1 appendix 1 - extract from memorandum of...
TRANSCRIPT
5
Appendix 1 - Extract from Memorandum of Information
2.1 Background and Context to the Community Health Services for North Somerset
The North Somerset Clinical Commissioning Group (CCG) is the organisation responsible for making sure that the people of North Somerset have the NHS health services they need. NHS England currently has responsibility for Health Visitors until transferred to the Local Authority’s Public Health along with Public Health Children’s Services.
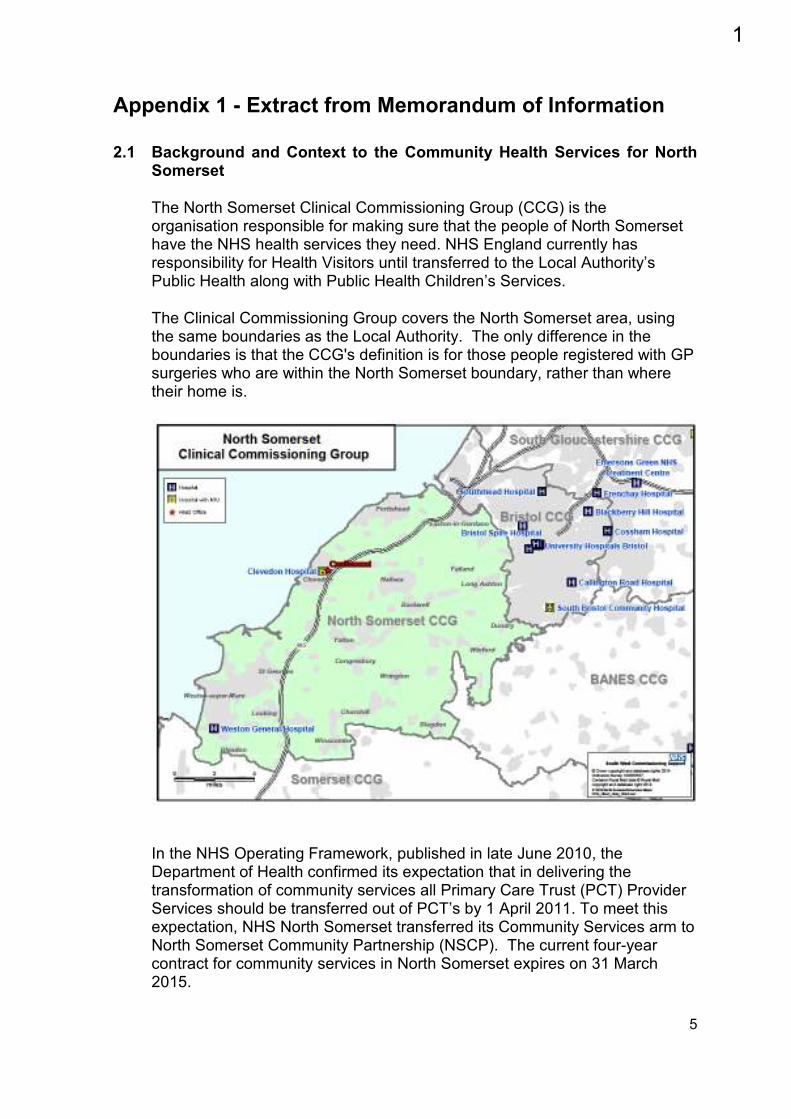
The Clinical Commissioning Group covers the North Somerset area, using the same boundaries as the Local Authority. The only difference in the boundaries is that the CCG's definition is for those people registered with GP surgeries who are within the North Somerset boundary, rather than where their home is.
In the NHS Operating Framework, published in late June 2010, the Department of Health confirmed its expectation that in delivering the transformation of community services all Primary Care Trust (PCT) Provider Services should be transferred out of PCT’s by 1 April 2011. To meet this expectation, NHS North Somerset transferred its Community Services arm to North Somerset Community Partnership (NSCP). The current four-year contract for community services in North Somerset expires on 31 March 2015.
1
6
In August 2013, the North Somerset Clinical Commissioning Leadership Group reached a decision to extend the contract for a period of one year to March 2016 to allow time to conduct a procurement exercise to appoint a suitable Provider. North Somerset’s current Provider of Community Health Services provides NHS services including District Nursing, Children's Community Nursing, Therapy Services and other Specialist Services supporting people in their own homes. It is made up of a staff of over 600 healthcare support professionals who provide Community Healthcare Services to the population of North Somerset; approximately 210,000 people. The currently commissioned services include, although not limited to:
• Bladder and bowel • CHC and FNC assessors • Clevedon Community Hospital • Community home oxygen • Community in-reach • Community IV service • Community pulmonary
rehabilitation • Community teams • Diabetes specialist nursing (Adult) • Diabetes specialist nursing
(Paediatric) • Disabled adults’ rehabilitation and
resource team • Enablement • End of Life coordination centre • Falls prevention and management • Heart failure
• Integrated teams • LD intensive support • Learning disabilities • Lymphoedema • Mental health placement
assessors • Minor injuries unit • Musculo-skeletal interface and
physiotherapy • Out of Hours nursing • Parkinson's specialist nurse • Podiatry • Residential home support • Single point of access • Specialist Community Public
Health Nursing • Tissue viability
2
Appendix 2Community Health Services for North Somerset Call for Final Tenders
The table below lists the critical success factors (CSFs) of the project, and Call for Final Tender questions.
In this document, the term “people” is defined as: Adults of working age, older people, children, and young people in North Somerset.
For any named or material sub-contractors please include formal evidence in the form of a letter of intent, a Memorandum of Understanding, or equivalent.
The contract for Community Health Services for North Somerset will be subject to annual price review and negotiation. Bidders should be aware and accept that answers or part answers at this stage may be inserted directly into the contract.
Please ensure that all responses are DDA compliant when printed on A4 paper https://www.gov.uk/definition-of-disability-under-equality-act-2010
Please note that during the pre-procurement and procurement process to date, we have provided or signposted a number of information sources. We expect bidders to demonstrate use of this information.
This includes The North Somerset CCG Plan on a Page The North Somerset Council Corporate Plan The Memorandum of Information (included in the PQQ documentation) The Joint Strategic Needs Assessment The Stakeholder Engagement Report The Bidder Information Pack for ITN1 The Bidder Information Pack for ITN2 The presentations and the questions and answers from the Prior Information
Notice (PIN) event, and the bidder event held during the PQQ stage Feedback from negotiation meetings throughout the process
We also expect bidders to use information available on the CCG and Local Authority websites, including the following new information:
3
Community Health Services for North Somerset – Call for final tender questions – FINAL
Page 2 of 10 4 June 2015
The presentations and Q&A from the April 2015 stakeholder engagement event
The consultation feedback report The websites are:
North Somerset CCG: https://www.northsomersetccg.nhs.uk/ North Somerset Council: http://www.n-somerset.gov.uk/
All queries not addressed by the information provided at this stage should be addressed via the In-Tend system.
4

Community Health Services for North Somerset – Call for final tender questions – FINAL
Page 3 of 10 4 June 2015
Service model
Description This information is required but will not be marked. It will be used to provide context for your answers to the subsequent questions.
Service model – Word limit: 5,000 words
Describe your final service model and how this will deliver the outcomes framework (link below) in North Somerset? The outcomes framework is contained in the ITN 2 bidder information pack, available from the CCG website: https://www.northsomersetccg.nhs.uk/media/medialibrary/2015/01/Bidder_information_pack_ITN_2.pdf
5
Community Health Services for North Somerset – Call for final tender questions – FINAL
Page 5 of 10 4 June 2015
CSF 1 – Quality, Clinical Safety and Effectiveness
Description – a system focused on the person to provide a needs-led citizen-centred service delivered in a safe and effective manner
Question 1 – 30% - Word limit: 2,500 words
a) (15% 1,250 words) Within the context of a whole-life approach to universal service delivery in North Somerset, describe your final approach and governance structure for delivering quality, clinical safety, and effectiveness in your service model.
This should include how you deliver quality, clinical safety, and
effectiveness in your service model and your relationships with other partners
b) (15% 1,250 words) What are the key workforce implications of your outlined
service model, and how would you go about assessing the effectiveness of your model from a workforce perspective. This should include
Your approach to assessing the workforce requirements of the model. An organisational diagram detailing your management structure at day 0,
and futher diagrams if required detailing transformed structures, and at what point in the contract these occur.
How will this deliver both the locality model and area-wide specialist services.
How you will manage staff caseloads across the services, ensuring you have flexibility to cover sickness, maternity leave, etc.
How you will manage demand and changes in the acuity profile of your caseload
Delivery of cultural changes Any additional capacity or capability required to deliver transformation
6
Community Health Services for North Somerset – Call for final tender questions – FINAL
Page 6 of 10 4 June 2015
CSF 2 – Engagement
Description – to work with communities and citizens
Question 2 – 15% - Word limit: 750 words
In a tabular format of two columns: “You said”, and “We will”, provide examples of how our engagement and consultation feedback reports and other information have been used in the development of your model.
7
Community Health Services for North Somerset – Call for final tender questions – FINAL
Page 7 of 10 4 June 2015
CSF 3 – Integration CSF 4 – Partnership working
Description To integrate with, and positively contribute to, the local healthcare community; to organise care around citizens and communities, blurring the boundaries between primary, community and secondary health, social care and the third sector, and between formal and informal support.
Description To effectively become an integral part of local health and social care provision working across the system
Question 3 – 15% - Word limit: 1,250 words
Having described your model, which providers would you integrate with, and which would you work in partnership with? Describe how this would work in practice and provide evidence of your agreements and partnering arrangements across the model. This should include:
What steps you would take to implement these arrangements How you will manage risks across organisations to include governance and
financial risks For any named or material sub-contractors, formal evidence in the form of a
letter of intent, a Memorandum of Understanding, or equivalent. Your place as a partner in the system
8
Community Health Services for North Somerset – Call for final tender questions – FINAL
Page 8 of 10 4 June 2015
CSF 5 - Social Value CSF 7 - Strategic Fit CSF 8 - Innovative transformation
Description To have a substantive positive impact on the local community of North Somerset beyond the direct remit of the contract.
Description To provide a service that meets national and local strategic aims and objectives for North Somerset
Description
To understand and assess the different options available to challenge the status quo of provider configuration as well as being clear on the benefits to organisations involved and organisational accountability
Question 4 – 20% - Word limit: 2,000 words
a) (10%, 1,000 words) How has consideration of North Somerset’s wide strategic aims and objectives influenced your model? This should include:
Referencing and evidencing the provided information. Evaluation of your model against North Somerset needs. Specific community benefits beyond health and social care Your part in system-wide Operational Resilience and Capacity
Planning (ORCP)
b) (10%, 1,000 words) Describe the innovative elements of the model you have proposed, and how they will deliver qualitative benefits to North Somerset? This should include:
Describing the element and the tangible outcomes. What is the evidence your innovation will deliver the qualitative
benefits. Who you are working with to deliver the system-wide innovation with
specific examples of the provider and the service. Evidence the cost benefits including applications and sources. How you will manage any investment/disinvestment
9
Community Health Services for North Somerset – Call for final tender questions – FINAL
Page 9 of 10 4 June 2015
CSF 6 – Business Needs CSF 9 – Value for money and affordability
Description To provide a service that meets the national and local business needs for community services. This includes the need for flexibility in response to future service changes, outcomes, performance and information requirements
Description To provide a service that is affordable within the resources available and provides value for money whilst maintaining quality and standards of care in the delivery of the service. Evidences a reduction in acute admissions to secondary care and importantly, costs and capacity of secondary care services
Question 5 – 20% Word limit: 2,500 words
a) (5%,500 words) Describe your funding proposals and assumptions through mobilisation and into implementation. This should include:
how you would manage your cash flow the effects on your working capital billing arrangements pension arrangements funding of any planned investments funding of any capital investment tax and VAT arrangements redundancy plans pension arrangement for TUPE’d staff service changes compliance with any regulatory requirements decision making process if successful
Please complete the finance schedules in full. This should include:
Compliance with the financial workbook guidance Internal consistency Clarity of assumptions. Please note guidance point 1, which may require, in discussion,
amendments to be made to the finance schedules following initial review
b) (5%,500 words) How do you propose to use the national standard contract to deliver an outcomes based service? This should include:
Incentives and supporting system changes, and the avoidance of perverse incentivisation.
Demonstrable contribution to system and broader sustainability
10

Community Health Services for North Somerset – Call for final tender questions – FINAL
Page 10 of 10 4 June 2015
c) (5%, 750 words) Describe how you will deliver : Your strategy for IT support to the proposed delivery model How this strategy will be implemented and managed and
Your plans for managing the transition to the new contract including; data migration, testing and training. Include key considerations and risks and how these will be managed.
You responsibility and ongoing commitment to the roll-out of EMIS You responsibility and ongoing commitment to Connecting Care How you will manage any investment/disinvestment
d) (5%, 750 words) Please provide the following documentation: A mobilisation and implementation plan in Gantt chart format Risks, Actions, Issues and Dependencies (RAID) log Outcomes scorecard (Key performance indicators)
11
Appendix 3
Mobilisation, Transition and Integration Plan
1.1 Introduction
1.1.1 The CCG and Local Authority will work with the local health economy and the Lead Provider(s) to ensure collaborative, robust governance during mobilisation, throughout the term of the Contract.
1.1.2 There are three specific phases to consider:
Mobilisation Phase – the period from Awarded bidder(s) selection until theService Commencement Date (the Contract Transition Period):
Operational Phase – the delivery of the Service (Service Delivery), and finally;
Exit Phase – the exit arrangements on termination of the currentContract (Exit) that will run concurrently with the final phase of Service Delivery
1.1.3 The three phases require different management structures. The Provider(s) will be expected to ensure that the appropriate skill sets are applied to each phase. For example, the composition of teams will require an understanding of project management during the Contract Transition Period and Exit in order to ensure that deliverables and milestones are met, whilst Patient focus, contract management and commercial skills will be required during the Service Delivery phase.
1.1.4 The awarded bidder has submitted as part of its Final Tender a detailed mobilisation plan and associated documentation. This plan and documentation will form the basis of discussions during the mobilisation period, and any significant variance from the submitted plans will be escalated to the Mobilisation, Transition and Integration Board.
2.2 Contract Transition Period
2.2.1 The Provider must provide the detailed Contract Transition Plans that cover all aspects of their proposed Contract Transition Period.
12
2.2.2 During the Contract Transition Period, the CCG will undertake the following activities:
Creating as Mobilisation Board. The CCG and Awarded bidder(s) will establish a Mobilisation Board with supporting governance structures. The Mobilisation Board membership comprises representatives from the CCG, Local Authority, NHS England and Awarded bidder. The Mobilisation Board’s role is to monitor the progress of both the Provider(s) and the relevant members of the local health economy against the integrated transition plan. The Mobilisation Board will operate to enable stakeholders to raise local issues arising out of the Contract.
