潛伏性結核病之診斷與結核病 之預防性投藥 · 2009-02-18 · tb: a leading...
TRANSCRIPT

潛伏性結核病之診斷與結核病之預防性投藥
台中榮總
胸腔內科
沈光漢醫師
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com


美國LTBI的治療情況
n Based on population and tuberculosis case rate data, it was estimated that 291,000 to 433,000 persons in the United States initiated treatment for latent tuberculosis infection in 2002
n It was also estimated that this prevented 4000 to 11,000 tuberculosis cases.
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Latent Infection of Tuberculosis in China
.
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
TB: A leading infectious killer- top 3 infectious killer
TB kills about 2 million people each year
8 million people become sick with TB each year
TB is the leading killer of HIV/AIDS patients
50 million people infected with drug-resistant TB
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

HIV and Drug-resistant TB – A lethal combination and a major threat to TB control
WHO declared TB a global emergency in 1993
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

DOTS-The Best TB Therapysince 1991
DOTS: 6 month therapy - The best therapy against TB (78%-96% cure rate).
Initial phase (daily, 2 months) with 4 drugs: INH, RMP, PZA, Ethambutol.
Continuation phase (3 times a week, 4 months) with 2 drugs: INH and RMP.
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Disease Burden of Tuberculosis in China, 2000 data
Prevalence of active pulmonary diseases is 367/
100,000
Prevalence of Sear positive pulmonary diseases is
122/100,000
130,000 patients die from tuberculosis every year
No data of latent tuberculosis in China up to now
China CDC 2006
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
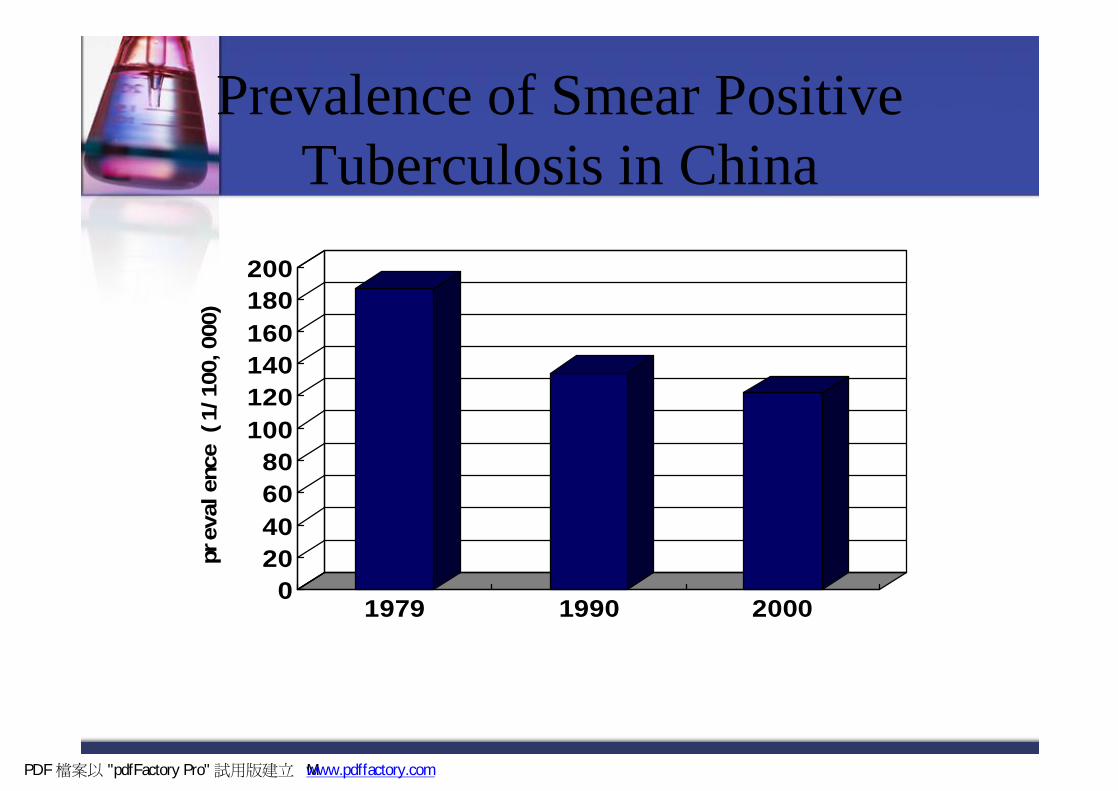
Prevalence of Smear Positive Tuberculosis in China
0
20
40
60
80
100
120
140
160
180
200
prevalence (1/100,000)
1979 1990 2000
PDF 檔案以 "pdfFactory Pro" 試用版建立 M www.pdffactory.com

Incidence of tuberculosis according to the report from China CDC
But incidence do not decrease!
0
200000
400000
600000
800000
1000000
1200000
1400000
1600000
2003 2004 2005 2006
China CDC 2006
PDF 檔案以 "pdfFactory Pro" 試用版建立 香ÿ www.pdffactory.com

Factors contribute to tuberculosis reemerging in China
nMDR TB?n HIV increasing?n Latent infection?n Diagnosis tools are more accurate to find more new cases?
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

HIV infected Tuberculosis Cases < 1/100,000 population in China
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

New TB cases are driven by the reservoir of latently infected people.
If we want to stop active TB cases, we need to eliminate this reservoir of infection.
This “hidden epidemic” of people infected with latent TB is enormous.
The growth in latent TB is becoming a clinical time bomb.
We need to defuse this bomb by increasing our efforts to identify and treat latently infected people.
Latent tuberculosis is the reservoir of active tuberculosis
Active TB
Latent TB
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Epidemiology of latent infection in the world
Frothingham R, et al.International Journal of Infectious Diseases (2005) 9, 297—311
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

45%
55%
Infected No infection
TST positive in China, 2000
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Shortage of TST
Poor specificity: antigenic cross-reactivity of
PPD with BCG and environmental mycobacteria
Poor sensitivity: 75-90% in active disease
(lower in disseminated TB and HIV infection;
unknown for latent infection)
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Factors leading to False-Positive TST Reactions
Nontuberculous mycobacterian Reactions caused by nontuberculous mycobacteria are
usually ≤ 10 mm of indurationBCG vaccination
n Reactivity in BCG vaccine recipients generally wanes over time; positive TST result is likely due to TB infection if risk factors are present
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
T SPOTTM detect INF-r released by specific T cells
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

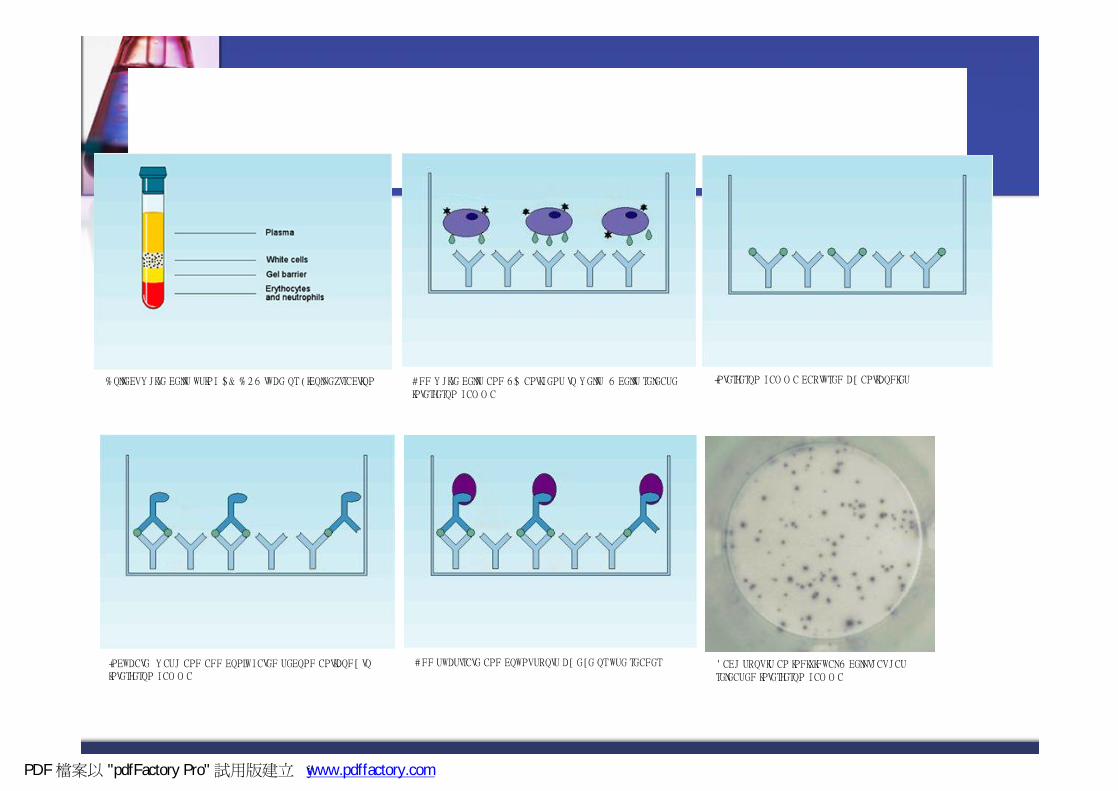
How does T-spot Technology Work
Patient Whole blood Sample
PBMC ESAT-6 CFP10
T cell secreting INF
Ab capture INF
Blue spot
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com


