1 new developments in the management of advanced breast cancer supported by an educational grant...
TRANSCRIPT
1
New Developments in the New Developments in the Management of Advanced Breast Management of Advanced Breast CancerCancer
Supported by an educational grant from Roche Laboratories
Including Updates from ASCO 2007
Jointly Sponsored by:
2
Course ObjectivesCourse Objectives
At the conclusion of this course, participants should be able to:
1. Describe the latest advances in cellular biomarkers in determining disease prognosis and predicting response to/effectiveness of therapy.
2. Review the role of chemotherapy in the management of advanced breast cancer and discuss its impact on patient outcomes.
3. Review the role of targeted therapies (eg, small molecule
tyrosine kinase inhibitors and monoclonal antibodies) in the management of advanced breast cancer and discuss their impact on patient outcomes.
4. Explain the potential use of combination targeted therapies to replace, in some instances, chemotherapy.

3
Program AgendaProgram Agenda
Prognostic and Predictive Biomarkers of BC
Cytotoxic and Targeted Therapy- Chemotherapy- Tyrosine Kinase Inhibitors- Lapatinib Combinations- Monoclonal Antibodies
New Couplets in Advanced Breast Cancer

4
Prognostic and Predictive Prognostic and Predictive Biomarkers of Breast CancerBiomarkers of Breast Cancer

5
Prognostic and Predictive BiomarkersPrognostic and Predictive Biomarkers
Prognostic biomarker- Used to identify patients with inherently good prognosis
who may be cured with locoregional therapy alone and have low risk of metastatic relapse
- Associated with disease-free or overall survival in the absence of adjuvant therapy
Predictive biomarker- Allows identification of individuals who will benefit from a
particular drug treatment regimen

6
Circulating Tumor Cells (CTCs)Circulating Tumor Cells (CTCs)
CTCs may be predictive of prognosis and treatment efficacy in BC
Preliminary data suggest that 5 CTCs/7.5 mL blood associated with worse progression-free survival (PFS) and overall survival (OS)- Persistence of 5 CTCs/7.5 mL blood after therapy initiation predicts
treatment failure1
Prospective study conducted to measure serial CTCs in patients with MBC2
- 10-mL blood samples collected at baseline and at 3- to 4-week intervals; CTC enumeration performed using CellSearch technology
- All subjects followed for PFS and OS- Clinical outcomes based on radiographic studies and physical
examination in accordance with Response Evaluation Criteria in Solid Tumors (RECIST) criteria
1. Cristofanilli M et al. N Engl J Med. 2004;351:781-791. 2. Liu MC et al. J Clin Oncol. 2007;25(Suppl 18S):10535.

7
CTCs:CTCs:Study ResultsStudy Results
46 of 100 subjects have been accrued; 33 have completed 1 radiographic staging evaluation (median followup 7 mo)
Treatment for 33 evaluable patients:- Cytotoxic chemotherapy (27%)- Endocrine therapy (46%)- Combination therapy with biologic agent (27%)
CTCs at baseline (per 7.5 mL blood)- 28/33 (85%) had 1 - 9/33 (27%) had 5
Median PFS - 2.57 mo for subjects with 5 CTCs/7.5 mL at baseline- 6.77 mo for subjects with <5 CTCs/7.5 mL at baseline (P=0.02)
Liu MC et al. J Clin Oncol. 2007;25(Suppl 18S):10535.
8
CTCs in Progression of MBC:CTCs in Progression of MBC:Study DesignStudy Design
20 patients with MBC; 25 healthy controls
8-mL blood samples drawn at beginning of new chemo or hormonal treatment line
Blood samples screened for presence of CTCs with quantitative PCR method using molecular probes for human mammaglobin (hMAM) and cytokeratin 19 (CK19)
Relative quantification of hMAM and CK19 RNA obtained using blood sample infected with known concentrations of MDA-MB453 cells as calibrator
Median followup 7+4.5 mo
Altimari A et al. J Clin Oncol. 2007;25(Suppl 18S):21066.

9
CTCs in Progression of MBC:CTCs in Progression of MBC:Results and ConclusionsResults and Conclusions
18/20 (90%) patients CTC+ (1 marker) 15/20 (75%) patients CK19+ 9/20 (45%) patients hMAM+
Disease progression- 7/14 patients with disease progression died- All 14 patients with disease progression CTC+- 7/9 hMAM+ (78%) patients had disease progression- 11/15 (73%) patients CK19+
Multiple- vs single-marker detection preferred for CTC blood screening in BC
Combined hMAM and CK19 evaluation might identify patients at higher risk of tumor progression and might aid in stratification and decision making in MBC
Altimari A et al. J Clin Oncol. 2007;25(Suppl 18S):21066.

10
Lymph Node-negative Breast CancerLymph Node-negative Breast Cancer
Presence or absence of axillary lymph node (ALN) involvement most significant prognostic indicator in early-stage BC- Untreated patients with lymph node-negative cancer
have better clinical outcome than untreated patients with lymph node-positive cancer
Sentinel lymph node (SLN) biopsy is standard of care in assessing ALN status
Cianfrocca M, Goldstein LJ. The Oncologist. 2004;9:606-616.

11
Survival in Node-negative BC Patients:Survival in Node-negative BC Patients:SLN Biopsy vs ALN Dissection (ALND)SLN Biopsy vs ALN Dissection (ALND)
355 node-negative patients with early-stage BC- Underwent either ALND (n=178) in 1990−1997 or SLN biopsy (n=177) in
1998−2004
Primary outcome measures- Long-term disease-free and overall survival
SLN group had significantly better disease-free (P=0.012) and overall survival (P=0.04) compared with ALND group
Langer I et al. J Clin Oncol. 2007;25(Suppl 18S):609.

