¿ qué aporta la cirugía - oncopromesas-oncosaurios.com · peritonitis recto-vaginal fistula...
TRANSCRIPT

Coordinación científica:Dr. Fernando RiveraHospital Universitario Marqués de Valdecilla,
Santander
Organizado por: Fundación para el progreso
de la oncología en Cantabria
Novedades quirúrgicas en cáncer de ovarioSergio Martínez Román
Director clínico territorial y jefe de servicio de Ginecología
Hospital Universitario Germans Trias I Pujol, Badalona

Disclosure
Yo hice E.G.B.

¿ Qué aporta la cirugía ?

Cytoreductive surgery: a different oncologic
surgery
• Joe V. Meigs MD, 1934
• Mass. Gen. Hosp. US
“enhance the effects of radiation therapy”

Biologic rationale for cytoreduction
• Goldie y Coldman mathematical model (Cancer Treat Rep, 1979)
– Definition: a mathematic model that predicts that tumor cells mutate to a resistant phenotype at a rate dependent on their intrinsic genetic instability.
– “The probability that a cancer would contain drug-resistant clones depends onthe mutation rate and the size of the tumor.”
quimioresistenciaquimioterápia
Primaria Adquirida

The role of the surgical effort. 8.674 pt
68
4033
81
35 30
72
37 33
78
50
36
86
4637
110
54
0
20
40
60
80
100
120
MICROSCOPIC < 1 CM >1 CM
SU
RV
IV
AL M
ON
TH
S
MINIMAL RESIDUAL DISEASE AFTER DEBULKING
BOOKMAN DUBOIS QUERLEU CHI CHANG IP LANDRUM
PRIMARY DEBULKINGSTAGES IIIC-IV
72 MONTHS
44MONTHS
32MONTHS
Cortesía Dr. Luis Chiva

5-year survival rate
du Bois A, Reuss A, Pujade-Lauraine E, et al. Cancer 2009;15:1234–44
The impact of residual tumour on outcome in advanced ovarian cancerData from an individual patient meta-analysis of three randomised phase III trials with 3,126 patients
log-rank: p<0.0001
0%
25%
50%
75%
100%
0 12 24 36 48 60 72 84 96 108 120 132 144
Ove
rall
surv
ival
(%
)
0mm
1–10mm>10mm
Time (months)

5-year survival rate
du Bois A, Reuss A, Pujade-Lauraine E, et al. Cancer 2009;15:1234–44
The impact of residual tumour on outcome in advanced ovarian cancerData from an individual patient meta-analysis of three randomised phase III trials with 3,126 patients
log-rank: p<0.0001
0%
25%
50%
75%
100%
0 12 24 36 48 60 72 84 96 108 120 132 144
Ove
rall
surv
ival
(%
)
0mm
1–10mm>10mm
Time (months)
2 %
Defining cohorts
according to potential
benefit from surgery

5-year survival rate
du Bois A, Reuss A, Pujade-Lauraine E, et al. Cancer 2009;15:1234–44
The impact of residual tumour on outcome in advanced ovarian cancerData from an individual patient meta-analysis of three randomised phase III trials with 3,126 patients
log-rank: p<0.0001
0%
25%
50%
75%
100%
0 12 24 36 48 60 72 84 96 108 120 132 144
Ove
rall
surv
ival
(%
)
0mm
1–10mm>10mm
Time (months)
2 %2 %
33 %
Defining cohorts
according to potential
benefit of surgery

5-year survival rate
du Bois A, Reuss A, Pujade-Lauraine E, et al. Cancer 2009;15:1234–44
The impact of residual tumour on outcome in advanced ovarian cancerData from an individual patient meta-analysis of three randomised phase III trials with 3,126 patients
log-rank: p<0.0001
0%
25%
50%
75%
100%
0 12 24 36 48 60 72 84 96 108 120 132 144
Ove
rall
surv
ival
(%
)
0mm
1–10mm>10mm
Time (months)
2 %2 %
33 %
60 %
Defining cohorts
according to potential
benefit of surgery

5-year survival rate
du Bois A, Reuss A, Pujade-Lauraine E, et al. Cancer 2009;15:1234–44
The impact of residual tumour on outcome in advanced ovarian cancerData from an individual patient meta-analysis of three randomised phase III trials with 3,126 patients
log-rank: p<0.0001
0%
25%
50%
75%
100%
0 12 24 36 48 60 72 84 96 108 120 132 144
Ove
rall
surv
ival
(%
)
0mm
1–10mm>10mm
Time (months)
2 %
2 %2 %
33 %
60 %
Defining cohorts
according to potential
benefit of surgery

¿A quién y cuando?