Creating an Integrated Transition Plan. The CCG will work with the relevant members and the Awarded bidder(s) to ensure that all relevant members are incorporated into the Provider(s) Transition Plan to form and overall, integrated plan (Integrated Transition Plan). This Plan defines the required deliverables, timescales and resources for the Contract Transition Period and helps to ensure that the Services are ready to start on the Service Commencement Date. This includes identification and development of critical interfaces to integrate the Services into the local health economy.
Creating joint workstream teams. The Integrated Transition Plan is organised
by the appropriate workstream. The CCG will work with the relevant members and the Provider(s) to form joint workstream teams to deliver the activities identified in the Integrated Transition Plan. The workstream leads report progress to the Mobilisation Board.
2.2.3 The Contract Transition Plan must cover the key tasks the Provider(s) will complete
during the Contract Transition Period and clearly highlight key milestones such as the following:
All Conditions Precedents are satisfied;
Phased works and reconfiguration is complete and/or all work and reconfiguration
is complete;
Phased logistics is complete and/or all logistics is operational;
All staff in place to satisfy Service Commencement and/or all staff in place as per workforce plan;
IM&T ready for phased operations and/or full service commencement;
Communications Plan delivered, and;
Full Service Commencement Date
2.2.4 Key tasks and milestones will be assigned to each of the following workstreams:
Clinical / workforce / quality
13
IM&T and Finances
Estates
2.2.5 The Provider(s) must ensure that there is sufficient corporate human resource available during the Contract Transition Period. Bidders must provide a detailed plan that clearly identifies the Provider’s human resources during the Contract Transition Period, with a supporting narrative.
2.2.6 The appropriate management of risk is key strategy in avoiding Adverse Incidents and achieving continuity of the Services. The Provider(s) must submit a risk strategy which identifies, as a minimum, ownership of risk, escalation and governance.
2.2.7 The Provider(s) must identify both opportunities and risks they believe exist. An assessment of the magnitude of these opportunities and risks and how they plan to manage them effectively, including timeframes and resources, is required.
2.2.8 Agree any variation to plans that arise through unforeseen issues during the transition period.
2.3 Communications Plan and Stakeholder Engagement
2.3.1 The Mobilisation Plan must incorporate a suitable and appropriate Communications Plan that details Provider(s) intentions to manage communications and stakeholder engagement.
2.4 Operational and Business Continuity Plans 2.4.1 Provider(s) must develop and submit a suitable and appropriate operational plan that
details the Provider(s) arrangements for business continuity in the event of an Incident or Emergency that impacts on the Provider(s) ability to deliver the Services and in the event of a Major Incident. Bidders must give particular attention to the following workstreams:
Clinical;
Workforce;
IM&T, and;
Estates
2.5 Exit Management
2.5.1 During the Exit Phase of the existing Contract, the CCG will undertake the following key activities:
14
Creating an Integrated Exit Plan from existing services and ensuring the Commissioners’ deliverables are incorporated into the Provider(s) Exit Plan to form an overall, Integrated Exit Plan. This Plan defines the required deliverables, timescales and resources for the Exit phase and ensures that the Provider(s) is ready to end its provision of the Services in a manner that is clinically safe and handover to an incoming Service Provider on the expiry date or date of earlier termination, and;
Creating joint workstream teams. The Integrated Exit Plan is organised by the
appropriate workstream. The CCG will work with the Provider(s) to form joint workstream teams to deliver the activities identified in the Integrated Exit Plan. The workstream leads report progress to the Exit Project Board.
3.1 Approvals
3.1.1 Contract signature is subject to the approval of the Mobilisation Board. Until all necessary approvals are obtained, the Contract will not be executed.
5.1 Contract Award and Signature
5.1.1 The Contract will take the form of the NHS Standard Contract
5.1.2 No offer or bid is deemed accepted until the relevant contractual documents have been duly signed on behalf of the Provider, the Awarded bidder(s) and all other relevant parties and declared unconditional. No dialogue or communication with the Provider whether prior, during or subsequent to the submission of any bid imply acceptance of any offer or constitute an indication that the Bidder will be awarded the Contract. Only the express terms of any written Contract(s) which is finally agreed and signed for and on behalf of the relevant parties and which is duly declared unconditional shall have any contractual effect.
5.1.3 It is intended that the Contract will be signed within three months of appointment of Awarded bidder(s). Mobilisation will commence on the Contract Signature Date and will end at full service commencement. The Awarded bidder(s) is at liberty to commence Mobilisation prior to the Contract Signature Date, but this will be at the Awarded bidder(s) risk and cost.
6.1 Expiration of Bids
6.1.1 Bidders will be required to ensure that their bids do not expire and are capable of being accepted until the completion of the Project and Service Commencement.
15
Page 1 of 2
Appendix 416
Page 2 of 2
17
Appendix 5 – Public Service (Social Value) Act 2012
1 Purpose
The purpose of this paper is to demonstrate the CCG’s compliance with the Public Service (Social Value) Act 2012. This is with regard the commissioning of Community Health Services.
2 Background
The Public Services (Social Value) Act 2012 (hereafter ‘the Act’) places a requirement on the CCG to consider the economic, environmental and social benefits of its approach to procurement. The CCG also has to consider whether it should consult on these issues. The Act does not prescribe how the results of the consideration of these impacts should shape any procurement which is undertaken. It does enable the service user and carer, and wider stakeholder, perspectives on potential services to be taken into account in the development of outcomes and specifications for the services.
3 Compliance with the Act
The CCG consulted widely and extensively on the services. This consultation, in association with the CCG’s other pre-procurement activity, covered the requirements of the Act in a proportionate manner. The CCG set up various engagement events across North Somerset to find out how service users, Carers, GP’s and other key stakeholders viewed the provision of services. A significant number of events were held, and people involved in this engagement. This report was concluded in the May of 2015 and fed back to all interested parties. New services were created through the engagement process, services that would directly impact the social, economic and environmental wellbeing of the local population. The received feedback was also incorporated into final tender submissions in July 2015. In terms of the management of the pre-procurement process, it was led operationally by a multi-agency Programme Board that included representation from the Local Authority (Public Health), an organisation with clear interests in the social, economic and environmental wellbeing of the local population beyond the remit of the NHS. Service users and carers were also involved at the Programme Board level (through Healthwatch) to ensure the local population’s wellbeing was being fully considered. Within the procurement, the use of social capital was included as an evaluated element of every bid, and bidders were specifically tested on it. Tender evaluation panel members were drawn from a number of stakeholder organisations with an interest in social, economic or environmental wellbeing, and those factors were generally brought in to the evaluation of bids.
18

Evaluators were drawn from the CCG, the Local Authority, Public Health, service users, carers and other independent experts (for example with regard Workforce).
19
Appendix 6
Equality Impact Assessment
on the procurement of
Community Health Services
in North Somerset
Authors Peter Purdie, Project Manager Julie Kell, Head of Joint Commissioning
Approved By Project Board
Ratification Date August 2015
Review Date This document constitutes the EIA at the mid-point of the procurement project. This will be revised and re-published following the consultation period in the first quarter of 2015.
20
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
2
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Contents
Step Title Page
Front Sheet 3
1 Getting started 5
2 Establishing relevance to the public sector equality duty
7
3 Scoping the equality impact assessment 9
4 Analysing equality information 21
5 Monitoring and review 25
6 Publication 25
Appendices:
1. Action Plan
2. Highlights of the Equality Act 2010
26
21
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
3
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
FRONT SHEET
Name of the project being assessed:
Procurement of Community Services in North Somerset Is this a new or existing project? Existing
State the context for this EIA (eg service redesign, service commissioning, a QIPP programme, policy or strategy development)
Service commissioning
On which protected characteristics has this Equality Impact Assessment been
carried out?
Race Y Disability Y Sex Y Religion or Belief
Y Marriage/ Civil Partnership
Y
Age Y Sexual Orientation
Y Gender reassignment
Y Pregnancy and Maternity
Y Health impact
Y
Name of person carrying out this Equality Impact Assessment
Peter Purdie, Project Manager South, Central, and West CSU
Senior manager responsible for this project
Julie Kell, Head of Joint Commissioning North Somerset Clinical Commissioning Group
Signature
Date July 2015
22
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
4
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Names and roles of other people involved in carrying out this Equality Impact Assessment (ie the Steering Group):
Project Senior Responsible Officer
Jeanette George, Chief Operating Officer, North Somerset CCG Project Director
Julie Kell, Head of Joint Commissioning, North Somerset CCG Project Board
Faye Robinson, Director of Procurement, South, Central, and West CSU Eileen Jacques, Chief Officer, Healthwatch North Somerset Miriam Ainsworth, Clinical Lead for Community and Long Term Conditions,
North Somerset CCG John Wilkinson, Head of Transformation and Policy, North Somerset Council Gerald Hunt, Assistant Director - Finance, Resources & Strategic
Commissioning, North Somerset Council James Bolt, Head of Public Health Commissioning, NHS England Mary Adams, Patient and Public Engagement Manager,
North Somerset CCG Mike Vaughton, Chief Finance Officer, North Somerset CCG
Subject matter expert
David Harris, Senior Equality Advisor, South, Central, and West CSU
Members of related sub-groups / working groups:
Communications and engagement group Advisory group
23
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
5
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Step 1: Getting started
Brief description of the project
“We know that for people to be truly healthy it is not only the quality of healthcare services that matters. That is why we are committed to working together with our whole population, individuals, and other organisations to create the healthiest communities.”
North Somerset CCG vision statement
North Somerset Clinical Commissioning Group (North Somerset CCG) is the lead partner in the project to jointly re-commission Community Health Services for the people of North Somerset. North Somerset CCG, as the lead commissioning partner, also has responsibility for leading the engagement, involvement, and consultation processes. The other partner organisations undertaking the project comprise North Somerset Council (“the Local Authority”) and the NHS England Area Team.
Document glossary We have referenced the following documents to conduct this assessment:
The North Somerset Joint Strategic Needs Assessment The project Stakeholder Engagement Report The project Stakeholder Consultation Report The project Memorandum of Information The project draft Outcomes Framework The NHS standard contract
In addition, the assessment has been carried out in consultation with the Senior Equalities Advisor, Davis Harris. Who is responsible for implementing, monitoring, and/or developing the project?
The Project Board decides the direction of travel of the project and takes overall responsibility for its success or failure. This means agreeing what will be delivered by when with the Project Owner (Chief Operating Officer, North Somerset CCG), as well as the Project Manager and the Clinical Lead. It is also responsible for securing the resources the Project Manager needs to deliver the project.
The membership of the Project Board is:
24
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
6
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Project Senior Responsible Officer
Chief Operating Officer, North Somerset CCG Project Director
Head of Joint Commissioning, North Somerset CCG Project Board
Director of Procurement, South, Central, and West CSU Chief Officer, Healthwatch North Somerset Clinical Lead for Community and Long Term Conditions,
North Somerset CCG Head of Transformation and Policy, North Somerset Council Assistant Director - Finance, Resources & Strategic Commissioning, North
Somerset Council Head of Public Health Commissioning, NHS England Patient and Public Engagement Manager, North Somerset CCG Chief Finance Officer, North Somerset CCG
25
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
7
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Step 2: Establishing relevance to the public sector equality duty
Does the project affect service users, employees or the wider community and,
therefore, potentially have a significant effect in terms of equality?
Yes.
The project will result in the award of a contract to a provider of community health services to the population of North Somerset.
Is it a major project, significantly affecting how the commissioners operate in terms of equality?
No.
The commissioning organisations routinely give due regard to equality and diversity. Their approaches are in the public domain and can be found here:
Organisation Link to equalities information
North Somerset CCG www.northsomersetccg.nhs.uk/about-us/edhr/equality-and-diversity
North Somerset Council www.n-somerset.gov.uk/community/equalities/Pages/Equalities
NHS England www.england.nhs.uk/about/equality
The successful conclusion of this project will result in the award of a contract to a provider of community services and will not have a significant effect on the operation of the commissioning organisations in terms of equality and diversity.
Will it have a significant effect on how other organisations operate in terms of equality (such as service providers or contractors)?
Yes.
The Memorandum of Information states that we expect the provider to deliver a system focused on people and communities which reduces health and social care inequalities by working in partnership.
The project has been designed to generate innovative new service delivery models to benefit the population served. While the specifics of these models will not be known until the end of the process, the outcomes required of providers are specified. This outcomes specification was developed through a robust process of engagement and involvement and constituted one of the three strands of the consultation.
Does or could the project affect different “protected groups” differently?
Yes.
26
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
8
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
As identified in the North Somerset Joint Strategic Needs Assessment (JSNA), our population profile comprises people who are ‘seldom heard from’; this includes, for example, looked after children, people from Gypsy and Traveller communities, and people who are socially isolated.
These people usually have a number of ‘protected characteristics’ that we need to attend to and consider from an equality perspective within both our engagement plans and the services which will be delivered. We recognise that we cannot rely on a ‘blanket’ approach to engagement, involvement, and consultation, and must tailor and target this work appropriately and proportionately. The diversity of local people’s views is especially important for services that are universal and available to all.
In a previous procurement exercise in another geographical area, some smaller Voluntary and Community Sector organisations providing elements of the existing service were unable to submit a bid, as the services were bundled for re-procurement. This resulted in a loss of income which had the potential to cause a negative impact on the sustainability of services offered by these organisations to the protected groups they served. In this project, to avoid this happening, all interested provider organisations were invited to attend bidder events prior to the commencement of the procurement, which provided a forum for partnerships to be formed for the purpose of submitting a joint bid.
Does it relate to an area with known inequalities?
Yes. Our goal is to improve the health and wellbeing of the people of North Somerset and to provide them with effective, accessible, and modern services. We also aim to tackle health inequalities, especially those based on the characteristics which are protected from discrimination by the Equality Act 2010.
Children from deprived families are far more likely to be killed, disabled or seriously injured in preventable accidents There is an interplay between ethnicity and deprivation. Compared to white families, families from certain black and minority ethnic communities are over-represented on several indices of deprivation linked to childhood death and serious injury in preventable accidents.
Making the Link topic briefing1
Conclusion
This project is relevant to the public sector equality duty and will proceed to a full assessment, as detailed below.
1 http://www.makingthelink.net/topic-briefings/inequalities-and-deprivation
27
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
9
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Step 3: Scoping the equality impact assessment
Note on the assessing the equality impact of the project against the equality impact of the procured service
The project will procure a provider of community services for the population of North Somerset. An assessment of the procurement project would assess the equality impact of conducting the procurement exercise. However, as the exercise will result in the delivery of services, a decision has been made to assess the equality impact of the resulting service model, and how the commissioners will fulfill their Public Sector Equality Duty in this regard.