2 commercial Kit available for detecting latent or active tuberculosis
T cell-based assay for interferon gamma, the enzyme-linked
immunosorbent spot test (ELISPOT), has promise in the diagnosis
of Mycobacterium tuberculosis infection after exposure to a
known tuberculosis (TB) patient.
Commercialisation of two T cellbased tests for the diagnosis of M.
tuberculosis infection (T Spot TB by Oxford Immunotec and
Quantiferon-TB Gold by Cellestis)
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

T-cell based assay is recommended for detecting infection of M. Tb
measures individual reacting T cells:n Even individual cells can be detected in a sample.n Therefore even those who are severely immunocompromised, if a single cell
reacts then it can be detected.
measures all types of T cells:n Both CD4 and CD8 type T cells are detected.n Therefore if one type of T cells is depleted in a patient (e.g. CD4 T cells in HIV
infected patients) a response can still be detected from the CD8 T cells.
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com


The strategic for treating latent infection of tuberculosis in China?
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Lifetime Risk of Reactivation Tuberculosis
C. Robert Horsburgh. n engl j med 2004;350;20:2060-7
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
Latent infection of tuberculosis in China: Treat or not Treat?
BCG strategic or “find and treat” strategic?Conditionally treatment focusing high-risk groups: close house
contacts and immunocompromised casesChemotherapy or Immunotherapy?
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Trends in TB Cases in Foreign-born Persons, United States, 1986-2003
0
2,000
4,000
6,000
8,000
10,000
86 87 88 89 90 91 92 93 94 95 96 97 98 990102030405060
No. of Cases Percentage of Total Cases
No. of Cases Percentage
000102 03
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Reported TB Cases by Age Group United States, 2003
25 - 44 yrs(34%)
<15 yrs
(6%)15 - 24
yrs(11%)
45 - 64 yrs(29%)
65+ yrs(20%)
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿÿ www.pdffactory.com
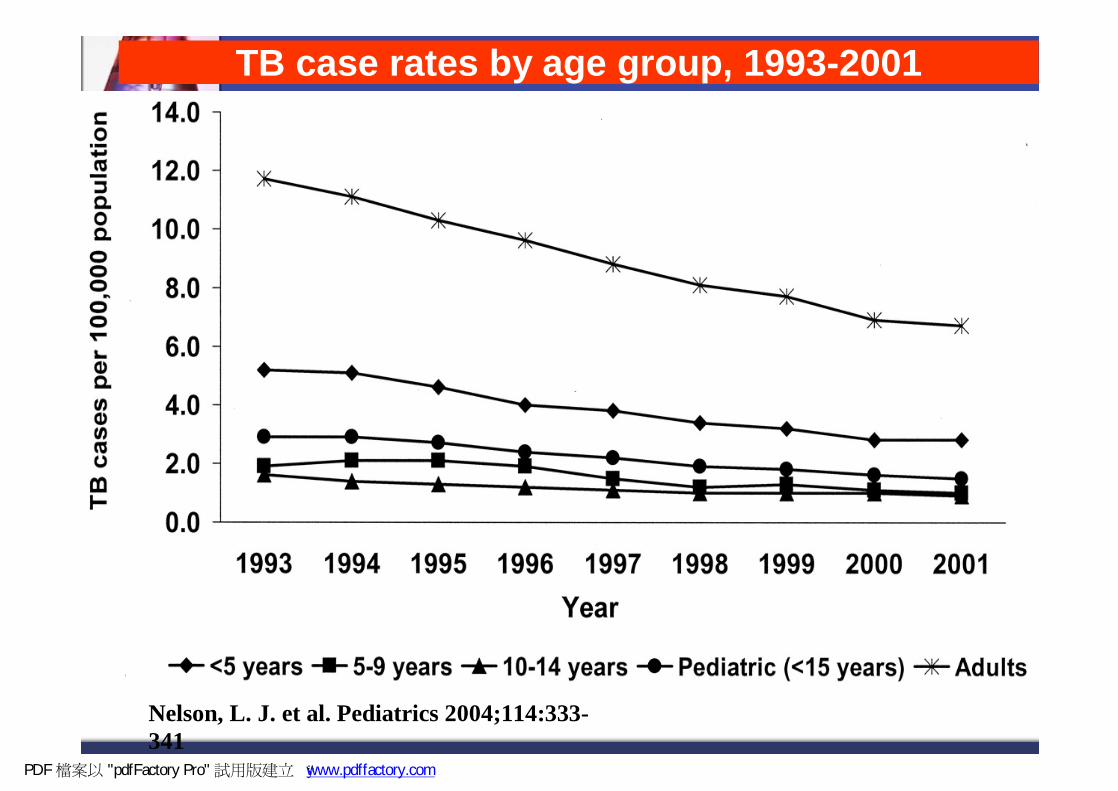
Nelson, L. J. et al. Pediatrics 2004;114:333-341
TB case rates by age group, 1993-2001
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Children <15 years with TBby Site of Disease
Extrapulmonary20%
Pulmonary75%
Pulmonary &Extrapulmonary
5%
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com


Latent TB Infection (LTBI)潛伏肺結核的定義
LTBI is the presence of M. tuberculosisorganisms (tubercle bacilli) without symptoms or radiographic evidence of TB disease.
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com


TB Control In the United States
Identification of new cases of TBn Initiation of appropriate treatmentn Directly observed therapy
Contact Investigationsn Identify persons at risk for infection
Targeted tuberculin testing n Identifies persons at high risk for TB who would
benefit by treatment of LTBIn Treatment of latent TB infection (LTBI)
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
Treatment of Latent Tuberculosis Infection in Children
INH 10 mg/kg (max., 300 mg) PO daily for 270 dosesAlternative: Twice weekly directly observed (DOT) INH 20-40 mg/kg
(max., 900 mg) PO for 72 dosesMonitor index case isolate sensitivitiesHepatotoxicity from INH is rare in children:n A monthly assessment for clinical evidence of hepatotoxicity
should be made: loss of appetite or weight, nausea, vomiting, abdominal pain, jaundice
n Routine monitoring of LFTs is not indicated
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Tuberculosis Control in the United States
Contact Investigations The most reliable TB control program is based upon aggressive and expedient contact investigations, rather than routine screening of large populations with low risk.
Can be complex, require experience and often a lot of detective work.
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com











預防結核病前瞻治療政策
疾管局第三組
2008.03.19肺結核接觸者接受胸部x光片檢查與皮膚試驗
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Concentric-Circle Approach to Contact Tracing
HomeEnvironment
IndexCase
Close
Casual
LeisureEnvironment
Work/SchoolEnvironment
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Calculated from data from:Grzybowski S, et al. Bull Int Union Tuberc Lung Dis 1975;50:90-106
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

We are fighting a large & growing epidemic with old tools
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com
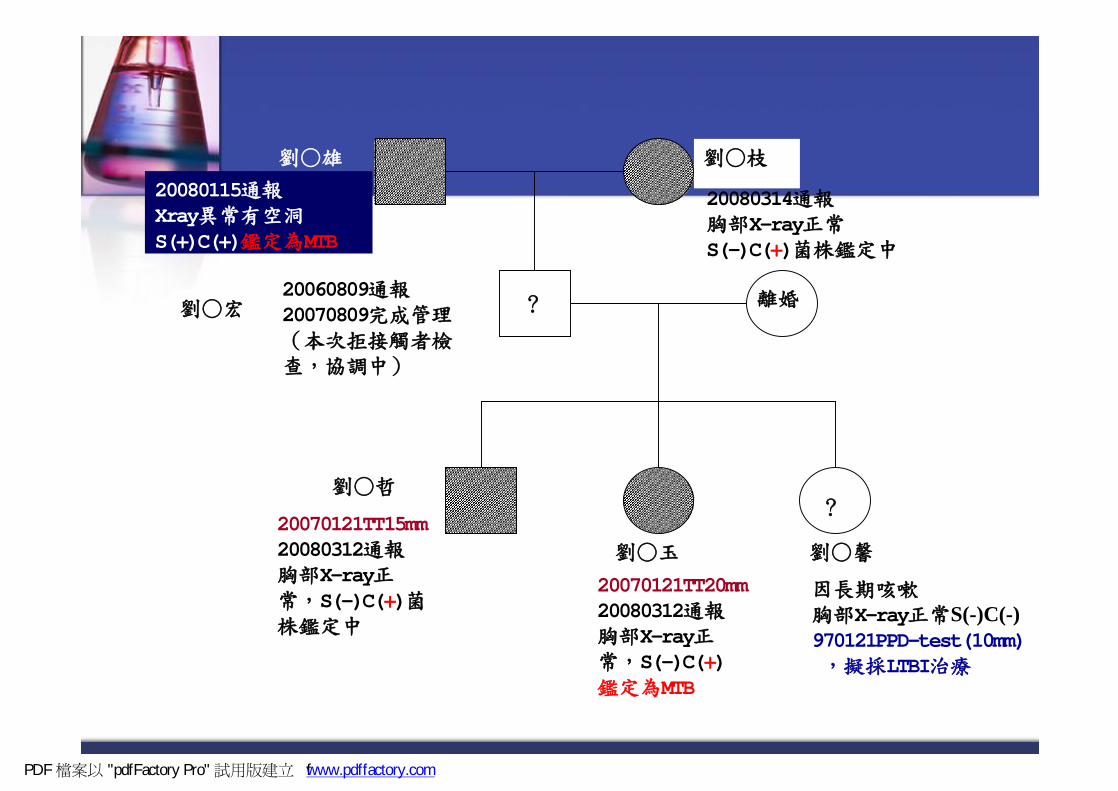
劉○雄 劉○枝
20060809通報20070809完成管理(本次拒接觸者檢查,協調中)
劉○宏
20080115通報Xray異常有空洞S(+)C(+)鑑定為MTB
離婚
劉○哲
20070121TT15mm20080312通報胸部X-ray正常,S(-)C(+)菌株鑑定中
20070121TT20mm20080312通報胸部X-ray正常,S(-)C(+) 鑑定為MTB
劉○玉 劉○馨
因長期咳嗽胸部X-ray正常S(-)C(-) 970121PPD-test(10mm),擬採LTBI治療
20080314通報胸部X-ray正常S(-)C(+)菌株鑑定中
?
?
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com

