013.systemic diseases in the etiology of periodontal disease
TRANSCRIPT
Dr Jaffar Raza Page 1
Systemic Diseases in the etiology of PDD
primary etiological agent in periodontal disease is bacterial plaque.
systemic factors that can alter the response of the tissue to plaque.
certain systemic disorders can have a direct effect on the periodontal tissues and these represent the periodontal manifestations of systemic diseases.
Dr Jaffar Raza Page 2
DIETARY AND NUTRITIONAL ASPECTS OF PERIODONTAL DISEASE
The Consistency of Diet
Firm and fibrous diet beneficial
Softer diet greater deposits and increase in plaque
A coarse diet, requires vigorous mastication
Dr Jaffar Raza Page 3
Protein Deficiency and Periodontal Disease
The integrity of the periodontal ligament is also dependent upon proteins
Deprivation of protien marked degeneration of periodontal support
Vitamins and Periodontal Disease
Vitamin C
Its deficiency in humans results in scurvy, a disease characterized by hemorrhagic susceptability and retardation of wound healing.
Dr Jaffar Raza Page 4
Clinical Manifestations
1. Increased susceptibility to infections.
2. Impaired wound healing.
3. Bleeding and swollen gums.
4. Mobile teeth.
Dr Jaffar Raza Page 5
Periodontal Features of Scurvy
chronic gingivitis which can involve the free gingiva, attached gingiva and alveolar mucosa
gingiva becomes brilliant-red, tender and swollen
The spongy tissues are extremely hyperemic and bleed spontaneously.
the tissues attain a dark blue or purple hue.
Alveolar bone resorption with increased tooth mobility.
Dr Jaffar Raza Page 6
Vitamin D Deficiency
Vitamin D is essential for the absorption of calcium from the gastrointestinal tract and the maintenance of calciumphosphorus balance.
Radiographically, there is a generalized partial to complete disappearance of the lamina dura
Reduced density of supporting bone.
Dr Jaffar Raza Page 7
Vitamin E
vitamin E acts as a antioxidant
plays an important role in maintaining the stability of cell membranes
protecting blood cells against hemolysis.
interfere with the production of prostaglandins.
Dr Jaffar Raza Page 8
Vitamin A
It is essential for growth, differentiation and maintenance of epithelial tissues
For bone growth and embryonic development.
Vitamin B-Complex
Oral changes common to—Vitamin B-complex deficiencies are gingivitis, glossitis, glossodynia, angular cheilitis inflammation of the entire oral mucosa
Dr Jaffar Raza Page 9
EFFECTS OF HEMATOLOGICAL DISORDERS ON PERIODONTIUM
Disorders of the blood and blood forming tissues can have a profound effect on the periodontal tissues and their response to bacterial plaque.
There can be a defect in the vascular constriction, platelet adhesion and aggregation, coagulation and fibrinolysis
Dr Jaffar Raza Page 10
White Blood Cell Disorders
The WBC’s disorders that affect the periodontium can be categorized as either a disorder of numbers or defect in function. Neutropenias
a. Cyclic neutropenia.
b. Chronic benign neutropenia of childhood.
c. Benign familial neutropenia.
d. Severe familial neutropenia.
e. Chronic idiopathic neutropenia.
Dr Jaffar Raza Page 11
Periodontal manifestations of neutropenias oral ulceration,
inflamed gingiva,
rapid periodontal breakdown,
alveolar bone loss.