What are the aims of the project?
In the NHS Operating Framework, published in late June 2010, the Department of Health confirmed its expectation that, in delivering the transformation of community services, all services provided by Primary Care Trusts (PCTs) should be transferred out of PCT’s by 1 April 2011. To meet this expectation, NHS North Somerset transferred its Community Health Services arm to North Somerset Community Partnership (NSCP). The current four-year contract for community services in North Somerset expires on 31 March 2015.
In August 2013, the North Somerset Clinical Commissioning Leadership Group reached a decision to extend the contract for a period of one year to March 2016 to allow time to conduct a procurement exercise to appoint a suitable provider.
We have worked to ensure that we have used the views of patients and the public to shape our plans.
The project looks to develop and implement national policies for local benefit taking a whole system approach across health and social care.
Service users’ and carers’ interests are paramount
Proposals must reduce age discrimination and develop functional need-specific services as opposed to age-specific.
Proposals must enable joined up health and social care service , third / voluntary sector provision
Report on procurement of community services to the Health Overview and Scrutiny Panel, April 2014
28
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
10
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
We want to work with a provider who recognises the need to move away from simply commissioning quantities of activity and towards measuring outcomes as defined by the patient or service user themselves. We want to change the way that we jointly commission services to put the patient first.
We expect the provider to deliver the following objectives:
A system which
is focused on people and communities reduces urgent and emergency care, and works together to get people back home again
The services being procured for adults and children include, but are not limited to:
All community-based services, including social care services provided or commissioned as part of integrated services
Both mental and physical community care Services for people with dementia Midwife-led birthing centre (subject to confirmation) Health visitors School nurses Children’s Community Therapy Services Childhood immunisations (school based) Specialist community services for adults, for example, Parkinson’s disease
services
Which aspects are most relevant to equality?
Access to services can vary for children and young people, people with mental impairment, and members of certain national and ethnic groups.
“Coming from a black or minority ethnic (BME) background can impact negatively on your health. This might be because of passive or active discrimination or may be linked to other factors which can include deprivation, poverty, and/or from a genetic predisposition to certain illnesses. Overall this means that people from some BME backgrounds have poorer health and shorter life expectancy than the general population.”
North Somerset Joint Strategic Needs Assessment
Staff delivering services need to be aware of, sensitive to, and responsive to individual requirements related to faith and cultural norms.
29
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
11
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
What is the intended benefit to patients, communities and employees, with reference to all the nine characteristics protected by the Equality Act 2010?
For each of the protected characteristics, the intended benefit for people, communities and employees is to eliminate discrimination, harassment, and victimisation, to advance equality of opportunity and to foster good relations.
Further intended benefits, particular to each characteristic, are:
1. Age. To improve transition from child to adult services. To provide services designed to address the needs of the frail elderly.
2. Disability including physical and mental impairment. To help people with a learning disability to have the same chances as anyone else to lead a full and interesting life, and to improve their ability to access services.
3. Gender re-assignment. No further benefits specific to this group. 4. Marriage and civil partnership. No further benefits specific to this group. 5. Pregnancy and maternity. To increase the choice of birth settings for
pregnant women and their partners. 6. Race, including nationality, ethnicity and cultural norms. To improve
access to services and service experiences for disadvantaged groups. 7. Religion or belief. To maximise service responsiveness to a diverse range of
needs related to faith. 8. Sex. To improve access to single sex accommodation for all inpatients. 9. Sexual orientation. No further benefits specific to this group.
Which protected groups and which parts of the public sector equality duty is the project relevant to (see Appendix 2)?
The CCG meets its public sector equality duty in relation to Community Health Services in a variety of ways, and not solely via this document.
Beyond the generic consideration of the Public Sector Equality Duty, this project has particular relevance to the following protected characteristics:
1. Age. 2. Disability including physical and mental impairment. 5. Pregnancy and maternity. 6. Race including nationality, ethnicity, and cultural norms. 7. Religion and belief. 8. Sex
All parts of the public sector equality duty are relevant to this project. The context of the application of the duty is to give due regard to the need to:
a) eliminate discrimination, harassment, victimisation and any other conduct that is prohibited by or under this Act;
this relates to the provider organisation’s duty to manage their staff and create an inclusive and supportive service delivery environment
it is further supported by the use of the NHS standard contract
30
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
12
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
b) advance equality of opportunity between persons who share a relevant
protected characteristic and persons who do not share it; the provider organisations can comply with the duty by advancing
equality of opportunity in regard of both access to services, and in their employment of staff
the commissioners’ duty lies in designing the procurement process to enhance the success of this strand of the duty, for example, encouraging organisations which are particularly relevant to the protected groups, to become part of the bidding consortia, such as voluntary sector organisations with expertise in delivering appropriate services to a particular protected group
c) foster good relations between persons who share a relevant protected characteristic and persons who do not share it.
the provider organisations can comply with the duty by fostering good relations between staff members and between staff members and people using the services
once again, the commissioners’ duty lies in designing the procurement process to enhance the success of this part of the duty
Performance of the commissioners’ duty is demonstrated in the service outcomes framework for the project, which specifies that within the selected provider organisation:
“Staff are supported and trained to understand and take into account a diversity of social and cultural norms, values and beliefs in their decision making and delivery of care and support.”
Draft outcomes framework (ITN 2)
In addition, the successful bidder will be commissioned using the NHS Standard Contract 2016-17. The current version of the contract (2015-16) contains the following conditions:
Service Condition SC13: Equity of Access, Equality and Non-Discrimination 13.1 The Parties must not discriminate between or against Service Users, Carers or Legal Guardians on the grounds of age, disability, marriage or civil partnership, pregnancy or maternity, race, religion or belief, sex, sexual orientation, gender reassignment, or any other non-medical characteristics, except as permitted by the Law. 13.2 The Provider must provide appropriate assistance and make reasonable adjustments for Service Users, Carers and Legal Guardians who do not speak, read or write English or who have communication difficulties (including hearing, oral or learning impairments). The Provider must carry out an annual audit of its
31
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
13
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
compliance with this obligation and must demonstrate at Review Meetings the extent to which Service improvements have been made as a result. 13.3 In performing its obligations under this Contract the Provider must comply with the obligations contained in section 149 of the Equality Act 2010 and section 6 of the Human Rights Act 1998. If the Provider is not a public authority for the purposes of those sections it must comply with them as if it were. 13.4 In consultation with the Co-ordinating Commissioner, and on reasonable request, the Provider must provide a plan or plans setting out how it will comply with its obligations under SC13.3. If the Provider has already produced such a plan in order to comply with the Law, the Provider may submit that plan to the Co-ordinating Commissioner in order to comply with this SC13.4. 13.5 The Provider must
13.5.1 implement EDS2; and 13.5.2 implement the National Workforce Race Equality Standard and submit an annual report to the Co-ordinating Commissioner on its progress in implementing that standard.
Service Condition SC14: Pastoral, Spiritual and Cultural Care 14.1 The Provider must take account of the spiritual, religious, pastoral and cultural needs of Service Users and must liaise with the relevant authorities as appropriate in each case. General Condition GC5: Staff
5.3 The Provider must ensure that all Staff:
5.3.5 are aware of and respect equality and human rights of colleagues, Service Users, Carers and the public.
32
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
14
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Evidence about how the project actually operates
What equality information is available about the relevant protected groups?
This section describes the scope of the available information. The equalities profile detail follows shortly after.
The North Somerset CCG Equality Information Statement 2014 contains demographic profiles related to each of the protected characteristics in North Somerset.
The North Somerset Joint Strategic Needs Assessment (JSNA) contains demographic information relating to age, gender, and race, including nationality and ethnicity.
Very little published information is available which describes the profile of patients and service users. It is, therefore, not possible to comment definitively on the equity of access to current services and service experiences. Low take up of services by a particular population group could indicate that this group is in less need of the services; or it could mean that patients are choosing to access the relevant services elsewhere; or it could be that patients are experiencing barriers to the service, resulting in discriminatory outcomes. One exception to the lack of published information is an equality impact assessment on the commissioning of future clinical services at Clevedon Community Hospital carried out in 20142. This included an analysis of the age, sex and ethnic origin of inpatients and outpatients.
Summarise the key findings of this evidence in relation to actually or potentially discriminatory outcomes
The equality impact assessment into the commissioning of services at the community hospital highlighted the following:
Age
As expected, older people, aged 65+, are the main users of both inpatient and outpatient services. This is particularly so for inpatients, where 96.5% of patients are aged 65+. The main explanation is that the hospital does not provide these services to children (although 8 outpatients were children). Furthermore, it could partly be because people in this older age group are more likely to experience the types of illness and disease which require outpatient care and hospital admission.
2 Available at https://www.northsomersetccg.nhs.uk/about-us/edhr/equality-impact-assessments-eia/ (as at 27 July 2015)
33
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
15
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
This finding reinforces the conclusion that existing or future services need to consider the additional needs of the older population which can impact on an individual’s access to services and experience of services. Such needs might include mobility, visual and hearing impairment, dementia and social isolation.
Sex
Men are significantly underrepresented in inpatient services (42% compared to 58% women) and even more underrepresented in outpatient services (36% compared to 74%). Some underrepresentation is to be expected, since, within the older age group, men are also underrepresented in the general population. However, it is also possible that older men are experiencing some barriers to accessing outpatient services in particular; or are seeking medical services less often than older women.
Ethnic Group
Whilst a full data set was collected at the community hospital with regard to age and sex for ethnic group, information was not available for 14% of inpatients or for 46% of outpatients. This means that any attempt to compare patient data with the local population profile should be treated with extreme caution. For inpatients, the proportion of patients for whom ethnic group data is unknown had shrunk significantly to 1.7% by 2013/14 (year to date), which is a very encouraging trend. Therefore, the following commentary relates only to inpatient data for 2013/14 (year to date.
Ethnic group figures for this period show that White British patients are slightly overrepresented when compared to the local adult population (97% vs 94.4%). Other ethnic groups appear to be significantly underrepresented at 1.8% of total inpatients, compared to 5.6% of the adult population.
The main factor to consider in interpreting these figures is that older people, aged 65+, form the main body of inpatients. The proportion of this age group in the general population who are not White British is likely to be much lower than 5.6%. However, 1.8% represents an extremely low take-up of inpatient services by minority ethnic groups. This is something which the service commissioner and provider should be looking to investigate for inpatient, outpatient and diagnostics services.
Equality impact assessment on the commissioning of future clinical services at Clevedon Community Hospital
What is the equality profile of the population and/or workforce that is intended to benefit from the project?
The project will result in the provision of Community Services in North Somerset which are available to any member of the public. The equality profile of the population is as follows for age, disability, and race:
Age The age breakdowns from the 2011 Census for North Somerset are:
34
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
16
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Aged 0-14 years – 17% Aged 15-64 years - 62% Aged 65+ years – 21%
In 2011, the proportion of people in North Somerset aged 65+ was 21%, compared to 19.6% in the South West and 16.4% nationally. Source: CCG equality statement The age structure in North Somerset was older with fewer young dependents and people aged under 40 years. Compared to the national average, North Somerset has a larger proportion of older people. One in five people are aged over 65 years compared to 16% in England and Wales. In contrast, fewer people are aged between 20 and 39 years old (21% of the population compared to 27% in England and Wales) Source: JSNA
Disability including physical or sensory impairment, mental health problems, learning difficulties and long term conditions Disability The 2011 Census records disability as whether or not activity is limited. For North Somerset, the following information is provided; Activity limited a lot – 17,335 (8.6%) Activity limited a little – 21,405 (10.6%) Activity not limited – 163,826 (80.9%) Source: CCG equality information statement Mental health In 2010/11 North Somerset had a higher level of GP diagnosed depression (16.5%) than England (11.7%). Prevalence had increased by 10.8% over the previous 4 years. Modelled data, which takes into account the population characteristics, indicates that North Somerset should have 7% fewer common mental health problems than the national average. The reason for this discrepancy is unclear. Rates of serious mental health problems (0.8%) recorded in GP practices were similar to the England average (0.8%) and were higher in more deprived areas. The number of cases rose by 14% in the previous 5 years. An estimated 3,420 people in North Somerset had dementia although GP practices only recorded 1,415 patients with dementia. The GP recorded prevalence of dementia (0.7%) was higher than England (0.5%), in part reflecting the relatively elderly population. Source: JSNA Learning difficulties (or learning disabilities) People with learning disabilities have poorer health than their non-disabled peers. They have higher levels of mental illness, chronic health problems, epilepsy, and sensory problems. In 2011, the life expectancy of people with learning disabilities in North Somerset was 64 years, much lower than the North Somerset average of all residents of 79.9 for men and 83.9 for women.
