1 part 1 dermatologic surgery - newbooks services · chapter 1:cutaneous anatomy in dermatologic...
TRANSCRIPT
PART 1
Dermatologic Surgery 1
COPYRIG
HTED M
ATERIAL


3
Dermatologic Surgery: Step by Step, First Edition. Edited by Keyvan Nouri.
© 2013 Blackwell Publishing Ltd. Published 2013 by Blackwell Publishing Ltd.
CHAPTER 1
Cutaneous a natomy in d ermatologic s urgery Diana Bolotin 1 , Lucille White 2 , and Murad Alam 3 1 Section of Dermatology, University of Chicago, Chicago, IL, USA 2 Pearland Dermatology, Pearland, TX, USA 3 Department of Dermatology, Northwestern University, Chicago, IL, USA
Introduction
Knowledge of anatomy is essential to every surgeon. The
subtleties of surface anatomy require a special, fi ne - tuned
understanding and are meaningful for a successful der-
matologic procedure in both cutaneous oncology and
cosmetic surgery. Understanding the cutaneous anatomy
of the head and neck is essential in directing appropriate
anesthesia, reducing postoperative complications, and
providing for an acceptable cosmetic outcome. The
anatomy of the face is often regarded in terms of cosmetic
subunits and will be discussed as such in this chapter.
Scalp and f orehead
The frontal hairline separates the forehead from the scalp
superiorly and laterally, and the temporal region is sepa-
rated from the scalp by the temporal hairline. 1 The fore-
head ends at the zygomatic arch inferiorly, while the
inferior scalp is separated from the neck by the nuchal
line inferiorly. The anatomy of the layers of the scalp can
be recalled by the mnemonic S - C - A - L - P, which refers to
the s kin, c onnective tissue, a poneurotic galeal layer, l oose
connective tissue, and p eriosteum. In its most anterior
segment, the skin of the scalp measures about 3 – 4 mm in
thickness and reaches up to 8 mm in the more posterior
segments. Blood vessels, lymphatics, and cutaneous
adnexa reside within the connective tissue layers, while
the underlying musculature connects to the galea apone-
urotica. Muscles of the forehead and scalp include fron-
talis, temporalis, procerus, corrugator supercilii, and
superior fi bers of the orbicularis oculi (Figure 1.1 a).
Deep to the aponeurotic layer is the loose connective
tissue that is largely avascular but does contain perforat-
ing emissary veins. Lastly, the periosteum envelops the
bony skull and contains another layer of vasculature.
Vasculature The blood supply to the forehead and scalp subunits is
