1. hypertension 1998 kilander 780 6
DESCRIPTION
jurnalTRANSCRIPT

Lena Kilander, Håkan Nyman, Merike Boberg, Lennart Hansson and Hans LithellHypertension Is Related to Cognitive Impairment : A 20-Year Follow-up of 999 Men
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1998 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.31.3.780
1998;31:780-786Hypertension.
http://hyper.ahajournals.org/content/31/3/780World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on March 21, 2013http://hyper.ahajournals.org/Downloaded from

Hypertension Is Related to Cognitive ImpairmentA 20-Year Follow-up of 999 Men
Lena Kilander, Håkan Nyman, Merike Boberg, Lennart Hansson, Hans Lithell
Abstract—Recent findings of a linkage between high blood pressure (BP) and later development of dementia have given newprospects on cerebral target-organ damage in hypertension and have added substance to the concept of “preventablesenility.” The aim of this study was to analyze the impact of hypertension, circadian BP profile, and disturbed glucosemetabolism on cognitive function. The study population consisted of 999 seventy-year-old men from a population-basedcohort study in Uppsala, Sweden, followed with respect to cardiovascular risk factors since the age of 50 years. At the ageof 70, 24-hour ambulatory BP was monitored together with measurements of insulin sensitivity, glucose tolerance, serumlipids, and lipoproteins. Cognitive function was assessed by the Mini-Mental State Examination and the Trail-Making Test.High diastolic BP at baseline predicted later impaired cognitive performance, even after excluding men with a previousstroke (n570). Cross-sectional measurements at age 70 showed that high 24-hour BP, nondipping, insulin resistance, anddiabetes all were related to low cognitive function. The relationships between hypertension and cognitive impairmentwere strongest in untreated men. These data from a general population of healthy elderly men indicate that hypertensionand associated metabolic disturbances might be susceptibility factors for cognitive disorders. The findings add support topossibilities of intervention in early stages in cognitive decline, ie, before manifest dementia. (Hypertension.1998;31:780-786.)
Key Words: cognition n blood pressure monitoring, ambulatory n diabetes n insulin resistance
The question of whether some degree of cognitive deterio-ration is an inevitable part of aging or should be considered
as a pathological prestage of dementia is currently debated.This is a field in need of research1 because further decline incognition might be preventable in the early stages of “cogni-tive impairment nondementia.” Vascular dementia is a com-mon form of dementia; in the oldest elderly patients it is asfrequent as Alzheimer’s disease.2 Recently, a 15-year follow-upstudy showed that high BP predicted dementia in the oldestelderly patients, irrespective of subtype.3 Little is known abouthow cognitive function is affected by vascular risk factors in thegeneral population. The aim of the present study was toanalyze the associations between BP, diurnal BP variation,disturbances in glucose and lipid metabolism, and cognition.We examined cognitive functions in a population-based co-hort of 70-year-old men in which longitudinal measurementsof vascular risk factors were available.
MethodsThe study population consisted of 999 men. They were participants ina health survey focusing on cardiovascular risk factors that was startedin the beginning of the 1970s in Uppsala, Sweden. The original cohortwas defined as all men born in 1920 to 1924, who resided in themunicipality of Uppsala in 1970 to 1973 (n52841). A total of 2322(81.7%) men participated in the baseline examination at 50 years ofage.4 As a result of this first survey, medical and/or dietary treatmentwere offered to 126 men with hypertension, to 363 men withhyperlipidemia, and to 112 men with impaired glucose tolerance.5 A
new examination was carried out when they were 60 years of age, inwhich 1860 of the 2130 remaining men from the original study cohortparticipated. In January of 1991, 422 subjects from the 50-year studyhad died. Of the 1900 men still alive, those who lived in Uppsalacounty (n51681) were invited to a more extensive health examina-tion, in which 1221 men (72.6%) took part. These men were alsoinvited to a psychometric testing, in which 999 men (82%) took part.Their mean age was 72.4 years (range, 69 to 75 years).
Vascular Risk FactorsFrom the baseline examination at age 50 years, data for the followingmeasurements were collected: office SBP and DBP measured in thesupine position after 10 minutes rest with a mercury manometer to thenearest 0 or 5 mm Hg; BMI calculated as weight (in kilograms)divided by the height squared (in meters); and fasting concentrationsof blood glucose, serum insulin (n5815), HDL cholesterol (n5801),and serum triglycerides. The study protocol has previously beendescribed in detail.6 Values of serum lipids and lipoproteins were laterstandardized to correspond to the methods used for the 70-yearsurvey. From the 60-year survey, data on office BP, measured asdescribed above, and antihypertensive treatment from a questionnairewere collected. At the 70-year survey, the investigations includedoffice SBP and DBP in the supine position, measured with asphygmomanometer to the nearest 2 mm Hg (mean of two measure-ments), calculation of BMI, analyses of fasting plasma concentrationsof insulin and glucose, and serum lipids and lipoproteins.7 Twenty-four-hour ABPMs were completed in 950 of the participants in thecognitive study, using the Accutracker 2 equipment (Suntech MedicalInstruments Inc). BP recordings were made every 20 minutes duringdaytime (6:00 AM to 11:00 PM) and every 20 or 60 minutes duringnighttime (11:00 PM to 6:00 AM). The following variables were used
Received May 20, 1997; first decision June 30, 1997; revision accepted October 6, 1997.From the Department of Geriatrics (L.K., M.B., L.H., H.L.), Uppsala, and the Department of Clinical Neurosciences (H.N.), Karolinska Hospital,
Stockholm, Sweden.Correspondence to Dr Lena Kilander, Department of Geriatrics, Kålsangsgrand 10 D, PO Box 609, S-751 25 Uppsala, Sweden.© 1998 American Heart Association, Inc.
