digitallibrary.health.nt.gov.au · web viewwhat is stakeholder engagement? to participate is to...
TRANSCRIPT
Stakeholder Engagement Framework
Aboriginal Policy & Stakeholder Engagement BranchOctober 2012
DEPARTMENT OF HEALTH
Effective stakeholder engagement enables better planned and more informed policies, projects, programs and services.1
Stakeholder engagement should be managed as one would manage any other business function. It should be made systematic by integrating it with core business activities.2
1 Department of Education and Early Childhood Development, Victoria. Stakeholder Engagement Framework, Melbourne, 2011, p2. 2 International Finance Corporation, World Bank Group, Stakeholder Engagement: A Good Practice Handbook for Companies Doing Business in Emerging Markets, 2007 p. 97.
Department of Health is a Smoke Free Workplace ii
DEPARTMENT OF HEALTH
Table of ContentsTable of Contents............................................................................................ivList of TablesviList of Figures..................................................................................................viSection A – The Business Case......................................................................11. What is Stakeholder Engagement?..........................................................12. Stakeholder Engagement – An Imperative..............................................1
2.1 Person-Centred Orientation of Health Care..........................................................................22.2 Requirements of Contemporary Governance.......................................................................32.3 The Changing Operational Environment of Government......................................................42.4 The Engagement Drivers for the Department of Health.......................................................52.5 Stakeholder Engagement – An Imperative of Our Time and Place........................................8
Section B – The Practice of Engagement......................................................93. Stakeholder Engagement – How, When and Why...................................93.1 Principles of Stakeholder Engagement............................................................................113.2 Leading Practice Guidelines............................................................................................11
4. The Impact of Stakeholder Engagement................................................134.1 The Capacity to Effectively Engage......................................................................................134.2 The Benefits of Engagement...............................................................................................134.3 The Risks of Engagement....................................................................................................144.4 The Evaluation of Engagement...........................................................................................16
Section C – Pathway to Stakeholder Engagement.....................................185. Engagement in the Department of Health..............................................18
5.1 Levels of Stakeholder Engagement.....................................................................................185.2 Role of the Stakeholder Engagement Branch......................................................................195.2.1 Governance and Monitoring Function................................................................................205.3 Current Status.....................................................................................................................215.4 The Way Forward for the Department................................................................................22
6. Engagement as an Enabler of Health.....................................................23Appendix A ..................................................................................................24Appendix B – Capable organisations and Capable Stakeholders.............25Appendix C – Spectrum of Stakeholder Engagement - Includes Capacity
Development of Organisations and Stakeholders..............26Appendix D – Case Studies Demonstrating the Spectrum of Stakeholder
Engagement............................................................................27References ...............................................................................................30
Department of Health is a Smoke Free Workplace iii

DEPARTMENT OF HEALTH
List of TablesTable 1 Spectrum of Stakeholder Engagement...............................................................10
Table 2 Leading Practice Guidelines...............................................................................12
Table 3 Evaluation Model.................................................................................................16
Table 4 SWOT Analysis...................................................................................................21
Table 5 Stakeholder Engagement Implementation Process............................................22
List of FiguresFigure 1 Risk Management Strategy.................................................................................15
Figure 2 Department of Health – Levels of Stakeholder Engagement..............................19
Figure 3 Governance Function of Stakeholder Engagement Branch................................20
Department of Health is a Smoke Free Workplace iv

DEPARTMENT OF HEALTH
Section A – The Business Case 1. What is Stakeholder Engagement?
To participate is to be human.3
Stakeholder engagement is the meaningful and purposeful involvement in the process of decision-making by persons or groups who have a vested interest in the decision and/or its outcomes. Essentially, the opportunity for people to have a say on issues that matter to them is fundamental to the democratic process.4
Stakeholder engagement can come under a variety of banners that range from citizen or consumer engagement to public or community participation. These terms are often used interchangeably. A variety of definitions that give clarity to the wider concept of engagement are presented in Appendix A.
According to Desley Renton of the International Association for Public Participation Australasia [the not-for-profit organisation established to promote public participation], stakeholder engagement is a way to ‘bridge the gap between people and the services that we provide and the policies that we deliver’.5 It is a vehicle to accountability and transparency.
2. Stakeholder Engagement – An Imperative Despite the recognition of the need to engage patients, advocates and other vested interest groups in the sphere of health care decision making, and despite the increase in consultations with the range of stakeholders and partners, there is still little shared understanding of what stakeholder engagement is and what it could be.
Across the Western World, the case for the engagement of health care stakeholders has arguably emanated from the paradigm shift that put people at the centre of their health care experience. More recently, the case has been emboldened by the engagement requirements of contemporary governance and the recognition that environment in which governments govern has irretrievably changed. Closer to home in the Northern Territory [NT], with its unique demography and complex health care challenges, the case for ‘collaboration and alignment’ between a wide variety of stakeholders is unequivocal.6
The influences and drivers for stakeholder engagement in the NT will be further explored below. In summary they are:
1. The influence of person-centric orientation of health care delivery. 2. The requirements of contemporary governance. 3. The changing operational environment of government.4. The engagement drivers for the Department of Health.
2.1 Person-Centred Orientation of Health CareIf the whole point of citizen-centred services really is to organize services around citizen’s needs and preferences, the obvious way to settle the question of how services should be joined up is to ask the users for their views.7
3 Peter Boothroyd, Canadian planning academic and practitioner.4 Department of Sustainability and Environment, Victoria. Effective Engagement: Building Relationships with Community and Other Stakeholders – Book 1 An Introduction to Engagement. Community Engagement Network, East Melbourne, 2005, p6.5 Renton D. Engaging rural communities to produce a sustainable decision. Key note address to 11th National Rural health Conference, Perth, March 2011.6 Lenihan D. Rethinking the Public Policy Process – A Public Engagement Framework. Ottawa, Public Policy Forum, 2009, p29. 7 Lenihan D. Rescuing Policy – The Case for Public Engagement. Ottawa, Public Policy Forum, 2012, p87.
Department of Health is a Smoke Free Workplace 1