provided by branches of both the internal and the exter-
nal carotid arteries. The supratrochlear and supraorbital
arteries supply the central forehead and anterior scalp
and originate from the ophthalmic artery branch of the
internal carotid (Figure 1.1 b). The lateral forehead and
scalp are supplied by the superfi cial temporal and poste-
rior auricular branches of the external carotid artery
(Figure 1.1 c). The posterior scalp is supplied by the
occipital artery, another branch of the external carotid
(Figure 1.1 c).
Nerves The motor and sensory anatomy of the forehead and
scalp are a crucial part of surgery on these subunits.
Motor innervation of the forehead is provided by the
temporal branch of the facial nerve (CN VII). This
branch runs along the temple and the zygomatic arch
but courses more superfi cially superiorly to innervate the
1
4 PART 1: Dermatologic Surgery
(a)
(b)
Deep branch,supraorbital nerve
Facial nerve branchesTemporal
Zygomatic
Supraorbital nerveFrontalis muscleProcerus muscle
Depressor supercilii muscle Corrugator supercilii muscle
Orbicularis oculi muscle
Infratrochlear nerve
Supratrochlear nerve
Deep temporal artery
External nasal artery
Angular artery
Superior labial artery
Inferior labial artery
Dorsal nasal artery
Zygomatico-orbital artery
Supraorbital artery
Frontal branch ofsuperficial temporal artery
Supratrochlear artery
Infraorbital artery
Buccal artery
Facial artery
Mental artery
Submental artery
Transverse facial artery
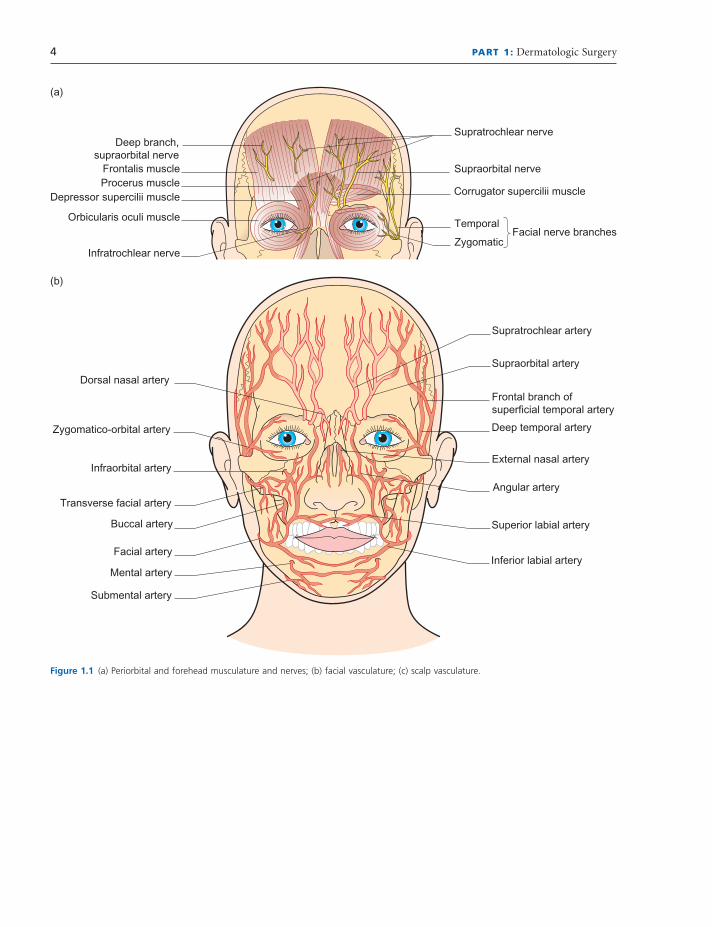
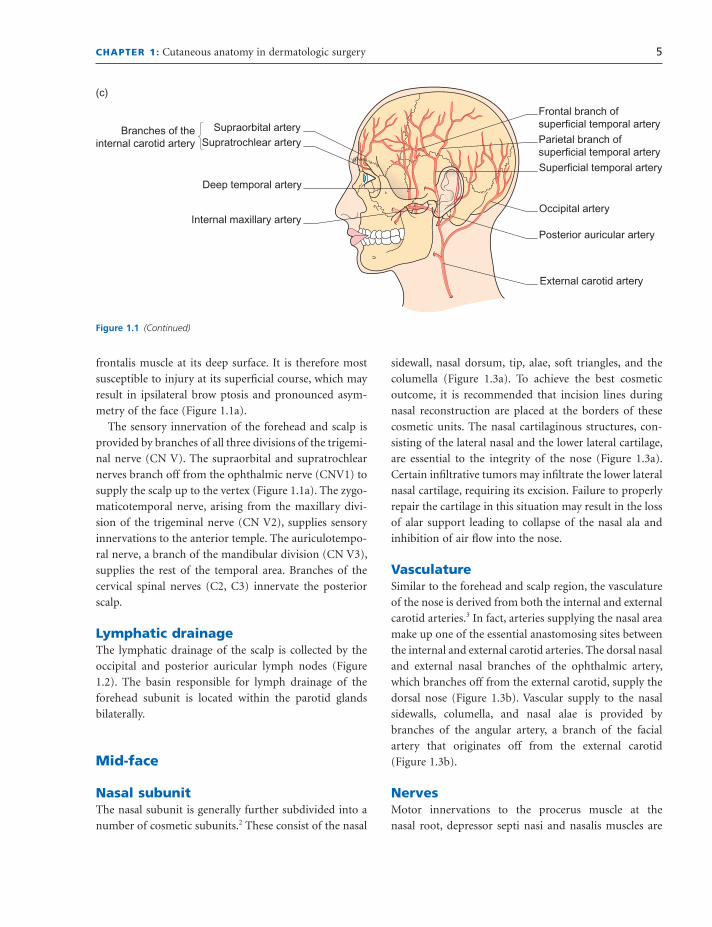
Figure 1.1 (a) Periorbital and forehead musculature and nerves; (b) facial vasculature; (c) scalp vasculature.
CHAPTER 1: Cutaneous anatomy in dermatologic surgery 5
sidewall, nasal dorsum, tip, alae, soft triangles, and the
columella (Figure 1.3 a). To achieve the best cosmetic
outcome, it is recommended that incision lines during
nasal reconstruction are placed at the borders of these
cosmetic units. The nasal cartilaginous structures, con-
sisting of the lateral nasal and the lower lateral cartilage,
are essential to the integrity of the nose (Figure 1.3 a).
Certain infi ltrative tumors may infi ltrate the lower lateral
nasal cartilage, requiring its excision. Failure to properly
repair the cartilage in this situation may result in the loss
of alar support leading to collapse of the nasal ala and
inhibition of air fl ow into the nose.