12
Cytotoxic and Targeted TherapyCytotoxic and Targeted TherapyChemotherapy

13
Ixabepilone - BackgroundIxabepilone - Background
A semisynthetic analog of epothilone B
Belongs to new class of microtubule-stabilizing agents, epothilones, derived from fermentation of myxobacterium Sorangium cellulosum1
- Epothilones bind tubulin and result in apoptotic cell death division2
- Epothilones compete with paclitaxel for binding to microtubules3
Epothilones appear to possess several advantages over paclitaxel- Avoid development of resistance4
- Have greater polymerizing activity than paclitaxel3
Ixabepilone has demonstrated consistent preclinical activity and seems active against various taxane-sensitive and taxane-resistant cell lines1
1. Pivot X et al. Clin Breast Cancer. 2007;7:543-549.2. Cortes J, Baselga J. Oncologist. 2007;12:271-280.3. Kowalski RJ et al. J Biol Chem. 1997;272:2534-2541.4. Bollag DM et al. Cancer Res. 1995;55:2325-2333.

14
Capecitabine (C) + Ixabepilone (IXA) vs Capecitabine (C) + Ixabepilone (IXA) vs C Alone: Study DesignC Alone: Study Design
C showed ORR 9−14% in phase 3 trials for women previously treated with anthracycline and/or taxane
IXA shows synergy with C; low susceptibility to resistance mechanisms- Phase 1/2 data show activity in anthracycline/taxane pretreated tumors
Study Eligibility Metastatic or locally
advanced BC
Resistant to taxanes or anthracyclines
n=375
Vahdat LT et al. J Clin Oncol. 2007;25(Suppl 18S):1006.
IXA 40 mg/m2 IV over 3 hr day 1 q3 wk+
C 2000 mg/m2/day PO in 2 divided doses days 1−14 q3 wk
R
A
N
D
O
M
I
Z
E
D
C 2500 mg/m2/day PO in 2 divided doses days 1−14 q3 wk
n=377

15
Capecitabine (C) + Ixabepilone (IXA) vs Capecitabine (C) + Ixabepilone (IXA) vs C Alone: Response RatesC Alone: Response Rates
Investigator IRR
IXA + C
(N=375)
C
(N=377)
IXA + C
(N=375)
C
(N=377)
ORR (CR + PR) 42 23 35 14
P< 0.0001 P<0.0001
Stable Disease 36 38 41 46
Progressive Disease 14 29 15 27
Unable to Determine 8 10 9 12
Median Progression-Free Survival
5.8 mo 4.2 mo
HR 0.75, P=0.0003
Vahdat LT et al. J Clin Oncol. 2007;25(Suppl 18S):1006.

16
Vinflunine - BackgroundVinflunine - Background
A third-generation vinca alkaloid microtubule inhibitor- Binds to beta tubulin and accumulates in G2/M phase of cell cycle- Promotes cellular apoptosis- Demonstrates antiangiogenic and vascular disrupting properties
Evidence of promising activity in patients with anthracycline- and taxane-pretreated MBC
Campone M et al. Br J Cancer. 2006;95:1161-1166.

17
Vinflunine (V) in First-line MBC:Vinflunine (V) in First-line MBC:Study DesignStudy Design
Phase 2, open-label, multicenter, 2-arm trial- 96 patients to be enrolled (48 per cohort)- 18 patients currently enrolled; 12 evaluable for response and
13 evaluable for toxicity
HER2-- V 320 mg/m2 IV q21 days (n=3)- Patients treated until disease progression or toxicity
HER2+ (FISH)- V 280 mg/m2 IV q21 days and trastuzumab 8 mg/kg IV loading
dose, followed by 6 mg/kg IV q21 days (n=10)- Patients treated with minimum of 6 cycles or until maximal
tumor response, then continue with trastuzumab monotherapy until disease progression
Peacock NW et al. J Clin Oncol. 2007;25(Suppl 18S):1043.
18
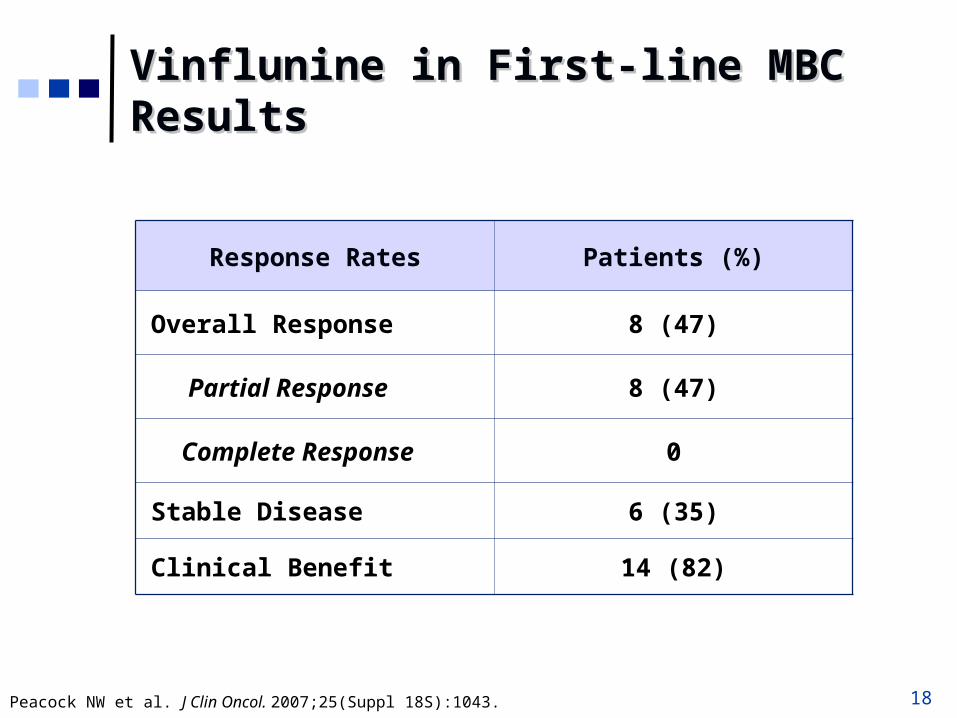
Vinflunine in First-line MBCVinflunine in First-line MBCResultsResults
Response Rates Patients (%)
Overall Response 8 (47)
Partial Response 8 (47)
Complete Response 0
Stable Disease 6 (35)
Clinical Benefit 14 (82)
Peacock NW et al. J Clin Oncol. 2007;25(Suppl 18S):1043.

