· twap and cmap were found reduced while ct was found increased in icu pts when compared to...
TRANSCRIPT

www.fisiokinesiterapia.biz

Knee extensor
J Appl. Physiol. 1997:82;182-188

TwAP and CMAP were found reduced while CT was found increased in ICU pts when compared to controls. Muscle weakness is common in ICU.
AM J Respir. Care Med 2000:162;240-245

TRIAGE 1TRIAGE 1>20>20
TRIAGE 2TRIAGE 2(16(16--20)20)
TRIAGE 3TRIAGE 3(11(11--15)15)
TRIAGE 4TRIAGE 4(6(6--10)10)
TRIAGE 5TRIAGE 5(0(0--5)5)
PuntiPunti 00 11 22 33 44 PunPuntiti
Pattern Pattern RespiratorioRespiratorio
Pattern Pattern Regolare Regolare
RR 12RR 12--2020
AumentatoAumentato
RR 21RR 21--2525
Dispnea da Dispnea da sforzo, pattern sforzo, pattern irregolare irregolare RR 26RR 26--3030
Riduzione Riduzione Della Della CapacitCapacitààVitale*Vitale*RR 31RR 31--3535
Severo SOB,Severo SOB,uso dei muscoli uso dei muscoli accessoriaccessoriRR>35RR>35
StatoStatoMentaleMentale
Vigile,Vigile,orientato, orientato, collaborantecollaborante
Letargico, Letargico, segue i segue i comandicomandi
Confuso, non Confuso, non segue i segue i comandicomandi
SoporosoSoporoso ComatosoComatoso
Rumori Rumori RespiratoriRespiratori
AuscultazAuscultaz..Chiara Chiara
Ridotti Ridotti unilateralmentunilateralmentee
Ridotti Ridotti bilateralmentbilateralmentee
Crepitii alle Crepitii alle basibasi
Dispnea e/o Dispnea e/o ronchironchi
TosseTosse Spontanea,Spontanea,energica, energica, nonnonproduttivaproduttiva
Energica,Energica,produttivaproduttiva
Debole,Debole,non non produttivaproduttiva
Debole, Debole, produttiva produttiva o debole o debole con ronchicon ronchi
Non tosse Non tosse spontanea o spontanea o necessitnecessitàà di di aspirazioneaspirazione
Livello di Livello di AttivitAttivitàà
DeambulantDeambulantee
Deambulante Deambulante con assistenzacon assistenza
Non Non deambulantedeambulante
ParaplegicoParaplegico TetraplegicoTetraplegico
TRIAGE RIABILITATIVO (ASSESSMENT)
(Stoller JK Respiratory Care 38: 1143-1154.)

SCHEDA DI VALUTAZIONE PER IMPOSTAZIONE FKT
Controllo troncoMovimentiCamminoDispnea da sforzoScore vita premorbidità
0 1 2 3 4
Score totale =
Score trattamento<4 A1 palestra A + all. sforzo arti inf. cycl. + 6 min4-6 A2 palestra gruppo A + 6 min7-9 B1 gruppo B + all. sforzo pedivella + 6 min10-12 B2 gruppo B + deambulaz. + 6 min13-15 I indiv. + deambulaz. + arm> 16 I mobil. Pass. Att. +allin. post.

SCHEDA DI VALUTAZIONE trattamenti complementari
A Stato polmonareB interv. ChirurgiciC tosseD RX torace
0 1 2 3 4
Score totale =
Score trattamento
A >3 ass. tosse o PEPB > 2 threshold e spir. incent.C > 2 ass. tosse + presidio + drenaggioD > 2 stop programma o valut. Indiv.

68%
12%
12%8%
denervazionesevera P iniziale Pnormale
Danni neuromuscolari diagnosticati con tests elettrofisiologiciin 25 pazienti con sospetto clinico su 313 ammessi in UTIR
M. Vitacca Rassegna App. Respiratorio 2004

0.7030.020.0440.700.6930.023P1000005002Normali
10000001003Polineuropatia
iniziale
6733660331003Polineuropatiasevera
76707618418217
Denervazione
Deambulazione alla dimissione
, %
MIP< 45 cmH2O
Aminoglicosidi,%
Steroidi %
Diabete,%
VMin
UTIR, %
N°
M. Vitacca Rassegna App. Respiratorio 2004
Danni neuromuscolari diagnosticati con tests elettrofisiologiciin 25 pazienti con sospetto clinico su 313 ammessi in UTIR

La fisioterapia

L’umidificazione delle vie aeree


La terapia rotazionale

Tecniche di disostruzione

0
100
200
300
400
0 3 7 14
TESTCONTROL
0102030405060708090
100
TEST CONTROL
Raoof S. CHEST 1999
% of atelectasisresolution
PaO2/FiO2
# days
CONTROL (n=7)
KT with P(n=17)
p value
intubated, % 29 47 NS
entire lung atelectasis, % 14 29 NS
lobar lung atelectasis, % 86 59 NS
bronchoscopy, % 43 0 0.02

