zydelig accessconnect™ patient enrollment form · preferred sp: avella biologics diplomat onco360...
TRANSCRIPT
Patient Signature:
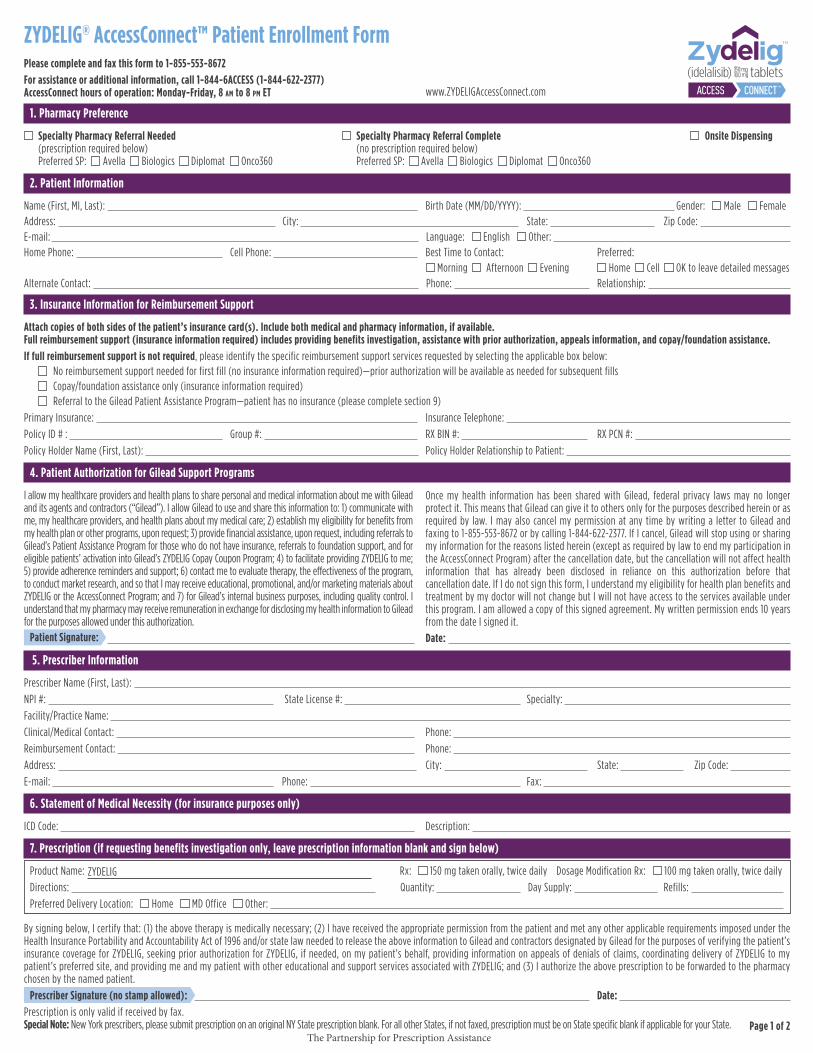
1. Pharmacy Preference
Specialty Pharmacy Referral Needed Specialty Pharmacy Referral Complete Onsite Dispensing (prescription required below) (no prescription required below) Preferred SP: Avella Biologics Diplomat Onco360 Preferred SP: Avella Biologics Diplomat Onco360
2. Patient Information
Name (First, MI, Last): Birth Date (MM/DD/YYYY): Gender: Male FemaleAddress: City: State: Zip Code: E-mail: Language: English Other: Home Phone: Cell Phone: Best Time to Contact: Preferred:
Morning Afternoon Evening Home Cell OK to leave detailed messagesAlternate Contact: Phone: Relationship:
3. Insurance Information for Reimbursement Support
Attach copies of both sides of the patient’s insurance card(s). Include both medical and pharmacy information, if available. Full reimbursement support (insurance information required) includes providing benefits investigation, assistance with prior authorization, appeals information, and copay/foundation assistance. If full reimbursement support is not required, please identify the specific reimbursement support services requested by selecting the applicable box below:
No reimbursement support needed for first fill (no insurance information required)—prior authorization will be available as needed for subsequent fillsCopay/foundation assistance only (insurance information required) Referral to the Gilead Patient Assistance Program—patient has no insurance (please complete section 9)
Primary Insurance: Insurance Telephone: Policy ID # : Group #: RX BIN #: RX PCN #: Policy Holder Name (First, Last): Policy Holder Relationship to Patient:
4. Patient Authorization for Gilead Support Programs
I allow my healthcare providers and health plans to share personal and medical information about me with Gilead and its agents and contractors (“Gilead”). I allow Gilead to use and share this information to: 1) communicate with me, my healthcare providers, and health plans about my medical care; 2) establish my eligibility for benefits from my health plan or other programs, upon request; 3) provide financial assistance, upon request, including referrals to Gilead’s Patient Assistance Program for those who do not have insurance, referrals to foundation support, and for eligible patients’ activation into Gilead’s ZYDELIG Copay Coupon Program; 4) to facilitate providing ZYDELIG to me; 5) provide adherence reminders and support; 6) contact me to evaluate therapy, the effectiveness of the program, to conduct market research, and so that I may receive educational, promotional, and/or marketing materials about ZYDELIG or the AccessConnect Program; and 7) for Gilead’s internal business purposes, including quality control. I understand that my pharmacy may receive remuneration in exchange for disclosing my health information to Gilead for the purposes allowed under this authorization.
Date:
5. Prescriber Information
Prescriber Name (First, Last): NPI #: State License #: Specialty: Facility/Practice Name: Clinical/Medical Contact: Phone: Reimbursement Contact: Phone: Address: City: State: Zip Code: E-mail: Phone: Fax:
6. Statement of Medical Necessity (for insurance purposes only)
ICD Code: Description:
7. Prescription (if requesting benefits investigation only, leave prescription information blank and sign below)
Product Name: Rx: 150 mg taken orally, twice daily Dosage Modification Rx: 100 mg taken orally, twice dailyDirections: Quantity: Day Supply: Refills: Preferred Delivery Location: Home MD Office Other:
By signing below, I certify that: (1) the above therapy is medically necessary; (2) I have received the appropriate permission from the patient and met any other applicable requirements imposed under the Health Insurance Portability and Accountability Act of 1996 and/or state law needed to release the above information to Gilead and contractors designated by Gilead for the purposes of verifying the patient’s insurance coverage for ZYDELIG, seeking prior authorization for ZYDELIG, if needed, on my patient’s behalf, providing information on appeals of denials of claims, coordinating delivery of ZYDELIG to my patient’s preferred site, and providing me and my patient with other educational and support services associated with ZYDELIG; and (3) I authorize the above prescription to be forwarded to the pharmacy chosen by the named patient.
Prescriber Signature (no stamp allowed): Date: Prescription is only valid if received by fax. Special Note: New York prescribers, please submit prescription on an original NY State prescription blank. For all other States, if not faxed, prescription must be on State specific blank if applicable for your State.
ZYDELIG® AccessConnect™ Patient Enrollment FormPlease complete and fax this form to 1-855-553-8672 For assistance or additional information, call 1-844-6ACCESS (1-844-622-2377) AccessConnect hours of operation: Monday-Friday, 8 am to 8 pm ET
Once my health information has been shared with Gilead, federal privacy laws may no longer protect it. This means that Gilead can give it to others only for the purposes described herein or as required by law. I may also cancel my permission at any time by writing a letter to Gilead and faxing to 1-855-553-8672 or by calling 1-844-622-2377. If I cancel, Gilead will stop using or sharing my information for the reasons listed herein (except as required by law to end my participation in the AccessConnect Program) after the cancellation date, but the cancellation will not affect health information that has already been disclosed in reliance on this authorization before that cancellation date. If I do not sign this form, I understand my eligibility for health plan benefits and treatment by my doctor will not change but I will not have access to the services available under this program. I am allowed a copy of this signed agreement. My written permission ends 10 years from the date I signed it.