35
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
17
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Nationally, the number of adults with learning disabilities was increasing in 2011 and was predicted to increase by 1% each year for the following 15 years. The prevalence of learning disabilities recorded by GP practices (0.48%) was higher than the average for England (0.45%) and had increased over the previous few years. The prevalence of children reported as having learning disabilities in North Somerset (12.3 per 1000) was much lower than the national rate (24.6 per 1000) and had declined over time. People with learning disabilities are more likely to be exposed to the social determinants of poor health such as poverty, poor housing conditions, unemployment, discrimination, and social isolation. Source: JSNA
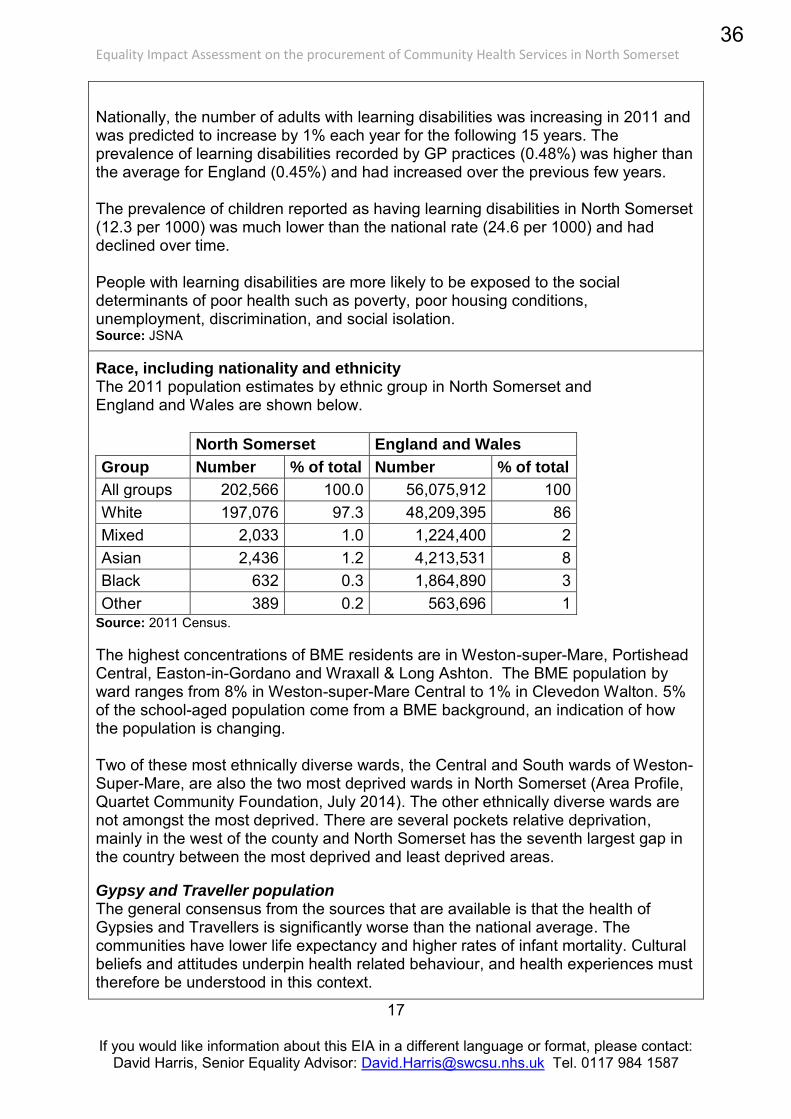
Race, including nationality and ethnicity The 2011 population estimates by ethnic group in North Somerset and England and Wales are shown below. North Somerset England and Wales
Group Number % of total Number % of total
All groups 202,566 100.0 56,075,912 100 White 197,076 97.3 48,209,395 86 Mixed 2,033 1.0 1,224,400 2 Asian 2,436 1.2 4,213,531 8 Black 632 0.3 1,864,890 3 Other 389 0.2 563,696 1
Source: 2011 Census. The highest concentrations of BME residents are in Weston-super-Mare, Portishead Central, Easton-in-Gordano and Wraxall & Long Ashton. The BME population by ward ranges from 8% in Weston-super-Mare Central to 1% in Clevedon Walton. 5% of the school-aged population come from a BME background, an indication of how the population is changing. Two of these most ethnically diverse wards, the Central and South wards of Weston-Super-Mare, are also the two most deprived wards in North Somerset (Area Profile, Quartet Community Foundation, July 2014). The other ethnically diverse wards are not amongst the most deprived. There are several pockets relative deprivation, mainly in the west of the county and North Somerset has the seventh largest gap in the country between the most deprived and least deprived areas. Gypsy and Traveller population The general consensus from the sources that are available is that the health of Gypsies and Travellers is significantly worse than the national average. The communities have lower life expectancy and higher rates of infant mortality. Cultural beliefs and attitudes underpin health related behaviour, and health experiences must therefore be understood in this context.
36
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
18
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
There have however also been reports of a lower prevalence of diabetes, stroke and cancer in the Gypsy and Traveller population. In addition, aspects of the close social network and cohesion within the community will have benefits to health. Recent research confirms the need to deliver culturally appropriate services for the community. Conclusions include:
“A lack of trust and understanding between Gypsy and Traveller communities, their neighbours and mainstream service providers was identified as a factor in many of the problems.”
“Some Gypsies & Travellers are unable or unwilling to engage with public services, contributing to the poor outcomes highlighted in this report. In turn some services are not appropriately equipped to engage with Gypsies and Travellers and do not always make efforts to reach out to them.”
North Somerset Council commissioned a health needs assessment from Buckinghamshire University to investigate the health needs of Gypsies and Travellers in North Somerset. The findings of this assessment can be found in the North Somerset Joint Strategic Needs Assessment
What are your information gaps?
At time of publication, it had not been possible to gather any data on the equalities profile of users of the existing services, apart from the limited analysis carried out on the age, sex and ethnic origin of a community hospital’s patients in 2014.
What engagement and involvement activities have already been undertaken regarding this project?
The Stakeholder Engagement Report3 - describes the arrangements that North Somerset CCG made for engaging and involving public stakeholders from March to May 2014, prior to the start of the procurement exercise.
Public stakeholders here means adults, children, young people, parents and carers and professional stakeholders from health, social care, education and the voluntary and independent sectors.
The report provides a summary of the feedback that people have contributed, and an overview of the next phases of involvement as the procurement process evolves.
Members of the following groups participated in the engagement exercise:
Black and Minority Ethnic (BME) Network Faithnet Lesbian, Gay, Bisexual and Transgender Forum Mental Health Partnership Board
3 Available at: https://www.northsomersetccg.nhs.uk/get-involved/changes-community-health-services/
37
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
19
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Older People Champions Group Senior Community Links North/South Patient participation groups Care home coffee morning Healthwatch North Somerset Voluntary Action North Somerset (VANS) Health and Well Being Forum Clevedon Hospital League of Friends Learning Disabilities Partnership Improving Outcomes for Older People Carers Strategy Group Health Overview and Scrutiny Panel (North Somerset Council) Local parish councils GP Forum
These groups have a particular interest in the following protected characteristics, presenting the opportunity for relevant issues to be raised and considered:
Race Religion and Belief Sexual Orientation Disability (mental health, learning difficulties and long term conditions) Gender Reassignment, and Age (older people).
Healthwatch North Somerset have been involved with the procurement at all stages and a panel of lay members have been a significant component of the wider panel of markers assessing the bidder submissions. The draft Outcomes Framework has been reviewed at a focus group run at the Healthy-Living Centre, within one of the more-deprived areas in North Somerset, to involve members of this seldom-heard-from community. A stakeholder engagement online survey was carried out, which included questions on the respondents’ age, disability, sex, and sexual orientation. There were a total of 46 responses to the survey, of which, 29 contained detailed comments. However, it is was not possible to link the recorded protected characteristics to the comments, so equalities analysis of the responses was not possible.
State the key outcomes of the engagement and involvement
The feedback from the engagement events was analysed and summarised in the Stakeholder Engagement Report, and the emergent themes were around access, integration, and service development.
The “Response to Stakeholder Engagement” report identifies how this feedback was incorporated into the Memorandum of Information, specifically influencing the project objectives and critical success factors.
38
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
20
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
In addition, following the engagement exercise, and the focus group examination of the draft outcomes framework, an additional outcome requirement was added to the draft framework as a result of the feedback received. While the conditions of the contract described above in the box on pages 12 and 13 require the provider to comply with their public sector equality duty, it was decided to make this explicit within the draft outcomes framework. The following outcome was added:
Overarching domain A: Ensure people have an excellent and equitable experience of care and support with care organised around the individual
Outcome A.1 People and carers have an equally excellent experience of care and support, regardless of protected characteristics
Detailed outcome A.1.1 There are no unreasonable differentials in reported experience or outcomes related to a protected characteristic group.
Which additional groups could usefully be engaged?
All groups listed above which were involved in the engagement, were invited to take part in the consultation exercise, in addition to representative groups who did not take part in the engagement.
Although the targeted engagement and involvement activities have covered most of the protected characteristics, a key risk is that, within broad categories like “Race” or “Sexual Orientation” some particular characteristics may not have been adequately considered. Furthermore, the following protected characteristics appear to have featured less prominently. However, for some of them, it is likely that particular issues have had a good chance of being raised in the activities which have already taken place:
Age (children and young people) Disability (physical and sensory impairment) Marriage and Civil Partnership Sex Pregnancy and Maternity
To minimise this risk, the design of the consultation phase considered how best to secure inclusion/representation around the following protected characteristics:
Age (children and young people) Disability (deaf, blind) Race (Gypsies and Travellers)
39
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
21
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
State the key outcomes of the consultation
The Consultation Feedback Report4 - describes the arrangements that North Somerset CCG made for consulting with public stakeholders from February to April 2015, prior to the call for final tenders from the remaining bidders for the contract..
Public stakeholders here means adults, children, young people, parents and carers and professional stakeholders from health, social care, education and the voluntary and independent sectors.
The consultation techniques and methods described in section 8 of the report describe how we consulted with users of North Somerset’s children’s centres, readers of the local authority schools’ newsletter, Baytree Special School, Weston College, the Gypsies and Travellers Strategic Group, and the North Somerset Black and Minority Ethnic Network.
The feedback received during the consultation phase was themed, and the draft outcomes framework was reviewed to ensure that all issues and concerns raised were addressed by the outcomes specification.
4 Available at: https://www.northsomersetccg.nhs.uk/get-involved/changes-community-health-services/
40
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
22
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Step 4: Analysing equality information
Equality impact assessment is not simply about identifying and removing negative effects or discrimination, but it is also an opportunity to identify ways to advance equality of opportunity and to foster good relations.
Using information to understand the effect on equality
Assessment of the outcomes of the project
In setting out the CCG’s ambitions for Community Health Services, a set of service outcomes have been developed by the project team. This team includes Healthwatch and commissioning experts in the areas of older people, child and adolescent services, mental health services, patient and public engagement, and equalities.
The outcomes have been developed in the light of the feedback from the extensive engagement exercise which was conducted prior to initiating the procurement exercise.
The project is looking for the bidders to develop service models to deliver these outcomes, and the models will be assessed accordingly, taking into account consideration of the potential for discrimination identified above.
The successful bidder will be bound by the conditions of the NHS Standard Contract. Implementing the Equality Delivery System (EDS2) and the NHS Workforce Race Equality Standard, are now requirements for all providers.
Assessment of the legality of the project (see Appendix 2)
The methodology and approaches described above are expected to fulfill the Commissioners Public Sector Equality Duty.
41
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
23
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
How does the project help to deliver the organisation’s wider business
objectives?
We expect the provider to deliver the following objectives:
A system focused on people and communities Reductions in urgent and emergency care Working together to get people back home again
Furthermore, North Somerset CCG’s business objectives reflect the principles and requirements of:
the NHS Constitution the NHS Outcomes Framework CQC Essential Standards for registered providers
The NHS Equality Delivery System (EDS2) is a tool which helps Commissioners and providers to deliver against these principles and requirements. Since implementing EDS2 has been a requirement of the NHS Standard Contract from 2015-16 onwards, the providers of Community Health Services in North Somerset will be actively engaged in meeting the business objectives of the CCG and the wider NHS.
The CCG has a key role in monitoring the compliance of providers with those principles and requirements which relate to equality and diversity, such as the requirement to implement EDS2 and to comply with the public sector Equality Duty.
Are there any risks associated with the implementation of the project, which could detract from its effectiveness in helping the NHS to comply with equality legislation and improve its performance for patients, carers and employees?
Any risks will be identified and managed through contract performance management of both the conditions around EDS2 and WRES, and of Service Outcome A.1.1
These are described above on pages 12-13, and page 20 respectively.
Health Impact
Identify the effect of the project on the physical and mental health of
employees and the wider community from any information that is available.
The service outcomes have been developed to improve the health outcomes of the population of North Somerset.
Recommendations
What steps will you take in response to the findings of your impact
assessment?
42
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
24
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
1. No major change – Your impact assessment demonstrates that the project is robust and the evidence shows no potential for discrimination and that you have taken all appropriate opportunities to advance equality and foster good relations between groups.
2. Adjust the project – This involves taking steps to remove barriers or to better advance equality. It can mean introducing measures to mitigate the potential effect.
3. Continue the project – This means adopting your proposals, despite any
adverse effect or missed opportunities to advance equality, provided you
have satisfied yourself that it does not unlawfully discriminate.
4. Stop and remove the project – If there are adverse effects that are not justified and cannot be mitigated, you will want to consider stopping the project altogether. If a project shows unlawful discrimination it must be removed or changed.
Action planning
Developing an action plan at this stage will help you to implement your decisions and recommendations (see Appendix 1). Be clear about who, at senior management level, is responsible for overseeing implementation of the action plan.
43
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
25
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Step 5: Monitoring and review
How will you review the actual effects of the project after implementation?
Appendix 1 contains the monitoring and review action plan.
Step 6: Publication
This document was approved in July 2015 by the project board listed on p4
It is available on the CCG website:
https://www.northsomersetccg.nhs.uk/about-us/edhr/equality-impact-assessments-eia/ (as at August 2015)
44
Equality Impact Assessment on the procurement of Community Health Services in North Somerset
26
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
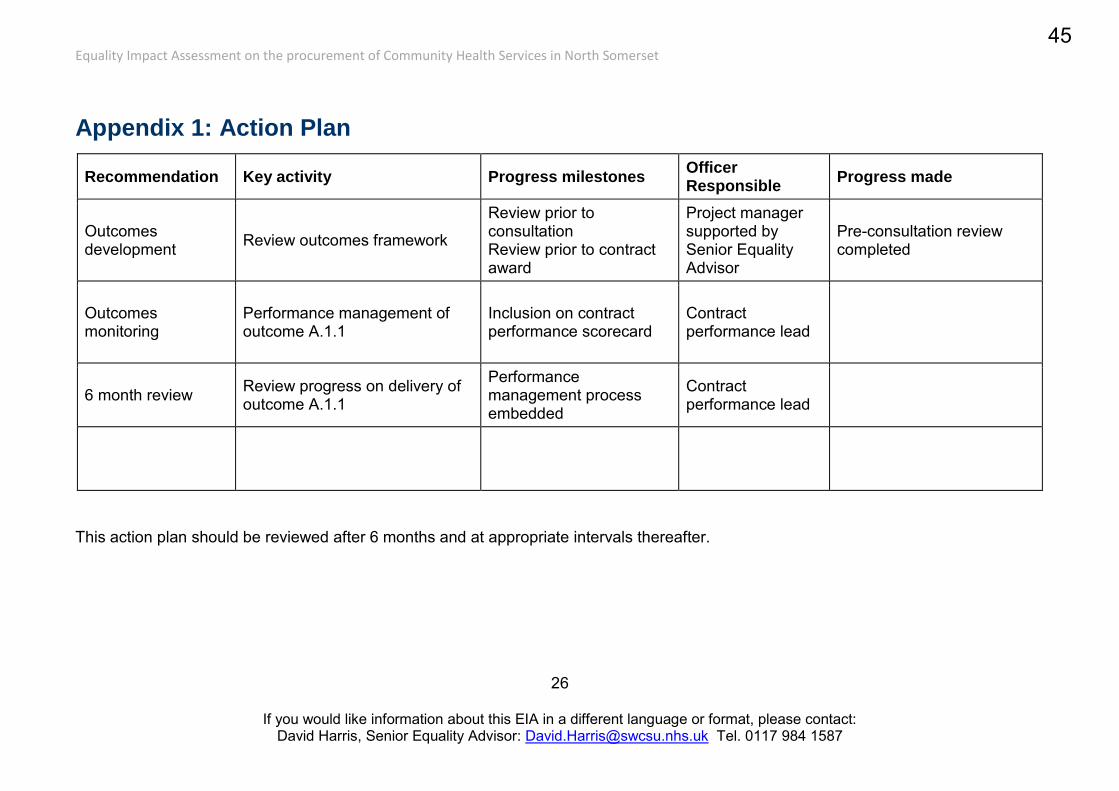
Appendix 1: Action Plan
Recommendation Key activity Progress milestones Officer Responsible
Progress made
Outcomes development Review outcomes framework
Review prior to consultation Review prior to contract award
Project manager supported by Senior Equality Advisor
Pre-consultation review completed
Outcomes monitoring
Performance management of outcome A.1.1
Inclusion on contract performance scorecard
Contract performance lead
6 month review Review progress on delivery of outcome A.1.1
Performance management process embedded
Contract performance lead
This action plan should be reviewed after 6 months and at appropriate intervals thereafter.