Vasculature Similar to the forehead and scalp region, the vasculature
of the nose is derived from both the internal and external
carotid arteries. 3 In fact, arteries supplying the nasal area
make up one of the essential anastomosing sites between
the internal and external carotid arteries. The dorsal nasal
and external nasal branches of the ophthalmic artery,
which branches off from the external carotid, supply the
dorsal nose (Figure 1.3 b). Vascular supply to the nasal
sidewalls, columella, and nasal alae is provided by
branches of the angular artery, a branch of the facial
artery that originates off from the external carotid
(Figure 1.3 b).
Nerves Motor innervations to the procerus muscle at the
nasal root, depressor septi nasi and nasalis muscles are
frontalis muscle at its deep surface. It is therefore most
susceptible to injury at its superfi cial course, which may
result in ipsilateral brow ptosis and pronounced asym-
metry of the face (Figure 1.1 a).
The sensory innervation of the forehead and scalp is
provided by branches of all three divisions of the trigemi-
nal nerve (CN V). The supraorbital and supratrochlear
nerves branch off from the ophthalmic nerve (CNV1) to
supply the scalp up to the vertex (Figure 1.1 a). The zygo-
maticotemporal nerve, arising from the maxillary divi-
sion of the trigeminal nerve (CN V2), supplies sensory
innervations to the anterior temple. The auriculotempo-
ral nerve, a branch of the mandibular division (CN V3),
supplies the rest of the temporal area. Branches of the
cervical spinal nerves (C2, C3) innervate the posterior
scalp.
Lymphatic d rainage The lymphatic drainage of the scalp is collected by the
occipital and posterior auricular lymph nodes (Figure
1.2 ). The basin responsible for lymph drainage of the
forehead subunit is located within the parotid glands
bilaterally.
Mid - f ace
Nasal s ubunit The nasal subunit is generally further subdivided into a
number of cosmetic subunits. 2 These consist of the nasal
Branches of theinternal carotid artery
External carotid artery
Deep temporal artery
Internal maxillary artery
Supraorbital artery
Frontal branch ofsuperficial temporal artery
(c)
Parietal branch ofsuperficial temporal artery
Superficial temporal artery
Occipital artery
Posterior auricular artery
Supratrochlear artery
Figure 1.1 (Continued)
6 PART 1: Dermatologic Surgery
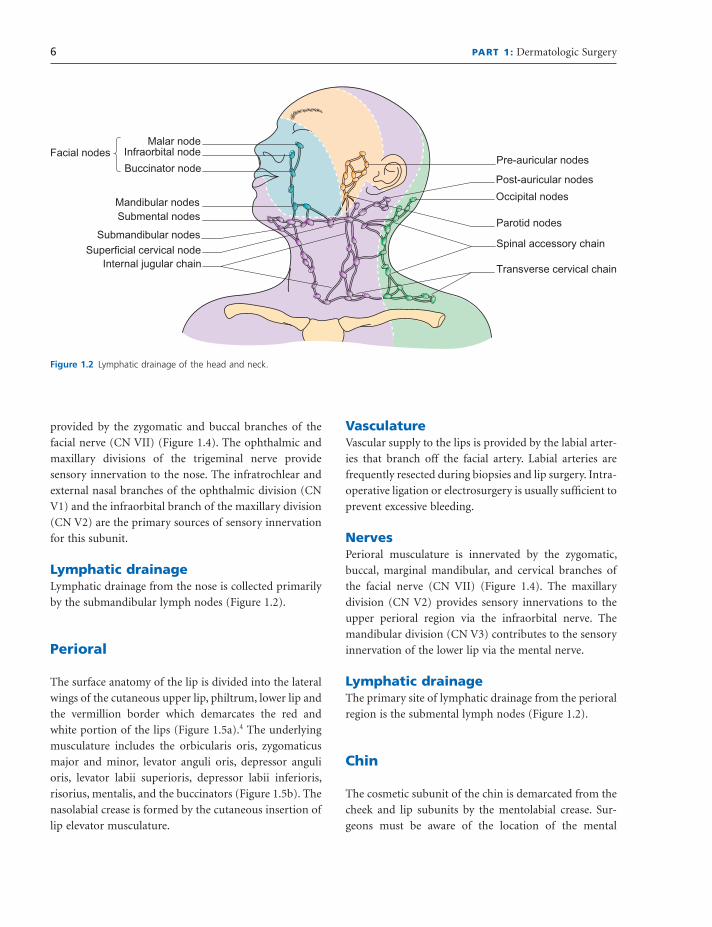
Figure 1.2 Lymphatic drainage of the head and neck.
