1 how far we’ve come integrating primary & behavioral healthcare
TRANSCRIPT

1
How far we’ve come
Integrating Primary & Behavioral
Healthcare
2
My Background
Medicaid Director Previously DMH Medical Director – 20 years
– Practicing Psychiatrist– CMHCs – 10 years– FQHC – 18 years
Distinguished Professor, Missouri Institute of Mental Health, University of Missouri St. Louis
3
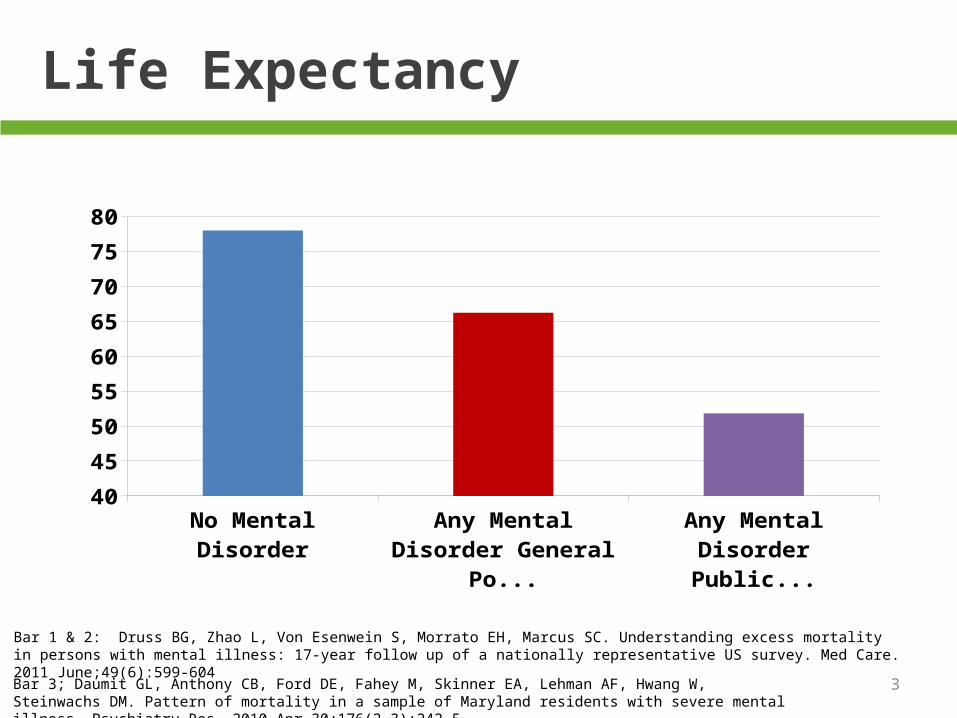
Life Expectancy
No Mental Disorder Any Mental Disorder General Population
Any Mental Disorder Public Sector
40
45
50
55
60
65
70
75
80
Bar 1 & 2: Druss BG, Zhao L, Von Esenwein S, Morrato EH, Marcus SC. Understanding excess mortality in persons with mental illness: 17-year follow up of a nationally representative US survey. Med Care. 2011 June;49(6):599-604
Bar 3; Daumit GL, Anthony CB, Ford DE, Fahey M, Skinner EA, Lehman AF, Hwang W, Steinwachs DM. Pattern of mortality in a sample of Maryland residents with severe mental illness. Psychiatry Res. 2010 Apr 30;176(2-3):242-5

What are the Causes of Morbidity and Mortality in People with Serious Mental Illness?
88% of the deaths and 83% of premature years of life lost in persons with serious mental illness are due to “natural causes”
– Cardiovascular disease– Diabetes– Respiratory diseases– Infectious diseases

5
-60
-50
-40
-30
-20
-10
0
10
79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95
Dec
line
(%)
Noncardiovascular Disease
Coronary Heart Disease (CHD)
Stroke
Morbidity and Mortality Weekly Report. 1999; 48(30):649-656.
Change in US General Population Age-Adjusted Mortality (1979-1995)
Year

