main lipids in the blood are the triglycerides and cholesterol. insoluble in the water. transport...
TRANSCRIPT

LIPIDS AND LIPOPROTEINS

LIPID CHEMISTRY AND CARDIOVASCULAR PROFILE
Main lipids in the blood are the triglycerides and cholesterol.
Insoluble in the water. Transport in the blood is via
lipoproteins
TRIGLYCERIDES
Glycerol with 3 attached fatty acids
Exogenous source : Dietary Endogenous : Liver and tissue storage
95 % of body fat is triglycerides Energy source when plasma glucose is
decreased Triglyceride catabolism is regulated by lipase,
epinephrine and cortisol
Triglycerides transported by Chylomicrons ( exogeneous ) and VLDL ( endogenous )

CHOLESTEROL
Found only in animals Important component of membranes, steroid
hormones, bile and Vitamin D
Exogeneous cholesterol comes from diet Endogeneous cholesterol is synthesized by the liver
70 % of cholesterol associated with cellular components
30 % is in the plasma ( ⅓ free form , ⅔ esterfied )
Transported by HDL and LDL
4
Fatty acids are short to long carbon chained molecules
Saturated fatty acids Unsaturated fatty acids
Phospholipids
Important components of cell membranes Lecithin and sphingomyelin are utilized to
determine fetal lung maturity from amniotic fluid ( L / S Ratio )
Glycolipids
Lipids with a carbohydrate component ABO antigen are glycolipids

LIPOPROTEINS
Lipoprotein is a complex spherical structure that has a hydrophobic core wrapped in hydrophilic coating.4 major classes of lipoproteins.
ChylomicronsVery low density lipoproteins (VLDL)Low density lipoproteins (LDL)High density lipoproteins (HDL)
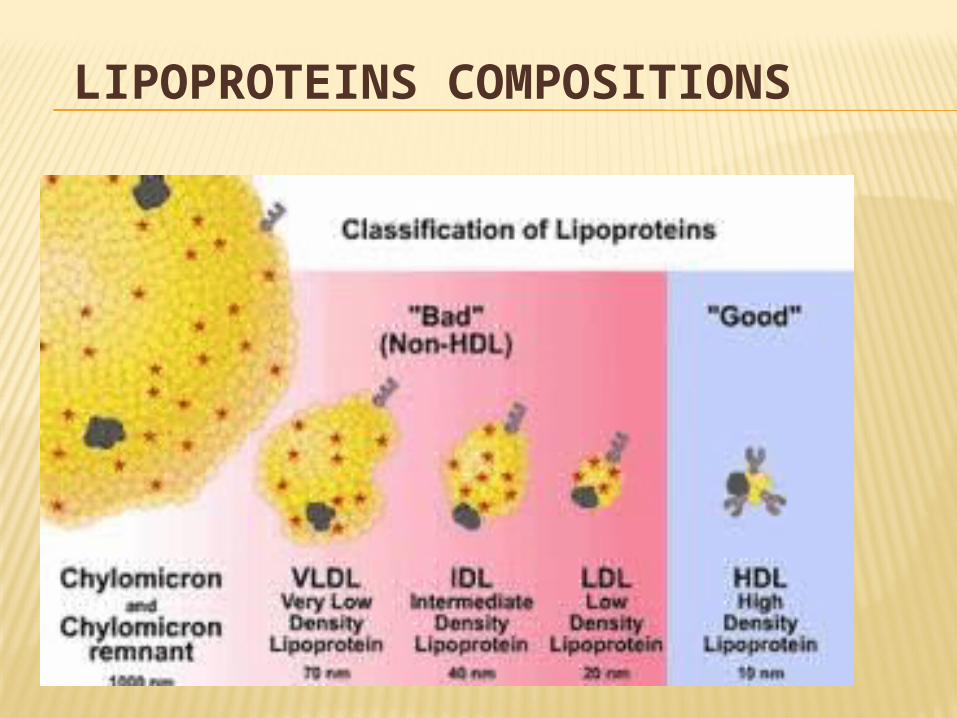
LIPOPROTEINS COMPOSITIONS

COMPOSITION OF LIPOPROTEINS
Class Diameter (nm)
% protein
% cholesterol
% phospholipid
% triacylglycerol& cholesterol ester
HDL 5–15 33 30 29 4
LDL 18–28 25 50 21 8
IDL 25–50 18 29 22 31
VLDL 30–80 10 22 18 50
Chylomicrons 100-1000 <2 8 7 84