4 歲 2005/10/14 TT(1)2008/1/29 TT(22) x光正常 2/4 LTBI
2歲 2008/1/29 TT(16)X光正常2/4 LTBI
案三 56歲營造包商2005/10/14x光正常2008/3/7M-C+通報
案一 49歲家管2005/8因病就醫2005/10/11通報M-C+2006/5/26完治 2008/1/24正常
案二 32歲營造包商2005/10/14x光正常2008/1/22M+C+通報
30 歲 家管2008/1/25有一白點已建議進一步檢查
2年3個月
2年5個月
陽轉
PDF 檔案以 "pdfFactory Pro" 試用版建立 fÿÿ www.pdffactory.com

Patient's delay
Doctor's delay
Transmission
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

結核病防治
結核潛隱性
感染
傳染性結核病
非傳染性結核病
化學治療
卡介苗接種
病人延誤
醫師延誤
傳染 transmission
死亡接觸
預防性治療方式:INH每日1次口服,治療
9個月
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Zhang Y, et al. In: Hatfull GF, et al.Molecular Genetics of Mycobacteria, 2000
Model of Isoniazid Action
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Combined Drug Resistance, 2003-5
6.6 2.2 1.3 6.1 10.4 1.7
Taiwan Surveillance of Drug Resistance in Tuberculosis (TSDRTB), 2003-5
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com
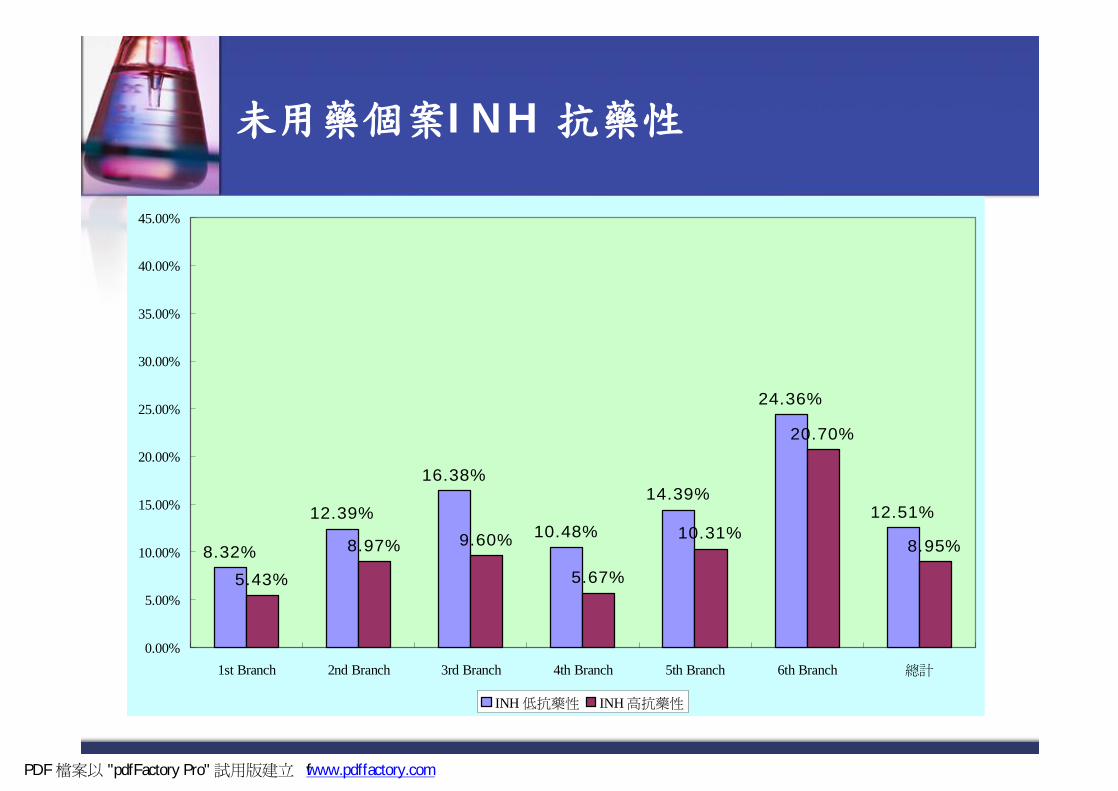
未用藥個案INH 抗藥性
8.32%
16.38%
10.48%
14.39%
24.36%
12.51%
5.43%
8.97% 9.60%
5.67%
10.31%
20.70%
8.95%
12.39%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
1st Branch 2nd Branch 3rd Branch 4th Branch 5th Branch 6th Branch 總計
INH 低抗藥性 INH 高抗藥性
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com
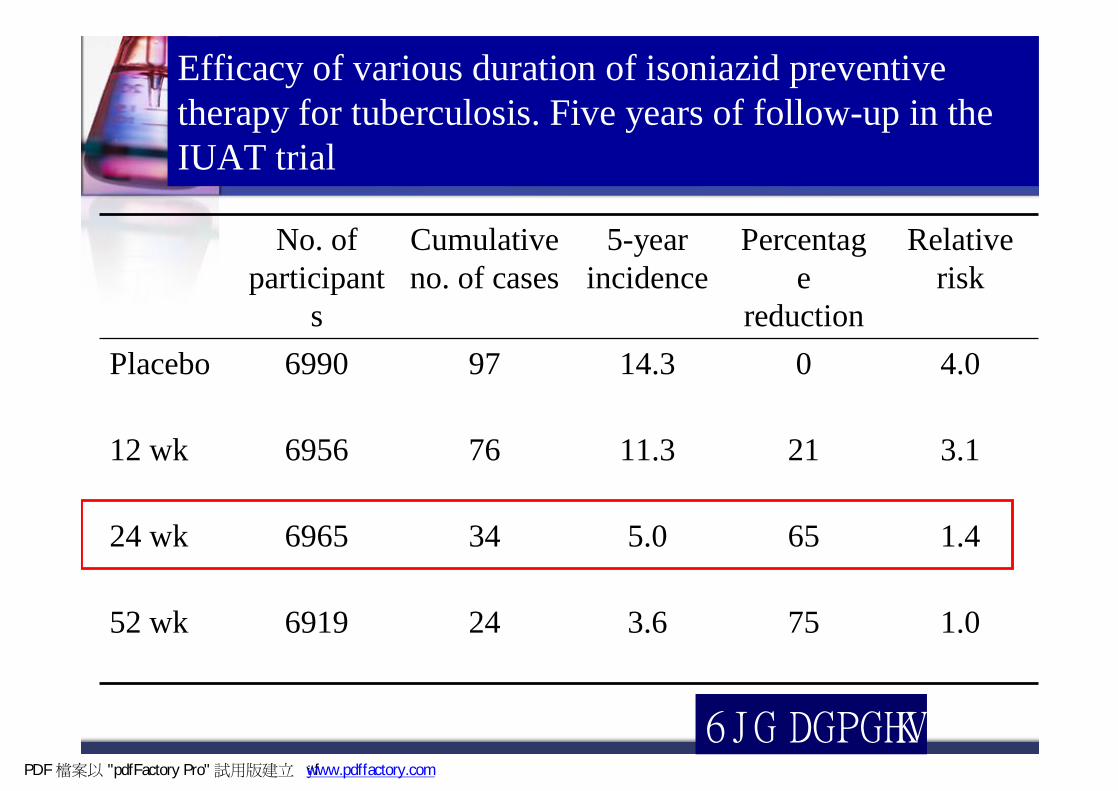
Efficacy of various duration of isoniazid preventive therapy for tuberculosis. Five years of follow-up in the IUAT trial
1.0753.624691952 wk
1.4655.034696524 wk
3.12111.376695612 wk
4.0014.3976990Placebo
Relative risk
Percentage
reduction
5-year incidence
Cumulative no. of cases
No. of participant
s
Bull. WHO. 1982;60:555-64
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ f www.pdffactory.com

Five years of follow-up in the IUAT trial Benefit-to-risk ratio
2.15.210.753 weeks
2.63.69.324 weeks
1.22.53.012 weeks
Benefit-to-risk ratio
Cumulative no. of hepatitis
cases incurred+
Cumulative no. of tuberculosis cases
prevented*
* Reduction in cases over placebo regimen (per 1000 persons)+ Excess of cases over placebo regimen (per 1000 persons)
PDF 檔案以 "pdfFactory Pro" 試用版建立 � www.pdffactory.com