Facial nodesMalar node
Submandibular nodes
Superficial cervical nodeInternal jugular chain
Pre-auricular nodes
Parotid nodes
Post-auricular nodes
Spinal accessory chain
Transverse cervical chain
Occipital nodes
Infraorbital node
Buccinator node
Mandibular nodesSubmental nodes
provided by the zygomatic and buccal branches of the
facial nerve (CN VII) (Figure 1.4 ). The ophthalmic and
maxillary divisions of the trigeminal nerve provide
sensory innervation to the nose. The infratrochlear and
external nasal branches of the ophthalmic division (CN
V1) and the infraorbital branch of the maxillary division
(CN V2) are the primary sources of sensory innervation
for this subunit.
Lymphatic d rainage Lymphatic drainage from the nose is collected primarily
by the submandibular lymph nodes (Figure 1.2 ).
Perioral
The surface anatomy of the lip is divided into the lateral
wings of the cutaneous upper lip, philtrum, lower lip and
the vermillion border which demarcates the red and
white portion of the lips (Figure 1.5 a). 4 The underlying
musculature includes the orbicularis oris, zygomaticus
major and minor, levator anguli oris, depressor anguli
oris, levator labii superioris, depressor labii inferioris,
risorius, mentalis, and the buccinators (Figure 1.5 b). The
nasolabial crease is formed by the cutaneous insertion of
lip elevator musculature.
Vasculature Vascular supply to the lips is provided by the labial arter-
ies that branch off the facial artery. Labial arteries are
frequently resected during biopsies and lip surgery. Intra-
operative ligation or electrosurgery is usually suffi cient to
prevent excessive bleeding.
Nerves Perioral musculature is innervated by the zygomatic,
buccal, marginal mandibular, and cervical branches of
the facial nerve (CN VII) (Figure 1.4 ). The maxillary
division (CN V2) provides sensory innervations to the
upper perioral region via the infraorbital nerve. The
mandibular division (CN V3) contributes to the sensory
innervation of the lower lip via the mental nerve.
Lymphatic d rainage The primary site of lymphatic drainage from the perioral
region is the submental lymph nodes (Figure 1.2 ).
Chin
The cosmetic subunit of the chin is demarcated from the
cheek and lip subunits by the mentolabial crease. Sur-
geons must be aware of the location of the mental

CHAPTER 1: Cutaneous anatomy in dermatologic surgery 7
Nerves Motor innervation to the chin is provided by the mar-
ginal mandibular branch of the facial nerve (CN VII).
Injury to this nerve may occur as it crosses the mandible
at the medial edge of the masseter muscle within the
superfi cial soft tissue (Figure 1.4 ). Marginal mandibular
injury is manifested as ipsilateral asymmetry of the lip
and chin during smiling. The mental nerve, entering via
the mental foramen, provides the sensory innervation to
the chin subunit.
foramen that carries the mental nerve and vessels to the
chin, and is located below the second mandibular premo-
lar tooth in the majority of the population. Musculature
of the chin consists of the mentalis, depressor anguli oris,
and depressor labii inferioris (Figure 1.5 b).
Vasculature The mental and submental arteries branch off the
external carotid artery to form the vascular supply of
the chin.
Figure 1.3 (a) Landmarks in nasal anatomy; (b) nasal vasculature and sensory nerves.
Sidewall
Dorsum
Softtriangle
Supratip
(a)
(b)
Infratip
Columella
Lobule
Ala
Alar margin
Tip
External nasalartery and nerve
Lateral nasalartery
Angular artery
Superior labialartery
Transversefacial artery
Infratrochlearnerve
Infratrochlear/dorsal nasal artery
Infraorbitalartery andnerve
Facial artery
8 PART 1: Dermatologic Surgery
branch of the internal carotid system anastomoses with
the angular branch of the facial artery in the vicinity
of the medial canthus (Figure 1.6 b). Supraorbital and
supratrochlear artery branches of the internal carotid
system also supply the upper eyelid area (Figure 1.6 b).
The external carotid artery supplies vasculature to the
lower eyelid by the infraorbital branch of the maxillary
artery and to the lateral periorbital area via the superfi cial
temporal artery.
Nerves Knowledge of neural anatomy of the periocular region is
crucial both to proper anesthesia and to botulinum toxin
treatment of the motor component of the eyelid region.
Sensory innervation is provided by the ophthalmic divi-
sion (CN V1). The glabella is innervated by the supratro-
chlear branch of the ophthalmic division. Sensation to
the lower eyelid is mediated by the infraorbital nerve. The
zygomatic branch of the facial nerve (CN VII) provides
motor innervations to the orbicularis oculi, levator
palpebrae superioris, and parts of the procerus muscles
(Figure 1.4 ). The temporal branch of facial nerve is
responsible for motor innervations of the corrugators
and procerus.
Lymphatic d rainage The submental lymph node basin collects lymphatic
drainage from the chin subunit (Figure 1.2 ).