DEPARTMENT OF HEALTH
Patient or person-centred care is care that is ‘relationship-based with an orientation toward the whole person’.8 The paradigm shift that placed the person at the centre of their health care experience is rooted in social justice and human rights values and was spearheaded by the World Health Organization. Today, this orientation is guaranteed by the Patient Bill of Rights and the proscriptions of the National Safety and Quality Standards. Some of the incremental shifts to person-centeredness in health care include, but are not limited to, the following:
In the immediate post-World War II period – a time when the dehumanization of war was re-appraised and the world community strove for improvements in the human condition – the newly formed World Health Organization adopted a new definition of health.9 This definition broadened the established medical definition to one that captured subjective wellbeing of the person. Just as significantly, it also coupled health with basic human rights.
The International Conference on Primary Health Care’s Declaration of Alma-Ata enshrined the principles of primary health care – principles that put people firmly at the centre of their health care experience and held out to them the previously unrealized nobility of mutual participation in their health care decision-making.10
The Ottawa Charter [plus the subsequent Jakarta Declaration and the Bangkok Charter] ushered in a new era in public health, one that differed from the traditional public health approach in its recognition of the complex inter-play of non-health factors that contribute to health and wellbeing.11 12 13 By also identifying the need for community participation and intersectoral actions in health promotion – the Charter firmly established the need for effective engagement of a range of stakeholders from inside as well as outside the traditional health care system.
The Australian Charter of Healthcare Rights is applicable to health settings anywhere in Australia. It guarantees that patients, consumers, families, carers and services providers have an understanding of their healthcare rights as well as a voice in their healthcare experience.14
The National Safety and Quality Health Service Standards are integral to the accreditation processes of all Australian health care organisations. There are ten standards, but the first two ‘set the overarching requirements for effective implementation of the remaining eight standards’.15 The first standard addresses governance and the second standard addresses partnering with consumers. The second standard calls for the ‘effective and meaningful engagement of patients in the review, design and implementation
8 US Department of Health and Human Services, Agency for Healthcare Research and Quality. Coordinating Care for Adults with Complex Care Needs in the Patient-Centred Medical Home – Challenges and Solutions [White Paper], January 2012, p4.9 The Preamble to the Constitution of the World Health Organization, adopted by the International Health Conference, New York, 1946, states:
Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.
10 The 1978 Declaration of Alma-Ata states: Article IV states – The people have the right and duty to participate individually and collectively in the planning and implementation of their health care.Article VI states – Primary health care is essential health care … made universally accessible to individuals and families in the community through their full participation. It is the first level of contact of individuals, the family, and community with the national health system bringing health care as close as possible to where people live and work, and constitutes the first elements of a continuing health care process.
11 World Health Organization. Ottawa Charter for Health Promotion – First International Conference on Health Promotion, Ottawa, Canada, November 21, 1986. 12 World Health Organisation. Jakarta Declaration on Leading Health Promotion into the 21st Century, Jakarta, Indonesia, July 1997.13 World Health Organization. Bangkok Charter for Health Promotion in a Globalized World – Sixth Global Conference on Health Promotion, Bangkok, Thailand, August 11, 2005.14 Australian Charter of Health Care Rights available at – http://www.healthdirect.org.au/download.cfm?downloadfile=859D44E0-7908-11DF-9A4B0016CBAC49B9 15 Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards, Sydney, September 2011, p4.
Department of Health is a Smoke Free Workplace 2
DEPARTMENT OF HEALTH
of services as there is evidence that suggests that engaging patients can result in improved safety, quality and efficiency’.16
2.2 Requirements of Contemporary Governance Around the world, greater engagement of citizens, clients, consumers and communities is becoming a feature of many governments and both public and private organisations. People are expecting to be able to be involved and to have a say in the business of government and in the decisions of organisations that affect their interests.17
In public purpose organizations, good governance is about more than getting the job done. Especially in non-profits and government agencies, where values typically play an important role in determining both organizational purpose and style of operation, process is as important as product. Good governance becomes more than only a means to organizational effectiveness and becomes an end in itself. Good governance is about both achieving desired results and achieving them in the right way.18
Citizen participation in decision-making is now recognized as a fundamental pre-requisite of sustainable development and is a core principle in good governance. Governance is defined as ‘the set of responsibilities and practices, policies and procedures, exercised by an agency’s executive, to provide strategic direction, ensure objectives are achieved, manage risks and use resources responsibly and with accountability’.19 Good governance is about performance as well as conformance. [Performance is how an agency uses governance arrangements to contribute to its overall performance and the delivery of goods, services or programs. Conformance is how an agency uses governance arrangements to ensure it meets the requirements of the law, regulations, published standards and community expectations of probity, accountability and openness].20 In essence, governance arrangements provide the structure to set corporate and/or clinical objectives and the means of monitoring performance against these objectives.21
Some high profile stakeholder engagement protocols in the fields of sustainable business and governance include:
The UN Division on Sustainable Development [part of the United Nations Department of Economic and Social Affairs] has established that broad public participation in decision-making is one of the fundamental prerequisites for the achievement of sustainable development.22
Triple Bottom Line Reporting [or 3P reporting – people, profits and planet] is a trend, largely driven by the stakeholders and shareholders of business and industry, where a greater emphasis is being placed on the environmental and social/community impacts of their operations in addition to the economic impacts.23
Ahead of the Game – Blueprint for the Reform of Australian Government Administration aims to improve outcomes for citizens, through more integrated services, better policy advice, maximising value for taxpayer’s money and a closer alignment of government activity to the community’s preferences. Within a culture of continuous improvement, the Blueprint encourages greater feedback from the public, better links with stakeholders,
16 ibid.17 International Conference on Engaging Communities, Brisbane, 14 – 17 August, 2005. Conference web site – accessed 13 March 2012. http://www.engagingcommunities2005.org/overview.html18 Canadian Institute on Governance Web Site – accessed 16 May 2012.http://iog.ca/en/about-us/governance/what-good-governance 19 Cancer Australia and Cancer Voices Australia. National Framework for Consumer Involvement in Cancer Control, Cancer Australia, Canberra, ACT, 2011, p15.20 ibid.21 Australian Commission on Safety and Quality in Health Care, p9. 22 United Nations Division for Sustainable Development web site – accessed 8 March 2012. http://www.un.org/esa/desa/aboutus/dsd.html23 Group of 100 Incorporated [An Association of Australia’s Senior Finance Executives from the Nation’s Business Enterprises]. Sustainability: A Guide to Triple Bottom Line Reporting. 2003, pp5,13.
Department of Health is a Smoke Free Workplace 3
DEPARTMENT OF HEALTH
and clearer accountability for the outcomes of citizens rather than individual programs.24
The first standard of the National Safety and Quality Health Service Standards addresses governance in health service organisations. It mandates that ‘health service organisations leaders implement governance systems to set, monitor and improve the performance of the organisation and communicate the importance of the patient experience and quality management to all members of the workforce’.25
2.3 The Changing Operational Environment of GovernmentGovernments need to recognize that achieving goals like a healthy population …requires collaboration and alignment between themselves and a wide variety of stakeholders. This, in turn, requires a process that involves real dialogue, ownership and responsibility, rather than competition, theatrics and intransigence.26
Health policy today is a maze of connections to other areas….It not only raises alls sorts of new cross-cutting issues – the whole policy field increasingly cross-cuts other ones. In fact, this is all part of the growing networked nature of our society.27
Technology has irrevocably changed our world and the rate of this change is rapid and far reaching – information and interconnectedness is instant. Successful corporations have adapted to this new world order – they are no longer self-contained entities that own each stage of their business process. Instead, corporations are now ‘nodes in an ever-expanding global network’ availing them of the flexibility to rapidly adapt to changing circumstances and times. 28 Governments are not currently positioned to be so nimble. The reality is that the environment in which governments govern has changed forever.29 According to the Canadian Crossing the Boundaries National Council [a not-for-profit national forum whose mission is to foster the development of Canada as an information society through a more citizen-centred approach to government and governance], governments have not adapted to this new world order because:30
Conventional government was not designed to manage complex tasks as they usually have a ‘singular’ or ’silos’ focus.
Today’s issues, like the global warming, organized crime and integrated health care systems, are exceedingly complex and require a coordinated response from a range of departments and with a high level of policy and technical expertise. Collaboration and partnerships are critical to addressing these issues – for to look at issues holistically is to bring complexity into the equation.31
The speed of change is often faster than governments’ ability to respond because governments ‘remain trapped in bureaucratic processes and structures from the past’.
An increasing array of private and non-government organizations are now players in the traditional ‘government’ space. These organizations increasingly have resources [including policy expertise] to usurp, appropriate or frustrate a government’s agenda, attract media attention and gain public support.
24 Advisory Group on Reform of Australian Government Administration. Ahead of the Game – Blueprint for the Reform of Australian Government Administration. Barton ACT, Australian Government Department of the Prime Minister and Cabinet, 2010, pp32, 74. 25 Australian Commission on Safety and Quality in Health Care, p14. 26 Lenihan 2009, p29. 27 Crossing the Boundaries/Canada 2020 Working Group. Progressive Governance for Canadians – What You Need to Know. 2007, p24.28 ibid, p20.29 ibid, p23.30 ibid, pp23-24.31 Lenihan 2009, p23.
Department of Health is a Smoke Free Workplace 4
DEPARTMENT OF HEALTH
People and organizations are connected in all kind of new ways – traditional boundaries are flexible and porous. In essence, the network has replaced the pyramid as the new metaphor of choice. The world of self-contained jurisdictions, hierarchy and silos reflects the past rather than the future.32
Not only do many governments continue to govern from within the old paradigm, public debate in the media also still proceeds as though there were simple solutions to complex problems.33
2.4 The Engagement Drivers for the Department of HealthTo encourage citizen feedback, consultation and engagement processes should be adaptable and diverse….Improving the quality and diversity of citizen feedback will help the public service to continually improve. Citizen feedback is particularly important to connect front line service delivery to policy designers. Without information on whether progress has been made, it is difficult to adjust or re-design policies and program. To improve outcomes for citizens, strong partnerships between agencies and across state, territory and local government boundaries are important.34
There was a lack of policy development process or consultation with stakeholders outside central government. Policy decisions focused on the clinical and logistical aspects of the child health checks, and engagement with the NT health sector was largely about specific implementation issues. The lack of suitable policy development meant there was insufficient regard for the diversity of the people, systems and processes already operating in the NT and insufficient focus on existing bottlenecks in the NT health care system.35
The Northern Territory [NT] is a unique jurisdiction. Despite being the third largest jurisdiction in Australia in terms of landmass, its population of only 221,000 makes it the least populated of all Australian jurisdictions. The Territory’s demographic is also very different from the rest of Australia. For example, the median age of residents is 30.3 years which is almost six years younger than the national median age; 44% of Territorians live in remote or very remote areas compared with the rest of Australia where only 2% live remotely; 33% of Territorians are of Aboriginal or Torres Strait Islander decent; and, 70% of these individuals speak English as their second, third or fourth language.36 From an economic growth perspective, in 2009 the NT’s demand for goods and services increased by 9.4% compared to a 3.3% increase nationally.37
The NT also has to address the complex challenges faced by the rest of the Australian health care system. Some of these challenges include: increasing costs; aging population; increasing burden of chronic and complex conditions including multiple co-morbidities; increasing demand for and rising cost of advanced technologies; supply and distribution of the health workforce; quality and safety challenges; and, health disparities especially for Indigenous Australians.38
While the above challenges can only be addressed by partnerships and collaboration, there are other initiatives that have explicitly called for the engagement of stakeholders. Some of these are:
The engagement of stakeholders is integral to Australian health reform. For example, the Local Hospital Networks and Medicare Locals are required to take into account the views of communities and consumers in responding to local health needs. In many cases this will mean a consumer representative
32 Crossing the Boundaries/Canada 2020 Working Group, p22.33 ibid, p23.34 Advisory Group on Reform of Australian Government Administration, p17. 35 Australian Department of Health and Aging. Evaluation of the Child Health Check Initiative and the Expanding Health Service Delivery Initiative Summary Report. Commonwealth of Australia, Canberra, 2011, p6.36 Northern Territory Department of Health. Annual Report 2010 – 2011, Casuarina, NT, 2011.37 Growing the Territory web site – accessed 16 May 2012. http://www.growing.nt.gov.au/growing_territory/nt_statistics.html 38 Armstrong BK, Gillespie JA, Leeder SR, Rubin GL, Russell LM. Challenges in health and health care for Australia. Medical Journal Australia 2007; 187[9]: pp485-489.
Department of Health is a Smoke Free Workplace 5
DEPARTMENT OF HEALTH
is included on the governing board. It is also anticipated that advisory bodies set up to advise these boards will include a consumer perspective.39
The Northern Territory Emergency Response has brought into play the need for inter-sectoral, cross-jurisdictional and multi-stakeholder engagement processes.
The NT Aboriginal Health Forum40 has called for ‘greater levels of community involvement’ as a means to benefit Aboriginal Territorians through ‘a more responsive health and family services system, improved quality and cultural security of services and improved levels of family and community functioning; all contributing to improved levels of health and wellbeing’.41 The Forum emphasises that community engagement is ‘essential to successful reform’ and indeed to the Forum meeting its objectives.42
A variety of national health care strategies have clear consumer engagement directives. For example: Fourth National Mental Health PlanConsumers, their carers and families should be actively engaged at all levels of policy and service development. They should be fully informed of service options, anticipated risks and benefits.43
National Framework for Consumer Involvement in Cancer ControlEvery aspect of the cancer journey stands to benefit from consumer involvement, at an individual level, service level, local and organisational levels, and at regional, state, national and international levels. There is sound evidence that involving consumers will lead to improved outcomes.44
National Disability Strategy It is important that people with disability have the opportunity to participate in decisions that affect their lives.
The views of people with disability are central to the design, funding, delivery and evaluation of policies, programs and services which impact on them, with appropriate support and adjustment for participation.45
Territory 2030 – Territory 2030 is the government’s 20 year strategic plan. Developed in consultation with the Territory communities, this roadmap to the future is a ‘complete package’ that sets ‘priorities for society, economic sustainability, health and wellbeing, the environment and knowledge, creativity and innovation’.46 The interrelatedness of many of the targets and the means to achieve them has firmly brought horizontal and vertical engagement into play. In fact, the plan states that one of the solutions to the Territory’s health and wellbeing challenges is the ‘need to invest in a greater service-provider mix, leveraging partnerships and collaboration to deliver improved health services in our cities, towns and communities’.47
39 Australian Department of Health and Aging web site – accessed 15 June 2012. http://www.yourhealth.gov.au/internet/yourhealth/publishing.nsf/Content/reformQA03#engaging%20consumers 40 Northern Territory Aboriginal Health Forum is a collaborative partnership consisting of the NT Government, AMSANT and the Australian Government Department of Health and Aging.41 Northern Territory Aboriginal Health Forum [NT Government, AMSANT and Australian Department of Health and Aging]. Pathways to Community Control. NT Government, No date, p3.42 Northern Territory Aboriginal Health Forum, p25.43 Commonwealth of Australia. Fourth National Mental Health Plan – An Agenda for Collaborative Government Action in Mental Health 2009 – 2014. Barton, ACT, 2009, p13,44 Cancer Australia and Cancer Voices Australia, p1. 45 Commonwealth of Australia. National Disability Strategy – 2010 – 2020. Commonwealth of Australia, Canberra, 2011, pp17, 23.46 Northern Territory Government. Territory 2030 – Strategic Plan 2009. Darwin, Department of the Chief Minister, 2009, p6.47 ibid, p44.
Department of Health is a Smoke Free Workplace 6