Jindani A, et al. Am Rev Respir Dis 1980;121:939-49
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Jindani A. Thesis. University of London, 1979
別小看INAH單一藥物的威力
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Patient's delay
Doctor's delay
Transmission
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Ferebee SH, et al. Am Rev Respir Dis 1963;88:161-75Mount FW, et al. Am Rev Respir Dis 1962;85:821-7Comstock GW. Am Rev Respir Dis 1962;86:810-22
Horwitz O, et al. Bull World Health Organ 1966;35:509-26PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Veening GJJ. Bull Int Union Tuberc 1968;41:169-71Egsmose T, et al. Bull World Health Organ 1965;33:419-33
Ferebee SH, et al. Am Rev Respir Dis 1962;85:490-521Bush OB, et al. Am Rev Respir Dis 1965;92:732-40
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

International Union Against Tuberculosis Committee on ProphylaxisBull World Health Organ 1982;60:555-64
Ferebee SH. Adv Tuberc Res 1969;17:28-106Katz J. Am Rev Respir Dis 1962;86:8-15
John GT, et al. Transplantation 1994;57:1683-4Hong Kong Chest Service / Tuberculosis Research Centre, Madras /
British Medical Research Council. Am Rev Respir Dis 1992;145:36-41
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Comstock GW. Int J Tuberc Lung Dis 1999;3:847-50
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

International Union Against Tuberculosis Committeeon Prophylaxis. Bull World Health Organ 1982;60:555-64
Ferebee SH. Adv Tuberc Res 1969;17:28-106Horwitz O, et al. Bull World Health Organ 1966;35:509-26
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Whalen CC, et al. N Engl J Med 1997;337:801-8Hong Kong Chest Service, et al. Am Rev Respir Dis 1992;145:36-41
Mwinga A, et al. AIDS 1998;12:2447-57
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Hong Kong Chest Service, et al. Am Rev Respir Dis 1992;145:36-41Gordin F, et al. JAMA 2000;1445-50
Halsey NA, et al. Lancet 1998;786-92Mwinga A, et al. AIDS 1998;12:2447-57
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com






潛伏結核菌感染檢測的最新進展-針對長期照護機構
台中榮總胸腔內科沈光漢
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com


LTBI vs. Pulmonary TB Disease
Latent TB Infection
TST* or QFT† positive
Negative chest radiograph
No symptoms or physical findings suggestive of TB disease
Pulmonary TB Disease
TST or QFT usually positive
Chest radiograph may be abnormal
Symptoms may include one or more of the following: fever, cough, night sweats, weight loss, fatigue, hemoptysis, decreased appetite
Respiratory specimens maybe smear or culture positive
M. tuberculosis
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Mantoux test曼陀氏測驗
皮膚試驗標準方法
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

台灣目前結核病接觸者檢查規範-97年6月制定
對象 :n 與指標個案共同居住者。
n 與指標個案一天內接觸8小時以上之接觸者。n 其他有必要進行接觸者檢查之個案另行專案處理。
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com

紫色柱狀是接觸者第一年的tb疾病率,黃色柱狀是台灣2005年一般族群的tb發生率,
紫色線是2組相比較的RR
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

12歲以下的RR是206倍,隨著年齡增長,RR就隨之而下降,至65歲以上,RR剩下6倍
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

檢查方式
滿12歲以上接觸者進行胸部X光檢查。惟如半年內曾照胸部X光,並能提出診斷正常之證明者,可不必再作第一次檢查
小於等於十二歲以下兒童接觸者,一律作結核菌素測驗及X光檢查等二項
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

結核菌素測驗判讀結果The new criteria of Taiwan’s CDC 2007
(1)以≥ 5 mm作為判讀基準:n人類免疫不全病毒感染、惡性疾病、器官移
植與其他免疫功能不全病患 (包括類固醇治療劑量相當於15 mg/day prednisone以上超過一個月)之接觸者
n (HIV, immunocompromised and immnosuppresant )
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
(2)以≥ 10 mm作為判讀基準:a.接觸具傳染性之結核病患(close contact with infectious
TB patients)b.接觸不具傳染性之結核病患,但符合以下條件:(a)卡介苗注射時間與執行結核菌素測驗間隔 > 6年以上者。
(b)從未接種過卡介苗者。(unvaccinated)(c)具有罹患結核病之危險因素者:例如有結核病家族史、糖尿病、慢性腎衰竭、胃部切除、小腸繞道手術、生長遲滯、營養不良、注射藥癮者
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

(3)以≥ 15 mm作為判讀基準:接觸不具傳染性之結核病患且卡介苗注射時間與執行結核菌素測驗間隔 ≤ 6年者
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com


12歲以下之接觸者結核菌素反應陽性且排除「活動性結核病」者,應積極勸導並安排感染接觸者以直接觀察預防治療(DOPT ,Directly Observed Prevention Therapy)方式進行潛伏結核感染治療(Treatment of LTBI)
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

False-positive tuberculin skin tests: what is the absolute effect
of BCG and non-tuberculous mycobacteria?
Farhat M, Greenaway C, Pai M, Menzies DThe international journal of tuberculosis and lung disease. 2006
Nov;10(11):1192-204
皮膚試驗是否會受卡介苗或非結核分枝桿菌的影響??
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ � www.pdffactory.com

Methods: NTM effect evaluation
n Positive TST: reaction to PPD ≥ 10 mmn Positive NTM: reaction to NTM antigens ≥ 5 mmn TST or NTM cross-reactions: dual TST simultaneously with PPD
and NTM antigensà the reaction to one antigen larger than the other, the smaller reaction was a cross-reaction
n TST dominant: TST reaction≥NTM reactionà the reaction to the NTM was assumed to be a cross-reaction
n NTM dominant: reaction to NTM antigen ≥ 1 mm larger than the TST reaction
n FP-TSTNTM: TST was 10–14 mm and the dual NTM reaction was larger (dominant)
n Dual mycobacterial infection: TST ≥ 15 mmàTB infection (true positive), even if the NTM reaction is larger
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Results:False-positive TST from BCG
8.5% 41.8%
PDF 檔案以 "pdfFactory Pro" 試用版建立 � www.pdffactory.com
卡介苗接種對象
n 新生兒:出生體重達2500克以上,出生24小時後直接接種,由各醫院卡介苗工作人員辦理。
n 嬰幼兒:
n 嬰兒:一歲以內兒童,採直接接種,於各鄉鎮
市區衛生所卡介苗門診辦理。
n 幼兒:一歲以上六歲以下幼兒先給予結核菌素測驗,反應陰性者接種卡介苗。
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com




IGRA特異性相當高(92-97%)
皮膚試驗
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com


本研究樣本之性別及年齡分布
(5.2%)7未註明
(3.7%)5>90歲(14.2%)1981-90歲(14.9%)2071-80歲(15.7%)2161-70歲(23.1%)3151-60歲(14.2%)1941-50歲(7.5%)1031-40歲(1.5%)221-30歲
年齡
(50.7%)68女
(49.3%)66男
性別
(n=134)病患
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

(35.8%)48五樓病房
(31.3%)42三樓病房
(32.8%)44二樓病房
病房
(63.4%)85有
(36.6%)49無
卡介苗疤
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

(2.0%)1(5.6%)1(9).工讀生
(2.0%)1(5.6%)1(8).廚師
(4.1%)2(11.1%)2(7).助理
(12.2%)6(33.3%)6(6).書記
(14.3%)7(38.9%)7(5).行政人員
(2.0%)1(5.6%)1(4).藥師
(24.5%)12(38.7%)12(3).看護人員
(30.6%)15(48.4%)15(2).護理人員
(8.2%)4(12.9%)4(1).醫師
職稱
(n=49)(n=18)(n=31)
合計員工醫療照護
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

(22.4%)11(61.1%)11(0.0%)0(4).其他
(16.3%)8(5.6%)1(22.6%)7(3).醫院病房
(10.2%)5(0.0%)0(16.1%)5(2).RCW
(51.0%)25(33.3%)6(61.3%)19(1).護理之家
目前工作單位
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

本研究樣本經結核菌素皮膚試驗﹙T.T﹚之結果 (N=183)
(43.5%)57(41.2%)7(75.9%)22(32.9%)28陽性
(56.5%)74(58.8%)10(24.1%)7(67.1%)57陰性15
(70.2%)92(70.6%)12(100%)29(60.0%)51陽性
(29.8%)39(29.4%)5(0.0%)0(40.0%)34陰性10有接種
(42.3%)22(100%)1(100%)2(38.8%)19陽性
(57.7%)30(0.0%)0(0.0%)0(61.2%)30陰性10未接種
(n=183)(n=18)(n=31)(n=134)結果Cut off卡介苗
合計員工醫療照護病患結核菌素皮膚試驗
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

38.8%
60.0%
32.9%
100% 100%
75.9%
100%
70.6%
41.2%
0%
20%
40%
60%
80%
100%病患醫療照護員工
陽
性
率
結核菌素皮膚試驗
T.T cut off (10)結核菌素皮膚試驗
T.T cut off (10)結核菌素皮膚試驗
T.T cut off (15)
未接種卡介苗 有接種卡介苗
PDF 檔案以 "pdfFactory Pro" 試用版建立 À www.pdffactory.com