19
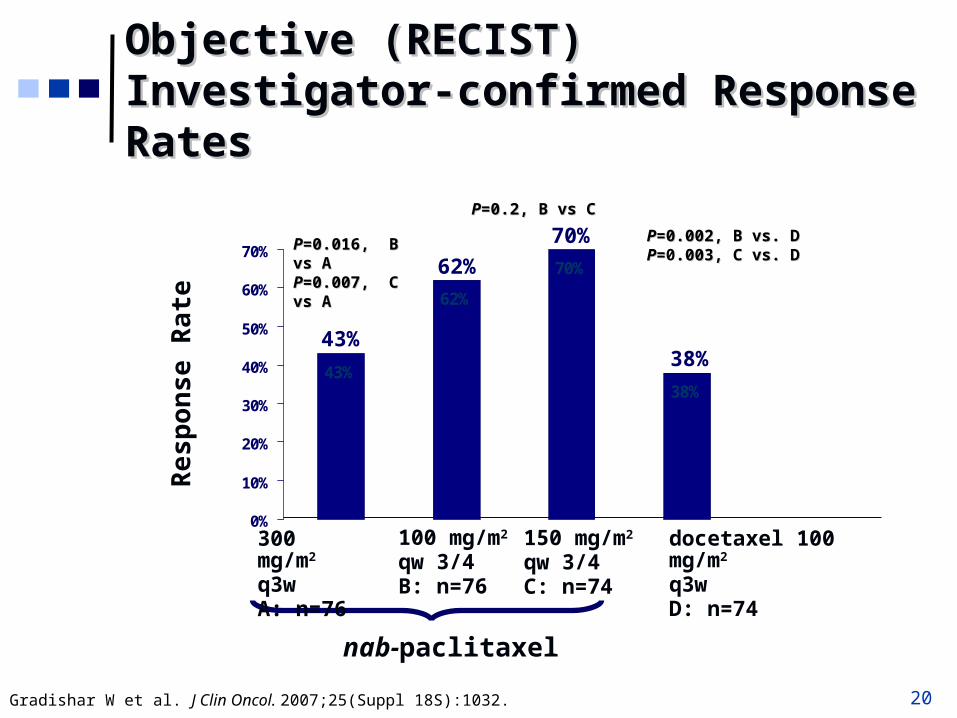
Nanoparticle albumin-bound (Nanoparticle albumin-bound (nab)nab)--Paclitaxel in First-line MBC: Study DesignPaclitaxel in First-line MBC: Study Design
Comparisonsnab-paclitaxel vs docetaxel (A, B, C vs D)
weekly vs q3w nab-paclitaxel (B, C vs A)
Low- vs high-dose weekly nab-paclitaxel (B vs C)
Arm A: nab-paclitaxel 300 mg/m2 q3 wk
Arm B: nab-paclitaxel 100 mg/m2
weekly 3 out of 4 wk
Arm C: nab-paclitaxel 150 mg/m2
weekly 3 out of 4 wk
Arm D: docetaxel 100 mg/m2 q3 wk
RANDOMIZED
n=300; Arms A, C and D administered at the MTD
Gradishar W et al. J Clin Oncol. 2007;25(Suppl 18S):1032.
20
43%
62%
70%
38%
0%
10%
20%
30%
40%
50%
60%
70% PP=0=0.016, .016, B vs AB vs APP=0.007,=0.007, C vs A C vs A
Objective (RECIST) Objective (RECIST) Investigator-confirmed Response RatesInvestigator-confirmed Response Rates
PP=0.002, B vs. D=0.002, B vs. DPP==0.003,.003, C vs. DC vs. D
Re
sp
on
se
Ra
te
nab-paclitaxel
PP=0.2, B vs C=0.2, B vs C
300 mg/m2
q3wA: n=76
100 mg/m2
qw 3/4B: n=76
150 mg/m2
qw 3/4C: n=74
docetaxel 100 mg/m2
q3wD: n=74
43%
62%
70%
38%
Gradishar W et al. J Clin Oncol. 2007;25(Suppl 18S):1032.
21
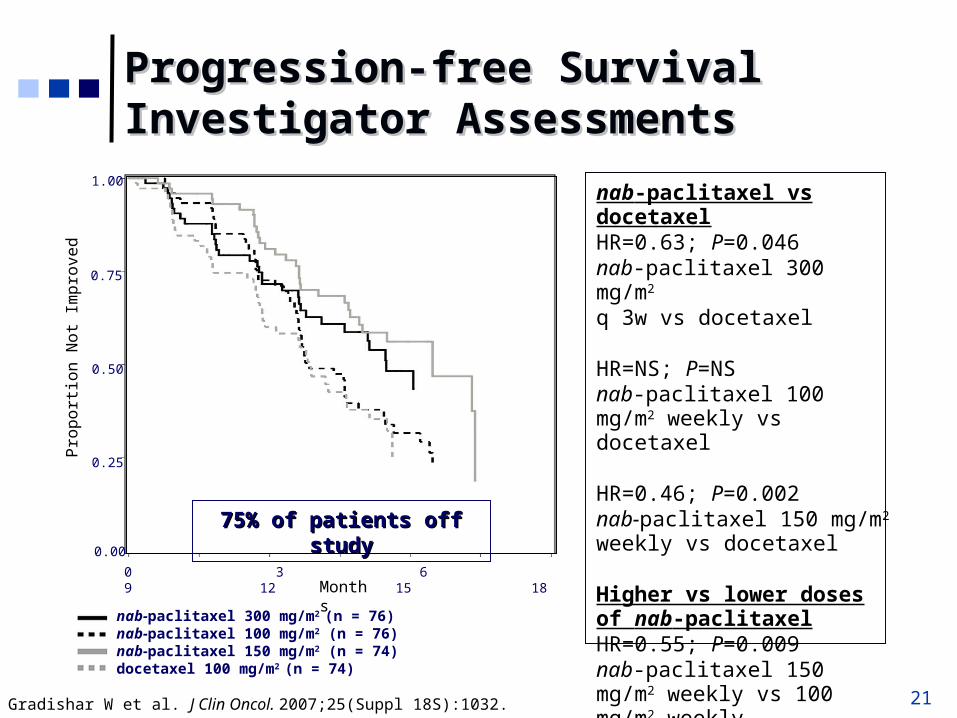
nab-paclitaxel vs docetaxelHR=0.63; P=0.046nab-paclitaxel 300 mg/m2 q 3w vs docetaxel
HR=NS; P=NSnab-paclitaxel 100 mg/m2 weekly vs docetaxel
HR=0.46; P=0.002nab-paclitaxel 150 mg/m2 weekly vs docetaxel
Higher vs lower doses of nab-paclitaxelHR=0.55; P=0.009nab-paclitaxel 150 mg/m2 weekly vs 100 mg/m2 weekly
75% of patients off study75% of patients off study
nab-paclitaxel 300 mg/m2 (n = 76)nab-paclitaxel 100 mg/m2 (n = 76)nab-paclitaxel 150 mg/m2 (n = 74)docetaxel 100 mg/m2 (n = 74)
Gradishar W et al. J Clin Oncol. 2007;25(Suppl 18S):1032.
Progression-free Survival Progression-free Survival Investigator AssessmentsInvestigator Assessments
1.00
0.75
0.50
0.25
0.00
0 3 6 9 12 15 18
Pro
po
rtio
n N
ot
Imp
rove
d
Months