DEPARTMENT OF HEALTH
2.5 Stakeholder Engagement – An Imperative of Our Time and PlaceComplexity defines the public policy context of our times and the right response is to make the policy process more collaborative. Public engagement provides a sound methodology for achieving this goal. It places a new and powerful tool in our hands for building sustainable, cohesive communities at the local, regional, national and even international levels.48
While the case for stakeholder engagement has been progressive, the effective engagement of stakeholders has often been ‘ad hoc’ or even an ‘after-thought’ in the busyness and immediacy of health care at the ‘coal-face’. On the flipside, it is important to acknowledge that until recently there has never been a credible stakeholder engagement methodology, especially one that could be applied across the myriad of situations that call for the participation of people in the wider health care domain.
A credible methodology is now available for stakeholder engagement – one that is underpinned by an internationally recognized methodology that can be calibrated for the situation at hand and one that is capable of withstanding the scrutiny of evaluation. Therefore, the power inherent in the meaningful engagement of people in decisions that impact on their lives and their world is now more than an ‘idea whose time has come’49 – it is an imperative for our time and our place.
48 Lenihan 2012, p43. 49 Victor Hugo [1802 – 1885] – French poet, novelist and dramatist.
Department of Health is a Smoke Free Workplace 7

DEPARTMENT OF HEALTH
Section B – The Practice of Engagement3. Stakeholder Engagement – How, When and
Why Improving the quality and diversity of citizen feedback will help the public service to continually improve. Citizen feedback is particularly important to connect front line service delivery to policy designers. Without information on whether progress has been made, it is difficult to adjust or re-design policies and programs….To improve outcomes for citizens, strong partnerships between agencies and across state, territory and local government boundaries are important. Systems should be able to communicate with each other to ensure that all services to the public are connected and citizens only have to tell government once.50
Most jurisdictions, both within Australia and internationally, have adopted and/or modified the International Association for Public Participation’s spectrum for engagement as their practice methodology.51 This methodology outlines the spectrum of engagement activities with increasing levels of stakeholder participation and expectations.
The spectrum establishes ‘up front’ the scope of engagement activities, the level of involvement and the expectations for stakeholders. This clarity around the rules of engagement reduces the potential for conflict and false expectations and it saves time and resources. 52 For example, the model underscores how organisations should not establish a steering committee when they only want to convey information to consumers and that formal committee structures are actually required when stakeholders are expected to have a higher degree of control in the decision-making processes.
A model for engagement is presented below. This model is an adaptation of best practice models from other jurisdictions.53 54 55 56 57 58
50 Advisory Group on Reform of Australian Government Administration, p17. 51 International Association for Public Participation is a not-for-profit organisation established to advance the practice of public participation. The engagement spectrum is available at http://www.iap2.org.au/ 52 Cancer Australia and Cancer Voices Australia, 2011.53 International Association for Public Participation.54 Department of Education and Early Childhood Development, Victoria. Stakeholder Engagement Framework, Melbourne, 2011.55 Tasmania Department of Health and Human Services. Your Care, Your Say – Consumer and Community Engagement [Consultation Paper], Tasmania Government, No Date.56 Planning NSW [in partnership with NSW Department of Local Government]. Community Engagement in the NSW Planning System, Department of Planning, Sydney, 2003.57 Health Consumers Queensland. Consumer and Community Engagement Framework, Queensland Government, Brisbane, 2012.58 Government of Western Australia, Department of Health. WA Health Consumer Carer and Community Engagement Framework – For Health Services, Hospitals and WA Health following consultation across WA Health, April 2007.
Department of Health is a Smoke Free Workplace 8

DEPARTMENT OF HEALTH
Table 1 Spectrum of Stakeholder Engagement
Increasing Levels of Stakeholder Impact [Left to Right]
Inform Consult Involve Collaborate Empower
Information Giving Information Seeking
Information Sharing & Joint Planning
Participatory Decision Making
Stakeholder Leadership
Purpose of Engaging Stakeholders
To provide information to consumers and stakeholders to assist them in understanding issues, alternatives and/or solutions.
To gather information from consumers, communities and stakeholders, especially to capture ‘lived’ experiences.
To involve communities and stakeholders in the planning, policy development, delivery and evaluation of services.
To work in partnership with communities and stakeholders.
To place final decision-making in hands of stakeholders.
When to Use One-way exchange of information, eg, to assist in access to and management of health issues.
Two-way exchange of information, share views, needs and interests.
To ensure communities and stakeholders views are considered and reflected in decisions and outcomes.
To jointly develop solutions and initiatives.
To enable communities and stakeholders to decide and implement solutions/ outcomes [often within specified guidelines].
Commitment to Stakeholders
We will keep you informed.
We will keep you informed, listen to you, acknowledge your views and provide feedback.
We will work with you, consider your views and provide feedback on how your input influenced the outcomes.
We will look to you for advice and innovation in the formulation of solutions and incorporate your advice to maximum extent.
We will implement your decisions and support and complement your actions.
Methods of Engagement
Public meetings Public notices Announcements Website Fact sheets Newsletters Educations
programs
Public meetings Public hearings Focus groups [eg
CALD and communities in need]
Surveys e-Consult [Web
2.0 tools].
Workshops Forums Deliberative
polling Panels Taskforces Working parties e-Consult [Web
2.0 tools].
Reference groups
Facilitated consensus building forums
Advisory committees
Policy roundtables
Clinical networks.
Steering committees
Quality committees
Boards Participatory
governance Standing
strategic committees.
Level of Stakeholder Influence
Minimal influence. Low influence. Moderate influence.
High involvement and influence.
Community/ Stakeholder control.
*refer Appendix D - Case Studies Demonstrating the Spectrum of Stakeholder Engagement
Department of Health is a Smoke Free Workplace 9

DEPARTMENT OF HEALTH
3.1 Principles of Stakeholder EngagementThe International Conference on Engaging Communities – an initiative of the United Nations and the Government of the Queensland – was held in Brisbane in August, 2005. One of the key outcomes of this conference was the Brisbane Declaration which endorsed the core principles of community engagement. These principles are:
Integrity – when there is openness and honesty about the scope and purpose of engagement.
Inclusion – when there is an opportunity for a diverse range of values and perspectives to be freely and fairly expressed and heard.
Deliberation – where there is sufficient and credible information for dialogue, choice and decisions, and when there is space to weigh options, develop common understanding and to appreciate respective roles and responsibilities.
Influence – when people have input in designing how they participate, when policies and services reflect their involvement and when their impact is apparent.59
3.2 Leading Practice GuidelinesStakeholder engagement has to be conducted in ‘a clear, transparent manner that provides the public and all participants with a realistic understanding of the policy and decision making process and the range of possible solutions’.60 Effective engagement is premised on trust, goodwill and respect. In order to engender trust, it is critical to clarify the limits of the stakeholder’s influence in the process, especially in cases when the ultimate decision-making power rests with the government.61 The purpose of the engagement and its constraints need to be explained in an honest and clear manner so that the community understands the process and purpose. It is particularly important to be clear about the time, costs, resources and expectations.62 Unless the extent of the community’s influence is clearly articulated in the design and implementation of the engagement process, there is a real risk that this trust, goodwill and respect will be lost.63 To paraphrase Don Leinhan – it takes trust to build trust.64
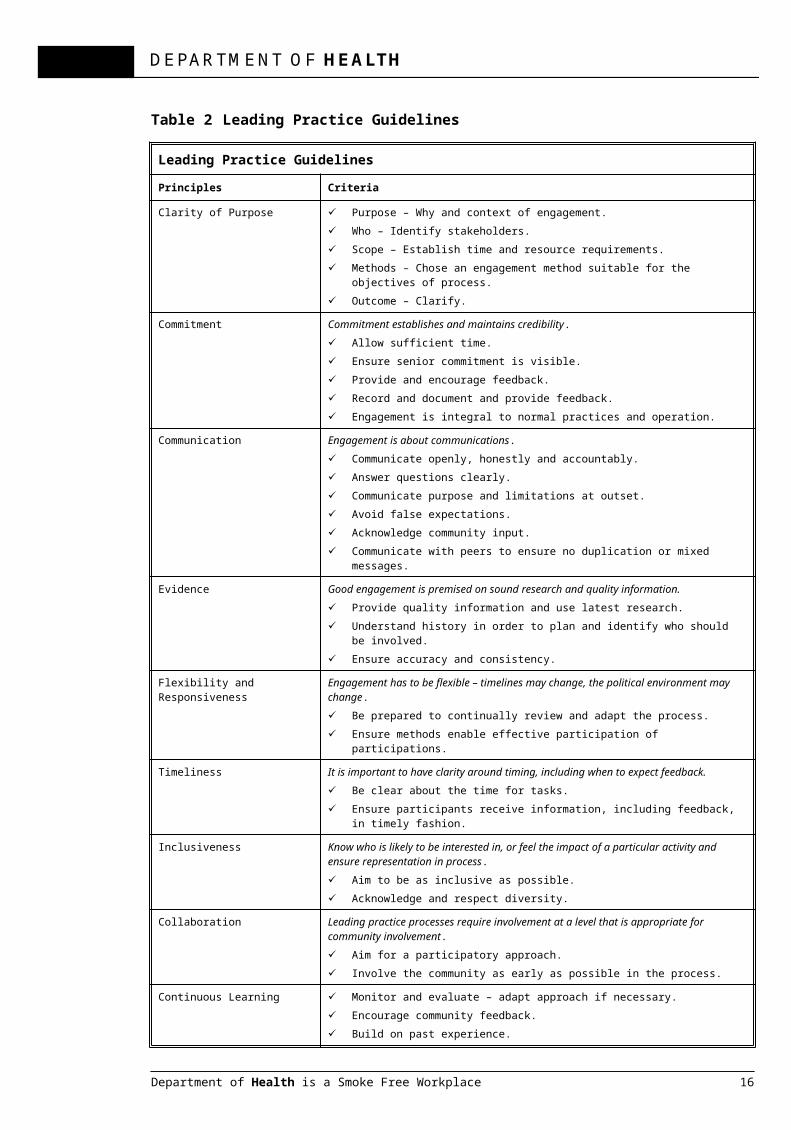
Planning NSW and the NSW Department of Local Government in their manual Community Engagement in the NSW Planning System have outlined practice guidelines to support engagement activities and to generate trust.65 These are presented in Table 2.
59 Brisbane Declaration available at Engagement Communities web site – accessed 13 March, 2012. http://www.engagingcommunities2005.org/home.html60 Planning NSW and NSW Department of Local Government. Community Engagement in the NSW Planning System, NSW Premier’s Department, Sydney, 2003, pA02-007. 61 ibid.62 ibid, ppA003-014. 63 ibid, ppB005-029. 64 Lenihan, 2012, p124.65 Planning NSW and NSW Dept of Local Government, ppB05-029, 032.
Department of Health is a Smoke Free Workplace 10

