wound assessment, documentation & types of dressing · wound assessment, documentation &...
TRANSCRIPT
WOUND ASSESSMENT, DOCUMENTATION & TYPES OF DRESSING
ABDUL MANAN BIN OTHMAN BSc (Hons) NPD Northumbria, UK
Assistant Medical Officer
Champion Wound Care Unit
Kota Tinggi District Health Office
email: [email protected]
WHAT…..WHEN WHO…WHERE…
HOW..

Wound bed preparation
Care Cycle
Start with the patient
Identifying wound
aetiology
Perform TIME assessment
Agree goals
Treat & evaluate
TIME interventions
Healed
GOAL IN WOUND CARE CYCLE
No
Yes Prevention
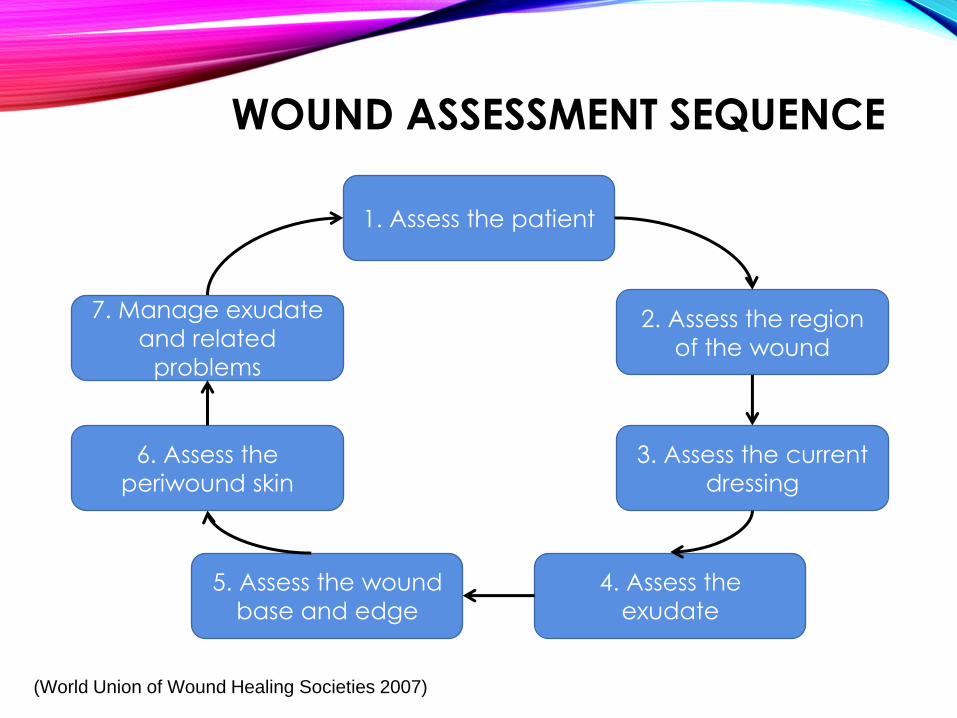
WOUND ASSESSMENT SEQUENCE
1. Assess the patient
2. Assess the region
of the wound
3. Assess the current
dressing
4. Assess the
exudate
5. Assess the wound
base and edge
6. Assess the
periwound skin
7. Manage exudate
and related
problems