22
Cytotoxic and Targeted TherapyCytotoxic and Targeted Therapy Tyrosine Kinase Inhibitors Lapatinib Combinations

23
Axitinib - BackgroundAxitinib - Background
A potent oral tyrosine kinase inhibitor and selective inhibitor of vascular endothelial growth factor receptors
Previous phase I/II study identified appropriate doses of docetaxel and axitinib- Docetaxel 80 mg/m2 q3w with axitinib 5 mg bid
Rugo HS et al. San Antonio Breast Cancer Symposium; December 8-11, 2005; San Antonio, Texas. Abstract 1067.
24
Axitinib (A) + Docetaxel (D) vs Axitinib (A) + Docetaxel (D) vs Docetaxel (D) + Placebo (PL): Docetaxel (D) + Placebo (PL): Study DesignStudy Design
Randomized, double-blind, phase 2 study
Patients- Locally recurrent or metastatic HER2- BC- No prior chemotherapy for MBC- Adjuvant chemotherapy >12 months
Primary endpoint- Time to progression (TTP)
Rugo HS et al. J Clin Oncol. 2007;25(Suppl 18S):1003.

25
Axitinib (A) + Docetaxel (D) vs Axitinib (A) + Docetaxel (D) vs Docetaxel (D) + Placebo (PL): ResultsDocetaxel (D) + Placebo (PL): Results
A + D
N=112
N (%)
D + PL
N=56
N (%)
Complete response 1 (0.9) 0
Partial response 44 (39.3) 13 (23.2)
Stable disease 10 (8.9) 9 (16.1)
Progressive disease 38 (33.9) 24 (42.9)
Indeterminate/unknown 19 (17.0) 10 (17.9)
Rugo HS et al. J Clin Oncol. 2007;25(Suppl 18S):1003.
Response Rate by RECIST

26
Axitinib (A) + Docetaxel (D) vs Axitinib (A) + Docetaxel (D) vs Docetaxel (D) + Placebo (PL): ResultsDocetaxel (D) + Placebo (PL): Results
0 100 200 300 400 500 600 700
TTP (Days)
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n n
ot
Pro
gre
sse
d A + D
D + PL
N=112, Median TTP= 8.2 mo
N=56, Median TTP= 7.0 mo
Rugo HS et al. J Clin Oncol. 2007;25(Suppl 18S):1003.
Hazard ratio=0.73 (one-sided P=0.052) 95% CI: 0.49, 1.07
Time to Progression (TTP)

