1 myocardial and pericardial disease j.b handler, m.d. physician assistant program university of new...
TRANSCRIPT

1
Myocardial and Pericardial DiseaseMyocardial and Pericardial Disease
J.B Handler, M.D.J.B Handler, M.D.
Physician Assistant Program Physician Assistant Program
University of New EnglandUniversity of New England
2
AbbreviationsAbbreviations LV/RV- left ventricle/right ventricleLV/RV- left ventricle/right ventricle EF- ejection fractionEF- ejection fraction IVCD-intraventricular conduction delayIVCD-intraventricular conduction delay MR- mitral regurgitationMR- mitral regurgitation LVOT- left ventricular outflow tractLVOT- left ventricular outflow tract SAM- systolic anterior motionSAM- systolic anterior motion IVS- interventricular septumIVS- interventricular septum DHP- dihydropyridineDHP- dihydropyridine Rx- treatmentRx- treatment Bx- biopsyBx- biopsy FH- family historyFH- family history HJR- hepato-jugular refluxHJR- hepato-jugular reflux MVOMVO22- myocardial oxygen consumption- myocardial oxygen consumption OP- out patientOP- out patient
Nl- normalNl- normal LSB- left sternal borderLSB- left sternal border PND- paroxysmal nocturnal dyspneaPND- paroxysmal nocturnal dyspnea JVD- jugular venous distentionJVD- jugular venous distention RA- rheumatoid arthritisRA- rheumatoid arthritis SLE- systemic lupus erythematosisSLE- systemic lupus erythematosis Dx- diagnosisDx- diagnosis ARB’s- angiotensin receptor blockersARB’s- angiotensin receptor blockers ICD- inplantable cardioverter-ICD- inplantable cardioverter-
defibrillatordefibrillator HF- heart failureHF- heart failure HF=CHF- congestive heart failureHF=CHF- congestive heart failure CHD- coronary heart diseaseCHD- coronary heart disease ASH- asymmetric septal hypertrophyASH- asymmetric septal hypertrophy

3
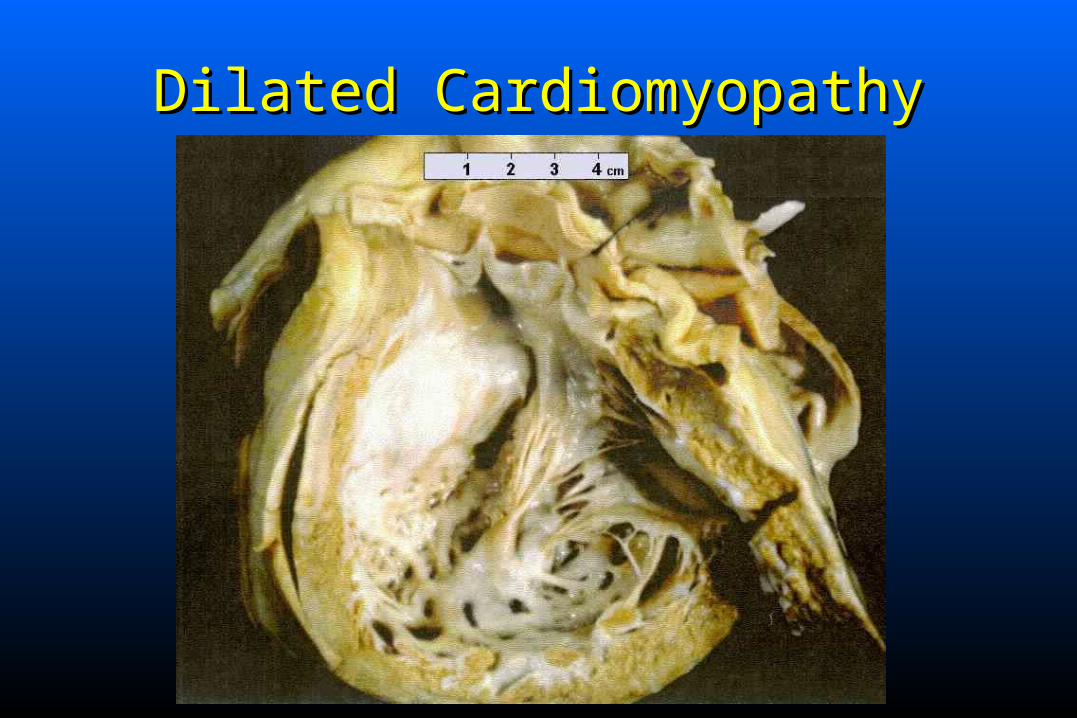
Dilated CardiomyopathyDilated Cardiomyopathy
PrimaryPrimary: : idiopathicidiopathic - unknown cause - unknown cause Secondary: Secondary:
– Toxic - alcohol, adriamycin, etc. Toxic - alcohol, adriamycin, etc. – Post-partumPost-partum– Post infectious - myocarditisPost infectious - myocarditis– Endocrine: hypothyroidism, pheochromocytoma, Endocrine: hypothyroidism, pheochromocytoma,
acromegaly and hyperthyroidismacromegaly and hyperthyroidism– ““Ischemic Cardiomyopathy”- Ischemic Cardiomyopathy”- avoidavoid this terminology this terminology