本研究樣本經QuantiFERON-TB Gold試驗之診斷結果 (N=183)
183(13.7%)25(14.2%)26(72.1%)132合計
18(0.0%)0(5.6%)1(94.4%)17員 工
31(7.4%)2(12.9%)4(80.6%)25醫療照護
134(17.2%)23(15.7%)21(67.2%)90病 患
Total
陽性Positive
不確定Indeterminate
陰性Negative
身份
QuantiFERON-TB Gold 試驗結果
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

研究樣本身份別與QuantiFERON-TB Gold 試驗結果的關係
0.000.0%017員 工
0.5910.368%225醫療照護
Referent20.4%2390病 患
p值R.R陽性率陽性陰性身份別
QuantiFERON-TB Gold 試驗
註: R.R:Relative Risk
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com


3009.53 13.12 17陽 性
#陽性>陰性
3507.96 17.76 17不確定
0.013*4.473107.38 11.69 97陰 性有接種n=167
25124.92 18.67 9陽 性
#陽性>陰性26011.36 12.50 8不確定
0.000*** 13.03 2506.36 5.71 35陰 性未接種n=13
p值F值Max.Min.SDMeanN結核菌素皮膚試驗T.T值QFT
結果
卡介苗
統計方法: One-way ANOVA *:p<0.05 **:p<0.01 ***:p<0.001
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Recommendations for Use of QFT-G
Recommendations for Use of QFT-G
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
Contact investigationsEvaluation of recent immigrants who have
had BCG vaccinationTB screening of health-care workers and
others undergoing serial evaluation for M. tuberculosis infection
QFT-G can be used in all circumstances in which the TST is used, including
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Follow up of Positive QFT-G
Follow up of Positive QFT-G
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

No reason exists to follow a positive QFT-G with a TST
Persons with a positive QFT-G result should be evaluated for TB disease before LTBI is diagnosed
After TB has been excluded, treatment of LTBI should be considered
A positive QFT-G should prompt the same health and medical interventions as a positive TST result
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Follow up of Negative QFT-G
Follow up of Negative QFT-G
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
The majority of healthy adults who have negative QFT-G results are unlikely to have M. tuberculosis infection and do not require further evaluation
The majority of healthy adultswho have negative QFT-G results are unlikely to have
M. tuberculosis infection and do not require further evaluation
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Follow up of Indeterminate QFT-G
Follow up of Indeterminate QFT-G
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

An indeterminate QFT-G result does not provide useful information regarding the likelihood of M. tuberculosis infection
Optimal follow up of persons with indeterminate QFT-G results has not been determined
Options are to repeat QFT-G with a new blood sample, administer a TST, or do neither
Decision should be based on pre-test likelihood of M. tuberculosis infection
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Contact Investigations
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

For persons with recent contact to an infectious TB patient, negative QFT-G results should be confirmed with a repeat test 8-10 weeks after exposure (end of window period) as is recommended for a negative TST
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
預防結核病前瞻治療計畫
依據:傳染病防治法
目的:降低結核菌潛伏感染者發病機率
實施階段及目標
n以對感染後發病機會高、順服度高、藥物成本及安全性高等方向考量
n第一階段(2008年4月1 日起)確診肺結核接觸者12歲(含)以下潛伏感染者
n第二階段:確診肺結核接觸者之HIV(+)、矯正機關及醫護人員之潛伏感染者
n第三階段:確診肺結核接觸者之潛伏感染者全面
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
Latent TB治療前須仔細評估
An Official ATS Statement: Hepatotoxicity of
Antituberculosis Therapy
Am J Respir Crit Care Med Vol 174. pp 935–952, 2006
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Isoniazid-related hepatitis
0
5
10
15
20
25
< 20 20-34 35-49 50-64 > 64
Age Group (yr)
Cas
e R
ate
(/100
0)
ProbablePossible
Kopanoff DE et al. Am Rev Respir Dis 1978;117:991-1001.
PDF 檔案以 "pdfFactory Pro" 試用版建立 f f www.pdffactory.com
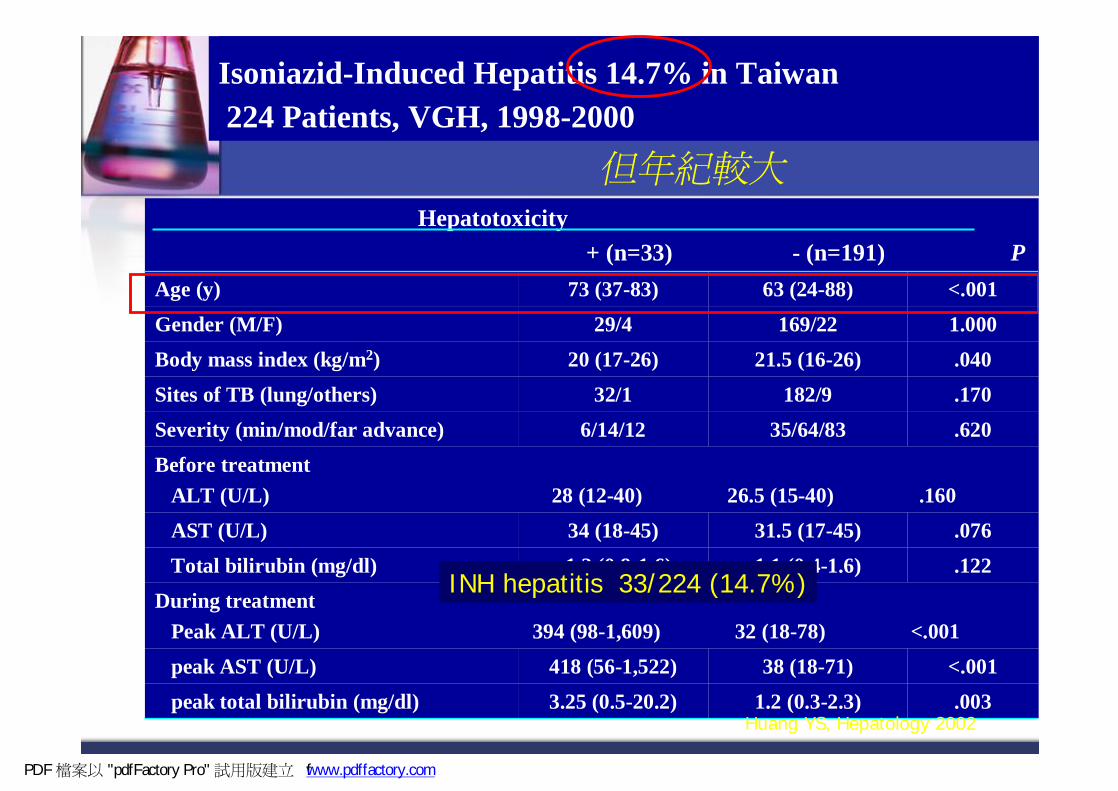
.0031.2 (0.3-2.3)3.25 (0.5-20.2)peak total bilirubin (mg/dl)<.00138 (18-71)418 (56-1,522)peak AST (U/L)
During treatmentPeak ALT (U/L) 394 (98-1,609) 32 (18-78) <.001
.1221.1 (0.4-1.6)1.2 (0.8-1.6)Total bilirubin (mg/dl)
.07631.5 (17-45)34 (18-45)AST (U/L)
Before treatmentALT (U/L) 28 (12-40) 26.5 (15-40) .160
.62035/64/836/14/12Severity (min/mod/far advance)
.170182/932/1Sites of TB (lung/others)
.04021.5 (16-26)20 (17-26)Body mass index (kg/m2)1.000169/2229/4Gender (M/F)<.00163 (24-88)73 (37-83)Age (y)
Hepatotoxicity+ (n=33) - (n=191) P
Isoniazid-Induced Hepatitis 14.7% in Taiwan 224 Patients, VGH, 1998-2000
Huang YS, Hepatology 2002
INH hepatitis 33/224 (14.7%)
但年紀較大
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com
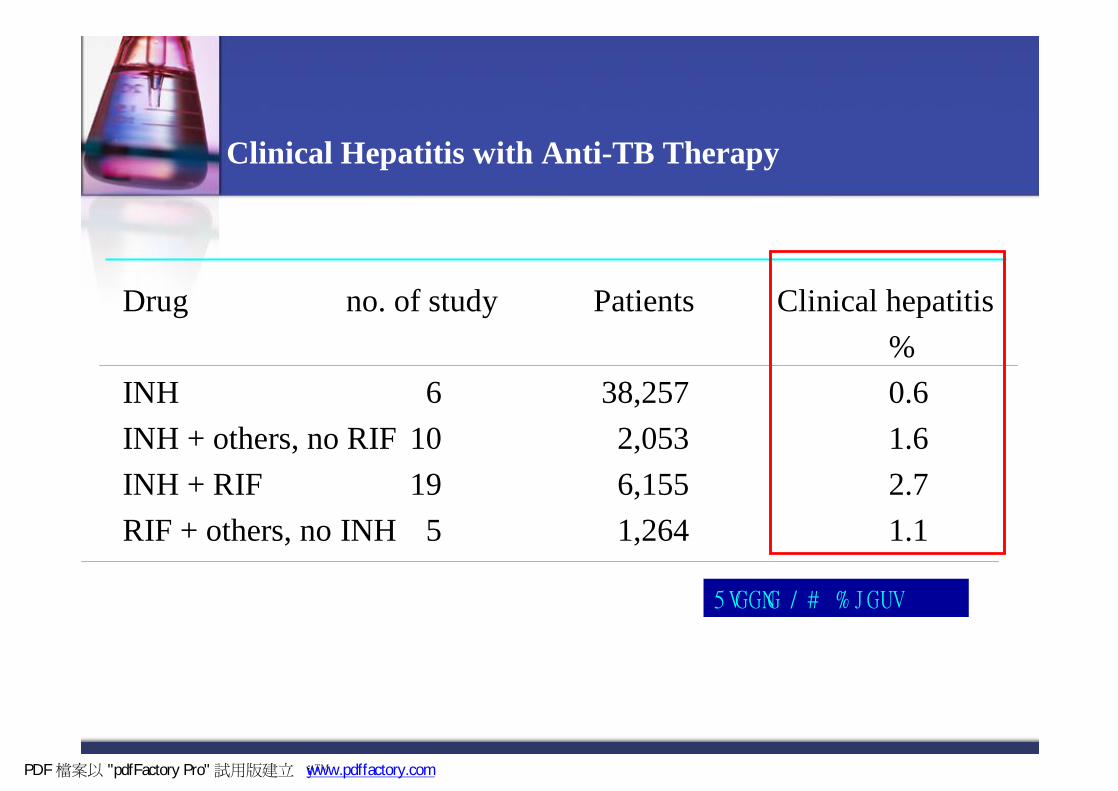
Clinical Hepatitis with Anti-TB Therapy
Drug no. of study Patients Clinical hepatitis%
INH 6 38,257 0.6INH + others, no RIF 10 2,053 1.6INH + RIF 19 6,155 2.7RIF + others, no INH 5 1,264 1.1
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ � www.pdffactory.com