27
Lapatinib (L) + Capecitabine (C):Lapatinib (L) + Capecitabine (C):Study DesignStudy Design
Recently published results of a phase 3, randomized, open-label study demonstrated that L+C improved time to progression (TTP)1
Current study conducted to update efficacy data and results of correlative studies2
- To determine if gene expression levels in 5-FU and HER pathways associated with clinical benefit in L+C
Tumor blocks available on 217/399 patients; tumors evaluated for expression of:- HER 1−4- Thymidylate synthase- Thymidine phosphorylase- PTEN (tumor suppressor protein)- cMYC
1. Geyer CE et al. N Engl J Med. 2006;355:2733-2743.2. Geyer CE et al. J Clin Oncol. 2007;25(Suppl 18S):1035.
28
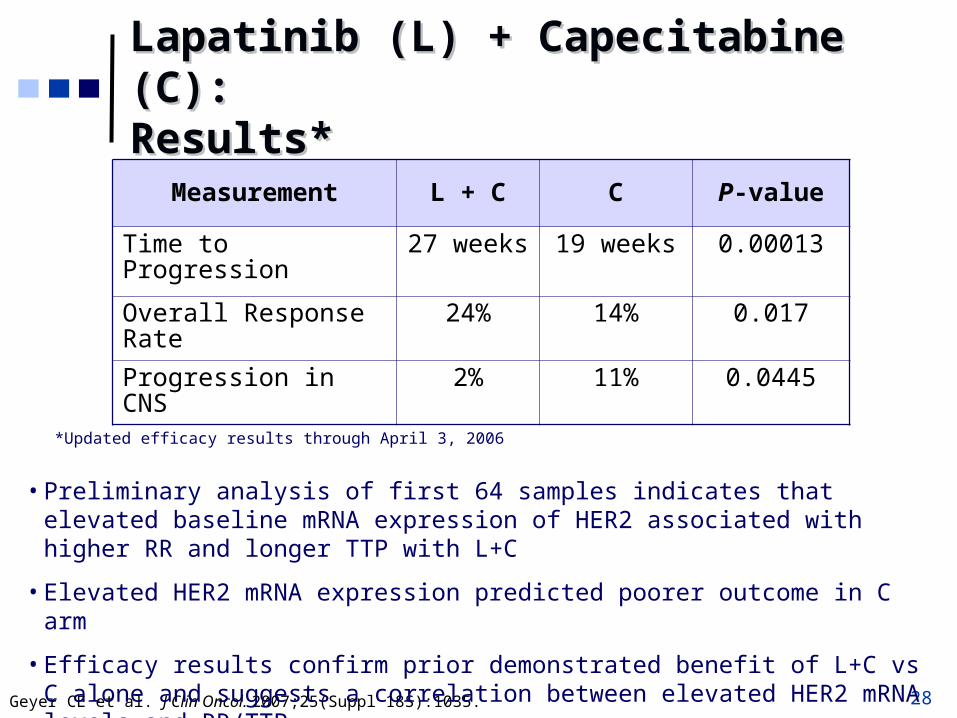
Lapatinib (L) + Capecitabine (C):Lapatinib (L) + Capecitabine (C):Results*Results*
Measurement L + C C P-value
Time to Progression 27 weeks 19 weeks 0.00013
Overall Response Rate 24% 14% 0.017
Progression in CNS 2% 11% 0.0445
Geyer CE et al. J Clin Oncol. 2007;25(Suppl 18S):1035.
*Updated efficacy results through April 3, 2006
• Preliminary analysis of first 64 samples indicates that elevated baseline mRNA expression of HER2 associated with higher RR and longer TTP with L+C
• Elevated HER2 mRNA expression predicted poorer outcome in C arm
• Efficacy results confirm prior demonstrated benefit of L+C vs C alone and suggests a correlation between elevated HER2 mRNA levels and RR/TTP

29
Lapatinib (L) + Capecitabine (C):Lapatinib (L) + Capecitabine (C):Safety ResultsSafety Results
Adverse EventL + C
(no. of patients)C
(no. of patients)Grade 3 Grade 4 Grade 3 Grade 4
Diarrhea 13 1 10 0
PPE 12 0 14 0
Nausea 2 0 2 0
Vomiting 2 0 2 0
Fatigue 2 0 1 1
Rash 2 0 1 0PPE=palmar-plantar erythrodysesthesia
Most Frequent Grade 3/4 Adverse Events
Geyer CE et al. J Clin Oncol. 2007;25(Suppl 18S):1035.
30
Lapatinib (L) + Paclitaxel (P):Lapatinib (L) + Paclitaxel (P):Study DesignStudy Design
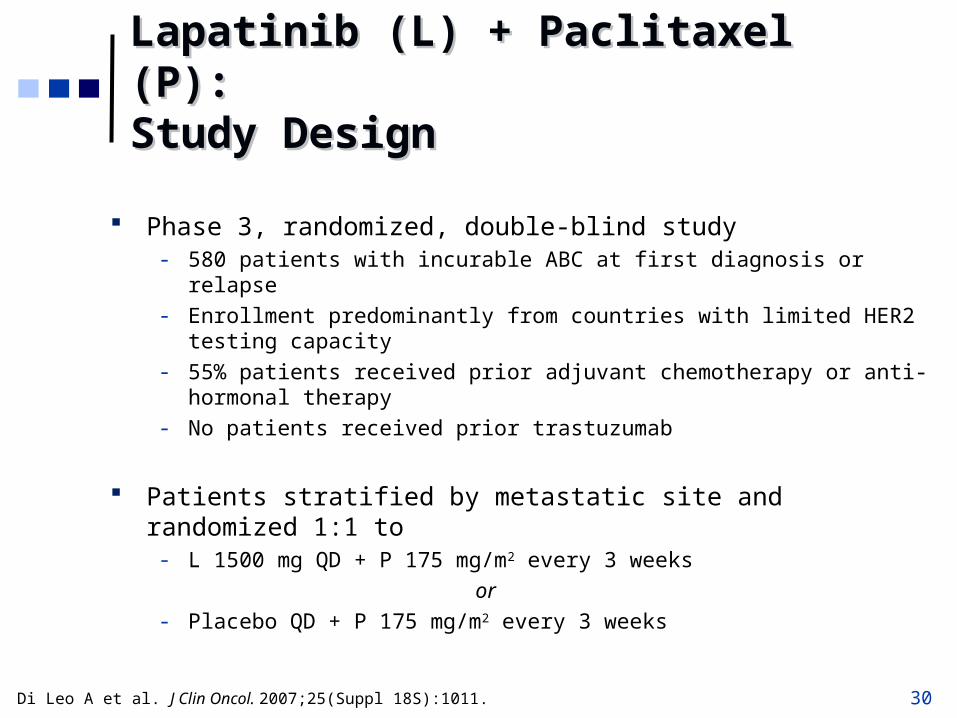
Phase 3, randomized, double-blind study- 580 patients with incurable ABC at first diagnosis or relapse- Enrollment predominantly from countries with limited HER2 testing capacity- 55% patients received prior adjuvant chemotherapy or anti-hormonal therapy- No patients received prior trastuzumab
Patients stratified by metastatic site and randomized 1:1 to- L 1500 mg QD + P 175 mg/m2 every 3 weeks
or- Placebo QD + P 175 mg/m2 every 3 weeks
Di Leo A et al. J Clin Oncol. 2007;25(Suppl 18S):1011.