(World Union of Wound Healing Societies 2007)
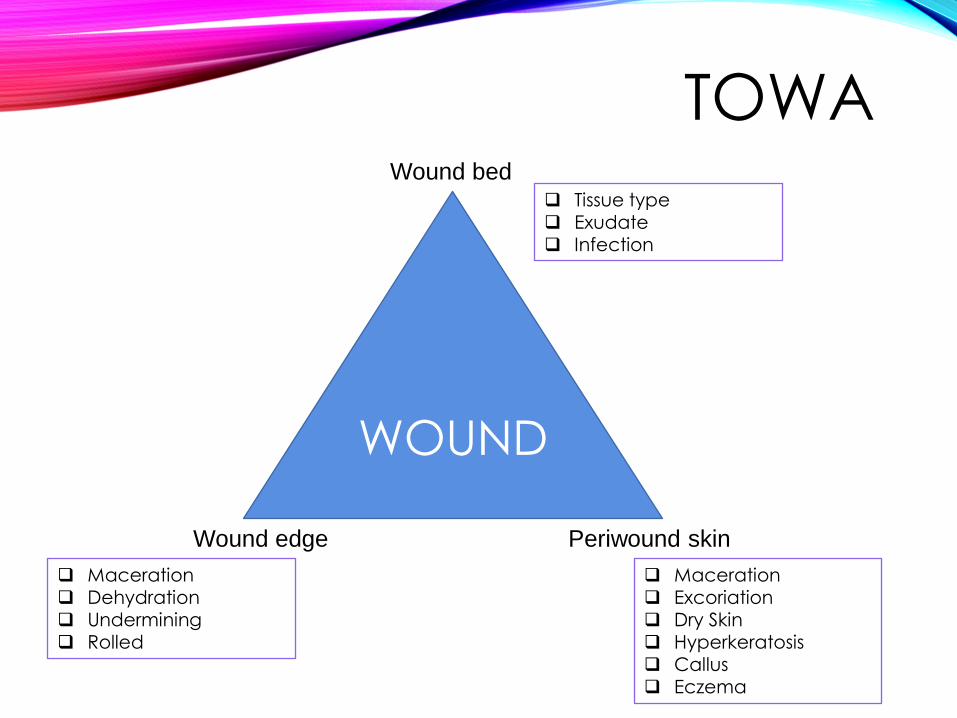
TOWA
WOUND
Wound bed
Wound edge Periwound skin
Tissue type
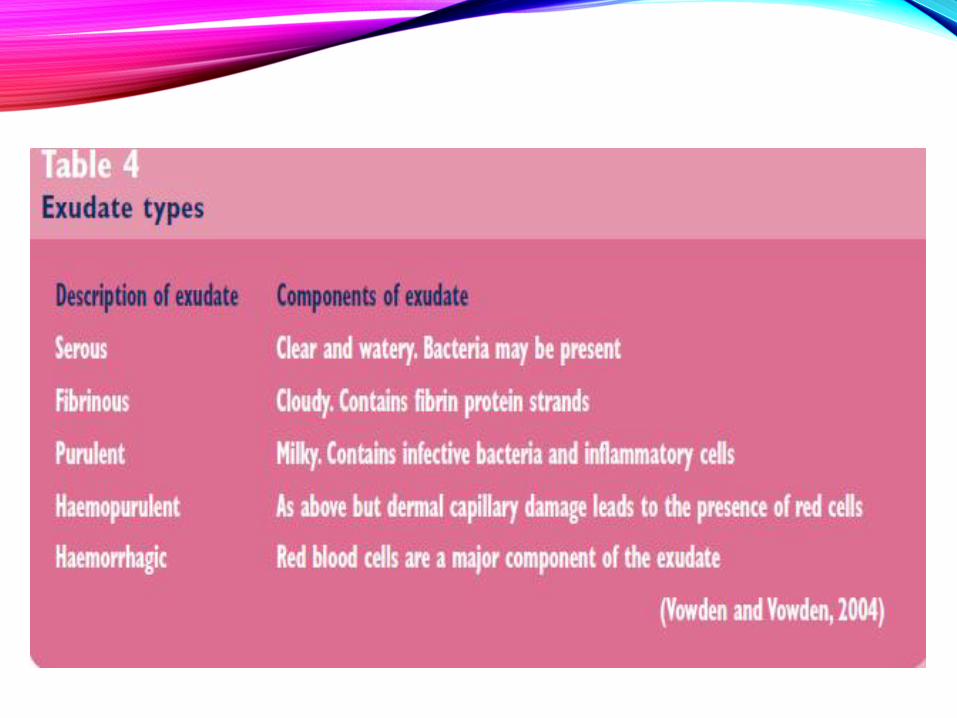
Exudate Infection
Maceration Excoriation Dry Skin
Hyperkeratosis Callus Eczema
Maceration Dehydration Undermining
Rolled
OUTLINE
•Wound assessment
•Wound cleansing
•Types of wound dressing
•Types of debridement
•Putting in together (Algorithm)
•Practise cases
WOUND ASSESSMENT
• Age (extreme of age)
• Disease and co-morbid (DM,
malignancy)
• Obesity
• Medication (steroid,
chemotherapy)
• Nutrition
• Impaired blood supply
(arterial and venous ulcer)
• Lifestyle (smoking)
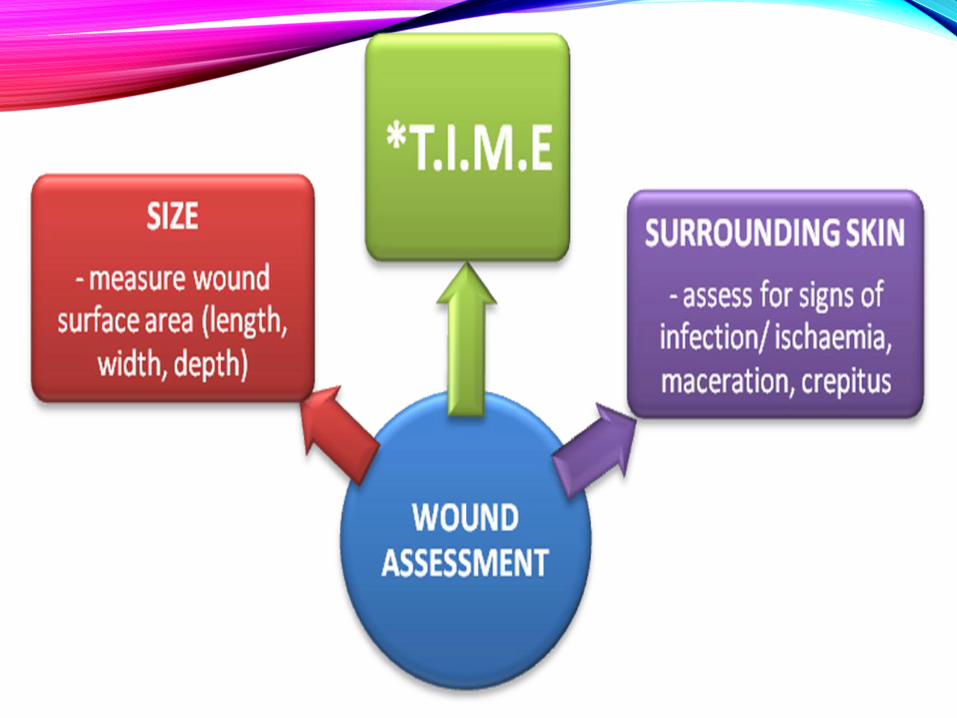
T.I.M.E • A tool during wound assessment to
identify barriers to healing
• Implement a plan to remove barriers and promote healing
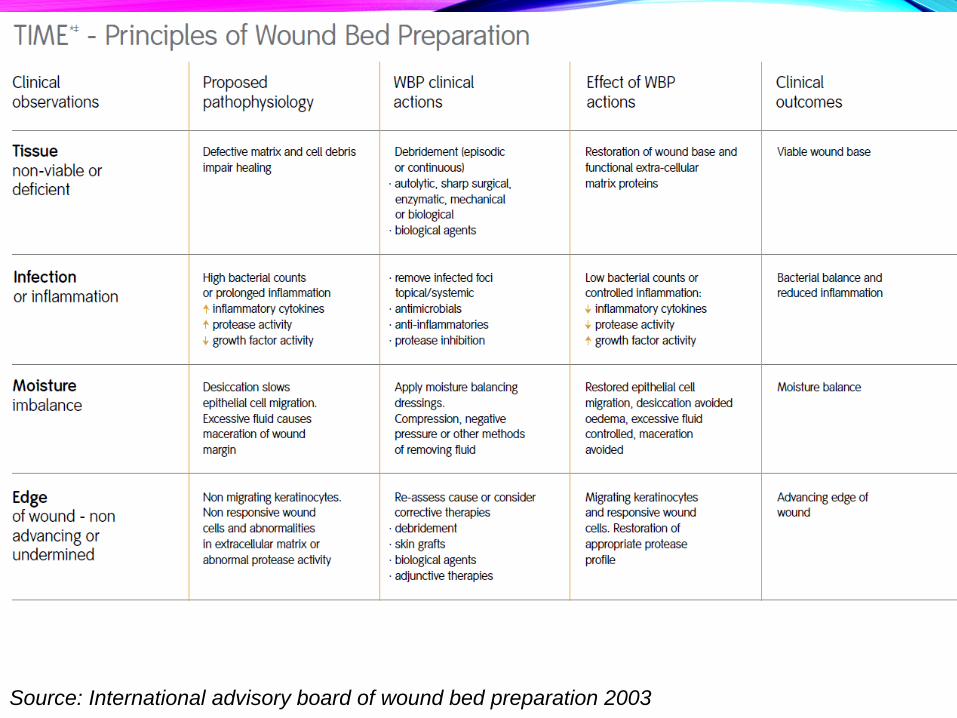