Periorbital
An understanding of periorbital anatomy is key to avoid-
ance of ectropion and entropion complications of cuta-
neous surgery in this region. The eyelids are made up of
the skin, orbicularis oculi muscle, the tarsus, and the
conjunctiva. 5 Overall structural support to the eyelids is
provided by the medial and lateral canthal tendons. The
superior and inferior lacrimal canaliculi are enveloped by
the medial canthal tendon and are the means of passage
of tears to the lacrimal sac. Disruption of the canaliculi
will lead to a defect in tear drainage. Glands of Zeis and
meibomian glands are large sebaceous glands that reside
in the eyelids (Figure 1.6 a). Glands of Moll are apocrine
glands of the eyelids (Figure 1.6 a).
Vasculature The internal and external carotid arteries provide a vas-
cular supply to the periorbital area. The dorsal nasal
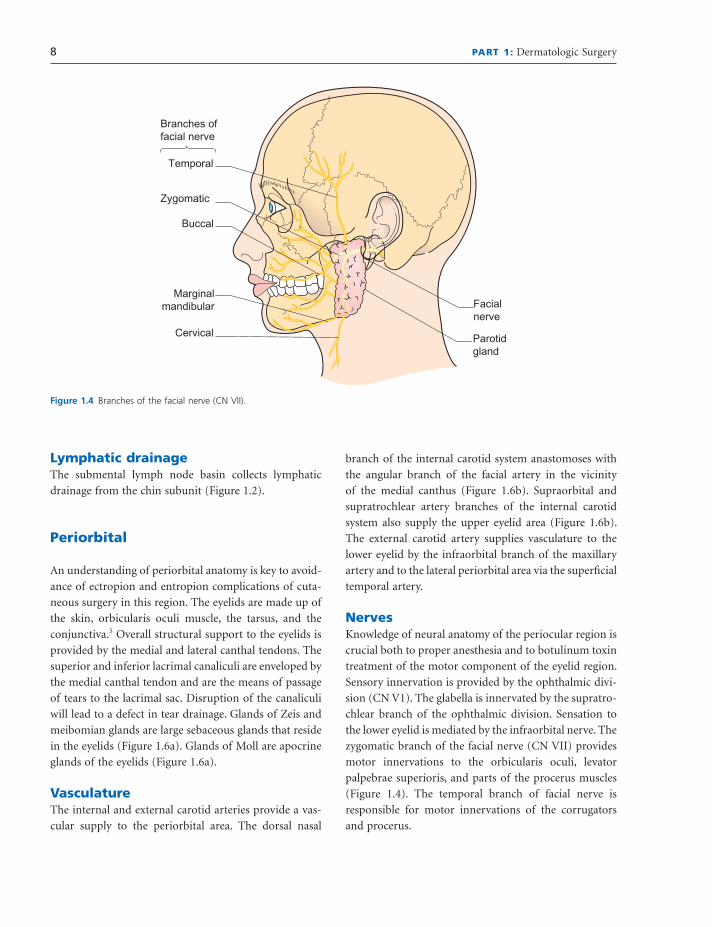
Figure 1.4 Branches of the facial nerve (CN VII).
Branches offacial nerve
Temporal
Zygomatic
Buccal
Cervical
Marginalmandibular Facial
nerve
Parotidgland

CHAPTER 1: Cutaneous anatomy in dermatologic surgery 9
subdivided into the medial, zygomatic, buccal, and lateral
cheek units. Each of these has unique surface charac-
teristics and sebaceous nature that must be taken into
account during reconstruction. 6
Vasculature Vasculature supplying the cheek subunit is derived from
the external carotid artery system. The transverse facial
artery supplies the lateral cheek. The angular branch of
the facial artery and the infraorbital artery supply the
medial aspects of the cheeks (Figure 1.1 b). Multiple anas-
tomotic connections within the cheek make this subunit
a highly vascularized skin surface.
Lymphatic d rainage The lymphatic drainage basin of the lateral eyelid area
lies primarily within the parotid lymph nodes. Medial
canthus lymph drains to the submandibular lymph node
basin.
Cheeks
The cheek is the largest facial subunit. Its superior border
is made of the infraorbital rim and zygomatic arch.
The nasolabial and melolabial folds mark the medial
border and the pre - auricular crease makes up the lateral
border of the cheek. The cheek subunit can be further
Figure 1.5 (a) Perioral anatomic landmarks; (b) perioral musculature.
Cutaneoousupper lip
Vermillionborder
Labiomentalgroove
Labialtubercle
Oral fissure
Labialcommissure
Philtrum
(a)
Superficial Deep
Risorius muscle
Platysma muscle
Levator labi superiorisalaeque nasi muscle Levator labi
superioris muscleLevator angularis
oris muscle
Facial nerve,zygomatic branches
Zygomaticusminor muscle
Zygomaticusmajor muscle
Orbicularis oris muscle
Infraorbital nerve
Nasalis muscle
Mental nerve
Mental muscle
Depressor labiinferioris muscle
Depressor angulioris muscle
(b)
10 PART 1: Dermatologic Surgery
of the cheek subunit. The auriculotemporal nerve
innervates parts of the lateral cheek with the buccal
nerve providing sensation to the lateral and buccal
portions. The mental nerve innervates the inferior
medial aspects.