4
Clinical FeaturesClinical Features
Patients present with signs and symptoms of HF Patients present with signs and symptoms of HF which usually develops slowly.which usually develops slowly.
Left or biventricular failureLeft or biventricular failure Left sided: DOE, orthopnea, PND, weakness, Left sided: DOE, orthopnea, PND, weakness,
fatigue, peripheral edema, etc.fatigue, peripheral edema, etc. Right sided: unexplained weight gain, peripheral Right sided: unexplained weight gain, peripheral
edema, abdominal fullness (hepatomegaly, edema, abdominal fullness (hepatomegaly, ascites).ascites).
Dilated CardiomyopathyDilated Cardiomyopathy

6
Physical ExamPhysical Exam
Cardiomegaly (PMI displaced laterally), low Cardiomegaly (PMI displaced laterally), low pulse amplitude (pulsus alternans when severe), pulse amplitude (pulsus alternans when severe), often with often with BP, pulmonary congestion, crackles, BP, pulmonary congestion, crackles, SS33 gallop, MR murmur. gallop, MR murmur.
Elevated JVP, hepatomegaly, HJR, pitting edema, Elevated JVP, hepatomegaly, HJR, pitting edema, TR murmur.TR murmur.
7
Diagnostic StudiesDiagnostic Studies CxR: Cardiomegaly, pulmonary congestion, CxR: Cardiomegaly, pulmonary congestion,
pleural effusions.pleural effusions. Echocardiography/Doppler: LV/RV dilation, Echocardiography/Doppler: LV/RV dilation,
global LV dysfunctionglobal LV dysfunction with with reduced EF;reduced EF; Mitral Mitral regurgitation common.regurgitation common.
EKG- NSST-T changes, IVCD (wide QRS), EKG- NSST-T changes, IVCD (wide QRS), PVC’s.PVC’s.
Cardiac Cath: only when necessary to Cardiac Cath: only when necessary to exclude exclude alternative diagnosisalternative diagnosis i.e CHD; documents low i.e CHD; documents low EF, global dysfunction, high filling pressures.EF, global dysfunction, high filling pressures.
8
TreatmentTreatment
Management for HFManagement for HF:: Afterload reduction: ACEI or alternatives (ARB’s)Afterload reduction: ACEI or alternatives (ARB’s) Preload reduction: Diuretics, nitratesPreload reduction: Diuretics, nitrates Beta BlockersBeta Blockers SpironlolactoneSpironlolactone Digoxin Digoxin ICD’s if indicated, +/- antiarrhythmicsICD’s if indicated, +/- antiarrhythmics Anticoagulation unless contraindicatedAnticoagulation unless contraindicated

9
Clinical Course and PrognosisClinical Course and Prognosis
Dependent on length of Sx and functional class. If Dependent on length of Sx and functional class. If onset recent, some recovery of ventricular onset recent, some recovery of ventricular function can occur.function can occur.
Class IV patients: 50% one year mortalityClass IV patients: 50% one year mortality Unpredictable course, often progressiveUnpredictable course, often progressive Only meds that may improve survival are Only meds that may improve survival are
ACEI (or ARB’s), ACEI (or ARB’s), ßß-Blockers and -Blockers and Spironolactone.Spironolactone.
Cardiac Transplantation: >70% 5yr. survivalCardiac Transplantation: >70% 5yr. survival
10
Hypertrophic CardiomyopathyHypertrophic Cardiomyopathy
Genetically transmitted in >50% of cases.Genetically transmitted in >50% of cases. Autosomal dominant with high penetrance.Autosomal dominant with high penetrance.
– Must perform echocardiography on all siblings and Must perform echocardiography on all siblings and offspring of a patient with HCM.offspring of a patient with HCM.
Remaining cases occur spontaneously; de novo Remaining cases occur spontaneously; de novo gene mutations common.gene mutations common.
Genetic counseling is essential.Genetic counseling is essential.