31
Lapatinib (L) + Paclitaxel (P):Lapatinib (L) + Paclitaxel (P):Efficacy ResultsEfficacy Results
579 patients analyzed; 87% presented with Stage IV BC
At time of analysis, 561 patients (97%) progressed or otherwise withdrew
Median TTP 25 weeks
ORR 30%
Blinded analyses of HER2, ER, and PR are ongoing- Final biomarker evaluations will be presented with unblinded
efficacy data
Di Leo A et al. J Clin Oncol. 2007;25(Suppl 18S):1011.
32
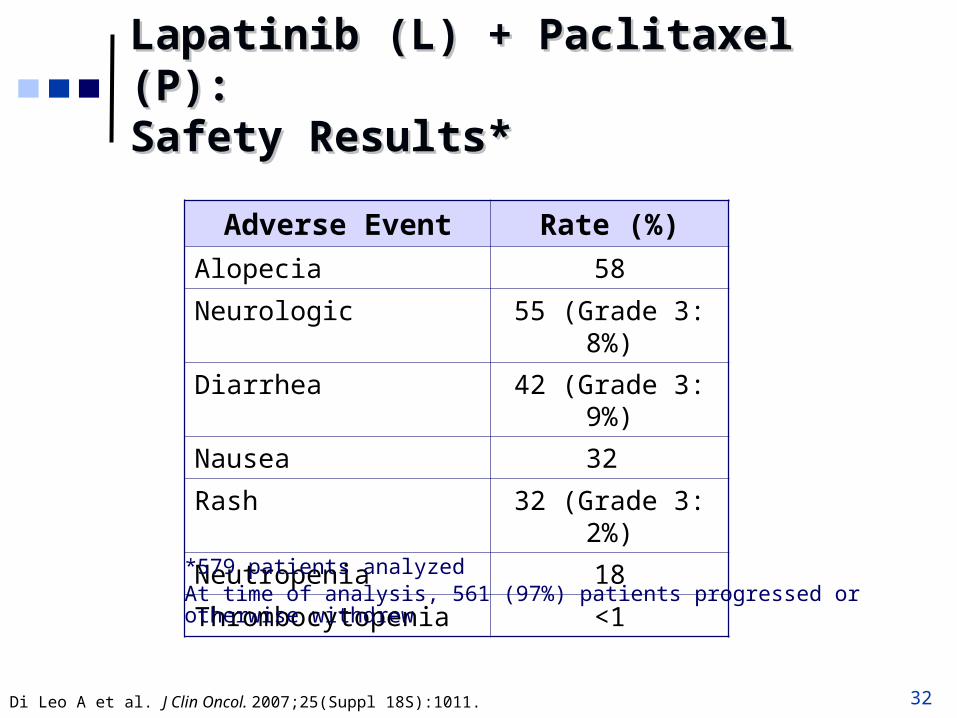
Lapatinib (L) + Paclitaxel (P):Lapatinib (L) + Paclitaxel (P):Safety Results*Safety Results*
Adverse Event Rate (%)
Alopecia 58
Neurologic 55 (Grade 3: 8%)
Diarrhea 42 (Grade 3: 9%)
Nausea 32
Rash 32 (Grade 3: 2%)
Neutropenia 18
Thrombocytopenia <1
*579 patients analyzedAt time of analysis, 561 (97%) patients progressed or otherwise withdrew
Di Leo A et al. J Clin Oncol. 2007;25(Suppl 18S):1011.

33
Cytotoxic and Targeted TherapyCytotoxic and Targeted Therapy Monoclonal Antibodies

34
Pertuzumab (P) and Trastuzumab (T): Pertuzumab (P) and Trastuzumab (T): BackgroundBackground
P and T are monoclonal antibodies that target different epitopes of HER receptor- P is first of a new class of HER2 inhibitors (HER dimerization
inhibitors) that binds to dimerization domain of HER2 receptor1
- T binds to extracellular domain of HER2 receptor and blocks intracellular signalling1
Preclinical models support hypothesis that complementary mechanisms of action for P and T could result in augmented efficacy when these agents are used in combination2
1. Bianco AR. J Chemother. 2004;16(Suppl 4):52-54.2. Arpino G et al. J Natl Cancer Inst. 2007;99:694-705.

35
Pertuzumab (P) + Trastuzumab (T):Pertuzumab (P) + Trastuzumab (T):Study DesignStudy Design
2-phase study - Recruitment into stage 1 complete; recruitment into stage 2 in
progress- Criteria to proceed to stage 2
2 partial responses or 1 partial response and 12 stable diseases or 13 stable diseases
Inclusion criteria- 24 patients with measurable, centrally-tested HER2+ breast
cancer- Up to 3 lines of prior chemotherapy plus T- Disease progression during T therapy - Baseline left ventricular ejection fraction (LVEF) 55% and no
decrease of LVEF below 50% during prior T therapy
Baselga J et al. J Clin Oncol. 2007;25(Suppl 18S):1004.

36
Pertuzumab (P) + Trastuzumab (T):Pertuzumab (P) + Trastuzumab (T):Study Design (cont.)Study Design (cont.)
Dosing- T 2 mg/kg IV weekly or 6 mg/kg IV q3 weeks (with reloading
dose if required) plus P 420 mg IV q3 weeks following loading dose of 840 mg
Baselga J et al. J Clin Oncol. 2007;25(Suppl 18S):1004.

37
Pertuzumab (P) + Trastuzumab (T):Pertuzumab (P) + Trastuzumab (T):ResultsResults
Response status- 5 confirmed partial responses (21%)- 12 stable disease (50%)
Adverse events (AEs)- Most mild to moderate and none treatment limiting- Main AEs
Diarrhea (71%) Fatigue (46%) Nausea/vomiting (38%) Rash (25%)
- No clinical cardiac events; no cases of LVEF decrease 10% and to ≤50%
Baselga J et al. J Clin Oncol. 2007;25(Suppl 18S):1004.