0102030405060708090
100
UK Australia HK UK2
% of MH
L Denehy Eur Respir. J 1999
01020304050607080
secr
etio
ns
ATE
L:
FiO
2
coug
h
LV
CO
M.
ausc
ulta
tion
% of R
% of responders during MH in ICU

Design: prospective controlled trial setting: ICUpatients:60 intubated pts under MVInterventions: CP (24) vs sham (36)CP: twice daily: drainage, positioning, expiratory vibrations, suctioning, coughing when extubatedsham: nurse positioning and suction
Results: VAP occurred in 8% of CP vs 39% of sham (OR 0.14)after adjustment for Apache II, MV gg, trach., GCS (OR 0.16)

Design: prospective randomized controlled trial Setting: RICUPatients: 27 COPD with exacerbationInterventions: group A : PEP mask plus ass. coughgoup B cough alone
Results: Amount of sputum was stat. higher and weaning time lower
Mortality and ETI were not.
Short term effects of expiration under positive pressure in patients with acute exacerbation of COPD and
mild acidosis requiring NPPV
Bellone et al (Intenive Care Med 2002;28 (5):581-5)

Design: prospective randomized controlled trial setting: ICU
patients: 236 intubated pts under MV (EI) after cardiac surgical operation Interventions: FKT under EI vs FKT only after extubation
Results:EI duration, ICU stay, hospital stay, spirometric valuespulmonary complications between groups were similar.
Fisioterapia dopo cardiochirurgia: è necessaria duranteil periodo di intubazione ?
Patman S et al (Aust J Physiother 2001; 47:7-16)

Design: prospective randomized controlled trial Setting: ICUPatients: 46 trauma patients under MV Interventions:group A: physiotherapygroup B: control
Results: % of weaning %, ICU time, MV time and pneumonia were notstatistically different
The effect of manual lung hyperinflation and postural drainage on pulmonary complications in
mecahnically ventilated trauma patients
Ntoumenopoulos (Anaesth Intensive Care 1998; 26:492-6)

La misura della MIP e MEP
Per svezzare indice di outcome
per decannulare
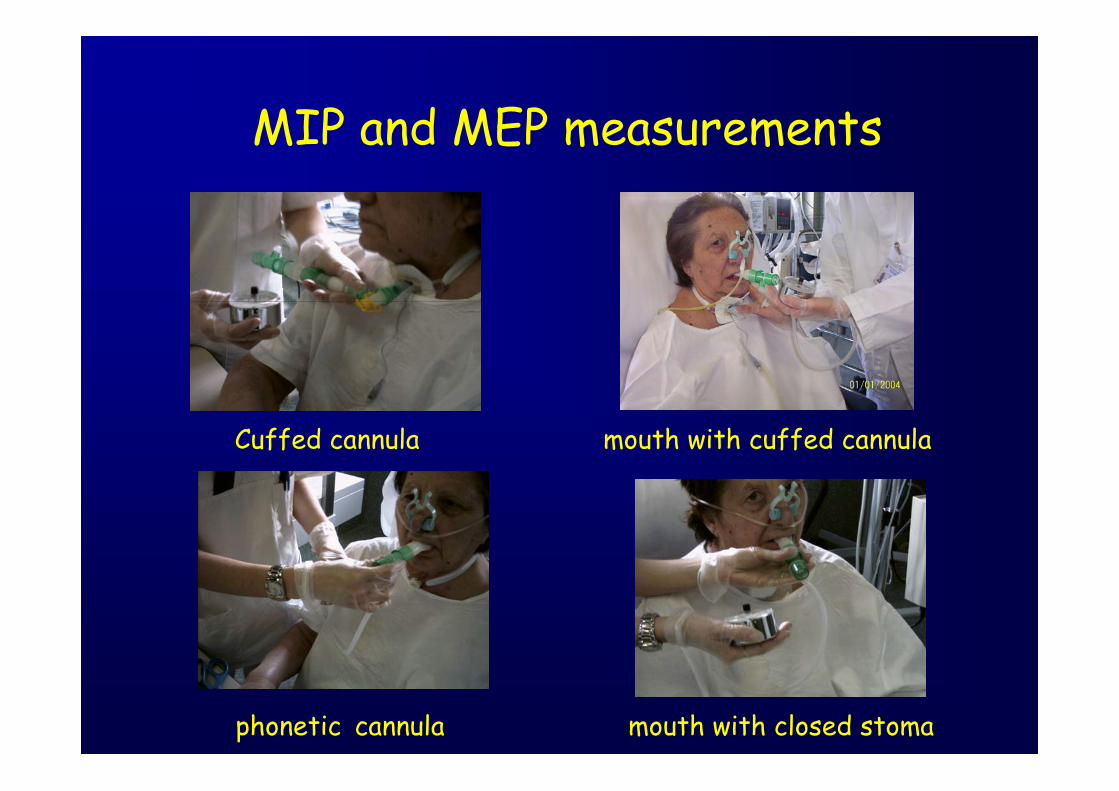
MIP and MEP measurements
Cuffed cannula mouth with cuffed cannula
phonetic cannula mouth with closed stoma

