!! program progress report - d10k7k7mywg42z.cloudfront.net · 7. project goal:! to reduce the...
TRANSCRIPT
!
! !Program Progress Report !Eradicate Childhood Malnutrition Program Madhya Pradesh, India Fourth Quarter – October – December 2013 !!Date: Prepared by: February 24, 2014 Michael Matheke-Fischer, Santosh Pal & Amit Purohit
I. Demographic Information
1. Districts and State: Jhabua, Alirajpur, Khandwa, Barwani, Khargone districts in Madhya Pradesh, India
2. Organization: Real Medicine Foundation, India (www.realmedicinefoundation.org)
3. Project Title: “Eradicate Childhood Malnutrition”
4. Reporting Period: October 1, 2013 – December 31, 2013
5. Project Location (region & city/town/village): Southwestern Madhya Pradesh, India
6. Target Population: Malnutrition support to approximately 100,000 children under age 5 Messages reach a population of over 500,000 people
II. Project Information

7. Project Goal: !To reduce the prevalence of underweight children under 5 years old and to reduce child mortality from malnutrition by strengthening communities and village level government facilities’ capacity to identify, treat, and prevent malnutrition. This project aims to prove that a holistic, decentralized, community-based approach to malnutrition eradication will have better health outcomes, be more inclusive for children under 5 and will be more cost-effective in the long-run than centralized approaches, especially for rural, marginalized tribal communities. !This project empowers communities through health literacy and connects rural communities with the government health and nutrition services available. !RMF does not just act as a catalyst mobilizing communities to the resources available, but also works on a more intimate level with government health and nutrition workers and Village Health and Sanitation Committees to help build their capacity towards social mobilization, referrals, and provision of effective nutrition counseling. Throughout this year RMF is gradually transferring the responsibilities of our CNEs to government supervisors and Anganwadi workers, helping integrate RMF’s work into the government framework to ensure long-term sustainability.
8. Project Objectives during this reporting period: • Continue to identify new SAM and MAM cases, refer complicated cases to the NRC and provide home-based
counseling for all malnourished children • Review all program data and make necessary changes in program reporting system • Refer 1,000 SAM children to government centers for treatment with a 50% success rate • Conduct 2,500 Community Nutrition Meetings • Conduct 9,000 Individual Family Counseling Sessions • Send CNEs to Nutrition Rehabilitation Centers (NRCs) to help counsel families present • Continue to develop linkages with government health and nutrition services • Continue pilot with Digital Green Trust to produce and screen nutrition and health based videos in Khandwa,
Madhya Pradesh • Strengthen institutional capacity with support from World Bank’s India Development Marketplace Award
9. Summary of activities carried out during the reporting period under each project objective (note any changes from original plans): !• Paid salary and travel expenses to 60 Community Nutrition Educators and 6 District and Block Coordinators • Printed weekly reporting sheets for the CNEs to compile indicators from their daily reports, including amount of
SAM and MAM diagnosed, successful referrals, Family and Community Counseling sessions, and improved children
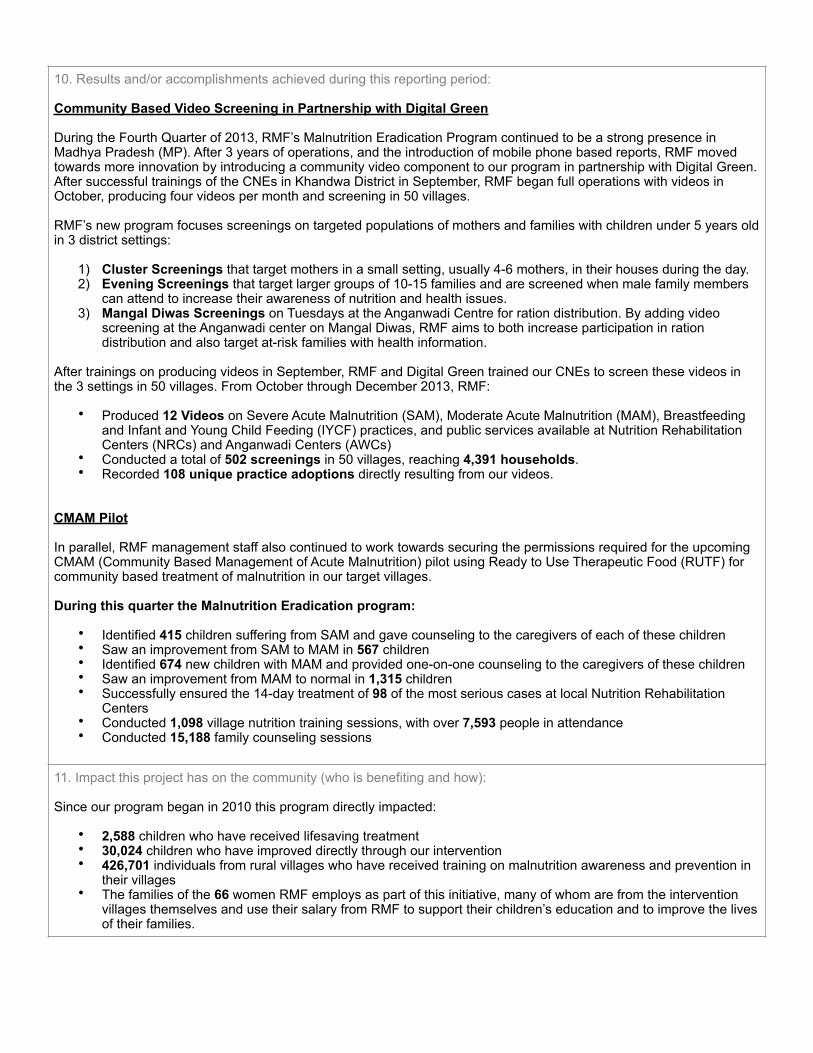
