H, Tanaka S, Iimuro S, Tanaka S, Oida K, Yamasaki Y,et al. Long-term lifestyle intervention lowers the incidence ofstroke in Japanese patients with type 2 diabetes: a nationwidemulticentre randomised controlled trial (the Japan DiabetesComplications Study). Diabetologia 2010;53:419–28.
[19] Trento M, Passera P, Bajardi M, Tomalino M, Grassi G, Borgo E,et al. Lifestyle intervention by group care preventsdeterioration of Type II diabetes: a 4-year randomizedcontrolled clinical trial. Diabetologia 2002;45:1231–9.
[20] Ali M, Schifano F, Robinson P, Phillips G, Doherty L, Melnick P,et al. Impact of community pharmacy diabetes monitoringand education programme on diabetes management: arandomized controlled study. Diabet Med 2012;29:e326–33.
[21] Crasto W, Jarvis J, Khunti K, Skinner TC, Gray LJ, Brela J, et al.Multifactorial intervention in individuals with type 2 diabetesand microalbuminuria: the Microalbuminuria Education andMedication Optimisation (MEMO) study. Diabetes Res ClinPract 2011;93:328–36.
[22] Salinero-Fort MA, Carrillo-de Santa Pau E, Arrieta-Blanco FJ,Abanades-Herranz JC, Martín-Madrazo C, Rodés-Soldevila B,et al. Effectiveness of PRECEDEmodel for health education onchanges and level of control of HbA1c, blood pressure, lipids,and body mass index in patients with type 2 diabetesmellitus. BMC Public Health 2011;11:267.
[23] Ko GT, Li JK, Kan EC, Lo MK. Effects of a structured healtheducation programme by a diabetic education nurse oncardiovascular risk factors in Chinese Type 2 diabeticpatients: a 1-year prospective randomized study. Diabet Med2004;21:1274–9.
[24] Uusitupa M, Laitinen J, Siitonen O, Vanninen E, Pyorala K. Themaintenance of improved metabolic control after intensifieddiet therapy in recent type 2 diabetes. Diabetes Res Clin Pract1993;19:227–38.
[25] Wisse W, Boer Rookhuizen M, de Kruif MD, van Rossum J,Jordans I, ten Cate H, et al. Prescription of physical activity isnot sufficient to change sedentary behavior and improveglycemic control in type 2 diabetes patients. Diabetes Res ClinPract 2010;88:e10–3.
[26] Krein SL, Klamerus ML, Vijan S, Lee JL, Fitzgerald JT, Pawlow A,et al. Case management for patients with poorly controlleddiabetes: a randomized trial. Am J Med 2004;116:732–9.
[27] Dobrosielski DA, Gibbs BB, Ouyang P, Bonekamp S, Clark JM,Wang NY, et al. Effect of exercise on blood pressure in type 2diabetes: a randomized controlled trial. J Gen Intern Med2012;27:1453–9.
[28] Balducci S, ZanusoS,Nicolucci A, De Feo P, Cavallo S, Cardelli P,et al. Effect of an intensive exercise intervention strategy onmodifiable cardiovascular risk factors in subjects with type 2
347M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 4 ( 2 0 1 5 ) 3 3 8 – 3 4 7
diabetes mellitus: a randomized controlled trial: the ItalianDiabetes and Exercise Study (IDES). Arch Intern Med 2010;170:1794–803.
[29] Kirk A, Mutrie N, MacIntyre P, Fisher M. Effects of a 12-monthphysical activity counselling intervention on glycaemiccontrol and on the status of cardiovascular risk factors inpeople with Type 2 diabetes. Diabetologia 2004;47:821–32.
[30] SevickMA,KorytkowskiM,StoneRA, PirainoB,RenD,SereikaS,et al. Biophysiologic outcomes of the Enhancing Adherence inType 2 Diabetes (ENHANCE) trial. J Acad Nutr Diet 2012;112:1147–57.
[31] Chan CW, Siu SC, Wong CK, Lee VW. A pharmacist careprogram: positive impact on cardiac risk in patients with type2 diabetes. J Cardiovasc Pharmacol Ther 2012;17:57–64.