45
27
If you would like information about this EIA in a different language or format, please contact: David Harris, Senior Equality Advisor: [email protected] Tel. 0117 984 1587
Appendix 2: Highlights of the Equality Act 2010
The Equality Act 2010 outlaws direct and indirect discrimination, including less favourable treatment, harassment and victimisation of people based upon their protected characteristics. The Act applies to all individuals, providers of services and employers.
Direct discrimination means less favourable treatment of a person compared with another person because of a protected characteristic.
Indirect discrimination means the use of an apparently neutral practice, provision or criterion which puts people with a particular protected characteristic at a disadvantage compared with others who do not share that characteristic, and applying the practice, provision or criterion cannot be objectively justified.
The public sector equality duty, arising from Section 149(1) of the Act, applies to public authorities, such North Somerset CCG. A public authority must, in the exercise of its functions, have due regard to the need to —
a) eliminate discrimination, harassment, victimisation and any other conduct that is prohibited by or under this Act;
b) advance equality of opportunity between persons who share a relevant protected characteristic and persons who do not share it;
c) foster good relations between persons who share a relevant protected characteristic and persons who do not share it.
S149 (3) of the Act states that having due regard to the need to advance equality of opportunity between persons who share a relevant protected characteristic and persons who do not share it involves having due regard, in particular, to the need to —
a) remove or minimise disadvantages suffered by persons who share a relevant protected characteristic that are connected to that characteristic;
b) take steps to meet the needs of persons who share a relevant protected characteristic that are different from the needs of persons who do not share it;
c) encourage persons who share a relevant protected characteristic to participate in public life or in any other activity in which participation by such persons is disproportionately low.
46
Appendix 7Community Health Services in North Somerset
Consultation Feedback Report
June 2015
Feedback from the consultation on
community health services
in North Somerset
2 February to 24 April 2015
47
Consultation on the procurement of community services in North Somerset – June 2015
Page 2 of 23
Table of Contents 1. Introduction – Our vision for joint commissioning ......................................................................... 3
2. Purpose of this report ..................................................................................................................... 3
3. Background to the project .............................................................................................................. 4
3.1 Commissioning ........................................................................................................................ 4
3.2 How the pre-procurement public engagement shaped the formal consultation .................. 4
4. Consultation timetable ................................................................................................................... 6
5. The North Somerset CCG’s duty to involve patients and the public .............................................. 6
6. Consultation context ....................................................................................................................... 7
7. Equality matters .............................................................................................................................. 7
8. Consultation techniques and methods ........................................................................................... 8
8.1 Our presentation pack ............................................................................................................ 8
8.2 Our consultation methodology: .............................................................................................. 8
8.2.1 Publication ...................................................................................................................... 8
8.2.2 Events and meetings ..................................................................................................... 10
8.2.3 Feedback ....................................................................................................................... 10
9. Consultation meeting and event record ....................................................................................... 11
10. What did we ask in the consultation? ....................................................................................... 13
11. What have you said to us in the consultation and what have we changed in response? ........ 14
12. What were the limitations of this public consultation? ........................................................... 21
13. What happens next? ................................................................................................................. 22
Appendices ............................................................................................................................................ 23
48
Consultation on the procurement of community services in North Somerset – June 2015
Page 3 of 23
1. Introduction – Our vision for joint commissioning
“We know that for people to be truly healthy it is not only the quality of healthcare
services that matters. That is why we are committed to working together with our
whole population, individuals and other organisations to create the healthiest
communities.”
North Somerset Clinical Commissioning Group (the CCG) is the lead partner in the project to jointly commission community health services for the people of North Somerset. The CCG, as the lead commissioning partner, also has responsibility for leading the public consultation. The other partner organisations undertaking the project comprise North Somerset Council (the Local Authority) and the NHS
England Area Team.
2. Purpose of this report
This report describes the CCG’s public consultation exercise for our joint project for the commissioning of community health services in North Somerset. It first describes the arrangements that the CCG made for consulting public stakeholders on the key areas, which were identified during the pre-procurement engagement phase, and have subsequently been developed. It then provides a themed summary of the feedback that people have contributed, detailing how this feedback is reflected in the future stages of the procurement process.
Public stakeholders in the context of this project means: adults, children, young people, parents and carers and professional stakeholders from health, social care, education and the voluntary and independent sectors.
The consultation commenced on 2 February 2015 and ran until 24 April 2015.
49
Consultation on the procurement of community services in North Somerset – June 2015
Page 4 of 23
3. Background to the project
3.1 Commissioning
The North Somerset CCG Governing Body made the decision to undertake a full procurement of Community Health Services on 15th October 2013. The ‘trigger’ for this process was the fact that the contract with North Somerset CCG’s current provider of Community Health Services for North Somerset expiries on 31 March 2016 (extended from March 2015).
The health and social care services that are included within the scope of this commissioning project include, but are not limited, to:
All community-based services, including social care services provided, or commissioned, as part of integrated services.
Both mental and physical community care Existing sub-contracted services Services for people with dementia Health visitors School nurses Children’s Community Therapy Services, e.g., Speech And Language
Therapy, Occupational Therapy Childhood immunisations (school based) Specialist community services, for example, Parkinson’s disease services Any service that can demonstrate and deliver the Commissioners’
system wide savings and efficiencies
At the end of the procurement process, the successful bidder will provide community health services for the North Somerset population from April 2016 for the next five years
3.2 How the pre-procurement public engagement shaped the formal
consultation
Before embarking on the procurement process, and in partnership with Healthwatch North Somerset, we carried out an extensive pre-procurement public engagement exercise. This involved key stakeholders and a wide ranging number of community groups across a three month period. The report from this stage of the process is available on the CCG website here:
https://www.northsomersetccg.nhs.uk/library/community-health-services-stakeholder-engagement-r/
The feedback from people who participated in this was used to develop the requirements for the bidders. These requirements were contained within the Memorandum of Information and other bidder information documents. The feedback was also used alongside further involvement and co-production activities, to develop the outcomes framework.
50
Consultation on the procurement of community services in North Somerset – June 2015
Page 5 of 23
This outcomes framework forms the foundation of the Commissioning for Outcomes approach we are using.
The feedback from this stage and our learning from this process also helped to shape the formal consultation, which is reported here.
51
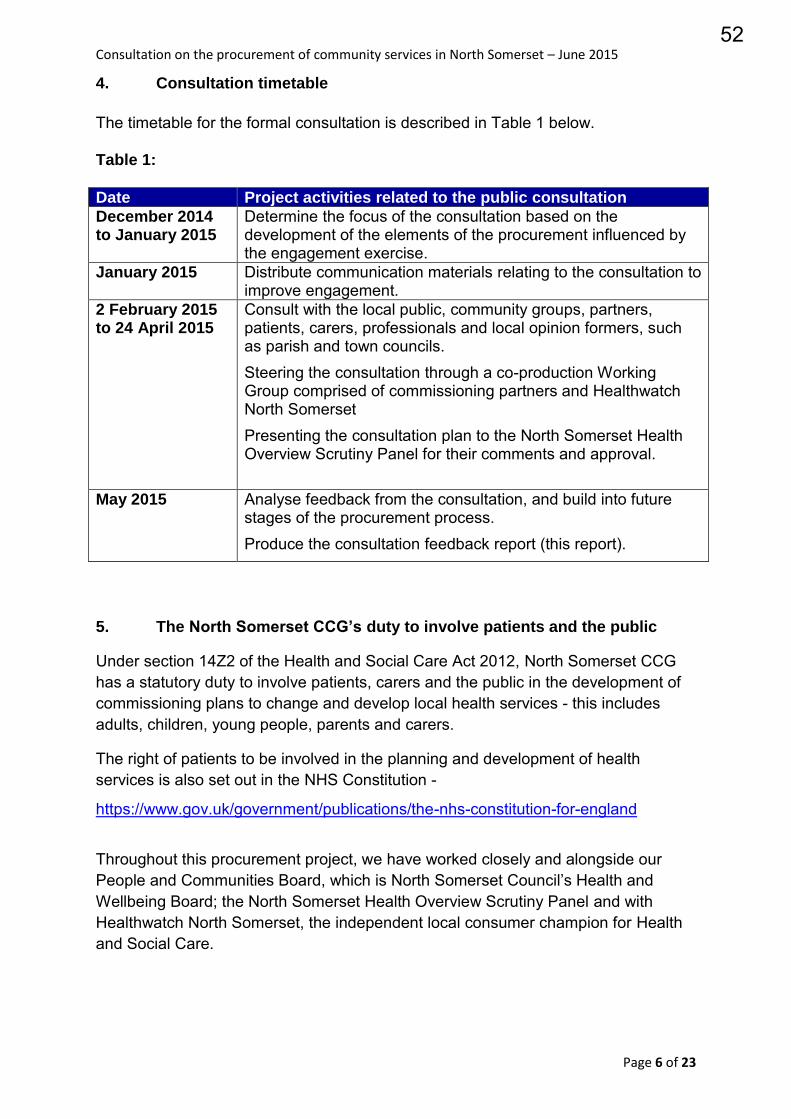
Consultation on the procurement of community services in North Somerset – June 2015
Page 6 of 23
4. Consultation timetable
The timetable for the formal consultation is described in Table 1 below.
Table 1:
Date Project activities related to the public consultation
December 2014 to January 2015
Determine the focus of the consultation based on the development of the elements of the procurement influenced by the engagement exercise.
January 2015 Distribute communication materials relating to the consultation to improve engagement.
2 February 2015 to 24 April 2015
Consult with the local public, community groups, partners, patients, carers, professionals and local opinion formers, such as parish and town councils. Steering the consultation through a co-production Working Group comprised of commissioning partners and Healthwatch North Somerset Presenting the consultation plan to the North Somerset Health Overview Scrutiny Panel for their comments and approval.
May 2015 Analyse feedback from the consultation, and build into future stages of the procurement process. Produce the consultation feedback report (this report).
5. The North Somerset CCG’s duty to involve patients and the public
Under section 14Z2 of the Health and Social Care Act 2012, North Somerset CCG has a statutory duty to involve patients, carers and the public in the development of commissioning plans to change and develop local health services - this includes adults, children, young people, parents and carers.
The right of patients to be involved in the planning and development of health services is also set out in the NHS Constitution -
https://www.gov.uk/government/publications/the-nhs-constitution-for-england
Throughout this procurement project, we have worked closely and alongside our People and Communities Board, which is North Somerset Council’s Health and Wellbeing Board; the North Somerset Health Overview Scrutiny Panel and with Healthwatch North Somerset, the independent local consumer champion for Health and Social Care.
52
Consultation on the procurement of community services in North Somerset – June 2015
Page 7 of 23
6. Consultation context
The population of North Somerset is changing - it is both growing in numbers and also it is becoming more diverse. In particular, new housing developments in Weston, Worle and Portishead are attracting a younger population with young families and we also have an ageing population with the numbers of frail elderly people increasing significantly over the next ten to twenty years. This demographic context has a significant impact on health and social care as both young families and the elderly are the highest users of services.
7. Equality matters
Our population profile also comprises people who are ‘seldom heard from’ and people who are vulnerable; this means, for example, people from Black and Minority Ethnic communities, people who are socially isolated for one reason or another, and children and younger people. We attended to, and carefully considered, the needs of these groups within our consultation plans. The North Somerset CCG cannot rely on a ‘blanket’ approach to consultation and takes steps to ensure that it tailors and targets the work it undertakes appropriately and proportionately. The diversity of local people’s views is especially important for services that are universal and available to all so we need to ensure that they are also truly accessible to all. We aimed to ensure that all people wishing to could access the consultation process and provide their feedback in ways that were easiest for them.
53
Consultation on the procurement of community services in North Somerset – June 2015
Page 8 of 23
8. Consultation techniques and methods
North Somerset CCG planned and delivered a range of consultation techniques to make the process of listening to information and providing feedback both attractive and easily accessible to local people.
A stakeholder analysis, using equality based ‘protected characteristics’ as a further aid, was undertaken to identify all key stakeholders at the pre-procurement engagement phase. This learning and experience meant that we could then ensure that most effort and resource was directed towards the patients, users and carers receiving community health and social care services to consult with them and listen to their views.
We took great care to arrange to listen to people in places that were convenient for them and at times of the day that people could meet with us. This included events outside of office hours so that working age people could attend.
8.1 Our presentation pack
A presentation pack of consultation materials was co-produced with lay people and partner organisations and comprised:
Three versions of the consultation document, each containing details of feedback methods:
o An easy-read consultation document, suitable for people with a learning disability and for people with literacy needs
o An accessible “public” consultation document o A detailed consultation document
An event presentation, available in digital form, but also presented in hard copy from interactive display boards
An electronic survey, hosted online and accessible through the North Somerset CCG website.
A flyer detailing the public meetings and contact methods
A presenter feedback form to capture questions and answers from the events.
A full set of the consultation documentation is available as Appendices 1a to 1g
8.2 Our consultation methodology:
8.2.1 Publication
The consultation was publicised using: Notices in the local media advertising the consultation process
Promotion at the Your North Somerset event, held on 25 January 2015 at the Winter Gardens, Weston-super-Mare, which had a footfall of over 1500 local people.
Direct mail to all stakeholders contacted at the engagement phase, including
54
Consultation on the procurement of community services in North Somerset – June 2015
Page 9 of 23
o voluntary, community and social enterprise sector organisations, and o all nursing and residential care homes
Information posted in all GP surgeries and Pharmacies in North Somerset
Inclusion in a number of newsletters, including o The North Somerset Healthwatch newsletter o “Noticeboard”, the local authority schools’ newsletter o A CCG stakeholder newsletter
Via social media, comprising o The CCG Facebook page and Twitter feed o Tweet chats at specific times during the consultation period o Streetlife.com local forums for
Clevedon Nailsea Portishead, and Weston-super-Mare
The North Somerset CCG website
People were invited to participate in the consultation by attending a public meeting; requesting a presentation at a group meeting of their own; or by reviewing the documentation published on the CCG website.