OPERATE OR NOT?
PATIENT
Operability
DISEASE
Resectability
SURGICAL TEAM
Performance

Aletti criteria
Age≥75 years
PS (ASA)/Nutritional (albumin ≤3)
Stage IV/extensive surgery

¿Podemos predecir la resecabilidad
antes de ir a quirófano?

• Rule out extraabdominal disease
• Number, size, anatomical relationships
• Estimation of resectability
FDG-glucose PET-CT

Valoración temprana respuesta a neoadyuvancia



Molecular Imaging
Marcaje de dianas moleculares sobreexpresadas en
células tumorales
• Estadificación no invasiva
• Cirugía radioguiada
• Biomarcadores predictivos
• Monitorización de respuesta terapéutica


Introperative PET probes• Radioguided surgery
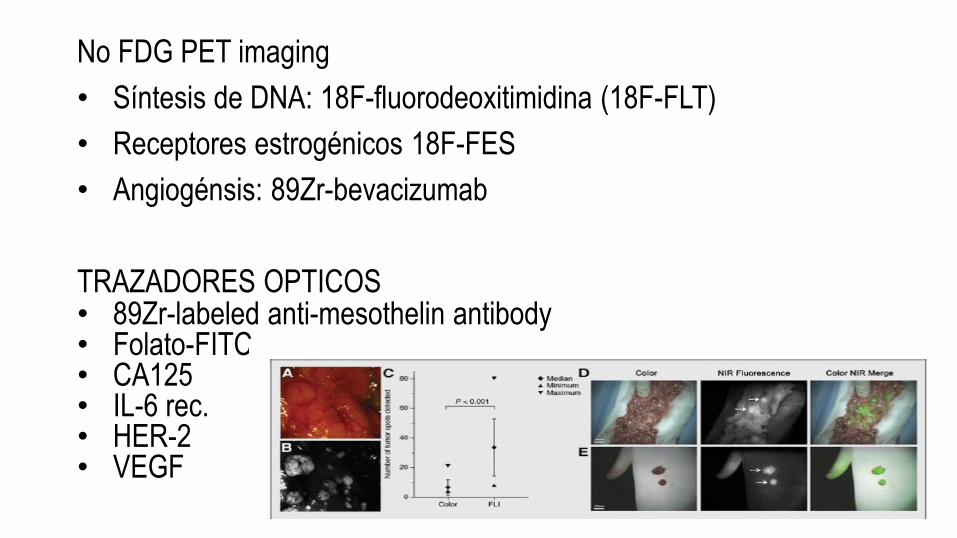
No FDG PET imaging
• Síntesis de DNA: 18F-fluorodeoxitimidina (18F-FLT)
• Receptores estrogénicos 18F-FES
• Angiogénsis: 89Zr-bevacizumab
TRAZADORES OPTICOS• 89Zr-labeled anti-mesothelin antibody• Folato-FITC• CA125 • IL-6 rec.• HER-2• VEGF

Gynecol Oncol 2009, 112 (1): 6–10
• There was no threshold CA-125 level that accurately
predicted cytoreductive outcome.
• CA-125 values >500 U/mL, 50% (57/113) of patients
required extensive upper abdominal surgery to achieve
RD ≤1 cm, compared to 27% (25/93) for those with CA-
125 <500 U/mL (P=0.001).