bleeding on probing
areas of desquamation,
varying degrees of gingival recession
pocketing
edematous and bright-red appearance of gingiva
persistant recurrent infections throughout life
Dr Jaffar Raza Page 12
Treatment:
Plaque control,
supportive measures like antiseptic mouth wash,
antimicrobial therapy
Dr Jaffar Raza
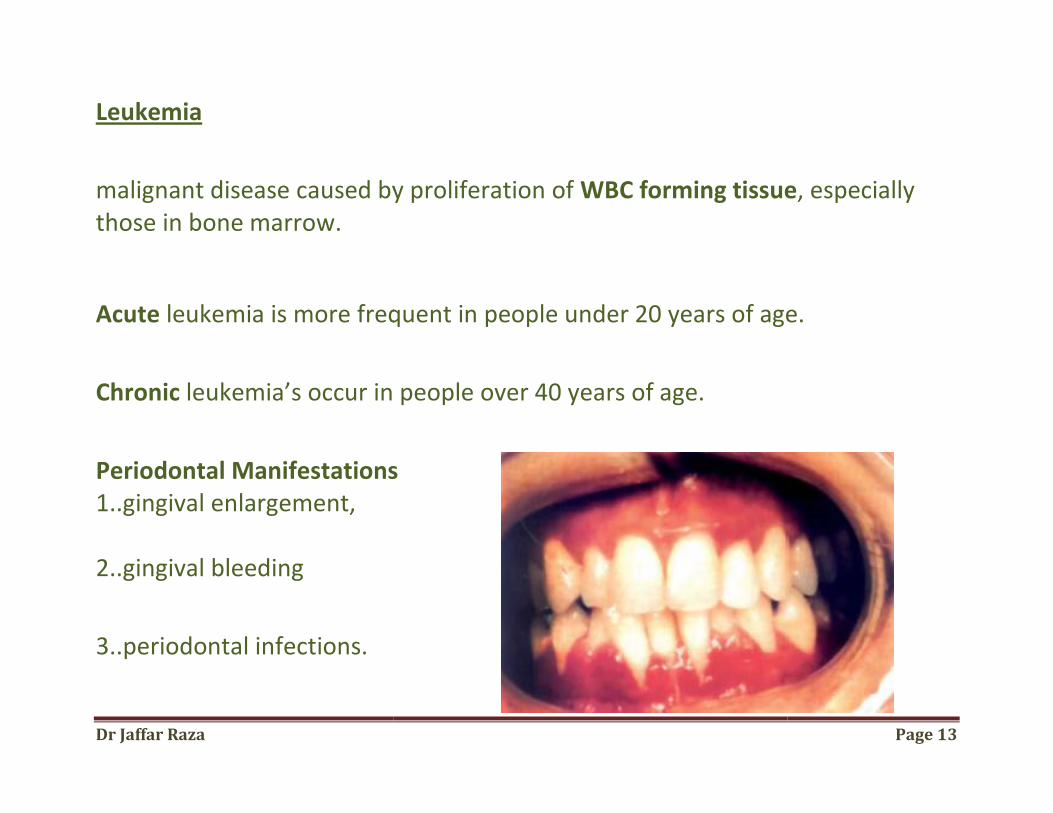
Leukemia
malignant disease caused by proliferation of those in bone marrow.
Acute leukemia is more frequent in people under 20 years of age.
Chronic leukemia’s occur in people over 40 years of age.
Periodontal Manifestations1..gingival enlargement, 2..gingival bleeding
3..periodontal infections.
malignant disease caused by proliferation of WBC forming tissue
leukemia is more frequent in people under 20 years of age.
leukemia’s occur in people over 40 years of age.
Periodontal Manifestations
Page 13
WBC forming tissue, especially
leukemia is more frequent in people under 20 years of age.
Dr Jaffar Raza Page 14
a. Gingival enlargement is due to a massive leukemic cell infiltration into the gingival connective tissue. The enlarged gingiva will hinder mechanical plaque removal
b. Gingival bleeding is a common oral manifestation of acute leukemia.
The bleeding is secondary to thrombocytopenia that accompanies leukemia.
c. Infections of the periodontal tissues secondary to leukemia can be of two types,
1.. exacerbation of an existing periodontal disease
2.. increased susceptibility of the periodontium to fungal, viral or bacterial infections.