Riska N. Bull Int Union Tuberc 1976;51:203-8
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Riska N. Bull Int Union Tuberc 1976;51:203-8PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com


Will we meet the MDG-STOP TB Partnership goal by 2015
Using the old DOTS approach and with current progressnNo
Two other important reasons for potential failurenAfrica: HIV/AIDS (--80% of all HIV-TB)nEast Europe/China/India: MDR-TB (--75% of
all MDR-TB
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Dual infection
n 14 million people co-infected with HIV and M.TB in the world
n 11 million people co-infected with HIV and M.TB in sub-Saharan Africa (80%)
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Global Plan to Stop TB, 2006-2015
n Pursue high quality DOTS expansion n Address HIV/TB and MDR/XDR-TBn Contribute to health system strengtheningn Engage all care providersn Empower people with TB, and communitiesn Enable and promote research
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com



Isoniazid preventive therapy:excellent efficacy
n Primary prevention in HIV+ve persons:uReduces frequency of TB by 43% (CI, 21-
59%)n Secondary prevention in HIV-infected patients
with successfully treated TB:uReduces frequency of recurrent TB by 50-80
%
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Pape JW, et al. Lancet 1993;342:268-72Mwinga A, et al. AIDS 1998;12:2447-57
Whalen CC, et al. N Engl J Med 1997;337:801-8Gordin FM, et al. N Engl J Med 1997;337:315-20
Hawken MP, et al. AIDS 1997;11:875-82
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com
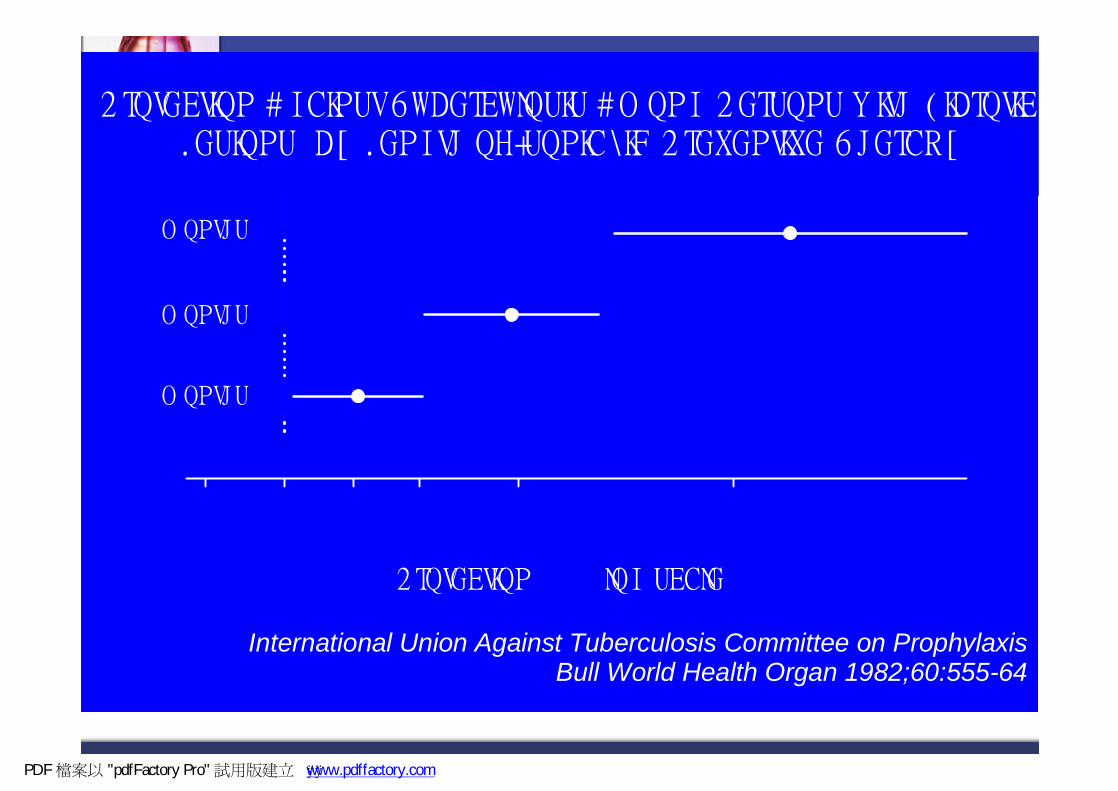
International Union Against Tuberculosis Committee on ProphylaxisBull World Health Organ 1982;60:555-64
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Isoniazid preventive therapy[implementation straightforward]S0, why has it not been scaled up??
n We do not know where to set up IPT clinics or who should take responsibility
n Concerns about difficulties in excluding active TB in HIV-infected persons
n Fear of creating INH resistance
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
(μg/mL)( R ) ( S)
TotalNo (%) No. (%)
RMP(1.0) 357 4.60 % 7400 95.40% 7757
EMB-H (10.0) 73 0.94 % 7684 99.06% 7757
EMB-L(5.0) 261 3.36 % 7496 96.64% 7757
INH-H(1.0) 607 7.83 % 7150 92.17% 7757
INH-L(0.2) 918 11.83 % 6839 88.17% 7757
SM-H(6.0) 408 5.26 % 7349 94.74% 7757
SM-L(2.0) 668 8.61 % 7089 91.39% 7757
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ f www.pdffactory.com

Data from Brazil: risk of TB in relation to ART/IPT
n Adjusted hazard ratiouNo ART 1uART only 0.55uIPT only 0.36uART and IPT 0.23
Colub et al AIDS 2007
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Combined QuantiFERON Assay and Tuberculin Skin Test to Detect Latent Tuberculosis
Infection in Rheumatoid Arthritis Patients Treated with Adalimumab
Der-Yuan Chen, Gwan-Han Shen, Tsu-Yi Hsieh, Joung-Liang Lan
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
TB is a major threat for RA patients with anti-TNF therapy in
Taiwan
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

Current methods in detection of Latent TB Infection Current methods in detection of Latent TB Infection (LTBI)(LTBI)
nn Abnormal Chest XAbnormal Chest X--ray ray nn Positive tuberculin skin test Positive tuberculin skin test nn InterferonInterferon--γγassays (+)assays (+)uuThe The QuantiFERONQuantiFERON--TB assayTB assayuuThe T SPOTThe T SPOT--TB assay TB assay
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com


1900
2000
2006
Use blood tests, if available, in:
NICE reviewed 11 studies published before July 2005: 6 papers used ELISpot, 5 used ELISA. They will revise the recommendations as new evidence emerges
Recent HPA guidelines very similar
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

From bench to bedside to policy: National TB Guidelines endorsing use of TIGRAs over the last two years
Use TIGRA as replacement for TST in all patient groups
n USAn Canada
Use TIGRA in individuals who have tested positive by TST and in individuals in whom TST is unreliable (NICE)
n UKn Italyn Germanyn Francen Spainn Hollandn Switzerlandn Norwayn Denmarkn Icelandn Czech Republic
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com

Latent TB infection
Transient infection with clearance
Long-term immune control
Primary TB in the first 1-2 years after infection
Lifelong containment
Reactivation TB
No infection Infection
Exposure to M. tuberculosis
5% 95%
5% 90%
?
Flow Chart: The natural history of M. tuberculosis infection
Clinical utility in LTBI
- HIV: TIGRA > TST
Children: TIGRA > TST
- Concomitant illness (renal failure, diabetes etc): TIGRA ≥ TST
Iatrogenic immunosuppression:TIGRA vs TST ?
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