Gynecol Oncol, 2014; 134(3): 455-61
Prospectivo multicéntrico
669 pacientes
Tasa de citoreducción 1ª 75%
3 criterios clínicos
6 criterios radiológicos

Gynecol Oncol, 2014; 134(3): 455-61
Aplicabilidad clínica:
Puntuación superior a 9 predice
citoreducción subóptima en 74%
Precisión AUC 0.758
0.5 – 0.6 test malo
0.6 – 0.75 test regular
0.75- 0.9 test bueno
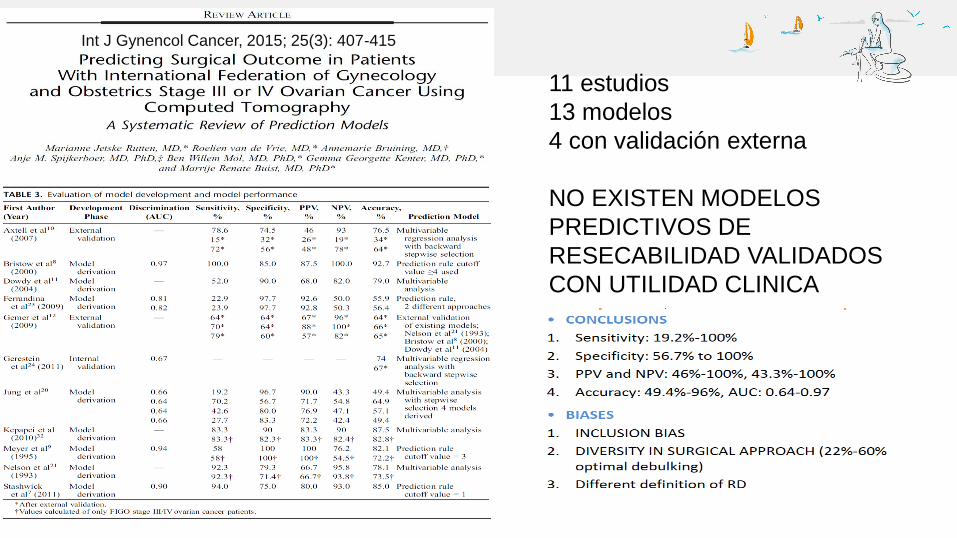
11 estudios
13 modelos
4 con validación externa
NO EXISTEN MODELOS
PREDICTIVOS DE
RESECABILIDAD VALIDADOS
CON UTILIDAD CLINICA
Int J Gynencol Cancer, 2015; 25(3): 407-415

¿Podemos predecir la resecabilidad
antes de abrir el abdomen?




Predictive parameter Value
Omental cake 2
Peritoneal carcinomatosis 2
Diaphragmatic carcinomatosis 2
Mesenteric retraction 2
Bowel infiltration 2
Stomach infiltration 2
Liver superficial metastasis 2
Prediction of suboptimal cytoreduction
Score ≥ 8
Sensitivity 30%
Specificity 100%
PPV 100%
NPV 74%

Trocars en linea media. Resección de puertos
Limitaciones de la laparoscopia
Utilización HALS
Momento de laparoscopia
• Unico procedimiento y cirugía diferida
• Previo inmediato a laparotomía
¿Qué hacemos con los estadíos IV-A ?



Resección nódulo diafragmático

• Derrame pleural : VATS : 57 % enfermedad pleural
• Cambio de estadío y cambio de tratamiento en 41 %
• Citología pleural:
positiva 73% VATS +
27 % VATS –
negativa 23,5 % VATS +
Citología pleural carece de sensibilidad - especificidad

Está justificado el máximo esfuerzo de citorreducción en IVA ? DEPENDE
Carga tumoral en abdomen
Complejidad quirúrgica en abdomen
Tamaño de la enfermedad pleural (<1cm)

¿Cómo operamos con la mayor
posibilidad de R0 y menor riesgo?