11
Pathophysiology of HCMPathophysiology of HCM
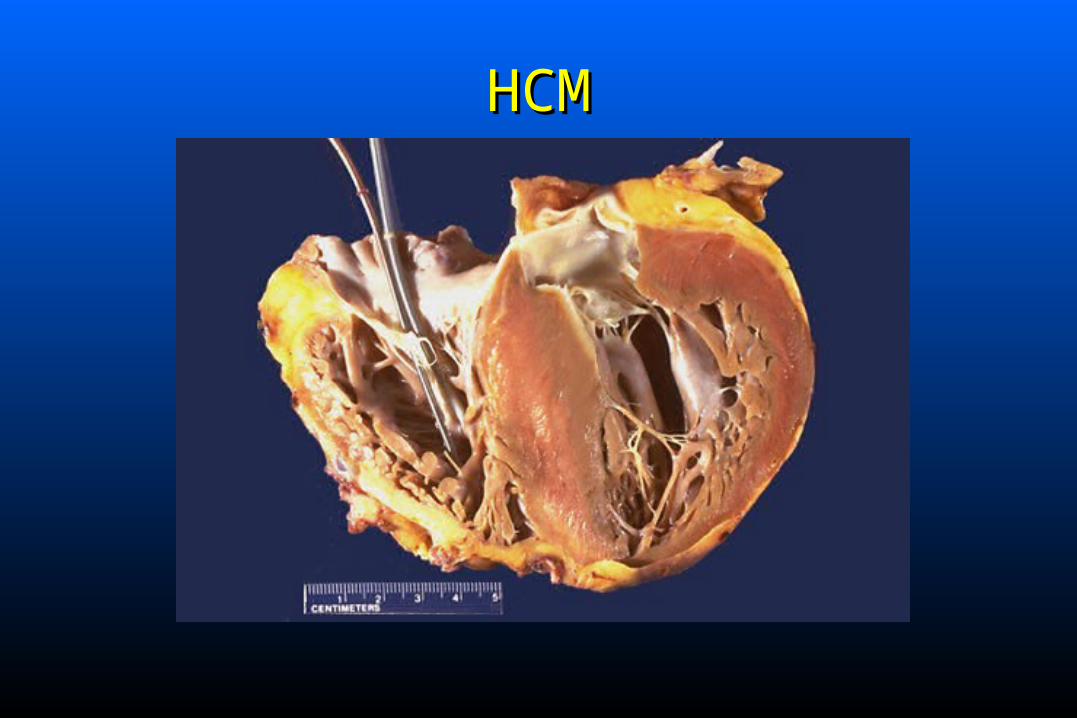
Marked increase in left ventricular mass, especially the Marked increase in left ventricular mass, especially the septum - marked hypertrophyseptum - marked hypertrophy; remaining LV segments ; remaining LV segments hypertrophied to a lesser degree; septal/posterior wall hypertrophied to a lesser degree; septal/posterior wall thickness > 1.5/1 “ASH”. Hypertrophy is unrelated to thickness > 1.5/1 “ASH”. Hypertrophy is unrelated to pressure overload; often present at birth, progessively pressure overload; often present at birth, progessively worsens during childhood.worsens during childhood.
LV cavity small, systolic function normal or LV cavity small, systolic function normal or hyperdynamic early on.hyperdynamic early on.
Diastolic dysfunctionDiastolic dysfunction common common Obstructive and non-obstructive formsObstructive and non-obstructive forms
HCMHCM
13
When present LVOT obstruction is When present LVOT obstruction is dynamicdynamic and and varies with activity/rest, and LV volume.varies with activity/rest, and LV volume.– Obstruction: MV moves abnormally towards the IVS, Obstruction: MV moves abnormally towards the IVS,
obstructing the LVOT.obstructing the LVOT. Pathology: myocardial fiber hypertrophy and Pathology: myocardial fiber hypertrophy and
disarray, primarily in IVS.disarray, primarily in IVS. Mitral valve often thickened and moves Mitral valve often thickened and moves
abnormally as noted above, well seen on abnormally as noted above, well seen on echocardiogram.echocardiogram.