Effects of controlled inspiratory muscle training in patients withCOPD: a meta-analysis
F Lotters et al (2002; 20:570-576)
BerryGoldesteinLarsontotal pimax > 60DekhuijzenWeankeWeinertotal Pimax < 60
-2 -1 0 1 2 3 Favours favourscontrol treatment
BerryGoldestein
total pimax > 60Dekhuijzen
Weinertotal Pimax < 60
-2 -1 0 1 2 3 Favours favourscontrol treatment
IMS EC
Design: prospective trial setting: ICUpatients: 10 pts who had failed to wean from MV with 2.1±3.4 h of SB.Interventions: IMST of 4 sets of 6 breaths with threshold with anintensity to yield an exertion rating of 6 to 8.
Results: IMST pressure from 7±3 cmH20 to 18±7; 9 out 10 weaned after 44±43 days
CHEST 2002:122;192-6

L’allenamento allo sforzo

L’allenamento allo sforzo

Design: prospective randomized controlled trial Setting: RICUPatients: COPD recovering from ARF Interventions: early PRP vs Standard MT alone;
step 1: 2/d 30-45 min postural position, sitting in bed or chair, lower extremities training, postural drainage, coughstep 2: rolling , walk , step 3: muscle training, lower extremity training, cycling, climbingstep 4: treadmill sessions
Results: Effort tolerance, MIP, dyspnoea were better for PRP group
Rehabilitation of patients admitted to a respiratory intensive care unit
Nava S. (Arch Phys Med Rehabil 1998; 79:849-854)

PRP plus
SAEX :15 daily supervised consecutive sessions of actual 20minutes of upper arm cycling with an arm ergometer.
the load was increased by 2,5 Watt/session according to Borg D and Funtil the 70% of W max reached baseline
PRP: 45 minutes/daily sessions (6 days/week)
chest physiotherapypassive and active lower and upper-limb mobilisationreinforcement tecniques for head and trunk control sitting and standing balanceassisted deambulation
according to clinical triage (every 3° day)
All patients
Only Study group

0
5
10
15
20
25
T0 T1
Wat
t
0
5
10
15
20
25
T0 T1
Min
utes
IT ET
p=0.0029p=0.021
Incremental and endurance variation after training
Study groupcontrols
§
#
§
#

20
30
40
50
60
70
T0 T1
cmH
2O
MIP variation
p= 0.002
Study groupcontrols
p=0.08
p= 0.02
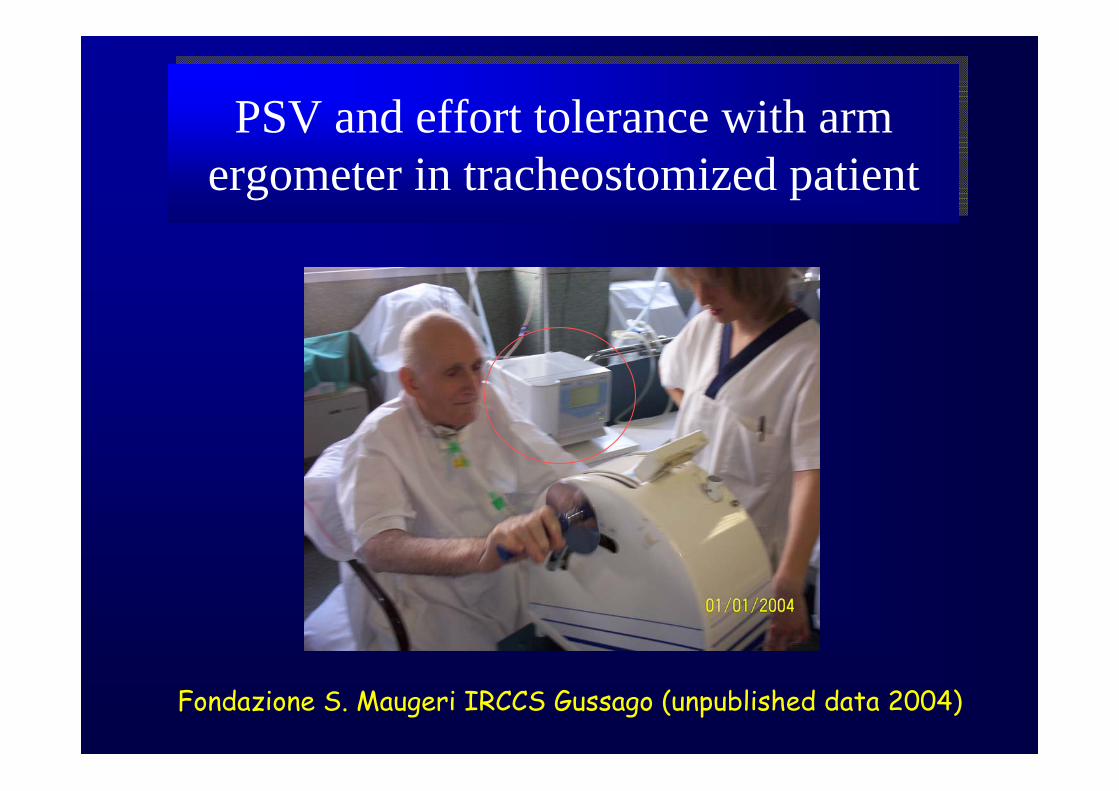
PSV and effort tolerance with armergometer in tracheostomized patientPSV and effort tolerance with arm
ergometer in tracheostomized patient
Fondazione S. Maugeri IRCCS Gussago (unpublished data 2004)