CHYLOMICRON STRUCTURE
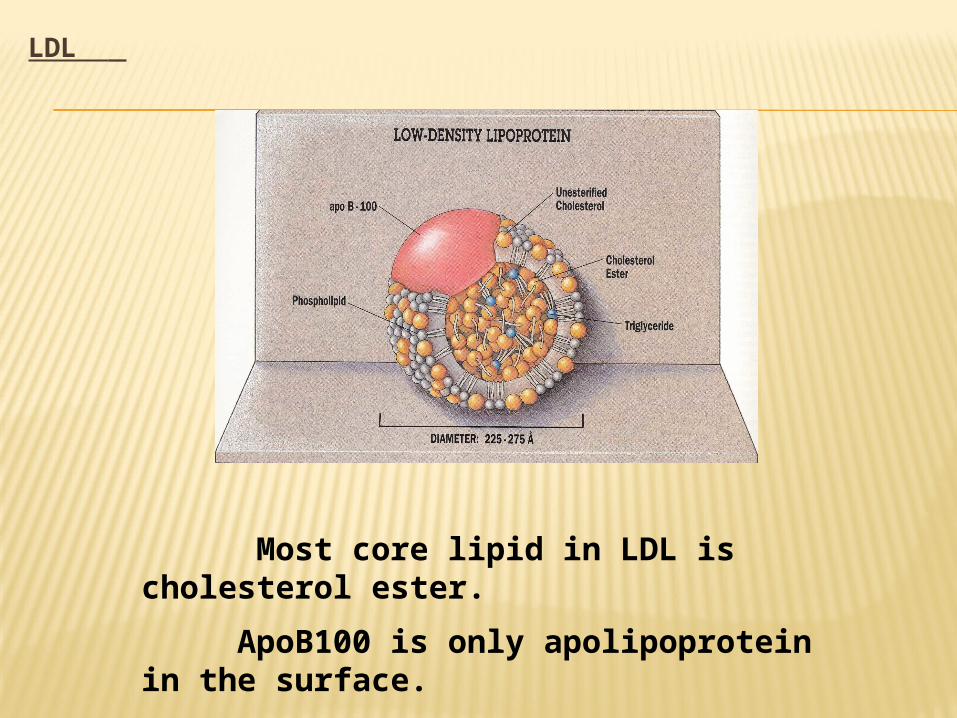
LDL
Most core lipid in LDL is cholesterol ester.
ApoB100 is only apolipoprotein in the surface.

LDL RECEPTOR
Also named as apoB-100/apoE receptors LDL receptors exist in the liver and in most peripheral tissues The complexes of LDL and receptor are taken into the cells by
endocytosis, where LDL is degraded but the receptors are recycled Number and function of the receptor shows LDL levels. LDL cholesterol levels are positively related to risk of
cardiovascular disease Therefore, cholesterol in LDL has been called “bad cholesterol”

APOLIPROPROTEINS
Outer protein “shell” of the lipoprotein molecule
The protein – lipid interaction allows the water insoluble lipid to become soluble in plasma
12

CLASSES OF APOLIPOPROTEINS
A, B, C, D, E are major classes Subclasses: apo A-1, apo C-II N.B. function of all apolipoproteins are not yet
known
• Act as structural components of lipoproteins
• Recognize the lipoprotein receptors on cell membrane surface as ligand
• Activate/inhibit enzymes involved in lipoprotein metabolism
METABOLISM
Exogenous Endogenous
Lipoprotein lipase release FFA and glycerol from chylomicron
and VLDL
Lecithin Cholesterol acyl transferase LCAT
Forms cholesteryl esters from free cholesterol and fatty acids


LIPID AND LIPOPROTEIN POPULATION DISTRIBUTIONS
Serum lipoprotein concentrations differ between adult men and women,
Primarily as a result of differences in sex hormone levels, Women having, on average, higher HDL
cholesterol levels and lower total cholesterol and triglyceride levels than men.
The difference in total cholesterol, however, disappears after menopause as estrogen decreases
HYPERCHOLESTEROLEMIA
Familial hypercholesterolemia (FH) (7.5- 12 mmol/L) Primarily LDL elevations Synthesis may be normal but decrease or lack
LDL receptors due to mutation in LDL receptor gene.
Therefore LDL builds-up in serum Since cells cannot acquire from LDL therefore
increase internal synthesis of cholesterol. Tendon xanthomatas Early occurrence of coronary artery disease
M. Zaharna Clin. Chem. 2009
18
HYPERTRIGLYCERIDEMIA
Triglycerides Borderline = 150-200 mg/ dl High 200-500 mg/dl Very High > 500 mg/dl
Familial hypertriglyceridemia Genetic
Secondary hypertriglyceridemia Hormonal imbalances Imbalance between synthesis and clearance of
VLDL
M. Zaharna Clin. Chem. 2009
19

HYPERTRIGLYCERIDEMIA
Generally caused by deficiency of LPL or LPL cofactor. (LPL hydrolyzes triglycerides in chylomicrons and VLDL)
Deficiency prevents processing and clearing of triglycerides
Elevated even with fasting
M. Zaharna Clin. Chem. 2009
20

FAMILIAL COMBINED HYPERLIPIDEMIA
Presence of elevated levels of serum total cholesterol and triglycerides
Hepatic overproduction of apo B Increased VLDL and LDL
M. Zaharna Clin. Chem. 2009
21

FAMILIAL HYPERCHYLOMICRONEMIA
Genetic mutation of LPL or apo C-II gene
Recurrent abdominal pain Pancreatitis