Aproximación quirúrgica
• Laparoscopia +/- VATS (si indicado)
• Incisión medial Xipho-pubica medial
• Buena exposición
• Evaluación sistemática
• Check points de “stop-or-go” decisión 1 y 2

Point of “stop-or-go” decision 1
2 Mobilization of colonic right flexure
1 Section ligamentum teres and falciforme hepatis
3 Dissection of the omentum from the transverse colon
4 Evaluation of lesser sac, pancreas, truncus coeliacus,
and porta hepatis

Point of “stop-or-go” decission 2
Radix mesenterii
Small bowell surface

First expose the upper abdomen and do the hard work

Spleen +/- pancreas tail:
Bleeding
Pancreatic fistula

Medial mobilization of the liver

Diaphragm stripping

Diaphragm nodule resection

Liver resection
Hepato-renal reflection


Modified posterior pelvic exenteration
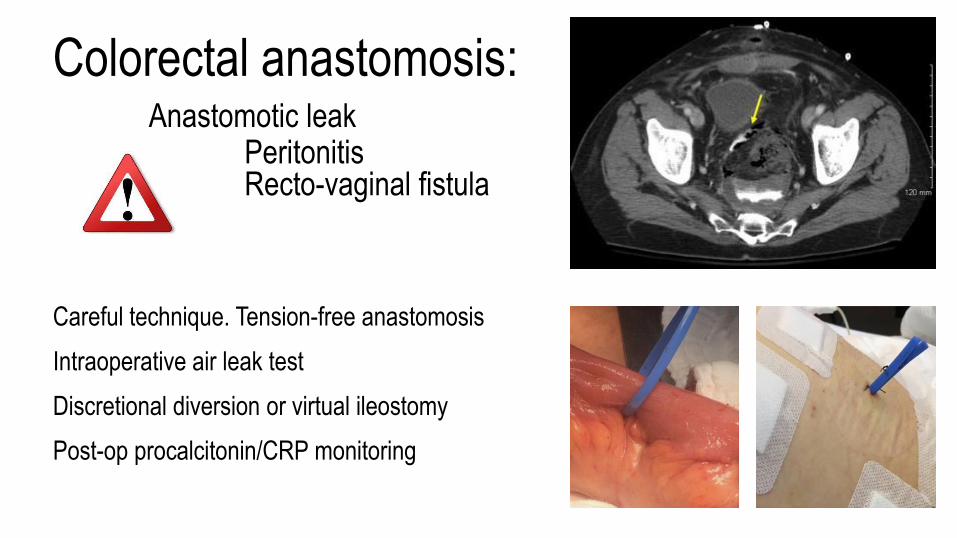
Colorectal anastomosis:Anastomotic leak
PeritonitisRecto-vaginal fistula
Careful technique. Tension-free anastomosis
Intraoperative air leak test
Discretional diversion or virtual ileostomy
Post-op procalcitonin/CRP monitoring

¿Y los ganglios?

Cava Aorta
Mesentérica inf.
Ureter
Vena renal Izq.
Vena ovárica Vena ovárica
1 Aórticos, entre art. Renal y mesentérica inf.
2 Aórticos, por debajo mesentérica inf.
3 Ilíacos primitivos y sacros
4 Ilíacos internos, externos y fosa obturatriz


¿Cirugía primaria o neoadyuvancia?

QT neoadyuvante → CCI : RCTs EORTC–GCG 55971

◼ N = 718
◼ Follow-up 4,8 a.
◼ OS: 29 vs 30 m.
◼ PFS: 12 vs. 12 m.
◼ Menos morbilidad
“optimal debulking surgery was the strongest independent prognostic for OS in both groups”
“OPTIMAL DEBULKING STILL MATTERS MOST, SURGICAL TIMING DOES NOT”

SI, es un RCT ….. PERO• Sólo residual <1cm) en 42%
– (NCI standard guidelines > 75%)

SI, es un RCT ….. PERO• Sólo residual <1cm) en 42%

CONCLUSION de EORTC–GCG 55971
• CONCLUSION:
–Cirugía
–no es peor que NA

CONCLUSION de EORTC–GCG 55971
• CONCLUSION:
–Cirugía subóptima
–no es peor que NA

SI, es un RCT ….. PERO• Sólo residual <1cm) en 42%
• Resultados de difícil comprensión y conclusiones
• capciosas
19 % 51 %
“optimal debulking surgery was the strongest independent prognostic for OS in both groups”
“OPTIMAL DEBULKING STILL MATTERS MOST, SURGICAL TIMING DOES NOT”

N = 316
90 % PDS 10% NACT
Optimal cytoreduction (<1cm) en 71%

SI, es un RCT ….. PERO• Sólo residual <1cm en 42%
• Resultados de difícil comprensión y conclusiones capciosas
• Supervivencias de casos y controles < ½ de la de cohortes con estadío III y citorreducción completa ( 29 m vs. 70 m)

Quimioresistencia inducida por NAC


¿Que debemos hacer para mejorar el
desempeño quirúrgico y los resultados?