Lymphatic d rainage The parotid and submandibular nodes collect the lym-
phatic drainage from the cheek subunit.
Nerves The muscles of the cheek are supplied with motor inner-
vation by the zygomatic and buccal branches of the
facial nerve (CN VII) (Figure 1.4 ). The infraorbital,
zygomaticofacial, and zygomaticotemporal branches of
the maxillary division of the trigeminal nerve supply
sensation to the medial and zygomatic aspects of the
cheek. Nerves emanating from the mandibular division
of the trigeminal nerve provide sensation to the rest
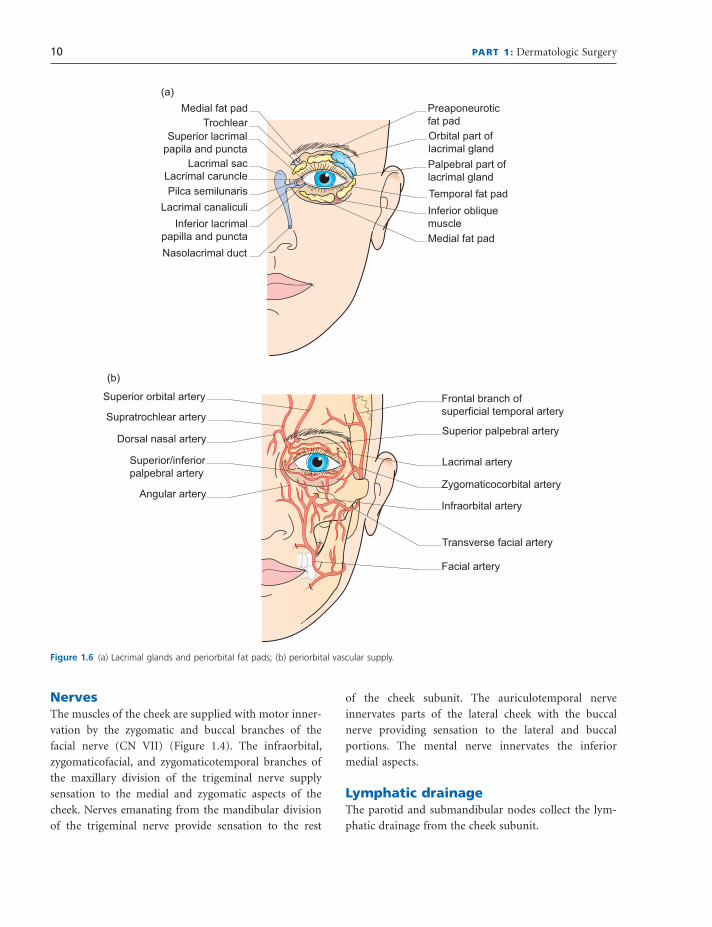
Figure 1.6 (a) Lacrimal glands and periorbital fat pads; (b) periorbital vascular supply.
Medial fat pad Preaponeuroticfat pad
Temporal fat pad
Medial fat pad
Inferior obliquemuscle
Superior lacrimalpapila and puncta
Pilca semilunarisLacrimal caruncle
Orbital part oflacrimal glandPalpebral part oflacrimal gland
Lacrimal sac
Nasolacrimal duct
Lacrimal canaliculiInferior lacrimal
papilla and puncta
Trochlear
(a)
(b)
Superior/inferiorpalpebral artery
Superior palpebral artery
Lacrimal artery
Angular arteryZygomaticocorbital artery
Superior orbital artery Frontal branch ofsuperficial temporal artery
Transverse facial artery
Facial artery
Dorsal nasal artery
Supratrochlear artery
Infraorbital artery
CHAPTER 1: Cutaneous anatomy in dermatologic surgery 11
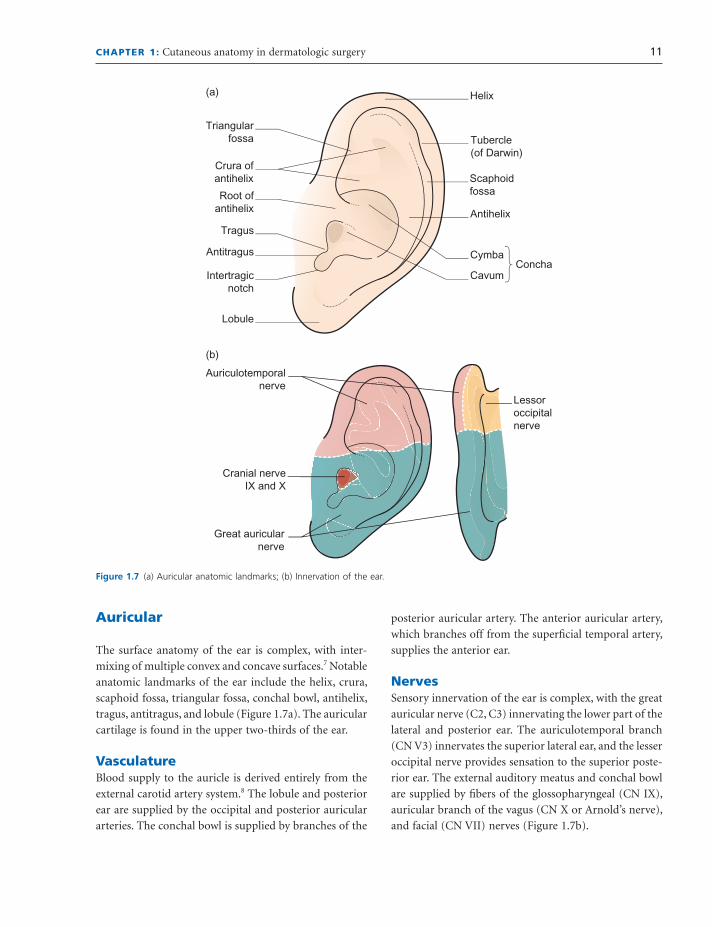
posterior auricular artery. The anterior auricular artery,
which branches off from the superfi cial temporal artery,
supplies the anterior ear.