Dr Jaffar Raza Page 15
Treatment Plan for Leukemic Patients
1. Referral for medical evaluation and treatment.
2. Prior to chemotherapy, a complete periodontal plan should be developed.
a. Monitor hematologic laboratory values. b. Administer suitable antibiotics before any periodontal treatment. c. scaling and root planing + 0.12 percent chlorhexidine gluconate
3. During the acute phases of leukemia: a. Cleanse the area with 3% (H2O2) or 0.12% chlorhexidine. b. remove any etiologic local factors. c. Re-cleanse the area with 3 percent H2O2. d. Place a cotton pellet soaked in thrombin against the bleeding point. e. Cover with gauze and apply pressure for 15 to 20 minutes.
Dr Jaffar Raza Page 16
f. Acute gingival or periodontal abscesses are treated by systemic antibiotics, gentle incision and drainage or by treating with 3% H2O2/0.12% chlorhexidine
g. Oral ulcerations should be treated with antibiotics and bland mouth rinses.
4. In patients with chronic leukemia, scaling and root planing can be performed but periodontal surgery should be avoided.
Dr Jaffar Raza
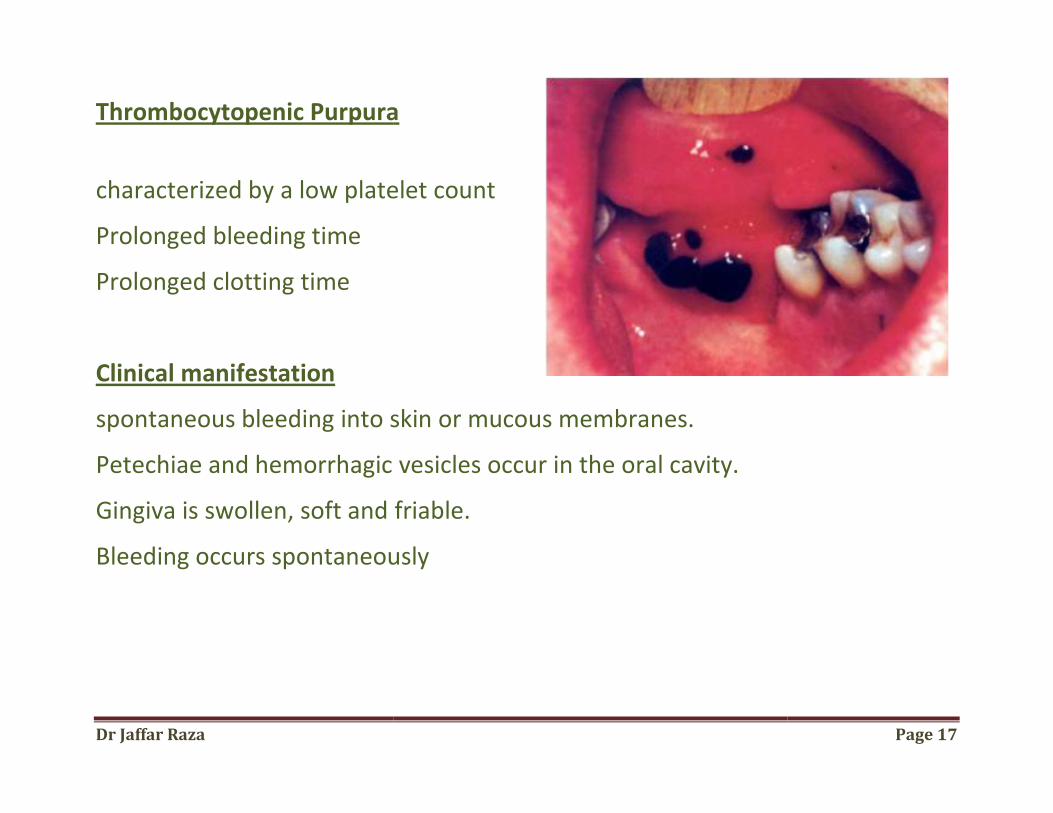
Thrombocytopenic Purpura
characterized by a low platelet count
Prolonged bleeding time
Prolonged clotting time
Clinical manifestation
spontaneous bleeding into skin or mucous membranes.
Petechiae and hemorrhagic vesicles occur in the oral cavity.
Gingiva is swollen, soft and friable.