DEPARTMENT OF HEALTH
Table 2 Leading Practice Guidelines
Leading Practice Guidelines
Principles Criteria
Clarity of Purpose Purpose – Why and context of engagement. Who – Identify stakeholders. Scope – Establish time and resource requirements. Methods – Chose an engagement method suitable for the objectives of process. Outcome – Clarify.
Commitment Commitment establishes and maintains credibility. Allow sufficient time. Ensure senior commitment is visible. Provide and encourage feedback. Record and document and provide feedback. Engagement is integral to normal practices and operation.
Communication Engagement is about communications. Communicate openly, honestly and accountably. Answer questions clearly. Communicate purpose and limitations at outset. Avoid false expectations. Acknowledge community input. Communicate with peers to ensure no duplication or mixed messages.
Evidence Good engagement is premised on sound research and quality information. Provide quality information and use latest research. Understand history in order to plan and identify who should be involved. Ensure accuracy and consistency.
Flexibility and Responsiveness Engagement has to be flexible – timelines may change, the political environment may change. Be prepared to continually review and adapt the process. Ensure methods enable effective participation of participations.
Timeliness It is important to have clarity around timing, including when to expect feedback. Be clear about the time for tasks. Ensure participants receive information, including feedback, in timely fashion.
Inclusiveness Know who is likely to be interested in, or feel the impact of a particular activity and ensure representation in process. Aim to be as inclusive as possible. Acknowledge and respect diversity.
Collaboration Leading practice processes require involvement at a level that is appropriate for community involvement. Aim for a participatory approach. Involve the community as early as possible in the process.
Continuous Learning Monitor and evaluate – adapt approach if necessary. Encourage community feedback. Build on past experience. Feedback to own organisation.
Department of Health is a Smoke Free Workplace 11

DEPARTMENT OF HEALTH
4. The Impact of Stakeholder EngagementAs the word ‘delivery’ suggests, government services are viewed as things that government creates on its own and then leaves on citizens’ doorsteps, much like the morning paper or the mail. A real service partnership between government and the public must overcome a huge hurdle. It must change the way the service-delivery system [and culture] works.66
4.1 The Capacity to Effectively EngageThe National Framework for Consumer Involvement in Cancer Control has recognized that the parties to engagement – governments, consumers and organizations need the requisite capacity to support effective engagement and deliver meaningful outcomes. Organizations that are committed to stakeholder engagement should integrate consumers and other stakeholders into their organisational governance and involve them transparently in strategic planning and decisions about resource allocation.67 Consumers are described as capable when they have developed knowledge that is relevant to the engagement activity and when they are prepared and informed and able to optimise their involvement and to act as advocates.68
According to the National Framework for Consumer Involvement in Cancer Control, stakeholder engagement capable organisations and stakeholder engagement capable consumers exhibit the criteria described in Appendix B. These criteria have been added to the Stakeholder Engagement Spectrum and shown in Appendix C.
4.2 The Benefits of Engagement Policy is no longer the domain of government.69
There are significant benefits of engagement for both governments and the range of stakeholders.70 71 72 73
The benefits for governments include: Credibility and accountability
o Provides an opportunity for involvement by broader community and satisfies community expectations, desires and demands.
o Enhances the reputation of government as open, accountable and willing to listen.
o Statutory requirements are fulfilled.o Increased efficiency and effectiveness of service delivery.
Improved risk managemento Allows early identification of risks thereby reducing further costs. o Provides early notice of emerging issues – can enable government to
proactively deal with issues, thereby avoiding conflict. o Provides an opportunity for government to check its reputation and
status. Improved quality of policies and services.
o Policy and service are more practical and relevant to local communities.
66 Lenihan 2012, p75.67 Cancer Australia and Cancer Voices Australia, pp4 - 8. 68 ibid. 69 Crossing the Boundaries/Canada 2020 Working Group, p111.70 Tasmanian Alcohol, Tobacco and Other Drug Treatment Services. A Guide to Consumer Engagement, No Date.71 Department of Sustainability and Environment, Victoria. Effective Engagement: Building Relationships with Community and Other Stakeholders – Book 1 An Introduction to Engagement. Community Engagement Network, East Melbourne, 2005.72 Department of Education and Early Childhood Development, Victoria. 73 Planning NSW and NSW Department of Local Government.
Department of Health is a Smoke Free Workplace 12

DEPARTMENT OF HEALTH
The benefits of engagement for stakeholders include:
Increased access and sense of involvement.o People are more able to take part in decisions and process which interest
or affect them.o Opportunities are open for people to make informed input into planning,
policy and proposals. o The mutual sense of ‘ownership’ for all parties is enhanced through
engagement processes.o Outcomes can be achieved that more fully reflect the aspirations of the
community.o There will be more ownership of solutions to problems.o Individuals can become empowered to find local solutions.
4.3 The Risks of Engagement The core of all relationships is communication, and stakeholder engagement is essentially a complex relationship.74
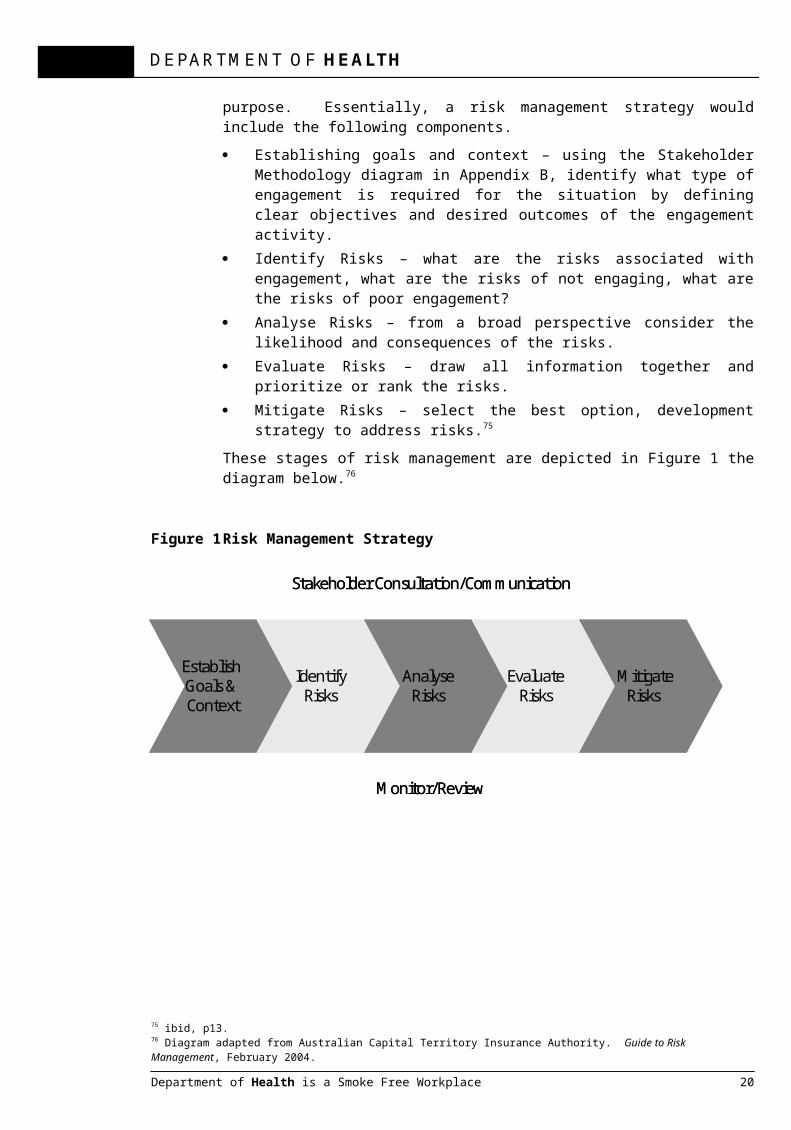
For engagement with a range of stakeholders it is recommended to have a risk management strategy in place. A risk management strategy requires a thorough understanding of the context and will of necessity be an iterative process. The Department of Health is currently revising its risk management protocols and should be utilized for this purpose. Essentially, a risk management strategy would include the following components.
Establishing goals and context – using the Stakeholder Methodology diagram in Appendix B, identify what type of engagement is required for the situation by defining clear objectives and desired outcomes of the engagement activity.
Identify Risks – what are the risks associated with engagement, what are the risks of not engaging, what are the risks of poor engagement?
Analyse Risks – from a broad perspective consider the likelihood and consequences of the risks.
Evaluate Risks – draw all information together and prioritize or rank the risks. Mitigate Risks – select the best option, development strategy to address
risks.75
These stages of risk management are depicted in Figure 1 the diagram below.76
Figure 1 Risk Management Strategy
74 Australian Department of Immigration and Citizenship. Stakeholder Engagement – Practitioner Handbook. Belconnen, ACT, 2008, p15.75 ibid, p13.76 Diagram adapted from Australian Capital Territory Insurance Authority. Guide to Risk Management, February 2004.
Department of Health is a Smoke Free Workplace 13
Establish Goals & Context
IdentifyRisks
AnalyseRisks
EvaluateRisks
MitigateRisks
Stakeholder Consultation/Communication
Monitor/Review
Establish Goals & Context
IdentifyRisks
AnalyseRisks
EvaluateRisks
MitigateRisks
Stakeholder Consultation/Communication
Monitor/Review