10. Results and/or accomplishments achieved during this reporting period: !Community Based Video Screening in Partnership with Digital Green !During the Fourth Quarter of 2013, RMF’s Malnutrition Eradication Program continued to be a strong presence in Madhya Pradesh (MP). After 3 years of operations, and the introduction of mobile phone based reports, RMF moved towards more innovation by introducing a community video component to our program in partnership with Digital Green. After successful trainings of the CNEs in Khandwa District in September, RMF began full operations with videos in October, producing four videos per month and screening in 50 villages. !RMF’s new program focuses screenings on targeted populations of mothers and families with children under 5 years old in 3 district settings: !
1) Cluster Screenings that target mothers in a small setting, usually 4-6 mothers, in their houses during the day. 2) Evening Screenings that target larger groups of 10-15 families and are screened when male family members
can attend to increase their awareness of nutrition and health issues. 3) Mangal Diwas Screenings on Tuesdays at the Anganwadi Centre for ration distribution. By adding video
screening at the Anganwadi center on Mangal Diwas, RMF aims to both increase participation in ration distribution and also target at-risk families with health information. !
After trainings on producing videos in September, RMF and Digital Green trained our CNEs to screen these videos in the 3 settings in 50 villages. From October through December 2013, RMF: !
• Produced 12 Videos on Severe Acute Malnutrition (SAM), Moderate Acute Malnutrition (MAM), Breastfeeding and Infant and Young Child Feeding (IYCF) practices, and public services available at Nutrition Rehabilitation Centers (NRCs) and Anganwadi Centers (AWCs)
• Conducted a total of 502 screenings in 50 villages, reaching 4,391 households. • Recorded 108 unique practice adoptions directly resulting from our videos. !!
CMAM Pilot !In parallel, RMF management staff also continued to work towards securing the permissions required for the upcoming CMAM (Community Based Management of Acute Malnutrition) pilot using Ready to Use Therapeutic Food (RUTF) for community based treatment of malnutrition in our target villages. !During this quarter the Malnutrition Eradication program: !
• Identified 415 children suffering from SAM and gave counseling to the caregivers of each of these children • Saw an improvement from SAM to MAM in 567 children • Identified 674 new children with MAM and provided one-on-one counseling to the caregivers of these children • Saw an improvement from MAM to normal in 1,315 children • Successfully ensured the 14-day treatment of 98 of the most serious cases at local Nutrition Rehabilitation
Centers • Conducted 1,098 village nutrition training sessions, with over 7,593 people in attendance • Conducted 15,188 family counseling sessions
11. Impact this project has on the community (who is benefiting and how): !Since our program began in 2010 this program directly impacted: !
• 2,588 children who have received lifesaving treatment • 30,024 children who have improved directly through our intervention • 426,701 individuals from rural villages who have received training on malnutrition awareness and prevention in
their villages • The families of the 66 women RMF employs as part of this initiative, many of whom are from the intervention
villages themselves and use their salary from RMF to support their children’s education and to improve the lives of their families.