Bleeding occurs spontaneously
Thrombocytopenic Purpura
characterized by a low platelet count
spontaneous bleeding into skin or mucous membranes.
and hemorrhagic vesicles occur in the oral cavity.
swollen, soft and friable.
Bleeding occurs spontaneously
Page 17
Dr Jaffar Raza Page 18
Treatment
1. Physician referral for a definitive diagnosis. 2. Oral hygiene instructions. 3. Prophylactic treatment of potential abscesses. 4. No surgical procedures are indicated unless platelet count is at least 80,000 cells/mm3. 5. Scaling and root planning.
Disorders of WBC Function
Chédiak-Higashi Syndrome
Lazy Leukocyte Syndrome
Chronic Granulomatous Disease
Dr Jaffar Raza Page 19
METABOLIC AND ENDOCRINE DISORDERS
Diabetes Mellitus and Periodontal Disease
diabetic patient is more susceptible to periodontal breakdown, which is characterized by
extensive bone loss,
increased tooth mobility,
widening of periodontal ligament space,
suppuration and abscess formation.
Dr Jaffar Raza Page 20
Pathogenesis
1. Vascular changes:
thickening and hyalinization of vascular walls.
swelling and occasional proliferation of the endothelial cells
changes in the capillary basement membrane may have an inhibitory effect on
the transport of oxygen, white blood cells, immune factors and waste products
Dr Jaffar Raza Page 21
2. PMNL’s function
Reduced Phagocytosis
Reduced intracellular killing
Reduced adherence
Impaired chemotaxis
3. crevicular fluid:
Alterations in the constituents and flow rate of crevicular fluid is noted
Dr Jaffar Raza Page 22
Treatment
a. Periodontal treatment in patient with uncontrolled diabetes is contraindicated.
b. If suspected to be a diabetic, following procedures should be performed:
1. Consult the patient’s physician.
2. Analyze laboratory tests, FBS, RBS and GTT
3. prophylactic antibiotics should be given.
4. Glucose levels should be continuously monitored and periodontal treatment
should be performed when the disease is in a wellcontrolled state.
5.Prophylactic antibiotics should be started 2 days preoperatively
Dr Jaffar Raza Page 23
Thyroid Gland
Hypothyroidism leads to cretinism in children and myxedema in adults.
There are no notable periodontalchanges.
Treatment
1. Patients with thyrotoxicosis should not receive periodontal therapy until the condition is stabilized.
2. Medications such as epinephrine, atropine should be given with caution.
3. caution with administration of sedatives and narcotics because of their diminished ability to tolerate drugs.
Dr Jaffar Raza Page 24
Pituitary Gland
Hyperpituitarism causes enlarged lips localized areas of hyperpigmentation. It is also associated with food impaction hypercementosis is seen. Hypopituitarism leads to crowding and malposition of teeth.
Dr Jaffar Raza Page 25
Parathyroid Glands Parathyroid hypersecretion produces generalized demineralization of the skeleton.
Oral changes include malocclusion and tooth mobility,
radiographically alveolar osteoporosis, widening of the periodontal space and absence of lamina dura.
Treatment:
Routine periodontal therapy must be instituted but the dental practitioner must be attuned to the oral and dental changes.