Nerves Sensory innervation of the ear is complex, with the great
auricular nerve (C2, C3) innervating the lower part of the
lateral and posterior ear. The auriculotemporal branch
(CN V3) innervates the superior lateral ear, and the lesser
occipital nerve provides sensation to the superior poste-
rior ear. The external auditory meatus and conchal bowl
are supplied by fi bers of the glossopharyngeal (CN IX),
auricular branch of the vagus (CN X or Arnold ’ s nerve),
and facial (CN VII) nerves (Figure 1.7 b).
Auricular
The surface anatomy of the ear is complex, with inter-
mixing of multiple convex and concave surfaces. 7 Notable
anatomic landmarks of the ear include the helix, crura,
scaphoid fossa, triangular fossa, conchal bowl, antihelix,
tragus, antitragus, and lobule (Figure 1.7 a). The auricular
cartilage is found in the upper two - thirds of the ear.
Vasculature Blood supply to the auricle is derived entirely from the
external carotid artery system. 8 The lobule and posterior
ear are supplied by the occipital and posterior auricular
arteries. The conchal bowl is supplied by branches of the
Figure 1.7 (a) Auricular anatomic landmarks; (b) Innervation of the ear.
Triangularfossa
Scaphoidfossa
Crura ofantihelix
Antihelix
ConchaCymba
Cavum
Root ofantihelix
Tragus
Intertragicnotch
Lobule
Tubercle(of Darwin)
Helix
Antitragus
(a)
(b)
Cranial nerveIX and X
Great auricularnerve
Auriculotemporalnerve
Lessoroccipitalnerve
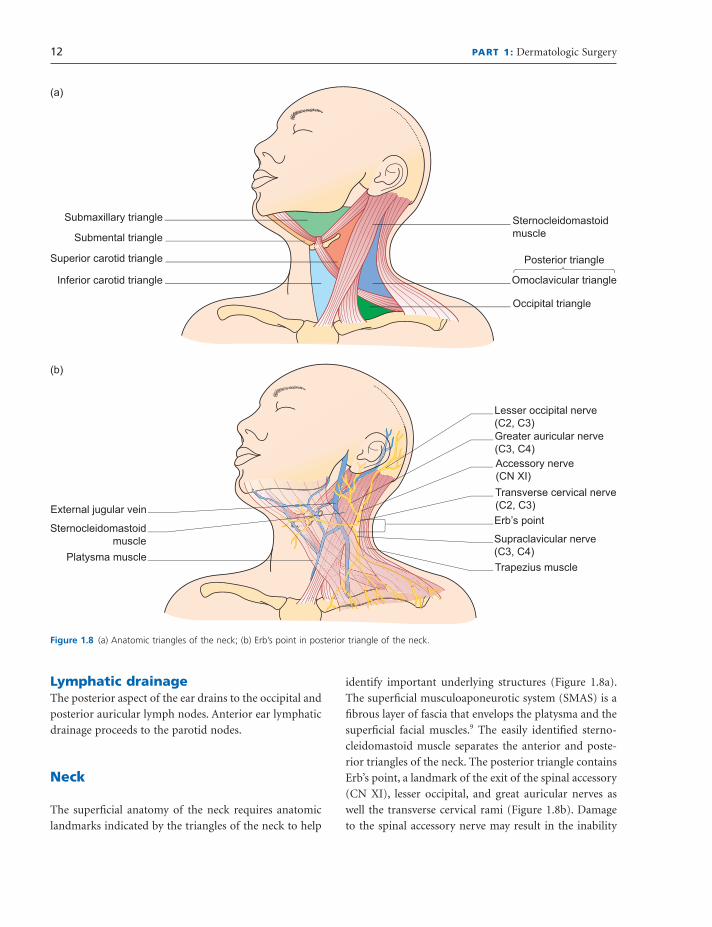
12 PART 1: Dermatologic Surgery
identify important underlying structures (Figure 1.8 a).