38
Bevacizumab (B) + Trastuzumab (T):Bevacizumab (B) + Trastuzumab (T):Study DesignStudy Design
To assess pathologic complete response (pCR) in patients with doxorubicin/cyclophosphamide (A/C)-resistant and AC-sensitive inflammatory BC
106 patients with Stage II-IV BC on neoadjuvant studies - Treated with either 2 or 4 cycles of dose-dense A/C
neoadjuvant chemotherapy (2 cycles if AC-resistant; 4 cycles if AC-sensitive) If HER2-, with or without B If HER2+, with T
Mehta RS et al. J Clin Oncol. 2007;25(Suppl 18S);591.

39
Bevacizumab (B) + Trastuzumab (T):Bevacizumab (B) + Trastuzumab (T):ResultsResults
Characteristic HER2+
(%)
HER2-
(%)
P-value
AC-resistant 65 16 0.0017
AC-sensitive 79 32 0.007
Pathologic Complete Response Rates in BC Subsets
• 38 of 85 (45%) accessable tumors had pathologic complete response • 56 of 84 (67%) tumors were reduced to ≤5 mm
Mehta RS et al. J Clin Oncol. 2007;25(Suppl 18S);591.
40
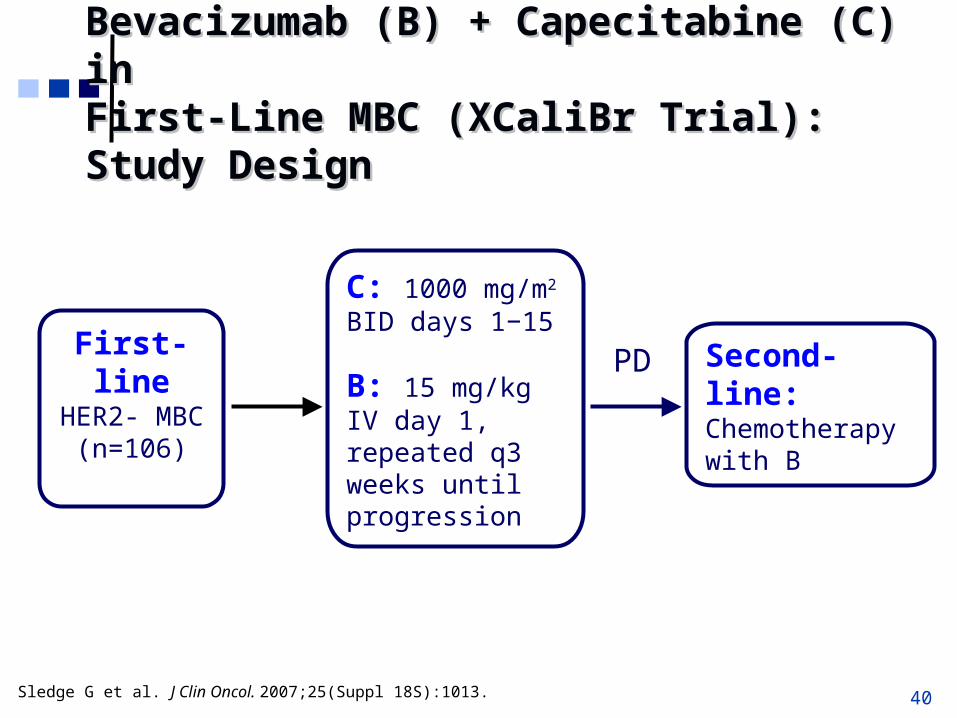
Bevacizumab (B) + Capecitabine (C) in Bevacizumab (B) + Capecitabine (C) in First-Line MBC (XCaliBr Trial):First-Line MBC (XCaliBr Trial):Study DesignStudy Design
First-line HER2- MBC
(n=106)
C: 1000 mg/m2
BID days 1−15
B: 15 mg/kg IV day 1, repeated q3 weeks until progression
Second-line:Chemotherapy with B
PD
Sledge G et al. J Clin Oncol. 2007;25(Suppl 18S):1013.

41
Bevacizumab (B) + Capecitabine (C):Bevacizumab (B) + Capecitabine (C):Efficacy ResultsEfficacy Results
Sledge G et al. J Clin Oncol. 2007;25(Suppl 18S):1013.
ITT
(n=106)
ER+
(n=57)
ER-
(n=49)
Overall Response Rate
38% 47% 27%
Median Time To Progression
5.7 months 8.9 months 4.0 months
95% CI: 4.9−8.4
95% CI: 7.5−13.6
95% CI: 3.0−4.9
Median Overall Survival
16.0+ months 16.6+ months 7.5 months
95% CI: 12.9−NR
95% CI: 15.1−NR
95% CI: 5.6−16
• Primary TTP endpoint was met (extension from 4 to > 5.6 months)• Combination of C + B was tolerable• Combination appears to be more active in ER+ patients
42
Bevacizumab (B) + Capecitabine (C):Bevacizumab (B) + Capecitabine (C):11
Safety ResultsSafety Results
Lower incidence of adverse events compared with previous study2
- 1250 mg/m2 bid dose used
Most common adverse events:- Diarrhea- Stomatitis- HFS- DVT- PE
22 non–drug-related deaths
2 drug-related deaths (cerebral hemorrhage, sepsis)
1. Sledge G et al. J Clin Oncol. 2007;25(Suppl 18S):1013. 2. Miller KD et al. J Clin Oncol. 2005;23:792-799.
43
Bevacizumab (B) + Albumin-bound Bevacizumab (B) + Albumin-bound (nab) Paclitaxel: Study Design(nab) Paclitaxel: Study Design
Retrospective analysis of patient records (March 2005 to December 2006) to obtain patients treated consecutively with:
- nab-paclitaxel 80−125 mg/m2 days 1, 8, 15 or 170−200 mg/m2 every 14 days on a 28-day cycle
+- B 10 mg/kg every 14 days
40 patients identified- All patients had received minimum of 3 prior chemotherapy regimens
(including anthracyclines 34/40 and taxanes 35/40)
Patients monitored for response using RECIST criteria on PE and PET/CT imaging
Link JS et al. J Clin Oncol. 2007;25(Suppl 18S):1101.
44
Bevacizumab (B) + (nab) Paclitaxel: Bevacizumab (B) + (nab) Paclitaxel: ResultsResults
Response rates- 20 women (50%) had objective responses to B/nab-paclitaxel.
3 complete responses 17 partial responses
- 7 women had stable disease for average duration of >200 days.- Objective response rate + stable disease = 67%
Mean time to progression = 132 days
Regimen well tolerated with acceptable toxicity.- Fatigue, neuropathy, anemia, hypertension most common AEs.- 2 patients discontinued because of CNS hemorrhage into metastatic brain
lesion.
Link JS et al. J Clin Oncol. 2007;25(Suppl 18S):1101.
45
New CoupletsNew Coupletsin Advanced Breast Cancerin Advanced Breast Cancer