7.18±4.5010±6.12
Max load SBMax load MV
1.01±0.290.66±0.41
1.67±0.841.0±0.63
1.20±0.60.61±0.3
WOBes (J/L) SBWOBes (J/L) MV
0.62±1.060.8±1.13
2.25±3.21.87±1.55
0.25±0.701.12±0.64
PEEPi-dyn (cmH2O) SBPEEPi-dyn (cmH2O) MV
0.16±0.050.04±0.03
0.32±0.240.19±0.20
0.17±0.080.08±0.06
Pes/Pesmax SBPes/Pesmax MV
24±717±5
27±525±6
23±818±7
f (a/min) SBf (a/min) MV
0.5±0.91.2±1.06
4.8±34.1±2.2
0.4±10.6±1
Borg F SBBorg F MV
1.8±1.771.3±1
6.2±2.45.2±2.3
1.9±1.31±0.8
Borg D SBBorg D MV
RecoveryIsowattBaseline
Fondazione S. Maugeri IRCCS Gussago (unpublished data 2004)




Time (hours)
Pro
babi
lity
to re
mai
n un
der M
V
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 100 200 300 400 500 600 700 800 900 1000 1100
p<0.0001
Vitacca M. Am J Respir Crit Care Med 2001; 164: 225-230

0102030405060708090
100
0 1 3 5 15 25
control (151pts)intervention(149 pts)
Ely N. Engl J Med 1996
Duration of MV after a succesfull weaning test
% of ptson MV
Days
Self extubation, reintubation,tracheostomy

0102030405060708090
100
tosse dren. ric. diafr. PEP
0102030405060708090
mobili. bronco posture NIV Bellone Rassegna Pat. App. Respir. 2001
%
%
Lavorano in UTIR 54%lavorano in UTIR solo 1 volta/die 53%lavorano il sabato mattina 53%usano indici di outcome 63%
Rapporto paz/FDR5/1

RECCOMENDATIONS FOR FKT IN ICU
• Evidence A in acute lobaratelectasis.
• prone position > Oxygenationin ARDS
• side lying > Oxygen inunilateral lung disease
• Haemodinamic monitoringis mandatory.
• Sedation before FKT preventshaemodynamic effects
• Preox. sedation are necessarybefore suction
• Rotation therapy< Pulmonary complications
K. Stiller CHEST 2000

• FKT has short beneficialeffects on respir. function
• MH with monitoring has short beneficial effects on respir. function
• ICP and CPP should bemonitored during FKT
K. Stiller CHEST 2000
RECCOMENDATIONS FOR FKT IN ICU

• FKT+ nursing < complicationsin ICU
• FKT is effective to improvepulmonary derangement
• FKT < weaning, stay in ICU and hospital, mortality, morbility
• Positioning + lung FKT are effective
• limb exercises prevent loss of joint range or > muscle strenghtand function.
K. Stiller CHEST 2000
RECCOMENDATIONS FOR FKT IN ICU

Conclusions: Pulmonary R. in ICU
controlled studies ?controlled studies ?
RationalisationRationalisation of programs:of programs:assessmentassessmenttriagetriageexclusion criteriaexclusion criteriaspecific programs specific programs respiratory musclesrespiratory musclesperipheral muscles peripheral muscles timing timing intensityintensityspecificity for diseasesspecificity for diseases
The futureThe future !!