6
Mortality Risk From all causes and cardiovascular disease increased in patients with schizophrenia between 1970-2003
70-74 75-79 80-84 85-89 90-94 95-99 00-030
0.5
1
1.5
2
2.5
3
1970-1974
1975-1979
1980-1984
1985-1989
1990-1994
1995-1999
2000-2003
0
0.5
1
1.5
2
2.5
Test for time trends of excess relative risks for SMRs were statistically significant (P<0.001) for all causes of mortality due to cardiovascular disease.
Men Women
Ösby U et al. BMJ. 2000;321:483-484, and unpublished data courtesy of Urban Osby.
All causes Cardiovascular Disease

7
Maine Study Results Comparison of health disorders between SMI & Non-SMI groups
59.4
33.930 28.6 28.4
22.8 21.7
16.5
11.5 11.1
6.3 5.9
0
20
40
60
80
% M
embe
rs
SMI (N=9224)
Non-SMI(N=7352)
8
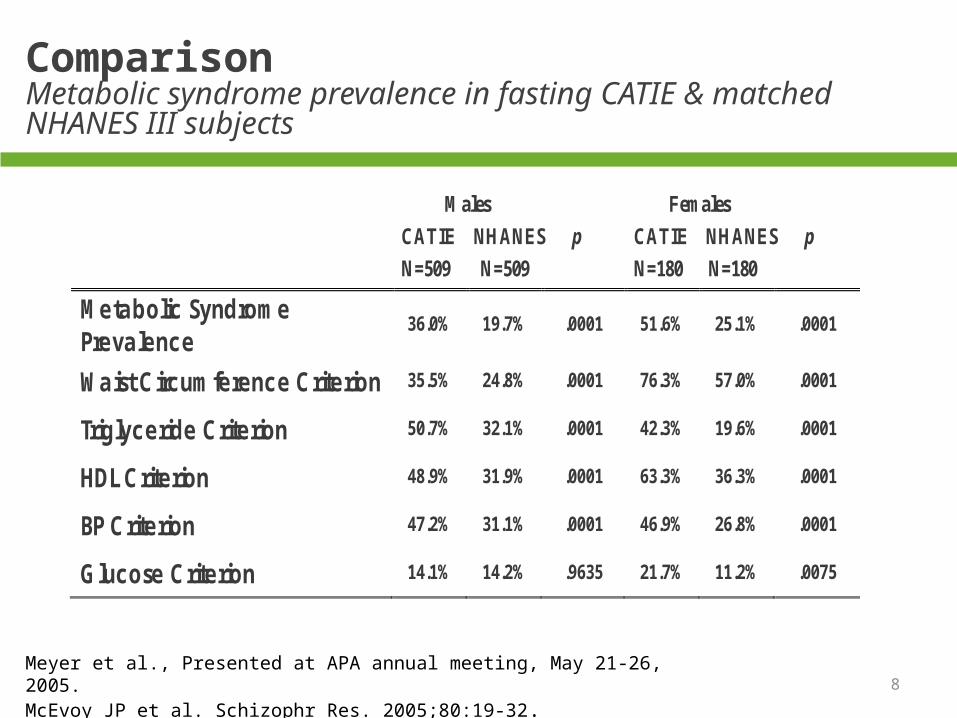
Comparison Metabolic syndrome prevalence in fasting CATIE & matched NHANES III subjects
Males
CATIE NHANES p
N=509 N=509
Females
CATIE NHANES p
N=180 N=180
Metabolic Syndrome Prevalence
36.0% 19.7% .0001 51.6% 25.1% .0001
Waist Circumference Criterion 35.5% 24.8% .0001 76.3% 57.0% .0001
Triglyceride Criterion 50.7% 32.1% .0001 42.3% 19.6% .0001
HDL Criterion 48.9% 31.9% .0001 63.3% 36.3% .0001
BP Criterion 47.2% 31.1% .0001 46.9% 26.8% .0001
Glucose Criterion 14.1% 14.2% .9635 21.7% 11.2% .0075
Meyer et al., Presented at APA annual meeting, May 21-26, 2005. McEvoy JP et al. Schizophr Res. 2005;80:19-32.

9
The CATIE Study
At baseline investigators found that:
88.0% of subjects who had dyslipidemia
62.4% of subjects who had hypertension
30.2% of subjects who had diabetes
were NOT receiving treatment.