14
Clinical ManifestationsClinical Manifestations
Often asymptomatic in childhood; may be detected via Often asymptomatic in childhood; may be detected via ultrasound in the offspring of patients with known ultrasound in the offspring of patients with known disease.disease.
Symptoms: dyspnea, chest pain and syncope are most Symptoms: dyspnea, chest pain and syncope are most common. In some, sudden death may be presenting common. In some, sudden death may be presenting symptom. One of few causes of symptom. One of few causes of sudden death in young sudden death in young athletes.athletes.
Sudden deathSudden death often occurs during strenuous activity. often occurs during strenuous activity. Arrhythmias are common: ventricular and Arrhythmias are common: ventricular and
supraventricular; supraventricular; Afib may lead to sudden Afib may lead to sudden decompensation and is a bad prognostic signdecompensation and is a bad prognostic sign..
15
Physical ExamPhysical Exam
Pulse brisk, often. with bisferiens carotid pulse.Pulse brisk, often. with bisferiens carotid pulse. Double or triple apical impulse due to atrial Double or triple apical impulse due to atrial
filling wave and early and late systolic impulses.filling wave and early and late systolic impulses. Loud SLoud S44 and S and S33 gallops. gallops.
Loud harsh Loud harsh aortic outflow murmur aortic outflow murmur (creshendo-(creshendo-decreshendo) best heard along left sternal borderdecreshendo) best heard along left sternal border with characteristic features with characteristic features (see below); MR (see below); MR common.common.

16
Effects of Maneuvers on MurmurEffects of Maneuvers on Murmur
Most cardiac murmurs are increased by squatting Most cardiac murmurs are increased by squatting and decreased by standing or with valsalva.and decreased by standing or with valsalva.
The murmur of HCM is The murmur of HCM is increased increased with with standing & valsalvastanding & valsalva and decreased with and decreased with squatting. This is the opposite of how the squatting. This is the opposite of how the murmur of aortic stenosis acts. Other things that murmur of aortic stenosis acts. Other things that the murmur include hypovolemia, tachycardia the murmur include hypovolemia, tachycardia or increases in cardiac contractility (inotropes, or increases in cardiac contractility (inotropes, exercise). exercise).

17
Diagnostic StudiesDiagnostic Studies
ECG- LVH with secondary ST-T changes ECG- LVH with secondary ST-T changes common. Septal Q waves may mimic MI.common. Septal Q waves may mimic MI.
Echocardiogram/Doppler diagnosticEchocardiogram/Doppler diagnostic CxR often unimpressive.CxR often unimpressive.
18
HCM: ManagementHCM: Management
Essential to minimize strenuous physical exertion.Essential to minimize strenuous physical exertion. Beta BlockersBeta Blockers: slow HR, : slow HR, ’s diastolic filling ’s diastolic filling
time, time, ’s MVO’s MVO22 with additional anti-arrhythmic with additional anti-arrhythmic
effects:effects:– Angina, dyspnea and presyncope may all improve. Angina, dyspnea and presyncope may all improve.
Beta blockers also may prevent the increase in Beta blockers also may prevent the increase in outflow obstruction that occurs with exercise. outflow obstruction that occurs with exercise. Large doses of Large doses of ßß-blockers well tolerated.-blockers well tolerated.

19
Calcium channel antagonistsCalcium channel antagonists ( (verapamilverapamil)- used )- used withwith (or as an alternative) to (or as an alternative) to ßß-blockers.-blockers.– Only time when verapamil Only time when verapamil addedadded to to ßß-blocker-blocker
Improve diastolic filling and compliance via Improve diastolic filling and compliance via negative inotropic and chronotropic effects negative inotropic and chronotropic effects decrease LVEDP. decrease LVEDP. – Symptomatic improvement and improved exercise Symptomatic improvement and improved exercise
tolerance in over 2/3 of treated patients.tolerance in over 2/3 of treated patients.
VerapamilVerapamil in high dosage is well tolerated. in high dosage is well tolerated. Don’t use DHP Ca blockersDon’t use DHP Ca blockers can worsen Sx. can worsen Sx.
HCM: ManagementHCM: Management
20
HCM: Interventional TherapyHCM: Interventional Therapy
Surgery or procedures to reduce septal muscle: Surgery or procedures to reduce septal muscle: myomectomy, alcohol ablation: severe myomectomy, alcohol ablation: severe obstruction or symptoms.obstruction or symptoms.
Dual chamber pacemaker may improve septal Dual chamber pacemaker may improve septal motion and decrease progression of obstruction if motion and decrease progression of obstruction if severe.severe.
ICD: high risk patients (documented v-tach, ICD: high risk patients (documented v-tach, aborted sudden death) or FH of sudden death.aborted sudden death) or FH of sudden death.

21
Restrictive and Infiltrative Restrictive and Infiltrative CardiomyopathiesCardiomyopathies
Hallmark: Hallmark: Abnormal diastolic function.Abnormal diastolic function. Ventricular walls excessively rigid and impede Ventricular walls excessively rigid and impede
diastolic filling; systolic function may be normal diastolic filling; systolic function may be normal or reduced.or reduced.
Pathophysiology resembles constrictive Pathophysiology resembles constrictive pericarditis.pericarditis.
Least commonly seen of the cardiomyopathies.Least commonly seen of the cardiomyopathies.