46
Gemcitabine (G) + Paclitaxel (P) or Gemcitabine (G) + Paclitaxel (P) or Docetaxel (D) in First- or Second-Line MBC:Docetaxel (D) in First- or Second-Line MBC:11
Study DesignStudy Design
Combination of G + P2 and combination of G + D3 have shown efficacy in treatment of MBC
50 patients with locally advanced or MBC randomized to - G 1250 mg/m2 IV Days 1 and 8 + P 175 mg/m2 IV Day 1 (n=25)
or- G 1000 mg/m2 IV Days 1 and 8 + D 75 mg/m2 IV Day 1 (n=25)
Primary outcome measure- Tumor response using RECIST criteria
1. Boccia RV et al. J Clin Oncol. 2007;25(Suppl 18S):1046. 2. Delfino C et al. Oncology. 2004;66:18-23.3. O’Shaunessey JA et al. Clin Breast Cancer. 2006;6:505-510.

47
Gemcitabine (G) + Paclitaxel (P) or Gemcitabine (G) + Paclitaxel (P) or Docetaxel (D): Efficacy ResultsDocetaxel (D): Efficacy Results
Efficacy
(evaluable patients)
Patients (%)
G+P
(n=23)
G+D
(n=25)
Overall Response Rate 10 (43%) 12 (48%)
Partial Response 10 (43%) 10 (40%)
Complete Response 0 2 (8%)
Stable Disease 6 (26%) 5 (20%)
Clinical Benefit Rate 16 (70%) 17 (68%)
Boccia RV et al. J Clin Oncol. 2007;25(Suppl 18S):1046.
48
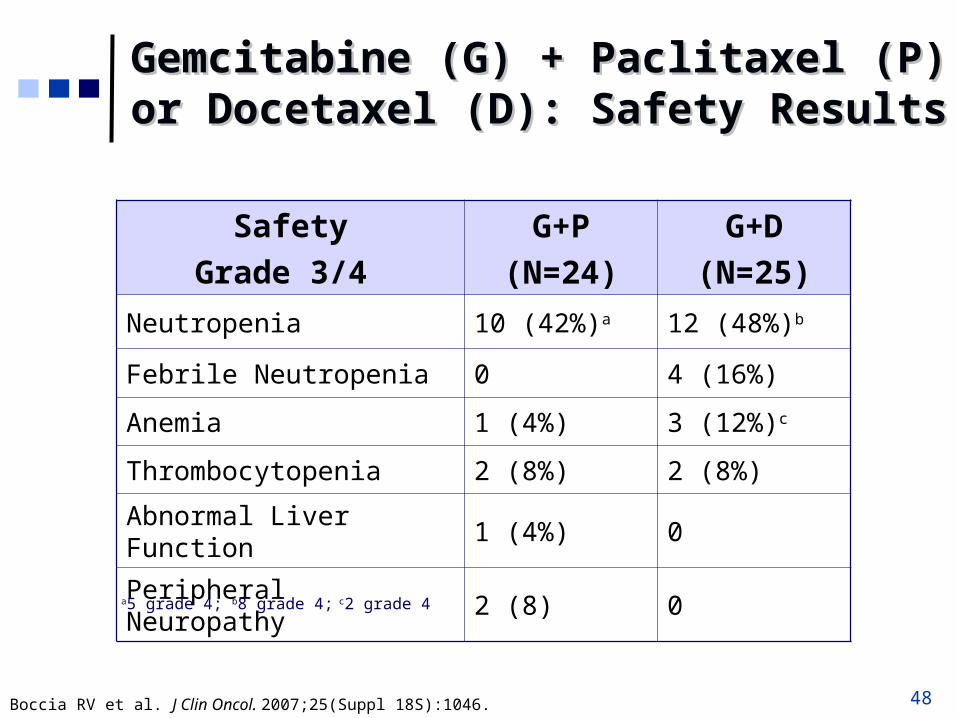
Gemcitabine (G) + Paclitaxel (P) or Gemcitabine (G) + Paclitaxel (P) or Docetaxel (D): Safety ResultsDocetaxel (D): Safety Results
Safety
Grade 3/4
G+P
(N=24)
G+D
(N=25)
Neutropenia 10 (42%)a 12 (48%)b
Febrile Neutropenia 0 4 (16%)
Anemia 1 (4%) 3 (12%)c
Thrombocytopenia 2 (8%) 2 (8%)
Abnormal Liver Function 1 (4%) 0
Peripheral Neuropathy 2 (8) 0a5 grade 4; b8 grade 4; c2 grade 4
Boccia RV et al. J Clin Oncol. 2007;25(Suppl 18S):1046.
49
Course SummaryCourse Summary
CTCs now show more evidence as predictive markers in MBC and could be used more often
SLN is the superior and less invasive surgical method in lymph node-negative BC patients
New chemotherapeutic agents and treatment regimens are emerging, and a few of these will soon be available to our patients
New biologic agents (eg, small molecules and monoclonal antibodies) show promising activity and add good efficacy in combinations with other agents, with relative modest toxicity