780 by guest on March 21, 2013http://hyper.ahajournals.org/Downloaded from
in the analyses: MAP, SBP, DBP, and HR during 24 hours; DSBP andDDBP; and NSBP and NDBP. The difference between mean DSBPand mean NSBP was calculated. Nondipping was defined asD(DSBP2NSBP) of #0 mm Hg. SBP variability was estimated as thequotient between the mean standard deviation SBP divided by themean SBP. An OGTT was carried out (n5976), and subjects wereclassified as having normal or impaired glucose tolerance or diabetesaccording to the criteria of the National Diabetes Data Group.8 Ahyperinsulinemic euglycemic clamp7 was performed (n5965) and theM/I was calculated as glucose uptake per minute divided by meaninsulin concentration during the clamp, 60 to 120 minutes. Repro-ducibility was tested in 21 subjects. The coefficients of variation were24-hour DBP, 5%; plasma glucose, 6%; M/I, 14%; serum triglycerides,15%; and plasma insulin, 20%.
Cognitive FunctionThe psychometric testing included the MMSE9 (n5891) (MMSE wasadded to the protocol after the start) and the TMT-A (n5998) andTMT-B (n5996).10 Standardized procedures from published manualswere used in the administration and evaluation. The maximal time setfor TMT-B was 240 seconds. MMSE is a widely used instrument inthe screening for cognitive disorders, and the TMT was selected toassess psychomotor speed and shifting capacity. The testing wasperformed in connection with the ABPM in some cases, but in othersthe time interval was longer (mean, 18 months). After a logarithmictransformation of the test results, a z transformation was applied, anda composite cognitive score was calculated for each subject as themean sum of the test scores. Cognitive score was treated both as acontinuous outcome variable and as a dichotomous variable, settingthe cutoff level for low results at the lowest quintile.
Potential ConfoundersAll pharmacological treatment with agents affecting BP, irrespective ofindication (ie, b-blockers, calcium antagonists, angiotensin-convert-ing enzyme inhibitors, diuretics, and a-blockers), was recorded in aquestionnaire at age 70 years. Educational level was stratified as low(elementary school only, 6 to 7 years, n5530), medium (secondaryschool, n5309), or high (university studies, n5160). Main previousoccupational level was divided into three categories: low (manualworkers, n5406), medium (foremen, clerks, salesmen, n5388), andhigh (major professionals, business managers, n5193). The followingare diagnoses of stroke according to the ICD-8 or ICD-9 before thecognitive testing results were collected from the Swedish NationalInpatient Register and cover all diagnoses in hospitalized patients from1970 and onward: intracerebral hemorrhage (431), thromboembolicstroke (433 to 434), transient ischemic attack (435), and acute“ill-defined” cerebrovascular disease (436). Informed consent wasobtained from the participants after the nature of the procedures had
been fully explained. The study was approved by the Ethics Com-mittee at Uppsala University.
StatisticsA logarithmic transformation was applied to all variables not normallydistributed. Student’s unpaired t test was applied for comparisonsbetween independent groups, the x2 test was used for analysis ofrelationships between categorical variables, and linear relationshipswere examined with Pearson’s correlation coefficient. In the analysesof determinants of cognitive function, adjustment was made forpotential confounders, ie, socioeconomic factors (educational andoccupational levels) and age. ANCOVA was applied in multivariatemodels with continuous dependent variables, and logistic regressionwas used when the outcome variable was binary. The odds ratio forcontinuous explaining variables was calculated per increase with 1 SDwithin a 95% confidence interval or per year (age). Testing for trendwas performed according to Spearman.