RA Patients Treated with Adalimumab in Taichung Veterans General Hospital, Taiwan
43 patients with active RA were enrolled. n 35 F/8 M, mean age 52.6 ± 10.2 yearsn Prospective cohort study
Medication n low doses of oral prednisolone 5-10 mg dailyn NSAIDsnMethotrexate (MTX) p.o. 12.5-17.5 mg weeklyn No other DMARDs.
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com

Adalimumab12 mns
Patients enrolledN= 43
TST Positive
N=8 (18.6%)
TST Negative
N=35 (81.4%)
No TB (0%)No hepatotoxicity/allergy
Adalimumab 18th mns
2nd TST positive
N=10
2nd TST negative
N=17
Medication: Adalimumab, MTX12.5-17.5/QW, Prednisolone 5-10mg QD
INH Prophylaxis for 9 months
Withdrawal N=6, No TB
Baseline screening: Risk factor survey, History of active TB, CXR (PA view)
Active TB infection
N=2No TB
N=27
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
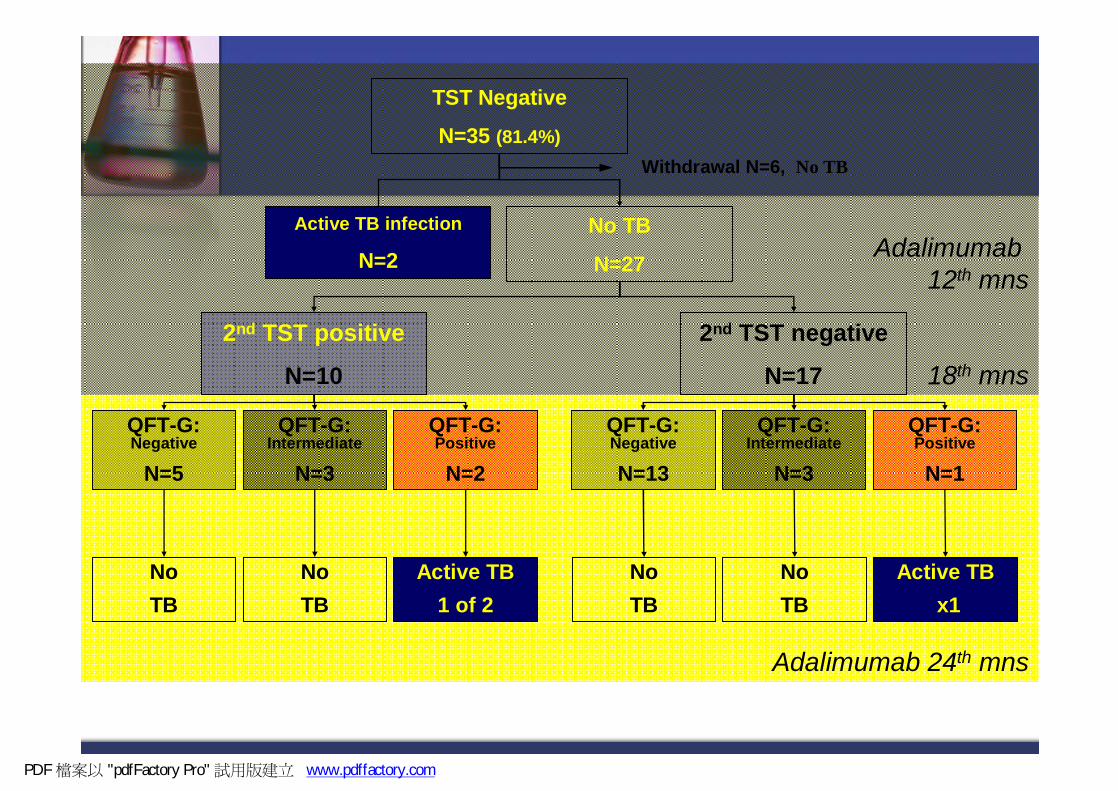
Adalimumab 24th mns
Adalimumab 12th mns
18th mns
TST Negative
N=35 (81.4%)
2nd TST positive
N=10
2nd TST negative
N=17
Withdrawal N=6, No TB
Active TB infection
N=2No TB
N=27
QFT-G: Negative
N=5
QFT-G: Intermediate
N=3
QFT-G: Positive
N=2
QFT-G: Negative
N=13
QFT-G: Intermediate
N=3
QFT-G: Positive
N=1
No TB
No TB
Active TB1 of 2
No TB
No TB
Active TBx1
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Age(years)
Sex UsedTNF-αblocker
TSTresult
CXR Months to active TB
Locationof TB
Concomitmedication
63 F Adalimumab Normal 19 Joint MTX, pred
55 F Adalimumab Normal 10 LN MTX, pred
57 M Adalimumab Normal 12 Pleura MTX, pred
41 M Adalimumab Normal 16 Pleura,LN
MTX, pred
43 F Etanercept ND Normal 11 Pulmon MTX, pred
M: male; F: female; TST: tuberculin skin test; CXR: chest radiograph; MTX: methotrexate; pred: prednisolone 5-10 mg/day; ND: not done
Characteristics of TB cases found in RA patients receiving TNF-αantagonists in Taiwan (VGH-TC)
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com
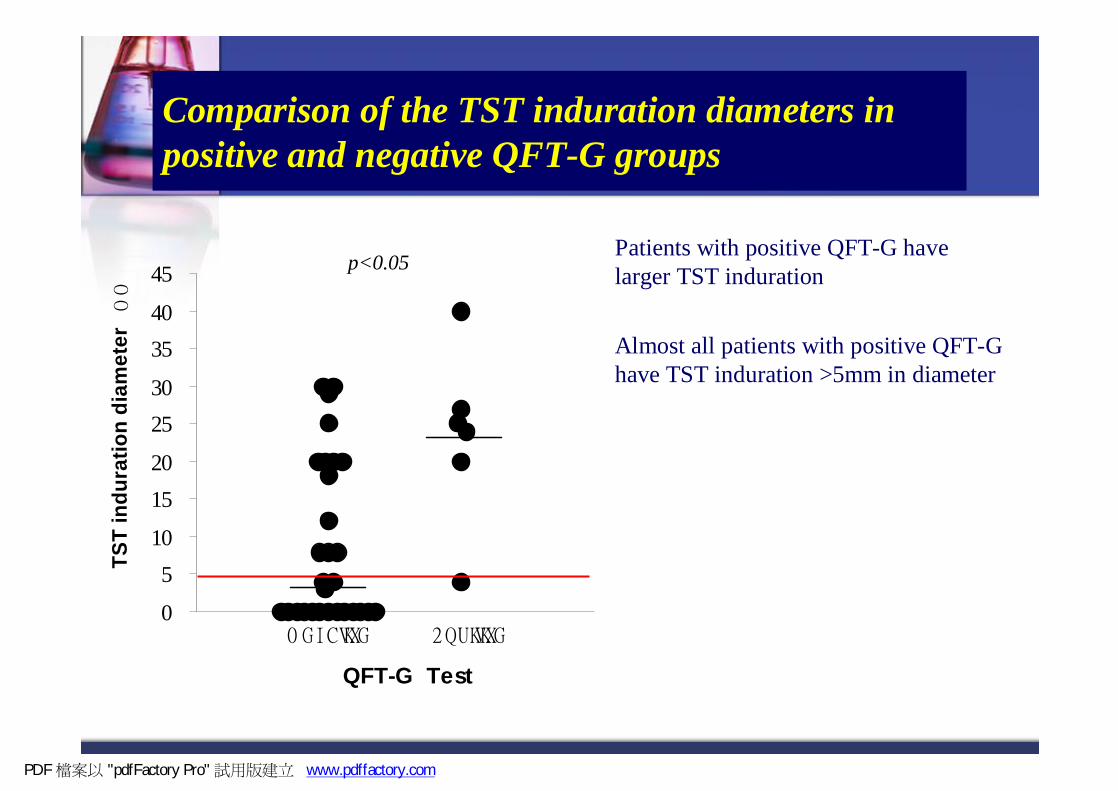
Comparison of the TST induration diameters in positive and negative QFT-G groups
Patients with positive QFT-G have larger TST induration
Almost all patients with positive QFT-G have TST induration >5mm in diameter
0
510
1520
2530
3540
45
p<0.05
QFT-G Test
TST
indu
ratio
n di
amet
er
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Summary
n Traditional (single) TST is lack of enough specifityand sensitivity in detecting LTBI or new TB infection in RA on anti-TNF therapy in Taiwan
n INH therapy is effective and safen Quantiferon-G test correlate better to risk of TB
infectionn Concordance between QFT-G & TST might be
different in CFP-10 & ESAT-6
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

HIV的病患與RA接受anti-TNF-α都可以使用
INH preventive therapy (IPT)來避免病患發病,更不論其他病患
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ f www.pdffactory.com


IS 61 1 0 R FL P
IS6 1 10 R FL P
ESAT6
CFP10
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com

預防結核病前瞻治療(Treatment of LTBI)執行說明
LTBI(treatment of latent tuberculosis infection)潛伏結核感染之治療
DOPT (directly observed preventive therapy) 直接觀察預防治療法
PDF 檔案以 "pdfFactory Pro" 試用版建立 f www.pdffactory.com