A total of 700 public consultation documents were distributed at public venues, consultation events, and by direct mail to:
o All North Somerset libraries o For All Healthy Living Centre, Weston o Marina Healthcare Centre, Portishead o The North Somerset Lesbian, Gay, Bisexual and Transgender Forum o Faithnet o Nailsea and District, Diabetes UK o Addaction, Weston o ARA (Addiction Recovery Agency, Weston) o Clevedon Community Hospital o Clevedon Community Hospital League of Friends o All North Somerset Children's Centres o All North Somerset care homes o Healthwatch North Somerset o Weston General Hospital
Electronic copies of the public consultation document were sent to:
o A carer who could not attend the public meetings o Gypsies and Travellers Strategic Group o Weston college and staff o All North Somerset GP Practices o All North Somerset Pharmacies o North Somerset Health Overview and Scrutiny Panel o All North Somerset town and parish councils
55
Consultation on the procurement of community services in North Somerset – June 2015
Page 10 of 23
8.2.2 Events and meetings
The events and meetings included:
Four open public meetings, one in each of the four localities where health and social care are provided – these are:
o Weston o Worle o “Gordano Valley” including Clevedon, Portishead and Pill o “The Rurals”, including Nailsea, and Backwell
The Worle meeting was chosen to be an evening meeting to accommodate full time workers, as it was the most accessible venue. Other evening meetings and groups were attended by request.
Joining existing community meetings, for example, o Alzheimer’s Society o District Diabetes Support Group o North Somerset Black and Minority Ethnic Network Focus Group
A focus group held in an area of higher deprivation
Presentations to partner meetings
Presentations to wider CCG meetings – to raise awareness, such as the GP membership forum and provider forum
North Somerset Health Overview Scrutiny Panel paper and presentation
8.2.3 Feedback
The ways in which people could give us their feedback were:
Direct feedback at a consultation event or meeting, recorded on the presenter feedback form (Appendix 1g)
Use of the electronic survey
By e-mail, at the address provided on the consultation documents
By telephone, on the number provided on the consultation documents
By posting on the CCG Facebook page or Twitter feed.
In addition to being able to provide feedback electronically, collection points for feedback forms in hard copy were also made available across all GP surgeries and pharmacies in North Somerset.
56
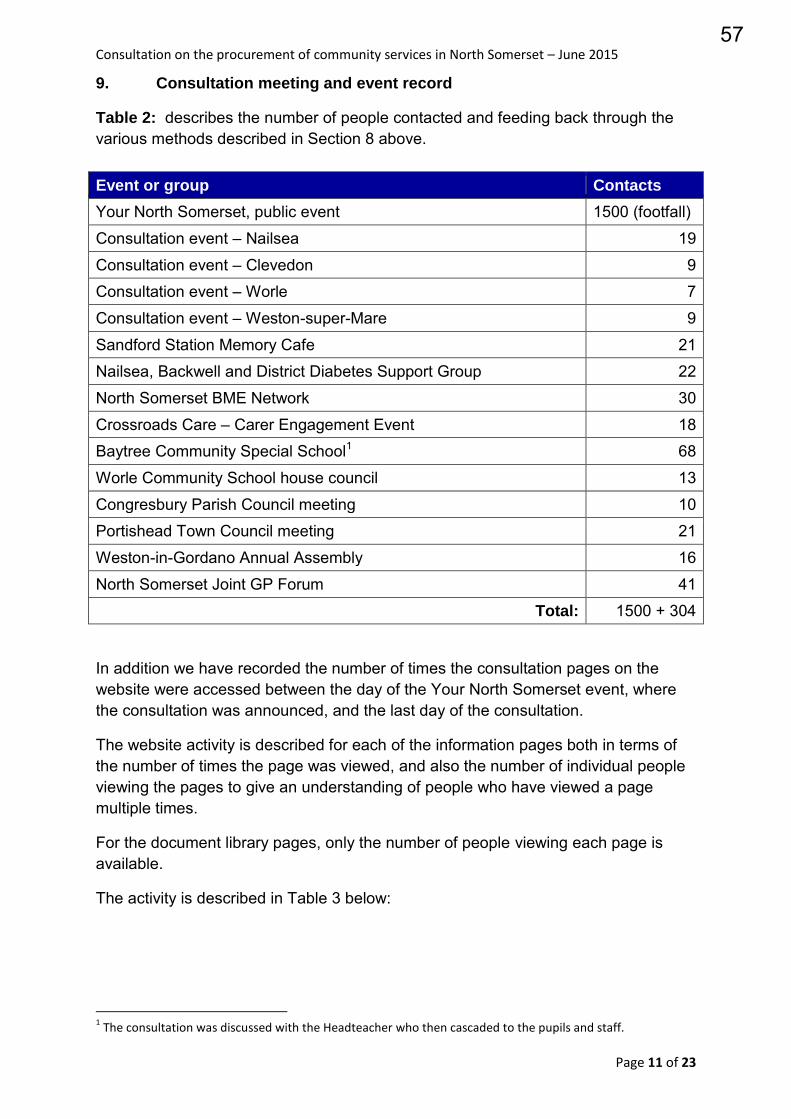
Consultation on the procurement of community services in North Somerset – June 2015
Page 11 of 23
9. Consultation meeting and event record
Table 2: describes the number of people contacted and feeding back through the various methods described in Section 8 above. Event or group Contacts
Your North Somerset, public event 1500 (footfall)
Consultation event – Nailsea 19
Consultation event – Clevedon 9 Consultation event – Worle 7
Consultation event – Weston-super-Mare 9
Sandford Station Memory Cafe 21 Nailsea, Backwell and District Diabetes Support Group 22
North Somerset BME Network 30
Crossroads Care – Carer Engagement Event 18 Baytree Community Special School1 68
Worle Community School house council 13
Congresbury Parish Council meeting 10 Portishead Town Council meeting 21
Weston-in-Gordano Annual Assembly 16
North Somerset Joint GP Forum 41 Total: 1500 + 304
In addition we have recorded the number of times the consultation pages on the website were accessed between the day of the Your North Somerset event, where the consultation was announced, and the last day of the consultation.
The website activity is described for each of the information pages both in terms of the number of times the page was viewed, and also the number of individual people viewing the pages to give an understanding of people who have viewed a page multiple times.
For the document library pages, only the number of people viewing each page is available.
The activity is described in Table 3 below:
1 The consultation was discussed with the Headteacher who then cascaded to the pupils and staff.
57
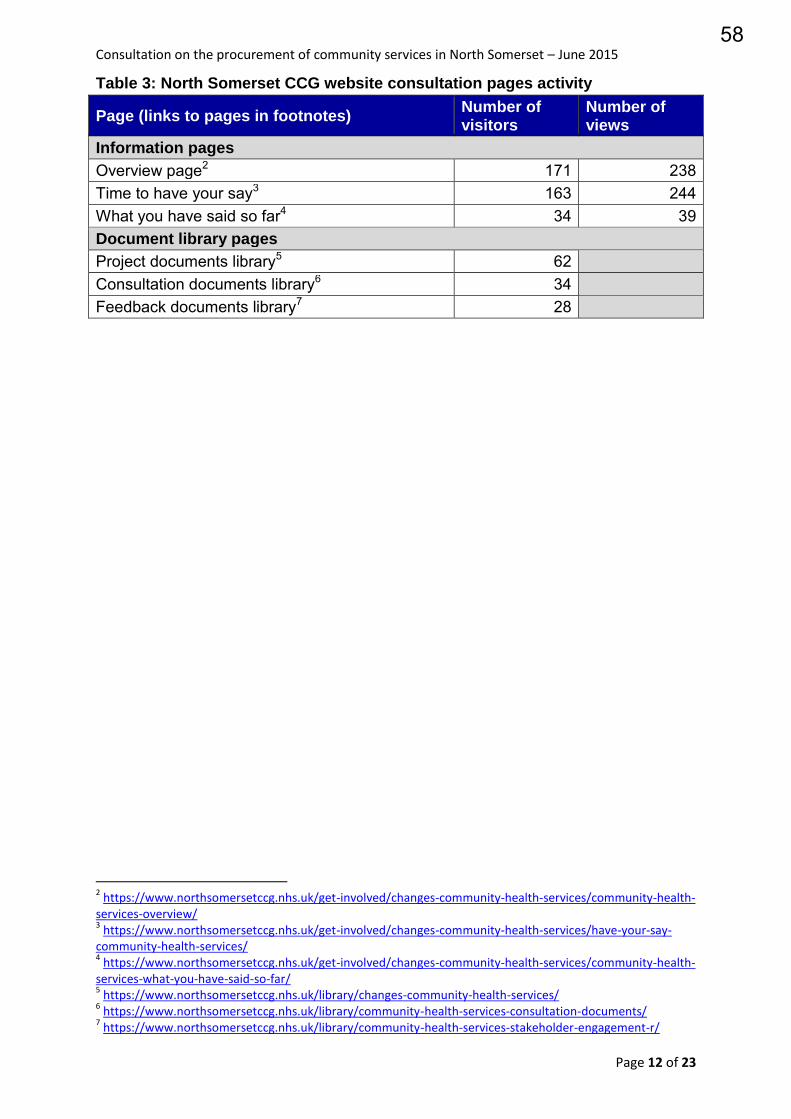
Consultation on the procurement of community services in North Somerset – June 2015
Page 12 of 23
Table 3: North Somerset CCG website consultation pages activity
Page (links to pages in footnotes) Number of visitors
Number of views
Information pages
Overview page2 171 238 Time to have your say3 163 244 What you have said so far4 34 39 Document library pages
Project documents library5 62 Consultation documents library6 34 Feedback documents library7 28
2 https://www.northsomersetccg.nhs.uk/get-involved/changes-community-health-services/community-health-
services-overview/ 3 https://www.northsomersetccg.nhs.uk/get-involved/changes-community-health-services/have-your-say-
community-health-services/ 4 https://www.northsomersetccg.nhs.uk/get-involved/changes-community-health-services/community-health-
services-what-you-have-said-so-far/ 5 https://www.northsomersetccg.nhs.uk/library/changes-community-health-services/
6 https://www.northsomersetccg.nhs.uk/library/community-health-services-consultation-documents/
7 https://www.northsomersetccg.nhs.uk/library/community-health-services-stakeholder-engagement-r/
58
Consultation on the procurement of community services in North Somerset – June 2015
Page 13 of 23
10. What did we ask in the consultation?
A principal aim of the formal consultation process was to check with the people of North Somerset that we had captured their main points about what matters most to them about community health and care services
This had the additional benefit of assurance to the commissioners that the feedback from the pre-procurement public engagement exercise had been accurately reflected in the development of what we all require from the bidders.
The feedback from the formal consultation also allows for adjustment of the requirements, before the call for final tenders, which is the final stage of the selection process.
In this context the following four consultation questions were asked:
Do you think the proposed outcomes will result in better services? Do you think that the proposed opportunity services will enhance the current
services offered? Do you think the proposal to group services around the four localities will
improve access and integration; For adults? For children? Do you have any other comments or suggestions about the proposed
outcomes? The first three questions above concern how we require the successful bidder to provide community health and care services, based on what you told us in the pre-procurement public engagement. We gave you information in the public consultation document, and also in the presentations and on the CCG website, to help you to be fully informed and to be in the best position to answer these three questions. The final question was to give you a further opportunity to let us know of anything else that was really important to you.
59
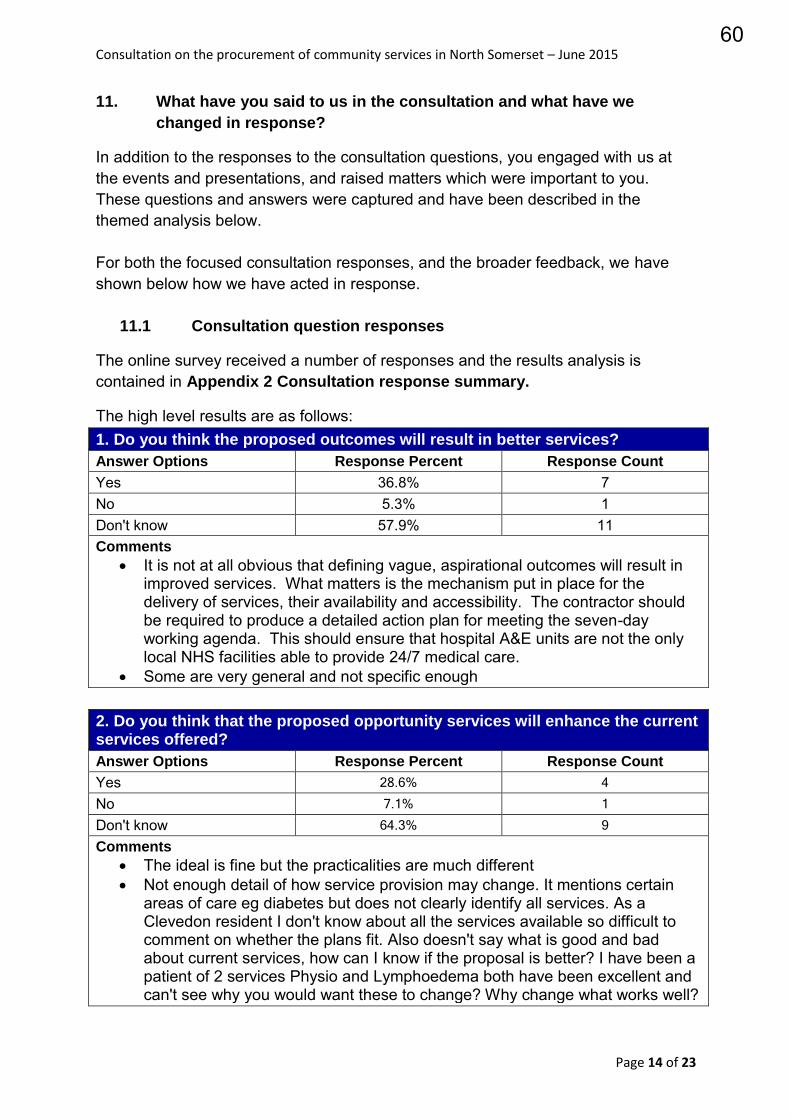
Consultation on the procurement of community services in North Somerset – June 2015
Page 14 of 23
11. What have you said to us in the consultation and what have we
changed in response?