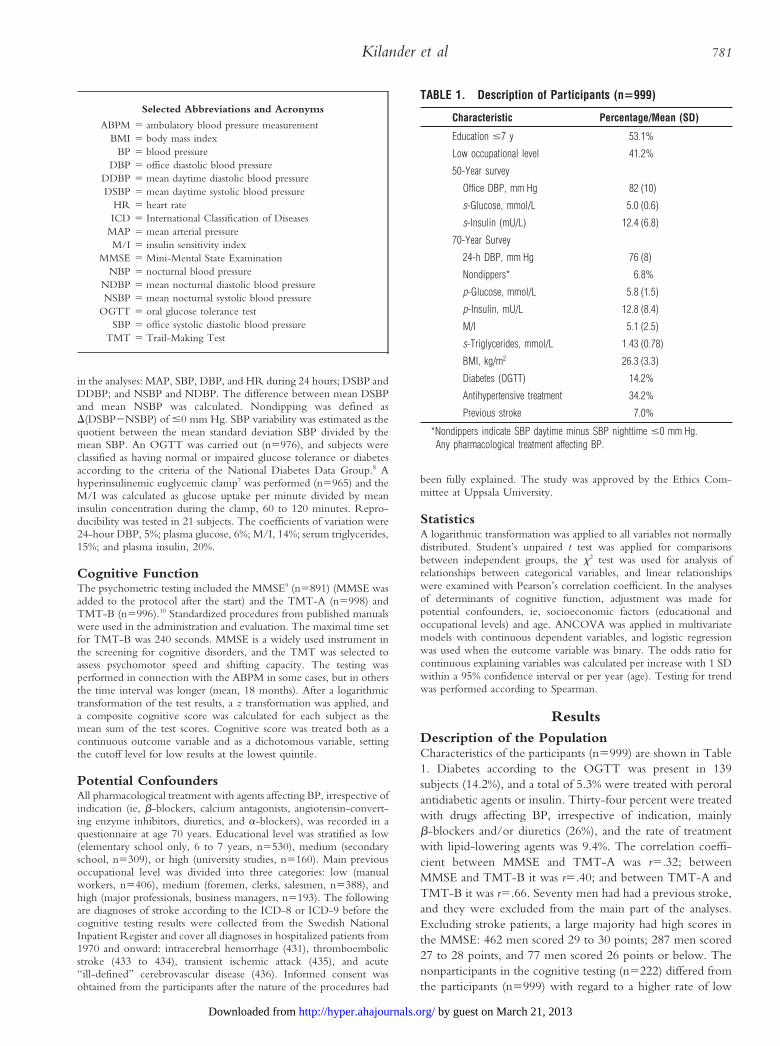
ResultsDescription of the PopulationCharacteristics of the participants (n5999) are shown in Table1. Diabetes according to the OGTT was present in 139subjects (14.2%), and a total of 5.3% were treated with peroralantidiabetic agents or insulin. Thirty-four percent were treatedwith drugs affecting BP, irrespective of indication, mainlyb-blockers and/or diuretics (26%), and the rate of treatmentwith lipid-lowering agents was 9.4%. The correlation coeffi-cient between MMSE and TMT-A was r5.32; betweenMMSE and TMT-B it was r5.40; and between TMT-A andTMT-B it was r5.66. Seventy men had had a previous stroke,and they were excluded from the main part of the analyses.Excluding stroke patients, a large majority had high scores inthe MMSE: 462 men scored 29 to 30 points; 287 men scored27 to 28 points, and 77 men scored 26 points or below. Thenonparticipants in the cognitive testing (n5222) differed fromthe participants (n5999) with regard to a higher rate of low
Selected Abbreviations and Acronyms
ABPM 5 ambulatory blood pressure measurementBMI 5 body mass index
BP 5 blood pressureDBP 5 office diastolic blood pressure
DDBP 5 mean daytime diastolic blood pressureDSBP 5 mean daytime systolic blood pressure
HR 5 heart rateICD 5 International Classification of Diseases
MAP 5 mean arterial pressureM/I 5 insulin sensitivity index
MMSE 5 Mini-Mental State ExaminationNBP 5 nocturnal blood pressure
NDBP 5 mean nocturnal diastolic blood pressureNSBP 5 mean nocturnal systolic blood pressure
OGTT 5 oral glucose tolerance testSBP 5 office systolic diastolic blood pressure
TMT 5 Trail-Making Test
TABLE 1. Description of Participants (n5999)
Characteristic Percentage/Mean (SD)
Education #7 y 53.1%
Low occupational level 41.2%
50-Year survey
Office DBP, mm Hg 82 (10)
s-Glucose, mmol/L 5.0 (0.6)
s-Insulin (mU/L) 12.4 (6.8)
70-Year Survey
24-h DBP, mm Hg 76 (8)
Nondippers* 6.8%
p-Glucose, mmol/L 5.8 (1.5)
p-Insulin, mU/L 12.8 (8.4)
M/I 5.1 (2.5)
s-Triglycerides, mmol/L 1.43 (0.78)
BMI, kg/m2 26.3 (3.3)
Diabetes (OGTT) 14.2%
Antihypertensive treatment† 34.2%
Previous stroke 7.0%
*Nondippers indicate SBP daytime minus SBP nighttime #0 mm Hg.†Any pharmacological treatment affecting BP.
Kilander et al 781
by guest on March 21, 2013http://hyper.ahajournals.org/Downloaded from

education (72%, P,.0001 compared with participants). Inaddition, they had higher office DBP at age 50 and higherplasma concentrations of insulin at age 70 (both P,.05). Thedistributions of 24-hour DBP were equal in participants andnonparticipants.
Interrelationships Between Risk FactorsThe correlation coefficients between office and 24-hour measure-ments were r5.58 for SBP and r5.62 for DBP. There were onlyweak linear relationships between BP and metabolic measure-ments. The correlation coefficients between metabolic measure-ments and 24-hour DBP were as follows: plasma glucose, r5.12(P5.003); plasma insulin, r5.08 (P5.05); M/I, r52.12(P5.003); and BMI, r5.13 (P5.0007). Serum lipids were notsignificantly related to 24-hour DBP. Concentrations of serumtriglycerides were closely related to M/I (r52.39) and to plasmaglucose (r5.27). Plasma glucose was significantly higher in non-dippers (6.3 mmol/L) than in dippers (5.7 mmol/L), independentof 24-hour DBP (P5.008, logistic regression).