22
Restrictive Cardiomyopathy: Restrictive Cardiomyopathy: FindingsFindings
Jugular venous distentionJugular venous distention SS33 and/or S and/or S44
Inspiratory increase in venous pressure Inspiratory increase in venous pressure (Kussmaul’s sign)(Kussmaul’s sign)
Findings of Rt. Heart Failure may predominate Findings of Rt. Heart Failure may predominate i.e. edema, hepatomegaly.i.e. edema, hepatomegaly.
Symptoms include dyspnea, exercise intolerance Symptoms include dyspnea, exercise intolerance and fatigue.and fatigue.

23
RestrictiveRestrictiveCardiomyopathyCardiomyopathy
Echo-doppler findings include: LV wall Echo-doppler findings include: LV wall thickening; decreased diastolic relaxation.thickening; decreased diastolic relaxation.
Systolic function-preserved or diminishedSystolic function-preserved or diminished Disease process may have characteristic echo Disease process may have characteristic echo
findings i.e. amyloidosis.findings i.e. amyloidosis. Tricuspid and mitral regurgitation are common.Tricuspid and mitral regurgitation are common.
24
Natural HistoryNatural History
Relentless symptomatic progression; >90% dead Relentless symptomatic progression; >90% dead at 10 years.at 10 years.
No specific treatment other than symptomatic.No specific treatment other than symptomatic. Calcium Channel Antagonists may improve Calcium Channel Antagonists may improve
diastolic function in selected individuals.diastolic function in selected individuals.

25
EtiologiesEtiologies
AmyloidosisAmyloidosis HemochromatosisHemochromatosis Fabry DiseaseFabry Disease Gaucher DiseaseGaucher Disease Endomyocardial Fibrosis-Loeffler Endocarditis-Endomyocardial Fibrosis-Loeffler Endocarditis-
hypereosinofilia syndromehypereosinofilia syndrome

26
MyocarditisMyocarditis
A primary inflammatory process of the A primary inflammatory process of the myocardium, most often caused by an myocardium, most often caused by an infectious agent.infectious agent.
Unrecognized myocarditis may be the initial Unrecognized myocarditis may be the initial event culminating in an “idiopathic dilated event culminating in an “idiopathic dilated cardiomyopathy”.cardiomyopathy”.
27
Infectious MyocarditisInfectious Myocarditis
Viral - most commonViral - most common Bacterial- numerousBacterial- numerous Fungal-aspergillosis, candidiasis, etc.Fungal-aspergillosis, candidiasis, etc. Parasitic – Trypanosoma cruzi (Chagas’)Parasitic – Trypanosoma cruzi (Chagas’) RickettsialRickettsial SpirochetalSpirochetal

28
Viral Myocarditis and PericarditisViral Myocarditis and Pericarditis
Coxsackievirus (B>A)Coxsackievirus (B>A) CMVCMV EchovirusEchovirus AdenovirusAdenovirus HIVHIV InfluenzaInfluenza Infectious mononucleosisInfectious mononucleosis Rubella, RubeolaRubella, Rubeola

29
Clinical ManifestationsClinical Manifestations
May be asymptomaticMay be asymptomatic Prodromal viral syndromeProdromal viral syndrome followed followed
symptoms of symptoms of myopericarditismyopericarditis..– Chest pain, fatigue, dyspnea, palpitations are Chest pain, fatigue, dyspnea, palpitations are
common initial symptoms. Often progresses to common initial symptoms. Often progresses to HF.HF.
Initial presentation may be HFInitial presentation may be HF.. Exam : Tachycardia, elevated temp, Exam : Tachycardia, elevated temp,
muffled heart sounds; signs of HF in severe muffled heart sounds; signs of HF in severe cases.cases.