In addition to the responses to the consultation questions, you engaged with us at the events and presentations, and raised matters which were important to you. These questions and answers were captured and have been described in the themed analysis below. For both the focused consultation responses, and the broader feedback, we have shown below how we have acted in response.
11.1 Consultation question responses
The online survey received a number of responses and the results analysis is contained in Appendix 2 Consultation response summary.
The high level results are as follows: 1. Do you think the proposed outcomes will result in better services?
Answer Options Response Percent Response Count
Yes 36.8% 7 No 5.3% 1 Don't know 57.9% 11 Comments
It is not at all obvious that defining vague, aspirational outcomes will result in improved services. What matters is the mechanism put in place for the delivery of services, their availability and accessibility. The contractor should be required to produce a detailed action plan for meeting the seven-day working agenda. This should ensure that hospital A&E units are not the only local NHS facilities able to provide 24/7 medical care.
Some are very general and not specific enough 2. Do you think that the proposed opportunity services will enhance the current services offered?
Answer Options Response Percent Response Count
Yes 28.6% 4
No 7.1% 1
Don't know 64.3% 9
Comments The ideal is fine but the practicalities are much different Not enough detail of how service provision may change. It mentions certain
areas of care eg diabetes but does not clearly identify all services. As a Clevedon resident I don't know about all the services available so difficult to comment on whether the plans fit. Also doesn't say what is good and bad about current services, how can I know if the proposal is better? I have been a patient of 2 services Physio and Lymphoedema both have been excellent and can't see why you would want these to change? Why change what works well?
60
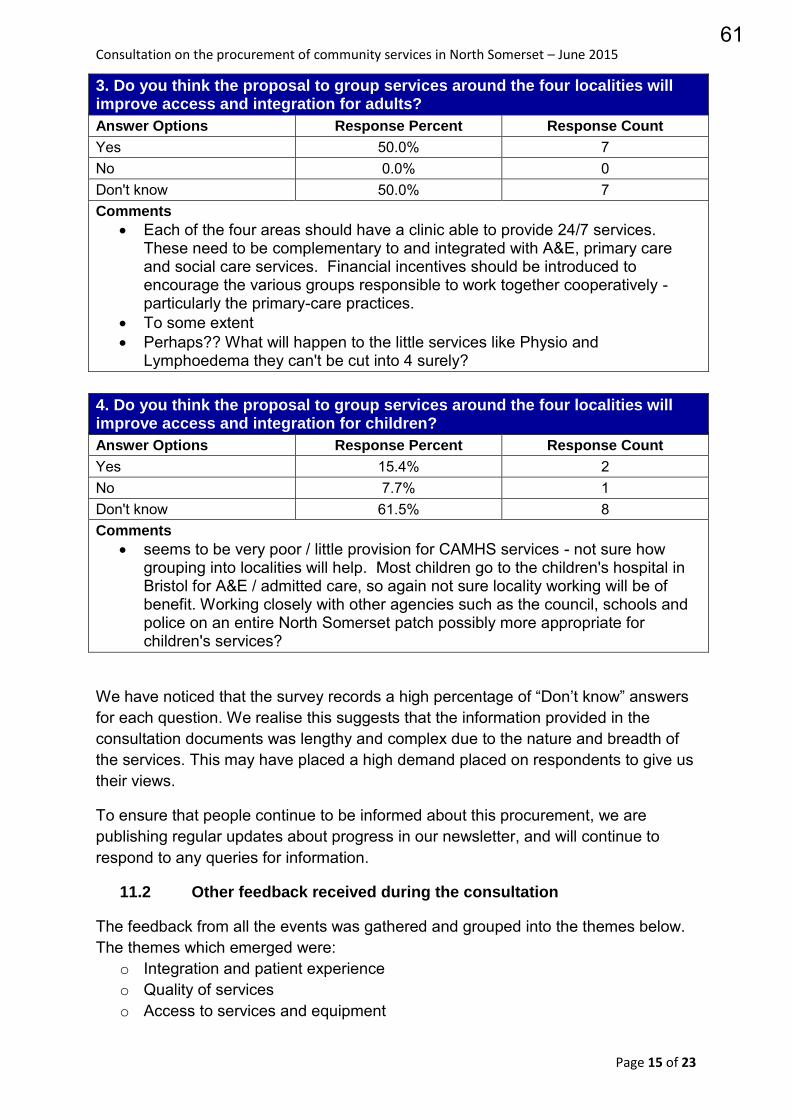
Consultation on the procurement of community services in North Somerset – June 2015
Page 15 of 23
3. Do you think the proposal to group services around the four localities will improve access and integration for adults?
Answer Options Response Percent Response Count
Yes 50.0% 7 No 0.0% 0 Don't know 50.0% 7 Comments
Each of the four areas should have a clinic able to provide 24/7 services. These need to be complementary to and integrated with A&E, primary care and social care services. Financial incentives should be introduced to encourage the various groups responsible to work together cooperatively - particularly the primary-care practices.
To some extent Perhaps?? What will happen to the little services like Physio and
Lymphoedema they can't be cut into 4 surely? 4. Do you think the proposal to group services around the four localities will improve access and integration for children?
Answer Options Response Percent Response Count
Yes 15.4% 2 No 7.7% 1 Don't know 61.5% 8 Comments
seems to be very poor / little provision for CAMHS services - not sure how grouping into localities will help. Most children go to the children's hospital in Bristol for A&E / admitted care, so again not sure locality working will be of benefit. Working closely with other agencies such as the council, schools and police on an entire North Somerset patch possibly more appropriate for children's services?
We have noticed that the survey records a high percentage of “Don’t know” answers for each question. We realise this suggests that the information provided in the consultation documents was lengthy and complex due to the nature and breadth of the services. This may have placed a high demand placed on respondents to give us their views.
To ensure that people continue to be informed about this procurement, we are publishing regular updates about progress in our newsletter, and will continue to respond to any queries for information.
11.2 Other feedback received during the consultation
The feedback from all the events was gathered and grouped into the themes below. The themes which emerged were:
o Integration and patient experience o Quality of services o Access to services and equipment
61
Consultation on the procurement of community services in North Somerset – June 2015
Page 16 of 23
o Innovation o Outcome-based commissioning and the procurement process o Financial sustainability
Integration and patient experience: Carers should be involved, with carers holding care plans and being present
when, for example, physiotherapy exercises are being taught to the cared-for Services need to respond to issues that arise, which may not necessarily be in
their field of expertise, i.e. a nurse reporting back to the nursing team that a person requires more assistance at home – and the OT service responding by providing new aids to assist.
Health professionals need to understand that teenagers need to be treated as neither children, nor as having the understanding of adults. If they felt more confident in a healthcare environment then they would engage better with the NHS and their health. This should include medical professionals trained to deal with teenagers.
Mental health needs to be part of an holistic assessment. Continuity of staff is important as trust is built over a period. At transition to adult
services, there is a handover to a new contact and a new relationship must be built. There have also been gaps in services, especially OT, when staff go on annual leave, or maternity leave.
Working in partnership beyond health and social care, for example links with local authority planning department to plan for population increase linked to new housing.
Discharge home from the hospital at the right time with the appropriate support is essential for ensuring the service outcomes are achieved.
An example: Appointments are not being automatically cancelled when an individual is an inpatient in hospital. In one case, this led to discharge of the individual from the outpatient consultant’s care as a result of a [Did Not Attend] DNA record.
Will I be able to get hold of someone who knows my case? Do GPs support the changes?
Quality of Services:
The importance of maintaining quality when moving services from acute to community
The final service needs the flexibility to allow different delivery models in the four localities to meet the different needs of their respective populations.
Access to services and equipment:
Seems to be very poor / little provision for CAMHS services - not sure how grouping into localities will help
Services need to be more visible, so that people are aware of what is available out there for them. Many positive experiences of existing community health services, but only once people knew to ask – some of which were several years down the line.
People were pleased when services are brought to them, particularly when there are issues of mobility, or lack of transport to get to traditional places of healthcare.
62
Consultation on the procurement of community services in North Somerset – June 2015
Page 17 of 23
For children with complex physical and mental health needs, delivery of services on school premises is beneficial for the pupils as it provides a familiar environment and prevents the time and resource taken to travel to off-site clinics. This is currently the case for school immunisations, orthotics, and eyes, and is a significant positive.
It has taken up to 6 months to rebook an appointment for a wheelchair assessment, which meant that a child was unable to receive the physical support required for them to learn effectively.
Will specialist teams work in localities as well? Elderly people can be discharged home from an acute provider on a Friday
evening and no support services are available. 7-day working is needed from all providers, and should include discharge programmes.
Any new services should remain free at the point of delivery. Enablement schemes should continue, with a focus on retaining community
rehabilitation. All current services should continue. Innovation
Each of the four areas should have a clinic able to provide 24/7 services. These need to be complementary to and integrated with A&E, primary care and social care services. Effective use of mobile technology to maximize time available for care. Financial incentives should be introduced to encourage the various groups responsible to work together cooperatively - particularly the primary-care practices.
Inclusion of telehealth and telecare Independent providers should have access to shared care plans and
assessments. Access other types of services, which would not necessarily be commissioned,
such as homeopathy Financial sustainability
People currently pay for social care services and not for health services. Will integration mean that the dividing line is movable?
The contract needs to provide flexibility to cope with the expansion of Portishead
11.3 How we have reflected your feedback in shaping the call for final
tenders
We are commissioning for outcomes. This means that the successful bidder chosen to deliver services will be required to ensure that all outcomes are met. We will monitor these outcomes to make sure this is happening. We have demonstrated below, grouped by the themes described above, selected elements from the outcomes framework which will encapsulates the feedback received. As the final outcomes framework will not be agreed until the contract is awarded in October 2015, the outcomes given below relate to the outcomes framework as
63
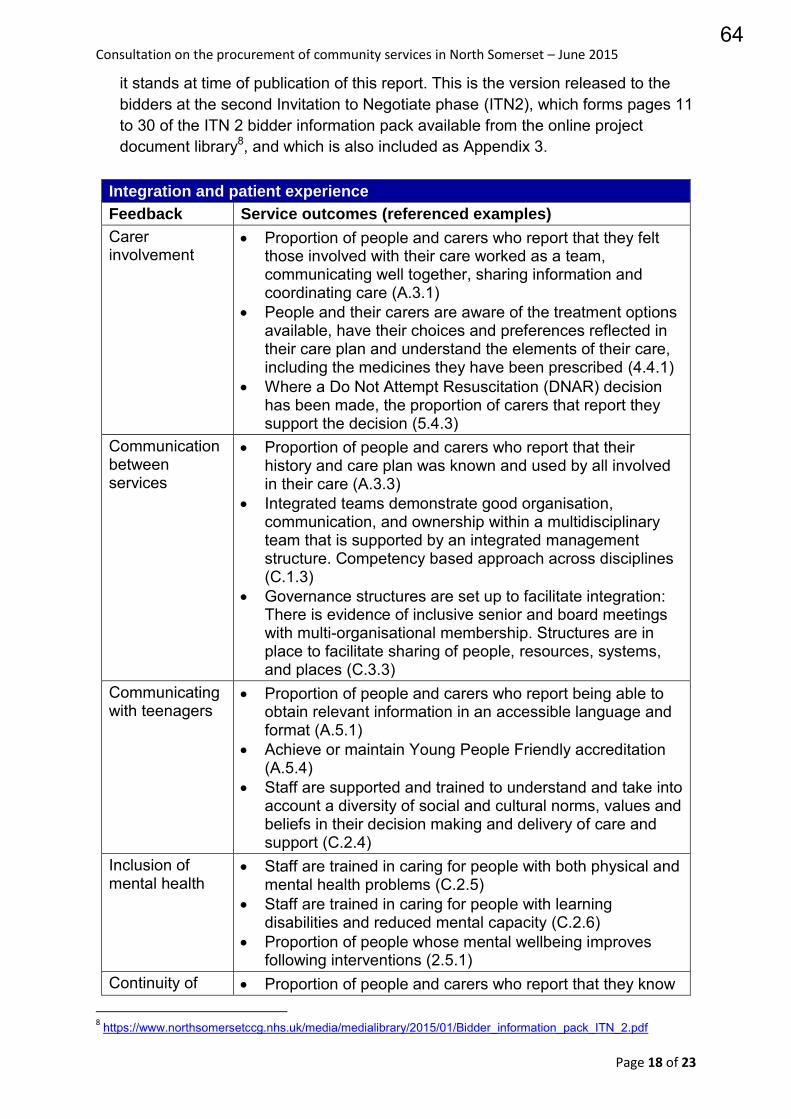
Consultation on the procurement of community services in North Somerset – June 2015
Page 18 of 23
it stands at time of publication of this report. This is the version released to the bidders at the second Invitation to Negotiate phase (ITN2), which forms pages 11 to 30 of the ITN 2 bidder information pack available from the online project document library8, and which is also included as Appendix 3.