Vascular Risk Factors and Cognitive FunctionThe mean cognitive z score in the entire cohort was 60.00(SD 0.82; range, 25.19 to 12.00). Cognitive score was equalin men with missing results from the ABPM, the clamp, or theOGTT compared with the others. Stroke patients (n570)were excluded from the analyses of determinants of cognitivefunction. Their results are shown separately. In all analyses,adjustment was made for age and educational and occupationallevels. The relationships with the composite cognitive scoredescribed below were unchanged when separate analysesbetween risk factors and the single test results (MMSE,TMT-A, TMT-B) were performed.
Longitudinal MeasurementsOffice DBP at baseline (age 50) was inversely related tocognitive function 20 years later. In the analysis, participantswere split into five DBP categories. Cognitive performance atage 70 was highest in men with the lowest baseline BP,DBP#70 mm Hg (n5147), and lowest in men withDBP$105 mm Hg (n536), adjusted value for trend P5.0040(Table 2). Rates of antihypertensive treatment and office DBPat age 60 and 70 years in each BP category are also shown inTable 2. Only 3 men with DBP$105 mm Hg were not treated20 years later; their mean cognitive score was 21.24. Serumconcentrations of insulin at age 50 were also inversely relatedto cognitive results at follow-up (Fig 1). Men within the lowesttertile of s-insulin had higher results than those in the highest
tertile; the difference was, however, not significant when DBPwas adjusted for. High systolic BP, BMI, or high levels ofblood glucose or serum lipids at baseline were not associatedwith later impaired performance.
Cross-sectional Measurements
Blood PressureThere was an inverse relationship between 24-hour ambula-tory SBP and DBP at age 70 years and cognitive score, NDBPshowing the strongest linear relationship (r52.15, P,.0001).Mean HR during 24 hours was also inversely related tocognitive z score (r52.12, P5.0015). Cognitive score bytertiles of 24-hour DBP are shown in Fig 2, with separateanalyses for untreated men (n5594) and treated men (n5289).The inverse relationship between BP and cognitive score wassimilar in both categories but significant for untreated menonly (P5.014 for trend). Mean cognitive score did not differbetween men with and without treatment (10.03 versus10.02, respectively, P5.941), despite higher mean 24-hourDBP in the latter group (75 versus 78 mm Hg, respectively,P,.0001). This finding is discussed further in the followingsections. Isolated systolic hypertension was not related toimpaired cognitive function.
Nondipping and BP VariabilityMean cognitive score was lower in nondippers (n559, 20.22,SD 0.95), than in dippers (n5824, 10.04 [0.77], P5.04). Inmultivariate analyses with cognitive score as a continuousoutcome variable, nondipping, mean 24-hour DBP, and mean24-hour HR were all significantly and inversely related to
Figure 1. Tertiles of serum insulin at age 50 years relative tocognitive score 20 years later. Cognitive score in tertile 1 versustertile 3, ANCOVA: P1 (adjusted for age, education, occupa-tion)5.031; P2 (as P11DBP at age 50)5.145.
TABLE 2. DBP at Age 50 Years in Relation to Cognitive Function at Age 70 Years
DBP at Age 50 yCognitive score,
Mean (SD) P* Treatment at 60 y DBP at 60 y Treatment at 70 y DBP at 70 y
#70 mm Hg (n5147) 10.17 (0.71) . . . 2.7% 78 (7) 8.2% 79 (10)
75–80 mm Hg (n5392) 60.00 (0.82) .0065 2.8% 85 (8) 23.2% 82 (9)
85–90 mm Hg (n5268) 10.04 (0.70) .0018 17.2% 90 (8) 39.9% 86 (9)
95–100 mm Hg (n586) 60.00 (0.89) .032 51.2% 95 (9) 70.9% 89 (9)
$105 mm Hg (n536) 20.33 (0.82) .0016 88.9% 96 (8) 91.7% 89 (9)
Treatment and DBP indicate rates of antihypertensive treatment and DBP at 60 and 70 years, respectively.*Comparisons with DBP #70 mm Hg, adjusted for age and educational and occupational levels. Test for trend: P5.0040; P5.034, including serum insulin at age 50.
782 Hypertension and Cognitive Impairment
by guest on March 21, 2013http://hyper.ahajournals.org/Downloaded from

cognitive performance, independent of each other. Cognitiveperformance in men with high NBP variability as measured bythe quotient between SD (of NSBP) divided by mean (ofNSBP), and in extreme dippers (D[DSBP2NSBP] of$20 mm Hg), was equal to the rest of the cohort. There wasno relationship between the number of missing single mea-surements due to technical reasons and cognitive performance.
Insulin Resistance and DiabetesAs shown in Fig 3, measurements of M/I was negativelyrelated to cognitive results (P5.048 for trend). When adjust-ment was made for 24-hour DBP and treatment, the value fortrend was P5.055. Men with diabetes according to the OGTT(n5130) performed worse than nondiabetic men (n5779,20.16 [0.90] versus 10.06 [0.75]), independent of 24-hourDBP (P5.005). In a multivariate model (n5868), diabetes,nondipping, and 24-hour DBP were all independently andinversely related to cognitive score as a continuous outcomevariable. In diabetic men, performance was equal in men withand without pharmacological treatment. Stratifying for diabe-tes did not alter the relationship between high DBP and lowcognitive results.