Dr Jaffar Raza
Sex Harmones
There are several types of gingival diseases in whichhormones is considered to be either
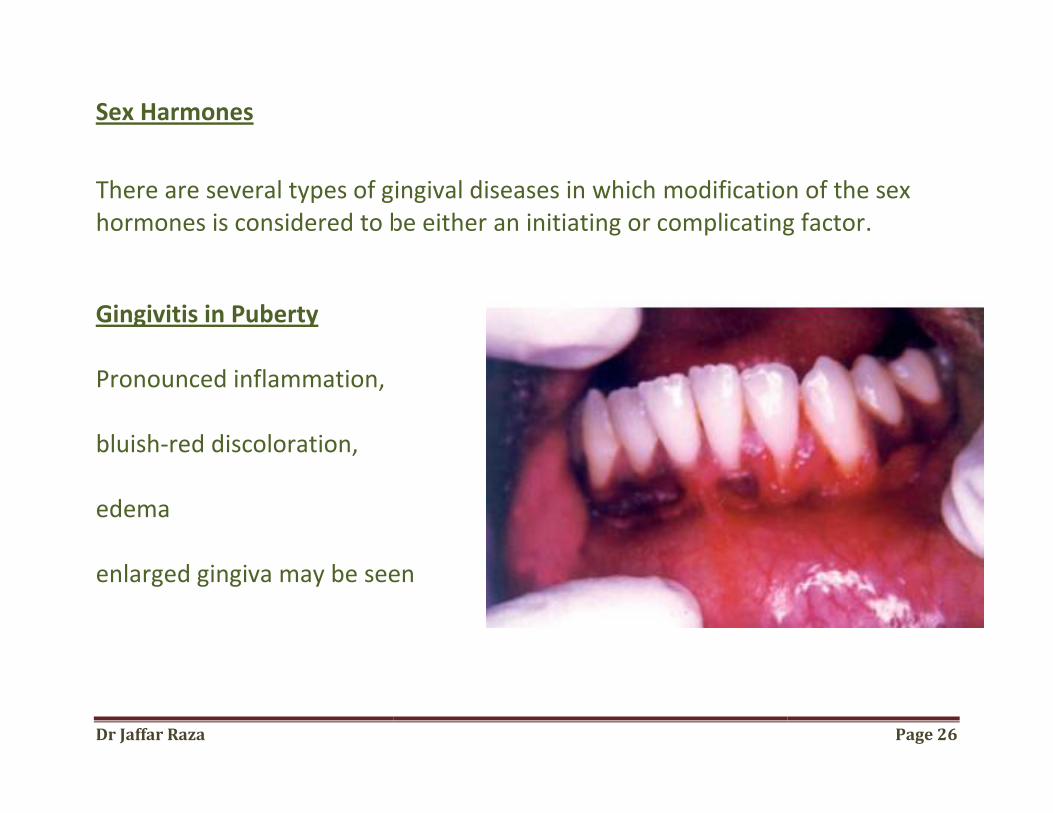
Gingivitis in Puberty Pronounced inflammation, bluish-red discoloration, edema enlarged gingiva may be seen
There are several types of gingival diseases in which modification of the sex hormones is considered to be either an initiating or complicating factor
enlarged gingiva may be seen
Page 26
modification of the sex an initiating or complicating factor.
Dr Jaffar Raza Page 27
Gingival Changes Associated with Menstrual Cycle
There is increased prevalence of gingivitis, bleeding gingiva. inreased Exudation from inflamed gingiva crevicular fluid flow is not affected. The salivary bacterialcount is increased.

Dr Jaffar Raza Page 28
Menopausal Gingivostomatitis
Clinical manifestations include
dry, shiny oral mucosa,
dry burning sensation of oral mucosa,
abnormal taste sensation
Dr Jaffar Raza
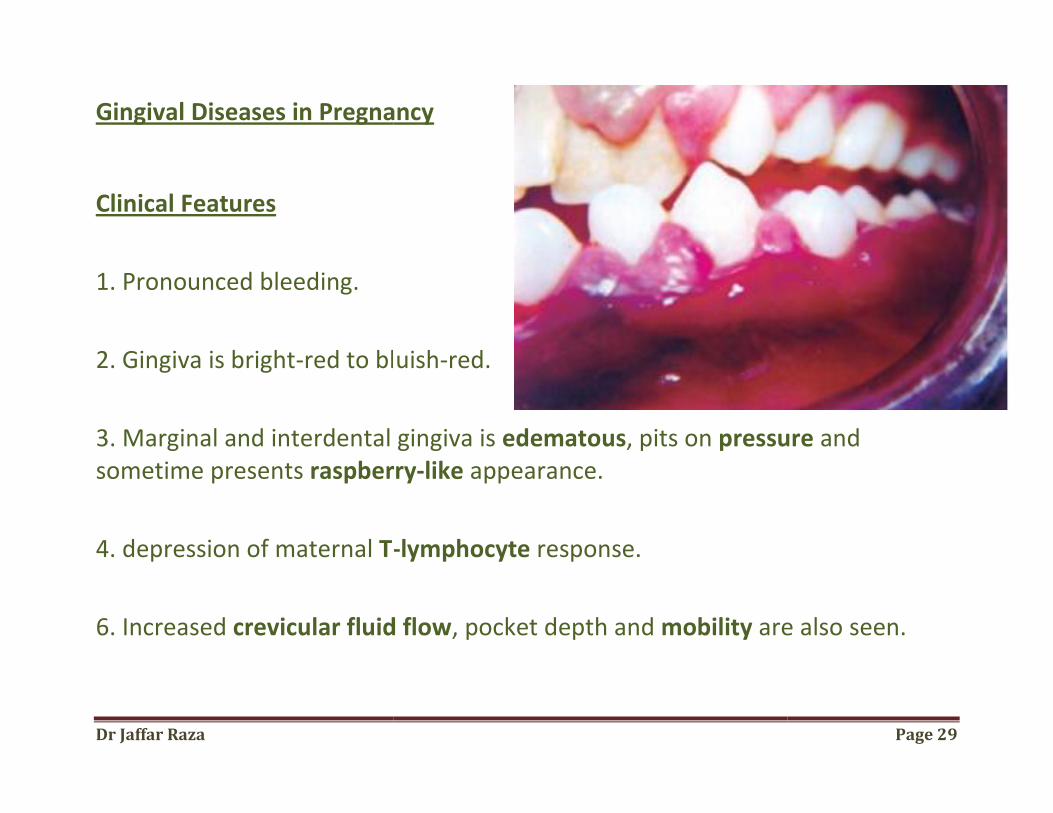
Gingival Diseases in Pregnancy
Clinical Features
1. Pronounced bleeding.
2. Gingiva is bright-red to bluish
3. Marginal and interdental gingiva is sometime presents raspberry
4. depression of maternal T-
6. Increased crevicular fluid flow
Gingival Diseases in Pregnancy
red to bluish-red.
3. Marginal and interdental gingiva is edematous, pits on pressureraspberry-like appearance.
-lymphocyte response.