CLINICAL DISORDERS OF LIPID METABOLISM
Primary Secondary
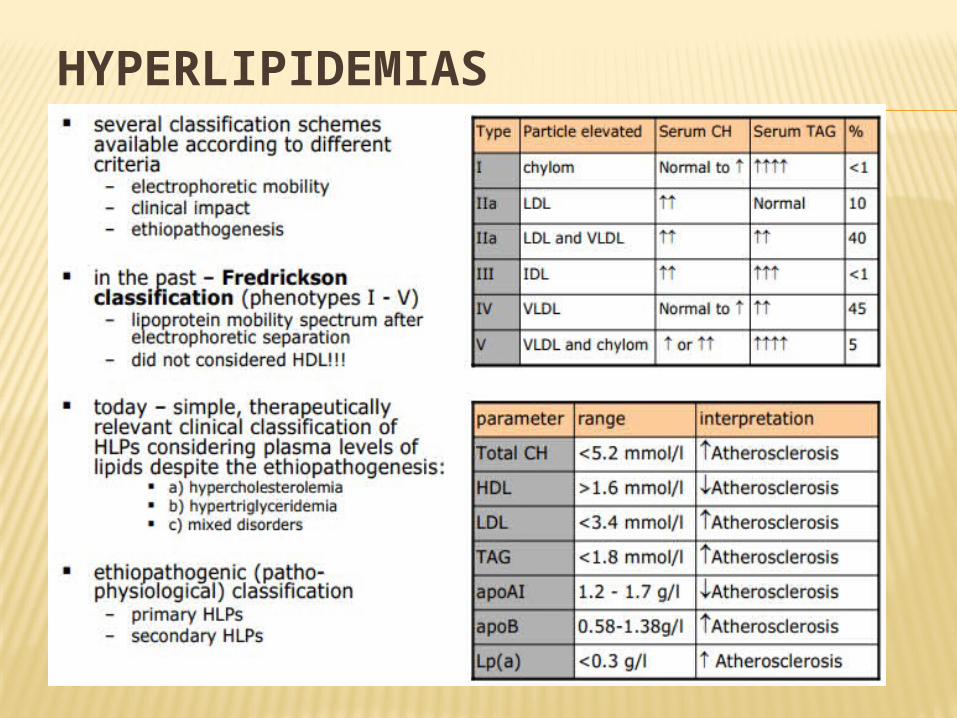
HYPERLIPIDEMIAS

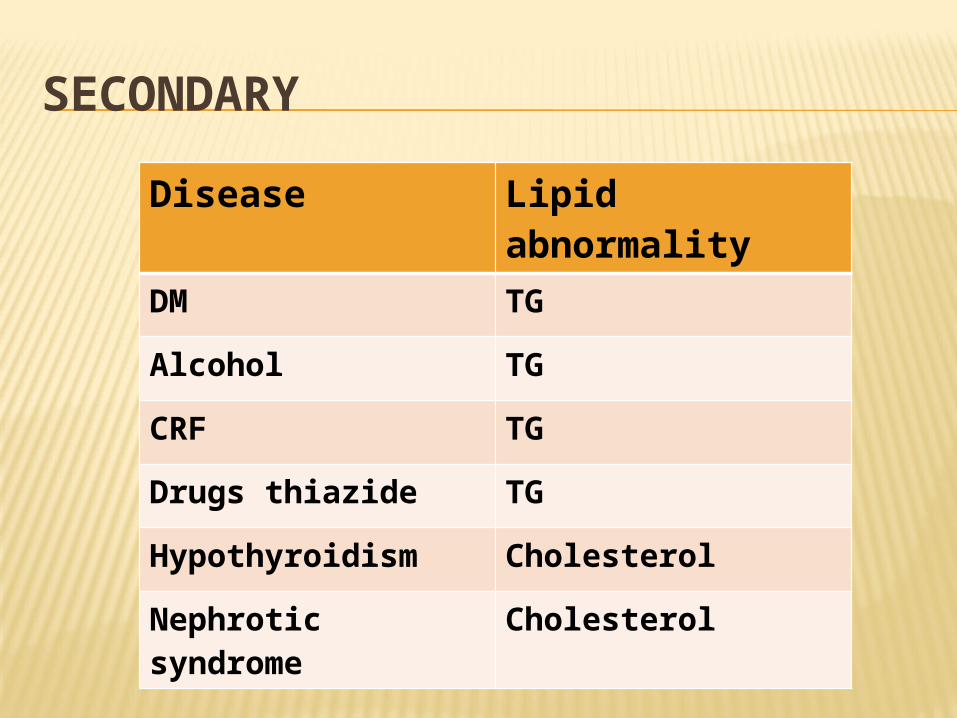
SECONDARY
Disease Lipid abnormality
DM TG
Alcohol TG
CRF TG
Drugs thiazide TG
Hypothyroidism Cholesterol
Nephrotic syndrome
Cholesterol