T.I.M.E 4 main components of wound bed
preparation:
1) Tissue Management
2) Control of Infection & Inflammation
3) Moisture Imbalance
4) Advancement of Epithelial Edge of the wound
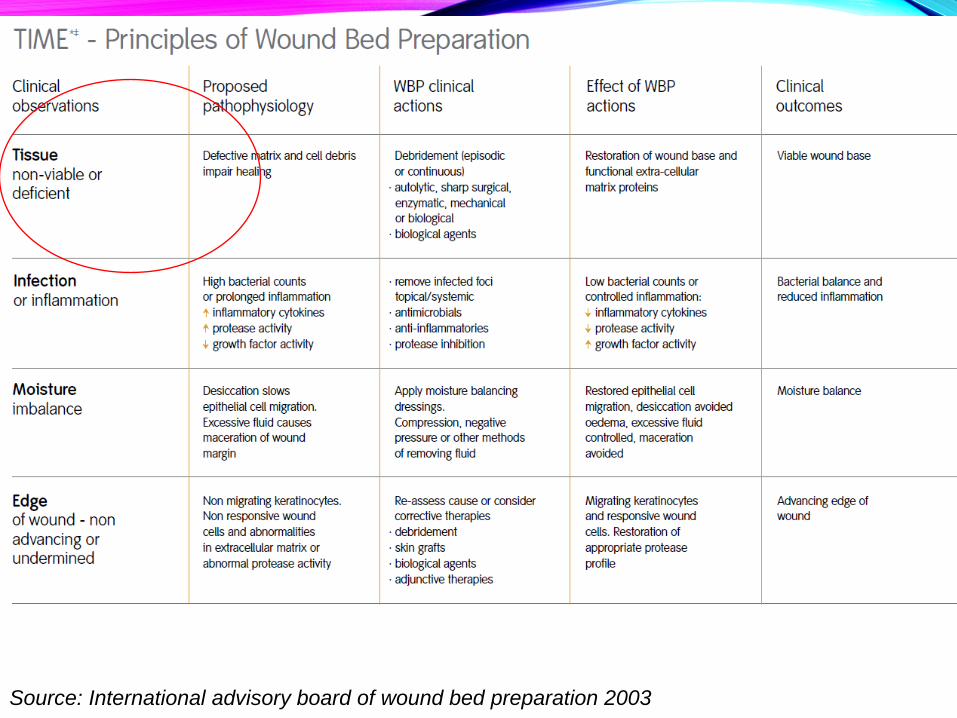
Source: International advisory board of wound bed preparation 2003
1) TISSUE MANAGEMENT
• Pathology : defective matrix, non-viable tissue and cell debris impairs healing
• Plan: Episodic or continuous debridement
• Effect of actions: restoration of wound base and functional extracellular matrix proteins (chronic ->acute wound)
• Clinical outcomes : Viable wound base
HOW TO IDENTIFIED VIABLE/ NON VIABLE
•4C FORMULA
-COLOUR
-CONSISTENCY
-CONTRACTION
-CIRCULATION
•non viable muscle/ tissue can be identified by its dark color, its mushy consistency, its failure to contract when pinched with forceps, and the absence of bleeding from a cut surface