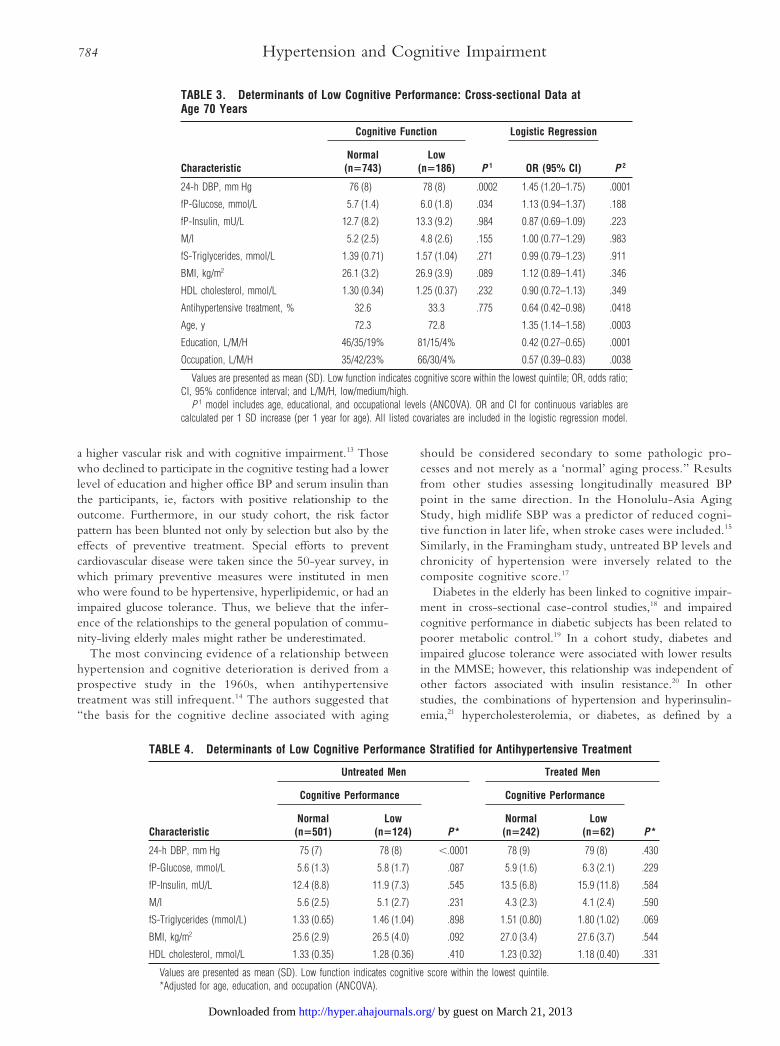
Multivariate AnalysisIn a logistic regression model, cognitive function was treated asa dichotomous variable with the cutoff level for low perfor-mance set at the lowest quintile. In univariate analysis, menwith low cognitive function had higher 24-hour DBP and
higher plasma glucose (Table 3). In a multivariate model thatincluded 24-hour DBP, p-glucose, p-insulin, M/I, s-triglycer-ides, BMI, HDL cholesterol, treatment, age, educational andoccupational levels, an increase of 24-hour DBP with 1 SDwas associated with an odds ratio of 1.45 (1.20 to 1.75) ofcognitive impairment. Despite higher DBP in treated men,antihypertensive treatment was associated with a decreasedrisk, ie, treatment was a negative confounder. As shown inTable 4, the association between hypertension and cognitiveimpairment was significant only in untreated men.
Stroke PatientsMen with a previous stroke (n570) had lower cognitiveresults; mean cognitive score (SD) was 20.43 (1.14) versus10.02 (0.78) for nonstroke subjects (P5.0001), and they hadhigher DBP at baseline. When stroke cases were included inthe analyses previously described, the relationships betweenvascular risk factors and low cognitive performance remainedalmost identical.
DiscussionHigh DBP at the baseline examination at age 50 years wasrelated to impaired cognitive performance 20 years later, evenafter exclusion of men with a previous stroke. Elevatedconcentrations of serum insulin also predicted later low cog-nitive function, but not independently of DBP. Cross-sec-tional measurements at age 70 showed that high 24-hour DBP,a nondipping nocturnal BP pattern, insulin resistance, anddiabetes all were related to low cognitive function. Therelationships between hypertension and cognitive impairmentwere strongest in men without antihypertensive treatment.High BP and impaired glucose metabolism11 are both inde-pendent predictors of cerebrovascular disease. We concludethat hypertension and factors linked to the syndrome of insulinresistance12 might contribute to cognitive disturbances in theelderly, mediated through functional changes, or by silentcerebral large- and small-vessel lesions.
This group was a healthy cohort in which only a minority ofthe participants scored below 27 points in the MMSE. Itconsisted of approximately half of the survivors from thebaseline examination only, but nonresponse to health surveyshas, on the other hand, been shown to be associated both with
Figure 2. Cognitive score by tertiles of 24-hour DBP at age 70.Tests for trend according to Spearman, adjusted for age, edu-cation, occupation, and M/I. P for trend5.014 in untreated men;P for trend5.272 in treated men.