Integration and patient experience
Feedback Service outcomes (referenced examples)
Carer involvement
Proportion of people and carers who report that they felt those involved with their care worked as a team, communicating well together, sharing information and coordinating care (A.3.1)
People and their carers are aware of the treatment options available, have their choices and preferences reflected in their care plan and understand the elements of their care, including the medicines they have been prescribed (4.4.1)
Where a Do Not Attempt Resuscitation (DNAR) decision has been made, the proportion of carers that report they support the decision (5.4.3)
Communication between services
Proportion of people and carers who report that their history and care plan was known and used by all involved in their care (A.3.3)
Integrated teams demonstrate good organisation, communication, and ownership within a multidisciplinary team that is supported by an integrated management structure. Competency based approach across disciplines (C.1.3)
Governance structures are set up to facilitate integration: There is evidence of inclusive senior and board meetings with multi-organisational membership. Structures are in place to facilitate sharing of people, resources, systems, and places (C.3.3)
Communicating with teenagers
Proportion of people and carers who report being able to obtain relevant information in an accessible language and format (A.5.1)
Achieve or maintain Young People Friendly accreditation (A.5.4)
Staff are supported and trained to understand and take into account a diversity of social and cultural norms, values and beliefs in their decision making and delivery of care and support (C.2.4)
Inclusion of mental health
Staff are trained in caring for people with both physical and mental health problems (C.2.5)
Staff are trained in caring for people with learning disabilities and reduced mental capacity (C.2.6)
Proportion of people whose mental wellbeing improves following interventions (2.5.1)
Continuity of Proportion of people and carers who report that they know 8 https://www.northsomersetccg.nhs.uk/media/medialibrary/2015/01/Bidder_information_pack_ITN_2.pdf
64
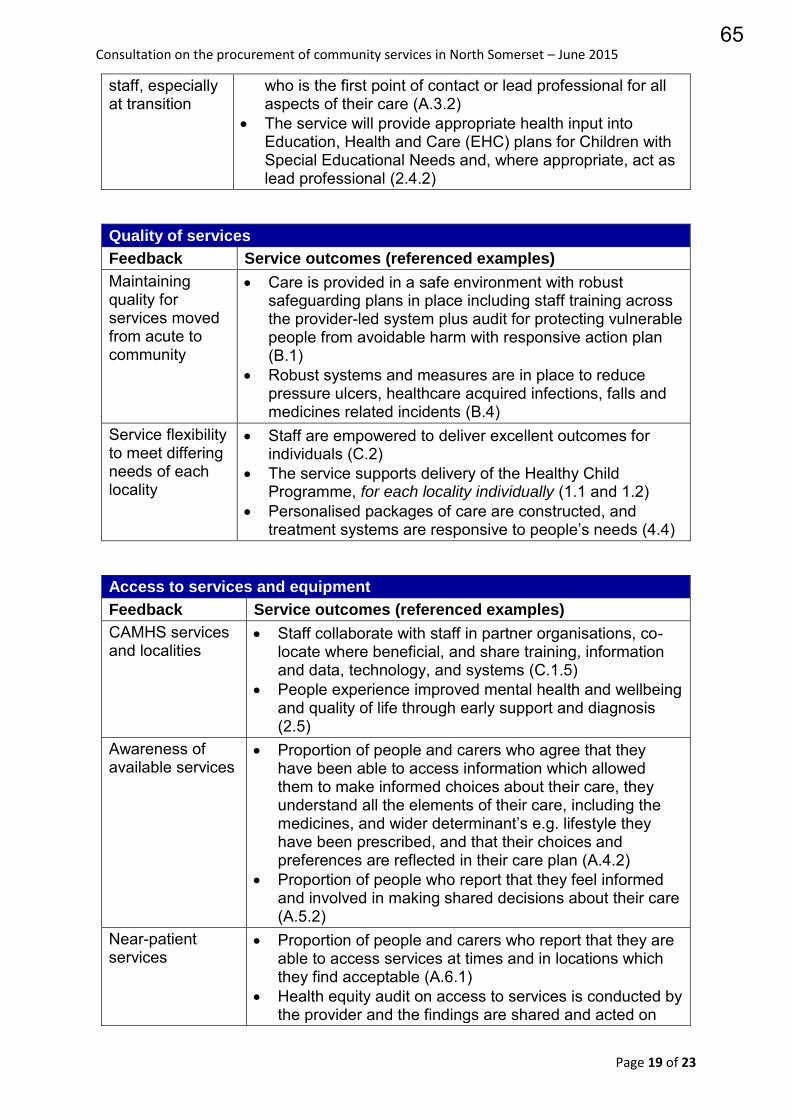
Consultation on the procurement of community services in North Somerset – June 2015
Page 19 of 23
staff, especially at transition
who is the first point of contact or lead professional for all aspects of their care (A.3.2)
The service will provide appropriate health input into Education, Health and Care (EHC) plans for Children with Special Educational Needs and, where appropriate, act as lead professional (2.4.2)
Quality of services
Feedback Service outcomes (referenced examples)
Maintaining quality for services moved from acute to community
Care is provided in a safe environment with robust safeguarding plans in place including staff training across the provider-led system plus audit for protecting vulnerable people from avoidable harm with responsive action plan (B.1)
Robust systems and measures are in place to reduce pressure ulcers, healthcare acquired infections, falls and medicines related incidents (B.4)
Service flexibility to meet differing needs of each locality
Staff are empowered to deliver excellent outcomes for individuals (C.2)
The service supports delivery of the Healthy Child Programme, for each locality individually (1.1 and 1.2)
Personalised packages of care are constructed, and treatment systems are responsive to people’s needs (4.4)
Access to services and equipment
Feedback Service outcomes (referenced examples)
CAMHS services and localities
Staff collaborate with staff in partner organisations, co-locate where beneficial, and share training, information and data, technology, and systems (C.1.5)
People experience improved mental health and wellbeing and quality of life through early support and diagnosis (2.5)
Awareness of available services
Proportion of people and carers who agree that they have been able to access information which allowed them to make informed choices about their care, they understand all the elements of their care, including the medicines, and wider determinant’s e.g. lifestyle they have been prescribed, and that their choices and preferences are reflected in their care plan (A.4.2)
Proportion of people who report that they feel informed and involved in making shared decisions about their care (A.5.2)
Near-patient services
Proportion of people and carers who report that they are able to access services at times and in locations which they find acceptable (A.6.1)
Health equity audit on access to services is conducted by the provider and the findings are shared and acted on
65
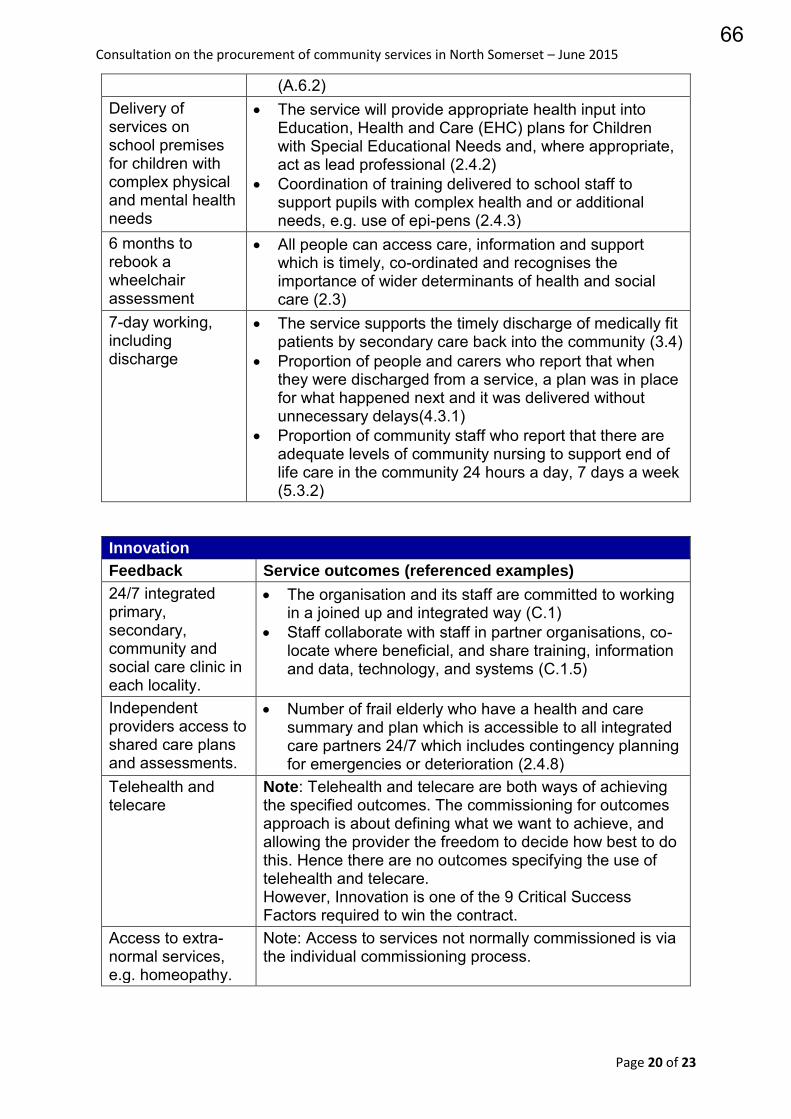
Consultation on the procurement of community services in North Somerset – June 2015
Page 20 of 23
(A.6.2) Delivery of services on school premises for children with complex physical and mental health needs
The service will provide appropriate health input into Education, Health and Care (EHC) plans for Children with Special Educational Needs and, where appropriate, act as lead professional (2.4.2)
Coordination of training delivered to school staff to support pupils with complex health and or additional needs, e.g. use of epi-pens (2.4.3)
6 months to rebook a wheelchair assessment
All people can access care, information and support which is timely, co-ordinated and recognises the importance of wider determinants of health and social care (2.3)
7-day working, including discharge
The service supports the timely discharge of medically fit patients by secondary care back into the community (3.4)
Proportion of people and carers who report that when they were discharged from a service, a plan was in place for what happened next and it was delivered without unnecessary delays(4.3.1)
Proportion of community staff who report that there are adequate levels of community nursing to support end of life care in the community 24 hours a day, 7 days a week (5.3.2)
Innovation
Feedback Service outcomes (referenced examples)
24/7 integrated primary, secondary, community and social care clinic in each locality.
The organisation and its staff are committed to working in a joined up and integrated way (C.1)
Staff collaborate with staff in partner organisations, co-locate where beneficial, and share training, information and data, technology, and systems (C.1.5)
Independent providers access to shared care plans and assessments.
Number of frail elderly who have a health and care summary and plan which is accessible to all integrated care partners 24/7 which includes contingency planning for emergencies or deterioration (2.4.8)
Telehealth and telecare
Note: Telehealth and telecare are both ways of achieving the specified outcomes. The commissioning for outcomes approach is about defining what we want to achieve, and allowing the provider the freedom to decide how best to do this. Hence there are no outcomes specifying the use of telehealth and telecare. However, Innovation is one of the 9 Critical Success Factors required to win the contract.
Access to extra-normal services, e.g. homeopathy.
Note: Access to services not normally commissioned is via the individual commissioning process.
66
Consultation on the procurement of community services in North Somerset – June 2015
Page 21 of 23
12. What were the limitations of this public consultation?
This public consultation was planned and developed to provide the best opportunities for access for our local population that we could undertake within the overall constraints of the project, such as time and resources available.
We used our existing communication channels and networks to help us to secure the broadest and deepest out reach into our local communities to inform them of what’s happening. However, we are aware that not all people will have heard or seen our communications and that some people may not have been able to provide feedback into our process because of this. The equality impact assessment at the pre-procurement stage identified opportunities for involving certain groups, and as a result of this analysis, a one-off focus group session was held at the For All Healthy Living Centre; the centre is situated in an area of North Somerset with a high deprivation index, and is a community centre with regular attendance from the immediately local population. The focus group was held in this location to ensure we were able to hear from a group who are seldom heard from.
To try to ensure that the community voice influencing the procurement is a strong as possible we have involved Healthwatch North Somerset from the very beginning of the project. We will continue to work closely with them until the chosen provider is delivering on the new contract. This will continue to help to ensure that the patient, carer, service user and public voice is ‘ever present’ during the procurement process and will continue to help us as commissioners to understand what matters most to our local people.
67
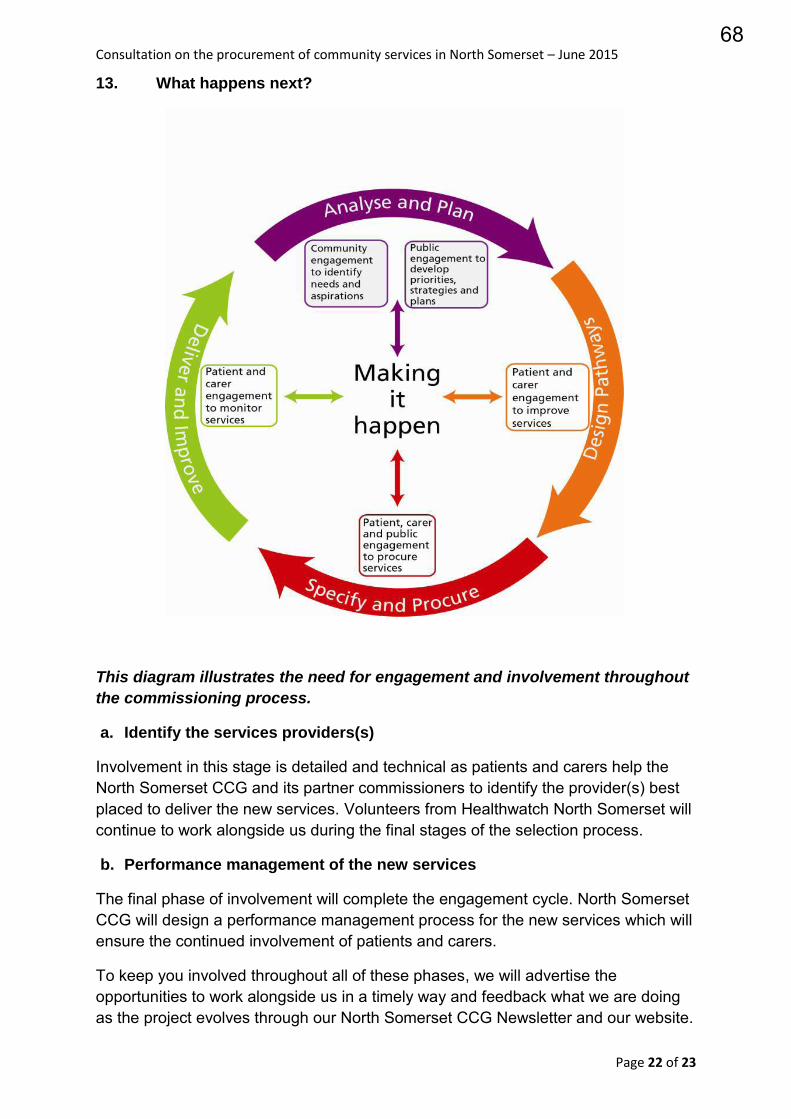
Consultation on the procurement of community services in North Somerset – June 2015
Page 22 of 23
13. What happens next?
This diagram illustrates the need for engagement and involvement throughout
the commissioning process.
a. Identify the services providers(s)
Involvement in this stage is detailed and technical as patients and carers help the North Somerset CCG and its partner commissioners to identify the provider(s) best placed to deliver the new services. Volunteers from Healthwatch North Somerset will continue to work alongside us during the final stages of the selection process.
b. Performance management of the new services
The final phase of involvement will complete the engagement cycle. North Somerset CCG will design a performance management process for the new services which will ensure the continued involvement of patients and carers.
To keep you involved throughout all of these phases, we will advertise the opportunities to work alongside us in a timely way and feedback what we are doing as the project evolves through our North Somerset CCG Newsletter and our website.
68
Consultation on the procurement of community services in North Somerset – June 2015
Page 23 of 23
Please contact us to make sure that you are included on our contact list at [email protected] or telephone 01275 547117.
Appendices
Appendix 1 Consultation documentation
a. Consultation pack – easy read b. Consultation pack – public c. Consultation pack – detailed d. Event presentation e. Consultation survey f. Consultation poster g. Presenter feedback form
Appendix 2 Consultation response summary
Appendix 3 ITN 2 Bidder information pack
Mary Adams
Patient and Public Engagement Manager
Peter Purdie
Project Manager
May 2015
69