DEPARTMENT OF HEALTH
4.4 The Evaluation of EngagementAs with other jurisdictions, the Department of Immigration and Citizenship has incorporated the benefits of stakeholder engagement into the design of its evaluation and performance measures.77 78 An adaptation of these indicators is presented below. It is suggested that these indicators could be considered by the Department in its evaluation of stakeholder engagement activities.
Table 3 Evaluation Model
DOH STAKEHOLDER ENGAGEMENT EVALUATION MODEL 2012Inputs/Process Output Measure
1. Comprehensive stakeholder engagement plan developed and implemented for each DoH Division (excluding Corporate Services)
o Plan addresses the Good Practice Planning Principles (refer page 7 of the Stakeholder Engagement Planning Guide)
o Data recording and management mechanisms established to enable measurement of success indicators
o Key Stakeholders agreement is established either through a Memorandum of Understanding or through consultation and written agreement/sign off
Success Indicator Success Measure
2. Enhanced reputation and community confidence in Department
o Majority of sentinel or significant events effectively managed to minimise impact on reputation
o Improved reputation in NT Household survey (or equivalent)
3. Improved access to emerging issues
o Majority of sentinel or significant events identified prior to escalation
o Increased actions taken in response to issues identified in Patient Satisfaction surveys
4. Forestalling negative client and/or media actions
o Reduced letter writing, online letters, internet campaigns or media coverage aimed at changing government policy
o Reduced negative media and/or media inquiries generated as a result of a complaint
o Increased compliments received either directly or through positive media
5. Improved conflict resolution o Reduced number of complaints received directly or through HCC, Ombudsman or Ministerial inquiries
o Stakeholder survey provided to all complainants post complaint resolution to ascertain satisfaction with complaints handling process
o Increased number of system changes in response to complaints and critical incidents
o Increased numbers of complainants feeling respected and heard through the complaint resolution process
6. Increased organisational effectiveness
o Reduced instances of poor performance of duties or inappropriate behaviour reported by stakeholders
o Increased number of internal stakeholders (staff) engaging through WPP’s
o Employee engagement measures developed and reported
77 Australian Department of Immigration and Citizenship, p33.78 REVIT [Revitalising Industrial Sites – Europe] Working Towards More Effective and Sustainable Brownfield Revitalisation Policies – Stakeholder Engagement – A Toolkit. Torfaen County Borough, UK, 2007.
Department of Health is a Smoke Free Workplace 14

DEPARTMENT OF HEALTH
against
7. Consumer engagement groups and a peak body established
o Consumer representatives identified and capacity/capability developed to enable effective engagement
o Funding for consumer peak body obtained
8. Specific communities or cultural groups
o Increased complaints by Aboriginal people (who historically have low levels of complaining)
o Increased use of interpreters
o Increased number of Aboriginal people and CALD people on advisory groups and committees
Department of Health is a Smoke Free Workplace 15
DEPARTMENT OF HEALTH
Section C – Pathway to Stakeholder Engagement5. Engagement in the Department of Health
…the old approach to governance is changing….there is a real and viable alternative to governing from the centre. It aims at de-concentrating power through collaboration; at governing more from the bottom-up by moving decisions making closer to the people and situations it affects. Such a change would also strengthen democracy. It would empower communities, organizations and citizens by giving them a bigger role in setting goals and priorities and in designing and delivering the programs and services they care about. 79
A patient and consumer-focused health system is shaped around the health needs of people, their families, carers and communities.80 Stakeholder engagement is a dynamic process that can involve consumers and stakeholders in a number of roles.
5.1 Levels of Stakeholder EngagementThe Department of Health’s stakeholders include, but are not limited to:
Individuals [be they called patients or consumers]. Families. Carers. Communities. Advocacy groups. Other representative and/or vested interest groups. Every one of our staff. [Engagement of staff is often called internal
stakeholder engagement]
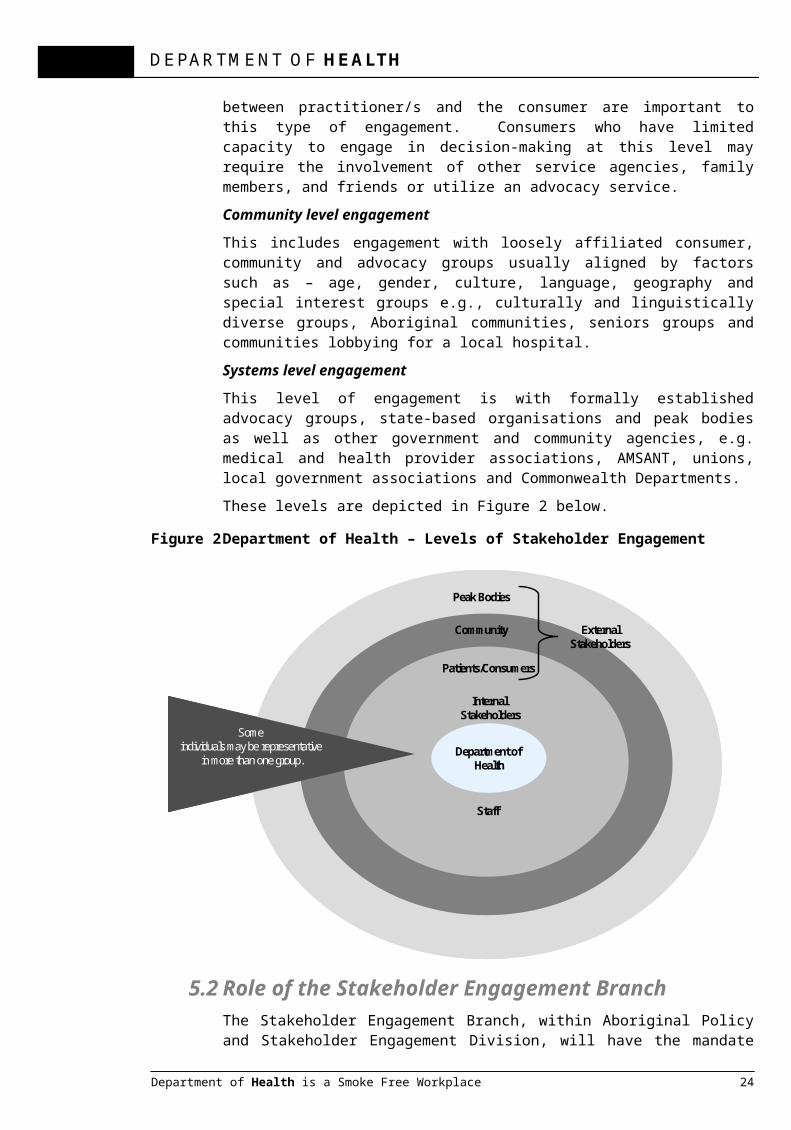
For the Department of Health, engagement of stakeholders can operate on three basic levels – the individual patient level, the community level and the systems level. These levels are somewhat artificial distinctions and are not mutually exclusive. The common dominator in all levels is the values inherent in patient and consumer-focused care/service.
Individual consumer level engagement This level involves engagement of the individual consumer or patient in decisions about their own treatment and care, and this usually would occur at the point of care. Rapport between practitioner/s and the consumer are important to this type of engagement. Consumers who have limited capacity to engage in decision-making at this level may require the involvement of other service agencies, family members, and friends or utilize an advocacy service.
Community level engagementThis includes engagement with loosely affiliated consumer, community and advocacy groups usually aligned by factors such as – age, gender, culture, language, geography and special interest groups e.g., culturally and linguistically diverse groups, Aboriginal communities, seniors groups and communities lobbying for a local hospital.
Systems level engagement This level of engagement is with formally established advocacy groups, state-based organisations and peak bodies as well as other government and
79 Crossing the Boundaries/Canada 2020 Working Group, p25.80 Tucker-Evans M [Chair, Health Consumers Qld]. How Consumers & Community Engagement Improves Health Outcomes? Presentation to Ministerial Consumer Advisory Committee – Your Voice in Health, 31 October 2011.
Department of Health is a Smoke Free Workplace 16
DEPARTMENT OF HEALTH
community agencies, e.g. medical and health provider associations, AMSANT, unions, local government associations and Commonwealth Departments.
These levels are depicted in Figure 2 below.
Figure 2 Department of Health – Levels of Stakeholder Engagement
5.2 Role of the Stakeholder Engagement BranchThe Stakeholder Engagement Branch, within Aboriginal Policy and Stakeholder Engagement Division, will have the mandate to set policy and develop a stakeholder engagement framework which will identify effective stakeholder engagement activities and structures.
The Stakeholder Engagement Branch will also have a monitoring and review function with respect to stakeholder engagement. In conjunction with the Executive Leadership Team, the Branch will identify key performance indicators [KPIs] which will apply to stakeholder engagement activities across the Department.
5.2.1 Governance and Monitoring FunctionAs the very act of monitoring can be a catalyst for improvement, it is proposed that a governance function should be implemented to monitor and to bring a quality assurance lens to stakeholder engagement activities. This would be accomplished via the development and monitoring of KPIs. The KPIs would be adopted in concert with Divisions and the Executive Leadership Team. [Note – Section 4.4 has examples of performance measures adopted by other jurisdictions.]
While engagement activities would reside with the relevant Divisions, the monitoring function would be centralized within the Stakeholder Engagement Branch. This governance function is depicted in Figure 3 below. It will be also noted that this diagram is in effect a quality improvement (or Plan-Do-Study-Act) cycle.
Department of Health is a Smoke Free Workplace 17
Department of Health
Patients/Consumers
Community
Peak Bodies
External Stakeholders
Staff
Some individuals may be representative
in more than one group.
Internal Stakeholders
Department of Health
Patients/Consumers
Community
Peak Bodies
External Stakeholders
Staff
Some individuals may be representative
in more than one group.
Internal Stakeholders