10
Causes of Excess Mortality
Smoking
Obesity
Inactivity
Polypharmacy
Under-diagnosis of medical conditions
Inadequate medical
treatment

11
Per Member Per Month Costs
Private Sector Medicare Medicaid$0
$200
$400
$600
$800
$1,000
$1,200
$1,400
$1,600
No Mental DisorderAny Mental Disorder
Melek et. al, Milliman, Inc., 2013

12
MH/SU costs in NY state’s Medicaid program
MH Disorder SU Disorder No MH/SU Disorder
$10,000
$12,000
$14,000
$16,000
$18,000
$20,000
$22,000
$24,000
$26,000
$28,000
$30,000
Behavioral Health costsPhysical Helath costsPhysical Health costs

13
Recovery for persons with serious mental illness (SMI)
CMHC Mission

14
CMHC Problem
Early death from physical illness prevents recovery from SMI

17
Big Trends
Increased coverage Increased demand Focus of high utilizers Increased desire for integration by payers Shrinking psychiatric workforce
18
Drivers of Increased Demand
ACA requires newly covered populations meet the parity requirements of Wellstone Domenici Parity Act
Multiple parts of ACA require or incentivize integration of Behavioral Health and general medical care
ACA insurance reforms and coverage expansions provide new coverage many people need and want BH services
Stigma continues to drop releasing pent up demand
In responding to recent press coverage of mass shootings increasing mental health services is more popular than gun control

19
So, what to do…
There is NO one magic bullet
Integration of behavioral health and primary care
Team care with everyone working at the top of their training
Population health management
Health care delivery based on deep partnerships

20
4 Strategies
1. Coordination of care
– EHR, CyberAccess, PROACT, and Missouri Health
Connection
– Care management – CMHC & FQHC as Health Homes
2. Co-Location/Integration of primary and behavioral healthcare –
CMHC/FQHC partnering and Health Homes
3. Medical disease management including for persons with mental
illness
4. BH interventions for medical risks
– Obesity/activity
– Smoking
– Screening for prevention and treatment

21
CMHC Health Home Performance Progress
LDL, A1C, and Blood Pressure

Outcomes | LDL Levels
CMHCs PCHHS100.0
105.0
110.0
115.0
120.0
125.0
130.0
135.0
130.3 130.3
115.0
121.5
111.5
117.2
Baseline Year 1 Year 2
10% ↓ in LDL level 30% ↓ in cardiovascular
disease

Outcomes | A1C Levels
CMHCs PCHHS7.50%
8.00%
8.50%
9.00%
9.50%
10.00%
10.50%
10.01%
9.81%
8.96%
9.20%
8.58%
9.07%
Baseline Year 1 Year 2
1 point drop in A1c
21% ↓ in diabetes-related deaths
14% ↓ in heart attack 31% ↓ in microvascular
complications

Outcomes | Hypertension and Cardio
Good Cholesterol for Clients w/ CVD(<100 mg/dL)
Normal Blood Pressure for Clients w/ HTN
(<140/90 mmHg)
0%
10%
20%
30%
40%
50%
60%
70%
21%24%
37%41%
49%
55%55%
62%
55%
65%
Feb'12Baseline
Feb'1312 Months
June'1318 Months
Jan'142 Years
June'142.5 Years
34% 41%

Outcomes | Diabetes
Good Cholesterol(<100 mg/dL)
Normal Blood Pressure(<140/90 mmHg)
Normal Blood Sugar(A1c <8.0%)
0%
10%
20%
30%
40%
50%
60%
70%
22%
27%
18%
38%
46%42%
47%
59%
53%50%
67%
57%59%
69%
64%
Feb'12Baseline
Feb'1312 Months
June'1318 Months
Jan'142 Years
June'142.5 Years
37% 42% 46%