2) CONTROL OF INFECTION & INFLAMMATION
• Pathology : high bacterial count/prolonged inflammation -> ↑ cytokines & protease activity, ↓ growth factor activity
• Plan: -remove foci of infection (local/systemic)
- antimicrobials/antiinflammatory
• Effect of actions: low bacterial count & controlled inflammation
• Clinical outcomes : bacterial balance and reduced inflammation

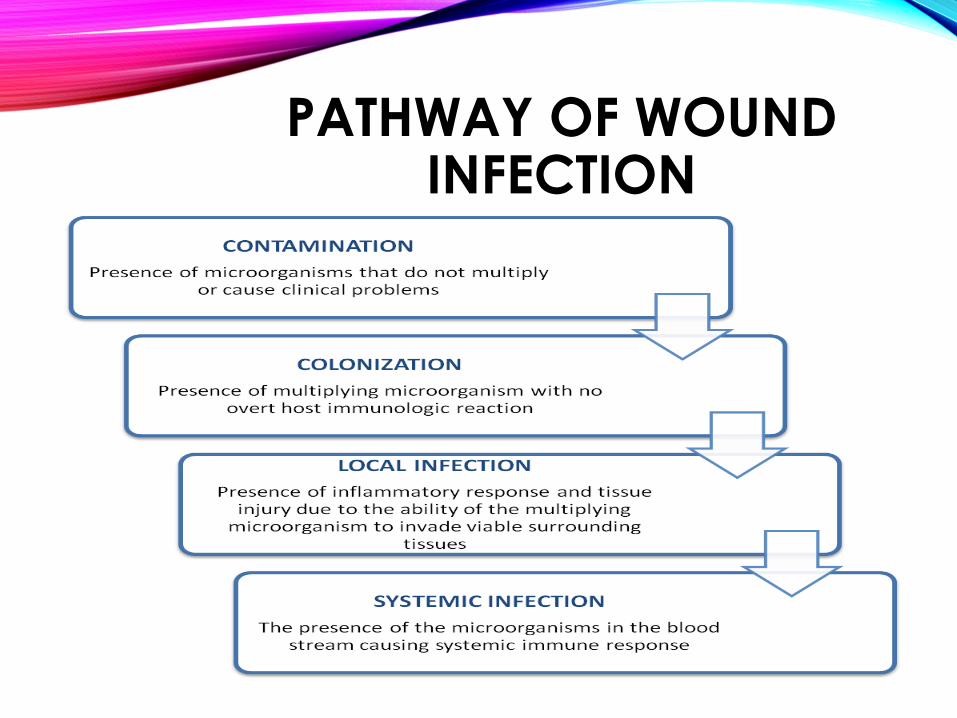
PATHWAY OF WOUND INFECTION
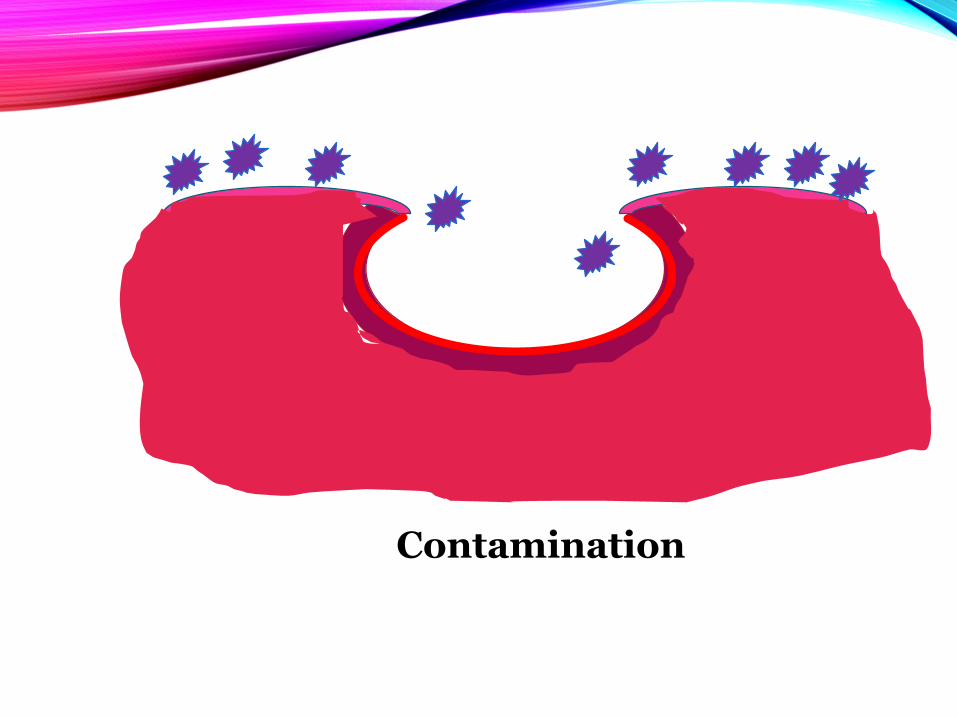
Contamination
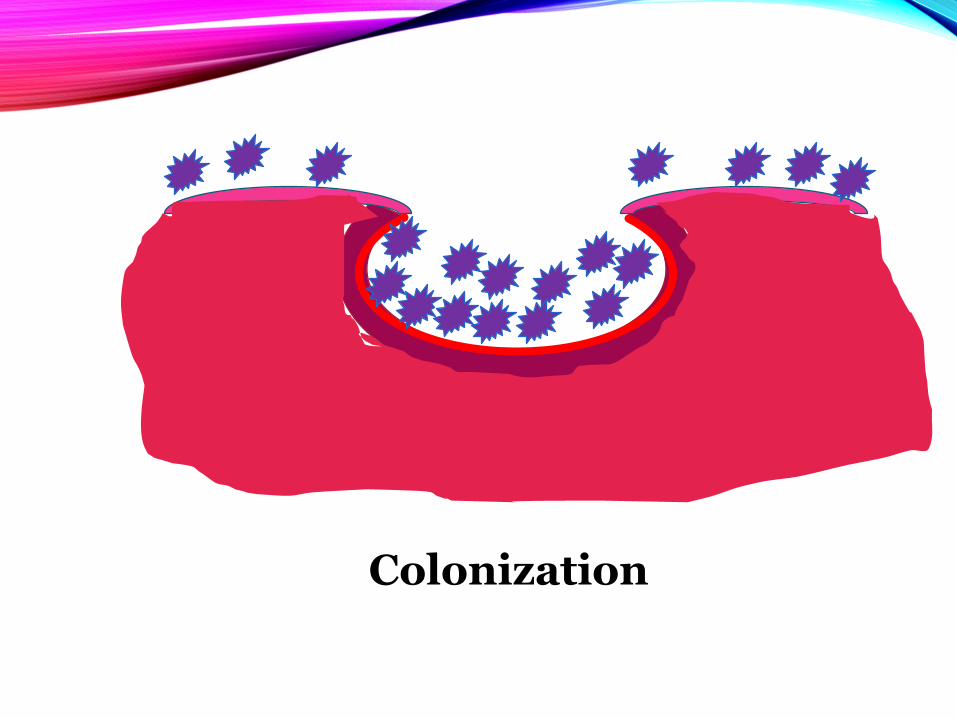
Colonization
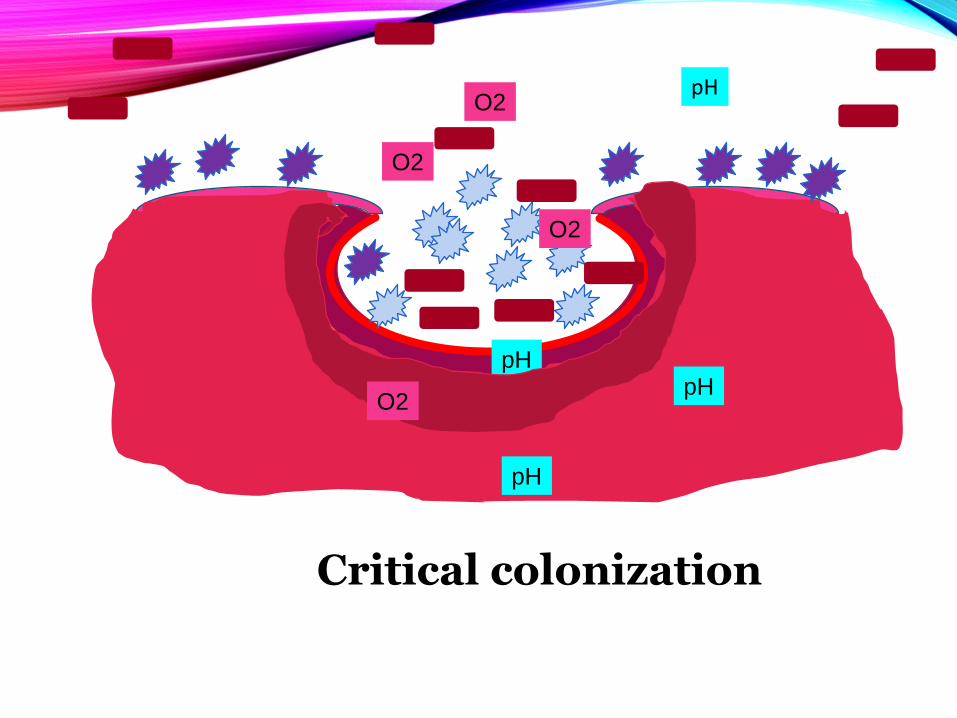
O2
O2
O2
pH
pH pH
pH
O2
Critical colonization
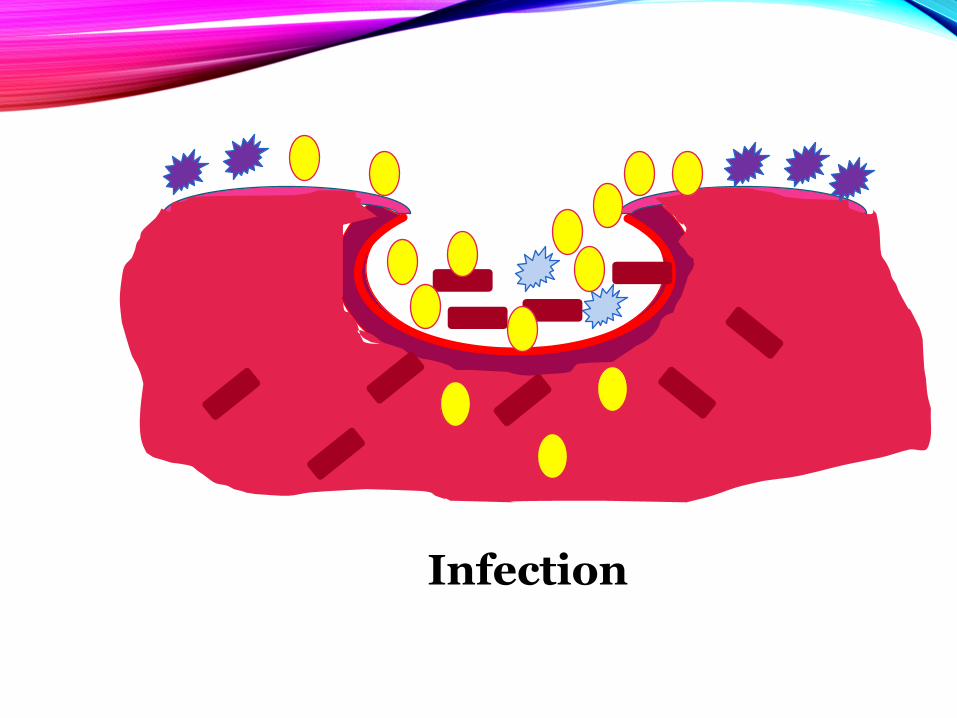
Infection
BIOFILM • Community of microorganisms encased
within an extracellular polymeric matrix, which accumulates at a surface.