預防結核病前瞻治療計畫
依據:傳染病防治法
目的:降低結核菌潛伏感染者發病機率
實施階段及目標
n以對感染後發病機會高、順服度高、藥物成本及安全性高等方向考量
n第一階段(2008年4月1 日起)確診肺結核接觸者12歲(含)以下潛伏感染者
n第二階段:確診肺結核接觸者之HIV(+)、矯正機關及醫護人員之潛伏感染者
n第三階段:確診肺結核接觸者之潛伏感染者全面
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

今年執行目標
n確診肺結核接觸者12歲(含)以下潛伏感染者60%加入LTBI n LTBI治療完成率達75%
PDF 檔案以 "pdfFactory Pro" 試用版建立 ! www.pdffactory.com

預防結核病前瞻治療
對象:
Ø 肺內確診結核病個案之接觸者經檢查為潛伏感染者
Ø 本年第一優先保護對象為等於小於12歲兒童目的:降低結核菌潛伏感染者的發病的機率。
治療:isoniazid 10 mg/kg (最高劑量300 mg),每日服用一次,持續9個月。
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

n指標個案如DST為INH 抗藥,其接觸者則不必再實施預防結核病前瞻治療,若指標個案無INH抗藥,前瞻治療可降低結核菌潛伏感染者九成的發病的機率。
n轉介個案給LTBI合作醫療院所之醫師診治,除了提TB接觸者轉介單內容外,另需提供指標個案之痰檢驗結果,供診治醫師參考。
注意事項
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com
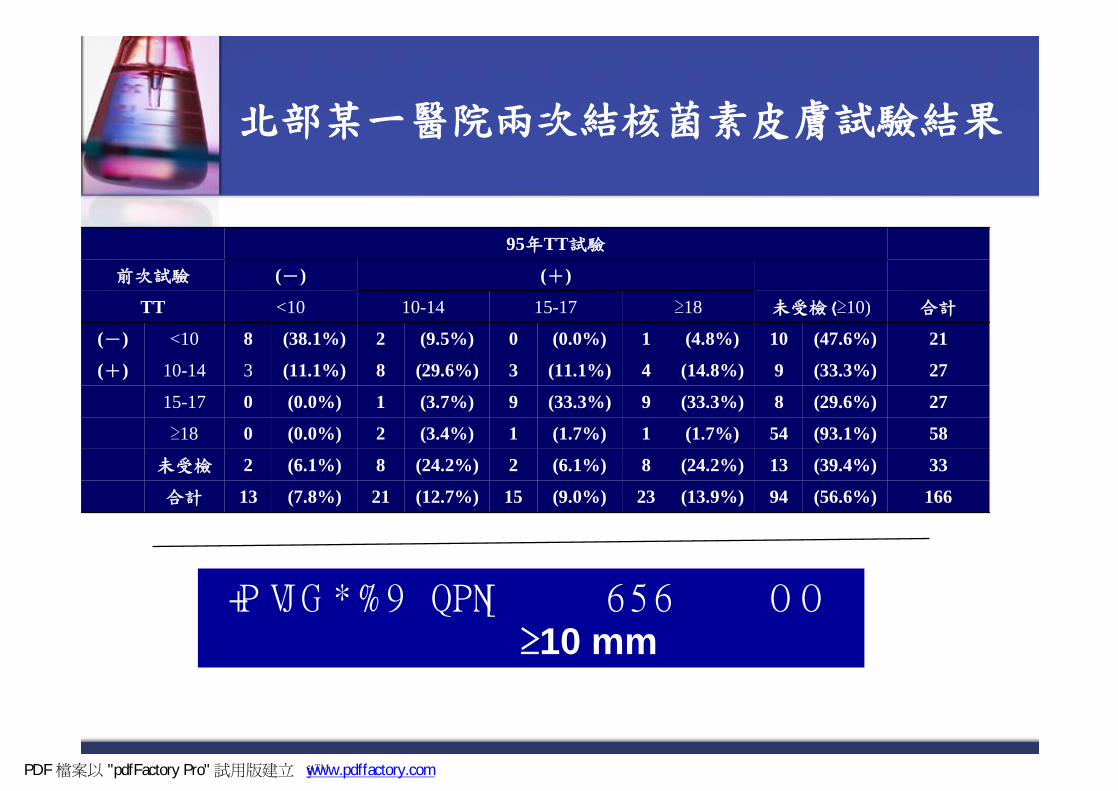
北部某一醫院兩次結核菌素皮膚試驗結果
166(56.6%)94(13.9%)23(9.0%)15(12.7%)21(7.8%)13合計
33(39.4%)13(24.2%)8(6.1%)2(24.2%)8(6.1%)2未受檢
58(93.1%)54(1.7%)1(1.7%)1(3.4%)2(0.0%)0≥18
27(29.6%)8(33.3%)9(33.3%)9(3.7%)1(0.0%)015-17
27(33.3%)9(14.8%)4(11.1%)3(29.6%)8(11.1%)310-14(+)
21(47.6%)10(4.8%)1(0.0%)0(9.5%)2(38.1%)8<10(-)
合計未受檢(≥10)≥1815-1710-14<10TT
(+)(-)前次試驗
95年TT試驗
≥10 mm
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ � www.pdffactory.com
小一,小六不再追加
n民國八十四年九月起,除反應陽性者不接種卡介苗外,凡已有卡介苗疤痕且PPD RT23結核菌素測驗反應硬結在6-9mm者亦不再追加接種卡介苗。
n民國八十六年七月起,依中央防癆委員會決議,停止所有卡介苗追加接種。
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Results:False-positive TST from NTM
Total 3.1%
PDF 檔案以 "pdfFactory Pro" 試用版建立 � www.pdffactory.com

行政院衛生署疾病管制局關心您!
TB接觸者就醫轉介單 *姓名: *身分證字號: 出生: 年 月 日 *住址: 縣市 鄉鎮市區 性別:□男□女 卡介苗疤痕:□有疤□無疤 結核菌素檢查:______mm(檢查日期 ) *指標個案資料(衛生所開立本欄勿填;醫院開立必填): 姓名:____________身分證字號_____________ 開立單位: ______縣_____衛生所 年 月 日(有效期限為一個月) * 醫院 年 月 日(有效期限為一個月) 連絡人: 連絡電話: *醫院檢查結果:
檢查日期 項目 結 果 結核菌素檢查
(第 12個月再進行追蹤者,本項目不需檢查)
mm 12歲
以
下 胸部 X光 □ 正常 疑似肺結核: □無空洞 □有空洞
□ 其他異常,註: 12歲
以
上
胸部 X光 □ 正常 疑似肺結核: □無空洞 □有空洞 □ 其他異常,註:
*建議: 12歲以上: □需進一步轉介給_________醫師診治□其他 12歲以下:□需進一步轉介給____________醫師診治□ 潛伏結核感 染治療 □其他 *醫院名稱: 回覆醫師簽章: 連絡電話: 備註:如檢查結果正常,但卻出現異常呼吸道症狀或咳嗽超過 3週,仍應
儘速就醫檢查,並告知接觸史。
第一聯:醫療院所將轉介單結果黏貼於個案病歷表上;第二聯:醫療院所把結果逕寄所屬衛生局或由個案交回衛生所;第三聯:存根
編號: 年 月;醫療院所代號 流水號
若由醫院端開立轉介單者”*”處為醫院必填之欄位
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ www.pdffactory.com



Patient's delay
Doctor's delay
Transmission
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com

Ferebee SH. Adv Tuberc Res 1969;17:28-106
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ ÿ www.pdffactory.com


12歲以下
n 初次陰性開始治療若3個月後再做陰性則停藥; 如果INDEX CASE的DST為INH R則停藥。(可吃RMP四個月)
n 初次檢查即陽性但因為特殊理由沒有開始做LTBI TX則發病及早就醫的衛教一定要有
n 若為尚未施打BCG的幼兒,則建議在完成治療後再施打BCG。
n 詳細請參考指引Chapter 8
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

管理方式
n 以DOPT方式執行n 居住地衛生所7天內收案管理n 公衛護士訪視頻度:
Ø第1個月:收案時訪1次,1個月內擇期再訪1次。
Ø第2個月至完成管理:每1至2個月訪視。
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

Now a 3-pronged approach to TB control
Summary
PDF 檔案以 "pdfFactory Pro" 試用版建立 ÿ昀ÿ www.pdffactory.com

ELISpot more sensitive than TST for active TB in iatrogenic immunosuppression
不論新舊方法找到LTBI早些加以治療
才是正確之道
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

請支持疾病管制局預防結核病前瞻治療計畫
作業分工
n 醫院
n協助診斷病患LTBIn協助給予病患INH或RMP藥物治療
n 疾管局各分局
n輔導縣巿推動、督導落實執行
n協助協調跨縣巿合作
n 疾管局
n研擬計畫作業標準
n爭取經費資源
n評估成效
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com

請支持疾病管制局預防結核病前瞻治療計畫
作業分工
n 衛生所
n接檢 發現目標 教育
n轉介至指定醫療院所
n執行及追踪管理
n 衛生局
n慎選及開闢合作醫療院所醫師,掌握地方資源
n聯結診療及公衛團隊
n督導執行
PDF 檔案以 "pdfFactory Pro" 試用版建立 www.pdffactory.com