Figure 3. Cognitive score by tertiles of M/I (insulin sensitivityindex) at age 70. P1 for trend (adjusted for age, education,occupation)5.048. P2 for trend (as P1124-hour DBP andtreatment)5.055.
Kilander et al 783
by guest on March 21, 2013http://hyper.ahajournals.org/Downloaded from
a higher vascular risk and with cognitive impairment.13 Thosewho declined to participate in the cognitive testing had a lowerlevel of education and higher office BP and serum insulin thanthe participants, ie, factors with positive relationship to theoutcome. Furthermore, in our study cohort, the risk factorpattern has been blunted not only by selection but also by theeffects of preventive treatment. Special efforts to preventcardiovascular disease were taken since the 50-year survey, inwhich primary preventive measures were instituted in menwho were found to be hypertensive, hyperlipidemic, or had animpaired glucose tolerance. Thus, we believe that the infer-ence of the relationships to the general population of commu-nity-living elderly males might rather be underestimated.
The most convincing evidence of a relationship betweenhypertension and cognitive deterioration is derived from aprospective study in the 1960s, when antihypertensivetreatment was still infrequent.14 The authors suggested that“the basis for the cognitive decline associated with aging
should be considered secondary to some pathologic pro-cesses and not merely as a ‘normal’ aging process.” Resultsfrom other studies assessing longitudinally measured BPpoint in the same direction. In the Honolulu-Asia AgingStudy, high midlife SBP was a predictor of reduced cogni-tive function in later life, when stroke cases were included.15
Similarly, in the Framingham study, untreated BP levels andchronicity of hypertension were inversely related to thecomposite cognitive score.17
Diabetes in the elderly has been linked to cognitive impair-ment in cross-sectional case-control studies,18 and impairedcognitive performance in diabetic subjects has been related topoorer metabolic control.19 In a cohort study, diabetes andimpaired glucose tolerance were associated with lower resultsin the MMSE; however, this relationship was independent ofother factors associated with insulin resistance.20 In otherstudies, the combinations of hypertension and hyperinsulin-emia,21 hypercholesterolemia, or diabetes, as defined by a
TABLE 3. Determinants of Low Cognitive Performance: Cross-sectional Data atAge 70 Years
Characteristic
Cognitive Function
P 1
Logistic Regression
P 2Normal(n5743)
Low(n5186) OR (95% CI)
24-h DBP, mm Hg 76 (8) 78 (8) .0002 1.45 (1.20–1.75) .0001
fP-Glucose, mmol/L 5.7 (1.4) 6.0 (1.8) .034 1.13 (0.94–1.37) .188
fP-Insulin, mU/L 12.7 (8.2) 13.3 (9.2) .984 0.87 (0.69–1.09) .223
M/I 5.2 (2.5) 4.8 (2.6) .155 1.00 (0.77–1.29) .983
fS-Triglycerides, mmol/L 1.39 (0.71) 1.57 (1.04) .271 0.99 (0.79–1.23) .911
BMI, kg/m2 26.1 (3.2) 26.9 (3.9) .089 1.12 (0.89–1.41) .346
HDL cholesterol, mmol/L 1.30 (0.34) 1.25 (0.37) .232 0.90 (0.72–1.13) .349
Antihypertensive treatment, % 32.6 33.3 .775 0.64 (0.42–0.98) .0418
Age, y 72.3 72.8 1.35 (1.14–1.58) .0003
Education, L/M/H 46/35/19% 81/15/4% 0.42 (0.27–0.65) .0001
Occupation, L/M/H 35/42/23% 66/30/4% 0.57 (0.39–0.83) .0038
Values are presented as mean (SD). Low function indicates cognitive score within the lowest quintile; OR, odds ratio;CI, 95% confidence interval; and L/M/H, low/medium/high.
P 1 model includes age, educational, and occupational levels (ANCOVA). OR and CI for continuous variables arecalculated per 1 SD increase (per 1 year for age). All listed covariates are included in the logistic regression model.
TABLE 4. Determinants of Low Cognitive Performance Stratified for Antihypertensive Treatment
Characteristic
Untreated Men Treated Men
Cognitive Performance
P*
Cognitive Performance
P*Normal(n5501)
Low(n5124)
Normal(n5242)
Low(n562)
24-h DBP, mm Hg 75 (7) 78 (8) ,.0001 78 (9) 79 (8) .430
fP-Glucose, mmol/L 5.6 (1.3) 5.8 (1.7) .087 5.9 (1.6) 6.3 (2.1) .229
fP-Insulin, mU/L 12.4 (8.8) 11.9 (7.3) .545 13.5 (6.8) 15.9 (11.8) .584
M/I 5.6 (2.5) 5.1 (2.7) .231 4.3 (2.3) 4.1 (2.4) .590
fS-Triglycerides (mmol/L) 1.33 (0.65) 1.46 (1.04) .898 1.51 (0.80) 1.80 (1.02) .069
BMI, kg/m2 25.6 (2.9) 26.5 (4.0) .092 27.0 (3.4) 27.6 (3.7) .544
HDL cholesterol, mmol/L 1.33 (0.35) 1.28 (0.36) .410 1.23 (0.32) 1.18 (0.40) .331
Values are presented as mean (SD). Low function indicates cognitive score within the lowest quintile.*Adjusted for age, education, and occupation (ANCOVA).