• It has been estimated that biofilms are associated with 65 percent of nosocomial infections.
• Play a significant role in a large number of infections in humans.
• due to the intrinsic resistance of these structures to antimicrobial agents and host defense mechanisms, wound with biofilm cannot be treated effectively with antibiotic.
3) MOISTURE IMBALANCE
• Pathology: dessication & excessive fluid- slows epithelial migration and margin maceration
• Plan: moisture balance dressing, compression , negative pressure dressing.
• Effect of actions: restored epithelial migration and avoidance of maceration
• Clinical outcomes : moisture balanced for wound healing

4) ADVANCEMENT OF EPITHELIAL
EDGE OF THE WOUND
• Pathology : non-migrating keratinocytes, non responsive wound cells, abnormal protease activity and ECM
• Plan: reassess cause (T.I.M, extrinsic factor) and consider; debridement, skin grafts, biologic agent
• Effect of actions: migrating keratinocytes and responsive wound cells
• Clinical outcomes :advancing epithelial edge

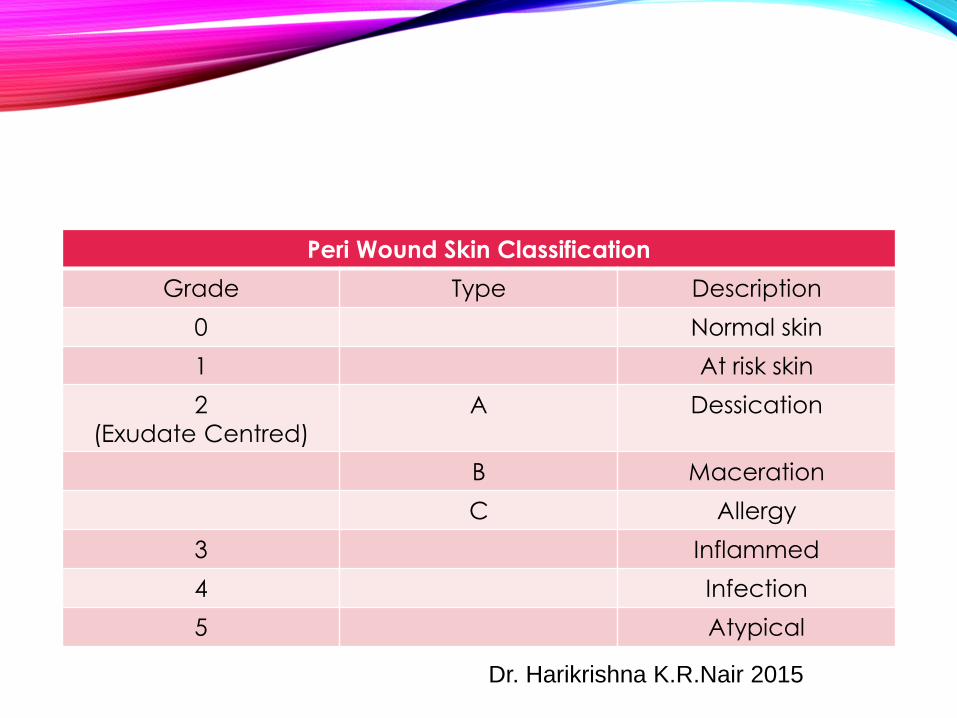
Peri Wound Skin Classification
Grade Type Description
0 Normal skin
1 At risk skin
2
(Exudate Centred)
A Dessication
B Maceration
C Allergy
3 Inflammed
4 Infection
5 Atypical
Dr. Harikrishna K.R.Nair 2015
Source: International advisory board of wound bed preparation 2003
WOUND COLOUR MODEL
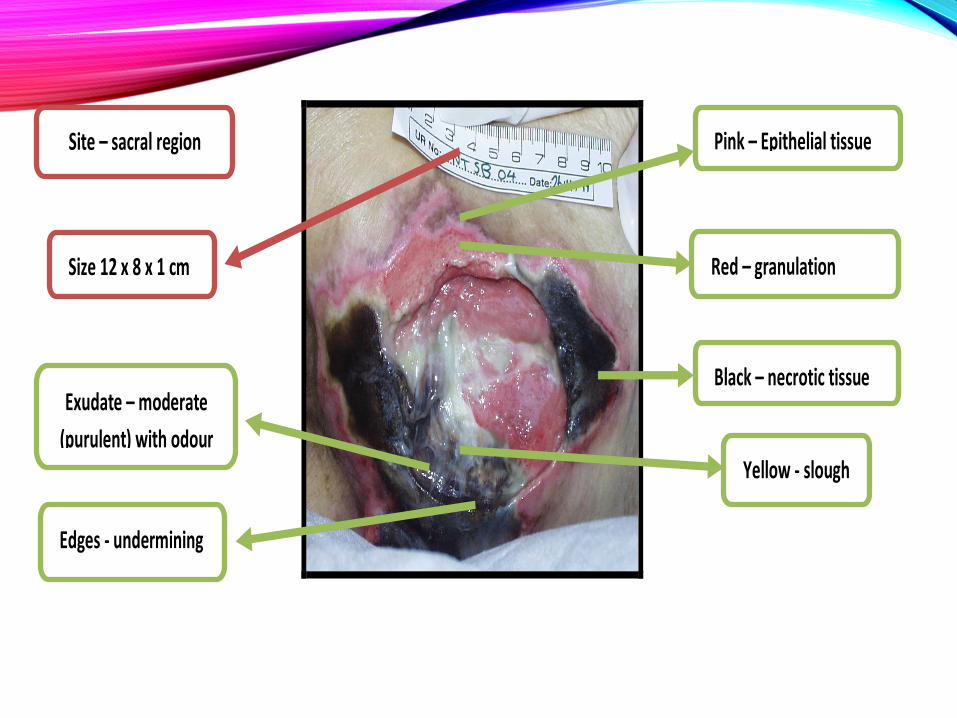
Black – necrotic tissue
Red – granulation
tissue
Yellow - slough
Exudate – moderate
(purulent) with odour
Pink – Epithelial tissue
Edges - undermining
Size 12 x 8 x 1 cm
Site – sacral region
OUTLINE
•Wound classification
•Wound assessment
•Wound cleansing solution
•Wound dressing material
•Putting in together (Algorithm)
•Practise cases

WOUND DRESSING SOLUTIONS
•Non Antiseptic Solutions
•Antiseptic Solutions
• Wound cleansing is a process of removing inflammatory contaminants from the wound surface
• These contaminants can impede healing and increase risk of infection
• The contaminants are:
Necrotic tissues
Excess exudates
Foreign objects
Infected tissues
NON-ANTISEPTIC SOLUTIONS
• Commonly used non-antiseptic solutions are:
Normal Saline
Water for irrigation
Normal Saline
• Preferred cleanser for most types of wounds (physiologic and safe).