The superfi cial musculoaponeurotic system (SMAS) is a
fi brous layer of fascia that envelops the platysma and the
superfi cial facial muscles. 9 The easily identifi ed sterno-
cleidomastoid muscle separates the anterior and poste-
rior triangles of the neck. The posterior triangle contains
Erb ’ s point, a landmark of the exit of the spinal accessory
(CN XI), lesser occipital, and great auricular nerves as
well the transverse cervical rami (Figure 1.8 b). Damage
to the spinal accessory nerve may result in the inability
Lymphatic d rainage The posterior aspect of the ear drains to the occipital and
posterior auricular lymph nodes. Anterior ear lymphatic
drainage proceeds to the parotid nodes.
Neck
The superfi cial anatomy of the neck requires anatomic
landmarks indicated by the triangles of the neck to help
Figure 1.8 (a) Anatomic triangles of the neck; (b) Erb ’ s point in posterior triangle of the neck.
Submaxillary triangle
Submental triangle
Superior carotid triangle Posterior triangle
Occipital triangle
Omoclavicular triangle
Sternocleidomastoidmuscle
Inferior carotid triangle
(a)
(b)
External jugular veinErb’s point
Supraclavicular nerve(C3, C4)Trapezius muscle
Platysma muscle
Sternocleidomastoidmuscle
Lesser occipital nerve(C2, C3)Greater auricular nerve(C3, C4)Accessory nerve(CN XI)Transverse cervical nerve(C2, C3)

CHAPTER 1: Cutaneous anatomy in dermatologic surgery 13
2. Burget GC , Menick FJ . The subunit principle in nasal recon-
struction . Plast Reconstr Surg 1985 ; 76 : 239 – 47 .
3. Oneal RM , Beil RJ . Surgical anatomy of the nose . Clin Plast
Surg 2010 ; 37 : 191 – 211 .
4. Gassner HG , Rafi i A , Young A , Murakami C , Moe KS ,
Larrabee WF , Jr . Surgical anatomy of the face: implications
for modern face - lift techniques . Arch Facial Plast Surg
2008 ; 10 : 9 – 19 .
5. Most SP , Mobley SR , Larrabee WF , Jr . Anatomy of the eyelids .
Facial Plast Surg Clin North Am 2005 ; 13 : 487 – 92 , v.
6. Dobratz EJ , Hilger PA . Cheek defects . Facial Plast Surg Clin
North Am 2009 ; 17 : 455 – 67 .
7. Shonka DC , Jr ., Park SS . Ear defects . Facial Plast Surg Clin
North Am 2009 ; 17 : 429 – 43 .
8. Park C , Lineaweaver WC , Rumly TO , Buncke HJ . Arterial
supply of the anterior ear . Plast Reconstr Surg 1992 ; 90 :
38 – 44 .
9. Mitz V , Peyronie M . The superfi cial musculo - aponeurotic
system (SMAS) in the parotid and cheek area . Plast Reconstr
Surg 1976 ; 58 : 80 – 8 .
to raise the ipsilateral shoulder. The jugular and carotid
vessels run through the carotid triangle (Figure 1.8 a). The
mental lymph node basin and lingual arteries occupy the
submental triangle. The submaxillary triangle includes
the lingual nerve, artery, and vein, and hypoglossal nerve.
Nerves The cervical branch of the facial nerve (CN VII) provides
the motor innervation to the platysma. Sensory innerva-
tion to this area is provided by the transverse cervical,
supraclavicular, and great auricular nerves.
Lymphatic d rainage Lymphatic nodes of the neck region are the secondary
lymph nodes that receive drainage from most nodes on
the face. These eventually empty into the venous circula-
tion via the thoracic duct.
References
1. Angelos PC , Downs BW . Options for the management of
forehead and scalp defects . Facial Plast Surg Clin North Am
2009 ; 17 : 379 – 93 .