DEPARTMENT OF HEALTH
Figure 3 Governance Function of Stakeholder Engagement Branch
Department of Health is a Smoke Free Workplace 18
MEASURE
Stakeholder Engagement Branch Governance & Monitoring Function
REVIEW
DivisionsReview Feedback
Implement Continuous QualityImprovement Initiatives
PLAN
APSEDevelop
Stakeholder Engagement Framework & Develop KPIs
for Engagement at Community Level &
Systems Level
APSEMonitor Performance
OutcomesAcross All Divisions & Provide Feedback
IMPLEMENT
DivisionsImplement Effective Stakeholder
Engagement Initiatives
MEASURE
Stakeholder Engagement Branch Governance & Monitoring Function
REVIEW
DivisionsReview Feedback
Implement Continuous QualityImprovement Initiatives
REVIEW
DivisionsReview Feedback
Implement Continuous QualityImprovement Initiatives
PLAN
APSEDevelop
Stakeholder Engagement Framework & Develop KPIs
for Engagement at Community Level &
Systems LevelPLAN
APSEDevelop
Stakeholder Engagement Framework & Develop KPIs
for Engagement at Community Level &
Systems Level
APSEMonitor Performance
OutcomesAcross All Divisions & Provide Feedback
IMPLEMENT
DivisionsImplement Effective Stakeholder
Engagement Initiatives
IMPLEMENT
DivisionsImplement Effective Stakeholder
Engagement Initiatives

DEPARTMENT OF HEALTH
5.3 Current Status The principle of patient-centred health care is almost universally accepted….but putting it into practice is not so easy. For one thing, we must be willing to work across or even redraw some deeply entrenched boundaries around roles and responsibilities, which, in turn, can and often does challenge powerful interests. Second, we must be willing to collect, use and share information in new ways, which, in turn, raises questions about personal privacy.81
Like patient-centred health care, the need for Stakeholder Engagement is almost universally accepted. However, to implement effective stakeholder engagement processes within the Department of Health will be an iterative process of ongoing refinement and adaptation.
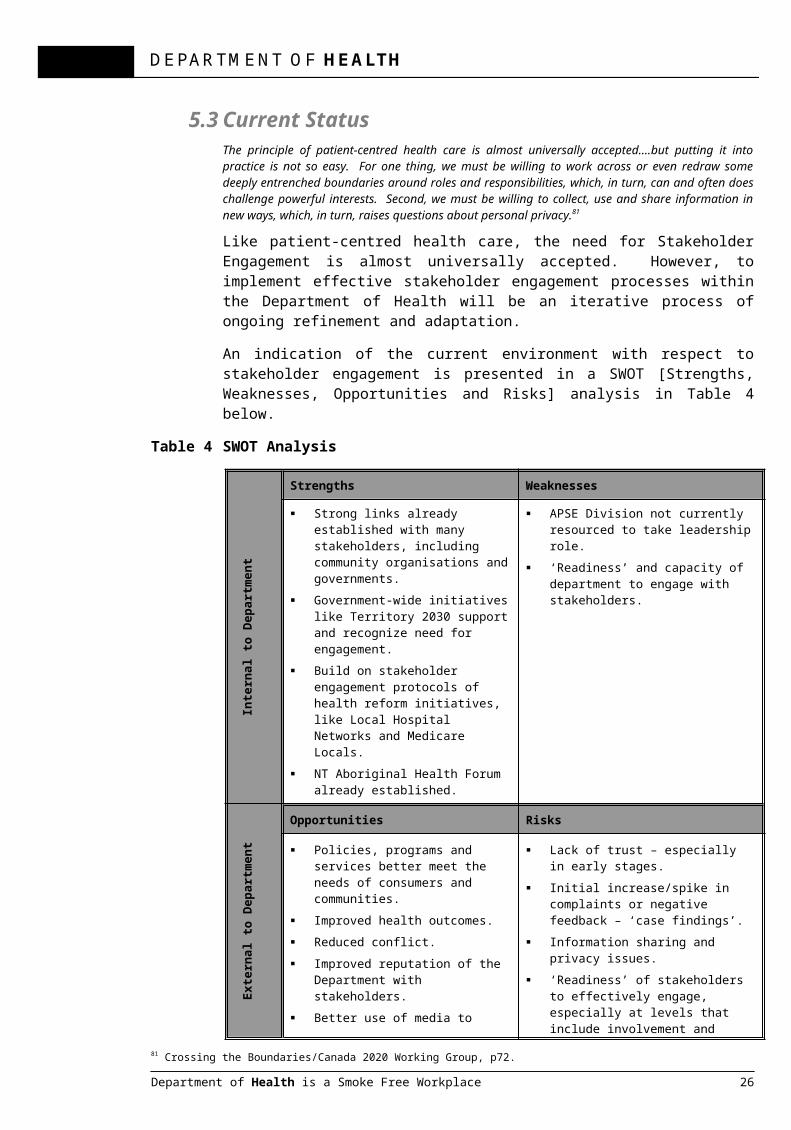
An indication of the current environment with respect to stakeholder engagement is presented in a SWOT [Strengths, Weaknesses, Opportunities and Risks] analysis in Table 4 below.
Table 4 SWOT Analysis
Inte
rnal
to D
epar
tmen
t
Strengths Weaknesses
Strong links already established with many stakeholders, including community organisations and governments.
Government-wide initiatives like Territory 2030 support and recognize need for engagement.
Build on stakeholder engagement protocols of health reform initiatives, like Local Hospital Networks and Medicare Locals.
NT Aboriginal Health Forum already established.
APSE Division not currently resourced to take leadership role.
‘Readiness’ and capacity of department to engage with stakeholders.
Exte
rnal
to D
epar
tmen
t
Opportunities Risks
Policies, programs and services better meet the needs of consumers and communities.
Improved health outcomes. Reduced conflict. Improved reputation of the
Department with stakeholders. Better use of media to understand
complexities of health care delivery in NT.
Lack of trust – especially in early stages.
Initial increase/spike in complaints or negative feedback – ‘case findings’.
Information sharing and privacy issues.
‘Readiness’ of stakeholders to effectively engage, especially at levels that include involvement and collaboration.
Expectations that NT will follow other jurisdictions and establish a consumer advisory group or the NT will be pressured to prematurely establish advisory group.
81 Crossing the Boundaries/Canada 2020 Working Group, p72.
Department of Health is a Smoke Free Workplace 19
DEPARTMENT OF HEALTH
5.4 The Way Forward for the DepartmentThe Department and a range of other organisations make up the Northern Territory health service system or sector. This system operates across vast and sometimes sparsely populated areas and serves a diverse range of individuals, families and communities with multiple health and wellbeing needs….The Department engages on many levels with a range of partner in the health service system. We aim to develop robust and transparent partnerships, based on mutual trust, with the non government sector and with other service providers in order to improve planning and delivery of services.82
It is acknowledged that going forward with Stakeholder Engagement will be an iterative process in order to develop the appropriate capacity, capabilities and resources.
A suggested way forward is to adapt the Western Australian staged approach to the uptake of stakeholder engagement. This approach positioned stakeholder engagement as a ‘core’ activity for all health services and included it in the cycle of planning, implementation, delivery and evaluation of all aspects of health service delivery. Its vision is to ultimately have consumer or community representation on all committees, reference or working groups that deal with any aspects of consumers and/or carers human or legal rights and/or health service provision.83
A proposed staged approach for the Department of Health’s Stakeholder Engagement Branch is presented in Table 5 below.
Table 5 Stakeholder Engagement Phased Implementation Plan
Phased Approach to Stakeholder Engagement Capacity and Capability
Timelines Actions by Stakeholder Engagement Branch
Phase 1/Year 1 Establish engagement structures and processes.Develop plans and policies.Identify and acquire resources.Assist Divisions with development of engagement plans.In conjunctions with Division, reach agreement on evaluation processes and/or KPIs.Facilitate engagement processes across Divisions.
Phase 2/Year 2 Review and revise relevant plans.Refine strategies and processes.
Phase 3/Year 3 Stakeholder engagement is ‘bedded down’ and is part of core business.
To achieve its goals of effective engagement of stakeholders, the Department of Health may wish to also adopt the Western Australian approach of supporting consumer and carer groups to build their engagement capacity and capability. The Stakeholder Engagement Branch could be positioned to develop this capacity with both external and internal stakeholders.
82 Northern Territory Department of Health. Annual Report 2010 – 2011, p141.83 Government of Western Australia, Department of Health, 2007, p14.
Department of Health is a Smoke Free Workplace 20

DEPARTMENT OF HEALTH
6. Engagement as an Enabler of HealthEffective stakeholder engagement enables better planned and more informed policies, projects, programs and services.84
Stakeholder engagement is recognized as an enabler of better health programs and services; and, better programs and services yield better health outcomes. Stakeholder engagement also embodies the values of human dignity and social justice. These values have anchored health care since the World Health Organisation’s proclamation of 1948 that stated:
The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.85
The achievement of this standard of health can be advanced by the effective engagement of health’s stakeholders – be they patients, carers, advocates or representative organisations.
84 Department of Education and Early Childhood Development, Victoria, p2. 85 Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19 June – 22 July, 1946 [signed on 22 July 1946 by the representatives of 61 states and entered into force on 7 April 1948].
Department of Health is a Smoke Free Workplace 21