crevicular fluid flow, pocket depth and mobility are also seen.
Page 29
pressure and
are also seen.
Dr Jaffar Raza
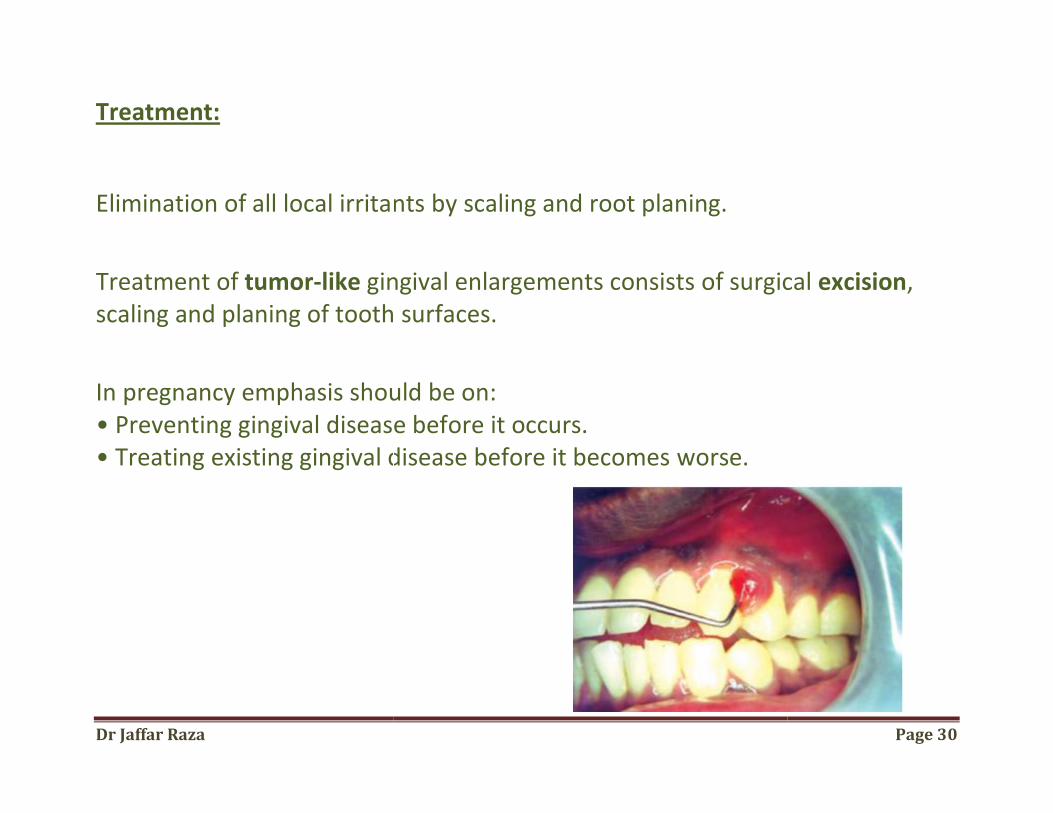
Treatment:
Elimination of all local irritants
Treatment of tumor-like gingival enlargements consistsscaling and planing of tooth surfaces.
In pregnancy emphasis should be on:• Preventing gingival disease bef• Treating existing gingival disease before it becomes
mination of all local irritants by scaling and root planing.
gingival enlargements consists of surgical scaling and planing of tooth surfaces.
In pregnancy emphasis should be on: • Preventing gingival disease before it occurs. • Treating existing gingival disease before it becomes worse.
Page 30
of surgical excision,
Dr Jaffar Raza Page 31
CARDIOVASCULAR DISEASES
Arteriosclerosis
In aged individuals, arteriosclerotic changes in the blood vessels are characterized by,
initial thickening, narrowing of lumen, thickening & hyalinization of media and adventitia
Dr Jaffar Raza Page 32
Congenital Heart Disease
oral changes includes purplish-red discoloration of the lips and gingiva sometimes severe marginal gingivitis periodontal destruction. The tongue appears coated, fissured and edematous extreme reddening of the fungiform and filliform papillae
Dr Jaffar Raza Page 33
HIV gingivitis:
In HIV gingivitis persistent, linear, easily bleeding, erythematous gingivitis.