www.ZYDELIGAccessConnect.com
Page 1 of 2
ZYDELIG
The Partnership for Prescription Assistance

1. Pharmacy Preference• Select “Specialty Pharmacy Referral Needed” if the patient will be receiving ZYDELIG from a Specialty Pharmacy that has NOT already received the patient’s ZYDELIG prescription. If a specific
Specialty Pharmacy is preferred, note the preference• Select “Specialty Pharmacy Referral Complete” if a pharmacy has already received the patient’s ZYDELIG prescription, and note the name of that Specialty Pharmacy• Select “Onsite Dispensing” if your clinic or onsite pharmacy will be dispensing ZYDELIG to the patient
2. Patient Information• Please include all available contact information for the patient including an alternate contact and the alternate contact’s preferred phone number
3. Insurance Information for Medical and Pharmacy Benefits (Attach a copy, front and back, of patient insurance card[s])• Select level of reimbursement support needed for the patient. If no option is selected, full reimbursement support will be provided including benefits investigation, prior authorization support,
appeals information, and copay/foundation assistance• Fill out this section for all forms of the patient’s insurance coverage or fax copies (front and back) of the patient’s insurance card(s) (may be 1 or more cards for both the patient’s medical and
pharmacy benefits) to 1-855-553-8672• If patient has no insurance, complete section 9 and fax both pages of enrollment form to 1-855-553-8672
4. Patient Authorization• Patient signature and date required for all services
5. Prescriber Information• Provide prescriber NPI and state license information• Include contact information for both clinical and reimbursement contacts in the prescriber’s office
6. Statement of Medical Necessity• Complete with appropriate ICD code and matching description
7. Prescription• Fully complete all areas of the prescription section of the form
Prescriber Signature• Prescriber signature and date required for reimbursement support, free goods programs, and prescriptions
8. QuickStart Opt-in—OPTIONAL (page 2)• Select if you would like your patient to receive a free 30-day QuickStart supply, if the patient experiences an insurance-related delay of greater than 5 business days. For ZYDELIG
Terms and Conditions, see page 2 of the ZYDELIG AccessConnect Patient Enrollment Form• Patient signature and Prescriber signature required on both page 1 and page 2 of the ZYDELIG AccessConnect Patient Enrollment Form to be enrolled in the QuickStart Program
9. Patient Assistance Program (PAP) Application—OPTIONAL (page 2)• For patients without insurance, complete household income information• Patient signature and Prescriber signature required on both page 1 and page 2 of the ZYDELIG AccessConnect Patient Enrollment Form to receive free product through the Patient Assistance Program
Fax enrollment form and copies of ALL patient medical and pharmacy insurance to ZYDELIG AccessConnect at 1-855-553-8672.For questions, contact ZYDELIG AccessConnect at 1-844-6ACCESS (1-844-622-2377).
ZYDELIG® AccessConnect™ Patient Enrollment Form Instructions
© 2014 Gilead Sciences, Inc. All rights reserved. GILP0224 07/2014 Gilead, the Gilead logo, ZYDELIG, and AccessConnect are trademarks of Gilead Sciences, Inc., or one of its related companies.