DEPARTMENT OF HEALTH
Appendix A Stakeholder engagement can come under a variety of banners that range from citizen or consumer engagement to public or community participation. These terms are often used interchangeably. Some definitions that add clarity to the wider concept of engagement are:
Stakeholders – persons or groups who are directly or indirectly affected by a project, as well as those who may have interest in a project and/or the ability to influence its outcome, either positively or negatively.86
Citizens – can refer to any or all of the following: the public, stakeholders, customers, clients, community organizations and the like.87
Engagement – a generic, inclusive term to describe the broad range of interactions between people.88
Key stakeholder – any stakeholder with significant influence on or significantly impacted by the work and where these interests and influence must be recognised if the work is to be successful.89
Stakeholder engagement – captures public processes in which the general public and other interested parties are invited to contribute to particular proposals or policy changes.90
Stakeholder engagement – is a way of thinking about external audiences and their relationship to organizational outcomes. It implies a longer term relationship where both parties have a mutual interest in, and ability to impact upon, the project outcomes.91
Community engagement – the arrangements for citizens and communities to participate in the processes used to make good policy and to deliver on programs and services.92
Consumer, carer and community engagement is the process by which the aspirations, concerns, needs and values of citizens and communities are incorporated in government, non-government and private sector decision making, planning service delivery and evaluation.93
86 International Finance Corporation [World Bank Group]. Stakeholder Engagement: A Good Practice Handbook for Companies Doing Business in Emerging Markets. Washington, DC, 2007, p10.87 Lenihan, 2012, pp61-75. 88 Department of Sustainability and Environment, Victoria, 2005, p10.89 Australian Department of Immigration and Citizenship, p3.90 Planning NSW and NSW Department of Local Government, ppA02-006. 91 Department of Sustainability and Environment, Victoria, p41.92 Health Consumers Queensland. Consumer Engagement Framework, Queensland Health, 2010, p6.93 Government of Western Australia, Department of Health, 2007, p4.
Department of Health is a Smoke Free Workplace 22

DEPARTMENT OF HEALTH
Appendix B – Capable organisations and Capable StakeholdersThe qualities of Stakeholder Engagement Capable Organisations include: Governance – governance structures [including boards and committees, policies and
procedures] incorporate the principles, values and elements of effective consumer participation.
Cultural elements – active involvement of people with respect to their cultural needs, e.g., Aboriginal and Torres Strait Islander communities, culturally and linguistically diverse communities and rural and remote communities.
Clear objectives – consumer involvement is informed by clear objectives in Terms of Reference documents, policies and procedures to assist consumers and departmental staff to understand their role requirements and the context within which they participate.
Resources and support – organisations adequately resource and provide appropriate support to enable engagement activities, including sitting fees, travel, accommodation and out-of-pocket expenses.
Education and training – training and development opportunities are made available to assist consumers and staff in their roles.
Facilitation – organisations actively facilitate and coordinate consumer involvement activities.
Research, data and evaluation – organisations monitor consumer involvement activities and research and evaluate strategies to build continuous quality improvement and benchmarking. 94 95
The qualities of Capable Stakeholders and Consumers include: Experience – consumers/stakeholders have experience relevant to the task at hand, this
may include experience as a patients, carer or family members. Motivation – consumers are motivated, with an interest in participating in a largely
voluntary role to improve outcomes for others. Capacity – consumers have or are able to develop their skills and capabilities to meet
the requirements of the role. [Consumers may need to undertake learning and development and/or mentoring opportunities to build their expertise.]
Understanding of context – consumers have an understanding of the context within which they participate and understand the types of engagement and the expectations.
Consumer networks – consumers may need to perform their role via involvement in consumer organisations or advocacy organisations, etc. 96 97
The capacity of consumers and organisations has been added to the Stakeholder Engagement Spectrum and is presented in Appendix C.
94 Cancer Australia and Cancer Voices Australia, p7ff. 95 Planning NSW and NSW Department of Local Government, ppA003-014. 96 Cancer Australia and Cancer Voices Australia, p7ff. 97 Planning NSW and NSW Department of Local Government, ppA003-014.
Department of Health is a Smoke Free Workplace 23
DEPARTMENT OF HEALTH
Appendix C – Spectrum of Stakeholder Engagement - Includes Capacity Development of Organisations and Stakeholders
Increasing Levels of Stakeholder Impact [Left to Right]Inform Consult Involve Collaborate Empower
Information Giving Information Seeking
Information Sharing & Joint Planning
Participatory Decision Making
Stakeholder Leadership
Purpose of Engaging Stakeholders
To provide information to consumers and stakeholders to assist them in understanding issues, alternatives and/or solutions.
To gather information from consumers, communities and stakeholders, especially to capture ‘lived’ experiences.
To involve communities and stakeholders in the planning, policy development, delivery and evaluation of services.
To work in partnership with communities and stakeholders.
To place final decision-making in hands of stakeholders.
When to Use One-way exchange of information, eg, to assist in access to and management of health issues.
Two-way exchange of information, share views, needs and interests.
To ensure communities and stakeholders views are considered and reflected in decisions and outcomes.
To jointly develop solutions and initiatives.
To enable communities and stakeholders to decide and implement solutions/ outcomes [often within specified guidelines].
Commitment to Stakeholders
We will keep you informed.
We will keep you informed, listen to you, acknowledge your views and provide feedback.
We will work with you, consider your views and provide feedback on how your input influenced the outcomes.
We will look to you for advice and innovation in the formulation of solutions and incorporate your advice to maximum extent.
We will implement your decisions and support and complement your actions.
Methods of Engagement
Public meetings Public notices Announcements Website Fact sheets Newsletters Educations
programs.
Public meetings Public hearings Focus groups
[eg CALD and communities in need]
Surveys e-Consult [Web
2.0 tools].
Workshops Forums Deliberative
polling Panels Taskforces Working parties e-Consult [Web
2.0 tools].
Reference groups
Facilitated consensus building forums
Advisory committees
Policy roundtables
Clinical networks.
Steering committees
Quality committees Boards Participatory
governance Standing strategic
committees.
Level of Stakeholder Influence
Minimal influence. Low influence. Moderate influence.
High involvement and influence.
Community/ Stakeholder control.
Consumer Capacity
Health literacy. Communication abilities.Understanding of context.
Understanding of objectives.Strategic thinking.Ability to represent the broad view.
Credible knowledge and experience.Shared responsibility.Produce mutual objectives.
Steer to clear objectives.
Organisational Capacity
Effective communication
Effective consultation
Building consumer involvement into all aspects of organisation.Networking.
Consumers fully integrated into boards, working parties, best practice improvements and all aspects of organisations.
Commits objective/s to consumers & acts on outcomes. Consumers involved in setting objectives, policies and strategic directions.
.
Department of Health is a Smoke Free Workplace 24

DEPARTMENT OF HEALTH
Department of Health is a Smoke Free Workplace 25
DEPARTMENT OF HEALTH
Appendix D – Case Studies Demonstrating the Spectrum of Stakeholder Engagement Case Study: InformEngaging stakeholders through information giving
The ‘Take Own Leave’ (TOL) project undertook qualitative research to understand, from a patient’s perspective, the decision making behind why patients leave Royal Darwin Hospital (RDH) without the agreement of their healthcare team. An important outcome of the project was to accurately inform hospital staff (internal stakeholders) about the rates and reasons people chose to take their own leave.
Historically, patients who take their own leave have been widely known as ‘absconders’; being ‘absent without leave’; or being ‘discharged against medical advice’. These terms are loaded with pejorative connotations and may be used to indicate a belief by staff that the patient is not concerned about their health, something that can lead to lower quality care for the patient and a reduction in job satisfaction and morale for hospital staff. Additionally the study uncovered a perception amongst some hospital staff that the rate which patients take their own leave from Royal Darwin Hospital (RDH) is high when compared with similar hospitals in the Territory.
The project was able to ascertain (and ultimately Inform staff) that RDH has a lower rate of TOL when compared to the average for the NT and that, from a patient’s perspective, their actions did not necessarily reflect a lightly made or ill-considered decision.
The reasons for people taking their own leave included a lack of understanding of the treatment they were receiving, loneliness, fear, communication and language barriers between staff and patient, unhappiness with the hospital service, feeling that the treatment had finished, and family obligations.
The recommendations from the study provided important information to the hospital and its staff about why people choose to take their own leave. Having access to this type of qualitative information enables hospital staff to be more aware of the issue from a patient perspective. Changes were made to the discharge codes on the hospital patient database to indicate whether a patient TOL without notifying staff or TOL following a discussion as to risk and therefore ‘discharged against medical advice’. This allows for more accurate data/reporting.
Case Study: ConsultEngaging stakeholders through information seeking
The Elective Surgery Waitlist Project was a project undertaken to gather information on why Aboriginal people have higher rates of non-attendance for elective surgery than members of the mainstream community.
A project officer was employed to consult with community Doctors, Nurses, Aboriginal Health Workers and Medical Boards in addition to a diverse selection of Aboriginal people in communities. Information was gathered about what people saw as the reasons for non-attendance and to gauge their understanding of RDH’s procedures and guidelines including what medical assistance was available. Information about where the current system could be improved and what measures had been successfully implemented to assist people when they needed to travel for elective surgery was also gathered.
The consultation revealed issues such as:
Department of Health is a Smoke Free Workplace 26