lesions may be localized or generalized in nature.
HIV periodontitis: NUP (Necrotizing ulcerative periodontitis)
characterized by soft tissue necrosis
rapid periodontal destruction, marked interproximal bone loss.
severely painful at onset.
Dr Jaffar Raza Page 34
Treatment:
a. Instruct the patient to perform meticulous oral hygiene.
b. Scale and polish affected areas.
c. Prescribe chlorhexidine gluconate mouth rinse.
d. Reevaluation and frequent recall visits.
e. Systemic antibiotics.
f.prophylactic antifungal medication should be considered.
Dr Jaffar Raza Page 35
Metal Toxications Ingestion of metals such as mercury, lead, bismuth may result in oral manifestations
Bismuth Intoxication
gastrointestinal disturbances,
nausea, vomiting and jaundice
ulcerative gingivostomatitis
metallic taste and a burning sensation of the oral mucosa.
The tongue may be sore and inflamed.
Urticaria, and different types, bullous and purpuric lesions
bluish-black discoloration of the gingival margin
Dr Jaffar Raza Page 36
Lead Intoxication
increased salivation,
coated-tongue,
peculiar sweetish taste,
gingival pigmentation and ulceration.
steel gray dicoloration, associated with local irritation.
Dr Jaffar Raza Page 37
Mercury Intoxication
ulceration of the gingiva
destruction of underlying bone
Other Chemicals may cause necrosis of the alveolar bone with loosening and exfoliation of teeth
Phosphorus
arsenic
chromium