30
ECG: sinus tachycardia with NSST-T changes. ECG: sinus tachycardia with NSST-T changes. Other findings: ST elevation consistent with Other findings: ST elevation consistent with pericarditis may occur.pericarditis may occur.
CXR: heart size normal or enlarged; pulmonary CXR: heart size normal or enlarged; pulmonary congestion may be present.congestion may be present.
Echo-doppler: some degree of LV dysfunction Echo-doppler: some degree of LV dysfunction (regional or global); LV size normal or increased, (regional or global); LV size normal or increased, wall thickness usually normal. Thrombus may be wall thickness usually normal. Thrombus may be present with severe dysfunction.present with severe dysfunction.
31
DiagnosisDiagnosis
Difficult to confirm acute diagnosisDifficult to confirm acute diagnosis Acute and convalescent viral titers; presence of Acute and convalescent viral titers; presence of
virus in other tissues.virus in other tissues. Troponin levels or CK-MB isoenzyme are often Troponin levels or CK-MB isoenzyme are often
normal but may be mildly elevated.normal but may be mildly elevated. Endomyocardial biopsy may isolate virus (rare), Endomyocardial biopsy may isolate virus (rare),
or show characteristic pathology of myositis-or show characteristic pathology of myositis-inflammatory infiltrate.inflammatory infiltrate.
32
TreatmentTreatment
Supportive RxSupportive Rx Rx HF if present. Important to limit activity.Rx HF if present. Important to limit activity. Specific anti microbial Rx if an infecting agent is Specific anti microbial Rx if an infecting agent is
identified (if treatable).identified (if treatable). Biopsy guided immunosuppressive and Biopsy guided immunosuppressive and
corticosteroid Rx is available under investigative corticosteroid Rx is available under investigative protocols - no proven benefit.protocols - no proven benefit.
Avoid NSAIDs: may increase myocardial damage.Avoid NSAIDs: may increase myocardial damage. Prognosis variable: Ranges from death to varying Prognosis variable: Ranges from death to varying
degrees of recoverydegrees of recovery

33
Acute PericarditisAcute Pericarditis
A syndrome due to inflammation of the A syndrome due to inflammation of the pericardium characterized by chest pain, a pericardium characterized by chest pain, a pericardial friction rub, and serial ECG pericardial friction rub, and serial ECG abnormalities.abnormalities.
34
Causes of PericarditisCauses of Pericarditis
Viral most commonViral most common;; same spectrum of viruses as same spectrum of viruses as seen with myocarditis- Coxsackie most commonseen with myocarditis- Coxsackie most common..
Idiopathic (non specific)Idiopathic (non specific) TuberculosisTuberculosis Acute bacterial infectionsAcute bacterial infections FungalFungal UremiaUremia-untreated or with dialysis.-untreated or with dialysis. RadiationRadiation Autoimmune-RA, SLE, scleroderma, PANAutoimmune-RA, SLE, scleroderma, PAN

35
Drug induced: hydralazine, procainamide, Drug induced: hydralazine, procainamide, isoniazid, penicillin.isoniazid, penicillin.
Trauma: Chest trauma; post thoracotomy; Trauma: Chest trauma; post thoracotomy; pacemaker insertion; post cath., PTCA.pacemaker insertion; post cath., PTCA.
Early post MIEarly post MI Delayed post myocardial-pericardial injury Delayed post myocardial-pericardial injury
syndromes: late post MI (Dressler’s syndrome) or syndromes: late post MI (Dressler’s syndrome) or post heart surgery (postpericardotomy syndrome).post heart surgery (postpericardotomy syndrome).
Neoplastic diseaseNeoplastic disease- lung cancer, breast cancer, - lung cancer, breast cancer, lymphoma, Hodgkins disease, leukemia.lymphoma, Hodgkins disease, leukemia.