Learning Training Improving
SURGICAL PERFORMANCE
CONCENTRATION OF EXPERTISE




QUALITY INDICATORS IN OVARIAN CANCER CARE IN CATALUNYA
AUDIT QUALITY OF PUBLIC HOSPITALS 2017
Benchmarking procedure:
Frequent lack of alignment to guidelines
Important differences between centers
Inequity in oncologic outcomes / survival
ACTION REQUIRED:
Centralization of ovarian cancer care in referral
tertiary hospitals matching quality criteria0
10
20
30
40
50
60
70
80
90
100
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29

¿Cuál es el papel de la cirugía en las
recidivas?


AGO-OVAR DESKTOP III (Protocol AGO - OVAR OP.4)
Página 1
CENTROS PARTICIPANTES – ESTUDIO DESKTOP III
Nombre Investigador Hospital
1 H. de Navarra
2
3
4 Instituto Valenciano de Oncología
5
6
7
8 H. Universitario la Fe
9
10
07/10/11
Dra. Nuria Lainez
Dra. Angela López H. Provincial de Castellón
Dra. Isabel Bover H. Son Llàtzer
Dr. Andrés Poveda
Dr. Yolanda García Consorci Sanitari Parc Taulí
Dra. Margarita Romeo Marín
ICO Badalona - Hospital Germans Trias i Pujol
Dr. Sergio Martinez H. Clinic I Provincial de Barcelona
Dra. Ana Santaballa
Dr. Jordi Ponce H. de Bellvitge
Dra. Belén Ojeda H. de la Santa Creu i Sant Pau
N= 408

Interim findings. DESKTOP III
DuBois SGO meeting, Chicago 2017
• Secondary cytoreductive surgery resulted in a clinically meaningful
increase in progression-free survival and time to first subsequent
therapy
• Median PFS 19.6 m vs 14 m. HR 0.66
• No differences in short term mortality or toxicity
• POSITIVE findings in favor of surgery
• Waiting for OS results

GOG 213 A phase III trial examining the role of secondary cytoreductive
surgery and bevacizumab in recurrent ovarian cancer.

¿HIPEC si o no? ¿Cuándo?

Coliseum Technique. Sugarbaker P


Racionalidad del HIPEC
• EFECTOS MECANICOS:
– Lavado continuo de la superfície intraabdominal
– Distribución homogenea y máximo contacto
• EFECTOS FISICOS: Calor (42ºC)
– Efectos citotóxicos e inducción de la apoptosis
– Inducción de Heat shock proteins (NK receptor) (respuesta inmune)
– Inhibición de la angiogénesis
• EFECTOS QUIMICOS: Sinergismo calor - QTs
Incremento de la quimiosensibilidad de les células tumorales
– Incremento de la penetración de los fármacos
– Incremento de la permeabilidad de la membrana celular
– Inhibición de la reparación del DNA ocasionada por platino

N = 30 cases 37 controls
HIPEC: OXA mg/m2

N= 60/60 EOC, HIPEC : CDDP+PCT or DOX+PCT
Platinum-sensitive Platinum-resistant
26 vs. 13 m OS

34 m
46 m

Comentarios finales• La enfermedad residual después de la cirugía primaria es el factor
modificable con mayor impacto en la supervivencia. La
neoadyuvancia es un recurso para las no operables o no resecables.
• Optimizar el desempeño quirúrgico requiere la adquisición de
competencias avanzadas, entrenamiento y concentración de la
experiencia.
• La cirugía de la recidiva tiene un papel en pacientes seleccionadas
• El papel del HIPEC debe ser reevaluado a la luz de la reciente
evidencia disponible