784 Hypertension and Cognitive Impairment
by guest on March 21, 2013http://hyper.ahajournals.org/Downloaded from

questionnaire,22 were related to impaired cognitive function.To our knowledge, ours is the first cohort study showing thatcognitive impairment is related to metabolic disturbanceslinked to the syndrome of insulin resistance, together withhypertension.
The finding that diastolic BP in middle age predicts latercognitive performance suggests a causal relationship. However,the data from the ABPM are cross-sectional, and causalmechanisms can only remain speculative. The causation mightbe reverse, ie, cognitive impairment and altered BP regulationmay both be secondary to silent cerebrovascular lesions. Incross-sectional studies, silent lacunar infarctions23 and vasculardementia characterized by extensive white matter lesions or bymultiple lacunar infarctions24 have been related to the absenceof NBP decrements. Changes in BP circadian variabilityindicate alterations of central nervous regulatory systems,mediated by sympathetic activation. However, on the otherhand, sympathetic overreactivity could also be etiologicallylinked to the syndrome of hypertension and insulin resistance25
and primarily affect cognitive function by vasoconstriction andcerebral small-vessel lesions. The TMT reflects subcorticofron-tal functions, among others, and impaired performance in theTMT has previously been associated with subcortical small-vessel lesions.26,27
Is low BP always desirable, or is there a lower limit belowwhich too-aggressive antihypertensive treatment might behazardous? It has been hypothesized that low systemic BPmight primarily contribute to dementia via impaired cere-bral perfusion and incomplete white matter infarctions inareas supported by stenosed vessels.28 Extreme dipping, aswell as nondipping, was associated with silent cerebrovas-cular disease identified by magnetic resonance imaging.23
Moderate or severe dementia is accompanied by lower BPlevels, but in advanced stages, this is most likely a secondaryphenomenon.29 A previous study showed that cognitivechanges in hypertensive subjects, hypothetically mediatedthrough metabolic or hemodynamic mechanisms, could berestored by treatment.30 In our cohort, there existed noJ-shaped relationship between BP and cognitive function,and there were also indications of a positive effect oftreatment. This latter finding should be interpreted withcaution, because it may be due to selection.
To summarize, our results support the hypothesis thatcerebral target-organ damage in hypertension contributes tocognitive impairment. Cognitive deterioration denotes animpaired quality of life and is also a predictor of dementia andmortality.31 Actions to prevent further decline must be con-sidered as early in the course of the disease as possible, ie,before clinical manifest dementia. Because a linkage with riskfactors for vascular disease has been established, it is urgent toinvestigate whether further cognitive decline can be postponedby a more intensive preventive treatment. There is convincingevidence of the importance of adequate antihypertensivetreatment in primary prevention of cerebrovascular diseaseeven in higher ages,32 and there are no indications of treatmentcausing cognitive deterioration.33 Our findings suggest thattreatment with pharmacological agents that maintain the nor-mal 24-hour BP profile and have no metabolic side effects
should be preferred in the management of elderly persons withhypertension.
AcknowledgmentsThe study was supported by grants from the Swedish MedicalResearch Council (grant 5446), The King Gustav V and QueenVictoria Foundation, The Foundation of Old Servants, The Alzhei-mer Foundation, The Dementia Foundation in Sweden, the SwedishStroke Foundation, and The Swedish Hypertension Society. We aregrateful to Paul McKeigue, Senior Lecturer, London School ofHygiene & Tropical Medicine, for valuable comments on the manu-script and to Gun-Britt Ångman for excellent coordination and care ofthe study participants.
References1. Hachinski V. Preventable senility: a call for action against the vascular
dementias. Lancet. 1992;340:645–648.2. Skoog I, Nilsson L, Palmertz B, Andreasson L-A, Svanborg A. A
population-based study of dementia in 85-year-olds. N Engl J Med. 1993;328:153–158.
3. Skoog I, Lernfelt B, Landahl S, Palmertz B, Andreasson L-A, Nilsson L,Persson G, Oden A, Svanborg A. 15-year longitudinal study of bloodpressure and dementia. Lancet. 1996;347:1141–1145.
4. Hedstrand H. A Study of Middle-Aged Men with Particular Reference to RiskFactors for Cardiovascular Disease. Uppsala, Sweden: Faculty of Medicine,Uppsala University; 1975. Thesis.
5. Lithell H, Åberg H, Selinus I, Hedstrand H. The Primary Preventive Studyin Uppsala: fatal and non-fatal myocardial infarction during a 10-yearfollow-up of a middle-aged male population with treatment of high-riskindividuals. Acta Med Scand. 1984;215:403–409.
6. Skarfors E. Risk Factors for Development of Diabetes Mellitus, Hypertension andCoronary Heart Disease. Uppsala, Sweden: Faculty of Medicine, UppsalaUniversity; 1989. Thesis.
7. Pollare T, Lithell H, Selinus I, Berne C. Application of prazosin is asso-ciated with an increase of insulin sensitivity in obese patients with hyper-tension. Diabetologia. 1988;31:415–420.
8. National Diabetes Data Group. Classification and diagnosis of diabetesmellitus and other categories of glucose intolerance. Diabetes. 1979;28:1039.