The Partnership for Prescription Assistance

Patient Signature:
Patient Signature:
ZYDELIG
60 tablets 30 days
Name (First, MI, Last): Birth Date (MM/DD/YYYY):
8. OPTIONAL—QuickStart Prescription Program
Complete this additional ZYDELIG QuickStart prescription for patients who experience insurance delays. ZYDELIG QuickStart Prescription Program can provide these patients with a one-time, 30-day supply of medication, free of cost. Terms and Conditions apply.*
Product Name: Rx: 150 mg taken orally, twice dailyDirections: Quantity: Day Supply: Preferred Delivery Location: Home MD Office Other:
* The QuickStart Program provides eligible patients with 1 free bottle that includes a 30-day supply of ZYDELIG 150 mg tablets. There is no purchase obligation by virtue of a patient’s participation in the QuickStart Program. A minimum 5-business-day insurance verification period is required for patients to be eligible for the QuickStart Program. Patients must have an on-label prescription for ZYDELIG, consistent with the FDA-approved label for ZYDELIG, and be enrolled in the ZYDELIG AccessConnect Program to qualify. Free product for the QuickStart Program will only be available through the QuickStart Specialty Pharmacy. Patients receiving free product under the QuickStart Program may not seek reimbursement or credit for this prescription from any insurer, health plan, or government program. For any patient that is a member of a Medicare Part D plan, this prescription, or any cost associated with it, may not be counted as part of their out-of-pocket cost for prescription drugs. An extension period beyond the initial 30-day supply is limited to commercially insured patients and individual approval is required.
By signing below, if I receive free product through the QuickStart Program, I certify that I will not seek reimbursement or credit for this prescription from any insurer, health plan, or government program. If I am a member of a Medicare Part D plan, I will not seek to have this prescription or any cost associated with it counted as part of my out-of-pocket cost for prescription drugs.
Date:
By signing below, I certify that this prescription is on label and the patient has not yet started ZYDELIG treatment. I read and understand the QuickStart Program terms and conditions and I agree that I shall not seek reimbursement for any Gilead medication dispensed to the patient through the QuickStart Program from any government program or third-party insurer.
Prescriber Signature (no stamp allowed): Date:
Prescription is only valid if received by fax.Special Note: New York prescribers, please submit prescription on an original NY State prescription blank. For all other States, if not faxed, prescription must be on State specific blank if applicable for your State.
9. OPTIONAL—Patient Assistance Program (PAP) Application
Phone Number: 1-855-536-7102 Fax Number: 1-855-850-3007
Current Annual Household Income: $ Number of persons in household: 1 2 3 4 5 6
(Please submit current documentation for all sources of income and proof of US Residency.)
Social Security Number:
I certify that all of the information provided in this application, including household income, is complete and accurate. I understand that program assistance will terminate if the program becomes aware of any fraud or if this medication is no longer prescribed for me. I understand that completing this application does not ensure that I will qualify for patient assistance. If I receive free product through the PAP, I certify that I will not seek reimbursement or credit for this prescription from any insurer, health plan, or government program. If I am a member of a Medicare Part D plan, I will not seek to have this prescription or any cost associated with it counted as part of my out-of-pocket cost for prescription drugs. I understand that the PAP reserves the right to modify the application form, modify or discontinue this program, or terminate assistance at any time and without notice. I authorize the PAP and its administrator to forward this prescription to a dispensing pharmacy on my behalf.
Date:
By signing this form, I certify that I am prescribing Gilead medication for the patient identified in Section 2, and I certify that this prescription medication is medically indicated for the patient and that it will be used as directed. I certify that I will be supervising the patient’s treatments and verify that the information provided is complete and accurate to the best of my knowledge. I agree that I shall not seek reimbursement for any Gilead medication dispensed to the patient through the Patient Assistance Program (PAP) from any government program or third-party insurer.
Prescriber Signature (no stamp allowed): Date:
© 2014 Gilead Sciences, Inc. All rights reserved. GILP0224 07/2014 Gilead, the Gilead logo, ZYDELIG, and AccessConnect are trademarks of Gilead Sciences, Inc., or one of its related companies. Page 2 of 2
ZYDELIG® AccessConnect™ Patient Enrollment FormPlease complete and fax this form to 1-855-553-8672 For assistance or additional information, call 1-844-6ACCESS (1-844-622-2377) AccessConnect hours of operation: Monday-Friday, 8 am to 8 pm ET www.ZYDELIGAccessConnect.com
x
The Partnership for Prescription Assistance