DEPARTMENT OF HEALTH
A lack of knowledge at the community level about RDH’s services, procedures and guidelines including what assistance/support is available for Indigenous people from remote areas
Poor communication about what medical procedures clients were having and what to do before having a procedure eg fasting
Poor communication about timing eg clients thought their surgery was cancelled when in fact it was rescheduled
The project demonstrated the need for resources to educate people about what elective surgery and waiting lists meant. As a result, a DVD in various NT Aboriginal languages and an accompanying flip chart were developed and distributed to clinics and hospitals. The project data was used by the Indigenous Services Support Unit at RDH to support a successful request for project funding from an NGO. The funding allows for two Indigenous Liaison Officers (ILOs) to regularly visit remote areas to educate people about elective surgery, conduct consumer consultation, and seek feedback on hospital services.
Case Study: InvolveEngaging stakeholders through information sharing and joint planning
The Northern Territory Aboriginal Health Forum (NTAHF or ‘the Forum’) has been established to:
Contribute to policy and planning in Aboriginal primary health care; Decide on key issues about regional planning; Provide a planning & policy interface between the partnership agencies and national
or external factors which impact on Aboriginal health in the NT.
The NTAHF is a partnership between the Aboriginal Medical Services Alliance of the Northern Territory (AMSANT), the Northern Territory Department of Health (NT DoH) and the Commonwealth Department of Health and Ageing (DoHA) through its Office of Aboriginal and Torres Strait Islander Health (OATSIH).
It is the vehicle through which the Northern Territory Agreement on Aboriginal Health is implemented. It has also developed the ‘Pathways to Community Control’ framework to further promote Aboriginal community control in the provision of Primary Health Care Services.
Case Study: CollaborateEngaging Stakeholders through participatory decision making
The Northern Territory Community Advisory Group on Mental Health (NTCAG) was established to provide an ongoing mechanism for consumer and carer input into mental health policy decision making processes, particularly in relation to the implementation of the National Mental Health Plan.
Among other advisory and representative functions, the Group assists the Minister in the formulation and implementation of mental health policies, plans and legislation to ensure they best meet the needs and requirements of people (and their carers) with mental health problems or mental disorders. An example of the work undertaken by the NTCAG is the collaboration with the Northern Territory Police Force and Department of Health to develop the Protocol for Cooperative Arrangements in Mental Health matters in line with the secure care amendments to the Mental Health and Related Services Act.
The NTCAG has also provided a Northern Territory consumer and carer perspective in the
Department of Health is a Smoke Free Workplace 27
DEPARTMENT OF HEALTH
development of National initiatives and polices including:
Roadmap for National Mental Health Reform – 2012-2022 National Mental Health Service Planning Framework National Mental Health Recovery Framework National Consumer Experiences of Care Project
Case Study: EmpowerEngaging stakeholders through stakeholder leadership
An Aboriginal Community Controlled Health Service is a primary health care service initiated and operated by the local Aboriginal community to deliver health care to that community, through a locally elected Board of Management.
Aboriginal communities operate over 150 ACCHS in urban, remote and regional and remote Australia. They range from large multi-functional services employing several medical practitioners and providing a wide range of services, to small services which rely on Aboriginal Health Workers and /or nurses to provide the bulk of primary care services, often with a preventive, health education focus. The services form a network, but each is autonomous and independent both of one another and of government.
The integrated primary health care model adopted by ACCHS’s is in keeping with the philosophy of Aboriginal community control and the holistic view of health. Addressing the ill health of Aboriginal people can only be achieved by local Aboriginal people controlling health care delivery.
In the Territory, the move to increased empowerment of Aboriginal communities through the implementation of ACCHS’s has not been without challenges, including difficulties accessing people with relevant skills/capacity and difficulties effectively managing the conflicting priorities of stakeholders. Overcoming these challenges requires commitment and determination, demonstrating the importance of allowing communities to determine the level of engagement that is appropriate for them.
Department of Health is a Smoke Free Workplace 28

DEPARTMENT OF HEALTH
ReferencesAdvisory Group on Reform of Australian Government Administration. Ahead of the Game – Blueprint for the Reform of Australian Government Administration. Barton ACT, Australian Government Department of the Prime Minister and Cabinet, 2010. http://www.dpmc.gov.au/publications/aga_reform/aga_reform_blueprint/docs/APS_reform_blueprint.pdf
Armstrong BK, Gillespie JA, Leeder SR, Rubin GL, Russell LM. Challenges in health and health care for Australia. Medical Journal Australia 2007; 187[9]: 485-489.
Australian Capital Territory Insurance Authority. Guide to Risk Management, February 2004.
Australian Charter of Health Care Rights is available at: http://www.healthdirect.org.au/download.cfm?downloadfile=859D44E0-7908-11DF-9A4B0016CBAC49B9
Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards, Sydney, September 2011. http://www.safetyandquality.gov.au/internet/safety/publishing.nsf/Content/CA1C4B7F4C5B5547CA257793000528D5/$File/NSQHS-Standards-Sept2011.pdf
Australia Department of Health and Aging. Evaluation of the Child Health Check Initiative and the Expanding Health Service Delivery Initiative Summary Report. Commonwealth of Australia, Canberra, 2011.
Australian Department of Immigration and Citizenship. Stakeholder Engagement – Practitioner Handbook. Belconnen, ACT, 2008. http://www.immi.gov.au/about/stakeholder-engagement/_pdf/stakeholder-engagement-practitioner-handbook.pdf
Brisbane Declaration web site: http://www.engagingcommunities2005.org/home.html
Canadian Institute on Governance web site: http://iog.ca/en/about-us/governance/what-good-governance
Cancer Australia and Cancer Voices Australia. National Framework for Consumer Involvement in Cancer Control, Cancer Australia, Canberra, ACT, 2011.
Commonwealth of Australia. Fourth National Mental Health Plan – An Agenda for Collaborative Government Action in Mental Health 2009 – 2014. Barton, ACT, 2009.
Commonwealth of Australia. National Disability Strategy 2010 – 2020. Commonwealth of Australia, Canberra, 2011.
Crossing the Boundaries/Canada 2020 Working Group. Progressive Governance for Canadians – What You Need to Know. 2007.
Department of Education and Early Childhood Development, Victoria. Stakeholder Engagement Framework, Melbourne, 2011. http://www.eduweb.vic.gov.au/edulibrary/public/commrel/policy/oct2011stakeholderengagement.pdf
Department of Sustainability and Environment, Victoria. Effective Engagement: Building Relationships with Community and Other Stakeholders – Book 1 An Introduction to Engagement. Community Engagement Network, East Melbourne, 2005.
Government of Western Australia, Department of Health. WA Health Consumer Carer and Community Engagement Framework – For Health Services, Hospitals and WA Health following consultation across WA Health, April 2007.
Group of 100 Incorporated [An Association of Australia’s Senior Finance Executives from the Nation’s Business Enterprises]. Sustainability: A Guide to Triple Bottom Line Reporting. 2003.
Health Consumers Queensland. Consumer and Community Engagement Framework, Queensland Government, Brisbane, 2012.
Health Consumers Queensland. Consumer Engagement Framework, Queensland Health, 2010.
Department of Health is a Smoke Free Workplace 29

DEPARTMENT OF HEALTH
International Association for Public Participation web site: http://www.iap2.org.au/
International Conference on Engaging Communities, Brisbane, 14 – 17 August, 2005 web site: http://www.engagingcommunities2005.org/overview.html.
International Finance Corporation [World Bank Group]. Stakeholder Engagement: A Good Practice Handbook for Companies Doing Business in Emerging Markets. Washington, DC, 2007. http://www.ifc.org/ifcext/enviro.nsf/attachmentsbytitle/p_stakeholderengagement_full/$file/ifc_stakeholderengagement.pdf
Lenihan D. Rethinking the Public Policy Process – A Public Engagement Framework. Ottawa, Public Policy Forum, 2009. http://www.ppforum.ca/sites/default/files/FRAMEWORK%20PAPER%20.pdf
Lenihan D. .Rescuing Policy – The Case for Public Engagement, Ottawa, Public Policy Forum, 2012. http://www.ppforum.ca/sites/default/files/rescuing_policy_ebook.pdf
Northern Territory Aboriginal Health Forum [Northern Territory Government, Aboriginal Medical Services Alliance Northern Territory and Australian Department of Health and Aging]. Pathways to Community Control. Northern Territory Government, No date. http://www.amsant.org.au/documents/article/114/Final_Pathways%20to%20Community%20Control.pdf
Northern Territory Department of Health. Annual Report 2010 – 2011, Casuarina, NT, 2011.
Northern Territory Government. Territory 2030 – Strategic Plan 2009. Darwin, Department of the Chief Minister, 2009.
Planning NSW and NSW Department of Local Government. Community Engagement in the NSW Planning System, NSW Premier’s Department, Sydney, 2003. http://www.communitybuilders.nsw.gov.au/community_engagement_handbook_part_1.pdf
Renton D. Engaging rural communities to produce a sustainable decision. Key note address to 11th National Rural health Conference, Perth, March 2011.
REVIT [Revitalising Industrial Sites – Europe] Working Towards More Effective and Sustainable Brownfield Revitalisation Policies – Stakeholder Engagement – A Toolkit. Torfaen County Borough, UK, 2007. http://www.revit-nweurope.org/download/REVIT_booklet.pdf
Tasmania Department of Health and Human Services. Your Care, Your Say – Consumer and Community Engagement [Consultation Paper], Tasmania Government, No Date.
Tasmanian Alcohol, Tobacco and Other Drug Treatment Services. A Guide to Consumer Engagement, No Date.
Tucker-Evans M [Chair, Health Consumers Qld]. How Consumers & Community Engagement Improves Health Outcomes? Presentation to Ministerial Consumer Advisory Committee – Your Voice in Health, 31 October 2011.
United Nations Division for Sustainable Development web site: http://www.un.org/esa/desa/aboutus/dsd.html
US Department of Health and Human Services, Agency for Healthcare Research and Quality. Coordinating Care for Adults with Complex Care Needs in the Patient-Centred Medical Home – Challenges and Solutions [White Paper], January 2012.
World Health Organization. Ottawa Charter for Health Promotion – First International Conference on Health Promotion, Ottawa, Canada, November 21, 1986. http://www.who.int/hpr/NPH/docs/ottawa_charter_hp.pdf
World Health Organisation. Jakarta Declaration on Leading Health Promotion into the 21st Century, Jakarta, Indonesia, July 1997. http://www.who.int/healthpromotion/conferences/previous/jakarta/declaration/en/index1.html
World Health Organization. Bangkok Charter for Health Promotion in a Globalized World – Sixth Global Conference on Health Promotion, Bangkok, Thailand, August 11, 2005. http://www.who.int/healthpromotion/conferences/6gchp/hpr_050829_%20BCHP.pdf
Department of Health is a Smoke Free Workplace 30