9. Folstein MF, Folstein SE, McHugh PR. ‘Mini-Mental State’: a practicalmethod for grading the cognitive state of patients for the clinician. J Psy-chiatr Res. 1975;12:189–198.
10. Lezak M. Neuropsychological Assessment. 3rd ed. New York, NY: OxfordUniversity Press; 1995.
11. Kuusisto J, Mykkanen L, Pyorala K, Laakso M. Non–insulin-dependentdiabetes and its metabolic control are important predictors of stroke inelderly subjects. Stroke. 1994;25:1157–1164.
12. Reaven G. Role of insulin resistance in human disease. Diabetes. 1988;37:1595–1607.
13. Launer LJ, Wind AW, Deeg DJH. Nonresponse pattern and bias in acommunity-based cross-sectional study of cognitive functioning among theelderly. Am J Epidemiol. 1994;139:803–812.
14. Wilkie F, Eisdorfer C. Intelligence and blood pressure in the aged. Science.1971;172:959–962.
15. Launer LJ, Masaki K, Petrovitch H, Foley D, Havlik RJ. The associationbetween midlife blood pressure and late-life cognitive function: theHonolulu-Asia Aging Study. JAMA. 1995;274:1846–1851.
16. Deleted in proof.17. Elias MF, Wolf PA, D’Agostino RB, Cobb J, White LR. Untreated blood
pressure level is inversely related to cognitive functioning: the FraminghamStudy. Am J Epidemiol. 1993;138:353–364.
18. Tun PA, Nathan DM, Perlmuter LC. Cognitive and affective disorders inelderly diabetics. Clin Geriatr Med. 1990;6:731–746.
19. Reaven GM, Thompson LW, Nahum D, Haskins E. Relationshipbetween hyperglycemia and cognitive function in older NIDDM patients.Diabetes Care. 1990;13:16–21.
20. Kalmijn S, Feskens EJM, Launer LJ, Stijnen T, Kromhout D. Glucoseintolerance, hyperinsulinaemia and cognitive function in a general popu-lation of elderly men. Diabetologia. 1995;38:1096–1102.
21. Kuusisto J, Koivisto K, Mykkanen L, Helkala E-L, Vanhanen M,Hanninen T, Pyorala K, Riekkinen P, Laakso P. Essential hypertension andcognitive function: the role of hyperinsulinemia. Hypertension. 1993;22:771–779.
Kilander et al 785
by guest on March 21, 2013http://hyper.ahajournals.org/Downloaded from

22. Desmond DW, Tatemichi TK, Paik M, Stern Y. Risk factors for cerebro-vascular disease as correlates of cognitive function in a stroke-free cohort.Arch Neurol. 1993;50:162–166.
23. Kario K, Matsuo T, Kobayashi H, Imiya M, Matsuo M, Shimada K.Nocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients. Hypertension. 1996;27:130–135.
24. Tohgi H, Chiba K, Kimura M. Twenty-four-hour variation of bloodpressure in vascular dementia of the Binswanger type. Stroke. 1991;22:603–608.
25. Reaven G, Lithell H, Landsberg L. Hypertension and associated metabolicabnormalities: the role of insulin resistance and the sympathoadrenalsystem. N Engl J Med. 1996;334:374–381.
26. Breteler M, van Amerongen N, van Swieten J, Claus J, Grobbee D, vanGijn J, Hofman A, van Harskamp F. Cognitive correlates of ventricularenlargement and cerebral white matter lesions on magnetic resonanceimaging. Stroke. 1994;25:1109–1115.
27. Ylikoski R, Ylikoski A, Erkinjuntti T, Sulkava R, Raininko R, Tilvis R.White matter changes in healthy elderly persons correlate with attentionand speed of mental processing. Arch Neurol. 1993;50:818–824.
28. Englund E, Brun A, Gustafson L. A white-matter disease in dementia ofAlzheimer’s type: clinical and neuropathological correlates. Int J GeriatrPsychiatry. 1989;4:87–102.
29. Guo Z, Viitanen M, Fratiglioni L, Winblad B. Low blood pressure anddementia in elderly people: the Kungsholmen project. BMJ. 1996;312:805–808.
30. Miller RE, Shapiro AP, King HE, Ginchereau EH, Hosutt A. Effect ofantihypertensive treatment on the behavioral consequences of elevatedblood pressure. Hypertension. 1984;6:202–208.
31. Bowen J, Teri L, Kukull W, McCormick W, McCurry S, Larson E.Progression to dementia in patients with isolated memory loss. Lancet.1997;349:763–765.
32. Dahlof B, Lindholm LH, Hansson L, Schersten B, Ekbom T, Wester P-O.Morbidity and mortality in the Swedish trial in old patients with hyper-tension (STOP-Hypertension). Lancet. 1991;338:1281–1285.
33. Applegate WB, Pressel S, Wittes J, Luhr J, Shekelle RB, Camel GH,Greenlick MR, Hadley E, Moye L, Perry HM, Schron E, Wegener V.Impact of the treatment of isolated systolic hypertension on behavioralvariables. Arch Intern Med. 1994;154:2154–2160.
786 Hypertension and Cognitive Impairment
by guest on March 21, 2013http://hyper.ahajournals.org/Downloaded from