36
Clinical ManifestationsClinical Manifestations Chest pain-frequent; quality and location variable; Chest pain-frequent; quality and location variable;
retrosternal and often left sided. retrosternal and often left sided. Pain is intense-Pain is intense-aggravated by lying supine, with inspiration, aggravated by lying supine, with inspiration, coughing, swallowing, laughing; improved coughing, swallowing, laughing; improved sitting up, leaning forward, shallow inspiration.sitting up, leaning forward, shallow inspiration.
Chest pain may be felt with each heart beat.Chest pain may be felt with each heart beat. On occasion pain may be identical in quality to the On occasion pain may be identical in quality to the
pain of myocardial infarction.pain of myocardial infarction. Dyspnea may be related to shallow breathing from Dyspnea may be related to shallow breathing from
inspiratory chest pain.inspiratory chest pain.
37
Pericarditis: Physical ExamPericarditis: Physical Exam
Pericardial Friction Rub-Pericardial Friction Rub-pathognomonicpathognomonic--scratching, grating, high pitched soundscratching, grating, high pitched sound due to due to friction between the pericardium and epicardium.friction between the pericardium and epicardium.
3 components related to cardiac motion: pre-3 components related to cardiac motion: pre-systole (atrial contraction), ventricular systole systole (atrial contraction), ventricular systole (loudest component), and early diastole. Usually (loudest component), and early diastole. Usually hear 2 components (S/D).hear 2 components (S/D).
Rub is evanescent; best heard with diaphragm at Rub is evanescent; best heard with diaphragm at LLSB; best heard with patient sitting, leaning LLSB; best heard with patient sitting, leaning forward in full expiration.forward in full expiration.
38
Diagnostic FindingsDiagnostic Findings
ECG: Changes begin within hours of the onset of ECG: Changes begin within hours of the onset of pain; several stages.pain; several stages.
ECG abnormalities reflect inflammation involving ECG abnormalities reflect inflammation involving the pericardium and epicardium. Initially there is the pericardium and epicardium. Initially there is diffuse ST segment elevationdiffuse ST segment elevation in all leads except in all leads except aVR and V1. Later ECG’s show normalization of aVR and V1. Later ECG’s show normalization of ST elevation followed by T wave flattening and T ST elevation followed by T wave flattening and T wave inversion.wave inversion.
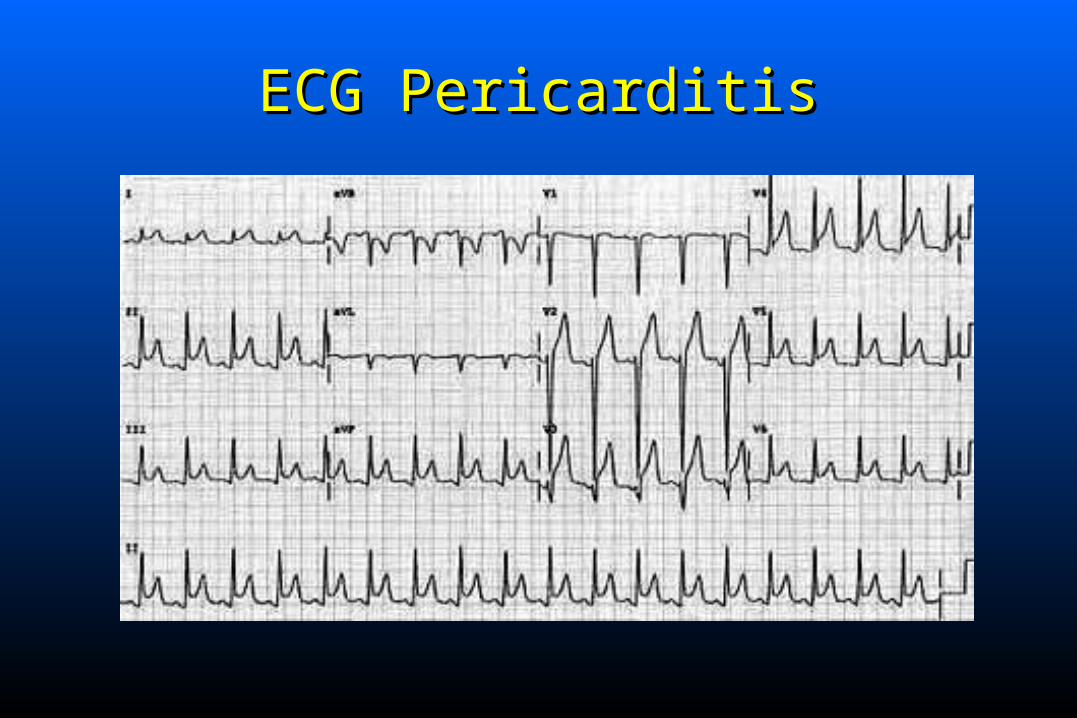
ECG PericarditisECG Pericarditis

40
Diagnostic Findings Cont....Diagnostic Findings Cont.... Early repolarization, a normal variant often seen in Early repolarization, a normal variant often seen in
young young healthyhealthy individuals (male> female) may individuals (male> female) may mimic the ECG findings seen in the acute phase of mimic the ECG findings seen in the acute phase of pericarditis, but less ST pericarditis, but less ST & seen in fewer leads. & seen in fewer leads.
Echo-doppler: nl LV size and function rules out Echo-doppler: nl LV size and function rules out myocarditis; a small myocarditis; a small pericardial effusionpericardial effusion may be may be seen; this rarely progresses with viral pericarditis, seen; this rarely progresses with viral pericarditis, but a repeat study to document resolution is but a repeat study to document resolution is indicated.indicated.
CXR: usually normal; occasionally cardiomegaly CXR: usually normal; occasionally cardiomegaly due to a pericardial effusion is seen.due to a pericardial effusion is seen.
41
ManagementManagement
Determine etiology where possible.Determine etiology where possible. Bed rest until pain and fever resolved.Bed rest until pain and fever resolved. Most patients Rx’d as OP. Hospitalization may be Most patients Rx’d as OP. Hospitalization may be
indicated if MI suspected or if large effusion present.indicated if MI suspected or if large effusion present. Pain rapidly responds to Pain rapidly responds to NSAIDsNSAIDs: Ibuprofen, high dose : Ibuprofen, high dose
ASA, etc; steroids rarely necessary.ASA, etc; steroids rarely necessary. Oral Oral anticoagulants should be avoided anticoagulants should be avoided in patients with in patients with
pericarditis.pericarditis. Symptoms usually resolve in 2-4 weeks.Symptoms usually resolve in 2-4 weeks.