• Less effective in dirty and necrotic wounds.
• Not advisable in MRSA and Pseudomonas infected wound.
(peter et al 2008)
• Once the container is opened, it should be used within 24 hours.
Water for irrigation
• Less physiologic compared to normal saline but still safe to be used.
• Can be used in MRSA and Pseudomonas infected wounds.
ANTISEPTIC SOLUTIONS
• Antiseptic solutions are used to clean the wound which are dirty and infected.
• Commonly used antiseptic solutions are:
Chlorhexidine gluconate 1:200 in Aqueous solution
Super-oxidized solution
Polyhexamethylene biguanide (PHMB) solution
Chlorhexidine gluconate 1:200 in Aqueous solution
• Effective against Gram positive bacteria, fungi and also enveloped viruses.
• Less effective against Gram negative bacteria.
• Has both bactericidal and bacterostatic action.
• Readily available in healthcare setting.
Super-oxidized solution
• Good bactericidal, virucidal, fungicidal and spongicidal.
• Also blocks the inflammatory process.
• May help in biofilm removal.
• Two components in this solution are oxidized water and chlorine.
• The oxidized water is broken down into oxygen, ozone and other oxidized species.
• Costly.
Polyhexamethylene biguanide (PHMB) solution
• Helps to soften and remove the slough.
• It can remove and reduce the biofilm formation.
• Less painful.
• Costly.
• These solutions besides painful on application also cause harm to the normal tissues if used as dressing solutions (cytotoxic), however a short term use may be permissible
Povidone iodine
Hydrogen peroxide
Sodium hypochlorite
Acetic acid
Eusol
OUTLINE
• Wound classification
• Wound assessment
• Wound cleansing
• Types of wound dressing material
• Putting in together (Algorithm)
• Practise cases
Types of wound dressing material
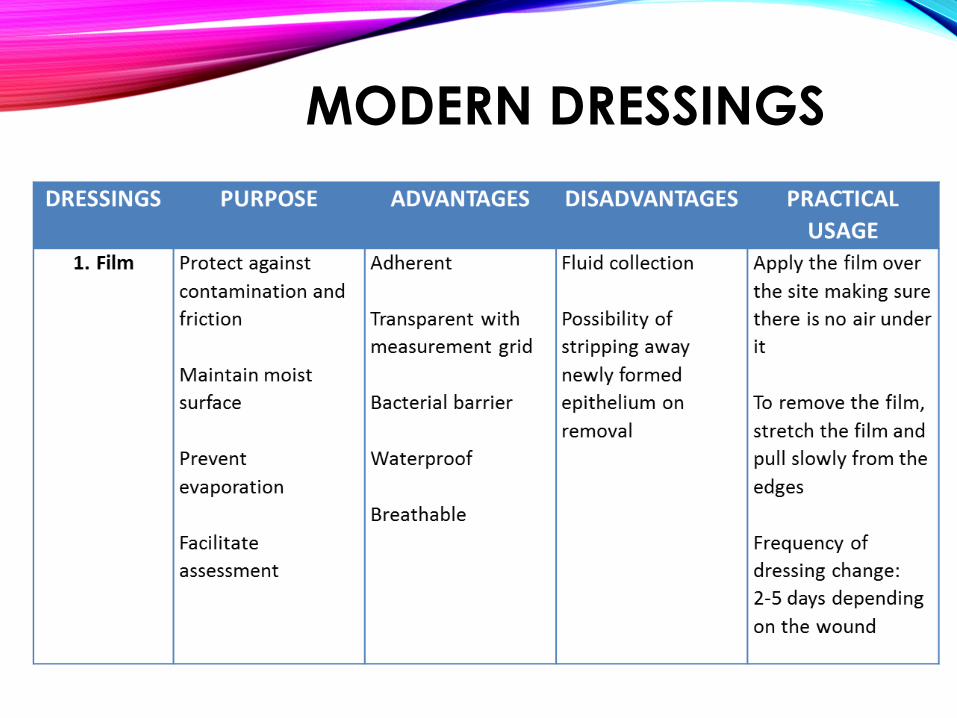