12. Number served/number of direct project beneficiaries (for example, average number treated per day or month and if possible, per health condition) !Month October November December TOTAL Severely Acute Malnourished (SAM) Children
New SAM Children Identified 136 128 151 415 Total Number of SAM Children ever reached 13056 13184 13335 13335
Old SAM Children Visited 1442 1136 956 3534 % of SAM Children Visited 11.04% 8.62% 7.17% 26.50%
SAM Children Improved (to MAM) 328 161 78 567 SAM Children ever improved 8795 8956 9034 9034
Improvement Rate (%) 67.36% 67.93% 67.75% 67.75% Moderately Acute Malnourished (MAM) Children
New MAM Children Identified (New Case + SAM to MAM) 206 239 229 674 Total Number of MAM Children ever reached 31247 31486 31715 31715
Old MAM Children Visited 4227 3526 2956 10709 % of MAM Children Visited 14% 11% 9% 34%
MAM Children Improved (to Normal) 646 382 287 1315 MAM Children ever improved 22018 22018 22305 22305
Improvement Rate (%) 69.24% 69.93% 70.33% 70.33% NRC Referrals
Children Referred to NRC (Parents Counseled and Referral Slips Issued) 126 136 148 410 Children that got admitted in NRC 26 32 40 98
Success Rate of NRC Admissions after Counseling Parents 20.63% 23.53% 27.03% 23.90% Total Number of Children Ever Admitted to the NRC 2516 2548 2588 2588
Follow Up of the Child at the Village (ever admitted to NRC) 350 324 172 846 Follow Up of the Child at NRC (ever admitted to NRC) 37 16 28 81
Family Counseling Sessions
Family Counseling Session - Total Numbers 5443 4955 4790 15188 Total Number of individuals present for a session 9713 8394 9080 27187
Community Group Sessions
Community Group Session- Total Numbers 370 340 388 1098 Total Number of individuals present for a session 2647 2114 2832 7593
Average attendees in the Community Group Session 7 6 7 7 Other Activities done by the CNEs
Cooking Demonstration 348 230 205 783 Meeting with Anganwadi workers 202 400 317 919
Meeting with other stakeholders in the village 175 68 66 309 Meeting with SHG members in the Village 3 0 0 3
13. Number of indirect project beneficiaries (geographic coverage): !Approximately 500,000
14. If applicable, please list the medical services provided: !Referrals to Nutrition Rehabilitation Centers for children with Severe Acute Malnutrition Referrals to public health centers and community health centers for MAM children with suspected complications Hospital referrals for children who need advanced care
!18. Success story(s) highlighting project impact !
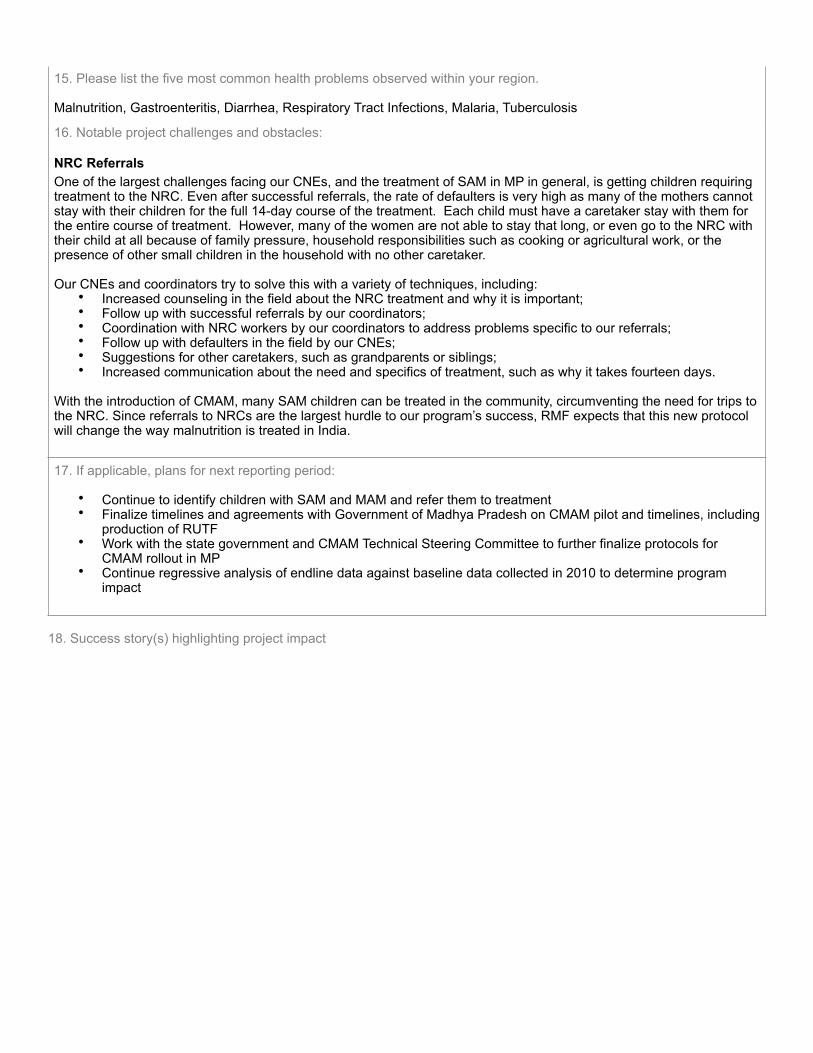
15. Please list the five most common health problems observed within your region. !Malnutrition, Gastroenteritis, Diarrhea, Respiratory Tract Infections, Malaria, Tuberculosis
16. Notable project challenges and obstacles:
NRC Referrals One of the largest challenges facing our CNEs, and the treatment of SAM in MP in general, is getting children requiring treatment to the NRC. Even after successful referrals, the rate of defaulters is very high as many of the mothers cannot stay with their children for the full 14-day course of the treatment. Each child must have a caretaker stay with them for the entire course of treatment. However, many of the women are not able to stay that long, or even go to the NRC with their child at all because of family pressure, household responsibilities such as cooking or agricultural work, or the presence of other small children in the household with no other caretaker. !Our CNEs and coordinators try to solve this with a variety of techniques, including:
• Increased counseling in the field about the NRC treatment and why it is important; • Follow up with successful referrals by our coordinators; • Coordination with NRC workers by our coordinators to address problems specific to our referrals; • Follow up with defaulters in the field by our CNEs; • Suggestions for other caretakers, such as grandparents or siblings; • Increased communication about the need and specifics of treatment, such as why it takes fourteen days. !
With the introduction of CMAM, many SAM children can be treated in the community, circumventing the need for trips to the NRC. Since referrals to NRCs are the largest hurdle to our program’s success, RMF expects that this new protocol will change the way malnutrition is treated in India.
17. If applicable, plans for next reporting period: !• Continue to identify children with SAM and MAM and refer them to treatment • Finalize timelines and agreements with Government of Madhya Pradesh on CMAM pilot and timelines, including
production of RUTF • Work with the state government and CMAM Technical Steering Committee to further finalize protocols for
CMAM rollout in MP • Continue regressive analysis of endline data against baseline data collected in 2010 to determine program
impact

! !Photo: Children attend screening with their mothers in Khandwa !The Steady Fight Against Malnutrition – RMF Community Nutrition Educators Work to Improve Health Outcomes !Convincing people to adopt healthier behaviors can be a difficult job. In Southwestern Madhya Pradesh, where RMF’s Community Nutrition Educators (CNEs) work in 600 villages across 5 districts every day, targeted health education is crucial to combating malnutrition (http://www.realmedicinefoundation.org/initiative/malnutrition-eradication-program-madhya-pradesh-india). !For four years, each CNE has patiently worked in communities, identifying children and families in need of counseling, referring serious cases to treatment, and building crucial bonds with the community. Since 2010, our program has reached over 400,000 people with targeted health and nutrition messages.
While not flashy or particularly glamorous, RMF’s boots-on-the-ground, or more accurately, chappals-on-the-ground, have been a steady and formidable force fighting malnutrition and increasing ownership of nutrition outcomes in some of the most difficult communities in the world. Each CNE’s relationship with her communities is crucial to improving nutrition and health related knowledge. These relationships are priceless, and earned through tireless efforts over four years of extremely hot summers and monsoon seasons of flooded and washed out roads. !
(Read about Gendha here: http://www.realmedicineblog.com/2013/04/11/voices-from-the-field-gendha-didi/). !!!