42
Pericardial Effusion Without Cardiac Pericardial Effusion Without Cardiac CompressionCompression
Can occur with all forms of pericarditisCan occur with all forms of pericarditis Symptoms (if present) include chest pressure, Symptoms (if present) include chest pressure,
dyspnea, hiccups, nausea, abd. fullness, cough.dyspnea, hiccups, nausea, abd. fullness, cough. CxR-mild cardiomegaly if >250 cc. fluid.CxR-mild cardiomegaly if >250 cc. fluid. ECG: NSST-T changes; ECG: NSST-T changes; decreased QRS voltagedecreased QRS voltage.. Echo: Best technique to Dx. and follow; useful to Echo: Best technique to Dx. and follow; useful to
determine presence of determine presence of tamponadetamponade.. Management-depends on the presence or absence Management-depends on the presence or absence
of hemodynamic compromise, and the underlying of hemodynamic compromise, and the underlying disease process.disease process.

43
Pericardial Effusion With Pericardial Effusion With Compression: TamponadeCompression: Tamponade
Increasing pericardial fluid raises intrapericardial Increasing pericardial fluid raises intrapericardial pressure resulting in compression of the heart.pressure resulting in compression of the heart.
There is progressive limitation of ventricular There is progressive limitation of ventricular diastolic filling leading to reduction of stroke diastolic filling leading to reduction of stroke volume and cardiac output.volume and cardiac output.
Fatal if not recognized and aggressively treated.Fatal if not recognized and aggressively treated.

44
Cardiac TamponadeCardiac Tamponade Hemodynamics - marked elevation and Hemodynamics - marked elevation and
equilibration of LV and RV diastolic pressuresequilibration of LV and RV diastolic pressures; ; LA and RA pressures elevated.LA and RA pressures elevated.
Marked decrease in CO.Marked decrease in CO. RA and RV collapse is seen on echo.RA and RV collapse is seen on echo. Beck’s triadBeck’s triad: decline in arterial pressure, : decline in arterial pressure,
elevation of systemic venous pressure, quiet heart.elevation of systemic venous pressure, quiet heart. Cardiac output is extremely volume sensitive.Cardiac output is extremely volume sensitive.

45
Pulsus ParadoxusPulsus Paradoxus Normally during inspiration-increase venous Normally during inspiration-increase venous
return, slight increase in RV volume, IVS return, slight increase in RV volume, IVS displaced from rt to lt- slight decrease in LV displaced from rt to lt- slight decrease in LV volume. RV output increases, LV output volume. RV output increases, LV output slightly slightly fallsfalls- results in minimal (2-3%) drop in systolic - results in minimal (2-3%) drop in systolic BP (2-4mm).BP (2-4mm).
Pulsus paradoxus is a marked exaggerationPulsus paradoxus is a marked exaggeration of of this process; intrapericardial pressure is markedly this process; intrapericardial pressure is markedly increased-RV and LV volumes are already increased-RV and LV volumes are already diminished; inspiration results in a marked diminished; inspiration results in a marked in LV in LV volume resulting in a volume resulting in a systolic BP drop > 10mm.systolic BP drop > 10mm.

46
Cardiac TamponadeCardiac Tamponade
CxR and ECG are ancillary tests.CxR and ECG are ancillary tests. Echocardiogram is often diagnostic.Echocardiogram is often diagnostic. PericardiocentesisPericardiocentesis: may be life saving; IV fluids given : may be life saving; IV fluids given
to increase preload; should be done with Rt Ht Cath to to increase preload; should be done with Rt Ht Cath to optimize hemodynamics; subxiphoid approach with optimize hemodynamics; subxiphoid approach with flouroscopic guidance is successful in 95%; fluid is flouroscopic guidance is successful in 95%; fluid is cultured and sent for cytology and chemistry analysis.cultured and sent for cytology and chemistry analysis.
Surgery: Pericardectomy and pericardotomy are Surgery: Pericardectomy and pericardotomy are necessary in 25% for recurrent tamponade.necessary in 25% for recurrent tamponade.