MODERN DRESSINGS

FILM
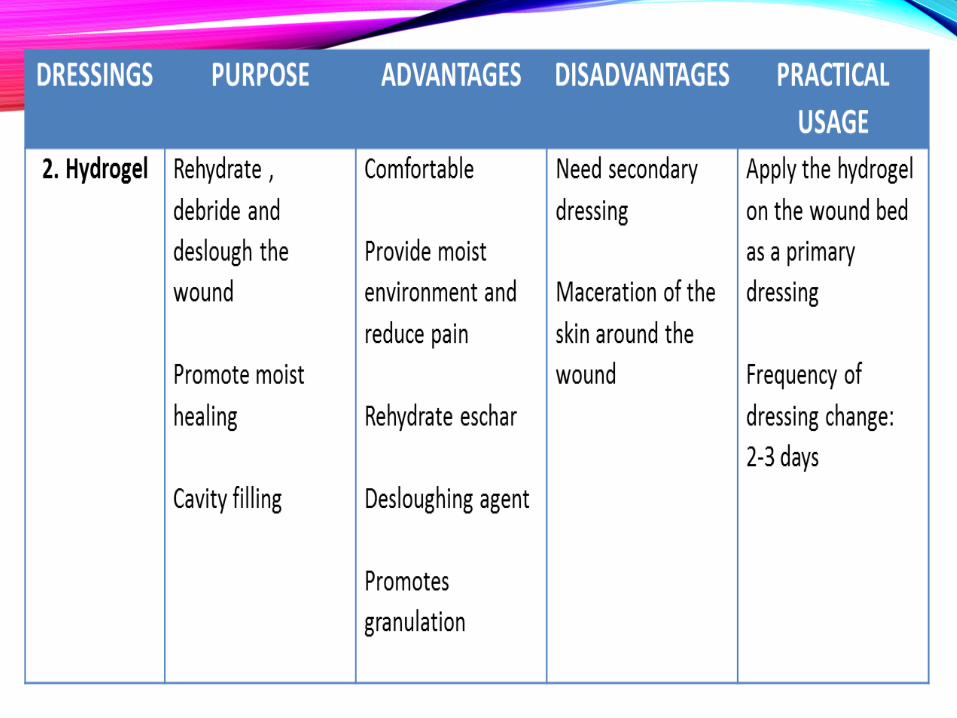

HYDROGEL
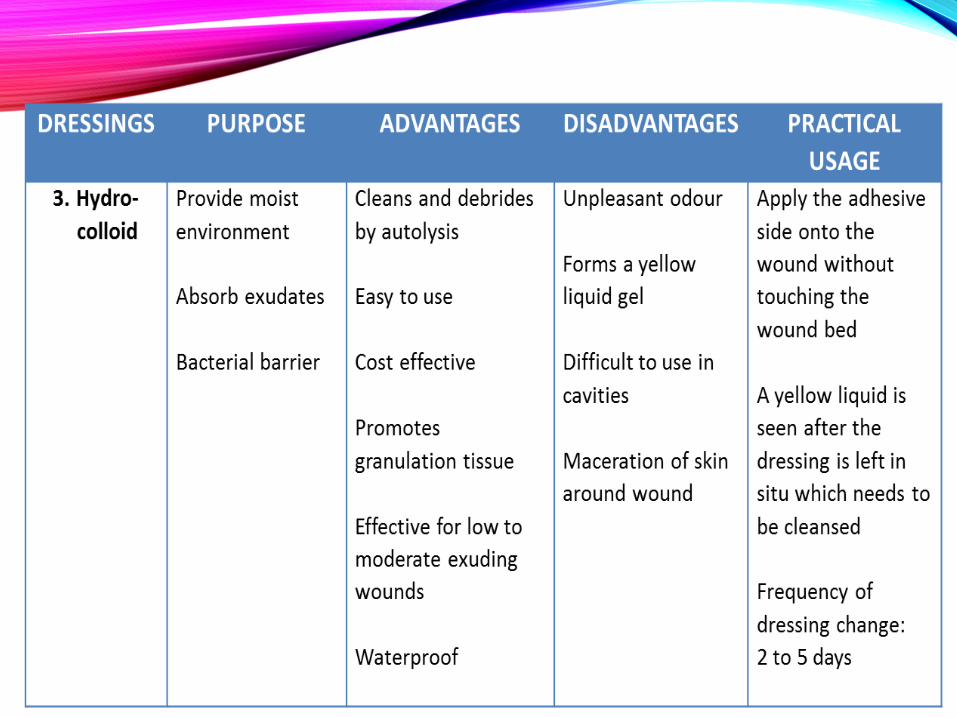

HYDROCOLLOID
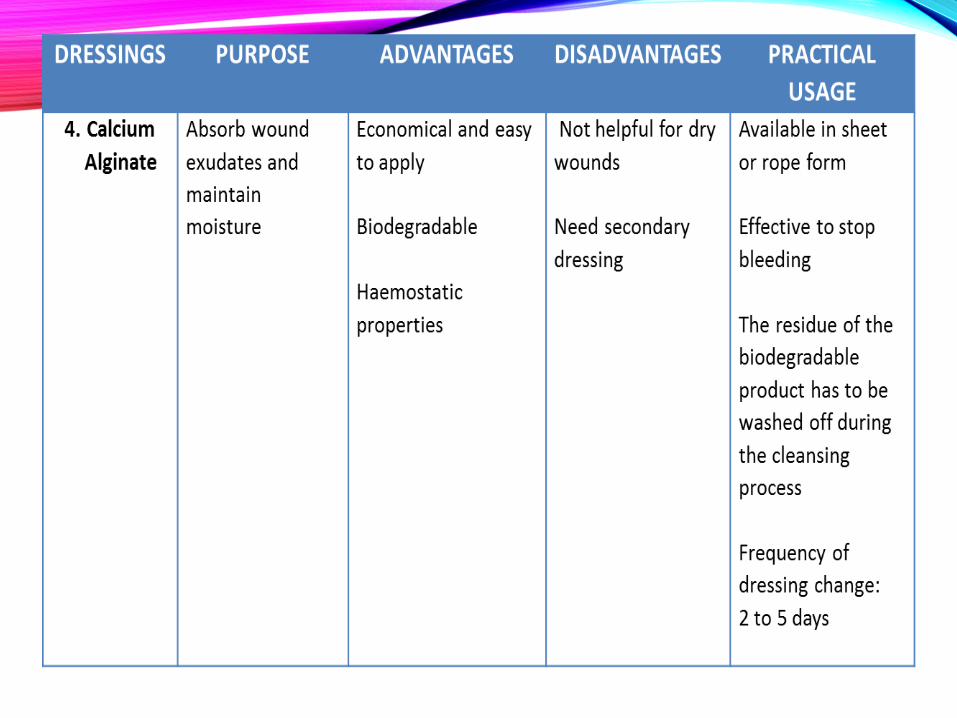
CALCIUM ALGINATE
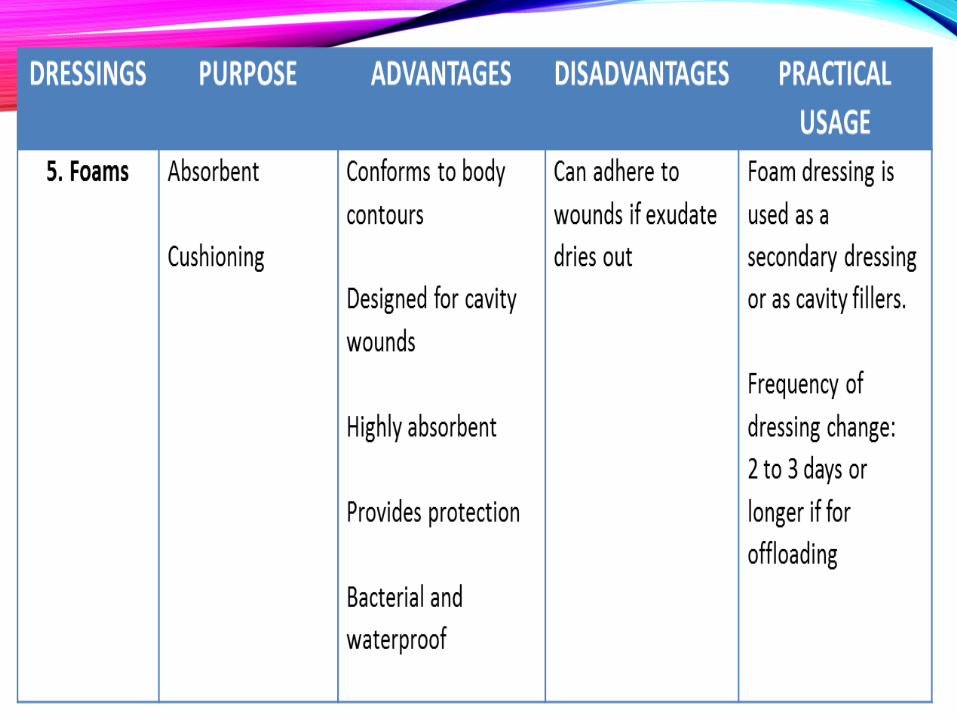

FOAM
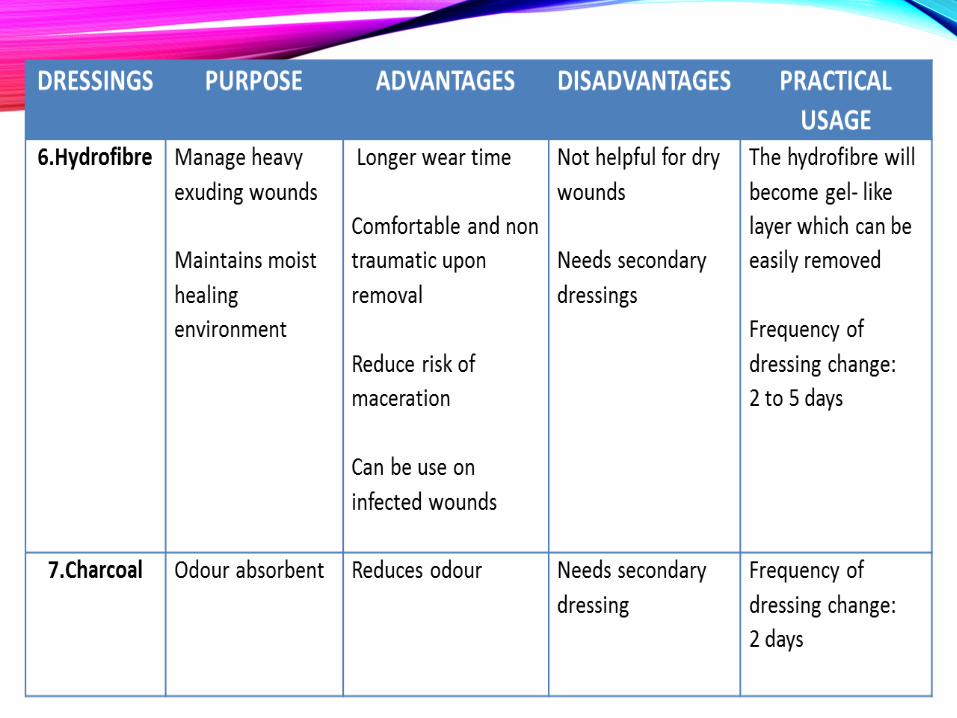
HYDROFIBER
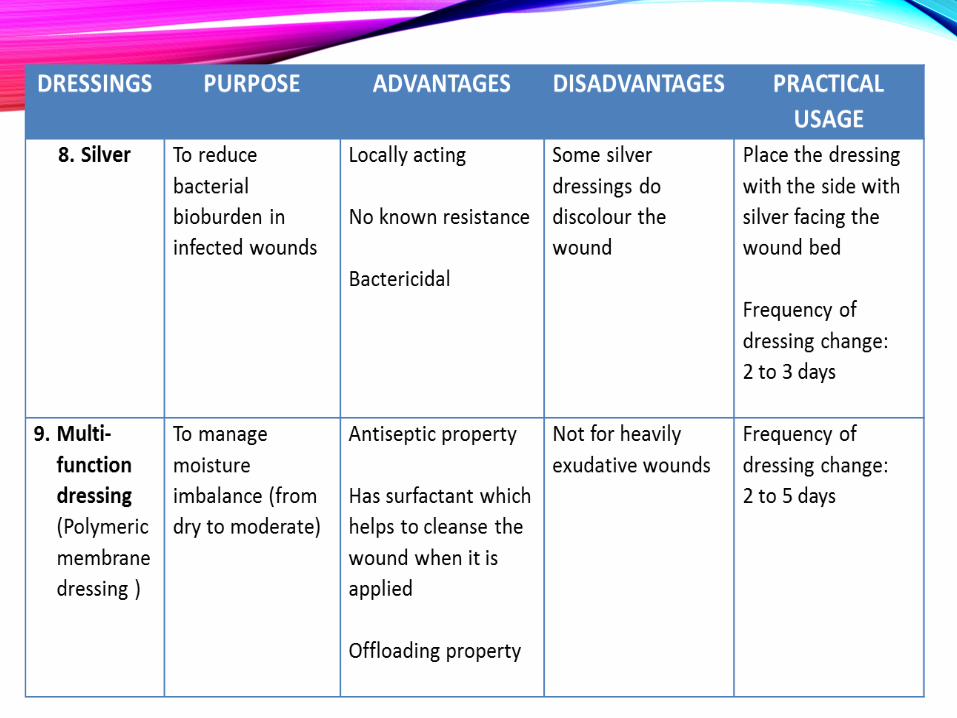
HYDROFIBER AG / SILVER
• People are often unreasonable and self-centered FORGIVE THEM ANYWAY..if you are kind, people may accuse you of ulterior motives..BE KIND ANYWAY…if you are honest, people may cheat you.. BE HONEST ANYWAY…if you find happiness, people may be jealous..BE HAPPY ANYWAY..the good you do today may be forgotten.. DO GOOD ANYWAY…give the world your best and it may never be enough…GIVE YOUR BEST ANYWAY…for you see, in the end it is between YOU AND GOD…it was never between you and them anyway…….
• Mother Teresa
‘WOUND HEALING WITH
PASSION’ -LEARN -HELP -HEAL

TERIMA KASIH