Outcomes | Metabolic Syndrome Screening
Metabolic Syndrome Screening (All HCH Enrollees)0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12%
46%
61%
80% 80%
86%
Feb'12Baseline
Feb'1312 Months
June'1318 Months
Jan'142 Years
June'142.5 Years
March '153 Years
74%
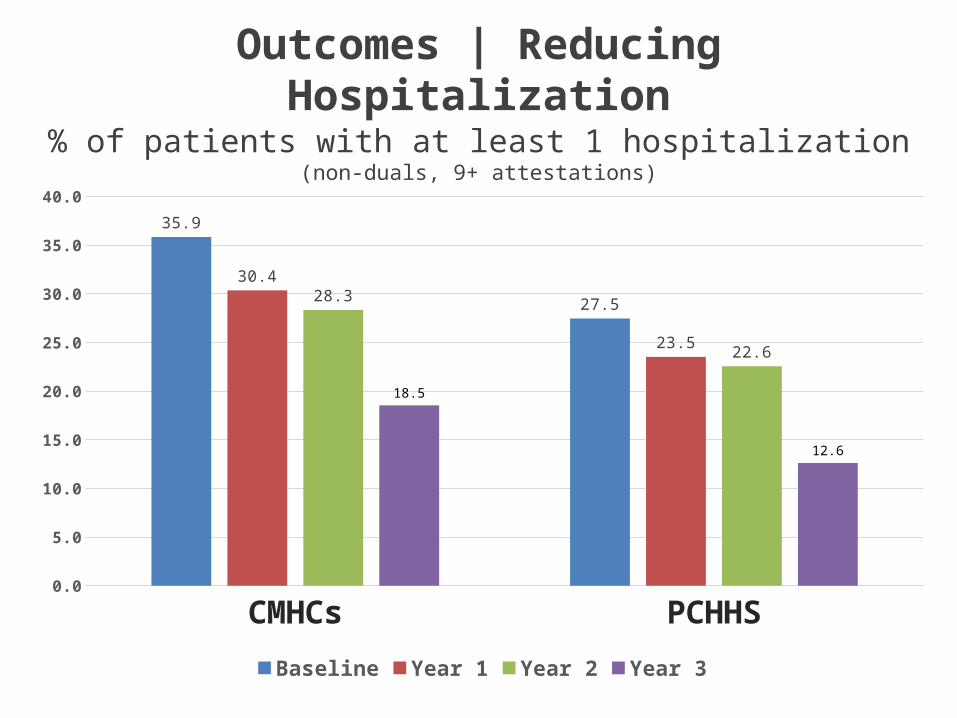
Outcomes | Reducing Hospitalization
CMHCs PCHHS0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
35.9
27.5
30.4
23.5
28.3
22.6
18.5
12.6
Baseline Year 1 Year 2 Year 3
% of patients with at least 1 hospitalization(non-duals, 9+ attestations)

CMHC Hospital Days Per 1000 Member Month
Pre4 Pre3 Pre2 Pre1 Post1 Post2 Post30
50
100
150
200
250
300
350
<18 18-64 65+ Total

CMHC ER Visits Per 1000 Member Month
(attestation method)

30
Initial Estimated Cost Savings After 18 Months
PC Health Homes
– 23,354 persons total served (includes Dual Eligibles)– Cost decreased by $30.79 PMPM– Total cost reduction $7.4 M
CMHC Health Homes
– 20,031 persons total served (includes Dual Eligibles)– Cost decreased by $76.33 PMPM– Total cost reduction $15.7 M

What Makes it Possible?
A Relationship of basic trust between:
– Department of Mental Health
– MO HealthNet (Medicaid)
– State Budget Office
– MO Coalition of CMHCs
– MO Primary Care Association Transparent use of data instead of
anecdotes to explore and discuss issues
Willingness of all partners to tolerate and share risk
Principled negotiation and Motivational Interviewing

Partnership Principles
DO
Ask about their needs first
Give something
Assist wherever you can
Make it about the next 10
Pursue common interest
Reveal anything helpful
Take one for the team
DON’T
Talk about your need first
Expect to get something
Limit assistance to a project
Make it about this deal
Push a specific position
Withhold information
Let them take their lumps

Character– Talk Straight– Demonstrate Respect– Create Transparency– Right Wrongs– Show Loyalty
Competence– Deliver Results– Get Better– Confront Reality– Clarify Expectations– Practice Accountability
Character & Competence– Listen First– Keep Commitments– Extend Trust
S.M.R. Covey, The Speed of Trust
Behaviors that Promote Trust

Resources
NASMHPD Technical Reportshttp://www.nasmhpd.org/publications/NASMHPDPublications.aspx
Healthcare Home Source documents pagehttp://dmh.mo.gov/mentalillness/introcmhchch.html
Missouri CMHC Healthcare Homeshttp://dmh.mo.gov/mentalillness/mohealthhomes.html