Photo: CNE Jamanti counseling during a film !The CNE’s task is not an easy one. According to the National Institute of Nutrition (NIN) 2011 survey, in Barwani District an estimated 34.8% of children suffer from acute malnutrition . In the same district, there are alarmingly poor indicators of 1
health and sanitation behaviors. Only 13% of mothers reported washing their hands before feeding their child, 53% reported washing their or their child’s hands after defecation, and only 5.8% use sanitary latrines. In addition, at the age of 5 months, only 41.2% of children were exclusively breastfed, and only 68% were breastfed within three hours of birth . 2!Three hours east of Barwani district by road, the situation in Khandwa district is just as dire. Facing rates of 29.8% acute malnutrition , only 18.3% of children aged 6 months were exclusively breastfed, only 8.4% of households use a toilet 3 4
facilities connected to or around their house. To add to the challenge, only 56.5% of rural women in Khandwa are 5
literate. 6!
! !Photo: CNE Kunti speaks with community after screening !In addition to the interpersonal communication that is the foundation of our program, RMF has also worked on developing and integrating technology solutions into our program in Madhya Pradesh. The technological solutions act as an extra tool in the CNE’s behavior change toolkit, complementing their comprehensive understanding of the grassroots realities of each community she works in. ! Assessment of Nutritional Status of under-five year rural children in the Districts of Madhya Pradesh State District: Barwani, National Institute of 1
Nutrition, Indian Council of Medical Research, Hyderabad, 2011
Assessment of Nutritional Status of under-five year rural children in the Districts of Madhya Pradesh State District: Barwani, National Institute of 2
Nutrition, Indian Council of Medical Research, Hyderabad, 2011
Assessment of Nutritional Status of under-five year rural children in the Districts of Madhya Pradesh State District: Khandwa, National Institute of 3
Nutrition, Indian Council of Medical Research, Hyderabad, 2011
DLHS-III, Government of India, 2007-8 4
DLHS-III, Government of India, 2007-8 5
Census of India, 2011 6

Having already introduced Commcare, a mobile phone based reporting, referral, and counseling tool in 2012 (links: http://www.realmedicineblog.com/2012/05/31/using-power-for-good-how-rmf-is-using-technology-to-transform-humanitarian-aid/ and http://www.realmedicineblog.com/2013/02/11/voices-from-the-field-commcare-and-the-struggle-against-poverty-and-inequality/), in 2013 RMF began piloting a program using community based videos on nutrition and health topics with Digital Green (http://www.realmedicineblog.com/2013/10/15/rmf-and-digital-green-partnership/). By equipping our CNEs in Khandwa with the tools to tell stories through movies, RMF provides targeted behavior change communication on health, nutrition and hygiene in a place where women have very little access to reliable health information and where only 56.5% of women can read posters, signs or brochures. The appeal of innovative medium and use of local themes draws attention, particularly in the land of Bollywood. !
! !Photo: RMF team interviews villagers to track behavior adoptions and practices !Since October 2013, RMF’s team has produced 15 videos (videos can be viewed here: http://www.digitalgreen.org/discover/RMNT/Madhya%20Pradesh/Hindi/Maternal-Child%20Health%20and%20Nutrition/) on topics including malnutrition and its causes, proper breastfeeding practices, and available government services to combat malnutrition. Armed with small PICO projectors, about the size of an iPhone, our CNEs have conducted 1,272 screenings in small targeted groups of six or more women and also to larger community groups, gaining a total attendance of 6,466 households across 90 villages. Screenings are followed by facilitated group discussions, which help clarify the messages viewed in the movies. !The results have been almost immediately visible. On a recent visit to Khandwa, I accompanied our team to villages to watch screenings and follow up with households that had previously seen our videos. In addition to the interest they generated, the movies had already proven effective in delivering much-needed messages. One mother, after viewing a film on Moderate Acute Malnutrition (MAM), confessed that prior to viewing RMF’s film, she used rations provided to her child by the Madhya Pradesh Government to supplement her entire family’s diet, and now uses those rations only for the recovery of her child. !

! !Photo: Screening for mothers in Khandwa !In four months, we have directly observed 179 adoptions of behaviors recommended in our videos, and are working on verifying the longer term effects of our videos, such as the increase in awareness of practices promoted in the videos. Our goal is to see 6,500 households practicing behaviors outlined in the movies after a year of screenings across the 90 targeted villages in Khandwa. !RMF’s CNEs are now armed with three distinct tools: information, technology, and tenacity. Any one of these is needed in the fight against malnutrition, but when combined they go a long way towards liberating human potential and eradicating malnutrition.